Clinical and Microbiological Profiles of Human Immunodeficiency Virus (HIV)–Seropositive...
10
Clinical and Microbiological Profiles of Human Immunodeficiency Virus (HIV)–Seropositive Brazilians Undergoing Highly Active Antiretroviral Therapy and HIV-Seronegative Brazilians With Chronic Periodontitis Lucio de Souza Gonc xalves,* So ˆnia Maria Soares Ferreira, † Celso Oliveira Souza, † Renata Souto,* and Ana Paula Colombo* Background: This study compares the periodontal clinical profile and the composition of the subgingival microbiota of human immunodefi- ciency virus (HIV)-seropositive and HIV-seronegative subjects with chronic periodontitis. Methods: A total of 172 subjects were distributed into two HIV-seropos- itive groups (37 chronic periodontitis [H+CP+] and 35 periodontally healthy [H+CP-] individuals) and two HIV-seronegative groups (49 chronic periodontitis [H-CP+] and 51 periodontally healthy [H-CP-] subjects). Subgingival samples were collected from six sites with the deepest probing depth in the periodontitis groups and six random sites in the groups with periodontal health. All HIV-infected patients had undergone highly active antiretroviral therapy (HAART) for at least 2 years. The presence and levels of 33 bacterial species were detected by DNA probes and the check- erboard method. Kruskal-Wallis and Mann-Whitney tests were used to seek for significant differences among and between groups. Results: H-CP+ patients showed significantly more periodontal de- struction and inflammation than H+CP+ patients, whereas H+CP- subjects presented a greater percentage of sites with bleeding than H-CP- subjects (P <0.01). Patients who were HIV seronegative showed higher prevalence and levels of most bacterial species than HIV seropositive patients. Peri- odontal pathogens including Tannerella forsythensis, Porphyromonas gin- givalis, Prevotella nigrescens, Eubacterium nodatum, Fusobacterium nucleatum, and Selenomonas noxia were more frequently detected in H-CP+ subjects compared to H+CP+ and controls. In contrast, Enterococ- cus faecalis and Acinetobacter baumannii were more commonly found in HIV-infected than in non–HIV-infected subjects (P <0.05). Conclusion: Putative periodontal pathogens are more prevalent in the subgingival microbiota of HIV-seronegative patients with chronic peri- odontitis, whereas species not usually associated with periodontitis are detected in higher frequency in HIV-seropositive subjects under HAART. J Periodontol 2007;78:87-96. KEY WORDS Highly active antiretroviral therapy; HIV infection; periodontitis. S everal studies 1-17 have examined the periodon- tal microbiota of hu- man immunodeficiency virus (HIV)-infected subjects. How- ever, these studies have faced many difficulties. For in- stance, some authors 3,6 have included different forms of periodontitis such as chronic, aggressive, and necrotizing diseases in the same micro- biologic analysis, leading to conflicting data. In regard to HIV-infected patients with chronic periodontitis, studies on the subgingival micro- biota have shown quite dis- tinct results. It has been shown that the subgingival microbiota of HIV-infected and non–HIV-infected indi- viduals are similar in compo- sition. 7,8 Other reports 9-12 have found a higher prev- alence of putative peri- odontal pathogens such as Aggregatibacter actinomyce- temcomitans, Fusobacterium * Institute of Microbiology, Federal University of Rio de Janeiro, Rio de Janeiro, RJ, Brazil. † Dental School, Federal University of Rio de Janeiro. doi: 10.1902/jop.2007.060040 J Periodontol • January 2007 87
Transcript of Clinical and Microbiological Profiles of Human Immunodeficiency Virus (HIV)–Seropositive...

Clinical and Microbiological Profilesof Human Immunodeficiency Virus(HIV)–Seropositive BraziliansUndergoing Highly Active AntiretroviralTherapy and HIV-SeronegativeBrazilians With Chronic PeriodontitisLucio de Souza Goncxalves,* Sonia Maria Soares Ferreira,† Celso Oliveira Souza,† Renata Souto,*and Ana Paula Colombo*
Background: This study compares the periodontal clinical profile andthe composition of the subgingival microbiota of human immunodefi-ciency virus (HIV)-seropositive and HIV-seronegative subjects with chronicperiodontitis.
Methods: A total of 172 subjects were distributed into two HIV-seropos-itive groups (37 chronic periodontitis [H+CP+] and 35 periodontallyhealthy [H+CP-] individuals) and two HIV-seronegative groups (49 chronicperiodontitis [H-CP+] and 51 periodontally healthy [H-CP-] subjects).Subgingival samples were collected from six sites with the deepest probingdepth in the periodontitis groups and six random sites in the groups withperiodontal health. All HIV-infected patients had undergone highly activeantiretroviral therapy (HAART) for at least 2 years. The presence andlevels of 33 bacterial species were detected by DNA probes and the check-erboard method. Kruskal-Wallis and Mann-Whitney tests were used toseek for significant differences among and between groups.
Results: H-CP+ patients showed significantly more periodontal de-struction and inflammation than H+CP+ patients, whereas H+CP- subjectspresented a greater percentage of sites with bleeding than H-CP- subjects(P <0.01). Patients who were HIV seronegative showed higher prevalenceand levels of most bacterial species than HIV seropositive patients. Peri-odontal pathogens including Tannerella forsythensis, Porphyromonas gin-givalis, Prevotella nigrescens, Eubacterium nodatum, Fusobacteriumnucleatum, and Selenomonas noxia were more frequently detected inH-CP+ subjects compared to H+CP+ and controls. In contrast, Enterococ-cus faecalis and Acinetobacter baumannii were more commonly found inHIV-infected than in non–HIV-infected subjects (P <0.05).
Conclusion: Putative periodontal pathogens are more prevalent in thesubgingival microbiota of HIV-seronegative patients with chronic peri-odontitis, whereas species not usually associated with periodontitis aredetected in higher frequency in HIV-seropositive subjects under HAART.J Periodontol 2007;78:87-96.
KEY WORDS
Highly active antiretroviral therapy; HIV infection; periodontitis.
Several studies1-17 haveexamined theperiodon-tal microbiota of hu-
man immunodeficiency virus(HIV)-infected subjects. How-ever, these studies have facedmany difficulties. For in-stance, some authors3,6 haveincluded different forms ofperiodontitis such as chronic,aggressive, and necrotizingdiseases in the same micro-biologic analysis, leading toconflicting data. In regard toHIV-infected patients withchronic periodontitis, studieson the subgingival micro-biota have shown quite dis-tinct results. It has beenshown that the subgingivalmicrobiota of HIV-infectedand non–HIV-infected indi-viduals are similar in compo-sition.7,8 Other reports9-12
have found a higher prev-alence of putative peri-odontal pathogens such asAggregatibacter actinomyce-temcomitans, Fusobacterium
* Institute of Microbiology, Federal University of Rio de Janeiro, Rio de Janeiro, RJ, Brazil.† Dental School, Federal University of Rio de Janeiro.
doi: 10.1902/jop.2007.060040
J Periodontol • January 2007
87

nucleatum, Porphyromonas gingivalis, Prevotella in-termedia, Tannerella forsythensis, and Treponema den-ticola, as well as combinations of these species, inHIV-seropositive patients compared to HIV-seronegativesubjects. Conversely, Patel et al.12 found P. gingivalisand T. denticola to be more prevalent in HIV-seroneg-ative individuals.
Microorganisms not commonly associated withchronic periodontitis have been frequently encoun-tered in the subgingival biofilm of HIV-infected pa-tients. Some of these species include Staphylococcusepidermidis, Candida albicans, Enterococcus faecalis,Clostridium clostridiiforme, Clostridium difficile, Klebsi-ella pneumoniae, and Mycoplasma salivarium.1,5,13
Recently, E. faecalis was found to be significantly moreprevalent in the subgingival microbiota of HIV-infectedsubjects with low levels of T CD4 lymphocytes (CD4<200 cells/mm3), suggesting that severe immunosup-pression may favor the colonization and overgrowth ofunusual and opportunistic pathogenic species.14
Strong evidence has shown that the introduction ofhighly active antiretroviral therapy (HAART) for themedical management of HIV-infected patients hasresulted in a marked decrease in the incidence and/or severity of periodontal diseases in this popula-tion.15,16 However, the impact of this therapy in theperiodontal microbiota needs to be determined.
The data in the literature clearly indicate that thecomplex relationship among the subgingival micro-biota, HIV infection, and periodontal disease remainspoorly understood. Thus, the present study comparedthe clinical profile and the composition of the subgin-gival microbiota between HIV-seropositive patientsundergoing HAART and HIV-seronegative Brazilianswith chronic periodontitis and periodontal health.
MATERIALS AND METHODS
Subject PopulationIn this case-control study, 172 subjects were selectedbetween 2003 and 2005 from the pool of patients ofthe University Hospital Clementino Fraga Filho andSchool of Dentistry of the Federal University of Riode Janeiro (UFRJ). All subjects were informed aboutthe aims of the study, risks, and benefits and signed aconsent form to participate. Information regarding de-mographic features, general health, and HIV infectionhistory were obtained from an anamnesis question-naire and patients’ medical records. Patients were>21 years of age and presented at least 20 teeth. Allpatients with chronic periodontitis were submitted toa full-mouth periapical radiographic examination.The patients were distributed into two HIV-seroposi-tive groups (37 chronic periodontitis [H+CP+] and35 periodontally healthy [H+CP-] individuals) andtwo HIV-seronegative groups (49 chronic periodonti-
tis [H-CP+] and 51 periodontally healthy [H-CP-] sub-jects). Patients with chronic periodontitis presented atleast three sites with probing depth (PD) ‡5 mm and/or clinical attachment level (CAL) ‡4 mm, whereasperiodontally healthy individuals showed no sites withPD >3 mm and/or CAL >4 mm. All HIV-infected pa-tients were using HAART for ‡2 years. In addition, theywere taking trimethoprim and sulfamethoxazole asprophylaxis for Pneumocystis carinii pneumonitis.Exclusion criteria included pregnancy, nursing, dia-betes, autoimmune diseases, and necrotizing periodon-tal diseases (necrotizing ulcerative gingivitis [NUG]and necrotizing ulcerative periodontitis [NUP]). Thestudy protocol was approved by the Review Commit-tee for Human Subjects of the University HospitalClementino Fraga Filho/UFRJ.
Clinical Measurements andTherapeutic ProceduresFull-mouth clinicalmeasurements, including PD(mm),CAL (mm), the presence or absence of bleeding onprobing (BOP), and supragingival plaque accumula-tion (PL) were recorded at six sites per tooth in all teethof all patients. These measurements were performedby two calibrated examiners using conventional man-ual periodontal probe.‡ After clinical examination, pa-tients with evidence of destructive periodontal diseasereceived full-mouth scaling and root planing (SRP)under local anesthesia and instructions for properhome care procedures. Periodontally healthy patientsreceived oral hygiene instructions, supragingival scal-ing, and prophylaxis.
Immunologic AssessmentIn HIV-infected subjects, laboratory analyses of TCD4, T CD8 lymphocyte, and neutrophil levels in peri-pheral blood were routinely performed every 4 monthsfor all patients at the University Hospital ClementinoFraga Filho/UFRJ. For comparison purposes, the lab-oratory data of each patient were obtained within thesame week that the periodontal clinical examinationwas performed.
Microbiologic AssessmentBefore clinical examination, individual subgingivalbiofilm samples were taken from the six deepest sitesof each subject with chronic periodontitis and six ran-domlyselected sites of subjectswith periodontalhealth,using sterile curets. The presence and levels of 33bacterial species (Table 1) were determined by amodification17 of the checkerboard DNA-DNA hy-bridization method described by Socransky et al.18
In brief, the samples collected were placed in separateEppendorf tubes, the cells were lysed, and denatured
‡ North Caroline Probe, Hu-Friedy, Chicago, IL.
Clinical and Microbiological Profiles of HIV Brazilians Volume 78 • Number 1
88

DNA was fixed in individual lanes on a nylon mem-brane§ using the checkerboard slot blot device.i
Thirty-three digoxigenin-labeled¶ whole genomicDNA probes were hybridized at 90� to the lanes ofthe plaque samples. Bound probes were detected us-ing phosphatase-conjugated antibody to digoxigenin#
and chemiluminescence.** Signals were evaluatedvisually by comparison with the standards at 105
and 106 bacterial cells for the test species on the samemembrane. They were recorded as follows: 0 = notdetected; 1, <105 cells; 2, ;105; 3, 105 to 106 cells;4, ;106; and 5, >106 cells. The sensitivity of this assaywas adjusted to permit detection of 104 cells of a givenspecies by adjusting the concentration of each DNAprobe. This procedure was carried out to provide thesame sensitivity of detection for each species. Failureto detect a signal was recorded as 0, although con-ceivably, counts in the 1 to 1,000 range could havebeen present.
Statistical AnalysisAll statistical tests were accomplished using a statis-tical program.†† Descriptive analysis of demographicand immunologic data was performed. The periodon-tal clinical measurements were averaged for eachsubject and across subjects within each group. Signif-icance of differences in these parameters among thefour groups was sought using the Kruskal-Wallisand x2 tests. Microbial data were expressed as meanpercentage of colonized sites (prevalence) and meancounts · 105 (levels) of each bacterial species com-puted for the six sites sampled in each subject andacross subjects within each group. Significant differ-ences in the prevalence and levels of these speciesamong all groups were determined using the Kruskal-Wallis test. The Mann-Whitney test was used to
Table 1.
Subgingival Species Used for Constructionof Whole Genomic DNA Probes TestedAgainst Subgingival Biofilm Samples
Bacterial Species Strain
A. actinomycetemcomitans 29523*
A. baumannii 19606*
A. naeslundii I 12104*
A. naeslundii II (A. viscosus) 43146*
Actinomyces odontolyticus 17929*
Campylobacter rectus 33238*
C. gingivalis 33624*
E. corrodens 23834*
E. coli 33780*
E. faecalis 29212*
E. nodatum 33099*
F. nucleatum ss. vincentii 49256*
G. morbillorum 27824*
Leptotrichia buccalis 14201*
Micromonas micros 33270*
Neisseria mucosa 19696*
P. aeruginosa 27853*
P. gingivalis 33277*
P. intermedia 25611*
P. melaninogenica 25845*
P. nigrescens 33563*
P. acnes 11827*
Streptococcus anginosus 33397*
Streptococcus constellatus 27823*
S. gordonii 10558*
S. intermedius 27335*
S. mitis 49456*
Streptococcus oralis 35037*
S. sanguinis 10556*
S. noxia 43541*
Table 1. (continued)
Subgingival Species Used for Constructionof Whole Genomic DNA Probes TestedAgainst Subgingival Biofilm Samples
Bacterial Species Strain
T. forsythensis 43037*
T. denticola B1†
Veillonella parvula 10790*
* ATCC, American Type Culture Collection, Rockville, MD.† The Forsyth Institute, Boston, MA.
§ Amersham Biosciences do Brasil, Sao Paulo, SP, Brazil.i Minislot 30, Miniblotter 45, Immunetics, Cambridge, MA.¶ Roche Molecular Systems, Alameda, CA.# Roche Molecular Systems.** Amersham Biosciences do Brasil.†† Statistical Package for the Social Sciences, Release 10.0, SPSS,
Chicago, IL.
J Periodontol • January 2007 Goncxalves, Soares Ferreira, Souza, Souto, Colombo
89

evaluate significant differences between two groups.Analysis of variance and covariance (multivariategeneral linear model [GLM] test) were performedto study the possible effects of age and smoking(covariates) in the differences of clinical and microbi-ologic parameters between groups. Adjustments formultiple comparisons were made as described bySocransky et al.19 Associations between clinicaland microbiologic parameters were tested using thePearson correlation coefficient. Statistical signifi-cance was reached at a 5% level for all analysis.
RESULTS
Demographic, Clinical, and Laboratory Featuresof the Study PopulationThe epidemiologic and clinical profiles of the 172 in-dividuals evaluated in this study and the immunologicdata of the 72 HIV-infected patients are summarized inTable 2. Statistically significant differences amonggroups were observed for all parameters (P <0.01;Kruskal-Wallis and x2 tests), except for gender andmean percentage of sites with BOP. Periodontallyhealthy individuals (H-CP- and H+CP-) were signifi-cantly younger than H-CP+ patients (P <0.05),whereas no significant difference was observed be-
tween H+CP+ and H+CP- subjects (P >0.05; Mann-Whitney test). No smokers were present in the H-CP-group. After controlling for age and smoking ascovariates, significant differences among groupswere observed for all periodontal clinical parameters(P <0.01; GLM test). When pairs of groups were com-pared, individuals with chronic periodontitis pre-sented significantly more disease than periodontallyhealthy subjects, regardless of HIV infection status(P <0.01; Mann-Whitney test). Interestingly, H-CP+showed significantly more periodontal destruction andinflammation than H+CP+ (P <0.01; Mann-Whitneytest). In contrast, H+CP- subjects presented a signifi-cantly higher mean percentage of sites with BOP thanH-CP- subjects (P <0.01; Mann-Whitney test). Theimmunologic data of the HIV-infected patients showedno significant differences between the H+CP- andH+CP+ groups for all the laboratory parameters eval-uated (P >0.05; Mann-Whitney test). The data in-dicated that most of the HIV-seropositive patientswere immunosuppressed (i.e., they presented lowmean levels of T CD4 lymphocytes [H+CP- = 333 –195 cells/mm3; H+CP+ = 382 – 268 cells/mm3]).Moreover, both groups had very high viral load meancounts (H+CP- = 23,960 – 65,673 copies/ml; H+CP+ =
Table 2.
Demographic, Clinical, and Laboratory Features of the HIV-Seropositive andHIV-Seronegative Subjects With Chronic Periodontitis or Periodontal Health
HIV Seronegative HIV Seropositive
Clinical Parameters Chronic Periodontitis Periodontal Health Chronic Periodontitis Periodontal Health
N 49 51 37 35
Age (mean – SD; years)* 43.4 – 9 34.4 – 11 40.0 – 8 37.0 – 8
Smokers (%)† 28.6 0.0 23.5 32.4
Men (%) 59.2 43.1 70.3 60.0
Mean – SE
PD*‡ 3.3 – 0.12 2.0 – 0.07 2.3 – 0.07 1.8 – 0.06
CAL*‡ 3.8 – 0.16 2.1 – 0.07 2.6 – 0.08 2.0 – 0.07
Mean – SD percentage of sites with:
BOP‡ 44.3 – 25.0 3.7 – 5.7 38.9 – 19.6 14.6 – 12.7
Visible plaque*‡ 62.9 – 23.4 17.4 – 12.0 41.2 – 24.0 20.5 – 18.3
Mean – SD
Neutrophils§ NT NT 2,888 – 1,538 2,829 – 856
T CD4§ NT NT 382 – 268 333 – 195
T CD8§ NT NT 1,182 – 503 1,025 – 547
Viral loadi NT NT 33,071 – 92,139 23,960 – 65,673
NT = not tested.* P <0.01, Kruskal-Wallis test.† P <0.01, x
2 test.‡ P <0.01, analysis of covariance (GLM test), using age and smoking as covariates.§ Cells per cubic millimeter of blood.i Values provided in copies per milliliter of blood.
Clinical and Microbiological Profiles of HIV Brazilians Volume 78 • Number 1
90

33,071 – 92,139 copies/ml). Regarding HAART, lam-ivudine (3TC) was the most frequently used drug(45.9%), followed by zidovudine (azidothymidine[AZT]) (36.5%), ritonavir (28.4%), stavudine (18.9%),lopinavir (17.6%), and efavirens (14.9%). Eighty-nine percent of all HIV-infected patients used combi-nations of two or more drugs. Inaddition, they were taking trimeth-oprim and sulfamethoxazole asprophylaxis for P. carinii pneumo-nitis (data not shown).
Microbiologic DataThe microbial profiles of all HIV-seropositive and HIV-seronega-tive subjects are shown in Figures1 and 2. The 33 bacterial speciestested were ordered accordingto the microbial complexes de-scribed by Socransky et al.20 Ap-proximately 73% of the specieswere more frequently detected inthe non–HIV-infected group, re-gardless of the periodontal status.After controlling for age andsmoking, A. actinomycetemcomi-tans, Actinomyces naeslundii,Capnocytophaga gingivalis, Pre-votella nigrescens, Prevotella mel-aninogenica, and T. forsythensiswere significantly more prevalentin HIV-seronegative than HIV-seropositive patients, whereasAcinetobacter baumannii, Propi-onibacterium acnes, and Strepto-coccus sanguinis were morefrequently detected in the HIV-infected group (P <0.05; Mann-Whitney and GLM tests; adjustedfor multiple comparisons; Fig. 1).Similar results were obtained forthe mean counts of the bacterialspecies (Fig. 2). The periodontalpathogens A. actinomycetemco-mitans, F. nucleatum, P. gingiva-lis, P. nigrescens, P. intermedia,Streptococcus intermedius, Sele-nomonas noxia, and T. forsythen-sis, as well as Actinomycesviscosus, Gemella morbillorum,and Streptococcus spp., werefound in significantly higher meanlevels in the HIV-seronegativecompared to the HIV-seropositivegroup. In contrast, HIV-infectedsubjects presented higher levels
of C. gingivalis, Eubacterium nodatum, and Eikenellacorrodens (P <0.05; Mann-Whitney and GLM tests;adjusted for multiple comparisons).
When the subgingival microbiota of HIV-infectedand non-infected subjects with periodontitis and peri-odontal health was compared, most of the bacterial
Figure 1.Microbial profiles of the mean frequency of 33 oral species examined in subgingival biofilmsamples from 72 HIV-seropositive and 100 HIV-seronegative individuals. The percentage ofsites colonized by each species was computed for each patient and averaged across subjectswithin the groups. The species were ordered according to the microbial complexes described bySocransky et al.18 The Mann-Whitney test was used to determine the significance of differencesbetween groups. Analysis of covariance (GLM test) was performed using age and gender ascovariates. *P < 0.05, Mann-Whitney test, and †P < 0.05, GLM test, using age and smoking ascovariates; adjusted for multiple comparisons.
Figure 2.Microbial profiles of the mean counts (·105) of 33 oral species examined in subgingival biofilmsamples from 72 HIV-seropositive and 100 HIV-seronegative individuals. The percentage of sitescolonized by each species was computed for each patient and averaged across subjects withinthe groups. The species were ordered according to the microbial complexes described bySocransky et al.18 The Mann-Whitney test was used to determine the significance of differencesbetween groups. Analysis of covariance (GLM test) was performed using age and gender ascovariates. *P < 0.05, Mann-Whitney test, and †P < 0.05, GLM test, using age and smoking ascovariates; adjusted for multiple comparisons.
J Periodontol • January 2007 Goncxalves, Soares Ferreira, Souza, Souto, Colombo
91

species were detected in greater prevalence and/orlevels in the H-CP+ group than in the other groups(Tables 3 and 4). However, significant differenceswere observed only for T. forsythensis, P. gingivalis,
S. intermedius, Streptococcus gordonii, and S. noxia,after controlling for age and smoking (P <0.05, GLMtest; adjusted for multiple comparisons). In addition,the species C. gingivalis, E. nodatum, F. nucleatum,
Table 3.
Mean Frequency (– SD) of the 33 Subgingival Species Examined in Biofilm SamplesFrom HIV-Seropositive and HIV-Seronegative Subjects With Chronic Periodontitisand Periodontal Health
HIV Seronegative HIV Seropositive
Subgingival Species* Chronic Periodontitis Periodontal Health Chronic Periodontitis Periodontal Health
A. naeslundii†‡ 53 – 27 33 – 23 26 – 33 21 – 28
A. viscosus 56 – 24 61 – 18 41 – 39 43 – 34
A. odontolyticus (purple) 40 – 21 32 – 25 33 – 36 43 – 38
V. parvula 57 – 21 41 – 21 29 – 32 26 – 33
S. gordonii†‡§i (yellow) 56 – 22 29 – 26 14 – 25 17 – 28
S. intermedius 58 – 23 29 – 28 37 – 45 30 – 46
S. mitis†‡ 55 – 23 23 – 28 30 – 36 21 – 37
S. oralis 63 – 18 45 – 37 40 – 35 50 – 38
S. sanguinis 56 – 26 37 – 36 56 – 31 70 – 35
A. actinomycetemcomitans (green) 40 – 25 27 – 20 34 – 35 34 – 41
C. gingivalis†‡§¶ 44 – 26 39 – 24 10 – 17 13 – 22
E. corrodens†‡§ 47 – 28 48 – 22 8 – 17 21 – 26
C. rectus (orange) 55 – 23 62 – 36 58 – 40 60 – 42
E. nodatum†‡§¶ 29 – 23 25 – 29 10 – 15 2 – 7
F. nucleatum†‡§i 57 – 25 22 – 23 21 – 32 27 – 32
M. micros 51 – 28 27 – 24 46 – 36 38 – 37
P. intermedia†i 58 – 19 18 – 24 37 – 39 38 – 42
P. nigrescens†‡§i 50 – 24 11 – 11 16 – 22 12 – 20
S. constellatus 41 – 19 31 – 28 31 – 27 25 – 32
T. forsythensis†‡i (red) 58 – 27 12 – 15 44 – 36 31 – 35
P. gingivalis†‡i 63 – 19 12 – 19 42 – 40 27 – 33
T. denticola†i 29 – 23 3 – 8 14 – 21 10 – 23
G. morbillorum†‡§ (other species) 54 – 25 45 – 22 11 – 30 11 – 22
L. buccalis 30 – 23 18 – 16 29 – 38 29 – 44
P. acnes 13 – 16 16 – 21 32 – 36 27 – 37
N. mucosa†‡i 43 – 25 68 – 26 32 – 36 15 – 23
P. melaninogenica 27 – 20 25 – 27 24 – 22 27 – 28
S. anginosus 43 – 20 29 – 25 26 – 28 24 – 38
S. noxia†‡i 45 – 30 18 – 19 19 – 30 4 – 11
A. baumannii 20 – 20 12 – 12 32 – 37 48 – 45
E. coli 26 – 19 14 – 14 18 – 28 28 – 44
E. faecalis†‡i¶ 38 – 24 9 – 18 68 – 32 87 – 30
P. aeruginosa 22 – 21 13 – 16 48 – 44 45 – 43
* The species were ordered according to the microbial complexes described by Socransky et al.18
† P <0.05, Kruskal-Wallis test among all groups.‡ P <0.05, analysis of covariance (GLM) among all groups.§ P <0.05, Mann-Whitney test between H-CP+ and H+CP+, using age and smoking as covariates (adjusted for multiple comparisons).i P <0.05, Mann-Whitney test between H-CP+ and H-CP-, using age and smoking as covariates (adjusted for multiple comparisons).¶ P <0.05, Mann-Whitney test between H-CP- and H+CP-, using age and smoking as covariates (adjusted for multiple comparisons).
Clinical and Microbiological Profiles of HIV Brazilians Volume 78 • Number 1
92
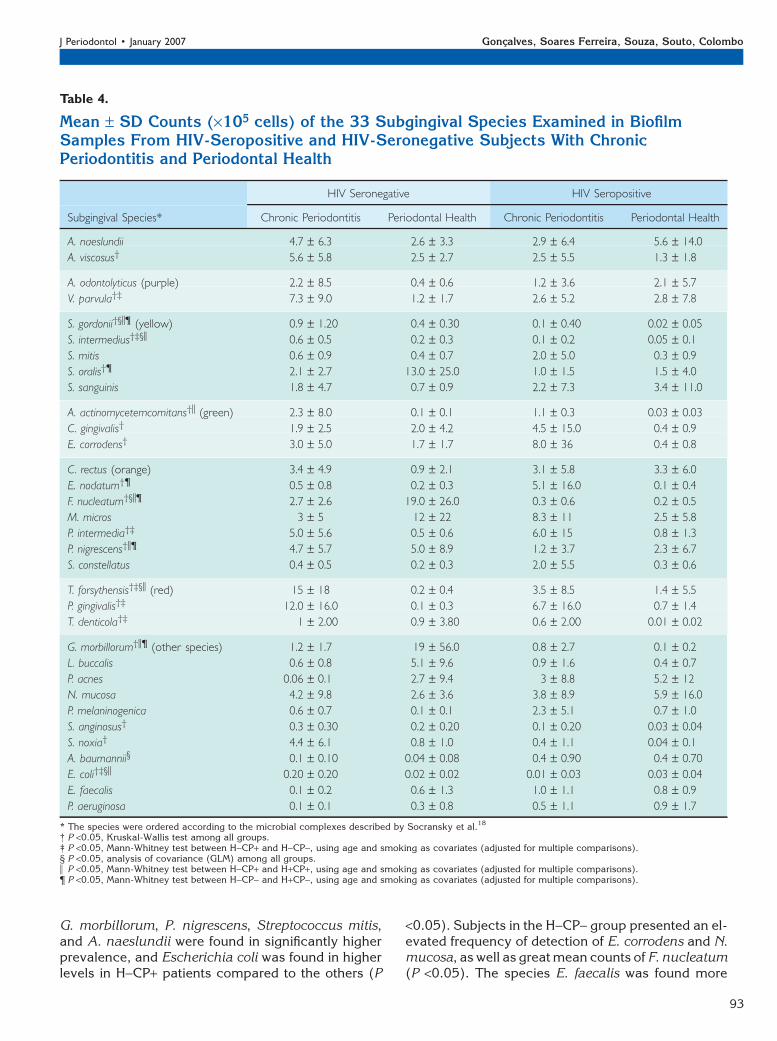
G. morbillorum, P. nigrescens, Streptococcus mitis,and A. naeslundii were found in significantly higherprevalence, and Escherichia coli was found in higherlevels in H-CP+ patients compared to the others (P
<0.05). Subjects in the H-CP- group presented an el-evated frequency of detection of E. corrodens and N.mucosa, as well as great mean counts of F. nucleatum(P <0.05). The species E. faecalis was found more
Table 4.
Mean – SD Counts (·105 cells) of the 33 Subgingival Species Examined in BiofilmSamples From HIV-Seropositive and HIV-Seronegative Subjects With ChronicPeriodontitis and Periodontal Health
HIV Seronegative HIV Seropositive
Subgingival Species* Chronic Periodontitis Periodontal Health Chronic Periodontitis Periodontal Health
A. naeslundii 4.7 – 6.3 2.6 – 3.3 2.9 – 6.4 5.6 – 14.0
A. viscosus† 5.6 – 5.8 2.5 – 2.7 2.5 – 5.5 1.3 – 1.8
A. odontolyticus (purple) 2.2 – 8.5 0.4 – 0.6 1.2 – 3.6 2.1 – 5.7
V. parvula†‡ 7.3 – 9.0 1.2 – 1.7 2.6 – 5.2 2.8 – 7.8
S. gordonii†§i¶ (yellow) 0.9 – 1.20 0.4 – 0.30 0.1 – 0.40 0.02 – 0.05
S. intermedius†‡§i 0.6 – 0.5 0.2 – 0.3 0.1 – 0.2 0.05 – 0.1
S. mitis 0.6 – 0.9 0.4 – 0.7 2.0 – 5.0 0.3 – 0.9
S. oralis†¶ 2.1 – 2.7 13.0 – 25.0 1.0 – 1.5 1.5 – 4.0
S. sanguinis 1.8 – 4.7 0.7 – 0.9 2.2 – 7.3 3.4 – 11.0
A. actinomycetemcomitans†i (green) 2.3 – 8.0 0.1 – 0.1 1.1 – 0.3 0.03 – 0.03
C. gingivalis† 1.9 – 2.5 2.0 – 4.2 4.5 – 15.0 0.4 – 0.9
E. corrodens† 3.0 – 5.0 1.7 – 1.7 8.0 – 36 0.4 – 0.8
C. rectus (orange) 3.4 – 4.9 0.9 – 2.1 3.1 – 5.8 3.3 – 6.0
E. nodatum†¶ 0.5 – 0.8 0.2 – 0.3 5.1 – 16.0 0.1 – 0.4
F. nucleatum†§i¶ 2.7 – 2.6 19.0 – 26.0 0.3 – 0.6 0.2 – 0.5
M. micros 3 – 5 12 – 22 8.3 – 11 2.5 – 5.8
P. intermedia†‡ 5.0 – 5.6 0.5 – 0.6 6.0 – 15 0.8 – 1.3
P. nigrescens†i¶ 4.7 – 5.7 5.0 – 8.9 1.2 – 3.7 2.3 – 6.7
S. constellatus 0.4 – 0.5 0.2 – 0.3 2.0 – 5.5 0.3 – 0.6
T. forsythensis†‡§i (red) 15 – 18 0.2 – 0.4 3.5 – 8.5 1.4 – 5.5
P. gingivalis†‡ 12.0 – 16.0 0.1 – 0.3 6.7 – 16.0 0.7 – 1.4
T. denticola†‡ 1 – 2.00 0.9 – 3.80 0.6 – 2.00 0.01 – 0.02
G. morbillorum†i¶ (other species) 1.2 – 1.7 19 – 56.0 0.8 – 2.7 0.1 – 0.2
L. buccalis 0.6 – 0.8 5.1 – 9.6 0.9 – 1.6 0.4 – 0.7
P. acnes 0.06 – 0.1 2.7 – 9.4 3 – 8.8 5.2 – 12
N. mucosa 4.2 – 9.8 2.6 – 3.6 3.8 – 8.9 5.9 – 16.0
P. melaninogenica 0.6 – 0.7 0.1 – 0.1 2.3 – 5.1 0.7 – 1.0
S. anginosus† 0.3 – 0.30 0.2 – 0.20 0.1 – 0.20 0.03 – 0.04
S. noxia† 4.4 – 6.1 0.8 – 1.0 0.4 – 1.1 0.04 – 0.1
A. baumannii§ 0.1 – 0.10 0.04 – 0.08 0.4 – 0.90 0.4 – 0.70
E. coli†‡§i 0.20 – 0.20 0.02 – 0.02 0.01 – 0.03 0.03 – 0.04
E. faecalis 0.1 – 0.2 0.6 – 1.3 1.0 – 1.1 0.8 – 0.9
P. aeruginosa 0.1 – 0.1 0.3 – 0.8 0.5 – 1.1 0.9 – 1.7
* The species were ordered according to the microbial complexes described by Socransky et al.18
† P <0.05, Kruskal-Wallis test among all groups.‡ P <0.05, Mann-Whitney test between H-CP+ and H-CP-, using age and smoking as covariates (adjusted for multiple comparisons).§ P <0.05, analysis of covariance (GLM) among all groups.i P <0.05, Mann-Whitney test between H-CP+ and H+CP+, using age and smoking as covariates (adjusted for multiple comparisons).¶ P <0.05, Mann-Whitney test between H-CP- and H+CP-, using age and smoking as covariates (adjusted for multiple comparisons).
J Periodontol • January 2007 Goncxalves, Soares Ferreira, Souza, Souto, Colombo
93

often in H+CP- subjects, whereas H+CP-/H+CP+ pa-tients showed significant high mean counts of A. bau-mannii (P <0.05; Kruskal-Wallis and GLM tests;adjusted for multiple comparisons). Comparisonsbetween non–HIV-infected and HIV-infected patientswith chronic periodontitis showed that some peri-odontal pathogens, including A. actinomycetem-comitans, T. forsythensis, P. nigrescens, E. nodatum,and F. nucleatum, were significantly more prevalentin the H-CP+ group (Tables 3 and 4; P <0.05; Mann-Whitney test, adjusted for multiple comparisons).E. faecalis was detected significantly more often inH+CP- than H-CP- subjects (Table 3). Within thenon–HIV-infected groups, patients with periodontitishad significant higher mean frequency and levels ofspecies of the orange and red complexes, as well asE. coli and E. faecalis, compared to individuals withperiodontal health (Tables 3 and 4; P <0.05; Mann-Whitney test, adjusted for multiple comparisons). In-terestingly, no significant differences were observedfor any bacterial species between H+CP- and H+CP+ subjects.
Using the Pearson correlation coefficient, a signifi-cantly positive correlation between the mean fre-quency of T. forsythensis (r = 0.440/PL; r = 0.750/BOP; r = 508/PD; r = 0.460/CAL; P <0.05), P. gingiva-lis (r = 0.470/PL; r = 0.696/BOP; r = 538/PD; r = 0.462/CAL; P <0.05), P. nigrescens (r = 0.524/PL; r = 0.680/BOP; r = 397/PD; r = 0.386/CAL; P <0.05) and all peri-odontal clinical parameters was observed. Con-versely, E. faecalis showed a negative associationwith PL (r = -0.281; P = 0.02) and PD (r = -0.232;P = 0.045; data not shown).
DISCUSSION
Over the last years, studies regarding the oral micro-biota of HIV-infected patients with chronic periodontitishave presented quite conflicting results.1,5,7-10,12-14,21
The present study showed that the non–HIV-infectedpatients presented higher mean prevalence and countsof most of the microorganisms tested compared toHIV-infected subjects under HAART, regardless ofperiodontal status. Of interest, HIV-seropositive sub-jects with chronic periodontitis harbored less bacterialspecies, including several periodontal pathogens,than HIV-seronegative individuals with periodontitis.Similar results were reported by Patel et al.12 andTenenbaum et al.10 Other studies found no significantdifferences between HIV and non–HIV-infected patientsregarding periodontopathogens,7,8,21 whereas Crossand Smith9 showed that these species were more fre-quently detected in HIV-infected subjects with peri-odontitis. Major differences among these studies maybe because of the distinct methods used for detectionand identification of microorganisms; the number of
plaque samples analyzed; the type of periodontal in-fection studied; and the ethnic, geographic, and envi-ronmental features of the population studied.22-24 Themajority of the studies reported in the literature exam-ined very few bacterial species in a limited number ofsubgingival plaque samples. The methods commonlyused included culture,7,8,21 polymerase chain reac-tion,12,21 DNA probes,9,10 and darkfield microscopy.7
The reduced number of samples and species evalu-ated may result in an underestimation or overestima-tion of specific microorganisms on the microbiotaassociated with periodontal disease in any subjectpopulation. Haffajee and Socransky23 showed that,on average, a species was not detected in 68% ofthe positive subjects if only the upper right first molarwas sampled; 60% of subjects if the deepest pocketwas sampled, and 25% of subjects if the four deepestpockets were sampled. These authors concluded thatmultiple plaque samples are needed to minimizefalse-negative rates. Examination of complex micro-bial ecosystems such as the periodontal microbiotarequires the use of techniques that allow the enumer-ation of large numbers of bacterial species in largenumbers of plaque samples.25,26 Therefore, we usedthe checkerboard DNA-DNA hybridization method14
for the detection of 33 microbial taxa, including peri-odontopathogens and species associated with peri-odontal health and opportunistic species.
The microbial profiles observed in the current studymay also reflect the periodontal clinical status of thesubject population. Thus, an accurate definition ofthe disease under study is a very important issue.Some authors27 have used simplified index systemsfor the scoring of periodontal clinical parameters.We performed a full-mouth clinical examination in-cluding PD, CAL, BOP, and PL in all patients. Chronicperiodontitis was defined as the presence of at leastthree sites with PD ‡5 mm and/or CAL ‡4 mm. Basedon these criteria, we observed that most of the sub-jects in the H+CP+ group presented a moderate dis-ease. In fact, this group showed significantly lessperiodontal destruction and inflammation than non–HIV-infected patients with periodontitis. This findingcould explain the lower prevalence and levels of puta-tive periodontal pathogens in this group compared tothe H-CP+ group. As previously reported, several ofthese pathogens, including members of the orangeand red complexes, have been strongly associatedwith clinical measures of periodontal disease, partic-ularly PD and BOP.20,26
Another aspect to be considered in the studies ofthe periodontal microbiota of HIV-infected subjectsrelates to the degree of immunosuppression of theseindividuals. T CD4 counts and HIV viral load havebeen used as markers of immunosuppression inthis population.28 One could expect that severely
Clinical and Microbiological Profiles of HIV Brazilians Volume 78 • Number 1
94

immunosuppressed HIV-infected patients with peri-odontitis would be more readily infected by peri-odontopathogens. In this study, we found that theHIV-infected groups presented low T CD4 mean levelsand high viral load. Despite this, these patients didnot harbor higher counts of periodontal pathogensin relation to HIV-seronegative patients. Conceivably,the establishment of HAART may have provided aprotective effect, keeping the pathogenic subgingivalmicrobiota of these subjects under control, even in acondition of severe immunosuppression.14
The microbiologic studies in HIV-infected patientscould be divided into two phases. Studies publishedbefore the introduction of HAART showed a higherprevalence of periodontitis and periodontal patho-gens in HIV-infected patients compared to non–HIV-infected individuals.9 Nowadays, the establishmentof HAART has resulted in a significant improve-ment in the quality of life of these patients.15 Like-wise, this antiretroviral therapy has also improvedthe clinical periodontal status of HIV-infected pa-tients, associated with a decrease in the incidenceand prevalence of periodontitis and of periodontalpathogens in the subgingival microbiota of these indi-viduals.7,8,10,12,16,21 We reported that the protease in-hibitors ritonavir and lopinavir were frequently used inthis population. Evidence has shown that proteaseinhibitors may also inhibit proteinases of other micro-organisms such as species ofCandida.29 Nevertheless,the effectiveness of these drugs on the inhibition oforal bacteria proteases needs to be further studied.
Species not usually detected in the subgingivalplaque of periodontal lesions have been found to beelevated in the microbiota of HIV-infected patientswith periodontitis.1,5,13 However, the role of these un-usual species in the pathogenesis of periodontitis inthis population is not fully understood. The high prev-alence of opportunistic microorganisms may be asso-ciated to the immunosuppression present in thosepatients. For instance, E. faecalis has been frequentlyencountered in the subgingival microbiota of HIV-infected individuals with levels of T CD4 lymphocytes<200 cells/mm.3,14 Ourdata showed that A. baumannii,E. faecalis, and Pseudomonas aeruginosa were moreprevalent in HIV-infected than non–HIV-infectedpatients, regardless of periodontal status. Of interest,these species tended to be more prevalent in HIV-seropositive patients with periodontal health than withchronic periodontitis. This fact was reinforced bythe negative correlation between E. faecalis and PD(data not shown). E. faecalis has recently emergedas a leading cause of nosocomial infection30 and isquite resistant to several antimicrobial therapies.31
One could speculate that the HIV-infected populationof our study harbored great numbers of these micro-organisms in their subgingival microbiota because of
the fact that those patients are constantly treated inthe hospital environment.
Ecological changes in the composition of the sub-gingival microbiota of HIV-infected individuals mayalso result from the regular use of antimicrobials toprevent opportunistic infections. All HIV-infectedpatients participating in this study were taking tri-methoprim and sulfamethoxazole as prophylaxis forP. carinii pneumonitis. It has been shown that over-treatment with antimicrobials may cause a significantreduction in the proportion of periodontal pathogensin the subgingival microbiota, which in turn may facil-itate the overgrowth of unusual species, as observedin subjects with refractory periodontitis.32
CONCLUSIONS
The data presented in this study support the recentevidence that the long-term use of HAART in an HIV-infected population seems to result in a decrease inthe severity of chronic periodontitis.15,33 Likewise,this antiretroviral therapy may also account for thelower prevalence of putative periodontal pathogensin these patients in relation to HIV-seronegative sub-jects with periodontitis. Moreover, HIV-infected patientsseem to harbor microorganisms not commonly asso-ciated with periodontitis, regardless of clinical peri-odontal status.
ACKNOWLEDGMENTS
This work was supported in part by the Program of Re-search Support for Groups of Excellence (PRONEX),the National Council for Scientific and TechnologicalDevelopment (CNPq), and the Foundation for Re-search Financial Support in the State of Rio de Janeiro(FAPERJ), Rio de Janeiro, Brazil.
REFERENCES1. Zambon JJ, Reynolds HS, Genco RJ. Studies of the
subgingival microflora patients with acquired immuno-deficiency syndrome. J Periodontol 1990;61:699-704.
2. Zambon JJ, Reynolds HS, Smutko J, et al. Are uniquebacterial pathogens involved in HIV-associated peri-odontal diseases? In: Greenspan D, Greenspan JS,eds. Oral Manifestation of HIV Infection. Chicago:Quintessence; 1995:257-262.
3. Murray PA, Winkler JR, Peros WJ, French CK, LippkeJA. DNA probe detection of periodontal pathogens inHIV-associated periodontal lesions. Oral MicrobiolImmunol 1991;6:34-40.
4. Rams TE, Andriolo M Jr., Feik D, Abel SN, McGivernTM, Slots J. Microbiological study of HIV-related peri-odontitis. J Periodontol 1991;62:74-81.
5. Moore LV, Moore WE, Riley C, Brooks CN, BurmeisterJA, Smibert RM. Periodontal microflora of HIV positivesubjects with gingivitis or adult periodontitis. J Peri-odontol 1993;64:48-56.
6. Lucht E, Heimdahl A, Nord CE. Periodontal disease inHIV-infected patients in relation to lymphocyte subsets
J Periodontol • January 2007 Goncxalves, Soares Ferreira, Souza, Souto, Colombo
95

and specific micro-organisms. J Clin Periodontol 1991;18:252-256.
7. Brady LJ, Walker C, Oxford GE, Stewart C, MagnussonI, McArthur W. Oral diseases, mycology and peri-odontal microbiology of HIV-1-infected women. OralMicrobiol Immunol 1996;11:371-380.
8. Tsang CS, Samaranayake LP. Predominant cultivablesubgingival microbiota of health and HIV-infectedethnic Chinese. APMIS 2001;109:117-126.
9. Cross DL, Smith GL. Comparison of periodontal dis-ease in HIV seropositive subjects and controls. (II)Microbiology, immunology and predictors of diseaseprogression. J Clin Periodontol 1995;22:569-577.
10. Tenenbaum H, Elkaim R, Cuisinier F, Dahan M,Zamanian P, Lang JM. Prevalence of six periodontalpathogens detected by DNA probe method in HIV vsnon-HIV periodontitis. Oral Dis 1997;3(Suppl. 1):S153-S155.
11. Scully C, Porter SR, Mutlu S, Epstein JB, Glover S,Kumar N. Periodontopathic bacteria in English HIV-seropositive persons. Aids Patient Care STDS 1999;13:369-374.
12. Patel M, Coogan M, Galpin JS. Periodontal pathogensin subgingival plaque of HIV-positive subjects withchronic periodontitis. Oral Microbiol Immunol 2003;18:199-201.
13. Jabra-Rizk MA, Ferreira SM, Sabet M, Falkler WA,Merz WG, Meiller TF. Recovery of Candida dublinien-sis and other yeast from human immunodeficiencyvirus associated periodontal lesions. J Clin Microbiol2001;39:4520-4522.
14. Goncxalves L deS, Ferreira SM, Silva A Jr., et al. Asso-ciation of TCD4 lymphocyte levels and subgingivalmicrobiota of chronic periodontitis in HIV-infectedBrazilian under HAART. Oral Surg Oral Med OralPathol Oral Radiol Endod 2004;97:196-203.
15. Ryder MI. An update on HIV and periodontal disease.J Periodontol 2002;73:1071-1078.
16. Goncxalves L de S, Ferreira SM, Silva A Jr., Villoria GE,Costinha LH, Colombo AP. Association of T CD4lymphocyte levels and chronic periodontitis in HIV-infected Brazilian patients undergoing highly activeanti-retroviral therapy. Clinical results. J Periodontol2005;76:906-913.
17. Haffajee AD, Cugini MA, Dibart S, Smith C, Kent RLJr., Socransky SS. The effect of SRP on the clinicaland microbiological parameters of periodontal dis-eases. J Clin Periodontol 1997;24:324-334.
18. Socransky SS, Smith CM, Martin L, Paster BJ, DewhirstFE, Levin AE. ‘‘Checkerboard’’ DNA-DNA hybridiza-tion. BioTechniques 1994;17:788-792.
19. Socransky SS, Haffajee AD, Smith C, Dibart S. Rela-tion of counts of microbial species to clinical statusat the sampled site. J Clin Periodontol 1991;18:766-775.
20. Socransky SS, Haffajee AD, Cugini MA, Smith C, KentRL Jr. Microbial complexes in subgingival plaque.J Clin Periodontol 1998;25:134-144.
21. Teanpaisan R, Douglas CW, Nittayananta W. Isolationsand genotyping of black-pigmented anaerobes fromperiodontal sites of HIV-positive and non-infected sub-jects in Thailand. J Clin Periodontol 2001;28:311-318.
22. Loesche WJ, Lopatin DE, Stoll J, van Poperin N,Hujoel PP. Comparison of various detection methodsfor periodontopathic bacteria: Can culture be consid-ered the primary reference standard? J Clin Microbiol1992;30:418-426.
23. Haffajee AD, Socransky SS. Effect of sampling strat-egy on the false-negative rate for detection of selectedsubgingival species. Oral Microbiol Immunol 1992;7:57-59.
24. Loos BG, van Winkelhoff AJ, Dunford RG, et al. Astatistical approach to the ecology of Porphyromonasgingivalis. J Dent Res 1992;71:353-358.
25. Socransky SS, Haffajee AD, Smith C, et al. Use ofcheckerboard DNA-DNA hybridization to study com-plex microbial ecosystems. Oral Microbiol Immunol2004;19:352-362.
26. Socransky SS, Haffajee AD. Periodontal microbialecology. Periodontol 2000 2005;38:135-187.
27. Papapanou PN, Lindhe J. Epidemiology of periodon-tal diseases. In: Lindhe J, Karring T, Lang NP, eds.Clinical Periodontology and Implant Dentistry, vol. 4.Oxford: Blackwell Munksgaard; 2003:50-73.
28. Mellors JW, Munoz A, Giorgi JV, et al. Plasma viralload and CD4+ lymphocytes as prognostic marker ofHIV-1 infection. Ann Intern Med 1997;126:946-954.
29. Munro CA, Hube B. Anti-fungal therapy at the HAARTof viral therapy. Trends Microbiol 2002;10:173-177.
30. Richards MJ, Edwards JR, Culver DH, Gaynes RP.Nosocomial infections in combined medical-surgicalintensive care units in United States. Infect ControlHosp Epidemiol 2000;21:510-515.
31. Peciuliene V, Balciuniene I, Eriksen HM, Haapasalo M.Isolation of Enterococcus faecalis in previously root-filled canals in a Lithuanian population. J Endod 2000;26:593-595.
32. Colombo AP, Haffajee AD, Dewhirst FE, et al. Clinicaland microbiological features of refractory periodontitissubjects. J Clin Periodontol 1998;25:169-180.
33. Tappuni AR, Fleming GJ. The effect of antiretroviraltherapy on the prevalence of oral manifestations inHIV-infected patients: A UK study. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2001;92:623-628.
Correspondence: Dr. Ana Paula V. Colombo, R. Gal.Dionısio, 60 Apt. 604, Humaita/CEP, 22271-050 Rio deJaneiro, RJ, Brazil. E-mail: [email protected].
Accepted for publication August 30, 2006.
Clinical and Microbiological Profiles of HIV Brazilians Volume 78 • Number 1
96