
Un modelo MIMIC para estudiar la Eficacia de la Ayuda Oficial al Desarrollo
Upload
independentCategory
view
3download
0
Occupational stress and psychopathology in health professionals:An explorative study with the Multiple Indicators Multiple Causes(MIMIC) model approach
PAOLO ILICETO1, MAURIZIO POMPILI1,2, SALLY SPENCER-THOMAS3,
STEFANO FERRACUTI1, DENISE ERBUTO1, DAVID LESTER4,
GABRIELLA CANDILERA5, & PAOLO GIRARDI1
1Department of Neurosciences, Mental Health and Sensory Organs, Suicide Prevention Center, Department of Psychiatry,
Sant’Andrea Hospital, Sapienza University of Rome, Rome, Italy, 2McLean Hospital, Harvard Medical School, Belmont,
MA, USA, 3Carson J Spencer Foundation, Denver, CO, USA, 4The Richard Stockton College of New Jersey, Galloway, NJ,
USA, and 5Clinical Psychologist, Private Practice, Rome, Italy
(Received 29 December 2011; revised 21 April 2012; accepted 26 April 2012)
AbstractOccupational stress is a multivariate process involving sources of pressure, psycho-physiological distress, locus of control,work dissatisfaction, depression, anxiety, mental health disorders, hopelessness, and suicide ideation. Healthcare professionalsare known for higher rates of occupational-related distress (burnout and compassion fatigue) and higher rates of suicide. Thepurpose of this study was to explain the relationships between occupational stress and some psychopathological dimensions ina sample of health professionals. We investigated 156 nurses and physicians, 62 males and 94 females, who were administeredself-report questionnaires to assess occupational stress [occupational stress inventory (OSI)], temperament (temperamentevaluation of Memphis, Pisa, Paris, and San Diego autoquestionnaire), and hopelessness (Beck hopelessness scale). The bestMultiple Indicators Multiple Causes model with five OSI predictors yielded the following results: x 2(9) ¼ 14.47 ( p ¼ 0.11);x 2/df ¼ 1.60; comparative fit index ¼ 0.99; root mean square error of approximation ¼ 0.05. This model provided a good fitto the empirical data, showing a strong direct influence of casual variables such as work dissatisfaction, absence of type Abehavior, and especially external locus of control, psychological and physiological distress on latent variable psychopathology.Occupational stress is in a complex relationship with temperament and hopelessness and also common among healthcareprofessionals.
Keywords: Health professionals, hopelessness, MIMIC model, occupational stress, psychopathology, temperament
Introduction
Selye defined stress as the nonspecific response of the
body to any demand, after subtraction of the specific
components from the total response, emphasizing that
the stress syndrome would result from exposure to any
stressor (the causative agent) retaining stress (the
resulting condition) (Selye 1936). He stated that
different biological responses could be predicted
based on the introduction of a toxin into a specific
bodily system. On the basis of these findings, he
developed his theory of the general adaptation
syndrome with three distinct stages: (1) alarm
reaction, (2) stage of resistance, and (3) stage of
exhaustion (Selye 1974). Another important contri-
bution was the distinction between the effects of
different types of stress: he considered that there was
eustress, which was harmless or seemingly beneficial
stress, and distress, which was harmful or bad stress
(Selye 1976). Regulation around an altered state is the
essence of allostasis, a term referring to the levels of
activity required for the individual to adapt and
maintain stability through change (McEwen 1998,
2000), while allostatic load refers to effects of
Correspondence: M. Pompili, Department of Psychiatry, Sant’Andrea Hospital, Sapienza University of Rome, 1035 Via di Grottarossa,00189 Rome, Italy. Tel: þ 39 06 33775675. Fax: þ 39 06 33775342. E-mail: [email protected]
Stress, 2012; Early Online: 1–10q Informa Healthcare USA, Inc.ISSN 1025-3890 print/ISSN 1607-8888 onlineDOI: 10.3109/10253890.2012.689896
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
icol
e H
arpo
le o
n 06
/07/
12Fo
r pe
rson
al u
se o
nly.

prolonged continuous or intermittent activation of
effectors involved in allostasis, and long-term allo-
static load provides a conceptual basis for studying
long-term health consequences of stress (McEwen
and Stellar 1993).
Occupational stress is the emotional, cognitive,
behavioral, and physiological reaction to aversive and
noxious aspects of work, work environments, and work
organizations and contributes to negative psychologi-
cal and physiological outcomes; moreover, in health
professionals, occupational stress involves client-
related difficulties, lack of resources, and workload
(Edwards and Burnard 2003; Mandy and Tinley
2004). Stress is a complex phenomenon with the three
key elements of sources, effects, and individual
differences, and it exists in a state of disequilibrium
in the system of variables relating people to their
environment that results in a change in their normal
levels of well-being (Hart et al. 1993). On the basis of
this definition, occupational stress cannot be expressed
as a single variable but as a multivariate process linked
to personality characteristics, coping processes, and
positive and negative work experiences (Hart and
Wearing 1995). Hence, occupational stress may be
considered as a lack of fit between subjects and the
work environment, and stress-related risk factors are
also linked with sociodemographic factors, subjective
perceptions of the work environment, and all the
processes of cognitive appraisal (Albini et al. 2011).
The relationship between stressors and disease is
affected by the nature and persistence of the stressors
as well as by an individual’s biological factors,
psychosocial resources, and learned patterns of coping
(Schneiderman et al. 2005). Work-related environmen-
tal conditions, acting as job stressors and pressures, may
be direct predictors of work dissatisfaction, negative
mental and physical health outcomes, and reduced
coping strategies, while this relationship may be
moderated by individual difference variables (Cooper
and Baglioni 1988; Baglioni et al. 1990).
Suicide risk in the healthcare professions is some-
what difficult to determine because of controversy in
the data collection process and the stigma surrounding
suicide in the helping professions. Aasland et al.
(2011) and Hem et al. (2005) reported in a
longitudinal study that Norwegian doctors had a
lower mortality rate than the general population for all
causes of death except suicide. The most compelling
research to date indicates that on average, death by
suicide is about 70% more likely among male
physicians in the USA than among other professionals
and 250–400% higher among female physicians
(American Foundation for Suicide Prevention, n.d.).
While most research has been on physicians and
medical students, there is evidence from several
countries that female nurses and nursing associate
professionals are also at a significantly increased risk of
suicide (Hawton and Vislisel 1999; Pompili et al.
2006; Agerbo et al. 2007). These increased risk rates
are sustained even after adjustments are made for
psychiatric admission, employment status, marital
status, and gross income. Many explain these findings
by noting that healthcare professionals work in a high
stress environment where they are not allowed to show
any weaknesses. They are supposed to be in the role of
helping save lives, but sometimes they are not able to
save their own because they are ashamed of having a
mental or substance abuse disorder. Combining these
factors with access to the lethal means of suicide and
in-depth knowledge of how to end life, it is evident
that those in the medical profession who are
committed to taking their lives are usually able to do
so in one lethal attempt.
The striking elevated suicide rate for female
physicians is particularly disturbing. According to
one reviewer (Alexander 2001), female physicians
tend to be more suicidal at the beginning of their
careers and in midlife, suggesting a conflict between
double duties as family providers and healthcare
providers. Furthermore, a review of the literature has
revealed that prejudices against women may also
contribute to their distress. Evidently, stigma prevents
those in the healthcare profession from seeking
medical care and often drives the suicidal person to
dangerous self-medication (Myers and Fine 2003).
Furthermore, Myers reports that the “conspiracy of
silence” following a physician’s death by suicide
compounds suffering, confuses surviving family
members and thwarts public health efforts at
prevention.
Many studies have documented that health workers,
especially emergency service workers and mental
health professionals, show higher levels of stress and
health problems than many other occupational groups
(Moore and Cooper 1996; O’Connor et al. 2000; Lee
and Wang 2002; Gellis and Kim 2004; Falkum and
Vaglum 2005; Marine et al. 2006; Oginska-Bulik
2006; Belkic and Nedic 2007; Augusto Landa et al.
2008; Ruotsalainen et al. 2008). Moreover, Bamber
and McMahon (2008) pointed out the high costs of
occupational stress and reported the need for
psychological interventions in reducing stress-related
disorders at work among healthcare workers, which
may influence the course of diseases. Furthermore,
stressful life event dimensions are related to the
development of neuroticism (Knussen and Niven
1999), major depression and generalized anxiety
(Kendler et al. 2003), mental health disorders
(McNally 2003) as well as hopelessness and suicide
ideation (O’Connor et al. 2004), and facets of
stress that act synergistically are more potent than a
single aspect, including the area of work stress
(Stanton et al. 2001).
This study aimed to provide empirical data about
occupational stress and its relationships with some
psychopathological dimensions in a sample of health
P. Iliceto et al.2
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
icol
e H
arpo
le o
n 06
/07/
12Fo
r pe
rson
al u
se o
nly.

workers. Specifically, it was hypothesized that there
are many sources of occupational stress, psychological
and physical diseases that may have a direct
relationship with psychopathology. We tested our
hypotheses with a Multiple Indicators Multiple
Causes (MIMIC) model (Joreskog and Goldberger
1975; Muthen 1989) that involves psychopathology as
a latent variable, defined by dysthymic/cyclothymi-
c/anxious temperament, irritable temperament, and
hopelessness as indicators.
Method
Participants
In the first half of 2010, all 230 health professionals
(nurses and physicians) from three hospitals in the
district of Rome (Italy; San Sebastiano Hospital,
Frascati, San Giuseppe Hospital, Marino, and A.C.
Cortoni Hospital, Rocca Priora) were handed an
envelope containing description of the aims of this
research. Of the 230 health professional contacted,
156 voluntarily participated in this study and each
subject provided written informed consent. The study
protocol received ethical approval from the local
research ethics review board in accordance with the
Helsinki Declaration. The participants were 62 males
(mean age ¼ 44.3 years, SD ¼ 11.18) and 94 females
(mean age ¼ 42.0 years, SD ¼ 8.49). Their socio-
demographic characteristics are shown in Table I. No
differences were found between the age of the females
and the age of the males (t(154) ¼ 1.46; p ¼ 0.14);
there were more female than male nurses (x 2(1) 4.41;
p ¼ 0.03); there were no differences for the years of
education (x 2(2) 5.00; p ¼ 0.08). Those who declined
the invitation to participate were not different with
regard to sociodemographic variables from partici-
pants enrolled in the study.
Instruments
The occupational stress inventory (OSI; Cooper et al.
1988) consists of 167 items with six-point Likert
response keys for all items and yields 25 subscales
divided into six areas. (1) How you feel about your job
assesses job satisfaction with 22 items and a response
key ranging from very much satisfaction to very much
dissatisfaction. There are five subscales: achievement,
value, and growth; job itself; organizational design and
structure; organizational processes; and personal
relationships. (2) How you assess your current state of
health is in two parts: part A is an 18-item (response
key: from very true to very untrue) measure of mental
ill-health, and part B is a 12-item measure of physical
ill-health (response key: from never to very frequently
experience the particular symptom). (3) The way you
behave generally is a type A behavior pattern measure
with 14 items (response key: from very strongly agree
to very strongly disagree). There are three subscales:
attitude to living, style of behavior, and ambition. (4)
How you interpret events around you is a measure of
workplace locus of control with 12 items (response
key: from very strongly agree to very strongly
disagree). It yields three subscales: organizational
forces, management processes, and individual influ-
ences. (5) Sources of pressure in your job has 61 items
(response key: very definitely is to very definitely is not
a source). Six subscales assess sources of pressure:
factors intrinsic to the job, managerial role, relation-
ships with others, career and achievement, organiz-
ational structure and climate, and home–work
interface. (6) How you cope with the stress you experience
has 28 coping items (response key: from never to very
extensively). There are six subscales that assess the
following coping strategies: social support, task
strategies, logic, home–work relationships, time
management, and involvement. The validated Italian
version of the questionnaire was used, and Cronbach’s
alpha for the subscale coefficients ranged from 0.72 to
0.86 (Sirigatti and Stefanile 2002).
The first version of Temperament Evaluation of
Memphis, Pisa, Paris and San Diego Autoquestionnaire
(TEMPS-A) contained 84 items (Akiskal and Akiskal
2005). Later, clinical and theoretical considerations
led to the addition of 26 new items describing the
anxious temperament, resulting in the 110-item-long
version of the TEMPS-A (Akiskal et al. 1998). The
scale is different from most other temperament scales,
in that it taps subaffective trait expressions as they
were conceptualized in Greek psychological medicine
and, in more modern times, German psychiatry. The
TEMPS-A has been validated in Italian populations
(Pompili et al. 2008; , in press). In that investigation, a
principal-component analysis resulted in a three-
factor solution: the first represented a combination of
dysthymic, cyclothymic, and anxious (Dys/Cyc/Anx)
temperaments; the second represented irritable
temperament; and the third represented hyper-
thymic temperament. Kuder–Richardson reliability
coefficients ranged from 0.90 for the Dys/Cyc/Anx
factor to 0.76 for the hyperthymic factor.
Table I. Sociodemographic characteristics of participants.
Characteristics
Males
(N ¼ 62)
Females
(N ¼ 94) Statistics p
Age (years) 44.3 ^ 11.18* 42.0 ^ 8.49* t(154) ¼ 1.46 0.14
Groups
Nurses (%) 34.3 65.7 x 2(1) ¼ 4.41 0.03
Physicians (%) 52.1 47.9
Education (years)
# 8 (%) 6.5 3.2 x 2(2) ¼ 5.00 0.08
# 13 (%) 35.4 53.2
. 13 (%) 58.1 43.6
* Values are mean ^ SD.
MIMIC and job stress in health workers 3
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
icol
e H
arpo
le o
n 06
/07/
12Fo
r pe
rson
al u
se o
nly.

The Beck hopelessness scale (BHS: Beck et al. 1974;
Beck and Steer 1989) is a 20-item scale for
measuring negative attitudes about the future. Beck
originally developed this scale in order to predict
who would commit suicide and who would not. This
powerful predictor of eventual suicide addressed
three major aspects of hopelessness: feelings about
the future, loss of motivation, and expectations.
Responding to the 20 true or false items on the
BHS, individuals can either endorse a pessimistic
statement or deny an optimistic statement. Research
consistently supports a positive relationship between
BHS scores and measures of depression, suicidal
intent and current suicidal ideation. Studies on the
Italian population were carried out (Pompili et al.
2007) and led to successful validation of the scale
(Pompili et al. 2009). Kuder–Richardson reliability
coefficient of the BHS total score was 0.89 (Pompili
et al. 2009).
Statistical analyses
The two-tailed t-test was used for continuous
variables, and chi-square tests were used with Yates’s
correction where appropriate to identify differences in
sociodemographic characteristics. We computed a test
for the mean of a normally distributed variable for
which the population standard deviation is known
(norm values) to compare the sample means.
Structural equation modeling (SEM) relies on
several statistical tests to determine the adequacy of
model fit to the empirical data, taking into account the
modeling of multiple latent independents each
measured by multiple indicators, and one or more
latent dependents also each with multiple indicators.
The process centers around two steps: validating the
measurement model and fitting the structural model.
This starts by specifying a model on the basis of theory
and prior empirical research, and two or more
Table II. Comparisons between normative sample and research sample (males).
OSI scales
Mean research
sample (n ¼ 62) SD
Mean normative
sample (n ¼ 319) SD z p
Job satisfaction
Achievement value and growth 22.0 3.69 22.0 5.25 20.02 n.s.
Job itself 16.8 2.12 16.7 2.87 0.58 n.s.
Organizational design and structure 16.9 3.51 17.4 4.45 0.04 n.s.
Organizational processes 15.3 2.74 15.0 3.62 1.03 n.s.
Personal relationships 11.2 2.15 11.7 2.67 20.47 n.s.
OSI1 82.2 11.85 82.8 16.58 0.26 n.s.
Health
OSI2 55.2 10.65 60.4 10.12 23.18 0.000
OSI3 28.9 8.62 29.1 9.66 1.27 n.s.
Type A behavior
Attitude to living 21.2 2.71 22.2 4.35 23.14 0.000
Style of behavior 19.5 3.61 18.5 4.66 2.05 0.02
Ambition 10.6 1.91 10.8 2.57 21.96 0.02
OSI4 51.3 5.41 51.5 8.05 21.09 n.s.
Locus of control
Organizational forces 20.4 3.66 18.9 4.14 4.04 0.000
Management processes 13.2 1.94 15.6 3.25 27.82 0.000
Individual influences 9.0 2.87 10.2 2.78 23.21 0.000
OSI5 42.5 4.93 44.7 6.29 22.57 0.005
Sources of pressure
OSI6 33.7 5.32 33.1 6.57 2.14 0.01
OSI7 44.6 7.77 44.0 7.61 1.31 n.s.
OSI8 37.6 7.14 36.4 6.86 1.88 0.03
OSI9 35.5 6.13 35.7 6.43 1.18 n.s.
OSI10 46.2 7.59 44.9 7.46 2.07 0.01
OSI11 43.7 7.14 43.5 8.18 1.06 n.s.
Coping strategies
Social support 16.4 3.03 15.8 3.61 1.59 0.05
Task strategies 27.6 3.70 27.0 4.62 2.93 0.001
Logic 13.2 2.05 13.2 2.55 1.42 n.s.
Home–work relationships 17.4 3.36 17.1 3.76 2.09 0.01
Effective use of time 16.7 2.15 16.8 2.71 20.88 n.s.
Involvement 26.3 4.10 25.8 3.82 2.44 0.007
Notes: OSI, occupational stress inventory; OSI1, total job satisfaction; OSI2, mental health; OSI3, physical health; OSI4, total type A; OSI5,
total locus of control; OSI6, factors intrinsic to the job; OSI7, managerial role; OSI8, relationships with other people; OSI9, career and
achievement; OSI10, organizational structure and climate; OSI11, home–work interface.
P. Iliceto et al.4
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
icol
e H
arpo
le o
n 06
/07/
12Fo
r pe
rson
al u
se o
nly.
alternative models are then compared in terms of
model fit, which measures the extent to which the
covariances predicted by the model correspond to
the observed covariances in the data, by means of the
statistical fitting of the factor model to the observed
data (variances and covariances or correlations), the
assessment of fit, and the interpretation of the results if
the model is consistent with the data (Bollen 1989).
The chi-square test indicates the amount of
difference between expected and observed covariance
matrices. A chi-square value close to zero indicates
little difference between the expected and the
observed covariance matrices. In addition, the
probability level must be greater than 0.05 when
chi-square is close to zero. The comparative fit index
(CFI) is equal to the discrepancy function adjusted for
sample size. The CFI ranges from 0 to 1 with a larger
value indicating better model fit. Acceptable model fit
is indicated by a CFI value of 0.90 or greater. Root
mean square error of approximation (RMSEA) is
related to the residual in the model. RMSEA values
range from 0 to 1 with a smaller RMSEA value
indicating better model fit. Acceptable model fit is
indicated by an RMSEA value of 0.06 or less (Hu and
Bentler 1998, 1999).
The MIMIC model (Joreskog and Goldberger
1975; Muthen 1989) involves latent variable(s) with
usual multiple indicators, but in addition, it is also
predicted by observed variables. A MIMIC model is a
specific application of SEM that contains one or more
latent variables simultaneously identified by multiple
endogenous indicators and multiple exogenous causal
variables. All analyses were carried out using SPSS
17.0. The hypothesized structural relations in the
model were assessed by using LISREL 8.80.
Results
With regard to OSI scales, we used the data from the
Italian normative sample that consisted of 534 women
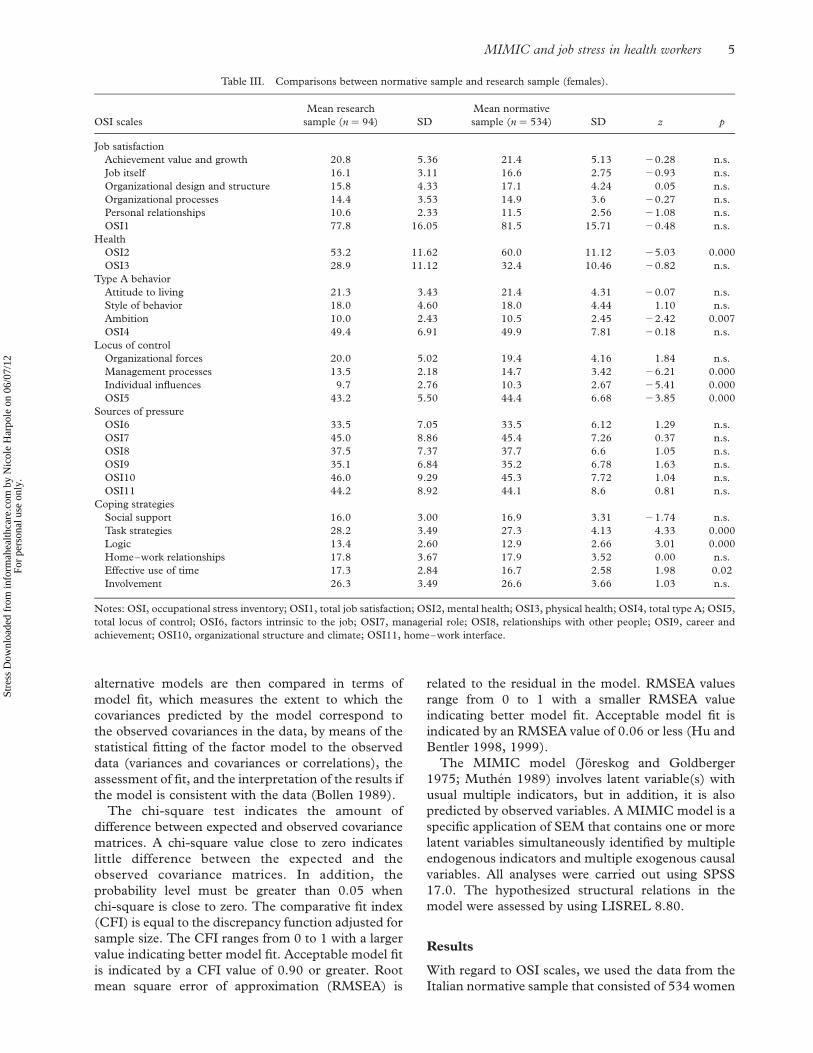
Table III. Comparisons between normative sample and research sample (females).
OSI scales
Mean research
sample (n ¼ 94) SD
Mean normative
sample (n ¼ 534) SD z p
Job satisfaction
Achievement value and growth 20.8 5.36 21.4 5.13 20.28 n.s.
Job itself 16.1 3.11 16.6 2.75 20.93 n.s.
Organizational design and structure 15.8 4.33 17.1 4.24 0.05 n.s.
Organizational processes 14.4 3.53 14.9 3.6 20.27 n.s.
Personal relationships 10.6 2.33 11.5 2.56 21.08 n.s.
OSI1 77.8 16.05 81.5 15.71 20.48 n.s.
Health
OSI2 53.2 11.62 60.0 11.12 25.03 0.000
OSI3 28.9 11.12 32.4 10.46 20.82 n.s.
Type A behavior
Attitude to living 21.3 3.43 21.4 4.31 20.07 n.s.
Style of behavior 18.0 4.60 18.0 4.44 1.10 n.s.
Ambition 10.0 2.43 10.5 2.45 22.42 0.007
OSI4 49.4 6.91 49.9 7.81 20.18 n.s.
Locus of control
Organizational forces 20.0 5.02 19.4 4.16 1.84 n.s.
Management processes 13.5 2.18 14.7 3.42 26.21 0.000
Individual influences 9.7 2.76 10.3 2.67 25.41 0.000
OSI5 43.2 5.50 44.4 6.68 23.85 0.000
Sources of pressure
OSI6 33.5 7.05 33.5 6.12 1.29 n.s.
OSI7 45.0 8.86 45.4 7.26 0.37 n.s.
OSI8 37.5 7.37 37.7 6.6 1.05 n.s.
OSI9 35.1 6.84 35.2 6.78 1.63 n.s.
OSI10 46.0 9.29 45.3 7.72 1.04 n.s.
OSI11 44.2 8.92 44.1 8.6 0.81 n.s.
Coping strategies
Social support 16.0 3.00 16.9 3.31 21.74 n.s.
Task strategies 28.2 3.49 27.3 4.13 4.33 0.000
Logic 13.4 2.60 12.9 2.66 3.01 0.000
Home–work relationships 17.8 3.67 17.9 3.52 0.00 n.s.
Effective use of time 17.3 2.84 16.7 2.58 1.98 0.02
Involvement 26.3 3.49 26.6 3.66 1.03 n.s.
Notes: OSI, occupational stress inventory; OSI1, total job satisfaction; OSI2, mental health; OSI3, physical health; OSI4, total type A; OSI5,
total locus of control; OSI6, factors intrinsic to the job; OSI7, managerial role; OSI8, relationships with other people; OSI9, career and
achievement; OSI10, organizational structure and climate; OSI11, home–work interface.
MIMIC and job stress in health workers 5
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
icol
e H
arpo
le o
n 06
/07/
12Fo
r pe
rson
al u
se o
nly.
with a mean age of 36.2 years (SD ¼ 11.8) and 319
men with a mean age of 34.4 years (SD ¼ 16.3), with
education from medium to high. The subjects were
primarily employees, teachers, engineers, and man-
agers involved in different areas, such as health,
communications, banking, and trading(Sirigatti and
Stefanile 2002). Compared with the normative
sample, both men (Table II) and women (Table III)
obtained lower scores on most OSI scales, such as
mental health (OSI2, z ¼ 3.18; p ¼ 0.000 and
z ¼ 5.03; p ¼ 0.000) and locus of control (OSI5,
z ¼ 2.57; p ¼ 0.005 and z ¼ 3.85; p ¼ 0.000); no
differences were found in job satisfaction and type A
behavior (OSI4), while only males showed higher
scores in some stress sources such as factors intrinsic
to the job (OSI6, z ¼ 2.14; p ¼ 0.01), relationships
with others (OSI8, z ¼ 1.88; p ¼ 0.03), and organiz-
ational structure and climate (OSI10, z ¼ 2.07;
p ¼ 0.01).
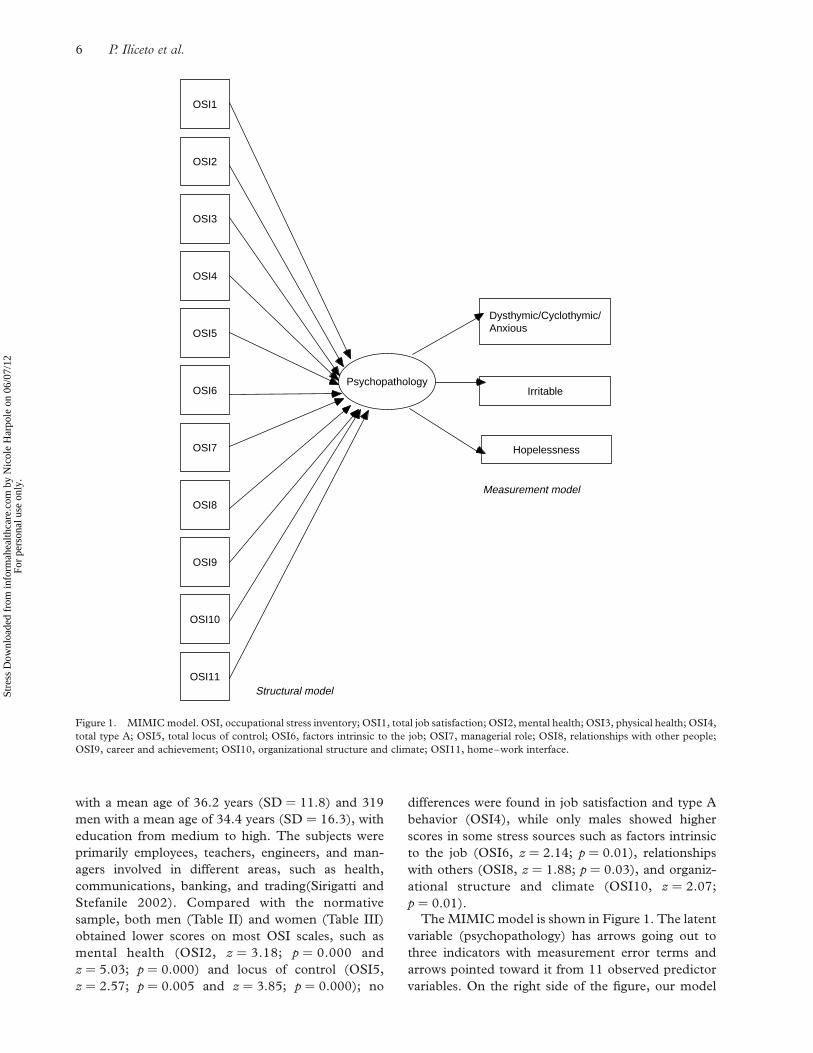
The MIMIC model is shown in Figure 1. The latent
variable (psychopathology) has arrows going out to
three indicators with measurement error terms and
arrows pointed toward it from 11 observed predictor
variables. On the right side of the figure, our model
Psychopathology
Dysthymic/Cyclothymic/Anxious
Irritable
Hopelessness
OSI11
OSI10
OSI9
OSI8
OSI7
OSI6
OSI5
OSI4
OSI3
OSI2
OSI1
Measurement model
Structural model
Figure 1. MIMIC model. OSI, occupational stress inventory; OSI1, total job satisfaction; OSI2, mental health; OSI3, physical health; OSI4,
total type A; OSI5, total locus of control; OSI6, factors intrinsic to the job; OSI7, managerial role; OSI8, relationships with other people;
OSI9, career and achievement; OSI10, organizational structure and climate; OSI11, home–work interface.
P. Iliceto et al.6
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
icol
e H
arpo
le o
n 06
/07/
12Fo
r pe
rson
al u
se o
nly.

represents a latent variable (psychopathology) that is
defined by dysthymic/cyclothymic/anxious tempera-
ment, irritable temperament, and hopelessness. On
the left side of the figure, the structural model relates
the latent variable to the causal variables; the OSI
scales: job satisfaction, psychological and physiologi-
cal illness, type A behavior, locus of control, and six
stress sources.
Table IV contains the results of the model selection
procedures, showing several fit indices. Initially, the
first model considers all 11 OSI scales as predictors
and showed the following results: x 2(22) ¼ 32.93
( p ¼ 0.06); x 2/df ¼ 1.49; CFI ¼ 0.99; RMSEA ¼
0.06. Despite the first model yielding a reasonably
acceptable global model fit of the structural model,
many predictors have low loadings. Then, we tested
a second model only with the six stress sources
as predictors, which produced fit indices as
follows: x 2(12) ¼ 35.91 ( p ¼ 0.000); x 2/df ¼ 2.99;
CFI ¼ 0.98; RMSEA ¼ 0.11; the hypothesis that this
model has a good fit to the data is easily rejected.
Finally, we tested a third model with only the
remaining five OSI predictors, which yielded
the following results: x 2(9) ¼ 14.47 ( p ¼ 0.11);
x 2/df ¼ 1.60; CFI ¼ 0.99; RMSEA ¼ 0.05, and this
model provided a good fit to the empirical data,
substantially better than the previous factor models.
All factor loadings of the measurement model were
high, all above 0.50; moreover, in terms of squared
multiple correlation coefficients (R 2) that describe the
amount of variance the common factor accounts for
in the indicator variables, in order of increasing
magnitude, the latent variable psychopathology
explains about 26% of the variance of hopelessness,
56% of the variance of irritable temperament, and
71% of dysthymic/cyclothymic/anxious temperament.
Table V contains the regression coefficients for this
final model.
Discussion
In this study, the MIMIC model framework was used
for understanding the relationship between stress
occupational variables and the possible onset of
psychopathology carefully assessed by other observed
variables as the affective temperaments and hope-
lessness. The present study showed that specific
sources of stress from factors intrinsic to the job such
as managerial role, relationships with other people,
career and achievement, organizational structure, and
home–work interface indicated only a moderate
relationship with psychopathology. In contrast, work
dissatisfaction, absence of type A behavior, and
especially external locus of control, psychological
and physiological distress showed a strong direct
influence on the latent variable psychopathology.
Langballe et al. (2011) investigated physician
burnout in association with individual factors, work
characteristics, and work–home interaction (job
performance-based self-esteem, goal orientation,
value congruency, workload, autonomy, work–home
conflict, and work–home facilitation). They found
that many of the assumed predictors play significant
roles in physician burnout. Specifically, work–home
conflict was a particularly strong burnout predictor in
female physicians, whereas workload was the strongest
burnout predictor in male physicians.
Work-related stress increases the risk of sick leave,
early retirement, and use of antidepressants in the
working population in all sectors of employment.
Different working conditions, such as work overload
and disparity between individual and work resources,
cause work-related stress, and prolonged work stress
has a negative effect on workers’ health; indeed, in
different studies associations between work-related
stress and cardiovascular diseases and depression have
emerged (Michie and Williams 2003; Bonde 2008).
Many studies have been carried out on different
work-related stress factors and their influence on
health and work ability of physicians and nurses in
healthcare. Often health professionals have tensions
specifically related to occupational stress, and, in
addition to psychological disorders, they suffer high
levels of stress (van der Doef and Maes 1999). The
relationship between psycho-physiological stressors
and chronic disease is complex, and adverse effects of
chronic stressors are particularly common in
health professionals with negative work experiences
Table IV. Global fit of factor models.
x 2 (df) p CFI RMSEA
Model 1 (OSI1–OSI11) 32.93 (22) 0.06 0.99 0.06
Model 2 (OSI6–OSI11) 35.91 (12) 0.000 0.98 0.11
Model 3 (OSI1–OSI5) 14.47 (9) 0.11 0.99 0.05
Notes: OSI1, total job satisfaction; OSI2, mental health; OSI3,
physical health; OSI4, total type A; OSI5, total locus of control;
OSI6, factors intrinsic to the job; OSI7, managerial role; OSI8,
relationships with other people; OSI9, career and achievement;
OSI10, organizational structure and climate; OSI11, home–work
interface; CFI, comparative fit index; RMSEA, root mean square
error of approximation.
Table V. MIMIC model results. Regression coefficients between
exogenous variables and latent factor.
Psychopathology
Total job satisfaction 20.09
Mental health 0.49*Physical health 0.27*Total type A 20.12
Total locus of control 0.22*
Note: MIMIC, Multiple Indicators Multiple Causes. *p , 0.05.
MIMIC and job stress in health workers 7
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
icol
e H
arpo
le o
n 06
/07/
12Fo
r pe
rson
al u
se o
nly.

(Kinnunen-Amoroso 2011). Irritable temperament,
dysthymic/cyclothymic/anxious temperament as well
as the component of hopelessness are associated with a
psychological condition in which individuals are
characterized by generally pessimistic and self-critical
cognition. This involves a negative temporal perspec-
tive of the future, and responses to stressful events that
are likely to be more hopeless and, as a result, such
individuals are at enhanced risk of suicidal behavior
(Pompili et al. 2004; Rihmer et al. 2007). Our present
results confirm this framework provides evidence for
the relationship of specific stressors, indicated above,
with psychopathology.
Currently in Europe, work-related stress is a major
problem (de Smet et al. 2005), and by improving the
working conditions that cause it, stress and its
consequences can be controlled (van der Klink et al.
2001; Lamontagne et al. 2007). Specifically, among
health professionals, there are stress sources, such as
contact with suffering and/or dying patients and the
need to hide negative emotional responses, which are
accompanied by reduced effectiveness, decreased
motivation, and development of dysfunctional beha-
vior and attitudes at the workplace that may have a
direct consequence for development of psychopathol-
ogy (Ruotsalainen et al. 2008) and that represent part
of findings of the present study.
This study has noteworthy limitations, including
only a moderate sample size, the use of self-reported
instruments to assess job stressors without objective
observations that are generally more difficult to
obtain, and a cross-sectional study design. Obviously,
longitudinal studies are more informative about
temporal features of the stress process. Moreover,
the number of participants allowed for an adequate
test of the MIMIC model, but it could not permit
measurement of the impact of sex (male/female) and
professional role (nurses/physicians). Furthermore,
throughout this paper, we referred to suicide risk by
measuring hopelessness as a proxy of such risk. This is
a limitation because, despite its predictive value,
hopelessness is a marker that can indicate false
positives when assessing suicide risk, while several
other contributing factors can increase suicide risk
(Pompili 2010; Fowler 2012). This points to the fact
that our emphasis on suicide risk using the
measurement of hopelessness could be mitigated by
taking into account contributing factors that were not
part of the data collection for this study. Another
important factor that may limit generalization of
present findings is that a possible causal link between
working as a doctor and suicide risk would be
hazardous to support, especially given that the risk
increases with age, way into retirement, at least for
males (Hem et al. 2000).
In conclusion, our MIMIC model provided a good
fit to the empirical data, showing a strong direct
influence of casual variables such as work dissatisfac-
tion, absence of type A behavior, and especially
external locus of control, psychological and physio-
logical distress on latent variable psychopathology.
This model allows testing concurrently numerous
variables as indices of both stress and psychopathol-
ogy, and in this way, it should be possible to monitor
the effectiveness of interventions in reducing stress at
the workplace for this specific population. The
MIMIC methodology has potential in exploring
these issues, and further research is needed on how
the links between occupational stressors and psycho-
pathology may involve other variables, such as
emotional distress, mood disorders, and insecure
attachment. Studies in other working environments
would also be of interest.
Declaration of interest: The authors report no
conflicts of interest. The authors alone are responsible
for the content and writing of the paper.
References
Aasland OG, Hem E, Haldorsen T, Ekeberg Ø. 2011. Mortality
among Norwegian doctors 1960–2000. BMC Public Health
11:173.
Agerbo E, Gunnell D, Bonde JP, Mortensen PB, Nordentoft M.
2007. Suicide and occupation: The impact of socio-economic,
demographic and psychiatric differences. Psychol Med 37(8):
1131–1140.
Akiskal HS, Akiskal KK. 2005. TEMPS-A: Temperament
evaluation of Memphis, Pisa, Paris and San Diego. J Affect
Disord 85(special issue):1–242.
Akiskal HS, Placidi GF, Maremmani I, Signoretta S, Liguori A,
Gervasi R, Mallya G, Puzantian VR. 1998. TEMPS-I:
Delineating the most discriminant traits of the cyclothymic,
depressive, hyperthymic and irritable temperaments in a
nonpatient population. J Affect Disord 51(1):7–19.
Albini E, Zoni S, Parrinello G, Benedetti L, Lucchini R. 2011. An
integrated model for the assessment of stress-related risk factors
in health care professionals. Ind Health 49(1):15–23.
Alexander RE. 2001. Stress-related suicide by dentists and other
health care workers. Fact or folklore? J Am Dent Assoc 132(6):
786–794.
American Foundation for Suicide Prevention. n.d. Physician
depression and suicide prevention project, available at http://
www.afsp.org/index.cfm?page_id ¼ 05804002-E8F4-13AB-
2D4B97A0815A2744 (accessed 19 August 2007).
Augusto Landa JM, Lopez-Zafra E, Berrios Martos MP,
Aguilar-Luzon Mdel C. 2008. The relationship between
emotional intelligence, occupational stress and health in nurses:
A questionnaire survey. Int J Nurs Stud 45(6):888–901.
Baglioni AJ, Cooper CL, Hingley P. 1990. Job stress, mental health
and job satisfaction among UK senior nurses. Stress Med
6:9–20.
Bamber M, McMahon R. 2008. Danger-early maladaptive schemas
at work!: The role of early maladaptive schemas in career choice
and the development of occupational stress in health workers.
Clin Psychol Psychother 15(2):96–112.
Beck AT, Steer RA. 1989. Manual for the Beck hopelessness scale.
San Antonio, TX: The Psychological Corporation.
Beck AT, Weissman A, Lester D, Trexler L. 1974. The
measurement of pessimism: The hopelessness scale. J Consult
Clin Psychol 42(6):861–865.
P. Iliceto et al.8
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
icol
e H
arpo
le o
n 06
/07/
12Fo
r pe
rson
al u
se o
nly.

Belkic K, Nedic O. 2007. Workplace stressors and lifestyle-related
cancer risk factors among female physicians: Assessment using
the occupational stress index. J Occup Health 49(1):61–71.
Bollen KA. 1989. Structural equations with latent variables. New
York: Wiley.
Bonde JP. 2008. Psychosocial factors at work and risk of depression:
A systematic review of the epidemiological evidence.
Occup Environ Med 65(7):438–445.
Cooper CL, Baglioni AJ, Jr. 1988. A structural model approach
toward the development of a theory of the link between stress
and mental health. Br J Med Psychol 61(Pt. 1):87–102.
Cooper CL, Sloan SJ, Williams S. 1988. Occupational Stress
Indicator management guide. Windsor: NFER-Nelson.
de Smet P, Sans S, Dramaix M, Boulenguez C, de Backer G,
Ferrario M, Cesana G, Houtman I, Isacsson SO, Kittel F,
Ostergren PO, Peres I, Pelfrene E, Romon M, Rosengren A,
Wilhelmsen L, Kornitzer M. 2005. Gender and regional
differences in perceived job stress across Europe. Eur J Public
Health 15(5):536–545, Epub 2005 Jul 21.
Edwards D, Burnard P. 2003. A systematic review of stress and
stress management interventions for mental health nurses. J Adv
Nurs 42(2):169–200.
Falkum E, Vaglum P. 2005. The relationship between interpersonal
problems and occupational stress in physicians. Gen
Hosp Psychiatry 27(4):285–291.
Fowler JC. 2012. Suicide risk assessment in clinical practice:
Pragmatic guidelines for imperfect assessments. Psychotherapy
49:81–90.
Gellis ZD, Kim JC. 2004. Predictors of depressive mood,
occupational stress, and propensity to leave in older and younger
mental health case managers. Community Ment Health J 40(5):
407–421.
Hart PM, Wearing AJ. 1995. Occupational stress and well-being:
A systematic approach to research, policy and practice. In:
Cotton P, editor. Psychological health in the workplace. Victoria:
Australian Psychological Society. p 185–216.
Hart PM, Wearing AJ, Headey B. 1993. Assessing police work
experiences: Development of the police daily hassle and uplifts
scales. J Crim Justice 21:553–572.
Hawton K, Vislisel L. 1999. Suicide in nurses. Suicide Life Threat
Behav 29(1):86–95.
Hem E, GrŁnvold NT, Aasland OG, Ekeberg O. 2000. The
prevalence of suicidal ideation and suicidal attempts among
Norwegian physicians. Results from a cross-sectional survey of a
nationwide sample. Eur Psychiatry 15:183–189.
Hem E, Haldorsen T, Aasland OG, Tyssen R, Vaglum P, Ekeberg O.
2005. Suicide among physicians. Am J Psychiatry 162(11):
2199–2200.
Hu L, Bentler PM. 1998. Fit indices in covariance structure
modeling: Sensitivity to underparameterized model misspecifi-
cation. Psychol Methods 4:424–453.
Hu L, Bentler PM. 1999. Cutoff criteria for fit indexes in covariance
structure analysis: Conventional criteria versus new alternatives.
Struct Equ Modeling 6:1–55.
Joreskog KG, Goldberger AS. 1975. Estimation of a model with
multiple indicators and multiple causes of a single latent variable.
J Am Stat Assoc 70:631–639.
Kendler KS, Hettema JM, Butera F, Gardner CO, Prescott CA.
2003. Life event dimensions of loss, humiliation, entrapment,
and danger in the prediction of onsets of major depression and
generalized anxiety. Arch Gen Psychiatry 60(8):789–796.
Kinnunen-Amoroso M. 2011. Finnish occupational physicians’ and
nurses’ experience of work related stress management: A
qualitative study. Ind Health 49(6):774–778.
Knussen C, Niven CA. 1999. Neuroticism and work-related stress
in a sample of health care workers. Psychol Health 14:897–911.
Lamontagne AD, Keegel T, Louie AM, Ostry A, Landsbergis PA.
2007. A systematic review of the job-stress intervention
evaluation literature, 1990–2005. Int J Occup Environ Health
13(3):268–280.
Langballe EM, Innstrand ST, Aasland OG, Falkum E. 2011. The
predictive value of individual factors, work-related factors, and
work-home interaction on burnout in female and male
physicians: A longitudinal study. Stress Health 7(1):73–87.
Lee I, Wang HH. 2002. Perceived occupational stress and related
factors in public health nurses. J Nurs Res 10:253–260.
Mandy A, Tinley P. 2004. Burnout and occupational stress. J Am
Pod Med Ass 94(3):282–291.
Marine A, Ruotsalainen J, Serra C, Verbeek J. 2006. Preventing
occupational stress in healthcare workers. Cochrane Database
Syst Rev (4):CD002892.
McEwen B, Stellar E. 1993. Stress and the individual. Mechanisms
leading to disease. Arch Intern Med 153:2093–2101.
McEwen BS. 1998. Stress, adaptation, and disease. Allostasis and
allostatic load. Ann N Y Acad Sci 840:33–44.
McEwen BS. 2000. Allostasis and allostatic load: Implications for
neuropsychopharmacology. Neuropsychopharmacology 22:
108–124.
McNally RJ. 2003. Psychological mechanisms in acute response to
trauma. Biol Psychiatry 53:779–788.
Michie S, Williams S. 2003. Reducing work related psychological ill
health and sickness absence: A systematic literature review.
Occup Environ Med 60(1):3–9.
Moore KA, Cooper CL. 1996. Stress in mental health professionals:
A theoretical overview. Int J Soc Psychiatry 42:82–89.
Muthen B. 1989. Latent variable modeling in heterogeneous
populations. Psychometrika 54:557–585.
Myers M, Fine C. 2003. Available at http://www.medscape.com/
viewarticle/462619 Suicide in physicians: Toward prevention.
Posted: 21 October 2003. Medscape Gen Med 5(4) .
O’Connor DB, O’Connor RC, White BL, Bundred PE. 2000.
Hopelessness, stress and perfectionism: The moderating effects
of future thinking. Cogn Emot 18:1099–1120.
O’Connor RC, O’Connor DB, O’Connor SM, Smallwood J,
Miles J. 2004. The effect of job strain on British general
practitioners’ mental health. J Ment Health 9:637–654.
Oginska-Bulik N. 2006. Occupational stress and its consequences in
healthcare professionals: The role of type D personality. Int J
Occup Med Environ Health 19(2):113–122.
Pompili M. 2010. Exploring the phenomenology of suicide. Suicide
Life Threat Behav 40:234–244.
Pompili M, Ruberto A, Girardi P, Tatarelli R. 2004. Suicidality in
DSM IV cluster B personality disorders. An overview. Ann Ist
Super Sanita 40(4):475–483.
Pompili M, Rinaldi G, Lester D, Girardi P, Ruberto A, Tatarelli R.
2006. Hopelessness and suicide risk emerge in psychiatric nurses
suffering from burnout and using specific defense mechanisms.
Arch Psychiatr Nurs 20:135–143.
Pompili M, Tatarelli R, Rogers JR, Lester D. 2007. The
hopelessness scale: A factor analysis. Psychol Rep 100(2):
375–378.
Pompili M, Girardi P, Tatarelli R, Iliceto P, De Pisa E, Tondo L,
Akiskal KK, Akiskal HS. 2008. TEMPS-A (Rome): Psycho-
metric validation of affective temperaments in clinically well
subjects in mid- and south Italy. J Affect Disord 107(1–3):
63–75.
Pompili M, Iliceto P, Lester D, Innamorati M, Girardi P, Tatarelli R.
2009. Beck hopelessness scale (BHS). Firenze: Organizzazioni
Speciali.
Pompili M, Iliceto P, Milelli M, Akiskal HS, Girardi P. 2012.
Presentazione e validazione italiana. Psicoterapia Cognitiva
e Comportamentale (in press).
Rihmer A, Rozsa S, Rihmer Z, Gonda X, Akiskal KK, Akiskal HS.
2007. Affective temperament-types and suicidal behaviour. Eur
Psychiatry 22(Suppl. 1):s244.
MIMIC and job stress in health workers 9
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
icol
e H
arpo
le o
n 06
/07/
12Fo
r pe
rson
al u
se o
nly.

Ruotsalainen J, Serra C, Marine A, Verbeek J. 2008. Systematic
review of interventions for reducing occupational stress in health
care workers. Scand J Work Environ Health 34(3):169–178.
Schneiderman N, Ironson G, Siegel SD. 2005. Stress and health:
Psychological, behavioral, and biological determinants. Annu
Rev Clin Psychol 1:607–628.
Selye H. 1936. Syndrome produced by diverse nocuous agents.
Nature 138:32.
Selye H. 1974. Stress without distress. New York: New American
Library.
Selye H. 1976. Stress in health and disease. Boston, MA:
Butterworth.
Sirigatti S, Stefanile C. 2002. Occupational Stress Indicator (OSI):
The Italian Test Manual. Firenze: Organizzazioni Speciali.
Stanton JM, Balzer WK, Smith PC, Parra LF, Ironson G. 2001. A
general measure of work stress: The stress in general scale. Educ
Psychol Meas 61:866–888.
van der Doef M, Maes S. 1999. The job demand-control (-support)
model and psychological well-being: A review of 20 years of
empirical research. Work Stress 13:87–114.
van der Klink JJ, Blonk RW, Schene AH, van Dijk FJ. 2001. The
benefits of interventions for work-related stress. Am J Public
Health 91(2):270–276.
P. Iliceto et al.10
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
icol
e H
arpo
le o
n 06
/07/
12Fo
r pe
rson
al u
se o
nly.
Copyright © 2022 FDOKUMEN




















