Femorofemoral bypass grafts: Analysis of patency and factors influencing long-term outcome
Upload
independentCategory
view
0download
0
DOI: 10.1016/j.athoracsur.2006.09.053 2007;83:517-525 Ann Thorac Surg
Goldman, Ericka J. Prechtel, Richard B. Schuessler and Ralph J. Damiano, Jr Yosuke Ishii, Russell T. Kronengold, Renu Virmani, Elias A. Rivera, Scott M.
PatencyNovel Bioengineered Small Caliber Vascular Graft With Excellent One-Month
http://ats.ctsnetjournals.org/cgi/content/full/83/2/517located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2007 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on May 29, 2013 ats.ctsnetjournals.orgDownloaded from

NWYERDP
bfbrmti
mweemofglr(sn
Civrlacavpsbcc
A
PS
ABw
©P
DIO
VA
SCU
LAR
ovel Bioengineered Small Caliber Vascular Graftith Excellent One-Month Patency
osuke Ishii, MD, Russell T. Kronengold, PhD, Renu Virmani, MD,lias A. Rivera, MHS, Scott M. Goldman, MS, Ericka J. Prechtel, MS,ichard B. Schuessler, PhD, and Ralph J. Damiano Jr, MDivision of Cardiothoracic Surgery, Washington University School of Medicine, St. Louis, Missouri; Kensey Nash Corp, Exton,
ennsylvania; and American Registry of Pathology, Washington, DCtEisH9iwwca
pltistn
CA
R
Background. A bioengineered microporous polycar-onate-siloxane polyurethane graft has been developedor coronary artery bypass grafting. Biological agents cane impregnated into its absorbable collagen and hyalu-onan microstructure and stable macrostructure to pro-ote patency. The objective of this study was to examine
he biological performance and biomechanical character-stics of this graft.
Methods. Heparin-sirolimus (HS) or heparin-siroli-us–vascular endothealial growth factor (HSV) graftsere manufactured for this study. Heparin (40 U) was
mbedded in the microstructure of the graft for earlylution from the graft wall. Heparin (100 U) and siroli-us (450 �g) were incorporated into the macrostructure
f the graft for late elution. Vascular endothelial growthactor was also embedded in the microstructure of theraft. Both grafts (3.6 mm internal diameter, 24 mmength) were implanted into the abdominal aortas ofabbits (n � 36) to compare with heparin-alone (H) graftsn � 9). At 4 hours, 1 day, and 1, 2, and 4 weeks afterurgery, the grafts were removed for histologic, immu-
ohistochemical, and biomechanical evaluations.dm
nSP(cDetlaectw
arnes-Jewish Hospital Plaza, St. Louis, MO 63110; e-mail: [email protected].
2007 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
Results. The patency rate of all grafts was 100% at eachime point. None of grafts had stenosis after surgery.ndothelial cells were observed at 4 weeks after surgery
n the HS, HSV, and H grafts. Although there was noignificant difference of neointima thickness among theS, HSV, and H grafts (136 � 75, 93 � 64, and 125 �
0 �m; p � 0.08), the H grafts did have more cellularnfiltration in the graft than the HS or HSV grafts. Thereas neocapillary formation inside the graft wall at 4eeks in all grafts. The graft macrostructure was un-
hanged based on biomechanical evaluation 4 weeksfter surgery.Conclusions. A unique drug-eluting graft had excellent
atency at 1 month and may encourage luminal endothe-ialization without excessive intimal hyperplasia. Al-hough vascular endothelial growth factor did not improventimal formation, cell infiltration, or vascularization,irolimus might inhibit cell proliferation. Further long-erm study would need to evaluate the efficacy of impreg-ated sirolimus.
(Ann Thorac Surg 2007;83:517–25)
© 2007 by The Society of Thoracic Surgeonsoronary artery bypass grafting (CABG) is now per-formed routinely around the world. The autologous
nternal mammary arteries, radial artery, and saphenousein are the most widely used conduits for coronaryevascularization. These autologous grafts provide excel-ent mechanical stability and their intimae have a naturalntithrombogenicity [1, 2]. However, they require surgi-al harvest procedures, are of variable quality and size,nd are limited by availability in some cases. Saphenousein conduits have the added disadvantage of relativelyoor long-term patency [3]. There would be severalignificant advantages if an effective synthetic graft coulde developed. It would have unlimited availability, andonsistent quality and patency. Moreover, the biome-hanical uniformity of a synthetic graft may allow for the
ccepted for publication Sept 7, 2006.
resented at the Poster Session of the Forty-first Annual Meeting of Theociety of Thoracic Surgeons, Tampa, FL, Jan 24–26, 2005.
ddress correspondence to Dr Damiano, Suite 3108, Queeny Tower,
evelopment of effective anastomotic devices for mini-ally invasive surgery.Unfortunately, satisfactory synthetic materials have
ot been developed in a size appropriate for CABG.ynthetic materials such as Dacron (C. R. Bard, Haverhill,ennsylvania) or expanded polytetrafluoroethylene
ePTFE) have been used successfully in peripheral revas-ularization but failed in coronary revascularization [4].acron grafts lead to thrombosis and neointimal thick-
ning in low blood flow. The ePTFE grafts also fail owingo surface thrombogenicity for small vessels [5]. Endothe-ial cell seeded grafts might be more effective for antico-gulation compared with nonseeded grafts [6, 7]. How-ver, the manufacturing process is complex, timeonsuming, and costly. Planned surgery is required forhis graft, but CABG is usually performed emergently,ithout such lengthy planning time.
Dr Kronengold and Mr Goldman disclose thatthey have a financial relationship with Kensey Nash
Corp.0003-4975/07/$32.00doi:10.1016/j.athoracsur.2006.09.053
by on May 29, 2013 als.org

ttbnha
acataTpn
M
GTwmpfPdmopcfltppt(hrcamd
iith
hggpcpmgmtgs
T
G
01
2
3
4
F rous m
518 ISHII ET AL Ann Thorac SurgBIOENGINEERED SMALL CALIBER GRAFT 2007;83:517–25
CA
RD
IOV
ASC
ULA
R
A synthetic small caliber graft should be resistant tohrombosis and biocompatible, resembling a native ar-ery. The graft should have excellent biomechanical sta-ility, and be able to withstand the long-term hemody-amic stress of the arterial circulation. Suturability andandling are also important factors in minimizing oper-tive time and risk.Our group has developed a microporous polycarbon-
te-siloxane polyurethane graft that incorporates solubleollagen and hyaluronic acid into the pores. Biologicalgents can be impregnated into the stable macrostruc-ure and absorbable microstructure of the graft, creating
two-tiered drug-release system to promote patency.he objective of this study was to examine the biologicalerformance and biomechanical characteristics of thisew graft.
aterial and Methods
raft Materialsest samples consisted of a small-caliber vascular graftith an internal diameter of 3.6 mm and a length of 24m. A porous tube consisting of polycarbonate-siloxane
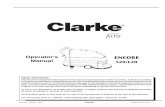
olyurethane was manufactured using proprietary PTMoaming technology (Kensey Nash Corporation, Exton,ennsylvania). This process created a tube with a largeistribution of interconnected pores, averaging approxi-ately 25 �m in diameter (Fig 1). The “macrostructure”
f this graft was designed to provide biomechanicalroperties comparable to native arteries, and allow forellular in-growth while producing minimal tissue in-ammatory response. The macrostructure also func-
ioned as a vehicle for delivery of biological agents, androved amenable to easy handling and suturing. Incor-orated into the pores of the polyurethane macrostruc-
ure was a “microstructure” consisting of hyaluronanLifeCore Biomedical, Chaska, Minnesota) and bovineide-derived acid-soluble collagen (Kensey Nash Corpo-ation). The microstructure was intended to create aell-friendly environment to encourage cell attachmentnd proliferation, prevent leakage through the porousacrostructure, and provide a secondary vehicle for the
ig 1. The synthetic small caliber graft with a bioengineered micropo
elivery of biological agents. Biological agents can be
ats.ctsnetjournDownloaded from
ncorporated into the vascular grafts during manufactur-ng with a goal of preventing short- and long-termhrombosis as well as chronic smooth muscle cellyperplasia.In this study, three types of graft were manufactured:
eparin-alone (H) grafts; heparin and sirolimus (HS)rafts; and heparin, sirolimus and vascular endothelialrowth factor (VEGF [HSV]) grafts. All grafts were im-regnated with 40 U heparin (Celsus Laboratories, Cin-innati, Ohio) in the microstructure for early elution torevent acute graft thrombosis and 100 U heparin in theacrostructure for prevention of late thrombosis. The HS
raft was impregnated with 450 �g sirolimus in theacrostructure for prolonged elution to discourage late
hrombosis and inhibit intimal hyperplasia. The HSVrafts also incorporated 450 �g sirolimus in the macro-tructure, and 650 ng VEGF (VEGF165; Peprotech, Rocky
able 1. Definition of Histologic Grading
rade Definition
(none) Not present or not appreciable.(minimal) Fibrin/platelet aggregation; or cellular
infiltration is present in or less than1/4 the thickness of the graftconduit wall; or 1/4 the cross-sectional luminal surface isendothelialized.
(mild) Fibrin/platelet aggregation; or cellularinfiltration is present in or equals1/2 the thickness of the graftconduit wall; or 1/2 the cross-sectional luminal surface isendothelialized.
(moderate) Fibrin/platelet aggregation; or cellularinfiltration is present in or equals3/4 the thickness of the graftconduit wall; or 3/4 the cross-sectional luminal surface isendothelialized.
(severe/marked) Fibrin/platelet aggregation; or cellularinfiltration present throughout thefull thickness of the graft conduitwall; or 4/4 the cross-sectional
atrix that did not contain cells and required no preclotting.
luminal surface is endothelialized.
by on May 29, 2013 als.org

Hesdtpmaas5
SA“t“
pltCi
taiccwleawgRsclai
dgtwhat
F
Fs
519Ann Thorac Surg ISHII ET AL2007;83:517–25 BIOENGINEERED SMALL CALIBER GRAFT
CA
RD
IOV
ASC
ULA
R
ill, New Jersey) within the microstructure to encouragendothelialization of the graft. All grafts were terminallyterilized by exposure to gamma radiation at a minimumose of 25 kGy. The drug delivery profile of heparin in
he graft was assessed in vitro by exposing the grafts tohosphate buffer solution at 37°C and 100 revolutions perinute (rpm) in an incubator-shaker over 40 days. Hep-
rin was quantified using a dimethylmethylene bluessay (DMMB) to determine eluted concentration inolution spectrophotometrically at a wavelength of25 nm.
urgical Procedurell animals received humane care in compliance with the
Principles of Laboratory Animal Care,” formulated byhe National Society for Medical Research, and theGuide for the Care and Use of Laboratory Animals,”
ig 2. The percentage of heparin eluted from the graft (in vitro).
ig 3. Explanted heparin-sirolimus (HS) (top) and heparin-sirolimus
tenosis at the anastomotic sites and center of the grafts.ats.ctsnetjournDownloaded from
repared by the National Academy of Science and pub-ished by the National Institutes of Health (NIH Publica-ion 86-23, revised 1985). In addition, the Animal Studiesommittee of the Washington University School of Med-
cine approved this study protocol.Forty-five New Zealand White rabbits weighing be-
ween 3 and 4 kg were used randomly in this study. Allnimals were anesthetized with ketamine (70 mg/kg)ntramuscularly, intubated with a 3-mm cuffed endotra-heal tube, and mechanically ventilated with a pressure-ontrolled ventilator. An adequate level of anesthesiaas maintained by inhaled isoflurane (1% to 3%). A
imb-lead electrocardiogram was monitored. A centralar artery catheter was inserted to monitor systemicrterial pressure continuously. Arterial blood samplesere drawn every 30 minutes to determine arterial oxy-en tension, acid-base balance, and electrolyte levels.inger’s lactate solution was infused continuously, andodium bicarbonate, potassium chloride, and calciumhloride were supplemented to maintain pH and electro-ytes within normal values. Enrofloxacin (5 mg/kg) wasdministrated preoperatively to reduce the risk ofnfection.
After a midline abdominal incision, the intestines wereisplaced to the right side and covered with moistenedauze. The infrarenal aorta was carefully dissected fromhe surrounding tissue. The lumbar arterial branchesere spared to avoid spinal cord ischemia. Intravenouseparin (200 U/kg) was administered. The abdominalorta was clamped by microapproximator clamps be-ween the lumbar branches and transected. The H, HS, or
lar endothelial growth factor (HSV) (bottom) grafts. There was no
vascuby on May 29, 2013 als.org

HeT(aYwp5d(
(tkofitdpcaT4a
BG
aaalvtPucicairtdtetwG
tgasst2wfw
lse
HGtgtetcAncca
RapdbbtptYDt
Ftar
520 ISHII ET AL Ann Thorac SurgBIOENGINEERED SMALL CALIBER GRAFT 2007;83:517–25
CA
RD
IOV
ASC
ULA
R
SV grafts were anastomosed to the aorta in an end-to-nd fashion with a continuous 7-0 polypropylene suture.he total anastomosis time was less than 30 minutes
22 � 3) in every animal. Blood flow was measured withn ultrasonic flow probe (Transonic System, Ithaca, Nework) proximally and distally. The abdominal incisionas closed. The animals received analgesia (buprenor-hine 0.3 to 0.5 mg/kg) and antibiotic (enrofloxacinmg/kg) treatments subcutaneously twice daily for 2
ays postoperatively. Postoperative antiplatelet therapyaspirin 15 mg/kg) was administered daily.
At 4 hours, 1 day, and 1, 2, and 4 weeks after surgeryn � 3, 3, 3, 4, and 5, respectively, for HS and HSV grafts),he animals were anesthetized again with intramuscularetamine (70 mg/kg). The abdominal incision was re-pened. The surgical site was examined for adhesions,brosis, postoperative bleeding or hematoma, and aor-
ovenous fistula. The blood flow at the proximal andistal anastomoses was measured with an ultrasonic flowrobe. The animal was euthanized, and the graft wasarefully removed for biomechanical characterization,nd histologic and immunohistochemical evaluations.he animals implanted with H graft were euthanized atweeks after surgery (n � 9) to compare data with the HSnd HSV grafts.
iomechanical CharacterizationRAFT COMPLIANCE TEST. The graft was removed from theorta, leaving approximately 1 cm intact aorta proximallynd distally. Both ends of the graft were tied securely tocustomized fixture designed to hold the sample at a set
ength. A pressure gauge (Digimano 1000; Netech, Hicks-ille, NY) was inserted in-line at the downstream end ofhe graft, while a calibrated repeat pipettor (Repeaterlus; Eppendorf, Westbury, NY) was placed in-line in thepstream end of the graft. Static, internal, and volumetricompliances were determined by increasing fluid volumencrementally and recording pressure. Percent radialompliance was calculated using the formula: % Compli-nce � (R � R0)/�P � 100, where R � graft radius, R0 �nitial graft radius, and �p � pressure changes. Internaladius was calculated from the volume with the assump-ion that the length remained constant. To obtain arterialata for comparison, porcine carotid arteries were ob-
ained from a local butcher on the day of sacrifice andxcess tissue was dissected free. Compliance testing onhree normal porcine carotid arteries was performedithin 24 hours of animal sacrifice.
RAFT TENSILE STRENGTH TEST. After grafts were removed,wo 5-mm segments were cut from the midportion of theraft for tensile strength testing. Graft thickness, length,nd outer diameter of each segment were carefully mea-ured. Two dowel pins were inserted within each 5-mmample and secured with custom fixtures to a Chatillonest stand (Model TCD200; Chatillon, Largo, FL) and-pound load cell (Model DFGS 2; Chatillon). The pinsere then pulled apart at a rate of 50 mm/min. Maximum
orce was recorded and ultimate tensile strength (UTS)
as calculated as: UTS � Max Load/(2 � thickness � gats.ctsnetjournDownloaded from
ength). To obtain arterial data for comparison, tensiletrengths of the thoracic arteries obtained from theuthanized rabbits (n � 18) were measured.
istologic and Immunohistochemical Evaluationsraft patency, neointima formation, endothelialization of
he graft, and tissue ingrowth and angiogenesis in theraft wall were examined histologically and immunohis-ochemically. The explanted graft was fixed in 10% buff-red formalin. Longitudinal and transverse sections fromhe proximal and distal anastomoses and through theenter of the graft were obtained for tissue processing.ll sections were dehydrated in a graded series of etha-ol and embedded in paraffin. The paraffin blocks wereut at 4 to 6 �m, and the sections were mounted on aharged glass slide and stained with hematoxylin-eosin,nd movat pentachrome.Immunohistochemical studies were performed for
am-11, von Willebrand factor (vWF), and �-actin. Dew-xed paraffin sections were treated with 0.3% hydrogeneroxide for 20 minutes to inactivate endogenous peroxi-ases. The sections were then immersed in protein-freelock (Dako, Carpinteria, California) for 10 minutes tolock non-specific binding of primary antibodies. Sec-
ions were incubated for 1 hour at room temperature withrimary antibodies against human smooth muscle �-ac-
in (clone HHF35, dilution 1:20; Enzo, Farmingdale, Nework), the macrophage marker Ram11 (dilution 1:200;ako), and a purified polyclonal antibody to vWF (dilu-
ion 1:2000; Strategic Biosolutions, Newark, Deleware).
ig 4. (A) Graft compliance at preoperative (white) and postopera-ive phase (black). (B) Graft tensile strength at preoperative (white)nd postoperative phase (black). (H � heparin alone; HS � hepa-in-sirolimus; HSV � heparin-sirolimus vascular endothelial
rowth factor.)by on May 29, 2013 als.org

adaew
agsdgg
SAcMvuo
R
A
521Ann Thorac Surg ISHII ET AL2007;83:517–25 BIOENGINEERED SMALL CALIBER GRAFT
CA
RD
IOV
ASC
ULA
R
The labeling of primary antibodies was achieved withn anti-mouse biotinylated link antibody from a peroxi-ase-based kit (LSAB; Dako). Positive staining (rose re-ction product) was visualized using a 3-amino-9-thylcarbazole substrate-chromogen system; the sectionsere counterstained with Gill’s hematoxylin.Luminal surface fibrin/platelet aggregation, endotheli-
lization, and cellular infiltration of the grafts wereraded from grade 0 to 4. The definition of the grade ishown in Table 1. Histological index was calculated byividing the sum of the grade by the number of samplerafts (grade/n) at the anastomotic sites and center of the
rafts. sats.ctsnetjournDownloaded from
tatistical Analysisll continuous values were expressed as mean � 1 SD. The
ontinuous variables were compared by an unpaired t test.ultigroup data were compared using the analysis of
ariance mode. Post hoc multiple comparisons were madesing Fisher’s least significant difference technique. A valuef p less than 0.05 was considered statistically significant.
esults
ll rabbits in groups H, HS, and HSV survived after
Fig 5. Serial change of endothelialization(top) and cellular infiltration (bottom) atanastomotic sites and center of the grafts. (A)Percentage of grafts that had endothelializa-tion or cellular infiltration. (B) Histologic in-dex, which was calculated by dividing thesum of the grade by the number of samplegrafts (grade/n). (Open bars � anastomosissite; hatched bars � center of graft.)
urgery. Paraplegia was not observed in any animals
by on May 29, 2013 als.org

dcveoa4
RTptpmiiflt(00
ealggmasg
BG
FmaewIctstw0aF2pg0G
wppags0sp
Fd4oscafCt
Fdtag
522 ISHII ET AL Ann Thorac SurgBIOENGINEERED SMALL CALIBER GRAFT 2007;83:517–25
CA
RD
IOV
ASC
ULA
R
uring the postoperative period in all groups. The per-entage of heparin eluted from the grafts based on the initro study is shown in Figure 2. Sixty percent of heparinluted within 1 day after soaking in the bath. Almost 80%f heparin eluted from the grafts within first the 10 daysfter soaking. Heparin continued eluting for at least0 days.
heological Data and Graft Morphologyhere were no significant differences in blood flow at theroximal and distal anastomoses after the initial implan-
ation and postoperatively in all groups. Blood flow at theroximal and distal anastomoses was 42 � 21 and 44 � 18L/min in group H (p � 0.9), 37 � 18 and 32 � 18 mL/min
n group HS (p � 0.4), and 43 � 24 and 40 � 22 mL/minn group HSV (p � 0.7) after initial implantation. Bloodow at the proximal and distal anastomoses before eu-
hanasia was 39 � 11 and 36 � 16 mL/min in group Hp � 0.6), 36 � 15 and 31 � 13 mL/min in group HS (p �.4), and 50 � 21 and 42 � 17 mL/min in group HSV (p �.3) at each postoperative time point.The patency rate of all grafts was 100% (45 of 45) at
ach time point. Although the grafts were covered by andhesion capsule, there was no stenosis observed histo-ogically at the proximal or distal anastomoses in anyroups (Fig 3). There were no apparent changes in theraft, including dilatation, dehiscence, or aneurysm for-ation in any of the grafts during the 4-week postoper-
tive period. None of the grafts was collapsed owing tourrounding tissue. There was no bleeding from therafts, and no arteriovenous fistulae formation.
ig 6. Histology and immunohistochemicalata of the heparin-sirolimus (HS) grafts atweeks. Moderate cellular infiltration was
bserved in the graft wall in hematoxylin-eo-in (H-E) stain. Normal-appearing endothelialells were aligned with the blood flow (right:rrows). There was moderate neocapillaryormation in the graft wall (left: arrows).lumps of red blood cells were observed inside
he neocapillaries.
ig 7. Histology and immunohistochemicalata of the heparin-sirolimus vascular endo-helial growth factor grafts at 4 weeks. Moder-te cellular infiltration was observed in theraft wall in hematoxylin-eosin (H-E) stain.
ats.ctsnetjournDownloaded from
iomechanical CharacterizationRAFT COMPLIANCE. The graft compliance data are shown inigure 4A. The H graft compliance between 80 and 120m Hg was 7.4% � 2.4% and 8.5% � 1.6% preoperatively
nd postoperatively, respectively (p � 0.55). The preop-rative and postoperative compliance of the HS graftsas 3.6% � 1.1% and 5.9% � 2.7%, respectively (p � 0.23).
n the HSV grafts, the preoperative and postoperativeompliance was 6.1% � 2.2% and 11.0% � 2.2%, respec-ively (p � 0.02). The postoperative graft compliance wasignificantly higher than the preoperative compliance inhe HSV grafts. Although the preoperative complianceas not different among the H, HS, and HSV grafts (p �
.13), there was a statistical significance in the postoper-tive compliance among the three grafts (p � 0.001).resh porcine carotid artery compliance was 9.4% �.2%. There was no significant difference between theorcine carotid arterial compliance and the postoperativeraft compliance of the H, HS, and HSV grafts (p � 0.6,.1, and 0.4, respectively).RAFT TENSILE STRENGTH. The tensile strength of the H graftas 490 � 77 and 690 � 99 kPa preoperatively andostoperatively (p � 0.002; Fig 4B). The preoperative andostoperative HS graft tensile strength was 468 � 75nd 354 � 77 kPa respectively (p � 0.01). In the HSVrafts, the preoperative and postoperative graft tensiletrength was 443 � 86 and 515 � 82 kPa respectively (p �.17). The HSV grafts had higher postoperative tensiletrength than the HS grafts (p � 0.01). Although thereoperative tensile strength was not different among the
by on May 29, 2013 als.org

Hstd4H
HAstHstslamggects
enes2tiaBa
staepaeol(Ht7(imgpt
elot
1n(csot
C
SaiaAgdwtbte
ftogrt[tttceeienHiaisHpa
igftfuttmwV
523Ann Thorac Surg ISHII ET AL2007;83:517–25 BIOENGINEERED SMALL CALIBER GRAFT
CA
RD
IOV
ASC
ULA
R
, HS, and HSV grafts (p � 0.50), there was a statisticalignificance in the postoperative tensile strength amonghe three grafts (p � 0.001). The tensile strength of theescending thoracic aorta was measured to be 1,436 �50 kPa, which was significantly higher than that of the, HS, and HSV grafts (p � 0.001).
istologic Evaluationsll the H, HS, and HSV grafts were patent and had no
tenoses histologically during the 4-week follow-up. Inhe early postoperative period (4 hours and 1 day) in the
S and HSV grafts, all grafts were covered with luminalurface fibrin. The graft wall was predominantly infil-rated by red blood cells and aggregates of platelets withome leukocytes. At 1 week after implantation, a thinayer of luminal surface fibrin with platelet aggregationnd inflammatory cells was observed in all grafts withinimal to mild cellular infiltration (grade 2) within the
rafts and neutrophil cell infiltration in the walls of bothraft groups. There were no significant histologic differ-nces between the HS and HSV grafts after 1 week. Serialhanges of graft luminal surface fibrin/platelet aggrega-ion, endothelialization, and cellular infiltration arehown in Figure 5A and B.
At 2 weeks, a layer of spindle-shaped, immature mes-nchymal cells covered the anastomotic site from theative aorta in the HS grafts, with occasional patches ofndothelial cells (grade 1). However, the HSV graftshowed no endothelialization in the anastomosis sites atweeks. There was no endothelialization in the midpor-
ion of any HS or HSV grafts. Mild inflammatory cellsnfiltrated into the pores in one-third of all the grafts,long with spindle-shaped cells in both graft groups.oth HS and HSV graft macrostructures appeared intactt 2 weeks.At 4 weeks after implantation, the HS and HSV grafts
howed a thin neointima with elongated endothelial cellshat extended smoothly into the adjacent graft from thenastomotic site. The presence of a functional layer ofndothelial cells was confirmed using vWF. Sixty-sevenercent of the HS grafts had endothelialization at thenastomotic sites and the graft midportion (Fig 6). How-ver, the HSV grafts did not show any endothelializationn the graft midportion despite the presence of endothe-
ial cells at the anastomosis sites in 67% of the graftsFig 7). There was no excessive intimal hyperplasia in any
S or HSV grafts. The average neointimal thickness athe region of anastomotic sites at 4 weeks was 136 �5 �m in the HS grafts and 93 � 64 �m in the HSV graftsp � 0.1). There were moderate neocapillary formationsnside the graft wall in the HS and HSV grafts. The graft
acrostructure appeared unchanged at 4 weeks in allrafts. Vascular endothelial growth factor did not im-rove intimal formation, cell infiltration, or vasculariza-
ion when compared with sirolimus only.All H grafts at 4 weeks had minimal neointima thick-
ning, surface thrombosis (fibrin/platelet), and endothe-ialization inside the graft. Graft endothelialization wasbserved at the anastomosis sites and center in 100% of
he grafts. The neointimal thickness of the H grafts was iats.ctsnetjournDownloaded from
25 � 90 �m. There was no significant difference ofeointima thickness among the H, HS, and HSV grafts
p � 0.08). However, the H grafts had moderate-severeellular infiltration (100%, grade 3 to 4) at the anastomosisites and center of the graft, which was more than the HSr HSV grafts. Neocapillary formation was observed inhe H grafts as in the HS and HSV graft.
omment
ynthetic small-caliber grafts will require patency equiv-lent to that of autologous arterial vessels. Bioengineer-ng innovations have enabled the seeding of endothelialnd smooth muscle cells onto synthetic grafts [6–9].lthough a seeded graft worked well experimentally,raft preparation was time consuming and technicallyifficult. If a synthetic graft had good endothelializationithout any seeding, it would be more practical to use
han a seeded graft. In the present study, this novelioengineered synthetic graft had a 100% patency rate in
he H, HS, and HSV grafts at 1 month. It had goodndothelialization 4 weeks after implantation.Synthetic small caliber grafts have not been practical
or CABG because of their poor patency rate. Grafthrombosis and intimal hyperplasia are the major causef graft failure. Studies have shown that heparin-coatedrafts prevent thrombogenicity compared with nonhepa-in-coated grafts [10, 11]. There are conflicting studies onhe beneficial effect of heparin on intimal hyperplasia10–14]. Animal and clinical studies have demonstratedhat the local delivery of sirolimus inhibits the prolifera-ion of smooth muscle cells and reduces neointimalhickening [15–18]. The graft used in the present studyontained drugs within the graft wall. Heparin wasmbedded in the microstructure of the graft for earlylution from the graft wall. Heparin and sirolimus werencorporated into the macrostructure of the graft for latelution from the graft wall. No thrombosis or excessiveeointima hyperplasia was observed in the H, HS, andSV grafts after 4 weeks. Although there was no signif-
cant difference in neointimal thickness among the H, HS,nd HSV grafts, the H grafts had more cellular infiltrationn the graft wall than the HS and HSV grafts. That mayuggest that sirolimus helped to inhibit cell proliferation.owever, the role of impregnated drugs in the long-termrevention of these complications remains unknown,nd will require further chronic studies.The HSV grafts did not improve intimal formation, cell
nfiltration, or vascularization compared with the HSrafts in this study. There could be two possible reasonsor this. First, the high blood flow rates encountered inhe aortic circulation might have caused VEGF to eluterom the microstructure too quickly for adequate cellularptake to occur, thus obviating any stimulation of endo-
helialization. The impregnated drug in the microstruc-ure begins eluting following graft implantation. Because
ost drugs were eluted from the graft microstructureithin the first 10 days (Fig 2), only a small amount ofEGF should have remained when cells started infiltrat-
ng into the micropores of the graft. In addition, the graft
by on May 29, 2013 als.org

mieoat
etntttlDpcfaThtf
rhuihtsTbotohpcpca
arohcTai4tachhtls
tpccwchrsbhwtttc
STbwtpdHboie
WTDWtA
R
524 ISHII ET AL Ann Thorac SurgBIOENGINEERED SMALL CALIBER GRAFT 2007;83:517–25
CA
RD
IOV
ASC
ULA
R
acrostructure itself supplies a scaffold for endothelial-zation and cellular infiltration. The HS grafts had goodndothelialization and cellular infiltration without VEGFr any cell-seeding process. Therefore, the benefit ofdding VEGF to the scaffold might be overshadowed byhe advantages of the scaffold itself.
There are several hypotheses on the source of thendothelial cells found inside the graft [19]. First, endo-helial cells may have migrated into the graft from theormal endothelium at both anastomotic sites. Second,
he source for the endothelial cells may have been fromhe circulating blood. Third, the source may be transin-erstitial ingrowth of either multipotent cells or endothe-ial cells from neocapillaries in the porous graft wall.etermining the source of the endothelialization is im-ortant in creating an efficacious graft that can be usedlinically. If endothelial cells inside the graft come onlyrom the anastomotic sites, the synthetic graft may havelimited graft length that reduces its clinical availability.his study demonstrated that the H, HS, and HSV graftsad neocapillary formation within 4 weeks after implan-
ation. Early neocapillary formation should be beneficialor graft endothelialization.
Polyurethanes have been used extensively as biomate-ials due to their desirable physical properties, such asigh tensile strength and elasticity [20]. However, poly-rethanes historically have had limited use in long-term
mplants owing to degradation. Polyester polyurethanesave been found to be susceptible to hydrolysis through
he ester linkage, while polyether polyurethanes werehown to be vulnerable to oxidative cleavage in vivo [21].he incorporation of polydimethylsiloxane and polycar-onate into the polymer backbone instead of polyetherr polyester segments has been shown to improvehe resistance of the material to both hydrolytic andxidative degradation [22]. Polycarbonate polyurethanesave been found to be more stable than traditionalolyurethanes against chronic biodegradation and stressracking [23]. The polyurethane used in this study is aolycarbonate and polydimethylsiloxane polyurethaneopolymer, which should enable it to resist degradationnd function as a long-term implantable vascular graft.Human saphenous vein and ePTFE graft compliance
re known to be 2.0% and 1.0% at 80 to 120 mm Hg,espectively [24, 25]. The postoperative graft compliancef the H, HS, and HSV grafts was higher than that ofuman saphenous vein or ePTFE grafts, and not signifi-antly different from that of the porcine carotid artery.herefore, the graft compliance of each graft was accept-ble for a synthetic graft. Although the graft compliancen this study was not significantly changed during the-week study period in the H and HS grafts, postopera-ive compliance of the HSV grafts increased significantlyfter surgery. The tensile strength of each graft was notonsistent during the 4-week study period. This mayave been caused by the degradation of the collagen/yaluronan microstructure, the infiltration of cells into
he graft, the normal variability of the materials, or theimited sample size. Histologic data showed the graft
tructure was still changing as cellular infiltration intoats.ctsnetjournDownloaded from
he pores of the grafts was observed over the 4-weekeriod while the microstructure degraded. The graftompliance and tensile strength will likely continue tohange as the graft becomes completely incorporatedith the host. The H grafts, which had much more
ellular infiltration at 4 weeks than the HS or HSV graft,ad higher tensile strength. Once the process of graftemodeling is completed, the conduit could reach atable condition in which its mechanical properties willecome equivalent over time. There was no visual oristological evidence to suggest that the macrostructureas degrading during the 4 weeks, so we conclude that
he microstructure is primarily responsible for the fluc-uations in the biomechanical stability of graft. A long-erm study is currently being conducted to evaluate serialhanges in the graft biomechanical stability.
tudy Limitationshis study was a preliminary evaluation of a novelioengineered synthetic small caliber graft. Since graftsere examined for histology and biomechanical proper-
ies at several different time points, the number of im-lanted grafts at each time point was small. However,ata of each time point were similar and consistent. The
grafts were evaluated at only 4 weeks after surgery toe compared with the HS and HSV grafts. Histologic dataf the H grafts revealed the effect of sirolimus on cellular
nfiltration. A longer term study is needed to evaluate thefficacy of the eluted drugs.
e acknowledge the excellent technical assistance of P. Dianeoeniskoetter, Kathryn L. Cook, Naomi R. Still, Geneva R. Baca,ina Harilal, Timothy Ringeisen, Louis Sessa, James Hill, andilliam Maas. We also thank Dawn G. Schuessler for prepara-
ion of the manuscript. This research was supported by the NISTdvanced Technology program (Award no. 70NANB1H3032).
eferences
1. Angelini GD, Newby AC. The future of saphenous vein as acoronary artery bypass conduit. Eur Heart J 1989;10:273–80.
2. Cameron A, Davis KB, Green G, Schaff HV. Coronary bypasssurgery with internal-thoracic-artery grafts—effects on sur-vival over a 15-year period. N Engl J Med 1996;334:216–9.
3. Loop FD, Lytle BW, Cosgrove DM, et al. Influence of theinternal-mammary-artery graft on 10-year survival andother cardiac events. N Engl J Med 1986;314:1–6.
4. Jones DN, Rutherford RB, Ikezawa T, Nishikimi N, IshibashiH, Whitehill TA. Factors affecting the patency of small-caliber prostheses: observations in a suitable canine model.J Vasc Surg 1991;14:441–8.
5. Esquivel CO, Blaisdell FW. Why small caliber vascular graftsfail: a review of clinical and experimental experience and thesignificance of the interaction of blood at the interface. J SurgRes 1986;41:1–15.
6. Pasic M, Muller-Glauser W, von Segesser LK, Lachat M,Mihaljevic T, Turina MI. Superior late patency of small-diameter Dacron grafts seeded with omental microvascularcells: an experimental study. Ann Thorac Surg 1994;58:677–83.
7. Laube HR, Duwe J, Rutsch W, Konertz W. Clinical experi-ence with autologous endothelial cell-seeded polytetrafluo-
roethylene coronary artery bypass grafts. J Thorac Cardio-vasc Surg 2000;120:134–41.by on May 29, 2013 als.org

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
525Ann Thorac Surg ISHII ET AL2007;83:517–25 BIOENGINEERED SMALL CALIBER GRAFT
CA
RD
IOV
ASC
ULA
R
8. Dunn PF, Newman KD, Jones M, et al. Seeding of vasculargrafts with genetically modified endothelial cells. Secretionof recombinant TPA results in decreased seeded cell reten-tion in vitro and in vivo. Circulation 1996;93:1439–46.
9. Niklason LE, Gao J, Abbott WM, et al. Functional arteriesgrown in vitro. Science 1999;284:489–93.
0. Walpoth BH, Rogulenko R, Tikhvinskaia E, et al. Improve-ment of patency rate in heparin-coated small syntheticvascular grafts. Circulation 1998;98(19 Suppl):II319–23.
1. Lin PH, Chen C, Bush RL, Yao Q, Lumsden AB, Hanson SR.Small-caliber heparin-coated ePTFE grafts reduce plateletdeposition and neointimal hyperplasia in a baboon model.J Vasc Surg 2004;39:1322–8.
2. Kiesz RS, Buszman P, Martin JL, et al. Local delivery ofenoxaparin to decrease restenosis after stenting: results ofinitial multicenter trial. Polish-American Local Lovenox NIRAssessment study (the POLONIA study). Circulation 2001;103:26–31.
3. Welt FG, Woods TC, Edelman ER. Oral heparin preventsneointimal hyperplasia after arterial injury: inhibitory po-tential depends on type of vascular injury. Circulation 2001;104:3121–4.
4. Esquivel CO, Bjorck CG, Bergentz SE, et al. Reduced throm-bogenic characteristics of expanded polytetrafluoroethyleneand polyurethane arterial grafts after heparin bonding.Surgery 1984;95:102–7.
5. Marx SO, Jayaraman T, Go LO, Marks AR. Rapamycin-FKBPinhibits cell cycle regulators of proliferation in vascularsmooth muscle cells. Circ Res 1995;76:412–7.
6. Burke SE, Lubbers NL, Chen YW, et al. Neointimal forma-tion after balloon-induced vascular injury in Yucatan minip-igs is reduced by oral rapamycin. J Cardiovasc Pharmacol
1999;33:829–35.ats.ctsnetjournDownloaded from
7. Gallo R, Padurean A, Jayaraman T, et al. Inhibition of intimalthickening after balloon angioplasty in porcine coronaryarteries by targeting regulators of the cell cycle. Circulation1999;99:2164–70.
8. Morice MC, Serruys PW, Sousa JE, et al, for the RAVELStudy Group. Randomized study with the sirolimus-coatedBx velocity balloon-expandable stent in the treatment ofpatients with de novo native coronary artery lesions. Arandomized comparison of a sirolimus-eluting stent with astandard stent for coronary revascularization. N Engl J Med2002;346:1773–80.
9. Greisler HP. Arterial regeneration over absorbable prosthe-ses. Arch Surg 1982;117:1425–31.
0. Brothers TE, Stanley JC, Burkel WE, Graham LM. Small-caliber polyurethane and polytetrafluoroethylene grafts: acomparative study in a canine aortoiliac model. J BiomedMater Res 1990;24:761–71.
1. Schubert MA, Wiggins MJ, Schaefer MP, Hiltner A, Ander-son JM. Oxidative biodegradation mechanisms of biaxiallystrained poly(etherurethane urea) elastomers. J BiomedMater Res 1995;29:337–47.
2. Hergenrother RW, Yu XH, Cooper SL. Blood-contactingproperties of polydimethylsiloxane polyurea-urethanes.Biomaterials 1994;15:635–40.
3. Eberhart A, Zhang Z, Guidoin R, et al. A new generation ofpolyurethane vascular prostheses: rara avis or ignis fatuus?J Biomed Mater Res 1999;48:546–58.
4. Sawyer P. Modern vascular grafts. New York: McGraw-Hill,1987:326.
5. Conklin BS, Richter ER, Kreutziger KL, Zhong DS, Chen C.Development and evaluation of a novel decellularized vas-
cular xenograft. Med Eng Phys 2002;24:173–83.by on May 29, 2013 als.org

DOI: 10.1016/j.athoracsur.2006.09.053 2007;83:517-525 Ann Thorac Surg
Goldman, Ericka J. Prechtel, Richard B. Schuessler and Ralph J. Damiano, Jr Yosuke Ishii, Russell T. Kronengold, Renu Virmani, Elias A. Rivera, Scott M.
PatencyNovel Bioengineered Small Caliber Vascular Graft With Excellent One-Month
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/83/2/517including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/83/2/517#BIBL
This article cites 24 articles, 9 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/83/2/517#otherarticles
This article has been cited by 1 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/coronary_disease Coronary disease
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on May 29, 2013 ats.ctsnetjournals.orgDownloaded from
Copyright © 2022 FDOKUMEN