
The Asymptomatic Patient with the Wolff-Parkinson-White Electrocardiogram
Upload
independentCategory
view
4download
0
Prognostic Value of Troponin T and I AmongAsymptomatic Patients With End-Stage Renal Disease
A Meta-Analysis
Nadia A. Khan, MD, MSc, FRCPC; Brenda R. Hemmelgarn, PhD, MD, FRCPC;Marcello Tonelli, MD, MSc, FRCPC; Christopher R. Thompson, MD, CM, FRCPC; Adeera Levin, MD, FRCPC
Background—The prognostic usefulness of troponin enzymes in end-stage renal disease (ESRD) patients is controversial.To resolve this uncertainty of troponin as a prognostic tool, we conducted a systematic review to quantify the associationbetween elevated troponin I or T and long-term total mortality among ESRD patients not suspected of having acutecoronary syndrome.
Methods and Results—We conducted an unrestricted search from the MEDLINE, EMBASE, and DARE bibliographicdatabases to December 2004 using the terms troponin.mp. or exp troponin and exp kidney, exp renal, exp kidney diseaseexp renal replacement therapy. We also manually searched review articles and bibliographies to supplement the search.Studies were included if they were prospective observational studies, used cardiac-specific troponin assays, andevaluated long-term risk of death or cardiac events for asymptomatic ESRD patients. Two authors independentlyabstracted data on study and patient characteristics. Studies findings were stratified according to troponin T or I levels.We used a random-effects model to pool study results and tested for heterogeneity using �2 testing and used funnel-plotinspection to evaluate the presence of publication bias. Data from 28 studies (3931 patients) published between 1999and December 2004 were included in this review. Patients received dialysis for a median duration of 4 years, with amean follow-up of 23 months. From the pooled analysis, elevated troponin T (�0.1 ng/mL) was significantly associatedwith increased all-cause mortality (relative risk, 2.64; 95% CI, 2.17 to 3.20). Although the prognostic effect sizes wereall consistent with a positive relationship between troponin T and mortality, there was significant heterogeneity in themagnitude of these effect sizes (P�0.015). The funnel plot showed evidence of publication bias. Elevated troponin Twas also strongly associated with increased cardiac death. Studies evaluating troponin I included a wide variety of assaysand differing cut points, rendering synthesis of the study findings difficult.
Conclusions—Elevated troponin T (�0.1 ng/mL) identifies a subgroup of ESRD patients who have poor survival and ahigh risk of cardiac death despite being asymptomatic. These findings suggest that troponin T is a promising riskstratification tool and may help frame therapeutic decisions. The clinical interpretation of elevated troponin I levels,however, remain unclear, largely because of the lack of standardization of assays. (Circulation. 2005;112:3088-3096.)
Key Words: kidney � mortality � troponin � meta-analysis
Cardiovascular disease accounts for approximately 50%of deaths in patients with end-stage renal disease
(ESRD).1,2 Identifying those ESRD patients at high risk forfuture events is challenging, because they often have silentischemia or atypical expressions of angina.3–5 Use of ECGdata as diagnostic and prognostic tools is also difficult in thispopulation because of the high prevalence of left ventricularhypertrophy and electrolyte disturbances, which themselvescause ECG abnormalities. Because traditional cardiac riskfactors only partially account for the increased cardiovasculardisease burden of ESRD patients, better tools for risk strati-fication are needed.
Editorial p 3036Clinical Perspective p 3096
Over the past decade, data have emerged that suggest thatelevated cardiac-specific troponins may predict death amongESRD patients without symptoms of acute coronary syn-drome. Although the mechanism of death is unknown, thecardiac-specific troponins T and I are expressed almostexclusively in cardiac muscle among patients with ESRD.6–9
Because troponin levels are widely used, the assays arerelatively inexpensive and unaffected by dialysis10; theselevels are a promising risk stratification tool. However, the
Received May 4, 2005; accepted July 25, 2005.From the Division of Internal Medicine (N.A.K.), Division of Cardiology (C.R.T.), and Division of Nephrology (A.L.), University of British Columbia,
and the Division of Nephrology, University of Calgary, Calgary (B.R.H.), and the Division of Nephrology, University of Alberta, Edmonton (M.T.),Alberta, Canada.
Correspondence to Nadia A. Khan, MD, 620-B 1081 Burrard St, Vancouver, BC, Canada, V6Z 1Y6 E-mail [email protected]© 2005 American Heart Association, Inc.
Circulation is available at http://www.circulationaha.org DOI: 10.1161/CIRCULATIONAHA.105.560128
3088 by guest on June 12, 2016http://circ.ahajournals.org/Downloaded from

overall prognostic usefulness of the troponins remains un-clear. Previous studies, based on retrospective study designsand multiple insensitive assays that cross-react with skeletaltroponin, have produced conflicting results.
To help resolve this uncertainty of troponin as a prognostictool, we conducted a systematic review to quantify theassociation between elevated troponin I or T and long-termtotal mortality among ESRD patients not suspected of havingacute coronary syndrome. To avoid the limitations of previ-ous published reviews,11,12 we included only prospectivestudy designs, excluded studies using assays that cross-reactwith skeletal troponin, stratified the analysis by type oftroponin assay (I versus T), and evaluated the impact of otherprognostic variables besides troponin. To explore the mech-anisms that potentially explain this relationship, we examinedthe additional outcome of cardiovascular death and describedthe relationship between troponin level and cardiovasculardeath in various prognostic subgroups. A defined level ofcardiac-specific troponin elevation that accurately predictedadverse cardiovascular events would be an invaluable asset intherapeutic decision-making for patients with ESRD.
MethodsThe methods used in this review are in accordance with theMeta-Analysis of Observational Studies in Epidemiology: A Pro-posal for Reporting.13
Research ObjectivesThe primary research objective was to determine, by use of system-atic review techniques, whether elevated serum troponin I or Tpredicted higher long-term risk of cardiac death or all-cause mortal-ity among asymptomatic patients with ESRD. A secondary objectivewas to assess whether study outcomes varied systematically withprognostic variables at the study level (history of cardiovasculardisease, diabetes mellitus, or diabetic nephropathy; duration ofdialysis; and length of follow-up).
Studies IncludedTo minimize differences between studies, we imposed the followingmethodological restrictions for the inclusion criteria: (1) prospectiveobservational study design; and studies that (2) evaluated prognosisof patients with abnormal levels of either troponin I or T, (3)examined all-cause mortality or cardiac death, or (4) included onlyasymptomatic patients (ie, no symptoms of acute coronarysyndrome).
We excluded studies based on qualitative assays or those that usedfirst-generation assays of troponin T, which cross-react with skeletalmuscle. Primary authors were contacted if the study did not reportdata amenable to the creation of 2�2 tables. (A rejection log isavailable on request.)
Finding Relevant StudiesTo identify relevant studies, MEDLINE (OVID 1966–December2004), EMBASE (1980–December 2004), the Cochrane review ofsystematic reviews, and the Database of Abstracts of Reviews ofEffects (fourth quarter 2004) were reviewed without languagerestrictions. The search strategy, developed with an experiencedlibrarian, included the following MeSH terms: troponin.mp or exptroponin and exp kidney, exp renal, exp kidney disease exp renalreplacement therapy. We also manually reviewed the bibliographiesof all relevant articles to supplement our search.
Quality Review and Data AbstractionTwo of the reviewers (N.A.K. and B.R.H.) independently reviewedeach study for the quality review and abstracted data on study and
patient characteristics as well as outcomes. Because there is nostandardized quality scoring system for observational studies, thecomponents of the quality review were derived largely from theEgger’s quality checklist for prognostic studies.14 Percentage agree-ment between the 2 reviewers on the 14 items on the quality reviewranged from 77% to 100%. Disagreements were resolved byconsensus.
Statistical AnalysisFor studies evaluating more than 1 troponin I assay,15–17 only themost common manufacturer’s assay was reported. For studiesevaluating more than 1 cut point,18–21 the most common cut pointamong the individual studies was used for analysis to improvebetween-study comparisons. To study the quality of the assays, weused the standards set by the European Society of Cardiology and theAmerican College of Cardiology for the definition of myocardialinjury.22 Troponin levels should exceed the 99th percentile value ofthe reference population to infer myocardial cell injury, the totalimprecision at this decision level should not exceed 10%, and thislevel should be at least 5-fold higher than the lower limit ofdetection.
For assessment of data quality and data abstraction, percentageagreement between the 2 reviewers was calculated. Patient, study,and assay quality components and study description were summa-rized by use of basic descriptive statistics (simple counts and means).Meta-analyses of all outcomes are reported using random-effectsmodels because fixed and random-effects model results were similarand random-effects models tend to produce more conservativeestimates. A �2 test for heterogeneity was used to assess between-study heterogeneity. Pooled relative risks were expressed with 95%CIs. We also evaluated studies for publication bias by visuallyinspecting funnel plots and by the Egger test. From univariateregression analysis, we assessed whether the association betweenelevated troponins and all-cause mortality varied systematically withcertain prognostic variables at the study level (history of cardiovas-cular disease, diabetes mellitus, or diabetic nephropathy; meandurations of dialysis; and length of follow-up). The regression modelrelates the prognostic effect of troponin T to the study levelcovariates, assuming a normal distribution for the residual errorswith both a within-study and an additive between-studies componentof variance, using an estimate that is based on the restrictedmaximum likelihood.
Values for some factors and the outcome of cardiac death were notavailable for several studies. For the outcomes of cardiac death andfor each meta-regression, only studies whereby the information wasavailable were included in the analysis. The analysis was performedby use of STATA statistical software (Version 7, intercooled,STATA Corp).
ResultsStudy SelectionFrom the search strategy, 80 full-text articles were retrieved.Of these, 28 studies met the inclusion criteria and were usedfor this review. The other 52 studies were excluded largelybecause they did not evaluate the prognosis of patients withabnormal levels of troponin (35/52), were retrospective anal-yses (5/52), did not report death or myocardial infarction asan outcome (3/52), evaluated patients with acute coronarysyndrome (7/52), included an acute renal failure cohort(1/52), or evaluated the first-generation troponin T assay(1/52).
Methodological QualityThe 28 prospective observational studies were determined tobe of fair quality. Of the primary studies, 100% had describedindependent, consecutive sampling of their cohort, and 64%had explicitly ascertained that patients did not have any acute
Khan et al Prognostic Value of Troponin Enzymes in End-Stage Renal Disease 3089
by guest on June 12, 2016http://circ.ahajournals.org/Downloaded from
symptoms or signs of acute coronary syndrome. The majorityof studies (75%) reported at least 1 cardiac risk factor, and89% reported baseline cardiovascular history. However, only18% of studies indicated the participants’ baseline medicationuse. All studies described the troponin assays used, and most(82%) used prespecified, rather than data-dependent, cutoffvalues used to define normal and abnormal levels. Troponinvalues were known for all patients. Few studies however,explicitly indicated whether the outcomes or troponin mea-surements were blinded (35%), and only 1 study describedany treatments or management of patients during follow-up.The majority (96%) of primary studies specified the numberof patients lost to follow-up, with most (82%) reporting thatno patients were lost to follow-up, and only 2 studies hadlosses that exceeded 20%.23,24
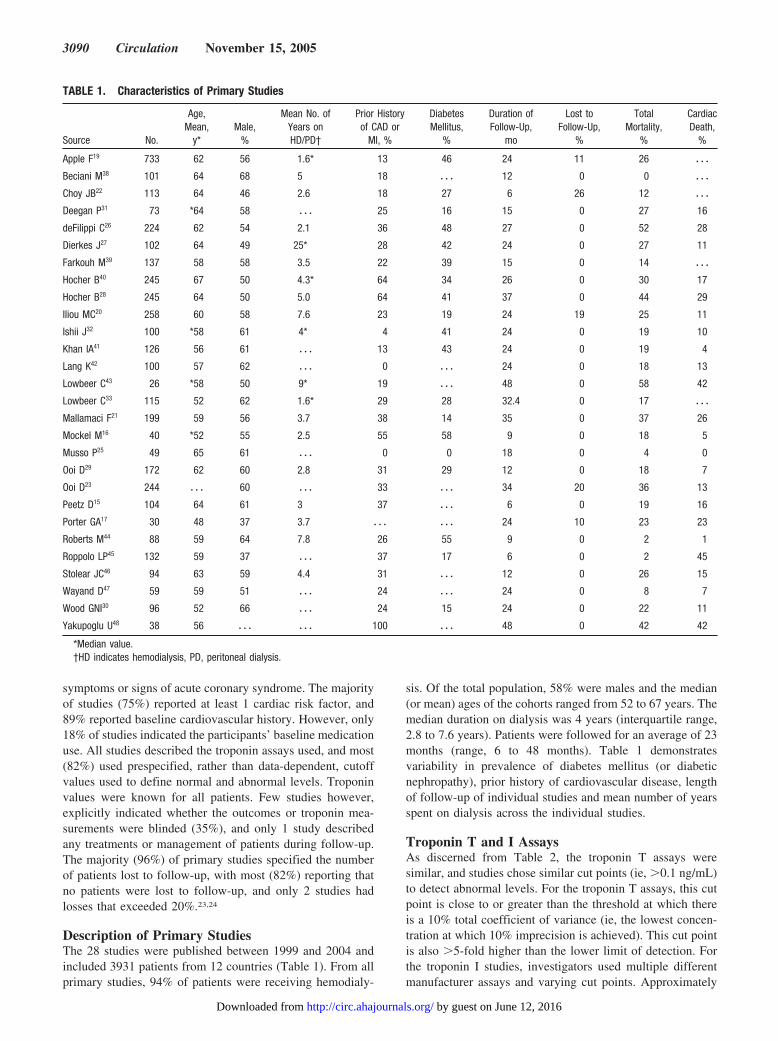
Description of Primary StudiesThe 28 studies were published between 1999 and 2004 andincluded 3931 patients from 12 countries (Table 1). From allprimary studies, 94% of patients were receiving hemodialy-
sis. Of the total population, 58% were males and the median(or mean) ages of the cohorts ranged from 52 to 67 years. Themedian duration on dialysis was 4 years (interquartile range,2.8 to 7.6 years). Patients were followed for an average of 23months (range, 6 to 48 months). Table 1 demonstratesvariability in prevalence of diabetes mellitus (or diabeticnephropathy), prior history of cardiovascular disease, lengthof follow-up of individual studies and mean number of yearsspent on dialysis across the individual studies.
Troponin T and I AssaysAs discerned from Table 2, the troponin T assays weresimilar, and studies chose similar cut points (ie, �0.1 ng/mL)to detect abnormal levels. For the troponin T assays, this cutpoint is close to or greater than the threshold at which thereis a 10% total coefficient of variance (ie, the lowest concen-tration at which 10% imprecision is achieved). This cut pointis also �5-fold higher than the lower limit of detection. Forthe troponin I studies, investigators used multiple differentmanufacturer assays and varying cut points. Approximately
TABLE 1. Characteristics of Primary Studies
Source No.
Age,Mean,
y*Male,
%
Mean No. ofYears onHD/PD†
Prior Historyof CAD or
MI, %
DiabetesMellitus,
%
Duration ofFollow-Up,
mo
Lost toFollow-Up,
%
TotalMortality,
%
CardiacDeath,
%
Apple F19 733 62 56 1.6* 13 46 24 11 26 � � �
Beciani M38 101 64 68 5 18 � � � 12 0 0 � � �
Choy JB22 113 64 46 2.6 18 27 6 26 12 � � �
Deegan P31 73 *64 58 � � � 25 16 15 0 27 16
deFilippi C26 224 62 54 2.1 36 48 27 0 52 28
Dierkes J27 102 64 49 25* 28 42 24 0 27 11
Farkouh M39 137 58 58 3.5 22 39 15 0 14 � � �
Hocher B40 245 67 50 4.3* 64 34 26 0 30 17
Hocher B28 245 64 50 5.0 64 41 37 0 44 29
Iliou MC20 258 60 58 7.6 23 19 24 19 25 11
Ishii J32 100 *58 61 4* 4 41 24 0 19 10
Khan IA41 126 56 61 � � � 13 43 24 0 19 4
Lang K42 100 57 62 � � � 0 � � � 24 0 18 13
Lowbeer C43 26 *58 50 9* 19 � � � 48 0 58 42
Lowbeer C33 115 52 62 1.6* 29 28 32.4 0 17 � � �
Mallamaci F21 199 59 56 3.7 38 14 35 0 37 26
Mockel M16 40 *52 55 2.5 55 58 9 0 18 5
Musso P25 49 65 61 � � � 0 0 18 0 4 0
Ooi D29 172 62 60 2.8 31 29 12 0 18 7
Ooi D23 244 � � � 60 � � � 33 � � � 34 20 36 13
Peetz D15 104 64 61 3 37 � � � 6 0 19 16
Porter GA17 30 48 37 3.7 � � � � � � 24 10 23 23
Roberts M44 88 59 64 7.8 26 55 9 0 2 1
Roppolo LP45 132 59 37 � � � 37 17 6 0 2 45
Stolear JC46 94 63 59 4.4 31 � � � 12 0 26 15
Wayand D47 59 59 51 � � � 24 � � � 24 0 8 7
Wood GNI30 96 52 66 � � � 24 15 24 0 22 11
Yakupoglu U48 38 56 � � � � � � 100 � � � 48 0 42 42
*Median value.†HD indicates hemodialysis, PD, peritoneal dialysis.
3090 Circulation November 15, 2005
by guest on June 12, 2016http://circ.ahajournals.org/Downloaded from

half of these chosen cut points were less than 5-fold higherthan the lower limit of detection, and only 63% were abovethe threshold associated with a 10% total coefficient ofvariation.
Association of Troponin T With Major OutcomesThere were 17 primary studies evaluating the association be-tween troponin T and all-cause mortality. In the forest plot ofindividual prognostic effect sizes in Figure 1, the lower bound-aries of the 95% CIs of almost all trials were greater than 1,
suggesting a consistent association between troponin and all-cause mortality. The two 95% CIs that crossed 1 were also widebecause of the small sample size and low event rates from thesestudies.16,25 From the pooled analysis, elevated troponin T wassignificantly associated with increased all-cause mortality (rela-tive risk RR, 2.64; 95% CI, 2.17 to 3.20). Although theprognostic effect sizes were all consistent with a positiverelationship between troponin T and mortality, there was signif-icant heterogeneity (P�0.015) in the magnitude of these effectsizes. The funnel plot (Figure 2) showed evidence of publication
TABLE 2. Characteristics of the Assays*
Source AssayAssay Name(Generation) Manufacturer
Cutpoint forNormal, ng/mL
Lower Limit ofDetection, ng/mL
TotalCV
90thPercentile
Apple F19 T Elecsys (3rd) Roche �0.1 0.01 7% at 0.07 ng/mL 0.01
Choy JB22 T Elecsys (2nd) Roche �0.1 *0.01 11.2% at 0.1 ng/mL 0.01
Deegan P31 T Elecsys (2nd) Roche �0.1 0.01 �6% at 0.1 ng/mL 0.01
deFilippi C26 T Elecsys (3nd) Roche �0.117 0.01 *10% at 0.03 ng/mL 0.01
Dierkes J27 T Elecsys (2nd) Roche �0.1 0.04 *10% at 0.04 ng/mL 0.01
Hocher B28 T Elecsys (3nd) Roche � � � *0.01 *10% at 0.03 ng/mL 0.01
Iliou MC20 T Elecsys (2nd) Roche �0.1 0.01 9% at 0.1 ng/mL 0.01
Ishii J32 T Elecsys (2nd) Roche �0.1 0.02 13.3% at 0.1 ng/mL 0.01
Lang K42 T Elecsys (2nd) Roche �0.1 *0.01 *10% at 0.04 ng/mL 0.01
Lowbeer C43 T Elecsys (2nd) Roche �0.1 *0.01 4.8% at 0.05 ng/mL 0.01
Mockel M16 T Elecsys (2nd) Roche �0.1 *0.01 *10% at 0.04 ng/mL 0.01
Musso P25 T Elecsys (2nd) Roche �0.10 0.012 *10% at 0.04 ng/mL 0.01
Ooi D23 T Elecsys (2nd, 3rd) Roche �0.1* *0.01 *10% at 0.04 ng/mL 0.01
Peetz D15 T Elecsys (3nd) Roche �0.1 0.01 *10% at 0.03 ng/mL 0.01
Porter GA17 T Elecsys (2nd) Roche �0.1 *0.01 *10% at 0.04 ng/mL 0.01
Roppolo LP45 T Elecsys (2nd) Roche �0.1 *0.01 *10% at 0.04 ng/mL 0.01
Stolear JC46 T Elecsys (3nd) Roche �0.1 0.01 *10% at 0.03 ng/mL 0.01
Wayand D47 T Elecsys (2nd) Roche �0.1 *0.01 9% at 0.1 ng/mL 0.01
Wood GNI47 T Elecsys (2nd) Roche �0.1 0.01 5.8% at 0.47 ng/mL 0.01
Apple F19 I Dimension RxL (2nd) Dade Behring �0.1 0.04 8.5% at 0.6 ng/mL 0.07
Beciani M38 I OPUS plus (2nd) Dade Behring �0.15 0.1 8.9% at 0.13 ng/mL 0.1
Choy JB22 I � � � Dade Behring �0.5 � � � 13.8% at 0.5 ng/mL � � �
Farkouh M39 I Stratus (2nd) Dade Behring �0.1 0.04 *10% at 0.10 ng/mL 0.07
Iliou MC20 I Dimension RxL (2nd) Dade Behring �0.15 0.04 *10% at 0.26 ng/mL 0.07
Ishii J32 I Access (2nd) Beckman-Coulter �0.1 0.03 26.4% at 0.1 ng/mL 0.04
Khan IA41 I Access (2nd) Sanofi �0.03 0.03 *10% at 0.06 ng/mL 0.04
Lang K42 I Stratus (2nd) Dade Behring �0.4 � � � *10% at 0.10 ng/mL 0.07
Mockel M16 I Stratus (2nd) Dade Behring �0.4 0.35 *10% at 0.10 ng/mL 0.07
Musso P25 I Stratus (2nd) Dade Behring �0.3 0.3 *10% at 0.10 ng/mL 0.07
Peetz D15 I Stratus (2nd) Dade Behring �0.1 � � � *10% at 0.10 ng/mL 0.07
Porter GA17 I Stratus (2nd) Dade Behring �0.4 � � � *10% at 0.10 ng/mL 0.07
Roppolo LP45 I Opus Dade Behring �0.5 � � � *10% at 0.90 ng/mL 0.1
Wayand D47 I Stratus (2nd) Dade Behring �0.4 � � � 20.2% at 0.4 ng/mL 0.07
Yakupoglu U48 I Immulite (1st) DPC �2.3 *0.2 *10% at 0.6 ng/mL 0.2
Mockel M16 I Opus (1st) Dade Behring �1.6 � � � *10% at 0.90 ng/mL 0.1
Musso P25 I Access (2nd) Sanofi �0.03 � � � *10% at 0.06 ng/mL 0.04
Peetz D15 I ACS: 180 (1st) Bayer �0.15 � � � *10% at 0.37 ng/mL 0.1
Iliou MC20 I Dimension RxL Dade Behring �0.10 *0.04 *10% at 0.14 ng/mL 0.07
*Refer to data from manufacturers of the troponin assays.49,50
Khan et al Prognostic Value of Troponin Enzymes in End-Stage Renal Disease 3091
by guest on June 12, 2016http://circ.ahajournals.org/Downloaded from

bias. When we removed the largest study, by Apple andcolleagues,19 heterogeneity among the remaining studies was nolonger significant. The study by Apple and colleagues demon-strated a strong association between troponin T and total mor-tality (RR, 1.72; 95% CI, 1.38 to 2.13). Apple’s study was
similar in quality and methodology to the remaining studiesexcept that the patient sample had a shorter mean duration ofdialysis (1.6 years).
There were 8 studies that evaluated the outcome of cardiacdeath. As depicted in Figure 3, each of these primary studies
Figure 1. Forest plot of primary studies evaluating abnormally elevated troponin T and all-cause mortality. Heterogeneity �2�30.55(df�16), P�0.015.
Figure 2. Begg’s funnel plot with 95% CIfor troponin T primary studies.
3092 Circulation November 15, 2005
by guest on June 12, 2016http://circ.ahajournals.org/Downloaded from
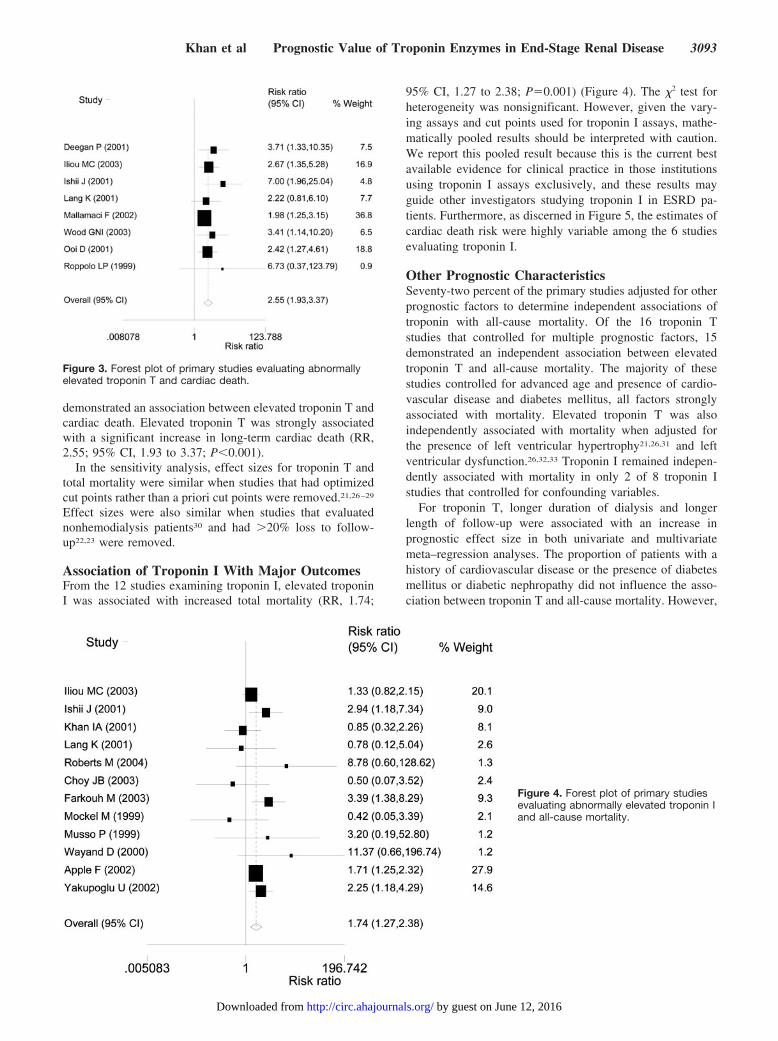
demonstrated an association between elevated troponin T andcardiac death. Elevated troponin T was strongly associatedwith a significant increase in long-term cardiac death (RR,2.55; 95% CI, 1.93 to 3.37; P�0.001).
In the sensitivity analysis, effect sizes for troponin T andtotal mortality were similar when studies that had optimizedcut points rather than a priori cut points were removed.21,26–29
Effect sizes were also similar when studies that evaluatednonhemodialysis patients30 and had �20% loss to follow-up22,23 were removed.
Association of Troponin I With Major OutcomesFrom the 12 studies examining troponin I, elevated troponinI was associated with increased total mortality (RR, 1.74;
95% CI, 1.27 to 2.38; P�0.001) (Figure 4). The �2 test forheterogeneity was nonsignificant. However, given the vary-ing assays and cut points used for troponin I assays, mathe-matically pooled results should be interpreted with caution.We report this pooled result because this is the current bestavailable evidence for clinical practice in those institutionsusing troponin I assays exclusively, and these results mayguide other investigators studying troponin I in ESRD pa-tients. Furthermore, as discerned in Figure 5, the estimates ofcardiac death risk were highly variable among the 6 studiesevaluating troponin I.
Other Prognostic CharacteristicsSeventy-two percent of the primary studies adjusted for otherprognostic factors to determine independent associations oftroponin with all-cause mortality. Of the 16 troponin Tstudies that controlled for multiple prognostic factors, 15demonstrated an independent association between elevatedtroponin T and all-cause mortality. The majority of thesestudies controlled for advanced age and presence of cardio-vascular disease and diabetes mellitus, all factors stronglyassociated with mortality. Elevated troponin T was alsoindependently associated with mortality when adjusted forthe presence of left ventricular hypertrophy21,26,31 and leftventricular dysfunction.26,32,33 Troponin I remained indepen-dently associated with mortality in only 2 of 8 troponin Istudies that controlled for confounding variables.
For troponin T, longer duration of dialysis and longerlength of follow-up were associated with an increase inprognostic effect size in both univariate and multivariatemeta–regression analyses. The proportion of patients with ahistory of cardiovascular disease or the presence of diabetesmellitus or diabetic nephropathy did not influence the asso-ciation between troponin T and all-cause mortality. However,
Figure 3. Forest plot of primary studies evaluating abnormallyelevated troponin T and cardiac death.
Figure 4. Forest plot of primary studiesevaluating abnormally elevated troponin Iand all-cause mortality.
Khan et al Prognostic Value of Troponin Enzymes in End-Stage Renal Disease 3093
by guest on June 12, 2016http://circ.ahajournals.org/Downloaded from

when Apple’s study19 was removed, none of the prognosticfactors were associated with a significant change in prognos-tic effect size.
DiscussionThe primary studies found moderate to large increases in riskof cardiac death and all-cause mortality with elevated tropo-nin T among asymptomatic ESRD patients. Our analysisfound heterogeneity in the estimates of prognosis and evi-dence for publication bias, suggesting that the actual pooledestimate for mortality is more modest. However, even con-sidering the outlier study by Apple et al, the association withtroponin T and mortality remains significant. The sensitivityanalysis and the independent association of troponin Tdespite adjustment for other prognostic factors support theoverall association between elevated troponin T and long-term mortality. A modest association between troponin T andmortality in an asymptomatic population that is otherwisechallenging to risk-stratify may have clinical usefulness.
The fraction of troponin-positive patients with ESRD isinfluenced by the assay technology and the discriminatorvalue chosen. Troponin T assays are produced by a singlemanufacturer, thereby standardizing the assay results. Thedecision cut point for these troponin T studies was generally0.1 ng/mL, above both the reference population threshold(0.01 ng/mL) for cardiac injury and the threshold associatedwith a 10% coefficient of variation, indicating reasonableprecision at the 0.1 ng/mL level. This cut point is alsoconsistent with other major prognostic studies of patientswith acute coronary syndrome with and without chronickidney disease.34,35
For the troponin I studies, investigators used multipledifferent manufacturer assays and varying cut points. Al-
though the troponin I studies were similar in design, patientpopulation, and outcome, this lack of standardization as wellas wide differences in the development of each troponin Iassay gave rise to major concerns about our ability tomathematically synthesize these results. Although individualstudies generally showed an association between troponin Iand long-term all-cause mortality, adjustment for other prog-nostic factors in these studies did not demonstrate an inde-pendent association between troponin I and long-term mor-tality. These findings suggest that troponin I may not be aviable marker for predicting outcomes. Thus, the controversysurrounding the association between troponin I and all-causemortality is justified, and the best available evidence does notclarify this association.
Understanding the mechanisms that underlie elevation introponin T levels among ESRD patients is of particularimportance to help frame appropriate therapeutic decisions.In non-ESRD patients, troponin isoenzymes are an extremelysensitive and specific marker for myocardial cell injury.Previous authors have suggested that the mechanism for a risein troponin among ESRD patients was a result of noncardiaccauses, such as uremic myopathy. However, multiple studieswere unable to identify troponin in noncardiac organs,6–9 andour analysis demonstrates a strong association between ele-vation in troponin T and cardiac death. Troponin T maydetect subclinical myocardial cell injury during the repetitivecardiac stresses provoked by hemodialysis. In addition, otherrelative ischemic stresses might include undetected heartfailure or myocardial remodeling in the setting of left ven-tricular hypertrophy. Several studies reported an associationwith elevated troponin T and left ventricular mass index.36,37
However, as several studies also determined, elevated tropo-nin T remained associated with total mortality despite adjust-ment for the presence of left ventricular hypertrophy or leftventricular dysfunction. In a prespecified subgroup analysis,deFilippi and colleagues26 reported that multivessel coronaryartery disease diagnosed by angiography was more prevalentwith progressively greater quartiles of troponin T. Ouranalysis demonstrates a strong relationship between elevatedtroponin T and cardiac death; however, additional mecha-nisms underlying the increased long-term mortality need tobe explored.
This systematic review serves to clarify the associationbetween troponin T and long-term all-cause mortality inasymptomatic ESRD patients using a large pool of studiesand also identified a strong association between troponin Tand cardiac death, implying a cardiovascular mechanism ofdeath. The association between elevated troponin T andall-cause mortality is concordant with an earlier review thatcombined 4 troponin T studies.12
There are several limitations to this study. The primarystudies had several methodological flaws, including lack ofreporting of blinding and treatment subsequent to entry intothe studies, which may have introduced bias into the results.Although we conducted an unrestricted literature search thatincluded the Database of Abstracts of Reviews of Effects,there was most likely publication bias in the troponin Tanalyses whereby larger trials had lower estimates of prog-nosis compared with smaller studies. This bias would tend to
Figure 5. Forest plot of primary studies evaluating abnormallyelevated troponin I and cardiac death.
3094 Circulation November 15, 2005
by guest on June 12, 2016http://circ.ahajournals.org/Downloaded from

overinflate the pooled estimate of prognosis. However, al-most all studies, including the largest study, by Apple et al,did demonstrate a significant association between troponin Tand mortality. Most troponin levels were ascertained from asingle measurement, rather than an average of repeatedmeasurements over time. Thus, given the recognized mea-surement error of biological variables, the true magnitude ofassociation between troponin and mortality may be greater.Although the primary studies did not each statistically adjustfor identical covariates or all prognostic factors, most studiescontrolled for similar and clinically important prognosticvariables (eg, age, cardiovascular disease, and diabetes mel-litus). Also, an important caveat of this study was that themortality risks were long term, and association with short-term mortality or diagnosis of acute myocardial infarctionusing troponin T is unclear.
ConclusionsIt is often difficult to risk-stratify stable, asymptomatic ESRDpatients without the use of costly noninvasive or invasivecardiac studies. Troponin T is a promising prognostic tool,because elevated levels identify a subset of ESRD patientswho have poor survival and higher risk of cardiac death.Furthermore, the assays are standardized and readily avail-able. The prognostic usefulness of troponin I, however,remain unclear, largely because of the lack of standardizationof assays. Thus, currently, troponin I should not be used toprognosticate risk in this patient population. This analysiscorroborates previous postulates that a cardiovascular causeunderlies the association between mortality and elevatedtroponin T. Future studies are needed to elucidate the specificpathogenic mechanisms, and the impact of potential thera-peutic interventions.
AcknowledgmentsDr Khan is supported by postdoctoral fellowship awards from theCanadian Institutes of Health Research (CIHR) and the MichaelSmith Foundation for Health Research. Drs Hemmelgarn and Tonellihave received New Investigator awards from the Alberta HeritageFoundation for Medical Research and CIHR. The authors thank theUniversity of British Columbia librarian and the administrative staffat the Center for Health Evaluation and Outcome Sciences forassistance in the literature search. We also gratefully appreciate DrsF. Mallamaci and C. Zoccali for providing raw data for thissystematic review and the insightful comments made by Dr AnitaPalepu on an earlier draft of the manuscript.
References1. Herzog CA, Ma JZ, Collins AJ. Poor long-term survival after acute
myocardial infarction among patients on long-term dialysis. N EnglJ Med. 1998;339:799–805.
2. Renal Data System. USRDS 1997 Annual Data Report. Bethesda, Md:National Institute of Diabetes and Digestive and Kidney Diseases; 1997:D1–D51. (NIH publication No. 97-3176.)
3. Aronow WS, Ahn C, Mercando AD, Epstein S. Prevalence of coronaryartery disease, complex ventricular arrhythmias, and silent myocardialischemia and incidence of new coronary events in older persons withchronic renal insufficiency and with normal renal function. Am J Cardiol.2000;86:1142–1143, A9.
4. Nakamura S, Uzu T, Inenaga T, Kimura G. Prediction of coronary arterydisease and cardiac events using electrocardiographic changes duringhemodialysis. Am J Kidney Dis. 2000;36:592–599.
5. Zawada ET Jr, Stinson JB, Done G. New perspectives on coronary arterydisease in hemodialysis patients. South Med J. 1982;75:694–696.
6. Davis GK, Labugger R, Van Eyk JE, Apple FS. Cardiac troponin T is notdetected in Western blots of diseased renal tissue. Clin Chem. 2001;47:782–783.
7. Ricchiuti V, Voss EM, Ney A, Odland M, Anderson PAW, Apple FS.Cardiac troponin T isoforms expressed in renal diseased skeletal musclewill not cause false positive results by the second generation cardiactroponin T assay by Boehringer Mannheim. Clin Chem. 1998;44:1919–1924.
8. Bodor GS, Peroterfield D, Voss EM, Smith S, Apple FS. Cardiac troponinI is not expressed in fetal and healthy or diseased adult human skeletalmuscle tissue. Clin Chem. 1995;41:1710–1715.
9. Haller C, Zehelein J, Remppis A, Muller Bardorff M, Katus HA. Cardiactroponin T in patients with end stage renal disease: absence of expressionin truncal skeletal muscle. Clin Chem. 1998;44:930–938.
10. Donnino MW, Karriem-Norwood V, Rivers EP, Gupta A, Nguyen HB,Jacobsen G, McCord J, Tomlanovich MC. Prevalence of elevatedtroponin I in end-stage renal disease patients receiving hemodialysis.Acad Emerg Med. 2004;11:979–981.
11. Freda BJ, Tang WH, Van Lente F, Peacock WF, Francis GS. Cardiactroponins in renal insufficiency: review and clinical implications. J AmColl Cardiol. 2002;40:2065–2071.
12. Needham DM, Shufelt KA, Tomlinson G, Scholey JW, Newton GE.Troponin I and T levels in renal failure patients without acute coronarysyndrome: a systematic review of the literature. Can J Cardiol. 2004;20:1212–1218.
13. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D,Moher D, Becker BJ, Sipe TA, Thacker SB. Meta-analysis of observa-tional studies in epidemiology: a proposal for reporting. Meta-analysis OfObservational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–2012.
14. Egger M, Smith G, Altman D. Systematic Reviews in Health Care. Ed 2.London, UK: Blackwell BMJ Books; 2001.
15. Peetz D, Schutt S, Sucke B, Faldum A, Wandel E, Hafner G, Lackner KJ.Prognostic value of troponin T, troponin I, and CK-MB mass in patientswith chronic renal failure. Med Klin (Munich). 2003;98:188–192.
16. Mockel M, Schindler R, Knorr L, Muller C, Heller G Jr, Stork TV, FreiU. Prognostic value of cardiac troponin T and I elevations in renal diseasepatients without acute coronary syndromes: a 9-month outcome analysis.Nephrol Dial Transplant. 1999;14:1489–1495.
17. Porter GA, Norton T, Bennett WM. Long term follow up of the utility oftroponin T to assess cardiac risk in stable chronic hemodialysis patients.Clin Lab. 2000;46:469–476.
18. Dierkes J, Domrose U, Westphal S, Ambrosch A, Bosselmann HP,Neumann KH, Luley C. Cardiac troponin T predicts mortality in patientswith end-stage renal disease. Circulation. 2000;102:1964–1969.
19. Apple FS, Murakami MM, Pearce LA, Herzog CA. Predictive value ofcardiac troponin I and T for subsequent death in end-stage renal disease.Circulation. 2002;106:2941–2945.
20. Iliou MC, Fumeron C, Benoit MO, Tuppin P, Calonge VM, Moatti N,Buisson C, Jacquot C. Prognostic value of cardiac markers in ESRD:Chronic Hemodialysis and New Cardiac Markers Evaluation (CHANCE)study. Am J Kidney Dis. 2003;42:513–523.
21. Mallamaci F, Zoccali C, Parlongo S, Tripepi G, Benedetto FA, Cutrupi S,Bonanno G, Fatuzzo P, Rapisarda F, Seminara G, Stancanelli B,Bellanuova I, Cataliotti A, Malatino LS. Troponin is related to leftventricular mass and predicts all-cause and cardiovascular mortality inhemodialysis patients. Am J Kidney Dis. 2002;40:68–75.
22. Apple FS, Wu AHB, Jaffe AS. Implementation of the ESC/ACCguidelines for redefinition of myocardial infarction using cardiac troponinassays with special attention to clinical trial issues. Am Heart J. 2002;144:981–986.
23. Choy JB, Armstrong PW, Ulan RA, Campbell PM, Gourishankar S,Prosser CI, Tymchak WJ. Do cardiac troponins provide prognostic insightin hemodialysis patients? Can J Cardiol. 2003;19:907–911.
24. Ooi DS, Zimmerman D, Graham J, Wells GA. Cardiac troponin Tpredicts long-term outcomes in hemodialysis patients. Clin Chem. 2001;47:412–417.
25. Musso P, Cox I, Vidano E, Zambon D, Panteghini M. Cardiac troponinelevations in chronic renal failure: prevalence and clinical significance.Clin Biochem. 1999;32:125–130.
26. deFilippi C, Wasserman S, Rosanio S, Tiblier E, Sperger H, Tocchi M,Christenson R, Uretsky B, Smiley M, Gold J, Muniz H, Badalamenti J,Herzog C, Henrich W. Cardiac troponin T and C-reactive protein forpredicting prognosis, coronary atherosclerosis, and cardiomyopathy inpatients undergoing long-term hemodialysis. JAMA. 2003;290:353–359.
Khan et al Prognostic Value of Troponin Enzymes in End-Stage Renal Disease 3095
by guest on June 12, 2016http://circ.ahajournals.org/Downloaded from

27. Dierkes J, Domrose U, Westphal S, Ambrosch A, Bosselmann HP,Neumann KH, Luley C. Cardiac troponin T predicts mortality in patientswith end-stage renal disease. Circulation. 2000;102:1964–1969.
28. Hocher B, Ziebig R, Krause R, Asmus G, Neumayer HH, Liefeldt L,Stasch JP. Relaxin is an independent risk factor predicting death in malepatients with end-stage kidney disease. Circulation. 2004;109:2266–2268.
29. Ooi DS, Veinot JP, Wells GA, House AA. Increased mortality in hemo-dialyzed patients with elevated serum troponin T: a one-year outcomestudy. Clin Biochem. 1999;32:647–652.
30. Wood GN, Keevil B, Gupta J, Foley R, Bubtana A, McDowell G, AckrillP. Serum troponin T measurement in patients with chronic renalimpairment predicts survival and vascular disease: a 2 year prospectivestudy. Nephrol Dial Transplant. 2003;18:1610–1615.
31. Deegan PB, Lafferty ME, Blumsohn A, Henderson IS, McGregor E.Prognostic value of troponin T in hemodialysis patients is independent ofcomorbidity. Kidney Int. 2001;60:2399–2405.
32. Ishii J, Nomura M, Okuma T, Minagawa T, Naruse H, Mori Y, IshikawaT, Kurokawa H, Hirano T, Kondo T, Nagamura Y, Ezaki K, Hishida H.Risk stratification using serum concentrations of cardiac troponin T inpatients with end-stage renal disease on chronic maintenance dialysis.Clin Chim Acta. 2001;312:69–79.
33. Lowbeer C, Gutierrez A, Gustafsson SA, Norrman R, Hulting J,Seeberger A. Elevated cardiac troponin T in peritoneal dialysis patients isassociated with CRP and predicts all-cause mortality and cardiac death.Nephrol Dial Transplant. 2002;17:2178–2183.
34. Aviles RJ, Askari AT, Lindahl B, Wallentin L, Jia G, Ohman EM,Mahaffey KW, Newby LK, Califf RM, Simoons ML, Topol EJ, Berger P,Lauer MS. Troponin T levels in patients with acute coronary syndromes,with or without renal dysfunction. N Engl J Med. 2002;346:2047–2052.
35. Ohman EM, Armstrong PW, Christenson RH, Granger CB, Katus HA,Hamm CW, O’Hanesian MA, Wagner GS, Kleiman NS, Harrell FE Jr,Califf RM, Topol EJ. Cardiac troponin T levels for risk stratification inacute myocardial ischemia. GUSTO IIA Investigators. N Engl J Med.1996;335:1333–1341.
36. Lowbeer C, Gustafsson SA, Seeberger A, Bouvier F, Hulting J. Serumcardiac troponin T in patients hospitalized with heart failure is associatedwith left ventricular hypertrophy and systolic dysfunction. Scand J ClinLab Invest. 2004;64:667–676.
37. Mallamaci F, Zoccali C, Parlongo S, Tripepi G, Benedetto FA, Cutrupi S,Bonanno G, Fatuzzo P, Rapisarda F, Seminara G, Stancanelli B,Bellanuova I, Cataliotti A, Malatino LS, Cardiovascular Risk ExtendedEvaluation in Dialysis Investigators. Diagnostic value of troponin T foralterations in left ventricular mass and function in dialysis patients.Kidney Int. 2002;62:1884–1890.
38. Beciani M, Tedesco A, Violante A, Cipriani S, Azzarito M, Sturniolo A,Splendiani G. Cardiac troponin I (2nd generation assay) in chronic hae-
modialysis patients: prevalence and prognostic value. Nephrol DialTransplant. 2003;18:942–946.
39. Farkouh ME, Robbins MJ, Urooj Zafar M, Shimbo D, Davidson KW,Puttappa R, Winston J, Halperin JL, Epstein EM, Patel M, Talor Z,Chesebro JH. Association between troponin I levels and mortality instable hemodialysis patients. Am J Med. 2003;114:224–226.
40. Hocher B, Ziebig R, Altermann C, Krause R, Asmus G, Richter CM,Slowinski T, Sinha P, Neumayer HH. Different impact of biomarkers asmortality predictors among diabetic and nondiabetic patients undergoinghemodialysis. J Am Soc Nephrol. 2003;14:2329–2337.
41. Khan IA, Wattanasuwan N, Mehta NJ, Tun A, Singh N, Singh HK,Vasavada BC, Sacchi TJ. Prognostic value of serum cardiac troponin I inambulatory patients with chronic renal failure undergoing long-termhemodialysis: a two-year outcome analysis. J Am Coll Cardiol. 2001;38:991–998.
42. Lang K, Schindler S, Forberger C, Stein G, Figulla HR. Cardiac troponinshave no prognostic value for acute and chronic cardiac events in asymp-tomatic patients with end-stage renal failure. Clin Nephrol. 2001;56:44–51.
43. Lowbeer C, Gutierrez A, Gustafsson SA, Norrman R, Hulting J,Seeberger A. Elevated cardiac troponin T in peritoneal dialysis patients isassociated with CRP and predicts all-cause mortality and cardiac death.Nephrol Dial Transplant. 2002;17:2178–2183.
44. Roberts MA, Fernando D, Macmillan N, Proimos G, Bach LA, PowerDA, Ratnaike S, Ierino FL. Single and serial measurements of cardiactroponin I in asymptomatic patients on chronic hemodialysis. ClinNephrol. 2004;61:40–46.
45. Roppolo LP, Fitzgerald R, Dillow J, Ziegler T, Rice M, Maisel A. Acomparison of troponin T and troponin I as predictors of cardiac events inpatients undergoing chronic dialysis at a Veteran’s Hospital: a pilot study.J Am Coll Cardiol. 1999;34:448–454.
46. Stolear JC, Georges B, Shita A, Verbeelen D. The predictive value ofcardiac troponin T measurements in subjects on regular haemodialysis.Nephrol Dial Transplant. 1999;14:1961–1967.
47. Wayand D, Baum H, Schatzle G, Scharf J, Neumeier D. Cardiac troponinT and I in end-stage renal failure. Clin Chem. 2000;46:1345–1350.
48. Yakupoglu U, Ozdemir FN, Arat Z, Haberal A, Agca E, Bilgin N. Cantroponin-I predict cardiovascular mortality due to myocardial injury inhemodialysis patients? Transplant Proc. 2002;34:2033–2034.
49. Apple FS, Quist HE, Doyle PJ, Otto AP, Murakami MM. Plasma 99thpercentile reference limits for cardiac troponin and creatine kinase MBmass for use with European Society of Cardiology/American College ofCardiology consensus recommendations. Clin Chem. 2003;49:1331–1336.
50. Panteghini M, Pagani F, Yeo KT, Apple FS, Christenson RH, Dati F,Mair J, Ravkilde J, Wu AH, Committee on Standardization of Markers ofCardiac Damage of the IFCC. Evaluation of imprecision for cardiactroponin assays at low-range concentrations. Clin Chem. 2004;50:327–332.
CLINICAL PERSPECTIVEWhether cardiac-specific troponin enzymes can predict death among patients with end-stage renal disease (ESRD) isunclear. To resolve this uncertainty, we conducted a systematic review to quantify the association between elevatedtroponin I or T and long-term total mortality among ESRD patients not suspected of having acute coronary syndrome. From17 studies, we found that elevated troponin T (�0.1 ng/mL) is significantly associated with increased all-cause mortality(relative risk, 2.64; 95% CI, 2.17 to 3.20). Although the prognostic effect sizes were all consistent with a positiverelationship between troponin T and mortality, there was significant heterogeneity in the magnitude of these effect sizes(P�0.015). Elevated troponin T was also strongly associated with increased cardiac death. Studies evaluating troponin Iincluded a wide variety of assays and differing cut points, rendering synthesis of the study findings difficult. Identifyingthose ESRD patients at high risk for future events is challenging, because they often have silent ischemia or atypicalexpressions of angina. Elevated troponin T (�0.1 ng/mL) identifies a subgroup of ESRD patients who have poor survivaland a high risk of cardiac death despite being asymptomatic. These findings suggest that troponin T is a promising riskstratification tool and may help frame therapeutic decisions. The clinical interpretation of elevated troponin I levels,however, remains unclear, largely because of the lack of standardization of assays.
3096 Circulation November 15, 2005
by guest on June 12, 2016http://circ.ahajournals.org/Downloaded from
Adeera LevinNadia A. Khan, Brenda R. Hemmelgarn, Marcello Tonelli, Christopher R. Thompson and
Renal Disease: A Meta-AnalysisPrognostic Value of Troponin T and I Among Asymptomatic Patients With End-Stage
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2005 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.105.560128
2005;112:3088-3096Circulation.
http://circ.ahajournals.org/content/112/20/3088World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 12, 2016http://circ.ahajournals.org/Downloaded from
Copyright © 2022 FDOKUMEN




















