
Disparities in psychological, neuroendocrine, and immunologic patterns in asymptomatic HIV1...
19
BIOL PSYCHIATRY 1023 1991;29:1023-1041 Disparities in Psychological, Neuroendocrine, and Immunologic Patterns in Asymptomatic HIV-1 Seropositive and Seronegative Gay Men Michael H. Antoni, Neil Schneidermao, Nancy Klimas, Arthur LaPerriere, Gail Ironson, and Mary Ann Fletcher The present study concurrently measured psychological distress (state anxiety, depression, confusion, and intrusive thoughts), neuroendocrine (plasma cortisol concentrations), and immunologic [lymphocyte proliferative responses to phytohemagglutinin (PHA ) and poke- weed mitogen (PWM)] changes in the 5-week periods preceding and following serostatus notification among asymptomatic Human lmmunodeficienc 3" Viras-type 1 (HIV-1) sero- positive and seronegative gay men. Seropositives, as opposed to seronegatives, showed a disparity in predicted relationships among aTstres~., cortisol, and immunologic measures across the prenotification to postnotification period. Individual difference analyses su,f- gested that among seropositives, in contrast to seronegatives, plasma cortisol concen- trations were negatively correlated with psychological distress and positively correlated with responses to PHA (assessed at study entry and after serestatus notification). This pattern in seropositives could not be explained by differences in prenotification perceived risk of infectivity, extraneous environmental stressors, or CD4 cell counts within the seropositive group. Introduction There is much current interest in applying a psychoneuroimmunologic framework to the study of immunological and psychological sequelae of the Human lmmunodeficiency Virus--type 1 (HIV-1) infection (Antoni et al 1990a; Glaser and Kiecoit-Gl:~ser 1987; Kiecolt-Glaser and Glaser 1988; Solomon 1987; Solomon and Temoshok 1987). In one commonly employed psychoimmunologic paradigm, immune functioning (e.g., lympho- cyte proliferative responses to mitogen challenge; natural killer cell cytotexic response to tumor targets) is assessed concurrently or before and after healthy individuals have experienced psychosocial stressors such as medical school or licensing examinations (Halvorsen and Vassend 1987; Kiecolt-Glaser et al 1984; Workman and LaVia 1987), death of a spouse (Irwin et al 1987), or nearby nuclear reactor accidents (McKmnon et From the ~ t of Psychology {MHA. NS, AL GI), ~e Depemr.,em of Med~cir~ ~,~¢. ,~K, MAP). the Depe, mm~ of Psychiatry (NS, AL. GIL Umver~ity of Mi~, Coral ~ . FL: ~ the ~ for 6~ Btop* ycl'm.t~'~d Sttmty of AID'~, Miami, L~L. Address reprint requests to Dr. MiclmelH~ . , ~ m , ~ | of Psyt.~gy, P.O~ Box 2 ~ !8,5 Umv~lt) of Mir,~. Co~ Gables, FL 33124~ Re,.~lved June 2, 1990, revised September 2t. 1990. © 1991 S~ie~y of Biological Psycbiawy O006-3~3~ltSG3..f)O
Transcript of Disparities in psychological, neuroendocrine, and immunologic patterns in asymptomatic HIV1...

BIOL PSYCHIATRY 1023 1991;29:1023-1041
Disparities in Psychological, Neuroendocrine, and Immunologic Patterns in Asymptomatic HIV-1 Seropositive and Seronegative Gay Men
Michael H. Antoni, Neil Schneidermao, Nancy Klimas,
Arthur LaPerriere, Gail Ironson, and Mary Ann Fletcher
The present study concurrently measured psychological distress (state anxiety, depression, confusion, and intrusive thoughts), neuroendocrine (plasma cortisol concentrations), and immunologic [lymphocyte proliferative responses to phytohemagglutinin ( PHA ) and poke- weed mitogen (PWM)] changes in the 5-week periods preceding and following serostatus notification among asymptomatic Human lmmunodeficienc 3" Viras-type 1 (HIV-1) sero- positive and seronegative gay men. Seropositives, as opposed to seronegatives, showed a disparity in predicted relationships among aTstres~., cortisol, and immunologic measures across the prenotification to postnotification period. Individual difference analyses su,f- gested that among seropositives, in contrast to seronegatives, plasma cortisol concen- trations were negatively correlated with psychological distress and positively correlated with responses to PHA (assessed at study entry and after serestatus notification). This pattern in seropositives could not be explained by differences in prenotification perceived risk of infectivity, extraneous environmental stressors, or CD4 cell counts within the seropositive group.
Int roduct ion
There is much current interest in applying a psychoneuroimmunologic framework to the study of immunological and psychological sequelae of the Human lmmunodeficiency Virus--type 1 (HIV-1) infection (Antoni et al 1990a; Glaser and Kiecoit-Gl:~ser 1987; Kiecolt-Glaser and Glaser 1988; Solomon 1987; Solomon and Temoshok 1987). In one commonly employed psychoimmunologic paradigm, immune functioning (e.g., lympho- cyte proliferative responses to mitogen challenge; natural killer cell cytotexic response to tumor targets) is assessed concurrently or before and after healthy individuals have experienced psychosocial stressors such as medical school or licensing examinations (Halvorsen and Vassend 1987; Kiecolt-Glaser et al 1984; Workman and LaVia 1987), death of a spouse (Irwin et al 1987), or nearby nuclear reactor accidents (McKmnon et
From the ~ t of Psychology {MHA. NS, AL GI), ~e Depemr.,em of Med~cir~ ~,~¢. ,~K, MAP). the Depe, m m~ of Psychiatry (NS, AL. GIL Umver~ity of M i ~ , Coral ~ . FL: ~ the ~ for 6~ Btop* ycl'm.t~'~d Sttmty of AID'~, Miami, L~L.
Address reprint requests to Dr. Miclmel H~ . , ~ m , ~ | of Psyt .~gy, P.O~ Box 2~ ! 8,5 Umv~lt) of Mir,~. C o ~ Gables, FL 33124~
Re,.~lved June 2, 1990, revised September 2t. 1990.
© 1991 S~ie~y of Biological Psycbiawy O006-3~3~ltSG3..f)O

1024 BIOL PSYCHIATRY M.H. Antoni et al 1991;29:1023-1041
al 1989). Alternatively, investigators have attempted to relate pathological distress states (e.g., major depressive disorder; Calabrese et al 1987; Schleifer et al 1984) or individual differences in the severity of distress responses (e.g., depressive symptoms; Irwin et al 1987; degree of intrusive thoughts about a stressor, Workman and LaVia 1987) to mitogen responsivity. Although some inconsistencies have emerged in t_his literature, a large number of studies have suggested that environmental stressors or affective states char- acterized by a perceived loss of personal control may have immunosuppressive effects (see Antoni et al 1990a for review).
Both animal (Laudenslager et al 1983; Pericic et al 1987) and human work (Antoni 1990b; Breier, et al 1987) has supported the case that stressors which decrease an or- ganism's sense of control may lead to a cascade of affective and neurt~ndocrine events with potential immunomodulatory properties. Indeed, it has been suggested that in un- predictable, uncontrollable, or unrelenting stressful situs,dons in which coping responses are unavailable or ineffective, a specific physiological response pattern--.hypothalamic- pituitary-adrenocortical (HPAC) activation--may predominate (McCabe and Schneider- man 1985). Activation of this axis is associated with elevations in corticotropin-releasing hormone (CRH), adrenocorticotropin hormone (ACTH) and cortisol, all of which have been shown to impair cellular immune functioning (Cupps and Fauci 1982; Kavelaars et al 1988; Pawlikowski et al 1988). Particularly intense or prolonged distress responses, by way of such neuroendocrine events, may therefore result in the suppression of important aspects of immune functioning. Despite the accumulation of psychoimmunologie and neuroimmunologic findings, very little work iJas assessed psychological distress, neu- roendocrine levels and irmnune functioning concurrently during periods preceding and following an acute life-threatening stressor such as a natural disaster or notification of a definitive medical diagnosis.
We have reported that in comparison with matched control subjects not awaiting HIV- 1 serostatus notification, seronegative gay men entering a protocol involving such noti- fication showed initially impaired proliferative responses to phytohemagglutinin (PHA) and pokeweed mitogen (PWM)---values that returned to the normal range 5 weeks later (Ironson et al 1990). These findings suggested that the decision to enter a study in which serostatus would be identified was operating as a potent acute stressor with immunological effects. Over this same 5-week period, individuals who were ultimately shown to be seroposifive displayed no such change in Lmmune functioning despite the fact that they evidenced a greater degre~ of distress than tbeir seronegative counterparts. Moreover we observed that while the seropositive group reported clinical levels of affective distress (anxiety and depression) and an increase in intrusive thoughts in response to antibody status notification, they showed virtually no change in mitogen responsivity prenotification to postnotification (lronson et al 1990).
To examine the disparity between psychological and immune responses evident in seropositive individuals, we assessed changes in psychological distress, plasma cortisol, and blastogenic responses to PHA and PWM preceding and following serostatus notifi- cation. We focused on the time points corresponding to entry into the study and the point of serostatus notification. We hypothesized that seropositives would differ significantly from seronegatives in plasma cortisol and mitogen response values at study entry. More- over, we predicted that seronegatives would show significant decrements in cortisol and psychological distress prenotification to postnotification whereas seropositives would show a dissociation between psychological distress and neuroendocrine markers over a similar
HIV-|: Psychology, Immunology, and Hormones BIOL PSYCHIATRY 1025 1991 ;29:1023-1041
period such that cortisol values would not increase in conjunction with large expected increases i~ not:fication-related psychological distress.
Me thods
Subjects
Seventy-one gay men who were ur,~vare of their t-/IV-I antibody status were recruited through newspaper advertisements, notices at gay community activities, and the Health Crisis Network (a gay men's information exchange center). All subjects were informed that they would be tested for and im'ormed of their HIV-I antibody status as part of the study.
To minimize error variance in psychological and physiological markers and to restrict alternative explanations of study findings, we employed strict exclusion criteria. A com- plete physical examination and medical history were performed before the commencement of the study; subjects were excluded for any of the following: (I) having been previously tested for and/or having a known diagnosis of HIV-I seropositivity, acquired immune deficiency syndrome (AIDS), or AIDS-related complex (ARC), (2) unexplained weight loss of > !0% or 15 Ib within the past 3 months, (3) mucocutaneous oral candidiasis, (4) lymphadenopathy other than inguinal or anterior cervical, (5) fever of unexplained origin, (6) unexplained night sweats or diarrhea, (7) herpes zoster within previous 3 months, (8) current drug or ethanol abuse, (9) use of anabolic steroids, (10) regular use of antihis- tamines, (11) being younger than 18 or older than 40 years, (12) participation in a regular aerobic exercise, meditation, or psychotherapy program, and (13) producing an estimated VO2,~_~ (an indicator of aerobic fitness) greater than 53 ml/kg/min if aged 18-29 years or 49 ml/kg/min if 30-39 years. As such our subjects were asymptomatic, healthy (though not aerobically trained) gay males who were members of one AIDS-risk group (i.e., h.~mosexuals) and therefore were likely to perceive themselves as potentially at risk for HIV-! seropositivity at study entry.
Procedure
Interestea subjects who satisfied the study criteria completed ~. informed consent and were entered into the study. Immunologic, neuroendocrine~ an~ psychological distress measu~s were obtained st baseline frO, 5 weeks later and 72 b.r before serostatus notification (T2), as well as 1 week (T3), 2 weeks (T4), 3 weeks ('is), and 5 weeks (I"6) posttesting. Blood was drawn for the HIV- 1 antibody test at T2 and subjects were informed of their serostatus 3 days later (time of notification), at which time they received counseling and were administered an anxiety questionnaire.
Control Measures
At baseline and T6 subjects were given a short q u e s t i ~ to check for potential immunomodulatory confounds such as antihistamine eonsuraption, drug or alcohol abuse, being sick, sleep loss, high-risk sexual behavior frequency, and vigorous physical activity levels. We also determined serum albumin levels and aerobic fitness capacity (using a predicted V O ~ procedure; Fox 1973) at each time point to control for any changes ha

1026 BIOL PSYCHIATRY M.H. Antoni et al 199t ;29:1023-10t, ~
broad nutritional status and htuess levels, respectively. At baseline all subjects completed the Life Experience Survey (LES, Saragon et al 1978)--an inventory that assesses self- reported life events experienced in the preceding 6-month period.
Blood Samples In order to control for diurnal variations, all blood samples were collected from fasting subjects between 7:30 AM and 10:30 AM. Peripheral venom, s blood samples were obtained from each subject in heparin tubes (Vacut.~ner-sodium Heparin, Becton-Dickinson, Ruth- erford, N J). Because heparinized blood specimens are not optimally counted with au- tomated hematology cell counters, a separate blood sample in ethylenediaminetetraacetic acid (EDTA) was collected on each subject with each heparinized specimen. These EDYA samples were used for complete blood counts (CBC) and plasma. Whole blood samples were held for no longer than 4 hr at room temperature before functional assay procedures (: 1etcher et a11987). For plasma, red cells and white cells were spun down in a refrigerated centrifuge. For serum samples, peripheral venous blood was collected in red top tubes (Vacutainer, Becton-Dickinson, Rutherford, N J) and allowed to clot at 23°C for 30 min. The serum was separated from the clot in a refrigerated centrifuge. Both serum and plasma samples were stored at -70°C until use.
Immunological and Neuroendocrine Measures
Lymphocyte Phenotypes. Helper/inducer (CD4) and suppressor/cytotoxic (CD8) cell counts we~ determined by two-color direct immunofluorescence using a whole blood staining technique and flow cytometric procedures that we have described in detail else- where (lronson et al 1990). These flow cytometry methods have been standardized with those of six other national centers under the auspices of the Transfusion Safety Study (Fletcher et al 1989).
Lymphocyte Proliferation Assays. Lymphocyte proliferation to mitogen stimulation was measured using a whole blood procedure (Fletcher et al 1987). Our laboratory has previously determined relative comparability of whole blood assays to separated cell assays and determined that these assays are highly useful in the lymphopenic antiHIV-I positive patient and may produce results more indicative of in vivo conditions (Fletcher et a! 1987; Baron et al 1985). Briefly, 100 iJ~! of diluted heparinized blood (1:5 with culture medium, CM) containing RPMI 1640, 100 units penicillin and 50 units strepto- mycin and 1 mMol/L glutamine (GIBCO, Grand Island, NY) was dispensed in triplicate to the wells of a U-bottom microtiter plate (Costar, Cambridge, MA). Mitogens were tested at the following levels to give final dilutions as follows: PHA (Wel'come Diag- nostics, Dartford, England) 10 ~g/ml and PWM (GIBCO, Chagrin Falls. OH) diluted 1:40. The mitogen concen~ations chosen reflect those levels that have been shown to provide optimum proliferative responses. In that our previous work has demonstrated that the optimum dose of PHA and PWM is similar among HIV-I infected indi-,iduals and healthy controls (Fletcher et al 1987), only a single concentration of each mitogen was tested. The details of these proliferation assay procedures are described in an earlier report (lronson et al 1990). Results were expressed as mean net counts per minute (cpm) incorporated. Mean of the net cpm was transformed to mean cpm/100,O00 lymphocytes.

HIV-!: Psychology, lmmunoIogy, and Hormones BIOL PSYCHIATRY 1027 J991;29:1023-1041
Viral Serology. HIV-1 antibody was measured using the ELISA method and Abbott reagents. Reactive samples were repeated and those that were doubly positive were confirmed by protein immunoblot, using HIV-I antigen from Hillcrest Laboratories (Cy- press, CA) and the methodology developed by the Centers for Disease Control. All subjects were informed of their antibody status on a face-to-face basis by a licensed clinical social worker using a standardized format for the communication of this infor- mation. Of the 71 men enrolled in this study, 25 were ultimately shown g-~ be HIV-I seropositiv~- and 46 were seronegative.
Plasma Cortisol. Cortisol levels were quantitated with a standard solid-phase radioim- munoassay procedure (Coat-A-Count, Diagnostic Products Corp.). Briefly, 25 I~1 of plasma was added to 1.0 ml of buffered 125I-labeled Cortisol (Diagnostic Products Corp., Los Angeles, CA) vortexed, and then incubated for 45 rain at 37°C. After thoroughly decanting, the samples were counted in a 1CN Micromedic gamma counter. Cortisol concentrations were determined from logit-log calibration curves supplied in ~dt form and these were expressed as nanograms per milliliter (ng,/ml). This procedure has demonstrated adequate intraassay [7.0% coefficient of variation (CV)], and ip.terassay (7.0 CV) reli- ability and the manufacturer reports sensitivity to 70 ng/ml ar.d no significant position effects in multiassay runs (Diagnostic Products Corp., Los Angeles, CA)
Psychological Distress Measures
Affective Distress. The state version of the State-Trait Anxiety Inventory (STAI; Spielberger et al 1970) was used as one index of anxiety in the present study. This 20- item self-report instrument is designed to measure the anxiety level of the respondent at the time of administration. Another ind-~.x of affective distress used in this study was the Profile of Mood States (POMS; MeNair et al 1981) a 65-item, pencil and paper, self- report test with subscales measuriee ~everal mood states experienced over the past week. The subscaies oi" interest in the present study were Tension-Anxiety, Depression-De- jection, and Confusion-Bewilderment. The POMS has been standardized on and designed for nonpsychiatric samples (McNair et al 1981) and was previously used in studies of affective functioning in AIDS populations (Donlou et ai i985; Levy et al 1989).
intrusive Thoughts. To assess the degree to which subjects experienced recurring thoughts related to the threat of AIDS in their lives, we administered the Impact of Events Scale (IES) (Horowitz et al 1979) at T1, T4, T5, and T6. The IES was originally designed to tap symptoms reflecting DSM-III-R criteria for posttraumatic stress disorder. This instrument yields a to~al impect score and two subscale scores. The intrusion subscale measures subjects' recent experiences of daydreams, unwanted images, and dreams as- sociated with a real or perceived stressor and the avoidance subscale reflects the recognized avoidance of certain ideas, feelings, and situations that are reminiscent of the stressor. Each subscale has demonsta'ated adequate internal consistency and test-retest reliability (Zilberg 1982), and has been employed in studies of chronic environmental stressors (Davidson and Baum 1986) and among persons with AIDS (Jacobsen et al 1988). In this study we asked subjects to endorse IES items in relation to the perceived threat of AIDS in their lives.

1028 BIOL PSYCHIATRY M.H. Antoni et al 19Q| ;29:1023-1041
Perceived Serostatus. Subjects were asked at study entry to respond to the item: "1 think my HIV-! test result will be positive or negative." This statement was embedded in the battery of questionnaires administered at I'~.
Statistical Analyses
The primary focus of the present study hypotheses was the examination of changes in several response measures over periods preceding and following serostatus notification. First we conducted several between serostatus group analyses to ascertain the equivalence of each group on sociodemographie and biobehavioral variables that might contribute systematically to psychological distress, neuroendocrine, or immunologic measures. We also analyzed between-group differences on each response measure at each time point. Due to the small sample size and violation of certain assumptions of parametric between- group tebts (e.g., homogeneit~ of v~,/ance) we decided to conduct nonparametfic between- group analyses (Mann-Whitney Ustatistic test). We conducted a series of repeated-mea- sures ANOVAs to asqess changes in psychological, neuroendocrine, and immunologic measures among seropositive~ across the T r T 6 observation period. Of specific interest were changes in these measures surrounding two "stressor" events. The first event, occurring at T,, involves the decision to enter the study and thereby agree to be observed for a 10-week period and tested for HIV-I antibodies. The second event, serostatus notification, involves the communication of life-threatening and life-changing informa- tion. In addition to assessing the significance of change across the 10*week observation period, we also correlated distress, cortisol, and immune markers at baseline and change (A) scores between several time points for each.
Resul ts
Demographic and Biobehavioral l~ormation
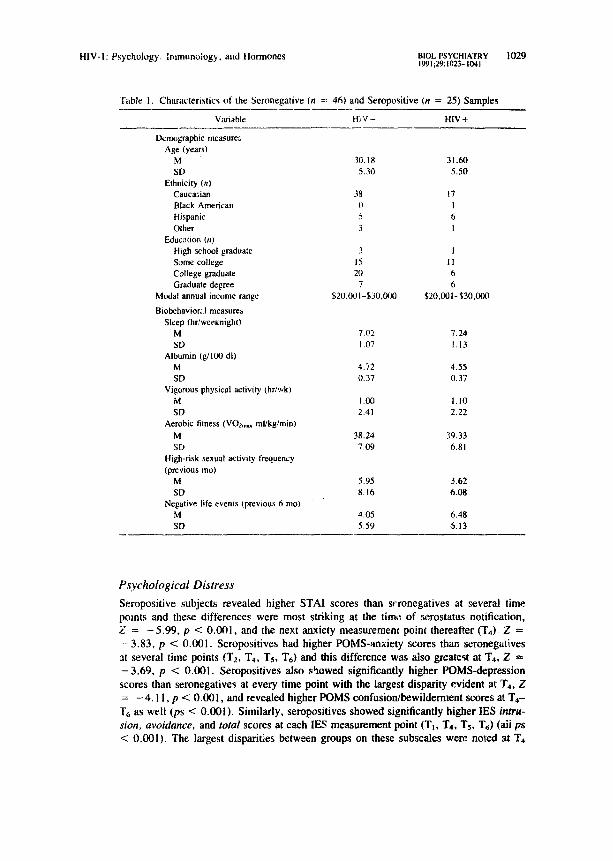
The demographic characteristics of the seropositive study subjects and the seronegative comparison group are displayed in Table 1. There were no significant differences in age, t = - 1.05, p > 0.10, nor ethnic group distribution, chi-squared (4) = 4.27, p > 0 .10 between these two groups. Further, the groups showed no difference in dis- tfioutions of educational experience, chi-squared (4) = 3.5, p > 0.10, annual income, chi-squared (6) = 5.17, p > 0.10, or sexual orientation, chi-squmed (3) = 1.79, p > 0.10, with most subjects classifying themselves as exclusively homosexual. In line with our previous work we assessed differences in environmental stressors (stress bur- den) between ~,~oups by comparing self-repe:;ed negative life events experienced in the previous t3 months (weighted by perceived impact) as measured by the LES. Results of this comparison suggested that subjects, overall, experienced few major aversive events in the recent 6-month period and showed no s:gnificant between-group differ- ences on weighted negative event scores, t = !.64, p > 0.10. There were no signif- icant differences between serostatus groups in weeknight sleep, serum albumin, pre- dicted VO2m~, vigorous physical activity l,evels, or high risk sexual activities at baseline (all ps > 0.10). Moreover, repeated measures ANOVAs indicated that none of these variables changed significantly over the 10-week observation period for either group (all ps > 0.10). The means and standara dev ~ons for each of these control measures are included in Table 1.
HIV-I: Psychology. Immunology. aqd Hormones B1OL PSYCHIATRY 1029 1991;29:1023-1041
Table 1. Characteristics of the Seronegative (n = 46) and Seropositive (n = 25) Samples
Variable H~ V - HIV -~-
Demographic measure:, Age (years)
M 30.18 31.60 SD 5.30 5.50
Ethnicity (n) Caucasian 3~, t7 Black American 0 I Hispanic 5 6 Other 3 I
Educ:mon (nl High school graduate 3 1 Some college 15 11 College graduate 20 6 Graduate degree 7 6
Modal annual income range $20,001-$30,000 $20,001-$30,000
Biobehavior; I measures Sleep (hr,'wee~:nigh0
M 7.02 7.24 SD 1.07 1.13
Albumin (g/100 dl) M 4.72 4.55 SD 0.37 0.37
Vigorous physical activity (hr/wk) M 1.0(3 1.10 SD 2.41 2.22
Aerobic fitness (VOe~ ml/kg/min) M 38.24 39.33 SD 7.09 6.81
High-risk sexual activity frequency (previous mot
M 5.95 3.62 SD 8.16 6.08
Negative life events (previous 6 tool M 4.05 6.48 SD 5.59 6.13
P~ychological Distress
Seropositive subjects revealed higher STAI scores than scronegatives at several time points and these differences were most striking at the time. of serostatus notification, Z = - 5 . 9 9 , p < 0.001, and the next anxiety measurement point thereafter ( T 4 ) Z = - 3 . 8 3 , p < 0.001. Scropositives had higher POMS-anxiety scores than seronegafives at several time points (T2, T,, T~, T6) and this difference was also greatest at T4, Z = - 3 . 6 9 , p < 0.001. Seropositives also showed significantly higher POMS-depression scores than seronegative~ at every time point with the largest disparity evident af. T4, Z = - 4 . I 1, p < 0.001, and revealed higher POMS confusion/bewilderment scores at T4-
T6 as well (ps < 0.001). Similarly, seropositives showed significantly higher IES intru- sion, avoidance, and total scores at each IES measurement point (T~, T4, T~, T6) (all ps < 0.001). The largest disparities between groups on these subscales were. no~ed at T4

1030 BIOL PSYCHIATRY M.H. Antoni et al 1991;29:1023-1041
Table 2. Means and S D for Severa l Dis t ress Measures at T i m e Points Preced ing and Fo l lowing Serostatus Notif icat ion (dx) A m o n g H I V - ! Seronega t ive and S e m p o s i t i v e G a y Males
Time point
HIV-I status TI T2 dx 1"4 T~ T6
State Anxiety Neg 34.48 3~ 10* 34.28* 35.73* 36.77 - - (8,66) (13.10) (9.12) (!1.82) (10.60)
Pos 39.00 43.53 54.75 43.25 39.71 (10.15) (12.78) ~11.21) (&59) (8.70)
POMS-Anxiety Neg 10.43 9.92* - - 6.28* 9 .91 ' 8.92* (7.29) (6.12) M (6.54) (7.44) (6.68)
Pos 11,80 12.07 ~ 14.81" 11.71" 11.93 (7.28) (5.08) - - (7.68) (6.73) (6.02)
POMS-Depression Neg 9.05* 7.82* - - 5.96* 8.74* 8,30* (9.65) (7.69) - - (9.45) (10.96) (9.43)
Pos 12.36 10.63 - - 17.83" 15.82 11.73 (9.29) (5.27) - - (12.64) (10.20) (8.06)
IF, S-Intrusion Neg 6,22* - - - - 5.00* 4.09* 5,49* (6.28) ~ - - 5.79 (4.38) (6.96)
Pos 13,40 - - - - 20.71 17.82 12.87 (10.32~ - - - - (7.97) (8.48) (7.26)
1ES-Avoidance Neg 5.44* - - - - 4.36* 3.64* 3,52* (5,04) - - - - (4.84) (3.72) (5.15)
Pos 9.16 - - - - 13.59 14.71 11.13 (6.54) - - - (4.99) (5.96) (5.55)
IES-Total Neg I 1.67* - - - - 9.36* 7.73* 9.00* (9.21) - - - (9.75) (6.66) ( i l . 64 )
Pos 22.56 - - - - 34.29 32.53 24.00 (14.20) - - M (10.94) (13.34) ( i l . 72 )
*p < 0.01 for Mann-Whitney U (significantly diffezer' fr-,nn the serolmsitive group).
and Ts. The descriptive statistics for STAI, POMS. and IE$ subscale scores for each group at each time ~o;" t are shown in Table 2.
Repeated measures ANOVA indicated that STAI values changed significantly over time among seropositives, F(4, 96) = 12.10, p < 0.001. Planned comparisons revealed a significant increase in anxiety from T2 to time of notification, t = - 3 . 4 7 , p < 0.001, suggesting that these individuals weft responding affectively to the news of seropositivity. We found that the tension-anxiety, depression, and confusion subscales of the POMS were highly intercorrelated. To minimize redundancy we combined these three subscales into a summative index which will be referred to subsequently as the POMS-dishe~ composite score. Similar to the findings for the STAI, ~ropositive subjects showed significant change in this composite score over the 10-week observation period, F(4, 96) = 2.81, p < 0.03. A planned comparison revealed a significant increase in this distress score between Tz and 1"4 (POMS was not administered at time of notification or T3), t = -2 .85 , p < 0.01. We also found a significant change over time for intrusion, F(3, 72) = p < 0.001, avoidance, F(3, 72) = 5.58, p < 0.002, and total IES scores, F(3, 72) = 7.39, p < 0~001. Planned comparisons between T~ and T4 for each subscale (IE$ was not administered at T2 or T3) revealed the expected increases in intrusion, t = -4 .09 , p < 0.001, avoidance, t = - 3 . 0 4 , p < 0.001, and total scores, t = - 3 . 8 5 ,
p < 0.0Ol. Together these findings suggested that seropositive subjects were responding

HIV- I: Psychology, lmanunology, and Hormones BIOL PSYCHIATRY 1031 1991;29:1023-1041
Q., o
< 3: =.
100000
80000
60000
aO000
20000 - PHA
t PLASMA CORTISOL
0 - ~ l J A i i i I T 1 T 2 / r ~ T 3 T 4 T 5 T 6
(:Ix T IME POINT
• 2 0 0 E t -
• 175 .J O
I- • 1 5 0 n'.
O O
" 1 2 5 ~
100 tt
Figure 1. Mean ( 4- SEM) cortisol and response to phytohemagglutinin (PHA) expressed as coauts per minute (epm) preceding and following serostatus no- tification (dx) among HIV-I semposi- tire gay males.
to serostatus notific~tion with increases in affective and cognitive manifestations of dis- 13"ess.
Neuroendocrine and immune Measures
The disparities in the PHA and cortisoi change patterns between sernpositives and seroneg- atives can be seen in Figures 1 and 2, respectively. Plasma cortisol values changed sigl~ificantly over the study period among seropositives, F(5, 120) = 5.40, p < 0.001 (Figure 1). These values were significantly lower than seronegative values at baseline, Z = -2 .17 , p < 0.03, and remained virtually unchanged between TI and 1"2. Cortisol values between T2 and T3 actaally declined (160.5 versus 142.96 ng/ml, t = 3.06, p < 0.005) for seropositives and continued to fall between "I"3 and "1"4. This pattern was striking in view of the previously noted increases in several measures of distress within this period.
Seropositives showed smaller responses to PHA and PWM than seronegatives at each time point (all ps < 0.001). However, seropositives showed no significant changes over time on responqes to PHA, F(5, 120) = 0.29, NS (see Figure !) and only a marginally
E Q. 0
< 3: o,.
129000
8 ~ 0 0 -
60000 -
4 0 0 0 0 ~ " - - ' - ~ P H ~
P L A S M A C O R T I S O L
"~.0000 . . ... , ,
T'I T~2 ~ T'3 T 4 T 5 T'6 dx
T IME POINT
- - - 200
e-
• 175 .,J 0
• 150 ~
8 • 125
1 lOO ..J
eL
Figure 2. Mean (-+ SEM) cortisol and response to phytohemagglutinin (PHA) preceding and following serostatus noti- fication (dx) among HIV-I seronegative gay males.

1032 alOL PSYCHIATRY M.H. Antoni et al 1991;2()' 1023- I (k t l
60-
40 -
20-
0- (D
-20 O
-40 . . . . . . . . "~)
$
~: anti-HI uJ
40
60,
20-
0-
-20-
-40 ,
--*-,'-IP--- CORT1SOL
nti-HIV-
Pre Post ch~
FiSu~ a. Cortisol, Profile of Mood States (POMS)- Composite scores and Impact of Event Scale tIES)- Total scores for anti-HIV + antiHIV- subjects ex- pressed as percentage ot cha~ge from prenotification levels. The pie time point refers to "!"2 for cortisol and POI~,IS and to Tt for the IES. Post values cor- respond to "1"4.
significant change in responses to PWM, F(5, 120) = 2.21, p < 0.10 (not shown). In contrast, seronegatives showed significant changes in PHA over the study period, F(5, 225) = 3.20, p < 0.001, with values increasing significantly between T~ and T2, t = 12.46, p < 0.02, reflecting initially low levels at the time of the first stressor (decision to enter study). As is evident in Figure 3, seropositives showed marked percentage increases ~ in psychological distress but an accompanying decline in plasma cortisol values over the prenotification to postnotification period, whereas seronegatives displayed a synchronous decrease in all of these markers prediagnosis to postdiagnosis--in line with the "relief" of a serouegative diagnosis.
To assess the degree of association among individual differences in response measures in this seropositive sample, we computed Pearson correlations at basei~.ae and T3 as well as on Ta-T2 A scores and T4-T5 z~ scores for all psychological, neuroendocrine, and immunological measures. 2 We found a positive correlation between plasma cortisol and PHA response values at T~, r = 0.65, p < 0.008, that was in contrast to that displayed by the seronegative group, r = - 0 . 3 6 , p < 0.05. Cortisol was also positively correlated with PHA values at the first postnotification time point (T3), r --=- 0.55, p < 0°05 for seropositives. Furthermore, changes in cortisol between T4 and T~ were positively e~,r- related with PHA T4-T5 A values, r = 0.56, yet negatively correlated in the ¢:ase of
)We computed the perccmage to change (% A) from prcnotilication to posla'~tiEcaticcl levels for POMS composite ~ores t% from T~ to T,). IFS focal scores (% A from T) to Td. arid plasnm co~tisol values (% A fn)m T2 to T() for each group.
~'vVc had convinced c~nclat~ng & scores for the inmze~atc pre-post scrosmats notification period. Because the postnotification measures w¢~ not collected cmlcurrentty (anxiety at timc of notification, blood n~asur~s m T~. and POMS and t~S at T~) we f~lt that individual difference analyses of this dat~ wo~ld produce potentially misleading findings and therefore limited chat~ge ~ore analyses to TI-T2 A scor~s ar~ T4-T5 A scoces.

HI V-I: Psychology, Immunology, and Hormones BIOL PSYCHIATRY 1033 1991;29:1023-1041
seronegatives, r = -0 .35 . Cortisol and PWM responses were not associated at baseline, though these two markers were positively correlated at T3, r = 0.56, p < 0.05, and at T4, r = 0.77, p < 0.02 in the seropositive group.
Neither PHA nor PWM TIn-T2 A scores were correlated with either state anxiety or POMS tension/anxiety A scores (ps > 0.20) among seropositives; again in contrast to the significant negative PHA A x state anxiety A, r = - 0 . 4 1 , p < 0.01, and PWM A × state anxiety A correlations, r = -0 .34 , p < 0.02, for seroaegatives. Cortisol A
scores were negatively correlated with state anxiety A scores, r = - 0 . 5 2 , and POMS- tension/anxiety A score~, r = --0.67, over a similar period for the seropositives. Gen- erally, additional psych~endocrine A score analyses for postnotification time points in- dicated either negative correlations between corfisol and distress or an absence of cor- relation for seropositive men.
We wondered if the pattern of results noted in the seropositive group might have been determined, to some degree, by subjects' prenotification perceptions of personal risk of seroposidvity. If so, those subjects who had entered the study and the prenotifica~ion period perceiving themselves to be at low risk for infectivity would have displayed lower psychological distress levels (and perhaps lower cortisol values) than their high perceived risk counterparts. Such differences in prenotification levels could effect the degree of any subsequent changes in these variables prenotification to postnotification thereby system- atically biasing our results. Before notification, subjects were asked at Tm to predict their antibody status. Among a sample of seropositive subjects who responded to this ques- tionnaire item (n = 21), nine subjects predicted that they were seropositive and 12 predicted seronegative. We compared distress measures (STAI, POMS, IES), plasma cortisol levels, and both mitogen response markers between these two belief groups at T~ and T2 and found no differences on any of these variables at either time point (all ps > 0.10). A similar set of analyses conducted on the seronegative sample levealed similar findings.
To assess the contribution of HIV- ! infection severity to the present findings we grouped seropositives according to their scale position on the Zolla-Pazner and colleagues (1987) immunological staging system. This system, based on a Guttman scalogram technique, classifies individuals with helper/suppressor-cytotoxic (CD4/CD8) cell ratios < 1.0 into those with helper cell (CD4) counts greater than (scale l) and less than (scale 2) 500 cells/ram 3. Here we found no differences between scale l (n = 19) and 2 (n = 6) groups on any response measure at TI or T2, and no differences in the magnitude of change across the T r T : period. In that our seropositive sample was skewed in tile direction of scale l Zolla-Pazner ranks and due to our concern that this particular classification sys- tem might not be sensitive to immunologic variability within the a~ymptomatic range of HIV-I infection, we also employed a statistical classification criterion for assessing the influence of infection severity. Here we divided ~roposifives into those subjects with CD4 values above and below the group median value (median -= 713.2 cells/ram 3) and found no differences between the high (n = 12) and low (n = 13) CD4 groups on any response measure at similar time points (all ps > 0.10).
Caveats. We viewed the repeated-measures ANOVAs for seropositives as the hy- pothesis testing sections of this study and the between-serostatus group analyses as the descriptive portion. In that several repeated-measures analyses (9 ANOVAs and 7 t-tests) were conducted it is arguable that our findings are extremely subject to Type I error.

1034 131oL PSYCmAT~V M.H. Antoni et al 1991 ;29:1023-1041
Several of the repeated-measures comparisons were, however, significant at p < 0.001 and the probability of obtaining the 13 dgnificant findings that we did in the 16 analyses conducted---even with a = 0.05---is (1 - 11 - a]~6) ~ ~ 0.00052. The fact that several of these 13 significant comparisons yielded p values at less than the 0.001 level makes this overall probability, estimate an extremely conservative one. The correlational findings should be viewed as exploratory in nature and were conducted to clarify the previously established repeated-measures ANOVA findings. A larger sample of seropositives will be needed before the stability of these correlations can be confidently stated.
Discussion
Our results suggested that a:aong asymptomatic HIV-I seropositive men, plasma co~isol concentrations are negatively correlated with psychological distress and positively cor~ related with lymphocyte responses to PHA (assessed basally and in response to serostatus notification). Both of these relationships are contrary to those previously documented in studies of acute (e.g., bereavement; Irwin et al 1987), and chronic (e.g., being a resident of Th,'ec Mile Island following the nuclear reactor accident; McKinnon et al 1989) s.-e~sors. Moreover, this pattern of psychoendocrine and endocrine-immune findings was also in opposition to the patterns shown by our soci~emogratahic.a_l!y equivalent HIV-I sen)negatives and may explain, to some degree, the discrepancy in psychoimmune re- lationships observed between seronegatives and seropositives. These findings could not be explained by individual differences in perceived risk of infectivity prior to serostatus notification, extraneous environmentel stressors, or CD4 cell counts within the seropos- itive group.
P~:ychological Distress
Concordance among psychometric distress measures was ascertained at key time points and a close relationship among measures was evident in :he magnitude of change between time points. As expected, seropositives showed greater distress than seronegatives on all of these measures at all postnotification time points, and significant increases prenotifi- cation to postnotification. Other work has documented similar significant increases in affective distress (e.g., depression) preseropositivity to postseropositivity notification using a similar inter-time point interval (2-4 weeks; Ostrow et al 1989). The increases in distress found in the present sample of seropositives were in contrast to seronegatives who showed a slight decrease in distress following notification reflecting, most likely, the relief of news of seronegativity. Hence, this battery of psychological distress indicators appears to be sensitive to the range of psychosocial stress responses stimulated by this stressor in this population.
Regarding the range of distress observed in this study, state anxiety values displayed by seropositives at the time of notification (mean =- 54.75) were nearly identical to those of neuropsychiatric patients diagnosed with depressive or anxiety reaction~ (Spielberger et al 1970). Similarly, postnotification POMS subscale elevations approached male psy- chiatric ou~.patient means (McNair et al 1981). Regarding the 1ES findings, seropositives revealed postnotific~fion total score values that were nearly double those noted among residents of Three Mile Island in the period following the nuclear reactor accident (Dav- idson and Baum 1986), higher than those observed in azymptomatic gay males partici- pating in an antiviral drug regimen (Jacobsen et al 1988), and equivalent to those evidenced by maie stress clinic patients presenting with "stress response syndromes" related to recent

HIV-I: Psychology, Immunology, and Hormones BIOL PSYCHIATRY 1035 1991 ;29:1023-1041
personal injury, bereavement, violence, illness, or surgery (Horowitz et al 1979). Further, the changes in these affective and cognitive distress markers suggest that seropositive subjects' psychological responses to the potification stressor are not blunted or repressed. As such it is unlikely that the absence of immunologic changes "in response to" this stressor are due to a dysfunction in the perceptual--cognitive-affective response system among seropositives.
Disparities Among Response Measures The mitog~.n response patterns di,~played in the present ~ample of 25 seropositives and 4( ~eronegatives mirrored the fndings that we have reported on a smaller sample (lronson et al 1990). The fact that seropositives showed poorer lymphocyte responses to mitogens than their seronegative counterparts at all 6 time points was not surprising and merely demonstrates the qualitative decrements in immune functioning that accompany HIV-I infection (Fletcher et al 1987). Of more interest to the present investigation was the virtual absence of PHA-induced blastogenic changes in response to seropositivity notification despite the concurrent changes in psychological distress prenotification to postnotification. Other psychoimmunological studies have provided evidence for decrements in lymphocyte proliferative responses to mitogens such as PHA or concanavalin A (ConA) among healthy individuals experiencing acute examination stress (Halvorsen and Vassend 1987; Kiecolt- Glaser et al 1984; Workman and LaVia 1987), among bereaving males predeath to postdeath of spouse (Schleifer et al 1983; Irwin et al 1987), and in patients suffering from major depressive diso~er (Schleifer et al 1984). Impaired mitogen responses have also been correlated with severity of depressive symptoms (Irwin et al 1987) and degree of intrusiveness of stressors as measured by the IES (Workman and LaVia 1987) sug- gesting that individual differences in psychological distress responses also impact this index of cellular immunity. Given this empirical literature we were impressed by the absence of a PHA-response change in our seropositives who (1) were exposed to a potent psychosocial stressor, and (2) were displaying clinical elevations in several ¢;istress mark- ers characterizing anxiety, depression, confusion, and intrusive thoughts.
Our model for stressor-induced immunomodulation, based on the extant human and animal literature, proposes that one mediational pathway for the effects of psychosocial stressors and affective disturbances on immune functioning is through activation of the HPAC system with consequent release of ACTH and cortisol tA~ltoni et al 1990a). For instance, corticosteroids are known to have immunosuppressive properties that extend to several components of cell-mediated immunity including cytokine production in response to PHA (Hahn et al 1976; see also Cupps and Fanci 1982 for review). To assess the role of HPAC activity in the disparity between psychological and immune measures previously noted in seropositives we measured plasma cortisol concentrations concurrendy with distress and immune markers.
Interestingly, seropositives showed lower cortisol concentrations than seronegatives at several time points and most notably at the two consecutive points following notification. Importantly, this time period was one in which the two groups showed the largest disparity in psychological distress scores--with the seropositive ~'roup displaying greater distress! Furthermore, within-group analyses of seropositive res!t~onse measures indicated that (1) distress and cortisoi values were inversely related at baseline and after notification, and (2) pre-postnotificafion cortisol decreases were accompanied by pro-post distress in- creases. In contrast, seronegative subjects showed concomitant movement in cortisol and distress levels--both decreasing--across an identical observation period. Other work has
1036 slot. r'SYCHtA'rl~¥ MH. Antoalet al
suggested that psychologic,I distress reactions (e.g., anxiety related to bereavement) may be accompanied by elevations in the rate of excretion of urinary free cortisol (see Irwin et al 1987 for review). The degree of IES intrusiveness of a chronic stressor (threat of radioactivity) has also been positively correlated with urinary cortisol levels in healthy normals (Davidson and Baum ~986).
Beyond these psycheendocrine pettems we found that plasma cortisol concentrations were actually positively correlated with PHA responsivity values at both prenotiflcation and I~stnotitication measurement points for seropositives. Taken together, the inverse p~ychoen&;crine relationships and ;he positive endocrine-irturJune correlations shown by ~ropositives during this stressful period (in comparison to the expected positive pay. choendecrine and inverse endocrine-immune associations found in seronegatives) suggest that dysregutation in the neuroendocrine and/or immune systems and disparities among psychological, neuroendocrine, and immunologic responses may explain, to some degree, the dampened immune "reactivity" to the notification stressor in the HIV- 1 infected group.
What characteristic(s) of HIV-! infectivity per se dete,mines the disparities among response measures that ware apparent in our data? Some possibilities might include a neurotropic effect of HIV-I perhaps affecting (i) the availability of HPAC neuropeptides (CRH, ACTH) and regulation in long and short I-IPAC feedback loops (Lewi et al 1989; Falkenhacfi et al 1989)0 or (2) a muted responsivity of the autonomic nervous ;/stem to challenge (Cohen and Laudenslager 1989; Kumar et al 1991) with secondary clarets o~ HPAC potentiation (Axelrod and Reisine 1984). Importantly, however° th= only empirical evidence to dale suggesting endocrine abnormalities in HIV-I infected populations has been restricted to samples of AIDS patients, where the likelihood is high that adrenal dysfunctions are caused by opportunistic infections (e.g., cytomegalovirus) and neoplasnis (Kaposi's sarcoma), the agents utilized in their treatment, and/or the host's production of cytokines in response to th ~ infection (Area 1989; Lahdevirta et al 1988; Tapper et al 1988). We are unaware of any work indicating that asymptomadc HIV-I seropositive individuals show such endocrine changes, however. Especially relevant to the atypical endocrine-immunologic relationships noted in the present sample of infected individuals, HIV- I may compromise neureendocrine target (CIM cells) availability by depleting helper cell numbe~ below some critical threshold (e.g., 900 eells/mm~), by inducing a state of corticosteroid resistance in mononuclear ceils (Balotta et al 1989), or by altering lym- phocyte intracellular phenomena (Bourguignou et al 1990) necessary for i=~corporating steroid ligands.
Alternative Explanations
By way of exclusion criteria and repe~ted mea.~urement of potential immunomoduiatory confounds we establi~hed that there were no baseline between-group differences in ate=aid ,~r antihistamine use, alcohol or recreational drug abuse, nutritional levels (as indexed by serum albumin), recent viral infection symptoms, high-risk sexual behaviors, sleep, aerobic fitness, frequency of vigorous physical activity, or recently experienced stressful life events. It i, conceivable, however, that other potential immunomodulatory ~:onfounds (e.g., changes in diet, cigarette smoking, caffeine consumption, alcohol and recreational drug use ) theft were not assessed, may have contributed to our results (Streeten et al i~82).
We also assessed individual differences in perceived risk of infectivity at baseline among seropositives as a possible determinant of the pattern of findings noted in this

HIV-I: Psychology, Immunology, and Hornmnc~ BIOl. PSYCHIATRY 1037 1991 ~Zg: t02:3,,, 1041
group. These analyses suggested that there were no differences in any respond: measures at either prenotification time point as a function of perceived serostatus within either the HIV-I seropositive or seronegative group. Given that perceived serostatus was assessed by a single, forced-choice questionnaire item, the possibility exists, however, that se- ropositives had a greater suspicion of HIV-1 infexrtion than they admitted on self-repotl, On the other hand, the fact that both groups reported an equivalent frequency of high. risk sexual behaviors (in the past month) may lend some support to the notion of equality in perceived risk of infectivity between g,xmps at study entry, Assumir, g that the psy. choimmunologic dissociation was (I) cvldent in seropositives before and after serostatus notification but at neither set of lime points in the seronegative group, {2) independent of negative life events experienced in the subjects' environment, and (3) unrelated to perceived risk of infectivity, this suggests that this phenomenon is not a stress-induced one but is likely determined by the presence of HIV-I.
Others have provided evidence that perceived lymphadenopathy-positive status among HIV-I seropositive males with and without later physical confirmation of lymphadenop- athy was associated w~th a greater degree of depressed affect but not with differences in T-helper/suppressor cell ratios (Ostrow et al 1986). Interestingly, perceived lymphade. nopathy-positive status was associated with both greater depression and lower CIM/CD8 ratios in a seronegative group of lymphadenopathy-positive and -negative men. The~ investigators came ~,,o the conclusion that the "modest" effects of psychological stressors on immune functioning will be difficult to document until we can "factor out" the larger contribution of the viral infection itself,
Althougil there is as yet no reliable procedure available for assessing the precise amount of"viral burden or load" that an infected host is enduring, some have attempted to classify the severity of the infection on the basis of immunologic (CD4, CD4/CD8 ratios) cell counts (Zolla-Pazner et al 1987)---this index being presumably related, inversely, to the number of immunologic targets infected by HIV-I. We dichotomized our seropositive sample on the basis of their CD4 cell counts and compared these two "severity" subgroups on all respon,~e measures, The absence of subgroup differences on any measure at either prcnotification time point and the similarity of change scores between time points between these two groups suggested that the presence but not necessarily the severity of H!V-I infection determines the unique pattern of response values noted in this study, Such conclusions arc, however, limited by the fact ',hat the severity sta~ing criteria employed in !his st~,dy (median CIM counts and the Zolla-Pazner et al scale) 8re somewhat gross and are li.:~y to have more clinical utiiit) than research prc~ ision. A more precise marker of the infectiof ~. process {e.g,, B2-microglobulin; Fahey et al l';~g.3) may have elucidated the role of HIV-I infection severity in the phenomena noted in this study.
Methodological Issues
Several caveats are noteworthy here. First, this sample was self-selected, In that partic- ipants were highly educated men who learned of the study through gay newspapers and a community information exchange, it is likely that they may have been a particularly health-conscious and/or alu'uistic group, Thus the present findings may not be general- izable to other HIV-! infected individutds or AIDS risk group members (e,g,, IV-drug abusers, poor ethnic minority women). Second, although statistically significant, the changes in cortisol ob~rved in this study were small and within the normal range for early morning samples (50-250 ng/ml). Therefore, whereas the present findings may be

1038 BlOt- PSYCHIATRY M,H. A~toni el al pE0 U29; 1023 llMt
u~eful in providi:lg a potential explanation for disparate psychoimmunologic co relations t~bserved between HIV-I seronegative and seropositive men, these cortisol fluctuations are of unknown biological significance. Third, given the fact that seropositive~ showed lower cortisol values than seronegatives at baseline, the possibility exists that s~bseq~tent changes reflect statistical regression or scale attenuation effects rather than stressor- induced movements. However, given that seropositives showed lower baseline values, regression or floor effect influences would favor an upward movement in cortisol values; not the decrements that we observed. These baseline differences did, however, svggest that asymptomati~ HIV-! infected men may differ in chronic plasma cortisol levels. It will be necessary to assess urinary-free cortisol values in cor.:~l groups of irdividue~ls who have already been notified of their serostatus (seropositive attd seronegative ) in order to sort out the significance of the baseline differences observed in this study.
A fourth issue concerns the sampling strategy used to determine plasma eordsols. To minimize cortisol error variance we collected only early AM san,pies. It shouLi be kept in mind that cortisol concentrations displayed in this window ,ff time are kn~ ~wn to be the least sensitive to influence of environmental stressors with stressor-relatc,l changes being more pronounced in protocols conducted after 11 AM (Sachar 1981). Hen~:e we may ha~c observed larger cortisol effects across the pre-posmotification period had sam- ples been collected later in the day. The fact that we used only a single meas~,rement of plasma cortisol at each time point seriously limits our ability to make state, tents con- cerning the secretory rate and/or regulation of this hormone. Future work should utilize mid-day s~quential samples collected over 15-min intervals preceding and following an acute stressor by employing an exfusion pump (Kuhn 1989).
A final measurement issue applies to the timing of neuroendocrine samples relative to the notifica6on stressor. In that the first postnotification cortisol value (T3) i.~ obtained 72 hr after the fact° it is conceivable that the cortisol concentration at this poim it; reflective of a rebound effect rather than an initial response. As such, initial cortisol "responses"-- at the time of nt,ification---may actually be manifest as a sharp increase followed, at T3, by a greater decrease. Although it was impossible to test this hypothesis in the present protocol, it is noteworthy that if such a rebound phenomenon was responsible for this pattern then one would have expected higher cortisol valnes at the subsequent time point (T4F--reflecting a "return to baseline" in the seropositive group. In contrast, T4 cortisol values were actually lower than T3 values and cortisol levels did not reseml:le prenoti- fication values until 2~ weeks postnotification (T~). A related issue regards the temporal relationship between neurocndocrinc and immunologic responses. Specificall,/, different response latencies for cortisol and mitogen responsivity--a likely scenario-complicate the evaluation of intersystem relationships and would seriously limit the degr~:e to which concurrent measurement designs (such as the present one) can directly addres,,, this issue. However, our observations that seroposidves (in opposition to seronegatives) displayed (i) sustained lower cor~isol values at T3 and T4, and (2) positive cortisol-irnmune and negative cortisol-distress change score correlations at both prenotification and posmoti- tication time points suggests that this design was able to document a consistent pattern of disparities among psychological, neuroen&,crine, and immunologic response measures in HIV-I infected men.
Future work will need to examine the nature of the findings presented herein by assessing basal levels and stress responsivity across multiple channels including cogni- tive/affective, neuroendocrine/neuropeptide, cytokine, prelymphocyte, and postlympho- cyte, rcceptor response systems as well as with additional functional immune measures

HIV-I: Psychology, Immunology, and Hormones IIIOL PSYO:~ATRY 1039 1991;29:1023-1041
(e.g., natural killer cell activity). Ideally such r ,easurernents could be collected at regular intervals over longer, more clinically meaningful longitudinal perkds and correlated with HIV-1 related disease progression markers (e.g. , incidence of oppo~anistic infections). These phenomena could be studied in seropositives and matched seronegatives with standardized laboratory stressors in order to control extraneous sources of variance and to assess the time course of stressor reactivity in systems which as yet remain unstudied. Such a paradigm might help to explain the pattern of responses that we observed in HW- i infected individuals exposed to a potent life-threatening stressor in the present study and may provide important information regarding the generalizability of previously doc- umented psychoneuroimmunologic relationships to the study of the HIV-1 infected host,
'this research was supported by NIMH grant number P50MH4355.
Refe rences
Antoni MH, Schneiderman N, Fletcher MA, LaPerriere A, Goldstcin D, ironson G (1990a): Psychoneuroimmunology and HIV-1. J ConsuB Clin Psychol 58:38-49.
Antoni MH, August S, LaPerriere A. et al (1990b): Psychological and .neuroendocrine measures related to functional immune changes in anticipation of HIV- I serostatus notification. P~chosom Med 52:496-.510,
Aron DC (I 989): Endocrine complications of the acquired immunodeficiency syndrome. Arch Intern Med 149:330-333.
Axelrod J, Reisine T (1984): Stress hornmnes: Their interaction and regulation. Science 224:452- 459.
Balotta C, Vago T, Bevilacqua M, Galli M, Norbiato G, Moroni M (1989): HIV induces gluco- corticoid resistance in mononuclear cells. Paper presented at the V International Conference on AIDS, June, Montreal,
Bar~,n GA, Klimas NG,-lzi]~chl MA, Fletcher MA (1985): Decreased natural ceil-mediated cyto- t~Jxiei~y pe~ effc~iot cell n acq.;red immunodeficiency syndrome. Diagn Clin Immunol 3:i97- 204.
P, ourguignon L, Walker G, Huang H (1990): Interactions between a lymphoma membrane-asso- ciated GTP-binding protein and the eytoskeleton during receptor patching and capping. J Im- munol 1,~4:2242-2252
Breier A, Albus M, Pickar D, et al (1987): Controllable and uncontrollable stress in humans: Alterations in mood and neuroendocrine and psychophysiological functions. Am J Psychiat~. 144:1419-1425.
Calabrese J, Kling M. Gold P (1987): Alterations in immune, competence during stress, bereavement, and depression: Focus on neuroendocrine regulation. Am J P~chiatty 144:1123 -! !34
Cohen J, Laudenslager M (1989): Autonomic nervous system involvement in patients with human immunodeficiency virus infection. Neurology 39:11 t 1-1112.
Cupps T, Fauci A (! 982): Corticosteroia-mediated immunoregulation in man. lmmunol Rev 65:133- 135.
Davidson r , Baum A (1986): Chronic stress and posttraumatic stress disorders. J Consult Clin Psychol 54:303-308.
Donlou J, Wolcott M, Gottlieb M, Landsverk J (1985): Psyehosoci~ aspects of AIDS and AIDS- related complex: A pilot study. J Psychosoc Oncol 3:39-55.
Fahey JL, Taylor J M, Detels R, et al (1990): The prognostic value of cellular and serologic markers in infection with human immunoaeficiency viru. ~ype I. N Engl J Med 322:166-172.

I(MO atot, PSVCttIATaV MH. Antoni et al p~)l ;29:1023.- 1041
Falkenbach A, St. Klanke B, Michels P, Hunold E, Schifferdecker P (1989): Deficiency ofglu- cocorticoids in AIDS. Paper presented at the V International Conference on AIDS, Montreal.
Fletcher I~AA, Baron G, Ashman M, Fischl M, Klimas N (1987): Use of whole blood methods in assessment of immune parameters in immunodeficiency states~ Diagn Clin lmmunol 5:69-81.
Fletcher MA, Azen S, Adelbetg B, et al 0989): lmmunophenotyping in a multiceneer study: The transfusion safety exlx:rience~ Clin Immunol lmmunopothol 52:38---47.
Fox E, Billings C, Barrels R, Bason R, Mathews D (1973): Fitness standards for male college students, lnt Z Angewandte Physiol Einschliesslich ArbeJtsphysiol 31:231-236.
Glaser R, Kiecolt~Glaser J (1987): Stress-associated depression in cellular immunity: Implications for acquired immune defic:ency syndrome (AIDS). Brain Betulv hnmunol 1:107-112.
Hahn T, Levin S, Handzel Z (1976): Leukocyte migration inhibition factor (LIF) production by lymphocytes of normal children, newborns, and children with immunt~ deficiency. Clm Exp lmmunol 24:448-454.
Halvorsen R, Vassend O (1987): Effects of examina,'ion stress on some cellular immunity functions. J Psychosom Res 31:693-70 L
Horowitz M, Wilner N, Alvarez W (1979): impact of event scale: A measure of subjecuve stress. Psychosom Med 41:209-218.
lronson G, LaPerrier¢ A, Antoni MH, et al (1990): Changes in immune and psychological measures as a function of anticipation and reaction to news of H1V-I ~:ntibody status. Psychosom Med
~:247-270.
Irwin M, Daniels M, Wether H (1987): lrra'nune and neurccndocrine changes during bereaverr~ent. i~sychiatr Clin North Am 10:449-465.
Jacobsen PB, Perry S, Hirsch D, Scavuzzo D, Roberts RB (1988): Psychological reactions of individuals at risk for AIDS during all experimental drug trial. Psychosomatics 29:182-187.
Kavelaars A, Ballieux RE, Heijnen C (1988): Modulation of the immune response by proopiome- ianocortin derived peptides: 2. Brain Behav Immunol 2:57-66.
Kiecolt-Glaser J, Glaser R (1988): Methodological issues in behavioral immunology research with humans. Brain Behav lmmunol 2:67-67.
Kiecolt-Glaser J, Garner W, Speicher C, Penn GM, Holliday J, Glaser R (1984): Psychosocial modifiers of immunocompetence in medical students~ Psychosom Med 50:7-14.
Kuhn C (1989): Adranocortical and gonadal steroids in behavioral cardiovascular medicine. In Schpeiderman N, Weiss S, Kaufmann P (eds), Handbook of Research Methods in Cardiovascular Behavioral Medicine. New York: Plenum, pp 185-204.
Kumar M, Morgan R, Szapocznik J. Eisdorfer C (1991): Norepinephrine response in c",u'ly HIV infection. J AIDS (in press).
Lahdevirta J~ Maury C, Teppo A, Repo H (1988): Elevated levels of circulating cachectin/tumor necrosis factor in patients with acquired immunodeficie:~cy syndrome. Am J Med 85:289-291.
Laudenslager M. Ryan S. Drugan R, Hyson R, Mater S (198~:): Coping and immunosuppression. Inescapable hut not escapahle shock suppresses lymphocyte proliferation. Science 221:568-570.
Levy E, Cottrell M, Black P (1989). Psychological and immunological associations in men with AIDS pursuing a macrobiotic regimen as an alternative therapy: A pilut study. Brain Behav Immunol 3:175-182.
Lcwi D, Acetturi C, Sader H, Dias R, Kater C, Motta P (1989): Reduced co~iL31 production and adrenal uecro~is in patients with AIDS. Paper presented at the V International Conference on AIDS, June, Montreal,
McCabe PM, Schneiderman N (1985): Psychophys,ologic reactions to stress, in Schneiderman N, Tapp J (edsL Behavioral Medicit,e: The Biopsychosocial Approach. Hill3dale, N J: Erlbaum, pp 99-131.
McKinnon W, Weisse C, Reynolds C, Bowles C, Baum A (1989): Chronic stress, leukocyte subpopulations, and humoral response to latent viruses. Health P~ychol 8:389-4L02.

HIV-I: Psychology, Immunology, and Hormones BIOL PSYCrlIATRY 1041 1991;29:102J-.l(,t41
McNair D, Lorr M, Dropplema~ L (198!): EITS Manual for the Profile of Mood States. San Diego: Educational and Industrial Testing Service.
OsIrow D, Joseph J, Monjan A, et al ( 19~,6): Psychosocial aspects of AIDS risk. Psychopharmaeol Bull 22:678-683.
Ostrow D, Joseph J, Kessler R, et al (1989): Disclosure of HIV antibody status: Behavioral and mental health correla,es. AIDS Ed Prevent | , t - I 1,
Pawlikow.ski M, Zelazowski P, Dohler K. Stepien H (1988): Effects of two neutopeptide~, so- matolibetin (GRF) and corlicoliberin ~CRF). on human lymphocyte natural killer activity, Brain Behav lmmunol 2;50--56.
Pericic D. Maney H, Boranic M, Poljak-Blazi M. Lakic N (1987): Effect of diazepam ¢'n brain neurotransmitters, plasma cortisol, and the immunc sy,;tem of stre,,sed rats. Ann NY Aead Sci 496:450-458.
Sachar E (1981): Psychobiology of affective disorders. In K~md,:l E, Sch~,artz J (eds), Principles ~fNeural Science. New York: Elsevier.
Sarason 1, Johnson J, Siegel J (1978): Assessing the impact of life change~': Development of the Life Experiences Survey. J Cot;suit Clin Psychol 46:932-946.
Schleifer S, Keller S, Meyerson A, Raskin M, Davis K, Stein M ( 1984): Lymph,-,cyte functio~t in major depressive disorder. Arch Gen Psychiatry 41:484-486.
Schleifer S J, Keller SE, Caminero M, Thorntm, JC Stein M (1983): Suopressi~:~ of lymphocyte stimulation fol;owing bereavement. JAMA 15:374-377.
Solomon GF (1987): Psychoneuroimmt, aologic approaches to research on A!DS. Ann NY Aead Sci 496:628-636.
Solomon GF, Temoshok L (1987): A psychoneuroimmunologic perspective on AIDS research: Questions. preliminary findings and sugge:~tions. J Appl Soc Psychol t7:286-308.
Spielberger C, Gorusch R, Lushene R (1970): State-Trait Attrie~, Inventory manual. Palo Alto. Consulting Psychologists Press,
Streeten D. ,~nderson G. Dalakos T, et al ( 1982): Normal and abnormal function of the hyp<)thalamic pituitary adrenocorfical system in man. Emlocr Rev 5:371-394.
Tapper M, Rottc~dam i-I, Lerner C, Al'Khafaji K, Seitzman P (1988): Adrenal necrosis in the acqui:ed immunodeficietley syndrome. Ann Intern Med 1090:239-241.
Wmkman E, LaVia M (1987): T-lymphocyte polyclonal proliferation: Effects of sW:gs and stress response s~.yle on rr;,~dii:al students taking National Board Examinations. Clin Irr~nunol bnmu- nopathol 43:308-?~ i 3
Zilbetg N. Weiss D. Horowitz M 11982): Impact o1' eve,at scale: A cross-vahdation study alid some empirical evidence supporting a conceptual model of stre~s response syndromes. J Cousuh Clin Psychol 50:407-414.
Zolla-Pazner S, DesJarlais D, Friedman S, et al (1987): Non~'andorn development ,ff imcalanologic abnormalities after infection with human, iml:,anodeficiency virus: Implications for immunologic classification of the disease. Proc Nat Acad Sci USA 84:5404--5408.




















