
Patellar Cartilage: T2 Values and Morphologic Abnormalities at 3.0-T MR Imaging in Relation to...
12
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. ORIGINAL RESEARCH n MUSCULOSKELETAL IMAGING Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 509 Patellar Cartilage: T2 Values and Morphologic Abnormalities at 3.0-T MR Imaging in Relation to Physical Activity in Asymptomatic Subjects from the Osteoarthritis Initiative 1 Christoph Stehling, MD Hans Liebl, MS Roland Krug, PhD Nancy E. Lane, MD Michael C. Nevitt, PhD John Lynch, PhD Charles E. McCulloch, PhD Thomas M. Link, MD, PhD Purpose: To study the interrelationship between patella cartilage T2 relaxation time, other knee abnormalities, and physical activity levels in asymptomatic subjects from the Osteoar- thritis Initiative (OAI) incidence cohort. Materials and Methods: The study had institutional review board approval and was HIPAA compliant. One hundred twenty subjects from the OAI without knee pain (age, 45–55 years) and with risk factors for knee osteoarthritis (OA) were studied by using knee radiographs, 3.0-T knee magnetic resonance (MR) images (including intermediate-weighted fast spin- echo and T2 mapping sequences), and the Physical Ac- tivity Scale for the Elderly. MR images of the right knee were assessed by two musculoskeletal radiologists for the presence and grade of abnormalities. Segmentation of the patella cartilage was performed, and T2 maps were gener- ated. Statistical significance was determined by using anal- ysis of variance, x 2 analysis, correlation coefficient tests, the Cohen k, and a multiple linear regression model. Results: Cartilage lesions were found in 95 (79.0%) of 120 knees, and meniscal lesions were found in 54 (45%) of 120 knees. A significant correlation between patella cartilage T2 val- ues and the severity and grade of cartilage ( P = .0025) and meniscus ( P = .0067) lesions was demonstrated. Subjects with high activity levels had significantly higher prevalence and grade of abnormalities and higher T2 values (48.7 msec 6 4.35 vs 45.8 msec 6 3.93; P , .001) than did sub- jects with low activity levels. Conclusion: Middle-aged asymptomatic individuals with risk factors for knee OA had a high prevalence of cartilage and me- niscus knee lesions. Physically active individuals had more knee abnormalities and higher patellar T2 values. Addi- tional studies will be needed to determine causality. © RSNA, 2010 1 From the Musculoskeletal and Quantitative Imaging Group in the Department of Radiology (C.S., H.L., R.K., T.M.L.) and the Department of Epidemiology and Biostatistics (M.C.N., J.L., C.E.M.), University of California San Francisco, 185 Berry St, Suite 350, San Francisco, CA 94107; Department of Clinical Radiology, University of Muenster, Muenster, Germany (C.S.); Medical School, Technical University of Munich, Munich, Germany (H.L.); and Center for Healthy Aging, University of California Davis, Sacramento, Calif (N.E.L.). Received April 5, 2009; revision requested May 30; final revision received July 17; accepted July 29; final version accepted August 18. Supported in part by Merck Research Laboratories, Novartis Pharmaceuticals, Glaxo- SmithKline, and Pfizer. Private-sector Osteoarthritis Initiative funding managed by Foundation for the National Institutes of Health. C.S. supported by Deutsche Forschungsgemein- schaft (grant STE 1829/1–1). Address correspondence to C.S. (e-mail: [email protected]). © RSNA, 2009
Transcript of Patellar Cartilage: T2 Values and Morphologic Abnormalities at 3.0-T MR Imaging in Relation to...

Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.
ORIGINAL RESEARCH n
MUSCULOSKELETAL IM
AGING
Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 509
Patellar Cartilage: T2 Values and Morphologic Abnormalities at 3.0-T MR Imaging in Relation to Physical Activity in Asymptomatic Subjects from the Osteoarthritis Initiative 1
Christoph Stehling , MD Hans Liebl , MS Roland Krug , PhD Nancy E. Lane , MD Michael C. Nevitt , PhD John Lynch , PhD Charles E. McCulloch , PhD Thomas M. Link , MD , PhD
Purpose: To study the interrelationship between patella cartilage T2 relaxation time, other knee abnormalities, and physical activity levels in asymptomatic subjects from the Osteoar-thritis Initiative (OAI) incidence cohort.
Materials and Methods:
The study had institutional review board approval and was HIPAA compliant. One hundred twenty subjects from the OAI without knee pain (age, 45–55 years) and with risk factors for knee osteoarthritis (OA) were studied by using knee radiographs, 3.0-T knee magnetic resonance (MR) images (including intermediate-weighted fast spin-echo and T2 mapping sequences), and the Physical Ac-tivity Scale for the Elderly. MR images of the right knee were assessed by two musculoskeletal radiologists for the presence and grade of abnormalities. Segmentation of the patella cartilage was performed, and T2 maps were gener-ated. Statistical signifi cance was determined by using anal-ysis of variance, x 2 analysis, correlation coeffi cient tests, the Cohen k , and a multiple linear regression model.
Results: Cartilage lesions were found in 95 (79.0%) of 120 knees, and meniscal lesions were found in 54 (45%) of 120 knees. A signifi cant correlation between patella cartilage T2 val-ues and the severity and grade of cartilage ( P = .0025) and meniscus ( P = .0067) lesions was demonstrated. Subjects with high activity levels had signifi cantly higher prevalence and grade of abnormalities and higher T2 values (48.7 msec 6 4.35 vs 45.8 msec 6 3.93; P , .001) than did sub-jects with low activity levels.
Conclusion: Middle-aged asymptomatic individuals with risk factors for knee OA had a high prevalence of cartilage and me-niscus knee lesions. Physically active individuals had more knee abnormalities and higher patellar T2 values. Addi-tional studies will be needed to determine causality.
© RSNA, 2010
1 From the Musculoskeletal and Quantitative Imaging Group in the Department of Radiology (C.S., H.L., R.K., T.M.L.) and the Department of Epidemiology and Biostatistics (M.C.N., J.L., C.E.M.), University of California San Francisco, 185 Berry St, Suite 350, San Francisco, CA 94107; Department of Clinical Radiology, University of Muenster, Muenster, Germany (C.S.); Medical School, Technical University of Munich, Munich, Germany (H.L.); and Center for Healthy Aging, University of California Davis, Sacramento, Calif (N.E.L.). Received April 5, 2009; revision requested May 30; fi nal revision received July 17; accepted July 29; fi nal version accepted August 18. Supported in part by Merck Research Laboratories, Novartis Pharmaceuticals, Glaxo-SmithKline, and Pfi zer. Private-sector Osteoarthritis Initiative funding managed by Foundation for the National Institutes of Health. C.S. supported by Deutsche Forschungsgemein-schaft (grant STE 1829/1–1). Address correspondence to C.S. (e-mail : [email protected] ).
© RSNA, 2009

510 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
fornia Committee for Human Research. This article received the approval of the OAI Publications Committee on the basis of a review of its scientifi c con-tent and data interpretation. The study protocol, amendments, and informed consent documentation were reviewed and approved by the local institutional review boards.
Subjects The right knees of 120 subjects were included in our analysis, which is a subset of the 4796 participants in the OAI. Data were obtained from the OAI database, which is publicly accessible (http://www.oai.ucsf.edu/) . The specifi c data sets used were baseline clinical data set 0.2.2 and baseline image data set 0.E.1. Subjects analyzed were from the incidence subcohort of the OAI, who were characterized by the absence of symptomatic knee OA and presence of risk factors for OA. These risk factors included knee symptoms (ie, pain, ach-ing, or stiffness in or around the joints) during the past 12 months, obesity,
as a biomarker to noninvasively assess cartilage quality and susceptibility to injury. Characterization of the cartilage matrix integrity with T2 relaxation time measurements could potentially help in prevention of OA progression by en-abling identifi cation of individuals at risk for OA who may benefi t from treat-ment or behavioral interventions before irreversible morphologic changes occur ( 10,11 ). Researchers in a number of studies ( 12–16 ) have examined OA risk factors in relation to quantitative and qualitative cartilage loss at MR imaging. However, there is a paucity of data ana-lyzing cartilage changes on MR images, particularly T2 cartilage matrix measure-ments, in relation to physical activity as biomarkers for early OA changes.
To better understand the natural evolution of OA by using MR imag-ing, the National Institutes of Health (Bethesda, Md) launched the Osteoar-thritis Initiative (OAI). It is a multi-center longitudinal observational study of 4796 persons with, or at risk for de-veloping, knee OA that has created a public archive of data, biologic samples, and joint images. T2 relaxation times and measures of physical activity were also obtained as part of the OAI MR imaging protocol.
The aim of our study was to assess the cartilage T2 relaxation time in rela-tion to knee abnormalities on 3.0-T MR images and the physical activity levels in asymptomatic subjects from the inci-dence cohort of the OAI.
Materials and Methods
This Health Insurance Portability and Accountability Act–compliant study was performed in accordance with the rules and regulations of the University of Cali-
Osteoarthritis (OA) is a multifac-torial degenerative joint disease and a leading cause of disability
worldwide, with radiographic evidence seen in at least 70% of the population over age 65 ( 1 ). Nearly 27 million indi-viduals have clinically symptomatic OA, with the knee being the most com-monly affected joint ( 2 ). OA is charac-terized by the progressive loss of hyaline articular cartilage; however, cartilage loss and OA symptoms are preceded by damage to the collagen-proteoglycan matrix and elevation of cartilage water content ( 3,4 ). Therefore, a sensitive method for detecting structural and functional changes in the early stages of OA would be valuable for assessing the progression of disease and for thera-peutic monitoring. Magnetic resonance (MR) imaging has an increasing role in the diagnosis and monitoring of OA ( 5 ), with typical MR characteristics includ-ing cartilage defects, meniscal and liga-mentous abnormalities, bone marrow edema–like lesions, and subchondral cysts ( 2,6 ).
In addition to enabling semiquantita-tive assessment of cartilage morphology and quantifi cation of its thickness and volume, MR imaging has been shown ( 7,8 ) to have potential for the charac-terization of changes in the biochemical composition of cartilage during early OA. Techniques include T2 quantifi ca-tion ( 9 ), which may be able to be used
Implications for Patient Care
T2 relaxation time measurements n
at the patella may be a marker for internal joint derangement in terms of cartilage and meniscal lesions.
Subjects with higher physical n
activity levels and high T2 have more cartilage and meniscal degeneration.
Advances in Knowledge
Middle-aged asymptomatic indi- n
viduals with risk factors for knee osteoarthritis had a high preva-lence of cartilage and meniscus lesions.
A signifi cant correlation between n
patellar cartilage T2 values and the presence and severity of car-tilage and meniscus lesions was found.
Physically active individuals n
showed signifi cantly more carti-lage and meniscus abnormalities; in addition, a signifi cant correla-tion between physical activity level and T2 values was also demonstrated.
Published online before print10.1148/radiol.09090596
Radiology 2010; 254:509–520
Abbrevations: KOOS = Knee Injury and Osteoarthritis Outcome Score OA = osteoarthritis OAI = Osteoarthritis Initiative PASE = Physical Activity Scale for the Elderly SE = spin-echo WOMAC = Western Ontario and McMaster University WORMS = Whole-Organ Magnetic Resonance Imaging
Score
Author contributions: Guarantors of integrity of entire study, C.S., R.K., N.E.L., T.M.L.; study concepts/study design or data acquisition or data analysis/interpretation, all authors; manuscript drafting or manuscript revision for important intellectual content, all authors; approval of fi nal version of submitted manuscript, all authors; literature research, C.S., H.L., R.K., N.E.L., J.L., T.M.L.; clinical studies, C.S., H.L., R.K., T.M.L.; statistical analysis, C.S., R.K., N.E.L., J.L., C.E.M., T.M.L.; and manuscript editing, C.S., R.K., N.E.L., M.C.N., J.L, C.E.M., T.M.L.
Funding: This research was supported by the National Institutes of Health (grants N01-AR-2–2258, N01-AR-2–2259, N01-AR-2–2260, N01-AR-2–2261, and N01-AR-2–2262).
Authors stated no fi nancial relationship to disclose.

Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 511
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
Ambient light was reduced during the reading session, and no time constraints were used. Radiologists had access to all sequences acquired, and the sequences listed in Table 1 were used for the analysis.
The Whole-Organ Magnetic Reso-nance Imaging Score (WORMS) was used to evaluate the images for OA- related abnormalities of the knee ( 28–30 ). The original 15 WORMS regions at the knee were condensed to six regions for our study: patella, trochlea, medial femur, lateral femur, medial tibia, and lateral tibia. By using the semiquantita-tive scoring system, the following joint structures were separately evaluated: (a) cartilage, (b) ligaments, (c) menisci, (d) bone marrow edema pattern, (e) osteophytes, (f) synovitis or effusion, (g) subarticular cysts, (h) fl attening or depression of the articular surfaces, (i) loose bodies, and (j) popliteal cysts.
Cartilage signal intensity and mor-phology were scored together by using an eight-point scale: 0 = normal thick-ness and signal intensity; 1 = normal thickness but increased signal intensity on T2-weighted images; 2.0 = partial-thickness focal defect less than 1 cm at its greatest width; 2.5 = full-thickness focal defect less than 1 cm at its great-est width; 3 = multiple areas of partial-thickness (grade 2.0) defects inter-mixed with areas of normal thickness or a grade 2.0 defect wider than 1 cm but occupying less than 75% of the re-gion; 4 = diffuse ( � 75% of the region) partial-thickness loss; 5 = multiple ar-eas of full-thickness loss (grade 2.5) or a grade 2.5 lesion wider than 1 cm but occupying less than 75% of the region; and 6 = diffuse ( � 75% of the region) full-thickness loss.
Alterations in meniscal morphology were assessed separately in six regions (medial and lateral aspects of the ante-rior, body, and posterior portions of the meniscus) by using a four-level scale: 0 = normal, 1 = intrasubstance abnormali-ties, 2 = nondisplaced tear, 3 = displaced or complex tear, and 4 = complete destruction or maceration. Meniscal extrusion was graded as follows: 0 = none and 1 = meniscal extrusion more than 3 mm beyond the tibial plateau.
Subjects completed a 400-m walk and isometric muscle strength tests. The time (in seconds) to complete the 400-m walk was recorded for each subject ( 24 ). The maximum isometric strength of the right knee was obtained in newtons in maximum force fl exion and extension by using the Good Strength Chair (Metitur, Jyvaskyla, Finland) ( 25 ).
Imaging Bilateral standing posteroanterior fi xed-fl exion knee radiographs were obtained. Knees were positioned in a Plexiglas frame (SynaFlexer; CCBR-Synarc, San Francisco, Calif ) with 20°–30° fl exion and 10° internal rotation of the feet bi-laterally. A focus-to-fi lm distance of 72 inches (1 inch = 2.54 cm) was used. All radiographs were evaluated by two radi-ologists (T.M.L. and C.S., with 20 and 4 years experience in musculoskeletal imaging, respectively) in consensus, who graded the images by using the Kellgren-Lawrence technique ( 6,26 ).
MR images were obtained with a 3.0-T MR imager (Trio; Siemens, Erlangen, Germany). Both knees were examined with standard morphologic sequences, and T2-mapping sequences were used for the right knee only. A standard knee coil was used. For the right knee, the images obtained with the following sequences were analyzed: (a) coronal intermediate-weighted two-dimensional fast spin-echo (SE), (b) sagittal three-dimensional dual-echo steady-state with selective water excitation with coronal and axial reformations, (c) sagittal two-dimensional intermediate-weighted fast SE with fat suppression, (d) sagittal T2-weighted two-dimensional multiecho SE, and (e) coronal T1-weighted three-dimensional fast low-angle shot with water excitation ( 27 ). The sequence pa-rameters are presented in Table 1 .
Image Analysis Semiquantitative morphologic analyses.— MR images of the right knee were reviewed on picture archiving and communication system workstations (Agfa , Ridgefi eld Park, NJ) by two musculoskeletal radiologists (T.M.L. and C.S.). If scores were not identical, consensus readings were performed.
a history of knee surgery or injury, a family history of total knee replace-ment, Heberden nodes, and repetitive knee-bending activities. Exclusion cri-teria were rheumatoid arthritis, bilat-eral severe knee joint space narrowing, and contraindications to or inability to undergo MR imaging. Specifi c inclusion criteria were (a) a baseline Western On-tario and McMaster University (WOMAC) Osteoarthritis Index pain score of zero for both knees, (b) age of 45–55 years, and (c) a body mass index (BMI) of 19–27 kg/m 2 . These criteria were used to exclude obesity as a risk factor and to focus on younger subjects. On the basis of these criteria, 120 patients (mean age, 50.8 years 6 2.84 [standard deviation ]; range, 45–55 years), includ-ing 60 women (mean age, 50.88 years 6 2.72) and 60 men (mean age, 50.72 years 6 2.97), were identifi ed and included.
Questionnaires and Clinical Examination The WOMAC Osteoarthritis Index is a multidimensional health status instru-ment that is used to assess pain, stiff-ness, and physical function in patients with OA of the knee and hip ( 17,18 ). We included only subjects with a WOMAC pain score of zero for both knees for the 7 days preceding the baseline clinic visit. OAI participants with a WOMAC pain score higher than zero (3485 of 4796) were excluded.
Physical activity level was assessed by using the Physical Activity Scale for the Elderly (PASE), an established ques-tionnaire for measuring physical activ-ity in older individuals ( 19 ) that has also been validated in younger subjects ( 20–22 ). Washburn et al ( 19 ) found the PASE to be a reliable and valid instru-ment for the assessment of physical ac-tivity in epidemiologic studies.
The Knee Injury and Osteoarthritis Outcome Score (KOOS) is an extension of the WOMAC Osteoarthritis Index for evaluating short- and long-term symp-toms and function in subjects with knee injury and OA. The KOOS adds three subscales to the WOMAC Osteoarthri-tis Index: other knee symptoms, physi-cal function in sport and recreation, and knee-related quality of life ( 23 ).

512 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
images of the right knee, T2 maps were created and provided exponential curve fi ts and T2 for each pixel. Images were transferred to a remote workstation (SPARC; Sun Microsystems, Mountain View, Calif). The relaxation time, T2, was estimated by fi tting an exponential function to the signal intensity at dif-ferent echo times as follows : SI(TE) ~ exp(–TE/T2), where SI(TE) is signal intensity as a function of echo time, TE is echo time, and T2 is the transverse relaxation time. Investigators have sug-gested that articular cartilage has a multiexponential T2 decay, with a short (eg, microseconds ) component and a longer component. Without the use of unvalidated specialized hardware, echo times on the order of microseconds cannot be obtained; thus, we did not attempt to measure the multiexponen-tial relaxation times. We used a simpli-fi ed monoexponential decay model that
WORMS score for each abnormality was calculated by adding the scores for all subregions in a knee.
Cartilage lesions were also graded by using the MR imaging classifi cation described by Recht et al ( 31 ) that is based on the arthroscopic Noyes and Stabler scoring system ( 32 ): I = areas of inhomogeneous signal intensity on intermediate-weighted fast SE fat- saturated sequences, II = defects involv-ing less than half of the articular car-tilage thickness, III = defects involving more than half of the cartilage but less than full thickness, and IV = full thick-ness defects exposing the bone. In addition, the largest diameter of the cartilage lesion in the sagittal, coro-nal, or axial plane and the two largest diameters of bone marrow edema in the sagittal plane were measured.
T2 measurements.— By using the sagittal two-dimensional multiecho SE
Subarticular bone marrow abnormali-ties were defi ned as poorly marginated areas of increased signal intensity in the normal subchondral and epiphyseal bone marrow on T2-weighted fast SE fat-suppressed MR images. This feature was graded on a four-point scale on the basis of the extent of regional involvement: 0 = none, 1 = 25% of the region or less, 2 = 25%–50%, and 3 = more than 50%. Ligaments were evaluated by using a four-point scale: 0 = no lesion, 1 = grade 1 sprain (signal intensity changes around ligament), 2 = grade 2 sprain (partial tear), and 3 = complete tear. Joint effu-sion was evaluated by using a four-point scale: 0 = normal, 1 = less than 33% of maximum potential distention, 2 = 33%–66%, and 3 = greater than 66%.
On the basis of MR fi ndings, a knee was defi ned as abnormal if a WORMS value of 1 or higher was found in any of the subregions evaluated. A summary
Table 1
MR Imaging Parameters
ParameterCoronal Intermediate-weighted 2D Fast SE
Sagittal 3D Dual-Echo Steady-State with Water-Excitation
Coronal T1-weighted 3D FLASH with Water-Excitation
Sagittal T2-weighted 2D Multiecho SE
Sagittal Intermediate-weighted 2D Fast SE Fat-suppressed
Matrix phase 307 307 512 269 313Matrix frequency 384 384 512 384 448No. of sections 35 160 80 21 37Field of view (mm) 140 140 160 120 160Section thickness (mm) 3 0.7 1.5 3 3Section gap (mm) 0 0 0 0.5 0Flip angle (degrees) 180 25 12 … 180Repetition time (msec) 3700 16.3 20 2700 3200Echo time (msec) 29 4.7 7.57 10, 20, 30, 40, 50, 60, 70 30Bandwidth (Hz/pixel) 352 185 130 250 248Chemical shift (pixels) 1.3 0 0 1.8 0No. of signals acquired 1 1 1 1 1Echo train length 7 1 1 1 5Phase encode axis R/L A/P R/L A/P A/PDistance factor (%) 0 0 0 16 0Phase oversampling 20 0 0 0 40Section oversampling 0 10 0 0 0Phase resolution 80 80 100 70 70Phase partial Fourier 1 1 1 0.875 1Readout partial Fourier 1 1 1 1 1Section partial Fourier 1 0.75 0.75 0.75 1X-axis resolution (mm) 0.365 0.365 0.313 0.313 0.357Y-axis resolution (mm) 0.456 0.456 0.313 0.446 0.511
Note.—A/P = anterior/posterior, FLASH = fast low-angle shot, R/L = right/left, 3D = three-dimensional, 2D = two-dimensional.

Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 513
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
less than .05 was considered to indicate a signifi cant difference.
Results
Subject Characteristics Table 2 shows baseline characteristics, including risk factors, for all subjects and for subject by sex. While there were no sex-related differences in age, Kellgren-Lawrence scores, PASE scores, or the
Institute, Cary, NC). Descriptive sta-tistics were obtained, and differences between measurements for men and those for women were determined by using one-way analysis of variance and the Pearson x 2 test. A multiple linear regression model was used to correct correlation data for the effects of age, sex, BMI, and other risk factors (eg, history of knee injury or surgery, fam-ily history of knee replacement, and Herbeden nodes in hands). A P value of
has been previously described ( 9 ). The seven echoes (10, 20, 30, 40, 50, 60, and 70 milliseconds) that are available from the OAI image database provided stable T2 data.
Images were transferred to the re-mote workstation and analyzed by us-ing software developed at our institution with an interactive display language (Re-search Systems, Boulder, Colo) environ-ment. An interactive display language routine was used for segmentation of the patella cartilage to simplify the manual drawing of splines delineating cartilage areas. Each patella had a range of 8–15 sections, and all sections with well- visualized artifact-free cartilage were seg-mented. Tissue contrast was excellent, and water-fat shift artifacts occurring at the bone-cartilage interface were well visualized on the fi rst echo time images of the multiecho sequence, whereas fl uid was shown well on the sagittal T2 maps. To exclude both fl uid and water-fat shift artifacts from the regions of interest, adjustment of the splines was performed simultaneously by opening both image panels and using a synchro-nized cursor, section number, and zoom ( Fig 1 ). An interactive display language routine was used to calculate the mean T2 values from the regions of interest created in the T2 maps.
Reproducibility measurements.— Re producibility for the semiquantitative analyses of cartilage with the WORMS for each compartment was calculated in a sample of 12 OAI image data sets that were each assessed twice by the two ra-diologists. Each subregion was graded by using the cartilage WORMS, and grades given by each radiologists were compared ( 30 ). Cohen k statistics were calculated for inter- and intraobserver agreement.
The coeffi cient of variation was cal-culated for patella cartilage to deter-mine reproducibility of the quantitative T2 measurements ( 33 ). To test intrao-bserver reliability, 12 data sets were randomly selected and segmented three times by the same investigator.
Statistical Analysis Statistical processing was performed by using software (JMP, version 6; SAS
Figure 1
Figure 1: Sagittal (a, c) two-dimensional T2-weighted fi rst-echo SE MR images and (b, d) corresponding T2 maps show manually drawn region of interest (white outline) of patella cartilage as (a) originally drawn, which reveals cartilage quantifi cation bias owing to fl uid artifacts seen (b) when the T2 map is overlaid. Images c and d show region of interest corrected to exclude fl uid artifacts.

514 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
lent in women. Cartilage lesions at the patella were found in a high percentage (40.0%, 48 of 120) of subjects, with the fi nding more frequent in women (45%, 27 of 60) than in men (35%, 21 of 60) . If cartilage lesions at the patella were found, subjects had a greater number of
Semiquantitative Morphologic Analyses A high prevalence of meniscal (45.0%, 54 of 120) and overall cartilage (79.0%, 95 of 120) lesions (WORMS . 0) was found in all subjects ( Table 3 ). Meniscal lesions were found more frequently in men, while cartilage lesions were more preva-
time required for the 400-m walk, women had signifi cantly lower mean BMI ( P = .002), KOOS ( P = .026), and muscle strength ( P , .001). On the basis of physical activity level, subjects were divided into two groups: a low-activity group (PASE score: 0–199) and a high-activity group (PASE score: 200–400). The threshold PASE score of 200 sepa-rated subjects into two equal groups of 60. The range of the PASE is from zero to 400. The mean PASE scores for the low- and high-activity groups were 95.87 6 34.63 (range, 27–149) and 295.15 6 39.4 (range, 244–400), respectively. The median PASE score for all subjects was 196.5. There were no signifi cant differences in BMI, age, KOOS, 400-m walk, or muscle strength between subjects in the low- and high-activity groups.
Radiographic Evaluation Kellgren-Lawrence scores of 0, 1, 2, and 3 were found in 87, 29, two, and two right knees, respetively. Separate data for men and women are listed in Table 2 .
Table 2
Subject Characteristics
Characteristic All Subjects (n = 120) Men (n = 60) Women (n = 60) P Value
Risk factors* History of knee injury 33 19 14 .2798†
History of knee surgery 13 8 5 .3782†
Family history of knee replacement 16 11 5 .0993†
Heberden nodes in hands 17 4 13 .0185†
Kellgren-Lawrence score‡ 0.6 6 0.054 0.37 6 0.61 0.28 6 0.58 .446§
0* 87 41 46 1* 29 17 12 2* 2 1 1 3* 2 1 1PASE score|| 195.51 6 106.66 (27–400) 202.45 6 98.05 (27–400) 188.57 6 115.04 (27–371) .478§
Age (y)‡ 50.8 6 2.84 50.72 6 2.97 50.88 6 2.72 .749§
BMI (kg/m2)‡ 24.2 6 1.93 24.75 6 1.57 23.67 6 2.13 .002§
KOOS‡ 93.94 6 9.34 92.00 6 11.29 95.89 6 6.41 .026§
400-m walk (sec)‡ 272.57 6 30.8 275.21 6 34.59 269.65 6 26.02 .372§
Maximum force Flexion (N)‡ 168.46 6 64.54 200.43 6 64.05 137.20 6 47.96 , .001§
Extension (N)‡ 405.61 6 116.53 464.3 6 118.83 348.22 6 80.92 , .001§
* Data are numbers of patients.† Pearson x 2 test.‡ Data are means 6 standard deviations.§ Analysis of variance.|| Data are means 6 standard deviations, with ranges in parentheses.
Table 3
Prevalence of Focal Knee Abnormalities on MR Images
Lesion All Subjects (n = 120) Men (n = 60) Women (n = 60) P Value*
Meniscus 54 (45.0) 30 (50.0) 24 (40.0) .2709Ligament 28 (23.3) 17 (28.3) 11 (18.3) .1953Cartilage WORMS . 0 95 (79.2) 45 (75.0) 50 (83.3) .2611 WORMS . 1 65 (54.2) 34 (56.7) 31 (51.7)Bone marrow edema 51 (42.5) 29 (48.3) 22 (36.7) .1961Articular surface depression 0 (0) 0 (0) 0 (0) …Subarticular cyst 7 (5.8) 4 (6.7) 3 (5.0) .6969Osteophyte 47 (39.2) 24 (40.0) 23 (38.3) .8516Joint effusion 32 (26.7) 21 (35.0) 11 (18.3) .0390Loose body 4 (3.3) 3 (5.0) 1 (1.7) .3091Popliteal cyst 31 (25.8) 18 (30.0) 13 (21.7) .2971
Note.—Unless otherwise specifi ed, data are numbers of subjects, with percentages in parentheses.
* Pearson x 2 test.

Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 515
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
The interobserver agreement was 95.3%, and the intraobserver agree-ments were 95.4% and 95.1%. Ad-ditionally, inter- and intraoberserver agreement were evaluated by using the Cohen k . Values over 0.61 showed good reproducibility. The interobserver agreement k value was 0.67, and in-traobserver agreements k values were 0.69 and 0.72.
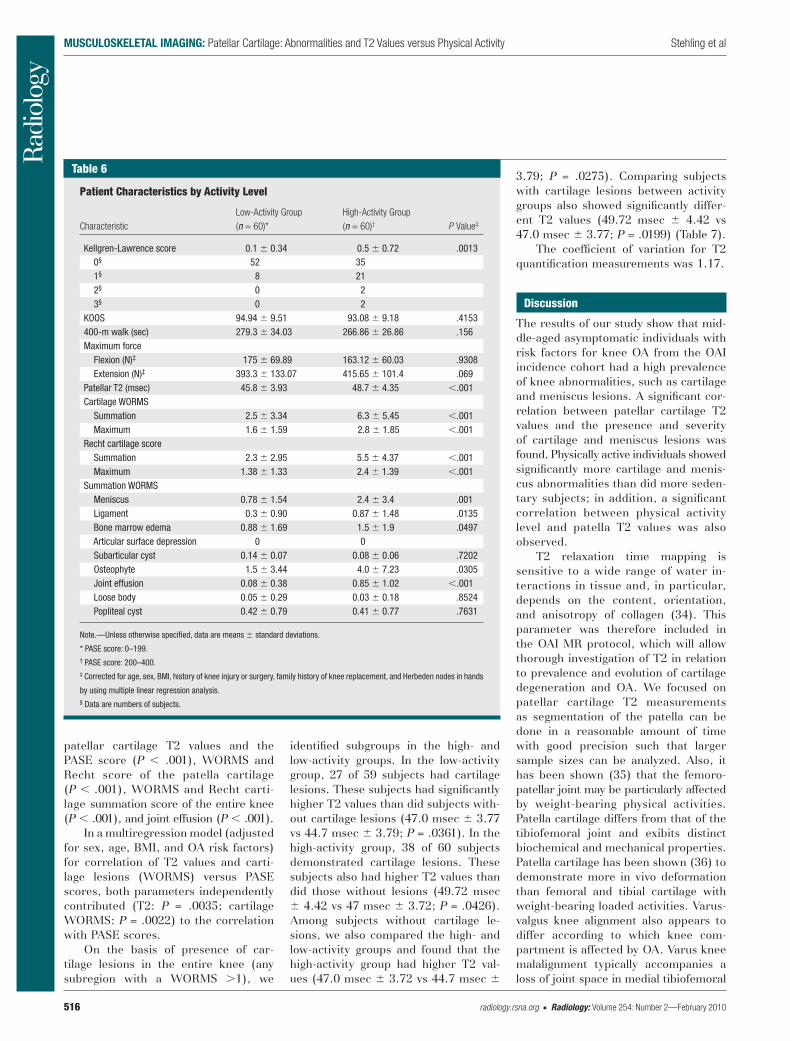
When subjects were separated into low-activity (PASE score: 0–199) and high-acitivity (PASE score: 200–400) groups, a signifi cantly higher preva-lence of abnormalities was found in the high-activity group for the menis-cus, cartilage, ligaments, bone marrow edema, and joint effusion. Cartilage le-sions (WORMS . 0) were found in 56 (93.3%) of the 60 highly active subjects versus in 39 (65.0%) of the 60 less ac-tive subjects. In addition, lesions seen in the active subjects were more severe, as evidenced by the signifi cantly higher maximum cartilage WORMS and Recht scores, than those in less active sub-jects ( Tables 5,6 ). The same results were found by using PASE as a continu-ous scale.
T2 Measurements Owing to MR artifacts, one male sub-ject in the low-activity group was ex-cluded from T2 analysis. In comparison to T2 values of patella cartilage in sub-jects without abnormalities, those in subjects with cartilage abnormalities in the whole knee (44.6 msec 6 3.51 vs 47.94 msec 6 4.35; P = .0025) and at the patella (45.9 msec 6 3.62 vs 49.94 msec 6 4.75; P , .001) were signifi -cantly higher. Similar fi ndings of higher T2 values were seen in subjects with meniscus abnormalities (46.2 msec 6 3.92 vs 48.5 msec 6 4.63; P = .0067) and those with joint effusion (46.3 msec 6 4.16 vs 49.71 msec 6 4.08; P � .0018) versus patients without those abnormalities.
The T2 values of the patella cartilage were signifi cantly higher in the high-activity group than in the low-activity group (48.7 msec 6 4.4 vs 45.8 msec 6 3.9; P , .001) ( Table 6 ; Figs 2,3 ). At multiple linear regression analysis, high correlation was observed between the
tendon (all WORMS = 2; all subjects: 8.3% [10 of 120]; men: 11.7% [seven of 60]; women: 5.0% [three of 60]) and the anterior cruciate ligament (all subjects: 6.7% [eight of 120]; men: 8.3% [fi ve of 60]; women: 5.0% [three of 60]).
more severe cartilage lesions in all other regions ( Table 4 ). Ligament lesions, bone marrow edema, joint effusion, and popliteal cysts were seen more frequently in men than in women. Ligament lesions were found most frequently at the patella
Table 4
Prevalence of Nonpatellar Cartilage Lesions in Subjects with and Those without Patellar Cartilage Lesions
Cartilage lesionNo Patellar Cartilage Lesions (n = 72)*
Patellar Cartilage Lesions (n = 48)† P Value‡
Location§
Trochlea 10 (13.89) 23 (47.92) , .001 Medial femur 13 (18.06) 21 (43.75) .0032 Lateral femur 8 (11.11) 11 (22.92) .0715 Medial tibia 4 (5.56) 10 (20.83) .0051 Lateral tibia 13 (18.06) 19 (39.58) .0123WORMS||
Trochlea 0.167 6 0.44 1.36 6 1.81 , .001 Medial femur 0.46 6 1.14 1.61 6 2.07 , .001 Lateral femur 0.25 6 0.74 0.70 6 1.34 .0129 Medial tibia 0.06 6 0.23 0.66 6 1.40 , .001 Lateral tibia 0.36 6 0.97 0.77 6 1.29 .111
* WORMS = 0.† WORMS = 1–6.‡ Corrected for age, sex, BMI, history of knee injury or surgery, family history of knee replacement, and Herbeden nodes in hands by using multiple linear regression analysis.§ Data are numbers of subjects, with percentages in parentheses.|| Data are means 6 standard deviations.
Table 5
Prevalence of Knee Abnormalities by Activity Level
LesionLow-Activity Group (n = 60)*
High-Activity Group (n = 60)† P Value‡
Meniscus 19 (31.7) 35 (58.3) .0018Ligament 9 (15.0) 19 (31.7) .0111Cartilage WORMS . 0 39 (65.0) 56 (93.3) , .001 WORMS . 1 27 (45.0) 38 (63.3) .0180Bone marrow edema 17 (28.3) 34 (56.7) , .001Articular surface depression 0 (0) 0 (0) …Subarticular cyst 3 (5.0) 4 (6.7) .3447Osteophyte 19 (31.7) 28 (46.7) .1727Joint effusion 3 (5.0) 29 (48.3) , .001Loose body 2 (3.3) 2 (3.3) .7685Popliteal cyst 15 (25.0) 16 (26.7) .8638
Note.—Unless otherwise specifi ed, data are numbers of subjects, with percentages in parentheses.
* PASE score: 0–199.† PASE score: 200–400.‡ Corrected for age, sex, BMI, history of knee injury or surgery, family history of knee replacement, and Herbeden nodes in hands
by using multiple linear regression analysis.
516 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
3.79; P = .0275). Comparing subjects with cartilage lesions between activity groups also showed signifi cantly differ-ent T2 values (49.72 msec 6 4.42 vs 47.0 msec 6 3.77; P = .0199) ( Table 7 ).
The coeffi cient of variation for T2 quantifi cation measurements was 1.17.
Discussion
The results of our study show that mid-dle-aged asymptomatic individuals with risk factors for knee OA from the OAI incidence cohort had a high prevalence of knee abnormalities, such as cartilage and meniscus lesions. A signifi cant cor-relation between patellar cartilage T2 values and the presence and severity of cartilage and meniscus lesions was found. Physically active individuals showed signifi cantly more cartilage and menis-cus abnormalities than did more seden-tary subjects; in addition, a signifi cant correlation between physical activity level and patella T2 values was also observed.
T2 relaxation time mapping is sensitive to a wide range of water in-teractions in tissue and, in particular, depends on the content, orientation, and anisotropy of collagen ( 34 ). This parameter was therefore included in the OAI MR protocol, which will allow thorough investigation of T2 in relation to prevalence and evolution of cartilage degeneration and OA. We focused on patellar cartilage T2 measurements as segmentation of the patella can be done in a reasonable amount of time with good precision such that larger sample sizes can be analyzed. Also, it has been shown ( 35 ) that the femoro-patellar joint may be particularly affected by weight-bearing physical activities. Patella cartilage differs from that of the tibiofemoral joint and exibits distinct biochemical and mechanical properties. Patella cartilage has been shown ( 36 ) to demonstrate more in vivo deformation than femoral and tibial cartilage with weight-bearing loaded activities. Varus-valgus knee alignment also appears to differ according to which knee com-partment is affected by OA. Varus knee malalignment typically accompanies a loss of joint space in medial tibiofemoral
identifi ed subgroups in the high- and low-activity groups. In the low-activity group, 27 of 59 subjects had cartilage lesions. These subjects had signifi cantly higher T2 values than did subjects with-out cartilage lesions (47.0 msec 6 3.77 vs 44.7 msec 6 3.79; P = .0361). In the high-activity group, 38 of 60 subjects demonstrated cartilage lesions. These subjects also had higher T2 values than did those without lesions (49.72 msec 6 4.42 vs 47 msec 6 3.72; P = .0426). Among subjects without cartilage le-sions, we also compared the high- and low-activity groups and found that the high-activity group had higher T2 val-ues (47.0 msec 6 3.72 vs 44.7 msec 6
patellar cartilage T2 values and the PASE score ( P , .001), WORMS and Recht score of the patella cartilage ( P , .001), WORMS and Recht carti-lage summation score of the entire knee ( P , .001), and joint effusion ( P , .001).
In a multiregression model (adjusted for sex, age, BMI, and OA risk factors) for correlation of T2 values and carti-lage lesions (WORMS) versus PASE scores, both parameters independently contributed (T2: P = .0035; cartilage WORMS: P = .0022) to the correlation with PASE scores.
On the basis of presence of car-tilage lesions in the entire knee (any subregion with a WORMS . 1), we
Table 6
Patient Characteristics by Activity Level
CharacteristicLow-Activity Group (n = 60)*
High-Activity Group (n = 60)† P Value‡
Kellgren-Lawrence score 0.1 6 0.34 0.5 6 0.72 .0013 0§ 52 35 1§ 8 21 2§ 0 2 3§ 0 2KOOS 94.94 6 9.51 93.08 6 9.18 .4153400-m walk (sec) 279.3 6 34.03 266.86 6 26.86 .156Maximum force Flexion (N)‡ 175 6 69.89 163.12 6 60.03 .9308 Extension (N)‡ 393.3 6 133.07 415.65 6 101.4 .069Patellar T2 (msec) 45.8 6 3.93 48.7 6 4.35 , .001Cartilage WORMS Summation 2.5 6 3.34 6.3 6 5.45 , .001 Maximum 1.6 6 1.59 2.8 6 1.85 , .001Recht cartilage score Summation 2.3 6 2.95 5.5 6 4.37 , .001 Maximum 1.38 6 1.33 2.4 6 1.39 , .001Summation WORMS Meniscus 0.78 6 1.54 2.4 6 3.4 .001 Ligament 0.3 6 0.90 0.87 6 1.48 .0135 Bone marrow edema 0.88 6 1.69 1.5 6 1.9 .0497 Articular surface depression 0 0 Subarticular cyst 0.14 6 0.07 0.08 6 0.06 .7202 Osteophyte 1.5 6 3.44 4.0 6 7.23 .0305 Joint effusion 0.08 6 0.38 0.85 6 1.02 , .001 Loose body 0.05 6 0.29 0.03 6 0.18 .8524 Popliteal cyst 0.42 6 0.79 0.41 6 0.77 .7631
Note.—Unless otherwise specifi ed, data are means 6 standard deviations.
* PASE score: 0–199.† PASE score: 200–400.‡ Corrected for age, sex, BMI, history of knee injury or surgery, family history of knee replacement, and Herbeden nodes in hands
by using multiple linear regression analysis.§ Data are numbers of subjects.

Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 517
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
that risk increases with intensity and duration of activity.
A number of studies have examined the infl uence of age on the risk of de-veloping knee OA in physically active individuals. Most of these investigators examined individuals in a specifi c stage of the lifespan. A lower prevalence of OA has been reported ( 50 ) in middle-aged (range, 48–60 years) physically active teachers as compared with con-trol subjects. In contrast to these re-sults, McAlindon et al ( 51 ) examined
ous studies ( 44–48 ) have shown simi-lar results in smaller populations and younger subjects with higher physical activity levels. Stahl et al ( 29 ) examined 10 marathon runners and 12 physically active asymptomatic subjects. They also found a high prevalence of carti-lage abnormalities in the marathon run-ners (60%) and active control subjects (50%). Vignon et al ( 49 ) stated in their review that the activities of daily life, as well as sports and recreational activi-ties, are risk factors for knee OA and
joint OA. Patella malalignment within the femoral trochlea is commonly ex-hibited by patients with patellafemoral joint OA ( 37 ).
Multiple risk factors have been linked to OA in epidemiologic studies ( 38–40 ), including age, female sex, obe-sity, sports activities, previous injury, proprioceptive defi cits, and genetic el-ements. Knowledge of the relationship of physical activity and the evolution of OA is limited, as researchers ( 39,41–43 ) investigating the effect of physical activity on weight-bearing joints have reported confl icting results. Investiga-tors in a number of studies ( 12–16 ) examined OA risk factors in relation to quantitative and qualitative carti-lage loss determined with MR imaging. However, there is a paucity of data ana-lyzing cartilage degeneration by using MR imaging in relation to physical ac-tivity. Therefore, the aim of out study was to assess the prevalence of carti-lage, meniscal, and ligamentous dam-age; bone marrow edema; and cartilage T2 in relatively healthy young subjects from the incidence cohort of the OAI who had no pain and either high or low levels of physical activity. We focused on younger subjects because they could potentially best benefi t from preven-tive intervention. Researchers in previ-
Figure 2
Figure 2: Color-coded T2 maps overlaid on fi rst-echo MR images obtained with multiecho SE sequence show (a) low patellar T2 values in a sedentary patient and (b) high patellar T2 values in an active patient of the same age.
Figure 3
Figure 3: Mean patellar T2 values in subjects in low-activity (left, 1) and high-activity (right, 2) PASE groups (P , .001). Signifi cance was determined by using a multivariate regression model. P value refl ects a test of dependent T2 variable by ordinal PASE variable adjusted for sex, age, BMI, and OA risk factors.
Table 7
Mean T2 Values by Activity Level and Presence of Cartilage Lesions
No. of Subjects Mean T2 (msec) P Value*
Low-activity group 59† 45.8 6 3.93 .0361‡
No cartilage lesions 32 44.7 6 3.79 Cartilage lesions§ 27 47.0 6 3.77High-activity group 60 48.7 6 4.35 .0426||
No cartilage lesions 22 47.0 6 3.72 .0275#
Cartilage lesions§ 38 49.7 6 4.42 .0199**
* Corrected for age, sex, BMI, history of knee injury or surgery, family history of knee replacement, and Herbeden nodes in hands by using multiple linear regression analysis.† Owing to MR artifacts, one low-activity male subject was excluded from T2 analysis.‡ In low-activity group, subjects with vs those without cartilage lesions.§ Defi ned as WORMS . 1.|| In high-activity group, subjects with vs those without cartilage lesions.# Versus subjects in low-activity group without cartilage lesions.
** Versus subjects in low-activity group with cartilage lesions.

518 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
biochemical composition of cartilage. Unfortunately, the OAI protocol only includes a T2 mapping sequence. Prom-ising new techniques like T1 r and de-layed gadolinium-enhanced MR imaging of cartilage, or dGEMRIC, ( 10 ) are not available. The advantage of T1 r and T2 measurements is that these techniques are noninvasive and do not require spe-cial preparation (eg, administration of contrast agent in dGEMRIC). Stahl et al ( 35 ) pointed out that T1 r is well suited to differentiate healthy subjects and early OA patients and is more sensitive than T2 relaxation times.
Another limitation of our study was that, although images were scored sepa-rately, a consensus reading was per-formed if scores were not identical. A separate reading for both observers and a comparison of the results might be bet-ter. We also performed a reproducibility measurement for 12 subjects and calcu-lated the inter- and intraobserver agree-ments only for the WORMS cartilage score. Further, the WORMS does not in-clude the patella tendon. To include the patella in our scoring system, we defi ned patella tendinosis as a grade 2 sprain and added the score to the WORMS summation for ligaments. The PASE is intended for the elderly, but it has been validated for subjects with mean ages of 52 (standard deviation, 16) ( 20 ), 54 (range, 30–68 years) ( 21 ), and 56 (range, 37–73 years) ( 22 ) years.
In conclusion, our fi ndings show that middle-aged asymptomatic individuals with knee OA risk factors have a high prevalence of knee abnormalities on MR images, particularly cartilage and meniscus lesions. Physically active indi-viduals showed signifi cantly more car-tilage and meniscus abnormalities and higher patellar T2 values. Our results indicate that T2 relaxation time at the patella may be a marker for internal joint derangement in terms of cartilage and meniscal lesions.
References 1 . Lane NE , Thompson JM . Management of
osteoarthritis in the primary-care setting: an evidence-based approach to treatment . Am J Med 1997 ; 103 : 25S – 30S .
lesions based on the WORMS and Recht scores. Stahl et al ( 34 ) showed, in a small sample, that T2 relaxation times were signifi cantly higher in the tibiofemoral cartilage of patients with early knee OA compared with healthy controls, allowing differentiation of patients with disease from those without. In another study with asymptomatic physically active and sedentary subjects, Stahl et al ( 35 ) found that T1 r and T2 relaxation times were not different between younger active sub-jects and sedentary controls; however, a signifi cant difference in these param-eters in active subjects with and those without cartilage defects was found. In contrast to their results, we found a sig-nifi cant correlation between physical ac-tivity level and T2 values. Interestingly, we also found an association between T2 and prevalent cartilage lesions, and this association was present in both ac-tivity groups. When cartilage lesions are present, T2 is elevated. On the basis of these fi ndings, we hypothesize that T2 is a measure of cartilage quality and that subjects who develop cartilage lesions during physical activity have a higher T2. Since we included only subjects without pain in our analysis, we conclude that these fi ndings may indicate that higher T2 values are associated with higher risk for development of morphologic cartilage lesions. It is also possible that, during the process of focal cartilage lesion develop-ment, substances are released into the synovial fl uid that serve as mediators and initiate cartilage breakdown in areas that are not visually affected by OA. Further longitudinal studies are necessary to de-termine the role of T2 measurements in the evolution of OA.
A limitation of our study was that we only obtained T2 values of the pa-tella. However, cartilage segmentation is a time-consuming process, which may take up to 4 hours for one knee. Our goal was establish a more feasible and faster technique that would also potentially allow clinical application of T2 quantifi cation in the future. Future studies, however, will have to show whether patella T2 may be used as a surrogate measure for whole knee car-tilage T2. Another limitation is that we only used T2 mapping for assessing
the level of physical activity and the risk of radiographic and symptomatic knee OA in an elderly population of the Framingham Study. They found that heavy physical activity is an important risk factor for the development of knee OA in elderly patients. These investiga-tors, however, based their diagnosis on radiographs, which unfortunately show advanced disease stages, limiting pos-sible preventive measures. Findings in several studies ( 52,53 ) have shown the age dependency of cartilage T2 maps. Mosher et al indicated in studies of asymptomatic male and female volun-teers that aging is associated with an increase in T2 of articular cartilage. We only examined middle-aged individuals and did not fi nd a correlation between age and T2 values or age and cartilage lesions in our small age range.
A small number of studies have used MR imaging to assess the relationship between physical activity and knee joint structure. Stahl et al ( 35 ) examined the relationship in a smaller cohort than we did. Physically active subjects (mean age, 33 years) had a high prevalence of focal cartilage abnormalities. In some studies ( 54–56 ), the most frequent fi nd-ings in physically active subjects were abnormalities in meniscal signal inten-sity or tears (13%–50%), bone marrow edema (up to 41%), or joint effusion (up to 35%). Two studies performed at 1.5 T also found cartilage lesions: Kaplan et al ( 56 ) examined both knees of 20 basketball players. In 47.5% of the knees, articular cartilage lesions were detected. Most of them were seen at the patella (35%) or trochlea (25%). Ma-jor and Helms ( 55 ) performed a study with 17 varsity basketball players; eight (24%) of the 34 knees had abnormal signal intensity in the patellar and tro-chlear cartilage, and six (18%) had focal cartilage lesions. These studies clearly show that high-level physical activity in young and middle-aged individuals is as-sociated with cartilage lesions. In our study, lesions were found with a higher prevalence, which is most likely related to differences in age between studies.
We also found a signifi cant correla-tion between patella cartilage T2 values and the severity of cartilage and meniscus

Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 519
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
28 . Peterfy CG , Gold G , Eckstein F , Cicuttini F , Dardzinski B , Stevens R . MRI protocols for whole-organ assessment of the knee in osteoarthritis. Osteoarthritis Cartilage 2006 ;14(suppl A):A95–A111.
29 . Stahl R , Luke A , Ma CB , et al . Prevalence of pathologic fi ndings in asymptomatic knees of marathon runners before and after a competition in comparison with physically active subjects: a 3.0 T magnetic resonance imaging study . Skeletal Radiol 2008 ; 37 : 627 – 638 .
30 . Peterfy CG , Guermazi A , Zaim S , et al . Whole-Organ Magnetic Resonance Imag-ing Score (WORMS) of the knee in osteo-arthritis . Osteoarthritis Cartilage 2004 ; 12 : 177 – 190 .
31 . Recht MP , Piraino DW , Paletta GA , Schils JP , Belhobek GH . Accuracy of fat-suppressed three-dimensional spoiled gradient-echo FLASH MR imaging in the detection of patel-lofemoral articular cartilage abnormalities . Radiology 1996 ; 198 : 209 – 212 .
32 . Noyes FR , Stabler CL . A system for grad-ing articular cartilage lesions at arthros-copy . Am J Sports Med 1989 ; 17 : 505 – 513 .
33 . Gluer CC , Blake G , Lu Y , Blunt BA , Jergas M , Genant HK . Accurate assessment of preci-sion errors: how to measure the reproduc-ibility of bone densitometry techniques . Osteoporos Int 1995 ; 5 : 262 – 270 .
34 . Stahl R , Blumenkrantz G , Carballido-Gamio J , et al . MRI-derived T2 relaxation times and cartilage morphometry of the tibio-femoral joint in subjects with and without osteoarthritis during a 1-year follow-up . Osteoarthritis Cartilage 2007 ; 15 : 1225 – 1234 .
35 . Stahl R , Luke A , Li X , et al. T1rho, T(2) and focal knee cartilage abnormalities in physi-cally active and sedentary healthy subjects versus early OA patients: a 3.0-Tesla MRI study. Eur Radiol 2009;19(1):132–143.
36 . Eckstein F , Lemberger B , Gratzke C , et al . In vivo cartilage deformation after differ-ent types of activity and its dependence on physical training status . Ann Rheum Dis 2005 ; 64 : 291 – 295 .
37 . Hinman RS , Crossley KM . Patellofemoral joint osteoarthritis: an important subgroup of knee osteoarthritis . Rheumatology (Ox-ford) 2007 ; 46 : 1057 – 1062 .
38 . Felson DT . An update on the pathogenesis and epidemiology of osteoarthritis . Radiol Clin North Am 2004 ; 42 : 1 – 9 .
39 . Urquhart DM , Soufan C , Teichtahl AJ , Wluka AE , Hanna F , Cicuttini FM . Factors that may mediate the relationship between physical activity and the risk for developing
erative changes in osteoarthritis . NMR Biomed 2006 ; 19 : 822 – 854 .
16 . Felson DT , Zhang Y , Hannan MT , et al . The incidence and natural history of knee osteoarthritis in the elderly: the Framing-ham Osteoarthritis Study . Arthritis Rheum 1995 ; 38 : 1500 – 1505 .
17 . Bellamy N , Buchanan WW , Goldsmith CH , Campbell J , Stitt LW . Validation study of WOMAC: a health status instrument for measuring clinically important patient rele-vant outcomes to antirheumatic drug thera-py in patients with osteoarthritis of the hip or knee . J Rheumatol 1988 ; 15 : 1833 – 1840 .
18 . Bellamy N . The WOMAC Knee and Hip Osteoarthritis Indices: development, vali-dation, globalization and infl uence on the development of the AUSCAN Hand Os-teoarthritis Indices . Clin Exp Rheumatol 2005 ; 23 : S148 – S153 .
19 . Washburn RA , Smith KW , Jette AM , Janney CA . The Physical Activity Scale for the Elderly (PASE): development and evalu-ation . J Clin Epidemiol 1993 ; 46 : 153 – 162 .
20 . Johansen KL , Painter P , Kent-Braun JA , et al . Validation of questionnaires to es-timate physical activity and functioning in end-stage renal disease . Kidney Int 2001 ; 59 : 1121 – 1127 .
21 . Stibrant Sunnerhagen K . Circuit training in community-living “younger” men after stroke . J Stroke Cerebrovasc Dis 2007 ; 16 : 122 – 129 .
22 . Willen C , Grimby G . Pain, physical activ-ity, and disability in individuals with late effects of polio . Arch Phys Med Rehabil 1998 ; 79 : 915 – 919 .
23 . Roos EM , Lohmander LS . The Knee in-jury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthri-tis . Health Qual Life Outcomes 2003 ; 1 : 64 .
24 . Simonsick EM , Montgomery PS , Newman AB , Bauer DC , Harris T . Measuring fi tness in healthy older adults: the Health ABC Long Distance Corridor Walk . J Am Geriatr Soc 2001 ; 49 : 1544 – 1548 .
25 . Rantanen T , Era P , Heikkinen E . Physical activity and the changes in maximal iso-metric strength in men and women from the age of 75 to 80 years . J Am Geriatr Soc 1997 ; 45 : 1439 – 1445 .
26 . Kellgren JH , Lawrence JS . Radiological as-sessment of osteoarthritis . Ann Rheum Dis 1957 ; 16 : 494 – 501 .
27 . Peterfy CG , Schneider E , Nevitt M . The os-teoarthritis initiative: report on the design rationale for the magnetic resonance im-aging protocol for the knee . Osteoarthritis Cartilage 2008;16:1433–1441.
2 . Lawrence RC , Felson DT , Helmick CG , et al . Estimates of the prevalence of ar-thritis and other rheumatic conditions in the United States. II . Arthritis Rheum 2008 ; 58 : 26 – 35 .
3 . Mankin HJ , Brandt KD . Pathogenesis of ar-thritis . In: Kelley WN, Harris ED Jr, Ruddy S, Clement B. Textbook of rheumatology , 4th ed. Philadelphia, Pa : Saunders , 1993 .
4 . Liess C , Lusse S , Karger N , Heller M , Gluer CC . Detection of changes in cartilage wa-ter content using MRI T2-mapping in vivo . Osteoarthritis Cartilage 2002 ; 10 : 907 – 913 .
5 . Burstein D , Gray M . New MRI techniques for imaging cartilage . J Bone Joint Surg Am 2003 ; 85-A ( suppl 2 ): 70 – 77 .
6 . Link TM , Steinbach LS , Ghosh S , et al . Os-teoarthritis: MR imaging fi ndings in differ-ent stages of disease and correlation with clinical fi ndings . Radiology 2003 ; 226 : 373 – 381 .
7 . Eckstein F , Heudorfer L , Faber SC , Burg-kart R , Englmeier KH , Reiser M . Long-term and resegmentation precision of quantitative cartilage MR imaging (qMRI) . Osteoarthritis Cartilage 2002 ; 10 : 922 – 928 .
8 . Eckstein F , Tieschky M , Faber SC , et al . Effect of physical exercise on cartilage vol-ume and thickness in vivo: MR imaging study . Radiology 1998 ; 207 : 243 – 248 .
9 . Dunn TC , Lu Y , Jin H , Ries MD , Majumdar S . T2 relaxation time of cartilage at MR im-aging: comparison with severity of knee os-teoarthritis . Radiology 2004 ; 232 : 592 – 598 .
10 . Link TM , Stahl R , Woertler K . Cartilage imaging: motivation, techniques, current and future signifi cance . Eur Radiol 2007 ; 17 : 1135 – 1146 .
11 . Mosher TJ , Dardzinski BJ . Cartilage MRI T2 relaxation time mapping: overview and applications . Semin Musculoskelet Radiol 2004 ; 8 : 355 – 368 .
12 . Sharma L , Eckstein F , Song J , et al . Relation-ship of meniscal damage, meniscal extrusion, malalignment, and joint laxity to subsequent cartilage loss in osteoarthritic knees . Arthri-tis Rheum 2008 ; 58 : 1716 – 1726 .
13 . Ding C , Martel-Pelletier J , Pelletier JP , et al . Meniscal tear as an osteoarthritis risk factor in a largely non-osteoarthritic cohort: a cross-sectional study . J Rheuma-tol 2007 ; 34 : 776 – 784 .
14 . Felson DT . Relation of obesity and of vo-cational and avocational risk factors to osteoarthritis . J Rheumatol 2005 ; 32 : 1133 – 1135 .
15 . Eckstein F , Burstein D , Link TM . Quanti-tative MRI of cartilage and bone: degen-

520 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
MUSCULOSKELETAL IMAGING: Patellar Cartilage: Abnormalities and T2 Values versus Physical Activity Stehling et al
knee osteoarthritis . Arthritis Res Ther 2008 ; 10 : 203 .
40 . Dekker J , van Dijk GM , Veenhof C . Risk factors for functional decline in osteoar-thritis of the hip or knee . Curr Opin Rheu-matol , 2009;21(5):520–524.
41 . Szoeke C , Dennerstein L , Guthrie J , Clark M , Cicuttini F . The relationship be-tween prospectively assessed body weight and physical activity and prevalence of radiological knee osteoarthritis in post-menopausal women . J Rheumatol 2006 ; 33 : 1835 – 1840 .
42 . Chakravarty EF , Hubert HB , Lingala VB , Zatarain E , Fries JF . Long distance run-ning and knee osteoarthritis: a prospec-tive study . Am J Prev Med 2008 ; 35 : 133 – 138 .
43 . Racunica TL , Teichtahl AJ , Wang Y , et al . Effect of physical activity on articular knee joint structures in community-based adults . Arthritis Rheum 2007 ; 57 : 1261 – 1268 .
44 . Beattie KA , Boulos P , Pui M , et al . Abnor-malities identifi ed in the knees of asymp-tomatic volunteers using peripheral mag-netic resonance imaging . Osteoarthritis Cartilage 2005 ; 13 : 181 – 186 .
45 . Boks SS , Vroegindeweij D , Koes BW , Hunink MM , Bierma-Zeinstra SM . Magnetic resonance imaging abnormalities in symp-tomatic and contralateral knees: prevalence
and associations with traumatic history in general practice . Am J Sports Med 2006 ; 34 : 1984 – 1991 .
46 . Zanetti M , Pfi rrmann CW , Schmid MR , Romero J , Seifert B , Hodler J . Patients with suspected meniscal tears: prevalence of abnormalities seen on MRI of 100 symp-tomatic and 100 contralateral asymptom-atic knees . AJR Am J Roentgenol 2003 ; 181 : 635 – 641 .
47 . Hill CL , Gale DR , Chaisson CE , et al . Peri-articular lesions detected on magnetic res-onance imaging: prevalence in knees with and without symptoms . Arthritis Rheum 2003 ; 48 : 2836 – 2844 .
48 . Tschirch FT , Schmid MR , Pfi rrmann CW , Romero J , Hodler J , Zanetti M . Prevalence and size of meniscal cysts, ganglionic cysts, synovial cysts of the popliteal space, fl uid-fi lled bursae, and other fl uid collections in asymptomatic knees on MR imaging . AJR Am J Roentgenol 2003 ; 180 : 1431 – 1436 .
49 . Vignon E , Valat JP , Rossignol M , et al . Osteoarthritis of the knee and hip and activity: a systematic international review and synthesis (OASIS) . Joint Bone Spine 2006 ; 73 : 442 – 455 .
50 . White JA , Wright V , Hudson AM . Rela-tionships between habitual physical activity and osteoarthrosis in ageing women . Pub-lic Health 1993 ; 107 : 459 – 470 .
51 . McAlindon TE , Wilson PW , Aliabadi P , Weissman B , Felson DT . Level of physical activity and the risk of radiographic and symptomatic knee osteoarthritis in the el-derly: the Framingham study . Am J Med 1999 ; 106 : 151 – 157 .
52 . Mosher TJ , Dardzinski BJ , Smith MB . Human articular cartilage: infl uence of aging and early symptomatic degeneration on the spatial variation of T2–preliminary fi ndings at 3 T . Radiology 2000 ; 214 : 259 – 266 .
53 . Mosher TJ , Liu Y , Yang QX , et al . Age dependency of cartilage magnetic resonance imaging T2 relaxation times in asymptomatic women . Arthritis Rheum 2004 ; 50 : 2820 – 2828 .
54 . Ludman CN , Hough DO , Cooper TG , Gottschalk A . Silent meniscal abnormali-ties in athletes: magnetic resonance imag-ing of asymptomatic competitive gymnasts . Br J Sports Med 1999 ; 33 : 414 – 416 .
55 . Major NM , Helms CA . MR imaging of the knee: fi ndings in asymptomatic collegiate basketball players . AJR Am J Roentgenol 2002 ; 179 : 641 – 644 .
56 . Kaplan LD , Schurhoff MR , Selesnick H , Thorpe M , Uribe JW . Magnetic resonance imaging of the knee in asymptomatic pro-fessional basketball players . Arthroscopy 2005 ; 21 : 557 – 561 .




















