
Two-dose versus monthly intermittent preventive treatment of malaria with sulfadoxine-pyrimethamine...
10
Two-Dose versus Monthly Intermittent Preventive Treatment of Malaria with Sulfadoxine- Pyrimethamine in HIV-Seropositive Pregnant Zambian Women Davidson H. Hamer, 1 Victor Mwanakasale, 2 William B. MacLeod, 1 Victor Chalwe, 2 Doreen Mukwamataba, 2 Davies Champo, 2 Lawrence Mwananyanda, 2 Roma Chilengi, 5 Lwambwa Mubikayi, 3 Chikuli Kabika Mulele, 4 Modest Mulenga, 2 Donald M. Thea, 1 and Christopher J. Gill 1 1 Center for International Health and Development, Boston University School of Public Health, Boston, Massachusetts; 2 Tropical Diseases Research Centre and 3 Ndola Central Hospital, Ndola, and 4 Mines Hospital, Kitwe, Zambia; 5 Africa Malaria Network Trust, Dar es Salaam, Tanzania (See the editorial commentary by ter Kuile and Steketee and the article by Gill et al., on pages 1574 – 6 and 1577– 84, respectively.) Background. Intermittent preventive treatment of malaria during pregnancy (IPTp) reduces placental infection, maternal anemia, and low birth weight (LBW). However, the optimal dosing regimen in settings in which human immunodeficiency virus (HIV) is highly prevalent among pregnant women remains controversial. Methods. We conducted a randomized, double-blind, placebo-controlled study of IPTp comparing the standard 2-dose sulfadoxine-pyrimethamine (SP) regimen with monthly IPTp among a cohort of HIV-positive pregnant Zambian women. Primary outcomes included placental malaria (by smear and histology) and maternal peripheral parasitemia at delivery. Results. There were no differences between monthly IPTp (n 224) and standard IPTp (n 232) in placental malaria by histopathology (26% vs. 29%; relative risk [RR], 0.90 [95% confidence interval {CI}, 0.64 –1.26]) or placental parasitemia (2% vs. 4%; RR, 0.55 [95% CI, 0.17–1.79]). There also were no differences in maternal anemia, stillbirths, preterm delivery, LBW, or all-cause mortality of infants at 6 weeks. Conclusions. In an area of mesoendemicity in Zambia, monthly SP IPTp was not more efficacious than the standard 2-dose regimen for the prevention of placental malaria or adverse birth outcomes. IPTp policy recommen- dations need to take into account local malaria transmission patterns and the prevalence of HIV. Trial registration. ClinicalTrials.gov identifier: NCT00270530. Plasmodium falciparum malaria during pregnancy is a risk factor for fetal death, prematurity, intrauterine growth retardation, low birth weight (LBW), maternal anemia, and maternal mortality [1–5]. The risk is greater in women infected with HIV, who have higher rates of malarial parasitemia, higher parasite densities and ane- mia rates, and more frequent placental infections and birth complications than do HIV-negative women [6 – 8]. In Zambia, both HIV and malaria are common, so their interaction has important public health implica- tions. An estimated 3.4 million malaria cases, corre- sponding to 308 infections/1000 persons/year, occur in Zambia each year [9]. HIV seroprevalence among preg- nant women ranges from 14.4% in rural locales to 26.8% in urban areas [10]. To address this problem, Zambia’s Ministry of Health currently recommends intermittent preventive treat- ment of malaria during pregnancy (IPTp) using sulfadoxine-pyrimethamine (SP) [11]. However, the optimal dosing regimen in settings in which HIV is prev- alent among pregnant women remains controversial. A Received 20 December 2006; accepted 12 June 2007; electronically published 25 October 2007. Potential conflicts of interest: none reported. Financial support: Cooperative agreement S1954-21/21 between the Associa- tion of Schools of Public Health and the Centers for Disease Control and Preven- tion (Zambia Boston University Malaria Project); National Institute of Allergy and Infectious Diseases, National Institutes of Health (grant K23-AI062208-03 to C.J.G.). Presented in part: 54th Annual Meeting of the American Society of Tropical Medicine and Hygiene, Washington, DC, 11-15 December 2005 (abstract 54). Reprints or correspondence: Dr. Davidson H. Hamer, Center for International Health and Development, Boston University School of Public Health, 5th Fl., 85 E. Concord St., Boston, MA 02118 ([email protected]). The Journal of Infectious Diseases 2007; 196:1585–94 © 2007 by the Infectious Diseases Society of America. All rights reserved. 0022-1899/2007/19611-0004$15.00 DOI: 10.1086/522142 MAJOR ARTICLE Global Theme Issue: Poverty and Human Development IPT in HIV-Positive Pregnant Women ● JID 2007:196 (1 December) ● 1585 by guest on June 16, 2016 http://jid.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Two-dose versus monthly intermittent preventive treatment of malaria with sulfadoxine-pyrimethamine...

Two-Dose versus Monthly IntermittentPreventive Treatment of Malaria with Sulfadoxine-Pyrimethamine in HIV-Seropositive PregnantZambian Women
Davidson H. Hamer,1 Victor Mwanakasale,2 William B. MacLeod,1 Victor Chalwe,2 Doreen Mukwamataba,2
Davies Champo,2 Lawrence Mwananyanda,2 Roma Chilengi,5 Lwambwa Mubikayi,3 Chikuli Kabika Mulele,4
Modest Mulenga,2 Donald M. Thea,1 and Christopher J. Gill1
1Center for International Health and Development, Boston University School of Public Health, Boston, Massachusetts; 2Tropical Diseases ResearchCentre and 3Ndola Central Hospital, Ndola, and 4Mines Hospital, Kitwe, Zambia; 5Africa Malaria Network Trust, Dar es Salaam, Tanzania
(See the editorial commentary by ter Kuile and Steketee and the article by Gill et al., on pages 1574 – 6 and 1577–84, respectively.)
Background. Intermittent preventive treatment of malaria during pregnancy (IPTp) reduces placental infection,maternal anemia, and low birth weight (LBW). However, the optimal dosing regimen in settings in which humanimmunodeficiency virus (HIV) is highly prevalent among pregnant women remains controversial.
Methods. We conducted a randomized, double-blind, placebo-controlled study of IPTp comparing the standard2-dose sulfadoxine-pyrimethamine (SP) regimen with monthly IPTp among a cohort of HIV-positive pregnantZambian women. Primary outcomes included placental malaria (by smear and histology) and maternal peripheralparasitemia at delivery.
Results. There were no differences between monthly IPTp (n � 224) and standard IPTp (n � 232) in placentalmalaria by histopathology (26% vs. 29%; relative risk [RR], 0.90 [95% confidence interval {CI}, 0.64 –1.26]) orplacental parasitemia (2% vs. 4%; RR, 0.55 [95% CI, 0.17–1.79]). There also were no differences in maternal anemia,stillbirths, preterm delivery, LBW, or all-cause mortality of infants at 6 weeks.
Conclusions. In an area of mesoendemicity in Zambia, monthly SP IPTp was not more efficacious than thestandard 2-dose regimen for the prevention of placental malaria or adverse birth outcomes. IPTp policy recommen-dations need to take into account local malaria transmission patterns and the prevalence of HIV.
Trial registration. ClinicalTrials.gov identifier: NCT00270530.
Plasmodium falciparum malaria during pregnancy is a
risk factor for fetal death, prematurity, intrauterine
growth retardation, low birth weight (LBW), maternal
anemia, and maternal mortality [1–5]. The risk is greater
in women infected with HIV, who have higher rates of
malarial parasitemia, higher parasite densities and ane-
mia rates, and more frequent placental infections and
birth complications than do HIV-negative women [6–8].
In Zambia, both HIV and malaria are common, so
their interaction has important public health implica-
tions. An estimated 3.4 million malaria cases, corre-
sponding to 308 infections/1000 persons/year, occur in
Zambia each year [9]. HIV seroprevalence among preg-
nant women ranges from 14.4% in rural locales to 26.8%
in urban areas [10].
To address this problem, Zambia’s Ministry of Health
currently recommends intermittent preventive treat-
ment of malaria during pregnancy (IPTp) using
sulfadoxine-pyrimethamine (SP) [11]. However, the
optimal dosing regimen in settings in which HIV is prev-
alent among pregnant women remains controversial. A
Received 20 December 2006; accepted 12 June 2007; electronically published25 October 2007.
Potential conflicts of interest: none reported.Financial support: Cooperative agreement S1954-21/21 between the Associa-
tion of Schools of Public Health and the Centers for Disease Control and Preven-tion (Zambia Boston University Malaria Project); National Institute of Allergy andInfectious Diseases, National Institutes of Health (grant K23-AI062208-03 to C.J.G.).
Presented in part: 54th Annual Meeting of the American Society of TropicalMedicine and Hygiene, Washington, DC, 11-15 December 2005 (abstract 54).
Reprints or correspondence: Dr. Davidson H. Hamer, Center for InternationalHealth and Development, Boston University School of Public Health, 5th Fl., 85 E.Concord St., Boston, MA 02118 ([email protected]).
The Journal of Infectious Diseases 2007; 196:1585–94© 2007 by the Infectious Diseases Society of America. All rights reserved.0022-1899/2007/19611-0004$15.00DOI: 10.1086/522142
M A J O R A R T I C L EGlobal Theme Issue: Poverty and Human Development
IPT in HIV-Positive Pregnant Women ● JID 2007:196 (1 December) ● 1585
by guest on June 16, 2016http://jid.oxfordjournals.org/
Dow
nloaded from

subgroup analysis of HIV-positive pregnant women receiving
IPTp in Kenya suggested that, for HIV-positive women,
monthly SP was superior to 2 doses given once each in the latter
2 trimesters [12]. Given the post-hoc nature of this observation
and its evident public health implications, we conducted a trial
comparing the standard 2-dose SP IPTp regimen (S-IPTp) with
intensive monthly SP IPTp (I-IPTp) among a cohort of HIV-
positive pregnant Zambian women.
METHODS
Between January 2003 and October 2004, we conducted a ran-
domized, double-blind, placebo-controlled study. Our primary
outcomes were histological evidence of acute or chronic placen-
tal malaria, placental parasitemia, and maternal peripheral par-
asitemia at delivery. Secondary outcomes included birth weight
(including LBW), prematurity, cord blood parasitemia, sponta-
neous miscarriage, stillbirth or neonatal death, neonatal jaun-
dice, maternal anemia at delivery, third trimester maternal ane-
mia, severe maternal adverse reactions to SP, and symptomatic
maternal malarial infection during pregnancy.
Study setting. The study was conducted at 3 district health
clinics (Masala, Lubuto, and Chipokota-Mayamba) in Ndola, an
urban center in the Copperbelt Province of Zambia (population,
347,757) [13]. Malaria transmission in Ndola peaks during the
rainy season (November–March). Anopheles gambiae and An.
funestus are the main mosquito vectors.
Starting in December 2003, coincident with the start of our
study, the Ndola District Health Management Team launched a
campaign of indoor residual spraying (IRS) with pyrethroids
and DDT within the Masala catchment area but not in the other 2
study clinic neighborhoods (Lubuto and Chipokota-Mayamba).
During the study period, the National Malaria Control Center
carried out annual rounds of in vivo efficacy testing of SP in
children �5 years old at sentinel sites throughout Zambia. The
adequate clinical response to SP was 92% in 2002 in Mpongwe, a
district in the Copperbelt Province near Ndola [14]. In 2003 and
2004, testing was not performed in Mpongwe, but data from the
nearest sentinel site, Mansa, revealed a rise in SP total treatment
failure rates, from 14.5% in 2003 to 37% in 2004 [15].
Sample size. Assuming a frequency of smear-positive pla-
cental malaria among HIV-positive women of 25% (as in Parise
et al.’s study [12]) and a 15% decline in placental malaria in the
intervention group, with an � of 5% and 80% power, 113 HIV-
infected women were needed in each arm. Although Parise et al.
enrolled only primigravidae and secundigravidae, we assumed
similar rates of placental infection among women of all gravidity
[16]. Assuming that 90% of those delivering in the health facility
would have their placentas collected and 50% loss to follow-up
[12], our sample size target was 454 subjects.
Enrollment. At the start of the study, we helped expand vol-
untary counseling and testing (VCT) for HIV and nevirapine
availability at each clinic. HIV-positive women were offered ne-
virapine for prevention of mother-to-child transmission of HIV.
Potential participants were approached about the study only af-
ter completing VCT.
HIV-1–seropositive pregnant women of all gravidities who
were between 16 and 28 weeks of gestation, were free of an acute
illness requiring hospitalization, and were willing to deliver at a
study clinic were eligible. Exclusion criteria included age �18
years, prior enrollment in this study, residence outside of or in-
tent to move out of the clinics’ catchment area, severe anemia
(hemoglobin [Hb] level �6 g/dL), history of allergic reactions to
sulfa drugs, prior major pregnancy complications (e.g., breech
presentation, severe preeclampsia, and �2 cesarean sections),
and major illnesses likely to influence pregnancy outcomes.
To minimize stigma, we initially offered enrollment to every
tenth HIV-negative woman and later to every fifth HIV-negative
woman. HIV-negative women were not randomized but re-
ceived the standard 2-dose regimen.
Randomization. HIV-positive participants were assigned
sequential identification numbers during enrollment corre-
sponding to a sealed package of study drugs. Each pack con-
tained 6 medication sheets, representing single monthly doses of
medication or placebo. Each sheet consisted of 3 blister-packed
tablets. Active tablets contained a total of 500 mg of sulfadoxine
and 25 mg of pyrimethamine. Roche Pharmaceuticals prepared
the study drugs and placebos in individual patient drug packs
according to our randomization scheme.
HIV-positive mothers were randomized in blocks of 20 to 1 of
2 dosing schedules: 1 treatment course of SP per month (I-IPTp)
or 1 course of SP per trimester (S-IPTp). Randomization codes
were retained by the study statistician and stored in a locked
cabinet at Boston University. The code was broken when data
collection was complete and preliminary blinded analyses had
been performed. To ensure that all mothers received at least the
2-dose SP regimen, the first and fourth monthly sheets of each
pack always contained active SP, whereas sheets 2, 3, 5, and 6
contained SP (I-IPTp) or placebo (S-IPTp). Pregnant women
who began the study at weeks 25 or 26 of gestation were admin-
istered their second SP treatment course at their second
follow-up visit (i.e., 2 months after their initial study visit).
For quality control, we submitted 2 unused sets of drugs cor-
responding to the placebo and intervention arms to the World
Health Organization’s Centre for Quality Assurance of Medi-
cines (Potchefstroom, South Africa). Analysis by high-pressure
liquid chromatography confirmed that the intervening month
(months 2, 3, 5, and 6) tablets contained either SP or placebo,
whereas months 1 and 4 contained SP, as expected.
Study procedures. At baseline, we collected a mother’s de-
mographic information, measured fundal height, and obtained a
drop of blood by fingerprick to measure Hb level and for prep-
aration of thick and thin blood smears. Mothers were dewormed
with mebendazole, received their first study treatment, and were
1586 ● JID 2007:196 (1 December) ● Hamer et al.
by guest on June 16, 2016http://jid.oxfordjournals.org/
Dow
nloaded from

provided with monthly folate and iron supplements. At monthly
follow-up visits, participants completed a questionnaire, under-
went an obstetrical examination, and had measurements of tem-
perature and Hb. Study drug was administered monthly under
direct observation until mothers reached 36 weeks of gestation.
No doses were administered after 36 weeks because of the risk of
neonatal kernicterus from sulfonamides. Pregnant women with
documented fever or history of recent fever and a positive ma-
laria smear were treated with oral quinine. Team members at-
tempted to contact women if they were �2 days overdue for a
scheduled follow-up visit.
At delivery, we measured maternal axillary temperature and
maternal and infant Hb levels, obtained biopsy samples from the
maternal and fetal sides of the placenta, and prepared thick
blood smears of maternal peripheral blood, of maternal and fetal
sides of the placenta, and of fetal cord blood. We measured in-
fant weight and estimated the infant’s gestational age using the
Dubowitz criteria [17]. Mothers returned for follow-up visits at
1 and 6 weeks post partum for determination of the infant’s vital
status and screening for residual drug adverse effects.
Laboratory analyses. A 2-step HIV testing protocol using
Determine HIV 1/2 (Abbott Laboratories) as the screening test
and Capillus (Cambridge Biotech) as the confirmatory test was
performed, with the Bionor assay (Skien) used for indeterminate
or discordant results.
Hb levels were measured using a HemoCue machine
(HemoCue AB). Thick smears were prepared with a single drop
of peripheral or placental blood and air dried. Slides were fixed
in methanol and stained in 10% Giemsa at the Tropical Diseases
Research Centre (TDRC) and were read independently by 2 par-
asitologists. The parasite density per microliter was the number
of parasites per 200 leukocytes times 40 or the number per 500
leukocytes times 16 if no parasites were seen after counting 200
cells [18]. Slides were declared to be negative if no parasites were
seen after counting 500 leukocytes.
Two 1-cm-wide full-thickness wedge placental biopsy sam-
ples were taken by measuring 5 cm centrifugally from the cord.
Samples were fixed in 20% formalin and embedded in paraffin
wax. Sections that were 3 �m thick were cut using a Rotary mi-
crotome (Lipshaw Manufacturing), fixed to a glass slide, and
dehydrated in sequential ethanol baths. The slides were then
stained in 0.1% hematoxylin and 1% eosin stains for 5 and 1
min, respectively.
Each slide was read independently by 2 Zambian pathologists
(L.M. and C.K.M.). Slides were interpreted according to the clas-
sification scheme shown in table 1. Because pathological evi-
dence of malaria might not be uniformly distributed throughout
a placental sample, we assigned the interpretation with highest
malaria intensity as the final classification. Thus, if a slide from a
given section was interpreted as CN by one pathologist and as C3
on another section or by the second pathologist, the final reading
was classified as C3.
Definitions. Pregnant women who presented with fever or a
recent history of fever plus any level of parasitemia were catego-
rized as having symptomatic uncomplicated malaria. Maternal
peripheral parasitemia was defined as asexual stage parasites in
thick smears made from maternal venous blood; placental ma-
laria as positive histological evidence of malaria (C1, C2, or C3);
placental parasitemia as the presence of parasites in thick smears
of maternal-side placental blood; anemia as Hb level �11 g/dL;
severe anemia as Hb level �6 g/dL; LBW as birth weight �2500
g; prematurity as �37 weeks of gestation by the Dubowitz crite-
ria; stillborn as dead delivery after 28 weeks of gestation; spon-
taneously aborted as delivery before 28 weeks; and neonatal
death as death occurring between days 0 ansud 28 post partum.
Statistical analysis. Data were double-entered into CS-Pro
(United States Census Bureau). We used SAS (version 8.2; SAS
Institute) for all analyses. Mothers with twins were excluded
from the analysis of birth outcomes. We compared the propor-
tions of the main study outcomes by calculating relative risks
(RRs) and 95% confidence intervals (CIs) and compared con-
tinuous variables using independent t tests. Concordance be-
tween the pathologists’ readings was estimated with the � statistic.
Table 1. Pathological criteria used for staging of placental malaria.
Stage (code) Definition
Acute/active infection (C1) (1) Presence of parasitized intervillous erythrocytes(2) Presence of malaria pigment in intervillous erythrocytes(3) Presence of malaria pigment–laden intervillous monocyte/macrophage infiltrates
Recent infection (C2) (1) Absence of parasites(2) Presence of malaria pigment in intervillous erythrocytes, fibrin, or intervillous neutrophils(3) Presence of intervillous monocyte/macrophage infiltrates
Past infection (C3) (1) Absence of parasites(2) Presence of malaria pigment in fibrin only(3) Absence of pigmented intervillous erythrocytes(4) Absence of monocyte/macrophage infiltrates
Uninfected (CN) (1) Absence of any parasites or malaria pigment in cells or fibrin
IPT in HIV-Positive Pregnant Women ● JID 2007:196 (1 December) ● 1587
by guest on June 16, 2016http://jid.oxfordjournals.org/
Dow
nloaded from
Gestational age was estimated from the last menstrual period
(LMP) using a pregnancy calculator. Dubowitz scores were
translated into gestational age on the basis of the original regres-
sion equation Y � gestational age in weeks � 0.2642x � 24.595,
where x � the Dubowitz score [17]. If the discrepancy between
the LMP- and Dubowitz-derived gestational age was �14 days,
the Dubowitz score was used.
Ethical considerations. The Institutional Review Board of
the Boston University Medical Center and the TDRC Ethics
Committee approved the study. A data safety monitoring board
consisting of 2 experts in international child and maternal health
research and a statistician conducted a blinded interim safety
analysis contrasting rates of serious adverse events midway
through study enrollment.
RESULTS
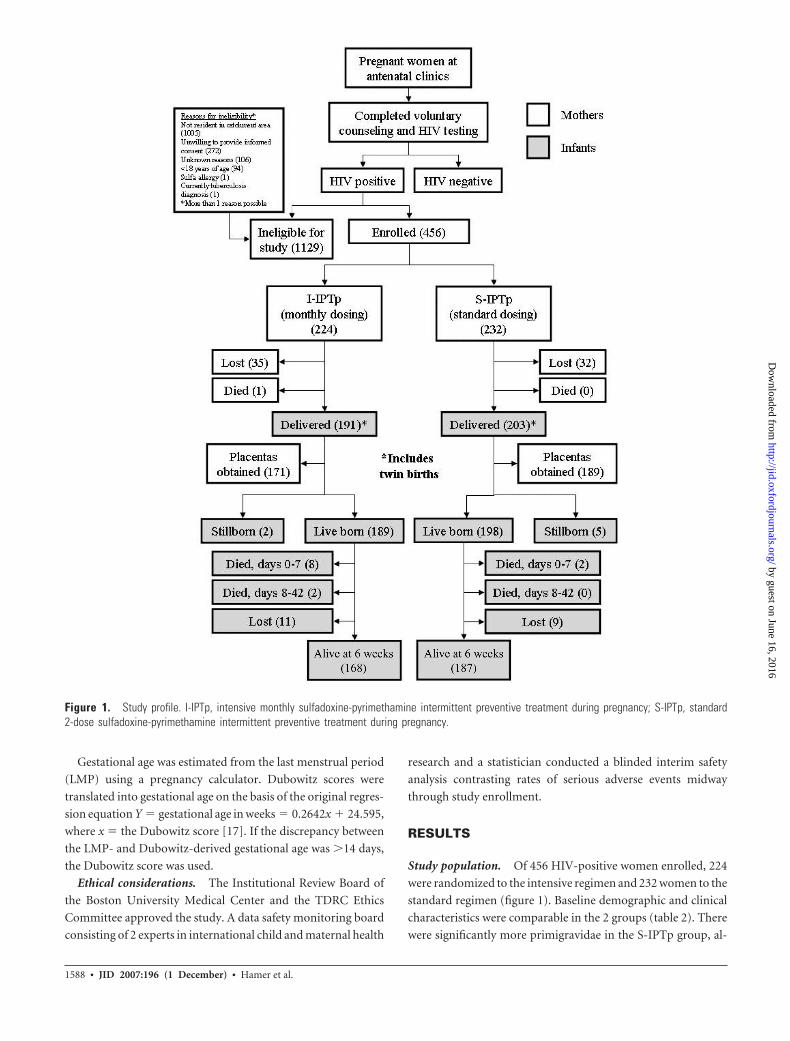
Study population. Of 456 HIV-positive women enrolled, 224
were randomized to the intensive regimen and 232 women to the
standard regimen (figure 1). Baseline demographic and clinical
characteristics were comparable in the 2 groups (table 2). There
were significantly more primigravidae in the S-IPTp group, al-
Figure 1. Study profile. I-IPTp, intensive monthly sulfadoxine-pyrimethamine intermittent preventive treatment during pregnancy; S-IPTp, standard2-dose sulfadoxine-pyrimethamine intermittent preventive treatment during pregnancy.
1588 ● JID 2007:196 (1 December) ● Hamer et al.
by guest on June 16, 2016http://jid.oxfordjournals.org/
Dow
nloaded from
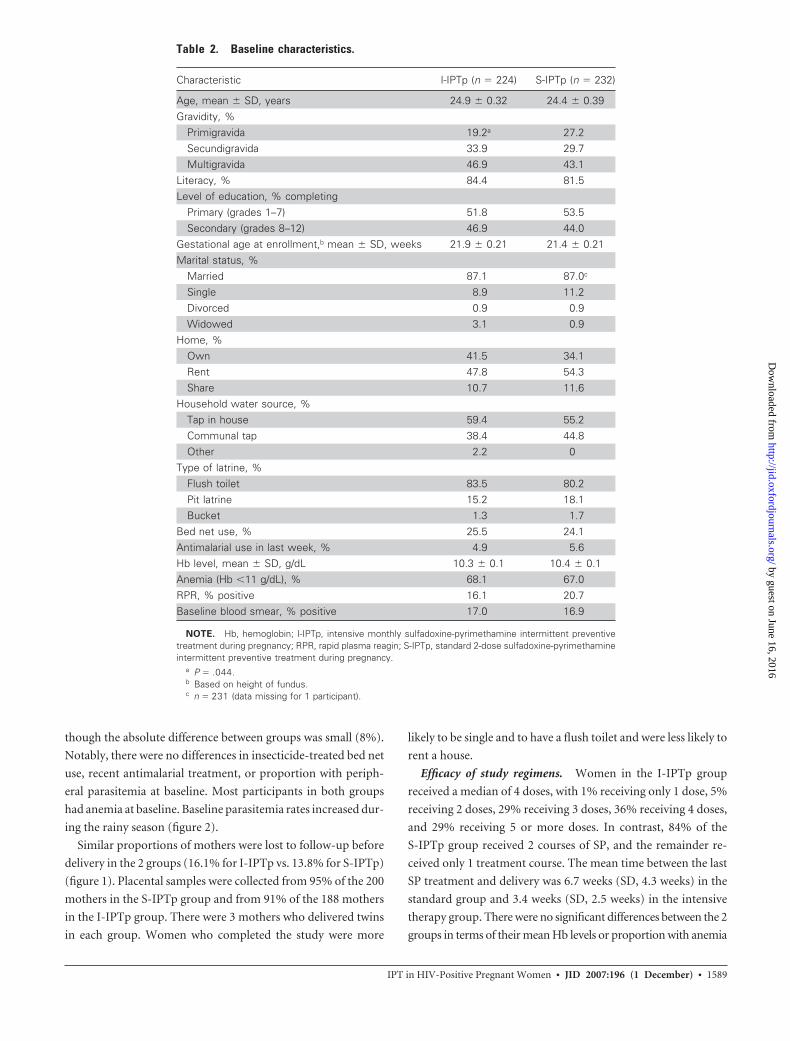
though the absolute difference between groups was small (8%).
Notably, there were no differences in insecticide-treated bed net
use, recent antimalarial treatment, or proportion with periph-
eral parasitemia at baseline. Most participants in both groups
had anemia at baseline. Baseline parasitemia rates increased dur-
ing the rainy season (figure 2).
Similar proportions of mothers were lost to follow-up before
delivery in the 2 groups (16.1% for I-IPTp vs. 13.8% for S-IPTp)
(figure 1). Placental samples were collected from 95% of the 200
mothers in the S-IPTp group and from 91% of the 188 mothers
in the I-IPTp group. There were 3 mothers who delivered twins
in each group. Women who completed the study were more
likely to be single and to have a flush toilet and were less likely to
rent a house.
Efficacy of study regimens. Women in the I-IPTp group
received a median of 4 doses, with 1% receiving only 1 dose, 5%
receiving 2 doses, 29% receiving 3 doses, 36% receiving 4 doses,
and 29% receiving 5 or more doses. In contrast, 84% of the
S-IPTp group received 2 courses of SP, and the remainder re-
ceived only 1 treatment course. The mean time between the last
SP treatment and delivery was 6.7 weeks (SD, 4.3 weeks) in the
standard group and 3.4 weeks (SD, 2.5 weeks) in the intensive
therapy group. There were no significant differences between the 2
groups in terms of their mean Hb levels or proportion with anemia
Table 2. Baseline characteristics.
Characteristic I-IPTp (n � 224) S-IPTp (n � 232)
Age, mean � SD, years 24.9 � 0.32 24.4 � 0.39Gravidity, %
Primigravida 19.2a 27.2Secundigravida 33.9 29.7Multigravida 46.9 43.1
Literacy, % 84.4 81.5Level of education, % completing
Primary (grades 1–7) 51.8 53.5Secondary (grades 8–12) 46.9 44.0
Gestational age at enrollment,b mean � SD, weeks 21.9 � 0.21 21.4 � 0.21Marital status, %
Married 87.1 87.0c
Single 8.9 11.2Divorced 0.9 0.9Widowed 3.1 0.9
Home, %Own 41.5 34.1Rent 47.8 54.3Share 10.7 11.6
Household water source, %Tap in house 59.4 55.2Communal tap 38.4 44.8Other 2.2 0
Type of latrine, %Flush toilet 83.5 80.2Pit latrine 15.2 18.1Bucket 1.3 1.7
Bed net use, % 25.5 24.1Antimalarial use in last week, % 4.9 5.6Hb level, mean � SD, g/dL 10.3 � 0.1 10.4 � 0.1Anemia (Hb �11 g/dL), % 68.1 67.0RPR, % positive 16.1 20.7Baseline blood smear, % positive 17.0 16.9
NOTE. Hb, hemoglobin; I-IPTp, intensive monthly sulfadoxine-pyrimethamine intermittent preventivetreatment during pregnancy; RPR, rapid plasma reagin; S-IPTp, standard 2-dose sulfadoxine-pyrimethamineintermittent preventive treatment during pregnancy.
a P � .044.b Based on height of fundus.c n � 231 (data missing for 1 participant).
IPT in HIV-Positive Pregnant Women ● JID 2007:196 (1 December) ● 1589
by guest on June 16, 2016http://jid.oxfordjournals.org/
Dow
nloaded from

during monthly antenatal visits (data not shown). Symptomatic
uncomplicated malaria occurred less frequently in the I-IPTp
group; this difference was significant (P � .048) (table 3).
Placental biopsy samples were available for 78% (355/456) of
the participants. At delivery, the proportion of women was sim-
ilar in the 2 groups for placental malaria, any evidence of placen-
tal malaria by histology (C1�C2�C3), or placental parasitemia
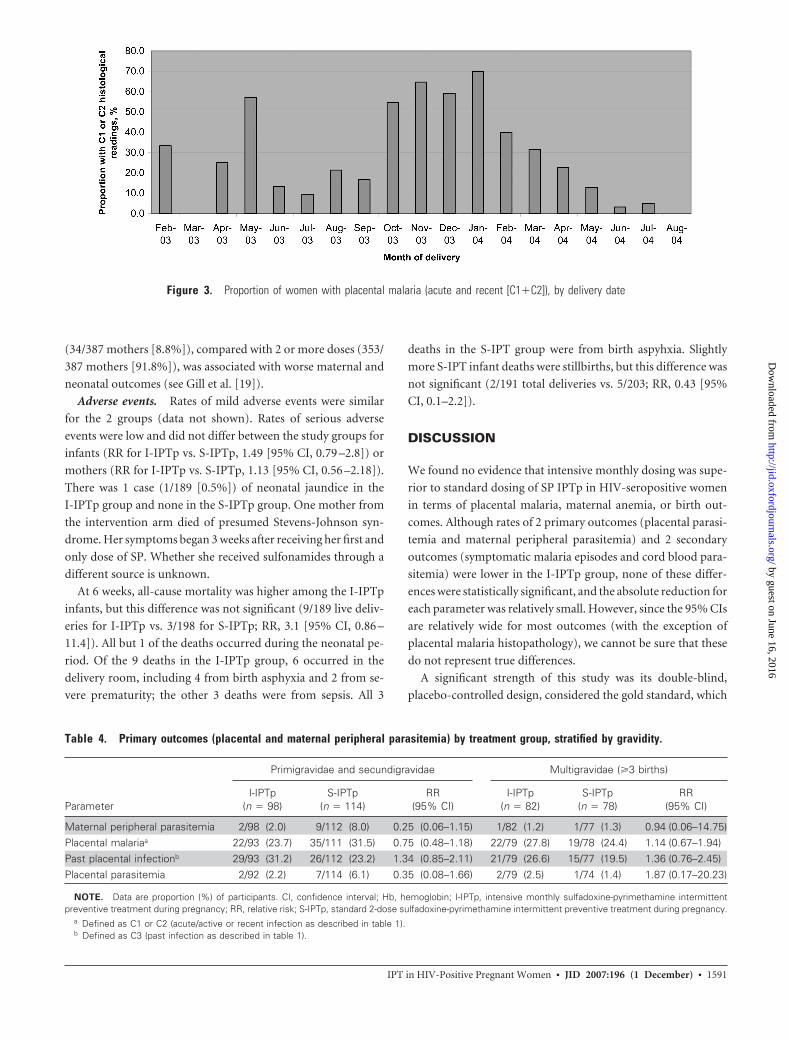
(table 3). Substantially more women delivering around the rainy
season had histological evidence of placental malaria (figure 3).
Similar seasonal trends were noted for placental parasitemia
(data not shown). There were also no differences for maternal
anemia at delivery, birth weight, or proportion with LBW.
Stratification of the study participants by gravidity revealed that
primigravidae and secundigravidae had a lower proportion of ma-
ternal parasitemia, placental malaria, and placental parasitemia in
the I-IPTp than the S-IPTp group (table 4); however, none of these
differences was statistically significant. There were no differences
for any of these outcomes between the multigravidae in the 2
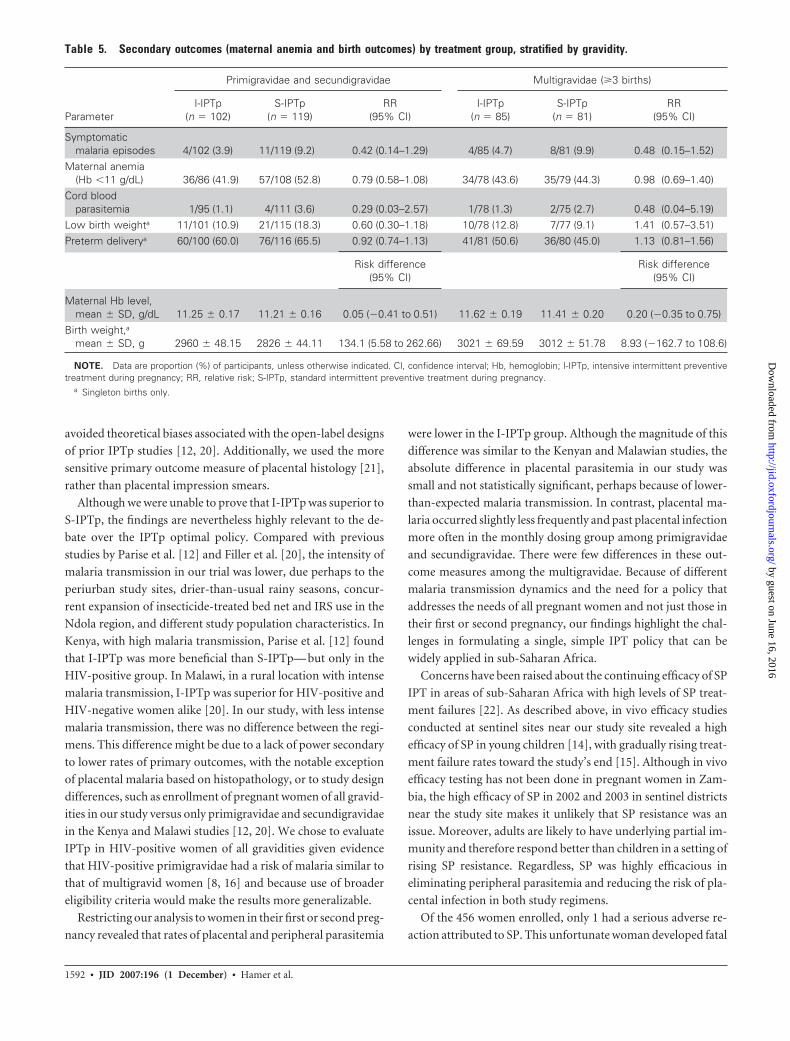
groups. Similarly, for secondary outcomes, there were lower rates of
symptomatic malaria, maternal anemia, cord blood parasitemia,
and LBW in the combined primigravidae and secundigravidae
group in the I-IPTp treatment arm relative to the S-IPTp arm (table
5), but these findings were also not statistically significant. With the
exception of symptomatic malaria episodes, which were nonsignif-
icantly lower in the I-IPTp group, there were no differences between
multigravidae in the 2 study arms.
When stratifying outcomes by the number of SP doses re-
ceived rather than by randomization group, single-dose SP IPTp
Figure 2. Proportion of women with baseline parasitemia, by enrollment date
Table 3. Delivery outcomes and anemia by treatment group.
Parameter I-IPTp (n � 187) S-IPTp (n � 200) RR (95% CI)
Symptomatic malaria episodes 8/187 (4.3) 19/200 (9.5) 0.45 (0.20–1.00)Maternal peripheral parasitemiaa 3/180 (2) 10/189 (5) 0.32 (0.09–1.13)Placental malariaa,b 44/172 (26) 54/189 (29) 0.90 (0.64–1.26)Past placental infectionc 50/172 (29) 41/189 (22) 1.41 (0.99–2.02)Placental parasitemiaa 4/171 (2) 8/188 (4) 0.55 (0.17–1.79)Maternal anemia (Hb �11 g/dL) 70/164 (43) 92/187 (49) 0.87 (0.69–1.09)Cord blood parasitemia 2/173 (1) 6/186 (3) 0.36 (0.07–1.76)Low birth weightd 21/179 (12) 28/192 (15) 0.80 (0.47–1.36)Preterm deliveryd 101/181 (56) 112/196 (57) 0.98 (0.82–1.17)
Risk difference (95% CI)
Birth weight, mean � SD, gd 2987 � 40.77 2902 � 34.16 85.42 (�18.65 to 189.49)Maternal Hb level, mean � SD, g/dL 11.4 � 0.13 11.3 � 0.13 0.08 (�0.28 to 0.43)
NOTE. Data are proportion (%) of participants, unless otherwise indicated. CI, confidence interval; Hb, hemoglobin; I-IPTp,intensive monthly sulfadoxine-pyrimethamine intermittent preventive treatment during pregnancy; RR, relative risk; S-IPTp,standard 2-dose sulfadoxine-pyrimethamine intermittent preventive treatment during pregnancy.
a Primary outcome.b Defined as C1 or C2 (acute/active or recent infection as described in table 1).c Defined as C3 (past infection as described in table 1).d Singleton births only.
1590 ● JID 2007:196 (1 December) ● Hamer et al.
by guest on June 16, 2016http://jid.oxfordjournals.org/
Dow
nloaded from
(34/387 mothers [8.8%]), compared with 2 or more doses (353/
387 mothers [91.8%]), was associated with worse maternal and
neonatal outcomes (see Gill et al. [19]).
Adverse events. Rates of mild adverse events were similar
for the 2 groups (data not shown). Rates of serious adverse
events were low and did not differ between the study groups for
infants (RR for I-IPTp vs. S-IPTp, 1.49 [95% CI, 0.79 –2.8]) or
mothers (RR for I-IPTp vs. S-IPTp, 1.13 [95% CI, 0.56 –2.18]).
There was 1 case (1/189 [0.5%]) of neonatal jaundice in the
I-IPTp group and none in the S-IPTp group. One mother from
the intervention arm died of presumed Stevens-Johnson syn-
drome. Her symptoms began 3 weeks after receiving her first and
only dose of SP. Whether she received sulfonamides through a
different source is unknown.
At 6 weeks, all-cause mortality was higher among the I-IPTp
infants, but this difference was not significant (9/189 live deliv-
eries for I-IPTp vs. 3/198 for S-IPTp; RR, 3.1 [95% CI, 0.86 –
11.4]). All but 1 of the deaths occurred during the neonatal pe-
riod. Of the 9 deaths in the I-IPTp group, 6 occurred in the
delivery room, including 4 from birth asphyxia and 2 from se-
vere prematurity; the other 3 deaths were from sepsis. All 3
deaths in the S-IPT group were from birth aspyhxia. Slightly
more S-IPT infant deaths were stillbirths, but this difference was
not significant (2/191 total deliveries vs. 5/203; RR, 0.43 [95%
CI, 0.1–2.2]).
DISCUSSION
We found no evidence that intensive monthly dosing was supe-
rior to standard dosing of SP IPTp in HIV-seropositive women
in terms of placental malaria, maternal anemia, or birth out-
comes. Although rates of 2 primary outcomes (placental parasi-
temia and maternal peripheral parasitemia) and 2 secondary
outcomes (symptomatic malaria episodes and cord blood para-
sitemia) were lower in the I-IPTp group, none of these differ-
ences were statistically significant, and the absolute reduction for
each parameter was relatively small. However, since the 95% CIs
are relatively wide for most outcomes (with the exception of
placental malaria histopathology), we cannot be sure that these
do not represent true differences.
A significant strength of this study was its double-blind,
placebo-controlled design, considered the gold standard, which
Figure 3. Proportion of women with placental malaria (acute and recent [C1�C2]), by delivery date
Table 4. Primary outcomes (placental and maternal peripheral parasitemia) by treatment group, stratified by gravidity.
Parameter
Primigravidae and secundigravidae Multigravidae (�3 births)
I-IPTp(n � 98)
S-IPTp(n � 114)
RR(95% CI)
I-IPTp(n � 82)
S-IPTp(n � 78)
RR(95% CI)
Maternal peripheral parasitemia 2/98 (2.0) 9/112 (8.0) 0.25 (0.06–1.15) 1/82 (1.2) 1/77 (1.3) 0.94 (0.06–14.75)Placental malariaa 22/93 (23.7) 35/111 (31.5) 0.75 (0.48–1.18) 22/79 (27.8) 19/78 (24.4) 1.14 (0.67–1.94)Past placental infectionb 29/93 (31.2) 26/112 (23.2) 1.34 (0.85–2.11) 21/79 (26.6) 15/77 (19.5) 1.36 (0.76–2.45)Placental parasitemia 2/92 (2.2) 7/114 (6.1) 0.35 (0.08–1.66) 2/79 (2.5) 1/74 (1.4) 1.87 (0.17–20.23)
NOTE. Data are proportion (%) of participants. CI, confidence interval; Hb, hemoglobin; I-IPTp, intensive monthly sulfadoxine-pyrimethamine intermittentpreventive treatment during pregnancy; RR, relative risk; S-IPTp, standard 2-dose sulfadoxine-pyrimethamine intermittent preventive treatment during pregnancy.
a Defined as C1 or C2 (acute/active or recent infection as described in table 1).b Defined as C3 (past infection as described in table 1).
IPT in HIV-Positive Pregnant Women ● JID 2007:196 (1 December) ● 1591
by guest on June 16, 2016http://jid.oxfordjournals.org/
Dow
nloaded from
avoided theoretical biases associated with the open-label designs
of prior IPTp studies [12, 20]. Additionally, we used the more
sensitive primary outcome measure of placental histology [21],
rather than placental impression smears.
Although we were unable to prove that I-IPTp was superior to
S-IPTp, the findings are nevertheless highly relevant to the de-
bate over the IPTp optimal policy. Compared with previous
studies by Parise et al. [12] and Filler et al. [20], the intensity of
malaria transmission in our trial was lower, due perhaps to the
periurban study sites, drier-than-usual rainy seasons, concur-
rent expansion of insecticide-treated bed net and IRS use in the
Ndola region, and different study population characteristics. In
Kenya, with high malaria transmission, Parise et al. [12] found
that I-IPTp was more beneficial than S-IPTp— but only in the
HIV-positive group. In Malawi, in a rural location with intense
malaria transmission, I-IPTp was superior for HIV-positive and
HIV-negative women alike [20]. In our study, with less intense
malaria transmission, there was no difference between the regi-
mens. This difference might be due to a lack of power secondary
to lower rates of primary outcomes, with the notable exception
of placental malaria based on histopathology, or to study design
differences, such as enrollment of pregnant women of all gravid-
ities in our study versus only primigravidae and secundigravidae
in the Kenya and Malawi studies [12, 20]. We chose to evaluate
IPTp in HIV-positive women of all gravidities given evidence
that HIV-positive primigravidae had a risk of malaria similar to
that of multigravid women [8, 16] and because use of broader
eligibility criteria would make the results more generalizable.
Restricting our analysis to women in their first or second preg-
nancy revealed that rates of placental and peripheral parasitemia
were lower in the I-IPTp group. Although the magnitude of this
difference was similar to the Kenyan and Malawian studies, the
absolute difference in placental parasitemia in our study was
small and not statistically significant, perhaps because of lower-
than-expected malaria transmission. In contrast, placental ma-
laria occurred slightly less frequently and past placental infection
more often in the monthly dosing group among primigravidae
and secundigravidae. There were few differences in these out-
come measures among the multigravidae. Because of different
malaria transmission dynamics and the need for a policy that
addresses the needs of all pregnant women and not just those in
their first or second pregnancy, our findings highlight the chal-
lenges in formulating a single, simple IPT policy that can be
widely applied in sub-Saharan Africa.
Concerns have been raised about the continuing efficacy of SP
IPT in areas of sub-Saharan Africa with high levels of SP treat-
ment failures [22]. As described above, in vivo efficacy studies
conducted at sentinel sites near our study site revealed a high
efficacy of SP in young children [14], with gradually rising treat-
ment failure rates toward the study’s end [15]. Although in vivo
efficacy testing has not been done in pregnant women in Zam-
bia, the high efficacy of SP in 2002 and 2003 in sentinel districts
near the study site makes it unlikely that SP resistance was an
issue. Moreover, adults are likely to have underlying partial im-
munity and therefore respond better than children in a setting of
rising SP resistance. Regardless, SP was highly efficacious in
eliminating peripheral parasitemia and reducing the risk of pla-
cental infection in both study regimens.
Of the 456 women enrolled, only 1 had a serious adverse re-
action attributed to SP. This unfortunate woman developed fatal
Table 5. Secondary outcomes (maternal anemia and birth outcomes) by treatment group, stratified by gravidity.
Parameter
Primigravidae and secundigravidae Multigravidae (�3 births)
I-IPTp(n � 102)
S-IPTp(n � 119)
RR(95% CI)
I-IPTp(n � 85)
S-IPTp(n � 81)
RR(95% CI)
Symptomaticmalaria episodes 4/102 (3.9) 11/119 (9.2) 0.42 (0.14–1.29) 4/85 (4.7) 8/81 (9.9) 0.48 (0.15–1.52)
Maternal anemia(Hb �11 g/dL) 36/86 (41.9) 57/108 (52.8) 0.79 (0.58–1.08) 34/78 (43.6) 35/79 (44.3) 0.98 (0.69–1.40)
Cord bloodparasitemia 1/95 (1.1) 4/111 (3.6) 0.29 (0.03–2.57) 1/78 (1.3) 2/75 (2.7) 0.48 (0.04–5.19)
Low birth weighta 11/101 (10.9) 21/115 (18.3) 0.60 (0.30–1.18) 10/78 (12.8) 7/77 (9.1) 1.41 (0.57–3.51)Preterm deliverya 60/100 (60.0) 76/116 (65.5) 0.92 (0.74–1.13) 41/81 (50.6) 36/80 (45.0) 1.13 (0.81–1.56)
Risk difference(95% CI)
Risk difference(95% CI)
Maternal Hb level,mean � SD, g/dL 11.25 � 0.17 11.21 � 0.16 0.05 (�0.41 to 0.51) 11.62 � 0.19 11.41 � 0.20 0.20 (�0.35 to 0.75)
Birth weight,a
mean � SD, g 2960 � 48.15 2826 � 44.11 134.1 (5.58 to 262.66) 3021 � 69.59 3012 � 51.78 8.93 (�162.7 to 108.6)
NOTE. Data are proportion (%) of participants, unless otherwise indicated. CI, confidence interval; Hb, hemoglobin; I-IPTp, intensive intermittent preventivetreatment during pregnancy; RR, relative risk; S-IPTp, standard intermittent preventive treatment during pregnancy.
a Singleton births only.
1592 ● JID 2007:196 (1 December) ● Hamer et al.
by guest on June 16, 2016http://jid.oxfordjournals.org/
Dow
nloaded from

Stevens-Johnson syndrome 3 weeks after her first SP treat-
ment. Prolonged delays from the time of treatment to the devel-
opment of a severe reaction are unusual but have been reported
[23–25], including fatal reactions in patients with AIDS receiv-
ing sulfonamides to prevent opportunistic infections [26, 27]. A
recent review estimated a risk of severe adverse reactions to in-
termittent SP (monthly or less often) of 0%– 6.3% [28]. Passive
surveillance for severe adverse events associated with SP and
trimethoprim-sulfamethoxazole in Malawi found that life-
threatening reactions (including Stevens-Johnson syndrome)
occurred infrequently [29]. Rates were highest in HIV-positive
adults (4.9/100,000 SP exposures). Fatal adverse reactions to SP
were estimated to be 0.11 deaths/100,000 SP exposures. Al-
though this is reassuring, the fatal reaction associated with SP in
the present study highlights the importance of careful monitor-
ing for serious reactions when SP is used for IPTp.
In conclusion, in contrast to prior studies of I-IPTp per-
formed in sites with more intense malaria transmission [12, 19],
we found no convincing evidence that I-IPTp was superior to
S-IPTp in an area of relatively mild malaria transmission. How-
ever, as described in the accompanying article [19], single-dose
SP IPTp is inferior to �2 doses for the prevention of maternal
anemia, LBW, and prematurity. In addition, inadvertent under-
dosing is a potential vulnerability of standard-dose SP IPTp.
From the efficacy standpoint, even though our study did not
show a clear advantage of a monthly dosing schedule, factors
related to effectiveness, such as the greater simplicity of monthly
dosing at a programmatic level, argue in favor of a more inten-
sive schedule.
Acknowledgments
We thank Dr. Carlos Abramowsky of Emory University for performingquality control on the histological samples and the National Malaria ControlCenter parasitologists in Lusaka for quality control on the malaria bloodsmears. We also thank Dr. Michael Macdonald and Ms. Christine Ayash fortheir assistance throughout the study with logistics.
References
1. Steketee RW, Nahlen BL, Parise ME, Menendez C. The burden of ma-laria in pregnancy in malaria-endemic areas. Am J Trop Med Hyg 2001;64:28 –35.
2. Guyatt HL, Snow RW. Malaria in pregnancy as an indirect cause ofinfant mortality in sub-Saharan Africa. Trans R Soc Trop Med Hyg2001; 95:569 –76.
3. Macgregor I, Wilson ME, Billewicz WZ. Malaria infection of the pla-centa in The Gambia, West Africa: its incidence and relationship tostillbirth, birthweight and placental weight. Trans R Soc Trop Med Hyg1983; 77:232– 44.
4. Van Geertruyden JP, Thomas F, Erhart A, D’Alessandro U. The contri-bution of malaria in pregnancy to perinatal mortality. Am J Trop MedHyg 2004; 71(Suppl 2):35– 40.
5. Guyatt HL, Snow RW. Impact of malaria during pregnancy on low birthweight in sub-Saharan Africa. Clin Microbiol Rev 2004; 17:760 –9.
6. van Eijk AM, Ayisi JG, ter Kuile FO, et al. Malaria and human immuno-deficiency virus infection as risk factors for anemia in infants in Kisumu,western Kenya. Am J Trop Med Hyg 2002; 67:44 –53.
7. Ayisi JG, van Eijk AM, ter-Kuile FO, et al. The effect of dual infectionwith HIV and malaria on pregnancy outcomes in western Kenya. AIDS2003; 17:585–94.
8. van Eijk AM, Ayisi JG, ter-Kuile FO, et al. HIV increases the risk ofmalaria in women of all gravidities in Kisumu, Kenya. AIDS 2003; 17:595– 603.
9. Center for Health Science and Social Research (CHESSORE). Report onthe Zambia roll back malaria (RBM) baseline study undertaken in tensentinel districts (July to August 2001). Lusaka, Zambia: CHESSORE, 2001.
10. Central Statistical Office (Zambia), Central Board of Health (Zambia),ORC Macro. Zambia demographic and health survey 2001–2002. Cal-verton, MD: Central Statistical Office and Central Board of Health andORC Macro, 2003.
11. Central Board of Health (Zambia). Guidelines for the diagnosis andtreatment of malaria in Zambia. Lusaka, Zambia: Central Board ofHealth, 2003.
12. Parise ME, Ayisi JG, Nahlen BL, et al. Efficacy of sulfadoxine-pyrimethamine for prevention of placental malaria in an area of Kenyawith high prevalence of malaria and human immunodeficiency virusinfection. Am J Trop Med Hyg 1998; 59:813–22.
13. Central Statistical Office (Zambia). Summary report for 2000 census ofpopulation and housing. Lusaka, Zambia: Central Statistical Office, 2003.
14. National Malaria Control Center (Zambia). Preliminary summary re-port: drug efficacy conducted in five sentinel sites (Chipata, Chongwe,Isoka, Mpongwe, and Mansa) March to May 2002. Lusaka, Zambia:Central Board of Health/Ministry of Health, 2002.
15. Chanda P, Sikaala CH, Kapelwa W, et al. Decreasing efficacy ofsulphadoxine-pyrimethamine (SP) in Zambian children [abstract 708].In: Program and abstracts of the 53rd annual meeting of the AmericanSociety of Tropical Medicine and Hygiene (Miami Beach, FL). Am JTrop Med Hyg 2004; 71(Suppl 4):209.
16. Steketee RW, Wirima JJ, Bloland PB, et al. Impairment of a pregnantwoman’s ability to limit Plasmodium falciparum by infection with hu-man immunodeficiency virus type 1. Am J Trop Med Hyg 1996;55(Suppl 1):42–9.
17. Dubowitz LMS, Dubowitz V, Goldberg C. Clinical assessment of gesta-tional age in the newborn infant. J Pediatr 1970; 77:1–10.
18. Trape JF. Rapid evaluation of malaria parasite density and standardiza-tion of thick smear examination for epidemiological investigations.Trans R Soc Trop Med Hyg 1985; 79:181– 4.
19. Gill CJ, MacLeod WB, Mwanakasale V, et al. Inferiority of single-dosesulfadoxine-pyrimethamine intermittent preventive therapy for malariaduring pregnancy among HIV-positive Zambian women. J Infect Dis2007; 196:1577– 84 (in this issue).
20. Filler S, Kazembe P, Thigpen M, et al. Randomized trial of 2-dose versusmonthly sulfadoxine-pyrimethamine intermittent preventive treatmentfor malaria in HIV-positive and HIV-negative pregnant women in Ma-lawi. J Infect Dis 2006; 194:286 –93.
21. Rogerson SJ, Mkundika P, Kanjala MK. Diagnosis of Plasmodium falcip-arum malaria at delivery: comparison of blood film preparation meth-ods and of blood films with histology. J Clin Microbiol 2003; 41:1370 – 4.
22. Newman RD, Parise ME, Slutsker L, Nahlen B, Steketee RW. Safety,efficacy and determinants of effectiveness of antimalarial drugs duringpregnancy: implications for prevention programmes in Plasmodiumfalciparum-endemic sub-Saharan Africa. Trop Med Int Health 2003; 8:488 –506.
23. Miller K, Lobel HO, Satriale R, Kuritsky J, Stern R, Campbell CC. Severecutaneous reactions among American travelers using pyrimethamine-sulfadoxine (Fansidar) for malaria prophylaxis. Am J Trop Med Hyg1986; 35:451– 8.
24. Hellgren U, Rombo L, Berg B. Adverse reactions to sulphadoxine-pyrimethamine in Swedish travellers: implications for prophylaxis. BMJ1987; 295:365– 6.
25. Hernborg A. Stevens-Johnson syndrome after mass prophylaxis withsulfadoxine for cholera in Mozambique. Lancet 1985; 2:1072–3.
IPT in HIV-Positive Pregnant Women ● JID 2007:196 (1 December) ● 1593
by guest on June 16, 2016http://jid.oxfordjournals.org/
Dow
nloaded from

26. Raviglione M, Dinan W, Pablos-Mendez A, Palagiano A, Sabatini M.Fatal toxic epidermal necroloysis during prophylaxis with py-rimethamine and sulfadoxine in a human immunodeficiency virus-infected man. Arch Intern Med 1988; 148:2683–5.
27. Centers for Disease Control. Fansidar-associated fatal reaction in an HIV-infected man. MMWR Morb Mortal Wkly Rep 1988; 37:571–2, 577.
28. Brentlinger PE, Behrens CB, Micek MA. Challenges in the concurrentmanagement of malaria and HIV in pregnancy in sub-Saharan Africa.Lancet Infect Dis 2006; 6:100 –11.
29. Gimnig JE, MacArthur JR, M‘bang’ombe M, et al. Severe cutaneous reac-tions to sulfadoxine-pyrimethamine and trimethoprim-sulfamethoxazolein Blantyre District, Malawi. Am J Trop Med Hyg 2006; 74:738–43.
1594 ● JID 2007:196 (1 December) ● Hamer et al.
by guest on June 16, 2016http://jid.oxfordjournals.org/
Dow
nloaded from




















