Exploring doctor-patient interactions in post-disaster Aceh ...
Upload
khangminh22Category
view
0download
0
1
Patient and Doctor Perceptions of Hypertension and its
Treatment: A Qualitative Study in Urban Hospitals of
Pakistan
Qurrat Ul Ain
Submitted to the University of Hertfordshire in partial fulfilment of the
requirements of the degree of Doctor of Philosophy
October 2019

2
Abstract
Hypertension (HTN) is a chronic disease that has become a growing public health problem in
countries around the world, including Pakistan. Successful HTN control is an essential
cornerstone in the prevention of morbidity and mortality associated with uncontrolled HTN.
However, patients’ beliefs about their disease, treatment and control are related to the
outcome of successful HTN control and management. Likewise, doctors’ understanding of
HTN and its treatment is equally important and can affect their practice and HTN
management. There is little qualitative research considering patients’ and doctors’
understanding of HTN, its treatment and how it influences HTN management in Pakistan.
Therefore, the current study aimed to elicit patients’ and doctors’ perceptions, attitudes and
beliefs about HTN and its treatment in urban areas of Pakistan.
A qualitative study that drew on grounded theory principles was undertaken in two public
hospitals of Pakistan. Thirty in-depth semi-structured interviews with hypertensive patients
and thirty interviews with doctors were conducted in two hospitals. Interviews were
translated and transcribed from Urdu into English and NVivo was used to organise the data in
a systematic way. Data were analysed using a constant comparative approach based on the
principles of grounded theory.
The study revealed that patients’ (n=30) beliefs were complex, deep-rooted and influenced
their attitude towards HTN treatment. Patients’ beliefs were informed by understanding
gleaned from the socio-cultural environment (local norms, social relations, religion),
individual factors (e.g. income, co-morbidities) and interactions with doctors. In contrast,
doctors’ (n=30) own understandings on what constitutes successful HTN management often
contradicted patients’ beliefs. Doctors’ reported that time restraints and work burden
affected their approach to treatment and the provision of information to patients.
Findings also revealed an overlap between patients’ and doctors’ beliefs, however, in relation
to adopting lifestyle changes for management of HTN. In general, though doctors paid less
consideration to patients’ beliefs in routine clinical practice and evaluated patients through
the filter of their own beliefs. The findings suggest that doctors could provide a better service
care by aligning with their patients on a common understanding about HTN management and
providing culturally appropriate information. Doctors should be aware of the understanding
hypertensive patients attach to HTN and avoid providing treatment based on their own
beliefs. Doctors must engage with patients’ beliefs and identify their particular healthcare
needs in order to achieve control of HTN in Pakistan.
Keywords: Hypertension, high blood pressure, lifestyle recommendations, understanding,
patient, doctor, Pakistan, qualitative research.

3
Declaration
I Qurrat ul Ain, declare that this dissertation is entirely my own work and has not been
submitted for any other degree or professional qualification.
Signed: Date: October 2019
Qurrat Ul Ain

4
Acknowledgments
First and foremost, I am thankful to Almighty Allah; due to His blessings I could finish my
research work and thesis. I would like to thank the following people for the help and support
they provided me during the course of this journey. I am grateful to my parents for their
endless support and encouragement. Words fail to describe my feelings of respect for my
supervisors Professor Wendy Wills and Doctor Angela Dickinson for providing guidance and
mentoring me throughout this study.
I also owe a special thanks to Waqar for keeping things light-hearted for me during the periods
of stress. Kudos to my colleagues Dr Iram Rasheed, Dr Saira Bilal, Dr Sumera Shahzad, Dr
Asghar, Dr Abdul Rasheed, Shahab, Zulqarnain and Adnan my brothers for their assistance
and for making things possible for me. I would also like to thank the management of two
hospitals for allowing me to recruit study participants and the participants themselves who
generously gave their time and took part in the study.
Finally, I would like to dedicate my work to my gorgeous grandmother Fahmeeda Begham,
who died due to hypertension related complications and is sadly no longer with us.

5
List of Abbreviations
CVD Cardiovascular Disease
BHUs Basic Health Units
HTN Hypertension
LHWs Lady Health Workers
OPD Out Patient Department
PMDC Pakistan Medical and Dental Council
THUs Tertiary Health Units
UK United Kingdom
WHO World Health Organization

6
TABLE OF CONTENTS Abstract...................................................................................................................................... 2
Declaration ................................................................................................................................ 3
Acknowledgments ..................................................................................................................... 4
List of Abbreviations ................................................................................................................. 5
Chapter One……………………………………………………………………………………………………………………11
Introduction ............................................................................................................................. 11
1.1 HTN and Cardiovascular Disease ............................................................................................ 12
1.2 Treatment of HTN ................................................................................................................. 12
1.3 Pakistani Context .................................................................................................................. 13
1.3.1 An overview of the situation regarding HTN in Pakistan ..................................................... 14
1.3.2 Healthcare system in Pakistan ............................................................................................. 15
1.4 HTN and Lifestyle Recommendations ..................................................................................... 17
1.4.1 Exercise ................................................................................................................................ 17
1.4.2 Diet ....................................................................................................................................... 18
1.4.3 High salt consumption ......................................................................................................... 19
1.4.4 Smoking ................................................................................................................................ 19
1.4.5 High alcohol intake ............................................................................................................... 20
1.5 Rationale for the Study .......................................................................................................... 21
1.6 Research Question, Aim and Objectives of the Study ............................................................... 23
1.7 Structure of the Dissertation .................................................................................................. 24
Chapter Two……………………………………………………………….…………………………………………….……25
Literature Review……………………………………………………………………………….……………………..…..25
2.1 Rationale for Systematic Review ............................................................................................ 25
2.2 The Review Protocol ............................................................................................................. 25
2.2.1 Inclusion and exclusion criteria ............................................................................................ 26
2.2.2 Search strategy..................................................................................................................... 26
2.3 Results from the Review ........................................................................................................ 27
2.3.1 Analysis of included studies ................................................................................................. 27
2.4 Patients’ Understanding of HTN and its Treatment .................................................................. 29
2.4.1 Understanding of HTN ......................................................................................................... 29
2.4.2 Causes of HTN ...................................................................................................................... 30
2.4.3 Drug non-adherence ............................................................................................................ 31
2.4.4 Using alternative treatments ............................................................................................... 33
2.4.5 Awareness about lifestyle changes ...................................................................................... 34

7
2.5 The Approach of Doctors to HTN Treatment ........................................................................... 36
2.6 Summary and Identification of Gaps ....................................................................................... 38
2.7 Search Strategy for the Broader Literature Review .................................................................. 39
2.8 Health Beliefs ....................................................................................................................... 40
2.8.1 The impact of socio-cultural context on beliefs and behaviour .......................................... 42
2.9 Living with HTN .................................................................................................................... 46
2.9.1 HTN drug adherence ............................................................................................................ 47
2.9.2 Difficulties in adopting lifestyle changes ............................................................................. 49
2.10 Doctors’ Understanding about Illness ................................................................................... 50
2.10.1 HTN treatment guidelines .................................................................................................. 51
2.10.2 Assumptions about patients .............................................................................................. 52
2.11 Conceptual Framework........................................................................................................ 54
2.12 Summary ............................................................................................................................ 55
Chapter Three .......................................................................................................................... 56
Methodology ........................................................................................................................... 56
3.1 The Nature of Qualitative Research ........................................................................................ 56
3.2 Methodological Paradigm for This Study ................................................................................ 56
3.2.1 Constructivism or constructionism? .................................................................................... 58
3.3 Choosing the Research Methodology ..................................................................................... 58
3.3.1 Debates in development of grounded theory approaches .................................................. 59
3.3.2 A critical discussion of a grounded theory approach ........................................................... 60
3.3.3 The present study ................................................................................................................ 61
3.4 Data Collection Methods for the Current Study ....................................................................... 62
3.4.1 Semi-structured interviews .................................................................................................. 62
3.5 Study Design ......................................................................................................................... 63
3.5.1 Pilot study ............................................................................................................................ 63
3.5.2 Recruitment of hospitals for the main study ....................................................................... 65
3.5.3 The recruitment of participants………………………………………………………………………………………70
3.5.4 Data collection…………………………………………………………………………………………………………………71
Table 3.1 Demographic characteristics of patients (n=30) ........................................................... 72
Table 3.2 Information about selected doctors (n=30) .................................................................. 74
3.6 Ethical Considerations ........................................................................................................... 76
3.6.1 Confidentiality of participants ............................................................................................. 76
3.6.2 Non-maleficence .................................................................................................................. 76
3.6.3 Informed written consent .................................................................................................... 77

8
3.6.4 An additional ethical protocol specific to this study ............................................................ 77
3.7 Consideration of Data Sources, Governance and Management ................................................ 78
3.7.1 Translation and transcription ............................................................................................... 78
3.7.2 Qualitative data analysis software ....................................................................................... 78
3.8 Data Analysis ........................................................................................................................ 79
3.8.1 Familiarisation with data and manual coding ...................................................................... 79
3.8.2 Generating initial codes and child nodes ............................................................................. 80
3.8.3 Selective/focused coding for theme identification .............................................................. 80
3.8.4 Data saturation .................................................................................................................... 81
3.9 Trustworthiness of Qualitative Data ....................................................................................... 82
3.9.1 A reflective stance ................................................................................................................ 82
3.10 Summary ............................................................................................................................ 84
Chapter Four ............................................................................................................................ 85
Patients’ Perceptions of HTN and its Treatment ................................................................... 85
4.1 Perceptions of HTN ............................................................................................................... 85
4.1.1 Diagnosis .............................................................................................................................. 85
4.1.2 Symptoms ............................................................................................................................ 86
4.1.3 Causes of HTN ...................................................................................................................... 88
4.2 Experiences and Attitude Concerning Taking Antihypertensive Drugs ....................................... 91
4.2.1 Lack of information about drugs in consultations ............................................................... 93
4.3 Perceptions About Lifestyle Management .............................................................................. 94
4.3.1 Understanding concerning exercise ..................................................................................... 95
4.3.2 Dietary management ........................................................................................................... 99
4.3.3 Salt consumption ............................................................................................................... 105
4.3.4 Smoking .............................................................................................................................. 106
4.3.5 Alcohol consumption ......................................................................................................... 109
4.4 Involvement in Alternative Strategies ................................................................................... 110
4.4.1 Consulting quacks and Hakeem ......................................................................................... 110
4.4.2 Alternative medicines use and/ home remedies ............................................................... 111
4.4.3 Faith healing ....................................................................................................................... 112
4.5 Summary ............................................................................................................................ 113
Chapter Five……………………………………………………….………………………………………………………..114
Doctors' perceptions of HTN and its Treatment………………………………………….…………………114
5.1 Perceptions about HTN........................................................................................................ 114
5.1.1 Awareness about HTN guidelines ...................................................................................... 116

9
5.1.2 Practicing HTN guidelines .................................................................................................. 117
5.2 Treating Patients with HTN .................................................................................................. 118
5.3 Perceptions Regarding Lifestyle Management ....................................................................... 121
5.3.1 Understanding concerning involvement in exercise .......................................................... 121
5.3.2 Dietary management ......................................................................................................... 124
5.3.3 Salt consumption ............................................................................................................... 127
5.3.4 Smoking cessation .............................................................................................................. 128
5.3.5 Alcohol consumption ......................................................................................................... 129
5.4 Informing Patients about HTN .............................................................................................. 130
5.6 Communication Issues in Clinical Interactions ....................................................................... 131
5.7 Summary ............................................................................................................................ 132
Chapter Six ................................................................................................................... 133
Discussion .................................................................................................................... 133
6.1 Discussion of Findings ......................................................................................................... 133
6.1.1 Patients' beliefs……………………………………………………………………………………….……………………134
6.1.2 Doctors’ beliefs .................................................................................................................. 138
6.1.3 A comparison between participants’ beliefs of HTN management ................................... 141
6.2 Doctor-patient Relationships ............................................................................................... 143
6.3 Recommendations .............................................................................................................. 146
6.3.1 For doctors ......................................................................................................................... 146
6.3.2 For patients ........................................................................................................................ 147
6.3.3 Recommendations for future research .............................................................................. 149
6.4 Study Strengths and Limitations ........................................................................................... 149
6.5 Conclusion .......................................................................................................................... 150
References ................................................................................................................... 151
Appendices………………………………………………………………………………………….……………………….214
Appendix 1: Search Strategy with a PRISMA flow diagram ........................................................ 214
Appendix 2: Table 2.1 Detail of the included studies ................................................................. 215
Appendix 3i: Table 2.2 CASP checklist ten questions ................................................................. 223
Appendix 3ii: Table 2.3 Quality assessment scores by using NHLBI criteria ............................... 224
Appendix 4: Changes made in topic guides after pilot study ..................................................... 226
Appendix 4i: Changes made in topic guide for patients after pilot study .................................. 226
Appendix 4ii: Changes made in topic guide for doctors after pilot study .................................. 227
Appendix 5i: Challenges associated with conducting the pilot study ......................................... 228
Appendix 5ii: Lessons learned from the pilot study.................................................................... 229

10
Appendix 6: (Interview topic guides in English) .......................................................................... 231
Appendix 6i: Interview topic guide for patients ......................................................................... 231
Appendix 6ii: Interview topic guide for doctors ......................................................................... 233
Appendix 7: (Interview topic guides in Urdu) ............................................................................. 235
Appendix 7i: Interview topic guide for patients (In Urdu) .......................................................... 235
Appendix 7ii: Interview topic guide for doctors (In Urdu) .......................................................... 237
Appendix 8: (Study Poster) ......................................................................................................... 239
Appendix 8i: (Study poster in English) ........................................................................................ 239
Appendix 8ii: (Study poster in Urdu) ........................................................................................... 240
Appendix 9i: Patient information sheet (English) ....................................................................... 241
Appendix 9ii: Patient consent form (English).............................................................................. 242
Appendix 10i: Patient information sheet (Urdu) ........................................................................ 244
Appendix 10ii: Patient consent form (Urdu) ............................................................................... 246
Appendix 11i: Doctor information sheet (English)...................................................................... 247
Appendix 11ii: Doctor consent form (English) ............................................................................ 248
Appendix 12: UH ethics approval ................................................................................................ 249
Appendix 13: Permission letters from Pakistan ......................................................................... 251
Appendix 14: The ethics protocol for medically-qualified research student .............................. 253
Appendix 15: A visual mapping to illustrate different concepts and issues emerging from data
.................................................................................................................................................... 254
Appendix 16: Visual representation of various coding steps ...................................................... 255
Appendix 17: Data coding frame ................................................................................................ 256
Appendix 17i: Patients’ coding frame ......................................................................................... 256
Appendix 17ii: Doctors’ coding frame ......................................................................................... 258

11
Chapter 1: Introduction
This dissertation focuses on patient and doctor understandings of hypertension (HTN) and its
management in Pakistan. This chapter introduces HTN and its treatment and then presents
details on the Pakistani context before discussing lifestyle recommendations that are
important for HTN management. The chapter will also describe the prevalence of HTN in Asia
and Pakistan and present the rationale, aim and objectives of the study.
Hypertension (HTN) - or high blood pressure is a chronic medical condition characterised by
an elevated blood pressure in the arteries. Blood pressure is the force of blood that is pushed
against the wall of arteries as it flows through them. The more pressure the blood exerts on
the artery walls the higher blood pressure becomes. Blood pressure is expressed by a
maximum and minimum arterial pressure which is termed as systolic and diastolic pressure.
HTN is defined as systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg
and is diagnosed if the blood pressure is at or above 140/90 mmHg at three consecutive
readings (James et al., 2014). These guidelines regarding HTN diagnosis are proposed by the
British Hypertension Society, the National Institute for Health and Clinical Excellence (NICE),
the International Society of Hypertension and the Sixth Report of Joint National Committee
(6-JNC) (Kjeldsen et al., 2014).
HTN is divided into two types:
• Primary or essential
• Secondary
HTN associated with another medical condition such as heart failure, renal disease or organ
failure is termed as secondary HTN. Effective treatment of secondary HTN often involves
control of both the underlying condition and high blood pressure, which reduces the risk of
serious complications such as kidney failure and stroke (Barrett et al., 2009; Cappuccio &
Miller, 2016). A number of factors such as obesity, high alcohol intake, unhealthy diet, high
salt consumption, smoking and a sedentary lifestyle are responsible for essential or primary
HTN1 (WHO, 2002; Kearney et al., 2005; Dhungana et al., 2016). It is reported that essential
HTN accounts for 95% of all cases of the condition (Staessen et al., 2003; Forouzanfar et al.,
2017) and this is what I will concentrate on in this study.
1 Primary or essential HTN (in contrast to secondary hypertension caused by another disease entity) was defined in the
Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of Hypertension (JNC-7) as a systolic (top) measurement greater than 139 and a diastolic (bottom) measurement greater than 89 (Chobanian, 2003).

12
1.1 HTN and Cardiovascular Disease
Hypertension is a strong and independent risk factor for cardiovascular disease (CVD)
(Franklin & Wong, 2013; Stewart et al., 2017; Kjeldsen, 2018). Evidence shows that HTN is a
silent killer that gradually damages the blood vessels, heart, brain and kidneys if it remains
undetected and untreated (Moore, 2005; Mensah, 2016). Prolonged high blood pressure can
cause long-term morbidity due to CVD and coronary heart disease (Miura et al., 2001; Lawes
et al., 2008; Stevens et al., 2016).
HTN is identified as the third risk factor for disability-adjusted life years and the leading cause
of death worldwide (Chockalingam et al., 2006; WHO, 2011; Bromfield & Muntner, 2013).
According to the World Health Organization (WHO), due to increases in the global population,
the number of people with uncontrolled HTN rose from 600 million in 1980 to nearly 1 billion
in 2008 (WHO, 2013). Likewise, Cappuccio and Miller (2016) highlighted that due to an
increased prevalence of HTN, CVD accounts for approximately 17 million deaths a year
globally and 80% of these deaths occur in low and middle-income countries.
Studies have shown that a reduction in blood pressure lowers the risk of CVD and other
vascular complications such as myocardial infarction, heart failure and kidney disease
(Ibrahim & Damasceno, 2012; Kintscher, 2013; Forouzanfar et al., 2017; Karmali et al., 2018).
Burrows and Muller (2007) have indicated that by controlling high blood pressure, the risk of
stroke can be reduced by 35-40%, the risk of myocardial infarction (heart attack) by 20-25%
and the risk of heart failure reduced by 50%. Therefore, prompt detection and control of high
blood pressure is essential to reduce HTN-related risks for CVD and renal morbidity and
mortality.
1.2 Treatment of HTN
Antihypertensive drugs and lifestyle recommendations are indicated as treatments for all
patients diagnosed with HTN (James et al., 2014). Antihypertensive medication was first used
in the 1960s. This was further encouraged and supported with HTN-related advancements in
the medical industry and as a result of these, the availability of cost-effective antihypertensive
drugs (Saklayen & Deshpande, 2016). The commonly used antihypertensive drugs prescribed
today are effective but also may have adverse side effects such as irregular heartbeat,
headache, muscular weakness and sleep disturbance.
The Joint National Committee on HTN for detection, control and treatment of HTN has also
highlighted that patient non-adherence to hypertensive drug therapy is a major problem in
HTN control (Chobanian et al., 2003; Nguyen et al., 2010). It is therefore important to
understand that compliance to treatment not only involves taking the prescribed drugs but
also adherence to the recommended lifestyle changes which are an essential part of HTN
treatment. It is useful to present details on Pakistan to assist the reader in understanding the
social, cultural and religious context of the country before discussion of HTN and lifestyle
factors that influence the condition.

13
1.3 Pakistani Context
Pakistan is the second largest South Asian country with a population of 156 million and is the
sixth most densely populated country in the world (Anwar et al., 2012; World Development
Indicators, 2013; Cassidy, 2018). The country is surrounded by Iran and Afghanistan to the
west, China to the north, India to the east and the Arabian Sea to the south (Fig 1.1).
Fig 1.1 Map of Pakistan showing boundaries and subdivisions (Wikimedia Commons, 2018)
Pakistan is divided into four provinces, namely: Punjab, Sind, North-West Frontier Province
(NWFP) and Baluchistan. In addition, a large area is federally administered, comprised of the
tribal areas, Northern Areas, Islamabad Capital Territory and the state of Azad Jammu and
Kashmir. At the time of independence, Pakistan and India planned to make Kashmir a
component of their respective unions and the former princely state became a disputed
territory (Sattar, 2003; Bose & Jalal, 2004). Consequently, Pakistan’s relationship with the
neighbouring country India has been beset by hostility and suspicion (Misra, 2010; Kelman et
al., 2018). The national language of Pakistan is Urdu, however, many public officials also speak
English (Khalique, 2007; Bughio, 2014). English is referred to as the informal official language
of Pakistan. While Urdu is common throughout the country, several other languages such as
Punjabi, Sindhi, Pushto, Balochi, Pothwari and Saraiki are also spoken in particular areas
(Malik, 2002; Khalique, 2007; Liljegren & Akhunzada, 2017). The Islamic republic of Pakistan
has a culture that encompasses religion, traditions and norms significant for the people who
live there; Pakistani culture and its social values revolve around the values of Islam (Haleem,
2013; Cassidy, 2018).
Pakistan is a Muslim country and Islam governs the personal and social lives of 97% of the
Pakistani population (Haleem, 2013; Zaman et al., 2018). Pakistani Muslims along with other
Muslim populations believe that Allah is the creator of everything in the universe and has
control over life and death. This concurs with the Islamic view that health can be defined as a
state of physical, psychological, social and spiritual well-being and is perceived as one of the
greatest blessings God has bestowed on humankind (Rassool, 2015). In the Pakistani context,
where religious culture is dominant in society, a tendency towards spirituality is seen as
having an impact on health.
Despite the modernisation of Pakistani society, social norms revolve around the teachings of
Islam and are highly influential in people’s lives (Burki & Ziring, 2017). However, certain norms

14
are interwoven into the culture and people find it difficult to distinguish between the two.
For example, the traditional joint or extended family system is the norm in Pakistan where
people share a common residence and system of mutual obligations (Itrat et al., 2007).
Parents are the most respected family members and serving them is considered a religious
and social obligation for the younger generation, particularly for sons and daughters (Critelli,
2012; Zaman et al., 2018).
Pakistani families are led by a male who makes decisions for the entire family. Women have
clearly defined, largely inflexible roles and constitute only one fourth of the country’s labour
force (Sarwar & Abbasi, 2013). The majority of women are economically dependent on men
and this dependency gives a greater level of control to men over decision-making (Fikree &
Pasha, 2004; Ali et al., 2011). In Pakistani society, women are generally considered to take
responsibility for the household, childcare and are primary carers for elderly family members
(Rabbani et al., 2008; Zarar et al., 2017; Bukhari et al., 2018). A low priority is given to women
in terms of their basic education and health status in rural areas of Pakistan (NIPS, 2008).
Overall, half of the Pakistani population (66%) live in rural areas of the country and poverty
coupled with illiteracy, unpaid jobs and unequal human rights have had a deep impact on
health indicators (WHO, 2007). Every sector of Pakistani society is being affected by poverty,
overpopulation, corruption, nepotism, income inequality, political instability and energy crisis
(Islam, 2004; Niaz, 2010; Anwar et al., 2012). Such a complex and pervasive picture of issues
has not only impacted society but also increased the burden of various health conditions such
as malnutrition in children, high maternal mortality, high neonatal mortality and increased
prevalence of chronic diseases (Shaikh & Hatcher, 2005; Roshan et al., 2018).
1.3.1 An overview of the situation regarding HTN in Pakistan
Pakistan, like many other developing countries is passing through a demographic transition.
The total population of Pakistan is over 156 million and displays one of the worst health
profiles in South Asia, due to a high population growth rate as a result of sustained fertility,
declining mortality and the dual burden of communicable and non-communicable diseases
(Hussain et al, 2009; Wasay & Jabbar, 2009; Anwar et al., 2012). However, according to the
National Health Survey which was conducted through a collaboration of the Pakistan Medical
Council and the Pakistan Federal Bureau of Statistics it was estimated that 18% of adults and
33% of the population above 45 years old had HTN (NHSP, 1998). It has been reported that
HTN prevalence is 22% in the urban Pakistani population and higher than in the rural
population possibly due to sedentary lifestyles (NHSP, 1998; Aziz et al., 2005).
A sedentary lifestyle may be more likely to develop in urban areas due to an extensive use of
automobiles, greater use of computer screens and time spent watching television and a
higher consumption of junk food (Din, 2014). Moreover, urbanisation in Pakistan is occurring
at a rapid rate, which is accompanied by better job availabilities and an improved economy.
Aziz et al. (2005) have also highlighted that factors such as obesity, smoking and sedentary
lifestyles are the main contributors to the increasing prevalence of HTN in Pakistan. By
contrast, another cross-sectional study has shown that inadequate knowledge about the
disease is a factor for uncontrolled HTN in Pakistan (Almas et al., 2012). However, this study

15
has not indicated whether inadequate knowledge about the disease or about treatment
adherence leads to poor control of HTN. Patient perceptions regarding management of HTN
including preventative factors affecting the control of the disease such as diet, exercise and
smoking have not been studied in depth amongst the Pakistani hypertensive population.
According to Saleem et al. (2011) there is inadequate data available on HTN and therefore the
knowledge amongst patients in Pakistan about the disease and its associated risk factors is
limited.
A particular challenge in disease management is related to the delivery of healthcare services
in Pakistan (Saleem et al., 2010; Arshad et al., 2016). The Pakistani public healthcare system
is beset with numerous issues such as structural fragmentation, scarcity of resources,
inefficacy and lack of functional capacity (Shaikh & Hatcher, 2005; Shaikh et al., 2010).
Therefore, it is imperative to understand how the healthcare system is structured in Pakistan.
1.3.2 Healthcare system in Pakistan
The healthcare system in Pakistan comprises of the public and private sector (Ghaffar et al.,
2000). The public healthcare system comprises of primary, secondary and tertiary levels and
every patient is entitled to free healthcare services. The primary level is for the rural
population and consists of Basic and Rural Health Units (BHUs and RHUs). The secondary level
of healthcare consists of Tehsil2 and District Headquarter Hospitals (THQH, DHQH) and
provides diagnostic and preventative care to the urban population. The tertiary level of care
consists of super specialist hospitals associated with medical colleges and provides care to the
urban population.
The nationwide network of health services consists of 4,616 BHUs, 482 RHUs and 796 public
hospitals (Shaikh & Hatcher, 2005; Arshad et al., 2016). However, the utilisation of BHUs is
generally low due to lack of facilities and staff absenteeism (Usman et al., 2015; Shah et al.,
2016). Other than BHUs, some basic health services are also delivered by Lady Health Workers
(LHWs) including child and maternal health-related messages, some medicines such as oral
rehydration salt, and contraceptives. LHWs are attached to the local health facilities (BHUs or
RHUs) from which they receive training and serve the female population (Ejaz et al., 2011;
Wajid et al., 2013). However, due to the absence of supervision and training, LHWs often fail
to guide patients appropriately (Afsar et al., 2003; Arshad et al., 2016).
There is no proper follow-up system available for patients and a vast number of individuals
directly approach the urban hospitals for treatment (Khowaja et al., 2009). As a result, this
increases the workload for the healthcare facility teams in urban hospitals. The private
healthcare is a fee-for-service system and therefore not within the reach of every person. The
private health sector serves 70% of the population through a diverse group of healthcare
team members to provide health services (Shaikh & Hatcher, 2007; Anwar et al, 2012). The
private health sector has demonstrated a great deal of responsiveness in terms of flexible
access, shorter waiting times and understanding patients’ healthcare needs (Irfan & Ijaz,
2 Tehsil is the sub-division of a district.

16
2011; Kumar & Bano, 2017). Yet, the sector is working independently and due to the absence
of any regulatory mechanism, their quality of service is often variable (Shaikh & Hatcher,
2005).
The private sector comprises of regulated hospitals and unregulated hospitals, unregistered
medical doctors and informal healthcare providers such as Hakeem3, Homeopaths,
spiritual/faith healers, Traditional Birth Attendants (TBAs), herbalists and quacks4 (Ejaz et al.,
2011; Arshad et al., 2016; Kumar & Bano, 2017). Most of these informal healthcare providers
are practicing without any formal qualification, training and certification in Pakistan (Shaikh
& Hatcher, 2005). Many efforts have been made by the Ministry of Health to eradicate
uncertified informal healthcare providers and quacks, however, they are still on the rise
(Farmer, 2019).
The healthcare system in Pakistan lacks a Health Management Information System (HMIS) in
the public health sector and has no well-defined policy and plans for technology
implementation and infrastructure development (Punjani et al., 2014; Kurji et al., 2016). The
country failed to achieve the goals of ‘Health for All’ established in the Alma Ata Declaration
and was unsuccessful in attaining Millennium Developmental Goals (MDGs) 2015 (Ali &
Horikoshi 2000; Kurji et al., 2016; Rasanathan et al., 2017). The Ministry of Health failed to
carefully allocate the available resources amongst the rural and urban populations due to
frequently changing authorities and deeply embedded corruption (Gohar Wajid & Al
Massoud, 2002; Khan & Van den Heuvel, 2007). Management responsibilities for healthcare
are divided between the federal, provincial and district governments, however, political
instability and limited administrative authorities have weakened the accountability of
performance and delivery of service (Ali & Horikoshi, 2000; Arshad et al., 2016). Previously,
provincial governments were responsible for health financing but now as a result of political
and administrative decentralisation district governments are empowered as central financial
intermediaries.
A further challenge faced by the healthcare system in Pakistan is in the arena of human
resources. It is estimated that annually 1,000 -1,500 doctors leave the country and only 10-
15% return after spending time abroad (Tahir et al., 2011; Higher Education Commission
Pakistan, 2019). Additionally, medical institutes in Pakistan are not producing sufficient
numbers of doctors to implement the standardised WHO criteria of the doctor-patient ratio
(1:300) in the country (Aly & Taj, 2008; Tahir et al., 2011). There are inadequate opportunities
for doctors in the fields of research, public health and professional development in Pakistan
and this sometimes encourages them to migrate to foreign countries (Shaikh et al., 2010).
Likewise, dentists, nurses and pharmacists are also in insufficient numbers as compared to
the population rate and the existing professionals are often underpaid (Astor et al., 2005;
Talati & Pappas, 2006; Kurji et al., 2016).
3 A person who practices traditional medicine 4 A person claimed to be skilled in medicine but who is not trained

17
The government acknowledges in its National Health Policy (2001) that good governance is
the key to attaining the quality of care, however, the government fails to provide
opportunities for good governance in Pakistan (Khan & Van den Heuvel, 2007; Kumar & Bano,
2017). Although the Ministry of Health has strategised by appointing more doctors, support
staff and increased the medical budgets of the government hospitals, little implementation
of this has been seen to date (Bashrat & Shaikh, 2011; Kurji et al., 2016; Khalid & Abbasi,
2018). The government of Pakistan provides free healthcare to the population although no
attention has been given to monitoring the quality of healthcare services according to
international standards, or to providing patients with a greater awareness of how to control
the burden of HTN. The next section will focus on another aspect of HTN treatment, that of
lifestyle recommendations.
1.4 HTN and Lifestyle Recommendations
Lifestyle recommendations, modifiable risk factors or lifestyle changes, previously termed as
non-pharmacological therapy, play a vital role in better health outcomes in hypertensive and
non-hypertensive individuals (Appel, 2003; Baena et al., 2014; Vamvakis et al., 2017). In
hypertensive patients, lifestyle changes can serve as an initial treatment before the start of
drug therapy and as an adjunct to drug therapy in persons already on medication (Dickinson
et al., 2006; Gupta & Guptha, 2010). Research has shown that lifestyle change is a cornerstone
of HTN management once HTN is first diagnosed, with or without starting antihypertensive
medication (Elhani et al., 2009; Mahmoud, 2012).
Moreover, lifestyle changes have the potential to prevent the onset and lower the risk of HTN-
related cardiac complications (Appel, 2003; Poirier et al., 2006; WHO, 2013). Therefore, it is
imperative to understand that non-adherence with lifestyle recommendations can nullify the
effects of the optimum treatment plan.
1.4.1 Exercise
Regular exercise has been shown to be beneficial for both prevention and treatment of HTN
(Blair et al., 2012; Diaz & Shimbo, 2013; Wasfy & Baggish, 2016; Williams et al., 2018; Rêgo et
al., 2019). Additionally, it has been reported that exercise reduces the risk of cardiovascular
complications and coronary artery disease amongst hypertensive patients (Lee et al., 1997;
Williams, 2001). With specific regard to HTN exercise has been advocated to be beneficial by
a number of organisations including the American College of Sports Medicine, the American
Heart Association, the National Institutes of Health, the Centres for Disease Control and
Prevention and the Surgeon General of the United States (Wallace, 2003).
Evidence supports that exercising as little as (15 minutes) one day per week is effective for
lowering high blood pressure amongst patients (Brown et al., 2013). Hayashi et al. (1999) in a
prospective cohort study found that for every 26.3 Japanese men who walk more than 20
minutes to work, one case of HTN will be prevented. Similarly, meta-analysis of three

18
randomised controlled trial studies have concluded that 30 minutes or less of aerobic exercise
per day lowered blood pressure by 5-6mmHg amongst hypertensive patients (Pescatello et
al., 2004; Cornelissen & Fagard, 2005; Cornelissen & Smart, 2013). Shorter exercise bouts
throughout the day (i.e. 10 minutes to total 30 minutes or more) have appeared to be the
beneficial option amongst hypertensive patients who have a busy routine (Angadi et al., 2010;
Powell et al., 2011; Faselis et al., 2012).
However, exercise carries some risks such as musculoskeletal injury (Hootman et al., 2002)
that increases with type, duration and volume of exercise (Prentice & Voight, 2001; MacAuley
& Best, 2002). The general principle that the volume of exercise should be increased gradually
over time is regarded as critical for reducing injury risk amongst patients (Thompson et al.,
2003; Melzer et al., 2004; Carlin et al., 2016). Walking is suggested as the standard example
of low-risk activity in the literature (Macera et al., 2003; Warburton et al., 2006; Thompson
et al., 2003; Lee & Buchner, 2008; Wolszakiewicz et al., 2015). Nevertheless, from the above-
mentioned studies, it is reasonable to suggest that the risk involved in exercise is outweighed
by its overall benefits in controlling HTN. However, multiple aspects such as duration,
intensity and frequency are important attributes to consider in patients when recommending
exercise (Hootman et al., 2002; Wasay & Baggish, 2016).
1.4.2 Diet
An unhealthy diet is one of the important modifiable risk factors in the development of HTN
(Appel et al., 2006; WHO, 2013; Pilakkadavat & Shaffi, 2016). A healthy diet implies
consumption of fruits, vegetables, whole grains, low-fat dairy products, fish and olive oil or
vegetable oils for cooking and a reduced intake of red meat, saturated fats, hydrogenated fat
and salt (Clark et al., 2011; Olinto et al., 2012). An increasing body of research has examined
the relationship between dietary patterns and the risk of developing HTN using dietary
pattern analysis (Nowson et al., 2004; Shin et al., 2013; Safdar et al., 2015; Zheng et al., 2016).
High intakes of fruits, vegetables, cereals, fish, nuts, low-fat dairy products and poultry in
addition to relatively low intakes of fat and sugars appeared to be effective in lowering blood
pressures and controlling HTN (Lee at al., 2010; Shin et al., 2013; Chiu et al., 2016).
Since HTN is a cardiovascular disease risk factor, several prospective cohort studies in a range
of populations have shown associations between unhealthy dietary patterns and CVD
(Landray et al., 2002; Shimazu et al., 2007; Shin et al., 2013). It has been suggested that a diet
rich in saturated fats is considered an important risk factor for developing HTN and CVD
(Azadbakht et al., 2007; Nettleton et al., 2017). Straznicky et al. (1993) for example, reported
increased blood pressure and heart rate in healthy participants after consuming a high-fat
diet compared with a low-fat diet in a two weeks crossover study. In a seminal study, Jakulj
et al. (2007) found that systolic and diastolic blood pressure was high in participants following
the consumption of a high-fat meal relative to a low-fat meal. Some researchers have
particularly focused on the effect of the intake of individual foods and nutrients in developing
HTN (Appel 2003; Appel et al., 2005; Shimazu et al., 2007; Zheng et al., 2016).

19
However, due to the complex nature of the relationship between diet and pathology with
specific regard to HTN it is not possible to ascribe this to a single food or nutrient but rather
to a mix of multiple foods and nutrients (Wang et al., 2010). Furthermore, studies (Wang et
al., 2008; Sacks & Campos, 2010) evaluating the risk posed by a single nutrient for HTN do not
allow one to consider the effect of the diet as a whole due to the collinearity of nutrients
within foods. Therefore, this creates difficulty in detecting smaller effects of individual foods
and nutrients on disease outcome. For example, in the European Prospective Investigation
into Cancer and Nutrition (EPIC)-Potsdam Study of 8,552 hypertensive women, no significant
difference was found between fat versus sugary dietary patterns and HTN (Schulze et al.,
2003). It might be possible that certain factors such as regular exercise had reduced the
effects of high fat and sugar intake amongst patients, however, the study failed to provide
further information.
1.4.3 High salt consumption
The amount of dietary salt consumed is an important determinant of blood pressure levels
and constitutes a risk factor for HTN (Conlin, 2007; He & MacGregor, 2009; Rasheed et al.,
2014). A daily intake of less than 2 grams of sodium per person is recommended by the World
Health Organization (WHO) to reduce the risk of developing HTN (WHO, 2007). Numerous
experimental and observational studies have confirmed the association of high salt
consumption with HTN (Michael, 2002; Gu et al., 2008; Alderman & Cohen, 2012; Yuan et al.,
2016; Chrysant, 2016).
A subsequent study by The Trials of Hypertension Prevention Collaborative Research Group
has identified that reduced sodium intake lowers blood pressure in addition to the possible
reduction of long-term cardiovascular events (Cook et al., 2007). Similarly, some clinical trials
and population-based studies have shown that reducing salt intake at the population-level is
associated with a reduction in rates of HTN and that such strategies are cost effective in
managing HTN (Asaria et al., 2007; Strazzullo et al., 2009; Miura et al., 2001; He & MacGregor,
2013). Given the adverse impact of excessive salt consumption on health and particularly on
blood pressure levels and CVD, WHO has urged nations to take action to reduce population-
wide wide dietary salt intake to decrease the number of deaths from HTN and CVD (He &
MacGregor, 2009; Ha, 2014).
1.4.4 Smoking
Smoking is considered one of the important causes of HTN and developing CVD amongst
patients (NICE, 2011; Gao et al., 2017; WHO, 2019). Tobacco contains nicotine, a powerful
addictive drug and tar-a carcinogenic agent, whilst carbon monoxide decreases oxygen supply
to the body, all of which, increases heart rate and blood pressure (Le Moal & Koob, 2007;
Farsalinos et al., 2016). Nicotine acts as an addictive substance and can produce toxic effects
on the cardiovascular system (Carpenter et al., 2007; Mishra et al., 2015). Evidence supports
that cigarette smoking causes various adverse cardiovascular events and increases the risk of

20
coronary artery disease (Ohira & Iso, 2013; Kim et al., 2016; Omboni et al., 2016). A
randomised controlled trial in urban areas of Pakistan found that the prevalence of multiple
CVD risk factors are present amongst smoker hypertensive patients and they were at high risk
of developing CVD mortality (Qamar et al., 2008). Similar results have been shown in a
systematic review in Iran that found smoking as the most common risk factor for developing
CVD amongst patients (Mohseni et al., 2017).
It has been reported that hypertensive patients who smoke develop a severe form of high
blood pressure called malignant HTN which causes organ damage (Mensah et al., 2003; Addo
et al., 2009; Virdis et al., 2010). A 14-year longitudinal cohort study in Japanese males has
revealed that smoking is independently related to the onset of HTN (Suwazono et al., 2008).
On the other hand, a cross-sectional study conducted in Iran evaluated that a high prevalence
of HTN was associated with increased consumption of cigarettes and that this in turn
decreased the effectiveness of HTN medication (Abtahi et al., 2011). Similar results have been
found in a prospective study that identified that cigarette smoking reduces the effects of
antihypertensive drugs in hypertensive patients due to the presence of nicotine metabolites
in the blood of smokers (Matsui et al., 2005). Furthermore, in some cross-sectional studies,
the amount of cigarette smoking is correlated to the stage and frequency of the increase in
blood pressure (Okubo et al., 2002; Okubo et al., 2004; Thuy et al., 2010; Li et al., 2017; Wu
et al., 2018).
Smoking cessation improves overall health and reduces the risk of heart disease and stroke,
however, the risk for CVD remains elevated for approximately a decade after discontinuation
(Burns, 2003; Buttar et al., 2005). For example, Wiggers et al. (2003) highlighted that after
one year of smoking cessation, the risk of CVD may be reduced by greater than 50% and within
several years of discontinuation the risk returns to that of life-long abstainers. However,
sustained health benefits and a decrease in blood pressure can be achieved by quitting
smoking as the results of above-mentioned studies suggest. Thus, like other lifestyle changes,
it is critical that people with raised blood pressure are advised to stop smoking for good health
outcomes and controlled blood pressure.
1.4.5 High alcohol intake
There is a general consensus on the detrimental effects of heavy alcohol consumption on
blood pressure (Fuchs et al., 2001; Panagiotakos et al., 2007; Jaubert et al., 2014). There have
been some systematic reviews and meta-analyses of studies that show the association
between consumption of alcohol and aggregated cardiovascular disease (Chen et al., 2008;
Brien et al., 2011; Fernández-Solà, 2015). A positive association between alcohol consumption
and increased blood pressure has been described in a number of population studies (Fuchs et
al., 2001; Nakanishi et al., 2001; Skliros et al., 2012; Cho et al., 2015; Kwon et al., 2016).
According to the quantity of alcohol intake, the alcohol consumption can be classified into
light to moderate (≤2 drinks/day, 30ml ethanol) and excessive (≤3 drinks/day, 45ml ethanol)
alcohol consumption (Abel et al., 1998; Brenner et al., 2017). Similarly, four cross-sectional

21
and prospective studies have revealed the deleterious effect of higher alcohol consumption
on HTN prevalence (Nakanishi et al., 2001; Ohmori et al., 2002; Klatsky, 2004; Saremi et al.,
2004). A meta-analysis of 15 randomised controlled trials in which the only intervention was
alcohol reduction between the active and control groups stated that a reduction in alcohol
consumption lowered systolic and diastolic blood pressure (Xin et al., 2001).
Although heavy alcohol consumption has been clearly associated with increased blood
pressure, the effects of light-to-moderate alcohol consumption on blood pressure are still
controversial with conflicting results obtained in different populations (Wakabayashi, 2008;
Cho et al., 2015). Some authors have speculated that ingestion of smaller quantities of alcohol
may reduce blood pressure (Okubo et al., 2001; Sesso et al., 2008; Bello et al., 2010). In
contrast, a study that examined the risk of cardiovascular sequelae separately in heavy
drinkers, light drinkers and abstainers found that negative outcomes were progressively
higher for increasing blood pressure across all alcohol consumption categories (Klatsky et al.,
2006). This indicates that the negative effects of alcohol truly matter for hypertensive patients
and therefore a patient with HTN who is a light, moderate or heavy drinker should be strongly
motivated to reduce his or her alcohol intake in order to control HTN. The results of the above-
mentioned studies clearly show that lifestyle interventions help to control HTN, and, if
adopted can reduce the need for drug therapy and favourably decrease the risk of developing
cardiovascular risk.
Particular attention has been paid to lifestyle recommendations and treatment compliance in
developed countries (Middleton et al., 2013; Modesti et al., 2015; Zhou et al., 2017).
However, almost three-quarters of people with HTN (639 million people) live in developing
countries (Chockalingam et al., 2006; Zhao et al., 2012). Kearney et al. (2005) reported that
the prevalence of HTN is increasing in developing countries and is predicted to grow by more
than 500 million in 2025. According to Ibrahim and Damasceno (2012), developing countries
in South Asia are experiencing an 'epidemiologic transition' in which the causes of death are
shifting from primarily infectious diseases to non-communicable diseases. The concomitant
decline of infectious diseases has enhanced the proportional disease burden due to increase
in diseases such as HTN and subsequent CVD.
1.5 Rationale for the Study
HTN is a global public health problem and is identified as the third most common risk factor
for disability-adjusted life years (WHO, 2002; Chockalingam et al., 2006; Kearney et al., 2005;
Murray et al., 2007; Forouzanfar et al., 2017). HTN causes 7.5 million deaths and accounts for
57 million Disability Adjusted Life Years (DALYs) worldwide (Danaei et al., 2011; Mohan et al.,
2013; WHO, 2014). The high prevalence of HTN and inadequate blood pressure control has
challenged public health around the world. The prevalence of HTN is very high in the South
East Asian Region and one out of three adults is affected by it (Neupane et al., 2014; Castillo,
2016; Beaney et al., 2018).

22
As highlighted earlier (section 1.3.1), Pakistan is facing a double burden of disease and as a
result of this, the burden of non-communicable chronic diseases such as HTN, heart disease
and diabetes are rising sharply. It has been reported that chronic diseases are projected to
account for 42% of all deaths in Pakistan and one in four adults over the age of 18 years is
hypertensive (Jafar et al., 2013; Vos et al., 2016; WHO, 2019). The National Health Survey of
Pakistan (NHSP) reported that only 50% of the individuals with HTN in Pakistan are diagnosed
with the condition and only half of those diagnosed are ever treated (Saleem et al., 2010;
Chow et al., 2013; Shafi & Shafi, 2017; Mehmood et al., 2018).
The duration of chronic diseases such as HTN can have a major influence on the individual
experience of disease management as well as on individual functional capacity5 (Bhatti et al.,
2011; Megari, 2013; Sharman et al., 2015; McPhail, 2016). The central characteristics of most
chronic conditions are that these are often permanent, progressive and can be debilitating.
However, chronic conditions such as HTN can be stabilised with an effective management
regime (Kim et al., 2015; Williams et al., 2018). HTN is one of the most preventable causes of
premature morbidity and mortality (Kearney et al., 2005; Pereira et al., 2009; Mills et al.,
2016) and its prevention is the common intervention (WHO, 2002; Vamvakis et al., 2017).
Moreover, morbidity, early deaths, medical care expenditures due to high blood pressure all
take their toll on families, communities and the national budget.
The loss of income due to living with a life-long chronic disease such as HTN-related morbidity
can be devastating not only for families but also leads to health inequalities due to poverty
(Singer & Clair, 2003; Vellakkal et al., 2015; Mendenhall et al., 2017). Thus, there is a
significant economic cost attached to lack of early detection, inadequate treatment and poor
control of blood pressure. Early detection, improving treatment adherence and management
of HTN could decrease the premature mortality (due to complications) leading to improved
health, well-being and economic improvement (James et al., 2014; Kuate Defo et al., 2017).
One major reason for the high rate of uncontrolled HTN is linked to patients’ suboptimal
treatment adherence in Pakistan (Saleem et al., 2011; Almas et al., 2012; Shafi & Shafi, 2017).
Another possible unexplored reason for the lack of effectiveness of HTN control in Pakistan
may be lack of doctors’ understanding of patient beliefs about HTN. Doctors play an important
role in helping patients to manage their HTN (Schroeder et al., 2004; Chung et al., 2008; Hill
et al., 2010; Kronish et al., 2012; Rahman et al., 2015). For instance, they can improve
adherence to antihypertensive medications by prescribing a simple medication regime and
can positively impact patients’ management through understanding their patients’ beliefs.
However, doctors might assess a patient informed by their beliefs, knowledge, previous
experience and disease signs without taking accounts of patients’ personal or social values
and experiences (Prior, 2003; Bramley & Matiti, 2014; Kennedy et al., 2017). Evidence
supports that the perspectives of patients are often very different from those of doctors and
are highly influenced by contextual factors (Epstein & Street, 2011; Marshall et al., 2012;
5 An individual capacity to function effectively.
23
Rahman et al., 2015; Telfer, 2018; Lang et al., 2018). If these differences remain
unacknowledged it can cause misunderstandings, bias decision-making and get in the way of
the specific health needs of patients.
In Pakistan, there is a paucity of qualitative data focusing on patients’ and doctors’
understanding of HTN and its treatment. Qualitative studies that explore the detailed
perceptions of patients regarding all aspects of HTN by taking account of socio-cultural
context are limited. Likewise, doctors’ understanding of HTN as a condition and issues
influencing its treatment have been inadequately reported. Moreover, the existing research
does not go far enough to explain how patients’ and doctors’ viewpoints may lead to
unrealistic expectations with regard to disease management. The gap between doctors’ and
patients’ common understanding of HTN may be especially large in public urban hospitals
where the workload for doctors is quite high. Hence to fill this gap and to elicit patients’ and
doctors’ perspectives about all aspects of HTN management and to address what may
contribute to a greater understanding of patients’ beliefs, an in-depth qualitative study is
required.
Research and evidence-informed policymaking is scant in Pakistan (Tarin et al., 2009; Jooma
& Sabatinelli, 2014; Zaidi et al., 2019). The findings of the current study will therefore
contribute to the existing evidence on the understandings of two main stakeholders (patients
and their doctors) about HTN management in Pakistan. Not only will this improve
understanding of HTN beliefs and attitudes in Pakistan, but it will better inform policymakers
and inform future culturally sensitive awareness campaigns. The findings will highlight the
similarities and differences in patients’ views, compared with those of doctors and identify
any misperceptions that could be addressed when designing interventions for HTN control in
Pakistan.
1.6 Research Question, Aim and Objectives of the Study
Research Question
What are patients’ and doctors’ perceptions, attitudes and beliefs regarding HTN and its
treatment in urban areas of Pakistan?
Aim
This study aims to explore the perceptions, attitudes and beliefs of patients and their doctors
regarding HTN and its treatment in urban areas of Pakistan.
Objectives
• To examine what is already known about patients’ and doctors’ understandings of
HTN and its treatment in urban areas of Pakistan.
• To elicit hypertensive patients’ perceptions, attitudes and beliefs regarding HTN and
its medical and lifestyle management in urban areas of Pakistan.

24
• To elicit doctors’ perceptions, attitudes and beliefs regarding HTN and its medical and
lifestyle management in urban areas of Pakistan.
1.7 Structure of the Dissertation
This dissertation is divided into six chapters. Chapter two presents a systematic review and
critically appraises the existing literature from Pakistan to address the first study objective.
The chapter then discusses the broader literature around health beliefs followed by patients’
and doctors’ beliefs about HTN and its management, which informs the study’s conceptual
framework.
Chapter three outlines the methodological approaches used in the study and justifies the
rationale for their use. The data collection tools, recruitment of study participants and how
data were collected are explained. Translation, transcription and steps of data analysis used
for the study are discussed in detail. Finally, the chapter presents a reflection on the research
journey of the author.
The first of two findings chapters (chapter four), then presents the study findings related to
patients’ perceptions of HTN and their attitudes and approach towards HTN treatment.
Chapter five presents study findings regarding doctors’ perceptions about HTN, its treatment
and the contextual factors considered to influence the adoption of lifestyle changes by
patients.
Chapter six provides a discussion of the key findings that arose from the study in relation to
other available evidence and in line with the study’s conceptual framework that focuses on
health beliefs. The chapter also describes possible implications for practice and policy arising
from the study and offers suggestions for future research and a reflection on the strengths
and limitations of the study. The dissertation concludes by summarising the study’s
contribution to knowledge regarding HTN and its management in Pakistan.

25
Chapter 2: Literature Review
This chapter is divided into two main parts. To address the first study objective, the systematic
review examines the existing body of knowledge on HTN understanding amongst patients and
doctors in Pakistan. The first section (2.1) begins by providing the rationale for carrying out a
systematic review and the second section (2.2) describes the review protocol, tools and
inclusion criteria used to identify relevant studies. Section 2.3 will provide a critique of the
studies from Pakistan identified in this review. The next two sections (2.4) and (2.5) will
present the themes that emerged from the review related to patients’ and doctors’
understanding about HTN and the gaps identified in the literature are discussed in section
2.6. The second part of the chapter (2.7) sets out a review of the literature covering a broader
range of areas that provided a conceptual framework for this study.
2.1 Rationale for Systematic Review
A systematic literature review is a means of identifying, evaluating and interpreting all
available research relevant to a research question, topic area or phenomenon of interest
(Petticrew & Roberts, 2008; Boland et al., 2013). The systematic review includes a critical
synthesis of research evidence that involves analysis of all available and relevant evidence in
a systematic, objective and robust manner (Bruce & Mollison, 2004; Smith & Noble, 2016).
Therefore, in the hierarchy of evidence-based medicine, systematic reviews are considered
the best method for identifying existing evidence (Aslam & Emmanuel, 2010).
The common reasons for undertaking a systematic review are:
• To summarise the existing evidence based on the review question.
• To identify any gaps in current research and suggest areas for further investigation.
• To provide a background to appropriately position new research activities
(Gopalakrishnan & Ganeshkumar, 2013).
One of the study objectives was to examine what is already known about the understanding
of patients and doctors regarding HTN and its treatment in Pakistan. Therefore, the purpose
of this review is to identify the primary studies relevant to the review question, critically
appraise and assess methodological limitations of the available studies, highlight the
emerging themes and identify the gaps in literature to guide the inquiry. In systematic review,
reviewers follow a strict protocol to ensure that the review process undertaken is transparent
with minimum bias or errors (Holly et al., 2012; Charrois, 2015). Reviewers start by defining a
review protocol that specifies the research question being addressed and inclusion/exclusion
criteria to assess each potential primary study. Therefore, the following section will present
the review protocol used in this study.
2.2 The Review Protocol
The first step during this review was to formulate a clear question: what is known about
patients’ and doctors’ understanding of HTN and its treatment in Pakistan?
26
Following formulation of the research question, a search strategy was planned. Inclusion and
exclusion criteria were set, terms and key words were developed, and relevant databases
identified.
2.2.1 Inclusion and exclusion criteria
Inclusion criteria for the review were as follows:
• Studies must contain data on hypertension and its treatment in a Pakistani population
• Studies must be conducted in Pakistan
• Studies must be primary research studies
• Studies must be published from 1990 to 2019
The exclusion criteria were applied as follows: ‘not about HTN’, ‘not in Pakistan’, ‘not a
primary study’. Pakistani journals are written in English and therefore searches were not
conducted in other languages.
2.2.2 Search strategy
The databases searched were Global Health, Medline and Scopus. Global Health is a
specialized public health database that contains details of international health research and
literature mainly from developing countries that is not covered by other databases. Medline
provides biomedical literature from a range of sources, covers 4,800 journals and contains
information of relevance to healthcare providers and researchers. Scopus is a bibliographic
database which includes citations and abstracts for academic journal articles within the field
of the social sciences.
In addition, the following extensive lateral search techniques were also used:
• Scanning reference lists of relevant articles
• Searching of grey literature (for example, WHO, Health Department of Pakistan,
National Institute of Health Pakistan, Pakistan Hypertension League, Health Services
Academy, Pakistan)
The following terms and key words were searched using Boolean operators: (Hypertension*
OR High blood pressure) AND (Understanding* OR Perception* OR Belief* View* OR
Interpretation*) AND (Patient*) AND (Doctor* OR Medical Practitioner) AND (Treatment* OR
Therapy* OR *Management) AND (Pakistan* OR South Asia*).
Literature was searched from 1990 onwards as the National Health Survey of Pakistan (NHSP)
conducted during 1990-94 reported high rates of HTN prevalence in Pakistan. Prior to this
there was no national data on the prevalence of HTN in Pakistan (Shafi & Shafi, 2017). The
titles and abstracts of the papers identified were screened against the inclusion and exclusion
criteria. Full papers of potentially relevant articles were then obtained and further screening
excluded papers that did not fit. A complete search strategy for the literature review with a
PRISMA style flow diagram has been included to present how the selected studies were
screened and identified (see Appendix 1). A table of included studies detailing the authors,
aim, method, sample, location and key findings is listed in Table 2.1 (see Appendix 2).

27
A data extraction tool was developed based on the Centre for Review and Dissemination
(2008) guidelines and used to retrieve necessary information about study characteristics and
findings. The data extraction headings were as follows: author(s), year of publication, journal,
article title, study aim and objectives, research question, study design, sampling method,
sample information, sample size, data collection method, data analysis, key results, study
limitations and conclusions.
Following data extraction, the methodological quality and rigour of the included studies was
assessed by using The Critical Appraisal Skills Programme (CASP) quality assessment tool for
qualitative studies and the National Heart, Lung and Blood Institute (NHLBI) quality
assessment tool for cross-sectional studies (NHLBI, 2017; CASP, 2018). These tools are widely
used for assessment of the methodological quality of qualitative and cross-sectional studies
in systematic reviews (Wardle & Roseen, 2014; Koppen et al., 2016; Smith & Noble, 2016;
Rosário et al., 2018). An appraisal checklist by using CASP and NHLBI quality assessment tools
to appraise the selected studies has been attached (see Appendix 3i and 3ii).
2.3 Results from the Review
A total of 21 studies (Appendix 1) that met the inclusion criteria are included in the review
(Jafar et al., 2005; Almas et al., 2006; Ashfaq et al., 2007; Hashmi et al., 2007; Ahmed et al.,
2008; Ladha et al., 2009; Rehman et al. 2011; Saleem et al., 2011; Almas et al., 2012; Saleem
et al., 2012; Aslam et al., 2013; Khan et al., 2014; Bilal et al., 2015; Hussain et al., 2015; Khan
et al., 2015; Gowani et al., 2016; Qamar et al., 2016; Malik et al., 2016; Ishtiaq et al., 2017;
Murad et al., 2017; Legido-Quigley et al., 2019).
2.3.1 Analysis of included studies
The review identified four qualitative studies that were related to patients’ views of HTN
treatment and management in Pakistan (Saleem et al., 2011; Saleem et al., 2012; Gowani et
al., 2016; Legido-Quigley et al., 2019). Of these four studies, two were carried out in Quetta
(Saleem et al., 2011; Saleem et al., 2012) capital and the largest city of Baluchistan, and two
conducted in two cities of the Pakistani province Sindh (Gowani et al., 2016; Legido-Quigley
et al., 2019). All four studies were published between 2011 and 2019 in peer-reviewed
journals and used semi-structured interviews or focus group discussions.
For the four qualitative studies, the quality score ranged from 5-7. The quality score for the
Legido-Quigley et al. (2019) study was seven and the highest amongst all the studies due to
reliability and the use of appropriate qualitative methodology. Legido-Quigley et al. (2019)
captured the views of hypertensive patients (n=60) living in rural areas of three South Asian
countries (Bangladesh, Pakistan, Sri-Lanka). However, a limitation of the Legido-Quigley et al.
(2019) study was a failure to provide justification of inclusion criteria used for the study
participants and not reporting information about the exclusion criteria. Likewise, Gowani et
al. (2016) did not report justification for the inclusion criteria used and failed to describe the
exclusion criteria for the study sample. In two qualitative studies (Saleem et al., 2011; Saleem
et al., 2012) researchers did not describe their qualitative data analysis methods and
therefore it is difficult to verify how robust the analysis of the data was. In general, the four

28
qualitative studies (Saleem et al., 2011; Saleem et al., 2012; Gowani et al., 2016; Legido-
Quigley et al., 2019) clearly reported their study aims and gave adequate descriptions of data
collection methods, however, except for the Legido-Quigley et al. (2019) study there was no
evidence of using a conceptual framework, justification of research design, triangulation and
consideration of potential bias.
Seventeen studies were cross-sectional surveys (Jafar et al., 2005; Almas et al., 2006; Ashfaq
et al., 2007; Ahmed et al., 2008; Ladha et al., 2009; Rehman et al., 2011; Almas et al., 2012;
Aslam et al., 2013; Khan et al., 2014; Bilal et al., 2015; Hussain et al., 2015; Khan et al., 2015;
Qamar et al., 2016; Malik et al., 2016; Hashmi et al., 2017; Ishtiaq et al., 2017; Murad et al.,
2017) in which 13 studies identified hypertensive patients’ understanding of HTN treatment
and adherence (Almas et al., 2006; Ashfaq et al., 2007; Ahmed et al., 2008; Ladha et al., 2009;
Almas et al., 2012; Aslam et al., 2013; Khan et al., 2014; Bilal et al., 2015; Khan et al., 2015;
Qamar et al., 2016; Hashmi et al., 2017; Ishtiaq et al., 2017; Murad et al., 2017) and four
provided details about doctors’ attitudes regarding adherence to HTN treatment guidelines
(Jafar et al., 2005; Rehman et al., 2011; Hussain et al., 2015; Malik et al., 2016). The overall
quality of patient focused cross-sectional studies was ‘poor’ using the NHLBI quality
assessment tool whilst two studies (Hussain et al., 2011; Malik et al., 2016) based on doctors’
awareness of HTN treatment guidelines were rated ‘fair’ and ‘good’, respectively.
Out of 17 cross-sectional studies, 12 were conducted in one city (Karachi), while five studies
took place in other Pakistani cities: Abbottabad (Ahmed et al., 2008), Peshawar (Khan et al.,
2015), Rawalpindi and Islamabad (Malik et al., 2016; Ishtiaq et al., 2017) and one in multiple
locations in rural Punjab and Sindh (Jafar et al., 2005). All the studies had an observational,
cross-sectional study design, used questionnaires as their measuring tool and were published
between 2005-2017. 10 studies (Jafar et al., 2005; Ashfaq et al., 2007; Hashmi et al., 2007;
Rehman et al., 2011; Almas et al., 2012; Khan et al., 2014; Hussain et al., 2015; Khan et al.,
2015; Bilal et al., 2015; Malik et al., 2016) piloted their data collection tool and tested it for
validity.
The survey duration was specified by 13 papers and varied considerably. Survey durations
were one month (Murad et al., 2017), six weeks (Ladha et al., 2009), three months (Rehman
et al., 2011; Khan et al., 2014; Hussain et al., 2015; Malik et al., 2016), six months (Ahmed et
al., 2008; Ishtiaq et al., 2017), eight months (Bilal et al., 2015), nine months, (Hashmi et al.,
2007), one year (Almas et al., 2006; Almas et al., 2012) and 18 months (Aslam et al., 2013).
Four studies (Jafar et al., 2005; Ashfaq et al., 2007; Khan et al., 2015; Qamar et al., 2016) failed
to indicate their study period. Study sample size ranged from 16-447 for patients and 100-
1,000 for doctors. Two studies (Aslam et al., 2013; Hussain et al., 2015) failed to provide
details regarding the sampling criteria used.
The age of the patient participants was recorded in only nine of the studies focusing on
patients (Almas et al., 2006; Ashfaq et al., 2007; Hashmi et al., 2007; Ahmed et al., 2008; Ladha
et al., 2009; Almas et al., 2012; Khan et al., 2014; Ishtiaq et al., 2017; Murad et al., 2017). In
the majority of these studies, the age range of patients was between 20 and 60 years, whereas
in only one study (Ladha et al., 2009) the recruited patients were older, aged 65 years and
above. The gender ratio of the participants was not mentioned in three studies (Rehman et

29
al., 2011; Aslam et al., 2013; Hussain et al., 2015). Out of the other 14 studies, eight studies
(Jafar et al., 2005; Almas et al., 2006; Ladha et al., 2009; Almas et al., 2012; Khan et al., 2014;
Khan et al., 2015; Malik et al., 2016; Murad et al., 2017) had a male ratio comparatively high
to female participants. In five studies, the female ratio was higher as compared to male
participants (Ashfaq et al., 2007; Hashmi et al., 2007; Ahmed et al., 2008; Bilal et al., 2015;
Ishtiaq et al., 2017) and in one study the gender ratio was equal (Qamar et al., 2016). Five
studies did not report whether or how informed consent was sought (Ashfaq et al., 2007;
Aslam et al., 2013; Hussain et al., 2015; Khan et al., 2015; Qamar et al., 2016) and three studies
(Ashfaq et al., 2007; Bilal et al., 2015; Khan et al., 2015) did not provide information regarding
permission from the respective hospitals to conduct the study.
From analysis of the selected studies and assessment of their quality it is evident that this
review identified studies with methodological limitations as well as imprecision in the
reporting of results. Details regarding eligibility criteria, informed consent, ethics approval
and data analysis procedures were inconsistent. Only four studies collected data qualitatively
and two qualitative studies failed to mention their analytical procedures which increases
doubts about the interpretation of the results. None of the reviewed qualitative studies
addressed doctors’ views of HTN and its treatment. Another surprising observation was that
most of the findings are from studies conducted in one city (Karachi) and provinces other than
Punjab. This represents a potentially significant threat to external validity as Punjab is the
most populated province of Pakistan.
The next two sections will present the findings in relation to the review question. Section 2.4
explores the body of literature related to the understanding of patients regarding HTN and its
treatment as identified in the reviewed studies. Section 2.5 will look at doctors’ understanding
of HTN treatment in Pakistan.
2.4 Patients’ Understanding of HTN and its Treatment
The following section presents findings from the review about patients’ understanding of
HTN, symptoms and treatment in Pakistan.
2.4.1 Understanding of HTN
Only five out of 21 studies collected information on patients’ understanding of HTN (Saleem
et al., 2012; Khan et al., 2015; Qamar et al., 2016; Ashfaq et al., 2017; Legido-Quigley et al.,
2019). The parameters highlighted in four studies which related to HTN understanding
amongst patients included blood pressure monitoring and the appearance of symptoms. For
example, Saleem et al. (2012) in a qualitative study interviewed 16 patients (male 12; female
4) and showed that understanding of HTN and its treatment was particularly dependent on
blood pressure monitoring and clinical symptoms amongst patients.
By using semi-structured interviews in a qualitative study carried out in three Asian countries
(Pakistan, Sri-Lanka, Bangladesh), Legido-Quigley et al. (2019) found that the appearance of
physical symptoms made participants aware of the disease. Symptoms such as a headache, a
general feeling of weakness, shortness of breath, dizziness and palpitations were identified
amongst hypertensive patients. Participants indicated that these symptoms were mild to

30
moderate in intensity and therefore they only sought care in the health facility when they
experienced such symptoms. This finding is consistent with a survey conducted in the same
city (Karachi) involving 200 hypertensive patients (male 100; female 100), which identified
that physical symptoms such as a headache, blurred vision and chest pain were considered
common indicators of high blood pressure amongst patients (Qamar et al., 2016).
A contrasting description can be found in a cross-sectional survey study (n=298) that was
conducted to identify primary causes of HTN amongst hypertensive patients (male 172;
female 126) in Peshawar (Khan et al., 2015). Researchers in this survey reported that 90% of
the patients stated HTN is a serious disease and that most patients were conscious of the
asymptomatic nature of HTN, conversely, 25% of the sampled participants did not consider
HTN a dangerous disease. The common reason for considering HTN less serious amongst
these patients was the belief that HTN is not a major cause of mortality. Ashfaq et al. (2007)
however, noted that 80% of patients attending tertiary care hospitals believed that HTN could
lead to CVD, whereas 58% attending primary healthcare centres considered HTN a risk factor
to heart disease. This cross-sectional survey (n=202) was conducted to compare the
awareness of HTN amongst patients attending primary healthcare centres and the outpatient
department (OPD) of a tertiary care hospital in Karachi. Researchers in this survey further
noted that 47% of patients in tertiary healthcare and 79% in primary healthcare did not know
about the readings at which blood pressure was considered high. Across five studies (Saleem
et al., 2012; Khan et al., 2015; Qamar et al., 2016; Ashfaq et al., 2017; Legido-Quigley et al.,
2019) that explored patients’ understandings of HTN, none of the studies included questions
to explore how patients define HTN or what meanings they associate with increased blood
pressure.
The review identified only two studies conducted in tertiary care hospitals (in Karachi) that
were able to provide data regarding patients’ understanding of HTN diagnosis (Hashmi et al.,
2007; Gowani et al., 2016). Hashmi et al. (2007) in a descriptive cross-sectional survey
recruited 438 hypertensive patients at two tertiary care hospitals to identify patients’
experiences of HTN and factors associated with treatment adherence. Researchers in this
survey reported that patients (70.8%) discovered they had HTN accidentally during a medical
check-up for symptoms related to HTN and its complications (Hashmi et al., 2007). In contrast,
Gowani et al. (2016) in a qualitative study that involved four focus group discussions with 30
participants at one tertiary care hospital found that patients’ diagnosis of a disease was often
a result of an acute medical event (such as myocardial Infarction or stroke). In focus group
discussions with 20 patients, researchers in this study found that patients identified HTN
when symptoms appeared or when they sought help for some other medical condition.
In the included studies on patients’ perspectives on HTN, some pointed to primary causes and
exacerbating factors for HTN. Studies related to this aspect are presented below.
2.4.2 Causes of HTN
Four studies included in the review that looked at hypertensive patients’ awareness have
reported a few factors linked to disease causes amongst participants (Aslam et al., 2013; Khan
et al., 2015; Gowani et al., 2016; Legido-Quigley et al., 2019). Two studies highlighted that

31
patients were believed to be susceptible to HTN due to genetic background and reported
positive family history as a cause for their disease (Khan et al., 2015; Gowani et al., 2016).
Participants who have had any other family member suffering from the disease had insight
that they were more likely to encounter HTN. Gowani et al. (2016) by using a semi-structured
topic guide with 30 participants in four focus group discussions highlighted that living an
unhealthy lifestyle was also recognised as a cause of HTN amongst patients.
In contrast to Gowani et al., (2016) two studies mentioned how patients attributed personal
stress and anxiety as a significant cause of their elevated blood pressure (Khan et al., 2015;
Legido-Quigley et al., 2019). Khan et al. (2015) exclusively focused on identifying factors that
led to HTN at the individual level. These included depression and anxiety (95%), lack of
exercise (71%), cigarette smoking (63%) and heavy alcohol intake (59%) and were seen as
contributing to increased blood pressure. Participants in this cross-sectional study strongly
associated stress and anxiety with HTN, both as an exacerbating factor and a consequence.
However, Khan et al. (2015) failed to provide sufficient detail on the factors responsible for
patients’ stress and anxiety. They did not comment on whether stress was due to the patients’
inability to perform daily activities as a result of the severity of their HTN symptoms or caused
by financial problems.
Aslam et al. (2013) conducted a cross-sectional study (n=176) over the duration of 18 months
to find out the prevalence of HTN and stress in four socioeconomic classes (lower class, lower
middle class, upper middle class, and higher class). The researchers found that levels of stress
increased consistently with deteriorating socioeconomic status and stress was observed to be
the highest in people living below the poverty line. Out of 54 participants of a higher class,
nine (16%) had high, 40 (74.1%) had moderate and five (9.3%) had a low risk of developing
stress (p <0.010) and on examination 15 (27.8%) people were identified to be hypertensive (p
<0.642). Of the group living below the poverty line, out of 44 participants 16 (36.4%) had high,
26 (59.1 %) had moderate and two (4.5%) had a low risk of developing stress (p <0.010) and
eight (18.2%) individuals were found to be hypertensive (p <0.642). Aslam et al. (2013) noted
a major difference between two social class (higher upper and lower class) groups and
reported that the higher upper class had the least likelihood of developing stress (16.7%)
whereas patients living below the poverty line had the highest prevalence of stress (36.4%)
due to financial instability.
In summary, authors of four studies (Aslam et al., 2013; Khan et al., 2015; Gowani et al., 2016;
Legido-Quigley et al., 2019) have attempted to identify some of the causes of HTN, however,
except for Khan et al. (2015) all three were conducted in one Pakistani province (Sindh). The
next theme common in many studies was patients’ knowledge and attitude towards drug
treatment, which is presented below.
2.4.3 Drug non-adherence
Nine studies gathered information on low awareness of HTN treatment and reported that
drug adherence is poor amongst hypertensive patients in Pakistan (Almas et al., 2006; Hashmi
et al., 2007; Ahmed et al., 2008; Saleem et al., 2010; Almas et al., 2012; Saleem et al., 2012;
Bilal et al., 2015; Gowani et al., 2016; Legido-Quigley et al., 2019). Knowledge (Hashmi et al.,

32
2007; Ahmed et al., 2008; Almas et al., 2012; Gowani et al., 2016) and attitudes (Almas et al.,
2006; Hashmi et al., 2007; Ladha et al., 2009; Saleem et al., 2011; Saleem et al., 2012; Bilal et
al., 2015; Gowani et al., 2016; Legido-Quigley et al., 2019) were the reasons identified in these
studies which influenced the adherence behaviour of participants.
Inadequate patient knowledge and awareness about blood pressure control were identified
as contributing factors for non-adherence to antihypertensive drugs and consequently high
rates of uncontrolled HTN in Pakistan by four studies (Hashmi et al., 2007; Ahmed et al., 2008;
Almas et al., 2012; Gowani et al., 2016). Hashmi et al. (2007) investigated the factors
associated with drug adherence in hypertensive patients (male 199; female 239) by using the
Morisky Medication Adherence Scale (MMAS) with score ranges from 0 (non-adherent) to 4
(adherent). The MMAS score was significantly higher (P ˂0.001) in the adherent group (2.7 ±
1.2) as compared to the non-adherent group (1.7 ± 61). One of the key findings of Hashmi et
al. (2007) was that the overall level of awareness about HTN and its treatment was very low
in the non-adherent group. Ahmed et al. (2008) in a cross-sectional study with 89
hypertensive patients noted that 51.7% of patients were not compliant with antihypertensive
drugs, however, they did not provide any information about the factors responsible for
patients’ non-adherence to drug treatment, limiting the usefulness of the findings.
In a cross-sectional study conducted at three tertiary care hospitals with 447 participants,
Almas et al. (2012) compared knowledge in patients with controlled (n=323) and patients with
uncontrolled (n=124) HTN. In the Almas et al. (2012) study a knowledge score was based on
15 questions developed by brainstorming with experts managing HTN and marked on a scale
of 1 to 5. Researchers noted that there was a statistically significant difference in knowledge
regarding the meaning of HTN, systolic and diastolic blood pressure readings, adherence to
antihypertensive drugs and about lifestyle changes to improve blood pressure between the
two groups. Almas et al. (2012) highlighted that knowledge scores in patients with
uncontrolled HTN were significantly lower and the formal education level did not relate to
knowledge of the disease in these patients. In contrast to Almas et al. (2012) a qualitative
study that was designed to explore how health perceptions correlate with behaviour revealed
that knowledge deficits regarding the illness, its parameters and management were related
to education level amongst patients (Gowani et al., 2016). The researchers reported that most
of the educated participants better understood their disease and treatment as compared to
their uneducated or less educated counterparts. It is therefore difficult to conclude from the
evidence how important formal education level is with regard to understanding of the
disease.
Attitudes towards taking medication
Eight studies noted that patients correlate the necessity of taking medication with the
appearance of symptoms and therefore felt less confident in managing their condition (Almas
et al., 2006; Hashmi et al., 2007; Ladha et al., 2009; Saleem et al., 2011; Saleem et al., 2012;
Bilal et al., 2015; Gowani et al., 2016; Legido-Quigley et al., 2019). Participants in a cross-
sectional survey (n=200) reported intentional non-adherence and missed taking
antihypertensive drugs from time to time due to forgetfulness and side effects (Almas et al.,
2006). This survey identified that 11.6% of patients were not taking the medicine due to side

33
effects and 10.4% missed a dose due to forgetfulness. Likewise, Hashmi et al. (2007) revealed
that once patients achieved control of their blood pressure and their symptoms disappeared,
they decided to discontinue their medication. The researchers identified that patients on
monotherapy were less drug adherent as compared to patients who were on three or more
drugs.
In two later studies, researchers used a qualitative approach and took issue with the
contention that hypertensive patients experience antihypertensive drug-related side effects
and as a result become non-adherent (Saleem et al., 2011; Saleem et al., 2012). They further
indicated that most hypertensive patients do not like taking medication, believing it to be
unnatural and harmful. Saleem et al. (2011) in focus group discussions with 19 patients
identified that patients believed traditional remedies were safer and less synthetic, with
fewer side effects than antihypertensive medication. Likewise, by conducting semi-structured
interviews with 16 hypertensive patients Saleem et al. (2012) noted that due to the fear of
medications being harmful patients reported often skipping a dose deliberately, in order to
avoid frequent exposure to their side effects. Apart from medication side effects, financial
constraints, a lack of availability of low-cost medications and scant information received from
doctors were all identified as important factors that influenced hypertensive patients’
attitudes to drug compliance, as identified in six studies (Ladha et al., 2009; Saleem et al.,
2011; Saleem et al., 2012; Bilal et al., 2015; Gowani et al., 2016; Legido-Quigley et al., 2019).
2.4.4 Using alternative treatments
Despite taking antihypertensive drug treatment some patients tried to treat the condition
themselves, independently of the recommended treatment from their doctor. This was
illustrated in four qualitative studies (Saleem et al., 2011; Saleem et al., 2012; Gowani et al.,
2016; Legido-Quigley et al., 2019). Saleem et al. (2011) noted that most patients indicated
that they were engaged with alternative treatments and highlighted other hypertensive
patients, peers and family members as their sources of information. Eating garlic, drinking
green tea, brisk walking, eating fruits and drinking liquids were mentioned as remedies
adopted by patients. In later interviews with 16 participants, Saleem et al. (2012) found that
complementary alternative medicine (CAM), traditional remedies and spiritual healing
treatments were used by hypertensive patients. Furthermore, their findings highlighted that
religious belief had a strong impact on hypertensive patients’ practices in relation to
treatment as many patients in the Saleem et al. (2012) study reported that they believed that
amulets, sacred water and religious treatment could cure disease.
Legido-Quigley et al., (2019) conducted 20 semi-structured interviews with Pakistani
hypertensive patients and looked at how patients reported using alternative therapies such
as herbal and informal treatments and faith healing. Faith-based treatments were described
as an adjunct to formal healthcare services and not seen as a replacement. In contrast to
Legido-Quigley et al. (2019), Gowani et al. (2016) highlighted patients’ fatalistic beliefs and
mentioned that disease occurrence was associated with events outside the control of an
individual. In this qualitative study, researchers explored participants’ perceptions of illness
and evaluated fatalistic beliefs as a barrier to drug treatment. They found that most of the
hypertensive patients believed that contracting a disease was their fate, that it was meant to

34
happen, unpreventable and unpredictable. The researchers reported that even after
identification of the risk factors patients still believed that nothing could prevent the
occurrence of a stroke or heart attack.
In summary, four qualitative studies (Saleem et al., 2011; Saleem et al., 2012; Gowani et al.,
2016; Legido-Quigley et al. 2019) included in this review highlight that patients’ specific
practices and personal beliefs can serve as barriers to accessing appropriate treatment,
particularly when it came to understanding disease within the context of their religion
combined with views on fate and that this could delay the use of available health services.
Educational interventions often assume poor treatment adherence is as a result of patients
lacking knowledge or not remembering to take their medication, however the findings
discussed above suggest that there may be other reasons for non-adherence to treatment.
The participants in these studies held more complex alternate explanations for their disease
and many intentionally chose to avoid medical treatment.
2.4.5 Awareness about lifestyle changes
Seven studies were identified that looked at the hypertensive patients’ awareness about
lifestyle changes (Ahmed et al., 2008; Khan et al., 2014; Khan et al., 2015; Gowani et al., 2016;
Qamar et al., 2016; Ishtiaq et al., 2017; Murad et al., 2017). Common themes emerging from
these studies were lack of knowledge, low adherence to lifestyle changes and the influence
of contextual factors.
A cross-sectional study that included 219 hypertensive patients (male 89; female 130) from
two cities (Rawalpindi and Islamabad) using a structured questionnaire estimated the
prevalence of HTN amongst the populations studied and explored the risk factors associated
with disease (Ishtiaq et al., 2017). The researchers found a high HTN prevalence rate (29.22%)
in both cities and reported that due to illiteracy patients were unaware about adopting
lifestyle changes such as increasing physical activity, eating a healthy diet, less salt
consumption and smoking cessation. Ishtiaq et al. (2017) stated that only 18 patients were
involved in physical activity while 40 mentioned living a sedentary lifestyle. However, the
researchers failed to provide details of how illiterate participants completed the
questionnaire and did not provide any explanation as to why alcohol intake was not included
in the list of risk factors for HTN. Ahmed et al. (2008) in a cross-sectional study found that out
of 89 hypertensive patients, 55.1% were restricting salt intake, whereas 44.9% were not and
23.6% were engaging in frequent exercise whereas 76.4% were not engaged in any type of
exercise. Researchers also compared risk factors amongst patients who had controlled and
uncontrolled HTN and reported that HTN control was significantly associated with these
changes (P=0.001), however, they did not comment on awareness levels amongst patients
with controlled and uncontrolled HTN.
Khan et al. (2015), however, highlighted that most of the hypertensive patients in their study
were not aware that a sedentary lifestyle contributes to HTN and that adopting healthy
lifestyle changes can assist in controlling HTN. The study illustrated that participants had a
lack of understanding regarding regular exercise, less salt consumption, a low-fat diet,

35
smoking cessation and alcohol consumption in relation to HTN treatment. The researchers
further noted that 23% of patients were unaware that smoking and heavy alcohol intake
contributed to HTN and due to this lack of awareness they continued their smoking and
drinking practices. This observation regarding smoking amongst hypertensive patients is
consistent with the findings of another cross-sectional study conducted at primary healthcare
and tertiary care hospitals in Karachi (Ashfaq et al., 2007). The study identified that generally
patients were unaware of the relationship between smoking and HTN and only half of the
patients were aware that exercise can assist in controlling high blood pressure. Compared to
other lifestyle changes, Ashfaq et al. (2007) focused only on collecting data regarding smoking
and exercise amongst patients without providing any information as to why other lifestyle
recommendations were excluded.
In contrast to the three studies under review (Ashfaq et al., 2007; Khan et al., 2015; Ishtiaq et
al., 2017) one cross-sectional study (n=50) conducted in Karachi reported contradictory
results and reported that 84% of hypertensive patients understood and had awareness that
lifestyle changes were helpful and the optimum way to maintain stable blood pressure
(Murad et al., 2017). The researchers found that 82% of participants with HTN did not smoke
cigarettes, 26% of respondents reported a low salt diet, 24% of respondents reported eating
a vegetarian diet, 73% of respondents performed regular exercise and 96% of participants
avoided drinking alcohol.
Some contextual factors that influenced patients’ behaviour regarding adopting a healthy
lifestyle were social and individual in nature (Aslam et al., 2013; Saleem et al., 2012; Khan et
al., 2014; Qamar et al., 2016; Gowani et al., 2016). Khan et al. (2014) in a descriptive cross-
sectional survey study considered how peer pressure negatively affected the adherence of
patients to dietary regimes to control HTN. The researchers found that in the presence of
family, friends and at social gatherings dietary restrictions left patients feeling under pressure
and eventually they became non-adherent to the diet recommended by doctors. The study
suggested that if patients were told about the severity of HTN and the benefits of eating a
healthy diet, compliance with dietary changes could increase irrespective of influence from
peers. However, this hypothesis and recommendation was not tested in the study.
Individual factors that influenced the decisions of patients to adhere to a particular lifestyle
were identified in three studies (Aslam et al., 2013; Gowani et al., 2016; Ishtiaq et al., 2017).
Aslam et al. (2013) in a cross-sectional study (n=176) identified how hypertensive patients
correlated less adherence to a healthy diet with factors such as monthly income and the cost
of fresh fruit and vegetables (Aslam et al., 2013). Ishtiaq et al. (2017), however, reported that
lack of motivation was a common factor amongst patients that led to non-adherence to
physical activity (Ishtiaq et al., 2017). Adopting an active lifestyle required patients to make
certain modifications in their lives which they could not do due to a lack of motivation.
Likewise, Gowani et al. (2016) by using a semi-structured interview guide with 20 patients in
four focus groups found that regular exercise was not part of all patients’ lifestyles as they
were unable to incorporate it into their daily lives due to laziness, lack of time, ignorance and
the presence of another chronic disease such as arthritis or vertigo.

36
From this body of literature, a picture emerges of the understanding of patients about HTN
and some explanations for non-adherence to drug treatment and lifestyle changes. Data on
hypertensive patients’ understanding of smoking and alcohol consumption were not available
in 20 selected studies and therefore three studies (Ashfaq et al., 2007; Khan et al., 2015;
Murad et al., 2017) could have been more useful if the researchers had provided a more
comprehensive picture about patients’ understanding regarding smoking and alcohol
consumption in HTN management. The following section will explore the literature
concerning the views of doctors with regard to HTN treatment in Pakistan.
2.5 The Approach of Doctors to HTN Treatment
Current understanding of HTN and its treatment in Pakistan comes primarily from studies on
the views of patients. Only four of the reviewed studies collected information regarding the
prescribing practices of doctors and their approach towards HTN treatment guidelines in
Pakistan (Jafar et al., 2005; Rehman et al., 2011; Hussain et al., 2015; Malik et al., 2016).
Therefore, the findings presented below are from quantitative studies.
Despite the availability of treatment guidelines, the literature suggested the existence of a
gap between the recommended guidelines and actual clinical practice in the treatment of
HTN as identified in four cross-sectional studies (Jafar et al., 2005; Rehman et al., 2011;
Hussain et al., 2015; Malik et al., 2016). These studies reported that poor blood pressure
control amongst patients was related to doctors not adhering to HTN treatment guidelines.
The limited adherence of doctors to treatment guidelines represents a barrier to their
successful implementation, however, only two studies provided a potential explanation for
low adherence to HTN treatment guidelines (Hussain et al., 2015; Malik et al., 2016). The
reported reasons were: a lack of knowledge about HTN guidelines and misconceptions about
the cost-effectiveness of antihypertensive agents.
Jafar et al. (2005) in a survey of 1,000 randomly selected male doctors from four Pakistani
cities tested their knowledge with a questionnaire to determine whether their approach to
HTN treatment is in accordance with international guidelines. The study questionnaire was
developed by the researchers and focused on five themes: type of practice, detection of high
blood pressure, evaluation of patients with high blood pressure, treatment of HTN and
sources of information about antihypertensive medication. Jafar et al. (2005) found that most
of the doctors were using incorrect blood pressure measurements in the diagnosis of HTN in
patients of 60 years or above, whilst appropriate HTN treatment in older people was initiated
by less than 40% of the doctors. The researchers identified that the therapy of choice for
lowering blood pressure was reported to be a sedative drug by 23.8% of doctors whereas
21.1% prescribed a combination of an antihypertensive drug and a sedative as an initial
therapy. Moreover, 63% of doctors in the Jafar et al. (2005) study relied on representatives
from pharmaceutical companies to update them on information regarding antihypertensive
drugs and only 31.1% reported reading medical journals for this purpose.
A later descriptive cross-sectional study (n=475) conducted at six hospitals in Karachi
highlighted deficiencies in the knowledge of junior doctors regarding the choice of

37
antihypertensive drugs in accordance with the recommended HTN guidelines (Rehman et al.
2011). The researchers created a structured questionnaire consisting of 11 multiple choice
questions (MCQs) encompassing aspects of HTN such as the definition, diagnostic modalities,
treatment, possible laboratory work to rule out underlying end organ damage and risk factors
for the development of HTN. The results obtained by Rehman et al. (2011) showed that only
42.9% of doctors knew how to define HTN in the presence of co-morbidities and ACE
inhibitors6 were the most common choice (45%) for the first line of treatment in
uncomplicated HTN, followed by thiazide7 diuretics. Overall Rehman et al. (2011) identified
an inadequate knowledge score regarding HTN treatment guidelines amongst junior doctors.
The results of two cross-sectional studies reported poor prescribing practices regarding
antihypertensive drugs amongst doctors (Hussain et al., 2015; Malik et al., 2016). Hussain et
al. (2015) by using a randomized stratified survey with doctors (n=100) and one within the
general population (n=400) illustrated that HTN guidelines were not followed amongst
doctors when choosing pharmacologic agents. The researchers reported that the majority of
doctors prescribed beta-blockers8 (33%) followed by ACE inhibitors (18%) and calcium-
channel blockers9(13%) to patients. The comparison of the annual cost of these drugs
amongst participants was also recorded. From the results, Hussain et al. (2015) also noted
that doctors had misconceptions about the cost-effectiveness of antihypertensive drugs and
therefore therapeutic guidelines were not followed when choosing pharmacologic agents.
Data obtained by Hussain et al. (2015) indicated that advice regarding non-pharmacologic
recommendations was given to patients as per the guidelines. However, inconsistencies in
presenting the results, failure to use inclusion and exclusion criteria for the study participants
and an inability to accurately define study participants presents a significant risk to the
reliability of data. A further limitation was not exploring the views of doctors regarding
compliance with international therapeutic guidelines.
A descriptive cross-sectional study (n=385) conducted in public and private hospitals with
doctors in two cities (Islamabad and Rawalpindi) reported a lack of awareness amongst
doctors of HTN treatment (Malik et al., 2016). Participants included clinicians, specialists,
physicians and doctors from academia working in public (53.7%) and private (46.3%)
healthcare facilities. The study found that generally knowledge amongst doctors regarding
HTN treatment was inadequate and there were issues related to the availability of and
accessibility to HTN guidelines. Issues highlighted by the participants included: patient-related
factors (87.5%), the absence of standard treatment guidelines in the healthcare facilities
(69.1%), lack of awareness amongst doctors regarding the guidelines (85.4%), experience of
doctors (82.3%) and lack of enforcement of guidelines (81.1%). Malik et al. (2016), however,
6 ACE inhibitors are one of four drug classes recommended for initial therapy for adults with elevated blood pressure (Herman & Bashir, 2019). 7 Thiazide diuretics drugs are commonly recommended as the first line of treatment for HTN and significantly reduce the rate of stroke and heart attacks (Grossman et al., 2011). 8 Beta-blockers are a class of medication that work mainly by decreasing the activity of the heart by blocking the action of hormones such as adrenaline (Kaplan, 2008). 9 Calcium-channel blockers are medications that are often used to treat HTN by slowing the movement of calcium into the cells of the heart and blood vessels (Ozawa et al., 2006).

38
identified greater knowledge scores amongst doctors who were working as specialists and
had clinical experience of more than 10 years.
In summary, four studies have identified ambiguities in the prescribing practices of doctors
and their inadequate reported knowledge of HTN treatment in Pakistan. Overall, only two
studies (Hussain et al., 2011; Malik et al., 2016) gained ‘fair’ and ‘good’ quality on the NHLB
assessment tool and clearly stated their research objectives and defined the populations
being studied. However, a common weakness amongst the four studies under review was the
failure of the researchers to define explicit criteria for adherence to HTN guidelines.
Additionally, the four studies did not conduct a review of the medical records of patients to
explore whether divergence from guidelines was justifiable. The studies relied on survey data
only for measuring adherence to guidelines.
2.6 Summary and Identification of Gaps
To the best of the author’s knowledge, this is the first systematic review of the literature
about patients and doctors understanding of HTN and its treatment in Pakistan and it helps
to highlight the issues that require further research. The aim of this review was to identify
what is already known about patients’ and doctors’ understandings of HTN and its treatment
in Pakistan. A total of 21 studies were included in the review in which 17 reported data on
patients’ understanding of HTN treatment and four studies looked at doctors’ awareness of
HTN treatment guidelines in Pakistan.
Four studies (Saleem et al., 2011; Saleem et al., 2012; Gowani et al., 2016; Legido-Quigley et
al., 2019) were qualitative and focused on patient HTN awareness; they reported some of the
contextual factors that are linked to treatment non-adherence amongst patients. Two studies
(Saleem et al., 2011; Saleem et al., 2012) did not describe their data analysis procedures and
scored lowest on the CASP assessment criteria. Moreover, all four qualitative studies were
limited to Sindh and Baluchistan provinces and did not recruit participants from Punjab, which
is the most densely populated province in the country, hence, it is difficult to determine if the
findings would resonate with the experiences of patients in Punjab province.
Thirteen cross-sectional quantitative studies provided data on patients’ knowledge of drug
treatment, lifestyle changes and reported low HTN awareness amongst patients. It is
surprising to note that most of the studies do not address important issues that influence HTN
management which includes lifestyle changes related to socio-cultural context. The review
identified four cross-sectional studies that focused on doctors (Jafar et al., 2005; Rehman et
al., 2011; Hussain et al., 2015; Malik et al., 2016). The evidence suggested a lack of adherence
by doctors to the recommended HTN treatment guidelines and variation in prescribing
practices. Awareness regarding HTN treatment guidelines varied between senior and junior
doctors, as highlighted by Malik et al. (2016) and this may be an influence on HTN
management.
The studies reviewed highlighted a lack of overall HTN awareness as the foremost reason for
poor HTN control in patients although inappropriate and inconsistent treatment practices

39
amongst doctors was also seen to have an impact. However, the quality assessment of the
studies reviewed demonstrates the need for further good quality research with robust
methodologies. Furthermore, the review was unable to identify any qualitative studies
focusing on doctors’ beliefs about HTN management and this highlights an important gap in
the literature. The following summarises the gaps in the existing knowledge about doctors’
and patients’ understanding of HTN management in Pakistan:
• Qualitative studies that explore patients’ understanding regarding all aspects of HTN
(lay definitions, causes, symptoms) in terms of treatment (antihypertensive drugs and
lifestyle recommendations) and the ways patients manage the disease is limited
overall and not available in Punjab province. Detailed evidence taking account of the
socio-cultural context is missing from the available literature.
• The review was unable to identify any studies on doctors’ understanding of HTN.
• As no qualitative study explored doctors’ viewpoints on HTN, it is difficult to ascertain
whether the finding from surveys in Pakistan about doctors’ non-adherence to HTN
treatment guidelines was due to a lack of knowledge or because of other issues.
In conclusion, the review highlights that a study of patients’ and doctors’ understanding
regarding HTN treatment and management is required, focusing particularly on the Pakistani
context. In addition to the available evidence from Pakistan about HTN, the following part of
this chapter considers the main concepts that will inform the context of the present study.
2.7 Search Strategy for the Broader Literature Review
The review focused on studies reporting beliefs and practices about chronic disease
management in Pakistan but also included studies from some Asian and Muslim-majority
countries because these countries share a similar socio-cultural context to Pakistan. The initial
literature search identified a very limited number of studies about doctors’ beliefs from
studies undertaken in Asia, therefore to overcome this limitation studies are also included
from European countries. European culture is different to that of Asian, however, due to
insufficient evidence from that region it was essential to broaden the search to ensure there
is sufficient literature to inform the study. The databases searched were Scopus, Medline
(PubMed) and Global Health. In addition to these databases, extensive lateral search
techniques were also used such as scanning the reference list of the relevant articles and
searching the grey literature. Substantive relevant seminal literature on health beliefs to
understand the concept and inform this study was also considered.
Table 2.2 summarises the search terms and keywords combined into four groups and used to
identify relevant studies.
Table 2.2 Keywords and terms used in the literature search
Condition Informer Views Context/Research Environment

40
Hypertension
High blood pressure
Chronic disease
Patient
Doctor
General Practitioner
Beliefs
Lay beliefs
Perceptions Perspectives
Treatment/Therapy Antihypertensive drugs Lifestyle changes
Adherence
Culture
Social norms
Religion
Asia
Muslim population
Europe
2.8 Health Beliefs
From the late 1970s there has been considerable growth in research concerned with eliciting
the subjective reality of illness in terms of lay explanations (Currer & Stacey, 1986; Lawton,
2003; Conrad, 2005). How patients make sense of an illness has been a major focus of
investigation in health and the social sciences. Beliefs are informed by perceptions and can
be judgements, predictions, ideas, interpretations and conclusions (Chaffee & Roser, 1986,
Breen et al., 2000; Aylward, 2006; Halligan, 2006). Illness perception comprises a number of
interrelated beliefs about illness and what it means for the patient’s life (Petrie & Weinman,
2012). As highlighted by Petrie and Weinman (2012) the major components of these beliefs
include how the illness was caused, how long it will last, what the consequences of the illness
are for the patient’s life, the symptoms that are part of the illness and how the condition is
controlled or cured.
According to Green et al. (2003, p.106) lay health beliefs can be defined as practices that are
socially embedded and ‘shaped by people’s situations in the social structure, their cultural,
personal biography and social identity’. Lay beliefs help predict the subjective experience of
illness, management, recovery (Diefenbach & Leventhal, 1996; Damasio, 2000) and treatment
compliance (Weinman & Petrie, 1997; Hassin et al., 2005). These are individuals’ ways of
understanding their bodies and explaining what is going on within them. Lay beliefs describe
the definitions, meanings and experience of health and illness and often include particular
ideas about the way the body functions (Bolam et al., 2003; Aylward, 2006).
Hence, attitude (mental dispositions to act), behaviour (established ways of responding to
people and situations) including spoken articulation and the ability to cope can be attributed
to implicit or explicitly held beliefs (Prior, 2003; Halligan, 2007). In this respect, the study of
lay beliefs may contribute to elevating the status of the patient in the context of healthcare
(Herzlich & Pierret, 1987, p.13).
Ascertaining people’s illness beliefs can help to explain the ways in which they live with the
complexities of chronic disease, behave towards their health, treatment plans and health
services (Nettleton, 2006). It may show a search for meaning that goes beyond the
straightforward empirical, personal experiences of people about health issues and crises.
Hence, lay explanatory models (Blaxter, 1997), illness narratives (Kleinman, 1988) and
insiders’ perspectives (Gerhardt, 1990) amongst other related terms have been suggested as
ways to conceptualise the lived experience of illness through the patients’ lens. The concept
of ‘lay expertise’ has gained credibility as a way of describing the process by which the patient

41
gains intellectual, psychological and physical mastery over their illness, thereby enabling
themselves to better cope with it (Morgan & Watkins, 1988; Williams, 2014). This is best
explored in relation to the management of chronic illness where the patient uses his or her
position as sufferer as a basis for becoming an expert in knowledge (including medical)
surrounding their condition but also utilizing the experience of suffering as a way of
negotiating or critiquing that knowledge (Shaw, 2002).
According to Prior (2003) the notion of lay expertise is used to refer to two distinct types of
knowledge. One is the experiential knowledge developed by the patient as a by‐product of
coping with daily practicalities of the disease as well as making sense of how the body reacts
to medication (Storni, 2015). The other is the expert knowledge as appropriated by non‐
experts that is used to contribute to (Rabeharisoa & Callon, 2002) but also challenge (Barbot,
2006) and dispute the biomedical perspective (Storni, 2015). Lay perspectives are now seen
as forms of knowledge which are of ‘equal worth’ to expert knowledge (Grundmann, 2017).
Where this expertise challenges the doctor’s knowledge and practice, conflicts can arise
(Popay et al., 1998). For instance, Kerr et al. (2007) explained that lay and professional
participants in the healthcare system have the knowledge and in applying it they demonstrate
expertise.
To deal with the intricacies and difficulties of everyday chronic disease management patients
develop different ways of knowing and dealing with the disease and this should be taken into
account when reorganising care delivery (Wagner & Groves, 2002; Henwood et al., 2003;
Williams, 2014). Education campaigns which aim to encourage people to take responsibility
for their health could prove ineffective if people hold fatalistic views about the causes of
disease (Nettleton, 2006). It is important to consider that a person may present to a doctor
with a variety of explanations based on the experience of their illness (Harmon et al., 2006;
Greenhalgh, 2009). This is especially true during periods when people are trying to make
sense of the problem and in doing so may move between a varied and complex set of beliefs.
These beliefs can be considered as their ‘maps of realities’, which either become firmer and
stronger or dismissed and replaced (Connors & Halligan, 2015). Undoubtedly, these beliefs
vary with gender, social class, ethnicity and from individual to individual (Nettleton, 2006;
Conner & Norman, 2008) and are not necessarily consistent with their own explanations of
health and illness depending on circumstances. In contrast to the clinical knowledge of
disease, understanding the meaning of illness and health for individuals who have
experienced this in terms of consequences and symptoms in everyday life provides subjective
and highly relevant evidence (Baker, 1987; Boruchovitch & Mednick, 2002).
People’s health beliefs are shaped by the interplay of various influences (Currer & Stacey,
1986; Kressin et al., 2007; Sathyanarayana Rao et al., 2009; Marshall et al., 2012). The sources
of beliefs include socio-cultural (e.g. religion, norms), socio-economic influences (e.g. income,
education, occupation), past experiences, knowledge and individual factors such as duration
of disease and co-morbidities. These influences are sometimes reported as barriers in the
management of chronic disease as these can limit undertaking of a required behaviour by
patients to achieve the recommended treatment (medication and/or lifestyle change)
adherence or follow up care (Siegel, 2005; Khatib et al., 2014; Devkota et al., 2016).
42
2.8.1 The impact of socio-cultural context on beliefs and behaviour
Illness is not merely a pathological condition for patients. It is expressed through the social
and cultural context in which they live and experience life (Conrad, 2005). Culture refers to
shared values, norms and codes that collectively shape the beliefs, attitudes and behaviour
of individuals through their interaction in and with their environments (Iwelunmor et al.,
2014). Culture is shared by at least two or more people and naturally societies consist of
greater numbers of individuals. If a solitary individual thinks and behaves in a unique way that
thought or action is idiosyncratic, not cultural (Cohen et al., 2005).
For an idea or behaviour to be considered cultural it must be shared by some type of social
group or society (Thonemann, 2013). Individual beliefs about health and illness are
representations of the culture and society in which people live (Conner & Norman, 2008;
Blaxter, 2010). For instance, in South Asian culture, demands for personal space can be
viewed as a rejection of togetherness and the strength of this shared belief is such that people
will often sacrifice their own health and individuality in order to conform (Malik, 2003). Hence
the experience of illness is mediated by lay beliefs that have a key impact on human behaviour
and it is important to take account of these in order to understand the effectiveness of health
interventions aimed at changing behaviours (Williams & Popay, 1994; Kelly & Barker, 2016).
People’s beliefs are often shaped by culture that are in accordance with religion, local norms
and traditions, therefore, the following sections will draw on literature from Pakistan and
other Muslim and Asian populations discussing the influence of religion and social norms on
beliefs and the behaviour of patients.
The role of religion, faith and fatalism
Religion and faith have a significant influence on human health and are important tools
people utilise when coping with life’s situations, stresses and illness (Koenig et al., 2001; Neal,
2013). Religion may be defined as any system of belief about a deity, often involving rituals,
a code of ethics, a philosophy of life and a world view (Etzelmuller & Weissenrieder, 2016).
Whilst faith is trust and confidence in a particular system of religious belief, faith has the
benefit of empowering the individual through connecting him or her to a community that
might, in turn, provide psychological stability (Basu-Zharku, 2011). Religious beliefs can be
helpful in disease management and assisting with coping strategies depending on how well
they are utilised.
A survey of 604 patients in one of the largest cities in Pakistan showed that 99.7% patients
believed that living a life compatible with traditional Islamic teachings led to better health
(Ahmed et al., 2007). They believed that undertaking the five daily obligatory prayers also led
to a healthier life. Religion according to study participants facilitated health and treatment via
three routes: (i) prevented them from drinking alcohol; (ii) prevented them from engaging in
gambling and bribery (iii); assisted them in abstaining from fornication. Furthermore, Ahmed
et al. (2007) emphasised that in Pakistan patients wanted their doctors to pray for them out
loud during clinical visits and 88% believed that having a doctor who was also a faithful
practicing Muslim would have a positive impact on the outcomes of their disease.

43
The results of a questionnaire-based cross-sectional survey in Pakistan undertaken by Qidwai
et al. (2009) revealed that the majority of respondents believed that prayer could heal. Three
quarters (75.3%) of them believed that prayers can curtail the duration of disease and 160
(40%) participants believed that prayer could prolong life. Methods used for healing by study
participants included: reciting verses from the Holy Quran, blowing these verses on water and
then drinking the water and wearing an amulet which was thought to speed up the healing
process. Some of the findings in the Qidwai et al. (2009) study are consistent with a qualitative
study conducted in Iran involving 27 hypertensive patients who reported that prayer helped
in healing and believed that religion played a positive role in their disease outcomes (Shamsi
et al., 2017). Furthermore, patients correlated listening to the Holy Quran with the healing
process and being distant from God was one of the most frequently cited factors by patients
for the development of disease.
Six studies conducted in various Muslim countries highlighted specifically the positive role of
religion in coping with disease, adopting a healthy lifestyle and adherence to treatment (Al-
Kandari, 2003; Alsolami et al., 2012; Hatah et al., 2015; Nayeri et al., 2015; Mizutani et al.,
2016; Mostafavi et al., 2016). It was revealed in a questionnaire survey involving 223 patients
that blood pressure control was improved in Kuwaiti patients who were spiritual and involved
in religious activities (Al-Kandari, 2003). 300 participants in the Hatah et al. (2015) cross-
sectional study indicated that religion helped people accept the disease, reduced stress and
that God helped with disease management and provided peace (Hatah et al., 2015). Likewise,
religion was viewed as an important source of managing stress and enhancing compliance to
lifestyle changes amongst hypertensive patients in Iran (Nayeri et al., 2015). Participants
mentioned that their body was on loan from God and they should pay careful attention to
what they eat and how they take care of this loan. In addition, being connected to positive
religious values to do with avoiding overeating and oversleeping had encouraged some
participants to change their lifestyles based on these beliefs.
Mostafavi et al. (2016) took issue with the contention that hypertensive patients viewed
disease treatment as a necessity instructed by God and therefore adopted careful behaviours
regarding drug adherence. The studies presented here suggest how religion is perceived as a
facilitator to healthcare and positive religious beliefs motivated individuals to engage in
healthy activities and comply with their treatment plans. In the available literature religion is
sometimes reported as a barrier to changing attitudes towards health and treatment
adherence when patients display negative religious beliefs regarding fatalism. Fatalism is
defined as a sense of lack of control and powerlessness over health and illness (Perfetti, 2017).
A person with fatalistic beliefs and a poor level of literacy can misunderstand religious
concepts and recognise health as being beyond one’s control and dependent on chance, luck,
fate or a powerful external agency (Boyer, 1994; Perfetti, 2017). If patients assume that they
do not have power and control over their lives and disease, the challenge for doctors is to
then convince patients regarding treatment and adherence.
Some of the studies identified were evident expressions that disease occurrence was
associated with events outside the control of an individual. For example, an ethnographic
study conducted by Shaikh et al. (2008) in the Northern areas of Pakistan found that illness

44
was often believed to be related to the ‘evil eye’ and possession by spirits amongst Muslim
patients and they approached spiritual healers for treatment as opposed to consulting
doctors. Likewise, Anwar et al. (2012) mentioned that the notion of the ‘evil eye’ was
frequently believed to be the cause of disease amongst patients and they reported treating
this by reading books of a holy nature. Some beliefs contribute to the practices of patients
with regard to taking medications and adopting treatment options.
Bukhari et al. (2002) identified superstitions associated with health beliefs amongst different
ethnic groups residing in Pakistan. The study found that many illiterate individuals correlated
superstitions with their religion and indicated that these beliefs had passed to them from
elders. However, the study failed to identify the types of superstitions derived from religion
and how these influenced disease management amongst participants. In contrast, a study
conducted in Iraq found the use of the traditional therapy ‘Al-Hijama’ (cupping) which is
popular in Islamic society was linked to HTN disease treatment amongst patients (Ibrahim et
al., 2016). Participants reported that it was urged by the religious precepts to cure disease
using different elements and therefore they found this treatment more effective than medical
treatment.
This is also the case for Iranian participants in a study conducted by Najimi et al. (2016) who
stated that participants thought that their HTN symptoms were due to fate and believed
illness was predetermined by God and therefore they were not required to intervene with
treatment. Perceiving disease to be in God’s hands demonstrated another aspect of fatalistic
beliefs that endangered a sense of responsibility towards one’s own health.
The role of social norms
Social norms are the customary rules that govern behaviour in groups and societies (Paluck &
Ball, 2010). Social norms provide direction and motivation, organise social interactions and
make people’s responses predictable and meaningful (Forsth, 2012). In other words, social
norms are the customary rules governing how to behave in certain ways within a society.
Social norms influence health-related attitudes and are reported to have powerful control
over human behaviour (Hechter & Opp, 2001).
Social norms are not formed in a vacuum, rather, they are shaped by larger environmental
forces including culture and religion and raise certain challenges for healthcare and behaviour
change (Rajiv & Kevin, 2005). Prevention strategies such as pharmaceutical interventions and
lifestyle changes might fail to achieve therapy goals if social norms are not considered or
appropriate adaptations made. For example, smoking is a socially acceptable norm for men
in Asian countries and in particular in the Bangladeshi community it represents a strong sense
of social bonding and a normal part of being male (Bush et al., 2003).
Social norms differ in practice from one country to another depending on the cultural contexts
(Hechter & Opp, 2001; Forsth, 2012). Despite the modernisation of Pakistani society social
norms revolve around the teachings of Islam and are highly influential in people’s lives (Burki
& Ziring, 2017). However, certain norms are interwoven into the culture and people find it
difficult to distinguish between the two, for example, the traditional joint or extended family
system in Pakistan. Fewer studies in Pakistan have suggested how social relationships and the
45
family system can influence and hinder adopting healthy attitudes (Khuwaja & Kadir, 2010;
Qureshi et al., 2016; Mahmood et al., 2017).
A qualitative study conducted on pregnant women in Pakistan that also included some
hypertensive patients identified that extended families were perceived as having a potentially
negative impact on women’s lives and health (Qureshi et al., 2016). Women reported being
confined to their homes to do housework for family members, given low status in the family
and were excluded from decision-making regarding their health, for example regarding
visiting doctors. Likewise, a survey study by Mahmood et al. (2017) involving 411 hypertensive
patients suffering with depression evaluated that women living in extended families in
Pakistan experience greater stress and depression due to their low social status and the
burden of responsibilities and relationships. Khuwaja and Kadir (2010) in a community-based
survey amongst 534 participants with non-communicable chronic diseases also identified
social norms that were specific to female patients in Pakistan. They indicated that women had
reported being restricted in walking outside unaccompanied by a male family member and
their extended family limited the time available for them to engage in exercise. Participants
in the study suggested that they would be better able to engage in physical activity if there
were exercise facilities designated for women only.
Studies conducted on participants in Asia have reported that social influence was reported to
be both a barrier and facilitator for HTN control (Kusuma, 2009; Shima et al., 2014; Elbur,
2015; Rahman et al., 2015; Nayeri et al., 2015; Shamsi et al., 2017). Two qualitative studies in
Malaysia and Iran pointed out that a lack of social support from family members affected
medication adherence and changes to lifestyle amongst patients (Shima et al., 2014; Nayeri
et al., 2015). Researchers using a range of methods found that having to cook for oneself
differently from the rest of the family was perceived to go against social norms in India,
Malaysia and Saudi Arabia (Kusuma, 2009; Mahmoud et al., 2012; Shima et al., 2014; Elbur,
2015). Norms specific to family obligations were also reported as a barrier to adopting healthy
attitudes and participants found it hard to prioritise clinic visits, diet and exercise over the
needs of family members (Shima et al., 2014; Risso-Gill et al., 2015).
A study done by Shuval et al. (2008) in Israel examined certain norms that were Muslim
women specific. Researchers found that women were not allowed to walk outside without
being accompanied by a male family member and were subject to verbal abuse from the
community when they attempted to engage in outdoor exercise. In two qualitative studies
undertaken in a range of Asian populations the majority of participants viewed the experience
of being supported by their families as a common norm (Rahman et al., 2015; Shamsi et al.,
2017). This support was in the form of cooking food according to their health needs, providing
information about the disease, accompanying the patient to the hospital and reminding them
to take their medication. Together the results provided important insights into the influence
of social norms on people’s health beliefs and behaviour. The following section now discusses
lay understandings of patients regarding HTN in various Muslim and Asian countries in order
to highlight different aspects of living with disease.

46
2.9 Living with HTN
Some of the studies that included details about living with HTN have particularly addressed
that accepting the disease diagnosis was difficult amongst patients (Rahman et al., 2015;
Nayeri et al., 2015; Shamsi et al., 2017). This was due to the absence of HTN symptoms upon
diagnosis and many patients could not remember when they had started feeling HTN
symptoms. For example, data from a large-scale international study in seven Asian countries
revealed that upon diagnosis of HTN patients reported feeling confused, worried and anxious
(Rahman et al., 2015). The study identified that patients experienced difficulties in initially
accepting their HTN diagnosis due to an absence of clinical symptoms. These results appear
consistent with prior research reporting that 59.9% of the patients with HTN were unaware
of their HTN due to the asymptomatic nature of the disease (Porapakkham et al., 2008).
Likewise, some participants in the Kusuma (2009) study expressed that it was difficult for an
individual to know his or her HTN status, unless checked by a doctor, due to the absence of
symptoms. A study by Shamsi et al. (2017) concluded that understanding HTN and its
diagnosis was dependent on clinical symptoms and severity amongst patients. A contrasting
description can be found in three qualitative studies conducted in various countries suggest
that the appearance of physical symptoms made participants aware of their disease and
diagnosis (Shima et al., 2014; Udompittayason et al., 2015; Najimi et al., 2016). Symptoms
such as headaches, dizziness, a general feeling of weakness and fatigue were commonly
reported in these studies amongst hypertensive patients. Indeed, symptoms are the most
common reasons for initiating medical treatment and feeling healthy is often equated with
being symptom-free (Nayeri et al., 2015).
Likewise, a study carried out on the perceptions of patients in Malaysia proposed that patients
generally experienced HTN symptoms and as a result sought medical attention for their
diagnosis (Shima et al., 2014). There was a range of perceptions from patients about the
nature of HTN and choices they made in the literature. Studies undertaken in Taiwan and Iran
highlighted that HTN was seen as a temporary condition amongst patients that would not
require long-term treatment (Hsiao et al., 2012; Shamsi et al., 2017). Likewise, HTN was not
viewed as a pathological condition by some of the participants in an interpretive ethnographic
study in Thailand (Udompittayason et al., 2015). Whilst two studies highlighted that patients
considered HTN as a serious disease that could cause complications such as stroke and heart
disease and understanding the risks associated with the disease was an important factor
influencing their attitudes towards treatment (Aslami & Jobby, 2015; Rahmawati & Bajorek,
2016).
Studies on the perceptions of hypertensive patients in the literature have reported a number
of reasons linked to HTN causes amongst participants. For instance, Najimi et al. (2016)
highlighted that patients believed themselves to be susceptible to HTN due to their genetic
background and reported family history and psychological factors as reasons for their disease.
Similarly, patients in two qualitative studies conducted in Iran considered that their HTN was
inherent and could not be treated (Nayeri et al., 2015; Shamsi et al., 2017). In contrast, many
patients in another study linked HTN to body temperature and ‘bad blood’ in their veins which
resulted in their illness (Udompittayason et al., 2015). However, in the findings of some

47
studies researchers identified that living an unhealthy lifestyle was recognised as a cause
amongst hypertensive patients in Iraq, Thailand and Indonesia (Udompittayason et al., 2015;
Ibrahim et al., 2016; Rahmawati & Bajorek, 2016).
A recurrent theme in a number of studies was how patients attributed personal stress as a
significant cause of their elevated blood pressure and as a result they viewed stress reduction
as an effective way to control HTN (Kamran et al., 2014; Shima et al., 2014; Rahman et al.,
2015; Nayeri et al., 2015; Ibrahim et al., 2016; Shamsi et al., 2017). It was reported in these
studies that hypertensives tended to attribute high blood pressure to life stresses caused by
interpersonal issues, unemployment and financial problems. Some researchers have also
reported techniques that patients used to reduce or avoid stress to control their HTN such as
trying to avoid arguments, sleeping and relaxing (Serour et al., 2007; Nayeri et al., 2015;
Mostafavi et al., 2016).
In an ethnographic study conducted using in-depth interviews a significant stressful event in
the past was thought to be responsible for the later development of HTN by a few participants
(Udompittayason et al., 2015). From a medical perspective, stress plays a small part in HTN
(Beevers et al., 2015) whereas a recurring theme in the studies presented here is that stress
was by far the most important cause of HTN according to the perceptions of patients. This
section has reviewed the literature focused on the lay understanding of patients about HTN,
its symptoms and causes; studies addressing understanding about drug treatment are
presented below.
2.9.1 HTN drug adherence
Adherence is defined by the WHO as the extent to which a person’s behaviour such as taking
medication, following a diet, and/or implementing lifestyle changes, corresponds with the
recommendations made by healthcare providers or doctors (WHO, 2014). However, there are
various issues in the lives of patients suffering with a chronic illness and therefore the
recommended treatment plans are often beset by challenges.
It has been reported in some studies that patients with a good knowledge of their disease
were more motivated to practice home blood pressure monitoring, had improved medication
adherence and blood pressure control (Heymann et al., 2011; Kamran et al., 2014; Elbur,
2015). In contrast, a few researchers have been able to conclude that antihypertensive drug
adherence was significantly associated with gender and was generally greater in men as
compared to women (Khalil & Elzubier, 1997). One study found in the literature suggested
that self-monitoring of blood pressure improved the adherence of hypertensive patients to
drugs (Nayeri et al., 2015). The interpretation of these results may be that females are more
likely to devote their time to their families instead of taking care of themselves. However, the
study did not take account of or question why drug adherence was better in male patients.
Critics have argued that economic reasons such as the high cost of the blood pressure
monitoring device and an absence of skills to monitor and understand blood pressure
readings act in conjunction with the barriers for patients to self-monitoring and drug
adherence (Tan et al., 2005; Rahman et al., 2015). The findings of a few studies have
suggested that medication adherence was found to be an independent predictor of blood

48
pressure control amongst patients (Behnood-Rod et al., 2016; Khayyat et al., 2017). However,
a number of studies in Asian countries have reported that adherence to drug treatment is
poor amongst hypertensive patients (Mahmoud et al., 2012; Ramli et al., 2012; Shima et al.,
2014; Nayeri et al., 2015; Behnood-Rod et al., 2016; Mostafavi et al., 2016; Khayyat et al.,
2017).
A few researchers have argued that patients correlate the necessity of taking drugs with the
appearance of symptoms and are not aware that HTN might be asymptomatic (Rahmawati &
Bajorek, 2016; Shamsi et al., 2017). They further claimed that the presence and severity of
symptoms were associated with the beliefs of patients about the need for medication and
their decision to take it. Another study associated patient non-adherence with therapy
requiring more than one pill per day compared to patients prescribed only one pill per day
(Bhandari et al., 2015). Antihypertensive drug non-adherence was also higher amongst
patients taking a greater number of pills in India (Srikanth & Kulkarni, 2015) and Malaysia
(Ramli et al., 2012). On the other hand, a couple of studies found that when patients had to
take multiple medications, they were less likely to fail to remember to take them, compared
to when only having one pill to take (Hassan et al., 2006; Srivastava et al., 2015).
In contrast, some researchers took issue with the contention that hypertensive patients
experience antihypertensive drug-related side effects such as dizziness, problems falling
asleep, a dry mouth and therefore decide not to take their medication (Khalil & Elzubier, 1997;
Shima et al., 2014; Nayeri et al., 2016; Khayyat et al., 2017). Qualitative studies undertaken in
Iran and Malaysia have further elucidated that most hypertensive patients do not like taking
drugs, finding these unnatural and harmful (Shima et al., 2014; Mostafavi et al., 2016). This
aligns with findings from other studies which revealed why hypertensive patients avoid taking
medication and demonstrate poor adherence (Aslami & Jobby, 2015; Ibrahim et al., 2016).
Common reasons to drug non-adherence that have been identified in the literature are
forgetfulness (Khalil & Elzubier, 1997; Jimmy & Jose, 2011; Shima et al., 2014; Nayeri et al.,
2015), fears about use of drugs due to dependence (Al Ghobain et al., 2016; Devkota et al.,
2016; Najimi et al., 2016; Rahmawati & Bajorek, 2016), duration of therapy (Kamran et al.,
2014; Devkota et al., 2016) and misconceptions about the dose of drugs (Panpakdee et al.,
2003; Udompittayason et al., 2015). Financial difficulties were the most strongly emphasised
barriers identified amongst hypertensive patients for drug non-adherence (Aslami & Jobby,
2015; Ibrahim et al., 2016; Khayyat et al., 2017). These studies found that medications were
expensive and therefore some hypertensive patients could only buy the quantity of drugs
they could afford, rather than relating to their clinical need.
Despite using antihypertensive drugs some patients try to manage their condition by
themselves, independently of recommended treatment from their doctor. For example,
qualitative studies conducted in Indonesia, Iraq, Iran, Nepal and Malaysia on disease
management by hypertensive patients identified that strategies such as using home remedies
were often used by patients to manage HTN alongside antihypertensive drugs (Ramli et al.,
2012; Ibrahim et al., 2016; Devkota et al., 2016; Rahmawati & Bajorek, 2016; Nayyeri et al.,
2017). The use of herbs, garlic and lemon in tea were the most commonly home or lay
remedies mentioned by hypertensive patients in a number of populations (Panpakdee et al.,

49
2003; Zinat Motlagh et al., 2016; Ibrahim et al., 2016; Shamsi et al., 2017). Patients in these
studies said they thought using herbal treatments was safer than using conventional medicine
as a cure for their disease.
2.9.2 Difficulties in adopting lifestyle changes
It has been reported that doctors advising patients that they must make changes to their
lifestyles and will have to take medication for the rest of their lives appeared contradictory
and confusing to many hypertensive patients (Rahman et al., 2015). Patients reported that if
changes in lifestyle can decrease blood pressure why was there an assumption that it will be
necessary to take medication? This may lead to ambiguity amongst patients’ beliefs about the
nature of the disease and create difficulties for their decision making. Likewise, a qualitative
study conducted in Indonesia showed that patients prefer lifestyle changes over medication
and suggested that such changes were sufficient to treat HTN (Rahmawati & Bajorek, 2016).
This is the only study that identified a preference in patients to adopt lifestyle changes over
medication. Although patients chose lifestyle changes due to fears of medication addiction,
the study did not adequately explore the awareness of patients with regard to the benefits of
lifestyle changes and its application in HTN management and control.
Some researchers revealed opposite findings and reported unsatisfactory levels of knowledge
amongst patients regarding lifestyle recommendations (Heymann et al., 2011; Kamran et al.,
2014). A cross-sectional survey (n=50) in India found that 42% of patients did not perform any
exercise, the majority were using excessive salt in their daily diet and 12% were consuming
fats on a daily basis due to lack of knowledge (Kaur et al., 2007). Similarly, a cross-sectional
study conducted in Egypt indicated that knowledge about all lifestyle recommendations
amongst hypertensive patients was inadequate (El-Hay & El Mezayen, 2015).
Some researchers have argued that a lack of motivation amongst patients was the most
common cause of poor adherence to lifestyle changes (Mahmoud et al., 2012) although
adopting an active lifestyle required patients to make certain modifications in their lives which
they could not do due to various factors or barriers. Barriers to not practicing a healthy
lifestyle commonly reported in the literature were personal, social and environmental. Some
identified factors in the literature that lead to non-adherence to exercise in hypertensive
patients are weather, disability, injury, time constraints/busy routine and a lack of social
support (Serour et al., 2007; Shima et al., 2014; Rahman et al., 2015; Khayyat et al., 2017).
Likewise, issues contributing to non-adherence to dietary changes in hypertensive patients in
a number of populations are the attraction to eating out, dietary habits and a taste for salt
and traditional foods (Shima et al., 2014; Aslami & Jobby, 2015; Nayeri et al., 2015; Zinat
Motlagh et al., 2016). In Saudi Arabia difficulties in preparing a specific diet with less salt and
oil was the most frequent cause for poor adherence to dietary regimes due to the tradition
of families and friends eating together (Mahmoud et al., 2012). Some hypertensive patients
correlated less adherence to a healthy diet with monthly income and the cost of fresh fruit
and vegetables; the influence of social gatherings was also indicated in four qualitative studies
(Serour et al., 2007; Elbur, 2015; Mahdavi et al., 2017).

50
A few studies in the review identified factors that have been attributed to the high incidence
of smoking amongst hypertensive patients, such as an addiction to nicotine and the social
requirements to relieve anxiety and frustration (Nizami et al., 2011; Kamran et al., 2014).
Compared to smoking, alcohol consumption remains low where the majority of the
population is Muslim (Nayeri et al., 2015). Alcohol is restricted for Muslims on religious
grounds and in Muslim countries there are strict laws against the consumption of alcohol.
Another reason may be the stigma surrounding its consumption and Muslims countries do
not allow people to drink publicly or in front of their families.
Some researchers (Shima et al., 2014; Elbur, 2015; Rahman et al., 2015; Mostafavi et al., 2016)
have highlighted that doctors also contribute to the non-adherence of patients to treatment
plans and found this to be a significant factor. Doctors counselling on an active lifestyle have
an independent effect on hypertensive patients’ reported adherence with the recommended
lifestyle advice (Heymann et al., 2011; Devkota et al., 2016). These researchers made an
attempt to explore how doctors often fail to recognise drug non-adherence in their patients,
do not explain the adverse effects of a drug effectively, over prescribe and inadequately
consider the burden of cost to the patient which can then lead to medication non-adherence.
For instance, a majority of hypertensive patients reported difficulty in recalling complex
nutritional advice received from doctors during time constrained consultations (Nayeri et al.,
2015). In contrast, many patients in various Asian countries indicated that they did not receive
any proper advice on drug use and lifestyle changes from doctors (Alsolami et al., 2012; Shima
et al., 2014; Devkota et al., 2016). Some hypertensive patients reported that encounters with
the doctor created nervousness and as a result that they did not ask all that they wanted to
know (Rahman et al., 2015; Rahmawati & Bajorek, 2016). From this body of literature, a
picture emerges of the lay understanding of patients about HTN and the causes of non-
adherence to drug treatment and lifestyle changes. The following section will explore the
literature concerning the understandings of doctors in general and with regard to HTN
management.
2.10 Doctors’ Understanding about Illness
The medical definition of illness is largely based on objective and demonstrable physical
changes in the body such as signs of disease and symptoms (Helman, 2007). This medical
explanation does not include the social, cultural and psychological dimensions of ill health
and the context in which it appears that determines the meaning of the disease for patients
(Nettleton, 2006). Without an understanding of patients’ explanations of illness and their
personal beliefs, doctors may make recommendations that are inconsistent with the beliefs
of their patients and the realities in their lives (Agyemang & de-Graft-Aikins, 2014). It has been
indicated that the awareness of doctors of cultural patterns in areas of practice help them
deal with the needs of the patient effectively and compassionately (Seibert et al., 2002;
Hausman & Mader, 2004). However, differences in cultural patterns within the same
geographical location make the knowledge of doctors about areas of practice particularly
important (Shortell & Singer, 2008; Marshall et al., 2012).

51
Helman (2007) points out that the medical model should not be seen as homogenous and
consistent; clinical practice may be influenced by the doctor's personality, training, speciality
and experience, as well as the socio-cultural context. Evidence supports that time pressure,
the need to make quick judgements, cognitive load, task complexity and busyness all impact
on the level and standard of treatment provision (Bodehausen & Lichtenstein, 1987, Gilbert
& Hixon, 1991). Doctors may be especially vulnerable to rely solely on their existing ideas and
understanding due to time pressure, brief consultations and the need to manage very
complex cognitive tasks which are the demanding characteristics of their work (Burgess et al.,
2004; Piko, 2006; Watt et al., 2008; Olson et al., 2009). As a result, they may fail to take into
consideration patients’ beliefs and be swayed by their personal beliefs regarding treatment
and management of the disease (FitzGerald & Hurst, 2017). Hence doctors’ understanding
regarding patient’s disease may become stereotypical if they fail to separate themselves from
their own beliefs.
Doctors may not always see how their understanding is in itself context specific rather than
universal and natural (Helman, 2007). For example, in some cultures joint pains are regarded
as part of the ageing process and therefore not a matter of medical concern for patients and
doctors (Gignac et al., 2006). Clearly, lay definitions and the common ideas surrounding illness
shape doctors’ understandings as well. Studies conducted in various countries indicated that
beliefs and attitudes within a particular socio-cultural context are broadly similar irrespective
of occupation and role (Chulze, 2007; Auber & Rossler, 2007). For instance, a study conducted
in Pakistan found that doctors also had beliefs about religious and supernatural forces such
as the ‘evil eye’ and disease being God’s punishment, in common with the beliefs of patients
(Haddad et al., 2016).
Ascertaining doctors’ understanding regarding HTN is also essential, given that the aetiology
of HTN is complex (Marx, 1976) and the nature of the interaction between relevant risk
factors is poorly understood (Marshall et al., 2012; Aston & Kaul, 2018). This lack of clarity in
the literature suggests that doctors’ perspectives will play a prominent role in their approach
towards treatment. Doctors’ understanding about HTN and its treatment has not been widely
examined in contrast to those of patients. Certainly, as potential consumers of health
services, the general public’s beliefs and attitudes are worthy of investigation due to their
possible influence on behaviours for seeking help and adherence to the advice given by
doctors (Feldman, 1988; Eagly & Chaiken, 1993; McShane & Mitchell, 2013; Al-Noumani et
al., 2019). However, it is equally important to identify doctors’ understanding regarding
aetiology, causes, symptoms, prognosis and goals of treatment and to compare that with
patients to identify differences that can be addressed in order to improve disease
management (Carr & Donovan, 1998; Prior, 2003; Rahman et al., 2015).
2.10.1 HTN treatment guidelines

52
To improve the control of HTN, treatment guidelines have been developed and disseminated
worldwide; the guidelines contain recommendations regarding screening, diagnosis and
treatment of HTN. Treatment guidelines aim to assist doctors in determining the appropriate
management of HTN in order to increase the percentage of patients with controlled blood
pressure (McManus et al., 2012, Kjeldsen et al., 2014; Burnier, 2018). However, the likelihood
of doctors to follow guidelines may depend on their views of them which is influenced by
their knowledge, past clinical experience and the characteristics of the guidelines themselves
(Carey et al., 2009; Appleby et al., 2015; Farshidi et al., 2018).
Knowledge about treatment guidelines
One essential factor for success is the knowledge of doctors about treatment and using the
recommended guidelines (Javadi et al., 2005; Lemos, 2007). Studies carried out in a range of
populations have indicated that poor blood pressure control amongst patients was related to
doctors not adhering to HTN treatment guidelines (Midlöv et al., 2008; Rahman et al., 2015;
Devkota et al., 2016; Teoh et al., 2017; Farshidi et al., 2018). Some researchers reported a
potential explanation for low adherence by doctors to the recommended HTN treatment
guidelines as a lack of knowledge about HTN guidelines, disagreement with the guidelines,
uncertainty about the stage of HTN and a belief that the guidelines are not easily applicable
to daily practice (Midlöv et al., 2008; Banegas et al., 2011; Lee et al., 2015; Rahman et al.,
2015; Barbouni et al., 2017).
An observational cross-sectional study undertaken in five regions of Kuwait has identified
barriers to knowledge and indicated that only 49.1% of the primary healthcare physicians
were familiar with WHO/ISH HTN guidelines and only 23.7% always follow the guidelines (Al-
Ali et al., 2013). In contrast, the results of a study by Windak et al. (2009) in Poland suggested
that lack of knowledge regarding HTN management was not a factor but there were reports
of unfamiliarity in how best to manage certain subgroups. As in the Windak et al. (2009) study,
doctors did not provide complete lifestyle recommendations particularly for patients with
cardiovascular risk. It was also observed that the depth of lifestyle information increased
when a patient presented with HTN in emergency care and additional risk factors and diseases
were also present. These results appear consistent with later studies conducted in other Asian
and European countries (Nayeri et al., 2015; Barbouni et al., 2017; Teoh et al., 2017; Setia et
al., 2017).
2.10.2 Assumptions about patients
By virtue of the technical knowledge and skills of doctors they are perceived to have an
authoritative role during the doctor-patient encounter and often make value judgements
about patients that influence disease outcome (Nettleton, 2006). Bury (1997) further
elaborates on this potential for conflict and suggested that its source lies in basic assumptions
held by doctors and guesses they make about how patients should behave. Doctors generally

53
believe that patient non-adherence to prescribed drug treatment is a significant barrier to
disease control. However, the literature does not support this contention and it has been
argued that patient non-adherence to treatment is also doctor related (Martin et al., 2005;
Kleinsinger, 2010; Rahman et al., 2015).
Aira et al. (2003) has found that some doctors were less likely to ask about smoking and
drinking in patients due to the assumption that such issues relate to their private lives.
Similarly, a survey study has indicated that doctors were less likely to recommend lifestyle
changes in elderly hypertensive patients due to the assumption that older patients are less
likely to adopt the changes in their lifestyle as compared to younger patients (Johansson et
al., 2005). Brobeck (2014) has highlighted that lifestyle recommendations were discussed
more often with men as compared to women due to doctors’ assumptions that women do
not adhere to healthy lifestyles.
Doctors are believed to be the main source of health information (Clarke et al., 2013) and not
only are ideally positioned to provide this information but are also viewed by patients as a
reliable source of disease-related information and treatment (Martin et al., 2005). However,
the evidence suggested that doctors had different expectations and wanted patients to take
charge in order to improve their blood pressure and lifestyles (Jallinoja et al., 2007; Banegas
et al., 2011; Barbouni et al., 2017). Banegas et al. (2011) have noted that doctors did not
change antihypertensive treatment in many uncontrolled hypertensive patients in Spain
because they assumed it to be unnecessary.
Many doctors in the study assumed that small elevations in blood pressure levels were not
important and posed little risk to patient health. This has also been explored further in a study
carried out in urban areas of India which indicated that most doctors believed that dietary
changes were difficult to adopt by the patients due to assumptions about the behaviour of
patients and affordability issues associated with healthy eating (George et al., 2016). Likewise,
a survey in Finland about the views of doctors in delivering lifestyle advice revealed that
doctors perceived the patients to be responsible for their own lifestyle management and the
role of the doctor being limited in terms of making change happen (Jallinoja et al., 2007). A
majority of doctors in the study agreed that a barrier to the treatment of lifestyle-related
conditions was the unwillingness of patients to change their habits. These studies were
conducted in three different countries and documented that doctors believe they can make
judgements and decisions about the information appropriate for their patients.
A cross-sectional study conducted in France evaluated that doctors with an optimistic
approach towards HTN appeared more empathetic and supportive towards patients and were
successful at controlling blood pressure (Consoli et al., 2010). However, a handful of studies
in the review suggested that doctors being judgemental led to differentials in decisions about
HTN treatment and conflict when encountering patients (Jallinoja et al., 2007; Shawahna et

54
al., 2012; George et al., 2016). For instance, literacy, educational background, dress and
appearance were important indicators at the time of clinical decision-making amongst
doctors originating from urban areas in Pakistan (Shawahna et al., 2012). The study also
suggested that the personal characteristics of doctors and beliefs about patients influenced
their behaviour and the quality of service provided. Likewise, it has been reported in another
study that some doctors may deliver less information to patients who have lower socio-
economic status because they assume them to be less educated, not intelligent and less
rational (Moret et al., 2017).
Hence doctors’ own beliefs not only shape their attitudes but also the clinical interaction,
information provision and interaction with patients. Research shows that patient satisfaction,
commitment to treatment and perceived outcomes of care are greater when the doctor and
patient achieve a shared understanding of disease (Thompson, 2007; Graham & Brookey,
2008; Vahdat et al., 2014; Kennedy et al., 2017). However, it is also clear from the review of
the above literature that doctors’ beliefs are influenced by complex and multifaceted
influences such as their knowledge, socio-cultural context and personal experiences.
2.11 Conceptual Framework
Review of the literature clearly shows that beliefs are important determinants of actions,
choices and decisions that people make. What people believe about the nature of an illness
and its symptoms affects how they deal with it. Hence, beliefs provide an explanatory
framework and help people to make sense of their ‘lifeworld’ and describe the definitions and
explanations of health made in a particular context (Blaxter, 1990; Williams & Popay, 1994;
Popay et al., 1998; Conner & Norman, 2008; Kennedy et al., 2017). Therefore, the concept of
health beliefs served as a conceptual framework for the current study as beliefs seek to
account for attitude and experiences.
The conceptual framework will guide the study in four important ways. Firstly, it will inform
the collection of qualitative data including accounts of social, cultural and ritual symbolism
(Bhui & Bhugra, 2002). This was considered important in the context of patients and doctors
in Pakistan as the literature review indicates that beliefs are influenced by the specific socio-
cultural context of living and working in Pakistan. Secondly, as evidence supports that causes,
symptoms and treatment often do not carry the same meanings when they are framed
differently or viewed from different experiences (Hannay, 1979; Kleinman, 1988; Conard &
Barker, 2010; Rosendal et al., 2013); it is likely that patients and doctors have their own
personal understandings regarding HTN management. Patients’ interpretation of HTN, causes
and treatment can vary too and may appear inconsistent to doctors.
Thirdly, within the belief framework, the position of all parties is given equal importance; in
other words, a patient’s experience of illness will be treated as being as important as the
doctors. Fourthly, the framework was chosen because it goes hand-in-hand with calls to

55
improve the quality of clinical care for patients with chronic illness (WHO, 2016). In the
therapeutic encounter the doctor’s role is important, and he or she should ascertain the
patient’s beliefs (Main et al., 2010; Nimmon & Stenfors-Hayes, 2016) so that the conversation
is geared towards the maximum production of new knowledge and learning. If a doctor is
unable to understand and address the patient’s beliefs, the person’s worldview will remain
intact and meaningful learning will not occur. However, doctors’ own understanding about
disease management is equally important and will determine the type and extent of
recommendations they might make to patients.
Studies conducted in countries other than Pakistan have found that variations between the
beliefs of patients and doctors regarding disease management are often associated with poor
HTN control (Gascón et al., 2004; Marshall et al., 2012; Rahman et al., 2015). Information
about the shared understanding of patients and doctors about HTN management in Pakistan
is lacking from the evidence base and therefore represents a major gap in the literature. As
the systematic review identified there is clearly a dearth of methodologically rigorous studies
looking at patients’ and doctors’ beliefs surrounding HTN, its treatment, particularly in Punjab
(the most populated province) and existing research does not go far enough to consider how
patients’ and doctors’ understanding may influence HTN management.
2.12 Summary
This chapter has presented and reviewed literature relevant to the current study. The beliefs
of patients and doctors about HTN in Pakistan have been explored by searching the relevant
databases to address the first research question. This is followed by looking at broader
literature to examine how culture, religion and social values may influence people’s health
beliefs within certain contexts. The chapter has presented a range of issues that influence
both the beliefs of patients and doctors and their experiences with regard to HTN
management.
Studies highlighting patients’ and doctors’ understanding of HTN, drug treatment and lifestyle
changes which include exercise, dietary changes, smoking cessation and low alcohol
consumption in relation to HTN have been explored. Finally, the chapter discusses that
patients’ and doctors’ understanding of HTN management can be understood within the
framework of health beliefs that centres on explanations and understanding acquired through
actions and experience. A lack of qualitative research about the views of patients and doctors
surrounding HTN management warrants further exploratory research in this area within the
Pakistani context. Therefore, the next chapter will discuss the research methodology and
design of the current study.

56
Chapter 3: Methodology
The intention of this study is to generate rich data from patients and doctors to give insights
into how beliefs informed their understanding of HTN and its management. In order to gather
insights, qualitative research was considered appropriate to achieve the aims of the study.
This chapter describes the theoretical viewpoint of social constructivism and the rationale for
selecting this to inform the methodology of this study. It is followed by a discussion of the
methodology used and the methods employed in data collection. The chapter will outline the
process of data analysis, ethical issues and measures used to establish rigour for the study.
Finally, the chapter will present the researcher’s reflections on the research process and the
dilemmas encountered during the data collection.
3.1 The Nature of Qualitative Research
Qualitative research is a systematic approach that covers different forms of enquiry and helps
to reveal a social phenomenon (Merriam, 1998; Grove et al., 2014). It helps researchers to
provide an interpretation of the social world of research participants by focusing on their
experiences, perspectives and histories (Ritchie & Lewis, 2003). According to Silverman (2010)
qualitative research is generally conducted in the natural setting of the subject in order to
gain an ‘emic’ perspective.
Some of the key defining qualities of qualitative research highlighted by Denzin and Lincoln
(1994) are that qualitative research is a naturalistic, interpretative approach concerned with
understanding the meanings which people attach to phenomena (actions, decisions, beliefs,
values) within their social worlds.
‘’The way in which people being studied understand and interpret their social reality is one of the
central motifs of qualitative research” (Bryman, 2012 p.8).
The essential characteristics of qualitative research include: a belief in social realities, focus
on the emic perspective, meanings and interpretations (Denzin & Lincoln, 2005).
3.2 Methodological Paradigm for This Study
A paradigm is a set of common beliefs and agreements shared amongst scientists and
researchers about how problems should be understood and addressed (Kuhn, 1962, Creswell,
2013). A clear consideration of the research paradigms is critical to ensure that the research

57
design is positioned in terms of ontology10, epistemology11, positivism12, post-positivism13 or
social constructivism.
Social constructivism is an approach that focuses on how individuals come to construct and
apply knowledge in socially mediated contexts (Thomas et al., 2014). Honebein (1996)
describes the constructivism philosophical paradigm as an approach that asserts that people
construct their own understanding and knowledge of the world through experiencing things
and reflecting on those experiences. The fundamental principle of this theory is that
knowledge is a human construction and that the learner is an active participant in the learning
process (Gergen, 2015). Constructivism resonates well with health beliefs framework as it
enables eliciting rich information related to people perceptions of issues (Arksey & Knight,
1999). As highlighted by Creswell (2007), constructivism asserts that people's beliefs about
illness are subjective, multiple and influenced by their social, cultural and historical context.
Constructivism is founded on three assumptions about learning (Savery & Duffy, 1995;
Gredler, 1997; Thomas et al., 2014). Firstly, learning is a result of the individual’s interaction
with the environment. Thus, according to this principle knowledge is constructed as the
learner makes sense of their experiences in the world. Secondly, cognitive dissonance, or the
uncomfortable tension that arises from holding two conflicting thoughts at the same time, is
the motivation for learning. Thirdly, the social environment plays a critical role in the
development of knowledge. Thus, researchers adhering to this paradigm try to understand
the world they live in, interpret the meanings of others and make sense of their day-to-day
life and interactions.
According to Denzin and Lincoln, (1994) the ontological and epistemological views considered
by researchers contributed to the existence of several approaches. The way in which
researchers plan their research questions is likely to be partly determined by their existing
ontological assumptions (Bryman, 2012). That is, the researcher’s perspective on the form
and nature of reality and, therefore, what there is that can be known about it (Denzin &
Lincoln, 1998). The formulation and approach I have adopted in developing and addressing
my research questions reflects my own ontological stance, which has been influenced by my
professional background.
As a Pakistani qualified medic, I have experience of working with doctors and hypertensive
patients in a hospital setting, as a former house officer. It was during the face-to-face
encounter that patients usually talked to me about different aspects of their lives and
circumstances that they believed were key influencing factors in the management of their
HTN. From this insider experience, I am interested in revealing the individual’s understanding
10 The term ontology refers to a branch of philosophy concerned with articulating the nature and structure of the world (Wand & Weber, 1993). It specifies the form and nature of reality and what can be known about it. 11 Epistemology refers to the nature of the relationship between the researcher (the knower) and it denotes “the nature of
human knowledge and understanding that can possibly be acquired through different types of inquiry and alternative
methods of investigation." (Hofer & Pintrich, 1997)
12 The positivists believe that the world is external (Carson et al., 2002) and that there is a single objective reality to any
research phenomenon or situation (Hudson & Ozanne, 1988). 13 Post-positivism has an ontological basis where reality is assumed to exist but is imperfectly understood because of the
complexity of human nature (Creswell, 2007).

58
of the phenomenon as contextualised in a social setting. In this study, my lens will be social
constructivism which seeks to explore how meanings are created from the standpoint of the
study participants.
3.2.1 Constructivism or constructionism?
The terms social constructivism and constructionism tend to be used interchangeably and are
considered under the generic term ‘constructivism’, particularly by Charmaz (2003). However,
the social context is at the centre of ‘meaning making’ in social constructionism and attention
is placed on the ‘knowing’ that is created through shared production (Crotty, 1998). In
contrast, within a social constructivist paradigm, the individual is at the centre of the meaning
making in the experience. Therefore, the focus of constructivism is on the individual’s learning
that takes place due to their interactions within a particular social context (Avis, 2005).
Constructivism is a research paradigm that rejects the existence of an objective reality,
“asserting instead that realities are social constructions of the mind, and that there exist as
many such constructions as there are individuals” (Guba & Lincoln, 1989 p.43). Moreover,
constructivism emphasises the importance of culture and context in an individual’s
understanding and as a result, construction of knowledge is based on this understanding (Kim,
2001).
In other words, constructivists believe that social reality is constructed by individuals as they
assign meaning to the world around them (Brekenridge et al., 2012). This concurs with the
argument that health means different things to different people in health or other settings
(Seedhouse, 2004). Within this perspective, the patient’s reality about health and disease can
be different to that of the doctor’s reality and expertise. This is due to the fact that different
people build the same phenomenon in different ways (Strauss & Corbin, 1990). Thus, there
are multiple ways to understand the world, each regarded as ‘true’ by the individuals who
describe them. For this, constructivist researchers try to understand the meaning of the
interpretations of the study participants and insist that truth is relative and dependent on
one’s viewpoint (Brekenridge et al., 2012).
3.3 Choosing the Research Methodology
The methodology is a strategy, plan of action, process or design, lying behind the choice and
use of a toolkit of research methods (Crotty, 1998). Many different methodologies may have
the same underlying theoretical perspective and each methodology may be implemented
using different combinations of research methods. Approaches to qualitative research, such
as ethnography, narrative research, phenomenology and case study were considered for the
current research, however, none provides a means to explore the perspectives of patients
and doctors about HTN and its management specific to the aims of the study.
Grounded theory approaches are concerned with human perceptions and how people manage problematic situations in their daily lives through a process of data collection that is often described as inductive in nature (Morse, 2001). Grounded theory research is a naturalistic enquiry and commonly used by constructivist researchers (Guba & Lincoln, 1989).
59
Glaser and Strauss who originated the process of grounded theory argue that a grounded theory study involves the generation or the discovery of a theory, which is ‘grounded’ in the data collected from participants (Glaser & Strauss, 1967). However, since this work researchers have used grounded theory without it being a ‘true’ or grounded theory study and used this approach as a set of methods (Morse et al., 2009; Charmaz, 2006). A critical discussion on the grounded theory approach is described later in this chapter (sections 3.3.2).
According to Guba and Lincoln (1994) grounded theory provides rigorous insights into the
areas that are unknown or hidden to the researcher. Theory induction is an evolutionary and
inductive process that happens as the research proceeds and in this way grounded theorists
explore individual accounts and explanations to generate a theory at the end of the research
process rather than testing hypotheses from existing theory (Charmaz, 2006). However,
researchers can also use grounded theory methods to analyse data and gain insights into a
social phenomenon to generate a theory as long as they avoid labelling their studies as
grounded theories (Foley & Timonen, 2015). The grounded theory principles used in this study
are provided in section 3.3.3.
3.3.1 Debates in development of grounded theory approaches
Since the development of grounded theory (Glaser & Strauss, 1965) the methodology has
passed through different stages and diverged into three different schools of thoughts. The
first is classic grounded theory, which is associated with Barney Glaser; the second is evolved
grounded theory linked with Anselm Strauss, Juliette Corbin and Adele Clarke; and the third
is a constructivist grounded theory, which stems from work by Kathy Charmaz.
Charmaz has reshaped grounded theory and methodology considering relativist ontology
(many possible realities) and subjectivist epistemology (understanding is constructed by a
researcher and research participant) (Charmaz, 2003). Constructivism assumes that there are
multiple social realities concurrently rather than one ‘real reality’. Charmaz argued that
Strauss and Corbin (1990) were being too unrealistic. She states that both approaches to
grounded theory assume an objective external reality that exists and can be identified and
therefore, takes a positivist and objectivist stance. This is due to the fact that Glaser warns
the researchers against exploring the literature before entering the research field. This
ignoring of the literature has been highly questioned by critics who propose that the literature
and preconceptions instead be ‘bracketed’ and used for comparison with emerging categories
(Hallberg, 2006).
Charmaz states that it is not possible to fully remove oneself from literature or previous
experiences to conduct a purely objective analysis of data. She further adds that the prior
knowledge of the researcher adds to the data collection and in the interpretation of that data.
Charmaz’s approach to grounded theory acknowledges the role of the researcher in
constructing meaning with the study participants. Hence, Charmaz advocates a constructive
approach that assumes multiple social realities.
According to Charmaz (2006) the researcher takes a reflexive stance and studies how, and
sometimes why, participants construct meanings and actions in specific situations. She asserts
that in qualitative research we have to enter the world we are studying and that we need to
60
learn from the outside (Charmaz, 2006). She states that this requires the focused attention of
the researcher to discover what is important from the viewpoint of participants and what
things really mean to them. Therefore, she stresses the importance of acknowledgement by
the researcher of their role as well as the role of respondents in constructing the research
data and theory. She states that the researcher’s analysis tells a story about people, social
processes and situations. The researcher constructs a story and it does not simply unfold
before the eyes of an objective viewer.
Thus, according to Charmaz, grounded theory approaches should focus on meanings, actions
and processes in the studied social context. Additionally, the analysis in grounded theory
which relates to time, culture and context reflect both the researcher’s and the participant’s
way of thinking (Mills et al., 2006). The researcher’s interpretative understanding, rather than
the researcher’s explanation of how the participant creates his or her understanding and
meaning of reality is the result of the analysis (Charmaz, 2006).
3.3.2 A critical discussion of a grounded theory approach
As highlighted in section 3.3.1, there are three main schools of thought in grounded theory
which appear to be partly in contradiction with each other due to variations in epistemological
positions. A review of the available literature provides a wealth of examples regarding a
chequered history of grounded theory and fundamental differences in the development of
the three strands (Glaser & Strauss, 1967; Strauss & Corbin, 1990; Charmaz, 2014). Some
critiques on the methodology of grounded theory presented in the literature are discussed
below.
A key feature and outcome of grounded theory is to generate or discover a theory from data
(Glasser and Strauss, 1967). However, one of the main criticisms of grounded theory is that it
does not result in the production or generation of a formal theory but provides a rigorous
approach to the generation of concepts (Bryman, 2008). To claim that application of grounded
theory always can and must result in a theory is misleading and has been criticized strongly
(e.g. Bryant, 2003; Timonen et al., 2018).
Later exponents of the methodology view grounded theory methods ‘as a set of principles
and practices, not as prescriptions or packages and emphasizes flexible guidelines, not
methodological rules, recipes and requirements’ (Charmaz, 2006, p.11). Scholars' attempts to
modify grounded theory have resulted in competing accounts that make it difficult to
determine the precise method of implementing the methodology (Bryman 2008; Lawrence &
Tar 2013). However, it has been suggested that the common outcome from a grounded
theory can result in a greater conceptual clarity, explanation of a social process, lift the data
to the conceptual level or develop a framework to explain a phenomenon (Thornberg, 2012;
Wu & Beaunae, 2014; Timonen et al., 2018).
There is an ongoing discussion about what the end product of a grounded theory study should
look like (Kelle, 2007; Thornberg, 2012). Becker (1993) argues that many researchers claim to
conduct a pure grounded theory study, but they deliver elaborate descriptive studies.
However, prominent scholars such as Strauss and Corbin (1990) acknowledge that formal
theory building should no longer be the only end goal and they support the wider application

61
of this methodology for different purposes such as conceptual understanding of a
phenomenon. Researchers are, therefore, advised to acknowledge the difference between
doing a grounded theory study (i.e. generating a theory) and drawing on grounded theory
principles/methods such as coding, constant comparative analysis and memo writing to
support the development of themes (Charmaz, 2006; Judilh & Holton, 2007; De Bie & De Poot,
2016).
Another critique associated with grounded theory is the variation in terminologies amongst
grounded theory strands (Brymat, 2008). For instance, Glaser and Strauss (1967) refer to a
process of substantive coding (also referred as open coding) followed by selective coding and
theoretical coding (Holton & Walsh, 2016). Charmaz, in contrast suggests initial (open line)
coding first followed by focused and theoretical coding (Charmaz, 2014). Likewise, Strauss
and Corbin (1990) introduced new concepts in their approach of grounded theory such as
code notes, matrix, traditional matrix, (another type of memo-writing) and dimensions. This
inconsistency in various terms between different grounded theory versions does not assist
researchers when deciding whether to use grounded theory.
An obvious noted limitation is the time it takes to conduct a grounded theory study (Bartlett
& Payne, 1997; Bryman, 2008). Hughes and Jones (2003) take issue with the contention that
implementing theoretical sampling in grounded theory lengthens the data collection process.
Theoretical sampling is the likely component of grounded theory that is not usually followed
due to time constraints. Hence, researchers often decide on the study sample before the
empirical work starts (Mirzaei et al., 2012; Naseeba, 2011; Davoudi et al., 2016). Likewise,
transcribing recorded data followed by analysis and returning to the relevant literature after
data analysis in grounded theory requires time that make this a lengthy process (Bartlett &
Payne, 1997; Thomas & James, 2006; Ke & Wenglensky, 2010; Elliot & Higgins, 2012).
3.3.3 The present study
Unlike a traditional grounded theory, this study does not aim to develop a formal theory
rather it seeks to glean insights that might explain or illuminate HTN management. The
researcher selected a conceptual framework (see chapter two) after reviewing relevant
literature to guide the inquiry, which departs from the foundational tenets of the
traditional/classic grounded theory whereby theories emerge from the data. Hence, this
qualitative study draws on grounded theory principles for guidance rather than adhering to
strict rules to develop a new theory from the data (Charmaz, 2006).
The study employed and adapted constructivist grounded theory principles as described by
Charmaz (2006), which means that the technique of constant comparison was used in order
to ground the findings in the data. In the current study, simultaneous involvement in data
collection and analysis, the use of constant comparative analysis technique, initial coding,
selective coding, generation of categories and memo writing were used. The grounded theory
processes such as theoretical coding, delimiting or sorting were not employed as these are
typically used for theory development. As explained earlier (chapter two), there are limited
rigorous qualitative studies available regarding hypertensive patients and the beliefs of
doctors about HTN in the Pakistani context. Moreover, the available literature does not go far

62
enough to explain patients’ and doctors’ beliefs of HTN management. Therefore, using
grounded theory techniques to analyse participant data, the present study aims to explore
how study participants construct their beliefs on HTN management. In order to achieve this,
the researcher needs to acknowledge her role in the construction of meaning, as she listens
to and understands the accounts of the informants. Therefore, an ongoing reflective approach
through the writing field notes and memo was adopted (Charmaz, 2006).
Reading relevant empirical literature highlighted two particular studies (Naseeba, 2011;
Namukwaya et al., 2017) that used ground theory principles, and this informed the use of
these principles for the study described here. A qualitative study undertaken in the United
Arab Emirates drew on grounded theory methods (e.g. a comprehensive literature review,
use of the constant comparative analysis technique, coding and memo writing) relevant to
the current study (Naseeba, 2011). Naseeba (2011) used the constructivist grounded theory
principles as described by Charmaz (2006) in order to explore patients’ and doctors’
perceptions of metabolic syndrome by using semi-structured interviews, in addition, to focus
group discussions to identify themes. Likewise, Namukwaya et al. (2017) study that explored
the understanding of and beliefs of patients with heart failure by using in-depth interviews
and this was guided by constructivist grounded theory principles. Researchers employed
some grounded theory data analysis principles similar to those selected for the current study
(e.g. line-by-line coding, focused coding and constant comparative analysis).
3.4 Data Collection Methods for the Current Study
In this study, the aim was to explore the views of patients and doctors about HTN and its
management in Pakistan. Thus, the following section explains the selected qualitative data
collection tool and rationale behind the choice in order to answer the research questions.
3.4.1 Semi-structured interviews
Qualitative research makes use of many methods to collect data, however, the interview is
the most frequently employed method. The purpose of a qualitative interview is to explore
the views, experiences and beliefs of individuals on a specific subject and to gain ‘deeper’
understanding of a social phenomenon (Edwards & Holland, 2013). Therefore, qualitative
interviews help us to share the world of others, to find out how people understand and make
sense of the world that sits within a social constructivist paradigm. Edwards and Holland have
highlighted the core features of semi-structured qualitative interviews:
” A thematic, topic-centred, a biographical or narrative approach where the researcher has
topics, themes or issues they wish to cover, but with a fluid and flexible structure.” (Edwards
& Holland, 2013. p.3).
A semi-structured interview is used when information of a more detailed and in-depth nature
is required. In the course of the semi-structured interview, the interviewer has a certain
amount of room to adjust the sequence of the questions to be asked and to add questions
based on the context of the responses of the participant. A typical semi-structured interview
schedule includes broad open-ended questions, allowing flexibility in the ordering or

63
rephrasing of questions and the inclusion of additional ones (Bryman, 2012; Fielding &
Thomas, 2016). The qualitative interviewer uses open-ended questions and this is an
appropriate technique when the depth of meaning is important and research is primarily
focused on gaining insight and understanding (Ritchie & Lewis, 2003). Therefore, semi-
structured in-depth individual interviews with patients and doctors have been used in this
study. The in-depth interviews focused on how individuals understand and manage their
condition and factors influencing the implications of lifestyle recommendations in HTN
treatment.
3.5 Study Design
The following section describes the pilot study, development of topic guides/questions,
selection of hospitals, recruitment of participants, data collection and analysis.
3.5.1 Pilot study
To confirm the feasibility of the current project, a pilot study (ethics protocol
cHSK/PGT/UH/02214) was conducted in one district hospital in December 2015-January 2016.
The district hospital is located in a city of the Punjab province. Written permission to conduct
a pilot study was obtained from the hospital medical superintendent in advance.
The aims of the pilot study were:
• To confirm the feasibility of the main research project.
• To assess whether patients and doctors could be recruited successfully in an
Outpatient Department14 (OPD).
• To assess whether interviews would be an appropriate method to use.
• To identify any ethical challenges the study would raise.
The pilot study helped to refine the study design for the main project in terms of methods.
For example, it demonstrated that semi-structured interviews were appropriate methods to
explore participants’ beliefs regarding HTN and lifestyle recommendations for the main study;
and it identified practical potential challenges associated with the recruitment of participants.
Twelve interviews (six hypertensive patients, six doctors) were conducted in the pilot phase.
Details of changes that were made after the pilot in terms of participant recruitment and topic
guides are discussed below.
Recruitment
• The pilot study identified that all hypertensive patients attend medicine OPD for
services such as HTN consultation, diagnosis and treatment. Hence patients were
recruited in the medicine OPD area for the pilot and main study.
14 Outpatient Department (OPD) also called outpatient clinic in the hospital that provides diagnostic service and treatment for patients who do not need to stay overnight. It is the section of the hospital where patients are provided with medical consultations.

64
• It was decided for the pilot study that the researcher would recruit the patients in the
OPD waiting area and visit their home later to conduct interviews. The pilot study
revealed that patients preferred to give the interviews in a hospital setting and
immediately following their recruitment rather than at a later time. Therefore, none
of the patients were interviewed at home for the main study.
• For the pilot study, it was anticipated that a quiet area of the hospital lawn would be
used to conduct patients’ interviews. However, the nursing staff allowed the
researcher to use one of their available empty rooms in the pilot phase. Therefore, an
empty treatment room was requested from each hospital medical superintendent
prior to conducting interviews in the main study.
• Some patients had difficulties in reading the participant information sheet and
consent form due to poor vision or literacy issues, therefore, the researcher did not
recruit them in the pilot phase. For the main study, it was decided that the researcher
would read the patient information sheet and consent form for patients with poor
vision and literacy issues. Moreover, based on the pilot findings a thumb impression
was used for those who could not provide a signature on the consent form.
• The pilot phase identified that recruitment of doctors was challenging due to their
busy schedule and constraints on time. Hence, to establish trust and familiarity was
essential to make recruitment efficient. The researcher showed personal interest in
doctors’ activities and often involved them in informal discussions to establish
rapport. This subsequently enabled the researcher to be recognised amongst doctors,
which led to more interactions and communication. The same strategy was adopted
in the main study.
• The pilot study identified that a snowball sampling technique15 was appropriate to
identify potential doctors. Some doctors nominated others and provided contact
details of colleagues who were on holiday. The researcher contacted these doctors by
making phone calls to inquire about willingness to participate. This snowball sampling
technique was implemented in the main study to recruit doctors.
• Patient recruitment was a time-consuming aspect of the pilot study as the number of
patients willing to participate varied each day. For instance, one day two patients were
recruited successfully, in the next four days the researcher was unable to recruit any
patients due to patient time constraints, lack of interest and unwillingness for an
interview to be audio recorded. Therefore, more time (3-4 months) in each hospital
was incorporated to recruit participants for the main study.
• The pilot study identified that doctors in the medicine OPD were an important way of
inviting hypertensive patients to participate in the study. Hence doctors were
provided with patient information leaflets to hand to the patient after a consultation.
This strategy was added to the main study for patient recruitment.
15 Snowballing sampling involves asking your current respondents who have already been interviewed to identify or
recommend other people they know who may fit the selection criteria (Crabtree & DiCicco-Bloom, 2006; Groenewald, 2014).

65
Topic guides
Based on the pilot interviews, some of the terminology in the topic guides was changed,
additional prompts were added, and the sequence of questions was further developed. It was
recognised in the pilot study that many patients had difficulty in understanding the term
‘hypertension’, consequently this was changed to high blood pressure throughout the
updated topic guide for patients. The tables (4i for patients and 4ii for doctors) in Appendix 4
lists the initially planned interview questions and the changes made after the pilot study. The
reasons for the individual changes, additions and deletions of questions are also explained.
If the interviewee had difficulty answering a question or provided only a brief response, the
researcher used cues or prompts in the pilot to encourage the interviewee to consider the
question further. The open-ended questions allowed for follow up questions and prompts
based on the answers given by the participant (Britten, 1995; Covell et al., 2012; Brinkmann,
2013; Singer & Couper, 2017). Consequently, in the main study, the researcher used a sheet
with planned prompts relevant to each question (see Appendix 4) to elicit information from
the participants.
The pilot interviews identified that it was possible to modify and change the order of any
question in response to the interviewee’s answers. Hence questions related to difficulties in
managing HTN were moved to the end of the interview. It emerged during the pilot study that
talking about high blood pressure at the beginning worked better for the interviewees.
Conversely, sharing difficulties in HTN control at the start put them under pressure. Overall
the pilot study provided a valuable opportunity to examine the feasibility of the main research
project, participant recruitment and interview topic guides. Moreover, it helped in identifying
practical challenges; lessons learned from the pilot study are further discussed in Appendix 5i
and 5ii. The pilot interviews were fully transcribed and then discussed with my supervisors.
This initial feedback from the supervisors assisted me in obtaining more information during
the interviews and also improve my interviewing skills.
The updated interview guides (see Appendix 6) were further tested with two hypertensive
patients and one doctor via Skype in Pakistan, who were approached through personal
contacts and the interviews were informal in nature. These updated topic guides were
translated into the national language Urdu before conducting any interviews (Appendix 7).
3.5.2 Recruitment of hospitals for the main study
The systematic review (chapter two) identified a paucity of rigorous qualitative research
exploring patients’ and doctors’ understanding of HTN particularly in the Punjab province.
Therefore, six urban government-run hospitals (three district and three tertiary) in four big
cities of Punjab were selected randomly to be approached by the researcher. After
identification of the potential hospitals, the medical superintendent of each hospital was
identified to approach regarding access.
After conducting a pilot study in one urban hospital in Pakistan, the researcher was fully aware
of the steps required to approach the medical superintendents. For instance, a brief
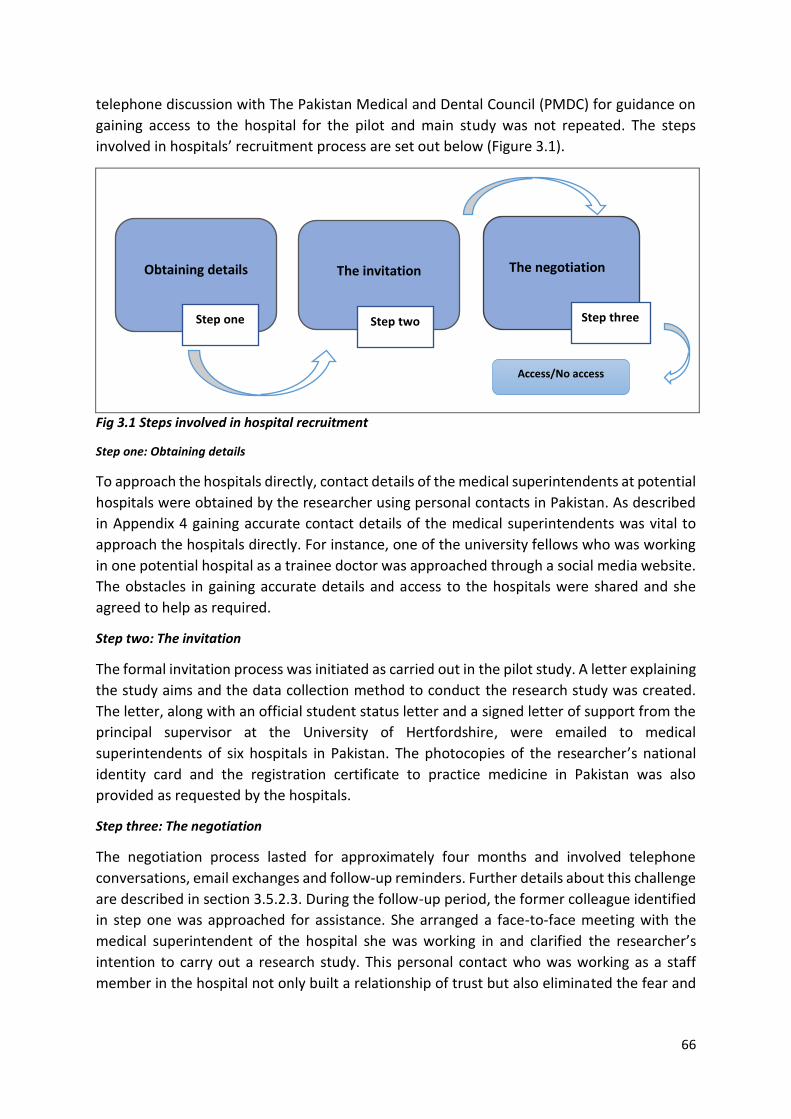
66
telephone discussion with The Pakistan Medical and Dental Council (PMDC) for guidance on
gaining access to the hospital for the pilot and main study was not repeated. The steps
involved in hospitals’ recruitment process are set out below (Figure 3.1).
Fig 3.1 Steps involved in hospital recruitment
Step one: Obtaining details
To approach the hospitals directly, contact details of the medical superintendents at potential
hospitals were obtained by the researcher using personal contacts in Pakistan. As described
in Appendix 4 gaining accurate contact details of the medical superintendents was vital to
approach the hospitals directly. For instance, one of the university fellows who was working
in one potential hospital as a trainee doctor was approached through a social media website.
The obstacles in gaining accurate details and access to the hospitals were shared and she
agreed to help as required.
Step two: The invitation
The formal invitation process was initiated as carried out in the pilot study. A letter explaining
the study aims and the data collection method to conduct the research study was created.
The letter, along with an official student status letter and a signed letter of support from the
principal supervisor at the University of Hertfordshire, were emailed to medical
superintendents of six hospitals in Pakistan. The photocopies of the researcher’s national
identity card and the registration certificate to practice medicine in Pakistan was also
provided as requested by the hospitals.
Step three: The negotiation
The negotiation process lasted for approximately four months and involved telephone
conversations, email exchanges and follow-up reminders. Further details about this challenge
are described in section 3.5.2.3. During the follow-up period, the former colleague identified
in step one was approached for assistance. She arranged a face-to-face meeting with the
medical superintendent of the hospital she was working in and clarified the researcher’s
intention to carry out a research study. This personal contact who was working as a staff
member in the hospital not only built a relationship of trust but also eliminated the fear and
Obtaining details
The invitation
The negotiation
Step three
Access/No access
Step two Step one

67
mistrust which was depicted in the beginning by the medical superintendent. As a result, a
written permission to conduct the study was granted from this hospital.
Four of the other five potential hospitals were not recruited; one expressed no interest and
did not reply to correspondence; three expressed concerns regarding researcher identity due
to residing in the UK. In the second hospital to be recruited, the medical superintendent
expressed an interest in participating and responded positively. To approve a signed written
permission, an additional letter from the principal supervisor was requested with a fresh date
on it. A later meeting with the medical superintendent before the start of fieldwork elicited
the reason behind the positive response. The medical superintendent had personal
experience of completing a research degree outside of Pakistan and could relate to the
challenges a native researcher might encounter (section 3.9.1). After four months of follow
up with potential hospitals, two were successfully recruited. Paperwork (the study protocol
participants’ information sheets and consent forms) were shared with the medical
superintendents of the recruited hospitals after successfully obtaining ethics approval from
the University of Hertfordshire Health and Humans Sciences Ethics Committee.
3.5.2.1 Hospital settings
The two recruited hospitals are situated in Punjab which is the second largest and most
populated province of Pakistan. The first hospital is located in one city of South Punjab and is
a tertiary care hospital. There are approximately 1600 beds and the hospital employ over
4000 staff. The hospital is a hub of clinical expertise in specialities such as medicine, surgery
and gynaecology. There are seventeen OPDs: medicine, chest medicine, surgery, ear, nose
and throat, gynaecology, dermatology, neurology, endocrinology, cardiology, physiotherapy,
pathology, orthopaedics, paediatrics, psychiatry, ophthalmology, rheumatology and urology.
The inpatient care16 units are: medicine, cardiology, intensive care unit, diagnostic imaging
and ultrasound, general surgery, gastroenterology, paediatrics, maternal and neonatal unit,
urology, dermatology, neurology, physiotherapy, rheumatology and renal unit. The hospital
accident and emergency department was established in 2005 with a capacity of 100 beds and
deals with emergency admissions twenty-four hours a day. The hospital is affiliated with a
medical college and provides training to undergraduates and post-graduate students.
The second hospital is a District Headquarter Hospital (DHQ), the largest in the city and
located in the north of Punjab. The hospital has approximately 250 beds and a workforce of
around 2500 staff. The hospital provides healthcare services such as diagnostic, clinical and
surgical to the residents of the city. Seven outpatient departments that are currently
operating in the hospital are medicine, surgery, ear nose and throat, gynaecology, paediatrics,
radiography and orthopaedics. More than 5000 patients are served on a daily basis across the
OPDs by 30 doctors in different departments. The hospital inpatient departments are
medicine, surgery, gynaecology, paediatrics and orthopaedics. The Urgent Accident and
Emergency Department operate twenty-four hours.
16 Inpatient care generally refers to any medical service that requires admission into a hospital.

68
The name of the hospitals, medical superintendents and study participants are not revealed
in this study to maintain confidentiality and protect privacy as per the study’s ethics approval.
3.5.2.2 The role of medical superintendents
As the chief supervisor of the hospital, the medical superintendent, commonly known as ‘MS’
in Pakistan has a legal obligation to ensure high-quality patient care and must strive to
improve medical services in the hospital (Pakistan Today, 2018; Sajid & Asad, 2018). The
medical superintendent assigns duties amongst heads of the departments, senior and junior
doctors, nursing, paramedic and administrative staff (Glouberman, 2013). They have
administrative powers to supervise all matters relating to hospital management, patient care,
discipline in the hospital including punctuality, conduct and performance.
Issuing necessary instructions and approval regarding professional events such as workshops,
seminars, refresher courses and activities in the hospital is also included in the duties of a
medical superintendent (Bliss, 2000). Likewise, medical superintendents have the right to
limit researchers access and may not support the conduct of research in their hospitals
(Stanton et al., 1996). In this study, the medical superintendents were the gatekeepers17 as
they had the power to grant or deny permission for access to potential research participants.
Positive influence from the gatekeepers can be invaluable to the research process by
facilitating the smooth running of research activity to completion (Wassenaar & Singh, 2016;
McFadyen & Rankin, 2017).
At times, gatekeeping can be problematic limiting or denying researchers access to study
sites. This may be based on gatekeepers’ assumptions and preconceptions about the
implications of the research (Okumus et al., 2007; Clark, 2011). For instance, feelings of
mistrust, scepticism and intimidation may arise due to the identity of the researchers and this
compounds fears related to the close scrutiny of records, caregiving or communication by
anyone external to the facility (Homan, 2001; Shenton & Hayter, 2004; Easterby-Smith et al.,
2008; Hayfield & Huxley, 2015). As a result, the gatekeepers may not believe that the benefits
of the study outweigh the risks and can deny access as described above. To abide with the
local ethical procedure, it was necessary to gain permission from the hospital medical
superintendents prior to commencing this study. Therefore, planning and contingency plans
that were put into place regarding hospitals recruitment are discussed below.
17 A term referring to the individuals who have the power or influence to grant or refuse access to a field or research setting. For example, the top manager or senior executive in an organization, or the person within a group or community who makes the final decision as to whether to allow the researcher access to undertake the research (de Laine, 2000).

69
3.5.2.3 Challenges and contingency plans for hospital recruitment
The pilot study ensured that many of the challenges were ‘known’ or anticipated before the
main study commenced, which meant fewer unexpected barriers in the field. As a PhD
student currently living in the UK, gaining access to hospitals for the recruitment of
participants was a complicated and lengthy process, partly due to the fact that some frontline
gatekeepers were suspicious of the researcher’s intentions, believing her purpose to be a
covert method of investigating their hospitals rather than a means of exploring the views of
participants. As the researcher is no longer a practising doctor in Pakistan, therefore, she was
often viewed as a foreign individual with the intention of being a ‘spy in the camp’ by some
of the frontline gatekeepers.
The following is an extract from a response received from a hospital medical superintendent.
‘Qurrat ul Ain. I know, you have made requests to conduct a research study in our hospital. You have sent me a
letter, but I’m not satisfied and sure what you want to achieve by interviews. I have concerns that you might be
a media person or there is something more going on. For this, you must need to come back to Pakistan and see
me face-to-face. Then I can decide’.
It was not easy to travel to Pakistan frequently due to full-time doctoral study commitments
in the UK and travel costs. Variation in the geographical locations of the study sites and
financial issues are cited as common barriers for researchers to engage in a successful
recruitment process and research (Pribulick et al., 2010; Newington & Metcalfe, 2014). Many
days were spent making several requests to selected hospitals with follow-up reminders and
phone discussions in order to gain access. Similar recruitment challenges have been
documented by another native researcher conducting a research study at Pakistani hospitals
(Yasir, 2014).
After months of continuous follow-up and with a few responses from the hospitals, it was
recognised that the researcher’s position as an outsider could obstruct access and threaten
the progress of the study. Therefore, as a contingency plan, it was decided to take an
authorised absence from the university and fly to Pakistan for face-to-face meetings with the
medical superintendents to resolve concerns. However, a few days before leaving for
Pakistan, permission from two hospital medical superintendents was granted (section 3.5.2).
Information regarding travel dates to Pakistan, booked flight tickets and data collection
timeframe was also shared with these medical superintendents in advance.
Building a relationship of trust through regular meetings with the gatekeepers, providing clear
and key information about the background and outcomes of the project and acknowledging
their contribution are effective strategies for maximising participation (Weierbach et al.,
2010; Miller et al., 2013; Daly et al., 2019). Therefore, before travelling to Pakistan, face-to-
face meetings with the medical superintendents were organised to build a relationship of
trust and familiarity. This gave them a feeling of ownership through involvement in the
process from the beginning of the study. This was an essential step to build good rapport to
70
initiate the recruitment process and is also noted by other researchers (de Laine, 2000; Clark,
2011; McAreavey & Das, 2013).
3.5.3 The recruitment of participants
The following recruitment procedures were adopted to identify and recruit participants for
the study.
3.5.3.1 Patients
Hypertensive patients were recruited from the OPD of the two hospitals with the help of
inclusion criteria.
Firstly, patients have a recorded diagnosis of essential or primary HTN. Secondly, the patients
should have a treatment plan that recommends taking tablets and conducting lifestyle
changes. Thirdly, hypertensive patients had to be ≥ 45 years of age, which is consistent with
evidence that the incidence of HTN rises as age increases (Carson et al., 2011) and according
to the National Health Survey of Pakistan the incidence of HTN in patients increases above
the age of 45 years (NHSP, 1998). Additionally, primary HTN is unusual in younger ages and
rarely lifestyle related.
The following exclusion criteria was used for hypertensive patients:
• Patients with secondary HTN were excluded due to the fact that the current study
focuses on patients with primary HTN.
• Patients with severe complications of HTN (e.g. stroke and heart failure) were not
recruited. This is in line with the argument that patients with severe complications
rely greatly on pharmacological therapy. Lifestyle changes are sometimes either
unmanageable (e.g. exercise) or less effective (e.g. stress management) in such
cases.
• Thirdly, people who were unable to give informed consent such as patients with
dementia, cognitive impairment and patients with severe and enduring mental
illness were excluded.
Four strategies outlined by Hennink et al. (2001) were employed which included using
gatekeepers, informal networks, advertisements and snowball sampling. According to
Silverman (2010) access to participants can raise many challenges for the researcher and the
importance of social networks, gaining access and other difficulties should be borne in mind.
Therefore, as discussed previously in section 3.5.2.3 face-to-face meetings were held with
hospital medical superintendents prior to approaching the study participants. To increase
participation in the study, a poster was designed (Appendix 8i) translated into Urdu (Appendix
8ii) and displayed at the entrances to the hospitals and medicine OPD. Patient information
leaflets were distributed to doctors in the medicine OPD to hand over to hypertensive
patients and to inform them about the researcher’s presence.
3.5.3.2 Doctors
The following inclusion criteria was used for doctors:

71
• In practice-at the study settings and treating hypertensive patients for HTN.
As identified in the pilot study, (section 3.5.1.1) a snowball sampling strategy was used to
identify the doctors for semi-structured interviews (Kirchherr & Charles, 2018). To invite the
doctors to take part in the study, the researcher requested that the medical superintendent
introduce her to the head of the medical department to ask for their co-operation. The
researcher required the contact details of doctors, which were not usually available, and
therefore had to depend on help from other doctors. This sampling strategy was practical and
convenient in terms of accessing and recruiting doctors. This was due to fact that those who
participated were keen and willing to take part and also available at the given time and date.
3.5.4 Data collection
The following sections set out the data collection process and methods used with patients
and doctors. In total 30 interviews were conducted with patients and 30 with doctors.
3.5.4.1 Conducting in-depth interviews with patients
Hypertensive patients were recruited from the medicine OPD of two hospitals using the
inclusion criteria as described in section 3.5.3.1. The researcher introduced herself as a PhD
student as mentioned on the participant information sheet. The researcher informed
participants that she was not an employee of the hospital to ensure obtaining non-prejudiced
views. The recruitment process regarding patients included identifying potential participants
based on the study inclusion criteria. For example, I would sit in the out-patient department
early in the morning as patients started to arrive at the hospital. After obtaining the informed
written consent, I would look through their medical files to confirm their HTN status using the
following:
• Verbal report of a history of taking antihypertensive drugs (only confirmed
hypertensive patients can take antihypertensive drugs which is 140/90mmHg).
• Confirming the diagnosis of essential HTN through checking available medical notes
and written prescription of antihypertensive drugs following their informed written
consent.
• Referral to the researcher by the doctor (after consultation).
If the patient fulfilled the inclusion criteria, then he/she was invited to take part in the study
and was provided with the patient information sheet and a consent form (see Appendix 9).
The information sheet and consent form were converted into Urdu prior to data collection
(see Appendix 10). The researcher read the participant information sheet and consent form
for illiterate patients. In Pakistan, it is an acceptable practice for an illiterate person to give a
thumb impression instead of signatures on all kinds of documents (Nabi et al., 2010).
Therefore, four patients provided a thumb impression on the consent form instead of
signatures.
The pilot phase has confirmed that patients preferred to give interviews on the same day in
the hospital setting rather than invite the researcher to their home. Therefore, interviews
were conducted on the same day for the convenience of the patients and in line with the
ethics approval granted for the study by the University of Hertfordshire. Patients were

72
approached either while they were waiting for their appointment or after they came out of
the consulting room. Participation was entirely voluntary, and the researcher respected the
decision if a participant did not wish to take part. Permission to record the interview was
obtained prior to commencing the interviews and this was also documented on the patient
information sheet and consent form.
It was made clear to the patients that they had the right to read the study information sheet
and take the time needed to think about whether or not they wanted to participate in the
study. Patients were assured that their personal details would remain confidential and they
had the right to withdraw at any given time without providing a reason. The name and contact
details of the researcher’s principal supervisor and the University of Hertfordshire Secretary
and Registrar were provided in the participant research information sheet (Appendix 9i)
should they need to report a complaint, or an issue related to the interview process.
A total of 15 patients were identified as eligible and invited to take part at hospital one, and
12 of the 15 agreed to participate. Three patients declined to take part due to demonstrating
a lack of interest in the study aims and others approached claimed to be ‘in a rush’ and did
not have time to listen to a brief introduction to the study. In the second hospital, 21 patients
were invited to take part and 18 agreed. Two further patients withdrew consent at the
beginning of the interview as they wanted to get home and one did not show interest in the
study. In total 30 face-to-face semi-structured interviews were conducted in two hospitals
with hypertensive patients.
In-depth face-to-face interviews were conducted with hypertensive patients in an available
empty treatment room at the two hospitals and interviews were audio-recorded. All the
patients chose to be interviewed without others present and spoke in the Urdu language,
occasionally speaking Punjabi words. The shortest interview with a patient lasted for 36
minutes and the longest lasted for one hour and four minutes. To achieve greater diversity in
the sample, various demographic characteristics were considered amongst the patients and
asked before the start of each interview. For example, male/female, obese/non-obese,
smokers/non-smokers, alcoholic/non-alcoholic, working and non-working hypertensive
patients were recruited. Comprehensive details about the demographics of patients are
provided in Table 3.1.
Table 3.1 Demographic characteristics of patients (n=30)
Patient No Age Gender-Male/Female
Education level
Employment status-
working/not working
Duration of HTN
Smoker/non-smoker
Obese/non-obese
1 70 Female Matric Not working 10 years Non-smoker Non-obese 2 55 Male Primary Working 1-2 years Non-smoker Non-obese 3 60 Male Masters Working 20 years Smoker Non-obese 4 46 Male Masters Working 2-3 years Non-smoker Obese
5 50 Male Primary Working 1 month Non-smoker Obese
6 46 Male Primary Working 6-7 years Smoker Obese
7 50 Female Primary Not Working
3 years Non-smoker Non-obese
8 47 Female Bachelors Working 8 years Non-smoker Obese
9 53 Female Secondary Not Working
6 months Non-smoker Obese
10 55 Male Bachelors Working 4 months Smoker Non-obese

73
11 80 Male Illiterate Not Working
2 years Smoker Non-obese
12 50 Female Primary Not Working
2-3 years Non-smoker Non-obese
13 56 Female Primary Not Working
10 years Non-smoker Non-obese
14 49 Female Bachelors Working 6-7 years Non-smoker Non-obese
15 52 Male Matric Working 3-4 years Smoker Obese
16 46 Female Matric Not Working
2-3 years Non-smoker Non-obese
17 56 Male Matric Not Working
2-3 years Smoker Non-obese
18 60 Female Primary Not Working
10 years Non-smoker Non-obese
19 61 Female Illiterate Not Working
3 years Non-smoker Non-obese
20 45 Female Bachelors Working 6-7 years Non-smoker Obese
21 46 Male Secondary Working 3-4 years Non-smoker Obese
22 50 Male Matric Working 5 years Smoker Non-obese
23 70 Female Illiterate Not Working
10 years Non-smoker Non-obese
24 60 Male Primary Working 3 years Smoker Non-obese
25 65 Female Illiterate Not Working
10 years Non-smoker Non-obese
26 72 Female Matric Not Working
7 years Non-smoker Non-obese
27 55 Male Matric Working 3 years Smoker Non-obese
28 70 Female Primary Not Working
6 years Non-smoker Non-obese
29 48 Female Primary Not Working
5 years Non-smoker Obese
30 54 Male Matric Working 3 years Smoker Non-obese
There was only one patient (11) who reported drinking hence a separate column is not
required in Table 3.1. At the end of each interview, the patient was thanked before leaving
the room and debriefed through an informal chat if necessary. If a patient asked for
information regarding their disease condition or treatment, they were directed to see their
doctor for advice.
3.5.4.2 Conducting in-depth interviews with doctors
The researcher was introduced to doctors working in the medicine department at each
hospital by following instructions from the medical superintendent. The names of doctors
expressing an interest in the study were noted down in a diary and followed up the next day
to confirm their willingness to take part. Contact details of those who were on leave were
provided by the available doctors, so they could also be invited. Senior and junior doctors
were provided with a doctor information sheet and a consent form (see Appendix 11). Doctors
could read and understand English without any difficulty, consequently, the doctor
information sheet and consent form was not converted into Urdu.
In-depth interviews were conducted with 18 doctors at hospital one. 8 doctors were senior
and 10 were junior. Junior doctors were house officers and within the first year of their clinical
experience. Among the senior doctors, 1 was a consultant physician and 3 were in post-
graduate training. 2 of the doctors qualified in China and 2 had work experience in foreign
countries. At hospital two, 12 doctors participated in semi-structured interviews out of which
8 were senior and 4 were junior. 4 of the doctors had qualified overseas. In total 30 face-to-

74
face semi-structured interviews were conducted in two hospitals and information regarding
selected doctors is provided in Table 3.2.
Table 3.2 Information about selected doctors (n=30)
Doctor No Gender- Male/Female Senior/Junior Time since qualified Time working in the hospital
1 Female Junior 7 months 6 months
2 Female Junior 6 months 5 months
3 Female Junior 7 months 6 months
4 Male Senior 8 years 5 years
5 Male Senior 10 years 5 years
6 Male Junior 9 months 6 months
7 Female Senior 7 years 4 years
8 Male Junior 5 months 4 months
9 Female Senior 10 years 6 years
10 Male Junior 2 months 1 ½ months
11 Male Senior 6 years 3 years
12 Female Junior 3 months 2 months
13 Female Senior 7 years 4 years
14 Male Senior 3 years 1 year
15 Female Senior 7 years 3 years
16 Male Junior 7 months 6 months
17 Female Junior 3 months 2 months
18 Male Junior 1 month 1 month
19 Female Junior 6 months 4 months
20 Male Junior 2 months 2 months
21 Female Junior 9 months 8 months
22 Female Junior 5 months 5 months
23 Male Senior 7 years 7 years
24 Male Senior 10 years 6 years
25 Male Senior 6 years 2 years
26 Male Senior 3 years 1 year
27 Male Senior 8 years 4 years
28 Female Senior 3 years 2 years
29 Female Senior 10 years 7 years
30 Female Senior 6 years 3 years
Interviews were conducted in an empty consulting room and audio-recorded. All the doctors
chose to give interviews in the Urdu language. The shortest interview lasted for 39 minutes
and the longest lasted for 1 hour and 41 minutes. All the doctors were aware of my
professional background as a medic and this has facilitated me in various ways. They believed
it was a professional obligation to take part in the study due to having the same profession as
was highlighted by some doctors. However, my status may have hindered their actual
responses due to the impression that they were being judged by a fellow doctor.
3.5.4.3 The challenges to data collection
Several key challenges were encountered during data collection and therefore some
contingency plans were implemented. For instance, travelling between two countries and
collecting data in hospitals located in separate cities was not a straightforward task to
accomplish. To deal with this issue, the data collection was divided into two phases. Phase
one was conducted in the first hospital (May 2016 - Aug 2016) with concurrent involvement
in data collection and analysis. Before beginning the data collection in the second hospital,
the researcher travelled to the UK for the doctoral review assessment and soon after
completing it returned to Pakistan for phase two (Dec 2016 - March 2017). In both cities,

75
private accommodation nearby to the hospitals was rented to overcome the travelling, as
well as cost and safety issues. Unaccompanied woman living and travelling alone in Pakistan
is not typical and can make them susceptible to sexual harassment (Azid, 2010; Ali et al., 2011;
LaBore et al., 2019). Consequently, family members of the researcher stayed with her and
provided support during fieldwork.
Scheduling face-to-face interviews with participants in the first hospital was slow during the
months of Ramadan. The holy month of Ramadan18 and long hours of fasting affected the
decisions of patients as to whether to take part in the study or not. Bearing in mind the
potential impact of fasting it was decided that early morning interviews would be preferable
to interviews conducted later in the day. Likewise, some doctors preferred to give interviews
in the evening after the iftar19 hence a flexible approach to arrange face-to-face interviews
was adopted in the month of Ramadan. Conducting interviews with senior doctors was more
challenging due to their work commitments and hectic routine. It was, therefore, required for
the researcher to be resilient and patient to gain their participation. On some occasions, the
researcher waited for several hours and rescheduled interviews many times at short notice.
Patient recruitment and conducting interviews was also a time-consuming and lengthy
process due to inflexible OPD hours. In the majority of Pakistani public hospitals, the OPDs
hours are from 9:00 a.m. to 2:00 p.m. on weekdays and Saturdays hence the patient
recruitment was carried out only within this timeframe. Sitting in the OPD with patients,
confirming their HTN diagnosis by looking at medical notes, identifying eligible patients,
reading the participants information sheets and consent form when required and conducting
face-to-face interviews were intensive features of data collection. The number of patients
recruited per day varied and, in some instances, the researcher was not able to recruit a single
patient in four to five consecutive days. In such a scenario, it was essential to remain
motivated to achieve patient recruitment for the study. The public holiday period and bad
weather also affected the data collection process twice as hospital OPDs do not operate
during public holidays and patients tend to avoid going out in bad weather conditions. During
these days, the researcher stayed at home and utilized this time in translation and
transcription of the participants’ interviews.
Qualitative research is not a commonly conducted activity in Pakistan, especially in the public
hospitals and this led the researcher to face some unique challenges. A female researcher
carrying and signing the consent forms and using an audio recording device attracted the
attention of many male patients. Several patients discussed the value of the consent form in
detail with researcher. Furthermore, some patients asked personal questions such as
researcher family background, why she preferred to study in the United Kingdom and how
18 Ramadan is the nine month of the Islamic lunar calendar and a month of fasting and praying for Muslims. During this
month, Muslims fast lasting 29-30 days and more emphasis is placed on spending time in prayer, helping the poor and reciting the holy book Quran at home or at mosque. 19 Iftar is the evening meal with which Muslims end their Ramadan fast at sunset.
76
she managed to pay tuition fees. In dealing with the dynamics of such conversations, the
researcher handled these questions diplomatically and tried not to offend the participants.
Gender segregation in public places is not a cultural norm in Pakistan (Shaheed, 2010; Ali et
al., 2011; Durrani & Halai, 2018). Males and females without marital status or immediately
related through family are not expected to be seen together behind closed doors. Whilst
conducting the interview with participants the researcher had to sit in a room with a closed
door to ensure the confidentiality of the interviewee. This was also seen as an unusual cultural
practice by some hospital staff and raised several questions as to researcher identity as a
Muslim female. In such cases, it was essential to explain the ethics behind qualitative
interviews and reasons for them being conducted behind closed doors.
3.6 Ethical Considerations
Ethics approval for the study was obtained from the University of Hertfordshire (UH) Health
and Human Sciences Ethics Committee with Delegated Authority cHSK/PGR/UH/02406 (see
Appendix 12). Permission letters from hospitals in Pakistan are attached after redacting
personal details for confidentiality purposes (see Appendix 13).
Ethical principles set out by the UH Ethics Committee were strictly followed, in addition to
research ethics and regulations set by PMDC. The four ethical principles of autonomy, non-
maleficence, beneficence and justice highlighted by Beauchamp and Childress (2001) were
considered throughout the study. Particular consideration has been given to ensure the
confidentiality, dignity and anonymity of the participants.
3.6.1 Confidentiality of participants
Participants were informed that it was entirely up to them whether to give answers or not
and they may withdraw at any point during the study without giving any reason. All data
electronically stored were password protected and under no circumstances will identifiable
responses be shared with anyone. All personal data were stored in a locked filing cabinet in
the researcher’s home and will be destroyed after submission of the dissertation. No personal
data were stored on a computer. Digital recordings were erased on completion of the study.
Care was taken while presenting the findings that the excerpts from transcripts used could
not be linked to individuals. Furthermore, identities of the patients who took part in the study
were not disclosed to their doctors.
3.6.2 Non-maleficence
Vulnerable subjects were not the focus of this study, although the challenge for researchers
is that harm can take many forms and is not always easy to predict (Sanjari et al., 2014).
Possible harm can be physical, social and emotional. The open-ended qualitative interview,
with its possibilities for discussing unexpected topics and therefore emotional dynamics, can
be significant for the interview process (Edwards & Holland, 2013).

77
This study does not address particularly sensitive issues; however, patients did require further
reassurance about their condition and when patients expressed a need for further
information they were directed to their doctor. During the interview, three patients became
emotional and upset by recalling previous stressful life events such as the death of a spouse
and domestic violence. I offered to stop the interview at this point, but they insisted the
interview be continued. All the participants cited the interview as a positive experience and
shared that it gave them an opportunity to think about and discuss their experiences in a way
that they would not normally do.
3.6.3 Informed written consent
Consent is an agreement provided by a person to participate in research once they have had
explained to them what is involved, and it helps to ensure that the person is not misled
(Silverman, 2010). Informed written consent was obtained from all the study participants
before the beginning of data collection. An informed decision to participate was facilitated by
the provision of a participant information sheet and a verbal explanation about the study.
As Urdu is the national language in Pakistan, I had the participant information sheet and
consent form translated into Urdu with all the information required in order for participants
to make a decision. The researcher was able to read and explain the participant information
sheet and consent form for illiterate patients. In Pakistan, it is an acceptable practice for an
illiterate person to provide a thumb impression instead of a signature on all kinds of
documents. Therefore, four illiterate patients gave their thumb impression on consent forms
instead of signatures.
3.6.4 An additional ethical protocol specific to this study
Researchers do not have an automatic right to intervene in the lives of participants. In this
study, the researcher is a qualified medic in Pakistan. In such instances, the researcher is
required to acknowledge the obligations to the professional code as a clinician (Holloway &
Wheeler, 2002). By the same token a commitment to ensure the integrity of the research is
also a priority. In such a scenario the researcher then possesses shared loyalties, and the
question arises as to whether the researcher is obliged to pay greater faithfulness to the
scientific method and the research or to the concerns of the participants (Jones & Jack, 1999;
Israel & Hay, 2006).
Elliot and Wright made the decision to only intervene in patient care in the event of an
emergency (Elliot & Wright, 1999). Similarly, Davies et al. (2000) only intervened directly in
caregiving when they predicted a situation to be possibly dangerous: for example, when the
observed nurse was about to make a drug error. These scenarios demonstrate the need for
an ethical protocol for the research. Therefore, prior to the commencement of fieldwork it
was decided to generate and adhere to an additional ethical protocol and this was generated
for the current study which was also in line with the PMDC ethics. This was also discussed in
advance with my supervisors and the hospital medical superintendents. The ethics protocol
with the associated actions has been attached (see Appendix 14).

78
As a qualified Pakistani medic, I was aware of my additional professional code of ethics and
moral responsibility. This additional responsibility and to follow the ethics protocol came into
practice during the data collection at site two, when I was called by a staff nurse to give a
patient cardiopulmonary resuscitation. The patient’s life was at risk and I therefore had to
acknowledge the obligations to the professional code as a doctor and continued help until
the duty doctor arrived.
3.7 Consideration of Data Sources, Governance and Management
The following section identifies the ways that data was recorded, transcribed and managed.
3.7.1 Translation and transcription
All interviews were recorded on a digital recording device. Recorded material was transferred
to a USB device which made transcribing on the computer convenient. Both English and Urdu
are the official languages of Pakistan; however, Urdu is the native language. Becker and Gee
(1957) argue that the researcher should be familiar with the language of the participant in
order to ask understandable questions and to interpret the responses correctly. As an insider,
my familiarity with medical jargon and fluency in both national and local languages assisted
me in reducing language barriers. Moreover, as a bilingual individual, I have been involved in
translation at different stages in my life, at school and in university projects, for my family
members who cannot speak English and during my professional development. It was essential
to translate and transcribe the interviews alongside the data collection phase in order to
become familiar and to involve myself in the immersion process. Therefore, I transcribed all
the interviews straight into English. Features of interviews such as emphasis, the tone of voice
and pauses were also transcribed (Bailey, 2008). Some doctors had qualified overseas and
were fluent in English, however, they were given the freedom to choose the language and
they preferred Urdu.
At the end of the transcription I double checked all the transcripts against the original audio
recordings to ensure local meanings were captured as far as possible. It also enabled the
researcher to add comments and compare the recorded material with interview notes in
order to remove any ambiguity. Preparing typed transcripts for all translated recordings took
a substantial amount of time and effort, particularly as it is sometimes challenging to find the
identical term in English. It was occasionally a challenge to convey the meaning of an Urdu
phrase or word into English; therefore, such contextual words or phrases have been used in
their original form in the transcripts and will be included in the dissertation, where needed or
appropriate.
3.7.2 Qualitative data analysis software
There has been some opposition to the use of computer-assisted qualitative data analysis
software. Some believe that using software may guide the researcher in different directions

79
and could distance the researcher from the data (Seidel, 1991; Thornberg & Charmaz, 2014).
According to Weitzman (2000) using software does not reduce familiarity but may alter the
researcher’s closeness to the data and for some this may assist in understanding their data
better when it comes to analysis.
Many of the critiques of computer-assisted software are as a result of misunderstanding the
software skills (John & Johnson, 2000; Lewins & Silver, 2007; Lu & Shulman, 2008). None of
the available programs actually analyse the data but rather help the researcher in managing
the analytical process. Without the aid of computer-assisted data analysis software, analysis
proceeds by cut and paste style methods, involving photocopying numerous copies of
transcripts and as a result, data becomes unmanageable, problematic and time-consuming.
There are several software programs available which assist with qualitative data analysis. In
this study, a computer-assisted qualitative data analysis software program called NVivo (QSR
Version 11) was used alongside manual coding techniques. This program was chosen due to
its availability to the researcher, but also due to its unique and flexible features required for
a grounded theory study: for instance, coding collected data, constructing network diagrams
out of coding and different visualisations of relationships between the data as well as a coding
scheme. Furthermore, the NVivo software proved to be a useful tool for coding, allowed
similar themes to be grouped together and redefining of the codes in order to support the
analysis process.
3.8 Data Analysis
There is no particular moment when data analysis starts. “Analysis is a matter of giving
meaning to first impressions as well as to final complications” (Richards, 2009. p.45).
With grounded theory approaches, data analysis occurs simultaneously with data collection
in a “zigzag“ fashion (Charmaz, 2006). The researcher’s visits to the data collection fields are
interrupted by concurrent phases of data analysis. This process of constant comparative data
analysis helps identify themes from subsequent interviews and compares them to previous
interviews (Creswell, 2013). The advantage of having a concurrent data collection and data
analysis enables a clear understanding of the social and cultural factors that impact the
phenomenon being investigated. This understanding provides the researcher with a cultural
lens with which they can analyse the study participants.
3.8.1 Familiarisation with data and manual coding
Through listening, transcribing, reading and re-reading the data, the collected data became
more familiar in order to gain a ‘general sense’. I printed off the transcripts in order to
highlight and carry out manual coding during the data collection. Initially, coding was done by
making notes on the transcripts by using different coloured pens to highlight different
themes. This manual coding helped to identify the basic themes and developing categories.

80
In the beginning of the coding process the use of simple logical flowcharts and diagrams are
common amongst grounded theorists to explain the different levels of connections (Strauss
& Corbin, 1990). Therefore, mapping diagrams sketched manually or by using Word SmartArt
assisted in making connections between various issues and factors (Appendix 15). This helped
me to understand how various relationships exist within a concept and how these were
related. Furthermore, examining the audio and transcription side by side assisted me in
probing and counter-checking the emerging issues with the subsequent participants.
3.8.2 Generating initial codes and child nodes
All recordings were typed into English in MS Word files and then imported into NVivo for
coding. According to Miles and Michael (1994, p.56) “Codes are tags or labels for assigning
units of meaning to the descriptive or inferential information compiled during a studyʺ. Codes
usually are attached to ‘chunks’ of varying size-words, phrases, sentences, or whole
paragraphs, connected or unconnected to a specific setting.
The function of codes is to indicate what is talked about in a segment of text. Therefore, the
identified text in the transcript is grouped into codes or nodes, and descriptive labels were
applied to the data. This resulted in segmenting the texts into units of meaning. Although this
generated a large number of codes it ensured that all instances of phenomenon were labelled.
After spending a lot of time in creation of the main nodes, data was re-read to identify deeper
patterns to identify the property which resulted in child nodes against sub-themes. A child
node is a node extending from the main node (Lichtman, 2001). For example, initially the main
node of high blood pressure had three child nodes named diagnosis, symptoms and causes.
Transcripts were defined separately in NVivo by ‘patient nodes’ and ‘doctor nodes’.
Words and lines were examined carefully, and hence line-by-line analysis was performed to
ensure that all data were handled systematically. The nodes were reviewed to identify the
areas of overlap or if linked were grouped together. Keywords and phrases were noted on
differently coloured post-it notes in a coherent order on a poster sheet. As more coding of
transcripts was completed the sheet started to look like a brainstorm map or a tree where
branches of thought grew from different categories. This strategy was particularly utilised
after the data collection at the first hospital one in order to understand what required more
exploration at the second.
3.8.3 Selective/focused coding for theme identification
Selective or focused coding serves to bring the data together in different ways and examines
the relationship between coded categories (Strauss & Corbin, 1990). This stage involved
collating all the coded data extracts within the category and all the identified categories into
one key theme. According to Charmaz (2006) focused coding involves using the codes that
are more significant and frequently used to explain larger amounts of data.
This stage involved going back and forth between the codes. Key codes were extracted such
as those that were used frequently and were grouped together. For example, ‘traditional

81
food’ ‘eating practices’ and ‘peer influence’ were grouped to develop the focused code. With
the next stage being a comparison of data to the focused codes, which assisted in refining
them in order to identify the theme. It was important to see the similarities and differences
in the views of participants about a particular concept by using a technique of constant
comparative analysis. Therefore, the coded data were merged into one single MS Word
document. In this way, one code in two different transcripts (patient, doctor) was compared
side by side. Using the technique of constant comparative analysis, I was able to compare
codes with codes, categories with categories and categories with concepts (Charmaz, 2014).
Memos help the researcher to write down questions, arguments, thoughts and emerging
hypotheses. Glaser mentioned memos as “the core stage in the process of generating theory,
the bedrock of theory generation” (Glaser, 1978, p. 83). Therefore, memos have been written
throughout the process of coding to keep track of the ideas regarding data. Memos helped
me to record my own thoughts and reflecting on the analysis process. A visual representation
of data coding steps employed in this study are presented in Appendix 16.
3.8.4 Data saturation
The term theoretical saturation in grounded theory approaches is used when researchers
reach a point in the analysis of their data that sampling more participants will not lead to
more information related to research questions (Charmaz, 2006). Therefore, researchers
check data for similar instances to ensure that no additional data can be found to develop
new properties of codes.
During the analysis process, sampling and interviewing continued until no new information
was found in the additional interviews. When using a grounded theory approach, there is a
set of processes that the researcher needs to adopt and by following these the researcher
ensures a robust exploration of the area under consideration. Flick (1998) states that
researchers need to pause and reflect on identified categories and then decide which codes
need further exploration in the light of the research questions. Ultimately the depth and
range of data analysis must be sufficient to enable the researcher to tell a plausible story
(Flick, 1998; Charmaz, 2006).
In this study, data were revisited many times to understand the issues and factors in the
management of HTN. The themes that emerged during the data collection in Pakistan were
regularly discussed with supervisors via Skype meetings in order to explore these themes
further with the next participants. For instance, some emerging issues in patient interviews
were counter-checked with doctors in their interviews. As the data collection progressed
accounts from subsequent participants did not add new information on factors influencing
the management of HTN. Therefore, I felt that saturation was achieved with 30 patient
interviews and 30 doctor interviews and no further themes emerged. To confirm the
saturation status, two further interviews were conducted. However, these additional
interviews were not found to produce any new themes. While data collection ceased at this
point, analysis continued until the final refinements to the core conceptual categories were
made.

82
The data coding frames used for patients’ and doctors’ data are presented in Appendix 17i
and 17ii. The coding frames helped to organise the findings as presented in the next two
chapters. Chapter four will present qualitative findings from the semi-structured interviews
conducted with patients and chapter five discusses the themes related to doctors’ interviews.
A consideration of the similarities and differences between the two sets of data is provided
in chapter 6, the discussion chapter.
3.9 Trustworthiness of Qualitative Data
Evaluating the validity and robustness of qualitative data analysis is essential for incorporating
the findings into practice and the delivery of care. However, qualitative researchers do not
speak about validity in the same way as quantitative researchers. Qualitative research is
frequently criticised for lacking the scientific rigour and lack of transparency in its analytical
procedures as compared to quantitative research (Rolfe, 2006; Silverman, 2010; Noble &
Smith, 2015). For the researcher, demonstrating rigour when undertaking a qualitative
research is challenging as the enquiry carries an element of subjectivity and personal bias.
I immersed myself in the data by undertaking translation, transcription and analysis, which
allowed me to understand the experiences of participants closely. Moreover, using external
checking from a bilingual colleague on transcription and from supervisors on the coding
process was another source of establishing the credibility of the qualitative data as suggested
by Silverman (1993). I reflected upon and acknowledged my role in the collection of data,
conducting interviews and during the analysis process. Being reflective gave me the
opportunity to learn the importance of self-critiquing and self-appraisal through every step
of the research process. I needed to carefully monitor my position in the research process and
the relationship with the study participants. I will now provide further reflections on this
process.
3.9.1 A reflective stance
Despite residing and studying in a foreign country for the past five years, I consider myself
primarily to be an insider due to having been born and raised in Pakistan and belonging to the
same professional group as the doctors involved in this study. The experience of working with
doctors and patients in Pakistan has sharpened my awareness of cultural nuances and meant
that I had a certain degree of prior knowledge about the study participants, surroundings and
the hospital environment. I was confident that my position as an insider would allow me to
be more easily accepted. However, this did not always mean that I was considered to be an
insider in the eyes of gatekeepers. Experiencing ‘strange’ and ‘familiar’ experiences at the
same time enabled me to understand that the experiences of a researcher from outside
Pakistan can be very different to those of a researcher considered to be an insider.
I spent many days making several requests to different hospitals, with follow-up reminders
and in phone discussions in order to gain written permission. At that point, I often felt myself
to be as much an outsider as a non-Pakistani national or someone with no prior experience in
the field. Eventually I gained permission from two hospitals where I had never worked in the

83
past. I remained focused that my aim as a qualitative researcher was to understand the ‘emic’
perspectives of study participants with reference to HTN and its management and in order to
achieve this I found myself busy establishing rapport, getting to grips with obtaining consents
and organising interviews. However, a number of challenges became evident and brought me
to the realisation that an external researcher may face many difficulties due to a number of
factors.
Declaring my profession to study participants assisted in establishing a good rapport with
them, although this self-presentation was often faced with a degree of criticism on several
occasions. While conducting the interviews, I came across some phrases such as ‘you know
better’, ‘you already know,’ ‘you know better than me’ which made me uncomfortable and
placed me under pressure. This was partly due to the fact that I wanted my participants to
see me differently as opposed to my previous role as a medic. At that point, I realised that it
was difficult to shift from my role from medic to the researcher. In an attempt to achieve a
balance, I would wear a researcher’s badge in the field displaying the University’s logo and
my name. I often found that I remained silent in the common room during discussions
confirming the diagnosis and commenting upon drugs, wondering whether anyone had
noticed that I was not contributing to the discussion.
Furthermore, some of the doctors revealed more information than they would have perhaps
been naturally comfortable with if they had not viewed me as a colleague, I, therefore learnt
when to turn off the tape recorder to strictly follow ethical standards. Any break down in the
boundaries between researcher and the individual under research may result in ethical issues
if participants treat the researcher as a confidante or counsellor, and therefore reveals more
than they would naturally feel comfortable with (Watts, 2006; Sanjari et al., 2014). I began to
appreciate my position as an insider clearly when an evening hospital medical superintendent
involved me in an informal discussion around HTN management. The medical superintendent
shared own valuable experience of being a research student in a foreign country and the
challenges involved in gaining access. At that point, I realised that access was granted, as the
medical superintendent was aware of the obstacles in the recruitment of hospitals and data
collection.
Being a Pakistani Muslim female brought up in an Islamic society, I felt a responsibility towards
my religious and traditional heritage. I had to act in a way that fulfilled the societal regulations
and expectations. Hence, I chose to wear a traditional Pakistani dress (salwar kameez)20 with
a ‘dupatta’21 to cover my head during the fieldwork. This did not pose a dilemma as it was not
incongruent with my personal life in Pakistan. Many scholars (Davis, 1992; Entwistle, 2000;
Ellingson, 2006; Okely, 2007; Lloyd et al., 2008; Wray & Bartholomew, 2010; Zubair et al.,
2012) have pointed to the important link between dress and identity whereby dress serves as
a visual metaphor for identity and as an insignia by which we are read and come to read
others. The insider role facilitated my recruitment of participants since patients usually have
20 The salwar kameez is the national dress of Pakistan and it is a cultural practice for women to cover their heads. 21 Dupatta is a shawl like scarf and worn across both shoulders and around the head. It is used most commonly as part of the women's shalwar kameez dress.

84
clear boundaries of self-disclosure and it can be difficult for them to reveal their personal
stories to an outsider. In a male-dominated Pakistani society, it is a common belief that
women who live in the West are usually open-minded and compromise on their moral values.
Wearing an Asian dress during fieldwork led to some doctors questioning why I was not
wearing a Western/modern dress in the hospital. Furthermore, some male doctors tried to
be somewhat informal and offered a lift home. Although I had to behave in a professional
way that did not compromise my respect within the environment and my own moral
standards. Therefore, the necessary action of involving the hospital medical superintendent
was taken when required.
During translation and interpretation, I had to make judgements about the meanings
contained within the language and spent a lot of time trying to estimate the degree to which
different cultures would identify with those meanings. I am fluent in the language of
participants in the study, and therefore had an advantage in terms of research methods over
other researchers in cross-cultural research who are not as proficient in the language. Using
a researcher’s diary to note down field notes and my own thoughts were one of the reflective
strategies I adopted during the data collection process. This involved me in asking myself
various questions throughout the data analysis, such as what led me to a particular perception
and why. Being reflexive (Etherington, 2004) enabled me to learn the importance of self-
critique and self-improvement through every step of the research process.
Dilemmas arise in research regardless of the position of the qualitative researcher, but what
is vital is to understand how these issues can be managed to be aware of one’s own position
and any blind spots within the field in order to enhance understanding and trustworthiness
of the data.
3.10 Summary
This chapter has presented the methodology employed and explained how the study was
conducted. Detailed information was provided about the sampling and recruitment of the
participants for the study. The chosen data collection method helped to explore an in-depth
understanding of the perceptions and experiences of patients and doctors. This chapter also
outlined how the data were collected, managed and the process of constant comparative
analysis. Finally, reliability and validity of the qualitative research through the consistency of
study procedures was explained.
The following two chapters present the findings from the data analysis regarding the
perspectives of patients and doctors about HTN management, respectively. Chapter four
presents the patients’ understanding of HTN management whilst chapter five presents the
themes related to doctors’ perspectives of HTN and its treatment.

85
Chapter 4: Patients’ Perceptions of HTN and its Treatment
The analysis revealed four main themes regarding patients’ understandings with regard to
HTN, treatment, lifestyle recommendations and involvement in alternative strategies. This
chapter will describe these themes and associated categories that emerged during interviews
with patients and presents evidence of how patients sought to manage HTN in their own
ways.
4.1 Perceptions of HTN
Patients were asked about HTN in terms of how they understood the disease and
conceptualised HTN in everyday life. The categories linked to this theme are diagnosis,
symptoms and causes of HTN.
4.1.1 Diagnosis
Diagnosis is the point at which patients receive confirmation of their condition through
consultation with a doctor. In this study, the responses of patients indicated that they were
able to recall and list their diagnosed HTN status as documented in their medical files. The
majority of patients interviewed cited that their diagnosis of HTN had occurred during routine
clinical visits for another medical condition. They provided detailed explanations of the events
that led up to diagnosis of HTN and how they became aware of their condition.
I was just sitting near to stove to make tea in the evening, one day; then I felt suddenly,
suddenly……something is wrong with me like my head was spinning. Then, I went to a nearby
hospital, there doctor told me that your blood pressure is very high. Then he gave me tablets
to take and placed one tablet under my tongue. He told me take a tablet every day and come
after a week…hmmm…when I went after a week it was again high. He then confirmed that
you have this disease. Umm. I was all right before that. (Patient 25)
Patients described their initial reaction to being diagnosed with HTN as one of confusion and
denial. The ‘sudden’ diagnosis of HTN and the instant necessity for reliance upon prescription
drugs came as a shock to many patients. This denial in relation to diagnosis was more common
amongst patients who perceived themselves to be physically ‘fit’ and had not previously
experienced any symptoms.
When…. my doctors [first] told me about disease diagnosis, I was shocked and worried. I
thought I was all right so how this can be possible? It was difficult for me in the beginning
but gradually I became used to it and started my treatment. (Patient 21)
They described that diagnosis of the disease requires physical symptoms and were therefore
uncertain about their diagnosis of HTN as they had not experienced any such indicators of the
disease.
I think, I was shocked in the beginning due to no symptoms and nothing. Disease must be
with some symptoms and warning signs. But gradually after the diagnosis, I had the disease
symptoms and then I thought oh yes, this disease can be without symptoms. (Patient 7)

86
Definitions and meanings of HTN
Most of the patients struggled to define high blood pressure. They reported their own
description such as ‘high blood’ or ‘tension’ and explained this as a pressure of blood
distributed in the veins to control the heart.
I think it’s the pressure of blood that run-in veins. It becomes high when pressure raises
and become low when it settles. Hmm… I think when the first one, the top one, not the
bottom one, crosses 130 number then it becomes dangerous and high. When it stays
below or on 120 then its normal. (Patient 1)
Some patients possessed awareness about systolic and diastolic blood pressure; however,
patients did not report that these levels were used to achieve optimal blood pressure control
and low blood pressure readings.
I don’t know what the top and bottom numbers [are] about blood pressure. I think they
are the same. What can I tell? I don’t know really, it seems complex and I really don’t
know. (Patient 7)
Most patients reported HTN to be a dangerous disease in the context of complications such
as the possibility of having strokes and were therefore concerned. They understood the
consequences of the disease but not necessarily the medical explanations of HTN which led
to these serious outcomes.
I have heard from many people that it can develop serious complications in the human
body very easily. I [have] heard that if the blood pressure shoots suddenly, it could even
result in the bursting of a blood vein. I have also heard that a patient can get a paralysis
due to the problem of high blood pressure. (Patient 30)
I think it’s a terrible disease, it can kill you gradually. It can cause stroke and heart attack
in people. I have seen many people suffering and heard about this. (Patient 11)
Whilst some patients attempted to explain HTN in the context of its severity, conversely,
many patients relied on descriptions of the symptoms and causes to understand HTN.
4.1.2 Symptoms
Medical literature often describes HTN as a silent killer (Zusman, 2009; Accad & Fred, 2010;
Makridakis & DiNicolantonio, 2014). However, many patients reported the manifestation of
three to four physical symptoms as the disease progressed, including headaches, muscle pain,
dizziness and fatigue, which they associated with increased blood pressure. Symptoms were
characterised as having serious features and were often gradual in onset.
Most patients reported frequent bodily aches and pains associated with tiredness and fatigue;
however, the most common complaint was a throbbing pain and unpleasant sensations to
the head. Some patients described experiencing problems with their sleep patterns, such as
frequent waking, sleep deprivation and nightmares. The impact and experience of such
symptoms gave rise to frustration and emotional distress amongst patients on many
occasions.

87
I feel so much pain in my whole body. I feel backache too. I feel headache and at times my
veins move very fast and I can even feel that sensation on both sides of my head. I feel
someone is hitting me on my head. I feel tiredness in my legs…you know in my legs, I feel no
energy and [I have] pain in my leg muscles. (Patient 17)
I feel headache and severe headache like throbbing. I become angry too and my mood
changes. Then I know that this is due to my high blood pressure. The headache and pain [is]
all over the body most of the time. (Patient 25)
Patients were concerned about the possibility of a recurrence of symptoms such as dizziness
and felt that they could tell if their blood pressure was better or worse by the intensity of
their physical symptoms. A few patients said they often experienced headaches and stated
that they would invariably self-treat the headaches with painkillers, drinking extra water,
having a rest, or simply just waiting for the headache to subside. They did not appear to regard
less severe symptoms as a serious risk and believed they could be minimised with stress-
reducing activities. However, they viewed a change in their heart rate, particularly with pain
to be a possible sign of a heart attack or stroke and therefore believed these symptoms to be
serious.
Many patients expressed that the onset of HTN symptoms had a negative impact on their
work productivity and reported a significant decline in their ability to focus. They described
that due to constant headaches and impaired vision as a result of HTN, they were unable to
work and focus as effectively as their co-workers. The appearance of such symptoms forced
patients to take sick leave from work and consequently consider taking early retirement due
to the impairments HTN was causing in their working lives.
When I have high blood pressure then I don’t go to work and send my sick leave to my officer.
I’m thinking to take retirement early due to this disease because I cannot work the way I was
used to do before this. My vision is badly affected, and I cannot concentrate much. I often have
headache. (Patient 22)
High blood pressure has affected my life because sometimes my blood pressure rises, and I
stop my trailer on the side of road until my blood pressure gets settled. Sometimes, I cannot
go to work and talk happily with people as I was used to do so. My company also advise
drivers not to drive if they are not feeling well. (Patient 15)
Some patients experienced impaired interpersonal relationships and family conflict following
the onset of the disease. Patients described experiencing changes in mood and anger issues
after the occurrence and exacerbation of their symptoms. Some men reported becoming
aggressive and physically violent towards their wives and children which often resulted in the
breakdown of relationships. One patient described experience as follows:
When my children don’t listen to me. I feel angry, very angry…. my heart says that I should
beat them hard. Then, I expel my anger on others like my wife and slap her or my kids,
sometimes. I know, it’s not good… Hmmm. But I cannot control my mood and anger due
to this disease. I often go to the room and close my door inside unless I feel better. (Patient
3)

88
One woman shared how her HTN symptoms had led to a breakdown in her relationship with
her husband. She cited not being able to tolerate the controlling nature of her husband after
her HTN diagnosis and this had a devastating effect on the stability of her marriage.
My husband was not able to understand my situation. He is very controlling. Ever since I
have high blood pressure, I have become impatient and I could not fulfil his demands and
orders. We had a fight and he has sent me to my parents’ home now. He says he will go for
another marriage now. (Patient 20)
Patients’ believed that the HTN affected many aspects of their daily life. They described how
mental, physical and family life had been affected in a number of ways after being diagnosed
as having HTN and experiencing its symptoms. The consistency and frequency of physical
symptoms had been the trigger for some patients to visit their doctors and receive a
confirmed diagnosis. By contrast, patients who had experienced no HTN symptoms were less
likely to take the condition seriously, considered the illness to be harmless showing that it is
therefore vital to gain insight into the beliefs of these patients with HTN management.
4.1.3 Causes of HTN
Stress due to financial problems and interpersonal issues was highlighted as a main cause of
HTN amongst patients. A few patients mentioned that eating an unhealthy diet increased
their blood pressure and this will be explored further in section 4.3
Stress
A stressful lifestyle was a common cause highlighted by most patients as hindering optimal
control of their HTN and this also included patients who claimed to be adhering to their
recommended treatment plan.
Stress was perceived as both a cause and a consequence of HTN by almost all patients and
they also identified specific sources of stress. Patients’ reported avoiding stressful situations
but frequently mentioned stress-inducing factors that they perceived out of their control,
such as the sudden death of loved ones or emotional tensions with their spouses and family
members. More generally, male hypertensive patients associated job-related stress and
unemployment as reasons for their constant high blood pressure, whereas female patients
reported stress caused by their husbands and in-laws.
I don’t think there is any other reason behind this disease than the tensions. In me, it
happened the day when my husband passed away on Eid day and went to Allah. After that
I started this disease due to stress because things had changed like my responsibilities and I
had no idea how to manage those. I was worried and took tensions and now I’m here with
high blood pressure. (Patient 12)
Many patients described tension and difficult relationships within their immediate
environment and felt that family members were unsupportive. When living within extended
family networks this situation was exacerbated due to the frequent contact with other
relatives. Most female patients reported feeling that there was a lack of adequate support

89
from their husbands. The following extract from an interview with a female patient illustrates
how family relationships were perceived to negatively influence the well-being of individuals,
which in turn was thought to impact the severity of HTN for patients.
K: My child, I have lot of tensions in my life. My elder son has left me and moved with his in laws.
I can’t live without his children. Without my grandchildren, I feel broken and incomplete. My
daughter-in-law don’t allow my grandchildren to come and live with me.
[Pause]
My husband…Umm… had diabetes due to that doctors had to cut his leg in an operation to
spread the infection… now my husband thinks I did this to him by allowing doctors due to my
evil intentions. But I had no evil intensions. Umm. Now I’m just passing my time here and feel
very helpless. He is taking revenge from me by giving me tensions and he knows tension is not
good for me.
[Crying]
Q: I can understand what you are going through. It must be so stressful.
K: My younger son… he has a wife and two children, but he doesn’t care about his family. He is
also a drug addict. I’m taking care of his wife and kids.
Q: I’m so sorry to hear this. Hopefully everything will be fine soon.
K: Now I’m affording the treatment cost of my son as well so that he should leave the drug
addiction. Due to these tensions I got this disease and now my blood pressure remains high.
(Patient 23)
Similarly, some female patients reported communication problems with their in-laws and as
a result felt helpless and depressed. They described that in-laws often viewed the cost of HTN
treatment as a financial burden on their sons which brought additional worries and
frustrations in family life. Due to these tense relationships with in-laws several female
patients experienced a lack of financial and emotional support from their husbands.
Financial difficulties directly affected the emotional well-being of patients and caused
uncertainty, insecurity and stress. Such situations had knock-on effects when it came to
choose a healthy diet and the acquisition of drugs that often led to poor HTN management in
hypertensive patients. As the following patient describes:
My father has separated me after marriage. Now, I live in a separate house, I have my family,
house rent, electricity bills, telephone bills, and children school fees, then my disease. When
I go to bed at night, everything comes into my mind. These tensions never spare me. I even
don’t buy healthy food and my medicine sometimes. This is really not good for my health, I
know. (Patient 6)
Limited financial resources and the need to keep within a fixed budget created a state
whereby compromises had to be made and less healthy, high calorie food was chosen over
more expensive healthier options. The recommendations of doctors to eat healthy food was
seen to be an additional source of stress for patients as this was not always possible on a daily
basis.

90
Difficulty meeting the cost of drugs was another reason to cause stress amongst hypertensive
patients. As a result of financial hardship, patients often delayed purchasing their
antihypertensive drugs, or sometimes stopped buying them altogether and this was
perceived to lead to further deterioration in the condition of their health.
When I don’t have money to afford my tablets then I don’t buy at all. Because income is
limited, and I have a lot of things to manage in life. Many times, when I cannot afford my
tablets [and] I become tense. That is another additional tension that I face, and I know it will
make me sicker. But this is another worry that I don’t have money to buy tablets for myself.
Hmmm…. (Patient 9)
‘A family disease’
Even though a majority of patients believed stress to be the cause of HTN, some viewed it as
an inherited condition, referring to it as a ‘family disease’. Patients reported family histories
of heart disease or HTN in close relatives, such as their mothers, fathers and siblings. Certain
common features in their family history strengthened their belief that the condition was
inherited, such as the number of family members affected, age at diagnosis and the severity
of the illness. By noticing the pattern of symptoms amongst family members, patients would
assess their own risk of becoming hypertensive.
If this disease is common in your family, then it happens to you. In my in-laws no one has
this disease but in my mother family; my father got it. My granddad had this too and he
died due to stroke. That’s why I have the same problem. (Patient 14)
Patients who had witnessed first-hand the suffering of hypertensive family members
expressed fear, anxiety and uncertainty about their future; a few patients made comparisons
between the physical symptoms of affected relatives and their own when considering the risk
of developing complications and considered HTN to be a contagious disease transferred from
one family member to another.
I think, in my case, my father has transferred this disease to me. My father had the same
disease and he passed away due to stroke. In early days of his disease he had the same
symptoms as I have. I had a doubt in the beginning when these started to appear that I have
the same disease as my father. It was true. (Patient 5)
Moreover, in order to avoid the negative consequences of the disease that their family
members had suffered some patients adopted a positive attitude towards drug adherence.
I had seen how badly my mother condition [was] when she had a stroke due to this blood
pressure. She was unable to stand and talk but not concerned about her drugs. Umm. That’s
why I take my drugs daily because I don’t want to die like her. (Patient 14)
In addition to identifying HTN as a family condition, a few patients had very particular beliefs
associated with the cause of the condition. For instance, constant disturbed sleep and fatigue
were considered to be the two main causes of increasing blood pressure amongst three
patients. They believed that rest and good sleep helped them in order to control the
prevalence of HTN symptoms and cope with the disease.

91
This disease is related to sleep, I think. When I don’t sleep well then, I get this high blood
pressure and when I take rest then it disappears. I lay and sleep mostly when this happens,
and blood pressure comes down. (Patient 27)
A patient who received a blood transfusion when undergoing uterine surgery stated that she
believed the blood transfusion of someone else’s blood to be the cause of her HTN; if she had
not undergone this surgery then she believed she would not have become a sufferer:
I underwent a uterine surgery five year ago and being transfused by someone else blood at
that time that’s why I got this disease. I have heard that when someone blood enters into
your body then you get this disease. Hmmm…Before that, I had no high blood pressure.
(Patient 16)
The accounts of patients surrounding HTN diagnosis, symptoms, causes and consequences
reflected their lay understandings of HTN as a condition. The following theme will present
patients’ experiences and attitudes regarding taking antihypertensive drugs.
4.2 Experiences and Attitude Concerning Taking Antihypertensive Drugs
The experiences of patients when taking antihypertensive drugs affected their adherence
attitude towards an overall optimal treatment plan. Some patients reported positive
experiences, but some had reservations and reported the negative effects of taking such
drugs. The positive effects of taking antihypertensive drugs were expressed by patients as
being the ability to control their blood pressure and prevent progression of the disease.
These patients reported that regular use of such prescription drugs had provided them with
beneficial outcomes such as better control of their blood pressure, a general feeling of well-
being and a relief of their symptoms. Some patients believed that adherence to the drugs was
an important factor in managing their blood pressure and stated that they had received
positive experiences with doctors encouraging them to take the drugs. As the following
patient described:
My doctor advised me to stick to your medicine. I also feel better when I take my tablets. My
blood pressure doesn’t give me any trouble like headache, fatigue nothing when I take my
tablets daily. I take these [pointing towards bag of medication] daily as my doctor
suggested. (Patient 22)
Many patients described that despite experiencing side-effects, antihypertensive drugs
continued to be taken.
I’m regular in taking my drugs, I feel better and this is my treatment. Sometimes, I do feel
side-effects like mild rash, but my doctor told me it is common with this tablet and you don’t
need to worry. Rash disappears gradually but I carry on with my tablets. (Patient 26)
On the other hand, some patients cited intentional non-adherence with regard to
antihypertensive drugs. They reported negative consequences such as side-effects and
dependence after taking prescribed antihypertensive drugs and as a result had decided to
stop taking them. They were concerned that antihypertensive drugs were toxic and harmful

92
in nature and produced more side-effects than they had benefits. Symptoms such as an upset
stomach, nausea and a dry mouth caused them to gradually skip doses and finally they gave
up without reporting these side-effects to their doctors or consulting with them first.
When I take tablets, my body starts to swell like a balloon then I left the tablets. My body
was not like that before. My stomach can’t tolerate these tablets too. I don’t want my
stomach troubling me all day, it is not good. (Patient 29)
The fear of developing side-effects after taking their tablets made patients anxious and they
questioned the efficacy of antihypertensive drugs. Missing doses and ceasing to take the
tablets altogether was also prevalent amongst those who believed that they would become
dependent or addicted to antihypertensive drugs for the rest of their lives. They had a
common belief that all drugs contained chemicals which were harmful in nature and therefore
prolonged use of tablets was dangerous.
Tablets make you addict and do more harm. These tablets contain chemicals and not good
to use for a longer period. I don’t use these tablets very often. I don’t want that my body rely
on these all the time. I’m just sick of these tablets. (Patient 3)
Some patients shared an intermittent pattern of using prescribed medications, reporting that
they would abruptly stop taking the antihypertensive drugs after just a few days. They cited
taking a full, regular dose one day and then no dose the next and not resume taking their
drugs after that. When asked why they were using their tablets in this way they responded
that they were curious to observe the effects of intentional non-adherence on their blood
pressure and would do so if they happened to be feeling particularly well.
Sometimes I leave the tablets by myself. Because I want to see what happens to my body if
I leave. This blood pressure tablets never spare a human body. So, I check what happens if I
leave the tablets. I don’t feel the need of taking these sometimes, when I feel better. (Patient
10)
Whilst a pattern started to emerge as to how patients understood and experienced taking
antihypertensive drugs, additional responses highlighted that unintentional non-adherence
was often due to simply forgetting to take their medications or put it down to the cost and
accessibility of them. Some patients reported forgetting to take their drugs if they were busy
or away from home. Older hypertensive patients also reported that they often forgot to take
their tablets and they ascribed this to memory loss or just general forgetfulness due to their
age.
Sometimes, I forget to take tablet then it misses. I usually can’t remember either I have taken
my tablet today or not. Either, I have taken my tablet in the morning or not. I do forget lots
of things now. It has started happening me just few years ago because I’m getting old.
(Patient 11)
Patients citing forgetfulness described how support and motivation from family members to
take their tablets with constant reminders resulted in improved adherence.

93
Many times, my daughter asked me either I have taken my tablets or not. She knows, I often
forget that’s why she always asks. Almost all the times [laughter] she never forgets. (Patient
25)
Many patients described that unintentional reasons for non-adherence to antihypertensive
drugs came down to the cost and accessibility of medication. The high cost of
antihypertensive drugs was highlighted as a common issue to compliance with their
recommended treatment plan.
The fact is that most of the times, I don’t have money to buy the tablets. This is difficult to
afford all because tablets are expensive. One blood pressure tablet cost around 200-250Rs
for 15 days. Sometimes, I borrow money too from here and there. So, a person like me who
has little money where he would go then? He/she will just ignore the tablets or only buy
when money have. Ummm. (Patient 2)
Besides cost, some hypertensive patients reported the unavailability of prescription drugs in
hospital pharmacies at certain times. They indicated that when their usual brand was not
available in the hospital pharmacy, they would often resort to buying the drugs from private
pharmacies. As a result, poorer patients were placed under greater financial burden and
inclined to be non-adherent until such time as their drugs became available again in the
hospital pharmacy. In addition, patients also reported that doctors did not provide sufficient
information regarding prescription antihypertensive drugs and this was another reason of
their non-adherence.
4.2.1 Lack of information about drugs in consultations
Most patients reported receiving little information regarding their drug treatment from their
doctors and indicated that the relationship was often problematic and disappointing. Patients
mentioned that doctors provided a generic and quick reminder about antihypertensive drugs
but without any specific or helpful information with regard to their use or the duration for
which they should be taken. As a result, patients felt frustrated when they were unable to
acquire sufficient information regarding their treatment and this often contributed to their
attitude to stop taking the drugs prescribed.
They don’t tell anything briefly. Even they don’t tell anything like here in this hospital. Here
they just tick the box, yes, we have seen this patient. Even, I came first time and diagnosed
as high blood pressure then doctor did not tell me anything after that. They just say to take
tablets, come again. Not when I have to stop the tablets or not. It can be a minor thing for
them but definitely not for me. (Patient 25)
Some patients reported that although they had been provided with some basic information,
they had faced difficulties when requiring greater clarification and additional support. The
responses of patients indicated a wish to receive detailed information about their drug
treatment; however, they felt reluctant to ask questions due to the busy routines of their
doctors and the style of communication with which information was imparted to them.
For instance, patient 4 illustrated a number of communication issues he experienced during
consultations with a busy doctor which had left him feeling passive and therefore unable to

94
ask questions about his treatment. The patient was afraid to ask for more information from
his doctor due to past experiences where he had perceived that his doctor did not appreciate
being questioned and that pressing him for further information may cause the doctor
irritation.
Doctors even don’t tell anything. I do ask questions from my doctor. For example, last time
I asked: my doctor, tell me what this high blood pressure is, please tell me about this disease.
He said just take these tablets you won’t understand what this is. Next patient [Laughter].
What I can say about this? I just obey him because I feel fear that he will be angry and upset
with us by asking questions [Laughter].
When your turn comes after waiting many hours then a patient tries not to displease doctor
[Laughter]. I don’t ask questions now no matter what [Laughter]. (Patient 4)
This illustrates that there is a concern amongst some patients about the quality of care they
are receiving and in particular the speed with which they are dealt with by some doctors and
the attitudes of those doctors towards their patients. A lack of essential information due to
breakdowns in communication may lead to failures in therapy for some patients and
ultimately delay their recovery. Further exploration of this issue revealed some interesting
findings as the following paragraph illustrates.
A few patients reported that doctors often encouraged them to visit them in their private
clinic where they would receive an improved service, additional information and shorter
waiting times. They described this as unacceptable and unprofessional practice and as a result
it had affected their level of trust in these doctors. This may suggest that some doctors are
adopting strategies to compel patients to use their private clinics and intentionally providing
less information as a means of encouraging this.
Sometimes, if you ask more information, they become irritated and simply ask you to come
to my private clinic in the evening if you want to know more and good service. If you go to
the same doctor in the evening in his private clinic he will behave in a totally different way.
When you come here to him in the government hospital, he will not give you even a smile.
He will suggest you come to his private clinic. This is very frustrating. (Patient 8)
Furthermore, some patients were concerned that they may face negative consequences in
the form of poor-quality care and inadequate communication at their next consultation if they
had not visited a doctor in the private clinic. To overcome this issue, a few patients suggested
increasing the number of doctors in public hospitals and that steps could be taken to prevent
them from working in private clinics.
I think more and more doctors should be there in public hospitals to deal with patient burden
and gain information that is needed. There should be a ban on doctor private practice, so
they won’t see us as a profit but as a patient. (Patient 17)
4.3 Perceptions About Lifestyle Management
Within this theme, five categories emerged that highlight lay beliefs of patients informing
their practices about exercise, diet, salt intake, smoking and alcohol consumption.

95
4.3.1 Understanding concerning exercise
In this study many patients reported awareness that exercise was beneficial to adopt in their
daily routine in order to stay active and should be undertaken as part of blood pressure
control. Their awareness of the benefits of exercise was wide-ranging and included sustaining
physical fitness, maintaining optimum body weight and improving general well-being. Some
patients were uncertain about the correct amount of exercise, type and intensity required for
hypertensive patients. They perceived exercise as a walk around the house, managing
household tasks and described a wide range of activities they were involved in. For instance,
some hypertensive patient cited common household tasks such as washing dishes, cooking
and cleaning as her main source of exercise.
I do clean with besom in all the house, clean the kitchen and washes the bath room and do
dish washing. I don’t think, I need any other exercise as these all tasks are my exercise and
my body remain active. So, in this way I do exercise all day by running here and there and by
doing household tasks. (Patient 1)
Similarly, moving things from room to room, shopping trips to the market and visiting relatives
that lived near to the house were also viewed as exercise amongst some patients. One female
patient indicated that her job provided the opportunity to walk around, although seemed
confused between the terms exercise and walking and used both interchangeably.
I work in a college and as a part of my job, I make many rounds like walk all over the place.
Sometimes 3-4 turns in a day. I have to go to many class rooms, so I make many rounds all over
the place and that exercise. What else do I need to do? I don’t think I need any more walk other
than these turns. (Patient 14)
Walking was most commonly cited by both male and female hypertensive patients when
asked about forms of regular exercise. They reported that undertaking a brisk walk led to
feelings of improvement both mentally and physically. For instance, a 56-year-old male
patient said:
I do walk daily, doctor has asked me to do walk. At night after meal I walk for 200-300 steps. I
prefer to do walk every day at least before sleep. Because, walk makes me feel good, happy,
and it is easy to do, it makes me comfortable and I enjoy it. (Patient 17)
However, a few patients stressed that walking and exercise should be specific to the daily life
routines of obese hypertensive patients and stated that their doctors had not considered
them to be overweight when they had sought advice about walking and exercise. As a result,
they did not make any effort to adopt exercise into their daily routine and distinguished
themselves from obese hypertensive patients on the basis of body weight alone.
In contrast, obese hypertensive patients were aware of the benefits of exercise in relation to
weight control and took a different viewpoint from the non-obese patients. Two obese
patients who were trying to lose weight reported doing vigorous exercise for a longer duration
every day. These hypertensive patients described their exercise routine in a broader context

96
that covered a range of structured exercises such as running, jumping, stretching and
weightlifting.
I used to run 2-3KM every day early in the morning, there were poles in the ground, so I used
to do exercise there too. I do a variety of exercises as jumping, climbing and stretching. The
exercises in sitting posture to burn only the belly fat and activities like this. (Patient 4)
I have a ladder at home, so I mostly use that ladder as an exercise. I keep ascending and
descending the ladder frequently in a day. Approximately 8-9 turns in a day. Sometimes, very
slow and sometimes very fast. I also use a pole in home for stretching and sometimes weight
lifting too. (Patient 5)
The effect of exercise in terms of weight loss motivated these patients to strictly adhere to a
pattern of regular exercise. For instance, an obese hypertensive patient reported a 10KG
weight loss over a three-month period as a result of undertaking exercises such as running
and weightlifting. He had strong faith in the benefits of adopting exercise in order to control
and manage his weight. In contrast, a few obese patients reported that they had received
negative comments about their weight, and it was this combined with a general stigma
surrounding obesity that had been the motivation behind their programme of weight loss.
They described being met with derision, adversely judged by family members and friends
about their eating habits, and it was this that had driven them to be more proactive in their
decisions about diet and exercise.
Nobody had realised me that my weight was increasing in the beginning but gradually
people made fun of me and poked me often. Then one day, I realised that I will show them
that I’m not a joker, you know and started doing vigorous exercise. I think, if they had not
realised me about my massive body maybe I would not have achieved my weight lose goal.
(Patient 9)
It seemed that these patients were maintaining an exercise routine in order to reduce their
weight to avoid discrimination, and not as part of HTN management. One obese patient
described how he tried for months to shed the extra weight but without success and most
days he went for a brisk hour-long walk, describing himself as almost like a paratrooper in
terms of his intensity. However, when he saw no apparent change in his weight reduction, his
motivation waned, and he ceased exercising. During this period of intense activity, he neither
felt the need to monitor his body weight nor the effect of exercise on his blood pressure
readings, as described below:
I could not check and truly I did not consider that I should also monitor my blood pressure or
check my weight during that period. But when physically I did not see any difference in my
body size at that point, I thought my weight is the same and I’m not slim and that is why I
left exercise. I was just tired. (Patient 4)
The insights of patients’ understandings highlighted the wide range of issues in place to
adopting and maintaining exercise and that some of these were related to personal and social
aspects of the lives of patients. Therefore, the following section will reveal four subcategories
which emerged from the main category.
Socio-cultural norms

97
Some Pakistani socio-cultural norms are believed to affect the ability to sustain a routine of
exercise, as highlighted by some of the study participants. Some patients indicated that due
to the absence of a culture of exercise they felt less committed and motivated in continuing
with it as a part of their daily routine. The lack of a culture of exercise in Pakistan restricted
the participation of patients in certain forms of exercise such as swimming and running.
Women for instance reported how they had been unable to follow the recommendations of
their doctors to visit the gym and workout due to the lack of availability of facilities and
trained instructors. The absence of public parks in every city limited the opportunities for
women to walk safely. One woman stated that it would be difficult for her to visit a gym as
she lived in a remote area.
It’s not easy for me to go to the main city only to join gym and then pay for the membership
and transport. Most of the times, I don’t have enough money to spend so how can I think to
get a gym membership. There are no public parks in the area where we can go and walk
easily. (Patient 12)
Further analysis of the responses from participants in the interviews revealed that some
socio-cultural norms were women-specific, and they were therefore restricted from
exercising. Some women referred to various responsibilities they had and what was expected
of them by their families after marriage. They described how they devoted much of their time
to the responsibilities associated with their roles as mothers, wives, sisters and daughters in
order to fulfil family demands.
Some participants described a socio-cultural norm whereby once a woman married, she was
expected to stay inside the home and attend to domestic chores. These women indicated
having extremely busy daily routines which made it difficult to find time for additional
exercise.
Every day I wake up early in the morning at 5am and then I run around the house to make
breakfast, sending the children and husband to school, office and then get ready myself.
Sometimes, I have preferred my children over my own choices, I think most of the times. (Patient
8)
I have so much work to do at home. I have to cook and provide meal to my kids, husband and
father in law on time. (Patient, 16)
There was a strong sense amongst many of the women that family is the first priority, with
their own interests and activities coming second to the obligations of family chores and
childcare. As a result, some women reported that taking time out for themselves for exercise
could be seen as selfish and therefore a culturally inappropriate activity. Patient 8, was the
only woman partially maintaining some form of daily exercise, even during the time she was
seeing the doctor, recounted in her interview that she had stopped going for a walk regularly
after her marriage as she felt she must always put the needs of her husband before her own:
I’m not regular in going for a walk from the last six months because before that I was not
married and had no responsibility. I think now I’m a wife too and I don’t want to make my
husband feel that I don’t look after him and he is not my priority, you know. (Patient 8)
Lack of time

98
Intensive work schedules and time restraints were barriers to exercise mentioned by most of
the male working-class patients. They described how work duties consumed much of the day
and left them with very few opportunities and little energy for exercise.
I have a treadmill at home, but I feel so tired after my job and go back home in the evening,
I feel so tired and cannot do this. When I finish all work by the end of the day, then it’s already
very late and my heart don’t admit doing anything. I just go to the bed. (Patient 10)
Working class patients cited long working hours as a barrier to them remaining physically
active. These patients described an intensive schedule of work involving long and anti-social
hours, often in retail with shops opening early in the morning and closing very late at night.
Individual factors and concurrent health conditions
A lack of motivation or interest in carrying out exercise was significant within this theme. A
few patients cited lack of inspiration and/or laziness when it came to exercise, and some
linked this with a lack of time. One patient reported his low mood and anxiety issues as
possibly being the underlying reason for him not engaging in exercise and an activity that he
found unpleasant:
My family go but I don’t feel good in my heart that’s why I don’t go. My hearts say to me
stay at home. That’s it. I stay at home. I don’t feel doing any exercise or walk. It is just laziness
maybe, what else I can say. I know, I have anxiety and mood problems and exercise is not
for me really. (Patient 15)
Poor weather conditions were also seen to be a contributing factor in preventing both men
and women engaging in exercise. They expressed a profound dislike of going out in cold and
windy weather. Two patients described how during the winter months they preferred to stay
indoors, go to bed early and used their cars and motor bikes for even very short journeys.
In winter it’s very cold and I don’t like going out in winter. Even for going to a grocery shop
I prefer my motor bike. In winter, it is hard to do any exercise. (Patient 21)
Besides climate conditions, some patients described co-existing health conditions such as
joint pain, blisters to the feet and injuries which impeded their ability to engage in exercise
and walking. These patients provided justifications for not walking more frequently.
Breathlessness, blisters to their feet and painful knees were given as justification by such
patients for not walking more regularly, thus making attempts at following even a simple
exercise regime highly challenging, and left some patients feeling frustrated and hopeless.
Due to this blister, I can’t go for a walk or move and that’s why I don’t walk at all. You
know…hmmm…. exercise is best of all and the most important thing to do but I’m helpless
in this matter. What can I do in this…...? (Patient 3)
Doctor said to me about exercise but how can I do exercise? I’m a patient of joint pains. I
don’t feel comfortable while walking. Exercise is just not for me. (Patient 9)
Some patients described how they had health conditions such as asthma which left them
feeling extremely weak and lethargic; one patient was recovering from an accident, another
had suffered paralysis following a fall resulting in becoming housebound.

99
The accounts of older patients tended to be fatalistic in outlook and demonstrated a strong
sense of powerlessness over their own bodies. They described ill-health and a general decline
in physical fitness as an inevitable part of the ageing process and believed their health would
continue to decline. A fear of falls or sustaining injury was responsible for a majority of older
patients developing a negative attitude towards exercise. The risk of falling due to poor
balance discouraged them from participating in exercise and strengthened their belief that
there was little they could do about their decline in physical fitness. They frequently
expressed a fear of not being able to get back up after having fallen. For example, an 80-year-
old male patient was fearful of exercise having sustained multiple fractures resulting from a
fall.
Two times I have been fallen and got leg and knee fractures. I’m trying to walk briskly once
and the other time while climbing the stairs. Before that I was used to walk but now I’m
scared and uncertain. I don’t think, I ‘m scared now, I won’t be able to get back on my feet
if I fall again. (Patient 11)
Another patient cited:
When I stand up from the bed, my body can’t bear my weight and I feel fear that I might
fallen away. That fear doesn’t allow me to exercise. I just sit on the bed or walk sometimes
in the room. I feel I might fall away, will get hurt and this will complicate my situation
more. (Patient 13)
Inability to actively participate in daily activities and having a sense of their deteriorating
health proved challenging for these patients.
Lack of exercise information from doctors
A majority of patients felt that lack of guidance and advice from their doctor was a significant
factor in their failure to maintain a regular programme of exercise. A common criticism was
that general advice was given but with no specific details as to frequency, duration of exercise
and what types of activity should be undertaken. Some patients indicated a strong desire for
greater information regarding the benefits of exercise and its relationship with high blood
pressure.
If I don’t have much information about exercise and why this should be done to control my
blood pressure, my doctor should tell me the benefits. Well, my doctor should inform me
about exercise and if he/she will explain me in detail then I will understand and take this
seriously. (Patient 7)
4.3.2 Dietary management
In this study, it was noted that failure to comply with dietary recommendations was
particularly common amongst hypertensive patients and this was found to be the case across
all age ranges. An unwillingness or inability to make changes to diet may be due to a number
of factors. Data analysis reveals four categories: (i) preference for traditional foods; (ii) socio-
cultural practices and influence of family and friends (iii) healthy food and personal
preferences; (iv) availability and accessibility to junk food (v) lack of dietary information
Preference for traditional foods

100
Eating traditional food strengthens feelings of belonging and is a vital part of cultural life
(Kittler et al., 2012). Traditional Pakistani food is aromatic, with spices added and generally
prepared with a generous quantity of oil, therefore it is often high in fat content. Traditional
dishes such as curry in Pakistan are commonly made with oil and Desi ghee (clarified butter)
and regularly use cooking methods such as shallow or deep fat frying. Patients in this study
described routinely eating traditional foods which they believed impacted their ability to
maintain a healthy diet. The following sections will illustrate these beliefs.
Paratha and oily food
A typical Pakistani breakfast, locally called ‘Nashta’, includes paratha (made by baking whole
wheat dough and finishing off with shallow frying) stuffed with Desi ghee. Eating paratha fried
with oil or Desi ghee is central to a traditional breakfast in Pakistan. Many patients reported
eating paratha with fried egg, omelette or curry in the morning and also at night. Some
patients shared concerns that eating oily paratha and the consumption of Desi ghee was not
good for their blood pressure, and doctors had suggested this, however they found it difficult
to change this eating practice.
Every day there is a paratha in breakfast daily as you know it’s our culture at home to eat
paratha in the breakfast so that also contains oil. So, you cannot avoid these things at all.
(Patient 10)
One patient reflected that eating oily paratha and fried snacks on a regular basis had caused
his blood pressure to rise on several occasions; he often felt discomfort after eating oily food
items and felt these to be ‘dangerous’ due to their high oil content.
When I eat something that I should not eat like when I take some ‘pokora’ (a piece of
vegetable or meat, coated in seasoned batter and deep-fried) or ‘samosa’ (a triangular
savoury pastry fried in ghee or oil, containing spiced vegetables or meat) and very oily food
hmmm like paratha then my blood pressure again rises and then I feel very uncomfortable.
(Patient 3)
A few patients claimed to have changed their diet following HTN diagnosis in an attempt to
manage their disease but appeared bound to their former eating habits. Patients in this study
were exposed to and had been dependent on oily foods since childhood and reported a
particular liking for the taste of such food. For instance, a 50-year-old patient described how
‘I need paratha in breakfast because I have been brought up on that’ (Patient 7). Many
patients linked their inability to resist traditional food due to the habit of eating the same
food for many years and to make changes to their diet was seen as a daunting task.
When I was young and was not sick, I was used to eat lot of oily food even I still remember I
used to eat parathas three times in a day. My mum used to cook different kind of parathas
like with potato and sugar and sometimes with green chilies. So, these habits develop since
childhood, you know. I feel difficult to change this. (Patient 13)
Some patients described the sensory satisfaction they derived from eating oily traditional
foods due to the mixture of ground spices and ingredients such as ginger, garlic, cinnamon
and cardamom, commonly used in their cooking. They indicated that the addition of such

101
ingredients helped to give flavour to these foods, and this combined with the aromas
generated during cooking made it difficult for them to resist traditional dishes.
We were used to cook ‘gosht karahi’ (a South Asian dish prepared with goat or lamb meat
instead of chicken with oil and spices) at home every day. Who can resist it? It is very tasty
dish and my wife add all the ingredients to make this good. When I enter the house... by
smell I can tell what she has cooked, and I cannot resist that nice smell… [Laughter]. (Patient
6)
Cultural practices and influence of family and friends
Although the majority of patients appreciated the attentiveness of their doctors regarding
diet, the most common problem recounted by patients was the incompatibility of the dietary
recommendations with their daily lives and their views surrounding food and the culture of
eating. In this context, the culture of eating is strongly connected to the social aspects of
eating and cooking, and the pleasure derived from enjoying a traditional meal.
In many societies eating out is a pleasurable experience, a way to honour guests and deepen
friendships. In Pakistan most, social gatherings involve eating with family and friends in order
to strengthen relationships. In this study many patients expressed difficulties in following a
particular diet plan alongside eating out with family and friends. At festivals and special
occasions such as weddings and religious gatherings many patients felt less able to maintain
control of their dietary plan.
In Ramadan, mostly I eat oily things. Why I would lie? I do because when everyone eats and cook the tasty things how can you avoid? After fasting your heart asks to eat tasty and spicy stuff. All the family sit together, and we eat delicious food after a long fast. (Patient 15)
A striking feature of Pakistani society is the importance attached to family members; a typical
Pakistani family consists of older and younger generations living together under the same roof
and their daily lives are closely interconnected. Therefore, eating patterns can also be
influenced positively or negatively by the experiences and opinions of family members.
For example, some patients described how all the family members sit together for their
evening meal of curry, under the same roof, prepared and served in a large pot called a
‘handi’. This cultural norm of preparing curries in one cooking pot from which it is then served
may make the elimination of unhealthy ingredients impractical. A few patients described
difficulties in complying with their recommended diet plan when food was brought by a
member of the family as a gift, and especially children from children. A 55-year-old man
shared his concerns:
Within the extended family it’s very difficult to do proper prevention and avoid oily food and
salt. I have lot of children so when one son comes, he brings one thing, the other brings
something totally different to eat. I cannot break their heart by returning food, you know.
(Patient 2)
Some patients described a culture of gift exchange whereby a meal was either given or
received on special occasions such as Eid, passing an exam, a wedding or the celebration of
the birth of a new baby. They felt uncomfortable refusing gifts of food from a loved one or
friend at such events in spite of how unhealthy the food proffered may be.

102
We exchange food like curry and rice with our neighbours and extended family members
when it is Eid, some similar occasions and sometimes when we make extra food. All made
with oil or desi ghee and it becomes difficult and seem impolite to say no to someone who
is bringing the meal for you. It is not acceptable in our culture. (Patient 7)
Some older patients described how they found it difficult to sustain the changes to their diet
in an extended family. Older family members hold a place of high respect in Pakistani society
due to their wealth of skills, life experience and hierarchical position within the family unit. In
this study some older patients described that the family often seek their advice on cooking
and preparing food, but the majority indicated that they had very little influence when it came
to promote healthier cooking - they had always been served food high in spice and oil content
and this was determined by the food choices of other family members.
When my daughters cook spicy food like rice and Biryani then I become annoyed with them
that you have added too much spice and oil in it. My daughters say mother it’s not too much
spice and oil, it’s just little spice, otherwise it will be tasteless…you are just feeling more.
Hmmm…. I can’t eat that food. I feel chest discomfort. They don’t listen. (Patient 23)
Sometimes, in curry they add more ghee, then I become irritable and annoyed with my family
that please don’t add this much ghee in the curry. They think about themselves only. (Patient
17)
Many older patients described skipping meals altogether if the food was unappetising in
appearance, was not flavoursome, contained ingredients they disliked or found difficult to
tolerate (such as hot spices), chew and digest. In Pakistan, women play an important role in
the selection, purchase and processing of food. Many older patients reported that they were
reliant upon the daughter-in-law for preparation of meals and choices over food and this was
a matter of concern for them.
A small number of older patients interviewed stated that they did not have a positive
relationship their daughter-in-law due to conflicts in a number of areas. A few patients felt
that they had little choice but to accept and get used to the food served by their daughter-in-
law and fear of repercussions made these patients reluctant to complain or voice their
concerns over food choices.
I don’t say anything to my daughter in law. She cooks food and in charge in house. Why I
should ask her to add little salt. If she insulted me? I don’t say anything to her. (Patient 1)
My daughter in laws fight with each other. As you know, fight in elder daughter in law and
younger daughter in law is common in Pakistan, that’s the reason. When I see they are
fighting and beating the kids I become upset and ask them not to do this. How can I ask her
to take care about me and my food? They all just fight all the time. (Patient 14)
By contrast patients who had understanding partners and a supportive family network
reported that they were more able to comply with their recommended diet plans. For
example, some elderly patients described how their spouse or children would remove the
unhealthy ingredients from meals or prepare a separate portion of food without the addition
of oil or spice. Two patients described how they had always been served carefully prepared
and cooked homemade food by their partner.
103
I have informed my wife in the house to add less salt in the curry. I told her that doctor has advised
me to eat less salt. She takes care now and put less salt in the curry. I forget often but she always
remembers. (Patient 5)
My husband is very nice; he has no comparison. He loves me unconditionally and his breath is
connected with my breath. He always takes care of my food and medicine. He never cooks or bring
the food that is unhealthy for me. (Patient 8)
The majority of patients described how cultural practices and the influence of others
impacted their food choices. However, analysis of the interviews further revealed that
patients’ personal preferences had also a strong influence on choices of food.
Healthy food and personal preferences
Besides socio-cultural influences, eating practices may also depend heavily on the personal
understanding of an individual as to what constitutes healthy food. A few patients believed
that a healthy diet consisted of fruit, vegetables and meat, but perceived such healthier
products to be more expensive. Some patients stated that they would purchase fruit and
vegetables when on special offer, but otherwise this did not form part of their regular buying
habits. Patients spoke of the difficulties they had in obtaining fresh fruit and therefore felt
unable to instigate the healthy food interventions necessary in controlling HTN.
In contrast, a few patients reported that they avoided these healthier options due to lack of interest
and found it difficult to resist fatty food because of lack of self-control and willpower. It appeared
that their desire to enjoy life outweighed any resolve they had to follow a healthy diet.
I’m a lion in matter of eating and drinking. I eat chicken, chicken leg piece, lamb. I cannot
live without meat. This is my life. I just only know one thing eat, drink and enjoy, that’s it.
(Patient 3)
Food in itself can carry many symbolic meanings and certain emotions may be associated with
the act of eating. Often people use food as a means of compensating or comforting
themselves at times of emotional distress or to satisfy a different need that they have been
unable to fulfil. For instance, a patient described how eating her favourite snack would at
times satisfy her cravings and act as a temporary form of escapism from the strict dietary rules
that seemed to govern her life.
When I come to the city then I request my daughters to buy some ‘pakoras’ (a piece of
vegetable or meat, coated in seasoned batter and deep-fried) and a naan (A South Asian
bread) and I eat not very often. My heart asks for eating fried thing occasionally. Yes, I feel
helpless in this matter at times. (Patient 13)
Other patients claimed to be under the influence of factors beyond their control, the
appetising appeal of delicious fatty food was virtually impossible to resist and made it all the
more difficult to comply with a healthy diet plan.
Availability and accessibility to fast food
Quick and easy access to fast food outlets was mentioned as a contributing factor in the over-
consumption of fatty food by both sets of respondents. When patients had easy access to

104
eating establishments such as hotels, takeaways and fast food restaurants they seemed to be
easily tempted. One patient, for instance, described how having a takeaway near to his house
provided him with comfort in the knowledge that he would be able to obtain ready to eat
food and this influenced his decisions when it came to making food choices.
When I was posted in Chistiyan city, I was used to eat from the nearby hotel. Every day I
used to go there and was eating oily and spicy food. Because it was very close to my house.
I think if you have a hotel or takeaway near to your house you can eat food there easily.
(Patient 4)
For a small number of working-class patients, they were habitually eating takeaways as their
long working hours left them with less time to prepare and cook a fresh meal at home. Many
patients were aware that eating fast food was not beneficial for health, although this was also
an option who found cooking too much of a chore and a time-consuming process.
A minority of patients described fast food as a treat when they fancied a change from
conventional homemade food and their usual meal routine. The variety of food items on offer,
the flavours and attractive colours of fast food were all mentioned as appealing factors when
it came to their consumption. A number of middle-aged patients cited fries, pizza and fizzy
drinks as the preferred fast food choices when eating out and spending time with friends and
family. One patient expressed how fast food was a way of eating something ‘different’,
socialising and spending time with friends and family members.
It happens that you can’t eat homemade food every day. Most of the time we eat homemade
food. But for something different and get rid of typical routine eating pizza and drinks
outside is not a bad option. When I go out with friends and family then we prefer to eat fast
food just to try out something new and different. I think these restaurants are a good source
to sit and eat together. (Patient 3)
Conversely, a few patients shared concerns with regard to fast food terming it as ‘bad for
health’ and therefore avoided eating it. For example, one male patient described that his main
concern originated from rumours with regard to the quality of ingredients used in fast food
as well as to the manner in which it was manufactured and prepared. Two patients expressed
concerns about the hygiene within fast food restaurants and stated that they had experienced
symptoms such as discomfort, constipation and stomach upsets after eating beef and cheese
burgers. They preferred to eat healthy meals cooked at home and prepared in a hygienic
environment and avoided takeaway and restaurant food. Patient 22 also described:
I saw myself once that person in the restaurant was using old and smelly oil in making food.
I left the place straight away! I also had problem of chest discomfort whenever I had eaten
food from restaurants. Now I avoid all these places. I like to eat home cooked food because
home cooked food is safe to eat, and my family make sure to add good quality ingredients.
(Patient 22)
Lack of dietary information
Most of the patients stated an overall lack of dietary advice from doctors. They desired for
detailed information about dietary changes in consultations to manage their high blood
pressure. Patients pointed out that information on changes in diet was often based on a
105
nonspecific suggestion of a healthy diet rather than specific food and nutrition advice
provided by doctors. They raised concerns that a simple indication to control the diet was
useless except when it was accompanied by concrete information about how to achieve this.
They don’t tell me anything about food. They are always in hurry. (Patient 7)
If they tell me in detail about food, then I can think this is good and why and that is not good and why.
They just tell me about high or low blood pressure, that’s it. (Patient 8)
4.3.3 Salt consumption
Many patients linked their dietary salt consumption with taste, customary practices and
information received from doctors. Most of the patients believed that salt was an essential
seasoning for their meals as it provided flavour and fragrance and made them delicious to eat
and extra salt was frequently added to boiled eggs and curries. One female patient described
an overwhelming sense of satisfaction when oranges, water melons and boiled eggs were
eaten with salt because she felt ‘unable to eat these food items without salt’. (Patient 23)
Increased salt consumption was also customary practice. Many patients were reluctant to
change their cooking practices and add less salt to curries for fear that the resulting meal
would lack flavour. They considered a meal to be unacceptable if it has no salt or less salt and
stated that this is a ‘basic ingredient’ when cooking traditional dishes. For instance, an older
patient recounted how:
Look, there is a rose petal that will not give fragrance till it will blossom properly. It will
blossom properly then it will give the fragrance fully. Similar is like my curry. When I add salt
in it that’s good, if no salt then…Yuk…hmmm…so in this way. So, I add more when I feel it’s
tasteless. (Patient 11)
Tea is consumed in most Pakistani families more than twice a day or even more and prepared
by boiling water, tea, milk and sugar in a saucepan. Some patients indicated that they
preferred the addition of salt to sugar in their tea and felt that without salt tea seemed raw
and unpalatable. These patients described how salty tea was served and enjoyed by family
members at breakfast and after dinner. It is also customary in Pakistan to offer tea to guests
with a small portion of biscuits and some snacks. One 56-year-old female patient described
how she was served a salty tea every time she visited her daughter-in-law’s home, ‘I don’t
know why they offer me salty tea every time, I think it’s common in that family, they all drink
this.’ (Patient 13)
Another patient expressed his reluctance to change a practice that he had been familiar with
since childhood, even though he had been diagnosed with HTN and his doctor had
recommended he reduce his salt intake.
If we don’t add salt in the tea, it remains semi boiled or like something remains raw or
uncooked. It tastes good with salt. From my childhood, I have seen this thing in my house.
This is childhood habit you can say. Children and all young and old people in the house like
salty tea. Doctor has asked me not to use too much salt, but it is difficult you know. (Patient
27)

106
One patient stated that the addition of salt in tea helped to relieve her headaches and
provided a soothing effect, whilst patient 9 expressed that taking salty tea with paratha
helped ease her digestion and tasted ‘delicious’. Further exploration relieved that some
patients also added salt to flour to improve the taste of parathas and chapatti. They held a
common belief that the addition of salt to the flour made chapatti and parathas easier to cook
and provided a ‘unique’ taste when accompanied with tea. The salty paratha was also
considered a substitute if there was no curry or eggs available to eat at breakfast. Patients who
were accustomed to a salty taste seemed reluctant to eat parathas and chapatti cooked without
salt.
I do add salt in tea and in flour, without salt chapatti don’t taste good. Otherwise, flour
seems tasteless and sweet and when I add salt in it then chapatti becomes tasty, easy to
cook and salty. In flour we must add. In tea, [Giggling] not very often but yes, sometimes. I
can’t eat my parathas and chapatti without salt. (Patient 25)
In contrast, some patients were familiar with the risks associated with high salt consumption
and indicated that they used less salt in preparation of meals. These patients described how
eating foods that were high in salt sometimes increased their blood pressure, made them feel
dizzy and suffer headaches. They reported that doctors had advised them during
consultations to reduce their salt consumption as a method of controlling their blood
pressure. They referred to food items with a high salt content as ‘dangerous’ for their health
and had frequently refused curries that they felt to be too salty. These patients described how
they would request of family members not to add excessive salt when preparing meals or ask
for a separate portion prior to salt being added.
As a high blood pressure patient, I know that there should be less salt in diet. My doctor told
me this in detail and I try not to eat too much salt. I have asked my family not to add too
much salt in cooking food or take my portion out soon before adding salt and they make this
sure. (Patient 10)
Doctor told me don’t eat too much salt. I don’t eat much salt, I use very little salt. I feel when
I use more salt; I feel problem inside my stomach. I hate salty curries and don’t eat that. My
daughters avoid adding excessive salt while making food. (Patient 13)
However, most patients had little or no knowledge about the maximum amount of salt
required per day for someone with a hypertensive condition. Almost all patients reported that
they were never informed by doctors as to the quantity of salt they were safely allowed to
consume. Patient 4 shared his concerns:
I don’t need how much amount of salt I should take daily and what is enough or excessive. My doctor
never told me how much is required to me and what was excessive. They just tell me add little, so how
much is little? I just add some that give good taste to my food. (Patient 4)
4.3.4 Smoking
In this study, all ten patients who were smokers were aware of the health risks surrounding
tobacco when it came to developing complications with their HTN. However, they had their
own beliefs in support of their smoking habit and seemed keen to discuss why they enjoyed
smoking and how they felt it had helped them to some extent. For instance, a few held the

107
belief that smoking stabilised their mood and provided relief from stress and anxiety during
difficult situations in life. They felt that this was not something that they would be able to
achieve without the aid of nicotine and it was for that reason that they found it very difficult
to quit smoking.
Sometimes, I smoke to release tensions and worries in my life. I just go outside and smoke,
sometimes two packs in a day. I know it is not good for my blood pressure as doctor told me,
but I can’t cope with stress without cigarettes. (Patient 10)
Two patients described how smoking aided their digestion and acted as a muscle relaxant to
the bowel, relieving them of constipation.
I started smoking to relieve indigestion and gas problem because I had heard smoking cures
indigestion and gas problem and it really works. I don’t feel relaxed and relieved unless I
smoke. After smoking when I go to toilet, I don’t feel any trouble in my bowel movements.
(Patient 27)
Some patients identified different stages of smoking from their ‘first puff’, experimentation,
through to social, casual and then fully established smoking. In this study there were emerging
themes relating to smoking and the role that family and friends played in its adoption.
Facilitating access to tobacco and socialisation with smokers were the common reasons that
had contributed to uptake of the habit in early life.
Socio-environment influences
When discussing smoking many patients highlighted the role of their environment and social
influences when it came to adopt the habit. Acquiring tobacco from family members and
friends was seen to be a common pathway into early experiments with smoking and was
mostly opportunistic in nature, facilitated by the availability of tobacco in the home. Some
patients had been supplied tobacco directly by family members, usually cousins, siblings and
also close friends. The smoking habits of loved ones greatly influenced a few patients and the
likelihood of them taking up the habit and their continued use of tobacco. As one patient
described:
My friend Syed, his brother was abroad, and he used to give me cigarettes from abroad, that
were in black in colour and smell was like a lychee. They were different than the local and
he always used to send me packs from abroad or brought himself. We both had to enjoy
smoking in each other’s company. He was the first person who started my smoking habit
because he was already into it and asked me to try as well. (Patient 17)
They stated that experimenting with smoking occurred usually between the ages of 10 and
13, resulting in increased nicotine dependence and greater consumption later in life. Those
who revealed that they had started smoking earlier generally lived with other smokers and
therefore had greater exposure to the behaviours of smokers and tobacco was readily
available to them. The main motivation for taking up smoking appeared to be curiosity,
watching others smoke and seeming to enjoy it and this was compounded by high exposure
amongst family and social networks.

108
The majority of smokers in this study were males and no females confessed to being smokers.
It is possible that they would hide this habit due to the social stigma associated with women
smoking in Muslim countries. A few female patients used negative terms to describe the
behaviours of the male smokers in their families, referring to them as ‘annoying’ and ‘bad’.
One female patient recalled the suffering and poor health that a smoker in her family had
experienced and this had been a sharp warning to her not to fall into the same trap.
My father died with a heart attack and in the start, he had high blood pressure. He was a
chain smoker. Many times, doctor asked him to quit but he couldn’t. That’s why I hate
smoking. I even can’t see someone smoking in front of me. This annoys me. (Patient 13)
Perhaps unsurprisingly, non-smoking patients appeared more strongly convinced of the
health risks associated with tobacco smoke than the smokers. They described that smoking
not only caused symptoms such as coughing, sneezing and irritation to the throat and eyes,
but also had serious consequences in terms of high blood pressure. These patients described
how they would request that smokers in the family go elsewhere to smoke outside the home
and that they would remove their children so as not to expose them to harmful tobacco
smoke.
Cost was also a concern and a few smokers mentioned the negative impact their habit had on
the family budget. They indicated that money spent on smoking was a waste and could be
better used to improve their economic circumstances. Many conceded that smoking had
detrimentally affected their relationships with family members. One patient described that
his family members hated the physical discomfort that tobacco smoke gave them, irritating
their eyes and how the smell made them feel sick. Another patient felt stigmatised by family
members, believing that they held him responsible for contracting his disease as a direct
result of his smoking habit.
I think, my family don’t like me due to my smoking habit. I don’t smoke in front of them now.
They blame I have brought this disease into me due to smoking. Many people have this
disease and they are not smokers. But my family blame me and don’t feel comfortable when
I smoke. (Patient 10)
Personal factors
Three patients said that in spite of advice from their doctor they felt hopeless in their bid to
quit smoking due to strong nicotine dependence and the potential for unpleasant withdrawal
symptoms. They described that they had attempted to quit on various occasions, this would
sometimes last a few days, sometimes only a few hours, but they would always relapse. One
patient described feelings of sadness and depression on quitting smoking and this had
eventually led to frustration, anxiety and ultimately a return to smoking.
A few patients who had previously been smokers described their dislike of being a smoker
and how they found the smell of cigarettes unpleasant and irritating. They were aware that
smoking was harmful to health and had received such warnings from their family members;
with family support and enough motivation they had been able to stop smoking.

109
It was really very difficult to quit but, in the end, I had to quit it for the sake of my health.
Nothing is more important than the health. It all depends on the personal choice,
determination and the priorities. My wife supported me in that. (Patient 5)
My family really helped me in coping with symptoms when I quit smoking. They always
supported me, but I think your own determination also plays a main part. (Patient 2)
It was noted that some patients did not view doctors as being of assistance in their efforts to
stop smoking. A few smokers felt that their inability to give up smoking had impacted
negatively on the behaviour of their doctor towards them and they felt they were deliberately
afforded less time and information as a result. They reported hiding the facts about their
smoking habit from doctors for fear of this reaction. Patient 11 stated:
I know that smoking is not good for my health and blood pressure and that’s why I don’t tell
doctor about this now. I know, he will be angry and blame me as used to do in past. He
doesn’t like to spend time on smokers in general. I don’t share with him that I still smoke. I
think he must be angry and will let me go quickly. (Patient 22)
4.3.5 Alcohol consumption
The religious beliefs of all patients strongly informed their attitudes towards alcohol
consumption. Alcohol consumption is explicitly prohibited in the Islamic faith and viewed very
much as a symbol of sin and evil in Muslim societies (Michalak & Trocki, 2006; Ghandour et
al., 2016). As with many other Muslim countries, sale and use of alcohol is illegal in Pakistan
and there are strict laws of enforcement (WHO, 2004). Despite it being illegal in Pakistan,
drinking and denying is a growing problem in the country (Haider & Chaudhry, 2008; Butt,
2015).
In this study, all patients stated that they did not partake of alcohol, except for one
respondent who belonged to the Sikh faith. It might possible that they tried to hide their
drinking habit, however, in discussions on alcohol consumption all patients described that
their religion promoted abstinence and that there were strict rules under Islam on alcohol
consumption. Some patients believed drinking alcohol as ‘Haram’ (forbidden by Islamic law)
and a shameful activity in accordance with Islamic teachings.
May Allah forbid me, it’s not a good thing to adopt in Islam. I stay away from such things.
Any kind of addiction is ‘Haram’ in my religion. Allah curse people who drink and like this evil
thing. (Patient 21)
No, no such things. I have never come across alcohol in my entire life. It’s a very bad thing
to think about in our religion. Allah forgives me. I never thought about this ever in my life.
Such things are ‘Haram’. (Patient 17)
It would seem that patients consider alcohol consumption to be a harmful activity on religious
grounds and their reported abstinence was not due to an awareness of the health hazards of
drinking in association with HTN. Other than taking antihypertensive drugs and managing
lifestyle, some patients reported involvement in alternative treatments as the following
theme explains.

110
4.4 Involvement in Alternative Strategies
Patients reported involvement in a variety of alternative strategies that they employed to
manage their HTN. Within this theme, identified categories were: consulting quacks and
Hakeem, using alternative medicine and home-remedies, and employing religious practices.
4.4.1 Consulting quacks and Hakeem
A majority of the patients believed visiting a quack and Hakeem in the hope of seeking an
alternate solution to their long-term HTN treatment. They were often referred by a family
member who had past experience with quacks and Hakeem treatments or patients had been
enticed by eye-catching advertisements on television.
According to some patients visiting quacks and practicing Hakeem medicine had been
effective in the early days of treatment and they felt energetic, happy and symptom-free.
However, gradually they experienced the deleterious effects of the medicine in the form of
severe symptoms and harmful side-effects.
I took Hakeem medicine 3-4 times and I got relief for time being for my breathing problem
due to blood pressure. But eventually I got swelling all over the body and my body was like
a balloon. I felt that my breathing problem is relieved but I’m getting some opposite and
awful results. My blood pressure never came down after that. (Patient 13)
First of all, I had only problem and then I took Hakeem medicine, after that I got only more
diseases and complications. Hmmm… He only treated my joint problem. He never asked
about my blood pressure, I took his medicine for six months and after that my health has
been ruined. I just gone very far away in my health. (Patient 22)
Patients cited that most of the medication used in HTN treatment by quacks and Hakeem
were loose packaged with no written information and could not be administered via injection.
Patients termed injectable medicine as ‘minerals’ which provided quick relief of their HTN
symptoms, however they were charged extra as a result of separate injection administration
fees. Suffering the slow but often risky side-effects, a worsening of their HTN and the appearance
of further complications caused patients to realise that they had made a misinformed choice in
adopting non-mainstream treatment. For example, patient 30 describes his experiences of
visiting a famous quack in his city in the following extract:
There is a fake doctor in our city. He is very famous. But he gives the same injection to every
patient. An injection ……… Now, everyone knows that injection is a very powerful medicine.
Even a very weak horse will feel powerful after that injection. The same happens with all
people. A very sick person feels better right after that injection. He gives very cheap and
almost same medicine to every patient. After some days very, bad results start to appear! I
feel regret now and advice people not to go to these people. Hmmm. (Patient 30)
Some patients expressed how quacks and Hakeem took advantage of their gullibility and
reflected upon the manipulated clinical tricks and their ability to exude self-confidence. Some
highlighted a technique whereby Hakeem exploited religious beliefs by associating their
treatment or services with an article of faith.
111
When I asked how useful the method is, he smiled and said: modern medical science is
actually nothing. Actual treatment is from ancient science of Unani medicine and that’s what
our religion also says. (Patient 27)
Hakeem told me that his treatment was according to what Quran says and not dangerous
and having side-effects. (Patient 12)
Moreover, a few patients were offered a cup of tea or drinks during the consultation to display
magnanimous hospitality, thereby building a good relationship. The secret of this art made
the patient believed that he/she cared about as a person as the following quote illustrates:
I think the tricks they use are very effective. They feel you very comfortable and important
person and treat you very well. They also offer tea or drink, and, in this way, you feel like a
family member really. I felt open up automatically in front of him because he felt me special
but now, I got it why he does all this just to gain my trust and make me fool. (Patient 10)
Most patients cited that they needed to visit quacks to monitor their blood pressure when
asked by their doctors to undertake blood pressure monitoring. With regard to blood pressure
monitoring the majority of patients reported having easy access to quacks and non-regulated
services for blood pressure monitoring. Easy access to clinics runs by quacks had created a
lack of interest amongst patients to monitor their own blood pressure, learn the necessary
skills or indeed purchase a monitor. As patients described:
I go to the dispensary nearby to my house. I mostly go to that dispenser for blood pressure
check-up. When I feel that my blood pressure is very high and uncontrolled then I mostly go
there and ask him to check my blood pressure. If I have a facility nearby, then what’s the big
deal? I go straight to the dispensary and they check and tell me my blood pressure. Main
thing is availability of a facility. If the facility is not available, then you think about checking
by your own but if the facility is not available then you don’t think in this way. (Patient 15)
We have a dispensary close to the house. My son brings me there every time for blood
pressure check-up. He takes some money for checking blood-pressure. That’s why I did not
think to buy a blood pressure monitor. (Patient 18)
Even patients who were highly educated also expressed reliance upon non-regulated services and quacks due to their ease of access and also seemed disinterested in monitoring their blood pressure at home. Unofficial service providers and quacks often scheduled visits to patients’ homes in order to check their blood pressure check and this had caused patients to place greater trust in these services.
4.4.2 Alternative medicines use and/ home remedies
Some patients believed in using herbal and home remedies to attempt to cure and manage
HTN. Herbal remedies were described as being ‘bitter’ in taste but were purchased locally
with herbs and roots forming the main ingredients. Some patients referred to interaction with
hypertensive friends and other sufferers in the community as being a source of information.
These remedies were taken in addition to prescription antihypertensive drugs for the
treatment of HTN. The patients reported that they did not inform doctors that they were
taking herbal remedies and had stopped taking their antihypertensive drugs; they felt that

112
their doctors would disapprove of their actions, perhaps not listen to them and make
judgements about their intellect. Many patients indicated that doctors did not understand
the efficacy or benefits of home remedies.
When I took garlic then I didn’t take my blood pressure tablets because I wanted to see either
garlic is doing some work in my body or not. I did not tell this to my doctor because he doesn’t
like such things and don’t believe on remedies. He will think I’m an idiot. (Patient 21)
In addition to home remedies, a few patients relied upon traditional therapies which they
believed would purify their blood. For example, a female patient cited that wearing a magnet
around her neck was a cultural practice amongst women in her area to cleanse the blood and
it was believed to restore energy which would help in dealing with HTN.
As you can see, I have a magnet necklace here. [Pointing towards neck] Some women in my
area asked me to wear this magnet all the time in the neck. Once I have started wearing this
I feel really good about my blood pressure. Other than this I don’t use anything. Many people
wear this. A magnet to control the blood pressure to clean blood and gain energy. Many
people wear this in my city and its common here. (Patient 28)
Religion was another significant component of patients’ lives and played an important role in
shaping beliefs, adopting certain attitudes and making decisions regarding HTN management
as discussed in the following category.
4.4.3 Faith healing
All patients in the interviews except for one were Muslims. Patients cited involvement in
religious practices in order to seek faith and strength during times of stress with the
appearance of HTN symptoms. Considering Allah as the ultimate authority on life and illness,
a dominant belief, helped and encouraged patients to cope. For example, some patients
reported connecting with Allah through prayer, whom they believed to have unlimited
powers and be infinitely merciful, this helped them to relax and made them feel more
optimistic about the future. They shared that the distress and suffering they experienced with
the disease would not continue forever and eventually they would be cured.
Moreover, some patients frequently recited the word ‘Alhamdulillah’ (I thank Allah) indicating
their appreciation and respect for Allah’s will when discussing their disease and its
management, stating “I have blood pressure but thanks to Allah I’m well” or “I take my tablets
but thanks to Allah - He has given me a lot’.’ (Patient 8). Positive religious beliefs seemed to
help patients cope with their disease and face its consequences. For example, when dealing
with stress they were encouraged by their faith to be optimistic, which afforded them a sense
of peace, tranquillity and diminished any self-blame.
However, negative beliefs adversely affected health and impacted upon their disease
management. For example, some patients in this study used religion frequently as a reason
to avoid taking responsibility for their own health and for not accepting medical intervention.
The potentially harmful effects of such beliefs were clear when patients refused to take drugs
and defended their non-adherence to HTN treatment in the context of religion. Perceiving

113
disease and its cure to be in Allah’s hands influenced some patients into thinking that
adherence to treatment plans were not essential unless Allah did not wish to grant a cure. As
a result, these patients decided to stop taking their drugs and failed to seek timely medical
attention.
The death is in Allah’s hand and it will come one day if you follow the treatment or not. That
day is written and final. What a human can do in front of Allah. I don’t tangle myself too
much in disease management. Only that will happen what Allah has written for us so why
so much preventions then? (Patient 4)
Some patients believed that HTN was a form of punishment from Allah as a result of sins
committed in a past life and this weakened their desire to take antihypertensive drugs. They
indicated that only Allah’s mercy could cure them and therefore turned to religious healers.
I still remember that I have done something bad to my younger sister and she was not worthy
of that. That’s why this blood pressure disease is punishment of my bad deed from Allah.
Only a religious and pious man can get me out of it. I know medicine won’t work in me.
(Patient 23)
In contrast, a few patients preferred to rely on destiny and fate, believing that everything, all
events and happenings in life have a purpose and there were no random accidents or
occurrences. They cited that their destiny was in Allah’s hands and they were not worthy to
ask ‘why me’? when they had first been diagnosed with the disease or developed
complications.
Life and death are in Allah’s hand. The day written in grave on that day you cannot be
outside whatever you do. But Alhumdolillah, (praise be to Allah) what Allah can do He can.
The life that has given by Allah and write for us will happen in that way no matter you have
disease or not. I have left everything in Allah hands. (Patient 10)
4.5 Summary
This chapter provided insights into understandings of patients which shaped their approach
towards managing the disease. The responses of patients regarding their understanding of
HTN in terms of diagnosis, symptoms, causes and justifications for intentional and
unintentional non-adherence to antihypertensive drugs have been presented. The analysis of
patients’ narratives illustrated how socio-cultural context and an inadequate information
regarding lifestyle changes shaped their practices. Finally, the chapter presented patients’
involvement in alternative treatment strategies as they perceive these to be effective and
made decisions to visit quacks, Hakeem and religious healers.

114
Chapter 5: Doctors Perceptions of HTN and its Treatment
Doctors’ understanding about HTN is also an important indicator of their practice and
approach towards disease management. This chapter will explore what emerged from
interviews with doctors regarding their understanding of HTN, its treatment and treating
hypertensive patients. The five main themes that emerged from the analysis of doctors’
interviews are: perceptions about HTN, treating hypertensive patients, perceptions regarding
lifestyle management, informing hypertensive patients about HTN and communication issues
during consultations.
5.1 Perceptions about HTN
All doctors at the beginning of the interviews were asked about HTN as a disease. They
described HTN as a chronic disease that is highly prevalent in Pakistan; they expressed
concerns that HTN and diabetes were the two main reasons for cardiovascular disease and
renal complications amongst patients in Pakistan. Most doctors reported a gradual increase
in the number of hypertensive patients with uncontrolled HTN visiting outpatient
departments in public hospitals.
Hypertension is very common in Pakistan and every second person is hypertensive nowadays
here. I see around fifty patients of HTN every day that come with BP problems. In every
family there are at least two hypertensive patients here in Pakistan. Their number is
increasing. (Doctor 5)
Doctors also cited HTN to be a silent disease that progresses slowly and causes organ damage
if it remains undiagnosed and untreated. Many doctors believed that the absence of
symptoms, non-specific symptoms and a delay in seeking appropriate medical advice by
patients made it difficult for them to detect and diagnose HTN in its early stages. Doctors
believed that it was the delay in diagnosis that adversely affected quality of life for patients
and ultimately impacted upon prognosis and survival rates; they explained that delays in
diagnosis allowed HTN symptoms to develop into complications in patients and a worsening
of their prognosis.
Frankly speaking the patients come to us with primary or essential hypertension very late
and without that specific time period. Sometimes we are unable to confirm and label as
primary hypertension due to delay in diagnosis. They develop the complications at that time
period when they come to us. (Doctor 6)
The doctors identified some particular risk factors; for example, many emphasised eating
unhealthy food and stress as a major reason of ineffective blood pressure control amongst
patients. There was a general concern in doctors that patients from urban areas in particular
were adopting sedentary lifestyles and as a result had become obese and hypertensive.
Doctors correlated their views with the medical literature and considered some patients to
be at greater risk of developing HTN than the others due to the presence of risk factors.
115
A few doctors highlighted that age was a factor in developing HTN due to the almost inevitable
process of hardening of the heart blood vessels with increased age. They cited that most of
the hypertensive patients who presented in the outpatient department were over the age of
forty and therefore inferred that increasing age was a cause of HTN.
HTN can be age related and the risk of having blood pressure increase with an increasing
age. When a patient comes to me, I first check the age of the patient, if it is above forty then
the risk of HTN is there and mostly these patients have HTN. Age is non-modifiable risk factor
and we cannot change this. (Doctor 8)
Whilst reporting causal factors many doctors indicated that HTN was a genetic disorder and
individuals with a family history of HTN were possibly at higher risk of developing HTN. They
explained that if one or more members of a family had HTN the likelihood of other individuals
within the same family developing HTN the condition in the future was doubled. The absence
of screening tools to evaluate the genetic risk earlier in these families was considered to be a
barrier to the control of HTN.
One of the main causes of HTN is a positive family history, you know. If it is genetic then you
can’t escape from it and in such families, the risk doubles among individuals. Unfortunately,
we don’t have any screening and evaluation tool to monitor such families and their blood
pressure annually. (Doctor 2)
Positive family history of HTN is the main cause in our patients, I think. If you have
hypertensive parents, then your chances of becoming hypertensive are double. How we can
screen these families this is the point to think. (Doctor 26)
A few senior doctors who had been working in hospitals for many years had a different
viewpoint and this was based on their extensive work experience. They expressed the opinion
that poor adherence to antihypertensive drugs and a lack of follow-up consultations were the
main factors of uncontrolled HTN amongst patients. These doctors highlighted that patients
often stopped taking their antihypertensive drugs on a regular basis with the disappearance
of their physical symptoms, ceased to attend appointments and therefore became non-
adherent. The doctors stated that patients often failed to attend their second appointment
and would only come back once the same symptoms had returned. This was highlighted by a
senior doctor who had been working in a hospital for four years in the following quotation:
Many patients come to us who have skipped their medicine. We recommend them to use
their medicine on regular basis but when their complaint resolves such as headache and
dizziness, they think they are ok now and then they stop taking medicine. They won’t come
for check up until they will get the same problem or symptoms again. So, this is the main
cause of high prevalence of HTN. (Doctor 7)
Most of the doctors indicated using HTN diagnostic criteria and guidelines to best determine
how to treat HTN. Further analysis of doctors’ interviews identified two categories: (I)
awareness about HTN guidelines (II) practicing HTN guidelines

116
5.1.1 Awareness about HTN guidelines
All the senior doctors were familiar with the national HTN guidelines produced by the Pakistan
Hypertension League and the NICE (the National Institute for Care and Health) guidelines that
are in line with the UK NICE guidelines for HTN detection, control and treatment (PHL, 1988;
NICE, 2011). They reported adherence to these guidelines when diagnosing and treating
hypertensive patients in consultations. Many doctors emphasised that they used the HTN
guidelines to prescribe appropriate antihypertensive drugs for patients. However, many
junior doctors reported that they were not updated regarding HTN treatment guidelines and
were unsure how to apply the guidelines in their clinical practice.
For example, a few junior doctors stated incorrect systolic and diastolic blood pressure
readings when describing how they labelled and documented HTN in patients. Some of these
doctors established an HTN diagnosis on the basis of only one reading at 130 mmHg and
reported starting drug treatment at this stage in their patients.
Hmm, you confirm this when you have a BP reading on 130 mmHg and then you label this
as HTN and start giving beta-blockers to patients, I think. (Doctor 12)
A family history of HTN and the age of the patient were other factors that some junior doctors
used to document HTN diagnosis and prescribe antihypertensive drugs. They reported
immediately commencing with antihypertensive drugs in these patients without confirming
their diagnosis via two further high blood pressure readings as recommended within the
guidelines.
Patients who are old and walk in patients while some with positive family history come with
high blood pressure reading then I think in my mind that he must be a case of primary
hypertension and prescribe them antihypertensive drugs accordingly. (Doctor 22)
Lack of awareness about HTN guidelines amongst junior doctors may go some way to
explaining why senior doctors would more commonly confirm the diagnosis in hypertensive
patients first seen by their junior peers. Furthermore, many doctors felt that junior doctors
were not given the opportunity to observe new cases, identify HTN and make a diagnosis or
to refresh knowledge throughout their training in public hospitals.
A number of senior doctors felt there to be gaps in the training of junior doctors with regard
to the management and treatment of HTN, mentioning that heavy workloads often meant
that junior doctors did not receive sufficient training and their knowledge were not kept up-
to-date with the recommended clinical guidelines.
I think the training of junior doctors is not up-to-mark. One reason is workload and in that
we cannot provide them enough time. Secondly, in medicine a house officer spends only 3
months when he/she starts dealing the disease, learns how to manage patients then he/she
moves to the next rotation. So, in three months under heavy patient load what kind of
learning will take place? (Doctor 13)
Senior doctors felt that inappropriate medical practice and inadequate training with regard
to disease management was compromising levels of patient care in public hospitals. However,
117
they expressed some concerns and reservations about the practicalities of HTN guidelines and
their uncertainties as emerged in the following sub-category.
5.1.2 Practicing HTN guidelines
The guidelines for HTN treatment were designed to assist doctors in determining the
appropriate management of HTN in order to increase the percentage of patients with
controlled blood pressure. However, in this study a few doctors expressed concerns regarding
the practicality of these guidelines in consultations such as implementing the HTN diagnostic
criteria in order to confirm the diagnosis.
According to some doctors, a lack of patient follow-up for second and third blood pressure
readings after two to four weeks made it difficult to confirm and diagnose HTN as
recommended by the guidelines. This concern was expressed in the following quotation:
In primary HTN you need a specific time period to label that as a primary. But patients they
don’t turn up usually in two to four weeks so how we can confirm HTN diagnosis as the
guidelines say? How we can actually implement these guidelines here in Pakistan, this is the
question. (Doctor 4)
Due to a lack of patient follow-up, doctors expressed uncertainty regarding the best way to
record and interpret the HTN diagnosis in practice. They suggested the need for a more
standardised approach to HTN diagnosis and felt that the guidelines needed to be more
relevant to general practice.
Some doctors highlighted that blood pressure recordings made by most patients were not
representative of accurate blood pressure measurements and as a result, they were not able
to document the HTN diagnosis and advice on changes to antihypertensive drugs in
accordance with the guidelines.
BP measurements are the core of HTN treatment guidelines and help us to document HTN
stage but if we have no readings or the false which are not the identical what we get in
consultation then how we can follow the next step of guidelines and treat patients properly.
(Doctor 19)
In explaining this further, they identified the greater reliance by patients on dispensary
services and quacks for blood pressure monitoring and expressed their frustration at the false
readings this often gave rise to. Many doctors believed this to be due to the inability of the
quacks and dispensaries to record blood pressure correctly and precisely and this was an
essential requirement for the management of HTN.
I will say everything is linked to BP monitoring. Either it is stage one HTN or that is stage two
HTN. When you have high BP on three different occasions and then you label the HTN. When
we know that monitoring is here then we can start antihypertensive to them. But most of the
patients go to the dispensers and ask them to monitor and then bring the wrong record to us.
Local dispensers and quacks have machines, but they don’t monitor blood pressure correctly.
(Doctor 23)

118
In exploring the methods doctors used to evaluate the status of patients with regard to HTN
in such circumstances, they reported being solely reliant on previous medical notes,
prescriptions and medical histories from patients. However, when evaluating the medical
notes in order to confirm HTN, a confirmed diagnosed of HTN was not always documented
on the most recent notes. Therefore, it was essential to explore the factors behind this
practice in order to identify the barriers to documenting a diagnosis of HTN and following the
recommended clinical guidelines.
When asked most of doctors seemed to be aware about the need to document the HTN
diagnosis and the stage at which it was at on the notes of their patients. However, a few
doctors stated that workload and the shortness of consultations had affected their adherence
to documenting the disease in accordance with the recommended clinical guidelines.
To write everything in such a shorter time is very difficult, I think. Sometimes, we forget when
we are in hurry. According to WHO [World Health Organization] criteria there should be 25
minutes consultation time for every patient but again patient load is too high and giving
proper time to every single patient is not possible. We are not practicing the way we should,
and mistakes happen like this. (Doctor 29)
It seemed that doctors were aware of the shortcomings of their practice at times but justified
that the pressure of work affected their approach towards treatment standards. Some
doctors stated that when treating patients sometimes more emphasis was placed on
prescribing antihypertensive drugs as opposed to discussing lifestyle changes with patients.
One explanation for this may lie in the preference of patients to take the drugs route first and
foremost, often believing this to be the only treatment available for HTN.
Every patient wants tablet, they think consultation useless if we don’t prescribe drugs. I
understand that lifestyle changes are equally important and often we should rely on these
solely, but we doctor admit this, some patients just want tablets and then we prescribe. They
are difficult to counsel really. (Doctor 22)
Such patients were described as ‘difficult’ and as a result doctors often reported prescribing
them nutritional supplements in order to satisfy their demands. Some doctors even reported
prescribing antihypertensive drugs without a clinical need because patients were so insistent
in their requests for it during consultations. Therefore, at times doctors were acting against
the recommended treatment standards and guidelines; their own judgements about patients
and failure to counsel them properly often influenced their decisions to deviate from the
treatment recommendations of the guidelines.
5.2 Treating Patients with HTN
When asked about their views of treating hypertensive patients they reported patient-related
factors that they perceived as barriers to successful HTN management. For example, the
failure of patients to accept their condition and remain in denial about their HTN diagnosis
were highlighted as important barriers influencing patient adherence to drugs and lifestyle
changes.

119
They don’t consider high blood pressure a serious disease because most of the time patient
has 180/120 mmHg blood pressure and he/she feel fine and does his/her daily activities.
They think we are all right and high blood pressure is nothing. So, when a patient thinks like
this how he/she can be compliant. This is the thing. (Doctor 18)
Many doctors reported that patients lacked an understanding that HTN was a chronic disease
and this only served to strengthen their denial with regard to treatment needs. Doctors
believed that due to this lack of awareness patients took antihypertensive drugs only for a
short time, did not comply with recommendations or advice and often failed to attend
scheduled check-up visits.
This is the fact that people don’t have awareness that once you are diagnosed with HTN you
must have taken the drugs lifelong and take the treatment throughout the life. They think
HTN is like a sessional flu, they take drugs for a day or two stopped and don’t come to us for
further check-ups. (Doctor 7)
Furthermore, the majority of doctors highlighted a lack of awareness amongst patients about
the benefits of controlling their HTN and there was a common concern that patients were not
aware of the consequences of uncontrolled HTN and as a result they would often go on to
develop complications. They considered that patients paid very little attention to adhering to
their plan of drugs and felt frustrated by the seeming lack of interest by patients in disease
management.
They even don’t bother what will happen if blood pressure will not control and they even
don’t know the consequences of high blood pressure and its complications. For example, a
patient with CVA (Cerebrovascular Accident) wants to go home after four days by own feet.
[Laughter] Due to lack of awareness they are not well informed about a proper HTN
treatment. (Doctor 4)
Some doctors mentioned that patients were reluctant to rely on lifestyle changes alone and
cited that their desire to enjoy life often overruled the need to regulate their lifestyle. They
considered it to be difficult to change the attitudes of such patients with regard to the efficacy
of an active lifestyle as opposed to antihypertensive drugs.
Patients think drugs are more effective and rely on this. To modify the lifestyle is difficult.
They think tablets will give instant cure and they expect after five minutes they will feel
better. They don’t get satisfied unless we write drugs because they have a typical mind-
setup. Who thinks to make efforts, everyone picks an easy option? (Doctor 21)
It was clear that the doctors felt frustrated by the non-adherence by their patients to drugs
plans and lifestyle changes, however, they also reported adherence to be a complex issue for
patients to adopt. To explain this further they highlighted economic barriers that may affect
the decisions of patients regarding HTN treatment, such as skipping doses and purchasing
alternatives to the drugs originally prescribed due to financial problems. One doctor felt that
financial difficulties and other priorities in the lives of patients often meant that the efforts
made by doctors to treat HTN were wasted to some extent:
Because the affordability issues here, not every patient can afford the treatment. Patients
who are poor, their tensions are something else. They think about money not about the

120
health. Sometimes, they buy the cheap medicine similar to the prescribed ones but relatively
less effective than the original so what will happen? Obviously if a patient cannot afford a
proper treatment due to economic issues then every effort, we make becomes zero. (Doctor
6)
There was a general perception amongst all the doctors that educated patients were better
able to follow their HTN treatment plans and take the advice provided in spite of financial
difficulties in their lives. The doctors believed that educated patients were better equipped
to understand the information provided and were aware of the consequences of
complications with their disease. By contrast, a few senior doctors believed the opposite and
that educated patients were more likely to adopt riskier behaviours than their non-educated
counterparts, such as eating junk food, not exercising and subjecting themselves to greater
levels of stress despite being fully aware of the consequences.
The educated patients mostly present with high incidence of HTN, unfortunately. They like
to eat junk food, stressed then go to restaurants and do hoteling more as compared to poor
people. Obviously, they have an office work such as contracts, tenders and office tensions
and job-related stress they have more blood pressure problem and very common in them as
compared to uneducated patients. They seem more stressed, forgetful, type [A] personality
due to work in competitive fields. So, we cannot say that educated people are more
compliant to treatment and advice given. (Doctor 14)
They further emphasised that educated hypertensive patients often smoked tobacco even
though they were aware of the health hazards associated with this habit. According to these
senior doctors’, patient behaviour was a key factor in treatment adherence and decision-
making as compared to educational status.
Educated patients tell us that they smoke and feel unable to stop this. Even if they have no
money or less still, they spend money on smoking, why? They should not smoke if education
is everything. The actual problem is their behaviour that develops from childhood and that’s
why patients are unable to change this or understand what is required for disease
management. Uncontrolled HTN is a consequence of it. (Doctor 9)
Seeking alternative treatment in the form of quacks and Hakeem medicine was perceived as
a reason associated with the choices of patients despite being aware of the consequences of
using such practices. Quack and Hakeem medicine was described as being fast-acting but
interfered with antihypertensive drugs and led to complications in patients which left doctors
with very few treatment options. A few doctors reported that quacks administered incorrect
intravenous medication such as steroids to treat hypertensive patients and put their lives at
risk.
Quacks are working because they are giving instant cure medicine. They give steroid
injections to hypertensive patients which further creates the problems. It is harmful for
patients to visit such healers, as they prescribe medication based on guesswork only. You
can’t start a drug without any true logic. (Doctor 24)
All the doctors interviewed felt frustrated by the actions of their patients in seeking
alternative treatments for their HTN. They stated that some hypertensive patients had a
strong faith only in Allah to heal their illness and treating such patients was considered to be

121
very difficult. Doctors stated that such patients would often attribute improvements in their
condition to prayer rather than drugs and believed that their faith and prayers would
eventually cure their disease. In addition to this, some doctors described how a few patients
asked them to pray for their health during consultations.
Religious patients ask us to pray for them and sometimes they say: oh, doctor you have
written a tablet for me, but nothing will happen unless Allah wants. I say Allah also says take
treatment when necessary. They also demand us to pray for them along the prescription
[Laughter] (Doctor 11)
Many doctors expressed concerns at the way in which the religious beliefs of patients often
led them to put their faith in spiritual healing for their illness. One doctor indicated that
patients often shared their spiritual treatment experience with her and assurances from a
spiritual healer had led patients to not adhere to their recommended treatment plan or seek
appropriate medical advice.
Patients tell us about their spiritual healing treatments. Like a patient told me that he went
to a saint and saint gave him a Tawiz (amulet) for dizziness and he told me that after wearing
that he did not feel dizziness. He continued saint treatment and also informed this to me.
(Doctor 3)
At the same time as highlighting the religious beliefs of patients the doctors emphasised that
faith in Allah had a strong role to play in the lives of Muslims, however, they disapproved of
the practice of patients consulting saints and spiritual healers for treatment. It appeared that
doctors had different explanations and expectations from patients when it came to manage
HTN and making choices about treatment.
5.3 Perceptions Regarding Lifestyle Management
This theme explores doctors’ understanding regarding exercise, dietary changes, salt intake,
smoking and alcohol consumption.
5.3.1 Understanding concerning involvement in exercise
A majority of doctors indicated that exercise is equally important to all, including obese and
non-obese hypertensive patients, for managing HTN, regardless of their body weight. They
believed exercise was more effective than antihypertensive drugs, highlighting medical
literature to this effect and shared their experiences with some patients. They pointed to the
need for exercise to progressively control high blood pressure. For instance, doctor 2
described how some patients who maintained exercise as part of their daily routine were
seen to have better control over their blood pressure than non-exercising patients:
First of all, the most, most important thing is exercise and then increase this gradually. It
does not matter either you are obese or not, exercise is must. It is for everyone. I have seen
many patients who do exercise daily and in better control of their blood pressure control as
compared to those who sits all day. (Doctor 2)

122
Doctors shared how patients indicated patients being aware of different types of exercise but
considered household activities such as washing, cutting vegetables and walking to a local
shop as an alternative to exercise. They highlighted a general lack of interest amongst patients
in exercise and that some patients expressed that it is difficult to ‘get going’, particularly in
the morning and evening. To improve the knowledge of patients some doctors highlighted
the need for education in schools to raise awareness about exercise and an active lifestyle.
The school and colleges should involve in this awareness. Children should be aware the
benefits of games and doing exercise from the childhood. So, when they grow-up, they will
have a clear understanding, I think. That is the way to create awareness and bring change
in behaviour. People will develop the habit of exercise and walk from childhood and that will
also grow with them and remain long lasting. (Doctor 13)
Doctors indicated that due to the busy nature of their lives, patients might think that they
may be undertaking adequate exercise already in form of work. They described how some
patients used their occupation and working hours as an excuse for not taking any exercise,
for example doctor 1 described a patient’s justification for not going for a walk after a long
day at work as follows:
I have a patient and yesterday when I asked him to do exercise, he used to tell me all his
routine [Laughter] he told me I come home at 5pm then two hours every day I spent with my
father and brothers to discuss current political issues then I eat dinner and go to bed. So how
can I find a time for exercise. [Laughter] So I think it is a matter of priority in patient life and
what is important to achieve. They have various excuses. (Doctor 1)
Many doctors viewed providing advice on exercise to hypertensive patients as part of their
role and reported promoting walking and cycling during consultations. The majority of doctors
claimed that whilst they had provided information during consultations, they felt patients
were not taking an interest in or responsibility for exercise, possibly due to an unwillingness
to change their behaviours. Only two doctors believed that they provided insufficient
information about exercise due to time restraints and thought this could potentially be a
barrier to patients achieving an active lifestyle.
Unfortunately, due to lack of time and patient burden we cannot do counselling in a proper
way. Even, we cannot tell everything in detail to our patients. Although, they need
motivation and more information how to adopt exercise in their life. (Doctor 24)
The insights from doctors’ accounts highlighted the wide range of issues in place to adopting
and maintaining exercise, and that some of these were related to personal and social aspects
of the lives of patients. Doctors often perceived these issues as ‘barriers’ to adopting and
maintaining a healthy lifestyle.
Socio-cultural norms
Many doctors indicated that it was not the norm within Pakistani culture to adopt exercise as
part of everyday life and therefore often not encouraged. They pointed that living in a society
where exercise is not viewed as a valuable practice contributes towards a lack patients’
involvement. The absence of cycling tracks, outdoor supports and absence of regular exercise
programs were pointed out by many doctors.

123
Most of the doctors believed that Pakistani society observes a lack of women outdoor
exercise. Doctors stated that the priorities of Pakistani women had shifted towards taking
care of their house and children and after marriage they had a sense of “it is no longer all
about me”. By contrast, some doctors felt that Pakistani men discourage outdoor exercise
for women due to social norms. For instance, they cited that in most Pakistani families it is
not acceptable to allow wives and daughters to run and walk along roads due to the
widespread prevalence of sexual harassment, such as whistling and catcalling. This was
thought to be one of the reasons that women preferred to stay indoors and attend to
domestic chores.
Women face social restraints like where they will go for a walk. They don’t have area to
walk, no permission from homes to go out, socially they are not allowed. In our society it’s
not acceptable to see a woman walking alone outside due to whistling and catcalls. All these
factors matter and make the situation difficult for them. (Doctor 19)
This is a fact because our culture is not so open. It’s not acceptable for a woman to go outside
and start running and jogging on the road. Walk is acceptable but not the exercise and these
are the hurdles a Pakistani female patient can face. (Doctor 26)
Doctors also cited women’s reluctance to join gyms due to difficult access, membership cost
and an overall lack of exercise culture. Some doctors highlighted the absence of female-only
gyms in most cities as an additional barrier for women.
Here, in Pakistan it’s uncommon for a woman to go outside and start doing exercise. There
should be gyms and health clubs from the government that should be less expensive or free
of cost so everyone can afford. (Doctor 18)
There are no female gyms and fitness centres from the government side. No health clubs are
available for women. The government should build free fitness centres for patients especially
for women. (Doctor 21)
Some doctors indicated that the socio-cultural restrictions made providing advice on exercise
to a female patient challenging and as a result they omitted such advice at times or modified
it according to the circumstances of the individual. A few doctors advised that instead of
joining a gym or running and jogging outside, women undertake regular and frequent
activities within their home setting.
Due to some socio-cultural restraints instead of asking them to go outside…. I ask my female
hypertensive patients that instead of short passage route take a longer passage when you
need to go somewhere and in their routine activities. Use stairs most of the time…. Try not
to sit all day and use stairs a lot and if you don’t have stairs at home then go to roof and
take rounds again and again, do walk around. (Doctor 19)
Concurrent health conditions
Some doctors indicated that co-existing health conditions often restricted them in providing
exercise-related advice to some patients. They pointed out that health conditions such as
joint pains restricted patients’ mobility therefore they considered such issues while
suggesting exercise to patients.

124
If he/she already have joint pains, then I cannot tell my patient about cycling and running.
How my patient will run or even walk briskly with joint pains. So, it happens that you become
conscious and aware that what kind of advice will suit patient and which one not. (Doctor 5)
Age-related factors in elderly hypertensive patients were commonly reported by doctors.
Many doctors felt that providing exercise advice is not valuable for older patients due to the
old age and as a result, they might get discomfort and disability. They reported that ageing
makes patients bones weak and as a result they often fall that can be prevented by less
physical activity.
Doctors expressed a fatalistic view describing exercise-related advice to be of no value for
older patients due to their increasing age, loss in muscle mass and decline in their ability to
balance. They frequently made reference that ageing inevitably involves a marked decline in
physical fitness. For instance, a doctor who had worked in a hospital for five years claimed
that exercise was not safe for anyone over a certain age:
For exercise, I mostly see the age of a patient. For example, if patient is very old because….
and about exercise sometimes he/she feels too odd to do exercise in old age. Because if
the patient is 60 or 65+ then how a patient can do exercise? Older patients cannot do
cycling and running they fell down and get hurt so it is not good to advise them exercise.
(Doctor 4)
Doctors displayed a tendency to neglect the notion of exercise as beneficial for older patients.
This is in stark contrast to research which suggests that the older population experiences a
greater decline in their physical functioning and an increase in disease through lack of exercise
(Ip et al., 2013).
5.3.2 Dietary management
A majority of doctors considered dietary management effective to control HTN and
considered it for all hypertensive patients. However, doctors indicated a number of issues
that were believed to influence patients’ adherence to healthy diet. These were (i) role of
traditional foods (ii) influence of family and friends and (iii) accessibility to junk food.
Role of traditional food
The majority of the doctors indicated that the use of traditional food high in saturated fats is
the major obstacle to an adjustment to a patient’s healthy diet plan. Doctors reported that
hypertensive patients should follow a diet that is lower in fat, spice and sugar content,
however, they felt there to be insufficient knowledge amongst patients with regard to eating
healthily. Eating traditional food cooked in oil and particularly paratha at breakfast was
believed by most doctors to be damaging the healthy eating plans of patients. Consumption
of fats in form of Desi ghee and developing a taste for this in childhood was perceived as a
near-unavoidable dietary habit amongst patients. They have one logic; that they eat one thing from the start and throughout the life and since
they born. Ghee and oil. Ghee and butter, they like the most and to leave these at once is
difficult for them. Most of them, they say it’s difficult and to leave this they have never
thought about this. (Doctor 19)
125
Our all traditional dishes like ‘Chicken Biryani’ (Biryani is normally made with basmati rice
and flavoured with cloves, cinnamon, cardamom, bay leaf, coriander, mint, ginger, garlic
and onions) and korma (a mildly spiced Indian curry dish of meat or fish marinated in yogurt
or curds) contain high cholesterol content. All this led towards unhealthy diet, but patients
cannot resist because of traditional foods. (Doctor 28)
The majority of the doctors indicated that patients held beliefs and misconceptions associated
with certain foodstuffs. One doctor, for instance described how his patients believed that a
healthy diet should consist of salad and vegetables and these were considered to be lacking
in flavour. One doctor indicated that the majority of patients were confused about the intake
of Desi ghee in their diet and assumed it to be a source of energy and high in calories. The
belief by patients that Desi ghee would supply them with high amounts of energy and strength
was illustrated by doctor 8 in the following quotation:
Here in Pakistan, people use ghee instead of cooking oil. Ghee contains cholesterol. They
think ghee is more beneficial for their health. They have in their minds that Desi ghee can
give us extra energy and make us strong. [Laughter]. (Doctor 8)
A senior doctor who had been working in a hospital for one year indicated that as opposed to
providing nutritional value, food had now become considered as a socially constructed status
symbol amongst some upper-class families and representative of their social standing. He
highlighted that serving a variety of expensive traditional dishes displayed a level of distinction,
wealth and power for individuals compared to that of other people in society. Moreover, this
custom was linked to the protocol and honour given to guests in providing a diversity of food
items, as doctor 14 highlighted below:
Nowadays it become our culture, if you have 10 dishes in an upper-class family dinner to
represent this as a status symbol. Plus, those 10 dishes would be definitely rich in oil. Food
has become a status symbol and presence of oily chicken dishes represents that you belong
to a respected and a wealthy family. People think if someone has invited me on dinner and
cooked 5-6 different variety of dishes then he/she will think an honour has been given. If a
person will not cook 5-6 dishes and invite someone the guest will think ‘Oh he/she has just
tried to get rid of me.’ People don’t think these are healthy or not, they count number. This
is the thing. (Doctor 14)
Some doctors reported that convincing patients to reduce their intake of ghee or change their
dietary patterns was challenging due to what they believed were misconceptions held by
patients. This view was echoed by a doctor who described how some patients would often
argue against making healthy food choices and would not make the recommended changes
in order to manage their disease.
I don’t think they understand what we told them about ghee or food. These patients are very
foody, if you tell them even 100 times don’t eat this, it is not good for you, but they will not
listen make arguments like ‘Look doctor you have stopped us eating too.’ They eat the food
they like, that’s it. (Doctor 18)
A lack of self-control
A few doctors stated that people in Pakistan are very fond of eating and enjoy great variety
in their food with family and friends. They described how at family reunions eating a meal

126
was a regular event and that it was often hard for patients to resist the temptation of fatty
foods at such gatherings.
Pakistani people are fond of eating and food contains a lot of spices, salt and oil. Due to company
people eat more and that is the cause of obesity and other diseases and patients don’t accept
dietary recommended suggested by their doctor and they eat whatever they want. (Doctor 29)
Patients in Pakistan are very fond of eating. They always want to eat oily and spicy food when they
eat together. I think they don’t find this useful that healthy food can be an option to their treatment.
They just want to eat what comes in front. (Doctor 27)
However, a majority of doctors recognised this a lack of self-control and/or an
unwillingness to stick to a healthy diet plan. They reported patients’ lack of interest in
making dietary changes and pointed that in family gatherings and presence of friends’
patients’ lack of self-control become prominent due to the temptation of tasty food.
Doctors pointed that patients believe taking the tablet to control HTN is enough rather
follow dietary restrictions. By taking tablets they had a reason to support their non-
adherence to dietary changes.
Accessibility to junk food
Doctors indicated that the consumption of fast food was very prevalent in major cities in
Pakistan due to the variety of fast food restaurants and outlets such as McDonald’s and KFC
offering pleasant surroundings and a varied menu. They believed that eating fast food was a
common practice for everyone in major cities of Pakistan. Some felt that the proliferation of
vendors and hawkers in major and minor cities selling low-cost unhealthy street food was
exacerbating the problem. They highlighted the fact that low quality fast food was readily
available and provided people with a sense of independence, joy and a wealth of opportunity.
Eating junk food is increasing day by day. In homes, who have money, they prefer and run to
eat from outside rather to cook inside the house. Because everywhere is fast food hawkers
and restaurants. The poor people eat fast food from hawkers and rich from McDonald and
KFC. Everyone is eating this unhealthy food. I think eating fast food give people an
independence that they have choices in life, and they feel happy (Doctor 27)
A few doctors also indicated experiencing difficulty in avoiding fast food due to the time it
took to prepare and cook traditional meals at home. The convenience of ready meals
combined with a busy schedule was one of the reasons given by doctors for opting for fast
food. One junior doctor reported feeling tired and unable to cook and eat a healthy meal
after a long shift at work and empathised with patients who felt the same way:
We doctor even don’t have time to make salads, we go towards readymade, not time to eat
fresh food every day. Even sometimes, we eat three days old food that is present in the
fridge. What comes front of us we do eat? We as doctors even cannot follow all this even,
we have greater knowledge and know everything. Then what we can say about patients who
even have less knowledge. This is the thing. (Doctor 21)
A few junior doctors described that due to their busy schedules they had adopted unhealthy
eating patterns such as skipping breakfast and snacking on small unhealthy meals throughout

127
their shifts. The availability and accessibility of energy-dense foods such as fries, pizza and
fizzy drinks and an absence of salad, fruit and vegetables at hospital canteens also played a
part in the eating choices of doctors. It was noted that fast food could cause heart problems
and unmanageable HTN, but many doctors viewed the easily accessible fast food outlets
selling low-quality fatty foods and sugary drinks as a contributing factor.
Who never wants to eat healthy but when it comes to choices, we see what is easily
available? Here in hospital canteen we have fast food and drinks because they get profit on
that. I myself don’t eat healthy all the times, I do eat fast food and drink Pepsi due to a lack
of time and easy access. Sometimes, I skip my breakfast and same others do. So, you can’t
stick to healthy food all the times, I know it’s not good but this is a fact, unfortunately.
(Doctor 3)
The majority of doctors felt that mass media could play an important role in the promotion
of healthy eating amongst the population and highlighted the need for local food authorities
to improve the availability of healthy food in schools and hospital canteens. This section has
illustrated the factors that doctors believed inform the food choices of patients. Moreover,
doctors have also revealed that their own eating behaviours can at times be found wanting
and that they sometimes hold erroneous views or stereotypical perceptions with regard to
their patients which may need to be addressed. The following category will examine the
views of doctors with regard to salt intake.
5.3.3 Salt consumption
Doctors indicated that hypertensive patients should cut down their salt intake, however, they
reported cultural practice and taste preferences as barriers to follow a less salt diet amongst
patients. The use of salt is firmly established within Pakistani cuisine hence the majority of
doctors believed it to be harmful to hypertensive patients following a healthy diet regime.
Doctors believed that the use of salt in tea instead of sugar was possibly a cultural practice in
certain Pakistani areas; being more prevalent in some specific villages, geographical areas and
to the north of Pakistan. For instance, a senior doctor described:
Once I was travelling and I used to stay at one place. It was a local hotel and you can say
poor people can afford this easily. So, I ordered the tea, when I took one sip, it was full of
salt. I asked from the hotel manager what this is. He said, sir here only bus drivers and truck
drivers come, and they used to take salty tea only. (Doctor 27)
Many doctors indicated that salt is used to flavour traditional foods in Pakistan and therefore
management of salt intake could prove challenging for patients. A junior doctor reflected that
a diet high in salt was prevalent amongst some of his hypertensive family members and this
was due to particular taste preferences. One doctor described how he had counselled his
mother about reducing her salt consumption and advised her to avoid salty tea. Initially she
was ambivalent but after some encouragement and explaining the risks associated with high
salt consumption, he was able to modify his mother’s behaviour:

128
In Kashmir, it’s a tradition to have a salt in tea instead of sugar. I myself a doctor, and my
mother used to take salty tea in front of me, what can I say more… What she does? She takes
her antihypertensive medicine with salty tea. If this is happening in a doctor’s house, then
you can understand what is happening elsewhere. I counselled and encourage her again and
again. Many times, even daily and now finally she doesn’t add salt. I counselled her not to
take this and the risks associated and finally she gave up salty tea. [Laughter] (Doctor 14)
Some doctors emphasised that patients with greater knowledge about the benefits of a
reduction in salt intake were more likely to be able to control their blood pressure. However,
a majority of the doctors were in opposition to this viewpoint and believed that knowledge
did little or nothing in changing the behaviour of patients since the practice was firmly
embedded within custom and preferences of taste. Only one doctor argued that an inability
to change behaviours may be linked to a lack of awareness and inadequate provision of
information during consultations.
In this public setup, we have too much patients then we cannot do counselling as it
required but we try to do our best as much as we can. Unfortunately, due to lack of time
and patient burden we cannot do in a proper way. We cannot tell them how much salt is
needed in diet and how much they need to cut off and also, we cannot tell in detail about
high salt foods. (Doctor 21)
Some doctors were familiar with how much patients understood about the dangers of high
salt intake and their current practices in that regard, however, a few confessed to being
unable to convey sufficient advice and counselling to patients during consultations due to a
lack of time and a heavy workload.
5.3.4 Smoking cessation
Doctors largely believed that smoking was harmful for all humans, whether hypertensive or
not. Despite being harmful to health, a majority of doctors mentioned that smoking cessation
was challenging for hypertensive patients due to some barriers. They highlighted a lack of
motivation, enjoyment and concealing their habit as main barriers behind patients taking up
the habit.
A lack of motivation by patients to quit smoking was criticised by many junior and senior
doctors and they believed that many patients did not wish to quit as they felt no detrimental
effects on their health, enjoyed smoking and made false promises that they would eventually
quit at some point in the future. Junior doctors believed that the common reasons for
smoking amongst patients were pleasure, relief from boredom and enjoying seeing others
smoke. Doctors indicated that patients often concealed their habit from them as well as from
other family members due to the stigma surrounding smoking and fear of embarrassment in
public.
I think they believe that this kind of information is very personal and confidential that’s why
they hesitate to tell us or maybe they feel shy and not respect worthy if they tell us about
this. Because no one like the smokers and smokers are socially stigmatised. (Doctor 5)

129
About smoking, no patient tells us or disclose us himself/herself and smoking is the universal
truth nowadays. Every second person is the smoker here except the few people. But patients
don’t tell us and even their families due to shame. (Doctor 2)
Interestingly many doctors displayed a lack of interest in asking questions from smokers and
providing them with support and counselling in order to help them quit. By way of explanation
they stated that smoking was difficult to quit and that patients were reluctant to discuss or
change their attitudes towards smoking cessation. Doctors indicated that the doctor-patient
relationship may be compromised if the patient was perceived to be uninterested in
discussing smoking cessation during a consultation. Some doctors admitted that they had on
occasions brought consultations to an end more rapidly if they felt the patient lacked interest
or appeared uncomfortable when the topic of conversation turned to their smoking habit.
Many doctors stated that lack of time was the main reason why they did not provide more
support and motivation to help patients quit smoking. A few doctors felt there was a need for
a separate service that paid specific attention to assisting hypertensive patients engage with
smoking cessation.
Smoking is a habit that is very difficult to leave. In one session, we cannot change who is
smoking from the past 20 years. It’s like their habit and due to nicotine, they become addicts.
We do ask them to quit and I especially emphasis on this, but we cannot achieve this in just
few short consultations. (Doctor 19)
Due to lack of time we do ask about their smoking status, but we cannot counsel them
briefly. This needs long discussions with patients and sessions to counsel them. I think there
should be a separate service for such patients and that should be paid so we can engage
doctors with these patients. (Doctor 23)
Some doctors also highlighted the need for a mass media campaign to raise awareness
amongst people about the risks surrounding smoking. Doctors pointed factors such as a lack
of a patients’ interest and time restraint for counselling in order to change their smoking
habit. The next section examines the views of doctors with regard to alcohol consumption.
5.3.5 Alcohol consumption
Excessive alcohol consumption was reported as damaging for HTN control amongst all
doctors. Almost all the doctors pointed to the role of religion in patient choice to drink. They
believed that patients with strong religious commitments did not consume alcohol of any
form. Doctors’ believed that in a Muslim society like Pakistan, drinking alcohol is seen as an
unacceptable practice and a symbol of evil.
However, the majority of doctors conceded that patients with weak religious commitments
did partake in the consumption of alcohol for enjoyment’s sake, but this was kept secret from
their families and doctors. Doctors stated that breaking Islamic laws bring shame and stigma
for patients within the society and that is the main reason they hide this habit. Many doctors
felt that the taboos surrounding drinking alcohol in Muslim countries would not allow patients
to openly acknowledge their habit. They described how such patients felt ashamed and

130
concerned that they would be met with family disapproval and therefore tended to avoid
such discussions.
No one discloses anything about alcohol, we have to ask them again and again. We try that
they tell us the truth, but patient often does these kinds of things by hiding from the family.
People drink but if they drink, they should not tell their doctors. Who admits that I’m a
drinker too? (Doctor 18)
If they are alcoholic, they won’t admit this and don’t let us know because drinking is not a
good practice in our culture and religion. (Doctor 23)
A few doctors indicated that despite the strict laws some hypertensive patients were still able
to illegally purchase alcohol of various brands provided they had sufficient purchasing power.
They also stated that patients who could not afford good quality alcohol often ended up
drinking toxic homemade liquor, often with fatal consequences.
The biggest problem of our society is that nothing is present at front but behind everything
exists and people do everything behind the closed doors. No one discloses anything about
alcohol, we have to ask again and again. We try that they tell us the truth, but some patients
often do these kinds of things and hide it from the family. (Doctor 2)
The majority of doctors stressed that time constraints prevented them from counselling patients
adequately about the hazards associated with alcohol and the consequences it could have on their
HTN. One senior doctor stated:
We don’t have so much time to follow up these patients or to counsel them. First of all, they
don’t share with us and if they do sometimes, we ask them to stop this habit as it is
dangerous for your health. We cannot counsel them briefly. (Doctor 11)
5.4 Informing Patients about HTN
A majority of the doctors reported providing information to patients about the disease and
the treatment of HTN during consultations and most stated that providing detailed
information was part of their role. By contrast, some perceived their role with regard to the
provision of information as being confined to treatment with drugs alone and referred to
other sources of information from nutritionists or the mass media.
A doctor can’t do everything, there should be other people like a nutritionist and sources like
media or the newspaper. I think in this way, things will get better, and patients will be more
informed. There should be a multi-disciplinary approach to deal with this problem, I think.
(Doctor 19)
Some doctors reported that due to insufficient time, provision of detailed information about
the treatment of HTN was often ignored or delayed. Similarly, information about specific
lifestyle changes tailored to the specific needs of the patient was not always discussed as
discussed previously (5.3). Doctors also believed that patients should take responsibility for
their own health and ask for more information if required.

131
We accept that we have a lack of time, but at the same time I think a patient should be
responsible for his/her health. They should ask us questions not silly ones [Laughter] and we
try to give them information despite the lack of time. (Doctor 12)
Though this assumption cannot under-estimate patients’ desire and need for more
information from their doctors. This is due to the reason that some patients’ felt hesitant to
ask questions and reported being shy by nature. It therefore seemed that doctors tried to
achieve satisfaction in the wake of their demanding job to neutralise the negative impacts of
less information. Owing to the limited time and the need to run to schedule for other patients
waiting, doctors stated they often lacked time to initiate a discussion about patient specific
needs and maintain a good doctor-patient relationship. A lack of time and work load resulted
in less interaction with patients which further created a sense of conflict for many patients.
Patient wants time and we don’t have enough. When there is a long queue waiting outside
how you can provide the information in a comprehensive way. It is very difficult in public
hospitals. (Doctor 23)
Due to lack of time, we cannot provide them proper time that they require and in this way
patient and doctor communication is affecting. (Doctor 2)
Only a few doctors acknowledged that lack of information regarding HTN was one of the
reasons of patients’ non-adherence to an optimal treatment plan. The next theme explores
the doctor’s perceptions in relation to communication issues in clinical interactions with
hypertensive patients.
5.6 Communication Issues in Clinical Interactions
In this study only, a few doctors reported having a satisfactory relationship with their
hypertensive patients. Most doctors had different expectations of clinical visits and they
recognised that there were certain issues that often had an impact on their interaction with
patients and the provision of information. Due to a shortage of time and the pressures of
work they were often left with less time for interaction with patients and could only counsel
them very briefly. Furthermore, providing treatment to large numbers of patients in a limited
timespan exposed doctors to high levels of stress and often resulted in a lack of tolerance that
raised communication problems.
Doctors are normal human being as well. How can a doctor manage the patient when doctor
is under pressure due to patients load and sometime administration put so much pressure
on doctors? Due to lack of time, we cannot provide them proper time that they require and
in this way patient and doctor relationship affects. (Doctor 28)
Some patients were described as ‘difficult’ and as a result doctors often reported prescribing
them nutritional supplements in order to satisfy their demands. Some doctors even reported
prescribing antihypertensive drugs without a clinical need because patients were so insistent
in their requests for it during consultations. In contrast, some junior doctors indicated that
they had experienced difficulties in explaining basic medical concepts to patients in Urdu;
patients would frequently request simple information to be provided to them in Urdu and
many doctors viewed their constant demands as a source of frustration. Continually being

132
asked to repeat the information caused doctors to make assumptions about their patients
and they described such patients as ‘illiterate’ and ‘fussy’ and deemed them to be over-
demanding.
Some patients become so fussy. They ask same questions every time and, on every visit,
again and again. Mainly, because they are illiterate. Doctor is also a human not a machine.
In that way, a doctor becomes rude and harsh. Then they complain doctor is rude. Why
patients ask same questions again and again, though they are aware of a long queue
outside? They are just…! (Angry) (Doctor 22)
Some patients ask same question over and over unless we become upset. I don’t know why
they do this. Maybe they are attention seekers. (Doctor 11)
Only two doctors felt empathy for their patients, stating that the individual life circumstances
of their hypertensive patients may cause them to experience emotional and psychological
problems such as stress and depression as a result of the chronic nature of their HTN.
We as doctors can do things in terms of disease management, but everything depends on
good doctor and patient relationship and that will not develop unless you don’t know the
principles of doctor-patient communication. If anywhere during the encounter; you feel
that other than the disease patient has some psychological issues coming up and you see
tears in patient eyes so give him/her a clue that I’m feeling and understanding that you’re
in trouble and you are stressed out. (Doctor 6)
A few doctors indicated that better communication was needed to ensure that patients
overcame any concerns about drugs and lifestyle changes, and this would in turn improve the
quality of their HTN management. To improve the service, they suggested extending the
outpatient clinic timings and the number of doctors in public hospitals to overcome
communication problems.
5.7 Summary
Findings presented in this chapter clearly showed that doctors had their own understandings
about HTN and its treatment. An inadequate awareness of the HTN guidelines amongst junior
doctors was evident due to deficiencies in their training and often fraught relationships with
senior doctors. Though generally they expected patients to take responsibility for the
management of HTN and discussed their patients lack of HTN awareness. This chapter has
also highlighted doctors’ understandings on drug adherence and provided insight into what
doctors believe about patients’ practices in terms of adopting lifestyle changes. Doctors
seemed aware of the socio-cultural influences, patients’ choices regarding seeking alternate
therapies and limited information provision in consultations. They acknowledged that
information to patients about HTN treatment and particularly lifestyle changes were often
curtailed due to the time constraints and their heavy workload. Consequently, this justified
the communication difficulties in consultations and as a result poor HTN management in
urban hospitals of Pakistan.

133
Chapter 6: Discussion
This chapter is comprised of four main sections. The first section 6.1 will summarize and
reflect upon key findings from the study described in the previous two chapters. Implications
of the study findings for practice, Pakistan’s policymakers and future research will be
discussed in section 6.2. Section, 6.3 will describe the strengths and limitations of the study
and finally, the chapter will discuss the contributions of the findings to current knowledge and
draw conclusions.
The objectives of the study were:
• To examine what is already known about patients’ and doctors’ understandings of
HTN and its treatment in urban areas of Pakistan.
• To elicit hypertensive patients’ perceptions, attitudes and beliefs regarding HTN and
its medical and lifestyle management in urban areas of Pakistan.
• To elicit doctors’ perceptions, attitudes and beliefs regarding HTN and its medical and
lifestyle management in urban areas of Pakistan.
The first objective of the study was addressed by conducting a systematic review that
summarised existing evidence and found a lack of HTN awareness regarding disease and poor
HTN control in patients and suboptimal treatment practices amongst doctors were identified.
Furthermore, the review showed a dearth of qualitative studies about hypertensive patients’
understanding of disease and no qualitative studies were found regarding doctors’ beliefs
about HTN management in Pakistan. Chapters four and five addressed the second and third
study objectives.
The findings revealed that patients understood their diagnosis, cause of illness and the
importance of the medicines differently from the way doctors did. Patients had insufficient
information on antihypertensive drugs and lifestyle changes, and all this influenced where
patients sought care, their adherence to treatment and management. A detailed discussion
of the study findings is presented below in relation to the conceptual framework that is based
on health beliefs as discussed in chapter two (2.11).
6.1 Discussion of Findings
Participants’ health beliefs were found to influence their understanding of illness, attitudes
and management of HTN (Shaw, 2002; Helman, 2007). Specifically, the findings of the current
study revealed how participants often drew on a range of frames of reference regarding
disease management in their everyday decision making. Patients’ beliefs underpinned how
they made sense of and experienced HTN in their daily lives that affected their interpretation
and perceptions regarding disease treatment and management. Likewise, doctors’ beliefs
rationalised their attitudes and approach towards HTN management and the provision of
treatment. Both patients and doctors possessed various beliefs and expertise that shaped
their thinking, attitudes and decisions regarding HTN management. Doctors were more
familiar with the medical definition of HTN, guidelines, prognosis, treatment options (mainly
medications) and outcome probabilities, whereas patients drew on a range of lay beliefs

134
regarding the HTN meanings, symptoms, causes and treatment. The following sections will
discuss patients’ and doctors’ findings separately and then a comparison is provided to discuss
what further understanding the findings from the current study may add.
6.1.1 Patients’ beliefs
Patients’ beliefs were complex, deep-rooted and informed by lay understanding gleaned from
their socio-cultural environment (local norms, social relations, religion), individual factors
(e.g. income, co-morbidities) and to a lesser extent interaction with doctors. These beliefs
influenced patients’ health-seeking behaviour, adherence to treatment and coping strategies.
The findings offer insights about the personal understanding of HTN and revealed that most
patients constructed the meaning of HTN in their everyday life based on symptoms, causes
and consequences that they experienced.
According to patients’ narratives, they were not constantly alert to their condition as they
performed their activities of daily living. These findings are consistent with a study conducted
in India amongst the Bondos tribe, which found that people defined illness as being unable to
work, feeling weak and being non-functional and not being able to carry out everyday tasks
(Dixit et al., 2008). A lack of symptoms at the initial stage of HTN made it difficult for patients
in this study to adopt an early and appropriate health-seeking behaviour. This finding is
comparable to those identified in other studies (Ypinazar & Margolis, 2006; Shamsi et al.,
2017; Ashoorkhani et al., 2018) where patients perceived illness to be associated with explicit
physical symptoms.
As the disease progressed, patients’ experienced daily symptoms of HTN and based on
severity of those, they explained that they could tell when their blood pressure was high.
Despite clinical literature that describes HTN as asymptomatic, the study findings are
consistent with other qualitative studies around the world where patients described
experiencing physical symptoms of HTN (Chow et al., 2013; Legido-Quigley et al., 2015;
Rahman et al., 2015; Kusuma, 2009; Shima et al., 2014; Shamsi et al., 2017). Patients
experiencing physical symptoms believed that their blood pressure was high, and they relied
on the intensity of symptoms to prompt them to take medication or see a doctor. A general
misconception that disease is always an episodic illness associated with physical symptoms is
a belief that discounts HTN as a chronic disease. Having symptoms did not equate to having
an illness, however, clearly patients understanding about the nature of HTN here reveals how
they managed it, which can explain their non-adherence towards medications.
Consistent with Boutain (2001), findings revealed that many patients in the current study
believed stress, tension and worries caused their elevated blood pressure and therefore they
reported avoiding stressful situations. One explanation, as suggested by Blumhagen (1980)
could be that lay people interpret ‘hypertension’ as excessive tenseness and refer to tension,
stress and worry as a cause of their high blood pressure; this was a commonly expressed belief
in the current study. Arguably these findings confirm that patients’ attitudes are influenced
by their beliefs and such beliefs impacted how they understand and experience disease
causes. Patients endorsed stress-producing factors (e.g. family problems, overwork,
emotional state) as the predominant cause of their HTN. This finding is consistent with studies

135
that explored HTN beliefs in several other populations around the world (Wilson et al., 2002;
Lukoschek, 2003; Legido-Quigley et al., 2015; Rahman et al., 2015). Patients indicated that
they avoid stressful situations in order to manage their HTN and there is increasing evidence
suggesting that psychosocial stress contributes in the development of HTN (Vrijkotte et al.,
2000; Cohen et al., 2007; Spruill, 2010). However, such stress avoiding techniques alone are
not sufficient to control HTN (Whelton et al., 2002). Patients need to be aware of the
multifaceted approach to the management of HTN and doctors must address this (WHO,
2009; Chow et al., 2013; Jung & Ihm, 2019).
Patients believed that taking antihypertensive drugs was necessary to control HTN, but they
frequently admitted intentional and non-intentional drug non-adherence. A review of the
literature on drug adherence has shown that non-adherence is a problem across all patient
groups and for all diseases (Martin et al., 2005; Jimmy & Jose, 2011), although this is
particularly common amongst people who experience unpleasant side-effects from drugs
(Saleem et al., 2012; Nayeri et al., 2015; Rahmawati & Bajorek, 2016). Patients who believe
and experience side-effects from hypertensive drugs cannot appreciate the physiological
benefits of continuing therapy (Enlund et al., 1991; Benson & Britten, 2002). Nichter (1996)
has identified that in Asian countries the concerns patients have about drugs may be derived
from the popular belief that Western drugs are powerful but inherently dangerous in nature.
If patients believe side-effects are an inevitable by-product of taking drugs they may not
present promptly when they feel unwell or volunteer information about side-effects in
consultations (Benson & Britten, 2002; Mostafavi et al., 2016). Findings from the current study
support this notion, where the patients even considered minor side effects as potentially
significant. This could mean patients were ready to quit the medicines at the first sign of a
side-effect. Moreover, patients in this study were not informed about the drug’s use and
coping with medicine adverse reactions. A study in North India reported that the provision of
appropriate medicines-related information, including information pertaining to side effects is
crucial to ensuring continuation of drug therapy.
A further influence on people’s health beliefs and attitudes is the impact of the socio-cultural
context in which they grow up and live (Kleinman, 1988; Lucire; 2003; White, 2005; Aylward,
2006). The meanings attached to health and illness experience are rooted in a socio-cultural
environment that provides a normative standard for decisions, ways of behaving, as well as
making treatment choices. Findings from the current study revealed that patients’ beliefs
were often contextual and dominated by the culture and norms of Pakistani society. For
instance, the socio-cultural aspects of eating, social interactions and following advice from
other lay people, had a major influence on patients’ HTN management.
Many patients in the study adopted limited changes to their diet following diagnosis of HTN
due to the key roles of commensality and the role that traditional food had played in their
lives since childhood. The etiquette of preparing traditional food with ghee and spices made
the removal of ‘unhealthy’ ingredients difficult. A central concern for these patients was the
continued enjoyment of their lives which came from eating delicious traditional food and
maintaining a social life. Certain social practices such as eating together and one dish for all
were seen to be norms that limited patients’ ability to make adaptations to controlling their

136
diet and this is consistent with other studies conducted in South Asian populations (Lawton
et al., 2008; Choudhury et al., 2009; Lucas et al., 2013). Probably, the presence of others
increases the amount consumed and thus extends the meal duration.
Similarly, women prioritised family over their individual health needs, reported a lack of an
exercise culture and as a result, they were less likely to adopt and integrate exercise into their
daily routine. This finding is in accordance with studies conducted in Saudi Arabia and Qatar,
which highlighted that women perceived exercise as beneficial but were restricted in their
adoption of outdoor exercise due to family obligations and lack of facilities (Donnelly et al.,
2011; Samara et al., 2015). Similar experiences have been noted in studies conducted with
British Pakistani women that highlighted how diabetic women were restricted in their
outdoor exercise due to family obligations and the absence of women-only facilities (Lawton
et al., 2006; Penn et al., 2014).
A qualitative study conducted amongst South Asians living in the UK stressed that
understanding external motivators and social context of the lives of patients is crucial for
developing successful exercise interventions (Jepson et al., 2012) and recommended strictly
women-only spaces, facilities and opportunities. Others argue that in order to effectively deal
with these issues, any interventions must acknowledge and incorporate patients’ lay
understandings they have acquired from their lived experiences with the illness (Kirmayer et
al., 2004; White, 2005; Marshall et al., 2012). For example, in this study obese hypertensive
patients believed exercise to be purely a strategy for weight loss; and controlling their HTN
was not the aim. Moreover, patients stopped taking exercise when they did not feel it was
making any change to their body weight.
The social unacceptability of tobacco use amongst women in Pakistan is also anchored in
socio-cultural meanings about being a ‘female smoker’. Women avoided smoking due to the
social norm and this finding is in line with a qualitative study conducted in the British Asian
population which observed social factors such as stigma associated with women smoking
(Bush et al., 2003). Due to the social taboos associated with women smoking, it may be
possible that women under-reported their smoking status in this study. In contrast to females,
smoking is a socially acceptable norm for men living in Pakistan (Shaheen et al., 2018) where
it represents a strong sense of social bonding and is seen as a normal part of ‘being male’
(Irfan et al., 2014). Male patients who smoked emphasised the influence of peers and believed
that family members and friends who smoked played an important role in the initiation of
their smoking and its continuation. These findings concur with the results of other studies
that reported smoking was common amongst people when they were in the company of
other smokers and would therefore spend time smoking with them (Rozi et al., 2005; Kelishadi
et al., 2007).
Likewise, patients’ religious beliefs played a crucial role in terms of how to manage, cope,
seek help and cure HTN. For instance, none of the patients were aware of the relationship
between high alcohol intake and HTN, however, the dominant Islamic belief that the
consumption of alcohol in any of its forms is forbidden, influences their attitude and decisions
regarding drinking. Findings revealed that patients also drew upon fatalistic beliefs when
coping with HTN, believing in destiny, or an act of fate, using this to explain what was

137
happening to them. The notion of a condition or disease being an act of fate, God or related
to chance or supernatural forces have been reported by other studies conducted in Asian
countries such as Malaysia and Iran (Swami et al., 2009; Shahrbabaki et al., 2017). In this
study, some patients believed that their disease was an unavoidable and uncontrollable
event.
Islamic teaching encourages Muslims to seek treatment when they fall sick and forbids acts
that will expedite suffering and ultimately death (Al-Shahri & Al-Khenaizan, 2005; Attum et
al., 2019). Farooqi et al. (2006) points out that such beliefs are associated with a lack of
understanding of Islamic principles and low literacy rates. Likewise, having the belief that a
religious healer can help cure disease compelled patients to the services of spiritual healers
claiming to provide treatment in the name of faith. In low income countries such as Pakistan,
it is common for saints, Hakeems and quacks to misuse religion and provide fake remedies
for personal financial gain (Qureshi & Shaikh, 2006; Sumbal, 2014). Khan et al. (1996) and
Farooqi (2006) have emphasised that traditional healers and other non-formal providers that
are less expensive and easily accessible play an important role in influencing the minds of
patients. Additionally, most traditional healers in Pakistan treat their patients in their religio‐
cultural context charging less than seeing a medical doctor (Saeed et al., 2000; Shaikh &
Hatcher, 2005; Farooqi, 2006). This appeared to contribute to why patients increasingly
choose to go to traditional healers rather than seeking timely treatment from qualified
doctors. In this study, the results illustrate that spiritual healers attracted some patients by
offering them amulets made from the Holy book and quacks linked their treatments with
religious teachings. With regard to Islam, as well as providing guidelines for leading a healthy
life, it encourages seeking orthodox medical care for alleviating sickness (Qureshi & Shaikh,
2006). However, traditional healers and quacks are involved in practices that contradict
Islamic teachings in Pakistan (Hunte & Sultana, 1992; Shaikh & Hatcher, 2005; Qidwai, 2009).
This clearly shows that traditional healers tend to emphasise building communication that is
consistent with cultural traditions and the religious belief of the patients. This has important
implications for the training of doctors in their approach to care and how to communicate
with patients.
Other than religion, findings of the current study identified that some individual factors such
as economic difficulties, availability of medication, a busy routine, comorbidities, a lack of
motivation also influenced patients’ disease management. For instance, cost of medication
as a reason for intentional non-adherence (Hugtenburg et al., 2013) was a noteworthy factor
amongst most of the patients in the current study which had a direct impact on their decision
to adhere to drug therapy or not. This finding corroborates the observed association between
poor drug adherence and lack of funds for the purchase of medications reported by Bilal et
al. (2015). People are not covered by medical insurance in the Pakistani healthcare system,
however, they receive medications and public health services at a very low cost. Poor
availability of prescription drugs at the public hospital’s pharmacy was a system related
problem affecting treatment. Another study conducted in Pakistan also found that
inadequate access to essential medicines in public hospitals leads to poor drug adherence in
patients (Zaidi et al., 2013) and therefore this could be a significant issue that needs
addressing. Similarly, a busy schedule and forgetfulness were other some of the non-

138
intentional non-adherence reasons presented by the patients for not adhering to medications
which are consistent with the experiences of participants in previous research (Almas et al.,
2006; Hashmi et al., 2007; Jimmy & Jose, 2011; Shima et al., 2014; Nayeri et al., 2015).
Whilst some individual factors shaped patients’ disease management, the findings of current
study exposed how a lack of information from doctors during a clinical interaction played a
crucial role in patients’ decisions about HTN management. Only a few patients in the study
reported that they were informed of changes adjunct to the management of HTN such as
regular exercise, reducing salt intake and eating a diet low in fat; a finding similar to some
other studies conducted in various countries (Gascón et al., 2004; Tan et al., 2017; Alefan et
al., 2019; Legido-Quigley et al., 2019). A number of patients reported not having received
adequate information and support from doctors and this put them at a significant
disadvantage in developing the understanding necessary to manage their condition.
Moreover, patients in the study were fearful of asking their doctors treatment-related
questions. Similar results have been obtained in a recent mixed-method study conducted in
Pakistan which found that due to the technical expertise of doctors, patients often believed
they were inferior and unable to raise their concerns (Jalil et al., 2017). Piette et al. (2004) in
their study highlighted that patients may not discuss issues with doctors when they think their
concerns are not important enough, feel embarrassment due to an inadequate understanding
of disease or are, deterred by the lack of time in the clinical consultation. As a result, patients
can feel disempowered and may be unable to achieve their health goals.
Patients’ in the current study refrained from sharing information with doctors as they felt
intimidated by the perceived attitude of doctors who were often overburdened and in a
hurry. Patients’ who used home remedies as well as alternative treatments were reluctant to
reveal this information to doctors due to the lack of doctor's interest and disapproval of such
practices. Perceived negative actions or responses by the doctor to patients could make them
even more reluctant to disclose their beliefs about using alternative treatments (Chan &
Wong, 2004; Stokols & Milden, 2004; Wahner-Roedler et al., 2006; Kelak et al., 2018). This
communication problem augments the risk of developing adverse drug reactions and
complications in patients by using allopathic and alternative therapies in combination.
Likewise, the sense of feeling blamed caused patients to conceal their smoking habit from
doctors and they no longer felt comfortable in discussions related to smoking. It is not
surprising, therefore, that patients felt upset when they perceived that they were being
judged and even blamed for developing their disease. Likewise, in a study by Chapple et al.
(2004) patients felt ashamed because of the association held between their disease and
smoking. People can become highly dependent on tobacco due to nicotine addiction and
complete cessation of smoking may be difficult which some doctors fail to recognise (Fowler,
2000). However, there is a dilemma for doctors in this study who take it as their responsibility
to deter people from smoking and to encourage them to stop, but without being seen to be
blaming their patients (Chapple et al., 2004; Stead et al., 2008; Meijer et al., 2018). The
following section will discuss the study findings related to doctors’ understandings of HTN and
how this influenced HTN management.
6.1.2 Doctors’ beliefs

139
Like patients, doctors exhibited their own understandings of HTN management, and their
beliefs were informed by bio-medical or scientific knowledge, socio-cultural context, work
experience, stereotype assumptions and encounters with patients. Doctors in this study
mentioned HTN as a chronic, often symptom-free condition which could be moderated by
biological and behavioural factors and requiring life-long treatment, as supported by bio-
medical evidence. This finding reflects a ‘scientific attitude’ in which the meaning of events is
provided through abstract rules derived by the scientific evidence (Arnold, 1989).
Likewise, the majority of doctors believed that reducing HTN complications such as stroke and
heart attack were not very important to their patients. They generally adopted a narrow
traditional biomedical belief reliant on medication for the management of HTN and concluded
that patient non-adherence to drugs was a deliberate and an unacceptable practice. It is not
realistic to expect patients to comply with treatment when a low level of disease-related
information from doctors exists. Arguably, if a doctor believes that drug non-adherence is the
main cause of increased disease burden and an unacceptable practice, he/she would avoid
providing advice on drug adherence or pay less consideration to other treatment options.
Doctors should acknowledge the challenges that patients might find with taking medication
regularly with very little information (Tuckett, 1985; Britten et al., 2000; Fischer et al., 2010).
Doctors need to set aside their own beliefs as this may help facilitate patient-doctor
discussion about treatment adherence (Stevenson & Scambler et al., 2005; Dyer, 2008;
Bezreh et al., 2012).
Socio-cultural context informs doctors’ understanding of HTN as well as the lay public with
studies indicating that beliefs and attitudes within a particular culture can be broadly similar
irrespective of occupation and role (Koeing, 2012; Richards et al., 2014; Haddad et al., 2016).
Doctors in the study pointed to the influence of social norms, cultural values and individual
factors which they believed to be barriers (traditional food, a lack of exercise culture in the
country, busy routine of patients, access to junk food and individual problems such as
economic difficulties). Doctors were aware of the cultural restrictions on women in Pakistan,
therefore, female patients were often not advised by doctors to undertake any outdoor
activities. In a conservative society such as Pakistan, where women are often expected to
cover their heads, wear ankle-length dresses and sometimes cover their faces, the notion of
running on roads and swimming was perceived by doctors and patients as daunting. Arguably,
the lack of an exercise culture and social limitations for women with regard to sporting and
outdoor activities presents a particular challenge for doctors like to prescribe exercise.
Likewise, doctors conceptualised falls as inevitable and advised older patients not to exercise
due to the risk of injury. In Pakistani culture, it is a common belief that older people should
rest often and slow down due to a decline in body functions (Cassidy, 2018). This finding
supports that due to a shared cultural/national background, doctors and patients from the
same country can have similar beliefs than doctors from different countries. However,
evidence supports that the beneficial effects of exercise are observed in older people with
non-communicable chronic health conditions such as HTN, diabetes, cardiovascular disease
and some cancers (Warburton et al., 2006; Blair et al., 2012; Taylor, 2014). Clearly, education
has a role to play here in addressing some of the challenges older patients faced with regard

140
to the uptake of exercise and may explain the lack of awareness amongst doctors about HTN
treatment guidelines and be aware of their own bias in clinical decision-making.
Due to sharing a similar religious background, doctors seemed aware that patients gain
strength from their religious faith in cases of illness and other major life events. Although the
fatalistic attitudes of patients such as seeking help from spiritual healers, quacks and, Hakeem
were considered as inappropriate. Doctors were unable to appreciate that patients who are
spiritual often utilise their religious beliefs in coping with illness and this can affect decision-
making and the treatment choices they make. This also highlights that doctors approached
patients through the filter of their own beliefs that resulted in stereotyping patients. Doctors
need to be fully aware about the choice’s patients make and why (Eisenberg, 1997; Haynes
et al., 2000; Helman, 2007; Wilson et al., 2007; Street et al., 2007; Street & Haidet, 2011).
Similarly, due to the use of alternative treatments patients were often perceived to be
‘difficult’. However, the use of alternative treatments amongst patients is common to all
cultures (Lee et al., 2004; Subramanian & Midha, 2016) and patient explanations of disease
management can be technically complex (Kleinman & Benson, 2006).
Doctors often highlighted the pressure of work in public hospitals and conflicts that arose
from encounters with patients. They acknowledged that information provided to patients in
the consultations was limited due to work pressure and being able to spend more time with
patients would be desirable in order to support them. Competing expectations, work pressure
and reported interpersonal conflict in consultations provided an insight into showing the real-
world working situation of doctors in Pakistani public hospitals. Scarcity of other resources
(nutritionists/dietitians, mass media messages) was also a source of frustration for some
doctors, who believed that more of their patients could benefit from a greater provision in
this area.
Owing to the limited time and the pressure to run to schedule for patients waiting, junior
doctors at times did not diagnose HTN according to the guidelines, prescribed unneeded
nutritional supplements and antihypertensive drugs without a clinical need in order to satisfy
patients. Prescribing non-essential drugs to patients is a serious concern (Basaran & Akici,
2012) and the choice of drug for a patient is one of the most important clinical decisions in
evidence-based medical practice (Masic et al., 2008; Chow et al., 2018; Lehane et al., 2019).
Moreover, taking antihypertensive drugs without a clinical need in undiagnosed patients
cause adverse consequences including making them hypertensive, drug resistance and other
side-effects (Wall et al., 2014). This finding is similar to the results of other studies which
reported that a substantial number of doctors agreed that most irrational prescriptions were
patient-driven (Bazigha et al., 2006; Ojo et al., 2014). However, doctors need to be fully aware
that irrational antihypertensive drug prescription contributes to the increased burden of HTN
and has severe health consequences in patients (Liu & Wang, 2008; Jarari et al., 2016).
This attitude shows that at times doctors were acting against the recommended treatment
guidelines and failure to counsel patients properly often influenced their decisions to deviate
from the standards required for HTN management in hospitals. However, it was also evident
that junior doctors were not given the opportunity to improve their existing knowledge due
to high workload, time restraints and poor working relationships with senior doctors. Whilst

141
doctors were open about the existence of work pressure, particularly inadequate time and a
desire not to run late, they were not able to recognise pragmatic decision-making in the
workplace. Evidence shows that a productive and healthy work environment is essential for
doctors to both achieve the goals of the organisation, patient care and derive personal
satisfaction from their work (Hyman & Pavlik, 2000; Van der Zwet et al., 2011; Patel et al.,
2018).
In contrast, a poor work environment contributes to medical errors, inaccurate decision-
making, stress and burn-out, absenteeism and high levels of staff turnover, which, in turn,
compromises the quality of care (Green & Ruff, 2005; Cook et al., 2013; Salyers et al., 2017;
West et al., 2018). Moreover, if doctors are unable to update their existing understanding,
they cannot construct an appropriate diagnosis or act upon new knowledge and translate
accurate information into their practice (Ely et al., 2002; Davis & Harrison, 2007). No doubt,
limited consultation time and patient burden was a constant source of stress for doctors.
However, Howie et al. (1991) contend that doctors who believed and committed to offer
longer consultation times that enable identification and treatment of more patient problems
result in greater satisfaction levels amongst patients. As a result of rushed consultations,
doctors in the current study experienced a lack of patient trust which affected their
communication and ultimately the doctor-patient relationship. These findings are consistent
with several studies conducted in Pakistan on patient satisfaction and medical interactions
related to chronic disease management (Saeed & Ibrahim, 2005; Khattak et al., 2012; Jalil et
al., 2017).
It is evident from the findings that doctors’ beliefs were influenced by their bio-medical
knowledge, socio-cultural context, working situations and daily encounters with patients. It is
clear that doctors’ own understanding shaped their practice, clinical decision-making and how
they managed HTN in Pakistani urban hospitals of Pakistan. The following section will provide
a comparison between patients’ and doctors’ beliefs to reveal similarities and differences
about HTN management across participants.
6.1.3 A comparison between participants’ beliefs of HTN management
Differences between doctors’ and patients’ beliefs were noted in this study regarding
understanding HTN and its management for HTN. High blood pressure was often defined by
patients as a varied personal experience rather than by a specific sphygmomanometer
reading, was equated with stress, characterised by physical symptoms, treated with
numerous home or alternative remedies and underestimated as a major cause of death
amongst patients. Patients in this study emphasised difficulties in the social domain and the
impact of HTN on their lives, while doctors perceived HTN primarily as a pathophysiological
problem with impact on the patients’ physical well-being. Patients evaluated HTN control in
terms of how they felt about symptoms while doctors evaluated blood pressure readings.
Many hypertensive patients mentioned a variety of physical symptoms of HTN as the disease
progressed and did not experience it as a silent chronic disease which is in sharp contrast to
what doctors believed. Likewise, the explanations of HTN differed widely from that of doctors
as increasing age, a positive family history and poor treatment adherence in patients were
142
considered prominent causes of HTN amongst doctors. A possible explanation for this
difference is that doctors have been trained according to the bio-medical model and hence
their disease explanations often exclude the social, cultural and psychological dimensions of
ill health (Nettleton, 2006). Eisenberg (1977) points out that for doctors, disease is an
abnormality in the structure and function of the body’s organs, and they try to fix it. In
contrast, for patients an illness is an individual personal experience which is embedded in
their everyday life.
With regards to adherence, doctors seemed frustrated about patients’ medicine non-
adherence and assumed that patients paid little attention to their treatment plan which is
significantly different compared to patients’ beliefs. These findings are consistent with other
studies suggesting that doctors’ beliefs may vary and are generally in opposition to what
patients think, regarding taking medicine according to a treatment plan (Gascón et al., 2004;
Richard & Haidet, 2011; Rahman et al., 2015). From the perspective of biomedicine, non-
adherence may seem irrational and incorrect. However, according to patients’, non-
adherence can be rational due to possible side-effects of the given treatment or considering
that HTN requires symptomatic treatment like other diseases. This highlights disparities in
doctors’ awareness of their patients’ beliefs, attitudes and treatment decisions. Eliciting
patients’ beliefs regarding prescribed treatment and related concerns is essential to support
informed choice and optimal adherence to appropriately prescribed treatment (Ross et al.,
2004; Shiyanbola et al., 2012; Horne et al., 2013).
Findings from the present study also revealed an overlap between beliefs of doctors and
patients in some areas about HTN management. For instance, alike patients, doctors also
reported how certain socio-cultural norms, concurrent health conditions, individual factors,
and religious beliefs influenced patient’s treatment adherence and approach to manage HTN.
However, patients were often criticised for showing an overall lack of interest in adopting
lifestyle changes that contradicted the aspects patients highlighted. Evidence supports that
doctors need to understand the reasons behind treatment non-adherence and raise
questions with the patient in a problem-solving and non-judgmental manner (Ley, 1988; Jin
et al., 2008; Kleinsinger, 2010) which is opposite to what is revealed in the current study.
In addition, doctors reported operating a paternalistic consulting style, deciding on
consultation time and the amount of information appropriate for patients without involving
them in the decision-making process. Patients also found consultations short, not helpful and
desired information regarding lifestyle changes from doctors. Lack of information is an
important reason for non-adherence to lifestyle changes amongst patients (Hamer, 2010;
Alefan et al., 2019). Evidence shows that patients’ information needs differ from doctors’
perception of those needs and when left unresolved, this may lead to lower adherence rates
(Broström et al., 2009; Stavropoulou, 2012). In contrast, sufficient information provided by
doctors on prescribed medicine and proposed lifestyle changes helps in adherence to drugs
and lifestyle recommendations (Gascón et al., 2004; Martin et al., 2005; Sharma & Agrawal,
2017). According to Hussain et al. (2015) the majority of hypertensive patients reported
doctors as being their primary source of information regarding advice about a healthy lifestyle
in Pakistan.

143
Previous research shows that doctors need to focus on delivering information in simple
language (Clarke, 2010; Ha & Longnecker, 2010; Eaton et al., 2015; Warde et al., 2018) which
informs patients about how to modify their lifestyle in terms of changes in exercise, diet, salt
and smoking, and ideally tailoring this to the personal situation and beliefs of patients
(Walseth et al., 2011; Noordman et al., 2013). Patients who feel that their doctor provides
them sufficient information, actively encourage them to be involved in adopting lifestyle
changes tend to be more motivated to adhere to these changes (Kerse et al., 2004; Bennet et
al., 2010; Vahdat et al., 2014; Elbur, 2015; Sharma & Agrawal, 2017). However, a lack of time
and work load can result in less information exchange with patients which further create a
sense of conflict for patients as acknowledged many doctors in the current study.
Consciously or unconsciously, doctors used social constructs (e.g. time) with patients to
manage HTN without taking account of their own biases. Doctors’ were unable to consider
how their own beliefs and attitudes may affect clinical practice and interactions with patients.
Due to time pressure and communication issues exchange of knowledge between patients
and doctors was not evident and consequently, patients could not construct a rationale (new
knowledge) for HTN treatment adherence. Whilst, patients’ health-seeking practices and
adherence to treatment were highly dependent on their lay beliefs. It is without doubt that
due to limited interaction and severe time constraints, doctors may make recommendations
that are inconsistent with beliefs of their patients and the realities in their lives (Heritage &
Maynard, 2006; Jin et al., 2008; Claramita et al., 2010; Turner, 2013; Currie et al., 2015).
Consequently, discordant understandings may result in conflict, poor adherence to medical
recommendations and patient’s dissatisfaction that is obvious in the current study.
It is evident from the findings that the beliefs held by both patients and doctors regarding
HTN management were multiple and diverse. Doctors’ beliefs were greatly influenced by their
bio-medical knowledge, working situations and daily encounters with patients. In general,
doctors seemed unaware that patients acquire a unique ‘expertise’ by experiencing a chronic
illness and most of the patients’ choices and decisions about HTN management can clash with
their beliefs and becomes a major barrier to effective disease management. Inevitably, a
shared understanding of HTN management by patient and doctor was not obvious in this
study, which advocates that there is plenty of room for improving doctor-patient
relationships. If the doctor is to improve a patient’s condition, the elicitation of the patient’s
beliefs should, therefore, occur at every stage of the clinical process (Tukett, 1985; Kleinman
& Benson, 2006; Ha & Longnecker, 2010; Basset, 2011; Rahman et al., 2015).
6.2 Doctor-Patient Relationships
By gaining a deeper understanding of patient beliefs and practices, doctors will be better able
to establish trust-based relationships with their patients and can provide a better service. A
way to improve service delivery for patients lies in creating a willingness amongst doctors to
engage in social, cultural and environmental aspects of illness that extend beyond the
biomedical model of disease (Thomas et al., 2014). It is vital to consider that a person may
present to a doctor with a variety of explanations for the illness experienced (Bolam et al.,

144
2003; Street & Haidet, 2011). Patient beliefs maybe different than biomedical explanation but
these are usually consistent and rationale in their own terms (Donovan, 1999).
As evident in this study, patients drew on their health beliefs to make treatment decisions.
Hence, to manage the disease effectively, a doctor should understand patient beliefs and
there is need for negotiation between patient and doctor ‘clinical realities’ or ‘social
construction of illness’ (Hardey, 1999; Conard & Barker, 2010; Ha & Longnecker, 2010;
Bassett, 2011; Mik-Meyer & Obling, 2012). It is evident that the clinician basic relational
attitudes, for instance, being friendly, being non-judgmental and taking interest in the
patients’ illness by eliciting their beliefs have a very positive influence on patients’ health
(Jagosh et al., 2011; King & Hoppe, 2013; Raja et al., 2015; Ranjan et al., 2015; Kornhaber et
al., 2016; Saqib et al., 2018). Several studies point out that doctors acknowledging patients’
beliefs can improve therapeutic outcomes, patient satisfaction and patient quality of life
(Rocco et al., 2011; Chipidza et al., 2015; Vahdat et al., 2014; Zanini et al., 2014; Kornhaber et
al., 2016; Kee et al., 2018).
Evidence supports that the fundamental component of patient-centred care is the doctor’s
interaction with patients and understanding of patients’ beliefs and concerns (Epstein &
Street, 2011; Mirzaei et al., 2013; Weiner et al., 2013; Kennedy et al., 2017). It requires a
strong doctor-patient relationship that is built through empathy and involves careful listening
and responding to patients' preferences and providing clear and simple information regarding
care (Roger et al., 2005; Halpern, 2003; Adams et al., 2012; Marcum, 2013). Empathy is known
to be an essential component in promoting patients’ empowerment following a clinical
consultation and patients expect compassion from their doctors (Kim et al., 2004; Mercer et
al., 2008; Hardy, 2017). This situates the doctor in a unique place of obligation and
opportunity to act not only as diagnostician but also as a confident patient educator and
listener.
In this respect, patients put emphasis on doctors’ empathetic qualities, in being interested,
listening and devoting time (Gascón et al., 2004; Anfossi & Numico, 2014; Mazzi et al., 2015;
Derksen et al., 2016; Hardy, 2017). Hence, instead of simply asking patients, ‘where does it
hurt’? -the doctor should focus on eliciting the patient’s answers to why, when, how and what
next (Gregory & Dowd, 2004). In the therapeutic alliance22, questions are the tools of the
therapist in a therapeutic conversation and they are to be guided and informed by the views
of the clients so that the conversation is geared toward the maximum production of new
knowledge (Anderson & Goolishian, 1992; Nørgaard et al., 2012; Kornhaber et al., 2016).
However, without eliciting patients’ beliefs about their illness, clinicians may make
recommendations that are incompatible with the expectations of patients and the realities in
their lives. This implies that a new perspective on healthcare in Pakistan, one which goes
beyond the biomedical side of medicine is needed and that doctors must become more active
in their interaction with the patients and be able to examine the patient's understanding of
the world (Gascón et al., 2004; Ranjan et al., 2015).
22 refers to the relationship between a healthcare professional and a client. It is an approach in which healthcare professional and a client connect and engage with each other (Muran & Baber, 2011).
145
Since the patient is at the heart of learning, a constructivist perspective suggests that it is
essential that doctors make the effort to try to understand the patient beliefs (Rashid &
Jaggar, 1996; Dennick, 2016). It involves finding out the background knowledge of the patient
(Sensky, 1996; Thomas et al., 2014), communicating with them (Silverman et al., 2005; Ali et
al., 2006; Kee et al., 2018) and then educating them in a way that they can understand (Savin-
Baden & Major, 2004). According to Dennick. (2016) that it is an engagement with an
individual that is analogue to the learner-centred approach and hence is stated as patient-
centred. However, it can be argued that physical barriers in health service availability such as
time constraints in public hospitals are an obstacle to addressing patients’ individual needs.
In putting doctors’ accounts into perspective within their work environment, the current
study’s findings cannot overlook the work load as a factor contributing to their practice. The
pressure to see next patient within a short period of time undoubtedly influenced doctors’
ability to create an active learning environment.
A study conducted in Britain found that increasing appointment times from 5 min per patient
to 7.5 min per patient was associated with identifying 50% more psychological problems
(Wagenaar et al., 2016). In countries like Pakistan, Bangladesh and China, an individual doctor
may undertake over 90 consultations per day with a substantial amount of time taken up
providing repeat prescriptions (Irving et al., 2017). In such circumstance, nurses’ importance
cannot be ruled out as they are generally good at communicating and explaining things to
patients (Balzer-Riley, 2004; Kourkouta & Papathanasiou, 2014). In developed countries such
as the United Kingdom, nurses not only play a vital role in providing clinical care in hospitals
but take part in a variety of health promotion activities, deliver counselling services, treat
patients and prescribe medications; tasks previously undertaken only by doctors. However,
in Pakistan the main responsibilities of the nurse are limited to administering medicine and
providing medicines-related information to inpatients in the public hospitals (Saqib et al.,
2018).
A randomised controlled trial conducted in Pakistan found that patient satisfaction with
doctors who were trained in scheduling follow-up visits, providing satisfactory consultation
sessions with an explanation of non-pharmacological interventions was 50% higher than in
those consulting untrained doctors (Abbasi et al., 2002). Similarly, Anderson and colleagues
in one hospital in Sweden trained doctors treating diabetic patients to capture the essence of
empathy in effective communication and to incorporate it into their day-to-day practice
(Anderson et al., 2000). Their evaluation demonstrated that as a result of a two-day
workshop, doctors were more understanding to the needs of patients, less judgemental and
provided detailed information regarding treatment. Hence, the Ministry of Health in Pakistan
needs to invest in coaching doctors throughout their medical training in how to conduct a
more ‘equal conversation’ with patients in order to improve service quality. In this way,
patients will be able to share their concerns, beliefs and socio-cultural practices with ease and
doctors will feel more confident in treating patients and obtain more validation from them
which will also lead to greater job satisfaction.
The association of findings between clinical workload, doctors’ inability to follow treatment
guidelines, ad hoc decision-making, and patient dissatisfaction, indicates that doctors were

146
less productive at handling hypertensive patients’ needs. However, there is much more than
the lack of time and work environment that hinders effective communication. Evidence
supports that patient satisfaction, commitment to treatment and perceived outcome of care
are greater when the doctor and patient achieve a shared understanding on issues such as
the patient’s role in decision-making, the meaning of information and the treatment plan
(Michie et al., 2003; Kleinman & Benson 2006; Epstein & Peters, 2009; Ha and Longnecker,
2010; Rathert et al., 2013; Kennedy et al., 2017). This dissertation takes forward the argument
that patients’ understandings of disease need to be heeded in routine clinical interaction and
addressing issues through a robust transferable healthcare delivery system is necessary if
hypertensive patients are to be effectively treated in public hospitals of Pakistan.
6.3 Recommendations
Following the insights of this study recommendations for practice, policy and future research
are detailed below:
6.3.1 For doctors
Key finding
Doctors made assumptions about patients due to lack of understanding of the importance of
patients’ beliefs which affected the effectiveness of the consultation in terms of treatment
outcomes.
• Medical education should incorporate learning from social science research.
• Promote patient-centred empathic consultations with hypertensive patients through
organising workshops or courses for qualified doctors to help them improve and
update their skills on a regular basis as a part of postgraduate training.
Address workload-related challenges that hinder doctor-patient relationships.
• Hospital administration, (mainly the Medical Superintendent) should consider how to
further foster a supportive work atmosphere for doctors. This could include the
establishment of supportive networks (e.g. clinical supervision, workgroups, peer
study support group, supervisor support).
• Junior doctors showed poor awareness of HTN guidelines, therefore, PMDC needs to
consider actions to address this. This might include regularly assessing junior doctors’
knowledge through workplace-based assessments and annual reviews. To improve
and update the knowledge of junior doctors’, the availability of a continual
professional development (CPD) programme is required. This might include regularly
assessing junior doctors’ knowledge through workplace-based assessments and
annual reviews.
• The government needs to pay particular attention to developing a strategy to organise
workforce planning in public hospitals.

147
6.3.2 For patients
Key finding
All patients wanted more information on HTN, its treatment and specifically more advice on
lifestyle changes.
• Provide patient information in an accessible format focused on its management,
specifically about the chronic nature of HTN, causes, benefits of controlling high blood
pressure, the association of lifestyle changes with HTN and risks involved in using
alternate therapies.
• Specific supportive training could be provided to other individuals (i.e. nurses, LHWs,
nutritionists) in order that they are able to transfer information to patients in a more
appropriate setting, either individually or by group sessions. Nurses can be trained by
to provide follow-up information about HTN, lifestyle changes and treatment
adherence to hypertensive patients soon after their consultation. Pamphlets (in Urdu),
clear messages and ‘signposting’ services can be provided as part of their everyday
contact with the public.
Recommendations specific to each lifestyle change
The study findings demonstrate the importance of tailoring lifestyle changes to patients’
socio-cultural context and individual needs.
Key finding
Hypertensive patients, particularly women, exhibited a lower level of engagement in adopting
an exercise routine.
• Local authorities and gyms should be encouraged by the health ministry to offer
discounted memberships for women in order to help alleviate their anxieties
associated with issues of high cost.
• Women would benefit from the provision and promotion of facilities such as women-
only gyms/sessions with same sex instructors. Address the known problems related to
women’s safety to create opportunities for women to exercise in a familiar setting
such as public parks and green areas.
• Work in partnership with religious centres and mosques to enhance understanding
about the benefits of exercise. Draw on role models from religious and political
backgrounds (at a local and national level) to provide inspiration and motivation to
the general public.
Key finding
The socio-cultural aspects of eating (e.g. traditional foods, family expectations) impacted
hypertensive patients’ choices of food.
• Information needs to be conveyed that healthy food options do not have to be bland
and tasteless. Patients should be informed that traditional dishes can be cooked in
healthy ways and eaten alongside high-fibre foodstuffs such as fruit and vegetables.

148
• Due to the shared consumption of food within families, it is recommended that
education and advice should be available to the whole family and not just the
hypertensive patient.
• Promote dietary changes which work with the types of foods Pakistani people are
already eating. In particular, this highlights the need for strategies to reduce the
consumption of fat whilst still focusing on traditional cooking practices and more
specifically, through the promotion of lower fat but authentic versions of recipes
which are commonly consumed dishes (Kassam-Khamis et al., 2000).
Key finding
Patients consumed a high salt diet and were unaware of the recommended amount of salt
per day.
• Conduct a national public education campaign and implement salt reduction
strategies in purchased food in conjunction with broader policies and programmes, as
has been conducted in Indonesia, Malaysia, Thailand and Finland (Cobb et al., 2012;
Batcagan-Abueg et al., 2013). The campaign should focus on sensitising the general
public to the addition of salt to homemade dishes and its effects, teaching them to
preserve natural flavours with better cooking methods and without the addition of
salt.
• Pamphlets and the Short Message Service (SMS) in local language (Urdu) on the
benefits of reducing salt consumption to help with controlling blood pressure could
be initiated by the Ministry of health as suggested by researchers in Iran (Golshahi et
al. 2015).
Key finding
The role of family and friends was seen as an important medium through which rules and
values associated with smoking were shaped.
• This finding provides a foundation for testing existing tobacco control intervention and
campaign ideas in Pakistan. Currently the role of family and friends is not given special
mention in the national policies on smoking cessation in Pakistan. Given that the
family plays an important role in the initiation and discontinuing smoking, tobacco use
prevention and cessation interventions should be focus on targeting the family role.
• It is imperative that the government and authorities should establish an appropriate
anti-smoking campaign and harness the power of positive peer influences to reduce
smoking.
• Religious leaders should be involved in disseminating information about the risks
associated with smoking such as lung cancer, stroke and high blood pressure.
• Effective tobacco control requires an anti-smoking policy backed by well-monitored
and strictly enforced national legislation in Pakistan. In addition, doctors need to place
greater emphasis on the availability of nicotine replacement therapy provided to
smokers by the government to handle addition and motivate patients to quit
successfully.

149
6.3.3 Recommendations for future research
The systematic review conducted has identified that there are a very few qualitative studies
carried out in Pakistan to understand the ‘emic’ understandings of patients and doctors
regarding HTN management. Therefore, further qualitative research is recommended
including observational studies to examine associations between doctors’ attitudes, their
consultation styles and referral decisions.
Studies are required to explore other areas such as cultural competence, consistency and
patient-centred healthcare approaches with doctors. An ethnographic study that explores
information exchange and communication in consultations through observations and in-
depth interviews with patients and doctors would provide a better understanding of what
actually occurs during the consultation, including what and how information is delivered
regarding HTN treatment in Pakistan. Some of the findings that arose from the study indicated
that HTN treatment guidelines were not followed by junior doctors in Pakistan. Therefore, for
future studies, it is vital to explore further contextual factors that affect the training of junior
doctors and the barriers to following HTN guidelines across various healthcare settings and
how these influence the management of hypertensive patients in Pakistan. In particular, there
is a pressing need to investigate whether findings obtained from this study are resonate in
the rural areas of Pakistan, where healthcare services are more dispersed.
In this study, none of the doctors mentioned the need for patients to undertake blood
pressure monitoring as a part of their HTN management and did not suggest it as an important
strategy. Pakistan does not have any national or regional blood pressure screening
programmes available (Ahmad & Jafar, 2005), therefore, HTN usually remains undiagnosed
unless patients visit a doctor for a routine examination and to have their blood pressure
checked. Future studies should look at the advantages and barriers to routine blood pressure
monitoring as currently people are diagnosed after seeking help for symptoms or consultation
for other health issues.
6.4 Study Strengths and Limitations
This is one of few qualitative studies in Pakistan that provides an in-depth insight into the
beliefs of patients as well as doctors with regard to HTN and, its management. A large amount
of data was collected during the study and the research design was strengthened due to my
language skills and sharing a similar professional background with doctors. My ability to speak
Urdu and Punjabi fluently helped me to establish a good rapport with the study participants.
Additionally, acknowledging my position as a Pakistani qualified medic, doctors demonstrated
an interest in the study and felt comfortable sharing their experiences in interviews.
In common with any research study, there were several limitations that should also be
recognised. The participants were recruited from two cities in Pakistan, therefore the sample
was not representative of all hypertensive patients and doctors in Pakistan. Nevertheless, as
the hospitals were typically representative of hospitals across Pakistan, patients were
recruited with a range of demographic characteristics, so the findings should be of wider use.
It is also important to be mindful of the limitations which may arise from using in-depth

150
interviews. As noted by Lawton (2003) interviews may invite a particular kind of account in
which people may be more concerned with presenting themselves in a socially favourable
light than conveying their beliefs and behaviours in literal and direct ways. Therefore,
ethnographic approaches using observation could be employed in future work to find if there
are any discrepancies between what participants say and what they actually do, in particular,
observation of consultations.
The study findings may be relevant to other Asian populations. Although when applying the
findings from this study to other populations, it is important to note that patients in this study
were from urban areas and included hypertensive patients who were already diagnosed with
HTN and on prescribed treatment. As a Pakistani qualified medic, I had my own set of beliefs
about HTN treatment, causes and management. In order to counteract any potential bias, I
constantly reflected on my thinking about the experiences of study participants’ and the
beliefs they held.
6.5 Conclusion
The present study is one of the few qualitative studies to offer insights into hypertensive
patients’ beliefs, one of the first studies to explore doctors’ beliefs about HTN and the first
study to provide a comparison between patients’ and doctors’ beliefs regarding HTN
management in Pakistan. This study complements and adds to the existing knowledge on
patients’ and doctors’ understanding regarding management of HTN and provides a detailed
picture of how beliefs shape attitudes and decision making. Additionally, the study highlights
important differences between doctors’ and patients’ beliefs about HTN management that
show the urgent need for educating and training doctors in patient-centred care.
It is evident that raising awareness about HTN amongst the Pakistan population is essential;
however, doctors must first recognise a patient's worldview to better understand the
meanings behind patients’ health decisions. This should focus on what matters most to a
patient (their personal goals) and the support they necessitate to manage their condition.
Therefore, the interactions between patients and doctors needs to be considered as one of
the main building blocks towards establishing an effective care plan for HTN. If the interaction
is effective and meaningful it could positively affect the outcome through improved HTN
control, fewer complications and better well-being. Doctors’ understanding of the difficulties
patients face and how they navigate the illness in their everyday life is a basis for being able
to facilitate an improved healthcare experience. To conclude, successful HTN management
will rely on doctor willingness to engage patients’ in every step of disease journey to form a
doctor-patient team in order to achieve the agreed goals.

151
References Abbasi, F., Brown, B. W., Jr., Lamendola, C., McLaughlin, T., Reaven, G. M. (2002). Relationship
between obesity, insulin resistance, and coronary heart disease risk. Journal of the American College
of Cardiology, 40(5), 937-943. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/12225719/
Abdullah, A., Othman, S. (2011). The influence of self-owned home blood pressure monitoring
(HBPM) on primary care patients with hypertension: A qualitative study. BMC family practice, 12(1),
143. doi: 10.1186/1471-2296-12-143
Abel, E. L., Kruger, M. L., Friedl, J. (1998). How do physicians define "light," "moderate," and "heavy"
drinking? Alcoholism Clinical and Experimental Research, 22(5), 979-984. doi: 10.1111/j.1530-
0277.1998.tb03692.x
Abtahi, F., Kianpour, Z., Zibaeenezhad, M. J., Naghshzan, A., Heydari, S. T., … Zamirian, M. (2011).
Correlation between cigarette smoking and blood pressure and pulse pressure among teachers
residing in Shiraz, Southern Iran. International Cardiovascular Research Journal, 5(3), 97-102.
Retrieved from
http://applications.emro.who.int/imemrf/Iran_Cardiovasc_Res_J/Iran_Cardiovasc_Res_J_2011_5_3
_97_102.pdf
Accad, M., Fred, H. L. (2010). On redefining hypertension. Texas Heart Institute Journal, 37(4), 439-
441. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2929868/
Adams, R. J. (2010). Improving health outcomes with better patient understanding and education.
Risk Management and Healthcare Policy, 3, 61-72. doi: 10.2147/RMHP.S7500
Adams, K., Cimino, J. E. W., Arnold, R. M., Anderson, W. G. (2012). Why should I talk about emotion?
communication patterns associated with physician discussion of patient expressions of negative
emotion in hospital admission encounters. Patient Education and Counselling, 89(1), 44-50.
doi:10.1016/j.pec.2012.04.005
Addo, J., Smeeth, L., Leon, D. A. (2009). Hypertensive target organ damage in Ghanaian civil servants
with hypertension. PloS One, 4(8), doi: 10.1371/journal.pone.0006672
Adib, S. M. (2004). From the biomedical model to the Islamic alternative: A brief overview of medical
practices in the contemporary Arab world. Social Sciences and Medicine (1982), 58(4), 697-702. doi:
10.1016/S0277-9536(03)00221-1
Afsar, H. A., Qureshia, A. F., Younusb, M., Gulb, A., Mahmood, A. (2003). Factors affecting
unsuccessful referral by the Lady Health Workers in Karachi, Pakistan. Journal of Pakistan Medical
Association, 53(11), 521-528. Retrieved from http://jpma.org.pk/full_article_text.php?article_id=299
Agyemang, C., de-Graft Aikins, A. (2014). Culture, Ethnicity and Chronic Conditions: A Global
Synthesis. London: Routledge.

152
Ahmad, K., Jafar, T. H. (2005). Prevalence and determinants of blood pressure screening in Pakistan.
Journal of Hypertension, 23(11), 1979-1984. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/16208138
Ahmad, S., Ahmad, T. (2015). Assessment of knowledge, attitude and practice among hypertensive
patients attending a health care facility in North India. International Journal of Research in Medical
Sciences 4(2), 122-127. Retrieved from
http://www.ijorim.com/siteadmin/article_issue/143825245725_Shiraj%20Ahmad_Community%20
Medicine....pdf.
Ahmad, N., Hassan, Y., Tangiisuran, B., Meng, O. L., Abd Aziz, N., Ahmad, F. U., Atif, M. (2013).
Guidelines adherence and hypertension control at a tertiary hospital in Malaysia. Journal of
Evaluation in Clinical Practice, 19(5), 798-804. doi: 10.1111/j.1365-2753.2012.01852.x
Ahmad, W., Krupat, E., Asma, Y., Fatima, N.-E., Attique, R., Mahmood, U., Waqas, A. (2015).
Attitudes of medical students in Lahore, Pakistan towards the doctor-patient relationship. PeerJ, 3,
e1050. doi: 10.7717/peerj.1050
Ahmed, W., Chaudhary, A., Alam, Y. A., Kaisar, F. (2007). Muslim patients’ perceptions of faith based
healing and religious inclination of treating physicians. Pakistan Heart Journal, 40(3), 61-65.
Retrieved from http://www.pkheartjournal.com/index.php/pkheart/article/viewFile/50/47
Ahmed, N., Abdul K M., Shah, SH., Anwar, W. (2008). Compliance to antihypertensive drugs, salt
restriction, exercise and control of systemic hypertension in hypertensive patients at Abbottabad.
Journal of Ayub Medical College Abbottabad, 20(2), 66-69. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/19385461
Aira, M., Kauhanen, J., Larivaara, P., Rautio, P. (2003). Factors influencing inquiry about patients'
alcohol consumption by primary health care physicians: Qualitative semi-structured interview study.
Family Practice, 20(3), 270-275. doi:10.1093/fampra/cmg307
Akl, O. A. M., El Mahalli, A. A., Elkahky, A. A., Salem, A. M. (2014). WHO/INRUD drug use indicators at
primary healthcare centers in Alexandria, Egypt. Journal of Taibah University Medical Sciences, 9(1),
54-64. doi: 10.1016/j.jtumed.2013.06.002
Alderman, M. H., Cohen, H. W. (2012). Dietary sodium intake and cardiovascular mortality:
controversy resolved? Current Hypertension Reports, 14(3), 193-201. doi: 10.1007/s11906-012-0275-
6
Alefan, Q., Huwari, D., Alshogran, O. Y., Jarrah, M. I. (2019). Factors affecting hypertensive patients'
compliance with healthy lifestyle. Patient Preference and Adherence, 13, 577-585.
doi:10.2147/PPA.S198446
Al-Ali, K. A., Al-Ghanim, F. A., Al-Furaih, A. M., Al-Otaibi, N., Makboul, G., El-Shazly, M. K. (2013).
Awareness of hypertension guidelines among family physicians in primary health care. Alexandria
Journal of Medicine, 49(1), 81-87. doi: 10.1016/j.ajme.2012.07.003

153
Al Ghobain, M., Alhashemi, H., Aljama, A., Bin Salih, S., Assiri, Z., … Mohamed, G. (2016).
Nonadherence to antihypertensive medications and associated factors in general medicine clinics.
Patient Preference and Adherence, 10, 1415-1419. doi: 10.2147/PPA.S100735
Ali, M., Horikoshi, Y. (2002). Situation analysis of health management information system in
Pakistan. Pakistan Journal of Medical Research, 41, 64-69.
Ali, N., Atkin, K., Neal, R. (2006). The role of culture in the general practice consultation process.
Ethnicity & Health, 11(4), 389-408. doi: 10.1080/13557850600824286
Ali, T. S., Krantz, G., Gul, R., Asad, N., Johansson, E., Mogren, I. (2011). Gender roles and their
influence on life prospects for women in urban Karachi, Pakistan: A qualitative study. Global Health
Action, 4, 7448-7448. doi: 10.3402/gha.v4i0.7448.
Al-Kandari, Y. Y. (2003). Religiosity and its relation to blood pressure among selected Kuwaitis.
Journal of Biosocial Science, 35(3), 463-472. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/12887224
Alkhazim, M. A., Althubaiti, A., Al-Ateeg, H., Alkhwaiter, M., AlNasser, M. M. (2015). Delivering
effective continuous medical education in Saudi Arabia: Some critical issues. Health Professions
Education, 1(1), 43-49. doi: 10.1016/j.hpe.2015.11.002
Almas, A., Hameed, A., Ahmed, B., Islam, M. (2006). Compliance to antihypertensive therapy. Journal
of the college of Physicians and Surgeons, 16(1), 23-26. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/16441983
Almas, A., Godil, S. S., Lalani, S., Samani, Z. A., Khan, A. H. (2012). Good knowledge about
hypertension is linked to better control of hypertension: A multicentre cross sectional study in
Karachi, Pakistan. BMC Research Notes, 5, 579. doi: 10.1186/1756-0500-5-579
Almas, A., Bhamani, F., Khan, A. H. (2014). Better physician-patient communication; an important
milestone in control of hypertension, a multicenter study from Karachi, Pakistan. Journal of College
of Physicians and Surgeons Pakistan, 24(12), 952-954. doi: 12.2014/jcpsp.952954
Al-Noumani, H., Wu, J. R., Barksdale, D., Sherwood, G., AlKhasawneh, E., Knafl, G. (2019). Health
beliefs and medication adherence in patients with hypertension: A systematic review of quantitative
studies. Patient Education and Counselling, 102(6), 1045-1056. doi: 10.1016/j.pec.2019.02.022
Al-Shahri, M. Z., Al-Khenaizan, A. (2005). Palliative care for Muslim patients. Journal of Supportive
Oncology, 3(6), 432-436. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/16350430
Alsolami, F., Hou, X., Correa-Velez, I. (2012). Factors affecting antihypertensive treatment
Adherence: A Saudi Arabian perspective. Clinical Medicine and Diagnostics, 2(4), 27-32. doi:
10.5923/j.cmd.20120204.02
Aly, Z., Taj, F. (2008). Why Pakistani medical graduates must remain free to emigrate. PLoS Medicine,
5(1), 0006-0008. doi: 10.1371/journal.pmed.0050002

154
Anderson, H., Goolishian, H. (1992). The client is the expert: A not-knowing approach to therapy. In
S. McNamee & K. J. Gergen (Eds.), Inquiries in social construction. Therapy as social construction (pp.
25-39). Thousand Oaks, US: Sage Publications, Inc.
Anderson, R., Funnell, M., Carlson, A., Saleh-Statin, N., Cradock, S., Skinner, T C. (2000). Facilitating
self‐care through empowerment. Psychology in diabetes care, 69-97. Retrieved from
https://onlinelibrary.wiley.com/doi/10.1002/0470846569.ch4
Anfossi, M., Numico, G. (2004). Empathy in the doctor-patient relationship. Journal of Clinical
Oncology. 22(11), 2258-2259. Retrieved from
https://ascopubs.org/doi/full/10.1200/JCO.2004.99.302
Angadi, S. S., Weltman, A., Watson-Winfield, D., Weltman, J., Frick, K., Patrie, J., Gaesser, G. A.
(2010). Effect of fractionized vs continuous, single-session exercise on blood pressure in adults.
Journal of Human Hypertension, 24(4), 300-302. doi: 10.1038/jhh.2009.110
Anwar, M., Green, J., Norris, P. (2012). Health-seeking behaviour in Pakistan: A narrative review of
the existing literature. Public Health, 126(6), 507-517. doi: 10.1016/j.puhe.2012.02.006
Appel, L. J. (2003). Effects of comprehensive lifestyle modification on blood pressure control: Main
results of the PREMIER clinical trial. The Journal of the American Medical Association, 289(16), 2083-
2093. doi: 10.1001/jama.289.16.2083
Appel, L. J. (2003). Lifestyle modification as a means to prevent and treat high blood pressure.
Journal of the American Society of Nephrology, 14(2), 99-102. doi:
10.1097/01.ASN.0000070141.69483.5A
Appel, L. J., Sacks, F. M., Carey, V. J., Obarzanek, E., Swain, J. F., Miller, E. R. (2005). Effects of protein,
monounsaturated fat, and carbohydrate intake on blood pressure and serum lipids: Results of the
OmniHeart randomized trial. The Journal of the American Medical Association, 294(19), 2455-2464.
doi: 10.1001/jama.294.19.2455
Appel, L. J., Brands, M. W., Daniels, S. R., Karanja, N., Elmer, P. J., Sacks, F. M. (2006). Dietary
approaches to prevent and treat hypertension: A scientific statement from the American Heart
Association. Hypertension 47(2), 296-308. doi: 10.1161/01.hyp.0000202568.01167.b6
Appleby, B., Roskell, C., Daly, W. (2015). What are health professionals' intentions toward using
research and products of research in clinical practice? A systematic review and narrative synthesis.
Nursing Open, 3(3), 125-139. doi: 10.1002/nop2.40
Arshad, S., Iqbal, J., Waris, S., Ismail, M., Naseer, A. (2016). Health care system in Pakistan: A review.
Research in Pharmacy and Health Sciences, 2(3), 211-216. doi: 10.32463/rphs. 2016.v02i03.41
Arksey, H., Knight, P. (1999). Interviewing for social scientists. London: Sage
Arnold, R. M. (1989). Elliot G. Mishler. the discourse of medicine: The dialectics of medical
interviews. Norwood, N.J., Ablex, 1984. pp. xii + 211. Language in Society, 18(1), 116-121.
doi:10.1017/S0047404500013361

155
Arthur, S. A., Geiser, H. R., Jacob Arriola, K. R., Kripalani, S. (2009). Health literacy and control in the
medical encounter: A mixed-methods analysis original communication. Journal of the National
Medical Association, 101(7), 677-683 Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3575736/
Asaria, P., Chisholm, D., Mathers, C., Ezzati, M., Beaglehole, R. (2007). Chronic disease prevention:
health effects and financial costs of strategies to reduce salt intake and control tobacco use. The
Lancet, 370(9604), 15-21. doi: 10.1016/S0140-6736(07)61698-5
Ashfaq, T., Anjum, Q., Siddiqui, H., Shaikh, S., Vohra, E. A. (2007). Awareness of hypertension among
patients attending primary health care centre and outpatient department of tertiary care hospital of
Karachi. Pakistan Journal of Medical Association, 57(8), 396-399. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/17902522
Ashoorkhani, M., Majdzadeh, R., Gholami, J., Eftekhar, H., Bozorgi, A. (2018). Understanding non-
adherence to treatment in hypertension: A qualitative study. International journal of community-
based nursing and midwifery, 6(4), 314-323. Retrieved from
www.ncbi.nlm.nih.gov/pmc/articles/PMC6226612/
Aslam, S., Emmanuel, P. (2010). Formulating a researchable question: A critical step for facilitating
good clinical research. Indian Journal of Sexually Transmitted Diseases and AIDS, 31(1), 47-50. doi:
10.4103/0253-7184.69003
Aslam, H., Alvi, A. A, Mughal, A., Haq, Z, Qureshi, W.A., … Aziz, S. (2013). Association of
socioeconomic classes with diet, stress and hypertension. The Journal of Pakistan Medical
Association, 63(2), 289-94. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/23894919
Aslami, A., Jobby, A. (2015). Compliance to hypertension treatment in residents of a fishermen
colony in District Kollam, Kerala. Nepal Journal of Epidemiology, 5(2), 480-487. Retrieved from
http://dx.doi.org/10.3126/nje.v5i2.12830.
Aston, I., Kaul, H. (2018). Making doctors better: Change doctors' beliefs rather than provide special
services. BMJ (Online), 363, 4657-4657. doi: 10.1136/bmj.k4657
Astor, A., Akhtar, T., Matallana, M. A., Muthuswamy, V., Olowu, F. A., Tallo, V., Lie, R. K. (2005).
Physician migration: Views from professionals in Colombia, Nigeria, India, Pakistan and the
Philippines. Social Science & Medicine, 61(12), 2492-2500. doi: 10.1016/j.socscimed.2005.05.003
Atif, M., Javaid, S., Farooqui, M., Sarwar, M. R. (2016). Rights and responsibilities of tuberculosis
patients, and the global fund: A qualitative study. PlosOne, 11(3). doi:10.1371/journal.pone.0151321
Atif, M., Azeem, M., Rehan Sarwar, M., Malik, I., Ahmad, W., Hassan, F., Rehman, A., Rana, M.
(2018). Evaluation of prescription errors and prescribing indicators in the private practices in
Bahawalpur, Pakistan. Journal of the Chinese Medical Association. Retrieved from
https://doi.org/10.1016/j.jcma.2017.12.002

156
Attum, B., Waheed, A., Shamoon, Z. (2019). Cultural competence in the care of Muslim patients and
their families. Available at: https://www.ncbi.nlm.nih.gov/books/NBK499933/
Auber, C., Rossler, W. (2007). Stigma towards people with mental illness in developing countries in
Asia. International Review of Psychiatry, 19(2), 157-178. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/17464793
Avis, M. (2005). Is there any epistemology for qualitative research. In I. Holloway (Ed.), Qualitative
Research in Healthcare. Berkshire: Open University Press.
Aylward, M. (2006). Beliefs: Clinical and vocational interventions; tackling psychological and social
determinants of illness and disability. In P.W. Halligan & M. Aylward (Eds.) The Power of Belief:
Psychosocial Influence on Illness, Disability and Medicine. Oxford: Oxford University Press.
Azadbakht, L., Mirmiran, P., Esmaillzadeh, A., Azizi, F. (2007). Better dietary adherence and weight
maintenance achieved by a long-term moderate-fat diet. British Journal of Nutrition, 97(2), 399-404.
doi: 10.1017/S0007114507328602
Azid, T., Khan, R. E. A. Alamasi, A. M. S. (2010). Labour force participation of married women in
Punjab (Pakistan). International Journal of Social Economics, 37(8), 592-612.
doi.org/10.1108/03068291011060643
Aziz, K., Faruqui, M., Abenathy, D. (2005). Blood pressure and hypertension distribution in a lower
middle class urban community in Pakistan. Journal of Pakistan Medical Association, 55(8), 333-338
Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/16164160
Baena, C. P., Olandoski, M., Younge, J. O., Buitrago-Lopez, A., Darweesh, S. K. L., Campos, N., …
Franco, O. H. (2014). Effects of lifestyle-related interventions on blood pressure in low and middle-
income countries: Systematic review and meta-analysis, Journal of Hypertension, 32(5), 961-973. doi:
10.1097/HJH.0000000000000136
Bailey, J. (2008). First steps in qualitative data analysis: transcribing. Family Practice, 25(2), 127-131.
doi: 10.1093/fampra/cmn003
Baker L. R. (1987). Saving Belief: A Critique of Physicalism. Princeton: Princeton University Press.
Balzer-Riley, J. W. (2004). Communication in nursing (5th ed.). St. Louis, Mo: Mosby.
Banegas, J., Lundelin, K., de la Figuera, M., de la Cruz, J. J., Graciani, A., … Puig, J. G. (2011). Physician
perception of blood pressure control and treatment behavior in high-risk hypertensive patients: A
cross-sectional study. PLoS One, 6(9), e24569. doi: 10.1371/journal.pone.0024569
Barbot, J. (2006). How to build an ‘active’ patient? The work of AIDS associations in France. Social
Science and Medicine, 62(3), 538-551. doi: 10.1016/j.socscimed.2005.06.025
Barbouni, A., Nalmpanti, M., Gennimata, D., Theodoridis, D., Merakou, K. (2017). Beliefs and
practices of Greek doctors in relation to patients’ adherence to antihypertensive medication. Journal
of Human Hypertension, 31(5), 341-346. doi: 10.1038/jhh.2016.84

157
Bartlett, D., Payne, S. (1997). Grounded theory – its basis, rationale and procedures, in McKenzie, G.,
Powell, J. and Usher, R. (Eds), Understanding Social Research: Perspectives on Methodology and
Practice, London. The Falmer Press.
Barrett, D., Wilson, B., Woollands, A. (2009). Care planning: A guide for nurses. Harlow, Pearson
Education.
Basaran, N. F., Akici, A. (2012). Patients’ experience and perspectives on the rational use of drugs in
Turkey: A survey study. Patient preference and adherence, 6, 719-724. doi: 10.2147/PPA.S34922
Basharat, S., Shaikh, B. T. (2011). Healthcare System in Pakistan - A Global Survey. New Delhi: New
Century Publications.
Basu-Zharku, I. O. (2011). The influence of religion on health. Inquiries Journal/Student Pulse, 3(1),
Retrieved from http://www.inquiriesjournal.com/a?id=367
Bassett, A. (2011). Multicultural clinical interactions: The importance of the explanatory model (EM)
concept in understanding the cultural dimensions of clinical practice, Nottingham Trent University.
Nottingham.
Batcagan-Abueg, A. P., Lee, J. J., Chan, P., Rebello, S. A., Amarra, M. S. (2013). Salt intakes and salt
reduction initiatives in Southeast Asia: A review. Asia Pacific Journal of Clinical Nutrition, 22(4), 490-
504. doi: 10.6133/apjcn.2013.22.4.04
Bazigha, A. K., Fahmyn, S. A., Abu, Gharbieh. E. F, Ali, H. S. (2006). Professional practices and
perception towards rational use of medicine according to WHO methodology in United Arab
Emirates. Pharmacy Practice, 8:70-6. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4140580/
Beaney, T., Schutte, A. E., Tomaszewski, M., Ariti, C., Burrell, L. M. (2018). May measurement month
2017: An analysis of blood pressure screening results worldwide. The Lancet Global Health, 6(7),
736-743. doi: 10.1016/S2214-109X(18)30259-6
Beauchamp, T. C., Childress, J. F., (2001). Principles of Biomedical Ethics. London: Oxford University
Press.
Beevers, D. G., Lip, G., Brien, E. (2015). ABC of Hypertension. England: Wiley and Sons.
Becker, H., Gee, B. (1957). Participant observation and interviewing: A Comparison. Human
Organization, 16(3), 28-32. doi: 10.17730/humo.16.3.k687822132323013
Becker, P. H. (1993). Common pitfalls in published grounded theory research. Qualitative Health
Research. 3. pp. 254-260.
Behnood-Rod, A., Rabbanifar, O., Pourzargar, P., Rai, A., Saadat, Z., ... Morisky, D. E. (2016).
Adherence to antihypertensive medications in Iranian patients. International Journal of
Hypertension, 2016: 7. doi: 10.1155/2016/1508752

158
Bello, S., Fatiregun, A., Oyo-Ita, A., Ikpeme, B. (2010). Dose-response relationship between alcohol
use and blood pressure among drivers of commercial vehicles in Calabar, Southern Nigeria. Journal
of Public Health in Africa, 1(1), e5. doi: 10.4081/jphia.2010.e5
Benson, J., Britten, N. (2002). Patients' decisions about whether or not to take antihypertensive
drugs: Qualitative study. BMJ : British Medical Journal, 325(7369), 873-873. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC129637/
Bennet, J.K., Fuertes, J.N., Phillips, R., (2010). The role of patient attachment and working alliance on
patient adherence, satisfaction, and health-related quality of life in lupus treatment, Patient
Education and Counselling, 85, 53-59. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/20869188
Bezreh, T., Barton Laws, M., Taubin, T., Rifkin, D. E., Wilson, I. B. (2012). Challenges to physician-
patient communication about medication use: A window into the skeptical patient's world. Patient
Preference and Adherence, 6, 11-18. doi:10.2147/PPA.S25971
Bhandari, B., Bhattarai, M., Bhandari, M., Ghimire, A., Pokharel, P. K., Morisky, D. E. (2015).
Adherence to antihypertensive medications: Population based follow up in Eastern Nepal. Journal of
Nepal Health Research Council, 13(29), 38-42. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/26411711
Bhatti, Z., Salek, S., Finlay, A. (2011). Chronic diseases influence major life changing decisions: A new
domain in quality of life research. Journal of the Royal Society of Medicine, 104(6), 241-250.
Retrieved from https://doi.org/10.1258/jrsm.2011.110010
Bhui, K., Bhugra, D. (2002). Explanatory models for mental distress: Implications for clinical practice
and research. The British Journal of Psychiatry, 181(1), 6-7. Retrieved from
https://www.researchgate.net/publication/11284889_Explanatory_models_for_mental_distress_Im
plications_for_clinical_practice_and_research
Bilal, A., Riaz, M., Shafiq, N. U., Ahmed, M., Sheikh, S., Rasheed, S. (2015). Non-compliance to anti-
hypertensive medication and its associated factors among hypertensives. Journal of Ayub Medical
College Abbottabad, 27(1), 158-163. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/26182765
Blair, S. N., Sallis, R. E., Hutber, A., Archer, E. (2012). Exercise therapy - the public health message.
Scandinavian Journal of Medicine & Science in Sports, 22(4), 24-28. doi: 10.1111/j.1600-
0838.2012.01462.x
Blaxter, M. (1990). Health and Lifestyles. London: Tavistock and Routledge.
Blaxter, M. (1997). Whose fault is it? People's own conceptions of the reasons for health
inequalities. Social Science & Medicine, 44(6), 747-756. doi: 10.1016/S0277-9536(96)00192-X
Blaxter, M. (2010). Health. Cambridge: Polity Press.
Bliss, M. (2000). William, Osler: A life in medicine, University of Toronto Press. Toronto.

159
Blumhagen, D. (1980). Hyper-tension: a folk illness with a medical name. Culture, Medicine and
Psychiatry, 197-22. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/7408522
Bodenhausen, G. V., Lichtenstein, M. (1987). Social stereotypes and information-processing
strategies: The impact of task complexity. Journal of Personality and Social Psychology, 52(5), 871-
880. doi: 10.1037/0022-3514.52.5.871
Bolam, B., Gleeson, K., Murphy, S. (2003). Lay person or health expert? Exploring theoretical and
practical aspects of reflexivity in qualitative health research. Forum Qualitative Sozialforschung, 4(2),
26. Retrieved from http://www.qualitative-research.net/index.php/fqs/article/viewArticle/699/1514
Boland, A., Cherry, M. G., Dickson, R. (2013). Doing a Systematic Review: A Student's Guide. London:
Sage Publications.
Boruchovitch, E., Mednick, B. R. (2002). The meaning of health and illness: Some considerations for
health psychology. Psico-USF, 7(2), 175-183. doi: 10.1590/S1413-82712002000200006
Bose, S., Jalal, A. (2004). Modern South Asia: History, Culture, Political Economy (2nd ed.). New York
and London: Routledge.
Boutain, D. M. (2001). Discourses of worry, stress, and high blood pressure in rural south Louisiana.
Journal of Nursing Scholarship, 33(3), 225-230. doi:10.1111/j.1547-5069.2001.00225.x
Boyer, P. (1994). The Naturalness of Religious Ideas: A Cognitive Theory of Religion. Los Angeles:
University of California Press.
Bramley, L., Matiti, M. (2014). How does it really feel to be in my shoes? Patients' experiences of
compassion within nursing care and their perceptions of developing compassionate nurses. Journal
of Clinical Nursing, 23(19-20), 2790-2799. doi: 10.1111/jocn.12537
Breen, N., Caine, C., Coltheart, M., Hendy, J., Roberts, C. (2000). Towards an understanding of
delusions of misidentification. In M. Coltheart & M. Davies (Eds.) Pathologies of Belief. Oxford:
Blackwell.
Brenner, D. R., Haig, T. R., Poirier, A. E., Akawung, A., Friedenreich, C. M., Robson, P. J. (2017).
Alcohol consumption and low-risk drinking guidelines among adults: a cross-sectional analysis from
Alberta's Tomorrow Project. Health Promotion and Chronic Disease Prevention in Canada: Research,
Policy and Practice, 37(12), 413-424. doi: 10.24095/hpcdp.37.12.03
Brekenridge, P. J., Jones, D., Elliot, I., Nicol, M. (2012). Choosing a methodological path: Reflections
on the constructivist turn Grounded theory review: An International Journal, 11(1), 64-71. Retrieved
from http://groundedtheoryreview.com/2012/06/01/choosing-a-methodological-path-reflections-
on-the-constructivist-turn/
Brien, S. E., Ronksley, P. E., Turner, B. J., Mukamal, K. J., Ghali, W. A. (2011). Effect of alcohol
consumption on biological markers associated with risk of coronary heart disease: Systematic review
and meta-analysis of interventional studies. The British Medical Journal, 342(7795), 480-480. doi:
10.1136/bmj.d636

160
Brinkmann, S. (2013). Qualitative interviewing (understanding qualitative research). Oxford
University Press, USA.
Britten N. (1995). Qualitative interviews in medical research. British Medical Journal, (Clinical
research ed.), 311(6999), 251-3. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/7627048
Britten, N., Stevenson, F. A., Barry, C. A., Barber, N., Bradley, C. P. (2000). Misunderstandings in
prescribing decisions in general practice: Qualitative study. The British Medical Journal, 320(7233),
484-488. doi:10.1136/bmj.320.7233.484
Brobeck E., Odencrants S., Bergh H., Hildingh C. (2014). Patients' experiences of lifestyle discussions
based on motivational interviewing: A qualitative study. BMC Nursing, 13(1), 1-7. doi: 10.1186/1472-
6955-13-13. doi: 10.1186/1472-6955-13-13
Bromfield, S., Muntner, P. (2013). High blood pressure: The leading global burden of disease risk
factor and the need for worldwide prevention programs. Current Hypertension Reports, 15(3), 134-
136. doi: 10.1007/s11906-013-0340-9
Broström, A., Strömberg, S., Ulander, A., Fridlund, B., Martensson, J., Svanborg, E. (2009). Perceived
informational needs, side‐effects and their consequences on adherence-a comparison between
CPAP treated patients with OSAS and healthcare personnel. Patient Education and Counselling, 74,
228-235. doi.org/10.1016/j.pec.2008.08.012
Brotons, C., Drenthen, A. J. M., Durrer, D., Moral, I. (2012). Beliefs and attitudes to lifestyle, nutrition
and physical activity: The views of patients in Europe. Family Practice, 29(1), i49-i55. doi:
10.1093/fampra/cmr091
Brown, R. E., Riddell, M. C., Macpherson, A. K., Canning, K. L., Kuk, J. L. (2013). The joint association
of physical activity, blood-pressure control, and pharmacologic treatment of hypertension for all-
cause mortality risk. American Journal of Hypertension, 26(8), 1005-1010. doi: 10.1093/ajh/hpt063
Brown, I. J., Tzoulaki, I., Candeias, V., Elliott, P. (2009). Salt intakes around the world: Implications for
public health. International Journal of Epidemiology, 38(3), 791-813. doi: 10.1093/ije/dyp139
Bruce, J., Mollison, J. (2004). Reviewing the literature: Adopting a systematic approach. Journal of
Family Planning and Reproductive Health, 30(1), 13-16. doi: 10.1783/147118904322701901
Bryant, A. (2003). A constructive/ist response to Glaser. Qualitative Social Research, 4(1), Retrieved
from http://www.qualitative-research.net/index.php/fqs/article/view/757/1642
Bryman, A. (2008). Of methods and methodology, Qualitative research in organizations and
management. An international Journal, 3(2), 159-168. doi: 10.1108/17465640810900568
Bryman, A. (2012). Social research methods. United States: Oxford University Press.
Bughio, Q. (2014). Determining the status and use of languages spoken in Pakistan. Sustainable
Multilingualism, 4(4), 46-56. doi: org/10.7220/2335-2027.4.3

161
Bukhari, A. H. S., Gaho, G. M., Soomro, K. H. (2018). Gender inequality problems and its solutions in
Pakistan. Research Journal of Political Science, 7(4), 47-58.
Bukhari, S. S., Pardhan, A., Khan, A. S., Ahmed, A., Choudiy, F. J., … Khan, M. (2002). Superstitions
regarding health problems in different ethnic groups in Karachi. The Journal of Pakistan Medical
Association, 52(8), 383-387. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/12481684
Burgess, D. J., Fu, S. S., van Ryn, M. (2004). Why do providers contribute to disparities and what can be done about it? Journal of general internal medicine, 19(11), 1154-1159. doi:10.1111/j.1525-1497.2004.30227.x
Burki, S. J., Ziring, L. (2017). Pakistan. Encyclopaedia Britannica. Retrieved from
https://www.britannica.com/place/Pakistan/Daily-life-and-social-customs
Burnier, M. (2018). Hypertension guidelines. European Heart Journal, 39(11), 908-910. doi:
10.1093/eurheartj/ehy063
Burns, D. M. (2003). Epidemiology of smoking-induced cardiovascular disease. Progress in
Cardiovascular disease, 46(1), 11-29. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/12920698
Burrows, L., Muller, R. (2007). Chronic kidney disease and cardiovascular disease: Pathophysiologic
links. Nephrology Nursing Journal, 34(1), 55-63. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/17345692
Bury, M. (1997). Health and Illness in a Changing Society. New York: Routledge.
Bush, J., White, M., Kai, J., Rankin, J., Bhopal, R. (2003). Understanding influences on smoking in
Bangladeshi and Pakistani adults: Community based, qualitative study. BMJ, 326(7396), 962. doi:
10.1136/bmj.326.7396.962
Butt , M. (2015). Use of illegal toxic alcohol is killing hundreds every year in pakistan ; family
physicians have to play a more proactive role in saving precious lives. Middle East Journal of
Business, 10(2), 48-54. doi:10.5742/MEJB.2015.92639
Buttar, H. S., Li, T., Ravi, N. (2005). Prevention of cardiovascular diseases: Role of exercise, dietary
interventions, obesity and smoking cessation. Experimental and clinical cardiology, 10(4), 229-249.
Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2716237/?report=classic
Bytheway, B. (2000). Youthfulness and agelessness: A comment. Ageing and society, 20(6): 781-789
Retrieved from https://www.cambridge.org/core/journals/ageing-and-society/article/youthfulness-
and-agelessness-a-comment/44F5002F723C2EEC1B259D1DF19B46CF
Cappuccio, F., Miller, M. A. (2016). Cardiovascular disease and hypertension in sub-Saharan Africa:
Burden, risk and interventions. Internal and Emergency Medicine, 11(3), 299-305. doi:
10.1007/s11739-016-1423-9.

162
Carey, M., Buchan, H., Sanson-Fisher, R. (2009). The cycle of change: Implementing best-evidence
clinical practice. International Journal for Quality in Health Care, 21(1), 37-43. doi:
10.1093/intqhc/mzn049
Carlin, A., Murphy, M. H., Gallagher, A. M. (2016). Do interventions to increase walking work? A
systematic review of interventions in children and adolescents. Sports Medicine (Auckland, N.Z.), 46,
515-530. doi: 10.1007/s40279-015-0432-6
Carpenter, C. M., G. F. Wayne and G. N. Connolly (2007). The role of sensory perception in the
development and targeting of tobacco products. Addiction, 102(1), 136-147. doi: 10.1111/j.1360-
0443.2006.01649.x
Carr, A. J., Donovan, J. L. (1998). Why doctors and patients disagree. Rheumatology, 37(1), 1-4. doi:
10.1093/rheumatology/37.1.1a
Carson, D., Gilmore, A., Perry, C., Gronhaug, K. (2001). Qualitative marketing research. London: Sage
Carson, A. P., Howard, G., Burke, G. L., Shea, S., Levitan, E. B., Muntner, P. (2011). Ethnic differences
in hypertension incidence among middle-aged and older adults: The multi-ethnic study of
atherosclerosis. Hypertension, 57(6), 1101-1107. doi: 10.1161/hypertensionaha.110.168005
Cassidy, T. (2018). Pakistan: A Contemporary History. Nutshell Books.
Castillo, R. (2016). SSA 03-1 prevalence and management of hypertension in Southeast Asia. Journal
of Hypertension, 34(1), doi: 10.1097/01.hjh.0000499881.98439.59
Chaffee, S., Roser, C. (1986) Involvement and the consistency of knowledge, attitudes and
behaviour. Communication Research, 13(3), 373-399. doi: 10.1177/009365086013003006
Chapple, A., Ziebland, S., McPherson, A. (2004). Stigma, shame, and blame experienced by patients
with lung cancer: Qualitative study. BMJ, 328(7454), 1470-1470. doi: 10.1136/bmj.38111.639734.7C
Chan, P. S., Wong, M. M. (2004). Physicians and complementary-alternative medicine: training,
attitudes, and practices in Hawaii. Hawaii Medical Journal. 63, 176-81. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/15298087
Charmaz, K. (2003). Grounded theory: Objectivist and constructivist methods. In N. K. Denzin & Y. S.
Lincoln (Eds.), Strategies of qualitative inquiry. Thousand Oaks: Sage Publications.
Charmaz, K. (2006). Constructing grounded theory: A Practical Guide Through Qualitative Analysis.
London: Sage Publications.
Charmaz, K. (2008). Constructionism and the Grounded Theory Method. New York: The Gilford press.
Charmaz, K. (2014). Constructing grounded theory. Thousand Oaks: Sage Publications.
Charrois, T. L. (2015). Systematic reviews: What do you need to know to get started? The Canadian
Journal of Hospital Pharmacy, 68(2), 144-8. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4414076/

163
Chen, L., Smith, G. D., Harbord, R. M., Lewis, S. J. (2008). Alcohol intake and blood pressure: A
systematic review implementing a Mendelian randomization approach. PLoS Medicine, 5(3), 0461-
0471. doi: 10.1371/journal.pmed.0050052
Chipidza, F. E., Wallwork, R. S., Stern, T. A. (2015). Impact of the doctor-patient relationship. The
primary care companion for CNS disorders, 17(5), 10.4088/PCC.15f01840. doi:10.4088/PCC.15f01840
Chiu, S., Bergeron, N., Williams, P. T., Bray, G. A., Sutherland, B., Krauss, R. M. (2016). Comparison of
the DASH (dietary approaches to stop hypertension) diet and a higher-fat DASH diet on blood
pressure and lipids and lipoproteins: A randomized controlled trial. American Journal of Clinical
Nutrition, 103(2), 341-347. doi: 10.3945/ajcn.115.123281
Cho, Y., Shin, S.-Y., Won, S., Relton, C. L., Smith, G. D., Shin, M.-J. (2015). Alcohol intake and
cardiovascular risk factors: A Mendelian randomisation study. Scientific Reports, 5(Article number:
18422). doi: 10.1038/srep18422
Chobanian, A. V., Bakris, G. L., Black, H. R., Cushman, W. C., Green, L. A., Izzo, J. L., Jr., Roccella, E. J.
(2003). The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation,
and Treatment of High Blood Pressure: the JNC 7 report. Jama, 289(19), 2560-2572.
doi:10.1001/jama.289.19.2560
Chockalingam, A., Campbell, N. R., Fodor, J. G. (2006). Worldwide epidemic of hypertension. The
Canadian Journal of Cardiology, 22(7), 553-555. doi: 10.1016/S0828-282X(06)70275-6
Choudhury, S. M., Brophy, S., Williams, R. (2009). Understanding and beliefs of diabetes in the UK
Bangladeshi population. Diabetic Medicine, 26(6), 636-640. doi:10.1111/j.1464-5491.2009.02741.x
Chow, C. K., Teo, K. K., Rangarajan, S., Islam, S., Gupta, R., Avezum, A. (2013). Prevalence, awareness,
treatment, and control of hypertension in rural and urban communities in high- middle and low-
income countries. The Journal of the American Medical Association, 310(9), 959-968. doi:
10.1001/jama.2013.184182
Chow, N., Gallo, L., Busse, J. W. (2018). Evidence-based medicine and precision medicine:
Complementary approaches to clinical decision-making. Precision Clinical Medicine, 1(2), 60-64.
doi:10.1093/pcmedi/pby009
Chrysant, S. G. (2016). Effects of high salt intake on blood Pressure and cardiovascular disease: The
role of COX inhibitors. Clinical Cardiology, 39(4), 240-242. doi: 10.1002/clc.22536
Chulze, B. (2007). Stigma and mental health professionals: a review of the evidence on an intricate
relationship. International Review of Psychiatry, 19(2), 137-155. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/17464792
Chung, N., Baek, S., Chen, M. F., Liau, C. S., Park, C. G., … Fujita, T. (2008). Expert recommendations
on the challenges of hypertension in Asia. International Journal of Clinical Practice, 62(9), 1306-1312.
doi: 10.1111/j.1742-1241.2008.01838.x

164
Clark, T. (2011). Gaining and maintaining access: Exploring the mechanisms that support and
challenge the relationship between gatekeepers and researchers. Qualitative Social Work, 10(4),
485-502. doi:10.1177/1473325009358228
Clark, A. M., Duncan, A. S., Trevoy, J. E., Heath, S., Chan, M. (2011). Healthy diet in Canadians of low
socioeconomic status with coronary heart disease: Not just a matter of knowledge and choice. Heart
Lung, 40(2), 156-163. doi: 10.1016/j.hrtlng.2010.01.007
Clarke, M. A., Belden, J. L., Koopman, R. J., Steege, L. M., Moore, J. L., … Kim, M. S. (2013).
Information needs and information-seeking behaviour analysis of primary care physicians and
nurses: A literature review. Health Information Libraries Journal, 30(3), 178-190. doi:
10.1111/hir.12036
Clarke, A. (2010). The sociology of healthcare (2nd ed.). Harlow: Longman.
Claramita, M., Utarini, A., Soebono, H., Dalen, J., Vleuten, C. (2010). Doctor-patient communication
in a southeast Asian setting: The conflict between ideal and reality. Advances in Health Sciences
Education, 16(1), 69-80. doi:10.1007/s10459-010-9242-7
Cobb, L. K., Appel, L. J., Anderson, C. A. M. (2012). Strategies to Reduce Dietary Sodium Intake.
Current Treatment Options in Cardiovascular Medicine, 14(4), 425-434. doi: 10.1007/s11936-012-
0182-9
Cohen, D., Olson, J. M., Sorrentino, R. M., Zanna, M. P. (2005). Culture and Social Behavior. Mahwah:
Lawrence Erlbaum Associates.
Cohen, S., Janicki-Deverts, D., Miller, G. E. (2007). Psychological stress and disease. The Journal of
American Medical Association, 298(14), 1685-1687. doi:10.1001/jama.298.14.1685
Conrad, P. (1990). Qualitative research on chronic illness: A commentary on method and conceptual
development. Social Science & Medicine, 30(11), 1257-1263. doi: 10.1016/0277-9536(90)90266-u
Conrad, P. (2005). The Sociology of Health & Illness: Critical Perspectives. New York: Worth
Publishers.
Conard, P., Barker, K. (2010). The social construction of illness: Key insights and policy implications.
Journal of Health and Social Behaviour, 51(S), 67-79. doi: 0.1177/0022146510383495
Conlin, P. R. (2007). Eat your fruits and vegetables but hold the salt. Circulation, 116(14), 1530-1531.
doi: 10.1161/CIRCULATIONAHA.107.729574
Consoli, S. M., Lemogne, C., Levy, A., Denis, P., Laurent, S. (2010). Physicians' degree of motivation
regarding their perception of hypertension, and blood pressure control. Journal of Hypertension,
28(6), 1330-1339. doi: 10.1097/HJH.0b013e32833815ee
Conner, M., Norman, J. (2008). Predicting Health Behaviour. New York: Open University Press.

165
Connors, M. H., Halligan, P. W. (2015). A cognitive account of belief: a tentative road map. Frontiers
in psychology, 5(1588). doi: 10.3389/fpsyg.2014.01588
Cook, N.R., Cutler, J. A., Obarzanek, E., Buring, J. E., Rexrode, K. M., Kumanyika, S. K., … Whelton, P.
K. (2007). Long term effects of dietary sodium reduction on cardiovascular disease outcomes:
Observational follow-up of the trials of hypertension prevention (TOHP). The British Medical Journal,
334(7599), 885-888. doi: 10.1136/bmj.39147.604896.55
Cook, D. A., Sorensen, K. J., Wilkinson, J. M., Berger, R. A. (2013). Barriers and decisions when
answering clinical questions at the point of care: A grounded theory study. JAMA Internal Medicine,
173(21), 1962-1969. doi:10.1001/jamainternmed.2013.10103
Corbin, J. S. (1990). Basics of Qualitative Research: Grounded Theory Procedures and Techniques.
Newbury Park: Sage Publications.
Cornelissen, V. A., Fagard, R. H. (2005). Effects of endurance training on blood pressure, blood
pressure-regulating mechanisms, and cardiovascular risk factors. Hypertension, 46(4), 667-675. doi:
10.1161/01.hyp.0000184225.05629.51
Cornelissen, V. A., Smart, N. A. (2013). Exercise Training for Blood Pressure: A Systematic Review and
Meta‐analysis. Journal of the American Heart Association, 2(1), e004473. doi:
10.1161/JAHA.112.004473
Covell, C. L., Sidani, S., Ritchie, J. A. (2012). Does the sequence of data collection influence
participants’ responses to closed and open-ended questions? A methodological study. International
Journal of Nursing Studies, 49(6), 664-671. doi: 10.1016/j.ijnurstu.2011.12.002
Crabtree, B. F., DiCicco-Bloom, B. (2006). The qualitative research interviews. Medical Education,
40(4), 314-318. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/16573666.
Creswell, J., W. (2007). Qualitative inquiry and research design: Choosing among five traditions.
London. Sage Publications.
Creswell, J. (2013). Research design: Qualitative, quantitative, and mixed methods approaches.
London: Sage Publications.
Critelli, M. F. (2012). Between law and custom: Women, family law and marriage in Pakistan. Journal
of Comparative Family Studies, 43(5), 673-693. Retrieved from
https://www.jstor.org/stable/23267840?seq=1#page_scan_tab_contents
Critical Appraisal Skills Programme (CASP). (2018). CASP Checklists. Retrieved from https://casp-
uk.net/casp-tools-checklists/
Crotty, M. (1998). The foundations of social research: Meaning and perspective in the research
process. St Leonards, NSW: Allen and Unwin.
Currer, C., Stacey, M. (1986). Concepts of Health, Illness and Disease: A Comparative Perspective.
Leamington Spa: Berg.

166
Currie, K., Strachan, P. H., Spaling, M., Harkness, K., Barber, D., Clark, A. M. (2015). The importance
of interactions between patients and healthcare professionals for heart failure self-care: A
systematic review of qualitative research into patient perspectives. European Journal of
Cardiovascular Nursing, 14(6), 525–535. https://doi.org/10.1177/1474515114547648
Daly, D., Hannon, S., Brady, V. (2019). Motivators and challenges to research recruitment -A
qualitative study with midwives. Midwifery, 74, 14-20. doi:10.1016/j.midw.2019.03.011
Damasio, A. R. (2000). Thinking about belief. In D. L. Schacter & E. Scarry (Eds.) Memory, Brain and
Belief. Cambridge: Harvard University Press.
Danaei, G., Finucane, M. M., Lin, J. K., Singh, G. M., Paciorek, C. J., … Ezzati, M. (2011). National,
regional, and global trends in systolic blood pressure since 1980: Systematic analysis of health
examination surveys and epidemiological studies with 786 country-years and 5.4 million
participants. The Lancet, 377(9765). Retrieved from https://www-sciencedirect-
com.ezproxy.herts.ac.uk/science/article/pii/S0140673610620363
Davies, S., Ellis, L., Laker, S. (2000). Promoting autonomy and independence for older people within
nursing practice: An observational study. Journal of Clinical Nursing, 9(127-136). doi: 10.1046/j.1365-
2702.2000.00348.x
Davis, F. (1992). Fashion, Culture and Identity, Chicago: Chicago University Press.
Davies, K., Harrison, J. (2007). The information-seeking behaviour of doctors: a review of the
evidence. Health Information and Libraries Journal, 24: 78-94. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/17584211
Davoudi, N., Dehghan Nayeri, N., Raiesifar, A., Poortaghi, S., Ahmadian, S. (2016). Issues of
theoretical sampling: A narrative review. Nursing and Midwifery Studies, 6(2),
doi:10.5812/nmsjournal.38284
Dean, B., Schachter, M., Vincent, C., Barber, N. (2002). Prescribing errors in hospital inpatients: Their
incidence and clinical significance. Quality & safety in health care, 11(4), 340-344. doi:
10.1136/qhc.11.4.340
De Bie, J. L., De Poot, C. J. (2016). Studying police files with grounded theory methods to understand
jihadist networks. Studies in Conflict & Terrorism, 39(7-8), 580-601.
doi:10.1080/1057610X.2016.1142241
de Castro, J. M., Brewer, E. M. (1992). The amount eaten in meals by humans is a power function of
the number of people present. Physiology & Behaviour, 51(1), 121-125. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/1741437/
De Henauw, S., De Bacquer, D., Fonteyne, W., Stam, M., Kornitzer, M., De Backer, G. (1998). Trends
in the prevalence, detection, treatment and control of arterial hypertension in the Belgian adult
population. Journal of Hypertension, 16(3), 277-284. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/9557920

167
DeJean, D., Giacomini, M., Vanstone, M., Brundisini, F. (2013). Patient experiences of depression and
anxiety with chronic disease: A systematic review and qualitative meta-synthesis. Ontario Health
Technology Assessment Series, 13(16), 1-33. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/24228079/
de Laine, M. (2000). Fieldwork, participation and practice: Ethics and dilemmas in qualitative
research. London, United Kingdom: Sage.
Denzin, N. K., Lincoln, S. (1994). Handbook of Qualitative Research. Thousand Oaks: Sage
Publications.
Denzin, N. K., Lincoln, Y. S. (1998). The Landscape of Qualitative Research: Theories and Issues.
Thousand Oaks: Sage Publications.
Denzin, N. K., Lincoln, Y. S. (2005). The Sage Handbook of Qualitative Research. London: Sage
Publications.
Dennick, R. (2016). Constructivism: Reflections on twenty-five years teaching the constructivist
approach in medical education. International Journal of Medical Education, 7, 200-205.
doi:10.5116/ijme.5763.de11
Derksen, F. A., Olde Hartman, T. C., Bensing, J. M., Lagro-Janssen, A. L. (2016). Managing barriers to
empathy in the clinical encounter: a qualitative interview study with GPs. The British journal of
general practice: The journal of the Royal College of General Practitioners, 66(653), 887-895.
doi:10.3399/bjgp16X687565
Devkota, S., Dhungana, R. R., Pandey, A. R., Bista, B., Panthi, S., … Gajurel, R. M. (2016). Barriers to
treatment and control of hypertension among hypertensive participants: A community-based cross-
sectional mixed method study in municipalities of Kathmandu, Nepal. Frontiers in Cardiovascular
Medicine, 3, 26. doi: 10.3389/fcvm.2016.00026
De Vries, T. P. (1993). Presenting clinical pharmacology and therapeutics: a problem based approach
for choosing and prescribing drugs. British Journal of Clinical Pharmacology, 35(6), 581-586
Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1381599/
Devi, P., Rao, M., Sigamani, A., Faruqui, A., Jose, M., Gupta, R., Xavier, D. (2013). Prevalence, risk
factors and awareness of hypertension in India: A systematic review. Journal of Human
Hypertension, 27(5), 281-287. doi:10.1038/jhh.2012.33
Dhungana, R. R., Pandey, A. R., Bista, B., Joshi, S., Devkota, S. (2016). Prevalence and associated
factors of hypertension: A community-based cross-sectional study in Municipalities of Kathmandu,
Nepal. International journal of hypertension, 1656938. doi:10.1155/2016/1656938
Diaz, K. M., Shimbo, D. (2013). Physical activity and the prevention of hypertension. Current
hypertension reports, 15(6), 659-668. doi :10.1007/s11906-013-0386-8

168
Dickinson, H. O., Mason, J. M., Nicolson, D. J., Campbell, F., Beyer, F. R., Cook, J. V., … Ford, G. A.
(2006). Lifestyle interventions to reduce raised blood pressure: A systematic review of randomized
controlled trials. Journal of Hypertension, 24(2), 215-223. doi: 10.1097/01.hjh.0000199800.72563.26
Dickinson, A., Horton, K., Machen, I., Bunn, F., Cove, J., Jain, D., Maddex, T. (2011). The role of health
professionals in promoting the uptake of fall prevention interventions : A qualitative study of older
people's views. Age and Ageing, 60(6), 724-730. doi: 10.1093/ageing/afr111
Dickinson, A., Machen, I., Horton, K., Jain, D., Maddex, T., Cove, J. (2011). Fall prevention in the
community: What older people say they need. British Journal of Community Nursing, 16(4), 174-180.
doi: 10.12968/bjcn.2011.16.4.174
Diefenbach, M.A., Leventhal, H. (1996). The common-sense model of illness representation. Journal
of Social Distress and the Homeless, 5(1), 11-38. Retrieved from
https://link.springer.com/article/10.1007/BF02090456
DiMatteo, M. R. (2004). Variations in patients’ adherence to medical recommendations: A
quantitative review of 50 years of research. Medical Care, 42(3), 200-209. doi:
10.1097/01.mlr.0000114908.90348.f9
Din, I. (2014). Health Outcome and the Pakistani Population. Newcastle: Cambridge Scholars
Publishing.
Dixit, S., Mishra, M., Sharma, A. K. (2008). Conceptualisation of health and illness: A study of social
representations among Bondos of Orissa. Psychology and Developing Societies, 20(1), 1-26.
doi:10.1177/097133360702000101
Donovan, J. (1991). Patient education and the consultation: The importance of lay beliefs. Annals of
the Rheumatic Diseases, 50(3), 418-421. doi:10.1136/ard.50.Suppl_3.418
Donnelly, T., Al Suwaidi, J., Al Bulushi, A., Al Enazi, N., Yassin, K., Rehman, A. M.,Hassan, A. A., Idris, Z.
(2011). The influence of cultural and social factors on healthy lifestyle of Arabic women. Avicenna
2011, 3. doi: 10.5339/avi.2011.3
Dugdale, D. C., Epstein, R., Pantilat, S. Z. (1999). Time and the patient-physician relationship.
Journal of General Internal Medicine, 14(Suppl 1), S34-S40. doi: 10.1046/j.1525-1497.1999.00263.x
Durrani, N., Halai, A. (2018). Dynamics of gender justice, conflict and social cohesion: Analysing
educational reforms in Pakistan. International Journal of Educational Development, 61, 27-39.
doi:10.1016/j.ijedudev.2017.11.010
Dyer, C. (2008). Doctors must put patients' needs ahead of their personal beliefs. BMJ (Clinical
research ed.), 336(7646), 685. doi:10.1136/bmj.39532.354907.DB
Eagly, A. H., Chaiken, S. (1993). The Psychology of Attitudes. Fort Worth, TX: Harcourt Brace
Jovanovich.

169
Easterby-Smith, M., Thorpe, R., Jackson, P. R. (2008). Management research (3rd ed.). London: Sage
Publications.
Eaton, S., Roberts, S., Turner, B. (2015). Delivering person centred care in long term conditions.
British Medical Journal, 350(1014), h181-h181. doi:10.1136/bmj.h181
Edwards, R., Holland, J. (2013). What is Qualitative Interviewing? London: Bloomsbury.
Egan, B. M., Zhao, Y., Axon, R. N. (2010). US trends in prevalence, awareness, treatment, and control
of hypertension, 1988-2008. The Journal of American Medical Association, 303(20), 2043-2050. doi:
10.1001/jama.2010.650
Eisenberg, L. (1977). Disease and illness: distinctions between professional and popular ideas of
sickness. Culture, Medicine and Psychiatry, 1,9-23. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/756356
Ejaz, I., Shaikh, B. T., Rizvi, N. (2011). NGOs and government partnership for health systems
strengthening: A qualitative study presenting viewpoints of government, NGOs and donors in
Pakistan. BMC Health Services Research, 11(1), 122-122. doi: 10.1186/1472-6963-11-122
Elbur, A. (2015). Level of adherence to lifestyle changes and medications among male hypertensive
patients in two hospitals in Taif; Kingdom of Saudi Arabia. International Journal of Pharmacy and
Pharmaceutical Sciences, 7(4), 168-172. Retrieved from
https://innovareacademics.in/journals/index.php/ijpps/article/view/4804
Elhani, S., Cleophas, T., Atiqi, R. (2009). Lifestyle interventions in the management of hypertension: A
survey based on the opinion of 105 practitioners. Netherlands Heart Journal, 17(1), 9-12. Retrieved
from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2626653/
El-Hay, S. A. A, El Mezayen, S. E. (2015). Knowledge and perceptions related to hypertension,
lifestyle behaviour modifications and challenges that facing hypertensive patients. Journal of Nursing
and Health Science, 4(6), 15-26. Retrieved from http://www.iosrjournals.org/iosr-jnhs/papers/vol4-
issue6/Version-1/C04611526.pdf
Ellingson, L. L. (2006). Embodied knowledge: Writing researchers’ bodies into qualitative health
research. Qualitative Health Research, 16(2), 298-310. doi:10.1177/1049732305281944
Elliott, R., Wright, L. (1999). Verbal communication: What do critical care nurses say to their
unconscious or sedated patients. Journal of Advanced Nursing, 29(6), 1412-1420. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/10354236
Elliott, N., Higgins, A. (2012). Surviving grounded theory research method in an academic world:
Proposal writing and theoretical frameworks. Grounded Theory Review: An International Journal,
11(2). Retrieved from http://groundedtheoryreview.com/2012/12/07/surviving-grounded-theory-
research-method-in-an-academic-world-proposal-writing-and-theoretical-frameworks/

170
Ely, J. W., Osheroff, J. A., Ebell, M. H., Chambliss, M. L., Vinson, D. C., Stevermer, J. J., Pifer, E. A.
(2002). Obstacles to answering doctors' questions about patient care with evidence: Qualitative
study. The British Medical Journal, 324(7339), 710-713. doi:10.1136/bmj.324.7339.710
Enlund, H., Vainio, K., Wallenius, S., Poston, J. W. (1991). Adverse drug effects and the need for drug
information. Medical Care, 29(6), 558-564. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/2046409
Entwistle, J. (2000). The Fashioned Body: Fashion, Dress and Modern Social Theory, Cambridge: Polity
Press.
Epstein, R. M., Peters, E. (2009). Beyond information: Exploring patients’ preferences. Journal of
American Medical Association. 302(2),195-7. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/19584351
Epstein, R. M., Street, R. L. (2011). The values and value of patient-centred care. Annals of Family
Medicine, 9(2), 100-103. doi: 10.1370/afm.1239
Essani, R.R., Ali, T. S. (2011). Knowledge and practice gaps among Paediatric nurses at a tertiary care
hospital Karachi Pakistan, ISRN Paediatrics. doi.org/10.5402/2011/460818.
Etherington, K. (2004). Becoming a reflexive researcher: Using ourselves in research. London: Jessica
Kingsley.
Etzelmuller, G., Weissenrieder, A. (2016). Religion and Illness. Germany: Cascade Books.
Faiz, R. (2015). work-family conflict: A case study of women in Pakistani banks. Doctoral dissertation,
The University of Hertfordshire, England.
Faghihi, S. A., Khankeh, H. R., Hosseini, S. J., Soltani Arabshahi, S. K., Faghih, Z., Parikh, S. V., Shirazi,
M. (2016). Improving continuing medical education by enhancing interactivity: Lessons from Iran.
Journal of advances in medical education & professionalism, 4(2), 54-63. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/27104199
Farmer, B. (2019, 10 March). Cash and camel steroids: Inside the anti-quackery raids targeting
Pakistan's backstreet clinics, The Telegraph.
Farooqi, Y. N. (2006). Traditional healing practices sought by Muslim psychiatric patients in Lahore,
Pakistan. International Journal of Disability, Development and Education, 53(4), 401-415. doi:
10.1080/10349120601008530
Farquhar, W. B., Edwards, D. G., Jurkovitz, C. T., Weintraubm, W. S. (2015). Dietary sodium and
health: More than just blood pressure. Journal of the American College of Cardiology, 65(10), 1042-
1050. doi: 10.1016/j.jacc.2014.12.039
Farsalinos, K., Cibella, F., Caponnetto, P., Campagna, D., Morjaria, J. B., … Polosa, R. (2016). Effect of
continuous smoking reduction and abstinence on blood pressure and heart rate in smokers

171
switching to electronic cigarettes. Internal and Emergency Medicine, 11: 85-94. doi: 10.1007/s11739-
015-1361-y
Farshidi, H., Nikparvar, M., Rostami-Qeshmi, I., Ezzati-Rad, R., Piroozan, A., Boushehri, E. (2018).
Physicians' knowledge, attitudes, and practice for hypertension management: A cross-sectional
study in Hormozgan province, Iran. ARYA Atherosclerosis, 14(3), 132-138. doi:
10.22122/arya.v14i3.1674
Faselis, C., Doumas, M., Kokkinos, J. P., Panagiotakos, D., Kheirbek, R., … Kokkinos, P. (2012). Exercise
capacity and progression from prehypertension to hypertension. Hypertension, 60(2), 333-338. doi:
10.1161/HYPERTENSIONAHA.112.196493
Feldman, S. (1988). Structure and consistency in public opinion: The role of core beliefs and values.
American Journal of Political Science, 32(2), 416-440. doi: 10.2307/2111130
Fernández-Solà, J. (2015). Cardiovascular risks and benefits of moderate and heavy alcohol
consumption. Nature Reviews Cardiology, 12(10), 576-587. doi: 10.1038/nrcardio.2015.91
Fielding, N., Thomas, H. (2016). Qualitative interviewing. In N. Gilbert & P. Stoneman (Eds.),
Researching Social Life. London: Sage Publications.
Fikree, F. F., Pasha, O. (2004). Role of gender in health disparity: The south Asian context. British
Medical Journal, 328(7443), 823-826. doi:10.1136/bmj.328.7443.823
Fischer, M. A., Stedman, M. R., Lii, J., Vogeli, C., Shrank, W. H., Brookhart, M. A., Weissman, J. S.
(2010). Primary medication non-adherence: Analysis of 195,930 electronic prescriptions. Journal of
General Internal Medicine, 25(4), 284-290. doi:10.1007/s11606-010-1253-9
FitzGerald, C., Hurst, S. (2017). Implicit bias in healthcare professionals: A systematic review. BMC
Medical Ethics, 18(1), 19. doi: 10.1186/s12910-017-0179-8
Flick, U. (1998). An Introduction to Qualitative Research. London: Sage Publications.
Foley, G., Timonen, V. (2015). Using grounded theory method to capture and analyse health care
experiences. Health Services Research, 50(4), 1195-1210. doi:10.1111/1475-6773.12275
Forouzanfar, M. H., Liu, P., Roth, G. A., Ng, M., Biryukov, S., Marczak, L., . . . Murray, C. J. L. (2017).
Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm hg, 1990-2015.
The Journal of the American Medical Association, 317(2), 165-182. doi:10.1001/jama.2016.19043
Forsth, D. (2012). Group Dynamics. Boston: Cengage.
Fowler, G. (2000). Proven strategies for smoking cessation: Adopting a global approach. The
European Journal of Public Health, 10(3), 3-4. doi: 10.1093/eurpub/10.suppl_3.3
Frank, E., Breyan, J., Elon, L. (2000). Physician disclosure of healthy personal behaviors improves
credibility and ability to motivate. Archives of family medicine, 9(3), 287-290. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/10728118/

172
Franklin, S. S., Wong, N. D. (2013). Hypertension and cardiovascular disease: Contributions of the
framingham heart study. Global Heart (Formerly CVD Prevention and Control), 8(1), 49-57.
doi:10.1016/j.gheart.2012.12.004
Freeman, T. (2006) ‘Best practice’ in focus group research: Making sense of different views. Journal
of Advanced Nursing, 56(5), 491-7. doi: 10.1111/j.1365-2648.2006.04043.x
Fuchs, F. D., Chambless, L. E., Whelton, P. K., Nieto, F. J., Heiss, G. (2001). Alcohol consumption and
the incidence of hypertension: The Atherosclerosis risk in communities study. Hypertension, 37(5),
1242-1250. doi: 10.1161/01.HYP.37.5.1242
Galletta, A. (2013). Mastering the semi-structured interview and beyond: From research design to
analysis and publication. New York: NYU Press.
Gao, K., Shi, X., Wang, W. (2017). The life-course impact of smoking on hypertension, myocardial
infarction and respiratory diseases. Scientific Reports, 7(1), 4330-4337. doi: 10.1038/s41598-017-
04552-5
Gascón, J.J., Sánchez-Ortuño, M., Llor, B., Skidmore, D., Saturno, J. P. (2004). Why hypertensive
patients do not comply with the treatment: Results from a qualitative study, Family Practice, 21(2),
125-130. doi: 10.1093/fampra/cmh202
Geboers, B., Brainard, J. S., Loke, Y. K., Jansen, C. J. M., Salter, C., Reijneveld, S. A., deWinter, A. F.
(2015). The association of health literacy with adherence in older adults, and its role in interventions:
A systematic meta-review. BMC Public Health, 15. 903. doi: 10.1186/s12889-015-2251-y
Gergen, K. J. (2015). An invitation to social construction (Third ed.). Los Angeles: Sage.
Gerhardt, U. (1990). Qualitative research on chronic illness: The issue and the story, Social Science
and Medicine, 30(11), 1149-1159. Retrieved from
http://www.sciencedirect.com/science/article/pii/0277-9536(90)90255-Q
George, C., Dhanya, R., Gift, N., Devashri, M., Tata, R. (2016). Barriers to cardiovascular disease risk
reduction: Does physicians’ perspective matter? Indian Heart Journal, 68(3), 278-285. doi:
10.1016/j.ihj.2015.08.014
Ghaffar, A., Kazi, B. M., Salman, M. (2000). Health care systems in transition III. Pakistan, Part I. An
overview of the health care system in Pakistan. Journal of Public Health Medicine, 22(1), 38-42. doi:
10.1093/pubmed/22.1.38
Ghandour, L., Chalak, A., El-Aily A, Yassin, N., Nakkash, R., Tauk, M., El Salibi, N., Heffron, M., Afifi, R.
(2016). Alcohol consumption in the Arab region: what do we know, why does it matter, and what are
the policy implications for youth harm reduction? The International Journal on Drug Policy. 28. 10-
33. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/26547300
Gignac, M. A. M., Davis, A. M., Hawker, G., Wright, J. G., Mahomed, N., … Badley, E. M. (2006).
"What do you expect? You're just getting older": A comparison of perceived osteoarthritis-related

173
and aging-related health experiences in middle- and older-age adults. Arthritis Care and Research,
55(6), 905-912. doi: 10.1002/art.22338
Gilbert, D. T., Hixon, J. G. (1991). The trouble of thinking: Activation and application of stereotypic
beliefs. Journal of Personality and Social Psychology, 60(4), 509-517. doi: 10.1037/0022-
3514.60.4.509
Glaser, B. G., Strauss, A. L. (1965). Awareness of dying. Chicago: Aldine Publishing.
Glaser, B. G., Strauss, A. L. (1967). The Discovery of Grounded Theory: Strategies for Qualitative
Research. Hawthorne: Aldine de Gruyter.
Glaser, B. G. (1978). Theoretical Sensitivity: Advances in the Methodology of Grounded Theory. Mill
Valley: Sociology Press.
Glouberman, S. (2013). The role of medical superintendent. Retrieved from
https://healthandeverythingblog.wordpress.com/2013/12/19/the-role-of-medical-
superintendent/comment-page-1/
Gohar Wajid, D. A., Al Massoud, H. A. (2002) Prospects, prerequisites and challenges for developing
a healthcare quality improvement strategy for Pakistani healthcare system. Pakistan Seventh
International Convention on Quality Improvement, 1-7.
Golshahi, J., Ahmadzadeh, H., Sadeghi, M., Mohammadifard, N., Pourmoghaddas, A. (2015). Effect of
self-care education on lifestyle modification, medication adherence and blood pressure in
hypertensive adults: Randomized controlled clinical trial. Advanced Biomedical Research, 4(204). doi:
10.4103/2277-9175.166140
Gopalakrishnan, S., Ganeshkumar, P. (2013). Systematic reviews and meta-analysis: Understanding
the best evidence in primary healthcare. Journal of Family Medicine and Primary Care, 2(1), 9-14.
doi: 10.4103/2249-4863.109934
Gowani, A., Ahmed, H. I., Khalid, W., Muqeet, A., Abdullah, S., … Kamal, A. K. (2016). Facilitators and
barriers to NCD prevention in Pakistanis - invincibility or inevitability: A qualitative research study.
BMC Research Notes, 9(282), doi: 10.1186/s13104-016-2087-2
Graham, S., Brookey, J. (2008). Do patients understand? The Permanente journal, 12(3), 67-69. doi:
10.7812/tpp/07-144
Gredler, E. M. (1997). Learning and Instruction. Theory into Practice. New Jersey: Merrill.
Gregory, V. G., Dowd, O. (2004). Doctor-patient communication: An introduction for medical
students. Available at: https://core.ac.uk/download/pdf/70359931.pdf
Gregory, V. G., Dowd, V. (2004). Doctor-patient communication: An introduction for medical
students. Available at https://core.ac.uk/download/pdf/70359931.pdf

174
Green, M. L., Ruff, T. R. (2005). Why do residents fail to answer their clinical questions? A qualitative
study of barriers to practicing evidence-based medicine. Academic Medicine, 80(2), 176-182.
doi:10.1097/00001888-200502000-00016
Green, L. A., Phillips, R. L., Fryer, G. E. (2003). The nature of primary medical care. In R. Jones, N.
Britten, L. Culpepper, et al. (Eds.) The Oxford Textbook of Primary Care. Oxford: Oxford University
Press.
Greenhalgh, T. (2009). Patient and public involvement in chronic illness: Beyond the expert patient.
The British Medical Journal, 338(171), b49-b49. doi: 10.1136/bmj.b49
Groenewald, T. (2004). A phenomenological research design illustrated. International Journal of
Qualitative Methods, 42-55. Retrieved from https://doi.org/10.1177/160940690400300104
Grossman, E., Verdecchia, P., Shamiss, A., Angeli, F., Reboldi, G. (2011). Diuretic treatment of
hypertension. Diabetes care, 34(2), 313-319. doi: 10.2337/dc11-s246
Grove, S. K., Burns, N., Gray, J. R. (2014). Understanding Nursing Research: Building an Evidence-
based Practice. St Louis: Elsevier Saunders.
Grundmann, R. (2017). The problem of expertise in knowledge societies. Minerva, 55(1), 25-48. doi:
10.1007/s11024-016-9308-7
Gu, J. W., Bailey, A. P., Tan, W., Shparago, M., Young, E. (2008). Long-term high salt diet causes
hypertension and decreases renal expression of vascular endothelial growth factor in Sprague-
Dawley Rats. Journal of the American Society of Hypertension, 2(4), 275-285. doi:
10.1016/j.jash.2008.03.001
Guba, E. G., Lincoln, Y. S. (1989). Fourth Generation Evaluation. Newbury Park: Sage Publications.
Guba, E. G., Lincoln, Y. S. (1994). Competing paradigms in qualitative research. In N. K. Denzin & Y. S.
Lincoln (Eds.), Handbook of Qualitative Research. Thousand Oaks: Sage Publications.
Gupta, R., Guptha, S. (2010). Strategies for initial management of hypertension. Indian Journal of
Medical Research, 132(5), 531-542 Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3028941/
Ha, J. F., Longnecker, N (2010). Doctor-patient communication: A review. The Ochsner Journal, 10(1),
38-43. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3096184/
Ha, S. K. (2014). Dietary Salt Intake and Hypertension. Electrolyte & Blood Pressure, 12(1), 7-18. doi:
10.5049/EBP.2014.12.1.7
Haddad, M., Waqas, A., Qayyum, W., Shams, M., Malik, S. (2016). The attitudes and beliefs of
Pakistani medical practitioners about depression: A cross-sectional study in Lahore using the revised
depression attitude questionnaire (R-DAQ). BMC Psychiatry, 16(1), 349. doi: 10.1186/s12888-016-
1069-1

175
Haider, W., Chaudhry, M.A., (2008). Prevalence of alcoholism in the Punjab, Pakistan. Available at:
https://www.semanticscholar.org/paper/PREVALENCE-OF-ALCOHOLISM-IN-THE-PUNJAB%2C-
PAKISTAN-Haider-Chaudhry/93786e22a3a4ac39ec548b2409fcb5d1f05305cf
Haleem, S. (2013). Pakistan - Culture Smart! The Essential Guide to Customs & Culture. England:
Kuperard.
Halpern, J. (2003). What is clinical empathy? Journal of general internal medicine, 18(8), 670-674.
doi:10.1046/j.1525-1497.2003.21017.x
Hallberg, L. R. M. (2006). The "core category" of grounded theory: Making constant comparisons.
International Journal of Qualitative Studies on Health and Well-being, 1(3), 141-148. doi:
10.1080/17482620600858399
Halligan, P. W. (2006). Beliefs: Shaping experience and understanding illness. In P.W. Halligan & M.
Aylward (Eds.) The Power of Belief: Psychosocial Influence on Illness, Disability and Medicine. Oxford:
Oxford University Press.
Halligan, P. W. (2007). Belief and illness. The Psychologist, 6(20), 358-361. Retrieved from
https://thepsychologist.bps.org.uk/volume-20/edition-6/belief-and-illness
Hamer, M. (2010). Adherence to healthy lifestyle in hypertensive patients: Ample room for
improvement? Journal of Human Hypertension, 24(9), 559-560. doi:10.1038/jhh.2010.61
Hannay, D. R. (1979). The Symptom Iceberg. A study of Community Health. London: Routledge and
Kegan Paul.
Hardey, M. (1999). Doctor in the house: The internet as a source of lay health knowledge and the
challenge to expertise. Sociology of Health & Illness, 21(6), 820-835. doi:10.1111/1467-9566.00185
Hardy, C. (2017). Empathizing with patients: The role of interaction and narratives in providing
better patient care. Medicine, Health Care and Philosophy, 20(2), 237-248. doi:10.1007/s11019-016-
9746-x
Harmon, G., Lefante, J., Krousel-Wood, M. (2006). Overcoming barriers: The role of providers in
improving patient adherence to antihypertensive medications. Current Opinion in Cardiology, 21(4),
310-315. doi: 10.1097/01.hco.0000231400.10104.e2
Hashmi, S. K., Afridi, M. B., Abbas, K., Sajwani, R. A., Saleheen, D., Frossard, P. M., … Ahmad, U.
(2007). Factors associated with adherence to anti-hypertensive treatment in Pakistan. PLoS One,
2(3), e280. doi: 10.1371/journal.pone.0000280
Hassan, N. B., Hasanah, C. I., Foong, K., Naing, L., Awang, R., … Rahman, A. R. (2006). Identification of
psychosocial factors of noncompliance in hypertensive patients. Journal of Human Hypertension,
20(1), 23-29. doi: 10.1038/sj.jhh.1001930
Hassin, R. R., Uleman, J. S., Bargh, J. A. (Eds.) (2005). The New Unconscious. New York: Oxford
University Press.

176
Hatah, E., Lim, K. P., Ali, A. M., Mohamed, S. N., Islahudin, F. (2015). The influence of cultural and
religious orientations on social support and its potential impact on medication adherence. Patient
Preference and Adherence, 9, 589-596. doi: 10.2147/PPA.S79477
Hausman, A. V., Mader, D. (2004). Measuring social aspects in the physician/patient relationship.
Health Mark Q, 21(3), 3-26. doi: 10.1300/J026v21n03_02
Hayashi, T., Tsumura, K., Suematsu, C., Okada, K., Fujii, S., Endo, G. (1999). Walking to work and the
risk for hypertension in men: the Osaka Health Survey. Annals of Internal Medicine, 131(1), 21-26.
Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/10391811
Hayfield, N., Huxley, C. (2015). Insider and outsider perspectives: Reflections on researcher identities
in research with lesbian and bisexual women. Qualitative Research in Psychology, 12(2), 91-106.
doi:10.1080/14780887.2014.918224
Haynes, R. B., Devereaux, P. J., Guyatt, G. H. (2002). Clinical expertise in the era of evidence-based
medicine and patient choice. Evidence-Based Medicine, 7(2), 36-38. doi:10.1136/ebm.7.2.36
He, F. J., MacGregor, G. A. (2009). A comprehensive review on salt and health and current
experience of worldwide salt reduction programmes. Journal of Human Hypertension, 23(6), 363-
384. doi: 10.1038/jhh.2008.144
He, F. J., Li, J., MacGregor, G. A. (2013). Effect of longer term modest salt reduction on blood
pressure: Cochrane systematic review and meta-analysis of randomised trials. British Medical
Journal, 346. Retrieved from http://www.bmj.com/content/346/bmj.f1325.abstract
Hechter, M., Opp, K. D. (2001). Social Norms. New York: Sage Publications.
Helman, C. G. (2007). Culture, Health and Illness. London: Hodder Arnold.
Hennink, M., Hutter, I., Bailey, A. (2001). Qualitative Research Methods. London: Sage Publications.
Henwood, F., Wyatt, S., Hart, A., Smith, J. (2003). ‘Ignorance is bliss sometimes’: Constraints on the
emergence of the ‘informed patient’ in the changing landscapes of health information. Sociology of
Health & Illness, 25(6), 589-607. doi: 10.1111/1467-9566.00360
Heritage, J., Maynard, D. W. (2006). Communication in medical care: Interaction between primary
care physicians and patients (1st ed.). Cambridge, Cambridge University Pres.
doi:10.1017/CBO9780511607172
Herman, L. L., Bashir, K. (2019). Angiotensin Converting Enzyme Inhibitors (ACEI). Retrieved from
https://www.ncbi.nlm.nih.gov/books/NBK431051/
Herzlich, C., Pierret, J. (1987). Illness and Self in Society. Baltimore: John Hopkins University Press.
Heymann, A. D., Gross, R., Tabenkin, H., Porter, B., Porath, A. (2011). Factors associated with
hypertensive patients’ compliance with recommended lifestyle behaviors. Israel Medical Association
Journal, 13(9), 553-557.

177
Higher Education Commission, Pakistan. (2019). Retrieved from
https://www.hec.gov.pk/english/pages/home.aspx
Hill, M. N., Miller, N. H., DeGeest, S. (2010). ASH position paper: Adherence and persistence with
taking medication to control high blood pressure. Journal of Clinical Hypertension, 12(10), 757-764.
doi: 10.1111/j.1751-7176.2010.00356.x
Hofer, B., Pintrich, P. (1997). The development of epistemological theories: Beliefs about knowledge
and knowing their relation to learning. Reviews of educational research, 1(67), doi: 10.2307/1170620
Holloway, I., Wheeler, S. (2002). Qualitative Research in Nursing. Oxford: Blackwell Publishing.
Holly, D. C., Saimbert, M. K., Salmond, D. S. (2012). Comprehensive Systematic Review for Advanced
Nursing Practice (1st ed.). New York: Springer Publishing Company.
Honebein, P. C. (1996). Seven goals for the design of constructivist learning environments. In
Wilson, Brent. G. (Ed.). (1996) Constructivist learning environments: case studies in instructional
design. Educational Technology Publications. New Jersey: Englewood Cliffs.
Homan, R. (2001). The principle of assumed consent: The ethics of gatekeeping. Journal of
Philosophy of Education, 35(3), 329-343. doi:10.1111/1467-9752.00230
Hootman, J. M., Macera, C. A., Ainsworth, B. E., Addy, C. L., Martin, M., Blair, S. N. (2002).
Epidemiology of musculoskeletal injuries among sedentary and physically active adults. Medicine &
Science in Sports & Exercise, 34(5), 838-844. doi: 10.1097/00005768-200205000-00017
Horne, R., Chapman, S. C., Parham, R., Freemantle, N., Forbes, A., Cooper, V. (2013). Understanding
patients' adherence-related beliefs about medicines prescribed for long-term conditions: a meta-
analytic review of the Necessity-Concerns Framework. PloS one, 8(12), e80633.
doi:10.1371/journal.pone.0080633
Howie, J. G., Porter, A. M., Heaney, D. J. Hopton, J. L. (1991). Long to short consultation ratio: a proxy
measure of quality of care for general practice. British Journal of General Practice, 41, 48-54.
Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1371550/?tool=pmcentrez&report=abstract
Hsiao, C. Y., Chang, C., Chen, C. D. (2012). An investigation on illness perception and adherence
among hypertensive patients. Kaohsiung Journal of Medical Sciences, 28(8), 442-447. doi:
10.1016/j.kjms.2012.02.015
Hudson, L., Ozanne, J. (1988). Alternative ways of seeking knowledge in consumer research. Journal
of Consumer Research, 14(4), 508-521. Retrieved from
https://www.jstor.org/stable/2489157?seq=1#page_scan_tab_contents
Hugtenburg, J. G., Timmers, L., Elders, P. J., Vervloet, M., van Dijk, L. (2013). Definitions, variants, and
causes of nonadherence with medication: A challenge for tailored interventions. Patient preference
and adherence, 7, 675-682. doi: 10.2147/PPA.S29549

178
Hughes, J., Jones, S., (2003). Reflections on the use of grounded theory in interpretive information
systems research, Electronic Journal of Information System Evaluation, Retrieved from
https://pdfs.semanticscholar.org/4938/016f7ea3e6e2e09e683b04f8bcd1681a53e8.pdf
Hunte, P., Sultana, F. (1992). Health-seeking behavior and the meaning of medications in
Balochistan, Pakistan. Social Science & Medicine, 34(12), 1385-1397. Retrieved from
https://doi.org/10.1016/0277-9536(92)90147-I
Hussain, S., Malik, S., Hayat, M. (2009). Demographic transition and ecnomic growth in Pakistan.
European Journal of Scientific Research, 31(3), 491-499. Retrieved from
https://www.researchgate.net/profile/Shahnawaz_Malik/publication/228856198_Demographic_tra
nsition_and_economic_growth_in_Pakistan/links/55b75d5f08ae092e96571222/Demographic-
transition-and-economic-growth-in-Pakistan.pdf
Hussain, I. M., Naqvi, Baqir S., Qasim, Rao M., Ali, Nasir. (2015). Current trends in treatment of
hypertension in Karachi and cost minimization possibilities. Pakistan Journal of Medical Sciences,
31(5), 1021-1026.10.12669/pjms.315.7438
Hyman, D.J., Pavlik, V. N. (2000). Self-reported hypertension treatment practices among primary
care physicians: blood pressure thresholds, drug choices, and the role of guidelines and evidence-
based medicine. Archivers of Internal Medicine, 160 (15), 2281-2286. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/10927724
Ibrahim, M. M., Damasceno, A. (2012). Hypertension in developing countries. Lancet, 380(9841),
611-619. doi: 10.1016/s0140-6736(12)60861-7
Ibrahim, I. R., Hassali, M. A., Saleem, F., Al Tukmagi, H. F. (2016). A qualitative insight on
complementary and alternative medicines used by hypertensive patients. Journal of Pharmacy &
Bioallied Sciences, 8(4), 284-288. doi: 10.4103/0975-7406.199349
Ip, E. H., T. Church, S. A. Marshall, Q. Zhang, A. P. Marsh, J. Guralnik, A. C. King and W. J. Rejeski
(2013). Physical activity increases gains in and prevents loss of physical function: Results from the
lifestyle interventions and independence for elders pilot study. The Journals of Gerontology Series A
Biological Sciences Medical Sciences, 68(4), doi 426-432.10.1093/gerona/gls186
Irfan, S. M., Ijaz, A. (2011). Comparison of service quality between private and public hospitals:
Empirical evidence from Pakistan. Journal of Quality and Technology Management, 7(1), 1-22.
Retrieved from http://results.pu.edu.pk/images/journal/iqtm/PDF-FILES/01-
Comparison%20of%20Service%20Quality%2026-5-2011.pdf
Irfan, M., Haque, A. S, Awan, S, Khan, J. A. (2014). Reasons of failure to quit smoking: a cross
sectional survey in major cities of Pakistan. European Respiratory Journal, 44(58). Retrieved from
https://erj.ersjournals.com/content/44/Suppl_58/P4466
Irving, G., Neves, A. L., Dambha-Miller, H., Oishi, A., Tagashira, H., Verho, A., Holden, J. (2017).
International variations in primary care physician consultation time: A systematic review of 67
countries. BMJ Open, 7(10), e017902. doi:10.17863/CAM.21761
179
Ishtiaq, S., Ilyas, U., Naz, S., Altaf, R., Afzaal, H., … Muhammad, S. (2017). Assessment of the risk
factors of hypertension among adult & elderly group in twin cities of Pakistan. Journal of Pakistan
Medical Association, 67(11), 1664-1669. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/29171556
Islam, N. (2004). Sifarish, sycophants, power and collectivism: Administrative culture in Pakistan.
International Review of Administrative Sciences, 70(2), 311-330. doi: /10.1177/0020852304044259
Israel, M., Hay, I. (2006). Research Ethics for Social Scientists. London: Sage Publications.
Itrat, A., Taqui, A. M., Qazi, F., Qidwai, W. (2007). Family systems: Perceptions of elderly patients and
their attendants presenting at a university hospital in Karachi, Pakistan. Journal of Pakistan Medical
Association, 57(2), 106-110. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/17370799
Iwelunmor, J., Newsome, V., Airhihenbuwa, C. O. (2014). Framing the impact of culture on health: A
systematic review of the PEN-3 cultural model and its application in public health research and
interventions. Ethnicity & health, 19(1), 20-46. doi: 10.1080/13557858.2013.857768
Jafar, T. H., Jessani, S., Jafary, F. H., Ishaq, M., Orakzai, R., … Chaturvedi, N. (2005). General
practitioners' approach to hypertension in urban Pakistan: Disturbing trends in practice. Circulation,
111(10), 1278-1283. doi: 10.1161/01.cir.0000157698.78949.d7
Jafar, T. H., Haaland, B. A., Rahman, A., Razzak, J. A., Bilger, M., … Hyder, A. A. (2013). Non-
communicable diseases and injuries in Pakistan: Strategic priorities. The Lancet, 381(9885), 2281-
2290. doi: 10.1016/S0140-6736(13)60646-7
Jagosh, J., Donald Boudreau, J., Steinert, Y., MacDonald, M. E., Ingram, L. (2011). The importance of
physician listening from the patients’ perspective: Enhancing diagnosis, healing, and the doctor-
patient relationship. Patient Education and Counselling, 85(3), 369-374.
doi:10.1016/j.pec.2011.01.028
Jakulj, F., Zernicke, K., Bacon, S. L., van Wielingen, L. E., Key, B. L., … Campbell, T. S. (2007). A high-fat
meal increases cardiovascular reactivity to psychological stress in healthy young adults. The Journal
of Nutrition, 137(4), 935-939. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/17374657
Jalil, A., Zakar, R., Zakar, M. Z., Fischer, F. (2017). Patient satisfaction with doctor-patient
interactions: A mixed methods study among diabetes mellitus patients in Pakistan. BMC Health
Services Research, 17, 155. doi: 10.1186/s12913-017-2094-6
Jallinoja, P., Absetz, P., Kuronen, R., Nissinen, A., Talja, M., … Patja, K. (2007). The dilemma of patient
responsibility for lifestyle change: Perceptions among primary care physicians and nurses.
Scandinavian Journal of Primary Health Care, 25(4), 244-249. doi: 10.1080/02813430701691778
James, P. A., Oparil, S., Carter, B. L., Cushman, W. C., Dennison-Himmelfarb, C., Handler, J., ... Ortiz,
E. (2014). Evidence-based guideline for the management of high blood pressure in adults: Report
from the panel members appointed to the eighth joint national committee (JNC 8). Journal of
American Medical Association, 311(5), 507-520. doi: 10.1001/jama.2013.284427

180
Jarari, N., Rao, N., Peela, J. R., Ellafi, K. A., Shakila, S., Said, A. R., … Peela, L. T. (2016). A review on
prescribing patterns of antihypertensive drugs. Clinical hypertension, 22, 7. doi:10.1186/s40885-016-
0042-0
Jaubert, M. P., Jin, Z., Russo, C., Schwartz, J. E., Homma, S., … Di Tullio, M. R. (2014). Alcohol
consumption and ambulatory blood pressure: A community-based study in an elderly cohort.
American journal of hypertension, 27(5), 688-694. doi: 10.1093/ajh/hpt235
Javadi, H., Barikani, A., Jalilolghadr, S. (2005). Evaluation of Qazvin general practitioners' attitude on
hypertension. Journal of Qazvin University of Medical Sciences, 8(4), 53-58. Retrieved from
https://pdfs.semanticscholar.org/2a42/c48d2aeddb1e30a85a1395e088d5f043d332.pdf
Jepson, R., Harris, F. M., Bowes, A., Robertson, R., Avan, G., Sheikh, A. (2012). Physical activity in
South Asians: An in-depth qualitative study to explore motivations and facilitators. PLoS One, 7(10),
e45333. doi: 10.1371/journal.pone.0045333
Jimmy, B., Jose, J. (2011). Patient medication adherence: Measures in daily practice. Oman Medical
Journal, 26(3), 155-159. doi: 10.5001/omj.2011.38
Jin, J., Sklar, G. E., Min Sen Oh, V., Chuen Li, S. (2008). Factors affecting therapeutic compliance: A
review from the patient’s perspective. Therapeutics and Clinical Risk Management, 4(1), 269-286.
Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2503662/
Johansson, K., Bendtsen, P., Åkerlind, I. (2005). Advice to patients in Swedish primary care regarding
alcohol and other lifestyle habits: How patients report the actions of GPs in relation to their own
expectations and satisfaction with the consultation. European Journal of Public Health, 15(6), 615-
620. doi: 10.1093/eurpub/cki046
John, W. S., Johnson, P. (2000). The pros and cons of data analysis software for qualitative research.
Journal of Nursing Scholarship, 32(4), 393-397. doi:10.1111/j.1547-5069.2000.00393.x
Jones, C., Jack, B. (1999). Dilemmas in the ethics of health-care research. Professional Nurse, 14(7),
452-455. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/10347524
Jooma, R., Sabatinelli, G. (2014). Political determinants of health: Lessons for Pakistan. Pakistan
Journal of Medical Sciences, 30(3), 457-461. doi: 10.12669/pjms.303.5487
Judith A., Holton, (2007). The coding process and its challenges’ in Antony Bryant and Kathy
Charmaz, eds., The Sage Handbook of Grounded Theory, London: Sage.
Jung, M. H., Ihm, S. H. (2019). Improving the quality of hypertension management: Multifaceted
approach. Korean circulation journal, 49(6), 528-531. doi:10.4070/kcj.2019.0055
Kamran, A., Azadbakht, L., Sharifirad, G., Mahaki, B., Sharghi, A. (2014). Sodium intake, dietary
knowledge, and illness perceptions of controlled and uncontrolled rural hypertensive patients.
International Journal of Hypertension, 2014: 245480. doi: 10.1155/2014/245480
181
Kamran, A., Sadeghieh Ahari, S., Biria, M., Malepour, A., Heydari, H. (2014). Determinants of
patient’s adherence to hypertension medications: Application of health belief model among rural
patients. Annals of Medical and Health Sciences Research, 4(6), 922-927. doi: 10.4103/2141-
9248.144914
Kaplan, N. M. (2008). Beta-blockers in hypertension. Journal of the American College of Cardiology,
52(18), 1490-1491. doi: 10.1016/j.jacc.2008.08.008
Karmali, K. N., Lloyd-Jones, D. M., van der Leeuw, J., Goff, D. C., Rahimi, K., Yusuf, S., …. (2018). Blood
pressure-lowering treatment strategies based on cardiovascular risk versus blood pressure: A meta-
analysis of individual participant data. PLoS Medicine, 15(3), e1002538. doi:
10.1371/journal.pmed.1002538
Kassam-Khamis, T., Judd, P. A., Thomas, J. E. (2000). Frequency of consumption and nutrient
composition of composite dishes commonly consumed in the UK by South Asian Muslims originating
from Bangladesh, Pakistan And East Africa (Ismailis). Journal of Human Nutrition and Dietetics,
13(3), 185-196. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/12383125
Kaur, K., Sharma, S. S, Kaur, G., Deepika, Sharma, D., Rai, H. (2007). Practices of hypertensive
patients visiting O.P.D at D.M.C & H, Ludhiana. Nursing and Midwifery Research Journal, 3(2), 65-70.
Retrieved from http://medind.nic.in/nad/t07/i2/nadt07i2p65.pdf
Kearney, P. M., Whelton, M., Muntner, P., Whelton, P. K., He, J. (2005). Global burden of
hypertension: Analysis of worldwide data. Lancet, 365(9455), 217-223. doi: 10.1016/s0140-
6736(05)17741-1
Kelak, J. A., Cheah, W. L., Safii, R. (2018). Patient's decision to disclose the use of traditional and
complementary medicine to medical Doctor: A descriptive phenomenology study. Evidence-based
complementary and alternative medicine, eCAM, 2018, 4735234. doi:10.1155/2018/4735234
Kelishadi, R., Mokhtari, M. R., Tavasoli, A. A., Khosravi, A., Ahangar-Nazari, I., Sabet, B., Kazemi, A.,
Amini, A. (2007). Determinants of tobacco use among youths in Isfahan, Iran. International Journal of
Public Health, 52(3), 173-179. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/17958284
Kelman, I., Field, J., Suri, K., Bhat, G. M. (2018). Disaster diplomacy in Jammu and Kashmir.
International Journal of Disaster Risk Reduction, 31, 1132-1140. doi: 10.1016/j.ijdrr.2018.02.007
Kelle, U. (2007) The Development of Categories: Different approaches in grounded theory, in Antony
Bryant and Kathy Charmaz, eds., Sage Handbook of Grounded Theory, London: Sage
Kelly, M. P., Barker, M. (2016). Why is changing health-related behaviour so difficult? Public Health,
136, 109-116. doi: 10.1016/j.puhe.2016.03.030
Kennedy, B. M., Rehman, M., Johnson, W. D., Magee, M. B., Leonard, R., Katzmarzyk, P. T. (2017).
Healthcare providers versus patients' understanding of health beliefs and values. Patient Experience
Journal, 4(3), 29. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/29308429

182
Kerr, A., Cunningham-Burley, S., Tutton, R. (2007). Shifting subject positions: Experts and lay people
in public dialogue. Social Studies of Science, 37(3), 385-411. doi: 10.1177/030631270606849
Kerse, N., Buetow, S., Mainous, A.G. Young, G., Coster, G., Arroll, B., (2004). Physician-patient
relationship and medication compliance: A primary care investigation, Annals of Family Medicine.
2(5), 455-461. Retrieved from www.ncbi.nlm.nih.gov/pubmed/15506581
Ke, J., Wenglensky, S. (2010). Grounded theory. Retrieved from: http://avantgarde-
jing.blogspot.com/2010/03/grounded-theory.html
Kee, J. W. Y., Khoo, H. S., Lim, I., Koh, M. Y. H. (2018). Communication skills in patient-doctor
interactions: Learning from patient complaints. Health Professions Education, 4(2), 97-106. Retrieved
from https://www.sciencedirect.com/science/article/pii/S2452301116301225
Khalid, F., Abbasi, N. A. (2018). Challenges faced by Pakistani healthcare system: Clinician’s
perspectives, Journal of the College of Physicians and Surgeons Pakistan, 28(12), 899-901. Retrieved
from https://jcpsp.pk/archive/2018/Dec2018/01.pdf
Khalil, S. A., Elzubier, A. G. (1997). Drug compliance among hypertensive patients in Tabuk, Saudi
Arabia Journal of Hypertension, 15(5), 561-565. doi: 10.1097/00004872-199715050-00013
Khalique, H. (2007). The Urdu-English relationship and its impact on Pakistan’s social development.
The Annual of Urdu Studies, (22), 99-112. Retrieved from
http://www.urdustudies.com/pdf/22/09HKhalique.pdf
Khan, M. I., Bhuiya, A., Chowdhury, M. (1996). Cultural construction of health and institutional
measures of change in rural Bangladesh: cases of BRAC's village organization and ICDDR,B's MCH-FP
programmes. Glimpse, 18(1), 8. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/12291504
Khan, M. M., Van den Heuvel, W. (2007). The impact of political context upon the health policy
process in Pakistan. Public Health, 121(4), 278-286. doi: 10.1016/j.puhe.2006.09.015
Khan, S., Mushtaq, S., Arshad, N., Lone, N. A. (2012). The current status of bioethics research in
Pakistan. Scientific reports, 1, 208. doi:10.4172/scientificreports.208
Khan, M. S., Bawany, F. I., Mirza, A., Hussain, M., Khan, A., Lashari, M. N. (2014). Frequency and
predictors of non-compliance to dietary recommendations among hypertensive patients. Journal of
Community Health, 39(4), 732-736. doi: 10.1007/s10900-014-9819-9
Khan, Z., Ahmed, M., Ghufran., Hameed, A. (2015) Assessing the primary causes of hypertension in
Khyber Pakhtunkhwa, Pakistan, Journal of Biology and Life Science, 6(2), 24-36. Retrieved from
http://www.macrothink.org/journal/index.php/jbls/article/view/7119
Khatib, R., Schwalm, J., Yusuf, S., Haynes, R. B., McKee, … Nieuwlaat, R. (2014). Patient and
healthcare provider barriers to hypertension awareness, treatment and follow up: A systematic
review and meta-analysis of qualitative and quantitative studies. PLoS One, 9(1), e84238. doi:
10.1371/journal.pone.0084238

183
Khattak, A., Alvi, M., Yousaf, M. (2012). Patient satisfaction - A comparison between public & private
hospitals of Peshawar. International Journal of Collaborative Research on Internal Medicine & Public
Health 4(5), 713-722. Retrieved from
https://www.researchgate.net/publication/268435751_Patient_Satisfaction_-
_A_Comparison_between_Public_Private_Hospitals_of_Peshawar
Khayyat, S. M., Khayyat, S. M., Hyat Alhazmi, R. S., Mohamed, M. M., Abdul Hadi, M. (2017).
Predictors of medication adherence and blood pressure control among Saudi hypertensive patients
attending primary care clinics: A cross-sectional study. PLoS One, 12(1), e0171255. doi:
10.1371/journal.pone.0171255
Khowaja, K. (2009). International perspective: Healthcare systems and care delivery in Pakistan
Journal of Nursing Adminstration, 39(6), 263-265.doi: 10.1097/NNA.0b013e3181a96473
Khuwaja, A. K., Kadir, M. A. (2010). Gender differences and clustering pattern of behavioural risk
factors for chronic non-communicable diseases: Community-based study from a developing country.
Chronic Illness, 6(3), 163-170. doi: 10.1177/1742395309352255
Kim, B. (2001). Social Constructivism. In M. Orey (Ed.), Emerging perspectives on learning, teaching
and technology.
Kim, S. S., Kaplowitz, S., Johnston, M. V. (2004). The effects of physician empathy on patient
satisfaction and compliance. Evaluation & the Health Professions, 27(3), 237-251.
doi:10.1177/0163278704267037
Kim, H. S., Cho, J. H., Yoon, K. H. (2015). New directions in chronic disease management.
Endocrinology and Metabolism (Seoul, Korea), 30(2), 159-166. doi: 10.3803/EnM.2015.30.2.159
Kim, Y., Jung, Y. H., Saposnik, G. (2016). Traditional risk factors for stroke in East Asia. Journal Of
Stroke, 18(3), 273-285. Retrieved from
http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=27733028&site=ehost-live
King, A., Hoppe, R. B. (2013). "Best practice" for patient-centred communication: a narrative review.
Journal of graduate medical education, 5(3), 385-393. doi:10.4300/JGME-D-13-00072.1
Kintscher, U. (2013). The burden of hypertension. Eurointervention, 9(R), 12-15. doi:
10.4244/EIJV9SRA3
Kirmayer, L. J., Groleau, D., Looper, K. J., Dao, M. D. (2004). Explaining medically unexplained
symptoms: 1. Canadian Journal of Psychiatry, 49(10), 663.
Kittler, P., Sucher, K. P., Nelms, M. N. (2012). Food and Culture. Belmont: Thomson Wadsworth.
Kjeldsen, S., Feldman, R. D., Lisheng, L., Mourad, J.- J., Chiang, C.-E., … Williams, B. (2014). Updated
national and international hypertension guidelines: A review of current recommendations. Drugs,
74(17), 2033-2051. doi: 10.1007/s40265-014-0306-5

184
Kjeldsen, S. (2018). Hypertension and cardiovascular risk: General aspects. Pharmacological
Research, 129, 95-99. doi: 10.1016/j.phrs.2017.11.003
Klatsky, A. L. (2004). Alcohol-associated hypertension: When one drinks makes a difference.
Hypertension, 44(6), 805-806. doi: 10.1161/01.hyp.0000146538.26193.60
Klatsky, A. L., Koplik, S., Gunderson, E., Kipp, H., Friedman, G. D. (2006). Sequelae of systemic
hypertension in alcohol abstainers, light drinkers, and heavy drinkers. The American Journal of
Cardiology, 98(8), 1063-1068. doi: 10.1016/j.amjcard.2006.05.029
Kleinman, A. (1988). The Illness Narratives: Suffering, Healing, and the Human Condition. New York:
Basic Book.
Kleinman, A., Benson, P. (2006). Anthropology in the clinic: The problem of cultural competency and
how to fix it. PLoS Medicine, doi:10.1371/journal.pmed.0030294.
Kleinsinger, F. (2010). Working with the noncompliant patient. The Permanente journal, 14(1), 54-60.
Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2912714/
Koenig, H. G., McCullough, M. E., Larson, D. B. (2001). Handbook of Religion and Health. New York:
Oxford University Press.
Koenig, H. G. (2012). Religion, spirituality, and health: The research and clinical implications.
International Scholarly Research Notices Psychiatry, 2012. 278730. doi: 10.5402/2012/278730
Koppen, I. J. N., Kuizenga-Wessel, S., Saps, M., Di Lorenzo, C., Benninga, M. A., … Tabbers, M. M.
(2016). Functional defecation disorders and excessive body weight: A systematic review. Paediatrics,
138(3), e20161417. doi:10.1542/peds.2016-1417
Kornhaber, R., Walsh, K., Duff, J., Walker, K. (2016). Enhancing adult therapeutic interpersonal
relationships in the acute health care setting: an integrative review. Journal of multidisciplinary
healthcare, 9, 537-546. doi:10.2147/JMDH.S116957
Kourkouta, L., Papathanasiou, I. V. (2014). Communication in nursing practice. Materia socio-medica,
26(1), 65-67. doi:10.5455/msm.2014.26.65-67
Kressin, N. R., Wang, F., Long, J., Bokhour, B. G., Orner, M. B., … Berlowitz, D. R. (2007). Hypertensive
patients’ race, health beliefs, process of care, and medication adherence. Journal of General Internal
Medicine, 22(6), 768-774. doi: 10.1007/s11606-007-0165-9
Kronish, I. M., Leventhal, H., Horowitz, C. R. (2012). Understanding minority patients’ beliefs about
hypertension to reduce gaps in communication between patients and clinicians. The Journal of
Clinical Hypertension, 14(1), 38-44. doi: 10.1111/j.1751-7176.2011.00558.x
Kuate Defo, B., Mbanya, J. C., Tardif, J., Ekundayo, O., Perreault, S., ... Dubois, C. (2017). Diagnosis,
prevalence, awareness, treatment, prevention, and control of hypertension in cameroon: Protocol
for a systematic review and meta-analysis of clinic-based and community-based studies. Journal of
Medical Internet Research Protocols, 6(5), e102. doi: 10.2196/resprot.7807

185
Kuhn, T. (1962). The Structure of Scientific Revolutions. Chicago: University of Chicago Press.
Kumar, S., Bano, S. (2017). Comparison and analysis of health care delivery systems: Pakistan versus
Bangladesh. Journal of Hospital and Medical Management, 3(1), 1-7. doi: 10.4172/2471-
9781.100020
Kurji, Z., Premani, Z. S., Mithani, Y. (2016). Analysis of the health care system of Pakistan: Lessons
learnt and way forward. Journal of Ayub Medical College Abbottabad, 28(3), 601-604. Retrieved
from https://www.ncbi.nlm.nih.gov/pubmed/28712245
Kusuma, Y. (2009). Perceptions on hypertension among migrants in Delhi, India: A qualitative study.
BMC Public Health, 9, 267-267. doi: 10.1186/1471-2458-9-267
Kwon, Y., Norby, F. L., Jensen, P. N., Agarwal, S. K., Soliman, E. Z., … Chen, L. Y. (2016). Association of
smoking, alcohol, and obesity with cardiovascular death and ischemic stroke in atrial fibrillation: The
Atherosclerosis Risk in Communities (ARIC) Study and Cardiovascular Health Study (CHS). PLoS One,
11(1), e0147065. doi: 10.1371/journal.pone.0147065.
LaBore, K., Ahmed, T., Rizwan-UR-Rashid, R., Ahmed, R. (2019). Prevalence and predictors of
violence against women in Pakistan. Journal of Interpersonal Violence,
doi:10.1177/0886260518824652
Ladha, A., Khan, RS., Malik, AA., Khan, SF., Khan, B., … Saleem, S. (2009). The health seeking
behaviour of elderly population in a poor-urban community of Karachi, Pakistan. The Journal of
Pakistan Medical Association, 59(2), 89-92. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/19260571
Landray, M. J., Edmunds, E., Li-Saw-Hee, F. L., Hughes, B. A., Beevers, D. G., … Lip, G. Y. (2002).
Abnormal low-density lipoprotein subfraction profile in patients with untreated hypertension.
Monthy Journal of the Association of Physicians, 95(3), 165-171 Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/11865172/
Lang, E., Bell, N. R., Dickinson, J. A., Grad, R., Kasperavicius, D., … Stacey, D. (2018). Eliciting patient
values and preferences to inform shared decision making in preventive screening. Canadian Family
Physician Medecin De Famille Canadien, 64(1), 28. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5962974/
Lawes, C. M., Hoorn, S. V., Rodgers, A. (2008). International Society of Hypertension. Global burden
of blood-pressure-related disease, 2001. Lancet, 371(9623), 1513-1518. doi:10.1016/S0140-
6736(08)60655-8
Lawrence, J., Tar, U. (2013). The use of grounded theory technique as a practical tool for qualitative
data collection and analysis. Electronic Journal of Business Research Methods, 11(1), 29-40. Retrieved
from https://pdfs.semanticscholar.org/1255/fb6a561e83eb23fad8490dfebd3c34b1a596.pdf
Lawton, J. (2003). Lay experiences of health and illness: Past research and future agendas. Sociology
of Health & Illness, 25, 23-40. doi: 10.1111/1467-9566.00338

186
Lawton, J., Ahmad, N., Hanna, L., Douglas, M., Hallowell, N. (2006). 'I can't do any serious exercise':
Barriers to physical activity amongst people of Pakistani and Indian origin with type 2 diabetes.
Health Education Research, 21(1), 43-54. doi: 10.1093/her/cyh042
Lawton, J., Ahmad, N., Hanna, L., Douglas, M., Bains, H., Hallowell, N. (2008). 'We should change
ourselves, but we can't': Accounts of food and eating practices amongst British Pakistanis and
Indians with type 2 diabetes. Ethnicity and Health, 13(4), 305-319. doi:
10.1080/13557850701882910
Lee, I. M., Paffenbarger, S., Hennekens, C. H. (1997). Physical activity, physical fitness and longevity.
Aging Clinical and Experimental Research, 9(1-2), 2-11. doi: 10.1007/BF03340123
Lee, G. B. W., Charn, T. C., Chew, Z. H., Ng, T. P. (2004). Complementary and alternative medicine use
in patients with chronic diseases in primary care is associated with perceived quality of care and
cultural beliefs. Family Practice, 21(6), 654-660. doi:10.1093/fampra/cmh613
Lee, I., Buchner, D. M. (2008). The importance of walking to public health. Medicine and Science in
Sports and Exercise, 40(7), S512-S518. doi: 10.1249/MSS.0b013e31817c65d0
Lee, H. S., Park, Y. M., Kwon, H. S., Lee, J. H., Park, Y. J., Lim, S. Y. (2010). Prevalence, awareness,
treatment, and control of hypertension among people over 40 years old in a rural area of South
Korea: The Chungju Metabolic Disease Cohort (CMC) Study. Clinical and Experimental Hypertension,
32(3), 166-178. doi: 10.3109/10641960903254497
Lee, P. Y., Liew, S. M., Abdullah, A., Abdullah, N., Ng, C. J., … Khoo, E. M. (2015). Healthcare
professionals' and policy makers' views on implementing a clinical practice guideline of hypertension
management: A qualitative study. PLoS One, 10(5). doi: 10.1371/journal.pone.0126191
Legido-Quigley, H., Lopez, P. A. C., Balabanova, D., Perel, P., Lopez-Jaramillo, P., Nieuwlaat, R., . . .
McKee, M. (2015). Patients' knowledge, attitudes, behaviour and health care experiences on the
prevention, detection, management and control of hypertension in Colombia: A qualitative study.
Plos One, 10(4), e0122112-e0122112. doi:10.1371/journal.pone.0122112
Legido-Quigley, H., Naheed, A., de Silva, H. A., Jehan, I., Haldane, V., Cobb, B., … Jafar, T. H. (2019).
Patients’ experiences on accessing health care services for management of hypertension in rural
Bangladesh, Pakistan and Sri Lanka: A qualitative study. PLoS One, 14(1), e0211100. doi:
10.1371/journal.pone.0211100
Lehane, E., Leahy-Warren, P., O’Riordan, C., Savage, E., Drennan, J., O’Tuathaigh, C., . . . Hegarty, J.
(2019). Evidence-based practice education for healthcare professions: An expert view. Evidence -
Based Medicine, 24(3), 103. doi:10.1136/bmjebm-2018-111019
Le Moal, M., Koob, G. F. (2007). Drug addiction: Pathways to the disease and pathophysiological
perspectives. European Neuropsychopharmacology, 17(6-7), 377-393. doi:
10.1016/j.euroneuro.2006.10.006
Lemos, N. (2007). An Introduction to the Theory of Knowledge. Cambridge: Cambridge University
Press.

187
Lewin, S. A., Skea, Z. C., Entwistle, V., Zwarenstein, M., Dick, J. (2001). Interventions for providers to
promote a patient-centred approach in clinical consultations. The Cochrane Database of Systematic
Reviews, (4), Cd003267. doi: 10.1002/14651858.cd003267
Lewins, A., Silver, C. (2007). Using software in qualitative research: A step-by-step guide using
software in qualitative research. London: Sage.
Ley, P. (1988). Communicating with patients: Improving communication, satisfaction and
compliance, New York, Croom Helm.
Li, G., Wang, H., Wang, K., Wang, W., Dong, F., … Shan, G. (2017). The association between smoking
and blood pressure in men: A cross-sectional study. BMC Public Health, 17(1), 797. doi:
10.1186/s12889-017-4802-x
Lichtman, M. (2001). Review: Patricia bazeley & lyn richards (2000). the NVivo qualitative project
book. Forum: Qualitative Social Research, 2(3), doi.org/10.17169/fqs-2.3.924
Liljegren, H., Akhunzada, F. (2017). Linguistic diversity, vitality and maintenance: A case study on the
language situation in Northern Pakistan. Retrieved from http://www.diva-
portal.org/smash/get/diva2:1155268/FULLTEXT01.pdf
Liu, PH., Wang, JD. (2008). Antihypertensive medication prescription patterns and time trends for
newly-diagnosed uncomplicated hypertension patients in Taiwan. BMC Health Services Research.
8:133. doi: 10.1186/1472-6963-8-133.
Lloyd, C. E., Johnson, M. R. D., Mughal, S., Sturt, J. A., Collins, G. S., Roy, T., Barnett, A. H. (2008).
Securing recruitment and obtaining informed consent in minority ethnic groups in the UK. BMC
Health Services Research, 8(1), 68-68. doi:10.1186/1472-6963-8-68
Lucas, A., Murray, E., Kinra, S. (2013). Heath beliefs of UK South Asians related to lifestyle diseases: A
review of qualitative literature. Journal of Obesity, 2013: 827674. doi: 10.1155/2013/827674
Lu, C., Shulman, S. W. (2008). Rigor and flexibility in computer-based qualitative research:
Introducing the coding analysis toolkit. International Journal of Multiple Research Approaches, 2(1),
105-117. doi:10.5172/mra.455.2.1.105
Lucire, Y. (2003). Constructing RSI: Belief and desire. University of New South Wales Press.
Lukoschek, P. (2003). African Americans’ beliefs and attitudes regarding hypertension and its
treatment: A qualitative study. Journal of Health Care for the Poor and Underserved, 14(4), 566-587.
doi:10.1353/hpu.2010.0690
MacAuley, D., Best, T. M. (2002). Reducing risk of injury due to exercise. British Medical Journal, 325-
451. doi: 10.1136/bmj.325.7362.451
Macera, C. A., Hootman, J. M., Sniezek, J. E. (2003). Major public health benefits of physical activity.
Arthritis and Rheumatism, 49(1), 122-128. doi:10.1002/art.10907

188
Mahdavi, R., Bagheri Asl, A., Abadi, M. A. J., Namazi, N. (2017). Perceived barriers to following
dietary recommendations in hypertensive patients. Journal of American College of Nutrition, 36(3),
193-199.doi: 10.1080/07315724.2014.966176
Mahmoud, M. I. H. (2012). Compliance with treatment of patients with hypertension in Almadinah
Almunawwarah: A community-based study. Journal of Taibah University Medical Sciences, 7(2), 92-
98. doi: 10.1016/j.jtumed.2012.11.004
Mahmood, S., Hassan, S. Z., Tabraze, M., Khan, M. O., Javed, I., Ahmed, A., … Fatima, K. (2017).
Prevalence and predictors of depression amongst hypertensive individuals in Karachi, Pakistan.
Cureus, 9(6), e1397. doi: 10.7759/cureus.1397
Main, C. J., Buchbinder, R., Porcheret, M., Foster, N. (2010). Addressing patient beliefs and
expectations in the consultation. Best practice & research. Clinical rheumatology, 24(2), 219-225.
doi: 10.1016/j.berh.2009.12.013
Makridakis, S., & DiNicolantonio, J. J. (2014). Hypertension: empirical evidence and implications in
2014. Open heart, 1(1), e000048. doi:10.1136/openhrt-2014-000048
Malik, H. I. (2002). Religious Minorities in Pakistan. United Kingdom: Minority Rights Group.
Malik, J. (2003). Muslim culture and reform in 18th century South Asia. Journal of the Royal Asiatic
Society, 13(2), 227-243. doi: 10.1017/S1356186303003080
Malik, M., Uzair, F., Hussain, A., Lubbe, M. (2016). Are JNC 8 guidelines well known and perceived by
the prescribers for the treatment of hypertension in Pakistan? A cross-sectional study. International
Journal of Pharmaceutical Research & Allied Sciences, 5(4), 45-55. Retrieved from
http://ijpras.com/vol5-iss4/45-55.pdf
Marcum, J. A. (2013). The role of empathy and wisdom in medical practice and pedagogy:
Confronting the hidden curriculum, Journal of Biomedical Education. doi.org/10.1155/2013/923810.
Marshall, I. J., Wolfe, C. D. A., McKevitt, C. (2012). Lay perspectives on hypertension and drug
adherence: Systematic review of qualitative research. British Medical Journal, 345. doi:
10.1136/bmj.e3953
Martin, L. R., Williams, S. L., Haskard, K. B., DiMatteo, M. R. (2005). The challenge of patient
adherence. Therapeutics and Clinical Risk Management, 1(3), 189-199. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1661624/
Marx, J. L. (1976). Hypertension: A complex disease with complex causes. Science, 194(4267), 821-
825. doi: 10.1126/science.194.4267.821. Retrieved from
https://science.sciencemag.org/content/194/4267/821
Masic, I., Miokovic, M., Muhamedagic, B. (2008). Evidence based medicine - new approaches and
challenges. Acta Informatica Medica: AIM: Journal of the Society for Medical Informatics of Bosnia &
Herzegovina : Casopis Drustva Za Medicinsku Informatiku BiH, 16(4), 219-225.
doi:10.5455/aim.2008.16.219-225

189
Matsui, Y., Kario, K., Ishikawa, J., Hoshide, S., Eguchi, K., Shimada, K. (2005). Smoking and
antihypertensive medication: Interaction between blood pressure reduction and arterial stiffness.
Hypertension Research, 28(8), 631-638. doi: 10.1291/hypres.28.631
Mazzi, M. A., Rimondini, M., Deveugele, M., Zimmermann, C., Moretti, F., van Vliet, L., Bensing, J.
(2015). What do people appreciate in physicians' communication? An international study with focus
groups using videotaped medical consultations. Health expectations: an international journal of
public participation in health care and health policy, 18(5), 1215-1226. doi:10.1111/hex.12097
McAreavey, R., Das, C. (2013). A delicate balancing act: Negotiating with gatekeepers for ethical
research when researching minority communities. International Journal of Qualitative Methods,
12(1), 113-131. doi:10.1177/160940691301200102
McFadyen, J., Rankin, J. (2017). The role of gatekeepers in research: Learning from reflexivity and
reflection. The Journal of Nursing and Health Care (JNHC), 4(1). Retrieved from
http://dl6.globalstf.org/index.php/jnhc/article/view/389.
McManus, R., Caulfield, M., Williams, B. (2012). NICE hypertension guideline 2011: Evidence based
evolution. BMJ (Online), 344(7841), 181. doi: 10.1136/bmj.e181
McPhail, S. M. (2016). Multimorbidity in chronic disease: impact on health care resources and costs.
Risk management and healthcare policy, 9, 143-156. doi: 10.2147/RMHP.S97248
McShane, M., Mitchell, E. W. (2013). Patient experience: Put individuals at the centre of care. Health
Service Journal, 123(6359), 26-27. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/24044265
Megari, K. (2013). Quality of life in chronic disease patients. Health psychology research, 1(3), doi:
10.4081/hpr.2013.e27
Mehmood, M., Mesiah, A., Raza, F. Z., Junaid, Z., Jamali, M., … Fatima, K. (2018). Prevalence and
predictors of blood pressure screening in Karachi: A cross-sectional study. Cureus, 10(7), doi:
10.7759/cureus.2967
Meijer, E., Kampman, M., Geisler, M. S., Chavannes, N. H. (2018). "It's on everyone's plate": a
qualitative study into physicians' perceptions of responsibility for smoking cessation. Substance
abuse treatment, prevention and policy, 13(1), 48. doi:10.1186/s13011-018-0186-x
Melzer, K., Kayser, B., Pichard, C. (2004). Physical activity: The health benefits outweigh the risks.
Current Opinion in Clinical Nutrition & Metabolic Care, 7(6), 641-647.
Mendenhall, E., Kohrt, B. A., Norris, S. A., Ndetei, D., Prabhakaran, D. (2017). Non-communicable
disease syndemics: Poverty, depression, and diabetes among low-income populations. The Lancet,
389(10072), 951-963. doi: 10.1016/S0140-6736(17)30402-6
Mensah, G. A., Croft, J. B., Giles, W. H. (2003). The heart, kidney, and brain as target organs in
hypertension. Current Problems in Cardiology, 28(2), 156-193. doi: 10.1016/S0146-2806(03)00017-3

190
Mensah G. A. (2016). Hypertension and target organ damage: Don't believe everything you think!
Ethnicity & disease, 26(3), 275-278. doi:10.18865/ed.26.3.275
Mercer, S. W., Neumann, M., Wirtz, M., Fitzpatrick, B., Vojt, G. (2008). General practitioner empathy,
patient enablement, and patient-reported outcomes in primary care in an area of high socio-
economic deprivation in Scotland-A pilot prospective study using structural equation modelling.
Patient Education and Counselling, 73(2), 240-245. doi:10.1016/j.pec.2008.07.022
Merriam, C. B. (1998). Qualitative Research and Case Study Application in Education. San Francisco:
Jossey-Bass.
Michael, H. (2002). Salt, blood pressure and health: A cautionary tale. International Journal of
Epidemiology, 31(2), 311-316. Retrieved from
https://academic.oup.com/ije/article/31/2/311/617695
Michalak, L., Trocki, K. (2006). Alcohol and islam: An overview. Contemporary Drug Problems, 33(4),
523-562. doi:10.1177/009145090603300401
Michie, S., Miles, J., Weinman J. (2003). Patient‐centredness in chronic illness: What is it and does it
matter? Patient Education and Counselling, 51(3), 197-206. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/14630376
Midlöv, P., Ekesbo, R., Johansson, L., Gerward, S., Persson, K., … Hedblad, Bo. (2008). Barriers to
adherence to hypertension guidelines among GPs in southern Sweden: A survey. Scandinavian
Journal of Primary Health Care, 26(3), 154-159. doi: 10.1080/02813430802202111
Middleton, K. R., Anton, S. D., Perri, M. G. (2013). Long-term adherence to health behavior change.
American Journal of Lifestyle Medicine, 7(6), 395-404. Retrieved from
http://doi.org/10.1177/1559827613488867
Mik-Meyer, N., Obling, A. R. (2012). The negotiation of the sick role: general practitioners'
classification of patients with medically unexplained symptoms. Sociology of health & illness, 34(7),
1025–1038. doi:10.1111/j.1467-9566.2011.01448.x
Miles, B., Michael, H. (1994). Qualitative Data Analysis: An Expanded Sourcebook. Beverly Hills, Sage
Publications.
Miller, W. R., Bakas, T., Buelow, J. M., Habermann, B. (2013). Research involving participants with
chronic diseases: Overcoming recruitment obstacles. Clinical Nurse Specialist, 27(6), 307-313.
doi:10.1097/NUR.0b013e3182a8725a
Mills, J., Bonner, A., Francis, K. (2006). The development of constructivist grounded theory.
International Journal of Qualitative Methods, 5(1), 25-35. doi:10.1177/160940690600500103
Mills, K. T., Bundy, J. D., Kelly, T. N., Reed, J. E., Kearney, P. M., … He, J. (2016). Global disparities of
hypertension prevalence and control: A systematic analysis of population-based studies from 90
countries. Circulation, 134(6), 441-450. doi: 10.1161/CIRCULATIONAHA.115.018912

191
Mirzaei, T., Oskouie, F., Rafii, F. (2012), Nursing students' time management, reducing stress and
gaining satisfaction: a grounded theory study. Nursing & Health Sciences, 14. 46-51.
doi:10.1111/j.1442-2018.2011.00661.x
Mirzaei, M., Aspin, C., Essue, B., Jeon, Y., Dugdale, P., Usherwood, T., Leeder, S. (2013). A patient-
centred approach to health service delivery: Improving health outcomes for people with chronic
illness. BMC Health Services Research, 13(1), 251-251. doi:10.1186/1472-6963-13-251
Mishra, A., Chaturvedi, P., Datta, S., Sinukumar, S., Joshi, P., Garg, A. (2015). Harmful effects of
nicotine. Indian journal of medical and paediatric oncology: official journal of Indian Society of
Medical & Paediatric Oncology, 36(1), 24-31. doi: 10.4103/0971-5851.151771
Misra, A. (2010). India-Pakistan: Coming to Terms. New York: Palgrave Macmillan.
Miura, K., Daviglus, M. L., Dyer, A. R., Liu, K., Garside, D. B., … Greenland, P. (2001). Relationship of
blood pressure to 25-year mortality due to coronary heart disease, cardiovascular diseases, and all
causes in young adult men: The Chicago Heart Association Detection Project in Industry. Archives of
Internal Medicine, 161(12), 1501-1508. doi: 10.1001/archinte.161.12.1501
Mizutani, M., Tashiro, J., Maftuhah., Sugiarto, H., Yulaikhah, L., Carbun, R. (2016). Model
development of healthy-lifestyle behaviours for rural Muslim Indonesians with hypertension: A
qualitative study. Nursing & Health Sciences, 18(1), 15-22. doi: 10.1111/nhs.12212
Moazam, F., Jafarey, A. M. (2005). Pakistan and biomedical ethics: Report from a Muslim country.
Cambridge Quarterly of Healthcare Ethics, 14(3), 249-255. doi:10.1017/S0963180105050346
Modesti, P. A., Perruolo, E., Parati, G. (2015). Need for better blood pressure measurement in
developing countries to improve prevention of cardiovascular disease. Journal of Epidemiology,
25(2), 91-98. doi: 10.2188/jea.JE20140146
Mohan, V., Seedat, Y. K., Pradeepa, R. (2013). The rising burden of diabetes and hypertension in
Southeast Asian and African regions: Need for effective strategies for prevention and control in
primary health care settings. International Journal of Hypertension, 2013(409083-14). doi:
10.1155/2013/409083
Mohseni, J., Kazemi, T., Maleki, M. H., Beydokhti, H. (2017). A systematic review on the prevalence
of acute myocardial infarction in Iran. Heart Views, 18(4), 125-132. doi:
10.4103/heartviews.heartviews_71_17
Moore, J. (2005). Hypertension: Catching the silent killer. The Nurse Practitioner, 30(10), 16-35.
doi:10.1097/00006205-200510000-00005
Moret, L., Anthoine, E., Pourreau, A., Beaudeau, F., Leclère, B. (2017). Inpatient satisfaction with
medical information received from caregivers: An observational study on the effect of social
deprivation. BMC health services research, 17(1), 769. doi: 10.1186/s12913-017-2728-8

192
Morgan, M., Watkins, C. J. (1988). Managing hypertension: Beliefs and responses to medication
among cultural groups. Sociology of Health & Illness, 10(4), 561-578. doi: 10.1111/1467-
9566.ep10837256
Morse, J. (2001). Situating grounded theory within qualitative inquiry. In R. Schreiber & P. N. Stern
(Eds.), Using Grounded Theory in Nursing. New York: Springer.
Mostafavi, F., Najimi, A., Sharifirad, G., Golshiri, P. (2016). Beliefs about medicines in patients with
hypertension: The instrument validity and reliability in Iran. Materia Socio-Medica, 28(4), 298-302.
doi: 10.5455/msm.2016.28.298-302
Mufti, G. (2011). Vacillating between distress and adaptation: A multi-perspective account of lived
experiences of thalassemia major. Doctoral dissertation, The University of Westminster, England.
Murad, H., Virani, S., Khan, A., Imran, M., Issani, F., Ali, S. (2017). Readiness of lifestyle modification
among hypertensive patients in a regional community at Karachi, Pakistan. International Journal of
Scientific & Engineering Research, 8(3), 906-909. Retrieved from https://www.ijser.org/research-
paper-publishing-march-2017_page4.aspx
Muran, J., Barber, J. (2011). Therapeutic alliance: An evidence-based guide to practice. New York:
Guilford Press.
Murray, C. J., Lopez, A. D., Black, R., Mathers, C. D., Shibuya, K., … Vos, T. (2007). Global burden of
disease 2005: Call for collaborators. Lancet, 370(9582), 109-110. doi: 10.1016/S0140-
6736(07)61064-2
Nabi, R., Rogers, A., Street, B. (2010). Hidden literacies: Ethnographic studies of literacy and
numeracy practices in Pakistan. England: Uppingham Press.
Najimi, A., Mostafavi, F., Sharifirad, G., Golshiri, P. (2016). Patients' beliefs about adherence to
medication toward hypertension: A qualitative study. International Journal of Advanced
Biotechnology and Research, 7(3), 1555-1561. Retrieved from
https://bipublication.com/files/201603183Arash.pdf
Nakanishi, N., Yoshida, H., Nakamura, K., Suzuki, K.,Tatara, K. (2001). Alcohol consumption and risk
for hypertension in middle-aged Japanese men. Journal of Hypertension, 19(5), 851-855. doi:
10.1097/00004872-200105000-00003
Namukwaya, E., Murray, S. A., Downing, J., Leng, M., Grant, L. (2017). ‘I think my body has become
addicted to those tablets’. chronic heart failure patients’ understanding of and beliefs about their
illness and its treatment: A qualitative longitudinal study from Uganda. Plos One, 12(9),
doi:10.1371/journal.pone.0182876
Naseeba, A. (2011). Patient and professional perceptions of metabolic syndrome and its
management: A qualitative study in the United Arab Emirates, Doctoral dissertation, The University
of Nottingham, Nottingham.

193
National Centre for Health Statistics (NCHS) of the Centre for Disease Control and Prevention (CDC),
US Public Health Service.
National Heart, Lung and Blood Institute (NHLBI). (2017). Study Quality Assessment Tools. Retrieved
from https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
National Institute of Population Studies (NIPS). (2008). Pakistan Demographic and Health Survey
2006-07. The National Institute of Population Studies Islamabad.
Nayeri, N., Dehghan, M., Iranmanesh, S. (2015). Being as an iceberg: Hypertensive treatment
adherence experiences in Southeast of Iran. Global Health Action, 8. doi: 10.3402/gha.v8.28814
Neal, J. (2013). Handbook of Faith and Spirituality in the Workplace: Emerging Research and Practice.
New York: Springer.
Nettleton, S. (2006). Sociology of Health and Illness. Cambridge: Polity Press.
Nettleton, J. A., Brouwer, I. A., Geleijnse, J. M., Hornstra, G. (2017). Saturated fat consumption and
risk of coronary heart disease and ischemic stroke: A science update. Annals of Nutrition &
Metabolism, 70(1), 26-33. doi: 10.1159/000455681
Neupane, D., McLachlan, C. S., Sharma, R., Gyawali, B., Khanal, V., … Kallestrup, P. (2014). Prevalence
of hypertension in member countries of South Asian Association for Regional Cooperation (SAARC):
Systematic review and meta-analysis. Medicine, 93(13), doi: 10.1097/MD.0000000000000074
Newington, L., Metcalfe, A. (2014). Factors influencing recruitment to research: qualitative study of
the experiences and perceptions of research teams. BMC medical research methodology, 14(1), 10-
10. doi:10.1186/1471-2288-14-10
Nguyen, Q., Dominguez, J., Nguyen, L., Gullapalli, N. (2010). Hypertension management: An update.
American Health & Drug Benefits, 3(1), 47-56.
NHSP. (1998). The National Health Survey of Pakistan 1990-1994. Islamabad, Pakistan. Pakistan
Niaz, I. (2010). The Culture of Power and Governance of Pakistan 1947-2008. Islamabad: Oxford
University Press.
NICE. (2011). Hypertension in Adults’ Diagnosis and Management. England: National Institute for
Health and Care Excellence.
Nichter, M. (1996). Anthropology and International Health: Asian Case Studies. London: Routledge.
Nimmon, L., Stenfors-Hayes, T. (2016). The "Handling" of power in the physician-patient encounter:
Perceptions from experienced physicians. BMC Medical Education, 16(114). doi: 10.1186/s12909-
016-0634-0

194
Nizami, S., Sobani, Z. A., Raza, E., Baloch, N. U., Khan, J. A. (2011). Causes of smoking in Pakistan: An
analysis of social factors. Journal of Pakistan Medical Association, 61(2), 198-201. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/21375182
Noble, H., Smith, J. (2015). Issues of validity and reliability in qualitative research. Evidence Based
Nursing, 18(2), 34-35. doi:10.1136/eb-2015-102054
Nørgaard, B., Ammentorp, J., Ohm Kyvik, K., Kofoed, P. (2012). Communication skills training
increases self‐efficacy of health care professionals. Journal of Continuing Education in the Health
Professions, 32(2), 90-97. doi:10.1002/chp.21131
Nowson, C. A., Worsley, A., Margerison, C., Jorna, M. K., Frame, A. G., … Godfrey, S. J. (2004). Blood
pressure response to dietary modifications in free-living individuals. The Journal of Nutrition, 134(9),
2322-2329. Retrieved from http://jn.nutrition.org/content/134/9/2322.long
Noorani, M. M., Khaliq, M. F., Shoaib, M., Sheikh, A., Moughal, U. E., Moazzum, W., Ali, S. A. (2014).
Time intervals and associated factors of emergency treatment: first insight into Pakistani system.
International archives of medicine, 7(1), 41. doi:10.1186/1755-7682-7-41
Noordman, J., Koopmans, B., Korevaar, J. C., Weijden, T. T. v. d., Dulmen, S. v. (2013). Exploring
lifestyle counselling in routine primary care consultations: The professionals' role. Family Practice,
30(3), 332-340. doi:10.1093/fampra/cms077
Ohira, T., Iso, H. (2013). Cardiovascular disease epidemiology in Asia: An overview. Circulation
Journal: Official Journal Of The Japanese Circulation Society, 77(7), 1646-1652. Retrieved from
http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=23803294&site=ehost-live
Ohmori, S., Kiyohara, Y., Kato, I., Kubo, M., Tanizaki, Y., … Fujishima, M. (2002). Alcohol intake and
future incidence of hypertension in a general Japanese population: The Hisayama study. Alcoholism
Clinical and Experimental Research, 26(7), 1010-1016. doi: 10.1111/j.1530-0277.2002.tb02635.x
Ojo, M. A., Igwilo, C. I., Emedoh, T. (2014). Prescribing patterns and perceptions of health care
professionals about rational drug use in a specialist hospital clinic. Journal of public health in Africa,
5(2), 242. doi:10.4081/jphia.2014.242
Okely, J. (2007). Fieldwork embodied. The Sociological Review, 55(1), 65-79. doi:10.1111/j.1467-
954X.2007.00693.x
Okubo, Y., Suwazono, Y., Kobayashi, E., Nogawa, K. (2001). Alcohol consumption and blood pressure
change: 5-year follow-up study of the association in normotensive workers. Journal of Human
Hypertension, 15(6), 367-372. doi: 10.1038/sj.jhh.1001191
Okubo, Y., Miyamoto, T., Suwazono, Y., Kobayashi, E., Nogawa, K. (2002). An association between
smoking habits and blood pressure in normotensive Japanese men. Journal of Human Hypertension,
16(2), 91-96. doi: 10.1038/sj.jhh.1001303

195
Okubo, Y., Suwazono, Y., Kobayashi, E., Nogawa, K. (2004). An association between smoking habits
and blood pressure in normotensive Japanese men: A 5-year follow-up study. Drug and Alcohol
Dependence, 73(2), 167-174. doi: 10.1016/j.drugalcdep.2003.10.005
Okumus, F., Altinay, L., Roper, A. (2007). Gaining access for research. Annals of Tourism Research,
34(1), 7-26. doi:10.1016/j.annals.2006.07.006
Olinto, M. T. A., Gigante, D. P., Horta, B., Silveira, V., Oliveira, I., Willett, W. (2012). Major dietary
patterns and cardiovascular risk factors among young Brazilian adults. European Journal of Nutrition,
51(3), 281-291. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/21681439
Olson, E. J., Drage, L. A., Auger, R. R. (2009). Sleep deprivation, physician performance and patient
safety. Chest, 136 (5), 1389-1396. doi: 10.1378/chest.08-1952
Omboni, S., Aristizabal, D., De la Sierra, A., Dolan, E., Head, G., Kahan, T. (2016). Hypertension types
defined by clinic and ambulatory blood pressure in 14 143 patients referred to hypertension clinics
worldwide. Data from the ARTEMIS study. Journal Of Hypertension, 34(11), 2187-2198. doi:
10.1097/HJH.0000000000001074
Ozawa, Y., Hayashi, K., Kobori, H. (2006). New generation calcium channel blockers in hypertensive
treatment. Current hypertension reviews, 2(2), 103-111. doi: 10.2174/157340206776877370
Paluck, E., Ball, L. (2010). Social norms marketing aimed at gender based violence: A literature
review and critical assessment. International Rescue Committee, Brazil.
Pakistan Today, (2018). Mozang hospital treating 600 patients at its OPD daily: MS. Retrieved from
https://www.pakistantoday.com.pk/2018/03/11/mozang-hospital-treating-600-patients-at-its-opd-
daily-ms/
Pakistan Medical and Dental Council (PMDC). (2006). Ethics. Retrieved from
http://www.pmdc.org.pk/Ethics/tabid/101/Default.aspx
Panagiotakos, D. B., Kourlaba, G., Zeimbekis, A., Toutouzas, P., Polychronopoulos, E. (2007). The J-
shape association of alcohol consumption on blood pressure levels, in elderly people from
Mediterranean Islands (MEDIS epidemiological study). Journal of Human Hypertension, 21(7), 585-
587. doi: 10.1038/sj.jhh.1002187
Panpakdee, O. H. S., Sritanyarat, W., Kompayak, J., Tanomsup, S. (2003). Self-care process in Thai
people with hypertension: An emerging model. Thai Journal of Nursing Research, 7(2), 121-136.
Retrieved from http://princess-srinagarindraaward.org/files/2011/05/tnc_journal-
611/thai_journal_of_nursing_research_vol_7_no_2_april_15585.pdf#page=37
Pardhan, A. (2010). Ethical dilemmas in research with young children - A field experience from
Pakistan. In: Shamim, F. & Qureshi, R. Perils, Pitfalls and Reflexivity in Qualitative Research in
Education. Oxford University Press Karachi.

196
Patel, R. S., Bachu, R., Adikey, A., Malik, M., Shah, M. (2018). Factors related to physician burnout
and its consequences: A review. Behavioural Sciences, 8(11), 98. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6262585/
Penn, L., Dombrowski, S. U., Sniehotta, F. F., White, M. (2014). Perspectives of UK Pakistani women
on their behaviour change to prevent type 2 diabetes: Qualitative study using the theory domain
framework. BMJ Open, 4(7). doi: 10.1136/bmjopen-2013-004530
Pereira, M., Lunet, N., Azevedo, A., Barros, H. (2009). Differences in prevalence, awareness,
treatment and control of hypertension between developing and developed countries. Journal of
Hypertension, 27(5), 963-975. doi: 10.1097/HJH.0b013e3283282f65
Perfetti, A. (2017). Fate and the clinic: A multidisciplinary consideration of fatalism in health
behaviour. Medical Humanities. doi: 10.1136/medhum-2017-011319
Pescatello, L. S., Franklin, B. A., Fagard, R., Farquhar, W. B., Kelley, G. A., Ray, C. A. (2004). American
College of Sports Medicine position stand. Exercise and hypertension. Medicine & Science in Sports &
Exercise, 36(3), 533-553
Petrie, K. J., Weinman, J. (2012). Patients' perceptions of their illness: The dynamo of volition in
health care. Current Directions in Psychological Science, 21(1), 60-65. doi:
10.1177/0963721411429456
Petticrew, M., Roberts, H. (2008). Systematic Reviews in the Social Sciences: A Practical Guide.
Malden: Blackwell Publishing. doi: 10.1002/9780470754887
Piette, J. D., Heisler, M., Wagner, T. H. (2004). Cost-related medication underuse: do patients with
chronic illnesses tell their doctors? Archivers of Internal Medicine, 164(16), 1749-1755. doi:
10.1001/archinte.164.16.1749
Piko, B. F. (2006). Burnout, role conflict, job satisfaction and psychosocial health among Hungarian
health care staff: A questionnaire survey. International Journal of Nursing Studies, 43(3), 311-318.
doi: 10.1016/j.ijnurstu.2005.05.003
Pilakkadavath, Z., Shaffi, M. (2016). Modifiable risk factors of hypertension: A hospital-based case-
control study from Kerala, India. Journal of family medicine and primary care, 5(1), 114-119. doi:
10.4103/2249-4863.184634
Poirier, P., Giles, T. D., Bray, G. A., Hong, Y., Stern, J. S., … Eckel, R. H. (2006). Obesity and
cardiovascular disease: Pathophysiology, evaluation, and effect of weight loss. Arteriosclerosis,
Thrombosis, and Vascular Biology, 26(5), 968-76. doi: 10.1161/01.ATV.0000216787.85457.f3
Popay, J., Williams, G., Thomas, C., Gatrell, A. (1998). Theorising inequalities in health: The place of
lay knowledge. Sociology of Health and Illness, 20(5), 619-644. doi: 10.1111/1467-9566.00122
Porapakkham, Y., Pattaraarchachai, J., Aekplakorn, W. (2008). Prevalence, awareness, treatment and
control of hypertension and diabetes mellitus among the elderly: The 2004 National Health

197
Examination Survey III, Thailand. Singapore Medical Journal, 49(11), 868-873. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/19037551
Powell, K. E., Paluch, A. E., Blair, S. N. (2011). Physical activity for health: What kind? How much?
How intense? On top of what? Annual Review of Public Health, 32(1), 349-365. doi:
10.1146/annurev-publhealth-031210-101151
Prentice, W. E., Voight, M. L. (2001). Techniques in musculoskeletal rehabilitation. London and New
York: McGraw-Hill.
Prior, L. (2003). Belief, knowledge and expertise: The emergence of the lay expert in medical
sociology. Sociology of Health & Illness, 25(3), 41-57. doi: 10.1111/1467-9566.00339
Pribulick, M., Willams, I. C., Fahs, P. S. (2010). strategies to reduce barriers to recruitment and
participation. Online Journal of Rural Nursing and Health Care: The Official Journal of the Rural Nurse
Organization, 10(1), 22. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3639431/
Punjani, N. S., Shams, S., Bhanji, S. M. (2014). Analysis of health care delivery systems: Pakistan
versus united states. International Journal of Endorsing Health Science Research, 2, 38-41.
Punjwani, S.K. (2015). Issues of research ethics in developing world. Journal of Clinical Research and
Bioethical, 6. doi: 10.4172/2155-9627.1000e113
Qamar, A., Khan, N.I., Yasmeen, G. (2008). Assessment and comparison of cardiovascular risk factors
among smokers and tobacco chewers. International journal of biological biotechnology, 5(3), 219-
224 Retrieved from https://inis.iaea.org/search/search.aspx?orig_q=RN:41090189
Qamar, F., Naveed, S., Alam, S., Hameed, A., Fatima, G., Naqvi., et. Al., Khan, A. (2016). Hypertension
symptoms, treatment and control among the Population of Karachi (Pakistan), a survey-based study.
Journal of Biotechnology and Biosafety. 4(4), 405-410. Retrieved from
https://www.researchgate.net/publication/308208615_HYPERTENSION_SYMPTOMS_TREATMENT_
AND_CONTROL_AMONG_THE_POPULATION_OF_KARACHI_PAKISTAN_A_SURVEY_BASED_STUDY
Qidwai, W., Tabassum, R., Hanif, R., Khan, F. (2009). Belief in prayers and its role in healing among
family practice patients visiting a teaching hospital in Karachi, Pakistan. Pakistan Journal of Medical
Sciences, 2(25), 182-189. Retrieved from
https://www.pjms.com.pk/issues/aprjun109/article/article4.html
Qureshi, N., Shaikh, B. (2006). Myths, fallacies and misconceptions: applying social marketing for
promoting appropriate health seeking behavior in Pakistan. Anthropology & Medicine, 13(2), 131-
139. doi: 10.1080/13648470600738716
Qureshi, R., Sheikh, S., Sheikh, S., Khowja, A., Dadelszen, P. (2016). Health care seeking behaviours in
pregnancy in rural Sindh, Pakistan: A qualitative study. Reproductive Health, 13(1), 34. doi:
10.1186/s12978-016-0140-1

198
Rabbani, F., Qureshi, F., Rizvi, N. (2008). Perspectives on domestic violence: Case study from Karachi,
Pakistan. Eastern Mediterranean Health Journal, 14(2), 415-426. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/18561735/448.
Rabeharisoa, V., Callon, M. (2002). The involvement of patients' associations in research.
International Social Science Journal, 54(171), 57-63. doi:10.1111/1468-2451.00359
Rahman, A., Wang, J. G., Kwong, G. M., Morales, D. D., Sritara, P., Sukmawan, R. (2015). Perception
of hypertension management by patients and doctors in Asia: Potential to improve blood pressure
control. Asia Pacific Family Medicine, 14(1), 2. doi: 10.1186/s12930-015-0018-3
Rahmawati, R., Bajorek, B. V. (2015). Perspectives on antihypertensive medication: A qualitative
study in a rural Yogyakarta province in Indonesia. Drugs & Therapy Perspectives, 32(2), 76-83. doi:
10.1007/s40267-015-0263-4
Raja, S., Hasnain, M., Vadakumchery, T., Hamad, J., Shah, R., Hoersch, M. (2015). Identifying
elements of patient-centered care in underserved populations: A qualitative study of patient
perspectives, PloS One, 10 (5), e0126708, 10.1371/journal.pone.0126708
Rajiv, N., Kevin, R. (2005). How behaviors are influenced by perceived norms: A test of the theory of
normative social behavior. Communication Research, 32(3), 389-414. doi:
10.1177/0093650205275385
Ramli, A. S., Ahmad, N. S., Paraidathathu, T. (2012). Medication adherence among hypertensive
patients of primary health clinics in Malaysia. Patient preference and adherence, 6: 613-622. doi:
10.2147/PPA.S34704
Ranjan, P., Kumari, A., Chakrawarty, A. (2015). How can doctors improve their communication skills?
Journal of clinical and diagnostic research: Journal of Clinical and Diagnostic Research, 9(3), JE01-JE4.
doi:10.7860/JCDR/2015/12072.5712
Rosário, F., Santos, M. I., Angus, K., Pas, L., Fitzgerald, N. (2018). Factors influencing the
implementation of screening and brief interventions for alcohol use in primary care practices: A
systematic review protocol. Acta Médica Portuguesa, 31(1), 45-50. doi:10.20344/amp.9753
Rasanathan, K., Bennett, S., Atkins, V., Beschel, R., Carrasquilla, G., Charles, J., Zaidi, S. (2017).
Governing multisectoral action for health in low- and middle-income countries. PLoS Medicine,
14(4), e1002285. doi: 10.1371/journal.pmed.1002285
Rasheed, S., Jahan, S., Sharmin, T., Hoque, S., Khanam, M. A., Land, M. A., … Bhuiya, A. (2014). How
much salt do adults consume in climate vulnerable coastal Bangladesh? BMC Public Health, 14(1),
584-584. doi: 10.1186/1471-2458-14-584
Rashid, A., Jagger, C. (1996). Patients' knowledge of anatomical location of major organs within the
human body: a comparison between Asians and non-Asians, Family Practice, 13(5), 450-454.
Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/8902514

199
Rassool, G. H. (2015). Cultural Competence in Nursing Muslim Patients. England: Macmillan
Publishing Ltd.
Rathert, C., Wyrwich, M. D., Boren S. A. (2013). Patient‐centred care and outcomes: A systematic
review of the literature. Medical Care Research and Review, 70(4), 351-379. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/23169897
Rêgo, M. L., Cabral, D. A., Costa, E. C., Fontes, E. B. (2019). Physical exercise for individuals with
hypertension: It is time to emphasize its benefits on the brain and cognition. Clinical Medicine
Insights: Cardiology, 13. doi: 10.1177/1179546819839411
Rehman, A., Rehman, T., Shaikh, M. A., Naqvi, S. A. (2011). Awareness of hypertension among the
medical students and junior doctors - a multicenter study from Pakistan. The Journal of Pakistan
Medical Association, 61(11), 1153-1157. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/22126006
Richard, S., Haidet, P. (2011). How well do doctors know their patients? Factors affecting physician
understanding of patients' health beliefs, Journal of General Internal Medicine, 26(1), 21-7. doi
10.1007/s11606-010-1453-3
Richards, L. (2009). Handling Qualitative Data: A Practical Guide. London: Sage Publications.
Richards, M., Hori, H., Sartorius, N., Kunugi, H. (2014). Cross-cultural comparisons of attitudes
toward schizophrenia amongst the general population and physicians: A series of web-based surveys
in Japan and the United states. Psychiatry Research, 215(2), 300-307.
doi:10.1016/j.psychres.2013.12.012
Risso-Gill, I., Balabanova, D., Majid, F., Ng, K. K., Yusoff, K., ... McKee, M. (2015). Understanding the
modifiable health systems barriers to hypertension management in Malaysia: A multi-method health
systems appraisal approach. BMC Health Services Research, 15(1), 254. doi: 10.1186/s12913-015-
0916-y
Ritchie, J., Lewis, J. (2003). Qualitative Research Practice: A Guide for Social Science Students and
Researchers. London: Sage Publications.
Rocco, N., Scher, K., Basberg, B., Yalamanchi, S., Baker-Genaw, K. (2011). Patient-centered plan-of-
care tool for improving clinical outcomes
Quality Management in Health Care, 20(2), pp. 89-97. doi: 10.1097/QMH.0b013e318213e728
Rogers, A., Kennedy, A., Nelson, E., Robinson, A. (2005). Uncovering the limits of patient-
centeredness: Implementing a self-management trial for chronic illness. Qualitative Health Research,
15(2), 224-239. doi:10.1177/1049732304272048
Rolfe, G. (2006). Validity, trustworthiness and rigour: Quality and the idea of qualitative research.
Journal of Advanced Nursing, 53(3), 304-310. doi: 10.1111/j.1365-2648.2006.03727.x

200
Rosário, F., Santos, M. I., Angus, K., Pas, L., Fitzgerald, N. (2018). Factors influencing the
implementation of screening and brief interventions for alcohol use in primary care practices: A
systematic review protocol. Acta Médica Portuguesa, 31(1), 45-50. doi:10.20344/amp.9753
Rosendal, M., Jarbøl, D. E., Pedersen, A. F., Andersen, R. S. (2013). Multiple perspectives on
symptom interpretation in primary care research. BMC family practice, 4(14), 167. doi:
10.1186/1471-2296-14-167.
Roshan, R., Hamid, S. Mashhadi, S. F. (2018) Non-communicable diseases in Pakistan; A health
system perspective, Pakistan Armed Forces Medical Journal, 2, 394-399. Retrieved from
http://www.pafmj.org/
Ross, S., Walker, A., MacLeod, M. J. (2004). Patient compliance in hypertension: Role of illness
perceptions and treatment beliefs. Journal of Human Hypertension, 18(9). doi:
10.1038/sj.jhh.1001721
Rozi, S., Akhtar, S., Ali, S., Khan, J. (2005). Prevalence and factors associated with current smoking
among high school adolescents in Karachi, Pakistan. Southeast Asian Journal of Tropical Medicine
and Public Health, 36(2), 498-504. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/15916062
Sacks, F. M., Campos, H. (2010). Dietary therapy in hypertension. The New England Journal of
Medicine, 362(22), 2102-2112. doi: 10.1056/NEJMct0911013
Saeed, K., Gater, R., Hussain, A., Mubbashar, M. (2000). The prevalence, classification and treatment
of mental disorders among attenders of native faith healers in rural Pakistan. Social Psychiatry and
Psychiatric Epidemiology, 35(10), 480-485. doi:10.1007/s001270050267
Saeed, A., Ibrahim, H. (2005). Reasons for the problems faced by patients in government hospitals:
Results of a survey in a government hospital in Karachi, Pakistan. The Journal of Pakistan Medical
Association, 55(1), 45-47. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/15816698
Safdar, N. F., Bertone-Johnson, E. R., Cordeiro, L., Jafar, T. H., Cohen, N. L. (2015). Dietary patterns
and their association with hypertension among Pakistani urban adults. Asia Pacific Journal of Clinical
Nutrition, 24(4), 710-719. doi: 10.6133/apjcn.2015.24.4.27
Sajid, I., Asad, A. Z. (2018). Perception of medical superintendents of public hospitals regarding
factors affecting health in Punjab, Pakistan. Journal of the Liaquat University of Medical and Health
Sciences, 17(2), 113-116. doi:10.22442/jlumhs.181720562
Saklayen, M. G., Deshpande, N. V. (2016). Timeline of history of hypertension treatment. Frontiers in
Cardiovascular Medicine, 3, 3. doi: 10.3389/fcvm.2016.00003
Saleem, F., Hassali, A. A., Shafie, A. A. (2010). Hypertension in Pakistan: Time to take some serious
action. British Journal of General Practice, 60(575), 449-450. doi: 10.3399/bjgp10X502182
Saleem, F., Hassali, M., Shafie, A. A., Bashir, S., Atif, M. (2011). Perceptions of disease state
management among Pakistani hypertensive patients: Findings from a focus group discussion.
Tropical Journal of Pharmaceutical Research, 10(6), 833-840. doi: 10.4314/tjpr.v10i6.18

201
Saleem, F., Hassali, M., Shafie, A., Atif, M. (2012). Drug attitude and adherence: A qualitative insight
of patients with hypertension. Journal of Young Pharmacists 4(2), 101-107. doi: 10.4103/0975-
1483.96624
Saleem, F., Hashmi, FK., Atif, N., Bukhari, NI., Ahsan, M. (2015). A cross sectional assessment of
health literacy among cardiovascular patients in Karachi, Pakistan. Health Economics and outcome
Research, 1(1). doi:10.4172/2471-268x/1000101
Salyers, M. P., Bonfils, K. A., Luther, L., Firmin, R. L., White, D. A., Adams, E. L., Rollins, A. L. (2017).
The relationship between professional burnout and quality and safety in healthcare: A meta-
analysis. Journal of General Internal Medicine, 32(4), 475-482. doi:10.1007/s11606-016-3886-9
Samara, A., Nistrup, A., AL-Rammah, T. Y., Aro, A. R. (2015). Lack of facilities rather than sociocultural
factors as the primary barrier to physical activity among female Saudi university students.
International Journal of Women's Health, 7, 279-286. doi: 10.2147/IJWH.S80680
Sanjari, M., Bahramnezhad, F., Fomani, F. K., Shoghi, M., Cheraghi, M. A. (2014) Ethical challenges of
researchers in qualitative studies: The necessity to develop a specific guideline. Journal of Medical
Ethics and History of Medicine, 7(14).
Saqib, A., Atif, M., Ikram, R., Riaz, F., Abubakar, M., Scahill, S. (2018). Factors affecting patients'
knowledge about dispensed medicines: A Qualitative study of healthcare professionals and patients
in Pakistan. PloS one, 13(6), e0197482. doi:10.1371/journal.pone.0197482
Saremi, A., Hanson, R. L., Tulloch-Reid, M., Williams, D. E., Knowler, W. C. (2004). Alcohol
consumption predicts hypertension but not diabetes. Journal of Studies on Alcohol and Drugs, 65(2),
184-190. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/15151348
Sarwar, S., Abbasi, S. A. (2013). An in-depth analysis of women’s labour force participation in
Pakistan. Middle-East Journal of Scientific Research, 15(2), 208-215. Retrieved from
https://www.researchgate.net/publication/286124495_An_in-
depth_analysis_of_women%27s_labor_force_participation_in_Pakistan
Sathyanarayana Rao, T. S., Asha, M. R., Jagannatha Rao, K. S., Vasudevaraju, P. (2009). The
biochemistry of belief. Indian Journal of Psychiatry, 51(4), 239-241. doi: 10.4103/0019-5545.58285
Sattar, A. (2003). Fifty years of Kashmir dispute: The diplomatic aspect. In K. R. Gupta (Ed), India-
Pakistan relations with special reference to Kashmir. New Delhi: Atlantic Publishers.
Savin-Baden, M., Major, CH. (2004). Foundations of problem-based learning. Maidenhead: Open
University Press; 2004.
Savery, J. D., Duffy, T. M. (1995). Problem based learning: An instructional model and its
constructivist framework. Educational Technology, 35, 31-38. Retrieved from
http://works.bepress.com/john_savery/4/
202
Schroeder, K., Fahey, T., Ebrahim, S. (2004). Interventions for improving adherence to treatment in
patients with high blood pressure in ambulatory settings. Cochrane Database of Systematic Reviews
(Online), 2: CD004804. doi: 10.1002/14651858.CD004804
Schulze, M. B., Hoffmann, K., Kroke, A., Boeing, H. (2003). Risk of hypertension among women in the
EPIC-Potsdam Study: Comparison of relative risk estimates for exploratory and hypothesis-oriented
dietary patterns. American Journal of Epidemiology, 158(4), 365-373. doi: 10.1093/aje/kwg156
Seedhouse, D. (2004). Health Promotion: Philosophy, Prejudice and Practice. West Sussex: John
Wiley and Sons.
Sensky, T. (1996). Eliciting lay beliefs across cultures: Principles and methodology. British Journal of
Cancer, 74(29), S63-S65. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2149866/
Seibert, P. S., Stridh-Igo, P., Zimmerman, C. G. (2002). A checklist to facilitate cultural awareness and
sensitivity. Journal of Medical Ethics, 28(3), 143-146. doi:10.1136/jme.28.3.143
Seidel, J. (1991). Methods and madness in the application of computer technology to qualitative
data analysis. In Nigel G. Fielding, & Raymond M. Lee (Eds.), Using computers in qualitative Research
(pp.107-116). London: Sage.
Serour, M., Alqhenaei, H., Al-Saqabi, S., Mustafa, A. R., Ben-Nakhi, A. (2007). Cultural factors and
patients’ adherence to lifestyle measures. The British Journal of General Practice, 57(537), 291-295.
Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2043336/
Sesso, H. D., Cook, N. R., Buring, J. E., Manson, J. E., Gaziano, J. M. (2008). Alcohol consumption and
the risk of hypertension in women and men. Hypertension, 51(4), 1080-1087. doi:
10.1161/HYPERTENSIONAHA.107.104968
Setia, S., Subramaniam, K., Tay, J. C., Teo, B. W. (2017). Hypertension and blood pressure variability
management practices among physicians in Singapore. Vascular Health and Risk Management, 13,
275-285. doi: 10.2147/VHRM.S138694
Shafi, S. T., Shafi, T. (2017). A survey of hypertension prevalence, awareness, treatment, and control
in health screening camps of rural central Punjab, Pakistan. Journal of Epidemiology and Global
Health, 7(2), 135-140. doi: 10.1016/j.jegh.2017.01.001
Shah, S. M., Zaidi, S., Ahmed, J., Rehman, S. U. (2016). Motivation and retention of physicians in
primary healthcare facilities: A qualitative study from Abbottabad, Pakistan. International journal of
health policy and management, 5(8), 467-475. doi:10.15171/ijhpm.2016.38
Shaheed, F. (2010). Contested identities: Gendered politics, gendered religion in Pakistan. Third
World Quarterly, 31(6), 851-867. doi:10.1080/01436597.2010.502710
Shaheen, K., Oyebode, O., Masud, H. (2018). Experiences of young smokers in quitting smoking in
twin cities of Pakistan: a phenomenological study. BMC public health, 18(1), 466.
doi:10.1186/s12889-018-5388-7

203
Shahrbabaki, P. M., Nouhi, E., Kazemi, M., Ahmadi, F. (2017). Spirituality: A panacea for patients
coping with heart failure. International Journal of Community Based Nursing and Midwifery, 5(1), 38-
48. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5219564/
Shaikh, B. T., Hatcher, J. (2005). Health seeking behaviour and health service utilization in Pakistan:
Challenging the policy makers. Journal of Public Health, 27(1), 49-54. doi: 10.1093/pubmed/fdh207
Shaikh, B. T., Haran, D., Hatcher, J. (2008). Where do they go, whom do they consult, and why?
Health-seeking behaviors in the northern areas of Pakistan. Qualitative Health Research, 18(6), 747-
755. doi: 10.1177/1049732308317220
Shaikh, B. T., Rabbani, F., Safi, N., Dawar, Z. (2010). Contracting of primary health care services in
Pakistan: Is up-scaling a pragmatic thinking? Journal of the Pakistan Medical Association, 60(5), 387-
389.
Shamsi, A., Nayeri, N., Esmaeili, M. (2017). Living with hypertension: A qualitative research.
International Journal of Community Based Nursing and Midwifery, 5(3), 219-230. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5478742/
Sharma, B., Agrawal, M. (2017). Factors affecting adherence to healthy lifestyle. International
Journal of Pure & Applied Biosciences, 5(4), 105-116.
doi.org/10.18782/2320-7051.5342
Sharman, J. E., La Gerche, A., Coombes, J. S. (2015). Exercise and cardiovascular risk in patients with
hypertension. American Journal of Hypertension, 28(2), 147-158. doi: 10.1093/ajh/hpu191
Shaw, I. (2002). How lay are lay beliefs? Health, 6(3), 287-299. doi: 10.1177/136345930200600302
Shawahna, R., Rahman, N. U., Ahmad, M., Debray, M., Declèves, X., … Blom, M. (2012). Prescribers’
perspectives of the socioeconomic status and important indicators affecting prescribing behavior in
a developing country. Central European Journal of Medicine, 7(1), 129-136. doi: 10.2478/s11536-
011-0123-0
Shenton, A. K., Hayter, S. (2004). Strategies for gaining access to organisations and informants in
qualitative studies. Education for Information, 22(3-4), 223-231. doi:10.3233/EFI-2004-223-404
Shima, R., Farizah, M. H., Majid, H. A. (2014). A qualitative study on hypertensive care behavior in
primary health care settings in Malaysia. Patient Preference and Adherence, 8, 1597-1609. doi:
10.2147/PPA.S69680
Shimazu, T., Kuriyama, S., Hozawa, A., Ohmori, K., Sato, Y., Nakaya, N., … Tsuji, I. (2007). Dietary
patterns and cardiovascular disease mortality in Japan: A prospective cohort study. International
Journal of Epidemiology, 36(3), 600-609. doi: 10.1093/ije/dym005
Shin, J.-Y., Kim, J.-M., Kim, Y. (2013). Associations between dietary patterns and hypertension among
Korean adults: The Korean National Health and Nutrition Examination Survey (2008-2010). Nutrition
Research and Practice, 7(3), 224-232. doi: 10.4162/nrp.2013.7.3.224

204
Shiyanbola, O. O, Farris, K. B, Chrischilles, E. (2012). Concern beliefs in medications: Changes over
time and medication use factors related to a change in beliefs. Research in Social and Administrative
Pharmacy, 9(4), 446-457. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/22999805
Shortell, S. M., Singer, S. J. (2008). Improving patient safety by taking systems seriously. The Journal
of the American Medical Association, 299(4), 445-447. doi: 10.1001/jama.299.4.445
Shuval, K., Weissblueth, E., Araida, A., Brezis, M., Faridi, Z., … Katz, D. L. (2008). The role of culture,
environment, and religion in the promotion of physical activity among Arab Israelis. Preventing
Chronic Disease, 5(3), 88. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2483551/
Siegel, D. (2005). Barriers to and strategies for effective blood pressure control. Vascular Health and
Risk Management, 1(1), 9-14. doi: 10.2147/vhrm.1.1.9.58940
Silverman, D. (1993). Interpreting Qualitative Data: Methods for Analysing Talk, Text and Interaction.
London: Sage Publications.
Silverman, J., Kurtz, S. M., Draper, J. (2005). Skills for communicating with patients (2nd ed.). Oxford:
Radcliffe.
Silverman, D. (2010). Doing Qualitative Research. London: Sage Publications.
Singer, M., Clair, S. (2003). Syndemics and public health: Reconceptualizing disease in bio-social
context. Medical Anthropology Quarterly, 17(4), 423-441. doi: 10.1525/maq.2003.17.4.423
Singer, E., Couper, M. P. (2017). Some methodological uses of responses to open questions and
other verbatim comments in quantitative surveys. Methoden, Daten, Analysen, 11(2), 115-135.
doi:10.12758/mda.2017.01
Skliros, E. A., Papadodima, S. A., Sotiropoulos, A., Xipnitos, C., Kollias, A., Spiliopoulou, C. A. (2012).
Relationship between alcohol consumption and control of hypertension among elderly Greeks. The
Nemea primary care study. Hellenic Journal of Cardiology, 53(1), 26-32.
Smith, J., Noble, H. (2016). Reviewing the literature. Evidence-Based Nursing, 19(1), 2-3. doi:
10.1136/eb-2015-102252
Srikanth, J., Kulkarni, S. (2015). Hypertension in elderly: Prevalence and health care seeking pattern
in an urban slum of Bangalore City. International Journal of Recent Scientific Research, 6: 2952-2957.
Retrieved from http://www.recentscientific.com/hypertension-elderly-prevalence-and-health-care-
seeking-pattern-urban-slum-bangalore-city?page=6
Srivastava, A., Kandpal, S., Sati, H. (2015). Predictors for adherence in hypertensive therapy - A study
in rural area of District Dehradun. Indian Journal of community health, 27(3), 320-326. Retrieved
from http://www.iapsmupuk.org/journal/index.php/IJCH/article/view/993/722
Spruill, T. M. (2010). Chronic psychosocial stress and hypertension doi:10.1007/s11906-009-0084-8

205
Staessen, A., Wang, J., Bianchi, G., Birkenhäger, W. H. (2003). Essential hypertension. Lancet,
361(9369), 1629-1641. doi: 10.1016/S0140-6736(03)13302-8
Stanton, R. W., Balanda, P. K., Gillespie, A. M., Lowe, B. J. (1996). Barriers to health promotion
activities in public hospitals. Australian and New Zealand Journal of Public Health, 20(5), pp. 500-
504. Retrieved from https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.1467-842X.1996.tb01629.x
Stavropoulou, C. (2012). Perceived information needs and non-adherence: evidence from Greek
patients with hypertension. Health expectations: an international journal of public participation in
health care and health policy, 15(2), 187-196. doi:10.1111/j.1369-7625.2011.00679.x
Stead, M., Angus, K., Holme, I., Cohen, D., Tait, G., Team, PER. (2009). Factors influencing European
GPs' engagement in smoking cessation: a multi-country literature review. The British Journal of
General Practice. 59(566), 682-690. doi: 10.3399/bjgp09X454007
Stevens, S. L., Wood, S., Koshiaris, C., Law, K., Glasziou, P., … McManus, R. J. (2016). Blood pressure
variability and cardiovascular disease: Systematic review and meta-analysis. The British Medical
Journal, 354(354), 4098. doi: 10.1136/bmj.i4098
Stevenson, F., Scambler, G. (2005). The relationship between medicine and the public: the challenge
of concordance. Health, 9(1), 5-21. doi.org/10.1177/1363459305048091
Stewart, J., Manmathan, G., Wilkinson, P. (2017). Primary prevention of cardiovascular disease: A
review of contemporary guidance and literature. JRSM cardiovascular disease, 6.
doi:10.1177/2048004016687211
Stokols, D., Milden, S. (2004). Physicians’ attitudes and practices regarding complementary and
alternative medicine, eScholarship, University of California.
Storni, C. (2015). Patients' lay expertise in chronic self‐care: A case study in type 1 diabetes. Health
Expectations, 18(5), 1439-1450. doi: 10.1111/hex.12124
Strauss, A., Corbin, J. (1990). Basics of Grounded Theory Methods. Beverly Hills: Sage Publications.
Straznicky, N. E., Louis, W. J., McGrade, P., Howes, L. G. (1993). The effects of dietary lipid
modification on blood pressure, cardiovascular reactivity and sympathetic activity in man. Journal of
Hypertension, 11(4), 427-437. doi: 10.1136/bmj.b4567
Strazzullo, P., D'Elia, L., Kandala, N. B., Cappuccio, F. P. (2009). Salt intake, stroke, and cardiovascular
disease: Meta-analysis of prospective studies. The British Medical Journal, 339: b4567. doi:
10.1136/bmj.b4567
Street, R. L., Gordon, H., Haidet, P. (2007). Physicians' communication and perceptions of patients: Is
it how they look, how they talk, or is it just the doctor? Social Science and Medicine, 65(3), 586-598.
doi: 10.1016/j.socscimed.2007.03.036

206
Street, Jr, R. L., Haidet, P. (2011). How well do doctors know their patients? factors affecting
physician understanding of patients’ health beliefs. Journal of General Internal Medicine, 26(1), 21-
27. doi:10.1007/s11606-010-1453-3
Study Quality Assessment Tools. The National Heart, Lung and Blood Institute (NHLBI) (2017).
Available at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
Subramanian, K., Midha, I. (2016). Prevalence and perspectives of complementary and alternative
medicine among university students in Atlanta, Newcastle upon Tyne, and new Delhi. International
Scholarly Research Notices, 2016, 9309534-9. doi:10.1155/2016/9309534
Sumbal, A. M. (2014, February 07). Pakistan: Quacks make killing with cheap cures, Gulf News Asia.
Suwazono, Y., Dochi, M., Sakata, K., Okubo, Y., Oishi, M., … Nogawa, K. (2008). Shift work is a risk
factor for increased blood pressure in japanese men: A 14-year historical cohort study. Hypertension,
52(3), 581-586. doi: 10.1161/HYPERTENSIONAHA.108.114553
Swami, V., Arteche, A., Chamorro-Premuzic, T., Maakip, I., Stanistreet, D., Furnham, A. (2009). Lay
perceptions of current and future health, the causes of illness, and the nature of recovery: Explaining
health and illness in Malaysia. British Journal of Health Psychology, 14(3), 519-540. doi:
10.1348/135910708X370781
Tahir, M. W., Kauser, R., Tahir, M. A. (2011). Brain drain of doctors; causes and consequences in
Pakistan, World Academy of Science, Engineering and Technology International Journal of
Humanities and Social Sciences, 5(3), doi: 10.5281/zenodo.1328497
Talati, J. J., Pappas, G. (2006). Migration, medical education, and health care: A view from Pakistan.
Academic Medicine, 81(12), S55-S62. doi: 10.1097/01.ACM.0000243543.99794.07
Tan, N., Khin, W. L., Pagi, R. (2005). Home blood-pressure monitoring among hypertensive patients
in an Asian population. Journal of Human Hypertension, 19: 559-564. Retrieved from
https://www.nature.com/articles/1001865.pdf?origin=ppub
Tan, C. S., Hassali, M. A., Neoh, C. F., Saleem, F. (2017). A qualitative exploration of hypertensive
patients' perception towards quality use of medication and hypertension management at the
community level. Pharm Pract (Granada), 15(4), 1074. doi: 10.18549/PharmPract.2017.04.1074
Tarin, E., Green, A., Omar, M., Shaw, J. (2009). Policy process for health sector reforms: A case study
of Punjab province (Pakistan). International Journal of Health Planning and Management, 24(4), 306-
325. doi: 10.1002/hpm.1010
Taylor, D. (2014). Physical activity is medicine for older adults. Postgraduate Medical Journal,
90(1059), 26. Retrieved from http://pmj.bmj.com/content/90/1059/26.abstract
Telfer, C. (2018). Patient perspectives: Exploring patient values and preferences. Canadian Family
Physician Medecin de Famille Canadien, 64(1), 10-11. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5962996/

207
Teoh, S. H., Razlina, A. R., Norwati, D., Siti Suhaila, M. Y. (2017). Patients’ blood pressure control and
doctors’ adherence to hypertension clinical practice guideline in managing patients at health clinics
in Kuala Muda district, Kedah. The Medical Journal of Malaysia, 72(1), 18-25. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/28255135
Timonen, V., Foley, G., Conlon, C. (2018). Challenges when using grounded theory: A pragmatic
introduction to doing GT research. International Journal of Qualitative Methods, 17(1),
160940691875808. doi:10.1177/1609406918758086.
Thomas, G., James, D. (2006). Reinventing grounded theory: Some questions about theory, ground
and discovery. British Educational Research Journal, 32(6), 767-795.
doi:10.1080/01411920600989412
Thomas, A., Menon, A., Boruff, J., Rodriguez, A. M., Ahmed, S. (2014). Applications of social
constructivist learning theories in knowledge translation for healthcare professionals: A scoping
review. Implementation Science, 9(1), 54. doi: 10.1186/1748-5908-9-54
Thompson, P. D., Buchner, D., Pina, I. L., Balady, G. J., Williams, M. A., … Wenger, N. K. (2003).
Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular
disease: A statement from the Council on Clinical Cardiology (Subcommittee on Exercise,
Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism
(Subcommittee on Physical Activity). Circulation, 107(24), 3109-3116. doi:
10.1161/01.cir.0000075572.40158.77
Thompson, A. G. H. (2007). The meaning of patient involvement and participation in health care
consultations: A taxonomy. Social Science & Medicine, 64(6), 1297-1310.
doi:10.1016/j.socscimed.2006.11.002
Thonemann, P. (2013). Roman Phrygia: Culture and Society. New York: Cambridge University Press.
Thornberg, R. (2012). Informed grounded theory. Scandinavian Journal of Educational Research,
56(3), 243-259. doi:10.1080/00313831.2011.581686
Thornberg, R., Charmaz, K. (2014). Grounded theory and theoretical coding.
Thuy, A. B., Blizzard, L., Schmidt, M., Luc, P. H., Granger, R., Dwyer, T. (2010). The association
between smoking and hypertension in a population-based sample of Vietnamese men. Journal of
Hypertension, 28(2), 245-250. doi: 10.1097/HJH.0b013e32833310e0
Tuckett, D. (1985). Meetings between experts: An approach to sharing ideas in medical
consultations. London: Tavistock.
Turner, J. R. (2013). Patient and physician adherence in hypertension management. The Journal of
Clinical Hypertension, 15(7), 447-452. doi:10.1111/jch.12105
Udompittayason, W., Boonyasopun, U., Songwathana, P. (2015). Perspectives on hypertension
among Thai-Melayu elderly in a province of Southern Thailand: An ethnographic study.

208
Songklanagarind Journal of Nursing, 35(2), 45-59. Retrieved from https://www.tci-
thaijo.org/index.php/nur-psu/article/view/38695/32012
Usman, A., Baig, A., Amjad, A., Amjad, U. (2015). Reformative measures for Basic Health Units in
Pakistan. Iranian Journal of Public Health, 44(8), 1158-1159 Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4645741/
Vahdat, S., Hamzehgardeshi, L., Hessam, S., Hamzehgardeshi, Z. (2014). Patient involvement in
health care decision making: A review. Iranian Red Crescent medical journal, 16(1), e12454. doi:
10.5812/ircmj.12454
Vamvakis, A., Gkaliagkousi, E., Triantafyllou, A., Gavriilaki, E., Douma, S. (2017). Beneficial effects of
nonpharmacological interventions in the management of essential hypertension. JRSM
cardiovascular disease, 6. doi: 10.1177/2048004016683891
Van der Zwet, J., Zwietering, P. J., Teunissen, P. W., van der Vleuten, C. P., Scherpbier, A. J. (2011).
Workplace learning from a socio-cultural perspective: creating developmental space during the
general practice clerkship. Advances in health sciences education: theory and practice, 16(3), 359-
373. doi:10.1007/s10459-010-9268-x
Vellakkal, S., Millett, C., Basu, S., Khan, Z., Aitsi-Selmi, A., Stuckler, D., Ebrahim, S. (2015). Are
estimates of socioeconomic inequalities in chronic disease artefactually narrowed by self-reported
measures of prevalence in low-income and middle-income countries? Findings from the WHO-SAGE
survey. Journal of Epidemiology and Community Health, 69(3), 218-225. doi: 10.1136/jech-2014-
204621
Virdis, A., Giannarelli, C., Neves, M. F., Taddei, S., Ghiadoni, L. (2010). Cigarette smoking and
hypertension. Current Pharmaceutical Design, 16(23), 2518-2525. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/20550499
Vos, T., Allen, C., Arora, M., Barber, R. M., Bhutta, Z. A. (2016). Global, regional, and national
incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A
systematic analysis for the global burden of disease study 2015. The Lancet, 388(10053), 1545-1602.
doi: 10.1016/S0140-6736(16)31678-6
Vos, T., Allen, C., Arora, M., Barber, R. M., Bhutta, Z. A., Medicinsk vetenskap. (2016). Global,
regional, and national incidence, prevalence, and years lived with disability for 310 diseases and
injuries, 1990–2015: A systematic analysis for the global burden of disease study 2015. The Lancet,
388(10053), 1545-1602. doi:10.1016/S0140-6736(16)31678-6
Vrijkotte, T. G. M. (2000). Effects of work stress on ambulatory blood pressure, heart rate, and heart
rate variability. The Journal of the American Medical Association, 284(1), 23. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/10775555
Wagner, E. H., Groves, T. (2002). Care for chronic diseases. The British Medical Journal, 325(7370),
913-914. doi: 10.1136/bmj.325.7370.913
209
Wagenaar, B. H., Gimbel, S., Hoek, R., Pfeiffer, J., Michel, C., Cuembelo, F., Sherr, K. (2016). Wait and
consult times for primary healthcare services in central Mozambique: a time-motion study. Global
health action, 9, 31980. doi:10.3402/gha.v9.31980
Wahner-Roedler, D. L., Vincent, A., Elkin, P. L., Loehrer, L. L., Cha, S. S., Bauer, B. A. (2006).
Physicians' attitudes toward complementary and alternative medicine and their knowledge of
specific therapies: a survey at an academic medical centre. Evidence-based complementary and
alternative medicine, eCAM, 3(4), 495-501. doi:10.1093/ecam/nel036
Wajid, A., White, F., Karim, M. S. (2013). Community health workers and health care delivery:
Evaluation of a women's reproductive health care project in a developing country. Plos One, 8(9),
e75476. doi: 10.1371/journal.pone.0075476
Wakabayashi, I. (2008). Influence of gender on the association of alcohol drinking with blood
pressure. American Journal of Hypertension, 21(12), 1310-1317. doi: 10.1038/ajh.2008.299
Walseth, L. T., Abildsnes, E., Schei, E. (2011). Patients' experiences with lifestyle counselling in
general practice: a qualitative study. Scandinavian journal of primary health care, 29(2), 99-103.
doi:10.3109/02813432.2011.553995
Wall, H. K., Hannan, J. A., Wright, J. S. (2014). Patients with undiagnosed hypertension: hiding in
plain sight. The Journal of the American Medical Association, 312(19), 1973-1974.
doi:10.1001/jama.2014.15388
Wallace, J. P. (2003). Exercise in hypertension. A clinical review. Sports Medicine, 33(8), 585-598
Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/12797840
Wand, Y., Weber, R. (1993). On the ontological expressiveness of information systems analysis and
design grammars. Journal of Information Systems, 3(4), 217-237.doi: org/10.1111/j.1365-
2575.1993.tb00127.x
Wang, L., Manson, J. E., Buring, J. E., Lee, I. M., Sesso, H. D. (2008). Dietary intake of dairy products,
calcium, and vitamin D and the risk of hypertension in middle-aged and older women. Hypertension,
51(4), 1073-1079. doi: 10.1161/HYPERTENSIONAHA.107.107821
Wang, L., Manson, J. E., Forman, J. P., Gaziano, J. M., Buring, J. E., Sesso, H. D. (2010). Dietary fatty
acids and the risk of hypertension in middle-aged and older women. Hypertension, 56(4), 598-604.
doi: 10.1161/hypertensionaha.110.154187
Warburton, D. E. R., Nicol, C. W., Bredin, S. S. D. (2006). Health benefits of physical activity: The
evidence. Canadian Medical Association Journal, 174(6), 801-809. doi: 10.1503/cmaj.051351
Warde, F., Papadakos, J., Papadakos, T., Rodin, D., Salhia, M., Giuliani, M. (2018). Plain language
communication as a priority competency for medical professionals in a globalized world. Canadian
Medical Education Journal. 39(2), e52-e59. PMID: 30018684; PMCID: PMC6044302.
Wardle, J., Roseen, E. (2014). Integrative medicine case reports: A clinicians' guide to publication.
Advances in Integrative Medicine, 1(3), 144-147. doi: 10.1016/j.aimed.2014.12.001
210
Wassenaar, D. R., Singh, S. (2016). Contextualising the role of the gatekeeper in social science
research. South African Journal of Bioethics and Law, 9(1), 42-46. doi:10.7196/SAJBL.2016.v9i1.465
Wasay, M., Jabbar, A., (2009). Fight against chronic diseases (high blood pressure, stroke, diabetes
and cancer) in Pakistan; cost-effective interventions. The Journal of Pakistan Medical Association,
59(4), 196-197. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/19402275
Wasfy, M., Baggish, A. L. (2016). Exercise dose in clinical practice. Circulation, 133(23), 2297-2313.
doi: 10.1161/CIRCULATIONAHA.116.018093
Watt, I., Nettleton, S. Burrows, R. (2008). The views of doctors on their working lives: A qualitative
study. Journal of the Royal Society of Medicine, 101, 592-597. doi: 10.1258/jrsm.2008.080195
Weierbach, F. M., Glick, D. F., Fletcher, K., Rowlands, A., Lyder, C. H. (2010). Nursing research and
participant recruitment: Organizational challenges and strategies. JONA: The Journal of Nursing
Administration, 40(1), 43-48. doi:10.1097/NNA.0b013e3181c97afb
Weiner, S.J., Schwartz, A., Sharma, G., Binns-Calvey, A., Ashley, N., Kelly, B., Harris, I. (2013). Patient-
centred decision making and health care outcomes: An observational study, Annuals of Internal
Medicine, 158 (8), 573-579, 10.7326/0003-4819-158-8-201304160-00001
Weinman, J., Petrie, K. J. (1997). Illness perceptions: A new paradigm for psychosomatics? Journal of
Psychosomatic Research, 42(2), 113-116. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/9076639
Weitzman, E. A. (2000). Software and qualitative research. In N. K. Denzin & Y. S. Lincoln (Eds.),
Collecting and Interpreting Qualitative Data. London: Sage Publications.
Wengraf, T. (2001). Qualitative research interviewing: Biographic narrative and semi-structured
methods. London: SAGE.
West, C.P., Dyrbye, L.N., Shanafelt, T.D. (2018). Physician burnout: Contributors, consequences and
solutions. Journal of Internal Medicine, 283, 516-529. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/29505159
Whelton, S. P, Chin, A., Xin, X., He J. (2002). Effect of aerobic exercise on blood pressure: A meta-
analysis of randomized, controlled trials. Annals of Internal Medicine. 136, 493-503. doi:
10.7326/0003-4819-136-7-200204020-00006
White, P. (2005). Biopsychosocial medicine. Oxford: Oxford University Press.
Wiggers, L. C. W., Smets, E. M. A., de Haes, J. C. J. M., Peters, R. J. G., Legemate, D. A. (2003).
Smoking cessation interventions in cardiovascular patients. European Journal of Vascular and
Endovascular Surgery, 26(5), 467-475. doi: 10.1016/S1078-5884(03)00347
Wikimedia Commons. (2018). Subdivisions of Pakistan. Retrieved from
https://commons.wikimedia.org/wiki/File:Pakistan_Dive.png
211
Williams, G. H., Popay, J. (1994). Researching the People's Health. Hoboken: Routledge.
Williams, G. H., Popay, J. (1994) Lay knowledge and the privilege of experience. In J. Gabe, D.
Kelleher & G. H. Williams (Eds.) Challenging Medicine. London: Routledge.
Williams, P. T. (2001). Physical fitness and activity as separate heart disease risk factors: A meta-
analysis. Medicine & Science in Sports & Exercise, 33(5), 754-761.
Williams, G. H. (2014). Lay expertise. In W. C. Cockerham (Ed.) The Wiley Blackwell Encyclopedia of
Health, Illness, Behavior, and Society, 1283-1288. Chichester: Wiley-Blackwell. doi:
10.1002/9781118410868.wbehibs555
Williams, B., Mancia, G., Spiering, W., Agabiti Rosei, E., Azizi, M., Burnier, M. (2018). 2018 ESC/ESH
guidelines for the management of arterial hypertension. European Heart Journal, 39(33), 3021-3104.
doi: 10.1093/eurheartj/ehy339
Wilson, R. P., Freeman, A., Kazda, M. J., Andrews, T. C., Berry, L., Vaeth, P. A. C., Victor, R. G. (2002).
Lay beliefs about high blood pressure in a low- to middle-income urban African-American
community: An opportunity for improving hypertension control. The American Journal of Medicine,
112(1), 26-30. doi:10.1016/S0002-9343(01)01049-X
Wilson, I. B., Schoen, C., Neuman, P., Strollo, M. K., Rogers, W. H., Chang, H., Safran, D. G. (2007).
Physician-patient communication about prescription medication nonadherence: a 50-state study of
America's seniors. Journal of general internal medicine, 22(1), 6-12. doi:10.1007/s11606-006-0093-0
Windak, A., Gryglewska, B., Tomasik, T., Narkiewicz, K., Grodzicki, T. (2009). Competence of general
practitioners in giving advice about changes in lifestyle to hypertensive patients. Medical Decision
Making: An International Journal of the Society for Medical Decision Making, 29(2), 217-223. doi:
10.1177/0272989x08324956
Wolszakiewicz, J., Piotrowicz, E., Foss-Nieradko, B., Dobraszkiewicz-Wasilewska, B., Piotrowicz, R.
(2015). A novel model of exercise walking training in patients after coronary artery bypass grafting.
Polish Heart Journal, 73(2), 118-126. doi: 10.5603/KP.a2014.0165
World Development Indicators. (2013). Pakistan. World Bank.
World Health Organization. (2002). The World Health Report 2002: Reducing Risks, Promoting
Healthy Life. Switzerland: WHO.
World Health Organization. (2004). Global status report on alcohol 2004. Geneva: WHO.
World Health Organization. (2007). Health System Profile Pakistan. Regional Health System
Observatory. WHO.
World Health Organization. (2007). Reducing salt intake in populations. France: WHO.

212
World Health Organization (2009) Global health risks: Mortality and burden of disease attributable
to selected major risks. Geneva: WHO.
World Health Organization. (2011). Global Status Report on Noncommunicable Diseases 2010.
Switzerland: WHO.
World Health Organization. (2013). A Global Brief on Hypertension: Silent Killer, Global Public Health
Crisis. Switzerland: WHO.
World Health Organization. (2014). Adherence to Long Term Therapies - Evidence for Action.
Switzerland: WHO.
World Health Organization. (2016). Patient Engagement: Technical Series on Safer Primary Care.
Switzerland: WHO.
World Health Organization. (2019). Tobacco. Switzerland: WHO.
World Health Organization. (2019). Facing the Facts: The Impact of Chronic Disease in Pakistan.
Switzerland: WHO.
Wray, S., Bartholomew, M. (2010). Some reflections on outsider and insider identities in ethnic and
migrant qualitative research, Migration Letters, 7(1), pp.7-16.
Wu, C. H. V., Beaunae, C. (2014). Personal reflections on cautions and considerations for navigating
the path of grounded theory doctoral theses and dissertations: A long walk through a dark for-est.
International Journal of Social Research Methodology, 17, 249-265.
doi:10.1080/13645579.2012.729392.
Wu, J., Li, T., Song, X., Sun, W., Zhang, Y., … Liu, B. (2018). Prevalence and distribution of
hypertension and related risk factors in jilin province, china 2015: A cross-sectional study. BMJ Open,
8(3), doi: 10.1136/bmjopen-2017-020126
Xin, X., He, J., Frontini, M. G., Ogden, L. G., Motsamai, O. I., Whelton, P. K. (2001). Effects of alcohol
reduction on blood pressure: A meta-analysis of randomized controlled trials. Hypertension, 38(5),
1112-1117. doi: 10.1161/hy1101.09342423
Yasir, N. (2014). Health implications of hospital waste management practices in Gujrat Pakistan.
Masters’ dissertation, Norwegian University of Life Sciences, Norway.
Ypinazar, V. A., Margolis, S. A. (2006). Delivering culturally sensitive care: The perceptions of older
Arabian gulf Arabs concerning religion, health, and disease. Qualitative Health Research, 16(6), 773-
787. doi:10.1177/1049732306288469
Yuan, M., Chen, W., Teng, B., Fang, Y. (2016). Occupational disparities in the association between
self-reported salt-eating habit and hypertension in older adults in Xiamen, China. International
Journal of Environment Research and Public Health, 13(1), doi: 10.3390/ijerph13010148

213
Zaidi, S. A., Bigdeli, M., Aleem, N., Rashidian, A. (2013). Access to essential medicines in Pakistan:
Policy and health systems research concerns. PLoS One, 8(5), e63515. doi:
10.1371/journal.pone.0063515
Zaidi, S. A., Bigdeli, M., Langlois, E. V., Riaz, A., Orr, D. W., Idrees, N., Bump, J. B. (2019). Health
systems changes after decentralisation: Progress, challenges and dynamics in Pakistan. The British
Medical Journal Global Health, 4(1), doi: 10.1136/bmjgh-2018-001013
Zaman, A. Q., Norton, A., Eickelman, D. (2018). Islam in Pakistan: A history. United Kingdom,
Princeton University Press.
Zanini, C., Sarzi-Puttini, P., Atzeni, F., Di Franco, M., Rubinelli, S. (2014). Doctors' insights into the
patient perspective: A qualitative study in the field of chronic pain. BioMed Research International,
2014, 514230-6. doi:10.1155/2014/514230
Zarar, R., Bukhsh, M. M., Khasheli, A. K. (2017). Causes and consequences of gender discrimination
against women in Quetta city. Arts and Social Sciences Journal, 8, 1-6.
Zhao, Y., Lu, F., Sun, H., Liu, Z., Zhao, Y., … Zhang, H. (2012). Trends in hypertension prevalence,
awareness, treatment, and control rates in Shandong province of China. The Journal of Clinical
Hypertension, 14(9), 637-643. doi: 10.1111/j.1751-7176.2012.00670.x
Zheng, P.-F., Shu, L., Zhang, X.-Y., Si, C.-J., Yu, X.-L., Gao, W., … Zhang, L. (2016). Association between
dietary patterns and the risk of hypertension among Chinese: A cross-sectional study. Nutrients, 8(4),
239. doi: 10.3390/nu8040239
Zhou, B., Bentham, J., Di Cesare, M., Bixby, H., Danaei, G., … Institute of Medicine, Department of
Public Health and Community Medicine. (2017). Worldwide trends in blood pressure from 1975 to
2015: A pooled analysis of 1479 population-based measurement studies with 19.1 million
participants. The Lancet, 389(10064), 37-55. doi: 10.1016/S0140-6736(16)31919-5
Zinat Motlagh, S. F., Chaman, R., Sadeghi, E., Eslami, A. A. (2016). Self-Care behaviours and related
factors in hypertensive patients. Iranian Red Crescent Medical Journal, 18(6), e35805. doi:
10.5812/ircmj.35805
Zubair, M., Martin, W., Victor, C. (2012). Embodying gender, age, ethnicity and power in 'the field':
Reflections on dress and the presentation of the self in research with older Pakistani Muslims.
Sociological Research Online, 17(3), 1-18. doi:10.5153/sro.2667
Zusman, R. M. (2009). Hypertension: Controlling the silent killer. Boston: Harvard Health Publications.

214
Appendices
Appendix 1: Search Strategy with a PRISMA flow diagram
No of articles screened by title and
abstract n=562
No of articles excluded n= 401
duplicates n=102
Total number of selected studies
n=21
Full-text screening of articles for
assessment n=59
Excluded n=40
Not about HTN n=25
Did not report an outcome
n=9
Not a primary study n=6
1,321 potentially relevant articles
identified through electronic
databases and hand searching
No of articles included
following reference list
reviewing n=2
Excluded n=759
Studies were not conducted in
Pakistan n=758
Full text not available n=1

215
Appendix 2: Table 2.1 Detail of the included studies
Authors Study location Aim of study Sample size Methods Key findings
1: Jafar et al., 2005 Karachi, Lahore, Quetta and Peshawar
To determine whether general practitioners’ approach to high BP is in accordance with international guidelines.
In total 1000 male doctors were randomly recruited from four cities (Karachi 701, Lahore 99, Quetta 99, Peshawar 99)
Cross-sectional study Deficiencies in the knowledge and approach of GPs in Pakistan toward treatment of high BP
2: Almas et al., 2006 Karachi To determine factors affecting compliance to antihypertensive therapy.
200 hypertensive patients (66% were male 33.5% female)
Cross-sectional study Factors of noncompliance were missed doses due to forgetfulness. 11.6% could not take the medicine due to side effects and 10.4% missed dose due to increased number of tablets.
3: Ashfaq et al., 2007 Karachi To compare awareness of hypertension among patients attending Primary Health Care Centre (PHC) and outpatient department (OPD) of a tertiary care hospital of Karachi.
202 hypertensive patients (male 49: female 153)
Cross-sectional survey The tertiary OPD patients had a better knowledge of regular medication use for HTN as compared to patients coming to the PHC centre.
4: Hashmi et al., 2007 Karachi To investigate the factors associated with adherence in the studied population.
438 hypertensive patients (male 199: female 239)
Cross-sectional study Key findings are younger age, monotherapy, poor awareness and symptomatic

216
treatment to be the strongest factors affecting adherence to anti-hypertensive medication amongst Pakistani patients.
5: Ahmed et al., 2008 Abbottabad To assess the relationship of control of hypertension with factors like compliance to antihypertensive drugs, salt restriction and exercise among the hypertensive patients
89 hypertensive patients (male 22: female 67)
Cross-sectional study 48.3% patients were compliant. 51.7% were not compliant to antihypertensive drugs, 55.1% were having salt restriction and 44.9% had no salt restriction. 23.6% were used to do physical activity while 76.4% were not involved in any physical activity.
6: Ladha et al., 2009 Karachi To presents socio-demographic characteristics and health seeking behaviour of elderly and to determine frequency of HTN and diabetes in elderly population.
438 hypertensive patients (male 280: female 158)
Cross-sectional study The elderly population of this urban community has financial constraints in seeking health care. Deterrence from seeking health care was associated with illiteracy (p=0.001) and living alone (p=0.06).

217
7: Saleem et al., 2011
Quetta To explore the perceptions of disease state management among Pakistani hypertensive patients.
19 hypertensive patients (male 12: female 4)
Qualitative study (four focus group discussions)
Hypertension management was influenced by peers, family and very little information received from doctors.
8: Rehman et al., 2011
Karachi To evaluate the awareness of HTN among medical students and junior doctors.
475 doctors (no male to female ratio was provided)
Cross-sectional study The result of study indicated an inadequate level of awareness of HTN diagnosis among doctors.
9: Saleem et al., 2012
Quetta To explore the perceptions and experiences of hypertensive patients toward medication use and adherence
16 hypertensive patients (no sex ratio was mentioned)
Qualitative study (semi-structured interviews)
Poor knowledge lay perceptions and doctor attitude were noted as major contributing factors that resulted in nonadherence to therapy prescribed.
10: Almas et al., 2012
Karachi To elucidate the knowledge about hypertension in hypertensive patients
447 hypertensive patients (male 262: female 262)
Cross-sectional study Knowledge score in hypertensive patients was not up to the mark. Furthermore, score in patients with

218
uncontrolled hypertension was significantly low
11: Aslam et al., 2013
Karachi To evaluate the relationship between diet and socioeconomic conditions among hypertensive patients
176 hypertensive patients (no male to female ratio was given)
Cross-sectional study Highest frequency of HTN was in high class and high middle-income group. Low social class has the highest ratio of stress
12: Khan et al., 2014 Karachi To determine factors which can help to increase dietary compliance in hypertensive patients
400 hypertensive patients (male 262: female 138)
Cross-sectional study Knowledge score in hypertensive patients was not up to the mark. Furthermore, score in patients with uncontrolled hypertension was significantly low

219
13: Bilal et al., 2015 Karachi To determine the frequency and factors associated with non-compliance to anti-hypertensive medications.
113 hypertensive patients (male 42: female 71)
Cross-sectional study Study revealed that 68.14% patients were non-compliant out of 77. Non-compliance was found to be associated with gender, occupation and monthly income. No association is found between non-compliance and positive family history of HTN Women were non-compliant than men.
14: Khan et al., 2015
Peshawar To access primary causes of HTN in hypertensive patients
298 hypertensive patients (male 172: female 126)
A survey study Study found phycological and individual level factors. Lack of exercise, sedentary lifestyle and less knowledge about disease was pointed.
15: Hussain et al., 2015
Karachi To find out drug usage trends in Stage I hypertensive patients without any compelling indications in Karachi
100 doctors (no sex ratio was provided for doctors) In general population 200 were male and 200 female)
Two randomized stratified surveys
Doctors have misconception about the cost effectiveness of certain antihypertensive agents. Feedback received from participants showed that therapeutic

220
guidelines were not followed for choosing pharmacologic agents by the doctors.
16: Gowani et al., 2016
Karachi To explore how health perceptions and beliefs influence behaviour for non-communicable diseases prevention
30 participants in total (20 hypertensive patients in total) (male 17: female 13)
Qualitative study A sense of personal invincibility, limited knowledge, inadequate health education, health care and financial constraints appeared as key barriers to the self-management of chronic disease in participants.
17: Malik et al., 2016 Islamabad-Rawalpindi To assess the knowledge and perceptions of doctors regarding adherence to guidelines for the treatment of HTN
385 doctors (male 58.2%: female 41.8%)
A descriptive, cross-sectional study
The knowledge of doctors working in public and private healthcare facilities regarding HTN guidelines is not adequate.
18: Qamar et al., 2016
Karachi To get knowledge regarding the treatment and lifestyle modification of a hypertensive patient
200 hypertensive patients (male 100: female 100)
Cross-sectional survey Use of drugs and lifestyle modifications are helpful to decrease the morbidity and mortality rates among hypertensive patients.

221
19: Ishtiaq et al., 2017
Rawalpindi-Islamabad To estimate the prevalence of hypertension and to explore the risk factors associated with it
219 hypertensive patients (male 89: female 130)
Cross-sectional study 62.5% individuals were not interested in maintaining their health status, and 7.8% patients were not currently taking medication to control their blood pressure. Marjory of the patients were not living healthy lifestyle.
20: Murad et al., 2017
Karachi To assess the readiness of lifestyle modification among hypertensive patients
50 hypertensive patients (male 30: female 20)
Cross-sectional study Out of 50 participants 84% respondents consider lifestyle modifications as a best way to maintain their blood pressure and only 16% respondents do not implement any lifestyle modification to maintain their blood pressure.

222
21: Legido-Quigley et al., 2019
Bangladesh, Sri-Lanka, Pakistan (District Thatta)
To identify patients’ experiences of symptoms, awareness of prevention, knowledge and control of HTN
60 hypertensive patients (20 in each country)
Qualitative study Patients mentioned several difficulties in accessing services. The main barriers to accessing health services, as reported by participants, were dearth and poor quality of existing facilities, the busyness of doctors, long transportation, long waiting times and medication shortages.

223
Appendix 3i: Table 2.2 CASP checklist ten questions
23 A number of prompts are given after each question that are assessible on source https://casp-uk.net/wp-content/uploads/2018/03/CASP-Qualitative-Checklist-2018_fillable_form.pdf
CASP checklist tool based on ten questions23 for qualitative studies (n=4)
Study 1: Is there
a clear
statement
of study
aims?
2: Is qualitative
methodology
appropriate?
3: Was study design
suit to address the
aims of research?
4: Was the
recruitment
strategy
appropriate?
5: Were the
data collected in
a way that it
addressed the
research issues?
6: Was the
relationship
between
researcher
and research
participants’
been
considered?
7: Have ethical
issues been
taken into
consideration?
8: Was the data
analysis
procedure
rigorous?
9: Is there a
clear statement
of findings?
10: Is the
research
valuable?
Total score
Saleem
et al.,
2011
Yes Yes No No No No Yes No Yes Yes 5
Saleem
et al.,
2012
Yes Yes No No No No Yes No Yes Yes 4
Gowani
et al.,
2016
Yes Yes No No No No Yes No Yes Yes 5
Legido-
Quigley
et al.,
2019
Yes Yes Yes No No No Yes Yes Yes Yes 7

224
Appendix 3ii: Table 2.3 Quality assessment scores by using NHLBI criteria
Quality assessment scores according to the NHLBI Quality Assessment Tool24 for observational cross-sectional survey studies (n=17)
Study
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12 Q13 Q14 Score
Jafar et al., 2005
Yes Yes Yes No Yes NR NR Yes Yes No No Yes NR No Fair
Almas et al., 2006 Yes Yes Yes No No NR NR Yes No No No No NR No Poor
Ashfaq et al., 2007 Yes No Yes No No NR NR Yes No No Yes No NR No Poor
Hashmi et al., 2007 Yes Yes Yes No No NR NR NA Yes NA Yes No NR No Poor
Ladha et al., 2007 Yes Yes No Yes Yes NR NR NA No NA No No NR No Poor
Ahmed et al., 2008 Yes Yes Yes No No NR NR Yes No No No No NR No Poor
Rehman et al., 2011 Yes Yes Yes Yes No NR NR Yes No No No No NR No Poor
Almas et al., 2012 Yes Yes Yes No No NR NR NA Yes NA No No NR Yes Poor
24 Available at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools NA, not applicable; NR, not reported. The quality assessment criteria consisted of fourteen questions
with five tools (Yes, No, Not Applicable NA, Not Relevant NR, Not Determined ND) and used to guide the overall rating for the quality of each study as ‘good’, ‘fair’ or ‘poor’.

225
Aslam et al., 2013
Yes Yes Yes Yes Yes NR NR Yes No No Yes No NR No Fair
Khan et al., 2014 Yes No Yes ND No NR NR Yes Yes No No No NR No Poor
Bilal et al., 2015 Yes No CD No No NR NR Yes No No No No NR No Poor
Hussain et al., 2015 Yes Yes Yes No No NR NR Yes Yes No Yes No NR No Fair
Khan et al., 2015 Yes Yes No No NR NR NR Yes Yes No No No NR No Poor
Qamar et al., 2016
No No No NR No NR NR NA No NA No No NR No Poor
Malik et al., 2016 Yes Yes Yes Yes Yes NR NR Yes Yes NR Yes No NR No Good
Ishtiaq et al., 2017 Yes Yes No No No NR NR Yes Yes Yes No No NR No Poor
Murad et al., 2017
No No No Yes No NR NR NA No NA No No NR No Poor

226
Appendix 4: Changes made in topic guides after pilot study
Appendix 4i: Changes made in topic guide for patients after pilot study
1: Initial demographic details of patients were limited to age, employment status and education. Change: More demographic details (gender, duration of HTN, smoker/non-smoker, obese/non-obese, alcoholic/non-alcoholic) of the patients were considered to sample a wider group of people.
2: Question 2 previously: Can you tell me what are hypertension (HTN) or high blood pressure symptoms? Change: deleted and replaced by (How is your experience about symptoms of high blood pressure?) this replacement better addressed the research question. Moreover, it was recognised that patients struggled to understand term ‘hypertension ‘as compared to high blood pressure. Therefore, the term was replaced with high blood pressure throughout for patients.
3: Question 3 previously: Do you think having HTN or high blood pressure has affected your life? Change: Reworded to (In any ways do you feel high blood pressure has affected your life?). The reason behind this change was to use an open-ended question to explore patients’ difficulties of living with a disease. Following prompts were then used:
• daily activities
• family obligations
• work commitments
4. Question 4 previously: What you do for your HTN or high blood pressure complications? Change Deleted and replaced with a clearer question (Have you had any complications from your high blood pressure?) Questions regarding high blood pressure treatment were moved into the second part of the topic guide which is related to patient understanding of HTN treatment.
5. Question 9 previously: Have you taken your tablets today? Change deleted and replaced with a more generic and less personal question (How long you have been taking tablets?) The reason for this was to keep questions open and to avoid using leading questions.
6. Question 10 and 11: (Do you take your tablets regularly or just occasionally?) (If occasionally, why it happens?) Change question 10 and 11 were merged together as question 10 (Do you take your tablets regularly or just occasionally? If occasionally, why it happens?) Various prompts were then used to get information about drug adherence and non-adherence such as cost, side-effects and availability of medicine at hospital.
7. Question 12: Do you think taking drugs regularly is necessary for controlling your blood pressure? Or taking only in periods of high blood pressure is important? Change deleted as this was the repetition of amendments to question 10 and 11.
8. Question 15 previously (Have you heard about self-management?) Change reworded (Have you heard anything about self-management or taken part in anything else?) The reason was to explore patient high blood pressure management strategies that they might adopt. Various prompts were used to explore their understanding such as blood pressure monitoring and use of home remedies.
9. Question 15 previously (Do you feel or experience any problems when you follow lifestyle changes?) Change deleted and replaced to (Have you experienced any problems/difficulties to adhere/follow these changes in life? If yes, what they are?). Various prompts were used such as: diet (the role of family members friends and peer, role of doctors’ advice) exercise (the role of family members and doctor, co-morbidities) salt intake (the role of family and friends, the role of doctor advice) smoking (the role of friends, family and doctor, any role of stress) alcohol intake (the role of friends, family and doctor advice)

227
10. Question 17 previously (Would you like to tell me how frequently you see your doctor and if he tells you about lifestyle changes?) Change deleted and replaced to (Do you feel doctor explains you about exercise, lower salt intake, and cessation of smoking, stress management and diet along the drug therapy? If no, what could be a reason?) This change was made as the question is a less personal and more generic and covers most issues. Following prompts were considered: the given advice, either specific or general and the depth of information
11. Question 20 and 21 previously were two separate questions (20. Do you think it is important to take care of your health and your blood pressure?) (21. If, not what do you think whose responsibility is this?) Change reworded and merged in one question (Do you feel it is important to take care of your health and your own blood pressure? If, not what do you think whose responsibility this should be?) In the pilot interviews, many patients answered question 20 with responses that linked to question 21. Hence it was essential to merge the questions together. Various prompts were then considered such as: family members, spouse (if married), own or doctor.
Appendix 4ii: Changes made in topic guide for doctors after pilot study
1: Question 3 previously (Can you tell me what the main issues of HTN are in Pakistani patient?) Change reworded and replaced to (What do you feel about the main reasons of HTN in Pakistani patients) that is more generic.
2: Question 4 previously (What do you think is the most important factor in controlling HTN in patient?) change reworded and reordered (11. In your opinion what is more important for hypertensive patients to control high blood pressure through drug treatment, lifestyle changes or both?) which is more explorative to elicit doctor views regarding two main components of HTN treatment: drug treatment and lifestyle changes.
3: Question 5 (Do you believe your patient know importance of HTN treatment?) change reworded and reordered (13. In your opinion do patients know the importance of HTN treatment?) which is not confusing, less personal and more generic.
4: Question 6 previously which is now number 5 (When you say HTN treatment for patient what you mean by this?) change reworded (5. What do you think about the types of treatment for hypertensive patients?). Pilot interviews showed that initial question was confusing and not clear to participants therefore it was essential to reword the question.
5: Question 8 previously (Can you tell me what lifestyle advice you provide to hypertensive patient?) change reworded (8. What lifestyle advice do you feel it to be essential to provide hypertensive patients?) it was recognised in the pilot interviews that the original question was leading, and the given response was not related to interviewees experience. Hence it was essential to refine and rephrase the original question and to explore participant awareness regarding a particular lifestyle change in relation to the need of hypertensive patients.
6: Question 11 and 12 previously (11. What do you think what they prefer more to follow and why?) (12. If they don’t follow what’s the reasons for this?) change reordered and reworded (16. In your experience, what do patients prefer more to follow and why?) which is more explorative, generic and linked to previous question.
7: Question 19 (Do you think that patients’ education level and social status play part in medical adherence?) change reworded into two clear and separate questions (19. Do you feel there are some issues arising in HTN control due to the low literacy levels of patients in Pakistan? If yes, can you describe these issues?) (20. In your opinion, does a patient’s social status play any part in their lifestyle?) It was noticed in the pilot interviews that the original question was not explorative to elicit doctors’ responses regarding patients’ literacy level and social status. Therefore, questions on the relationship between HTN treatment, patients’ literacy level and social status in were added separately to explore doctors’ responses.

228
Appendix 5i: Challenges associated with conducting the pilot study
The research culture in Pakistan, in general, been described as in its infancy (Pardhan, 2010,
p.33). Native scholars undertaking research in Pakistani hospitals have warned against the
lack of a research culture and can encounter unique challenges (Yasir, 2014). Moreover, the
Ethics Review Committee (ERC) in public hospitals is a relatively new phenomenon in Pakistan
and only a few private healthcare organisations have an ethics committee and staff members
who understand research ethics (Khan et al., 2012; Punjwani, 2015).
To date, the Aga Khan University Hospital in Karachi is the only private hospital with a formal
ethics committee that established in 2000 (Moazam & Jafarey, 2005). Previously, some native
scholars undertaking research in Pakistan have relied on ethics approval gained from their
universities where the study is being conducted (Mufti, 2011; Faiz, 2015). Hence, initially, this
study was intended to be conducted solely in accordance with the ethical principles of the
Research Ethics Policy of University of Hertfordshire. However, the pilot study identified that
it was essential to secure permission from the hospital medical superintendent in Pakistan in
order to gain access to potential research participants.
A brief telephone conversation with the Pakistan Dental and Medical Council25 resulted in
guidance on how a native researcher should approach the hospital management and
participants for a research study. PMDC recommends gaining approval from the review board
of the institution where the study is being conducted and informed written consent from the
study participants (PMDC, 2006). Therefore, before the commencement of the pilot study the
ethical approval to conduct the pilot study was gained from the University of Hertfordshire
Ethics Review Committee. Written permission to conduct the study was first obtained from
the medical superintendent of the hospital in Pakistan. After which each of the study
participant was approached and their informed written consent obtained. Identical ethical
procedures have been followed by many native and local researchers undertaking qualitative
and cross-sectional studies in Pakistani hospitals (Essani & Ali, 2011; Saleem et al., 2011;
Saleem et al., 2012; Yasir, 2014; Noorani et al., 2014; Saleem et al., 2015; Atif et al., 2016).
Gaining a signed letter of permission from the hospital medical superintendent in Pakistan
was challenging due to the lack of research culture and communication problems. However,
as a result of work experience in a Pakistani hospital, the researcher was aware of the
necessity of gaining accurate details of the medical superintendent in order to establish a
direct contact. Direct contact could mitigate unnecessary delays arising from common errors
such as failure of the administration staff to forward the documents, deleting emails by
mistake and lack of response. The pilot study underlined importance of using a personal
contact to gain the accurate details of the hospital medical superintendent.
Hence, one of the researcher’s personal contacts (brother) in Pakistan helped to obtain the
medical superintendents’ details. After a week, follow-up phone calls were made to confirm
the medical superintendent had received the application and required documents. However,
many times the researcher was unable to reach to the medical superintendent due to
25 The Pakistan Medical and Dental Council (PMDC) is the government regulating body that recognises all medical
universities and public hospitals in the country.

229
attendance at meetings and variations in working hours between the UK and Pakistan. On
some occasions the receptionist refused to direct the call to the medical superintendent.
During the follow up period, the researcher’s personal contact secured a face-to-face meeting
with the hospital medical superintendent and shared researcher previous professional
background as a Pakistani qualified medic. This meeting, along with the documents received
from the researcher, supported the medical superintendent decision to grant permission for
the pilot study to proceed.
Appendix 5ii: Lessons learned from the pilot study
The pilot study highlighted the significance of building up the relationship of trust with the
medical superintendent through effective communication to ensure recruitment was smooth
and effective. Therefore, prior to the fieldwork, a face-to-face meeting was scheduled with
the hospital medical superintendent to deliver a summary of the pilot study. The meeting
resulted in an informal discussion regarding the implications and future perspectives of
qualitative research in the country. It was agreed that the medical superintendent would
introduce the researcher to the head of the medicine department, duty doctors and medical
staff and make them aware of her presence in the hospital. Therefore, the researcher’s first
day at hospital involved a non-official meeting with the head of department, face-to-face
meeting with the medical staff (doctors and nurses) and a detailed visit to the hospital
building. This step assisted with breaking the ice and familiarity with the hospital setting,
environment and staff before commencing the study.
The pilot study identified that the process of patients’ recruitment was effective and many of
them showed interest in the study. A few patients approached the researcher directly after
reading the patient information leaflet or study poster at the hospital entrance, presented
their medical notes and asked the researcher if they were eligible to take part in the study. It
was recognised during the pilot study that whilst in the hospital, the researcher would wear
a badge with her name and the University of Hertfordshire logo on to make herself
approachable and recognised. The junior doctors expressed more interest to take part in the
study as compared to the senior doctors. The researcher had not previously been in contact
with the hospital but learned that the junior doctors’ co-operation was linked to their curiosity
about the research and that they considered the researcher to be a part of Pakistani doctors’
community. Additionally, the researcher spent time building a relationship of trust through
regular greetings, informal visits, active listening and showing an interest in the doctors’ daily
routine.
The audio recording was an issue for some patients who hesitated to share the information
even after they had been informed that audio recording would be used. In this situation, it
was necessary for researcher to build a bridge of trust between herself and the participants
and to clarify to them how highly privacy and confidentiality of data are valued in the
University of Hertfordshire regulations. Pre-interview conversations with patients also
focused on establishing empathic ties that put them at ease. The researcher reassured
participants’ about the confidentiality of their identity and that any information obtained
would only be used for the research purpose.

230
During the pilot study, the researcher learned that keeping a research diary in the field was
essential for writing notes, thoughts and her own assumptions to aid reflexivity in the
research process. For instance, after each interview reflections on the interview experience
were noted with comments on how well the researcher felt the interview went, what were
the practical issues, how the participant felt during the interview and any methodological
issues (e.g. by noticing the non-verbal aspects of the interviewee’s behaviour). Additionally,
the diary acted as a useful organizational aid to keep track of the research progress.
Therefore, for the main study, the researcher carried an A4 lined notebook as a research diary
to adopt a reflexive practice into the research process.
After the pilot study, the researcher transcribed the interviews audio recordings in Microsoft
Word and discussed them with the supervisors. This feedback obtained from the supervisors
along with the professional training and workshops attended at the University of
Hertfordshire helped improve interviewing skills. For instance, the researcher improved areas
in terms of identifying own bias, listening, probing and follow-up, where and when to pause,
using the funnelling technique26 and the emotional dynamics of qualitative interviews.
Overall, the pilot study gave valuable lessons in relation to various aspects of the study as
described above. However, the findings of the pilot interviews were not embedded in the
analysis for the main study as this was not the aim of the pilot study.
26 Funnelling technique involves starting from general questions before getting into the specifics and asking more detail at
each level (Wengraf, 2001; Galletta, 2013).

231
Appendix 6: (Interview topic guides in English)
Appendix 6i: Interview topic guide for patients
Interview topic guide for patient
An Exploration of the Perspectives of Hypertensive Patients and Doctors about
Hypertension and its Treatment in Pakistan
To be translated in Urdu
Age …………… Gender………………….
Education ………………. Employment status …………….
Duration of Hypertension………………….
Smoker………Non-Smoker………… Obese: Yes/No
Alcoholic: Yes/No
Date………………………. Time……………………………
Patient understanding of high blood pressure (HTN)
Ice breaking questions (Turn on tape recorder)
For how long have you been diagnosed with high blood pressure?
How did you find out that you have high blood pressure?
1. What do you understand by high blood pressure?
2. How is your experience about symptoms of high blood pressure?
3. In any ways do you feel high blood pressure has affected your life?
4. Have you had any complications from your high blood pressure?
5. Have you heard about anything you can do to reduce your blood pressure?
6. How would you like to monitor your blood pressure?
7. Personally, what do you feel is the most important thing you can do to control
high blood pressure?

232
Patient understanding of high blood pressure (HTN) treatment
8. I would like you to tell me what you use to control your high blood pressure?
Antihypertensive medication/lifestyle change/both?
9. How long you have been taking tablets?
10. Do you take your tablets regularly or just occasionally? If occasionally, why that
happens?
11. Have you experienced some side effects from your tablets? If yes, how do you
feel when you are taking them?
12. Have you heard anything about self-management or taken part in anything else?
13. I would like you to tell me the names of some lifestyle changes?
14. Are there any changes in your lifestyle in terms of exercise, weight reduction,
smoking cessation, dietary changes, low salt and alcohol intake after being
diagnosed as a patient with high blood pressure?
15. Have you experienced any problems/difficulties in adhering to or following these
changes in lifestyle? If yes, what they are?
16. Do you find that lifestyle changes are part of your disease treatment? Or is this
additional advice from the doctor?
17. What is your experience of your doctor’s role in providing lifestyle advice?
18. Do you feel that your doctor explains to you about exercise, lower salt intake and
cessation of smoking, stress management and dietary changes along with drug
therapy? If no, what could be a reason?
19. Do you feel lifestyle changes help to control high blood pressure? If yes, then
how and what motivate you?
20. Do you feel it is important to take care of your health and your own blood
pressure? If not, whose responsibility do you think this should be?
Is anything else you would like to add about your health condition or treatment?
Is there anything you would like to ask me?
Thank you for taking part in this interview.

233
Appendix 6ii: Interview topic guide for doctors
Interview topic guide for doctor
An Exploration of the Perspectives of Hypertensive Patients and Doctors about
Hypertension and its Treatment in Pakistan
Date………………Time………………………….
Ice breaking questions (Turn on tape recorder)
Before we start the interview, it would be very useful to find out a little bit about you:
• Would you like to tell me how long you have been working in this hospital?
• For how long have you been qualified as a doctor?
1. How many hypertensive patients do you usually see in a day?
2. I would like you to tell me what you hope to achieve before seeing a
hypertensive patient?
3. What do you feel about the main reasons of HTN in Pakistani patients?
4. When you say treatment for hypertensive patient what do you mean by this?
5. What do you think about the types of treatment for hypertensive patients?
6. How patients are usually diagnosed? Are there any guidelines?
7. In your experience, how do you usually decide whether or not to put the
patient on antihypertensive drugs?
8. What lifestyle advice do you feel it to be essential to provide hypertensive
patients?
9. How do you usually provide this advice? Oral or written?
10. Do you feel it is important to provide lifestyle recommendations along with
drug therapy to all diagnosed hypertensive patients or only some specific
patients? If yes to all then why? If no, then which patients require these
recommendations more?
11. In your opinion what is more important for hypertensive patients: to control
high blood pressure through drug treatment, lifestyle changes or both?
12. Do you think it is your duty to provide lifestyle advice to patients? Or should
someone else be responsible for this?

234
13. In your opinion do patients know the importance of HTN treatment?
14. How do you feel about the compliance of hypertensive patients to the
treatment you provide?
15. Do you feel patients understand the role of drugs and lifestyle advice separately
in the treatment of HTN? If no, then why?
16. In your experience, what do patients prefer more to follow and why?
17. If they don’t seem to follow lifestyle changes what the reason is for or barriers
to this from your point of view?
18. How do you deal with common queries from patients about lifestyle changes
and what is your experience of this?
19. Do you feel there are some issues arising in HTN control due to the low literacy
levels of patients in Pakistan? If yes, can you describe these issues?
20. In your opinion, does a patient’s social status play any part in their lifestyle?
21. Do you feel there are some barriers that affect patient adherence to HTN
treatment? For instance, stress, money and family burden.
22. What you would suggest to improve the understanding of HTN treatment for
patients in Pakistan?
23. Do you feel there is a need for health promotion activities for hypertensive
patients in Pakistan?
Is there anything you would like to ask me?
Thank you. Clarify arrangements for further contact if needed.

235
Appendix 7: (Interview topic guides in Urdu)
Appendix 7i: Interview topic guide for patients (In Urdu)

236

237
Appendix 7ii: Interview topic guide for doctors (In Urdu)

238

239
Appendix 8: (Study Poster)
Appendix 8i: (Study poster in English)

240
Appendix 8ii: (Study poster in Urdu)
241
Appendix 9i: Patient information sheet
i. Patient information sheet (English)
UH Ethics Protocol No: cHSK/PGR/UH/02406
An exploration of
the views of
patients and
its
treatment in
Pakistan
Contact Information
kindly
contact
Thank you very much for
Patient information leaflet 1
I am inviting you to take part in a study which will explore the views of patients and doctors about high blood pressure and its treatment in Pakistan. Before you decide, it is important for you to understand why the study is being done and what it will involve. Please take time to read the following information.
Purpose of Study
High blood pressure remains a common and an important risk factor for diseases including coronary heart disease, heart failure and kidney failure. Treatment guidelines are available for patients and doctors to control the disease. The study aims to explore patient and doctor views about high blood pressure and its treatment in Pakistan.
Who can take part in this study?
You can take part in this study if you are a patient with high blood pressure and are taking medicine for it.
What are the benefits of taking part?
This research will help to provide a detailed understanding of the views of patients and doctors about high blood pressure and its treatment, particularly in relation to lifestyle recommendations in Pakistan.
Do I have to take part?
No, it is entirely up to you whether or not you take part. You are free to withdraw at any time without giving any reason. Any data collected from you will be destroyed. The decision to withdraw from
the study will not affect your
medical care.
What will happen if I take part?
A face to face interview will be conducted with you which will last approximately 30 minutes. You will be asked whether you will allow the researcher to record this interview or not. It is entirely up to you whether you decide to take part or not. Will my taking part in this study be kept confidential?
All information regarding you will be
kept confidential. All collected data will
be stored on a password protected
computer. No personal data regarding
you will be recorded without consent.
Any personal data collected from you
will be destroyed at the end of the
study. Only the members of the
research team will be able to access the
data. At the end of the study all data will
be stored by the researcher in a locked
filing cabinet for five years before it is
destroyed.
Patient information sheet 2
What are the possible risks of taking part in the study? The researcher will ask questions regarding high blood pressure and its treatment which some might find uncomfortable. You do not have to answer every question. At any point, if you feel uncomfortable you can withdraw from the study without giving any reason. If you do not take part your medical care will not be affected in any way. Who has organised this study and who can I contact?
The study is being undertaken within the School of Health and Social Work, University of Hertfordshire, UK, for the award of a PhD degree. If you have concerns and complaints about any aspect of the way you have been treated during the course of this study, please contact my supervisor Professor Wendy Wills for more details about the organisation of this study. Alternatively, you can write to the University’s Secretary and Registrar, Sue Grant, at the University of Hertfordshire, College Lane campus, Hatfield AL10 9AB, UK. Who has reviewed this study?
Research projects are reviewed by the University of Hertfordshire, Health and Human Sciences Ethics Committee with Delegated Authority (ECDA) and their role is to protect the interests of everyone who takes part in this study.
242
Appendix 9ii: Patient consent form (English)
UH Ethics Protocol No: cHSK/PGR/UH/02406
An exploration of the views of patients and doctors about high blood pressure and its treatment in Pakistan
Patient Consent Form
(To be translated in Urdu)
Name of Researcher: Qurrat ul Ain Signature
1. I confirm that I have been given a patient information leaflet and I have been given
details of my involvement in the study.
2. I have allowed the researcher to access my prescription/medical notes.
3. I have been given the opportunity to ask questions.
4. I understand that I do not have to answer all the questions asked of me.
5. I agree that the interview will be audio recorded.
6. I have been informed that I might be asked sensitive questions in the interview,
however, it is entirely up to me whether I give answers or not.
7. I have been told that information related to me will be kept confidential and all data
regarding me will be stored in a password protected computer and will not be
accessed by anyone other than the research team.
8. I have been told that I may at some point in the future be contacted again in
connection with this study for follow up.
9. I have been informed that if I withdraw from the study it will not affect my medical
care in anyway.
10. I agree to take part in the above study.
One copy of this form to be signed/kept by the researcher and one copy by the participant.
Name of Participant ……………… Date ………… Signature…………………

243
Researcher……………………… Date ………….. Signature……………………

244
Appendix 10
Appendix 10i: Patient information sheet (Urdu)

245

246
Appendix 10ii: Patient consent form (Urdu)
247
Appendix 11
i. Doctor information sheet (English)

248
Appendix 11ii: Doctor consent form (English)
UH Ethics Protocol No: cHSK/PGR/UH/02406
UH Ethics Protocol No: cHSK/PGR/UH/02406
An exploration of the views of patients and doctors about high blood pressure and its treatment in Pakistan
Doctor Consent Form
Name of Researcher: Qurrat ul Ain Signature
1. I confirm that I have been given a doctor information leaflet and I have been given
details of my involvement in the study.
2. I understand that my participation is voluntary and I am free to withdraw at any time
without giving any reason. If I withdraw from the study any data collected from me
will be destroyed.
3. I have been given the opportunity to ask questions.
4. I agree that the interview will be audio recorded.
5. I understand that I do not have to answer all the questions asked of me.
6. I have been told that information related to me will be kept confidential and all data
regarding me will be stored in a password protected computer and will not be
accessed by anyone other than the research team.
7. I have been told that I may at some point in the future be contacted again in
connection with this study for focus group discussion.
8. I agree to take part in the above study.
One copy of this form to be signed/kept by the researcher and one copy by the participant.
Name of Participant ……………… Date ………… Signature………………………
Researcher……………………… Date ………….. Signature……………………..

249
Appendix 12: UH ethics approval

250

251
Appendix 13: Permission letters from Pakistan
i. Letter from the first hospital

252
ii. Letter from the second hospital

253
Appendix 14: The ethics protocol for medically-qualified research student
I, as a health clinician, will intervene in patient care only, when
1. A patient is experiencing a life-threatening event such as cardiac arrest
and no qualified staffs are present.
2. A patient is at risk of physical harm and no qualified staffs are present.
3. A patient safety risk is identified such as medical malpractice or
inappropriate treatment by a staff member or medical student and no
qualified staff are present.
The following actions will be undertaken for step 1:
Collapsed/Sick Patient
Shout for help and access the patient
Signs of life (consciousness, breathing, pulse rate, temperature and colour)
No Yes
Cardiopulmonary resuscitation (CPR) Call Resuscitation Team
(30 chest compressions and 2 rescue breaths)
(At least 5 times in 2 seconds)
Continue until help arrives
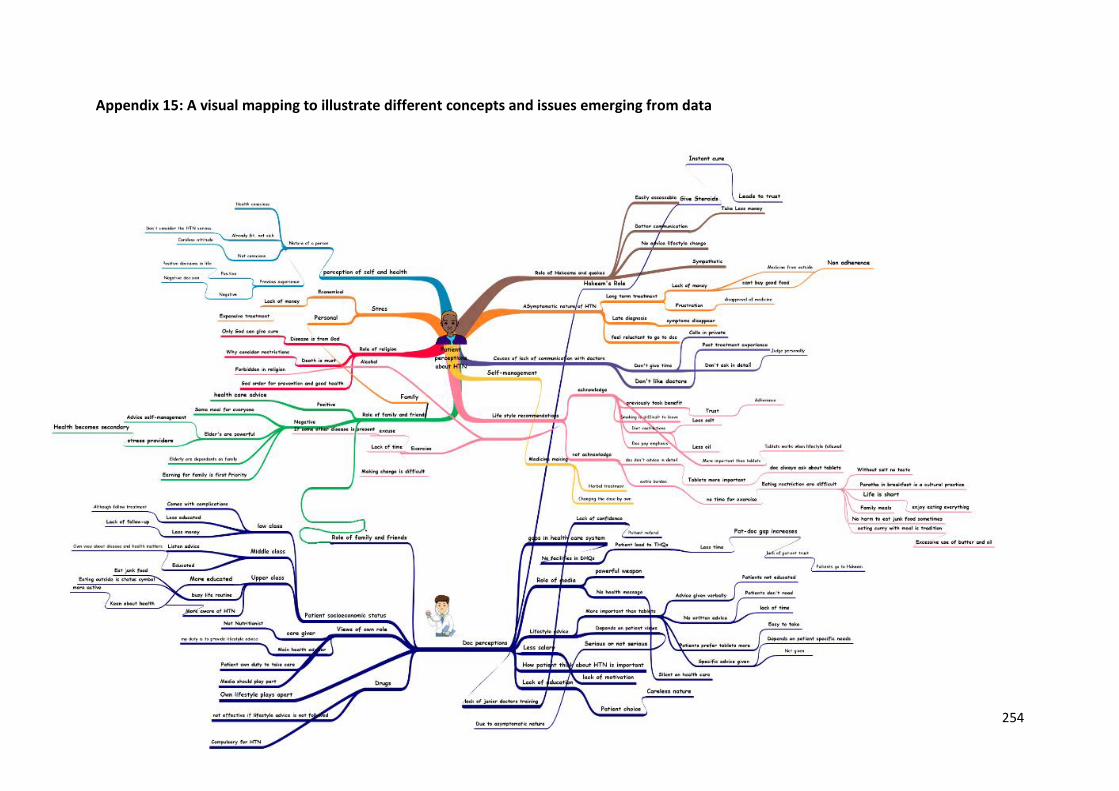
254
Appendix 15: A visual mapping to illustrate different concepts and issues emerging from data
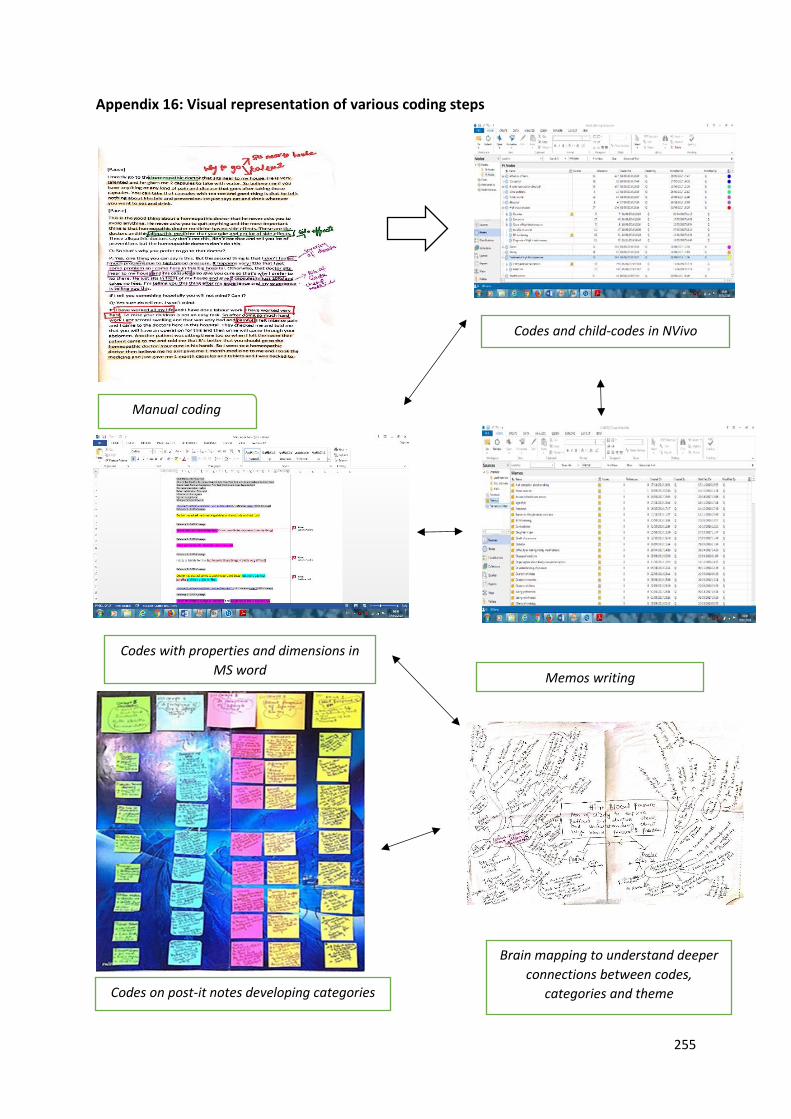
255
Appendix 16: Visual representation of various coding steps
Manual coding
Codes and child-codes in NVivo
Memos writing
Codes with properties and dimensions in
MS word
Codes on post-it notes developing categories
Brain mapping to understand deeper
connections between codes,
categories and theme

256
Appendix 17: Data coding frame
Appendix 17i: Patients’ coding frame
Main Theme Categories Codes and child-codes
➢ Perceptions of HTN
Diagnosis Definitions and meanings of HTN symptoms
I. Causes Stress
Family disease
Parent code: High blood pressure Child-codes: HTN diagnosis, physical symptoms, causes, family disease, meanings of HTN, stress
➢ Experiences and attitude concerning taking
antihypertensive drugs
I. Positive experiences
II. Negative experiences
III. Lack of information about drugs in consultations
Parent-code: HTN treatment Child-codes Anti-hypertensive drugs Child-codes reasons of drug adherence, reasons of drug non-adherence, less Information provision during consultation
➢ Perceptions about lifestyle management (exercise, diet, salt intake, smoking, alcohol
intake)
I. Understanding concerning exercise
II. Socio-cultural norms III. Lack of time IV. Individual factors
and concurrent health conditions
V. Lack of exercise information from doctors
Parent- code: Exercise or physical activity Child-codes: cultural practices, work commitment, time, weather, laziness, motivation, gender issues, another disease, less information on exercise
i. traditional foods
ii. Cultural eating practices and peer pressure
iii. Healthy food and personal preferences
iv. Access to fast food v. Lack of dietary
information
Parent-code: Food/diet Child-codes: Oily and spicy food, parathas, junk food, fruits and vegetables, self-control, social gatherings, eating together, family and friends, eating out, less information about diet

257
I. Flavour and customary practice
II. Information about salt intake
Parent-code: Salt intake Child-codes: salt and high blood pressure, quantity, salty tea, salty paratha, salt in flour, taste factor, seasoning, family and friends, information on salt consumption
i. Socio-environmental
influence
ii. personal factors
Parent-code: Smoking Child-codes: Smoking and high blood pressure, duration of smoking, family and friends, smoking with others, withdrawal effects, dependency, less motivation, Information on smoking cessation
i. Religious beliefs
Parent-code: Alcohol intake Child-codes: Role of Islam
➢ Involvement in alternative strategies
I. Consulting quack
and Hakeem II. Alternate medicine
use /home remedies
III. Faith healing
Parent- code: Alternative treatment strategies Child-codes: Quack and Hakeem, Hakeem medicine, Quack and Hakeem services, home and herbal remedies, traditional remedies, role of Allah, prayer, destiny.

258
Appendix 17ii: Doctors’ coding frame
Main Theme Categories Codes and child-codes
➢ Perceptions about HTN
Understanding about HTN
I. Awareness about HTN guidelines
II. Practicing HTN guidelines
Parent-code: HTN Child-codes: A chronic and silent disease, symptoms, diagnosis, causes, risk factors, HTN diagnostic criteria Parent-code: HTN guidelines Child-codes: Understanding related to HTN guidelines, issues in practicing HTN guidelines
➢ Treating patients with HTN
Patient-related factors
Parent-code: Treating hypertensive patients Child-codes: patient lack of awareness, patient responsibility, lack of interest, use of alternate treatments among patients
➢ Perceptions regarding lifestyle management (exercise, diet, salt intake, smoking, alcohol intake)
i. Understanding
concerning involvement in exercise
ii. Socio-cultural norms iii. concurrent health
conditions
Parent-code: Exercise Child-codes: exercise and HTN, patient lack of interest, information provision, social and cultural norms, gender issues, presence of another disease in patients
I. Role of traditional food
II. A lack of self-control III. Accessibility to junk
food
Parent-code: Diet Child-codes: dietary changes and HTN, traditional foods and society, Paratha, ghee intake, less motivation and control among patients, patient misconceptions, role of fast street food, easy access and busy life routine
I. Cultural practice
II. Taste preference
Parent-code: salt intake Child-codes: cultural practice, salt flavour, patient preference, knowledge about salt intake
I. Individual barriers Parent-code: Smoking Child-codes: Smoking and HTN, lack of patient motivation, nicotine dependency, role of family and friends, time constraints and less information provision

259
I. Religious commitment
Parent-code: Alcohol consumption Child-codes: Islamic laws, strong religious commitment and drinking, weak religious commitment and drinking, time constraints and less information
➢ Informing patients about HTN
I. Information provision
Parent-code: Informing patients about HTN Child-codes: Doctor’s role, lack of time and work pressure, patient responsibility
➢ Communication issues in
clinical interactions
I. Doctor-patient interactions
Parent code: Communication issues Child-codes: work pressure and stress, patient illiteracy, difficulty to explain medical concepts
Copyright © 2022 FDOKUMEN