
Psychometric Practice Test - Combined / English - Spring 2019
Upload
independentCategory
view
0download
0
Scandinavian Journal of Psychology, 2008, 49, 533–548 DOI: 10.1111/j.1467-9450.2008.00669.x
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations. Published by Blackwell Publishing Ltd., 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA. ISSN 0036-5564.
Blackwell Publishing Ltd Personality and Social Sciences
Adolescent coping scales: A critical psychometric review
SIGRUN SVEINBJORNSDOTTIR1 and EINAR BALDVIN THORSTEINSSON2
1University of Akureyri, Iceland2University of New England, Australia
Sveinbjornsdottir, S. & Thorsteinsson, E. B. (2008). Adolescent coping scales: A critical psychometric review. Scandinavian Journal of Psychology,49, 533–548.
Individual coping is identified as an important factor in relation to health and well-being. Although several coping scales have been developed, keyterms of coping such as nature and a number of primary and secondary factors (dimensions) are obscure. Coping scales, such as those that have beendeveloped through exploratory factor analysis (EFA), have been criticized for poor psychometric properties, yet the critique so far does not evaluatedevelopment of the scales against best test-theoretical practice. The present study reviews six adolescent coping scales against ten detailed psychometriccriteria in relation to statistical choices throughout the process of scale development. All six scales measured poorly on several criteria. Best practicehad not been followed throughout their development and they suffered serious psychometric limitations. These findings indicate that there still isempirical research to be pursued in search of latent constructs and possible dimensions of coping through the implementation of EFA.
Key words: Adolescence, review, coping scale, validity, reliability, best test-theoretical practice.
Dr Einar B. Thorsteinsson, Psychology School of Behavioural, Cognitive and Social Sciences, University of New England, NSW 2351, Australia.Tel: + 61 2 6773 2587; fax: + 61 2 6773 3820; e-mail: [email protected]
Diverse psychosocial disorders (e.g., antisocial behavior, druguse, depression, eating disorders) in the Western world occurfrequently in adolescence (Rutter, 1995; Smith & Rutter, 1995).The growing concern for adolescents who experience adjustmentproblems emphasizes the need for identification of protectiveand risk factors, and development of evidence-based preventions.Different types of individual coping strategies are identified aseither protective or risk factors in relation to health and well-being(Lazarus, 1993; Masten, Best & Garmezy, 1990; Seiffge-Krenke,1998). For instance, in adolescence, individual coping strategiesare found to interact with well-being and adjustment (Jorgensen& Dusek, 1990; Tolor & Fehon, 1987), success at school(Kristensson & Öhlund, 2005; Rijavec & Brdar, 1997; Whatley,Foreman & Richards, 1998), and physical and mental health(Graue, Hanestad, Wentzel-Larsen, Sövik & Bru, 2004; Reid,Dubow & Carey, 1995; Reid, Dubow, Carey & Dura, 1994;Seiffge-Krenke & Klessinger, 2000; Smith, Smoll & Ptacek,1990; Steiner, Erickson, Hernandez & Pavelski, 2002; Zeidner& Hammer, 1990).
Lazarus’s cognitive transactional theory of coping (Lazarus& Folkman, 1984) has been a major inspiration for copingresearch during the last two decades. Based on that theory, anumber of coping measures for adults (e.g., Billings & Moos,1984; Carver, Scheier & Weintraub, 1989; Endler & Parker,1990; Folkman & Lazarus, 1985, 1988; McCrae, 1984; McCrae& Costa, 1986; Pearlin & Schooler, 1978; Stone & Neale, 1984)and adolescents (e.g., Brodzinsky, Elias, Steiger, Simon &Gill, 1992; Dise-Lewis, 1988; Ebata & Moos, 1991; Fanshawe& Burnett, 1991; Frydenberg & Lewis, 1993; Seiffge-Krenke,1989) have been developed. Researchers generally agree on thefollowing issues related to coping: coping strategies (items)
cluster into primary coping factors; coping strategies may beof either a cognitive or behavioral nature; individuals eitherapproach a problem or avoid it; and there is an interactionbetween coping strategies and situation characteristics. However,confusion still exists around other key issues within the field,and consensus on how to define and hence measure copinghas not as yet been reached. For instance, Steger (2006) noteda different factor structure for each of the numerous post hocfactor analytical studies conducted between 1987 and 2000 onthe Folkman and Lazarus scale of adult coping. Adolescentcoping scales are also varied. For instance, while one researcherreports 80 strategies clustering into 18 primary factors(Frydenberg & Lewis, 1993), another suggests 20 strategiesclustering into three factors (Seiffge-Krenke, 1989). Further-more, conceptualization of second-order factors of coping isinconsistent in the literature. Lazarus and Folkman (1984)suggested that coping (adult) is either problem-focused oremotion-focused, the former aiming at changing the situation ormanaging the problem, and the latter at controlling the emotionsrelated to the problem. Although Lazarus and Folkman did notpresent that dichotomy as statistically derived second-orderfactors, some researchers on adult coping have done so, andhave suggested second-order factors relating either to the focus(e.g., Billings & Moos, 1981; Ebata & Moos, 1991, 1994; Pearlin& Schooler, 1978) or to the outcome of coping (i.e., positive ornegative) (e.g., McCrae & Costa, 1986; Parkes, 1986). However,distinction between problem- and emotion-focused second-order factors has not yet been statistically verified for adult oradolescent coping (Ficková, 1998; Jorgensen & Dusek, 1990;Tobin, Holroyd, Reynolds & Wigal, 1989; Watson, Willson &Sinha, 1998).

534 S. Sveinbjornsdottir and E. B. Thorsteinsson Scand J Psychol 49 (2008)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
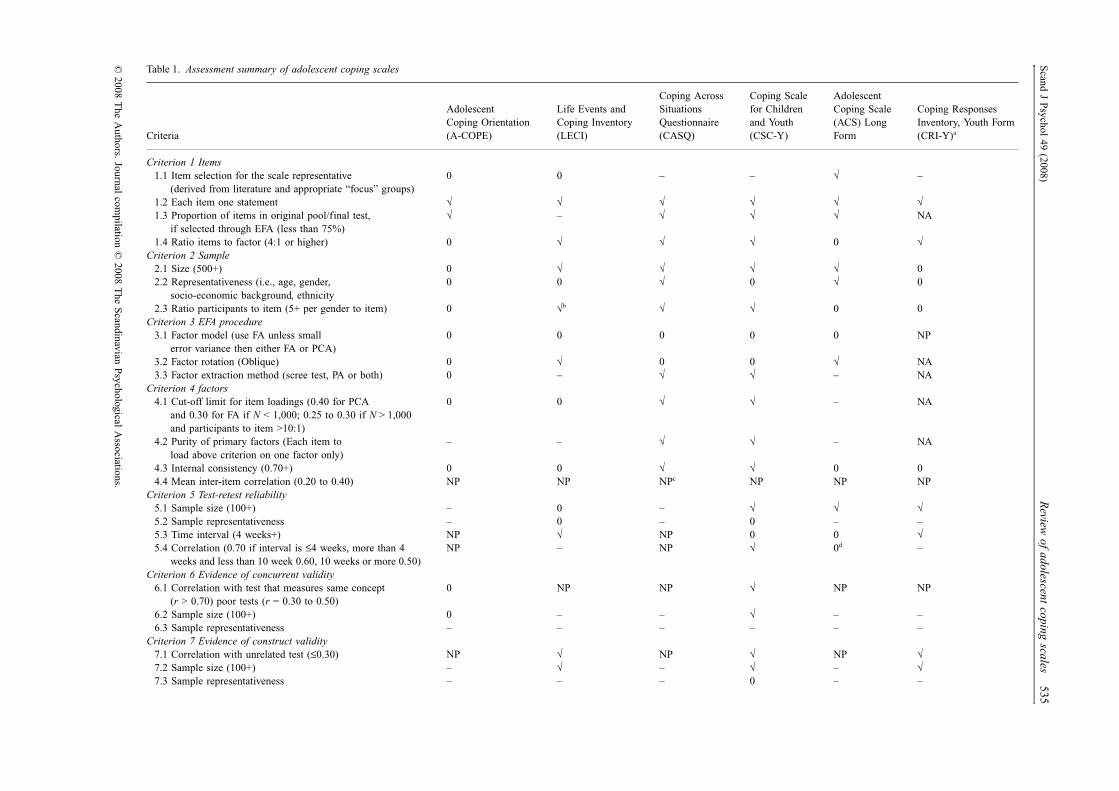
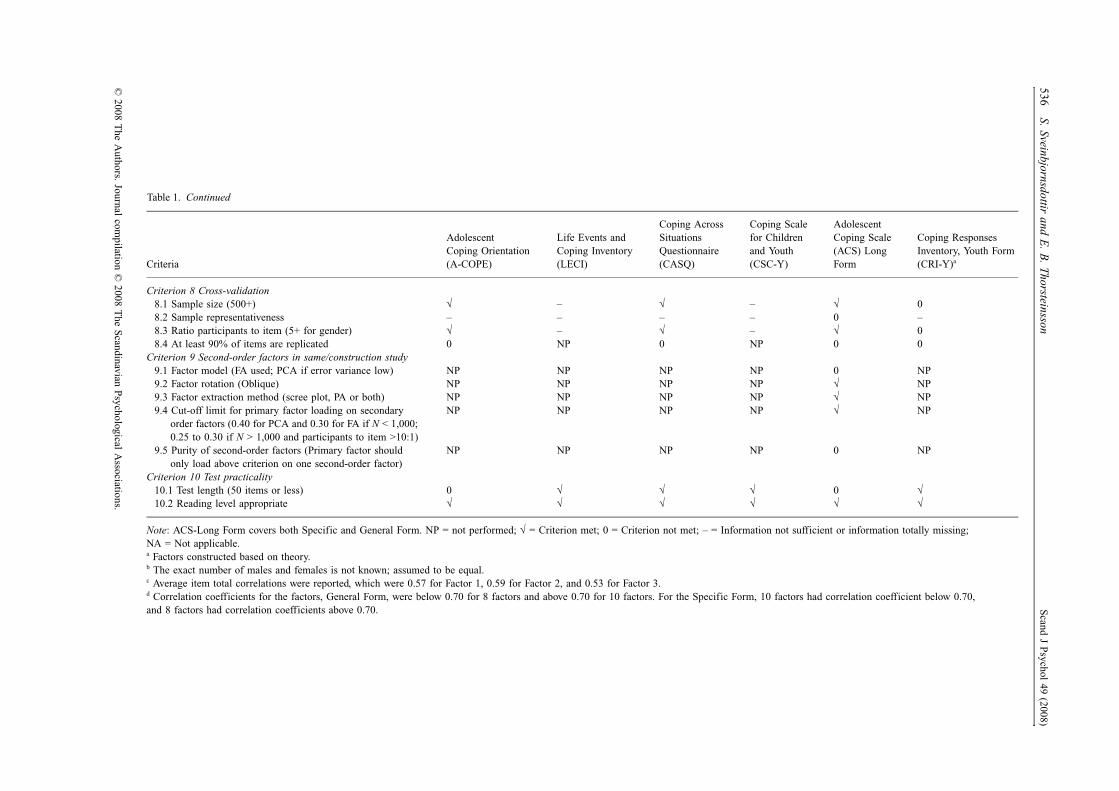
Researchers who use exploratory factor analysis (EFA) inpsychological research are frequently found to make poorstatistical decisions throughout the process of EFA (Conway &Huffcutt, 2003; Fabrigar, Wegener, MacCallum & Strahn, 1999;Ford, MacCallum & Tait, 1986), leading to spurious outcomes.Furthermore, psychological measures have been found to berationally derived rather than developed through systematicquantitative content validation (Haynes, Richard & Kubany,1995). Concerns about the methodological soundness of copingscales have been raised (Benson & Hagtvet, 1996; Compas,Connor-Smith, Saltzman, Thomsen & Wadsworth, 1999), andcoping scales of children, adolescents, and adults have beenreviewed (e.g., Compas, Connor-Smith, Saltzman, Thomsen &Wadsworth, 2001; Schwarzer & Schwarzer, 1996). Despite thefact that most coping scales are developed according to classicaltest-theory and through EFA, review of the development ofcoping scales in relation to test-theoretical criteria and theimplementation of EFA has, to our knowledge, not yet beenperformed. In a recent exhaustive review of coping assessmentsand the search for the structure of coping, it is suggested thatconfirmatory rather than exploratory factor analyses be usedfor construction of primary coping factors, and confirmatoryhierarchical analyses be used for determination of higher orderfactors or dimensions of coping (Skinner, Edge, Altman &Sherwood, 2003). However, we argue an investigation of thefoundations of the scales is needed, requiring an analysis of thequality of the EFA procedures throughout scale development.Our hypothesis is that poor quality EFA procedures, as earlierdetected in psychological research (Conway & Huffcutt, 2003;Fabrigar, Wegener, MacCallum & Strahn, 1999; Ford, MacCallum& Tait, 1986), might similarly be found in the development ofcoping scales. The aim of the present review is to criticallyexamine statistical choices throughout the development ofadolescent coping scales as suggested by classical best test-theoretical practice. A brief presentation of psychometric issuesand criteria used for the present review is outlined below. Seethe summary in Table 1.
Best-practice as suggested by classical test-theory for development of a psychological test
Item selection is the base of content validity. If a literaturesearch provides limited knowledge, information from informedindividuals is needed (Haynes et al., 1995; Kline, 1986). Testitems must be clear and easily understood, and must be keptshort, containing only one point or statement (DeVellis, 1991).For selection of the most salient items, up to twice as manyitems as will be included in the final version are needed in theinitial stage as suggested by Kline (1986). To support replicabilityof a test, different numbers of items per factor have beensuggested. MacCallum, Widaman, Zhang, and Hong (1999)have suggested a minimum of three to five items per factor,Fabrigar et al. (1999) have suggested four, while Gorsuch (1983)has suggested six items per factor. Four items per factor is thecriterion for the present review.
Size and representativeness of the construction sample isvital for construct validity, and gender, age, socioeconomicbackground, and ethnicity must be known. The ratio of participantsper test item affects the standard error, yet there is no clear ruleto follow. Ten participants to each item has been considered safe(Child, 1990), and actually recommended (Nunnally, 1978). Yetsome consider a ratio of five to one sufficient (Gorsuch, 1983;Tabachnick & Fidell, 1989) or even three to one for each gender(Kline, 1993). A recent study on best practice using EFAreported an error rate of 30% at a ratio of 20:1 on a sample sizeof 260 (Costello & Osborne, 2005), indicating an even greaterimportance of having a high ratio of participants per item thanpreviously believed. The criteria for the present review of scaleconstruction are a minimum of 10 participants per item (five ormore per gender) and a minimum of 500 participants.
Choices of EFA procedures concern (a) model of analysis,(b) factor rotation, and (c) factor extraction method. Model ofanalysis is most commonly a choice between common FactorAnalysis (FA) and Principal Components Analysis (PCA), thedefault extraction method in SPSS. PCA has proven to obscureoutcomes because of inflation of factor loadings, especiallythose of lower or moderate value, where FA has not (Fabrigaret al., 1999; Gorsuch, 1983; Widaman, 1993). Furthermore,there is no prior knowledge of unique variance within thecorrelation matrix when a test is being developed, and touncover latent factors that are as uncontaminated by that kindof variability as possible, the choice of model of analysis shouldbe FA rather than PCA (Conway & Huffcutt, 2003). The criterionfor the present review is FA.
Of a number of analytic rotation methods, the most essentialdistinction is between orthogonal and oblique rotation. Obliquerotation allows correlations between factors, and since charac-teristics of human behavior are believed to be interrelated(Child, 1990), the oblique factor rotation has been suggested asa first choice. The combination of oblique rotations and FAyields the simplest structure when compared with: obliquerotation and PCA; orthogonal rotation and PCA; and orthogonalrotation and FA (Fabrigar et al., 1999). This lends further supportfor the choice of FA and oblique rotation.
Factor extraction is a challenge: extracting too many factors(overfactoring) or too few factors (underfactoring) leads toerror. Two commonly cited extraction methods, often used incombination, are the latent root criterion (eigenvalue greaterthan one or Kaiser’s criterion) and Cattell’s scree test (Child,1990; Tabachnick & Fidell, 1989). Kaiser’s criterion is generallynot found to be a satisfactory method (Conway & Huffcutt,2003; Fabrigar et al., 1999; Velicer & Jackson, 1990). ParallelAnalysis (PA) is considered more accurate (Fabrigar et al., 1999;Hayton, Allen & Scarpello, 2004), especially when used incombination with a scree test. However, PA is not currentlyavailable in commonly used statistical programs like SPSS,although it is possible to conduct it stepwise (Hayton et al.,2004). Therefore, a scree test has been suggested by some asthe best choice for the time being (Costello & Osborne, 2005),and is the criterion for the present review. For future development
Scand J Psychol 49 (2008)R
eview of adolescent coping scales
535
© 2008 T
he Authors. Journal com
pilation © 2008 T
he Scandinavian Psychological Associations.
Table 1. Assessment summary of adolescent coping scales
Criteria
Adolescent Coping Orientation (A-COPE)
Life Events and Coping Inventory (LECI)
Coping Across Situations Questionnaire (CASQ)
Coping Scale for Children and Youth (CSC-Y)
Adolescent Coping Scale (ACS) Long Form
Coping Responses Inventory, Youth Form (CRI-Y)a
Criterion 1 Items1.1 Item selection for the scale representative
(derived from literature and appropriate “focus” groups)0 0 – – √ –
1.2 Each item one statement √ √ √ √ √ √1.3 Proportion of items in original pool/final test,
if selected through EFA (less than 75%)√ – √ √ √ NA
1.4 Ratio items to factor (4:1 or higher) 0 √ √ √ 0 √Criterion 2 Sample
2.1 Size (500+) 0 √ √ √ √ 02.2 Representativeness (i.e., age, gender,
socio-economic background, ethnicity0 0 √ 0 √ 0
2.3 Ratio participants to item (5+ per gender to item) 0 √b √ √ 0 0Criterion 3 EFA procedure
3.1 Factor model (use FA unless small error variance then either FA or PCA)
0 0 0 0 0 NP
3.2 Factor rotation (Oblique) 0 √ 0 0 √ NA3.3 Factor extraction method (scree test, PA or both) 0 – √ √ – NA
Criterion 4 factors4.1 Cut-off limit for item loadings (0.40 for PCA
and 0.30 for FA if N < 1,000; 0.25 to 0.30 if N > 1,000 and participants to item >10:1)
0 0 √ √ – NA
4.2 Purity of primary factors (Each item to load above criterion on one factor only)
– – √ √ – NA
4.3 Internal consistency (0.70+) 0 0 √ √ 0 04.4 Mean inter-item correlation (0.20 to 0.40) NP NP NPc NP NP NP
Criterion 5 Test-retest reliability5.1 Sample size (100+) – 0 – √ √ √5.2 Sample representativeness – 0 – 0 – –5.3 Time interval (4 weeks+) NP √ NP 0 0 √5.4 Correlation (0.70 if interval is ≤4 weeks, more than 4
weeks and less than 10 week 0.60, 10 weeks or more 0.50)NP – NP √ 0d –
Criterion 6 Evidence of concurrent validity6.1 Correlation with test that measures same concept
(r > 0.70) poor tests (r = 0.30 to 0.50)0 NP NP √ NP NP
6.2 Sample size (100+) 0 – – √ – –6.3 Sample representativeness – – – – – –
Criterion 7 Evidence of construct validity7.1 Correlation with unrelated test (≤0.30) NP √ NP √ NP √7.2 Sample size (100+) – √ – √ – √7.3 Sample representativeness – – – 0 – –
536S. Sveinbjornsdottir and E
. B. Thorsteinsson
Scand J Psychol 49 (2008)
© 2008 T
he Authors. Journal com
pilation © 2008 T
he Scandinavian Psychological Associations.
Criterion 8 Cross-validation8.1 Sample size (500+) √ – √ – √ 08.2 Sample representativeness – – – – 0 –8.3 Ratio participants to item (5+ for gender) √ – √ – √ 08.4 At least 90% of items are replicated 0 NP 0 NP 0 0
Criterion 9 Second-order factors in same/construction study9.1 Factor model (FA used; PCA if error variance low) NP NP NP NP 0 NP9.2 Factor rotation (Oblique) NP NP NP NP √ NP9.3 Factor extraction method (scree plot, PA or both) NP NP NP NP √ NP9.4 Cut-off limit for primary factor loading on secondary
order factors (0.40 for PCA and 0.30 for FA if N < 1,000; 0.25 to 0.30 if N > 1,000 and participants to item >10:1)
NP NP NP NP √ NP
9.5 Purity of second-order factors (Primary factor should only load above criterion on one second-order factor)
NP NP NP NP 0 NP
Criterion 10 Test practicality10.1 Test length (50 items or less) 0 √ √ √ 0 √10.2 Reading level appropriate √ √ √ √ √ √
Note: ACS-Long Form covers both Specific and General Form. NP = not performed; √ = Criterion met; 0 = Criterion not met; – = Information not sufficient or information totally missing; NA = Not applicable.a Factors constructed based on theory.b The exact number of males and females is not known; assumed to be equal.c Average item total correlations were reported, which were 0.57 for Factor 1, 0.59 for Factor 2, and 0.53 for Factor 3.d Correlation coefficients for the factors, General Form, were below 0.70 for 8 factors and above 0.70 for 10 factors. For the Specific Form, 10 factors had correlation coefficient below 0.70, and 8 factors had correlation coefficients above 0.70.
Criteria
Adolescent Coping Orientation (A-COPE)
Life Events and Coping Inventory (LECI)
Coping Across Situations Questionnaire (CASQ)
Coping Scale for Children and Youth (CSC-Y)
Adolescent Coping Scale (ACS) Long Form
Coping Responses Inventory, Youth Form (CRI-Y)a
Table 1. Continued

Scand J Psychol 49 (2008) Review of adolescent coping scales 537
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
of tests, PA combined with a scree test seems likeliest to berecommended as best practice.
Item loadings indicate factors, but test developers need to becautious. First, different models of analysis may produce loadingresults that differ for the same sample and variables. PCA mayproduce higher loadings than FA (Gorsuch, 1983), and theinflation is stronger for lower and moderate loadings, 0.40 orless, than for loadings of 0.80 or higher (Fabrigar et al., 1999;Sveinbjornsdottir, 2001; Widaman, 1993). Second, factor loadingsare partly due to sample size, and correlations for larger samplesare usually lower than for smaller samples (Tabachnick &Fidell, 1989). Therefore, a salient loading for one study maybe inappropriate for another. For the present review, if FA isemployed and the number of participants is at least 500, theloading criterion is 0.30 and as low as 0.25 if the number ofparticipants exceed 1,000. If PCA is employed, the criterion forminimum loading is 0.40 for 500 participants or more.
An item is expected to load saliently on one factor only, anda minimum internal consistency for a factor is 0.70 (Kline,1993; Nunnally, 1978). However, since high internal consistencymay carry a risk of items being only slight variations of eachother (Child, 1990; Kline, 1993, 1994; Tabachnick & Fidell, 1989),inter-item correlation for a factor is optimal when ≥ 0.20 and≤0.40 (Briggs & Cheek, 1986).
Minimum criteria for test-retest analysis are a correlation of0.70 (Kline, 1986) or even 0.80 (Kline, 1993), 100 participants,and a three-month interval. However, over a three-month perioda significant change in cognition may occur, affecting theadolescents’ coping behavior. Therefore, with a minimumsample of 100 the correlation criterion for the present review is0.70 for a four-week interval, 0.60 for a four- to ten-week interval,and 0.50 for an interval longer than ten weeks.
For further evidence of validity, administered simultaneouslyto the same minimum sample of 100, the correlation betweenan examined scale and another one measuring the same variable(concurrent), is expected to be at least 0.70 unless one or bothscales are of poor quality then only a moderate correlation of0.50 is expected (Kline, 1986). Low correlation is expected(<0.30) between an examined scale and another conceptuallydifferent (construct) scale. Replication, either through EFAcross-validation or confirmatory factor analysis (CFA) on arepresentative independent sample of at least 500, and parti-cipants five or more per gender, is proven if 90% of items andthe factor structure hold as suggested by Kline (1986).
Second-order (or any higher-order) factor analysis is safely con-ducted if earlier factor analysis used oblique rotation. The criteriafor the present review are FA, oblique rotation, and scree test (or PA).
Scale practicality is of value for a scale-taker as well as theadministrator. Issues of importance are the scale taker’s readinglevel, and the level of complexity and length of the scale. Nogeneral recommendations are found in the literature and criterionfor the present review is arbitrary. For the possibility of extractingfactors, a minimum of 20 items is suggested, and so as not tostrain the attention of scale-takers, a maximum of 50 items issuggested.
METHOD
Literature searches
An electronic search was performed for self-rating adolescent copingscales for general situations in the databases PsycINFO, Eric, PubMed,and Google Scholar. A large number of key articles on adolescent coping,limited to years 1980 through 2007 were also cross-referenced. Key-words for the search included various combinations of the followingconcepts: coping scale, adolescence, reliability, validity, psychometricproperties, test construction, scale construction. Six scales were foundthat fitted the following inclusion criteria.
Inclusion and exclusion criteria
Included in the present review are coping scales, where coping strategiesare clustered in factors, and specifically developed for adolescent popu-lations between 12 and 18 years of age. Therefore, a coping checklistsuch as Kidcope, a list of ten items (Spirito, Stark & Williams, 1988),is excluded. Cognitive skills affect thinking and hence coping, andbecause of adolescents’ growing meta-cognitive skills, their copingstrategies may include cognitive coping strategies, whereas children’scoping tends to be more concrete and related to observable behavior(for review see Boekaerts, 1996). Therefore, coping scales developedfor younger populations such as the Self-Reported Coping Measure(Causey & Dubow, 1992), and then tested on adolescents without furtherdevelopment or refinement (Ayers, Sandler & Twohey, 1998), wereexcluded. The same applied for coping scales developed for adults.Although adolescents and adults have similar cognitive capacities,adults have more experience and their social and economic circum-stances are different to those of adolescents. Thus adults belong to adifferent population. Scales developed for adults that have subsequentlybeen tested for use with adolescents with minimal modification wereexcluded. Examples of such scales include COPE (Carver et al., 1989)and the Ways of Coping Checklist (WCC; Folkman & Lazarus, 1980).The present review focuses on coping with general concerns or dailyhassles. Therefore, measures of situation-specific coping, such as theSchool Failure Coping Scale (SFCS; Rijavec & Brdar, 1997) and theResponses to Stress Questionnaire (Connor-Smith, Compas, Wadsworth,Thomsen & Saltzman, 2000) were excluded. Scenario-based instru-ments such as the Cross-Cultural Coping Scale (Kuo, Roysircar &Newby-Clark, 2006), and population-specific coping scales, such asthe Coping Function Questionnaire for adolescent sport participants(Kowalsky & Crocker, 2001), were likewise excluded.
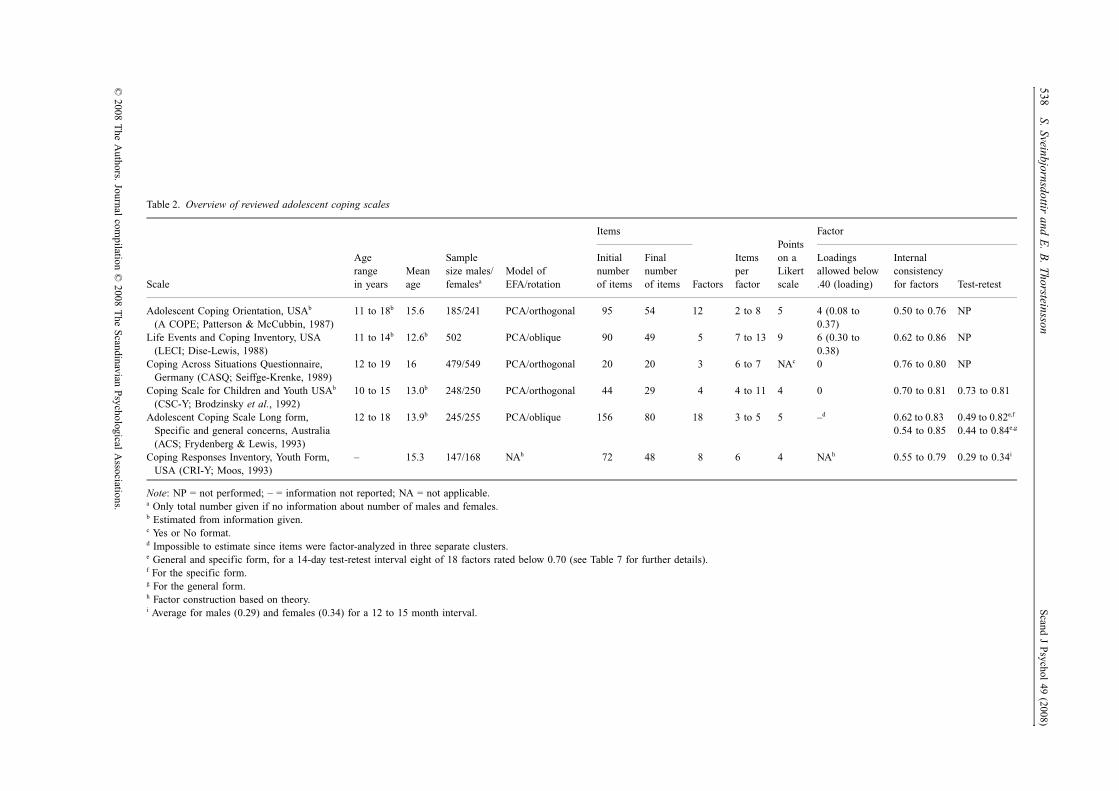
Six adolescent coping scales were identified for inclusion, fourdeveloped in the USA, one in Germany, and one in Australia: (1)Adolescent Coping Orientation, USA (A-COPE; Patterson & McCubbin,1987), (2) Life Events and Coping Inventory, USA (LECI; Dise-Lewis,1988), (3) Coping Across Situations Questionnaire, Germany (CASQ;Seiffge-Krenke, 1989), (4) Coping Scale for Children and Youth, USA(CSC-Y; Brodzinsky et al., 1992), (5) Adolescent Coping Scale, Australia(ACS; Frydenberg & Lewis, 1993), and (6), Coping Responses Inventory,Youth Form, USA (CRI-Y; Moos, 1993). An overview of the scales isprovided in Table 2.
RESULTS
(1) Adolescent Coping Orientation for Problem Experiences (A-COPE; Patterson & McCubbin, 1987)
The A-COPE is based on the Double ABCX model (McCubbin& Patterson, 1981, 1982, 1983), an extension of Hill’s theoryon family response to stress (Burr, 1982; McCubbin & Patterson,
538S. Sveinbjornsdottir and E
. B. Thorsteinsson
Scand J Psychol 49 (2008)
© 2008 T
he Authors. Journal com
pilation © 2008 T
he Scandinavian Psychological Associations.
Table 2. Overview of reviewed adolescent coping scales
Scale
Age range in years
Mean age
Sample size males/femalesa
Model of EFA/rotation
Items
Factors
Items per factor
Points on a Likert scale
Factor
Initial number of items
Final number of items
Loadings allowed below .40 (loading)
Internal consistency for factors Test-retest
Adolescent Coping Orientation, USAb (A COPE; Patterson & McCubbin, 1987)
11 to 18b 15.6 185/241 PCA/orthogonal 95 54 12 2 to 8 5 4 (0.08 to 0.37)
0.50 to 0.76 NP
Life Events and Coping Inventory, USA (LECI; Dise-Lewis, 1988)
11 to 14b 12.6b 502 PCA/oblique 90 49 5 7 to 13 9 6 (0.30 to 0.38)
0.62 to 0.86 NP
Coping Across Situations Questionnaire, Germany (CASQ; Seiffge-Krenke, 1989)
12 to 19 16 479/549 PCA/orthogonal 20 20 3 6 to 7 NAc 0 0.76 to 0.80 NP
Coping Scale for Children and Youth USAb (CSC-Y; Brodzinsky et al., 1992)
10 to 15 13.0b 248/250 PCA/orthogonal 44 29 4 4 to 11 4 0 0.70 to 0.81 0.73 to 0.81
Adolescent Coping Scale Long form, Specific and general concerns, Australia (ACS; Frydenberg & Lewis, 1993)
12 to 18 13.9b 245/255 PCA/oblique 156 80 18 3 to 5 5 –d 0.62 to 0.83 0.54 to 0.85
0.49 to 0.82e,f 0.44 to 0.84e,g
Coping Responses Inventory, Youth Form, USA (CRI-Y; Moos, 1993)
– 15.3 147/168 NAh 72 48 8 6 4 NAh 0.55 to 0.79 0.29 to 0.34i
Note: NP = not performed; – = information not reported; NA = not applicable.a Only total number given if no information about number of males and females.b Estimated from information given.c Yes or No format.d Impossible to estimate since items were factor-analyzed in three separate clusters.e General and specific form, for a 14-day test-retest interval eight of 18 factors rated below 0.70 (see Table 7 for further details).f For the specific form.g For the general form.h Factor construction based on theory.i Average for males (0.29) and females (0.34) for a 12 to 15 month interval.

Scand J Psychol 49 (2008) Review of adolescent coping scales 539
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
1983). The Double ABCX model refers to variables believedto be of importance for the well-being of the family as a unit,and for each individual family member (McCubbin & Patterson,1983, 1986; Patterson & McCubbin, 1987).
Items were generated through structured interviews with 30students of both sexes from a suburban mid-western high school,grades 10 through 12. A total of 95 coping items were identifiedand factor analyzed, using PCA with orthogonal rotation, on467 junior and senior high school students, 185 males and 241females (mean age of 15.6 years; gender information missingfor some participants). Participants were from suburban mid-westernschools, mainly of middle to upper-middle socioeconomic status(no further information). Responses on a five-point Likert scalewith minimal variance were removed from the scale, leaving 68of 95 items for factor analysis. Twelve factors with eigenvaluesof 1.0 or above were extracted, including 54 items, see Table 3.Factorial purity is unclear; information was provided on howeach item loaded on one factor only.
A second-order maximum likelihood (ML) analysis withoblique rotation was conducted on an independent sample of331 undergraduate volunteers (age 18; 192 females and 139males, no further information) (Jorgensen & Dusek, 1990). Twosecond-order factors with eigenvalues of 1.0 or greater emerged.Nine factors clustered together in a second-order factor namedSalutary Effort (i.e., Engaging in Demanding Activity, DevelopingSelf-Reliance and Optimism, Developing Social Support,Seeking Diversions, Solving Family Problems, Seeking SpiritualSupport, Investing in Close Friendships, Being Humorous,and Seeking Professional Support effort). The remaining threefactors reflected angry reactions and avoidance, and the second-order factor was named Stress Palliation (Relaxing, VentilatingFeelings, and Avoiding Problems). All factors loaded beyond0.30 on their second-order factor less one (Seeking Professionalhelp, loading 0.22).
Further information on validity. The A-COPE was examinedthrough relationships between adolescent substance use and
coping (Patterson & McCubbin, 1987). The number of partic-ipants and demographic information is confusing (see pp. 171and 177), and 3 of the 12 A-COPE factors were excluded.Therefore, the outcome for the full-length scale is blurred. Inanother study (Spirito et al., 1988), 49 students (demographicinformation unclear) completed A-COPE and Kidcope on thesame occasion. Correlations between A-COPE factors andKidcope items were mixed and somewhat difficult to interpret;they ranged from 0.08 to 0.62, where most of the highercorrelations were between conceptually similar Kidcope itemsand A-COPE factors.
Four independent studies failed to replicate the A-COPE factorstructure. Three performed EFA (Fanshawe & Burnett, 1991;Halvarsson, Lunner & Sjödin, 2001; Plancherel & Bolognini,1995), and one CFA (ACSS; Burnett & Fanshawe, 1996).Through a post hoc approach of the 54 A-COPE items, theresearchers created scales on their own data.
Limitations of the A-COPE. First, information was missingon: (a) demographics for the construction sample, and (b) theloadings of each item on all factors, informing on the degreeof factorial purity. Secondly, questionable methods wereemployed, such as: (a) initial selection of coping items, (b)PCA for factor analysis, (c) orthogonal rotation of factors,and (d) factor extraction based on eigenvalues. In addition,given the length of the scale, a second-order factor analysisshould have been performed on the construction data. Thirdly,some reported statistical properties of the scale were unsatis-factory, such as: (a) four factors were comprised of threeitems or fewer, (b) three factors had internal reliability below0.70, (c) four items loaded below 0.40 on their factor, and (d)one confirmatory factor analysis and three cross-validationstudies on independent samples failed to replicate the factorstructure of A-COPE. Finally, some important analyses werenot performed, such as: (a) inter-item correlations and (b)test-retest reliability, and (c) correlation with an unrelatedtest.
Table 3. A-COPE factor structure and internal consistency
Factors Items Example Internal consistency
Ventilating feelings 6 Get angry and yell at people 0.75Seeking diversions 8 Sleep 0.75Developing self-reliance and optimism 6 Try on your own to figure out how to deal
with your problems or tensions 0.69
Developing social support 6 Try to help other people solve their problems 0.75Solving family problems 6 Talk to your father about what bothers you 0.75Avoiding problems 5 Use drugs (not prescribed by a doctor) 0.71Seeking spiritual support 3 Go to church 0.72Investing in close friends 2 Be close to someone you care about 0.76Seeking professional support salutary effect 2 Get professional counseling
(not a school teacher or a school counselor)0.50
Engaging in demanding activity 4 Do a strenuous physical activity (jogging, biking etc.) 0.67Being humorous 2 Joke and keep a sense of humor 0.72Relaxing 4 Daydream about how you would like things to be 0.60

540 S. Sveinbjornsdottir and E. B. Thorsteinsson Scand J Psychol 49 (2008)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
(2) Life Events and Coping Inventory (LECI; Dise-Lewis, 1988)
The LECI assesses stressful life events and coping based on thetransactional model of stress and coping (Lazarus & Folkman,1984) and Holmes and Rahe’s (1967) “social consensus methodof operationalizing stress” (Dise-Lewis, 1988, p. 485), includingminor and major incidents. The scale was developed stepwise:(a) initial item generation (N = 104), (b) item refinement andaddition (N = 90), (c) data for scale construction (N = 502), (d)reliability data (N = 85), and (e) validity data (N = 198), with a totalnumber of 681 participants for all the steps (11 to 14 years of age,M = 12.6, SD = 0.5). Participants were mainly white, of middleand upper-middle class background, from Denver, Colorado.
Items were collected through individual and small groupinterviews of 104 participants, and were refined in three steps,using 90 participants. Wording was scrutinized, instructionsfinalized and two different types of rating systems compared.There was no information on number of items in the originalpool. The final scale included 125 life events and 49 copingitems. Here, only the coping part of the LECI is reviewed. PCAwith oblique rotation was conducted with answers rated on afive-point Likert scale, employing 502 participants. Five factorswere extracted; no information on factor extraction and factorialpurity is provided. Loading of items on factors is reported forone factor only. The factor Stress Recognition includes itemsthat mainly refer to seeking social support, yet the two highestloading items (“Cry” and “Scream”) on that factor do nothave face validity. For factor structure and internal consistency,see Table 4.
Further information on reliability and validity. A replicationsample of 85 participants completed the LECI twice with an11-week interval, and the correlation coefficient for individualitems ranged from −0.13 to 0.61 with a mean of 0.32. Thecorrelation coefficient was reported in this way – “the stabilityof the set of coping strategy ratings was .98” (Dise-Lewis, 1988,p. 493) – which is difficult to interpret with the item correlationranging from −0.13 to 0.61, and an interval of 11 weeks for12-year old participants. A subset of the construction sample,198 participants, was also administered the State-Trait AnxietyInventory for Children and the Children’s Depression Inventory.Correlation between LECI coping factors and these measuresranged from 0.00 to 0.30.
Limitations of the LECI. First, information was missing on (a)demographics for the construction sample, (b) the ratio offemales and males for the total sample of 681 adolescents, (c)what statistical methods were chosen for factor extraction, and(d) loadings of each item on all factors, informing on thedegree of factorial purity. Information on test-retest reliabilitywas unclear. Secondly, information provided for the constructionsample, including initial item generation, indicates homogeneity,and the choice of PCA for factor analysis is questionable.Thirdly, there were unsatisfactory statistical properties such as:(a) the sample did not represent all socio-economic groups,(b) internal consistency reliability was below 0.70 on one factor,(c) six items loaded below 0.40 on their factor, (d) two of thehighest loading items on the factor Stress-recognition wereconceptually unrelated to that factor. Finally, analyses concerning(a) inter-item correlations and (b) correlation with a related test,and (c) cross-validation of factor structure, were not performed.
(3) Coping Across Situations Questionnaire (CASQ; Seiffge-Krenke, 1989)
The CASQ was developed within the framework of cognitive-transactional theory (Lazarus & Folkman, 1984; Seiffge-Krenke& Shulman, 1993). Items were selected and developed in stages.First, adolescents’ main stressors and coping responses wereassessed from a sample of 107 adolescents, 12 to 18 years (nofurther information). The 110 identified coping responseswere categorized according to Westbrook’s coping scale (1979,as cited in Seiffge-Krenke, 1989, p. 208), and 95% of responsesfell within three of Westbrook’s five factors (i.e., Active Coping,Withdrawal, and Seeking Help from Others). Where themeaning of the adolescents’ coping responses correspondedwith the content of items from Westbrook’s scale, the itemsfrom Westbrook’s scale were translated into German and thewording adapted for adolescents. The final version of the CASQincluded twenty items, each containing only one statement.
PCA (this is assumed based on Kavsek & Seiffge-Krenke,1996) and orthogonal rotation (Seiffge-Krenke, 1989) wereperformed with yes or no ratings from 1,028 students aged 12through 19 years old (61 were 12, 70 were 13, 94 were 14, 119were 15, 220 were 16, 210 were 17, 182 were 18, and 72 were19) by Hessen, Nordrhein-Westfalen and Niedersachsen. Half
Table 4. LECI-Coping factor structure and internal consistency
Factors Items Example
Internal consistency
Construction sample
Replication sample
Aggression 7 Hit someone or hurt someone physically 0.86 0.85Stress-recognition 13 Write to someone else about it 0.79 0.80Distraction 12 Do a hobby or something I enjoy 0.76 0.83Self-destruction 8 Smoke cigarettes 0.86 0.85Endurance 9 Just hold it in 0.62 0.68

Scand J Psychol 49 (2008) Review of adolescent coping scales 541
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
of the sample was from urban, and half from rural areas andparental occupation was representative of Western Germany in1984 when the data was collected. Sixty percent of mothers werehomemakers or working part-time (no further information).Fathers were white collar workers (54%), blue collar workers(25%), self-employed (14%), and professionals (7%). A screetest revealed three factors, with item loadings 0.40 or beyond,and communality ranging from 0.26 to 0.62, see factor summaryin Table 5.
Further information on validity. The CASQ factor structurewas cross-examined in two independent studies and partlyreplicated (Seiffge-Krenke, 1992; Seiffge-Krenke & Shulman,1990). Ten of the CASQ items (50%) loaded on correspondingfactor for both the Israeli and the Finnish sample; the other tenitems were either mixed or omitted.
Limitations of the CASQ. First, it was unclear how well thesample represents the population. Secondly, questionable statisticalmethods were chosen for both construction and validation studiessuch as PCA and orthogonal factor rotation. Second-order factoranalysis was not performed despite the high correlation betweentwo of the three factors (which indicates that there may be twodistinct second-order coping factors rather than three). Thirdly,analyses concerning (a) test-retest, and (b) correlation withscales, related as well as unrelated, were not performed. Finally,two cross-validation studies with independent samples verified50% of the factor structure.
(4) Coping Scale for Children and Youth (CSC-Y; Brodzinsky et al., 1992)
The CSC-Y was developed with theoretical background inpre-existing coping research on adults, which was mainly basedon the transactional approach (Lazarus & Folkman, 1984).Literature search on children’s and adults’ coping revealed 44items. The authors assumed that youth might: (a) approach astressor to deal with or confront with it; (b) avoid a stressorto reduce tension; or (c) become passive and resign. They
furthermore assumed that whether they be approach oravoidant, coping responses would be either cognitive (affective) orbehavioral. The authors expected final selection of items forthe CSC-Y to fall into these categories: (a) cognitive/affectiveengagement; (b) behavioral engagement; (c) cognitive/affectiveavoidance; (d) behavioral avoidance; and (e) passive resignation.
PCA with orthogonal rotation was performed on a sample of498 Grade 6 and Grade 8 students (aged 10 through 15 years)recruited from a suburban, mostly white, middle-class community(no information on state or country). There were 224 Grade 6students (114 females and 110 males, M = 11.6 years), and 274Grade 8 students (136 females and 138 males, M = 13.7 years).Responses were rated on a four-point Likert scale. A scree testsuggested four factors and not five as originally assumed. Asecond PCA analysis with orthogonal rotation analysis callingfor four factors revealed 29 items of 44 (66%) with loading of0.40 or beyond on one factor only. Test-retest results (one-weekinterval) were based on 145 participants randomly chosen fromthe construction sample (i.e., 61 females and 84 males; 55 fromgrade 6 and 90 from grade 8), see Table 6.
Further evidence of validity. First, the authors (Brodzinsky et al.,1992) reported low to moderate correlation between the fourfactors of the CSC-Y and seven out of ten of Kidcope’s copingstrategies (Spirito et al., 1988), with coefficients ranging from0.30 to 0.62. Participants in that study were 60 boys and 60girls, with a mean age of 11.2 years, from a suburban com-munity. They were mostly white and middle class. Secondly, theauthors administered the four-factor CSC-Y and the six-factorSelf-Perception Profile for Children (SPPC) to 190 participants,12- or 13-year-old Grade 7 students, mostly white and froma middle-class suburban community. Correlations were low tomoderate (r ≤ 0.30) for 23 out of 24 relationships between thetwo tests (the correlation between SPPC/Global Self-Worth andCSC-Y/Cognitive –Behavioral Problem Solving was r = 0.35;p < 0.001). Furthermore, the CSC-Y and the Kidcope weresimultaneously administered in Slovenia to 166 high schoolstudents, 51 females and 36 males from a freshman class (meanage 14.9 years), and 54 females and 25 males from junior class
Table 5. CASQ factor structure, internal consistency, and average corrected item-total correlation
Factors Items ExampleInternal consistency
Average corrected item-total correlation
Active coping by means of social resources (Aktive Bewältigung unter Nutzung sozialer Ressourcen)
7 I try to solve the problems with the help of my friends (Ich versuche, mit Freunden meine Probleme gemeinsam zu lösen)
0.80 0.57
Internal coping (Internale Bewältungsstrategien)
6 I think about the problem and try to find different solutions (Ich denke über das Problem nach und spiele verschiedene Lösungsmöglichkeiten in Gedanke durch)
0.77 0.59
Withdrawal (Problemmeidendes Verhalten) 7 I let out my anger or desperation by shouting, crying, banging doors, and so on (Ich mache meinem Ärger und meiner Ratlosigkeit “Luft” durch Schreien, Heulen, Türenknallen, etc.)
0.76 0.53

542 S. Sveinbjornsdottir and E. B. Thorsteinsson Scand J Psychol 49 (2008)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
(mean age 16.9 years) (Ficková, 1998). Factor analysis wasperformed on the CSC-Y’s factors in combination with thestrategies of Kidcope using orthogonal rotation, and two factorswere extracted. However, much information is missing, such astranslation of the scales, the factor model, method of factorextraction, loadings of items on each of the factors, internalconsistency, and the correlation between factors – thereforeinterpretation of the results is difficult.
Limitations of the CSC-Y. First, PCA and orthogonal rotationof factors is questionable. The construction sample washomogeneous, predominantly white, and middle class. Itemswere derived from the literature only, to f it a priori iden-tified categories of coping. There were no items included inthe scale that addressed acting out or risky behavior, suchas fighting, hitting, and substance use. These usually areincluded in adolescent coping questionnaires. The interval fortest-retest was one week only. Secondly, inter-item correlation,cross-validation of factor structure, and confirmatory factoranalysis on an independent representative sample were notperformed.
(5) Adolescent Coping Scale (ACS; Frydenberg & Lewis, 1993)
The ACS was developed in stages (Frydenberg, 1989, 1991,1997; Frydenberg & Lewis, 1991; Frydenberg & Lewis, 1993),based on the transactional model of stress and coping (Lazarus& Folkman, 1984). The ACS consists of 79 coping items (plusone open-ended item) in 18 factors, measuring coping in relationto either specific (Specific Form) or general concerns (GeneralForm), see Table 7. Three second-order factors were identified:Solving the Problem, Reference to Others, and Non-ProductiveCoping, see Table 8. A short form of the scale including 18items was created out of the full scale (ACS Short Form). Itemswere derived from the literature, mainly from the Ways ofCoping Checklist (WOCC), developed by Folkman and Lazarus(Frydenberg, 1989), and also generated by 643 Year 11 (58.1%)and Year 12 (41.9%) students, 15 to 18 years old (Frydenberg& Lewis, 1993). Students surveyed for generation of copingresponses were derived from five co-educational, and two
single-sex schools, one for each of the sexes, in metropolitanMelbourne, Australia (44.4% females, 55.6% males). Socio-economic background was distributed through four groups offathers’ occupation: professional/administrative, white collar,blue collar, and unemployed (43.0% professional, 40.9% bluecollar). The majority of the students were born in Australia(72.8%). However, 31.3% of fathers were born in Australia and25% in Greece. The students responded to an open-ended questionon how they coped with a self-nominated major concern, anda total of 2,041 descriptions were generated. The number ofcoping responses was reduced to 156 distinct items, which weretested on 30 students, aged 12 to 15 years old, for comprehensionof content and language, and found satisfactory. The responseformat was a five-point Likert scale.
The 156 refined items were administered to 500 Year 7through Year 11 students in Melbourne, Australia; there was nofurther information on participants, factor model and rotation.A scree test indicated 9 factors including 96 items. The remaining60 items that failed to load on any factor were, nevertheless,factor analyzed separately, and five factors with eigenvaluesabove one were extracted, comprising 32 of those 60 items. Theauthors then scrutinized and refined the two lots of items, intotal 128 items (96 plus 32), which resulted in a 50-item ques-tionnaire. That questionnaire was then administered to 712 Year7 to Year 12 students from 44 secondary schools, and factoranalyzed, using orthogonal rotation; no further information onparticipants and factor model was provided. A scree plot revealed13 factors for those 50 items with internal consistency rangingfrom 0.34 to 0.80 when identified for specific concerns, andranging from 0.35 to 0.78 when identified for general concerns.For the Specific Form, 4 of the 13 factors had alpha valuesbelow 0.70; 2 had alpha values below 0.50. For the GeneralForm, 10 of 13 factors had alpha values below 0.70, and 4 factorshad alpha values below 0.50.
The final version of the ACS consists of 18 factors includingall the 50 items as explained above and an additional 29 itemsderived from the original pool of 156 items. How these factorswere derived is not known. No information was provided forfactor extraction methods, factor model, and methods forfurther refinement.
Table 6. CSC-Y factor structure, internal consistency, test-retest, and inter factor correlations
Factors Items ExampleInternal consistency Test-retest
Inter factor correlation
2 3 4
1. Assistance seeking (Assist) 4 I asked someone in my family for help with the problem
0.72 0.80 0.44* −0.32* –
2. Cognitive-behavioral problem solving (Probsol)
8 I thought about the problem and tried to figure out what I could do about it
0.81 0.80 −0.24* –
3. Cognitive avoidance (Cavoid) 11 I tried not thinking about the problem 0.80 0.81 0.37*4. Behavioral avoidance (Bavoid) 6 I stayed away from things that
reminded me about the problem0.70 0.73
Note: – = information not available.* p < 0.001.
Scand J Psychol 49 (2008) Review of adolescent coping scales 543
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
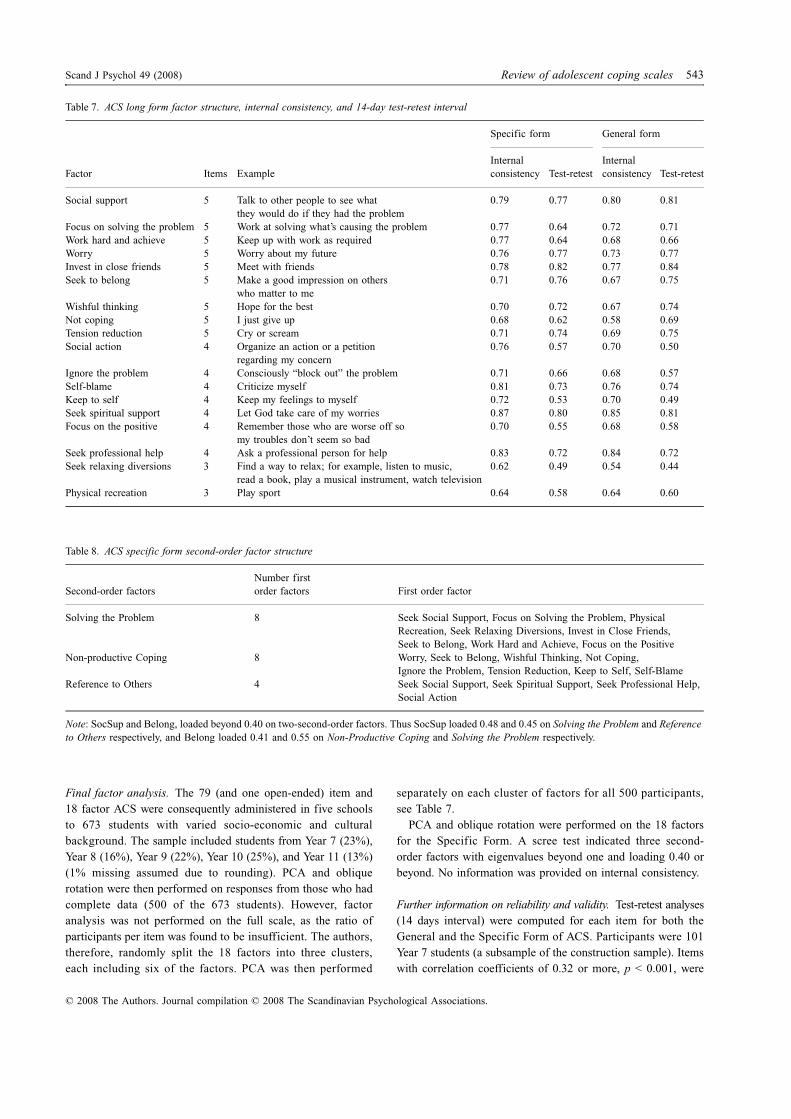
Final factor analysis. The 79 (and one open-ended) item and18 factor ACS were consequently administered in five schoolsto 673 students with varied socio-economic and culturalbackground. The sample included students from Year 7 (23%),Year 8 (16%), Year 9 (22%), Year 10 (25%), and Year 11 (13%)(1% missing assumed due to rounding). PCA and obliquerotation were then performed on responses from those who hadcomplete data (500 of the 673 students). However, factoranalysis was not performed on the full scale, as the ratio ofparticipants per item was found to be insufficient. The authors,therefore, randomly split the 18 factors into three clusters,each including six of the factors. PCA was then performed
separately on each cluster of factors for all 500 participants,see Table 7.
PCA and oblique rotation were performed on the 18 factorsfor the Specific Form. A scree test indicated three second-order factors with eigenvalues beyond one and loading 0.40 orbeyond. No information was provided on internal consistency.
Further information on reliability and validity. Test-retest analyses(14 days interval) were computed for each item for both theGeneral and the Specific Form of ACS. Participants were 101Year 7 students (a subsample of the construction sample). Itemswith correlation coefficients of 0.32 or more, p < 0.001, were
Table 7. ACS long form factor structure, internal consistency, and 14-day test-retest interval
Factor Items Example
Specific form General form
Internal consistency Test-retest
Internal consistency Test-retest
Social support 5 Talk to other people to see what they would do if they had the problem
0.79 0.77 0.80 0.81
Focus on solving the problem 5 Work at solving what’s causing the problem 0.77 0.64 0.72 0.71Work hard and achieve 5 Keep up with work as required 0.77 0.64 0.68 0.66Worry 5 Worry about my future 0.76 0.77 0.73 0.77Invest in close friends 5 Meet with friends 0.78 0.82 0.77 0.84Seek to belong 5 Make a good impression on others
who matter to me0.71 0.76 0.67 0.75
Wishful thinking 5 Hope for the best 0.70 0.72 0.67 0.74Not coping 5 I just give up 0.68 0.62 0.58 0.69Tension reduction 5 Cry or scream 0.71 0.74 0.69 0.75Social action 4 Organize an action or a petition
regarding my concern0.76 0.57 0.70 0.50
Ignore the problem 4 Consciously “block out” the problem 0.71 0.66 0.68 0.57Self-blame 4 Criticize myself 0.81 0.73 0.76 0.74Keep to self 4 Keep my feelings to myself 0.72 0.53 0.70 0.49Seek spiritual support 4 Let God take care of my worries 0.87 0.80 0.85 0.81Focus on the positive 4 Remember those who are worse off so
my troubles don’t seem so bad0.70 0.55 0.68 0.58
Seek professional help 4 Ask a professional person for help 0.83 0.72 0.84 0.72Seek relaxing diversions 3 Find a way to relax; for example, listen to music,
read a book, play a musical instrument, watch television0.62 0.49 0.54 0.44
Physical recreation 3 Play sport 0.64 0.58 0.64 0.60
Table 8. ACS specific form second-order factor structure
Second-order factorsNumber first order factors First order factor
Solving the Problem 8 Seek Social Support, Focus on Solving the Problem, Physical Recreation, Seek Relaxing Diversions, Invest in Close Friends, Seek to Belong, Work Hard and Achieve, Focus on the Positive
Non-productive Coping 8 Worry, Seek to Belong, Wishful Thinking, Not Coping, Ignore the Problem, Tension Reduction, Keep to Self, Self-Blame
Reference to Others 4 Seek Social Support, Seek Spiritual Support, Seek Professional Help, Social Action
Note: SocSup and Belong, loaded beyond 0.40 on two-second-order factors. Thus SocSup loaded 0.48 and 0.45 on Solving the Problem and Reference to Others respectively, and Belong loaded 0.41 and 0.55 on Non-Productive Coping and Solving the Problem respectively.

544 S. Sveinbjornsdottir and E. B. Thorsteinsson Scand J Psychol 49 (2008)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
considered reliable. For the General Form, eleven items failedto meet the criterion and the correlation ranged from 0.20 to 0.86(M = 0.48). For the Specific Form, seven items failed, andthe correlation ranged from 0.21 to 0.79 (M = 0.49). Test-retestcoefficients, as calculated for each factor, ranged from 0.44 to0.84 for the General Form (M = 0.68), and 8 of the 18 factorshad correlation coefficients below 0.70. For the Specific Formthe correlation ranged from 0.49 to 0.82 (M = 0.64), and 9 ofthe 18 factors had correlation coefficients below 0.70.
A Spanish version of ACS Long Form, where 800 13–15 yearold secondary school students from middle-class families inBueno Aires, Argentina, participated, did not replicate 18 ACSfactors successfully (Richaud de Minzi, 2003). Instead, throughseveral analyses, using FA and oblique rotation, 11 factorsemerged, including 47 of the 79 items from the ACS, droppingalmost half of the original coping items and fusing some of theoriginal coping factors.
Limitations of the ACS, Specific Form, and General Form. First,information regarding the scale’s development is insufficient forsome of the studies reported, such as on (a) participants’ back-ground, (b) choices of statistical methods (e.g., the rationale for18 primary factors), and (c) outcome (e.g., internal consistency ofsecond-order factors). Furthermore, reports on procedures arefrequently unclear, such as on how the number of factors wasderived and why information that could have led to furtherrefinement of the scale sometimes was ignored, as for instancewhen clearly imperfect items and factors of low internal relia-bility were included without further item refinement. Secondly,some questionable methods were chosen, such as: (a) PCA and(b) dividing items into three clusters and then factor analyzingeach cluster separately. Thus, two-thirds of the items wereexcluded when factors were explored, and consequently there isno information on how the excluded items may have affectedthe outcome for each cluster. Particularly, since coping factorsare believed to be interrelated, this method is unsatisfactory.Thirdly, some reported properties of the scale are poor. Forinstance: (a) two factors had fewer than four items each; (b)internal consistency was below 0.70 for 9 of 18 factors, GeneralForm, and the same applied for three of the factors for theSpecific Form; (c) test-retest reliability for a number of factorson both the Specific and the General Form was below 0.70; and(d) the ACS factor structure failed to replicate. Finally, someimportant analyses were not performed: (a) factor analysisincluding all items; (b) inter-item correlation, and (c) correlationwith related and unrelated scales. Psychometric limitations ofthe ACS are major and the scale is long (80 items).
(6) Coping Responses Inventory, Youth Form (CRI-Y; Moos, 1993)
The CRI-Y (Ebata & Moos, 1991) is based on the theory oftransactional model of stress and coping (Lazarus & Folkman,1984), and two second-order factors of coping are included intothe theoretical framework: (a) the focus such as problem-focused
versus emotion-focus, or approach versus avoidance, and, (b)the method – that is behavioral or cognitive (Compas, 1987;Compas, Malcarne & Fondacaro, 1988; Lazarus & Folkman, 1984).
Domains were identified through literature on coping, anditems developed to fit both focus and method. Items werederived in numerous ways: (a) reviewing descriptions of adoles-cents coping with life crisis and transitions; (b) looking intohow adolescents cope with serious illness and hospitalization;(c) interviewing adolescents; (d) examining concepts ofadolescent coping in the literature; and (d) adapting items fromthe CRI-adult scale. Next, 40 pilot interviews were conductedwith young people using about 100 coping items in ten potentialcoping factors. The group that was interviewed included bothsexes and healthy youth and youth with problems (no furtherinformation). This pilot study resulted in a 72 refined itemsquestionnaire, adapted to the reading level of Grade 6 students.
Factor analysis to identify underlying constructs or factorswas not conducted. The 72 items were administered to aconstruction sample of 315 adolescents, 168 females (meanage 15.3), and 147 males (mean age 15.2). Of these, 163 werehealthy (91 females and 72 males), 49 were depressed (30females and 19 males), 58 had conduct disorder (21 femalesand 37 males), and 45 had rheumatic disease (26 females and19 males). Part of the healthy group of the sample (n = 78) weresiblings of those included in the sample that had depression,conduct disorder, or rheumatic disease. Participants were mostlyCaucasians (70%). Parents were reported as “moderately”educated, and of various socio-economic backgrounds. Theanswering format was a four-point Likert scale. A revised formof the CRI-Y was administered in a 12 to 15 month follow-up,including 254 of the original 315 participants. In addition, 51youths with rheumatic disease and 34 of their siblings par-ticipated in this follow-up; hence the second constructionsample included 400 participants (221 females, 179 males).
Criteria for revision of the CRI-Y were: (a) good content andface validity for each item on the factor to which it belonged;(b) varied response distribution for each item; (c) at least amoderate level of internal consistency for each factor; and (d)minimized overlap between factors and combining of highlyinter-correlated factors. These criteria led to an eight factorsolution instead of the original ten factor solution, each factorincluding six items. Internal consistency ranged from 0.55–0.72for males and 0.59–0.72 for females, see Table 9.
Further information on reliability and validity. Test-retest correla-tions (12 to 15 months interval) were calculated for 254 adolescents,as the scale was implemented for the second time for theconstruction sample. The average correlation between occasionsfor the eight factors was r = 0.34 for females and r = 0.29 formales. Correlations between factors of r = ≥ 0.40 were numerousfor both sexes, the highest between “Logical Analysis” and“Problem Solving”, r = 0.61.
Correlations between the CRI-Y and depression, anxiety,alcohol and drug use, behavior problems, and self-confidencewere calculated using the same sample. Information on measures

Scand J Psychol 49 (2008) Review of adolescent coping scales 545
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
is limited – some are based on existing scales, others areself-rating questions prepared for the occasion. However, 45of a total of 48 correlations were low to moderate (r ≤ 0.30),indicating conceptual differences of measurements. The remainingcorrelations which indicated conceptual relationships were betweenDepression and Cognitive Avoidance (r = 0.36), Depression andEmotional Discharge (r = −0.34), and Alcohol and Drug Useand Emotional Discharge (r = 0.34).
Three independent cross-validation studies on the CRI-Yfailed to replicate the factor structure. Forns, Amador, Kirchner,Gómez and Muro (2005) tested the 8 factors on 1,401 adoles-cents (12–16 years) in Barcelona (FA, oblique rotation). Internalconsistency for all factors was below 0.70 (ranging between0.40 and 0.63, six of eight factors below 0.60). When testingfor higher dimensions, the distinction between cognitive andbehavioral coping was not supported. A distinction betweenapproach and avoidance coping was partially supported. Inthe other two validation studies the researchers, through a posthoc approach, created different scales on their own data basedon the original 48 CRI-Y items (Eyles & Bates, 2005; Griffith,Dubow & Ippolito, 2000).
Limitations of the CRI-Y. First, the criteria for selection of theconstruction sample is unclear and consequently, which popu-lation it is meant to represent. Information is missing on itemselection and on participants used in the development of theCRI-Y. Secondly, questionable methods were employed. Thefactor structure was theoretically derived, hypothetical, and nottested statistically. Furthermore, high correlations betweenseveral factors indicate a different factor structure and that somefactors should possibly be combined. Thirdly, some reportedpsychometric properties of the scale are not acceptable: (a)internal consistency of one factor was below 0.60; (b) low
test-retest reliability (around 0.30), but not easily interpretedsince the interval between tests was far beyond upper limits(roughly one year); and (c) the eight coping factors of CRI-Yfailed to replicate across samples. Finally, analyses such as (a)inter-item correlation, and (b) correlation with a related testwere not performed.
DISCUSSION
The aim of this study was to examine the design and constructionof adolescent coping scales and their psychometric propertiesin relation to best classical test-theoretical practice. Lack ofreport of important information as well as reporting of poorEFA choices, and therefore obscured outcomes, have frequentlybeen registered in psychological research (Conway & Huffcutt,2003; Fabrigar et al., 1999; Ford et al., 1986), and we presumeda similar outcome in the present review of adolescent copingscales. That, we assumed, might to some extent explain semanticinconsistencies and confusion within the research field ofcoping. We argued that meager psychometric quality of existingcoping scales developed through classical test-theory and EFAand imprecise statistical choices throughout the development ofthe scales are intertwined.
Six self-rating adolescent coping scales for general stressorsand daily hassles where coping strategies were clustered in factorswere reviewed. The scales were examined in relation to tendetailed test-theoretical criteria concerning reliability and evidenceof validity and the step-wise selection of statistical choiceswhen implementing factor analysis during scale development.Similar to earlier reports on EFA practices in psychologicalresearch, we observed omission of information for all thereviewed scales which limited our review. Furthermore, similarto previous findings on EFA practices, the information provided
Table 9. CRI-Y factor structure and internal consistency
Higher and first order factors Items Example
Internal consistency
Females (n = 221) Males (n = 179)
Approach coping responsesLogical Analysis 6 Did you think of different ways
to deal with the problem?0.68 0.69
Positive Reappraisal 6 Did you tell yourself things to make yourself feel better?
0.79 0.69
Seeking Guidance and Support 6 Did you talk with a parent or other family member about the problem?
0.69 0.72
Problem Solving 6 Did you decide on one way to deal with the problem and do it?
0.71 0.68
Avoidance responsesCognitive Avoidance 6 Did you try to forget the whole thing? 0.72 0.71Acceptance or Resignation 6 Did you feel that time would make a
difference – that the only thing to do was wait?0.59 0.55
Seeking Alternative Rewards 6 Did you get involved in new activities? 0.69 0.71Emotional Discharge 6 Did you take it out on other people
when you felt angry or sad?0.61 0.72

546 S. Sveinbjornsdottir and E. B. Thorsteinsson Scand J Psychol 49 (2008)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
by developers of the reviewed adolescent coping scales revealedpoor psychometric properties for each scale on numerous criteriathroughout their development. The shortcomings concernedseveral issues of psychometric importance and included: (a)poor choices of statistical (EFA) procedures (e.g., initial itemselection, model of factor analysis, and factor rotation); (b)insufficient statistical properties or values as compared withaccepted criteria (e.g., item loadings and internal reliability offactors, representativeness of samples); and (c) lack of importantreliability and or validity analyses (e.g., inter-item correlation,test-retest, cross-validation or confirmatory analysis).
None of the six scales was developed through the preferableFA. Rather, five were developed through PCA, and one scalewas hypothetical, based on a priori theory. Oblique rotation wasused for two of the five scales developed through EFA as persuggested best-practice allowing statistical analysis of second-order factors or dimensions and orthogonal rotation for theremaining three. None of the six scales was replicated acrosssamples. Instead, as with Steger’s (2006) notification of posthoc studies and diverse outcomes of the Ways of Coping Scaleacross samples, the outcomes for all replication studies of thereviewed adolescent coping scales revealed different numbersof coping items (strategies), factor structure, and dimensions ofcoping as compared with the original scales. These combinedshortcomings cast doubt on content and construct validity of thereviewed scales and leave both researchers and clinicians unableto interpret and rely on scale-scores and to compare researchoutcomes.
Imprecise psychometric procedures that are employed duringscale development are likely to obscure the outcome. Therefore,awareness of adverse consequences for reliability and validityof any construct, caused by poor test-theoretical practices, isneeded, and only through detailed information and explanationof the rationale for statistical choices is it possible (a) to examinehow closely a researcher follows best practice for test develop-ment, and (b) to repeat or replicate a study. The reason is notobvious why none of the reviewed adolescent coping scales wasdeveloped according to best-practice. Ford et al. (1986), Fabrigaret al. (1999), and Conway and Huffcutt (2003) have offeredsome possible explanations as to why researchers do not employhigh quality EFA procedures. One is that education and trainingin EFA procedures might be insufficient; another that traditionprefers PCA with orthogonal rotation; and finally that defaultoptions in statistical software lead researchers to use PCA andorthogonal rotation without questioning their choice. Theseexplanations, one or all, may well be true for the developmentof the reviewed adolescent coping scales. The EFA procedureis complex and requires that rationale for each decision mustbe understood and explained and that each step is carefullyand deliberately chosen to secure an outcome as best possible.Omission of crucial information, as observed in the presentreview, supports the presumption that researchers do not seemto find detailed information and careful choice of each statisticalstep in the procedure of scale development, including the EFA,all that important.
Although an agreement on the importance of individual copingfor well-being and health is reached, and research, includingdevelopment of coping scales, constantly adds information tothe area, there is still empirical research to be pursued. The presentreview of development of adolescent coping scales supports ourhypothesis that semantic confusion within the research fieldof coping and poor psychometric properties of scales are inter-twined. Given the importance of individual coping as eitherprotective or risk factors in relation to health and well-being, wesuggest that further research on adolescent coping with generalconcerns, in search for both latent primary factors as well asdimensions of coping, rely on precise methodology, includinghigh quality EFA procedures.
This project was supported by Rannís, http://www.rannis.is/
REFERENCES
Ayers, T. S., Sandler, I. N. & Twohey, J. L. (1998). Conceptualizationand measurement of coping in children and adolescents. In T. H.Ollendick & R. J. Prinz (Eds.), Advances in clinical child psychology(Vol. 20, pp. 243–301). New York: Plenum Press.
Benson, J. & Hagtvet, K. A. (1996). The interplay among design, dataanalysis, and theory in the measurement of coping. In M. Zeidner& N. S. Endler (Eds.), Handbook of coping: Theory, research,applications (pp. 83–106). New York: John Wiley and Sons.
Billings, A. G. & Moos, R. H. (1981). The role of coping responses andsocial resources in attenuating the stress of life events. Journal ofBehavioral Medicine, 4, 139–157.
Billings, A. G. & Moos, R. H. (1984). Coping, stress, and socialresources among adults with unipolar depression. Journal of Per-sonality and Social Psychology, 46, 877–891.
Boekaerts, M. (1996). Coping with stress in childhood and adolescence.In M. Zeidner & N. S. Endler (Eds.), Handbook of coping: Theory,research, applications (pp. 452–484). New York: John Wiley andSons.
Briggs, S. & Cheek, J. (1986). The role of factor analysis in the develop-ment and evaluation of personality scales. Journal of Personality,54, 106–148.
Brodzinsky, D., Elias, M., Steiger, C., Simon, J. & Gill, M. (1992).Coping Scale for Children and Youth: Scale development andvalidation. Journal of Applied Developmental Psychology, 13, 195–214.
Burnett, P. C. & Fanshawe, J. P. (1996). Measuring adolescent copingstrategies: Revalidation of the adolescent coping orientation forproblem experiences. The Australian Educational and DevelopmentalPsychologist, 13, 40–53.
Burr, W. (1982). Families under stress. In H. I. McCubbin, A. E. Cauble& J. M. Patterson (Eds.), Family stress, coping, and social support(pp. 5–25). Springfield, IL: Charles C. Thomas Publisher.
Carver, C. S., Scheier, M. F. & Weintraub, J. K. (1989). Assessingcoping strategies: A theoretically based approach. Journal ofPersonality and Social Psychology, 56, 267–283.
Causey, D. & Dubow, E. (1992). Development of a self-report copingmeasure for elementary school children. Journal of Clinical ChildPsychology, 21, 47–59.
Child, D. (1990). The essentials of factor analysis (2nd edn). London:Cassell Educational Ltd.
Compas, B. E. (1987). Coping with stress during childhood and adoles-cence. Psychological Bulletin, 101, 393–403.
Compas, B. E., Connor-Smith, J. K., Saltzman, H., Thomsen, A. H. &Wadsworth, M. (1999). Getting specific about coping: Effortful and
Scand J Psychol 49 (2008) Review of adolescent coping scales 547
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
involuntary responses to stress in development. In M. Lewis & D.Ramsey (Eds.), Soothing and stress (pp. 229–256). Mahawah, NJ:Lawrence Erlbaum Associates.
Compas, B. E., Connor-Smith, J. K., Saltzman, H., Thomsen, A. H. &Wadsworth, M. E. (2001). Coping with stress during childhood andadolescence: Problems, progress, and potential in theory andresearch. Psychological Bulletin, 127, 87–127.
Compas, B. E., Malcarne, V. & Fondacaro, K. (1988). Coping withstressful events in older children and young adolescents. Journal ofConsulting and Clinical Psychology, 56, 405–411.
Connor-Smith, J. K., Compas, B. E., Wadsworth, M. E., Thomsen, A.H. & Saltzman, H. (2000). Responses to stress in adolescence:Measurement of coping and involuntary stress responses. Journal ofConsulting and Clinical Psychology, 68, 976–992.
Conway, J. M. & Huffcutt, A. I. (2003). A review and evaluation ofexploratory factor analysis practices in organizational research.Organizational Research Methods, 6, 147–168.
Costello, A. B. & Osborne, J. W. (2005). Best practices in exploratoryfactor analysis: Four recommendations for getting the mostfrom your analysis. Practical Assessment, Research & Evaluation,10, 1–9.
DeVellis, R. F. (1991). Scale development: Theory and applications.Newbury Park, CA: Sage.
Dise-Lewis, J. E. (1988). The life events and coping inventory: Anassessment of stress in children. Psychosomatic Medicine, 50,484–499.
Ebata, A. T. & Moos, R. H. (1991). Coping and adjustment in distressedand healthy adolescents. Journal of Applied Developmental Psy-chology, 12, 33–54.
Ebata, A. T. & Moos, R. H. (1994). Personal, situational, and contextualcorrelates of coping in adolescence. Journal of Research on Adoles-cence, 4, 99–125.
Endler, N. S. & Parker, J. D. A. (1990). Multidimensional assessmentof coping: A critical evaluation. Journal of Personality and SocialPsychology, 58, 844–854.
Eyles, D. J. & Bates, G. W. (2005). Development of a shortened formof the Coping Responses Inventory-Youth with an Australiansample. North American Journal of Psychology, 7, 161–170.
Fabrigar, L., Wegener, D., MacCallum, R. & Strahn, E. (1999). Evalu-ating the use of exploratory factor analysis in psychologicalresearch. Psychological Methods, 4, 272–299.
Fanshawe, J. P. & Burnett, P. C. (1991). Assessing school relatedstressors and coping mechanisms in adolescents. British Journal ofEducational Psychology, 61, 92–98.
Ficková, E. (1998). Coping scales for children and adolescents: Psycho-metric relationships. Studia Psychologica, 40, 291–296.
Folkman, S. & Lazarus, R. S. (1980). An analysis of coping in amiddle-aged community sample. Journal of Health and SocialBehavior, 21, 219–239.
Folkman, S. & Lazarus, R. S. (1985). If it changes it must be a process:Study of emotion and coping during three stages of a collegeexamination. Journal of Personality and Social Psychology, 48,150–170.
Folkman, S. & Lazarus, R. S. (1988). Manual for the ways of copingquestionnaire (Research edition). Palo Alto, CA: ConsultingPsychologists Press.
Ford, J. K., MacCallum, R. C. & Tait, M. (1986). The application ofexploratory factor analysis in applied psychology: A critical reviewand analysis. Personnel Psychology, 39, 291–314.
Forns, M., Amador, J. A., Kirchner, T., Gómez, J. & Muro, P. (2005).Psychometric properties of the Spanish version of the MoosCoping Response Inventory for Youth. Psychological Reports, 97,777–789.
Frydenberg, E. (1989). The concerns and coping strategies of youth: Astudy of Australian adolescents. Unpublished Doctoral dissertation,La Trobe University, Melbourne.
Frydenberg, E. (1991). Adolescent coping styles and strategies: Is therefunctional and dysfunctional coping. Australian Guidance andCounselling Association, 1, 1–8.
Frydenberg, E. (1997). Adolescent coping: Theoretical and researchperspectives. London: Routledge.
Frydenberg, E. & Lewis, R. (1991). Adolescent coping in the Australiancontext. Australian Educational Researcher, 18, 65–82.
Frydenberg, E. & Lewis, R. (1993). Adolescent Coping Scale: Admin-istrator’s manual. Melbourne, Australia: ACER (The AustralianCouncil for Educational Research Ltd).
Gorsuch, R. (1983). Factor analysis (2nd edn). Hillsdale, NJ: LawrenceErlbaum Associates.
Graue, M., Hanestad, B. R., Wentzel-Larsen, T., Sövik, O. & Bru, E.(2004). The coping styles of adolescents with Type 1 diabetes areassociated with degree of metabolic control. Diabetes Care, 27,1313–1317.
Griffith, A. G., Dubow, E. F. & Ippolito, M. F. (2000). Developmentaland cross-situational differences in adolescents’ coping strategiesJournal of Youth and Adolescence, 29, 183–204.
Halvarsson, K., Lunner, K. & Sjödin, P. (2001). Development of aSwedish version of the Adolescent Coping Orientation for ProblemExperiences (A-Cope). Scandinavian Journal of Psychology, 42,383–388.
Haynes, S. N., Richard, D. C. S. & Kubany, E. S. (1995). Contentvalidity in psychological assessment: A functional approach toconcepts and methods. Psychological Assessment, 7, 238–247.
Hayton, J. C., Allen, D. G. & Scarpello, V. (2004). Factor retentiondecisions in exploratory factor analysis: A tutorial on parallelanalysis. Organizational Research Methods, 7, 191–205.
Holmes, D. & Rahe, R. (1967). The social readjustment rating scale.Journal of Psychosomatic Research, 11, 213–218.
Jorgensen, S. R. & Dusek, J. B. (1990). Adolescent adjustment andcoping strategies. Journal of Personality, 58, 503–513.
Kavsek, M. & Seiffge-Krenke, I. (1996). The differentiation of copingtraits in adolescence. International Journal of Behavioral Development,19, 651–668.
Kline, P. (1986). A handbook of test construction: Introduction topsychometric design. London: Methuen.
Kline, P. (1993). The handbook of psychological testing. London:Routledge.
Kline, P. (1994). An easy guide to factor analysis. London: Routledge.Kowalsky, K. C. & Crocker, P. R. E. (2001). Development and validation
of the Coping Function Questionnaire for adolescents in sport.Journal of Sport & Exercise Psychology, 23, 136–155.
Kristensson, P. & Öhlund, L. S. (2005). Swedish upper secondaryschool pupils’ sense of coherence, coping resources and aggressive-ness in relation to educational track and performance. ScandinavianJournal of Caring Sciences, 19, 77–84.
Kuo, B. C. H., Roysircar, G. & Newby-Clark, I. R. (2006). Developmentof the Cross-Cultural Coping Scale: Collective, avoidance, andengagement coping. Measurement and Evaluation in Counselingand Development, 39, 161–181.
Lazarus, R. S. (1993). Coping theory and research: Past, present, andfuture. Psychosomatic Medicine, 55, 234–247.
Lazarus, R. S. & Folkman, S. (1984). Stress, appraisal and coping. NewYork: Springer.
MacCallum, R. C., Widaman, K. F., Zhang, S. & Hong, S. (1999).Sample size in factor analysis. Psychological Methods, 4, 84–99.
Masten, A. S., Best, K. M. & Garmezy, N. (1990). Resilience anddevelopment: Contributions from the study of children whoovercame adversity. Development and Psychopathology, 2, 425–444.
McCrae, R. R. (1984). Situational determinants of coping responses:Loss, threat, and challenge. Journal of Personality and SocialPsychology, 46, 919–928.

548 S. Sveinbjornsdottir and E. B. Thorsteinsson Scand J Psychol 49 (2008)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
McCrae, R. R. & Costa, P. T. J. (1986). Personality, coping, and copingeffectiveness in adult sample. Journal of Personality, 52, 385–405.
McCubbin, H. I. & Patterson, J. M. (1981). Family stress and adaptationto crisis. A double ABCX model of family behavior. In D. Olson &B. Miller (Eds.), Family studies review yearbook (pp. 87–106). BeverlyHills, CA: Sage Publications.
McCubbin, H. I. & Patterson, J. M. (1982). Family adaptation to crisis.In H. I. McCubbin, A. E. Cauble & J. M. Patterson (Eds.), Familystress, coping, and social support (pp. 26–47). Springfield, IL:Charles Thomas Publisher.
McCubbin, H. I. & Patterson, J. M. (1983). The family stress process:The Double ABCX Model of Adjustment and Adaptation. In H. I.McCubbin, M. Sussman & J. M. Patterson (Eds.), Social stress andthe family: Advances and development in family (pp. 7–37). NewYork: Haworth Press.
McCubbin, H. I. & Patterson, J. M. (1986). Adolescent stress, copingand adaptation: A normative family perspective. In G. Leigh & G.Peterson (Eds.), Adolescents in a family context (pp. 256–276).Cincinnati, OH: South-Western Publishing Co.
Moos, R. M. (1993). Coping response inventory: Youth form: Profes-sional manual. Odessa, FL: Psychological Assessment Resources.
Nunnally, J. (1978). Psychometric theory. New York: McGraw Hill.Parkes, K. R. (1986). Coping in stressful episodes: The role of individual
differences, environmental factors, and situational characteristics.Journal of Personality and Social Psychology, 51, 1277–1292.
Patterson, J. M. & McCubbin, H. I. (1987). Adolescent coping styleand behaviors: Conceptualization and measurement. Journal ofAdolescence, 10, 163–186.
Pearlin, L. I. & Schooler, C. (1978). The structure of coping. Journalof Health and Social Behavior, 19, 2–21.
Plancherel, B. & Bolognini, M. (1995). Coping and mental health inearly adolescence. Journal of Adolescence, 18, 459–474.
Reid, G. J., Dubow, E. F. & Carey, T. (1995). Developmental andsituational differences in coping among children and adolescentswith diabetes. Journal of Applied Developmental Psychology, 16,529–554.
Reid, G. J., Dubow, E. F., Carey, T. C. & Dura, J. R. (1994). Contributionof coping to medical adjustment and treatment responsibility amongchildren and adolescents with diabetes. Journal of Developmentaland Behavioral Pediatrics, 15, 327–335.
Richaud de Minzi, M. C. (2003). Coping assessment in adolescents.Adolescence, 38, 321–330.
Rijavec, M. & Brdar, I. (1997). Coping with school failure: Developmentof the school failure coping scale. European Journal of Psychologyof Education, XII, 37–49.
Rutter, M. (Ed.) (1995). Psychosocial disturbances in young people:Challenges for prevention. New York: Cambridge University Press.
Schwarzer, R. & Schwarzer, C. (1996). A critical survey of copinginstruments. In M. Zeidner & N. S. Endler (Eds.), Handbook ofcoping: Theory, research, applications (pp. 107–132). New York:John Wiley and Sons.
Seiffge-Krenke, I. (1989). Bewältigung alltäglicher Problemsituationen:Ein Coping Fragebogen für Jugendliche. Zeitschrift für Differentielleund Diagnostische Psychologie, 4, 201–220.
Seiffge-Krenke, I. (1992). Coping behavior of Finnish adolescents:Remarks on a cross-cultural comparison. Scandinavian Journal ofPsychology, 33, 301–314.
Seiffge-Krenke, I. (1998). Adolescents’ health: A developmentalperspective. Mahwah, NJ: Lawrence Erlbaum Associates.
Seiffge-Krenke, I. & Klessinger, N. (2000). Long-term effects of avoidant
coping on adolescents’ depressive symptoms. Journal of Youth andAdolescence, 29, 617–630.
Seiffge-Krenke, I. & Shulman, S. (1990). Coping style in adolescence:A cross-cultural study. Journal of Cross-Cultural Psychology, 21,351–377.
Seiffge-Krenke, I. & Shulman, S. (1993). Stress, coping and relation-ships in adolescence. In S. Jackson & Rodriguez-Tomé (Eds.),Adolescence and its social world (pp. 169–196). East Sussex:Lawrence Erlbaum Associates.
Skinner, E. A., Edge, K., Altman, J. & Sherwood, H. (2003). Searchingfor the structure of coping: A review and critique of categorysystems for classifying ways of coping. Psychological Bulletin, 129,216–269.
Smith, D. J. & Rutter, M. (1995). Introduction. In M. Rutter & D. J.Smith (Eds.), Psychosocial disorders in young people: Time trendsand their causes (pp. 1–6). Chichester, UK: John Wiley & Sons.
Smith, R. E., Smoll, F. L. & Ptacek, J. T. (1990). Conjunctive moderatorvariables in vulnerability and resiliency research: Life stress, socialsupport and coping skills, and adolescent sport injuries. Journal ofPersonality and Social Psychology, 58, 360–370.
Spirito, A., Stark, L. J. & Williams, C. (1988). Development of a briefcoping checklist for use with pediatric populations. Journal ofPediatric Psychology, 13, 555–574.
Steger, M. F. (2006). An illustration of issues in factor extraction andidentification of dimensionality in psychological assessment data.Journal of Personality Assessment, 86, 263–272.
Steiner, H., Erickson, S. J., Hernandez, N. L. & Pavelski, R. (2002).Coping styles as correlates of health in high school students.Journal of Adolescent Health, 30, 326–335.
Stone, A. A. & Neale, J. M. (1984). New measure of daily coping:Development and preliminary results. Journal of Personality andSocial Psychology, 46, 892–906.
Sveinbjornsdottir, S. (2001). The assessment of adolescent coping:Development of a new measure. Unpublished Ph.D., La TrobeUniversity, Melbourne.
Tabachnick, B. G. & Fidell, L. S. (1989). Using multivariate statistics(2nd edn). New York: Harper Collins Publishers.
Tobin, D. L., Holroyd, K. A., Reynolds, R. V. & Wigal, J. K. (1989).The hierarchical factor structure of the coping strategies inventory.Cognitive Therapy and Research, 13, 343–361.
Tolor, A. & Fehon, D. (1987). Coping with stress: A study of maleadolescents’ coping strategies as related to adjustment. Journal ofAdolescent Research, 2, 33–42.
Velicer, W. F. & Jackson, D. N. (1990). Component analysis versuscommon factor analysis: Some issues in selecting an appropriateprocedure. Multivariate Behavioral Research, 25, 1–28.
Watson, D. C., Willson, L. R. & Sinha, B. K. (1998). Assessing thedimensional structure of coping: A cross-cultural comparison.International Journal of Stress Management, 5, 77–81.
Whatley, S. L., Foreman, A. C. & Richards, S. (1998). The relationshipof coping style to dysphoria, anxiety, and anger. PsychologicalReports, 83, 783–791.
Widaman, K. F. (1993). Common factor analysis versus principalcomponent analysis: Differential bias in representing modelparameters? Multivariate Behavioural Research, 28, 263–311.
Zeidner, M. & Hammer, A. L. (1990). Life events and coping resourcesas predictors of stress symptoms in adolescents. Personality andIndividual Differences, 11, 693–703.
Received 3 October 2007, accepted 3 March 2008
Copyright © 2022 FDOKUMEN




















