Transformation in mycosis fungoides: The role of methotrexate
8
Transformation in Mycosis Fungoides: The Role of Methotrexate Jasmin Abd-el-Baki, 1 Marie-France Demierre, 1 Ning Li, 2 and Francine 21/1. Foss3 Journal of Cutaneous Medicine and Surgery incorporating Medicoland 5urgketDermatology DOE 10.1007/s10227-00]-0040-y J Cutan Med Surg 2002; 109-116 Abstract Background: Large cell transformation in patients with mycosis fungoides (MF) has been well reported in the literature. Although the risk factors have not been clearly elucidated, advanced stage seems to be associated with a higher incidence of transfor- marion. Because MF is a rare disorder, little is known about the influence of other factors such as immunosuppressive therapy in the occurrence of transformation. Objective: We questioned the role of methotrexate (MTX) in the transformation of MF to large cell lymphoma (LCL). Methods: We identified all patients with MF who were registered in our cutaneous lymphoma database. Transformation was defined by the presence of large cells exceeding 25% of the infiltrate in at least one skin biopsy. In one patient, we followed the histo- logic, immunophenotypic, and genotypic changes taking place as transformation oc- curred. Results: A total of 134 patients with MF were identified. Of 21 patients who received MTX, 3 transformed, and of the 113 patients in the non-MTX group, only 2 trans- formed. The incidence of transformation in the patients who received MTX was sig- nificantly higher than in those who did not receive the drug (14.3% vs. 1.8%; p = 0.03). This significance was maintained, even after controlling for stage and sex. For one patient who transformed, we demonstrated an identical dominant T-cell clone in all skin specimens, including the large cell lymphoma. Conclusion: Our results demonstrate a significant association between MTX exposure and transformation to LCL in patients with MF. In light of the small sample size, short followup of patients, and the inherent tendency of mycosis fungoides to transform, the role for MTX in transformation is unproven and needs to be confirmed in a multicenter study. Sommaire Ante'ce'dents: Les publications sptcialis~es ont bien document6 les cas de transfor- mations cellulaires chez les patients atteints de mycosis fungoide. Bien que les facteurs de risques n'aient pas 4t6 enri~rement dlucid4s, le stade avanc6 de MF semble assocti8 h une plus forte incidence de transformations cellulaires. Puisque le mycosis fungoide est une maladie rare, l'influence d'autres facteurs, tels que la thtrapie immunosuppressive, sur 1'incidence de la transformation cellulaire reste peu connue. 1Department of Dermatology, Boston University School of Medicine, Boston, Massachusetts, USA ZDepartment of Dermatopathology, Boston University School of Medicine, Boston, Massachusetts, USA 3Department of Medicine, Division of Hematology/Oncology, Tufts University School of Medicine, Boston, Massachusetts, USA Online publication: 14 February 2002 Presented in part at the Annual Meeting of the American Academy of Dermatology, New Orleans, LA, March 22, 1999, Poster Presentation and presentation at the Residents/Fellows Symposium. Correspondence to: Marie-France Demierre, MD, FRCPC, 720 Harrison Avenue, D.O.B. 801A, Boston, MA 02118, USA. E-mail: marie [email protected] 109
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Transformation in mycosis fungoides: The role of methotrexate

Transformation in Mycosis Fungoides: The Role of
Methotrexate
Jasmin Abd-el-Baki, 1 Marie-France Demierre, 1 Ning Li, 2 and Francine 21/1. Foss 3
Journal of Cutaneous Medicine
and Surgery incorporating Medicol and 5urgket Dermatology
DOE 10.1007/s10227-00]-0040-y J Cutan Med Surg 2002; 109-116
Abstract
Background: Large cell transformation in patients with mycosis fungoides (MF) has been well reported in the literature. Although the risk factors have not been clearly elucidated, advanced stage seems to be associated with a higher incidence of transfor- marion. Because MF is a rare disorder, little is known about the influence of other factors such as immunosuppressive therapy in the occurrence of transformation.
Objective: We questioned the role of methotrexate (MTX) in the transformation of MF to large cell lymphoma (LCL).
Methods: We identified all patients with MF who were registered in our cutaneous lymphoma database. Transformation was defined by the presence of large cells exceeding 25% of the infiltrate in at least one skin biopsy. In one patient, we followed the histo- logic, immunophenotypic, and genotypic changes taking place as transformation oc- curred.
Results: A total of 134 patients with MF were identified. Of 21 patients who received MTX, 3 transformed, and of the 113 patients in the non-MTX group, only 2 trans- formed. The incidence of transformation in the patients who received MTX was sig- nificantly higher than in those who did not receive the drug (14.3% vs. 1.8%; p = 0.03). This significance was maintained, even after controlling for stage and sex. For one patient who transformed, we demonstrated an identical dominant T-cell clone in all skin specimens, including the large cell lymphoma.
Conclusion: Our results demonstrate a significant association between MTX exposure and transformation to LCL in patients with MF. In light of the small sample size, short followup of patients, and the inherent tendency of mycosis fungoides to transform, the role for MTX in transformation is unproven and needs to be confirmed in a multicenter study.
Sommaire
Ante'ce'dents: Les publications sptcialis~es ont bien document6 les cas de transfor- mations cellulaires chez les patients atteints de mycosis fungoide. Bien que les facteurs de risques n'aient pas 4t6 enri~rement dlucid4s, le stade avanc6 de MF semble assocti8 h une plus forte incidence de transformations cellulaires. Puisque le mycosis fungoide est une maladie rare, l'influence d'autres facteurs, tels que la thtrapie immunosuppressive, sur 1'incidence de la transformation cellulaire reste peu connue.
1Department of Dermatology, Boston University School of Medicine, Boston, Massachusetts, USA ZDepartment of Dermatopathology, Boston University School of Medicine, Boston, Massachusetts, USA 3Department of Medicine, Division of Hematology/Oncology, Tufts University School of Medicine, Boston, Massachusetts, USA Online publication: 14 February 2002 Presented in part at the Annual Meeting of the American Academy of Dermatology, New Orleans, LA, March 22, 1999, Poster Presentation and presentation at the Residents/Fellows Symposium. Correspondence to: Marie-France Demierre, MD, FRCPC, 720 Harrison Avenue, D.O.B. 801A, Boston, MA 02118, USA. E-mail: marie [email protected]
109

] 1 0 Journal of Cutaneous Medicine and Surgery Volume 6 Number 2 March 2002
Objectif'. Explorer le rtle du MTX dans la transformation des MF en lymphomes grandes cellules.
Mdthodes: Nous avons identifi6 tousles patients atteints de MF qui sont enregistrts dans notre base de donntes des lymphomes cutan&. Nous avons d6fini comme trans- formation les cas o~a la taille des grandes cellules dtpasse de 25% celle de l'infiltrat dans au moins une biopsie cutante. Nous avons suivi, chez un patient, les changements his- tologiques, immunophtnotypiques et gtnotypiques qui ont lieu durant la transformation cellulaire.
Re'sultats: Nous avons identifi4 un total de 134 patients atteints de MF. I1 y a eu transformation chez 3 des 21 patients recevant le MTX, alors que chez les 113 patients qui ne reqoivent pas le MTX, il y a eu transformation chez 2 seulement. L'incidence de transformations cellulaires chez les patients recevant le MTX 6tait consid~rablement sup~rieure fi celle des patients qui ne le reqoivent pas (14,3% contre 1,8%; p = 0,03). Cette diff6rence considerable s'est maintenue m~me apr~s avoir class4 les cas par stades de la maladie et sexe des patients. Chez Pun des patients qui a eu une transformation cellulaire, nous avons trouv6 un clone de cellule T dominante dans tous les 6chantillons cutan&, dont le lymphome ~ grandes cellules.
Conclusion: Nos r&ultats font 6tat d'une importante association entre l'exposition au MTX et ta transformation en lymphomes ~ grandes cellules chez les patients atteints de mycosis fungo. Vu la petite taille de l'4chantillon, le suivi de courte dur4e des patients et la tendance naturelle du mycosis fungo ?a se transformer, le r61e du MTX dans la transformation cellulaire n'est pas prouv~ et doit &re confirm6 par des 6tudes multi- centriques.
M Ycosis fungoides (MF) is histologically character- ized by an epidermotropic infiltrate of small
atypical lymphocytes and clinically by an indolent course. 1 However, MF can progress to a large-cell ma- lignant lymphoma which is histologically accompanied by a morphologic change (transformation) from the small cerebriform cell to a large-cell variant. Transformation is associated with a more aggressive biologic behavior leading to death within months. 2 It has been reported to occur in 8%-55% of MF patients and is associated with the appearance of nodules and tumors. 3'4 Although the risk factors associated with transformation have not been clearly elucidated, persistence of the same malignant T- cell clone has been documented in a number of cases indicating that the transformed cells have evolved from the original malignant cloned, s
Low-dose methotrexate (MTX) has been shown to be of value in the treatment of patients with erythrodermic MF. 6 Despite its weak oncogenic and immunosuppres- sive potential, several cases of lymphoproliferative dis- eases (LPD) have been reported in patients on low-dose MTX. To date, the majority of documented patients had rheumatoid arthritis (RA). 7'8 Many investigators, how- ever, believe that patients with RA have an increased risk of lymphoma, especially when complicated by Sj6gren's syndrome, Felty's syndrome, or immunosuppressive therapy. 9-13 These MTX-associated LPDs were charac- terized by extra nodal presentation, diffuse large cell histology, B-cell phenotype, association with Epstein- Barr virus (EBV), and partial or complete regres- sion of tumors after cessation of immunosuppressive therapy, t4,15
In light of the above observations, we addressed the possible role of MTX in transformation, keeping in mind that patients with MF have an inherent risk of developing secondary large-cell lymphoma (LCL). We reviewed the clinical course of 134 MF patients, with particular at- tention to those who had transformed and those who had received MTX.
For one patient, we also demonstrate the persistence of a dominant T-cell clone in multiple skin biopsies obtained from her progressing MF lesions as well as from the LCL that she developed. Clonal studies were not performed on the other patients.
Methods
We reviewed the clinical and histologic data on patients with MF who were registered in our cutaneous lym- phoma database between 1989 and 1999. All patients had a clinical diagnosis compatible with MF, and the patho- logic diagnosis was confirmed according to previously described criteria. 16 Staging criteria were used according to the Mycosis Fungoides Cooperative Group. 17 Patients had repeat skin biopsies performed at the onset of new tumors or at the time of clinical relapse or persistent disease while on therapy. If adenopathy developed during the course of followup, a fine-needle aspirate or biopsy was performed. In accordance with previously defined criteria, cases of MF were classified as having large-cell transformation if at least one biopsy showed large cells exceeding 25% of the infiltrate. ' In patient 2, a fine- needle aspirate from the tumor revealed the presence of

j . Abd-el-Baki et al. Tran~Cormation in Mycosis Fungoides 111
O 0 0
r . J 3 ~ r . 1 3
c~ 00 O 0~
03 03
4.o
~ . o o ' ~
~ " ~ . ~ ~:~r~ ~ ,.l~
~ -,~ ~ ~--~ o
-~ ~ ~ = = ..~ ~ - ~ ~
large anaplastic CD4+ CD7- lymphocytes. We did not quanti~ those cells; however, we assumed that the large cells occupied more than 25% of the infiltrate.
Patient 1 A total of 6 skin biopsy specimens obtained from patient 1, before and after the administration of MTX, were routinely processed for light microscopy. Portions of these specimens were snap frozen. Cryostat and paraffin sections were processed for immunophenotypic analysis as described previously. 19 The panel of monoclonal an- tibodies employed included the following: anti-CD2, anti-CD4, anti-CDS, anti-CD8, and anti-CD20, anti- CD22, anti-CD30, anti-CD43, and anti-CD45RO. 2~
Polymerase chain reaction (PCR) amplification of T- cell receptor gamma (TCRy) chains and denaturing gradient gel ectrophoresis (DGGE) was performed on all 6 specimens as follows: Fifteen to twenty 5-~m sections of tissue fixed in 10% neutral buffered formalin and embedded in paraffin were cut on a clean microtome and placed in a microcentrifuge tube. The tissue samples were deparaffinized for 30 minutes in xylene and pelleted in an ultracentrifuge. Deparaffinization was repeated and the pellet was washed with 100% ethanol. The tissue was digested overnight with proteinase K (Qiagen), extracted with a standard Qiamp tissue protocol (Qiagen), and the DNA was eluted in 400 pL of distilled water. DNA samples were concentrated to obtain a final volume of 100 ,L.
PCR for the TCR~ gene rearrangement was per- formed as previously describedfl 1'z2 Briefly, 10 ~L of genomic DNA was amplified using 40 pmol of nested oligonucleotide primers specific for T C R gene sequences V71-8. PCR reaction buffer composition and PCR con- dition were used as described previously, with 25 cycles of first-round "outer" PCR and 15 cycles of the second- round "inner" primer PCR. Appropriate controls, in- cluding a negative carryover control without target DNA, were used. One hundred microliters of PCR products were precipitated with one-tenth volume 3M NaOAc and two volumes of cold 100% ethanol at -70~ overnight. Samples were denatured by heating to 94~ for 5 min and incubated at 60~ for 1 h prior to loading on a parallel DGGE apparatus (CBS Scientific, Del Mar, CA). Samples were electrophoresed for 6 h on a 6.5% poly- acrylamide gel containing a continuous gradient (30%- 60%) of urea and formamide at 60~ Gels were removed and stained with ethidium bromide (1 gg/mL) and pho- tographed under UV light. Matching band positions in the different lanes of the same denaturing gradient gel were considered the same dominant TCRy gene rear- rangement in the respective lanes. 22'23
Data Analysis Statistical analysis was performed using SPSS Software version 8.0 for Microsoft Windows. The association of transformation with characteristics such as stage of the

112 Journal of Cutaneous Medicine and Surgo 7 Volume 6 Number 2 March 2002
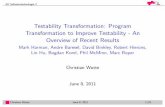
FIGURE 1 Specimen 1 obtained from a plaque from patient 1, before the intake of MTX showing (A) a lymphocytic infiltrate consisting predominantly of small atypical cerebriform cells, (B) strong expression of CD45RO antigen on the surface of the small lymphocytes.
TABLE II Characteristics of patients with and without
eventual transformation
Transformed patients
Characteristic No. of patients N % p value a
S e x
Male 69 4 5.8 Female 65 1 1.5 0.20
Stage at referral I-II A versus 93 3 3.2 IIB-1V 41 2 4.9 0.49 I versus 86 3 3.5 II-IV 48 2 4.2 0.59
MTX intake Yes 21 3 14.3 No 113 2 1.8 0.03
a By Fischer exact test.
disease at referral, sex, and previous M T X intake was assessed by Fisher exact test. 24 T o further elucidate the role of M T X in transformation, multivariate logistic re- gression analysis was conducted with transformation as the dependent variable and age, sex, and M T X intake as independent variables.
Survival was calculated from the time of the first bi- opsy that established transformation to the date of death or last followup evaluation.
Results
One hundred thirty-four patients with MF were seen at the Boston Medical Center during the study period. One hundred seven patients out of 134 were followed up for more than 2 years. A total of 5 patients, 4 men and 1 woman, demonstrated transformation to LCL (3.7%) (Table I). Of 21 patients who received MTX, 3 trans- formed, and of the 113 patients who never received MTX, only 2 transformed. The incident of transforma- tion to secondary cutaneous LCL was significantly higher in the M T X group (14% vs. 1.8%; p = 0.03; Table II).
Controlling for stage of disease at referral and sex, mul- tivariate analysis revealed that transformation in patients who received M T X was significantly higher than in those who did not receive M T X (OR = 19.5; 95% CI = 2.4- 161, p = 0.0059). The mean age at transformation and mean time to transformation in the M T X group was 70.3 years and 98 months versus 47 years and 108 months in the non-MTX group, respectively. The mean survival after transformation was shorter in the M T X group (8.7 months versus 24 months in the non-MTX group).
There was no difference in the sex distribution be- tween patients with and without eventual transformation (Table II). The i r mean age at transformation was 61 years (range = 19-87 years; median = 52 years). The mean time to transformation was 102 months (range = 18-216 months; median = 60 months), and the mean survival was 14.8 months (range = 3-60 months; median = 3 months). Only one patient transformed within less than two years of the diagnosis of MF. The remaining 4 transformed more than three years after MF was diagnosed. Four of the 5 patients who transformed had stage l ib disease or higher at the time of transformation. However, at refer- ral, 2 patients had stage IIB-III and higher and 3 pre- sented with stage IB. With regard to the site of transformation, tumors presented initially in the skin in 4 cases and in a lymph node in one case (Table I). Patients with eventual transformation were more likely to have stage IIB-IV disease at referral than stages I-IIA (p = 0.49; Table I1). Transformation was not seen in patients who presented with stage IA disease.
All three patients who transformed in the M T X group died: Patient 1 declined further therapy after transfor- mation and died of progressive cutaneous disease; patient 2 died from acute myelogenous leukemia; patient 3 de- veloped multiple ulcerated tumors on the scalp and died after an unprecedented loss of consciousness. No post- mortem studies were performed to assess for the presence of extracutaneous LCL in these patients. In the non- M T X group, only one patient died after developing nodal L C L and progressive cutaneous disease unresponsive to chemotherapy (Table I).

.7. Abd-el-Baki et al. Transformation in Mycosis Fungoides 113
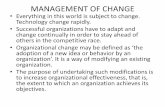
FIGURE 2 (A) New tumors on the thigh of patient 1 that appeared 10 months after the intake ofMTX. (B) Specimen 6 obtained from one of the new tumors showing cohesive sheets of large tumor cells. (C) These large tumor cells possessed prominent nuclei and abundant cytoplasm. (D) Strong expression of CD30 antigen on the surface of the large lymphocytes.
Patient 1 Table III summarizes the immunophenotypic and T-cell gene rearrangement findings in patient 1. Prior to the administration of MTX, the lymphocytic infiltrate was composed of small atypical hyperchromatic lymphocytes (Fig. 1A) staining positively with pan T-cell markers, in- cluding CD45RO (Fig. IB), but negative for CD30 and pan B-cell marker CD20. Ten months after the start of MTX, a biopsy (specimen 6) was obtained from a new tumor on the thigh (Fig. 2A). This time, the infiltrate comprised sheers of atypical lymphocytes, with large nu- clei and abundant cytoplasm (Fig. 2B, C). These enlarged lymphocytes were strongly positive with CD30 (Fig. 2D) but had lost expression of CD45RO, CD3, and CD43.
P C R / D G G E analysis of genomic DNA showed the presence of a dominant band for T C R 71-8 in each of the 6 tissue specimens (Table III). All 6 dominant bands oc- cupied matching positions on the gel, indicating a com- mon clonal origin of MF and LCL in patient 1 (Fig. 3).
Discussion
Cytological transformation in M F is associated with a poor prognosis and a markedly short survival, particularly with extracutaneous and systemic involvement. 3'25 In a recent series of 115 M F patients, the median time from diagnosis to transformation was less than 12 months (range = 1-128 months) and the median survival was 19.4 months (range = 2-138 months), e6 The incidence of transformation in that series was 22.6%. 26 Tumor stage disease and onset of transformation less than 2 years from diagnosis of M F were identified as adverse prognostic factors. 26
Our data demonstrate an incidence of transformation lower than that reported in the literature (3.7%). This finding could be explained by the fact that 27 patients were followed for a period of less than 2 years. The in- cidence of transformation in M F patients who received M T X was significantly higher than in those who did not, and this significance was maintained even after control-

114 y o u r ~ of Cutaneous Medicine and Surgery Volume 6 Number 2 March 2002
TABLE III Immunophenotypic and T-cell gene rearrangement in tissue specimens obtained from patient 1
Specimen number: Date Specimen: Lesion type lmmunophenotype V 7 (1) 08/20/96 MF-Tumor (2) 08/20/26 MF-Plaque (3) 09/10/96 MF-Plaque (4) 05/22/97 MF-Tumor
MTX (5) 10/03/97 MF-Plaque (6) 02/11/98 LCL-Tumor
CD45RO+, CD20-, CD30- V71-8 CD45RO+, CD20-, CD30- V71-8 CD2+, CD4+, CD5+, CD45RO+, CD8-, CD22-, CD30- V71-8 CD45RO+, CD20-, CD30- V71-8
CD45RO+, CD20-, CD30- CD45RO+ (weak), CD30+, CD20-
V71-8 V71-8
FIGURE 3 MF and LCL in patient 1 exhibit an identical TCRy gene rearrangement pattern. Ethidium bromide-stained dena- turing gradient gel showing results of PCR/DGGE analysis using primers for V71-8 and J71-8. Lanes 1-5 represent DNA obtained from specimens 1-5. Lane 6 represents DNA obtained from specimen 6.
TABLE IV
Stratification by stage of patients who received MTX
Stage at referral N No. of patients who received M T X
IA 45 4 IB 41 3 lEA 7 2 liB 8 3 III 24 7 IVA 6 2 IVB 3 0
ling for stage. Patients with advanced stages (II-IV) were more likely to receive MTX than patients with stage I disease (Table IV). However, transformation was docu- mented in one patient with stage IB disease (patient 5) who had not received MTX, emphasizing the inherent predisposition of the disease to undergo transformation. Because survival of patients with MF worsens with in- creasing skin stage, and the lack of response to initial treatment is predictive of disease progression, 27-29 a role for MTX in transformation is unproven and needs to be confirmed, preferably in a multicenter setting.
We also demonstrated that histologic transformation is associated not only with the appearance of CD30 on the surface of the enlarged lymphocytes but also with the loss of several pan T-cell markers such as CD3, CD43, and CD45RO. These results are similar to those of Wood et al., 4 who reported weak CD45RO expression in a case of L C L arising from MF, in contrast to the strong, bright CD45RO expression typical of patch/plaque MF. Despite immunohistochemical and morphologic trans- formation to L C L in this patient, we documented per- sistence of a T-cell clone, suggesting clonal evolution, as previously described. 5'3~
While the etiology of LPD arising in patients with rheumatologic disorders in the setting of M T X therapy is unclear, the spontaneous disappearance of lymphoma in these same patients after the withdrawal of M T X sug- gests that therapy was the most important factor in lymphoma generation.14'32 In this context, it is important to analyze the role of dosage and duration of MTX administration and how it relates to the onset of secondary LPD. In our 3 patients who transformed, MTX was administered for a minimum of 8 months; however, our database lacked information on dosage and duration in patients who received MTX but did not transform.
In vitro studies on peripheral mononuclear cells of patients with RA showed that M T X increased gene ex- pression of Th2 c~33okines and decreased gene expression of Thl cytokines. In MF, tumor-infiltrating lympho- cytes, present in early patch/plaque lesions, produce Thl cytokines (IL-2 and IFN-7), while in more advanced disease, Th2 cytokines, (IL-4 and IL-10) produced by the malignant lymphocytes, predominate. 34 The immuno-

J. Abd-el-Baki et aL TransCormation ira Mycosis Fungoides 115
modu la to ry effects o f M T X on the T h - 1 and T h - 2 sub- sets o f pe r iphera l lymphocytes could be faci l i ta t ing an ongoing process o f clonal select ion in M F pat ients . In contrast , studies o f pat ients wi th psoriasis and t r o p h o b - lastic tumors receiving M T X demons t r a t ed no increase in the inc idence o f L P D when c o m p a r e d wi th cont ro l s who had no t received M T X , 35-37 suggest ing that p red i spos ing
condit ion, such as a c o m p r o m i s e d i m m u n e status sec- ondary to the p r imary disease or to previous t rea tments , may be more re levant to the process o f t ransformat ion . T o date, no publ i shed series had ques t ioned the possible role o f immunosuppres s ive the rapy on t rans format ion in patients with M F . gVe had specula ted that the addit ive immunosuppress ive effect of chron ic low-dose M T X might pe rmi t a rapid clonal evolut ion o f ma l ignan t T - cells to a more aggressive pheno type in selected pat ients with M F . W h i l e our results appeared to be significant, four o f the pat ients who unde rwen t t r ans fo rmat ion had received mul t ip le therapies before M T X , inc luding mul t iagent c h e m o t h e r a p y and rad ia t ion therapy, m o d a l - ities that can con t r ibu te to i m m u n o s u p p r e s s i o n and sec- ondary mye lopro l i f e ra t ive / lymphopro l i f e ra t ive disease. Given the small n u m b e r o f pat ients in our study, un- known cumulat ive M T X dose received by each pat ient , radiat ion or c h e m o t h e r a p y as possible confound ing ele- ments, and shor t fol lowup, a mul t i cen te r s tudy would need to be pe r fo rmed to fur ther evaluate our hypothesis . In the absence of suppor t ing data, i.e., a large mul t i cen te r study, me tho t rexa te remains an i m p o r t a n t the rapy in the managemen t o f pat ients wi th M F .
Acknowledgment We are indebted to Abla M. Sibai, Ph.D., for her help with the statistical analysis.
References 1. Edelson RL. Cutaneous T-cell lymphoma. J Dermatol Surg Oncol
1980; 6:358-368. 2. Dmitrovsky E, Matthews MJ, Bunn PA, et al. Cytologic transfor-
mation in cutaneous T-cell lymphoma: A clinicpathologic entity associated with poor prognosis. J Clin Oncol 1987; 5:208-215.
3. Cerroni L, Rieger E, Hodl S, et al. Clinicopathologic and immu- nologic features associated with transformation of mycosis fungo- ides to large-cell lymphoma. Am J Surg Pathol 1992; 16:543-552.
4. Vonderheid EC, Tam DW, Johnson Vr et al. Prognostic sig- nificance of cytomorphology in the cutaneous T-cell l)maphomas. Cancer 1981; 47:119-125.
5. Wood GS, Bahler DW, Hoppe RT, et al. Transformation of mycosis fungoides: T-cell receptor 13 gene analysis demonstrates a common clonal origin for plaque-type mycosis fungoides and CD 30+ large-cell lymphoma. J Invest Dermatol 1993; 101: 296-300.
6. Zackheim HS, Kashani-Sahet M, Hwang ST. Low-dose methot- rexate to treat elTthrodermic cutaneous T-cell lymphoma: Results in twenty-nine patients. J Am Acad Dermatol 1996; 34:626-631.
7. Bachman TR, Sawitzke AD, Perkins SL, et al. Methotrexate- associated lymphoma in patients with rheumatoid arthritis: Report of two cases. Arthritis Rheum 1996; 39:325-329.
8. Kingsmore SF, Hall BD, Alien NB, et al. Association of methot- rexate, rheumatoid arthritis and lymphoma: report of 2 cases and literature review. J Rheumatol 1992;19:1462-1465.
9. Castor CW, Bull FE. Review of United States data on neoplasms in rheumatoid arthritis. AmJ Med 1985; 78(Suppl 1A):33-38.
10. Porter P, Madhok R, Capell H. Non-Hodgkin's lymphoma in rheumatoid arthritis. Ann Rheum Dis 1991; 50:275-276.
11. Gridley G, Klippel J, Hoover R, et al. Incidence of cancer among men with the Felty syndrome. Ann Intern Med 1994; 120:35-39.
12. Symmons DPM. Neoplasms of the immune system in rheumatoid arthritis. Am J Med 1985; 78 (Suppl IA):22-28.
13. Kassan SS, Thomas TL, Moutsopoulos HNI, et al. Increased risk of lymphoma in sicca syndrome. Ann Intern Med 1978; 89:888- 892.
14. Kamel OW, van de Rijn M, Weiss LM, et al. Reversible lympho- mas associated with Epstein-Barr virus occurring during methot- rexate therapy for rheumatoid arthritis and dermatomyositis. N EnglJ Med 1993; 328:1317-1321.
15. Liote F, Pertuiset E, Cochand-Priollet B, et al. Methotrexate re- lated B lymphoproliferative disease in a patient with rheumatoid arthritis: Role of Epstein-Barr virus infection. J Rheumatol 1995; 22:1174-1178.
16. Rappaport H, Thomas LB: Mycosis fungoides: The pathology of extracutaneous involvement. Cancer 1974; 34:1198-1229.
17. Bunn PAJr, Lamberg SI. Report of the Committee on Staging and Classification of Cutaneous T-Cell Lymphomas. Cancer 1979; 63:725-728.
18. Salhany KE, Cousar JB, Greer JP, et al. Transformation of cuta- neous T-cell lymphoma to large-cell lymphoma: A clinicopatho- logic and immunologic study. AnlJ Pathol 1988; 132:265-277.
19. Wood GS, Warnke R. The immunophenotyping of bone marrow biopsies and aspirates: Frozen section techniques. Blood 1982; 59:913-922.
20. Kanavaros P, Jiva NM, de Bruin PC, et al. High incidence of EBV genome in CD-30 positive non-Hodgkin's lymphoma. J Pathol 1992; 168:307-315.
21. Wood GS, Tung RM, Haeffiler AC, et al. Detection of clonal T-cell receptor 3' gene rearrangements in early mycosis fungoides/ Sezary syndrome by polymerase chain reaction and denaturing gradient gel electrophoresis (PCR/DGGE). J Invest Dermatol 1994; 103:34M-1.
22. Anderson WIC Li N, Bhawan J. Polymerase chain reaction-dena- turing gradient gel electrophoresis (PCR/DGGE) based detection of clonal T-cell receptor 3' gene rearrangements on paraffin-em- bedded cutaneous biopsies in cutaneous T-cell lymphoproliferative disorders. J Cutan Pathol 1999; 26:176-182.
23. Wood GS, Grooks CF, Uluer AZ. Lymphomatoid papulosis and associated cutaneous lymphoproliferative disorders exhibit a com- mon clonal origin. J Invest Dermatol 1995; 105:51-55.
24. Kaplan EL, Meier P. Non-parametric estimation from incomplete observations. J Am Stat Assoc 1958; 53:457.
25. YVillemze R, Beljaards RC. Spectrum of primary cutaneous CD30 (Ki-1)-positive lymphoproliferative disorders: A proposal for clas- sification and guidelines for management and treatment. J Am Acad Dermatol 1993; 28:973-980.
26. Diamandidou E, Colome-Grimmer M, Fayad L, et al. Transfor- marion of mycosis fungoides/Sezary syndrome: Clinical charac- teristics and prognosis. Blood 1998; 92:1150-1159.
27. Zackheim HS, Amin S, Kashani-Sabet M, et al. Prognosis in cu- taneous T-cell lymphoma by skin stage: Long-term survival in 489 patients. J Am Acad Dermatol 1999; 40:418--425.
28. Kim YH, Jensen RA, Watanabe GL, et al. Clinical stage 1A (lim- ited patch and plaque) mycosis fungoides: A long-term outcmne analysis. Arch Dermatol 1996; 132:1309-1313.
29. Kim YH, Chow S, Varghese A, et al. Clinical characteristics and long-term outcome of patients with generalized patch and/or pla- que (T2) mycosis fungoides. Arch Derrnatol 1999; 135:26-32.
30. Volkenandt M, Bertino JR, Shenoy V, et al. Molecular evidence for a clonal relationship between lymphomatoid papulosis and Ki-1 positive large cell anaplastic lymphoma. J Dermatol Sci 1993; 6:121-126.
31. Amagai M, Kawakubo Y, Tsuynki A, et al. Lymphomatoid papu- losis followed by Ki-1 positive anaplastic large cell lymphoma: Proliferation of a common T-cell clone. J Dermatol 1995; 22:743- 746.
32. Viraben R, Brousse P, Lamant L. Reversible cutaneous lymphoma occurring during methotrexate therapy. Br J Dermatol 1996; 135:116-118.

"l "16 Journal of Cutaneous Medicine and Surgery Volume 6 Number 2 March 2002
33. Constantin A, Loubet-Lescoulie P, Lambert N, et al. Anti-inflam- matory and immunoregulatory action of methotrexate in the treat- ment of rheumatoid arthritis: Evidence of increased interleukin-4 and interleukin- 10 gene expression demonstrated in vitro by competitive reverse polymerase chain reaction. Arthritis Rheum 1998; 41:48-57.
34. Vowels BR, Lessin SR, Cassin M, et al. Th2 cytokine mRNA ex- pression in skin in cutaneous T-cell lymphoma. J Invest Dermatol 1994; 103:619~573.
35. Stern RS, Zierler S, Parrish JA. Methotrexate used for psoriasis and the risk of noncutaneous or cutaneous malignancy. Cancer 1982; 50:869-872.
36. Bailin PL, Tindall JP, Roenigk HH, et al. Is methotrexate therapy for psoriasis carcinogenic? JAMA 1975; 232:359-362.
37. Rustin GJ, Rustin F, Rent J, et al. No increase in second tumors after cytotoxic chemotherapy for gestational trophoblastic tumors. N Engl J Med 1983; 308:473-476.