Periodo de adaptacion
10
Nitric Oxide Donor Improves Healing if Applied on Inflammatory and Proliferative Phase Thaís P. Amadeu, Ph.D.,* Amedea. B. Seabra, Ph.D.,† Marcelo G. de Oliveira, Ph.D.,† and Andréa Monte-Alto-Costa, Ph.D.* ,1 *Histology and Embryology Department, State University of Rio de Janeiro, Rio de Janeiro, Brazil; and †Chemistry Institute, State University of Campinas, UNICAMP, São Paulo, Brazil Submitted for publication June 27, 2007 Background. Nitric oxide (NO) is an important mol- ecule synthesized during wound repair. Studies have reported the use of NO donors on cutaneous wound repair, but their effects in different phases of healing are still not elucidated. The aim of this work was to investigate the effects of topical application of a NO donor (S-nitrosoglutathione, GSNO)-containing hy- drogel on excisional wounds in the inflammatory ( inf ), proliferative ( prol ), and inflammatory and proliferative phases ( infprol ) of rat cutaneous wound repair. Material and Methods. In each group (control, GSNO inf , GSNO prol , and GSNO infprol ), excisional wounds on the dorsal surface were made and wound contrac- tion and re-epithelialization were evaluated. Fourteen days after wounding, wounds and adjacent skin were formalin-fixed and paraffin-embedded. Collagen fibers organization, mast cells, myofibroblasts and vessels were evaluated. Results. Wound contraction of the GSNO infprol group was faster than control, GSNO inf , and GSNO prol groups, 5 and 7 d after wounding. Topical application of GSNO accelerated re-epithelialization 14 d after wounding, mainly in GSNO infprol group. In addition, the GSNO infprol group showed improved collagen fibers maturation and tissue organization, and lower amount of inflammatory cells in the superficial and deep areas of the granulation tissue, compared with the other groups. Conclusions. NO is important in all phases of rat cutaneous wound repair, but if applied on inflamma- tory and proliferative phases, the improvement in wound healing (accelerating wound closure, wound re-epithelialization, and granulation tissue organiza- tion) is more impressive. © 2008 Elsevier Inc. All rights reserved. Key Words: Nitric oxide; Pluronic F127 hydrogel; Re- epithelialization; S-nitrosoglutathione; Skin; Wound healing. INTRODUCTION Cutaneous wound healing is a dynamic and complex physiological process that represents a response to tis- sue damage. This process is subdivided into three com- plementary and overlapping phases: inflammation, granulation tissue formation (proliferative), and re- modeling [1]. Wound healing involves cytokines and growth factors, extracellular matrix components, and several cell types [1, 2]. For normal wound healing, all these phases and their behavior have to be strongly coordinated in a spatial and temporal manner [3]. The inflammatory phase initiates with a disruption of blood vessels and extravasation of blood constitu- ents, as well as with the production of provisional extracellular matrix [4]. At the same time, platelets release several vasoactive mediators and chemotactic factors, such as interleukin (IL), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), platelet-derived growth factor (PDGF), and transform- ing growth factor beta (TGF-), that recruit inflamma- tory cells such as neutrophils and macrophages and also fibroblasts and endothelial cells to the site of wound [1, 5, 6]. These stimuli lead to the next phase, granulation tissue formation, characterized by angio- genesis, myofibroblastic differentiation and fibroplasia [1, 4]. During this phase, many cells differentiate into myofibroblasts that synthesize extracellular matrix and generate mechanical force to allow wound closure [7]. Many events are crucial to promote re- 1 To whom correspondence and reprint requests should be ad- dressed at Histology and Embryology Department, State University of Rio de Janeiro (UERJ), Rua Professor Manuel de Abreu, 444, 3 0 andar, 20550-170, Rio de Janeiro, RJ, Brazil. E-mail: amacosta@ uerj.br Journal of Surgical Research 149, 84 –93 (2008) doi:10.1016/j.jss.2007.10.015 84 0022-4804/08 $34.00 © 2008 Elsevier Inc. All rights reserved.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Periodo de adaptacion
Journal of Surgical Research 149, 84–93 (2008)
Nitric Oxide Donor Improves Healing if Applied on Inflammatory andProliferative Phase
Thaís P. Amadeu, Ph.D.,* Amedea. B. Seabra, Ph.D.,† Marcelo G. de Oliveira, Ph.D.,† andAndréa Monte-Alto-Costa, Ph.D.*,1
*Histology and Embryology Department, State University of Rio de Janeiro, Rio de Janeiro, Brazil; and †Chemistry Institute, StateUniversity of Campinas, UNICAMP, São Paulo, Brazil
Submitted for publication June 27, 2007
doi:10.1016/j.jss.2007.10.015
Background. Nitric oxide (NO) is an important mol-ecule synthesized during wound repair. Studies havereported the use of NO donors on cutaneous woundrepair, but their effects in different phases of healingare still not elucidated. The aim of this work was toinvestigate the effects of topical application of a NOdonor (S-nitrosoglutathione, GSNO)-containing hy-drogel on excisional wounds in the inflammatory (inf ),proliferative (prol ), and inflammatory and proliferativephases (inf�prol ) of rat cutaneous wound repair.
Material and Methods. In each group (control,GSNOinf , GSNO prol , and GSNO inf�prol ), excisional woundson the dorsal surface were made and wound contrac-tion and re-epithelialization were evaluated. Fourteendays after wounding, wounds and adjacent skin wereformalin-fixed and paraffin-embedded. Collagen fibersorganization, mast cells, myofibroblasts and vesselswere evaluated.
Results. Wound contraction of the GSNOinf�prol groupwas faster than control, GSNOinf , and GSNO prol groups,5 and 7 d after wounding. Topical application of GSNOaccelerated re-epithelialization 14 d after wounding,mainly in GSNOinf�prol group. In addition, theGSNOinf�prol group showed improved collagen fibersmaturation and tissue organization, and loweramount of inflammatory cells in the superficial anddeep areas of the granulation tissue, compared withthe other groups.
Conclusions. NO is important in all phases of ratcutaneous wound repair, but if applied on inflamma-tory and proliferative phases, the improvement inwound healing (accelerating wound closure, wound
1 To whom correspondence and reprint requests should be ad-dressed at Histology and Embryology Department, State Universityof Rio de Janeiro (UERJ), Rua Professor Manuel de Abreu, 444,30 andar, 20550-170, Rio de Janeiro, RJ, Brazil. E-mail: amacosta@
uerj.br840022-4804/08 $34.00© 2008 Elsevier Inc. All rights reserved.
re-epithelialization, and granulation tissue organiza-tion) is more impressive. © 2008 Elsevier Inc. All rights reserved.
Key Words: Nitric oxide; Pluronic F127 hydrogel; Re-epithelialization; S-nitrosoglutathione; Skin; Woundhealing.
INTRODUCTION
Cutaneous wound healing is a dynamic and complexphysiological process that represents a response to tis-sue damage. This process is subdivided into three com-plementary and overlapping phases: inflammation,granulation tissue formation (proliferative), and re-modeling [1]. Wound healing involves cytokines andgrowth factors, extracellular matrix components, andseveral cell types [1, 2]. For normal wound healing, allthese phases and their behavior have to be stronglycoordinated in a spatial and temporal manner [3].
The inflammatory phase initiates with a disruptionof blood vessels and extravasation of blood constitu-ents, as well as with the production of provisionalextracellular matrix [4]. At the same time, plateletsrelease several vasoactive mediators and chemotacticfactors, such as interleukin (IL), vascular endothelialgrowth factor (VEGF), epidermal growth factor (EGF),platelet-derived growth factor (PDGF), and transform-ing growth factor beta (TGF-�), that recruit inflamma-tory cells such as neutrophils and macrophages andalso fibroblasts and endothelial cells to the site ofwound [1, 5, 6]. These stimuli lead to the next phase,granulation tissue formation, characterized by angio-genesis, myofibroblastic differentiation and fibroplasia[1, 4]. During this phase, many cells differentiate intomyofibroblasts that synthesize extracellular matrixand generate mechanical force to allow wound closure
[7]. Many events are crucial to promote re-
85AMADEU ET AL.: GSNO ON INFLAMMATORY AND PROLIFERATIVE PHASE
epithelialization, which occurs by proliferation and mi-gration of epithelial cells from the edge of the tissueacross the site of wound [8]. When this process occursrapidly, the restoration of skin functions are quickerand, consequently, a reduction of patient morbidityand mortality is observed. After complete re-epithelialization, the remodeling phase begins. Thisphase is characterized by the replacement of granula-tion tissue by a scar tissue, mainly by the activation ofmatrix metalloproteinases (MMPs) that degrade theextracellular matrix components [9].
Nitric oxide (NO) is synthesized by three isoforms ofnitric oxide synthase (NOS) [neuronal (nNOS), induc-ible (iNOS), and endothelial (eNOS)] from its sub-strate, L-arginine [10, 11]. NO plays many physiologi-cal functions such as vasodilatation, inhibition ofplatelet aggregation, and reduction of leukocyte-endothelial cell adhesion. Since NO is one of the mol-ecules present in the wound environment [12], its rolein cutaneous wound healing has been the focus of greatattention [13–17].
NO has been implicated as a regulator of all phasesof wound healing. Studies demonstrated the ability ofNO to modulate chemoattractant cytokines, such asIL-1, IL-6, IL-8, and TGF-�1, and to control collagendeposition, angiogenesis, cellular proliferation, and ap-optosis [17, 18].
Experimental studies reported beneficial effects of adiet rich in L-arginine on the healing and survival ofinjured rats [19–21]. Inhibitors of NOSs have beenreported to delay wound healing [14, 19, 20] and theadministration of NO donors or transfection of a woundwith the gene for iNOS have beneficial effects onwound repair [13, 15, 22–25]. Although the effects ofNO in wound healing have already been described, theeffects and the importance of NO in different phases ofcutaneous wound healing are still not completely elu-cidated.
S-nitrosoglutathione (GSNO) is a S-nitrosothiol en-dogenously found in mammals, which is known to actas a NO carrier and donor [26]. GSNO-containing plu-ronic F-127 hydrogel was already applied on the fore-arm skin of healthy human volunteers and led to anincrease in the local blood flow [27]. Recently, ourgroup reported an improvement of cutaneous woundhealing (acceleration of wound contraction, re-epithelialization, and granulation tissue organization)by topical administration of GSNO-containing hydro-gel during the first 5 d of wounding [15].
Considering that the importance of NO in each phaseof wound healing is unknown, although some studiessuggest that the main activity of NO is during inflam-matory phase [28], the purpose of this study was toinvestigate the effects of topical application of GSNO-
containing hydrogel in different phases of rat exci-sional cutaneous wound healing (inflammatory or pro-liferative or inflammatory and proliferative phases).
MATERIALS AND METHODS
Pluronic F-127 (poly(ethylene oxide)99-poly(propylene oxide)65-poly(ethylene oxide)99, PEO99-PPO65-PEO99, MW � 12,0000; ICICorp., Bridgewater, NJ), glutathione (�-Glu-Cys-Glu, GSH) (Sigma,St. Louis, MO), sodium nitrite (NaNO2) (Aldrich, St. Louis, MO) wereused as received. All of the experiments were carried out usinganalytical grade water from a Millipore Milli-Q gradient filtrationsystem (Barueri, SP, Brazil).
GSNO Synthesis
GSNO was synthesized as described previously [29]. In brief,reduced glutathione was reacted with an equimolar quantity of so-dium nitrite in aqueous HCl solution, under stirring, in an ice bathfor 40 min. The final solution was precipitated with acetone, filtered,and washed with cold water and acetone. The final precipitate wasfurther freeze-dried for 24 h. GSNO was stored at freezer tempera-ture (�20°C) protected from light.
Preparation of Pluronic F-127 Hydrogels
Hydrogels of pluronic F-127 (25 wt%) containing GSNO (100 �molL–1) were prepared as previously described [30]. In brief, solid plu-ronic F-127 was added to cold water (5°C). The solution was allowedto attain dissolution equilibrium at 5°C overnight. An appropriatevolume of GSNO solution (0.35 mmol L–1) was added to the pluronicF-127 solution under gentle stirring in an ice bath for homogeniza-tion. Control hydrogel was prepared by the same procedure, usingwater in the place of GSNO solution. The hydrogels were usedimmediately after preparation.
Wounding and Hydrogel Application
This study was approved by the Ethical Committee for AnimalUse of the State University of Rio de Janeiro. Male Wistar ratsweighing 250 to 300 g were anesthetized with intraperitoneal injec-tion of ketamine (5 mg/kg) and xylazine (2 mg/kg). The dorsal surfacewas shaved, a full-thickness excisional wound (1 cm2) was made onthe back of each rat by removing the skin (epidermis and dermis) andexposing Paniculus carnosus. The wounds were not sutured andwere allowed to heal by second intension, as already described [14,31].
Four groups (n � 6 in each group) were separated as follow: (A)control group (control): in which the hydrogel without GSNO wastopically applied daily on wound bed, beginning in the day of lesionuntil the sixth day after wounding; (B) GSNO in inflammatory phase(GSNOinf), in which GSNO-containing hydrogel was topically applieddaily on wound bed, beginning on the day of lesion until the secondday after wounding. In the next 4 d of application, only the hydrogelwithout GSNO was topically applied on the wound; (C) GSNO inproliferative phase (GSNOprol), in which the hydrogel without GSNOwas topically applied daily on wound bed on the day of lesion untilthe third day after wounding. In the next 3 d of application, GSNO-containing hydrogel was topically applied; (D) GSNO in inflamma-tory and proliferative phases (GSNOinf � prol), in which GSNO-containing hydrogel was topically applied daily on wound bed on theday of lesion until the sixth day after wounding. Two additionalgroups were created to evaluate if results obtained in GSNOinf � prol
group were due to longer exposition to GSNO; these two groups are(A) control2 where hydrogel without GSNO was topically appliedfrom day 3 until day 8 after wounding and (B) GSNOprol longer wherehydrogel containing-GSNO was topically applied from day 3 untilday 8 after wounding. All wounds were covered with 80 �L of cold
liquid F-127 solution, and after its application on the skin, liquid
86 JOURNAL OF SURGICAL RESEARCH: VOL. 149, NO. 1, SEPTEMBER 2008
F-127 solution underwent a rapid gelation yielding hydrogel. Theconcentration of GSNO in the hydrogel was 100 �mol L–1, whichcorresponds to a dose of 8 nmol of GSNO per application. GSNOincorporated in the hydrogel is quite stable during the 24 h periodsof application at the temperature of the wound lesion (36°C), withdecomposition smaller than 2%, as evaluated spectrophotometrically(data no shown).
After each daily application of the hydrogel (with or withoutGSNO), wound beds were covered with an occlusive wound dressing,until the sixth day after wounding. From the seventh day afterwounding, the wounds were left uncovered in all groups. In thegroups control2 and GSNOprol longer wounds were kept without dressinguntil the beginning of treatment (day 3) and after the end of treat-ment (day 9). The animals were housed in individual cages with freeaccess to food and water.
Wound contraction and re-epithelialization were evaluated; forthat, lesion tracings (total lesion perimeter and, 14 d after lesion,also non-re-epithelialized region perimeter) were performed on atransparent sheet on the day of lesion and 5, 7, and 14 d afterwounding, as already described [16]. Lesion tracings were digitalizedand analyzed using Zeiss image-processing system KS400 (Zeiss-Vision; Oberkochen, Germany). Data are expressed as percentage ofthe initial wound area and as percentage of re-epithelialized woundarea (mean � standard deviation).
Wound Tissue Processing and Staining
All animals were killed in a CO2 chamber 14 d after wounding.The lesions and the adjacent nonwounded skin were removed,formol-fixed (pH 7.2), and paraffin-embedded.
Sections (5 �m) were stained with hematoxylin-eosin for histolog-ical evaluation and quantification of epidermis and neoepidermisthickness with Sirius red for collagen analysis and with toluidineblue for mast cells evaluation.
Inflammatory and Mast Cells Quantification
To evaluate the inflammatory infiltrate, the amount of inflamma-tory cells was evaluated in HE-stained tissue sections. To quantifyinflammatory cells, 10 random fields (0.02 mm2) were counted using�100 objective (Olympus CBA; Olympus Optical Co., Ltd., Tokyo,Japan). All analyses were performed blindly and repeated withoutany difference between the replicates.
The number of mast cells and the percentage of degranulatingmast cells were evaluated in toluidine blue stained tissue sections.Fifteen random fields (0.119 mm2) were counted using a �40 objec-tive (Olympus BH-2, Olympus Optical Co., Ltd.) and the average cellcount per field was calculated for each animal. All analyses weredone blindly and repeated, without significant differences amongthem. Results are expressed as mean � standard deviation.
Quantification of Epidermis and Neoepidermis Thickness
The epidermis and neoepidermis thickness were evaluated inhematoxylin-eosin stained sections. Five random images of epider-mis and neoepidermis were captured for each animal using �20objective. For analysis, a videomicroscopic system (Axiolab Zeissmicroscope and a JVC video camera) and KS400 image program wereused. The epidermis and neoepidermis thickness (excluding the cor-nea layer) was measured in three different points for each image.The average of epidermis and neoepidermis thickness was calculatedfor each animal, data are expressed as mean � standard deviation.
Immunohistochemistry and Quantification
For assessment of blood vessels and myofibroblasts, mouse mono-clonal antibody against alpha-smooth muscle actin (�-SM actin) wasused and for proliferating cells, mouse monoclonal antibody against
proliferating cellular nuclear antigen (PCNA) (DAKO; Carpinteria,CA) was used, as already described [31]. Briefly, after antigen re-trieval (using trypsin digestion or citrate buffer pH 6.0), tissue sec-tions were incubated with primary antibody. For revelation theEnvision system (DAKO) was used. Diaminobenzidine was used aschromogen, and nuclei were stained with hematoxylin. Negativecontrols were performed replacing primary antibody by nonimmuneserum and no labeling was observed.
The distribution of blood vessels and myofibroblasts in granula-tion tissue was evaluated using a stereological method test systemwith cycloid arcs as already described [32]. Vessels were identified bythe presence of blood cells in their lumens or positive staining for�-SM actin in the wall (to confirm the presence of smooth musclecells or pericytes) [33]. Five random fields were analyzed in superfi-cial and deep regions of granulation tissue for each animal using �20objective for vessels and �40 for myofibroblasts. For analysis, avideomicroscopic system (Axiolab Zeiss microscope, a JVC video-camera and Sony Trinitron monitor; Sony, Pencoed, United King-dom) was used. Volume density of vessels was estimated in superfi-cial and deep regions and the volume density of myofibroblasts wasestimated in superficial region of granulation tissue.
The number of PCNA-positive cell nuclei was counted in neoepi-dermis. In neoepidermis, all basal cells were counted with a �40objective (Olympus BH-2; Olympus Optical Co. Ltd) and the result isexpressed as percentage of PCNA-positive basal cells. The data areexpressed as mean � standard deviation. All analysis were doneblindly and repeated, without significant difference among them.
Statistical Analysis
Analysis of wound contraction and re-epithelialized wound areaand inflammatory cells quantification were done using parametricUnpaired t-test with Welch correction. Mast cell quantification, epi-dermis and neoepidermis quantification and stereology evaluationwere analyzed with a nonparametric Mann-Whitney test. In allcases, P � 0.05 was considered statistically significant. Statisticalanalysis was done using the software Graph Pad Instat version 3.01(GraphPad Software Inc., San Diego, CA).
RESULTS
Macroscopic Evaluation
Scab was not observed along the experiment. Figure1 shows the macroscopic aspect of the wound areas inthe control, GSNOinf, GSNOprol, GSNOinfl�prol, andGSNOprol longer groups. A reduction in the wound areaand an improved re-epithelization was observed in allgroups, however these effects were more evident in theGSNOinfl�prol group (Fig. 1). The signs of re-epithelialization were observed only 14 d after wound-ing in all groups. However, at this time point only16.6% of animals in the control, GSNOinf, and GSNOprol
groups presented complete re-epithelialization while inthe GSNOinf�prol group, 50% of animals presented com-plete re-epithelialization (data not shown).
Analysis of the lesion areas showed that the woundcontraction was improved only in the GSNOinf�prol groupcompared with the control group (Fig. 2A). Two daysafter wounding, the percentage of initial wound areadid not present differences among the groups (Fig. 2A).Five and 7 d after wounding, wound areas of theGSNOinf and GSNOprol groups were similar to the con-trol group (Fig. 2A). Five days after wounding, the
lesion area was 18% higher in the control group com-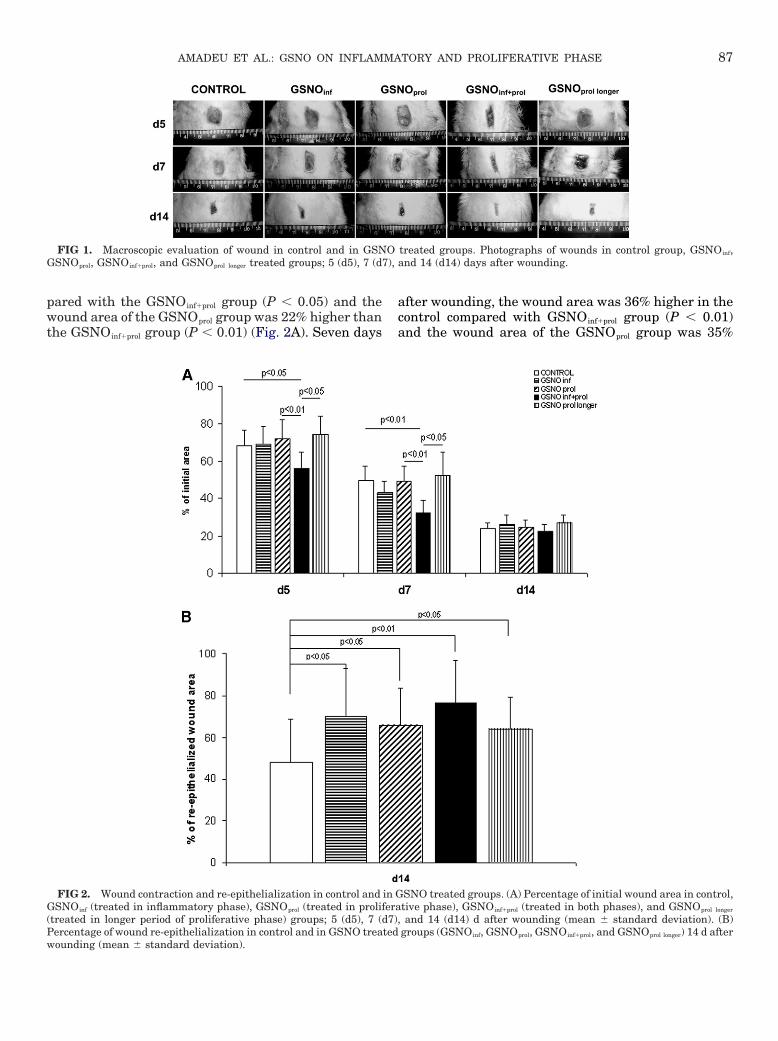
7),
87AMADEU ET AL.: GSNO ON INFLAMMATORY AND PROLIFERATIVE PHASE
pared with the GSNOinf�prol group (P � 0.05) and thewound area of the GSNOprol group was 22% higher thanthe GSNOinf�prol group (P � 0.01) (Fig. 2A). Seven days
FIG 1. Macroscopic evaluation of wound in control and in GSNGSNOprol, GSNOinf�prol, and GSNOprol longer treated groups; 5 (d5), 7 (d
FIG 2. Wound contraction and re-epithelialization in control andGSNOinf (treated in inflammatory phase), GSNOprol (treated in proli(treated in longer period of proliferative phase) groups; 5 (d5), 7 (Percentage of wound re-epithelialization in control and in GSNO trea
wounding (mean � standard deviation).after wounding, the wound area was 36% higher in thecontrol compared with GSNOinf�prol group (P � 0.01)and the wound area of the GSNOprol group was 35%
treated groups. Photographs of wounds in control group, GSNOinf,and 14 (d14) days after wounding.
SNO treated groups. (A) Percentage of initial wound area in control,tive phase), GSNOinf�prol (treated in both phases), and GSNOprol longer
and 14 (d14) d after wounding (mean � standard deviation). (B)groups (GSNO , GSNO , GSNO , and GSNO ) 14 d after
O
in Gferad7),ted
inf prol inf�prol prol longer
88 JOURNAL OF SURGICAL RESEARCH: VOL. 149, NO. 1, SEPTEMBER 2008
higher than the GSNOinf�prol group (P � 0.01) (Fig. 2A).At the end of the experiment (14 d after wounding),wound areas of all groups did not present differences(Fig. 2A). Fourteen days after wounding, the woundre-epithelialization was more advanced in the GSNOinf
(�45%), GSNOprol (�37%), and GSNOinf�prol (�59%)groups compared with the control group (P � 0.05, P �0.05 and P � 0.01, respectively), confirming the mac-roscopic results (Fig. 2B). There were no differencesamong control2 and control regarding wound contrac-tion or re-epithelialization in all time points studied.The results of wound contraction and re-epithe-lialization in the group GSNOprol longer were not differentfrom those observed in group GSNOprol, showing that alonger exposition to GSNO was not beneficial; so his-tological analysis was not performed in control2 andGSNOprol longer groups.
To evaluate epithelial cell proliferation, immunohis-tochemistry against PCNA was performed. Figure 3shows the percentage of PCNA-positive epithelialbasal cells in wound areas of all groups. It was ob-served that 14 d after wounding, epithelial cell prolif-eration was higher in the control group comparedwith GSNOinf (P � 0.05), GSNOprol (P � 0.01), andGSNOinf-prol (P � 0.01) groups. This result shows thatkeratinocyte proliferation was already reduced in allGSNO-treated groups since re-epithelialization wasmore advanced in those groups, while in the controlgroup keratinocyte were still proliferating.
Evaluation of Granulation Tissue
Figure 4 shows the granulation tissue pattern of thecontrol and the GSNO treated groups, 14 d afterwounding. It can be observed that the GSNOinf group(Fig. 4B) presented an intense cellularity, includingthe presence of inflammatory cells and “fibroblast-like”cells, in superficial and deep areas of granulation tis-sue, compared with the control group (Fig. 4A) and to
FIG 3. Percentage of PCNA-positive epithelial basal cells inwound area of control and GSNO treated groups (GSNOinf, GSNOprol,and GSNOinf�prol) 14 (d14) d after wounding (mean � standard devi-ation).
the others GSNO treated groups. The GSNOprol group
(Fig. 4C) presented a decrease in cellularity, as well asan increase of “fibroblast-like” cells, mainly in deeparea of the granulation tissue, in comparison with thecontrol group (Fig. 4A). The GSNOinf�prol group (Fig. 4D)presented a decrease in the amount of inflammatorycells and an increase in the amount of “fibroblast-like”(fusiform and parallel to surface) cells compared withthe control, GSNOinf and GSNOprol groups.
Fourteen days after wounding, the number of in-flammatory cells per field in the superficial area ofgranulation tissue was elevated in control group (41 �23) compared with GSNOinf (18 � 12), GSNOprol (17 �9), and GSNOinf�prol (14 � 8) groups (P � 0.0001, for all).The distribution of inflammatory cells in GSNOinf
group was not different when compared with GSNOprol
group. The number of inflammatory cells was higher inGSNOinf and GSNOprol groups than GSNOinf�prol (P �0.05, for both). In the deep area of granulation tissue,no difference was observed among the groups studied.
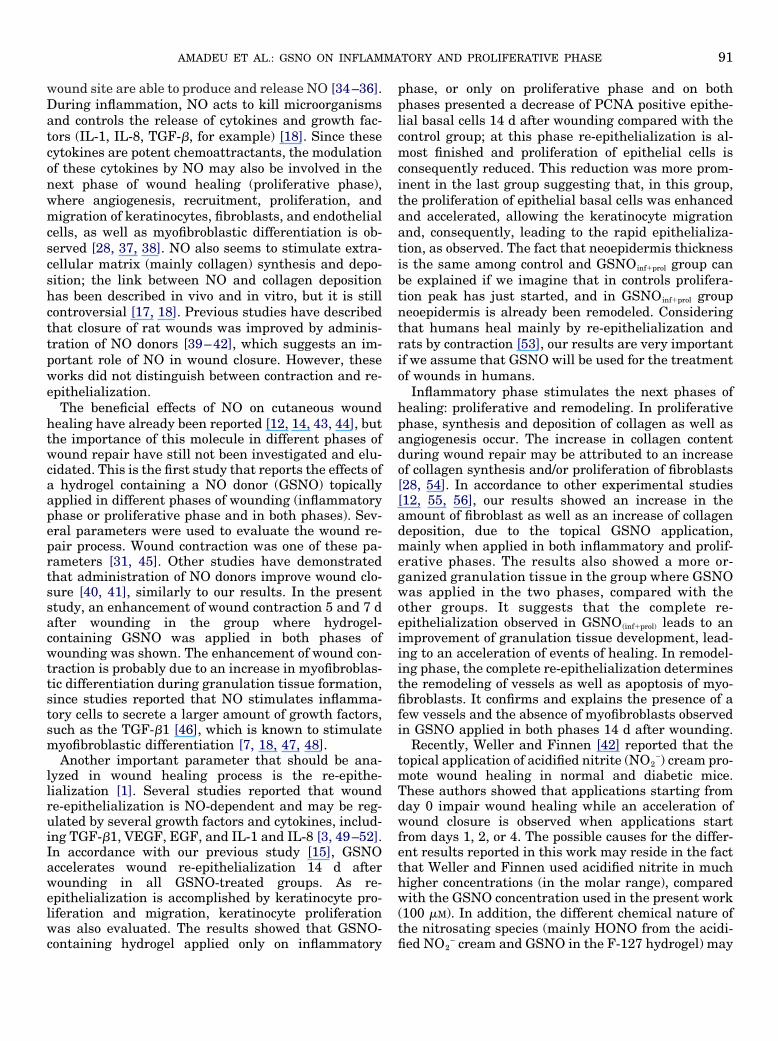
Figure 5 shows the collagen organization in woundareas of the control and GSNO treated groups, 14 dafter wounding. Collagen arrangement was analyzedin Sirius red stained sections observed under polariza-tion. The control group (Fig. 5A) showed, in superficialand deep areas of granulation tissue, thicker yellow-red collagen fibers arranged parallel to surface. In deeparea of GSNOinf group (Fig. 5B) reduced collagen fiberdensity and the presence of immature collagen fibers(thin yellow-greenish collagen fibers) were observed.The GSNOprol group (Fig. 5C) presented immature(thin yellow-greenish collagen fibers arranged perpen-dicularly to surface) and mature organized collagenfibers (thicker red-yellow collagen fibers arranged par-allel to surface). In deep area of GSNOinf�prol group (Fig.5D), a prevalence of organized mature fibers (thickred-yellow collagen fibers) was observed.
Figure 6 shows the immunohistochemistry againstalpha-smooth muscle actin (�-SMa) in the granulationtissue of control group and GSNO treated groups, 14 dafter wounding. It can be observed that the vascular-ization patterns of control and GSNO treated groupswere different. In control group (Fig. 6A), high amountof vessels was observed, some of the vessels presenteda thick wall. The GSNOinf group (Fig. 6B) presented adecrease in the amount of vessels in granulation tissueand these vessels were smaller than in the controlgroup. In granulation tissue of GSNOprol group, a de-crease in the amount of vessels was observed comparedwith the control and to the GSNOinf groups (Fig. 6C).The GSNOinf�prol group showed a decrease in vesselamount compared with all groups (Fig. 6D). In super-ficial region of granulation tissue, the volume densityof blood vessels of control group (22.5% � 8.1) waselevated compared with GSNOinf (8.8% � 8.0),GSNOprol (12.2% � 8.0), and GSNOinf�prol (5.8% � 7.3)
groups (P � 0.0001, P � 0.005, P � 0.0001, respec-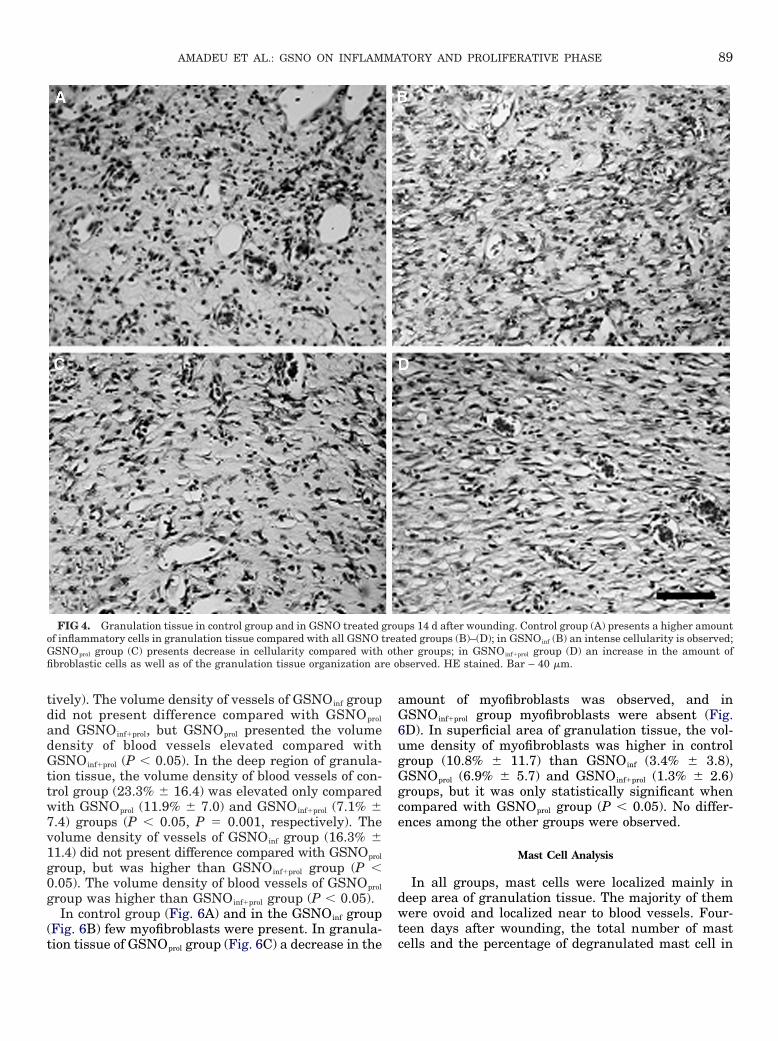
e o
89AMADEU ET AL.: GSNO ON INFLAMMATORY AND PROLIFERATIVE PHASE
tively). The volume density of vessels of GSNOinf groupdid not present difference compared with GSNOprol
and GSNOinf�prol, but GSNOprol presented the volumedensity of blood vessels elevated compared withGSNOinf�prol (P � 0.05). In the deep region of granula-tion tissue, the volume density of blood vessels of con-trol group (23.3% � 16.4) was elevated only comparedwith GSNOprol (11.9% � 7.0) and GSNOinf�prol (7.1% �7.4) groups (P � 0.05, P � 0.001, respectively). Thevolume density of vessels of GSNOinf group (16.3% �11.4) did not present difference compared with GSNOprol
group, but was higher than GSNOinf�prol group (P �0.05). The volume density of blood vessels of GSNOprol
group was higher than GSNOinf�prol group (P � 0.05).In control group (Fig. 6A) and in the GSNOinf group
(Fig. 6B) few myofibroblasts were present. In granula-
FIG 4. Granulation tissue in control group and in GSNO treated gof inflammatory cells in granulation tissue compared with all GSNO tGSNOprol group (C) presents decrease in cellularity compared withfibroblastic cells as well as of the granulation tissue organization ar
tion tissue of GSNOprol group (Fig. 6C) a decrease in the
amount of myofibroblasts was observed, and inGSNOinf�prol group myofibroblasts were absent (Fig.6D). In superficial area of granulation tissue, the vol-ume density of myofibroblasts was higher in controlgroup (10.8% � 11.7) than GSNOinf (3.4% � 3.8),GSNOprol (6.9% � 5.7) and GSNOinf�prol (1.3% � 2.6)groups, but it was only statistically significant whencompared with GSNOprol group (P � 0.05). No differ-ences among the other groups were observed.
Mast Cell Analysis
In all groups, mast cells were localized mainly indeep area of granulation tissue. The majority of themwere ovoid and localized near to blood vessels. Four-teen days after wounding, the total number of mast
ps 14 d after wounding. Control group (A) presents a higher amountted groups (B)–(D); in GSNOinf (B) an intense cellularity is observed;er groups; in GSNOinf�prol group (D) an increase in the amount of
bserved. HE stained. Bar – 40 �m.
roureaoth
cells and the percentage of degranulated mast cell in
90 JOURNAL OF SURGICAL RESEARCH: VOL. 149, NO. 1, SEPTEMBER 2008
deep area of granulation tissue did not present differ-ences among the groups (data not shown).
Epidermis and Neoepidermis Thickness
Figure 7 shows the epidermis and neoepidermisthickness of control and GSNO treated groups, 14 days
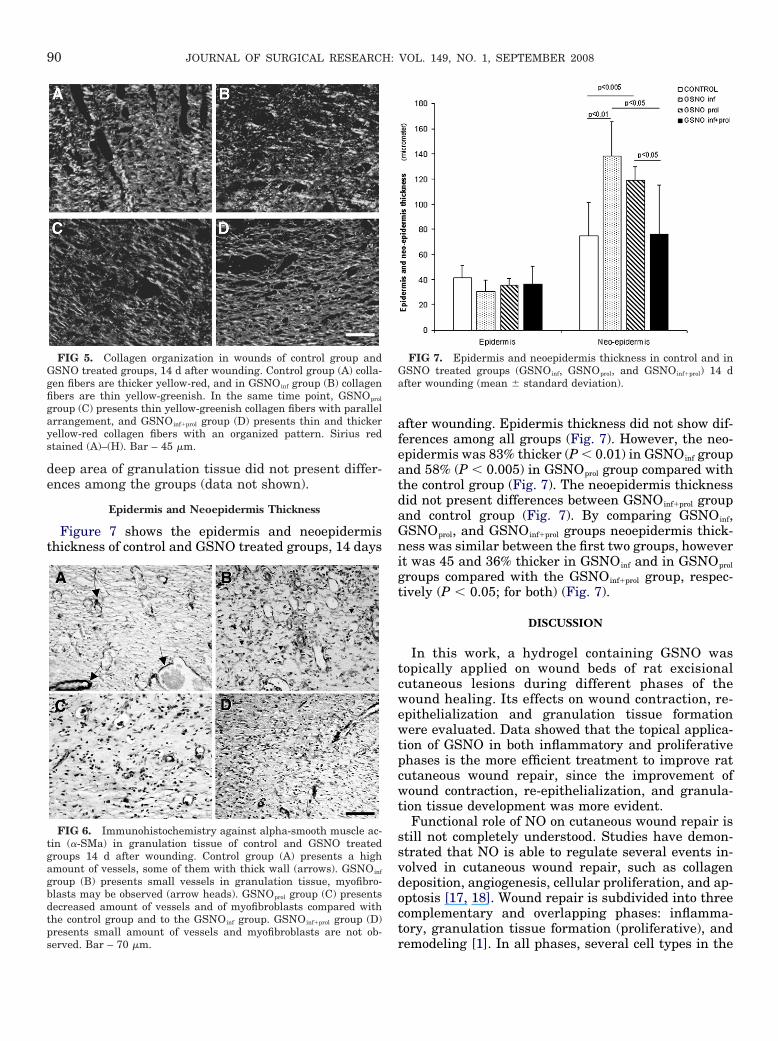
FIG 5. Collagen organization in wounds of control group andGSNO treated groups, 14 d after wounding. Control group (A) colla-gen fibers are thicker yellow-red, and in GSNOinf group (B) collagenfibers are thin yellow-greenish. In the same time point, GSNOprol
group (C) presents thin yellow-greenish collagen fibers with parallelarrangement, and GSNOinf�prol group (D) presents thin and thickeryellow-red collagen fibers with an organized pattern. Sirius redstained (A)–(H). Bar – 45 �m.
FIG 6. Immunohistochemistry against alpha-smooth muscle ac-tin (�-SMa) in granulation tissue of control and GSNO treatedgroups 14 d after wounding. Control group (A) presents a highamount of vessels, some of them with thick wall (arrows). GSNOinf
group (B) presents small vessels in granulation tissue, myofibro-blasts may be observed (arrow heads). GSNOprol group (C) presentsdecreased amount of vessels and of myofibroblasts compared withthe control group and to the GSNOinf group. GSNOinf�prol group (D)presents small amount of vessels and myofibroblasts are not ob-
served. Bar – 70 �m.after wounding. Epidermis thickness did not show dif-ferences among all groups (Fig. 7). However, the neo-epidermis was 83% thicker (P � 0.01) in GSNOinf groupand 58% (P � 0.005) in GSNOprol group compared withthe control group (Fig. 7). The neoepidermis thicknessdid not present differences between GSNOinf�prol groupand control group (Fig. 7). By comparing GSNOinf,GSNOprol, and GSNOinf�prol groups neoepidermis thick-ness was similar between the first two groups, howeverit was 45 and 36% thicker in GSNOinf and in GSNOprol
groups compared with the GSNOinf�prol group, respec-tively (P � 0.05; for both) (Fig. 7).
DISCUSSION
In this work, a hydrogel containing GSNO wastopically applied on wound beds of rat excisionalcutaneous lesions during different phases of thewound healing. Its effects on wound contraction, re-epithelialization and granulation tissue formationwere evaluated. Data showed that the topical applica-tion of GSNO in both inflammatory and proliferativephases is the more efficient treatment to improve ratcutaneous wound repair, since the improvement ofwound contraction, re-epithelialization, and granula-tion tissue development was more evident.
Functional role of NO on cutaneous wound repair isstill not completely understood. Studies have demon-strated that NO is able to regulate several events in-volved in cutaneous wound repair, such as collagendeposition, angiogenesis, cellular proliferation, and ap-optosis [17, 18]. Wound repair is subdivided into threecomplementary and overlapping phases: inflamma-tory, granulation tissue formation (proliferative), and
FIG 7. Epidermis and neoepidermis thickness in control and inGSNO treated groups (GSNOinf, GSNOprol, and GSNOinf�prol) 14 dafter wounding (mean � standard deviation).
remodeling [1]. In all phases, several cell types in the
91AMADEU ET AL.: GSNO ON INFLAMMATORY AND PROLIFERATIVE PHASE
wound site are able to produce and release NO [34–36].During inflammation, NO acts to kill microorganismsand controls the release of cytokines and growth fac-tors (IL-1, IL-8, TGF-�, for example) [18]. Since thesecytokines are potent chemoattractants, the modulationof these cytokines by NO may also be involved in thenext phase of wound healing (proliferative phase),where angiogenesis, recruitment, proliferation, andmigration of keratinocytes, fibroblasts, and endothelialcells, as well as myofibroblastic differentiation is ob-served [28, 37, 38]. NO also seems to stimulate extra-cellular matrix (mainly collagen) synthesis and depo-sition; the link between NO and collagen depositionhas been described in vivo and in vitro, but it is stillcontroversial [17, 18]. Previous studies have describedthat closure of rat wounds was improved by adminis-tration of NO donors [39–42], which suggests an im-portant role of NO in wound closure. However, theseworks did not distinguish between contraction and re-epithelialization.
The beneficial effects of NO on cutaneous woundhealing have already been reported [12, 14, 43, 44], butthe importance of this molecule in different phases ofwound repair have still not been investigated and elu-cidated. This is the first study that reports the effects ofa hydrogel containing a NO donor (GSNO) topicallyapplied in different phases of wounding (inflammatoryphase or proliferative phase and in both phases). Sev-eral parameters were used to evaluate the wound re-pair process. Wound contraction was one of these pa-rameters [31, 45]. Other studies have demonstratedthat administration of NO donors improve wound clo-sure [40, 41], similarly to our results. In the presentstudy, an enhancement of wound contraction 5 and 7 dafter wounding in the group where hydrogel-containing GSNO was applied in both phases ofwounding was shown. The enhancement of wound con-traction is probably due to an increase in myofibroblas-tic differentiation during granulation tissue formation,since studies reported that NO stimulates inflamma-tory cells to secrete a larger amount of growth factors,such as the TGF-�1 [46], which is known to stimulatemyofibroblastic differentiation [7, 18, 47, 48].
Another important parameter that should be ana-lyzed in wound healing process is the re-epithe-lialization [1]. Several studies reported that woundre-epithelialization is NO-dependent and may be reg-ulated by several growth factors and cytokines, includ-ing TGF-�1, VEGF, EGF, and IL-1 and IL-8 [3, 49–52].In accordance with our previous study [15], GSNOaccelerates wound re-epithelialization 14 d afterwounding in all GSNO-treated groups. As re-epithelialization is accomplished by keratinocyte pro-liferation and migration, keratinocyte proliferationwas also evaluated. The results showed that GSNO-
containing hydrogel applied only on inflammatoryphase, or only on proliferative phase and on bothphases presented a decrease of PCNA positive epithe-lial basal cells 14 d after wounding compared with thecontrol group; at this phase re-epithelialization is al-most finished and proliferation of epithelial cells isconsequently reduced. This reduction was more prom-inent in the last group suggesting that, in this group,the proliferation of epithelial basal cells was enhancedand accelerated, allowing the keratinocyte migrationand, consequently, leading to the rapid epithelializa-tion, as observed. The fact that neoepidermis thicknessis the same among control and GSNOinf�prol group canbe explained if we imagine that in controls prolifera-tion peak has just started, and in GSNOinf�prol groupneoepidermis is already been remodeled. Consideringthat humans heal mainly by re-epithelialization andrats by contraction [53], our results are very importantif we assume that GSNO will be used for the treatmentof wounds in humans.
Inflammatory phase stimulates the next phases ofhealing: proliferative and remodeling. In proliferativephase, synthesis and deposition of collagen as well asangiogenesis occur. The increase in collagen contentduring wound repair may be attributed to an increaseof collagen synthesis and/or proliferation of fibroblasts[28, 54]. In accordance to other experimental studies[12, 55, 56], our results showed an increase in theamount of fibroblast as well as an increase of collagendeposition, due to the topical GSNO application,mainly when applied in both inflammatory and prolif-erative phases. The results also showed a more or-ganized granulation tissue in the group where GSNOwas applied in the two phases, compared with theother groups. It suggests that the complete re-epithelialization observed in GSNO(inf�prol) leads to animprovement of granulation tissue development, lead-ing to an acceleration of events of healing. In remodel-ing phase, the complete re-epithelialization determinesthe remodeling of vessels as well as apoptosis of myo-fibroblasts. It confirms and explains the presence of afew vessels and the absence of myofibroblasts observedin GSNO applied in both phases 14 d after wounding.
Recently, Weller and Finnen [42] reported that thetopical application of acidified nitrite (NO2
–) cream pro-mote wound healing in normal and diabetic mice.These authors showed that applications starting fromday 0 impair wound healing while an acceleration ofwound closure is observed when applications startfrom days 1, 2, or 4. The possible causes for the differ-ent results reported in this work may reside in the factthat Weller and Finnen used acidified nitrite in muchhigher concentrations (in the molar range), comparedwith the GSNO concentration used in the present work(100 �M). In addition, the different chemical nature ofthe nitrosating species (mainly HONO from the acidi-
fied NO2– cream and GSNO in the F-127 hydrogel) may
92 JOURNAL OF SURGICAL RESEARCH: VOL. 149, NO. 1, SEPTEMBER 2008
also lead to different results. Other studies that admin-istrated NO donors suggest that exogenous NO has animportant and positive effect on cutaneous woundhealing [2, 13, 43, 44, 56, 57]. The biological effect ofNO is highly depending on its concentration. Highdoses of NO increase clot formation and reactive tissue,as well as impair collagen organization, which contrib-ute to cellular toxicity and to delayed wound repair[56]. On the other hand, low doses of NO (in the range25–100 �M) are reported to increase the collagen syn-thesis, which allows wound repair [58]. For this reason,the concentration of 100 �M of GSNO was used in thisstudy.
In summary, the results presented in this studydemonstrate that the topical application of GSNO onboth inflammatory and proliferative phases im-proves rat cutaneous wound repair by enhancingwound contraction and, mainly by accelerating re-epithelialization, show that NO is crucial in bothphases. Further studies should be performed to inves-tigate the effects of topical application of GSNO-containing hydrogel in models of impaired cutaneouswound repair and its influence on the expression ofseveral molecules such as TGF-�1, EGF, VEGF, andIL-1 to better understand the exact role of NO oncutaneous wound repair and to propose the use of thisformulation for the treatment of abnormal wound heal-ing.
ACKNOWLEDGMENTS
This study was partially supported by CNPq, FAPERJ, andFAPESP. TPA held a postgraduate fellowship from CAPES, and ABSfrom Fundaçao de Amparo à Pesquisa do Estado de Sao Paulo(FAPESP), project 01/07868-9.
REFERENCES
1. Singer AJ, Clark RA. Cutaneous wound healing. N Engl J Med341:738.1999;
2. Witte MB, Barbul A. General principles of wound healing. SurgClin North Am 1997;77:509.
3. Frank S, Stallmeyer B, Kampfer H, et al. Nitric oxide triggersenhanced induction of vascular endothelial growth factor ex-pression in cultured keratinocytes (HaCaT) and during cutane-ous wound repair. FASEB J 1999;13:2002.
4. Clark, RFA. The molecular and cellular biology of wound repair.New York: Plenum Press, 1996:3–50.
5. Amadeu TP, Coulomb B, Desmouliere A, et al. Cutaneouswound healing: Myofibroblastic differentiation and in vitromodels. Int J Low Extrem Wounds 2003;2:60.
6. Peled ZM, Chin GS, Liu W, et al. Response to tissue injury. ClinPlast Surg 2000;27:489.
7. Tomasek JJ, Gabbiani G, Hinz B, et al. Myofibroblast andmechano-regulation of connective tissue remodeling. Mol CellBiol 2002;3:349.
8. Usui ML, Underwood RA, Mansbridge JN, et al. Morphologicalevidence for the role of suprabasal keratinocytes in wound
reepithelialization. Wound Repair Regen 2005;13:468.9. Xue M, Le NT, Jackson CJ. Targeting matrix metalloproteasesto improve cutaneous wound healing. Expert Opin Ther Targets2006;10:143.
10. Rodeberg DA, Chaet MS, Bass RC, et al. Nitric oxide: An over-view. Am J Surg 1995;170:292.
11. Wolf G. Nitric oxide and nitric oxide synthase: Biology, pathol-ogy, localization. Histol Histopathol 1997;12:251.
12. Witte MB, Kiyama T, Barbul A. Nitric oxide enhances experi-mental wound healing in diabetes. Br J Surg 2002;89:1594.
13. Achuth HN, Moochhala SM, Mahendran R, et al. Nitrosogluta-thione triggers collagen deposition in cutaneous wound repair.Wound Repair Regen 2005;13:383.
14. Amadeu TP, Costa AMA. Nitric oxide synthesis inhibition al-ters rat cutaneous wound healing. J Cut Pathol 2006;33:465.
15. Amadeu TP, Seabra AB, Ganzarolli de Oliveira, M, et al.S-nitrosoglutathione accelerates rat cutaneous wound repair. JEur Acad Dermatol Venereol 2007;21:629.
16. Bruch-Gerharz D, Ruzicka T, Kolb-Bachofen V. Nitric oxide inhuman skin: Current status and future prospects. J. InvestDermatol 1998;110:1.
17. Rizk M, Witte MB, Barbul A. Nitric oxide and wound healing.World J Surg 2004;28:301.
18. Schwentker A, Vodovotz Y, Weller R, et al. Nitric oxide andwound repair: Role of cytokines? Nitric Oxide 2002;7:1.
19. Konturek SJ, Brzozowski T, Majka J, et al. Inhibition of nitricoxide synthase delays healing of chronic gastric ulcers. EurJ Pharmacol 1993;239:215.
20. Schaffer MR, Tantry U, Thornton FJ, et al. Inhibition of nitricoxide synthesis in wounds: Pharmacology and effect on accu-mulation of collagen in wounds in mice. Eur J Surg 1999;165:262.
21. Schaffer MR, Tantry U, van Wesep RA, et al. Nitric oxidemetabolism in wounds. J Surg Res 1997;71:25.
22. Elliott SN, McKnight W, Cirino G, et al. A nitric oxide-releasingnonsteroidal anti-inflammatory drug accelerates gastric ulcerhealing in rats. Gastroenterology 1995;109:524.
23. Lund JN, Scholefield JH. A randomized, prospective, double-blind, placebo-controlled trial of glyceryl trinitrate ointment intreatment of anal fissure. Lancet 1997;349:11
24. Thornton FJ, Schaffer MR, Witte MB, et al. Enhanced collagenaccumulation following direct transfection of the inducible ni-tric oxide synthase gene in cutaneous wounds. Biochem Bio-phys Res Commun 1998;246:654.
25. Burgaud JL, Riffaud JP, Del Soldato P. Nitric-oxide releasingmolecules: A new class of drugs with several major indications.Curr Pharm Des 2002;8:201.
26. Zhang Y, Hogg N. S-Nitrosothiols: Cellular formation andtransport. Free Radic Biol Med 2005;38:831.
27. Seabra AB, Fitzpatrick A, Paul J, et al. Topically appliedS-nitrosothiol-containing hydrogels as experimental and phar-macological nitric oxide donors in human skin. Br J Dermatol2004;151:977.
28. Witte MB, Thornton FJ, Efron DT, et al. Enhancement of fibro-blast collagen synthesis by nitric oxide. Nitric Oxide 2000;4:572.
29. Shishido SM, Seabra AB, Loh W, et al. Thermal and photo-chemical nitric oxide release from S-nitrosothiols incorporatedin pluronic F127 gel: Potential uses for local and controllednitric oxide release. Biomaterials 2003;24:3543.
30. Seabra AB, de Souza GF, da Rocha LL, et al. S-nitrosoglutathioneincorporated in poly(ethylene glycol) matrix: Potential use fortopical nitric oxide delivery. Nitric Oxide 2004;11:263.
31. Souza BR, Cardoso JF, Amadeu TP, et al. Sympathetic dener-
93AMADEU ET AL.: GSNO ON INFLAMMATORY AND PROLIFERATIVE PHASE
vation alters wound contraction and granulation tissueformation in cutaneous wound healing. Wound Repair Regen2005;13:498.
32. Amadeu T, Braune A, Mandarim-de-Lacerda C, et al. Vascular-ization pattern in hypertrophic scars and keloids: A stereologi-cal analysis. Pathol Res Pract 2003;199:469.
33. Sadoun E, Reed MJ. Impaired angiogenesis in aging is associ-ated with alterations in vessel density, matrix composition,inflammatory response, and growth factor expression. J Histo-chem Cytochem 2003;51:1119.
34. Jackson M, Frane F, Weller R, et al. Expression of nitric oxidesynthase III (eNOS) mRNA by human skin cells: Melanocytesbut not keratinocytes express eNOS mRNA. Arch Dermatol Res1998;290:249.
35. Wang R, Ghahary A, Shen YJ, et al. Human dermal fibroblastsproduce nitric oxide and express both constitutive and induciblenitric oxide synthase isoforms. J Invest Dermatol 1996;106:419.
36. Weller R. Nitric oxide–a newly discovered chemical transmitterin human skin. Br J Dermatol 1997;137:665.
37. Krischel V, Bruch-Gerharz D, Suschek C, et al. Biphasic effectof exogenous nitric oxide on proliferation and differentiation inskin derived keratinocytes but not fibroblasts. J Invest Derma-tol 1998;111:286.
38. Shizukuda Y, Tang S, Yokota R, et al. Vascular endothelialgrowth factor-induced endothelial cell migration and prolifera-tion depend on a nitric oxide-mediated decrease in proteinkinase C delta activity. Circ Res 1999;85:247.
39. Lee PC, Salyapongse AN, Bragdon GA, et al. Impaired woundhealing and angiogenesis in eNOS-deficient mice. J PhysiolHeart Circ Physiol 1999;277:H1600.
40. Shabani M, Pulfer SK, Bulgin JP, et al. Enhancement of woundrepair with a topically applied nitric oxide-realizing polymer.Wound Repair Regen 1996;4:309.
41. Yamasaki K, Edington HD, McClosky C, et al. Reversal ofimpaired wound repair in iNOS-deficient mice by topicaladenoviral-mediated iNOS gene transfer. J Clin Invest 1998;101:967.
42. Weller R, Finnen MJ. The effects of topical treatment withacidified nitrite on wound healing in normal and diabetic mice.Nitric Oxide 2006;15:395.
43. Masters KS, Leibovich SJ, Belem P, et al. Effects of nitric oxidereleasing poly(vinyl alcohol) hydrogel dressings on dermalwound healing in diabetic mice. Wound Repair Regen 2002;10:286.
44. Mittermayr R, Valentini D, Fitzal F, et al. Protective effect of a
novel NO-donor on ischemia/reperfusion injury in a ratepigastric flap model. Wound Repair Regen 2003;11:1.
45. Horan MP, Quan N, Subramanian SV, et al. Impaired woundcontraction and delayed myofibroblast differentiation inrestraint-stressed mice. Brain Behav Immun 2005;19:207.
46. Soneja A, Drews M, Malinski T. Role of nitric oxide, nitroxida-tive and oxidative stress in wound healing. Pharmacol Rep2005;57:108.
47. Desmouliere A. Factors influencing myofibroblast differentia-tion during wound healing and fibrosis. Cell Biol Int 1995;19:471.
48. Desmouliere A, Chaponnier C, Gabbiani G. Tissue repair, con-traction, and the myofibroblast. Wound Repair Regen 2005;13:7.
49. Brown LF, Yeo KT, Berse B, et al. Expression of vascularpermeability factor (vascular endothelial growth factor) by epi-dermal keratinocytes during wound healing. J Exp Med 1992;176:1375.
50. Heck DE, Laskin DL, Gardner CR, et al. Epidermal growthfactor suppresses nitric oxide and hydrogen peroxide produc-tion by keratinocytes. Potential role for nitric oxide in theregulation of wound healing. J Biol Chem 1992;267:21277.
51. Hill YM, Corbett JA, Kwon G, et al. Nitric oxide regulatesinterleukin 1 bioactivity released from murine macrophages.J Biol Chem 1996;271:22672.
52. Stallmeyer B, Kampfer H, Kolb N, et al. The function of nitricoxide in wound repair: Inhibition of inducible nitric oxide-synthase severely impairs wound reepithelialization. J InvestDermatol 1999;113:1090.
53. Davidson JM. Animal models for wound repair. Arch DermatolRes 1998;290(Suppl):S1.
54. Shukla A, Rasik AM, Shankar R. Nitric oxide inhibits woundscollagen synthesis. Mol Cell Biochem 1999;200:27.
55. Barbul A, Lazarou SA, Efron DT, et al. Arginine enhanceswound healing and lymphocyte immune responses in humans.Surgery 1990;108:331; discussion 336.
56. Bauer JA, Rao W, Smith DJ. Evaluation of linearpolyethyleneimine/nitric oxide adduct on wound repair: Ther-apy versus toxicity. Wound Repair Regen 1998;6:569
57. Amadeu TP, Seabra AB, Ganzarolli de Oliveira M, et al.S-nitrosoglutathione accelerates rat cutaneous wound repair. JEur Acad Dermatol Venereol (in press).
58. Shi HP, Most D, Efron DT, et al. The role of iNOS in wound
healing. Surgery 2001;130:225.