
Psychometric Properties of Pain Intensity Scales Comparing ...

2013
http://informahealthcare.com/dreISSN 0963-8288 print/ISSN 1464-5165 online
Disabil Rehabil, 2013; 35(26): 2181–2190! 2013 Informa UK Ltd. DOI: 10.3109/09638288.2013.774061
REVIEW
Psychometric evidence of self-reported questionnaires forpatellofemoral pain syndrome: a systematic review
Jean-Francois Esculier1,2, Jean-Sebastien Roy1,2, and Laurent Julien Bouyer1,2
1Centre Interdisciplinaire de Recherche en Readaptation et Integration Sociale (CIRRIS) and 2Faculty of Medicine, Universite Laval, Quebec City,
Canada
Abstract
Purpose: To conduct a systematic review of psychometric properties of self-reportedquestionnaires used to assess the level of symptoms and disability in individuals withpatellofemoral pain syndrome (PFPS). Methods: A structured search was conducted in fourdatabases (Medline, Embase, CINAHL, SportDiscus). A total of 24 studies about five differentself-reported questionnaires were analyzed. A pair of independent raters extracted data onvalidity, reliability and responsiveness to change, and performed critical appraisal (0–100%).Results: Activities of Daily Living Scale (ADLS), Anterior Knee Pain Scale (AKPS), InternationalKnee Documentation Committee (IKDC) and Lysholm Scale (LS) present excellent test–retestreliability (weighted average intraclass correlation coefficients [ICC]40.80), whereas FunctionalIndex Questionnaire (FIQ) is moderately reliable (ICC¼ 0.61). Minimal detectable change is 8.3%for ADLS, 9.0% for AKPS, 19% for FIQ, 8.5% for IKDC and 30% for LS. ADLS, AKPS, IKDC and LSare highly responsive (effect size/standardized response mean40.95) in individuals with PFPS,while FIQ is lowly responsive (effect size¼ 0.49). Conclusion: Based on available evidence,ADLS presents the best psychometric properties and should be preferred when evaluatingpatients with PFPS. AKPS and IKDC are also adequate, while FIQ and LS are not recommendedfor individuals with PFPS.
� Implications for Rehabilitation
� While several questionnaires have been developed to assess symptoms and functionallimitations caused by knee pain, their psychometric properties can vary depending on thecondition presented by the patient.
� The Activities of Daily Living Scale of the Knee Outcome Survey should be preferred byclinicians when evaluating a patient with PFPS.
� The Anterior Knee Pain Scale and International Knee Documentation Committee Subjectiveknee evaluation are also adequate for use with this population.
� The Functional Index Questionnaire and Lysholm Scale are not recommended for PFPS.
Keywords
Anterior knee pain, pain, patellofemoral painsyndrome, psychometric properties,questionnaires
History
Received 6 September 2012Revised 24 January 2013Accepted 4 February 2013Published online 29 April 2013
Introduction
Knee pain affects approximately 20–30% of the population andis one of the most prevalent musculoskeletal (MSK) conditions[1,2]. Among knee pain diagnoses in sports medicine clinics,patellofemoral pain syndrome (PFPS) is one of the most commonwith approximately 25% of all medical consultations for knee pain[3]. PFPS has been described as anterior or retropatellar kneepain or pain along the lateral and medial borders of the patella,which could be caused by anterior knee structures such as the
infrapatellar fat pad, patellar subchondral bone, anterior synoviumand medial or lateral retinaculae [3,4]. It is associated withactivities that load the patellofemoral joint such as going up anddown stairs, kneeling or running [5]. It is therefore recognizedthat PFPS is an activity-limiting condition that contributes todisability and impacts health-related quality of life [6].
Several self-administered scales have been developed to assessthe level of symptoms and disability of persons affected by kneepain. In clinical trials involving individuals with PFPS, question-naires are often used as primary outcomes to evaluate the effectsof interventions such as rehabilitation or surgery [7,8]. In clinicalsettings, self-reported questionnaires are used in this population asa basis for treatment decision-making, and for the determinationof treatment effectiveness following an episode of care. Therefore,psychometric properties such as validity, reliability and respon-siveness to change need to be established in order to justify thechoice of using a given scale. Both clinicians and researchers needto have a clear portrait of the measurement properties of these
Address for correspondence: Jean-Sebastien Roy, PhD, PT, CentreInterdisciplinaire de Recherche en Readaptation et Integration Sociale(CIRRIS), Universite Laval, Quebec City, G1M 2S8, Canada. Tel: 1-418-529-9141, Ext 6005. E-mail: [email protected]
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f L
aval
on
02/1
3/15
For
pers
onal
use
onl
y.

tools to make sure that the decision of using a specific scale isbased on the best evidence available.
Recently, three review articles have been published on thepsychometric properties of self-reported scales used for individ-uals with knee pain. Although recommendations were made forPFPS, none of these reviews were specific to this population.First, in 2009, a narrative review by Wright recommended theuse of the International Knee Documentation Committee (IKDC)Subjective Knee Evaluation Form or of the Knee OsteoarthritisOutcome Survey (KOOS) for individuals with PFPS [9].However, these recommendations were not based on psycho-metric evidence. This review also failed to include threequestionnaires that are widely used with PFPS (Anterior KneePain Scale (AKPS), Activities of Daily Living Scale (ADLS)and Functional Index Questionnaire (FIQ)). In 2010, a reviewby Wang et al. recommended the AKPS for individuals withPFPS based on the results of four studies specific to thispopulation [10]. Finally, in 2012, Howe et al. published asystematic review pertaining to the measurement properties of37 outcome measures used to evaluate all musculoskeletalconditions of the knee [11]. Based on only two studies,the authors also concluded that the AKPS should be preferredfor individual with PFPS [11]. Although documented searchesin databases were performed in the latter two review art-icles, they did not incorporate critical appraisal of the selectedpapers, which is considered a key step for a systematicreview [12].
While many questionnaires have been used to evaluatesymptoms and disability caused by PFPS, no systematic reviewon the psychometric properties of these scales has been specif-ically performed for this population. The objective of this studyis to systematically review the psychometric properties of self-administered questionnaires used to assess symptoms anddisability in individuals with PFPS.
Methods
Literature search
Database searches were performed in Medline, Embase, CINAHLand SportDiscus. A general search was first conducted to gather alist of existing self-administered questionnaires for individualswith knee pain using the following keywords: (knee or ‘‘kneepain’’ or patellofemoral or patello-femoral) and (‘‘Outcomemeasure’’ or Questionnaire or Scale) and (reliability or validityor responsiveness or ‘‘minimal detectable change’’ or ‘‘clinicallyimportant difference’’ or ‘‘factor analysis’’ or translation orvalidation). Then, a specific search was conducted by includingall previously found questionnaires and their abbreviationsin conjunction with the previously mentioned keywords.Keywords for this specific search are described in Figure 1.Hand searches of retrieved article reference lists were alsoconducted. Publications from January 1966 to August 2012 wereconsidered.
The titles and abstracts of each article were independentlyreviewed by two raters (JFE and JSR) and an article wasincluded for a full review if it met the following inclusioncriteria: (1) evaluated at least one psychometric property of aself-administered questionnaire, (2) included individuals withPFPS and (3) written in English or in French. Review articleswere excluded. When conducting a systematic review, it isimportant to have a sufficient number of studies to makemeaningful conclusions. As multiple questionnaires were found,and most of them had very little publications specifically on theirpsychometric properties in population with PFPS, a questionnairewas included only if at least five articles evaluating its
psychometric properties met the inclusion criteria of the presentsystematic review.
Study quality scoring
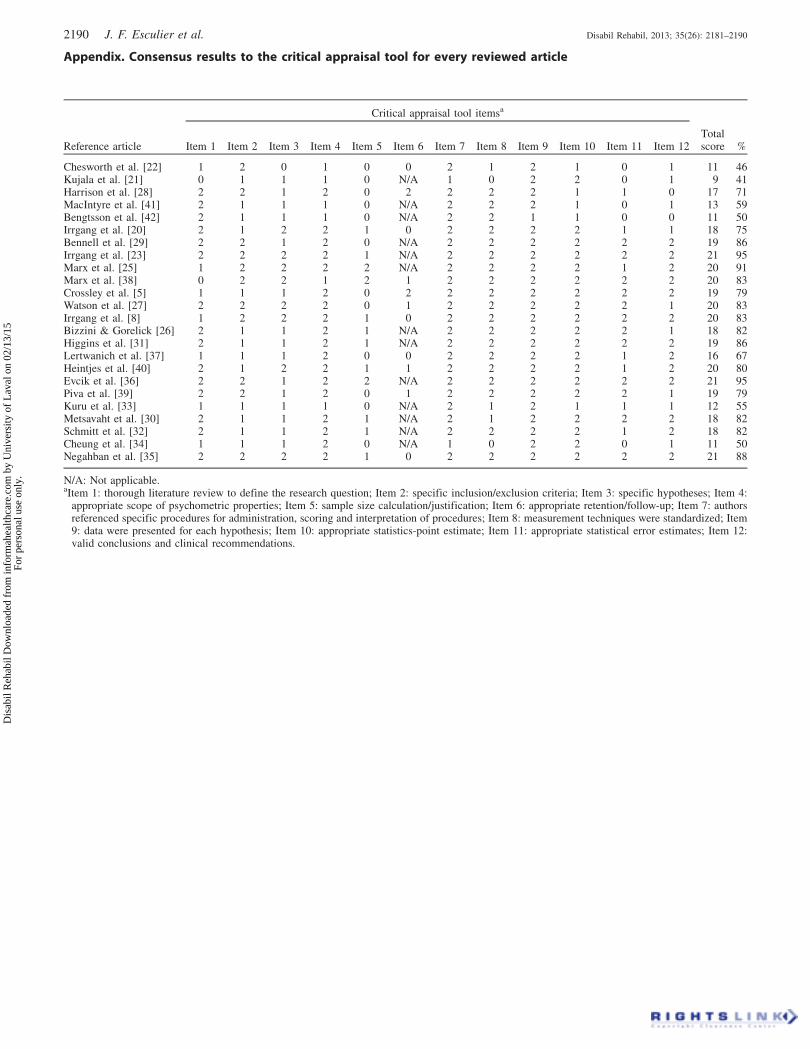
The two raters independently evaluated the methodologicalquality of each article that met the inclusion criteria using astructured critical appraisal tool [13] previously used in othersystematic reviews [14–16]. This tool has been shown to have anexcellent inter-rater reliability (intraclass correlation coefficients[ICC]40.90) [14–16]. It contains 12 scoring items, of which 1is about the study question, 5 about study design, 2 aboutmeasurements, 3 about analyses and 1 about recommendations.According to specific criteria, each item is scored as 2 (satisfac-tory), 1 (partially satisfactory) or 0 (unsatisfactory). The totalscore on 24 is then converted to a percentage score. The two ratersfirst met for a calibration review after having independentlyreviewed two papers. They discussed each item to clarify themeaning and interpretation of critical appraisal items. After theindependent evaluation of all included papers, the two raters metto discuss their scores. Each specific item on the quality appraisaltool was discussed to reach consensus. This process identifiedif differences were due to facts or to different application ofthe quality appraisal scorings. ICC was calculated to evaluatepre-consensus inter-rater reliability of the total score. Studieswere rank ordered for quality and this ranking was considered inconclusions and recommendations.
Data extraction
As single abstraction is known to generate more errors, the tworaters abstracted the data independently. A standardized datacollection form was used and testing was done on two articlesto ensure consistency in coding instructions and alleviatingpotential errors in data abstraction. Descriptive information forthe patient population (number of patients, age, sex and presenceof co-morbidities) and interventions (type of treatment) werecollected. Psychometric properties extracted were the following:validity (construct, content, factorial, known-group and floor/ceiling effects), reliability (test–retest ICC, standard error ofmeasurement [SEM], minimal detectable change [MDC] andinternal consistency), responsiveness (effect size [ES], standar-dized response mean [SRM], clinically important difference[CID] and longitudinal validity), administration burden and cross-cultural adaptation. Overall relative and absolute reliabilityand responsiveness were determined by calculating a weightedaverage over all studies (weighted by sample size). ICC wereconsidered excellent if �0.81, good from 0.61 to 0.80, moderatefrom 0.41 to 0.60, fair from 0.21 to 0.40 and poor if50.20 [17].ES and SRM were considered large if �0.8, moderate between0.50 and 0.80 and small between 0.20 and 0.50 [18], whilePearson or Spearman correlations were categorized as high if�0.70, moderate between 0.50 and 0.70, and low between0.26 and 0.50 [19].
Results
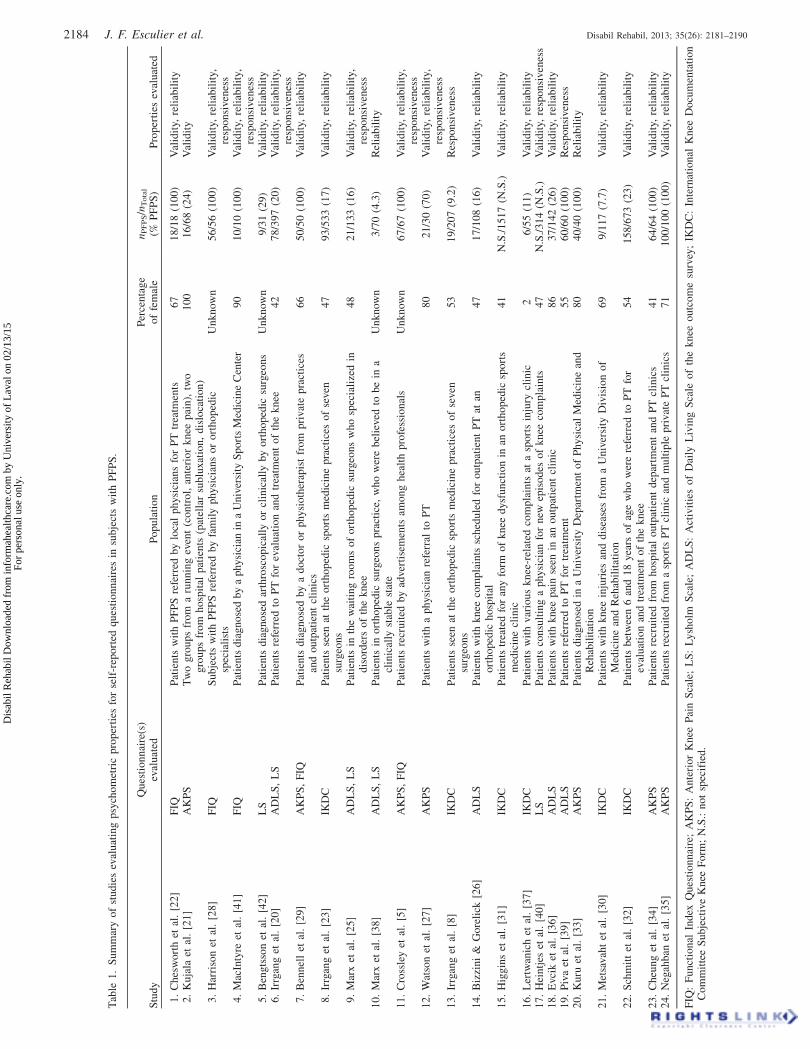
A total of 61 articles were reviewed. Twenty-four papers onfive self-reported questionnaires met all inclusion criteria andwere included (Table 1, appendix). Twenty-eight papers wereexcluded either because they did not include subjects with PFPS,did not evaluate any psychometric property, or were reviews.Furthermore, nine papers were excluded because they evaluated aquestionnaire that did not meet the inclusion criteria (less thanfive publications on its psychometric properties). Quality scoresfor included studies ranged between 41% and 95% (appendix),
2182 J. F. Esculier et al. Disabil Rehabil, 2013; 35(26): 2181–2190
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f L
aval
on
02/1
3/15
For
pers
onal
use
onl
y.
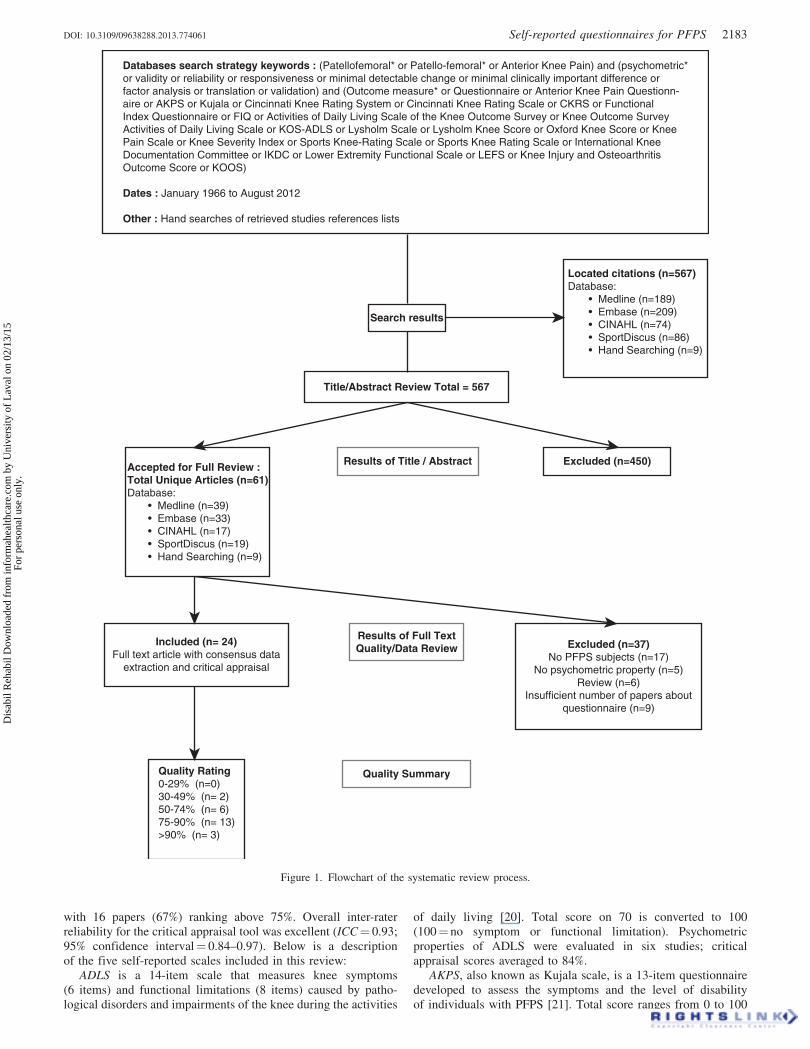
with 16 papers (67%) ranking above 75%. Overall inter-raterreliability for the critical appraisal tool was excellent (ICC¼ 0.93;95% confidence interval¼ 0.84–0.97). Below is a descriptionof the five self-reported scales included in this review:
ADLS is a 14-item scale that measures knee symptoms(6 items) and functional limitations (8 items) caused by patho-logical disorders and impairments of the knee during the activities
of daily living [20]. Total score on 70 is converted to 100(100¼ no symptom or functional limitation). Psychometricproperties of ADLS were evaluated in six studies; criticalappraisal scores averaged to 84%.
AKPS, also known as Kujala scale, is a 13-item questionnairedeveloped to assess the symptoms and the level of disabilityof individuals with PFPS [21]. Total score ranges from 0 to 100
Located citations (n=567)Database: • Medline (n=189) • Embase (n=209) • CINAHL (n=74) • SportDiscus (n=86) • Hand Searching (n=9)
Databases search strategy keywords : (Patellofemoral* or Patello-femoral* or Anterior Knee Pain) and (psychometric*or validity or reliability or responsiveness or minimal detectable change or minimal clinically important difference orfactor analysis or translation or validation) and (Outcome measure* or Questionnaire or Anterior Knee Pain Questionn-aire or AKPS or Kujala or Cincinnati Knee Rating System or Cincinnati Knee Rating Scale or CKRS or FunctionalIndex Questionnaire or FIQ or Activities of Daily Living Scale of the Knee Outcome Survey or Knee Outcome SurveyActivities of Daily Living Scale or KOS-ADLS or Lysholm Scale or Lysholm Knee Score or Oxford Knee Score or KneePain Scale or Knee Severity Index or Sports Knee-Rating Scale or Sports Knee Rating Scale or International KneeDocumentation Committee or IKDC or Lower Extremity Functional Scale or LEFS or Knee Injury and OsteoarthritisOutcome Score or KOOS)
Dates : January 1966 to August 2012
Other : Hand searches of retrieved studies references lists
Search results
Title/Abstract Review Total = 567
Accepted for Full Review : Total Unique Articles (n=61)Database: • Medline (n=39) • Embase (n=33) • CINAHL (n=17) • SportDiscus (n=19) • Hand Searching (n=9)
Included (n= 24)Full text article with consensus data
extraction and critical appraisal
Quality Rating0-29% (n=0)30-49% (n= 2)50-74% (n= 6)75-90% (n= 13)>90% (n= 3)
Quality Summary
Results of Full TextQuality/Data Review Excluded (n=37)
No PFPS subjects (n=17)No psychometric property (n=5)
Review (n=6)Insufficient number of papers about
questionnaire (n=9)
Excluded (n=450)Results of Title / Abstract
Figure 1. Flowchart of the systematic review process.
DOI: 10.3109/09638288.2013.774061 Self-reported questionnaires for PFPS 2183
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f L
aval
on
02/1
3/15
For
pers
onal
use
onl
y.
Tab
le1
.S
um
mar
yo
fst
ud
ies
eval
uat
ing
psy
cho
met
ric
pro
per
ties
for
self
-rep
ort
edqu
esti
on
nai
res
insu
bje
cts
wit
hP
FP
S.
Stu
dy
Qu
esti
on
nai
re(s
)ev
alu
ated
Po
pu
lati
on
Per
cen
tag
eo
ffe
mal
en
PF
PS/n
Tota
l
(%P
FP
S)
Pro
per
ties
eval
uat
ed
1.
Ch
esw
ort
het
al.
[22
]F
IQP
atie
nts
wit
hP
FP
Sre
ferr
edby
loca
lp
hysi
cian
sfo
rP
Ttr
eatm
ents
67
18
/18
(10
0)
Val
idit
y,re
liab
ilit
y2
.K
uja
laet
al.
[21
]A
KP
ST
wo
gro
up
sfr
om
aru
nn
ing
even
t(c
on
tro
l,an
teri
or
kn
eep
ain
),tw
og
rou
ps
fro
mh
osp
ital
pat
ien
ts(p
atel
lar
sub
luxat
ion
,d
islo
cati
on
)1
00
16
/68
(24
)V
alid
ity
3.
Har
riso
net
al.
[28
]F
IQS
ub
ject
sw
ith
PF
PS
refe
rred
by
fam
ily
physi
cian
so
ro
rth
op
edic
spec
iali
sts
Un
kn
ow
n5
6/5
6(1
00
)V
alid
ity,
reli
abil
ity,
resp
on
siven
ess
4.
Mac
Inty
reet
al.
[41
]F
IQP
atie
nts
dia
gn
ose
dby
ap
hysi
cian
ina
Un
iver
sity
Sp
ort
sM
edic
ine
Cen
ter
90
10
/10
(10
0)
Val
idit
y,re
liab
ilit
y,re
spo
nsi
ven
ess
5.
Ben
gts
son
etal
.[4
2]
LS
Pat
ien
tsd
iag
no
sed
arth
rosc
op
ical
lyo
rcl
inic
ally
by
ort
ho
ped
icsu
rgeo
ns
Un
kn
ow
n9
/31
(29
)V
alid
ity,
reli
abil
ity
6.
Irrg
ang
etal
.[2
0]
AD
LS
,L
SP
atie
nts
refe
rred
toP
Tfo
rev
alu
atio
nan
dtr
eatm
ent
of
the
kn
ee4
27
8/3
97
(20
)V
alid
ity,
reli
abil
ity,
resp
on
siven
ess
7.
Ben
nel
let
al.
[29
]A
KP
S,
FIQ
Pat
ien
tsd
iag
no
sed
by
ad
oct
or
or
physi
oth
erap
ist
fro
mp
riv
ate
pra
ctic
esan
do
utp
atie
nt
clin
ics
66
50
/50
(10
0)
Val
idit
y,re
liab
ilit
y
8.
Irrg
ang
etal
.[2
3]
IKD
CP
atie
nts
seen
atth
eo
rth
op
edic
spo
rts
med
icin
ep
ract
ices
of
seven
surg
eon
s4
79
3/5
33
(17
)V
alid
ity,
reli
abil
ity
9.
Mar
xet
al.
[25
]A
DL
S,
LS
Pat
ien
tsin
the
wai
tin
gro
om
so
fo
rth
op
edic
surg
eon
sw
ho
spec
iali
zed
ind
iso
rder
so
fth
ek
nee
48
21
/13
3(1
6)
Val
idit
y,re
liab
ilit
y,re
spo
nsi
ven
ess
10
.M
arx
etal
.[3
8]
AD
LS
,L
SP
atie
nts
ino
rth
op
edic
surg
eon
sp
ract
ice,
wh
ow
ere
bel
ieved
tob
ein
acl
inic
ally
stab
lest
ate
Un
kn
ow
n3
/70
(4.3
)R
elia
bil
ity
11
.C
ross
ley
etal
.[5
]A
KP
S,
FIQ
Pat
ien
tsre
cru
ited
by
adver
tise
men
tsam
on
gh
ealt
hp
rofe
ssio
nal
sU
nk
now
n6
7/6
7(1
00
)V
alid
ity,
reli
abil
ity,
resp
on
siven
ess
12
.W
atso
net
al.
[27
]A
KP
SP
atie
nts
wit
ha
physi
cian
refe
rral
toP
T8
02
1/3
0(7
0)
Val
idit
y,re
liab
ilit
y,re
spo
nsi
ven
ess
13
.Ir
rgan
get
al.
[8]
IKD
CP
atie
nts
seen
atth
eo
rth
op
edic
spo
rts
med
icin
ep
ract
ices
of
seven
surg
eon
s5
31
9/2
07
(9.2
)R
esp
on
siven
ess
14
.B
izzi
ni
&G
ore
lick
[26
]A
DL
SP
atie
nts
wit
hk
nee
com
pla
ints
sch
edu
led
for
ou
tpat
ien
tP
Tat
ano
rth
op
edic
ho
spit
al4
71
7/1
08
(16
)V
alid
ity,
reli
abil
ity
15
.H
igg
ins
etal
.[3
1]
IKD
CP
atie
nts
trea
ted
for
any
form
of
kn
eed
ysf
un
ctio
nin
ano
rth
op
edic
spo
rts
med
icin
ecl
inic
41
N.S
./1
51
7(N
.S.)
Val
idit
y,re
liab
ilit
y
16
.L
ertw
anic
het
al.
[37
]IK
DC
Pat
ien
tsw
ith
var
iou
sk
nee
-rel
ated
com
pla
ints
ata
spo
rts
inju
rycl
inic
26
/55
(11
)V
alid
ity,
reli
abil
ity
17
.H
ein
tjes
etal
.[4
0]
LS
Pat
ien
tsco
nsu
ltin
ga
physi
cian
for
new
epis
od
eso
fk
nee
com
pla
ints
47
N.S
./3
14
(N.S
.)V
alid
ity,
resp
on
siven
ess
18
.E
vci
ket
al.
[36
]A
DL
SP
atie
nts
wit
hk
nee
pai
nse
enin
ano
utp
atie
nt
clin
ic8
63
7/1
42
(26
)V
alid
ity,
reli
abil
ity
19
.P
iva
etal
.[3
9]
AD
LS
Pat
ien
tsre
ferr
edto
PT
for
trea
tmen
t5
56
0/6
0(1
00
)R
esp
on
siven
ess
20
.K
uru
etal
.[3
3]
AK
PS
Pat
ien
tsd
iag
no
sed
ina
Un
iver
sity
Dep
artm
ent
of
Physi
cal
Med
icin
ean
dR
ehab
ilit
atio
n8
04
0/4
0(1
00
)R
elia
bil
ity
21
.M
etsa
vah
tet
al.
[30
]IK
DC
Pat
ien
tsw
ith
kn
eein
juri
esan
dd
isea
ses
fro
ma
Un
iver
sity
Div
isio
no
fM
edic
ine
and
Reh
abil
itat
ion
69
9/1
17
(7.7
)V
alid
ity,
reli
abil
ity
22
.S
chm
itt
etal
.[3
2]
IKD
CP
atie
nts
bet
wee
n6
and
18
yea
rso
fag
ew
ho
wer
ere
ferr
edto
PT
for
eval
uat
ion
and
trea
tmen
to
fth
ek
nee
54
15
8/6
73
(23
)V
alid
ity,
reli
abil
ity
23
.C
heu
ng
etal
.[3
4]
AK
PS
Pat
ien
tsre
cru
ited
fro
mh
osp
ital
ou
tpat
ien
td
epar
tmen
tan
dP
Tcl
inic
s4
16
4/6
4(1
00
)V
alid
ity,
reli
abil
ity
24
.N
egah
ban
etal
.[3
5]
AK
PS
Pat
ien
tsre
cru
ited
fro
ma
spo
rts
PT
clin
ican
dm
ult
iple
pri
vat
eP
Tcl
inic
s7
11
00
/10
0(1
00
)V
alid
ity,
reli
abil
ity
FIQ
:F
un
ctio
nal
Ind
exQ
ues
tio
nn
aire
;A
KP
S:
An
teri
or
Kn
eeP
ain
Sca
le;
LS
:L
ysh
olm
Sca
le;
AD
LS
:A
ctiv
itie
so
fD
aily
Liv
ing
Sca
leo
fth
ek
nee
ou
tco
me
surv
ey;
IKD
C:
Inte
rnat
ion
alK
nee
Do
cum
enta
tio
nC
om
mit
tee
Su
bje
ctiv
eK
nee
Fo
rm;
N.S
.:n
ot
spec
ifie
d.
2184 J. F. Esculier et al. Disabil Rehabil, 2013; 35(26): 2181–2190
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f L
aval
on
02/1
3/15
For
pers
onal
use
onl
y.

(100¼ no symptom or disability). Psychometric properties of theAKPS were evaluated in seven studies; critical appraisal scoresaveraged to 69%.
FIQ is an 8-item questionnaire that evaluates functionallimitations caused by knee pain during activities of daily living.Scores are ranked as 0 (unable to do), 1 (can do with a problem)and 2 (no difficulty) for a total score on 16 (16¼ absenceof limitation) [22]. Psychometric properties of the FIQ wereevaluated in five studies; critical appraisal scores averaged to 68%.
IKDC Subjective Knee Evaluation Form was created by acommittee of international knee experts to measure knee symp-toms, function and participation to sports activities. Responsetypes for the 10 items are 5-point and 11-point Likert scalesand dichotomous response options (yes/no). Total score isconverted to a 0–100 scale (100¼ optimal function of the knee)[23]. Psychometric properties of the IKDC were evaluated in sixstudies; critical appraisal scores averaged to 83%.
Lysholm Scale (LS) is an 8-item questionnaire that wasoriginally developed to assess signs, symptoms and disabilityof patients after knee ligament surgery [24]. The score is on 100points, where points are given for subjective as well as objectiveaspects of the evaluation (100¼ excellent knee function).Psychometric properties of the LS were evaluated in five studies;critical appraisal score averaged to 76%.
Validity
Content validity
The content of the five questionnaires has been shown to bevalid in evaluating symptoms and/or disability caused by PFPS.More specifically, the face and content validity of ADLS and LShave been evaluated for various knee problems including PFPSby a committee of orthopedic surgeons, and found to be adequatefor both scales [25]. ADLS was also fully completed by all 58patients with knee pain (16% with PFPS) [26], while in a cohortof 30 patients with knee pain (70% with PFPS), only 4.4% of theitems of AKPS were left unanswered [27]. As for the FIQ, in astudy evaluating 56 patients with PFPS, 20–30% of patientsanswered ‘‘unknown’’ for two items that related to their capacityto walk or run [28]. However, in a study comparing differentoutcomes for PFPS (including FIQ and AKPS), FIQ was chosenas the easiest questionnaire to complete, but not good at depictingsymptoms, while AKPS was described as an easy questionnaireto complete and good to describe symptoms [29].
Construct validity
Correlations among included scales have only been performedbetween ADLS-LS, IKDC-LS and AKPS-FIQ for PFPS. Asexpected, given the similarity in their constructs, moderate(0.505r50.70) [29] to high (0.705r50.90 [20,30] or 0.705�50.90 [25]) correlations were observed in cohorts includingindividuals with PFPS. Moderate to strong correlations (�0.50)
were also observed between the studied questionnaires and otherscales, such as the Western Ontario and McMaster UniversitiesArthritis Index (WOMAC) [30], physical component of the Short-Form 36 (SF-36) and 12 (SF-12) [20,25,30,31] and pain visualanalog scale (VAS) [5,26]. Weaker correlations (0.30–0.50) wereobserved with less similar indices, such as the mental componentof the SF-36 [30,31].
Known-group validity
Known-group validity refers to the capacity of a test todiscriminate between a group of individuals known to have aparticular trait and a group who does not. Known-group validityhas shown that ADLS, AKPS and LS can differentiate betweendifferent populations (PFPS versus other knee conditions) and/ordisability levels (Table 2). Among included questionnaires, ADLShas been the most extensively studied for known-group validity inindividuals with PFPS, while this aspect of validity has not beenevaluated for FIQ and IKDC in this population.
Factorial validity
Only IKDC and ADLS had this structural aspect of validityinvestigated in individuals with PFPS. Three studies have evaluatedthe factorial structure of IKDC. In the original development studyof the IKDC, Irrgang et al. identified a single dominant componentthat had an eigenvalue much greater (9.03 or 50.2% of the totalvariance) than the others (eigenvalues of 1.76 and 1.19). As a singledominant component was found, they concluded that all questionsshould produce a single total score representing the construct ofsymptoms, function and sports activity [23]. Similarly, Schmittet al. identified a single dominant component with an eigenvalueof 8.64, and suggested a single construct [32]. In contrast, Higginset al. [31] also found a dominant component, but suggestedtwo main constructs, the first being ‘‘symptoms and kneearticulation’’ (11 items, eigenvalue 7.76) and the second being‘‘activity limitations’’ (4 items, eigenvalue 1.11) [31]. Therefore,all three studies identified a single dominant component, butconcluded that the IKDC is a one- or two-dimension scale. As forthe ADLS, its factorial validity has been evaluated in one study.In the original development study of the ADLS, two main factorsaccounted for 61–63% of total score variance [20]. The first factor(eigenvalue 8.2–8.6, 48–51% of total score variance) representsa combination of symptoms and functional limitations commonlyexperienced by individuals with knee impairments, and the secondfactor represents only symptoms (eigenvalue 1.8–2.3, 11–13% oftotal score variance). These two factors correspond to thetwo subscales of the ADLS, which are named ‘‘Symptoms’’ and‘‘Functional Limitations’’.
Floor/ceiling effect
Floor/ceiling effects have been addressed in individuals withPFPS for the five scales included. No floor or ceiling effect was
Table 2. Known-group validity for questionnaires evaluating subjects with PFPS.
ADLS Differentiates adjacent levels of self-perceived severity of PFPS [20]Discriminates adjacent levels of self-perceived and clinician-perceived severity of PFPS [25]‘‘Functional Activities’’ section can differentiate between PFPS and ACL injuries [26]Lower scores for subjects with PFPS compared to knee OA for ‘‘going down the stairs’’, ‘‘standing’’, ‘‘kneeling’’ and ‘‘squatting’’ [36]
AKPS Differentiates subjects with PFPS (83/100) from control subjects (100/100) [21]FIQ Not evaluated in subjects with PFPSIKDC Not evaluated in subjects with PFPSLS Discriminates between ACL injury and PFPS for total score (81.1 versus 73.4) and ‘‘Pain’’ section (21.9 versus 11.5) [42]
Discriminates adjacent levels of self-perceived severity of PFPS [25]
ACL: anterior cruciate ligament; OA: osteoarthritis.
DOI: 10.3109/09638288.2013.774061 Self-reported questionnaires for PFPS 2185
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f L
aval
on
02/1
3/15
For
pers
onal
use
onl
y.
observed as none of the scales had 15% or more of the participantsachieving the highest or the lowest possible scores.
Language and cultural adaptation
The AKPS, ADLS and IKDC have been translated and culturallyadapted to other languages. Psychometric properties of theTurkish [33], Chinese [34] and Persian [35] versions of AKPS,the Turkish [36] and German [26] versions of ADLS, as well asthe Thai [37] and Brazilian Portuguese versions of IKDC [30],have been evaluated in individuals with PFPS. Overall, translatedversions were considered to have adequate content validity for thispopulation, to be easily understood and to have psychometricproperties similar to the original English version.
Administration burden/time to administer
The time to administer the scale has only been established for theThai version of the IKDC (less than 10 minutes to complete thescale with a range of 4–10 min), while the administration burden(time taken to analyze the results) has not been established forindividuals with PFPS [37]. However, qualitatively, ADLS and LSwere described as ‘‘straightforward’’ in terms of time to completeand to calculate scores [25], while the Turkish version of theADLS was reported as ‘‘completed in a short time’’ [36].
Reliability
Test–retest reliability
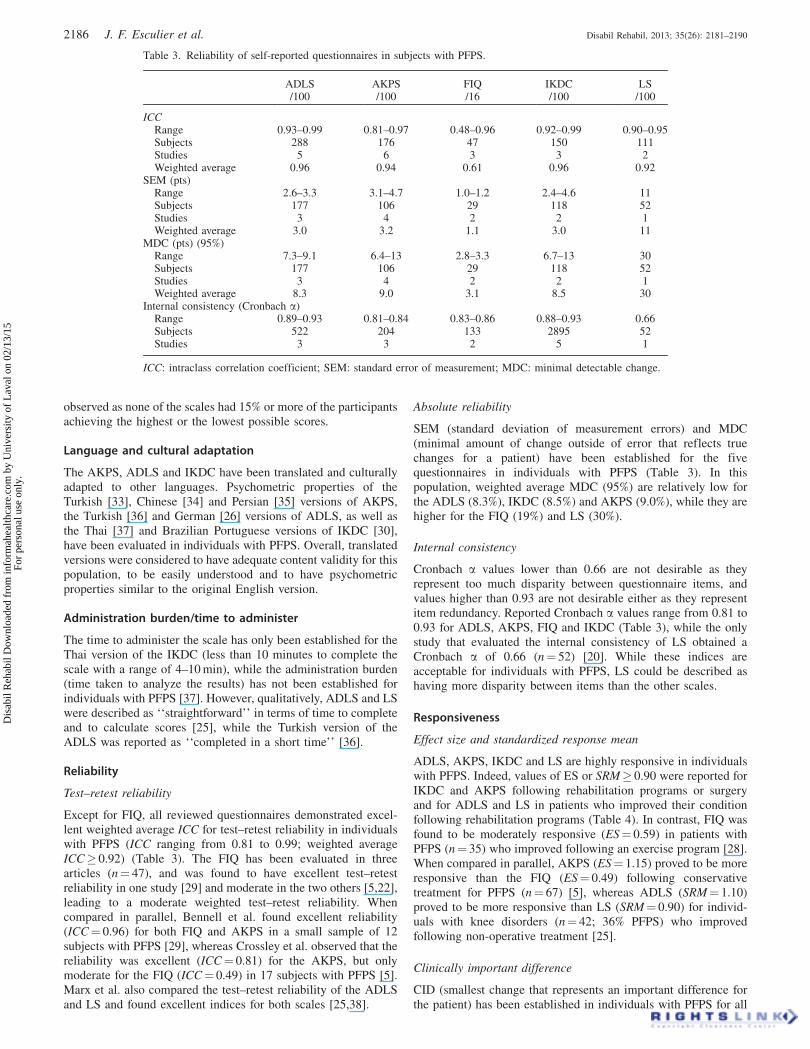
Except for FIQ, all reviewed questionnaires demonstrated excel-lent weighted average ICC for test–retest reliability in individualswith PFPS (ICC ranging from 0.81 to 0.99; weighted averageICC� 0.92) (Table 3). The FIQ has been evaluated in threearticles (n¼ 47), and was found to have excellent test–retestreliability in one study [29] and moderate in the two others [5,22],leading to a moderate weighted test–retest reliability. Whencompared in parallel, Bennell et al. found excellent reliability(ICC¼ 0.96) for both FIQ and AKPS in a small sample of 12subjects with PFPS [29], whereas Crossley et al. observed that thereliability was excellent (ICC¼ 0.81) for the AKPS, but onlymoderate for the FIQ (ICC¼ 0.49) in 17 subjects with PFPS [5].Marx et al. also compared the test–retest reliability of the ADLSand LS and found excellent indices for both scales [25,38].
Absolute reliability
SEM (standard deviation of measurement errors) and MDC(minimal amount of change outside of error that reflects truechanges for a patient) have been established for the fivequestionnaires in individuals with PFPS (Table 3). In thispopulation, weighted average MDC (95%) are relatively low forthe ADLS (8.3%), IKDC (8.5%) and AKPS (9.0%), while they arehigher for the FIQ (19%) and LS (30%).
Internal consistency
Cronbach a values lower than 0.66 are not desirable as theyrepresent too much disparity between questionnaire items, andvalues higher than 0.93 are not desirable either as they representitem redundancy. Reported Cronbach a values range from 0.81 to0.93 for ADLS, AKPS, FIQ and IKDC (Table 3), while the onlystudy that evaluated the internal consistency of LS obtained aCronbach a of 0.66 (n¼ 52) [20]. While these indices areacceptable for individuals with PFPS, LS could be described ashaving more disparity between items than the other scales.
Responsiveness
Effect size and standardized response mean
ADLS, AKPS, IKDC and LS are highly responsive in individualswith PFPS. Indeed, values of ES or SRM� 0.90 were reported forIKDC and AKPS following rehabilitation programs or surgeryand for ADLS and LS in patients who improved their conditionfollowing rehabilitation programs (Table 4). In contrast, FIQ wasfound to be moderately responsive (ES¼ 0.59) in patients withPFPS (n¼ 35) who improved following an exercise program [28].When compared in parallel, AKPS (ES¼ 1.15) proved to be moreresponsive than the FIQ (ES¼ 0.49) following conservativetreatment for PFPS (n¼ 67) [5], whereas ADLS (SRM¼ 1.10)proved to be more responsive than LS (SRM¼ 0.90) for individ-uals with knee disorders (n¼ 42; 36% PFPS) who improvedfollowing non-operative treatment [25].
Clinically important difference
CID (smallest change that represents an important difference forthe patient) has been established in individuals with PFPS for all
Table 3. Reliability of self-reported questionnaires in subjects with PFPS.
ADLS AKPS FIQ IKDC LS/100 /100 /16 /100 /100
ICCRange 0.93–0.99 0.81–0.97 0.48–0.96 0.92–0.99 0.90–0.95Subjects 288 176 47 150 111Studies 5 6 3 3 2Weighted average 0.96 0.94 0.61 0.96 0.92
SEM (pts)Range 2.6–3.3 3.1–4.7 1.0–1.2 2.4–4.6 11Subjects 177 106 29 118 52Studies 3 4 2 2 1Weighted average 3.0 3.2 1.1 3.0 11
MDC (pts) (95%)Range 7.3–9.1 6.4–13 2.8–3.3 6.7–13 30Subjects 177 106 29 118 52Studies 3 4 2 2 1Weighted average 8.3 9.0 3.1 8.5 30
Internal consistency (Cronbach a)Range 0.89–0.93 0.81–0.84 0.83–0.86 0.88–0.93 0.66Subjects 522 204 133 2895 52Studies 3 3 2 5 1
ICC: intraclass correlation coefficient; SEM: standard error of measurement; MDC: minimal detectable change.
2186 J. F. Esculier et al. Disabil Rehabil, 2013; 35(26): 2181–2190
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f L
aval
on
02/1
3/15
For
pers
onal
use
onl
y.

scales, except LS. Crossley et al. (n¼ 67, 100% PFPS) establishedthat the CID was lower for FIQ (1 point; 6.3%) than for AKPS(8 points; 8.0%). In contrast, Watson et al. found a CID of19 points (19%; Sn¼ 0.67, Sp¼ 0.67) for the AKPS (n¼ 30, 70%PFPS) [27]. However, the criteria for a clinically importantchange were different in these two studies [5,27]. As for theADLS, Piva et al. found a CID of 7 points (7.0%) in 60 individualswith PFPS [39]. Finally, a CID of 11.5% (Sn¼ 0.82, Sp¼ 0.64)was observed for the IKDC (n¼ 207); it must be noted, however,that only 9.2% of the sample size was diagnosed with PFPS [8].
Longitudinal validity
Changes in a global rating of change measure correlate moder-ately to strongly (r40.50) with changes in ADLS [20], moder-ately (0.505r50.70) with changes in LS [20] and FIQ [5] andlowly to moderately (0.305r50.70) with changes in AKPS[5,27]. The longitudinal validity of LS was unsatisfactory whenassessed in a cohort of adolescents and young adults with non-traumatic knee complaints, as low correlations (r50.50) wereobserved between changes in LS scores and recovery scores [40].
Discussion
The purpose of this study was to perform a systematic reviewof the psychometric properties of self-reported questionnairesused to assess the level of symptoms and disability of individualswith PFPS. Twenty-four papers about five commonly usedknee-specific scales met all inclusion criteria and were scoredfor their methodological quality. Available psychometric evidencewas compiled and summarized to compare these outcomemeasures for individuals with PFPS.
Based on psychometric evidence of high methodologicalquality, we recommend the use of ADLS for individuals withPFPS. Several factors explain this decision. First, ADLSdemonstrated satisfactory results for all evaluated psychometricproperties. It has been the most extensively studied scale in termsof number of patients with PFPS evaluated for known-groupvalidity, test–retest reliability and responsiveness. Among the fivescales reviewed, ADLS presents the highest weighed average ICCfor test–retest reliability (along with IKDC), and the lowestmeasurement error as defined by the MDC. It has constantlyshown its capacity to discriminate between knee conditions andlevels of severity in individuals with PFPS. In addition, it presentsthe highest responsiveness indices among improved individuals,suggesting that this questionnaire may be more effective indetecting positive treatment outcomes for patients with PFPS.
Finally, in studies evaluating multiple scales, it has been one ofthe top performers in terms of reliability [20,25,38] and respon-siveness [20,25]. With only 14 short questions, it covers commonsymptoms and functional limitations experienced by individualswith PFPS and can be completed in a short period of time.
Evidence also suggests that AKPS and IKDC would beappropriate to use with individuals with PFPS, but someproperties still need to be defined/evaluated in larger samplesbefore proper recommendations can be made. In fact, bothquestionnaires present excellent test–retest reliability, and showadequate validity and responsiveness in the samples evaluated.However, as AKPS has been widely used in clinical trials, it issurprising that responsiveness to change has only been evaluatedin one study in patients suffering from PFPS. Along with known-group validity, responsiveness benchmarks, such as CID, need tobe defined on large sample sizes, as they are the most usefulindices for the clinic. These benchmarks can be used to assistclinicians in determining the amount of change that is clinicallyrelevant and to set short- and long-term goals. AKPS includesspecific questions on common symptoms and functional limita-tions affecting individuals with PFPS, as it is the only includedscale that was purposely developed to assess this particular kneecondition. Even if studies on IKDC were of good methodologicalquality, its ability to differentiate between knee conditions hasnot yet been explored, and its responsiveness to change wasonly evaluated in one study in subjects with PFPS. It remains anexcellent questionnaire to evaluate symptoms and disabilitiescaused by PFPS.
The use of FIQ or LS is not recommended for individualswith PFPS for several reasons. FIQ demonstrates the lowestindices for both test–retest reliability and responsiveness, as wellas the highest measurement errors, as defined by MDC, of allstudied scales for individuals with PFPS. In addition, its known-group validity has never been evaluated in this population. FIQis a very short questionnaire evaluating exclusively functionallimitations, with no questions on symptoms. This would limit itsuse in the clinical setting. The average methodological quality forstudies on FIQ was also low at 68%. As for LS, its test–retestreliability is excellent, but it displays larger measurement errorscompared to ADLS, AKPS and IKDC [20]. The LS is moderatelyto highly responsive to change, but its longitudinal validityin young adults with non-traumatic knee injuries has beenquestioned [40], as this questionnaire was originally developedto assess ligamentous injuries. Thirty percent of its total scoreis related to knee instability, which is not a predominant symptomin PFPS.
Table 4. Responsiveness to change of self-reported questionnaires in subjects with PFPS.
ADLS AKPS FIQ IKDC LS
ES, all subjectsRange 0.63–1.26 1.15 0.32–1.29 1.13 0.76–1.13No. of subjects (no. of studies) 239 (2) 67 (1) 133 (3) 207 (1) 315 (2)Weighted average 1.10 1.15 0.49 1.13 0.97
ES, improved subjectsRange 1.19 N/E 0.59 N/E N/ENo. of subjects (no. of studies) 36 (1) 35 (1)Weighted average 1.19 0.59
SRM, all subjectsRange N/E N/E N/E 0.94 0.73No. of subjects (no. of studies) 207 (1) 136 (1)Weighted average 0.94 0.73
SRM, improved subjectsRange 1.10 N/E N/E N/E 0.90No. of subjects (no. of studies) 42 (1) 42 (1)Weighted average 1.10 0.90
ES: effect size; SRM: standardized response mean; N/E: not evaluated.
DOI: 10.3109/09638288.2013.774061 Self-reported questionnaires for PFPS 2187
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f L
aval
on
02/1
3/15
For
pers
onal
use
onl
y.

Mostly high correlations were found (0.705r50.90)between the included knee-specific questionnaires (three studiesfound high correlations, one study moderate correlations).This is not surprising as all the studied scales, except for theFIQ, include construct-oriented items on symptoms and func-tional limitations commonly encountered by patients sufferingfrom knee disorders. Moderate correlation between FIQ andAKPS could be attributed to the focus of FIQ on functionalactivities and lacking items concerned with symptoms.Furthermore, the weak to moderate correlations found betweenthe studied knee-specific questionnaires and the physical andmental components of the SF-36/SF-12 were to be expected,as the latter represents general health constructs which arenot likely to be highly correlated with constructs evaluated inknee-specific scales.
In the present systematic review, the use of the ADLSis recommended for individuals with PFPS. As previouslymentioned, three other reviews pertaining to the measurementproperties of self-reported scales used for individuals with kneepain have been published. In these reviews, different question-naires were recommended for individuals with PFPS. Onerecommended IKDS or KOOS, while the two others recom-mended AKPS. In contrast to our systematic review, none of thesereviews were specific to PFPS, used multiple raters for criticalappraisal, nor performed a quantitative synthesis of the studiesreviewed. Finally, one of these reviews was narrative with nosystematic search strategy. In the present review, our systematicsearch strategy allowed retrieving more articles about psycho-metric properties of scales for PFPS than previous reviews.We also used an appraisal tool to evaluate the methodologicalquality of included studies. Critical appraisal is recognized asa fundamental component of a systematic review [12]. Therecent development of structured critical appraisal scales foranalyzing the quality of psychometric studies now allows for amore structured approach. It was therefore possible to conducta systematic review using validated critical appraisal scalesto analyze both the quality and the content of psychometricevidences.
Several self-administered questionnaires assessing knee dis-orders have been developed over the past few years, and five wereincluded in this systematic review. Considering that severalstudies are necessary to make meaningful recommendations andconclusions about a questionnaire, we therefore only kept forfurther analysis questionnaires that had at least five publicationsevaluating their psychometric properties on individuals withPFPS. Using this criterion, 10 questionnaires had to be excluded,as their psychometric properties had not been sufficientlyevaluated in individuals with PFPS (Patellofemoral PainSyndrome Severity Scale [43], Lower Extremity FunctionalScale [27,44,45], Western Ontario and McMaster UniversitiesArthritis Index [30,40], Patient Specific Functional Scale [46],Flandry questionnaire [29,47], Edinburgh Knee Function Scale[48], Patellofemoral Function Scale [28], American Academyof Orthopaedic Surgeons Sports Knee-Rating Scale [25,38],Cincinnati Knee Rating Scale [25,38,49,50], MultidimensionalPain Inventory [51]). This led to the exclusion of nine articles[43–51]. Therefore, we cannot exclude the possibility that asuperior questionnaire exists. Future systematic reviews mightconsider other questionnaires when an appropriate quantityof evidence becomes available. A second limitation of thissystematic review is that all studies involving individuals withPFPS were kept for analysis, even the ones where other kneeconditions were included in studied samples. In fact, only ninepsychometric studies were performed exclusively on individualssuffering from PFPS; thus to make meaningful recommendations,all evidence had to be included. However, the percentage of
participants with PFPS in included studies was considered whenrecommendations were established.
Conclusion
Several self-reported questionnaires have been developedto assess the level of symptoms and disability of individualssuffering from knee pain. Based on the results from thissystematic review, we recommend the use of the ADLS whenevaluating patients with PFPS, as this scale has adequate validityand excellent indices of reliability and responsiveness. Thisrecommendation is based on high methodological quality studiesperformed in this population. IKDC and AKPS also demonstratedgood psychometric properties and seem to be adequate for thisspecific population. However, further high methodological qualitystudies are needed on large sample size before formal recom-mendations can be made. FIQ and LS are not recommended.Future studies should focus on the lack of evidence on respon-siveness and known-group validity for most of the studied scales.
Declaration of interest
This study was supported by a grant from the ‘‘OrdreProfessionnel de la Physiotherapie du Quebec (OPPQ)’’. Thefunding source was not involved in the study’s design, conduct orreporting. The authors report no conflicts of interest. The authorsalone are responsible for the content and writing of this article.
References
1. Taunton JE, Ryan MB, Clement DB, et al. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med 2002;36:95–101.
2. van Middelkoop M, van Linschoten R, Berger MY, et al. Kneecomplaints seen in general practice: active sport participants versusnon-sport participants. BMC Musculoskelet Disord 2008;9:36.
3. Fredericson M, Yoon K. Physical examination and patellofemoralpain syndrome. Am J Phys Med Rehabil 2006;85:234–43.
4. Witvrouw E, Werner S, Mikkelsen C, et al. Clinical classificationof patellofemoral pain syndrome: guidelines for non-operativetreatment. Knee Surg Sports Traumatol Arthrosc 2005;13:122–30.
5. Crossley KM, Bennell KL, Cowan SM, Green S. Analysis ofoutcome measures for persons with patellofemoral pain: which arereliable and valid? Arch Phys Med Rehabil 2004;85:815–22.
6. Heintjes E, Berger MY, Bierma-Zeinstra SM, et al. Exercise therapyfor patellofemoral pain syndrome. Cochrane Database Syst Rev2003;4:CD003472.
7. Earl JE, Hoch AZ. A proximal strengthening program improvespain, function, and biomechanics in women with patellofemoral painsyndrome. Am J Sports Med 2011;39:154–63.
8. Irrgang JJ, Anderson AF, Boland AL, et al. Responsiveness of theinternational knee documentation committee subjective knee form.Am J Sports Med 2006;34:1567–73.
9. Wright RW. Knee injury outcomes measures. J Am Acad OrthopSurg 2009;17:31–9.
10. Wang D, Jones MH, Khair MM, Miniaci A. Patient-reportedoutcome measures for the knee. J Knee Surg 2010;23:137–51.
11. Howe TE, Dawson LJ, Syme G, et al. Evaluation of outcomemeasures for use in clinical practice for adults with musculoskeletalconditions of the knee: a systematic review. Man Ther 2012;17:100–18.
12. Portney LG, Watkins MP. Foundations of clinical research: appli-cations to practice. 3rd ed. Upper Saddle River (NJ): PearsonEducation Inc.; 2009.
13. Law M, MacDermid J. Evidence-based rehabilitation: a guide topractice. 2nd ed. Thorofare (NJ): Slack Inc.; 2008.
14. MacDermid JC, Walton DM, Avery S, et al. Measurement propertiesof the neck disability index: a systematic review. J Orthop SportsPhys Ther 2009;39:400–17.
15. Roy JS, Desmeules F, MacDermid J. Psychometric propertiesof presenteeism scales for musculoskeletal disorders: a systematicreview. J Rehabil Med 2011;43:23–31.
2188 J. F. Esculier et al. Disabil Rehabil, 2013; 35(26): 2181–2190
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f L
aval
on
02/1
3/15
For
pers
onal
use
onl
y.

16. Roy JS, MacDermid JC, Woodhouse LJ. Measuring shoulderfunction: a systematic review of four questionnaires. ArthritisRheum 2009;61:623–32.
17. Streiner DL, Norman GR, eds. Reliability. In: Health measurementscales: a practical guide to their development and use. 2nd ed.New York (NY): Oxford University Press; 1995:104–27.
18. Cohen J. Applied multiple regression/correlation analysis forthe behavioral sciences. Hillsdale (NJ): Lawrence ErlbaumAssociates; 1983.
19. Munro BH. Statistical methods for health care research. Philadelphia(PA): JB Lippincott; 2000.
20. Irrgang JJ, Snyder-Mackler L, Wainner RS, et al. Development of apatient-reported measure of function of the knee. J Bone Joint Surg1998;80:1132–45.
21. Kujala UM, Jaakkola LH, Koskinen SK, et al. Scoring ofpatellofemoral disorders. Arthroscopy 1993;9:159–63.
22. Chesworth BM, Culham E, Tata GE, Peat M. Validation of outcomemeasures in patients with patellofemoral syndrome. J Orthop SportsPhys Ther 1989;10:302–8.
23. Irrgang JJ, Anderson AF, Boland AL, et al. Development andvalidation of the international knee documentation committeesubjective knee form. Am J Sports Med 2001;29:600–13.
24. Tegner Y, Lysholm J. Rating systems in the evaluation of kneeligament injuries. Clin Orthop Relat Res 1985;198:43–9.
25. Marx RG, Jones EC, Allen AA, et al. Reliability, validity, andresponsiveness of four knee outcome scales for athletic patients.J Bone Joint Surg Am 2001;83A:1459–69.
26. Bizzini M, Gorelick M. Development of a German version of theknee outcome survey for daily activities. Arch Orthop Trauma Surg2007;127:781–9.
27. Watson CJ, Propps M, Ratner J, et al. Reliability and responsivenessof the lower extremity functional scale and the anterior knee painscale in patients with anterior knee pain. J Orthop Sports Phys Ther2005;35:136–46.
28. Harrison E, Quinney H, Magee D, et al. Analysis of outcomemeasures used in the study of patellofemoral pain syndrome.Physiother Can 1995;47:264–72.
29. Bennell K, Bartam S, Crossley K, Green S. Outcome measuresin patellofemoral pain syndrome: test retest reliability and inter-relationships. Phys Ther Sport 2000;1:32–41.
30. Metsavaht L, Leporace G, Riberto M, et al. Translation and cross-cultural adaptation of the Brazilian version of the InternationalKnee Documentation Committee Subjective Knee Form: validityand reproducibility. Am J Sports Med 2010;38:1894–9.
31. Higgins LD, Taylor MK, Park D, et al. Reliability and validity of theInternational Knee Documentation Committee (IKDC) SubjectiveKnee Form. Joint Bone Spine 2007;74:594–9.
32. Schmitt LC, Paterno MV, Huang S. Validity and internal consistencyof the international knee documentation committee subjective kneeevaluation form in children and adolescents. Am J Sports Med 2010;38:2443–7.
33. Kuru T, Dereli EE, Yaliman A. Validity of the Turkish version ofthe Kujala patellofemoral score in patellofemoral pain syndrome.Acta Orthop Traumatol Turc 2010;44:152–6.
34. Cheung RTH, Ngai SPC, Lam PL, et al. Chinese translation andvalidation of the Kujala scale for patients with patellofemoral pain.Disabil Rehabil 2012;34:510–13.
35. Negahban H, Pouretezad M, Shaterzadeh Yazdi MJ, et al. Persiantranslation and validation of the Kujala Patellofemoral Scale inpatients with patellofemoral pain syndrome. Disabil Rehabil2012;34:2259–63.
36. Evcik D, Ay S, Ege A, et al. Adaptation and validation of turkishversion of the knee outcome survey-activities for daily living scale.Clin Orthop Relat Res 2009;467:2077–82.
37. Lertwanich P, Praphruetkit T, Keyurapan E, et al. Validity andreliability of Thai version of the International Knee DocumentationCommittee Subjective Knee Form. J Med Assoc Thai 2008;91:1218–25.
38. Marx RG, Menezes A, Horovitz L, et al. A comparison of two timeintervals for test-retest reliability of health status instruments. J ClinEpidemiol 2003;56:730–5.
39. Piva SR, Gil AB, Moore CG, Fitzgerald GK. Responsiveness ofthe activities of daily living scale of the knee outcome surveyand numeric pain rating scale in patients with patellofemoral pain.J Rehabil Med 2009;41:129–35.
40. Heintjes EM, Bierma-Zeinstra SMA, Berger MY, Koes BW.Lysholm scale and WOMAC index were responsive in prospectivecohort of young general practice patients. J Clin Epidemiol 2008;61:481–8.
41. MacIntyre DL, Hopkins PM, Harris SR. Evaluation of pain andfunctional activity in patellofemoral pain syndrome: reliability andvalidity of two assessment tools. Physiother Can 1995;47:164–70.
42. Bengtsson J, Mollborg J, Werner S. A study for testing thesensitivity and reliability of the Lysholm knee scoring scale.Knee Surg Sports Traumatol Arthrosc 1996;4:27–31.
43. LaPrade JA, Culham EG. A self-administered pain severity scale forpatellofemoral pain syndrome. Clin Rehabil 2002;15:780–8.
44. Binkley JM, Stratford PW, Lott SA, Riddle DL. The LowerExtremity Functional Scale (LEFS): scale development, measure-ment properties, and clinical application. Phys Ther 1999;79:371–83.
45. Cacchio A, De Blasis E, Necozione S, et al. The Italian version ofthe lower extremity functional scale was reliable, valid, andresponsive. J Clin Epidemiol 2010;63:550–7.
46. Chatman AB, Hyams SP, Neel JM, et al. The Patient-SpecificFunctional Scale: measurement properties in patients with kneedysfunction. Phys Ther 1997;77:820–9.
47. Hoher J, Munster A, Klein J, et al. Validation and application of asubjective knee questionnaire. Knee Surg Sports Traumatol Arthrosc1995;3:26–33.
48. Leigh Brown AP, Kennedy ADM, Grant AM, et al. The develop-ment and validation of the EKFS- a simple tool for outcomemeasurement in non-surgical patients. Knee 1999;6:115–23.
49. Barber-Westin SD, Noyes FR, McCloskey JW. Rigorous statisticalreliability, validity, and responsiveness testing of the CincinnatiKnee Rating Scale. Am J Sports Med 1999;27:402–16.
50. Jensen R, Hystad T, Baerheim A. Knee function and pain relatedto psychological variables in patients with long-termpatellofemoral pain syndrome. J Orthop Sports Phys Ther 2005;35:594–600.
51. Thomee P, Thomee R, Karlsson J. Patellofemoral pain syndrome:pain, coping strategies and degree of well-being. Scand J Med SciSports 2002;12:276–81.
DOI: 10.3109/09638288.2013.774061 Self-reported questionnaires for PFPS 2189
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f L
aval
on
02/1
3/15
For
pers
onal
use
onl
y.
Appendix. Consensus results to the critical appraisal tool for every reviewed article
Critical appraisal tool itemsa
Reference article Item 1 Item 2 Item 3 Item 4 Item 5 Item 6 Item 7 Item 8 Item 9 Item 10 Item 11 Item 12Totalscore %
Chesworth et al. [22] 1 2 0 1 0 0 2 1 2 1 0 1 11 46Kujala et al. [21] 0 1 1 1 0 N/A 1 0 2 2 0 1 9 41Harrison et al. [28] 2 2 1 2 0 2 2 2 2 1 1 0 17 71MacIntyre et al. [41] 2 1 1 1 0 N/A 2 2 2 1 0 1 13 59Bengtsson et al. [42] 2 1 1 1 0 N/A 2 2 1 1 0 0 11 50Irrgang et al. [20] 2 1 2 2 1 0 2 2 2 2 1 1 18 75Bennell et al. [29] 2 2 1 2 0 N/A 2 2 2 2 2 2 19 86Irrgang et al. [23] 2 2 2 2 1 N/A 2 2 2 2 2 2 21 95Marx et al. [25] 1 2 2 2 2 N/A 2 2 2 2 1 2 20 91Marx et al. [38] 0 2 2 1 2 1 2 2 2 2 2 2 20 83Crossley et al. [5] 1 1 1 2 0 2 2 2 2 2 2 2 19 79Watson et al. [27] 2 2 2 2 0 1 2 2 2 2 2 1 20 83Irrgang et al. [8] 1 2 2 2 1 0 2 2 2 2 2 2 20 83Bizzini & Gorelick [26] 2 1 1 2 1 N/A 2 2 2 2 2 1 18 82Higgins et al. [31] 2 1 1 2 1 N/A 2 2 2 2 2 2 19 86Lertwanich et al. [37] 1 1 1 2 0 0 2 2 2 2 1 2 16 67Heintjes et al. [40] 2 1 2 2 1 1 2 2 2 2 1 2 20 80Evcik et al. [36] 2 2 1 2 2 N/A 2 2 2 2 2 2 21 95Piva et al. [39] 2 2 1 2 0 1 2 2 2 2 2 1 19 79Kuru et al. [33] 1 1 1 1 0 N/A 2 1 2 1 1 1 12 55Metsavaht et al. [30] 2 1 1 2 1 N/A 2 1 2 2 2 2 18 82Schmitt et al. [32] 2 1 1 2 1 N/A 2 2 2 2 1 2 18 82Cheung et al. [34] 1 1 1 2 0 N/A 1 0 2 2 0 1 11 50Negahban et al. [35] 2 2 2 2 1 0 2 2 2 2 2 2 21 88
N/A: Not applicable.aItem 1: thorough literature review to define the research question; Item 2: specific inclusion/exclusion criteria; Item 3: specific hypotheses; Item 4:
appropriate scope of psychometric properties; Item 5: sample size calculation/justification; Item 6: appropriate retention/follow-up; Item 7: authorsreferenced specific procedures for administration, scoring and interpretation of procedures; Item 8: measurement techniques were standardized; Item9: data were presented for each hypothesis; Item 10: appropriate statistics-point estimate; Item 11: appropriate statistical error estimates; Item 12:valid conclusions and clinical recommendations.
2190 J. F. Esculier et al. Disabil Rehabil, 2013; 35(26): 2181–2190
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f L
aval
on
02/1
3/15
For
pers
onal
use
onl
y.
Copyright © 2022 FDOKUMEN




















