Involvement of interleukin-18 in the inflammatory response against oropharyngeal candidiasis
Upload
healthfoodinnovationmanagementCategory
view
2download
0
REVIEW ARTICLE
Psychometric Characteristics of Health-Related Quality-of-LifeQuestionnaires in Oropharyngeal Dysphagia
Angelique A. Timmerman • Renee Speyer •
Bas J. Heijnen • Iris R. Klijn-Zwijnenberg
Received: 16 July 2013 / Accepted: 14 December 2013 / Published online: 5 March 2014
� Springer Science+Business Media New York 2014
Abstract Dysphagia can have severe consequences for
the patient’s health, influencing health-related quality of
life (HRQoL). Sound psychometric properties of HRQoL
questionnaires are a precondition for assessing the impact
of dysphagia, the focus of this study, resulting in recom-
mendations for the appropriate use of these questionnaires
in both clinical practice and research contexts. We per-
formed a systematic review starting with a search for and
retrieval of all full-text articles on the development of
HRQoL questionnaires related to oropharyngeal dysphagia
and/or their psychometric validation from the electronic
databases PubMed and Embase published up to June 2011.
Psychometric properties were judged according to quality
criteria proposed for health status questionnaires. Eight
questionnaires were included in this study. Four are aimed
solely at HRQoL in oropharyngeal dysphagia: the deglu-
tition handicap index (DHI), dysphagia handicap index
(DHI0), M.D. Anderson Dysphagia Inventory (MDADI),
and SWAL-QOL, while the EDGQ, EORTC QLQ-STO 22,
EORTC QLQ-OG 25 and EORTC QLQ-H&N35 focus on
other primary diseases resulting in dysphagia. The psy-
chometric properties of the DHI, DHI0, MDADI, and
SWAL-QOL were evaluated. For appropriate applicability
of HRQoL questionnaires, strong scores on the psycho-
metric criteria face validity, criterion validity, and inter-
pretability are prerequisites. The SWAL-QOL has the
strongest ratings for these criteria, while the DHI0 is the
most easy to apply given its 25 items and the use of a
uniform scoring format. For optimal use of HRQoL ques-
tionnaires in diverse settings, it is necessary to combine
psychometric and utility approaches.
Keywords Oropharyngeal dysphagia � Health-related
quality of life � Questionnaires � Psychometric
characteristics � Deglutition � Deglutition disorders
Introduction
In clinical care there is a growing prevalence of chronic
over infectious diseases given the rise in life expectancy
since the 19th century due to better life conditions and
quality of care, resulting in a shift from cure to care when
measuring the effectiveness of treatment, i.e., from ‘‘life-
saving’’ to ‘‘life quality’’ [1, 2].
Quality of life (QoL) as a concept has increasingly been
recognized and used as an outcome measure of the effect of
(chronic) medical conditions (and their treatment) on daily
functioning, in agreement with the World Health Organi-
zation’s definition of health as ‘‘a state of complete phys-
ical, mental and social well-being, not merely the absence
of disease or infirmity’’ [3–5]. QoL has been broadly op-
erationalized as health-related quality of life (HRQoL) in
conceptual models and resulting instruments, and also
A. A. Timmerman (&)
Department of Family Medicine, Maastricht University,
PO Box 616, 6200 MD Maastricht, The Netherlands
e-mail: [email protected]
R. Speyer
School of Public Health, Tropical Medicine and Rehabilitation
Sciences, James Cook University, 43, James Cook Drive,
Townsville, QLD 4811, Australia
R. Speyer � B. J. Heijnen
Department of Otorhinolaryngology and Head and Neck
Surgery, Leiden University Medical Center, PO Box 9600,
2300 RC Leiden, The Netherlands
I. R. Klijn-Zwijnenberg
Emergency Medicine, Jeroen Bosch Hospital, Henri
Dunantstraat 1, 5223 GZ Den Bosch, The Netherlands
123
Dysphagia (2014) 29:183–198
DOI 10.1007/s00455-013-9511-8
includes symptom status, functional limitations (physical,
psychological, and social domains), and general health
perceptions as outcome measures. Functional health status
(FHS) is defined as the ability to perform tasks in multiple
domains (physical, social, role, and psychological func-
tioning) and measures the focus on (loss of) function due to
disease and/or treatment and the effects on daily life [6–9].
HRQoL measures are usually self-administered and
share a focus on the personal well-being of the patient in
broader personal and social contexts as relate to disease
(preferences for) treatment, disability, impairment, and
health [6–9]. Dysphagia is an example of a chronic con-
dition that usually has a big impact on the health and well-
being of patients because difficulty swallowing affects the
ability to eat and drink. The condition is often considered
symptom of another disease, e.g., head and neck cancer,
reflux, or Parkinson’s disease [10, 11]. In the literature, the
incidence of dysphagia in adults is described as ranging
from 6 to 50 % depending on the patient population studied
or the screening method used (e.g., videofluoroscopy or
fiberoptic endoscopy of the swallowing act) [12–14].
Dysphagia can have severe consequences for the patient’s
health as it can lead to dehydration, malnutrition, and
aspiration pneumonia [15, 16]. Dysphagia may show
effects on a psychological level, where risks of suffocation,
severe coughing, and vomiting may cause an increase in
anxiety and lower self-esteem [12]. From a social per-
spective, mealtimes may be very stressful and going to a
restaurant may no longer be a pleasure [17, 18].
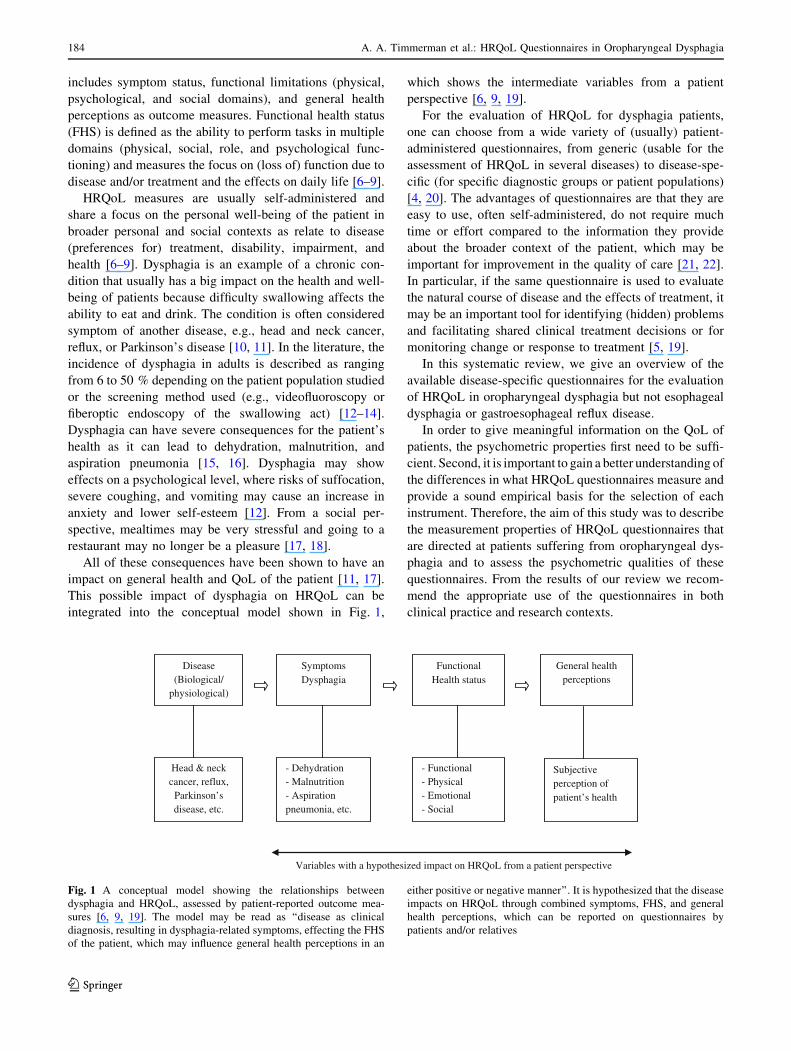
All of these consequences have been shown to have an
impact on general health and QoL of the patient [11, 17].
This possible impact of dysphagia on HRQoL can be
integrated into the conceptual model shown in Fig. 1,
which shows the intermediate variables from a patient
perspective [6, 9, 19].
For the evaluation of HRQoL for dysphagia patients,
one can choose from a wide variety of (usually) patient-
administered questionnaires, from generic (usable for the
assessment of HRQoL in several diseases) to disease-spe-
cific (for specific diagnostic groups or patient populations)
[4, 20]. The advantages of questionnaires are that they are
easy to use, often self-administered, do not require much
time or effort compared to the information they provide
about the broader context of the patient, which may be
important for improvement in the quality of care [21, 22].
In particular, if the same questionnaire is used to evaluate
the natural course of disease and the effects of treatment, it
may be an important tool for identifying (hidden) problems
and facilitating shared clinical treatment decisions or for
monitoring change or response to treatment [5, 19].
In this systematic review, we give an overview of the
available disease-specific questionnaires for the evaluation
of HRQoL in oropharyngeal dysphagia but not esophageal
dysphagia or gastroesophageal reflux disease.
In order to give meaningful information on the QoL of
patients, the psychometric properties first need to be suffi-
cient. Second, it is important to gain a better understanding of
the differences in what HRQoL questionnaires measure and
provide a sound empirical basis for the selection of each
instrument. Therefore, the aim of this study was to describe
the measurement properties of HRQoL questionnaires that
are directed at patients suffering from oropharyngeal dys-
phagia and to assess the psychometric qualities of these
questionnaires. From the results of our review we recom-
mend the appropriate use of the questionnaires in both
clinical practice and research contexts.
Variables with a hypothesized impact on HRQoL from a patient perspective
Disease(Biological/
physiological)
Symptoms Dysphagia
Functional Health status
General health perceptions
Head & neck cancer, reflux,
Parkinson’s disease, etc.
- Dehydration - Malnutrition - Aspiration pneumonia, etc.
- Functional - Physical - Emotional - Social
Subjective perception of patient’s health
Fig. 1 A conceptual model showing the relationships between
dysphagia and HRQoL, assessed by patient-reported outcome mea-
sures [6, 9, 19]. The model may be read as ‘‘disease as clinical
diagnosis, resulting in dysphagia-related symptoms, effecting the FHS
of the patient, which may influence general health perceptions in an
either positive or negative manner’’. It is hypothesized that the disease
impacts on HRQoL through combined symptoms, FHS, and general
health perceptions, which can be reported on questionnaires by
patients and/or relatives
184 A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia
123

Methods
A literature search was conducted independently by two
reviewers using the electronic databases PubMed and
Embase. All available inclusion dates up to January 2010
were used, followed by another literature search for the
period between January 2010 and June 2011 as an update.
The search was limited to English, German, French,
Spanish, and Dutch publications. MeSH or thesaurus terms
were supplemented by using free-text words (for the period
after January 2009). In PubMed, the MeSH terms deglu-
tition disorders and QoL were combined, and in Embase,
the thesaurus terms dysphagia and QoL, quality of life
index were used. To retrieve the most recent publications
(after January 2009), one of the free-text words dysphagia,
deglutition, and swallow was combined with QoL in both
databases..
All abstracts were read and all full text articles that
about the development of HRQoL questionnaires related
to oropharyngeal dysphagia and/or the psychometric
validation of those questionnaires were retrieved. The
following articles were excluded: (1) reviews, case
reports, and editorials; (2) articles on questionnaires not
related to oropharyngeal dysphagia, e.g., esophageal
dysphagia; (3) articles on questionnaires solely concerned
with FHS; (4) articles on generic questionnaires; (5)
articles in which the questionnaire was not the subject of
the study; and (6) studies without an adult patient
population.
The reference lists of all included articles were sear-
ched for additional literature on the subject. For each
included questionnaire an extended search was executed
to check whether all articles concerning its development
and validation were retrieved. The names of each ques-
tionnaire were combined with each of the MeSH terms
psychometrics, reproducibility of results, validation
studies as topic, and validation studies [publication type]
in PubMed and the thesaurus terms reliability, psy-
chometry, validity, validation study, and instrument vali-
dation in Embase. Difference of opinion on whether an
article should be included were settled by group discus-
sion to reach a consensus. The psychometric properties of
the questionnaires were judged using the quality criteria
for the measurement properties of health status ques-
tionnaires proposed by Terwee et al. [23] and adapted by
Timmerman et al. [24] for application in otitis media
with effusion. Any indeterminate psychometric ratings
were discussed and resolved in a consensus meeting by
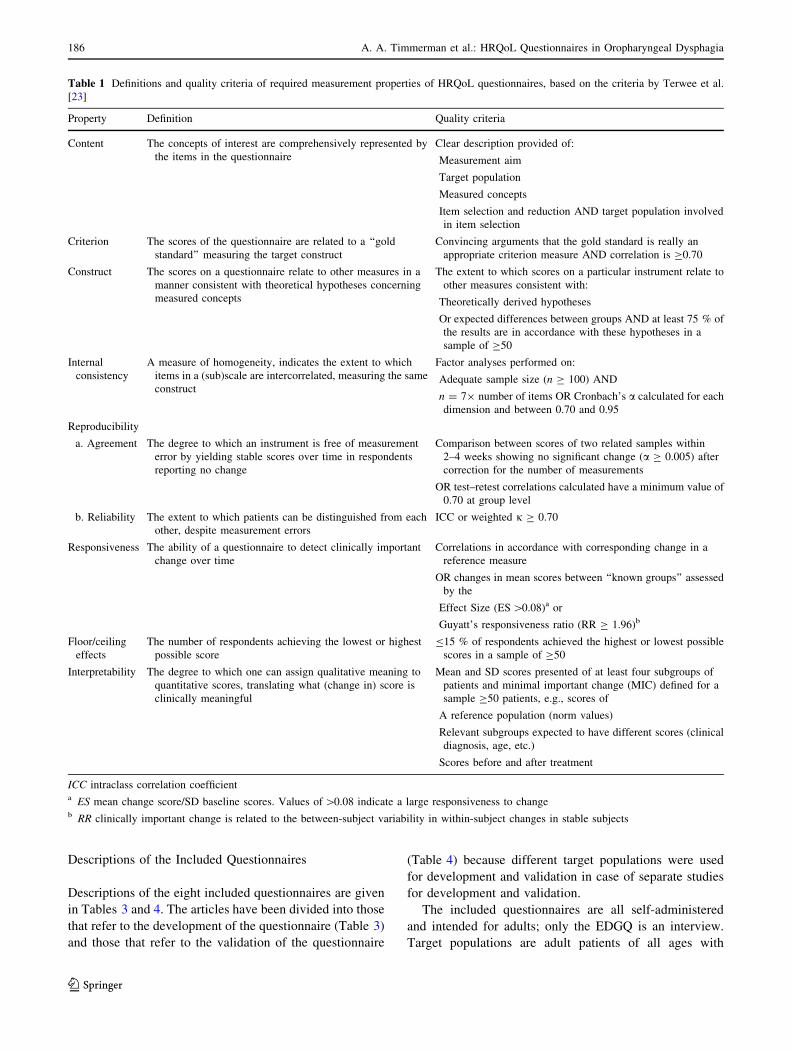
two of the authors (AT and RS). The definitions and
quality criteria of the ten psychometric properties used
for the evaluation of the questionnaires are shown in
Table 1.
Results
Findings of the Literature Search
The literature search using MeSH or thesaurus terms found
819 articles in PubMed and 966 in Embase. Another 112
articles were extracted from PubMed and 180 from Embase
using free-text words. From these articles a total of 1,923
references were found from both databases up to January
2010: 904 from PubMed articles and 1,019 from Embase
articles. The search update for the period January 2010 to
June 2011 yielded 827 articles, 73 from PubMed and 240
from Embase. When using free-text words, 210 and 304
references were found from PubMed and Embase articles,
respectively. Eighteen articles were included from the
initial search because they described the development of an
original questionnaire and/or the validation process of a
questionnaire related to oropharyngeal dysphagia. Table 2
lists the 14 questionnaires discussed in the included articles
and the reasons for final inclusion in or exclusion from this
study. The selection process excluded the following six
questionnaires: the University of Washington quality of life
questionnaire (UW QOL) [25], the head and neck quality
of life instrument (HNQOL) [26], and the European orga-
nisation for the research and treatment of cancer quality of
life questionnaire, module for the assessment of esophageal
cancer (EORTC QLQ-OES 18) [27] because they evaluate
only FHS, not HRQoL or they are related to head and neck
cancer or esophageal cancer; the functional assessment of
cancer therapy-head and neck scale (FACT-HN) [28] and
the Self-report symptom inventory [29] because they con-
tain too few items on oropharyngeal dysphagia-related
HRQoL; and the Klugman Quality of Life (QoL) ques-
tionnaire because it is an interview with open-ended
questions only [30].
The initially included questionnaires were SWAL-QOL
[31–33], M.D. Anderson dysphagia inventory (MDADI)
[34], deglutition handicap index (DHI) [35], dysphagia
handicap index (DHI0) [36], and the European dysphagia
group questionnaire (EDGQ) [12] and three questionnaires
that were modules developed for specific patient popula-
tions and used as a supplement to the European organisa-
tion for the research and treatment of cancer quality of life
questionnaire (QLQ-C30) [37]: the gastric cancer module
(EORTC QLQ-STO22) [38, 39], the esophageal, esoph-
agogastric junction, or gastric cancer module (EORTC
QLQ-OG25) [40], and the head and neck cancer module
(EORTC QLQ-H&N35) [41, 42]. (The number in the name
of the questionnaire indicates the number of items: 22
items in the QLQ-STO22, 25 in the QLQ-OG25, and 35 in
the QLQ-H&N35.) The final questionnaire was found in
the search update in June 2010: the DHI0 [36].
A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia 185
123
Descriptions of the Included Questionnaires
Descriptions of the eight included questionnaires are given
in Tables 3 and 4. The articles have been divided into those
that refer to the development of the questionnaire (Table 3)
and those that refer to the validation of the questionnaire
(Table 4) because different target populations were used
for development and validation in case of separate studies
for development and validation.
The included questionnaires are all self-administered
and intended for adults; only the EDGQ is an interview.
Target populations are adult patients of all ages with
Table 1 Definitions and quality criteria of required measurement properties of HRQoL questionnaires, based on the criteria by Terwee et al.
[23]
Property Definition Quality criteria
Content The concepts of interest are comprehensively represented by
the items in the questionnaire
Clear description provided of:
Measurement aim
Target population
Measured concepts
Item selection and reduction AND target population involved
in item selection
Criterion The scores of the questionnaire are related to a ‘‘gold
standard’’ measuring the target construct
Convincing arguments that the gold standard is really an
appropriate criterion measure AND correlation is C0.70
Construct The scores on a questionnaire relate to other measures in a
manner consistent with theoretical hypotheses concerning
measured concepts
The extent to which scores on a particular instrument relate to
other measures consistent with:
Theoretically derived hypotheses
Or expected differences between groups AND at least 75 % of
the results are in accordance with these hypotheses in a
sample of C50
Internal
consistency
A measure of homogeneity, indicates the extent to which
items in a (sub)scale are intercorrelated, measuring the same
construct
Factor analyses performed on:
Adequate sample size (n C 100) AND
n = 79 number of items OR Cronbach’s a calculated for each
dimension and between 0.70 and 0.95
Reproducibility
a. Agreement The degree to which an instrument is free of measurement
error by yielding stable scores over time in respondents
reporting no change
Comparison between scores of two related samples within
2–4 weeks showing no significant change (a C 0.005) after
correction for the number of measurements
OR test–retest correlations calculated have a minimum value of
0.70 at group level
b. Reliability The extent to which patients can be distinguished from each
other, despite measurement errors
ICC or weighted j C 0.70
Responsiveness The ability of a questionnaire to detect clinically important
change over time
Correlations in accordance with corresponding change in a
reference measure
OR changes in mean scores between ‘‘known groups’’ assessed
by the
Effect Size (ES [0.08)a or
Guyatt’s responsiveness ratio (RR C 1.96)b
Floor/ceiling
effects
The number of respondents achieving the lowest or highest
possible score
B15 % of respondents achieved the highest or lowest possible
scores in a sample of C50
Interpretability The degree to which one can assign qualitative meaning to
quantitative scores, translating what (change in) score is
clinically meaningful
Mean and SD scores presented of at least four subgroups of
patients and minimal important change (MIC) defined for a
sample C50 patients, e.g., scores of
A reference population (norm values)
Relevant subgroups expected to have different scores (clinical
diagnosis, age, etc.)
Scores before and after treatment
ICC intraclass correlation coefficienta ES mean change score/SD baseline scores. Values of [0.08 indicate a large responsiveness to changeb RR clinically important change is related to the between-subject variability in within-subject changes in stable subjects
186 A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia
123

oropharyngeal dysphagia (DHI [35], DHI0 [36], EDGQ
[12], and SWAL-QOL [31–33]), head and neck cancer
(MDADI [34] and EORTC QLQ-H&N35 [41, 42]), cancer
of the esophagus, the esophagogastric junction, or the
stomach (EORTC QLQ-OG25 [40]), and gastric cancer
(EORTC QLQ-STO22 [38, 39]). The patients included in
the development studies came mostly from private clinics
and hospitals across Europe or the US and ranged in
number from 52 patients for SWAL-QOL to 360 patients
for EDGQ. For the DHI there was one group of 96 patients
from one hospital (France) and a control group of 53
healthy people included (see Table 3). The EORTC QLQ-
STO22 was developed using a group of 58 patients and a
control group of 24 health professionals for item genera-
tion, and 115 patients with adenocarcinoma were used for
pretesting the developed questionnaire. The mean age of
the study populations in the nine studies listed in Table 3
ranged between 58 (MDADI) to 72 years (EDGQ). The
only exception was the DHI which had a mean age of
41 years for the patient group and 45 years for the control
group. A cross-sectional study design was used for the
development of all questionnaires.
The same target populations were used for development
and validation of the DHI, EORTC QLQ-OG25, and
MDADI, while there was no validation study for the EDGQ
(see Table 4). Four questionnaires were validated in separate
studies: the DHI0 [36] and SWAL-QOL [33] were validated
using a cross-sectional design, and the EORTC QLQ-STO22
[39] and EORTC QLQ-H&N35 [42] were validated by
prospective intervention studies. The populations used for
the validation studies were from multiple hospitals across
Europe and the US, except for the DHI0, which included data
from one hospital only. The patient populations of these val-
idation studies ranged from 214 for DHI0 to 500 for EORTC
QLQ-H&N35. For the validation of the SWAL-QOL
(n = 40) and the DHI0 (n = 74), a control group of healthy
volunteers from the general community was added instead of
a second palliative patient group, which was the case for the
EORTC QLQ-22 (n = 111). The DHI0 was administered to a
subset of patients with dysphagia on two occasions in a
follow-up study design (n = 63).
The mean ages of the patients in the development and
validation studies were quite comparable, the only excep-
tion being those for EORTC QLQ-STO22: mean age
60 years (range 22–80) in the development study and 65.1
(range 37–87) in the validation study because different
populations were used [38, 39]. For the validation studies,
the mean age of the patient groups ranged from 60 years
(range 20–92) for the females of the DHI0 to 67 years
(range 30–92) for the second patient group of the EORTC
QLQ-STO22.
Measurement Characteristics of the Questionnaires
The questionnaires were divided in two categories. The
first category contained four questionnaires that are aimed
solely at HRQoL of patients with oropharyngeal dysphagia:
DHI, DHI0, MDADI, and SWAL-QOL. These question-
naires are concerned primarily with HRQoL experienced
by the patient. The second group of questionnaires: the
EDGQ, EORTC QLQ-STO22, EORTC QLQ-OG25, and
EORTC QLQ-H&N35, combine FHS and HRQoL for
other primary diseases such as gastric (QLQ-STO22) or
head and neck cancer (QLQ-H&N35) and have a limited
number of dysphagia-related items or subscales. The
EDGQ was developed as part of an interview that assesses
the social and psychological burden of dysphagia, while the
EORTC QLQ-OG25 combines the EORTC QLQ-OES18
for esophageal [27] and the QLQ-STO22 for gastric cancer
[40], plus seven modified items.
Questionnaires Aimed at Oropharyngeal Dysphagia
Table 5 gives the measurement characteristics of the oropha-
ryngeal dysphagia-related HRQoL questionnaires. All ques-
tionnaires contain three domains, except for the SWAL-QOL
[33] which has ten domains related to oropharyngeal dyspha-
gia. These domains of the SWAL-QOL contain 44 items, plus
three anamnesis questions about food and liquid intake and a
Table 2 Overview of HRQoL questionnaires and reasons for inclu-
sion or exclusion in this study
Questionnaires Inclusion Exclusion
DHI [35] a
DHI0 [36] a
EDGQ [12] a
MDADI [34] a
SWAL-QOL [31–33] a
EORTC QLQ-STO22 [38, 39] b
EORTC QLQ-OG25 [40] b
EORTC QLQ-H&N35 [41, 42] b
EORTC QLQ-OES18 [27] c
HNQOL [26] c
UW-QOL [25] c
FACT-HN [28] d
Self-report symptom inventory [29] d
Klugman QoL questionnaire [30] e
a Mainly oropharyngeal dysphagia-related HRQoLb Combination of oropharyngeal dysphagia-related HRQoL and FHS
related to gastric, esophageal, or head and neck cancerc No oropharyngeal dysphagia-related HRQoL but FHS related to
head and neck cancer, esophageal cancerd Too few items on oropharyngeal dysphagia-related HRQoLe Interview with open-ended questions
A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia 187
123
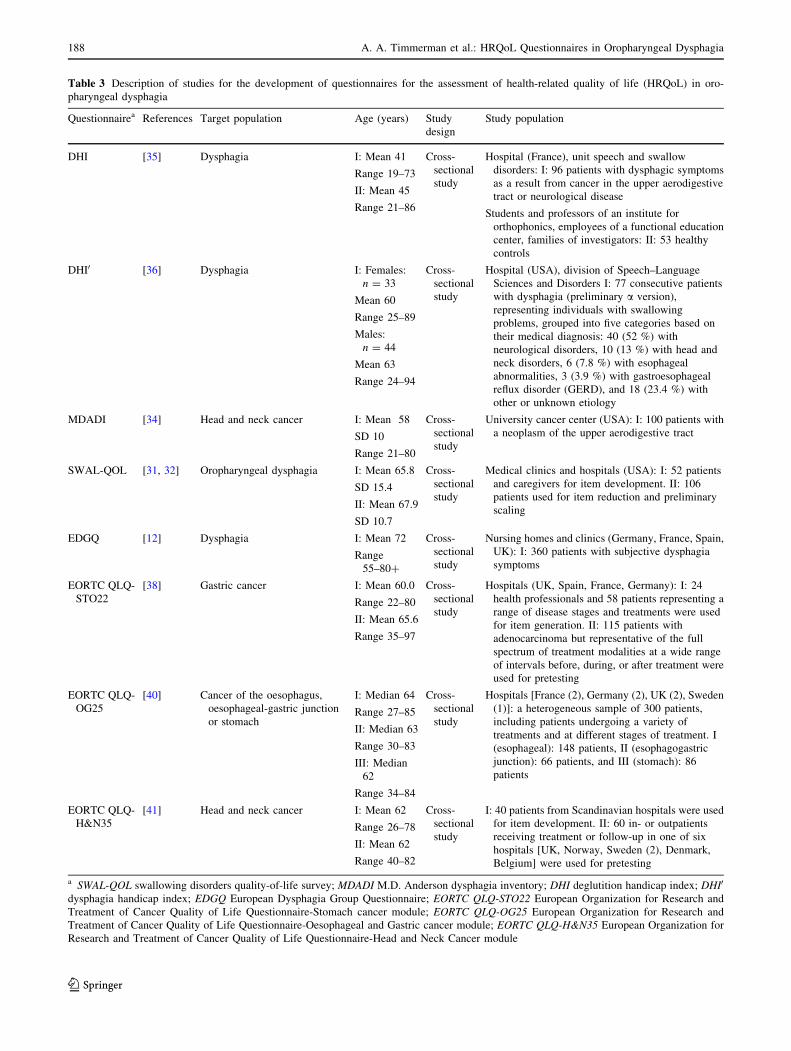
Table 3 Description of studies for the development of questionnaires for the assessment of health-related quality of life (HRQoL) in oro-
pharyngeal dysphagia
Questionnairea References Target population Age (years) Study
design
Study population
DHI [35] Dysphagia I: Mean 41
Range 19–73
II: Mean 45
Range 21–86
Cross-
sectional
study
Hospital (France), unit speech and swallow
disorders: I: 96 patients with dysphagic symptoms
as a result from cancer in the upper aerodigestive
tract or neurological disease
Students and professors of an institute for
orthophonics, employees of a functional education
center, families of investigators: II: 53 healthy
controls
DHI0 [36] Dysphagia I: Females:
n = 33
Mean 60
Range 25–89
Males:
n = 44
Mean 63
Range 24–94
Cross-
sectional
study
Hospital (USA), division of Speech–Language
Sciences and Disorders I: 77 consecutive patients
with dysphagia (preliminary a version),
representing individuals with swallowing
problems, grouped into five categories based on
their medical diagnosis: 40 (52 %) with
neurological disorders, 10 (13 %) with head and
neck disorders, 6 (7.8 %) with esophageal
abnormalities, 3 (3.9 %) with gastroesophageal
reflux disorder (GERD), and 18 (23.4 %) with
other or unknown etiology
MDADI [34] Head and neck cancer I: Mean 58
SD 10
Range 21–80
Cross-
sectional
study
University cancer center (USA): I: 100 patients with
a neoplasm of the upper aerodigestive tract
SWAL-QOL [31, 32] Oropharyngeal dysphagia I: Mean 65.8
SD 15.4
II: Mean 67.9
SD 10.7
Cross-
sectional
study
Medical clinics and hospitals (USA): I: 52 patients
and caregivers for item development. II: 106
patients used for item reduction and preliminary
scaling
EDGQ [12] Dysphagia I: Mean 72
Range
55–80?
Cross-
sectional
study
Nursing homes and clinics (Germany, France, Spain,
UK): I: 360 patients with subjective dysphagia
symptoms
EORTC QLQ-
STO22
[38] Gastric cancer I: Mean 60.0
Range 22–80
II: Mean 65.6
Range 35–97
Cross-
sectional
study
Hospitals (UK, Spain, France, Germany): I: 24
health professionals and 58 patients representing a
range of disease stages and treatments were used
for item generation. II: 115 patients with
adenocarcinoma but representative of the full
spectrum of treatment modalities at a wide range
of intervals before, during, or after treatment were
used for pretesting
EORTC QLQ-
OG25
[40] Cancer of the oesophagus,
oesophageal-gastric junction
or stomach
I: Median 64
Range 27–85
II: Median 63
Range 30–83
III: Median
62
Range 34–84
Cross-
sectional
study
Hospitals [France (2), Germany (2), UK (2), Sweden
(1)]: a heterogeneous sample of 300 patients,
including patients undergoing a variety of
treatments and at different stages of treatment. I
(esophageal): 148 patients, II (esophagogastric
junction): 66 patients, and III (stomach): 86
patients
EORTC QLQ-
H&N35
[41] Head and neck cancer I: Mean 62
Range 26–78
II: Mean 62
Range 40–82
Cross-
sectional
study
I: 40 patients from Scandinavian hospitals were used
for item development. II: 60 in- or outpatients
receiving treatment or follow-up in one of six
hospitals [UK, Norway, Sweden (2), Denmark,
Belgium] were used for pretesting
a SWAL-QOL swallowing disorders quality-of-life survey; MDADI M.D. Anderson dysphagia inventory; DHI deglutition handicap index; DHI0
dysphagia handicap index; EDGQ European Dysphagia Group Questionnaire; EORTC QLQ-STO22 European Organization for Research and
Treatment of Cancer Quality of Life Questionnaire-Stomach cancer module; EORTC QLQ-OG25 European Organization for Research and
Treatment of Cancer Quality of Life Questionnaire-Oesophageal and Gastric cancer module; EORTC QLQ-H&N35 European Organization for
Research and Treatment of Cancer Quality of Life Questionnaire-Head and Neck Cancer module
188 A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia
123

question about global health. The MDADI [34] consists of 20
items subdivided in emotional, functional, and physical health,
while there is one global item about limitations to daily activ-
ities due to swallowing ability. The DHI [35] consists of the
physical, functional, and emotional domains comprising 30
items, while the DHI0 [36] contains emotional, functional, and
physical scales comprising 25 items plus one severity item.
Most items of the SWAL-QOL involve the impact of
oropharyngeal dysphagia, except for five items related to
fatigue and sleep. For the MDADI, DHI, and DHI0, all
items are oropharyngeal dysphagia-specific. According to
the definition of HRQoL and FHS given in the Introduc-
tion, more than 50 % of the items of these four question-
naires are about symptoms and functional abilities (FHS)
resulting from dysphagia: 25 items for the SWAL-QOL, 12
for the MDADI, 18 for the DHI, and 17 for the DHI0.Response options for the DHI, MDADI, and SWAL-QOL
range from 1 to 5 on a 5-point Likert scale, i.e., from strongly
agree to strongly disagree. The DHI0 has three response
options: never, sometimes, and always. The total score for the
SWAL-QOL can range from 0 (least favorable state) to 100
(most favorable state) while that for the MDADI can range
from 20 (extremely low functioning) to 100 (high function-
ing). For the DHI and the DHI0, the lowest score is 0 (least
disabled) and the highest possible scores are 100 and 120
(most disabled), respectively. For two items of the MDADI, ‘‘I
do not feel self-conscious when I eat’’ (emotional subscale)
and ‘‘I feel free to go out to eat with my friends, neighbours and
relatives’’ (functional subscale), the scoring is reversed so that
higher scores reflect better functioning.
Questionnaires for Primary Diseases that often Result
in Oropharyngeal Dysphagia
Measurement characteristics of questionnaires aimed at
diseases that often result in oropharyngeal dysphagia are
given in Table 6. There is one interview (EDGQ [12]) and
three questionnaires (QLQ-STO22 [39], QLQ-OG25 [40],
QLQ-H&N35 [41, 42]). The EDGQ is aimed at the impact
of dysphagia on social and psychological well being. The
interview consists of 28 items covering five domains. One
of these domains, ‘‘personal feelings and importance’’,
contains four items and four contingency questions (to be
answered only if the patient answered ‘‘yes’’ to a foregoing
question) related to oropharyngeal dysphagia and HRQoL,
e.g., ‘‘Would you say that eating is an enjoyable part of
your day?’’ Response options are ‘‘yes’’, ‘‘no’’, and ‘‘do not
know’’ and no scoring range is available. The QLQ-
STO22, QLQ-OG25, and QLQ-H&N35 are all question-
naire modules to be used as supplements to the EORTC
QLQ-C30 questionnaire [37]. These questionnaires all
contain multiple-item scales and some single items in
differing numbers. The QLQ-STO22, QLQ-OG25, and
QLQ-H&N35 use the same 4-point scale response for-
mat—not at all, a little, quite a bit, and very much—for
most items, and the QLQ-H&N35 also has a yes/no
response format for the last five questions. Scores range
from 0 to 100 for the QLQ-OG25 and QLQ-H&N35 and
from 0 to 84 for the QLQ-STO22. The questionnaires
contain dysphagia-related HRQoL items that address the
impact of dysphagia on HRQoL; they are concerned with
the impact of the eating and/or swallowing problem on the
patient’s self-esteem and social life, which may result in
feelings of anxiety and/or shame. The QLQ-STO22 has
three such items, e.g., ‘‘Have you had discomfort when
eating?’’ The EORTC QLQ-OG25 has the same three
dysphagia-related HRQoL items and one additional item:
‘‘Have you had difficulty eating?’’ Only the QLQ-H&N35
summarizes the HRQoL items related to dysphagia in the
social eating domain, which contains four items: ‘‘Have
you had trouble eating?’’, ‘‘Have you had trouble eating in
front of your family?’’, ‘‘Have you had trouble eating in
front of other people?’’, and ‘‘Have you had trouble
enjoying your meals?’’.
Psychometric Qualities of Questionnaires Aimed
at Oropharyngeal Dysphagia
The psychometric properties of the questionnaires aimed
solely at the impact of oropharyngeal dysphagia were
judged using quality criteria that are used for health status
questionnaires [23, 24]. The EDGQ, QLQ-STO22, QLQ-
OG25, and QLQ-H&N35 did not contain the necessary
number of items related to oropharyngeal dysphagia for an
appropriate psychometric judgment of the impact of oro-
pharyngeal dysphagia. Ratings for the DHI [35], DHI0 [36],
MDADI [34], and SWAL-QOL [33] are given in Table 7.
The development and validation studies of the question-
naires aimed at oropharyngeal dysphagia used a cross-
sectional design, which implies that no clinically important
changes over time (responsiveness) could be assessed. The
psychometric qualities of each questionnaire are discussed
in the following subsections.
Deglutition Handicap Index (DHI)
For the DHI, clear descriptions of the goal of the mea-
surement and the measured concepts of the questionnaire
were provided. Information about the target population was
presented; however, the development and item selection
were not described, so it is not clear whether the target
population was involved in item selection, resulting in an
indeterminate rating for content validity. Internal consis-
tency also received an indeterminate rating because both
quality criteria were not fulfilled, the sample sizes for
healthy subjects (n = 53) and patients (n = 96) were
A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia 189
123

insufficient since the questionnaire contained 30 items,
which necessitated at least 210 subjects (7 9 30 items).
Cronbach’s a coefficients were [0.70 for the patient
sample, except for the physical domain (a = 0.60). The
combined patient and healthy samples had an a value of
0.81 for the physical domain, which is elevated by the
Table 4 Description of measurement characteristics of validation studies related to questionnaires for the assessment of health-related quality of
life (HRQoL) in dysphagia
Questionnaire Refs Target
population
Age (years) Study design Study population
DHI [35] Study for both development and validation: measurement characteristics in Table 3
DHI0 [36] Dysphagia I: experimental
group
A. Females:
n = 110
Mean 60, SD 16,
Range 20–92
B. Males:
n = 104
Mean 66, SD 13,
Range 19–96
II: controls
A. Females:
n = 40
Mean 60, SD 13,
Range 30–86
B. Males: n = 34
Mean 54, SD 14,
Range 30–80
I–II: cross-sectional
study
Hospital (USA), division of Speech–Language
Sciences and Disorders: I: 214 consecutive
patients with dysphagia (final b version) grouped
into six categories based on their medical
diagnosis: 72 (33.6 %) with neurological
impairment, 76 (35.5 %) with head and neck
disorders, 6 (2.8 %) with esophageal
abnormalities, 23 (10.7 %) with gastroesophageal
reflux disorder (GERD), 9 (4.2 %) with respiratory
disorders, and 28 (13.1 %) with other etiologies
such as diabetes, post-bariatric surgery, globus
sensation, or unknown causes
Individuals selected from within the community,
without dysphagia, history of head and neck
cancer, or surgery (with the exception of
tonsillectomy), history of neurological problems,
or feeding tube placement. II: 74 controls
III: Retest group
(n = 63)
A. Females:
n = 40
Mean 60
B. Males: n = 23
Mean: n = 66
III: Follow-up study
Time between
administrations of
the DHI was
7–116 days
(Mean = 36,
SD = 32,
Median = 21)
In a subgroup (of the experimental group) the DHI
was administered two times to individuals with
dysphagia who were not undergoing any
intervention for swallowing. Within this subgroup,
26 (41.3 %) had a diagnosis of neurological
disorder, 22 (35 %) with head and neck disorder, 1
(1.6 %) with esophageal abnormality, 7 (11.1 %)
with gastroesophageal reflux disorder (GERD), 7
(11.1 %) with other diagnoses. III: 63 patients
MDADI [34] Study for both development and validation: measurement characteristics in Table 3
SWAL-QOL [33] Oropharyngeal
dysphagia
I: Mean 66
SD 13
II: Mean 73
Cross-sectional study Medical outpatient speech, swallowing, neurology
clinics, ENT and other surgery clinics, VA
hospitals, (university) medical centers (USA): I:
386 patients with mechanical or neurological
oropharyngeal dysphagia
General community, hospital volunteer department,
and elder-hostel education program (USA): II: 40
healthy controls
EDGQ [12] No validation study present
EORTC
QLQ-
STO22
[39] Gastric cancer I: Mean 65
Range 37–87
II: Mean 67
Range 30–92
Prospective
intervention study
14 institutions in 8 different countries: 219 gastric
cancer patients. I: 108 (potentially curative)
patients, II: 111 (palliative treatment) patients
EORTC
QLQ-OG25
[40] Study for both development and validation: measurement characteristics in Table 3
EORTC
QLQ-
H&N35
[42] Head and neck
cancer
I: Mean 61
Range 18–88
Median 64
Prospective
intervention study
6 hospitals: I: 500 patients; 111 patients (Norway)
and 248 patients (Sweden) with head and neck
cancer, 141 patients (The Netherlands) with
squamous cell carcinoma
190 A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia
123

findings for the healthy sample (a = 0.74). For the
assessment of floor and ceiling effects, which indicate that
in the respective domains more than 15 % of respondents
achieved the highest or the lowest possible scores, scoring
patterns on individual items were used. For the DHI, this
indicates that for the healthy sample, the floor effects were
present for the ten items in the physical domain, the only
domain sampled in both groups. The number of subjects
with lowest possible score of ‘‘0’’ (never) ranged from 35
(66 %) to 49 (92 %) subjects, while the highest score was
‘‘2’’ (sometimes) on all items. For the patient sample, both
floor and ceiling effects were present. The pattern of floor
effects was convincing because it was present on all items
of the three domains, ranging from 19 (20 %) to 75 (78 %)
subjects with a score of ‘‘0.’’ Ceiling effects were less
extreme and differed between domains. For the physical
domain, the ceiling effects were present on four items;
between 18 (19 %) and 33 (34 %) of the subjects scored
‘‘4’’ (always), the highest possible score. The emotional
domain contained ceiling effects on three items, and a
range of 17 (18 %)–20 (21 %) subjects had a maximum
score. Ceiling effects were the strongest in the functional
domain, with 15 (16 %)–44 (48 %) scoring ‘‘4’’ (always)
on four items. DHI has not been related to another measure
resulting in an indeterminate rating for construct validity.
Only correlations between the domains and total DHI were
described, ranging from 0.59 between the functional and
physical domains to 0.67 between the functional and
emotional domains. Values were [0.80 between all
domains and total DHI scores, as should be expected for a
questionnaire. Criterion validity was calculated by corre-
lating the scores of the domains with different measures.
For the physical domain, scores were compared to the
physical pathological mechanisms assessed by videofluo-
roscopic examination, with no significant results (r = 0.17,
0.25, 0.29). The functional domain correlated with the
nutritional status and significant values were found for
meal duration (r = 0.32, p = 0.035), but the correlation
was reversed for the degree of severity (r = –0.51,
p = 0.018) with the functional and physical domains
(r = –0.38, p = 0.028), indicating that severity was less in
the case of higher scores on the functional and physical
domains. Correlation between the emotional domain and
the COOP/WONCA cards, which evaluate QoL in patients
with chronic diseases, was small (r = 0.40, not signifi-
cant), which may be due to the use of this generic measure
for HRQoL in chronic conditions [43, 44]. There was no
information that could be used to assess the reproducibility,
reliability, and interpretability of the DHI.
Dysphagia Handicap Index (DHI0)
The DHI0 received an indeterminate rating on content
validity, although clear descriptions were provided of the
measurement aim, target population, measured concepts,
and item reduction. It is not clear whether the target pop-
ulation was involved in final item selection or that their
scores were used only on the preliminary version to
Table 5 Measurement characteristics of dysphagia-specific questionnaires for the assessment of HRQoL
Questionnaire Domains (No. of items) Scales Item
no.
Response options Range
of
scores
DHI [35] Physical (10), functional (10), emotional (10) 3 30 Never, almost never, sometimes,
almost always, always
0–120
DHI0 [36] Physical (9), functional (9), emotional (7) 3 ? 1
severity
item
25 Never, sometimes, always 0–100
MDADI [34] Emotional (6), functional (5), physical (8)a 3 ? 1
global
item
20 Strongly agree, agree, no opinion,
disagree, strongly disagree
20–100
SWAL-QOL
[31–33]
Burden (2), eating duration (2), eating desire (3), food
selection (2), communication (2), fear (4), mental health
(5), social functioning (5), fatigue (3), sleep (2)
10 44 Strongly agree, agree, uncertain,
disagree, strongly disagree
Very much true, quite a bit true,
somewhat true, a little true, not at all
true
Almost always, often, sometimes,
hardly ever, never
All of the time, most of the time,
some of the time, a little of the time,
none of the time
0–100
a Reversed scoring for two items of the MDADI: ‘‘I do not feel self-conscious when I eat’’ (emotional subscale) and ‘‘I feel free to go out to eat
with my friends, neighbors and relatives’’ (functional subscale)
A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia 191
123

Table 6 Measurement characteristics of questionnaires for the assessment of health related quality of life (HRQoL) in primary diseases often
resulting in oropharyngeal dysphagia
Questionnaire Domains (no. of items) Scales Item
no.
Dysphagia-related HRQoL
items
Response options Range of
scores
EDGQ [12] 1. Background data (3)
2. Eating habits (4 ? 1a)
3. Personal feelings and
importance (4 ? 4a)
4. Seeking help (5 ? 3a)
5. Medical status (3 ? 1a)
5 multiple-item scales 28 Domain: ‘‘personal feelings
and importance’’
Yes, no, don’t know NA
QLQ-STO22
[38, 39]
1. Dysphagia (4)
2. Pain (3)
3. Reflux (3)
4. Eating (5)
5. Anxiety (3)
6. Single items (3) ? 1a
5 multiple-item scales,
3 single items
22 1. Discomfort when eating
2. Trouble enjoying meals
3. Trouble eating in front of
other people
Not at all, a little, quite a
bit, very much
0–84
QLQ-OG25
[40]
1. Dysphagia (3)
2. Eating restrictions (4)
3. Reflux (2)
4. Odynophagia (2)
5. Pain and discomfort (2)
6. Anxiety (2)
7. Single items (10)
6 multiple-item scales,
10 single items
25 1. Trouble enjoying meals
2. Difficulty eating
3. Discomfort when eating
4. Trouble with eating in
front of other people
Not at all, a little, quite a
bit, very much
Answer Q25 only if hair
loss present
0–100
QLQ-H&N35
[41, 42]
1. Pain (4)
2. Swallowing (4)
3. Senses (2)
4. Speech (3)
5. Social eating (4)
6. Social contact (5)
7. Sexuality (2)
8. Single items (11)
7 multiple-item scales,
11 single items
35 Domain ‘social eating’:
1. Trouble eating
2. Trouble eating in front of
family
3. Trouble eating in front of
other people
4. Trouble enjoying your
meals
Not at all, a little, quite a
bit, very much
Q31–35: no/yes
0–100
a Contingency question: Only to be answered if the foregoing question has been answered ‘‘yes’’
Table 7 Summary rating of psychometric qualities for questionnaires evaluating health-related quality of life (HRQoL) in oropharyngeal
dysphagia
Questionnaire
rating a,bContent
validity
Criterion
validity
Construct
validity
Internal
consistency
Reproducibility Responsiveness Floor or ceiling
effect
Interpretability
a. Agreement
b. Reliability
DHI [35] ? - - ? a. 0
b. 0
NA ? 0
DHI0 [36] - ? ? ? a. ?
b. ?
NA ? ?
MDADI [34] ? - ? ? a. ?
b. 0
NA - ?
SWAL-QOL
[33]
? ? ? ? a. ?
b. ?
NA ? ?
a ? positive rating, ? indeterminate rating, - negative rating, 0 no information available, NA not applicableb Indeterminate rating (?) means doubtful design or method (i.e., lacking a clear description or important methodological weakness) or only
fulfilling part of the requested psychometric quality
192 A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia
123

construct the final questionnaire version. Agreement was
assessed by test–retest correlations (Pearson’s correlation
coefficient) and all values were between 0.75 and 0.86 as
requested, but the period between tests, which ranged from
7 to 116 days (mean 36, SD 32.2), was less than 2 weeks
for part of the sample, resulting in an indeterminate rating.
No ceiling effects (\2.3 %) were present for the DHI0, but
the functional (24.8 %) and emotional (32.7 %) domains
showed floor effects, indicating that more than 15 % of
respondents received the lowest possible scores. Strong
psychometric qualities were found for internal consistency
and reliability. For internal consistency, sample size was
larger than 100 (n = 7 9 25 items = 175 items) and all
Cronbach’s a values were between 0.78 (physical) and 0.94
(total DHI0 score). Reliability received a positive rating
because the ICC values ranged between 0.75 (emotional)
and 0.86 (functional) for all domains and the total DHI0
score. Regarding validity aspects, it can be stated that
criterion validity was assessed by a measure of clinical
severity, a videofluorographic swallowing study (VFS). A
subgroup of 60 patients was assessed and subdivided in
three subgroups of normal (n = 19), mild (n = 29), and
moderate/severe (n = 12) based on the scores of the VFS.
The overall difference between these clinical severity
groups was significant for the mean total DHI0 (p = 0.003)
and the functional (p = 0.001), emotional (p = 0.009), and
physical (p = 0.049) subscales, as calculated with
ANOVA methods, resulting in a positive rating. Construct
validity received a positive rating and was measured in two
ways (n [ 50). First, Pearson correlations between several
subscales were calculated, with the highest correlation
between the emotional and functional subscales (r = 0.77)
and lowest between the physical and emotional subscales
(r = 0.66), while the correlation between the physical and
functional subscales was intermediate (r = 0.72). These
results imply that the functional limitations have more of
an impact on emotional functioning than the physical
limitations, which should be expected because of the
impact on social functioning, one of the greatest handicaps
caused by oropharyngeal dysphagia [17, 18]. Second,
Wilcoxon two-sample tests were used to assess the dif-
ference in DHI0 scores between the dysphagia and control
groups. The control group had significantly lower scores
for total DHI0 and subscales than the dysphagia group
(p \ 0.001). In the control group, almost all participants
responded ‘‘never’’ on the subscales, which is the expected
difference between patients and a population from the
general community. Interpretability received a positive
rating due to the presence of clinically meaningful scores
for four clinical severity subgroups (normal, mild, moder-
ate, and severe), as discussed under criterion validity. The
self-reported severity rating of the DHI0 was also grouped
into the following categories for the 214 dysphagia
patients: 1 = normal, 2 and 3 = mild, 4 and 5 = moder-
ate, and 6 and 7 = severe. The differences for these
severity groups were significant for total and all subscales
(p = 0.001), and post hoc analyses showed that all pairwise
comparisons were significant as well (p = 0.05).
M.D. Anderson Dysphagia Inventory (MDADI)
Measurement aim, target population and measured concepts
were all described for the MDADI, while the target popu-
lation was involved in item selection [34]. Information about
the process of item selection and reduction was absent,
resulting in an indeterminate rating for content validity.
Using a sample of 100 patients, Spearman correlation coef-
ficients were calculated between the domains of the MDADI
and the SF-36, which is a short-form general health survey of
the Medical Outcomes Study (MOS), as a measure of con-
struct validity [45, 46]. The results were in accordance with
expected hypotheses: Since the MDADI is intended to
measure the psychosocial aspects of dysphagia, the signifi-
cant correlations of the SF-36 mental components (i.e., social
functioning, role-emotional, and mental health) scores were
as expected with the domains global (0.44), emotional
(0.54), functional (0.51), and physical (0.54). There is no
information about the reproducibility aspect of the property
reliability present, resulting in a ‘‘0’’ rating, while the
property agreement received a positive rating. Correlations
within a 2-week period were 0.85 for both emotional and
physical domains, 0.89 for the functional domain, and 0.93
for the global domain. Both internal consistency and inter-
pretability received indeterminate ratings. Factor analyses
were performed on 100 patients, which is \7 times the
number of items, which is 20. Although the overall Cron-
bach’s a coefficient was 0.96, two values were\0.70: for the
functional domain it was 0.58 and for the emotional domain
it was 0.69. Interpretability was determined in only three
subgroups (site and pathological features of the head and
neck tumor and time elapsed since the last treatment), and
some of the subsamples were smaller than 50. An indeter-
minate rating was also given for floor and ceiling effects
because it was not clear from the table and text in the article
whether the numbers were questionnaire scores or patients
(n), which made judging this psychometric quality impos-
sible. Criterion validity received a negative rating because
there was no psychometric information for the Performance
Status Scale (PSS), a clinician-rated instrument that is used
as the gold standard. All correlations were\0.70, from 0.47
for the PSS eating in public domain and the MDADI global
domain to 0.61 for the PSS normalcy of diet and the MDADI
functional domain.
A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia 193
123

SWAL-QOL
Content validity and interpretability were the strongest
qualities for the SWAL-QOL: all criteria regarding mea-
surement aim, target population, measured concepts, and the
processes of item selection and reduction were described,
while the target population was involved in item selection
[33]. Relevant subgroups were selected for interpretability:
(1) dysphagic patients—normal swallowers, (2) dysphagic
patients with oral nutrition—tube feeding, (3) dysphagic
patients differing with respect to what food texture and liquid
consistency can be handled, and (4) relationship between
symptom severity and QoL. Differences between groups
were significant for almost all scores with the SWAL-QOL
(p \ 0.0001), except for domains related to liquid consis-
tency (p \ 0.10) and four domains related to tube feeding
status (p [ 0.060). For the SWAL-QOL domains, the rela-
tionship with symptom severity, considered a gold standard
for criterion validity, is highly significant (p = 0.0001). The
SF-36 was used to calculate convergent validity with the
SWAL-QOL domains, considered to be an indicator of
construct validity [45, 46]. The correlations between SWAL-
QOL domains and the SF-36 measures health perceptions,
social function, loneliness, and mental health are all signif-
icant at p \ 0.05 and range between 0.11 for the relationship
between SF-36 health perceptions and SWAL-QOL burden
and eating duration and 0.56 for the relationship between SF-
36 loneliness and SWAL-QOL social functioning. Internal
consistency was assessed with an adequate sample size
(n [ 100), and Pearson’s correlation coefficients were
mainly [0.70, indicating construct homogeneity. Repro-
ducibility, containing the properties agreement and reli-
ability, received an indeterminate rating. Agreement was
assessed by Pearson correlation coefficient within a 2-week
time frame, with values ranging from 0.60 to 0.91 for all
SWAL-QOL domains with burden (0.60) and eating dura-
tion (0.64) having values\ .70. Intraclass correlation (ICC),
a measure of reliability, ranged from 0.59 to 0.91, with the
values for burden (0.59) and eating duration (0.64) below
0.70. Ceiling effects were present for five of the ten domains
of the SWAL-QOL (food selection, social functioning, eat-
ing desire, communication, and sleep) and floor effects were
present for two domains (burden and eating duration).
Discussion
Evaluation of the Psychometric Qualities
of Questionnaires Evaluating HRQoL in Dysphagia
The psychometric qualities of questionnaires aimed solely
at HRQoL in oropharyngeal dysphagia were assessed. This
choice was informed by strong associations between
indicators of a condition, such as dysphagia, and evaluation
measures that are conceptually proximal to the disease (i.e.
disease-specific questionnaires) [4, 47].
The DHI0 and SWAL-QOL received the strongest psy-
chometric ratings, at least on all validity aspects and the
interpretability of the questionnaire. This implies that the
SWAL-QOL measures homogeneously what it is supposed to
measure in an appropriate target population of patients with
dysphagia. The SWAL-QOL differentiates on relevant clini-
cal characteristics such as normal swallowing, manner of food
intake, food texture, liquid consistency, and symptom sever-
ity. Shortcomings were found in reproducibility (stability over
time, distinguishing between patients) and floor and ceiling
effects for the score ranges. For several items of the SWAL-
QOL, patients’ scores may have indicated that they were
functioning better (underscoring) or worse than they experi-
enced (overscoring); this was a weakness of the other ques-
tionnaires as well. The DHI0 received positive ratings on
almost all validity aspects and the ability to distinguish
between patients at one point. Clinically meaningful sub-
groups were used to evaluate clinical severity through both
self-assessment and a measure of clinical severity, which is
closely related to the health condition (interpretability). Only
the face validity of the DHI0 was doubtful because it was not
clear if the target population was involved in item selection.
Comparison of the DHI0 and SWAL-QOL with the MDADI
and especially the DHI was complicated by weak psycho-
metric qualities or lack of information on validity aspects (e.g.,
content, criterion), internal consistency, floor and ceiling
effects, and interpretability.
The cross-sectional design of all included studies makes
conclusions about the ability to assess changes over time
(responsiveness) difficult. Responsiveness is an indicator
that is difficult to assess through changes in perceptions of
disease, which complicates the assessment of intervention
effects [48]. Another weakness for all the questionnaires is
the lack of information or indeterminate ratings for repro-
ducibility, which also contains valuable information about
changes over time. From a psychometric perspective, one
can draw conclusions about the possibility to discriminate
between patients at only one point in time, which makes
the SWAL-QOL and DHI0 appropriate for screening pur-
poses or needs assessment. No final conclusions can be
drawn about within-subject variability over time, an
important measure for the evaluation of the intervention
effects of a HRQoL questionnaire.
Applicability of a Questionnaire for Dysphagia Impact:
Constructs, Domains, Comprehensiveness, Scoring
Formats, Internal Standards, and Utility
The intrinsic value of a HRQoL questionnaire is closely
linked to its application and is dependent on a match
194 A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia
123

between intended purposes, the information the instrument
provides, and ease of use. Therefore, measurement prop-
erties need to be considered as well in order to provide a
sound judgment based on the needs in a specific context
such as research, clinical practice, or quality assurance
[19]. For the development of the SWAL-QOL, HRQoL in
oropharyngeal dysphagia was defined as ‘‘an overall state
of well-being that is a composite of the ability to fulfill
physical, role and social activities, and psychological
effectiveness with which one performs these activities,
satisfaction with health care services related to dysphagia
treatment and symptom status’’ [31, 49]. This definition
seems to cover the range of content properties needed in a
HRQoL questionnaire applied to assess dysphagia impact,
although the boundaries of definition depend on why one is
assessing the particular concerns of patients [22]. A dis-
tinction has been made between FHS and HRQoL for the
items of all questionnaires included in this study. It can be
stated that these constructs are quite proximal and in need
of clear definitions and boundaries to enable appropriate
evaluation. Ware [4] describes a so-called specific–generic
continuum, with physical and mental symptoms resulting
in physical limitations (FHS) and psychological distress
(HRQoL), respectively, combined in a subjective overall
evaluation of health in general (see also Fig. 1) [4, 7, 9].
The continuum implies that both physical and mental
symptoms need to be evaluated in order to get a complete
picture of the impact of oropharyngeal dysphagia experi-
enced by the patient. In the psychometrically evaluated
questionnaires this was the case, while only in the SWAL-
QOL was there one global question about general health,
representing the generic end of the continuum. All ques-
tionnaires contained items related to functional, physical,
and emotional health with respect to dysphagia, ranging
from 6 to 10 items for each domain. Only the SWAL-QOL
clearly defines the content of scales, e.g., eating duration,
eating desire, and food selection, mostly represented by
2–5 items for each construct. Multidimensional HRQoL
questionnaires are accurate and responsive for specific
patient outcomes only, if subscales are selected in accor-
dance with individual patient needs [5]. Given a positive
rating for internal consistency, the SWAL-QOL is infor-
mative for the assessment of the full range of possible
dysphagia effects in clinical care. The DHI0, also a
homogeneous measure, is easier to score due to three
response options, with the same textual anchors for all
items, which is not true for the 5-point scoring format of
the SWAL-QOL.
For all applications, meaningful interpretation of scores
may be easier if there is some estimate of the relative
importance of each of the included (impact) domains in a
questionnaire [50]. The concept of severity has been
described as an important causal mediator in scoring the
impact of a condition on domains that impact HRQoL [6, 7,
9]. The DHI0 contains a response scale ranging from nor-
mal to severe problem (score = 1–7) in response to the
item ‘‘swallowing difficulty’’ at the end of the question-
naire. The SWAL-QOL and the MDADI question severity
in terms of impact on ‘‘dealing with a swallowing prob-
lem’’ (only SWAL-QOL) and ‘‘experienced limitations in
daily life’’, both scored on a reversed 5-point scale (i.e.,
low score means more limitations). A severity item at the
start of a questionnaire may influence the scoring of dys-
phagia impact domains; for validity it may be important to
clarify how judgments of HRQoL are made when consid-
ering severity of impact first. In the DHI0, correlations
between self-reported clinical severity, total and domain
scores, and a gold standard (VFS) were calculated in an
attempt to arrive at an overall judgment of dysphagia
impact based on a triangulation of clinical and individual
measures, which is especially relevant when using short
measures [51]. HRQoL questionnaires need to be able to
assess both between-subject (reproducibility) and within-
subject (responsiveness) differences for purposes of dis-
crimination and evaluation, respectively [19, 52]. In this
study reproducibility was assessed by both stability over
time within patients (agreement) and the extent to which
patients can be distinguished from each other despite
measurement errors (reliability). As only the MDADI
received a positive rating for agreement and the DHI0 for
reliability, it cannot be assumed that the questionnaires are
appropriate for the assessment of between-subject variation
because of their indeterminate ratings or lack of informa-
tion. If within-person variability in otherwise stable sub-
jects is large, the questionnaire may be unresponsive to real
changes over time, something that has not been assessed
(Table 7) [19, 52]. For these questionnaires to be useful for
discrimination or evaluation, these psychometric properties
need to be evaluated first in future studies.
Emergent Issues When Choosing a HRQoL
Questionnaire: Classification vs. Individualized Use,
Generic or Disease-specific Measures, and Response
Shift
Several quality criteria are important for the clinical
applicability of questionnaires: determining whether the
patient group was involved in defining relevant content
(face validity), determining whether an appropriate clinical
gold standard for experienced distress and disability was
used (criterion validity), and determining the differentia-
tion between relevant subgroups of patients enabling
comparison (interpretability) [53]. The SWAL-QOL has
the strongest ratings for all three criteria; the DHI0 is sec-
ond, supporting the application of the questionnaire with
individual patients. HRQoL is a highly dynamic construct
A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia 195
123

based on personal values and changes in response to illness
[9]. Oropharyngeal dysphagia affects broader aspects of a
patient’s life, such as self-esteem, social contacts, and daily
functioning, and information about these aspects may
influence treatment decisions and assessment of health-care
needs (e.g., quality of survival) [12, 17, 18, 54].
Improvement of symptoms and functional capacity are
usually the main goals of patients seeking care and an
inclination to avoid states that are aversive or bad, such as
pain or physical incapacitation [21, 55]. It has been
increasingly recognized that HRQoL questionnaires can be
used to supplement more objective clinical or biological
measures of disease [50, 56]. Disease-specific measures are
appropriate for assessing dysphagia impact because of the
possibility of detecting relatively small clinically mean-
ingful differences, which are easier to interpret compared
to results of more generic measures such as the Sickness
Impact Profile or the MOS-SF-36 [4, 20, 57]. All patients
included in the studies in this review suffered from oro-
pharyngeal dysphagia, which resulted from cancer in the
upper or lower aerodigestive tract or a neurological con-
dition (see Tables 3, 4). This is important for assessing the
clinically appropriate constructs that really do matter to
patients. However, HRQoL judgments may be influenced
by variables other than the domains included in question-
naires, such as personal coping styles or traits and experi-
enced social support [4, 19]. Ferrans [9] reviewed evidence
on the value of QoL instruments in symptom management
trials. It was found that overall QoL may improve in a
progression-free (i.e., not recovering) group with cancer,
while it declines for a disease progression group, so that
changes in overall QoL were as large or larger than
changes in symptoms of pain, fatigue, insomnia, and
dyspnea [9, 58]. Such outcomes highlight the so-called
‘‘disability paradox,’’ which implies that patients change
their internal standards, values, or concept of QoL during a
period with disease and therefore assess it differently.
Especially in patients with chronic and life-threatening
diseases, changes in HRQoL may result in part from
adaptation to their situation, with existential, spiritual, and
social issues becoming more important [56]. This phe-
nomenon of adaptation has been called response shift:
individuals assess their HRQoL by comparing their
expectations with their experience. Current measures do
not take account of expectations and cannot distinguish
between changes in experience with the disease and in
expectations of health. Most HRQoL measures evaluate the
impact of disease or treatment, not the adaptation of the
patient. Several issues need to be taken into consideration
when using HRQoL measures in clinical settings: (1)
Expectations of health may differ between patients; (2) the
magnitude of disease impact may differ depending on
when the assessment is made in the disease trajectory; and
(3) HRQoL is a dynamic construct that changes over time,
e.g., in response to disease [54]. The evaluation of HRQoL
is of prime importance in chronic or life-threatening dis-
eases due to the focus on reducing the impact of the dis-
ease, which may often be the case in oropharyngeal
dysphagia. The impact of disease may be minimized by
helping patients adjust expectations and adapt to their
changed health status and functioning. From this perspec-
tive, HRQoL may be reflecting the discrepancy between
expectations and experience in patients, which raises pos-
sibilities for health education and counselling. The contents
of HRQoL measures need to be sufficiently broad and use
direct weighting systems, resulting in individualized mea-
sures. All questionnaires for dysphagia impact included in
this study used a scoring system that offered an equal
numerical value to each item before summing the scores
into an overall judgment. This reflects an individual
weighting of domains, which ideally needs to be combined
with a short interview with the patient comparing indi-
vidual impact with more objective clinical measures [50].
It enables physician and patient to determine which scores
are clinically important, as clinical decisions cannot be
made based only on statistically significant differences
with clinical standards [48]. The meaning of differences in
scores varies according to the particular scale, setting
(therapy, disease), and perspective (patient, physician).
However, brevity, ease of administration, and clinically
useful data are essential prerequisites for a measure to be
accepted by physicians [5]. In order for a questionnaire to
be useful in clinical situations, it is important that the
specific purpose, setting of application, and intended pop-
ulation are clearly defined. This is the case for all the
questionnaires used in this study, and when balancing this
with the rated psychometric properties, it seems that the
DHI0 is the most suitable for clinical purposes, given the 25
items and the use of a uniform simple scoring format, in
spite of a negative rating for content validity.
It is necessary to combine psychometric and utility
approaches for all applications of questionnaires for oropha-
ryngeal dysphagia impact and to further strengthen the empir-
ical evidence for selection of measures in the future. This is
possible through head-to-head comparisons of measures within
the same studies as this information would greatly increase
precision and justify the use of a particular questionnaire. A
better understanding of the differences in what HRQoL ques-
tionnaires measure and a sounder base for the assessed effec-
tiveness of clinical interventions will be the result.
References
1. Fries JF. Aging, natural death, and the compression of morbidity.
N Engl J Med. 1980;303:130–5.
196 A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia
123
2. Katz S. The science of quality of life. J Chronic Dis. 1987;
40:459–63.
3. International Health Conference. Constitution of the World Health
Organization. 1946. Bull World Health Organ. 2002;80:983–4.
4. Ware JE. The status of health assessment. Annu Rev Public
Health. 1994;16:327–54.
5. Higginson IJ, Carr AJ. Using quality of life measures in the
clinical setting. BMJ. 2001;322:1297–300.
6. Wilson IB, Cleary PD. Linking clinical variables with health-
related quality of life: a conceptual model of patient outcomes.
JAMA. 1995;273:59–65.
7. Smith KW, Avis NE, Assmann SF. Distinguishing between
quality of life and health status in quality of life research: a meta-
analysis. Qual Life Res. 1999;8:447–59.
8. Ferrans C, Zerwic J, Wilbur J, Larson J. Conceptual model of
health-related quality of life. J Nurs Scholarsh. 2005;37:336–42.
9. Ferrans CE. Differences in what quality-of-life instruments
measure. J Natl Cancer Inst Monogr. 2007;37:22–6.
10. Cook IJ, Kahrillas PJ. Technical review on management of oro-
pharyngeal dysphagia. Gastroenterology. 1999;116:445–58.
11. Garcia-Peris P, Paron L, Velasco C, de la Cuerda C, Camblor M,
Breton I, Herencia H, Verdaguer J, Navarro C, Clave P. Long-
term prevalence of oropharyngeal dysphagia in head and neck
cancer patients: impact on quality of life. Clin Nutr. 2007;26:
710–7.
12. Ekberg O, Hamdy S, Woisard V, Wuttge-Hannig A, Ortega P.
Social and psychological burden of dysphagia: its impact on
diagnosis and treatment. Dysphagia. 2002;17:139–46.
13. Crary M, Groher ME, editors. Introduction to adult swallowing
disorders. Waltham: Elsevier; 2003.
14. Murry T, Carrau RL, editors. Clinical management of swallowing
disorders. San Diego: Plural; 2006.
15. Nguyen NP, Frank C, Moltz CC, et al. Impact of dysphagia on
quality of life after treatment of head and neck cancer. Int J
Radiat Oncol Biol Phys. 2005;61:772–8.
16. Campbell BH, Spinelli K, Marbella AM, et al. Aspiration, weight
loss and quality of life in head and neck cancer survivors. Arch
Otolaryngol Head Neck Surg. 2004;130:1100–3.
17. Gustafsson B, Tibbling L. Dysphagia, an unrecognized handicap.
Dysphagia. 1991;6:193–9.
18. McHorney CA, Martin-Harris B, Robbins J, Rosenbek J. Clinical
validity of the SWAL-QOL and SWAL-CARE outcome tools
with respect to bolus flow measures. Dysphagia. 2006;3:141–8.
19. Spertus JA. Evolving applications for patient-centered health
status measures. Circulation. 2008;118:2103–10.
20. Patrick DL, Deyo RA. Generic and disease-specific measures in
assessing health status and quality of life. Med Care. 1989;27:
S217–32.
21. Feinstein AR. Benefits and obstacles for development of health
status assessment measures in clinical settings. Med Care. 1992;
30:MS50–6.
22. Guyatt GH, Feeny DH, Patrick DL. Measuring health-related
quality of life. Ann Intern Med. 1993;118:622–9.
23. Terwee CB, Bot SD, de Boer MR, Windt DA, van der Knol DL,
Dekker J, Bouter LM, de Vet HC. Quality criteria were proposed
for measurement properties of health status questionnaires. J Clin
Epidemiol. 2007;60:34–42.
24. Timmerman AA, Meesters CM, Speyer R, Anteunis LJ. Psy-
chometric qualities of questionnaires for the assessment of otitis
media impact. Clin Otolaryngol. 2007;32:429–39.
25. Hassan SJ, Weymuller EA Jr. Assessment of quality of life in
head and neck cancer patients. Head Neck. 1993;15:485–96.
26. Terrell JE, Nanavati KA, Esclamado RM, Bishop JK, Bradford
CR, Wolf GT. Head and neck cancer-specific quality of life. Arch
Otolaryngol Head Neck Surg. 1997;123:1125–32.
27. Blazeby JM, Conroy T, Hammerlid E, Fayers P, Sezer O, Koller M,
Arraras J, Bottomley A, Vickery CW, Etienne PL, Alderson D.
Clinical and psychometric validation of an EORTC questionnaire
module, the EORTC QLQ-OES18, to assess quality of life in
patients with oesophageal cancer. Eur J Cancer. 2003;39:1384–94.
28. Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A,
Silberman M, Yellen SB, Winicour P, Brannon J, Eckberg K,
Lloyd S, Purl S, Blendowski C, Goodman M, Barnicle M, Stewart
I, McHale M, Bonomi P, Kaplan E, Taylor S IV, Thomas CR Jr,
Harris J. The functional assessment of cancer therapy scale:
development and validation of the general measure. J Clin Oncol.
1993;11:570–9.
29. Wallace KL, Middleton S, Cook IJ. Development and validation
of a self-report symptom inventory to assess the severity of oral-
pharyngeal dysphagia. Gastroenterology. 2000;118:678–87.
30. Klugman TM, Ross E. Perceptions of the impact of speech,
language, swallowing and hearing difficulties on quality of life of
a group of South African persons with multiple sclerosis. Fol
Phoniatr Logop. 2002;54:201–21.
31. McHorney CA, Bricker DE, Kramer AE, Rosenbek JC, Robbins J,
Chignell KA, Logemann JA, Clarke C. The SWAL-QOL outcomes
tool for oropharyngeal dysphagia in adults: I conceptual foundation
and item development. Dysphagia. 2000;15:115–21.
32. McHorney CA, Bricker DE, Robbins J, Kramer AE, Rosenbek
JC, Chignell KA. The SWAL-QOL outcomes tool for oropha-
ryngeal dysphagia in adults: II item reduction and preliminary
scaling. Dysphagia. 2000;15:122–33.
33. McHorney CA, Robbins J, Lomax K, Rosenbek JC, Chignell K,
Kramer AE, Bricker DE. The SWAL-QOL and SWAL-CARE
outcomes tool for oropharyngeal dysphagia in adults: III docu-
mentation of reliability and validity. Dysphagia. 2002;17:97–114.
34. Chen AY, Frankowski R, Bishop-Leone J, Hebert T, Leyk S, Le-
win J, Goepfert H. The development and validation of a dysphagia-
specific quality-of-life questionnaire for patients with head and
neck cancer. Arch Otolaryngol Head Neck Surg. 2001;127:870–6.
35. Woisard V, Andrieux MP, Puech M. Validation of a self-
assessment questionnaire for swallowing disorders (deglutition
handicap index). Rev Laryngol Otol Rhinol. 2006;127:315–25.
36. Silbergleit AK, Schultz L, Jacobson BH, Beardsley T, Johnson
AF. The dysphagia handicap index: development and validation.
Dysphagia. 2012;27:46–52.
37. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A,
Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes JC.
The European organization for research and treatment of cancer
QLQ-C30: a quality-of-life instrument for use in international
trials in oncology. J Natl Cancer Inst. 1993;85:365–76.
38. Vickery CW, Blazeby JM, Conroy T, Arraras J, Sezer O, Koller
M, Rosemeyer D, Johnson CD, Alderson D. Development of an
EORTC disease-specific quality of life module for use in patients
with gastric cancer. Eur J Cancer. 2001;37:966–71.
39. Blazeby JM, Conroy T, Bottomley A, Vickery C, Arraras J, Sezer
O, Moore J, Koller M, Turhal NS, Stuart R, van Cutsem E,
D’haese S, Coens C. European organisation for research and
treatment of cancer Gastrointestinal and quality of life groups.
Clinical and psychometric validation of a questionnaire module,
the EORTC QLQ-STO 22, to assess quality of life in patients
with gastric cancer. Eur J Cancer. 2004;40:2260–8.
40. Lagergren P, Fayers P, Conroy T, Stein HJ, Sezer O, Hardwick R,
Hammerlid E, Bottomley A, van Cutsem E, Blazeby JM. Clinical
and psychometric validation of a questionnaire module, the EO-
RTC QLQ-OG25, to assess health-related quality of life in
patients with cancer of the oesophagus, the oesophago-gastric
junction and the stomach. Eur J Cancer. 2007;43:2066–73.
41. Bjordal K, Ahlner-Elmqvist M, Tollesson E, Jensen AB, Razavi
D, Maher EJ, Kaasa S. Development of a European organisation
A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia 197
123

for research and treatment of cancer (EORTC) questionnaire
module to be used in quality of life assessments in head and neck
cancer patients. Acta Oncol. 1994;33:879–85.
42. Bjordal K, Hammerlid E, Ahlner-Elmqvist M, Graeff A, de
Boysen M, Evensen JF, Bjorklund A, de Leeuw RJ, Fayers PM,
Jannert M, Westin T, Kaasa S. Quality of life in head and neck
cancer patients: validation of the European organisation for
research and Treatment of cancer quality of life questionnaire-
H&N35. J Clin Oncol. 1999;17:1008–19.
43. Jamoulle M. Traduction Francaise des COOP/WONCA charts
(French adaptation of the COOP/WONCA charts). Brussels:
FMMCSF; 1992.
44. Jamoulle M, Roland M, Blanc HW. Mesure de l’etat fonctionnel
en medecine generale: les cartes COOP/WONCA (Functional
measure in general medicine: the COOP/WONCA charts). Rev
Med Brux. 1994;15:329–32.
45. Stewart AL, Hays RD, Ware JE. The MOS short-form general
health survey: reliability and validity in a patient population. Med
Care. 1988;26:724–35.
46. Ware JE, Sherbourne CD. The MOS 36-item short-form health
survey (SF-36): I. Conceptual framework and item selection. Med
Care. 1992;30:473–83.
47. Brenner MH, Curbow B, Legro M. The proximal distal contin-
uum in multiple health outcome measures: the case of cataract
surgery. Med Care. 1995;33:AS236–44.
48. Wright JG. Interpreting Health-Related Quality of Life Scores -
The simple rule of seven may not be so simple. Med Care.
2003;5:597–8.
49. Gotay CC, Korn EL, McCabe MS, Moore TD, Cheson BD.
Quality-of-life assessment in cancer treatment protocols: research
issues in protocol development. J Natl Cancer Inst. 1992;84:
575–9.
50. Carr AJ, Higginson IJ. Are quality of life measures patient cen-
tred? BMJ. 2001;322:1357–60.
51. Bech P. Quality of life measurement in the medical setting. Eur J
Psychiatry. 1995;10:83s–5s.
52. Guyatt GH, Kirshner B, Jaeschke R. Measuring health status:
what are the necessary measurement properties? J Clin Epidem-
iol. 1992;45:1341–5.
53. Thier SO. Forces motivating the use of health status assessment
measures in clinical settings and related clinical research. Med
Care. 1992;30:MS15–22.
54. Carr AJ, Gibson B, Robinson PG. Is quality of life determined by
expectations or experience? BMJ. 2001;322:1240–3.
55. Faden R, Leplege A. Assessing quality of life - Moral implica-
tions for clinical practice. Med Care. 1992;30:MS166–75.
56. Addington-Hall J, Kalra L. Who should measure quality of life?
BMJ. 2001;322:1417–20.
57. Hays RD, Woolley JM. The concept of clinically meaningful
difference in health-related quality-of-life research—how mean-
ingful is it? Pharmaeconomics. 2000;18:419–23.
58. Osaba D, Brada M, Yung W, Prados M. Health-related quality of
life in patients with anaplastic astrocytoma during treatment with
temozolomide. Eur J Cancer. 2000;36:1788–95.
Angelique A. Timmerman PhD
Renee Speyer PhD
Bas J. Heijnen MSc, SLP
Iris R. Klijn-Zwijnenberg MD
198 A. A. Timmerman et al.: HRQoL Questionnaires in Oropharyngeal Dysphagia
123
Copyright © 2022 FDOKUMEN