
Overexpression of Interleukin-13 Receptor-α2 in Neuroendocrine Malignant Pheochromocytoma: A Novel...
19
Overexpression of Interleukin 13 Receptor 2 as a Novel Therapy for Malignant Pheochromocytoma Short title: IL-13 cytotoxin in pheochromocytoma Edwin W. Lai 1 *, Bharat H. Joshi 2 *, Lucia Martiniova 1 , Ritika Dogra 2 , Toshio Fujisawa 2 , Pamela Leland 2 , Ronald R. de Krijger 3 , Irina A. Lubensky 4 , Abdel G. Elkahloun 5 , John C. Morris 6 , Raj K. Puri 2 † and Karel Pacak 1 † *E.W.L. and B.H.J. contributed equally to this work. †R.K.P. and K.P. corresponding authors 1 Section on Medical Neuroendocrinology, Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, Bethesda, Maryland 20892, USA; 2 Tumor Vaccines and Biotechnology Branch, Division of Cellular and Gene Therapies, Center for Biologics Evaluation and Research, Food and Drug Administration, Bethesda, Maryland 20892, USA; 3 Department of Pathology, Josephine Nefkens Institute, Erasmus MC- University Medical Center, Rotterdam, The Netherlands; 4 Cancer Diagnosis Program, National Cancer Institute, Bethesda, MD 20892, USA; 5 National Human Genome Research Institute, Bethesda, MD, 20892, USA; 6 Metabolism Branch, Center for Cancer Research, National Cancer Institute, Bethesda, MD, 20892, USA. J Clin Endocrin Metab. First published ahead of print June 2, 2009 as doi:10.1210/jc.2009-0309 Copyright (C) 2009 by The Endocrine Society
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Overexpression of Interleukin-13 Receptor-α2 in Neuroendocrine Malignant Pheochromocytoma: A Novel...

Overexpression of Interleukin 13 Receptor �2 as a Novel Therapy for Malignant
Pheochromocytoma
Short title: IL-13 cytotoxin in pheochromocytoma
Edwin W. Lai1*, Bharat H. Joshi2*, Lucia Martiniova1, Ritika Dogra2, Toshio Fujisawa2, Pamela
Leland2, Ronald R. de Krijger3, Irina A. Lubensky4, Abdel G. Elkahloun5, John C. Morris6, Raj
K. Puri2† and Karel Pacak1†
*E.W.L. and B.H.J. contributed equally to this work.
†R.K.P. and K.P. corresponding authors
1Section on Medical Neuroendocrinology, Eunice Kennedy Shriver National Institute of Child
Health and Human Development, National Institutes of Health, Bethesda, Maryland 20892,
USA; 2Tumor Vaccines and Biotechnology Branch, Division of Cellular and Gene Therapies,
Center for Biologics Evaluation and Research, Food and Drug Administration, Bethesda,
Maryland 20892, USA; 3Department of Pathology, Josephine Nefkens Institute, Erasmus MC-
University Medical Center, Rotterdam, The Netherlands; 4Cancer Diagnosis Program, National
Cancer Institute, Bethesda, MD 20892, USA; 5National Human Genome Research Institute,
Bethesda, MD, 20892, USA; 6Metabolism Branch, Center for Cancer Research, National Cancer
Institute, Bethesda, MD, 20892, USA.
J Clin Endocrin Metab. First published ahead of print June 2, 2009 as doi:10.1210/jc.2009-0309
Copyright (C) 2009 by The Endocrine Society

2
Corresponding authors:
Karel Pacak, M.D., Ph.D., D.Sc.,
Section on Medical Neuroendocrinology
Reproductive and Adult Endocrinology Program, NICHD, NIH
Building 10, CRC, Room 1-3140, 10 Center Drive
Bethesda, Maryland 20892-1109
TEL: 1-301-402-4594, FAX: 1-301-402-0884,
E-mail: [email protected]
Raj K. Puri, M.D., Ph.D.
Division of Cellular and Gene Therapies
FDA, Center for Biologics Evaluation and Research
NIH Building 29B, Room 2NN20
29 Lincoln Drive
Bethesda, Maryland 20892-4555
TEL: 301-827-0471
FAX: 301-281-0449
E-mail: [email protected]
DISCLOSURE STATEMENT: The authors have no conflicts to disclose. “This is an un-copyedited author manuscript copyrighted by The Endocrine Society. This may not be duplicated or reproduced, other that for personal use or within the rule of “Fair Use of Copyrighted Materials” (section 107, Title 17, U.S. Code) without permission of the copyright owner, The Endocrine Society. From the time of acceptance following peer review, the full text of this manuscript is made freely available by The Endocrine Society at http://www.endojournals.org/. The final copy edited article can be found at http://www.endojournals.org/. The Endocrine Society disclaims any responsibility or liability for errors or omissions in this version of the manuscript or in any version derived from it by the National Institutes of Health or other parties. The citation of this article must include the following information: author(s), article title, journal title, year of publication, and DOI.”

3
Précis: Human and murine neuroendocrine pheochromocytoma tumors overexpress IL-13Rα2
chain, and IL-13PE based receptor directed anticancer approach may prove useful in treatment
for metastatic pheochromocytoma patients
Abstract: 235/250
Total word count: 1799/1800
Figure(s): 2 Table(s): 1, supplemental
Key words: immunotoxin, interleukin-13 receptor, pheochromocytoma, mouse model

4
ABSTRACT
Context. Pheochromocytomas and paragangliomas are rare catecholamine-secreting
neuroendocrine tumors arising from the adrenal medulla and sympathetic tissues. When
complete surgical resection is not an option, the treatment of pheochromocytoma is limited.
Objective. To identify and characterize overexpression of Interleukin-13 receptor-alpha-2 (IL-
13Rα2) gene expression in human and murine tumors, and to verify xenograft mouse
pheochromocytoma cell (MPC)-derived tumor’s response to a selective cytotoxin.
Design/Setting/Patients. Expression of IL-13Rα2 was evaluated in a panel of 25 human
pheochromocytoma clinical samples by RT-PCR and 8 MPC tumors by indirect immuno-
fluorescence assay (IFA) and RT-PCR.
Intervention. The function of IL-13Rα2 in these tumor cells were examined by evaluating
tumor sensitivity to a recombinant Interleukin-13-Pseudomonas exotoxin (IL-13PE).
Subcutaneous small and large MPC tumors in athymic nude mice (n=10) were treated
intratumorally with IL-13PE (100 μg/kg).
Main Outcome Measures. IC50 and tumor size.
Results. IL-13PE immunotoxin was highly cytotoxic to IL-13Rα2 overexpressing MPC cells
(IC50<2.5 ng/mL) in vitro. Furthermore, IL-13PE was highly cytotoxic to subcutaneous tumors.
Our results showed a statistically significant decrease in tumor size as early as 3 days after initial
treatment and further suppressed growth of MPC tumors. All tumors displayed a histological
evidence of necrosis in response to IL-13 immunotoxin without any adverse effects in host at this
dose.

5
Conclusions. Human and murine neuroendocrine pheochromocytoma overexpress the IL-13Rα2
chain, and an IL-13PE based receptor directed anticancer approach may prove useful in
treatment for metastatic pheochromocytoma patients.

6
INTRODUCTION
Despite advances in diagnosis and imaging, pheochromocytoma remains one of the tumors
where no cure exists when metastatic disease is present. The prognosis of benign and malignant
pheochromocytoma vastly differs. Benign tumors are generally amenable to complete surgical
resection and have a 10-year survival of up to 94% (1). Conversely, no curative treatment exists
for metastatic pheochromocytoma, and the 10-year survival rate is only 20% (1-3). Current
regimens for treating metastatic pheochromocytoma are limited to combination chemotherapy,
radioactive 131I-metaiodobenzylguanidine (131I-MIBG), local radiotherapy and more recently
radiofrequency ablation (3, 4). Therefore, novel therapeutic approaches for treating metastatic
malignant pheochromocytoma are urgently warranted.
Previously, we have demonstarted an overexpression of interleukin-13 receptor (IL-13R) in a
number of cancers. IL-13Rα2 is overexpressed in primary brain tumors, head and neck cancer,
renal cell carcinoma, ovarian carcinoma, and AIDS-related Kaposi sarcoma (5-7). Conversley,
little or no IL-13Rα2 is expressed in normal immune cells or tissues (8). IL-13 binds with
higher affinity to IL-13Rα2 compared to IL-13Rα1 chain. The IL-13R complex can be of three
different types and its structure varies in different cell types (9). IL-13 predominantly mediates
signaling through its heterodimer composed of the IL-4α and IL-13Rα1 chains and initiates
signalling events through JAK/STAT6 pathways (10-12). Recently, IL-13 has been shown to
mediate signaling through IL-13Rα2 chain in certain cell types (13). In this case, IL-13 signals
through the AP-1 pathway.
To target tumor cells overexpressing IL-13R, we have developed and produced an
immunotoxin, consisting of IL-13 and truncated Pseudomonas exotoxin A (IL-13PE). IL-13PE
produces IL-13R-specific cytotoxicity both in vitro and in vivo tumor models (8). The

7
mechanism of IL-13PE in receptor positive cells is extensively studied. Following endocytosis of
IL-13PE, the A chain translocates to the cytosol, cleaves ribosomal RNA, and thereby inhibits
protein synthesis and cells are killed (9, 10).
In this study, we demonstrate overexpression of IL-13Rα2 at the mRNA and protein levels in
animal and human pheochromocytoma tumor specimens. We also demonstrate that IL-13R
targeted cytotoxin IL-13PE is highly cytotoxic to pheochromocytoma tumors in vitro and in vivo
in a subcutaneous mouse pheochromocytoma cell (MPC) tumor model. Thus, IL-13Rα2 is a
novel target on pheochromocytoma that can be targeted by IL-13PE for cancer therapy.
8
MATERIALS AND METHODS
Recombinant Immunotoxin and Cell Lines
Recombinant IL-13PE was produced and purified as previously described (14). Mouse
pheochromocytoma cells (MPC 4/30/PRR), developed from NF1 knockout mice, were
generously provided by Dr. Arthur S. Tischler (15). PM-RCC is a IL-13Rα2 positive human
renal cell carcinoma and T98G is a IL-13Rα2 negative human glioma cell line (8, 10). Cells
were grown in appropriate medium as described previously (8, 10, 15).
Cell Viability Assay
The IC50 of IL-13PE against the above cell lines was determined by trypan blue dye exclusion.
Briefly, MPC, PM-RCC, and T98G were seeded at 5 x 106 cells in 25mm3 Corning Flasks
(Corning, NY) with increasing concentration of IL-13PE (0, 0.1, 1, 10, 100 and 1,000 ng/mL) at
37C for 24 h. The cells were incubated for an additional 4 days before viable cells were counted
by trypan blue dye exclusion technique and data expressed as percent positive cells.
Reverse Transcriptase-Polymerase Chain Reaction (RT-PCR)
Twenty-five human samples from patients evaluated and operated for pheochromocytoma were
collected at the National Institutes of Health (Bethesda, MD) and three normal human adrenal
tissues (Rotterdam, The Netherlands) after IRB approval. Pheochromocytoma was confirmed by
histology of surgically resected tumors. Adrenal medulla tissue was separated consisting of no
more than 50% cortex. RNA was extracted using TRIzol (Invitrogen, Carlsbad, CA) followed by
RNeasy Mini Kit (Qiagen, Valencia, CA). RT-PCR analysis was performed for IL-13Rα2 and β-
actin (internal control). The optimal conditions for human IL-13Rα2 RT-PCR and primers have
been published previously (16). The following primers were used for mouse IL-13R�2: 5�-
9
CGC-ATT-TGT-CAG-AGC-ATT-GT-3� (sense) and 5�-CCA-AGC-CCT-CAT-ACC-AGA-AA-
3� (antisense). All studies were done in triplicate for validation.
Histology and Immunohistochemistry
IFA for IL-13Rα2 and tyrosine hydroxylase (TH) was performed as previously described (5).
Biotin- streptavidin based IFA was used for red and green fluorescence and the sections were
viewed in a Nikon fluorescence microscope (200X).
Animal Studies
Six-to ten-week old female athymic nude mice (NCr-nu) were obtained from Taconic, Inc.
(Germantown, MD). Tumors were established by subcutaneous injection of MPC cells (5x106).
Mice were grouped by approximate tumor size (large >50mm3, and small <50mm3) prior to
treatment. Tumor size was calculated by measuring three diameters using a caliper multiplying
π/6 by height, length, and width and evaluated for statistical significance. Animals were treated
with 100 μg/kg IL-13PE or PBS intratumorally (IT) in three axes for three consecutive days and
were monitored for health and behavior for one week.
Statistical Analysis
The statistical significance of data was calculated by unpaired t-test.

10
RESULTS
Overexpression of IL-13R�2 in Human and Murine Pheochromocytoma
RNA microarray results were obtained from Brouwers, et. al. (17). 98 human
pheochromocytoma (from 90 patients) compared to normal human adrenal medulla polyA
reference and 20 MPC-derived tumors (10 subcutaneous & 10 liver metastasis) compared to
parental MPC (unpublished data) were examined for IL-13Rα2 mRNA expression. These results
showed increased levels of IL-13Rα2 expression compared to normal human adrenal medulla.
The expression ratio in benign tumors was median = 2.074 (IQR: 1.599, 3.504) compared to
malignant lesions median = 2.635 (IQR: 1.992, 3.236) (p=0.81). Mouse MPC-derived
subcutaneous tumors revealed a ratio of 2.10 (subcutaneous tumor compared to MPC) and mouse
MPC derived liver metastasis revealed a ratio of 2.06 compared to MPC. The ratio of liver
lesions compared to subcutaneous lesions was not significant (p=0.92). Ratios were calculated
based on the mean background subtracted intensities.
IL-13Rα2 expression was confirmed in mouse subcutaneous tumors (n=4) and mouse
liver tumors (n=4) (Fig. 1A) as well as twenty-five clinical samples of pheochromocytoma by
RT-PCR (Fig. 1B). Positive expression was observed in all tumors. Conversely, normal adrenal
medulla tissue did not reveal expression of IL-13Rα2 (Supplemental Table 1). Normal human
adrenal tissue immunostained for IL-13R�2 also confirmed absence or low expression of protein
(unpublished data).
Sensitivity of MPC Cell Line and Tumors to IL-13PE Immunotoxin
Both MPC cells (Fig. 1C) and in vivo tumors (Fig. 1D) demonstrated IL-13R�2
expression by IFA for plasma membrane as well as intracytoplasmic immunostaining. Biological
function of overexpressed IL-13R was evaluated by treating with IL-13PE. As shown in Fig. 1E,

11
MPC cells revealed moderately high sensitivity to IL-13PE (IC50<2.5 ng/mL), as compared to no
sensitivity in receptor negative T98G (IC50>1000 ng/mL), p<0.001. Receptor positive PM-RCC
served as a positive control with IC50=0.23 ng/mL.
IL-13PE Inhibits Pheochromocytoma tumor Growth in vivo
We developed an in vivo mouse model of pheochromocytoma by subcutaneously implanting
5x106 MPC cells. The tumors developed in 10-14 days and were sub-grouped by tumor size
(n=10 large, n=10 small). The animals were treated (n=5) with IL-13PE (100 μg/kg) or placebo
IT. IL-13PE treatment resulted in suppression of established tumors compared to placebo after 3
days initial treatment 75.1 ± 11.3 mm3 (mean±SEM) versus control 336.8 ± 57.7 mm3
(p=0.0021) and through the observation period 105.2 ± 58.5 mm3 compared to 1,113.2 ± 540.9
mm3 in control at day 9 (p=0.0032) (Fig. 2A). The study was repeated with smaller tumors and
showed comparable results 46.06 ± 3.900 mm3 versus control 74.89 ± 14.02 mm3 (p=0.0540) at
day 3 and 44.21 ± 5.084 mm3 compared to 221.4 ± 51.98 mm3 in control at day 9 (p=0.0095)
(Fig. 2B). Additionally, IL-13PE treatment demonstrated a histological response in these tumors
without any adverse effects (Fig. 2C).
DISCUSSION
Our study provides direct evidence that IL-13R�2 is overexpressed in pheochromocytoma
tumors. Furthermore, we show IL-13PE immunotoxin may be a novel therapeutic approach in
patients with IL-13R�2 positive metastatic pheochromocytoma. We identified an overexpression
of mRNA for IL-13R�2 in murine and human pheochromocytoma tumors compared to normal
adrenal tissues. These results are in corroboration with a previously published study of
expression profiling on pheochromocytoma, which confirmed overexpression of IL-13R�2 (18).

12
IFA studies in MPC cells and tumors demonstrate increased expression of the IL-13R�2, which
suggest that overexpressed mRNA for IL-13R�2 were translated into an immunoreactive protein.
The biological activity of IL-13R�2 chain was examined in vitro and in vivo in an animal
model of pheochromocytoma. In vitro, MPC demonstrated a dose dependent sensitivity to IL-
13PE. Similarly, IL-13PE caused regression of established tumors in vivo in mice. Previous
studies have shown IL-13R�2 negative tumors in vivo did not respond to IL-13PE treatment (19-
21). These results provide a proof-of-principle by demonstrating that IT injections of IL-13PE,
which binds IL-13R�2 with high specificity, reduced tumor growth followed by complete
regression in most animals. Nevertheless, the pheochromocytoma xenograft models can be
limited when extrapolated to more clinically relevant orthotopic or transgenic models (22, 23).
Currently, therapeutic options available to pheochromocytoma patients are limited.
Therefore novel therapeutic agents and approaches are needed. Various preclinical models have
been tested by administration of IL-13PE by different routes and its safety and efficacy against
different human cancers have been examined (9, 24). On the basis of these studies, several
clinical trials were intitiated in patients with malignant brain tumors (10). In the present study,
we have identified overexpression of IL-13R�2 in pheochromocytoma, another class of
endocrine tumors. Thus, IL-13R�2 overexpression may serve as a novel tumor target for IL-
13PE based receptor targeted therapy of pheochromocytoma. IL-13PE based approach may serve
beneficial with restricted adverse effects as it mediates its anti-cancer effects exclusively after
binding to IL-13R�2 in tumors. Thus, one would expect a low amount of toxicity to normal
tissues as they do not express this receptor chain. Indeed in clinical trials for malignant glioma,
no systemic toxicity was seen and no toxicity to normal brain was observed at the optimum dose
(25, 26).

13
However, to treat large metastatic pheochromocytomas, it may be necessary to optimize
effective delivery of the drug, which may require needle repositioning and geographic overlap
between successive zones for perfusion in the tumors. It is likely that tumors greater than 300
mm3 may be associated with a greater failure rate, most likely due to under-perfusion of the
tumors and failure to treat tissue beyond the tumor to create an adequate tumor-free margin.
Therefore, for large tumors, a continuous intratumor delivery method may need to be tested (6).
In addition, for metastatic pheochromocytoma, a combination approach of local administration
and systemic delivery may be needed. In that regard, it has been reported that IL-13PE is well
tolerated at a dosage of 2 μg/kg infused iv every alternate days for three injections.
In conclusion, the present study identified Interleukin-13 receptor overexpression in
neuroendocrine murine and human pheochromocytoma. Furthermore, this overexpression could
be exploited for IL-13PE based receptor directed therapy, which targets IL-13R�2. These results
should prove beneficial in clinical settings, as IT injections of IL-13PE reduced tumor growth
followed by complete regression in most animals.

14
ACKNOWLEDGEMENTS
This research was supported, in part, by the Intramural Research Program of the NIH, NICHD.
We would like to thank Ms. Stephanie Fliedner, Mr. Kyle T. Horak and Mr. Vishal Duggal their
support in the preparation of this manuscript.

15
REFERENCES
1. Manger WM 2006 An overview of pheochromocytoma: history, current concepts, vagaries, and diagnostic challenges. Ann N Y Acad Sci 1073:1-20
2. Pacak K, Linehan WM, Eisenhofer G, Walther MM, Goldstein DS 2001 Recent advances in genetics, diagnosis, localization, and treatment of pheochromocytoma. Ann Intern Med 134:315-329
3. Scholz T, Eisenhofer G, Pacak K, Dralle H, Lehnert H 2007 Clinical review: Current treatment of malignant pheochromocytoma. J Clin Endocrinol Metab 92:1217-1225
4. Eisenhofer G, Siegert G, Kotzerke J, Bornstein SR, Pacak K 2008 Current progress and future challenges in the biochemical diagnosis and treatment of pheochromocytomas and paragangliomas. Horm Metab Res 40:329-337
5. Joshi BH, Plautz GE, Puri RK 2000 Interleukin-13 receptor alpha chain: a novel tumor-associated transmembrane protein in primary explants of human malignant gliomas. Cancer Res 60:1168-1172
6. Kawakami K, Husain SR, Kawakami M, Puri RK 2002 Improved anti-tumor activity and safety of interleukin-13 receptor targeted cytotoxin by systemic continuous administration in head and neck cancer xenograft model. Mol Med 8:487-494
7. Kunwar S, Prados MD, Chang SM, Berger MS, Lang FF, Piepmeier JM, Sampson JH, Ram Z, Gutin PH, Gibbons RD, Aldape KD, Croteau DJ, Sherman JW, Puri RK 2007 Direct intracerebral delivery of cintredekin besudotox (IL13-PE38QQR) in recurrent malignant glioma: a report by the Cintredekin Besudotox Intraparenchymal Study Group. J Clin Oncol 25:837-844
8. Husain SR, Joshi BH, Puri RK 2001 Interleukin-13 receptor as a unique target for anti-glioblastoma therapy. Int J Cancer 92:168-175
9. Kawakami K, Kioi M, Liu Q, Kawakami M, Puri RK 2005 Evidence that IL-13R alpha2 chain in human glioma cells is responsible for the antitumor activity mediated by receptor-directed cytotoxin therapy. J Immunother 28:193-202
10. Joshi BH, Hogaboam C, Dover P, Husain SR, Puri RK 2006 Role of interleukin-13 in cancer, pulmonary fibrosis, and other T(H)2-type diseases. Vitam Horm 74:479-504
11. Obiri NI, Leland P, Murata T, Debinski W, Puri RK 1997 The IL-13 receptor structure differs on various cell types and may share more than one component with IL-4 receptor. J Immunol 158:756-764
12. Murata T, Husain SR, Mohri H, Puri RK 1998 Two different IL-13 receptor chains are expressed in normal human skin fibroblasts, and IL-4 and IL-13 mediate signal transduction through a common pathway. Int Immunol 10:1103-1110
13. Fichtner-Feigl S, Strober W, Kawakami K, Puri RK, Kitani A 2006 IL-13 signaling through the IL-13alpha2 receptor is involved in induction of TGF-beta1 production and fibrosis. Nat Med 12:99-106
14. Joshi BH, Kawakami K, Leland P, Puri RK 2002 Heterogeneity in interleukin-13 receptor expression and subunit structure in squamous cell carcinoma of head and neck: differential sensitivity to chimeric fusion proteins comprised of interleukin-13 and a mutated form of Pseudomonas exotoxin. Clin Cancer Res 8:1948-1956
15. Powers JF, Evinger MJ, Tsokas P, Bedri S, Alroy J, Shahsavari M, Tischler AS 2000 Pheochromocytoma cell lines from heterozygous neurofibromatosis knockout mice. Cell Tissue Res 302:309-320

16
16. Murata T, Obiri NI, Debinski W, Puri RK 1997 Structure of IL-13 receptor: analysis of subunit composition in cancer and immune cells. Biochem Biophys Res Commun 238:90-94
17. Brouwers FM, Elkahloun AG, Munson PJ, Eisenhofer G, Barb J, Linehan WM, Lenders JW, De Krijger R, Mannelli M, Udelsman R, Ocal IT, Shulkin BL, Bornstein SR, Breza J, Ksinantova L, Pacak K 2006 Gene expression profiling of benign and malignant pheochromocytoma. Ann N Y Acad Sci 1073:541-556
18. Thouennon E, Elkahloun AG, Guillemot J, Gimenez-Roqueplo AP, Bertherat J, Pierre A, Ghzili H, Grumolato L, Muresan M, Klein M, Lefebvre H, Ouafik L, Vaudry H, Plouin PF, Yon L, Anouar Y 2007 Identification of potential gene markers and insights into the pathophysiology of pheochromocytoma malignancy. J Clin Endocrinol Metab 92:4865-4872
19. Kawakami K, Kawakami M, Husain SR, Puri RK 2003 Potent antitumor activity of IL-13 cytotoxin in human pancreatic tumors engineered to express IL-13 receptor alpha2 chain in vivo. Gene Ther 10:1116-1128
20. Kawakami K, Kawakami M, Puri RK 2004 Specifically targeted killing of interleukin-13 (IL-13) receptor-expressing breast cancer by IL-13 fusion cytotoxin in animal model of human disease. Mol Cancer Ther 3:137-147
21. Kioi M, Kawakami M, Shimamura T, Husain SR, Puri RK 2006 Interleukin-13 receptor alpha2 chain: a potential biomarker and molecular target for ovarian cancer therapy. Cancer 107:1407-1418
22. Lai EW, Rodriguez OC, Aventian M, Cromelin C, Fricke ST, Martiniova L, Lubensky IA, Lisanti MP, Picard KL, Powers JF, Tischler AS, Pacak K, Albanese C 2007 ErbB-2 induces bilateral adrenal pheochromocytoma formation in mice. Cell Cycle 6:1946-1950
23. Korpershoek E, Loonen AJ, Corvers S, van Nederveen FH, Jonkers J, Ma X, Ziel-van der Made A, Korsten H, Trapman J, Dinjens WN, de Krijger RR 2009 Conditional Pten knock-out mice: a model for metastatic phaeochromocytoma. J Pathol 217:597-604
24. Joshi BH, Puri RK 2005 Optimization of expression and purification of two biologically active chimeric fusion proteins that consist of human interleukin-13 and Pseudomonas exotoxin in Escherichia coli. Protein Expr Purif 39:189-198
25. Husain SR, Puri RK 2003 Interleukin-13 receptor-directed cytotoxin for malignant glioma therapy: from bench to bedside. J Neurooncol 65:37-48
26. Kioi M, Husain SR, Croteau D, Kunwar S, Puri RK 2006 Convection-enhanced delivery of interleukin-13 receptor-directed cytotoxin for malignant glioma therapy. Technol Cancer Res Treat 5:239-250

17
Figure Legends
Figure 1. (A) RT-PCR reveals increased relative levels of IL-13Rα2 in SC and liver tumors as
assessed and normalized to ß-actin. (B) RT-PCR reveals levels of IL-13Rα2 mRNA expression
in normal adrenal medulla, positive control (PM-RCC) and a variety of tumor samples across
various genotype and tumor behavior backgrounds. Relative levels of IL-13Rα2 mRNA were
assessed and normalized to ß-actin. (C) Expression of IL-13R�2 in mouse pheochromocytoma
cells (MPC) and (D) mouse SC tumor tissue by immunohistochemical staining reveal positive
expression of IL-13R�2. (E) Cytotoxicity assay in MPC cells, negative control cells (T98G), and
positive control cells (PM-RCC).
Figure 2. Intratumoral treatment of subcutaneous implanted mouse pheochromocytoma tumors
with IL-13PE immunotoxin. Female nude mice were injected subcutaneously with 5x106 MPC.
(A) IL-13 PE was injected intratumoral (IT) in large (95 ± 17mm3, average ± SEM) and small
(53 ± 4mm3) tumors with 100μg dose/kg, 3 doses on consecutive days 1, 2 and 3 (arrows).
Significance compared to control by un-paired T-test *P<0.05, **P<0.01, ***P<0.001. (B) IL-
13PE treatment regressed tumors in treated tumors and (C) H&E staining of paraffin sections
(20x and 60x) also revealed necrotic regions and nuclear fragmentation in treated tumors
compared to untreated control.
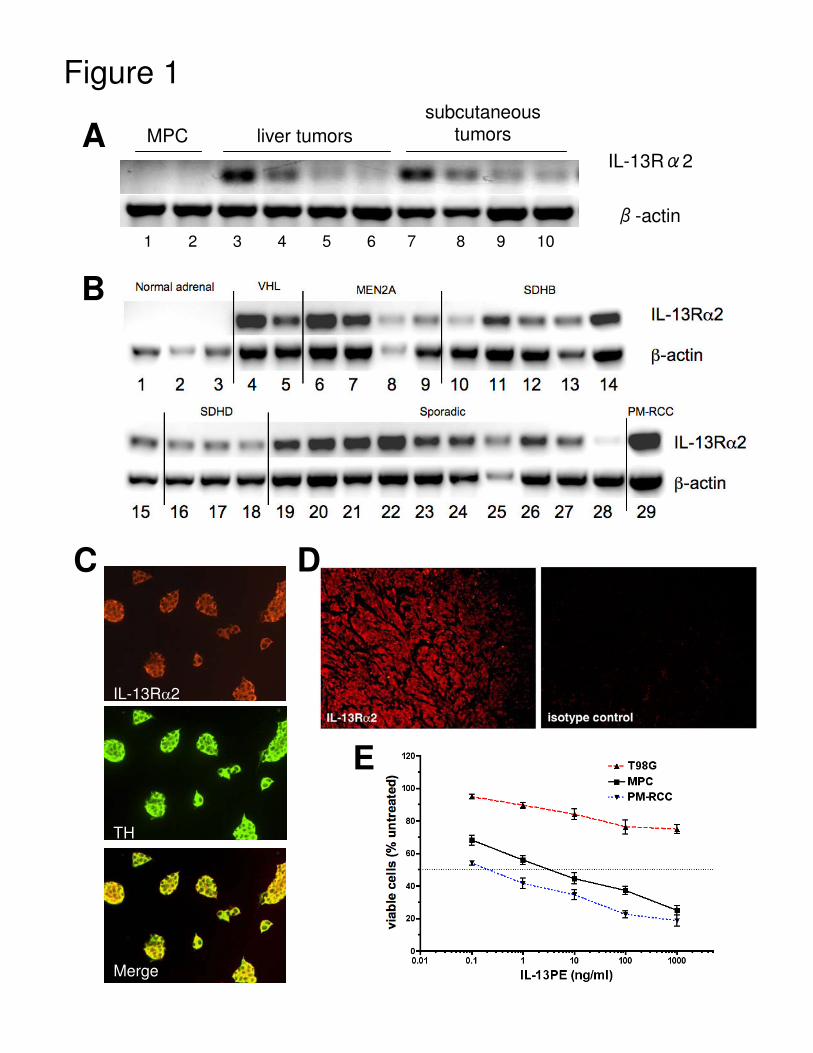
Figure 1
B
A
IL-13Rα2
TH
Merge
C D
IL-13R�2
�-actin
liver tumorssubcutaneous
tumors
E
1 2 3 4 5 6 7 8 9 10
MPC

Figure 2
UntreatedControl
Day 1
Day 9
Treated IT100ug/kg
Day 7
C
B
UntreatedControl
Treated IT100ug/kg
20x
A
60x
20x 60x
















![Usefulness of [18F]-DA and [18F]-DOPA for PET imaging in a mouse model of pheochromocytoma](https://static.fdokumen.com/doc/165x107/6325a7d9852a7313b70e9a7d/usefulness-of-18f-da-and-18f-dopa-for-pet-imaging-in-a-mouse-model-of-pheochromocytoma.jpg)


