Patellar Taping in the Treatment of Patellofemoral Pain: A Prospective Randomized Study
9
8/21/13 MD Consult - Print Previewer www.mdconsult.com/website/view/preview?printing=true&URL=http%3A//www.mdconsult.com/das/article/body/421319447-2/jorg%3Djournal%26source%3D%2… 1/9 Use of this content is subject to the Terms and Conditions Patellar Taping in the Treatment of Patellofemoral Pain A Prospective Randomized Study American Journal of Sports Medicine - Volume 24, Issue 1 (January 1996) - Copyright © 1996 American Orthopaedic Society for Sports Medicine 61 Patellar Taping in the Treatment of Patellofemoral Pain A Prospective Randomized Study * Mark G. Kowall , MD Gina Kolk , PT Gordon W. Nuber , MD Jeffrey E. Cassisi , PhD Steven H. Stern , MD Department of Orthopedic Surgery, Northwestern University Medical School Northwestern Memorial-Baxter Physical Therapy Center Illinois Institute of Psychology, Chicago, Illinois No author or related institution has received any financial benefit from research in this study. The purpose of this prospective study was to evaluate the efficacy of a patellar taping program in the conservative management of patellofemoral pain. Twenty-five patients with patellofemoral pain were randomized into two groups. One group underwent a standard physical therapy program for patellofemoral pain. The other group underwent the same physical therapy program, but use of a patellar taping technique was added to this program. Results of a subjective visual analog scale and changes in isokinetic strength and electromyographic activity of the quadriceps muscle were analyzed. Both the tape and no-tape groups experienced a statistically significant decrease in symptoms ( P < 0.05), but no difference in improvement of patellofemoral pain was noted between the groups. Likewise, both groups demonstrated significant improvement in quadriceps muscle isokinetic strength ( P < 0.05) and activity ( P < 0.001), but no difference in improvement was noted between groups. The results of this study suggest no beneficial effect of adding a patellar taping program to a standard physical therapy program in the conservative treatment of patellofemoral pain. Larger prospective studies are warranted to support this opinion. Patellofemoral pain is a common symptom in both the athletic and nonathletic population. Causes of patellofemoral pain include trauma (acute and repetitive), osteochondritis dissecans, synovial plicae, chondromalacia, and patellofemoral malalignment. The initial treatment of patellofemoral pain traditionally includes quadriceps muscle rehabilitation, which consists of straight leg raises, quadriceps muscle isometrics, and short-arc terminal extension exercises. [2] Braces have been advocated by several authors to improve patellar tracking and to decrease the pain associated with exercise. [18] [20] [31] Patellar taping, as described by McConnell, [23] [24] is a new technique to facilitate quadriceps muscle rehabilitation in the treatment of patellofemoral pain. The basic concept of taping is passive correction of patellar subluxation, tilt, and rotation to decrease pain during quadriceps muscle rehabilitation. By enabling a pain-free range of motion, isotonic and isokinetic exercises
Transcript of Patellar Taping in the Treatment of Patellofemoral Pain: A Prospective Randomized Study

8/21/13 MD Consult - Print Previewer
www.mdconsult.com/website/view/preview?printing=true&URL=http%3A//www.mdconsult.com/das/article/body/421319447-2/jorg%3Djournal%26source%3D%2… 1/9
Use of this content is subject to the Terms and Conditions
Patellar Taping in the Treatment of Patellofemoral Pain A Prospective Randomized Study
American Journal of Sports Medicine - Volume 24, Issue 1 (January 1996) - Copyright © 1996 American
Orthopaedic Society for Sports Medicine
61
Patellar Taping in the Treatment of Patellofemoral Pain A Prospective Randomized Study *
Mark G. Kowall , MD
Gina Kolk , PTGordon W. Nuber , MDJeffrey E. Cassisi , PhDSteven H. Stern , MD
Department of Orthopedic Surgery, Northwestern University Medical School Northwestern Memorial-Baxter Physical TherapyCenter Illinois Institute of Psychology, Chicago, Illinois
No author or related institution has received any financial benefit from research in this study.
The purpose of this prospective study was to evaluate the efficacy of a patellar taping program in the conservative managementof patellofemoral pain. Twenty-five patients with patellofemoral pain were randomized into two groups. One group underwent astandard physical therapy program for patellofemoral pain. The other group underwent the same physical therapy program,but use of a patellar taping technique was added to this program. Results of a subjective visual analog scale and changes inisokinetic strength and electromyographic activity of the quadriceps muscle were analyzed. Both the tape and no-tape groupsexperienced a statistically significant decrease in symptoms ( P < 0.05), but no difference in improvement of patellofemoralpain was noted between the groups. Likewise, both groups demonstrated significant improvement in quadriceps muscleisokinetic strength ( P < 0.05) and activity ( P < 0.001), but no difference in improvement was noted between groups. Theresults of this study suggest no beneficial effect of adding a patellar taping program to a standard physical therapy program inthe conservative treatment of patellofemoral pain. Larger prospective studies are warranted to support this opinion.
Patellofemoral pain is a common symptom in both the athletic and nonathletic population. Causes of patellofemoral pain includetrauma (acute and repetitive), osteochondritis dissecans, synovial plicae, chondromalacia, and patellofemoral malalignment.
The initial treatment of patellofemoral pain traditionally includes quadriceps muscle rehabilitation, which consists of straight legraises, quadriceps muscle isometrics, and short-arc terminal extension exercises. [2] Braces have been advocated by several
authors to improve patellar tracking and to decrease the pain associated with exercise. [18] [20] [31]
Patellar taping, as described by McConnell, [23] [24] is a new technique to facilitate quadriceps muscle rehabilitation in the
treatment of patellofemoral pain. The basic concept of taping is passive correction of patellar subluxation, tilt, and rotation todecrease pain during quadriceps muscle rehabilitation. By enabling a pain-free range of motion, isotonic and isokinetic exercises
8/21/13 MD Consult - Print Previewer
www.mdconsult.com/website/view/preview?printing=true&URL=http%3A//www.mdconsult.com/das/article/body/421319447-2/jorg%3Djournal%26source%3D%2… 2/9
may be employed for more effective quadriceps muscle strengthening in a functional arc of motion.
The initial results of a rehabilitation program using patellar taping have been excellent, with a success rate of 92%. [24] However,
this initial McConnell study does not contain a control group and lacks objective evidence to support the use of taping.
A prospective randomized study was designed to evaluate the results of a physical therapy program that used patellar taping ina group of patients with patellofemoral pain. These results were compared with results from a similar group of patients whounderwent a physical therapy program without patellar taping. The results were analyzed for both subjective pain relief andchanges in quadriceps muscle strength and activity. To our knowledge, our study is the first controlled study evaluating thisnew treatment of patellofemoral pain.
*Presented at the interim meeting of the AOSSM, San Francisco, California, February 1993.
Address correspondence and reprint requests to Mark G. Kowall, MD, Orthopedic Specialty Associates, 8390 Morro Road, Atascadero, CA
93422.
62
MATERIALS AND METHODS
Subjects
Approval from the Institutional Review Board was obtained before commencement of the study. Twenty-five patients werestudied (17 women and 8 men). The mean age was 29 years (range, 14 to 40 years). Fifteen patients had unilateral complaints, and10 patients had bilateral complaints. The duration of symptoms was 2.5 years (range, 1 month to 15 years). Patients wereincluded in this study if they met the following eligibility requirements: 1) unilateral or bilateral patellofemoral pain for more than1 month, 2) no history or clinical evidence of patellofemoral dislocation, synovial plicae, or meniscal or ligamentous injury, 3) nohistory of prior knee trauma or knee surgery, 4) patient age between 14 and 40 years, 5) ability to complete a 4-week formalphysical therapy program, and 6) ability to comply with a 4-week home exercise program.
Patients meeting the eligibility requirements were randomized into a patellar taping group (12 patients) and a no patellar tapinggroup (13 patients). Randomization was accomplished with a prerandomization technique in which patients were assigned to atreatment group before consenting to the assigned treatment. [5]
At the time of initial physical examination, specific attention was paid to patellar alignment, specifically tilt and subluxation. Theassessment of patellar tilt and subluxation was performed using the method described by Kolowich et al. [15]
Patients in the tape and no-tape groups began a similar physical therapy and home exercise program. The only difference inprotocol was the application of tape to the patients in tape group. On initial evaluation, patients in the tape group wereinstructed by the physical therapist to properly tape their knees for home exercises. Appropriate taping was ensured initially andverified during each follow-up visit for physical therapy. The sex and age of the patients and duration of symptoms wereessentially the same for Groups I and II.
Radiographs
Patients had standard AP and lateral radiographs of the affected knees. Additionally, each patient had two tangentialradiographs performed to assess the patellofemoral relationship. The Merchant view, performed in the described manner, [25]
was used to measure the sulcus angle and the congruence angle. Abnormalities of these measurements are consistent withpatellofemoral subluxation. [10] [25]
The second tangential radiograph, the Laurin view, was performed in the described manner [16] and was used to measure the
lateral patellofemoral angle and the patellofemoral index. Abnormalities of these measurements have been found to be consistentwith patellofemoral tilt. [10] [16]
Patients in the tape and no-tape groups were further classified according to the presence or absence of clinical and radiographicpatellofemoral tilt or subluxation or both.

8/21/13 MD Consult - Print Previewer
www.mdconsult.com/website/view/preview?printing=true&URL=http%3A//www.mdconsult.com/das/article/body/421319447-2/jorg%3Djournal%26source%3D%2… 3/9
Subjective Rating Scale
A visual analog scale was used to assess subjective pain. [9] The questions in the visual analog scale asked patients to
characterize their knee pain and relate it to various activities. Answers were based on a 10-point scale. The same visual analogscale was completed at the end of the study period. Final data analysis focused on four areas of the visual analog scale: painfrequency, severity of pain, effect of pain on athletic activities, and the effect of pain on adult daily living activities.
Physical Therapy Protocol
Each group underwent a 4-week, twice weekly course of formal physical therapy. The patients were treated by a physicaltherapist formally trained in the treatment of patellofemoral disorders and in the McConnell [23] [24] patellar taping technique.
Therapy consisted of an extensive stretching and quadriceps muscle-strengthening program. Quadriceps muscle strengtheninginvolved progressive isometric, isotonic, and isokinetic exercises.
Each group was instructed in a standard home exercise program. Patients were encouraged to perform the exercises on a dailybasis for approximately 30 minutes. The patients in the tape group taped their knees appropriately before exercise.
Compliance with the home exercise program was monitored with surface EMG electrodes and the Bio-Prompt portable EMGcomputer (Physical Health Devices, Inc., Fort Lauderdale, Florida). This device, which monitors home exercise compliance, isconsidered reliable. [4]
Isokinetic Muscle Testing
The Cybex II isokinetic dynamometer (Lumex, Inc., Ronkonkoma, New York) was used to assess peak torque (strength) in thepatients at the start and at the completion of the therapy program. A standard method [26] was used to test concentric strength
recorded over the whole range of motion at angular velocities of 60 deg/sec and 180 deg/sec. Test sessions consisted of fiveattempts with the peak torque recorded. In patients with unilateral knee complaints, the opposite knee was also tested forpurposes of comparison.
Quadriceps Muscle Activity
The activity of the vastus medialis and vastus lateralis muscles was assessed during closed kinetic exercise using surface EMGelectrodes. Silver-silver chloride surface electrodes were placed over the vastus lateralis muscle and the most prominent part ofthe vastus medialis obliquus muscle. Electrodes were held in place with a soft spandex belt and a VELCRO (VELCRO USA, Inc.,Manchester, New Hampshire) buckle. The location of the
63
strap was placed at a set distance above the patella. This location was recorded for repeat testing at the completion of the study.The repeatability of surface EMG electrodes as compared with intramuscular wire electrodes has been proven. [14]
Integrated EMG activity readings were digitized on-line with Bio-Prompt portable EMG computer software (Physical HealthDevices, Inc.). This apparatus permits the incorporation of automated gain adjustment throughout a dynamic range of 7 to 1800muV. The bandwidth was 100 to 540 Hz with a 60-Hz notch filter. The automated gain adjustment reportedly facilitates integratedEMG monitoring during closed kinetic exercise. Average integrated EMG activity readings were obtained for the vastus medialisand vastus lateralis muscles during a closed kinetic exercise, which consisted of step-up and step-down stair activity. IntegratedEMG activity readings were recorded during a 3-second period during which a patient would step up onto a 10-inch step. Thetest session consisted of five repetitions. The test was repeated if the patient completed the test either too quickly or too slowly.A similar procedure was performed for the step-down task.
Data Analysis
All data were analyzed with SPSS software (SPSS, Inc., Chicago, Illinois). Testing of the hypothesis was conducted withmultivariate analysis of variance. Simple contrast and post hoc analysis were performed with paired t-test and one-way analysesof variance.
8/21/13 MD Consult - Print Previewer
www.mdconsult.com/website/view/preview?printing=true&URL=http%3A//www.mdconsult.com/das/article/body/421319447-2/jorg%3Djournal%26source%3D%2… 4/9
RESULTS
Patient Data
Twenty-five patients (15 with unilateral knee complaints and 10 with bilateral knee complaints) accounted for 35 symptomaticknees and 15 asymptomatic knees. An equal number of patients in both groups had clinical and radiographic evidence of patellarmalalignment. Compliance with home exercise as calibrated by Bio-Prompt EMG computer software was statistically similar foreach group.
Subjective Data
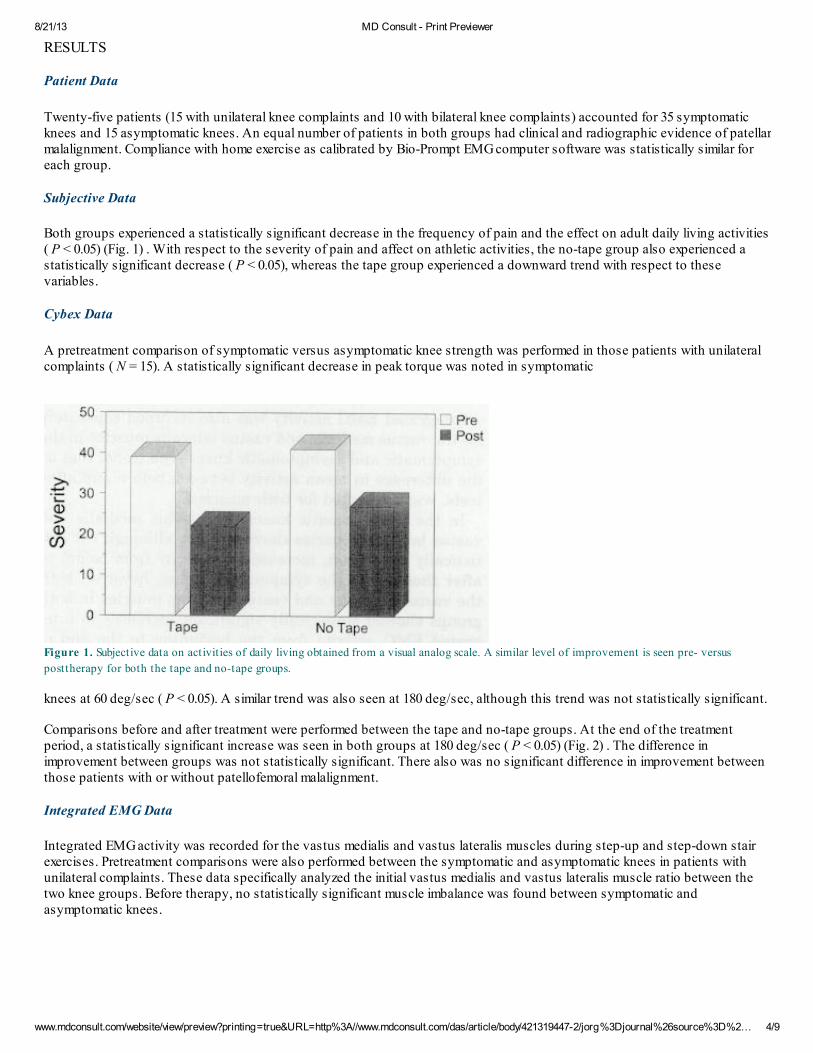
Both groups experienced a statistically significant decrease in the frequency of pain and the effect on adult daily living activities( P < 0.05) (Fig. 1) . With respect to the severity of pain and affect on athletic activities, the no-tape group also experienced astatistically significant decrease ( P < 0.05), whereas the tape group experienced a downward trend with respect to thesevariables.
Cybex Data
A pretreatment comparison of symptomatic versus asymptomatic knee strength was performed in those patients with unilateralcomplaints ( N = 15). A statistically significant decrease in peak torque was noted in symptomatic
Figure 1. Subjective data on activities of daily living obtained from a visual analog scale. A similar level of improvement is seen pre- versus
posttherapy for both the tape and no-tape groups.
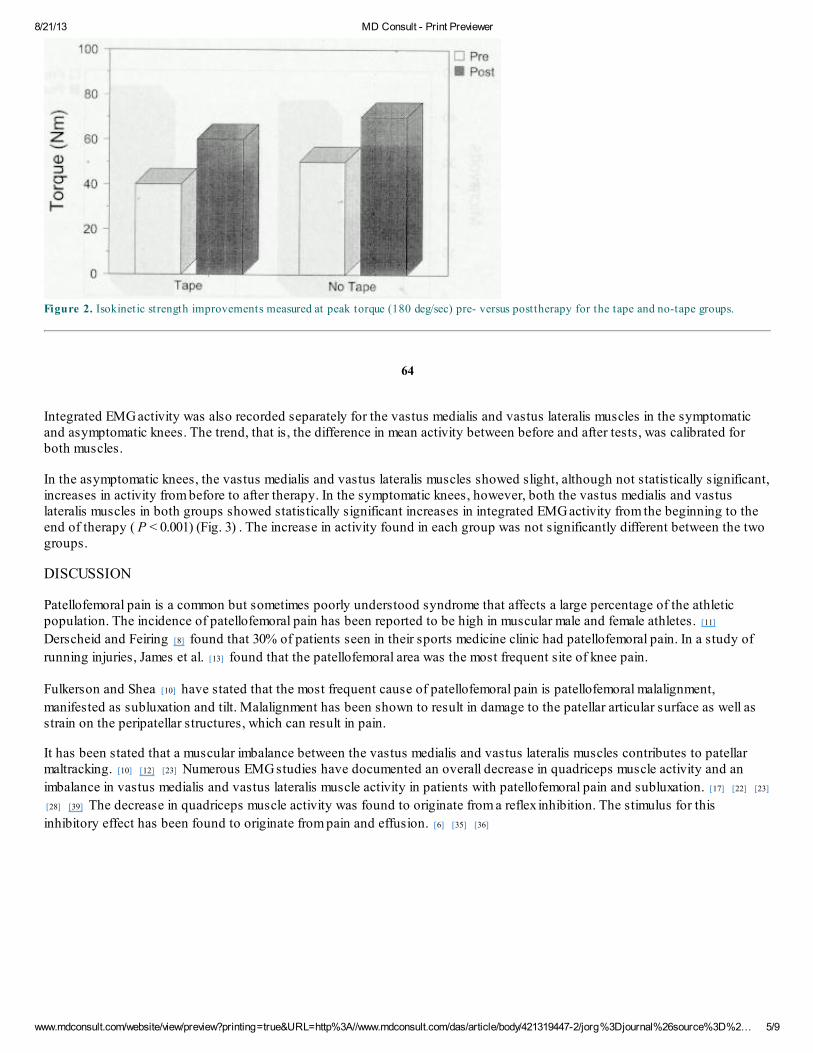
knees at 60 deg/sec ( P < 0.05). A similar trend was also seen at 180 deg/sec, although this trend was not statistically significant.
Comparisons before and after treatment were performed between the tape and no-tape groups. At the end of the treatmentperiod, a statistically significant increase was seen in both groups at 180 deg/sec ( P < 0.05) (Fig. 2) . The difference inimprovement between groups was not statistically significant. There also was no significant difference in improvement betweenthose patients with or without patellofemoral malalignment.
Integrated EMG Data
Integrated EMG activity was recorded for the vastus medialis and vastus lateralis muscles during step-up and step-down stairexercises. Pretreatment comparisons were also performed between the symptomatic and asymptomatic knees in patients withunilateral complaints. These data specifically analyzed the initial vastus medialis and vastus lateralis muscle ratio between thetwo knee groups. Before therapy, no statistically significant muscle imbalance was found between symptomatic andasymptomatic knees.
8/21/13 MD Consult - Print Previewer
www.mdconsult.com/website/view/preview?printing=true&URL=http%3A//www.mdconsult.com/das/article/body/421319447-2/jorg%3Djournal%26source%3D%2… 5/9
Figure 2. Isokinetic strength improvements measured at peak torque (180 deg/sec) pre- versus posttherapy for the tape and no-tape groups.
64
Integrated EMG activity was also recorded separately for the vastus medialis and vastus lateralis muscles in the symptomaticand asymptomatic knees. The trend, that is, the difference in mean activity between before and after tests, was calibrated forboth muscles.
In the asymptomatic knees, the vastus medialis and vastus lateralis muscles showed slight, although not statistically significant,increases in activity from before to after therapy. In the symptomatic knees, however, both the vastus medialis and vastuslateralis muscles in both groups showed statistically significant increases in integrated EMG activity from the beginning to theend of therapy ( P < 0.001) (Fig. 3) . The increase in activity found in each group was not significantly different between the twogroups.
DISCUSSION
Patellofemoral pain is a common but sometimes poorly understood syndrome that affects a large percentage of the athleticpopulation. The incidence of patellofemoral pain has been reported to be high in muscular male and female athletes. [11]
Derscheid and Feiring [8] found that 30% of patients seen in their sports medicine clinic had patellofemoral pain. In a study of
running injuries, James et al. [13] found that the patellofemoral area was the most frequent site of knee pain.
Fulkerson and Shea [10] have stated that the most frequent cause of patellofemoral pain is patellofemoral malalignment,
manifested as subluxation and tilt. Malalignment has been shown to result in damage to the patellar articular surface as well asstrain on the peripatellar structures, which can result in pain.
It has been stated that a muscular imbalance between the vastus medialis and vastus lateralis muscles contributes to patellarmaltracking. [10] [12] [23] Numerous EMG studies have documented an overall decrease in quadriceps muscle activity and an
imbalance in vastus medialis and vastus lateralis muscle activity in patients with patellofemoral pain and subluxation. [17] [22] [23]
[28] [39] The decrease in quadriceps muscle activity was found to originate from a reflex inhibition. The stimulus for this
inhibitory effect has been found to originate from pain and effusion. [6] [35] [36]

8/21/13 MD Consult - Print Previewer
www.mdconsult.com/website/view/preview?printing=true&URL=http%3A//www.mdconsult.com/das/article/body/421319447-2/jorg%3Djournal%26source%3D%2… 6/9
Figure 3. Integrated EMG activity increased pre- versus posttherapy for the tape and no-tape groups.
The conservative management of patellofemoral pain has focused on modification of activities, nonsteroidal antiinflammatorymedications, and quadriceps muscle strengthening. [2] [10] [12] The results of this approach have been successful for many
authors. [3] [7] [38]
As part of the conservative management, patellar braces have been used to decrease pain. Palumbo [31] found that a dynamic
patellar brace was effective in reducing symptoms in 93% of 62 patients. This brace is said to exert a medially displacing force tothe lateral border of the patella to maintain improved alignment during flexion and extension. Levine and Splain [18] reported that
77% of the patients with patellofemoral pain (54 of 70) experienced significant pain relief with an infrapatellar strap. The exact roleof bracing is unclear, but bracing may improve abnormalities in the patellofemoral relationship.
In an effort to improve patellar maltracking, McConnell [23] [24] has suggested a program that uses a taping technique to improve
patellofemoral alignment. In addition to addressing the glide component of maltracking, this taping technique is said to addresspatellar tilt and rotation abnormalities. It has been compared with a "custom brace" in that individual tracking abnormalities maybe treated in each patient. McConnell's program also involves specific stretching activities for tight peripatellar structures aswell as selective strengthening exercises for the vastus medialis muscle. In her original article, she states a 92% success rate in35 patients with a mean duration of symptoms of approximately 5 years. Eighty-three percent of these patients (29) reportedlyexperienced no pain in five or fewer treatment sessions. [24]
In our study, a favorable outcome with respect to pain was based on improvements in the visual analog scale. This scalequantitates the severity of symptoms and compares the effect of a treatment modality at the beginning of treatment with theeffect at the end of treatment. [9]
We report a marked reduction in pain symptoms among patients enrolled in the taping program as well as those with no patellartaping program. Statistically, patients reported less pain in all areas; nonstatistically, trends of improvement were also seen. Thedegree of improvement from before to after therapy in each group was not significantly different between the tape and no-tapegroups.
Patients with patellofemoral pain and chondromalacia have been found to have decreased strength of the affected limb. In astudy of 30 patients with patellofemoral disorders, Nordgren et al. [30] found that strength during maximal isokinetic knee
extension was significantly decreased compared with the strength of the contralateral uninvolved knee. Lysholm, [19] in a study
of patients with anterior knee pain, also reported a negative correlation between pain and peak torque.
We also found an initial imbalance in strength between symptomatic and asymptomatic knees in our patients with unilateralpain. The imbalance, present at both the slow (60 deg/sec) and fast (180 deg/sec) speeds, was statistically significant only at theslow speed. A study on isokinetic exercise found a significant increase in the reactive forces of the patellofemoral joint withCybex speeds of 30 deg/sec compared with faster speeds at 180 deg/sec. [29]
65
8/21/13 MD Consult - Print Previewer
www.mdconsult.com/website/view/preview?printing=true&URL=http%3A//www.mdconsult.com/das/article/body/421319447-2/jorg%3Djournal%26source%3D%2… 7/9
We speculate that the difference seen in the pretreatment comparison between the slow and fast Cybex speeds represents anincreased discomfort level associated with increased reactive forces of the patellofemoral joint. Increased discomfort wouldpresumably affect Cybex performance preferentially at the slower speeds.
In evaluating the strength improvement in each group after therapy, we found that both the tape and no-tape groups improvedas expected. Comparing the degree of improvement between the groups, we again found no statistical difference.
Cybex testing revealed a greater degree of improvement in strength at the 180 deg/sec versus the 60 deg/sec speed aftertreatment. This preferential improvement in strength at the high versus low Cybex speeds has been reported by others, but anexplanation for the improvement has been unclear. [32] In light of the fact that most functional activities exceed 200 deg/sec, we
speculate that the improvement at the more functional velocity (i.e., 180 deg/sec) would occur sooner than at the slower(nonfunctional) velocity.
Electromyography has been used to assess patients with patellofemoral pain. Special attention has been paid to the vastusmedialis muscle because of the suggestion that its dysfunctional activity may lead to patellar maltracking. However, studies arecontroversial with respect to the EMG activity of quadriceps muscles. Mariani and Caruso [22] demonstrated a vastus medialis
and vastus lateralis muscle imbalance in patients with patellar subluxation compared with a healthy, asymptomatic group. Thisimbalance returned to normal after surgery to correct malalignment of the extensor mechanism. Other authors have also reporteda vastus medialis and vastus lateralis muscle imbalance. [17] [23] [34] [39] The origin of this imbalance is thought to be from a
pain-mediated reflex inhibition of the quadriceps muscle, specifically the vastus medialis muscle. [1] [24] [35] [36] Studies have
also demonstrated similar levels of activity (i.e., no imbalance between the vastus medialis and vastus lateralis muscles) inhealthy individuals. [33] Caution must be used when comparing the results of healthy and affected knees because studies vary
with respect to the type of exercise performed while monitoring the EMG activities. For example, maximal effort isometric exercisewould be different from isotonic exercise.
Other studies looking at the existence of a vastus medialis and vastus lateralis muscle imbalance in patients with patellofemoralpain have shown no imbalance, [21] no imbalance but overall decreased activity, [27] [28] and a reversal of the normal firing order
of the vastus medialis muscle compared with the vastus lateralis muscle. [37]
Our study looked at the initial vastus medialis and vastus lateralis muscle ratio between symptomatic and asymptomatic kneesand found no difference. The result of this study, which used a closed kinetic exercise to record EMG, is supported by similarstudies. [21]
We analyzed the EMG results of before and after therapy, specifically the activity trend of the particular muscle. Results showedsignificantly increased activity in the vastus medialis and vastus lateralis muscles after therapy. These increases were notstatistically different between the tape and no-tape groups.
In this study, we attempted to compare two groups of patients with similar symptoms, examination, and radiographic findings,keeping the presence or absence of patellar taping as the key variable. The central issue in this study was that the key variable(i.e., the addition of a patellar taping technique) did not alter--favorably or adversely--the end result of a physical therapyprogram.
CONCLUSIONS
Results indicate that in similar groups of patients with patellofemoral pain, there is no beneficial effect of adding a patellar tapingprogram to a standard physical therapy program. A formal physical therapy program does appear to be beneficial, but our studydid not address this issue. This study was relatively small; therefore, larger prospective studies addressing this new modality ofphysical therapy are warranted to support the authors' opinions.
References
1. Arvidsson I, Eriksson E, Knutsson E, et al: Reduction of pain inhibition on voluntary muscle activation by epidural analgesia. Orthopedics 9:
1415-1419, 1986
2. Beckman M, Craig R, Lehman R: Rehabilitation of patellofemoral dysfunction in the athlete. Clin Sports Med 8: 841-860, 1989
3. Bennett JG, Stauber WT: Evaluation and treatment of anterior knee pain using eccentric exercise. Med Sci Sports Exerc 18: 526-530, 1986
4. Cassisi JE, Sexton-Radek K, Castrogiovanni M, et al: The use of ambulatory EMG-monitoring to measure compliance with lumbar strengthening
8/21/13 MD Consult - Print Previewer
www.mdconsult.com/website/view/preview?printing=true&URL=http%3A//www.mdconsult.com/das/article/body/421319447-2/jorg%3Djournal%26source%3D%2… 8/9
exercises. Biofeedback Self Regul 18: 45-52, 1993
5. Chang RW, Falconer J, Stulberg SD, et al: Prerandomization: An alternative to classic randomization. J Bone Joint Surg 72A: 1451-1455, 1990
6. deAndrade JR, Grant C, Dixon ASJ: Joint distension and reflex muscle inhibition in the knee. J Bone Joint Surg 47A: 313-322, 1965
7. DeHaven KE, Dolan WA, Mayer PJ: Chondromalacia patellae in athletes. Clinical presentation and conservative management. Am J Sports Med
7: 5-11, 1979
8. Derscheid GL, Feiring DC: A statistical analysis to characterize treatment adherence of the 18 most common diagnoses seen at the sports
medicine clinic. J Orthop Sports Phys Ther 9: 40-46, 1987
9. Flandry F, Hunt JP, Terry GC, et al: Analysis of subjective knee complaints using visual analog scales. Am J Sports Med 19: 112-118, 1991
10. Fulkerson JP, Shea KP: Current concepts review: Disorders of patellofemoral alignment. J Bone Joint Surg 72A: 1424-1429, 1990
11. Hughston JC: Subluxation of the patella. J Bone Joint Surg 50A: 1003-1026, 1968
12. Insall J: Current concepts review: Patellar pain. J Bone Joint Surg 64A: 147-152, 1982
13. James SL, Bates BT, Osternig LR: Injuries to runners. Am J Sports Med 6: 40-50, 1978
14. Kadaba MP, Wootten ME, Gainey WJ, et al: Repeatability of phasic muscle activity: Performance of surface and intramuscular wire electrodes in
gait analysis. J Orthop Res 3: 350-359, 1985
15. Kolowich PA, Paulos LE, Rosenberg TD, et al: Lateral release of the patella: Indications and contraindications. Am J Sports Med 18: 359-365,
1990
16. Laurin CA, Dussault R, Levesque HP: The tangential X-ray investigation of the patellofemoral joint. Clin Orthop 144: 16-26, 1979
17. LeVeau BF, Rogers C: Selective training of the vastus medialis muscle using EMG biofeedback. Phys Ther 60: 1410-1415, 1980
18. Levine J, Splain SH: Use of the infrapatella strap in the treatment of patellofemoral pain. Clin Orthop 139: 179-181, 1979
19. Lysholm J: The relation between pain and torque in an isokinetic strength test of knee extension. Arthroscopy 3: 182-184, 1987
20. Lysholm J, Nordin M, Ekstrand J, et al: The effect of a patella brace on performance in a knee extension strength test in patients with patellar
pain. Am J Sports Med 12: 110-112, 1984
21. MacIntyre DL, Robertson GC: Quadriceps muscle activity in women runners with and without patellofemoral pain syndrome. Arch Phys Med
Rehab 73: 10-14, 1992
66
22. Mariani PP, Caruso I: An electromyographic investigation of subluxation of the patella. J Bone Joint Surg 61B: 169-171, 1979
23. McConnell JS: Training the vastus medialis oblique in the management of patellofemoral pain. From the Proceedings of the Tenth International
Congress of WCPT. Sydney, Australia, 1987
24. McConnell JS: The management of chondromalacia patellae: A long term solution. Austr J Physiother 32: 215-223, 1986
25. Merchant AC, Mercer RL, Jacobsen RH, et al: Roentgenographic analysis of patellofemoral congruence. J Bone Joint Surg 56A: 1391-1396,
1974
26. Moffroid M, Whipple R, Hofkosh J, et al: A study of isokinetic exercise. Phys Ther 49: 735-746, 1969

8/21/13 MD Consult - Print Previewer
www.mdconsult.com/website/view/preview?printing=true&URL=http%3A//www.mdconsult.com/das/article/body/421319447-2/jorg%3Djournal%26source%3D%2… 9/9
27. Moller BN, Jurik AG, T idemand-Dal C, et al: The quadriceps function in patellofemoral disorders: A radiographic and electromyographic study.
Arch Orthop Trauma Surg 106: 195-198, 1987
28. Moller BN, Krebs B, T idemand-Dal C, et al: Isometric contractions in the patellofemoral pain syndrome: An electromyographic study. Arch
Orthop Trauma Surg 105: 24-27, 1986
29. Nisell R: Mechanics of the knee: A study of joint and muscle load with clinical applications. Acta Orthop Scand (Suppl) 216: 1-42, 1985
30. Nordgren B, Nordesjo LO, Rauschning W: Isokinetic knee extension strength and pain before and after advancement of the tibial tuberosity.
Arch Orthop Trauma Surg 102: 95-101, 1983
31. Palumbo PM: Dynamic patellar brace: A new orthosis in the management of patellofemoral disorders. A preliminary report. Am J Sports Med 9:
45-49, 1981
32. Pipes TV, Wilmore JH: Isokinetic vs isotonic strength training in adult men. Med Sci Sports 7: 262-274, 1975
33. Reynolds L, Levin TA, Mendeiros JM, et al: EMG activity of the vastus medialis oblique and the vastus lateralis in their role in patellar
alignment. Am J Phys Med 62: 61-70, 1983
34. Souza DR, Gross MT: Comparison of vastus medialis obliquus:vastus lateralis muscle integrated electromyographic ratios between healthy subjects
and patients with patellofemoral pain. Phys Ther 71: 310-316, 1991
35. Spencer JD, Hayes KC, Alexander IJ: Knee joint effusion and quadriceps reflex inhibition in man. Arch Phys Med Rehabil 65: 171-177, 1984
36. Stratford P: Electromyography of the quadriceps femoris muscles in subjects with normal and acutely effused knees. Phys Ther 62: 279-283,
1982
37. Voight ML, Wieder DL: Comparative reflex response times of vastus medialis obliquus and vastus lateralis in normal subjects and subjects with
extensor mechanism dysfunction. An electromyographic study. Am J Sports Med 19: 131-137, 1991
38. Whitelaw GP, Rullo DJ, Markowitz HD, et al: A conservative approach to anterior knee pain. Clin Orthop 246: 234-237, 1989
39. Wise HH, Fiebert IM, Kates JL: EMG biofeedback as treatment for patellofemoral pain syndrome. J Orthop Sports Phys Ther 6: 95-103, 1984
Copyright © 2013 Elsevier Inc. All rights reserved. - www.mdconsult.com
Bookmark URL: /das/journal/view/0/N/726431?ja=40325&PAGE=1.html&issn=0363-5465&source=
Client IP Address: 132.170.115.44DAS Host: isis