
Noninvasive quantitative evaluation of coronary artery stent patency using 64-row multidetector...
9
Review Article Noninvasive quantitative evaluation of coronary artery stent patency using 64-row multidetector computed tomography Murrad J. Abdelkarim, MD a, * , Naser Ahmadi, MD a , Ambarish Gopal, MD a , Yasmin Hamirani, MD a , Ronald P. Karlsberg, MD, FACP, FACC b , Matthew J. Budoff, MD, FACC a a Department of Medicine, Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, 1000 West Carson Street, Box 400, Torrance, CA 90509, USA and b Cardiovascular Medical Group, Beverly Hills, CA, USA KEYWORDS: 64-row multidetector computed tomography (MDCT); Cardiac computed tomographic angiography (CTA); Computed tomography (CT) density; Coronary stent patency; In-stent restenosis (ISR) BACKGROUND: Many studies have used multidetector computed tomography (MDCT) angiography to evaluate coronary stents qualitatively but not quantitatively. OBJECTIVES: This study sought to validate a method of quantitatively evaluating stent patency by using 64-row compared with invasive coronary angiography (ICA) and to evaluate the stent size thresh- old of MDCT in detecting stent patency. METHODS: Stented lesions (n 5 122) in 55 patients (age, 65 6 10 years; 90% men) who underwent both 64-row MDCT and ICA were studied. Density measurements in Hounsfield units (HUs) and stent diameters in millimeters were recorded in the stented segments, with the density of the ascending aorta (AO) taken as a reference. The ratio of the average of stent’s proximal, middle, and distal densities to mean AO density was defined as the AS/AO HU. Threshold values for the detection of stent patency were examined by using receiver operator characteristic (ROC) curve analysis. RESULTS: One hundred six of 122 stents were interpretable. By ICA, 24 stents were found to have in- stent restenosis (22 interpretable and 2 noninterpretable with MDCT). The ROC curve showed that the optimal cutoff value of AS/AO HU to predict stent patency on MDCT was 0.81 with sensitivity of 90.9%, specificity of 95.2%, and the optimal stent diameter cutoff value was R2.5 mm with a sensitivity of 91.8% and a specificity of 93.8%. CONCLUSION: With 64-row MDCT, coronary stent patency can be evaluated quantitatively with high sensitivity and specificity and with adequate diagnostic accuracy in stents R2.5 mm in diameter. Ó 2010 Society of Cardiovascular Computed Tomography. All rights reserved. Introduction Percutaneous coronary intervention (PCI) with coronary stent implantation has been increasingly used in the treat- ment of coronary artery disease. In 2005, an estimated 1,265,000 PCI procedures were performed in the United States. 1 Despite significantly reducing the occurrence of Conflict of interest: Dr. Budoff is on the GE Speaker Bureau. The remaining authors report no conflicts of interest. There was no source of funding for this study. * Corresponding author. E-mail address: [email protected] Submitted May 28, 2009. Accepted for publication October 23, 2009. 1934-5925/$ -see front matter Ó 2010 Society of Cardiovascular Computed Tomography. All rights reserved. doi:10.1016/j.jcct.2009.10.014 Journal of Cardiovascular Computed Tomography (2010) -, -–- FLA 5.0 DTD ĸ JCCT292_proof ĸ 19 December 2009 ĸ 2:13 am ARTICLE IN PRESS
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Noninvasive quantitative evaluation of coronary artery stent patency using 64-row multidetector...

Journal of Cardiovascular Computed Tomography (2010) -, -–-
ARTICLE IN PRESS
Review Article
Noninvasive quantitative evaluation of coronaryartery stent patency using 64-row multidetectorcomputed tomography
Murrad J. Abdelkarim, MDa,*, Naser Ahmadi, MDa, Ambarish Gopal, MDa,Yasmin Hamirani, MDa, Ronald P. Karlsberg, MD, FACP, FACCb,Matthew J. Budoff, MD, FACCa
aDepartment of Medicine, Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, 1000 West CarsonStreet, Box 400, Torrance, CA 90509, USA and bCardiovascular Medical Group, Beverly Hills, CA, USA
KEYWORDS:64-row multidetectorcomputed tomography(MDCT);Cardiac computedtomographic angiography(CTA);Computed tomography(CT) density;Coronary stent patency;In-stent restenosis (ISR)
Conflict of interest: Dr. Budoff is
remaining authors report no conflicts of
There was no source of funding for
* Corresponding author.
E-mail address: [email protected]
Submitted May 28, 2009. Accepted
1934-5925/$ -see front matter � 2010
doi:10.1016/j.jcct.2009.10.014
BACKGROUND: Many studies have used multidetector computed tomography (MDCT) angiographyto evaluate coronary stents qualitatively but not quantitatively.
OBJECTIVES: This study sought to validate a method of quantitatively evaluating stent patency byusing 64-row compared with invasive coronary angiography (ICA) and to evaluate the stent size thresh-old of MDCT in detecting stent patency.
METHODS: Stented lesions (n 5 122) in 55 patients (age, 65 6 10 years; 90% men) who underwentboth 64-row MDCT and ICA were studied. Density measurements in Hounsfield units (HUs) and stentdiameters in millimeters were recorded in the stented segments, with the density of the ascending aorta(AO) taken as a reference. The ratio of the average of stent’s proximal, middle, and distal densities tomean AO density was defined as the AS/AO HU. Threshold values for the detection of stent patencywere examined by using receiver operator characteristic (ROC) curve analysis.
RESULTS: One hundred six of 122 stents were interpretable. By ICA, 24 stents were found to have in-stent restenosis (22 interpretable and 2 noninterpretable with MDCT). The ROC curve showed that theoptimal cutoff value of AS/AO HU to predict stent patency on MDCT was 0.81 with sensitivity of90.9%, specificity of 95.2%, and the optimal stent diameter cutoff value was R2.5 mm with a sensitivityof 91.8% and a specificity of 93.8%.
CONCLUSION: With 64-row MDCT, coronary stent patency can be evaluated quantitatively with highsensitivity and specificity and with adequate diagnostic accuracy in stents R2.5 mm in diameter.� 2010 Society of Cardiovascular Computed Tomography. All rights reserved.
on the GE Speaker Bureau. The
interest.
this study.
for publication October 23, 2009.
Society of Cardiovascular Computed
FLA 5.0 DTD � JCCT292_proof �
Introduction
Percutaneous coronary intervention (PCI) with coronarystent implantation has been increasingly used in the treat-ment of coronary artery disease. In 2005, an estimated1,265,000 PCI procedures were performed in the UnitedStates.1 Despite significantly reducing the occurrence of
Tomography. All rights reserved.
19 December 2009 � 2:13 am

Figure 1 Cardiac CT angiography of patent left anterior descending (LAD) coronary stent. (A) Long-axis and (B) cross-sectional viewsof a left anterior descending coronary stent without any evidence of ISR. All density measurements taken in the marked areas on the long-axis view were between 479 and 490 HU. Also note moderate disease as marked distal to the stented segment well seen on the cardiac CT.
2 Journal of Cardiovascular Computed Tomography, Vol -, No -, -/- 2010
ARTICLE IN PRESS
restenosis2,3 compared with balloon angioplasty alone, thein-stent restenosis (ISR) rates remain high. ISR can occurin 16%–35% of bare-metal stents4–7 and in 4%–11% ofdrug-eluting stents.4–7 The ‘‘gold standard’’ for the detec-tion of ISR remains invasive coronary angiography (ICA),although it is limited as an invasive technique. Therefore,there is a need for an alternative, noninvasive techniquefor the detection of ISR.
Many studies have used multidetector computed tomo-graphic (MDCT) angiography to evaluate coronary stentsqualitatively but not quantitatively. The qualitative assess-ment of stent patency with MDCT angiography is difficult,mostly limited by artifact caused by small stent size anddesign type. Our goal in this study was to develop a methodof noninvasive quantitative assessment of coronary arterystent patency with the use of 64-row MDCT angiographyby comparison with invasive coronary angiography and toevaluate the stent size threshold of 64-row MDCT angiog-raphy in detecting stent patency.
Methods
The study protocol and consent form were approved bythe Institutional Review Board Committee of the LosAngeles Biomedical Research Institute at Harbor UCLAMedical Center, Torrance, CA.
Study population
This was a retrospective analysis of 55 patients whounderwent both 64-row MDCT coronary angiography andICA. Patients were referred by their physicians for MDCT
FLA 5.0 DTD � JCCT292_proof �
angiography for evaluation of their stent and native coro-nary arteries because of the presence of symptoms or anabnormal cardiac stress test. All patients received a subse-quent ICA. We assessed the diagnostic performance ofMDCT angiography on a per-stent basis, including allpatients and all vessels for final efficacy analysis.
Scan protocol
Patients underwent MDCT angiography before conven-tional ICA. All scans were performed with a 64-row detectorLightspeed VCT scanner (GE Healthcare, Milwaukee, WI).All patients were in normal sinus rhythm at the time of theMDCT scan. Persons presenting with baseline heartrates . 65 beats/min were administered oral and/or intrave-nous b-blocker therapy. Patients were not excluded fromMDCT when the heart rate remained .65 beats/min.
After a scout radiograph of the chest (anteroposterior andlateral), a timing bolus (with 10–20 mL contrast) was per-formed to detect the time to optimal contrast opacificationin the axial image at a level immediately superior to the os-tium of the left main artery. Nitroglycerine 0.4 mg sublingualwas administered immediately before contrast injection.During MDCT angiography acquisition, 60–80 mL iodinatedcontrast (Visipaque; GE Healthcare, Chalfont St Giles,United Kingdom) was injected with the use of a triple-phasecontrast protocol: 40 mL iodixanol, followed by 20–40 mLof a 50:50 mixture of iodixanol and saline, followed by a50-mL saline flush. Retrospective electrocardiogram(ECG)–gated helical contrast-enhanced MDCT angiographywas performed, with scan initiation of 10 mm above the levelof the left main artery to 10 mm below the inferior
19 December 2009 � 2:13 am

Figure 2 Cardiac CT angiography of 2 different-sized patent left anterior descending (LAD) coronary stents. (A) Long-axis and (B)cross-sectional views of 3-mm stent; (C) long-axis and (D) cross-sectional views of 4-mm stent. There is no evidence of ISR with all den-sity measurements between 349 and 385 HU.
Q1Abdelkarim et al Evaluating coronary artery stent patency with MDCT 3
ARTICLE IN PRESS
myocardial apex. The scan parameters were 64 ! 0.625 mmcollimation, tube voltage of 120 mV, effective tube current350–780 mA. Radiation reduction with ECG tube currentmodulation was used. After scan completion, multiphasic re-construction of MDCT angiography scans was performed,with reconstructed images from 70% to 80% by 5% andfrom 5% to 95% by 10% increment.
MDCT image reconstruction and interpretation
Individually scanned raw data sets were uploaded andanalyzed on dedicated workstations (Advantage Worksta-tion; GE Healthcare, Milwaukee WI). All stented segmentswere evaluated by a reviewer who was blinded to the ICAfindings. Image reconstruction was retrospectively gated to
FLA 5.0 DTD � JCCT292_proof �
an ECG, and the optimal cardiac phase showing the leastmotion artifact was determined. Stented segments wereviewed in their short and long axes by using both theoriginal 2-dimensional axial images and multiple imagereconstruction methods. In addition, they were viewed witha wide window width and the minimum image thicknesspossible. A fixed window width of 1200 Hounsfield units(HU) and window level of 240 HU were used for allinterpretations, to minimize interscan differences and toreduce a source of error for measurements.
The location of each stent (vessel and segment) wasrecorded. Image quality of each stented segment wasjudged as adequate or not for the evaluation of stentpatency and ISR. The stent was considered interpretableif the stent lumen was visible and the contrast density of the
19 December 2009 � 2:13 am

Figure 3 ICA of patent left anterior descending (LAD) coronarystent (patient from CT angiography in Fig. 1), with moderate dis-ease distal to stented segment.
4 Journal of Cardiovascular Computed Tomography, Vol -, No -, -/- 2010
ARTICLE IN PRESS
lumen could be evaluated without or with negligibleinfluence of image degrading factors. The reason fornoninterpretability was recorded such as partial volumeeffects, metal artifacts from stent struts (beam hardening),cardiac motion artifacts (banding artifacts), and calcifica-tion on the vessel wall.
Density measurements in Hounsfield units and stentdiameters in millimeters were recorded in the proximal,middle, and distal sections along the long axis of the stentedsegments in all interpretable stents (Fig. 1 and Fig. 2). Den-sity measurements were determined by using the exact centerpoint in the short axis of all the designated sections. Stentdiameters were determined by measuring the length of astraight line segment running from the middle of the stentrim from one end to the other through the center point alongthe short axis of all the designated sections. The density mea-surement of the ascending aorta was determined by using aregion of interest area (100 mm2) in the center of the short-axis view and was taken as the reference density measure-ment. The ratio of the average of the stent’s proximal, middle,and distal densities to mean ascending aorta (AO) densitywas defined as the average stent to AO (AS/AO) HU ratio.The average of the stent’s proximal, middle, and distal diam-eters was defined as the average stent size.
To determine observer variability, a subgroup of stentedsegments were reevaluated by the first reviewer and asecond who was also blinded to the ICA findings. Thirtystented segments in 20 patients were re-reviewed by thefirst reader and reviewed by a second reader to determinethe intra-reader and inter-reader variability associated withour method of quantitative evaluation of stent patency. Withthe use of the Pearson’s coefficient of correlation in thissubgroup, we found an r 5 0.86 for intraobserver andr 5 0.82 for interobserver evaluations. The mean intra-reader variability was 6.9% 6 9.7%, and the mean inter-reader variability was 9.9% 6 0.4%.
ICA procedure and analysis
Selective ICA was performed by standard transfemoralarterial catheterization. A minimum of 8 projections wereobtained with a minimum of 5 views for the left coronaryartery system and a minimum of 3 views for the right coronaryartery system. Figure 3 shows an example of one viewobtained of a patent left anterior descending coronary arterystent. All stented segments were qualitatively evaluated byan experienced cardiologist who was blinded to the resultsof the MDCT. ICAwas used as the ‘‘gold standard’’ for deter-mining stent patency, with ISR defined as a diameter reduc-tion of R50% compared with the original stent diameter.
Statistical analysis
Categorical variables are presented as frequencies andpercentages, and continuous variables are presented asmean 6 standard deviation (SD). The area under the
FLA 5.0 DTD � JCCT292_proof �
receiver operator characteristic (ROC) curve was calculatedfor MDCT angiography to identify obstructive coronaryartery stenosis at the 50% threshold in the stented segment.A second ROC was used to determine the minimum stentsize to predict feasibility of MDCT coronary angiographyin diagnosing stent patency. Pearson’s coefficient of corre-lation (r) was used in the subgroup analysis to evaluateintraobserver and interobserver variability. All statisticalanalyses were performed with the use of SAS ProprietarySoftware, Release 9.1 (SAS Institute Inc, Cary, NC).
Results
Patient/stent characteristics and angiographicfindings
A total of 122 stented segments in 55 patients (age,65 6 10 years; 90% men) were studied, among which 106stents (86.8%) were interpretable for evaluation of stentpatency by 64-row MDCT angiography. Reasons for nonin-terpretability of the 16 stents were caused by metal artifactsin smaller sized stents (7 stents), motion artifact (4 stents),partial volume effects (3 stents), and calcification on thevessel wall (2 stents). There was no difference in age,sex, or the vessels stented among interpretable and nonin-terpretable stents. The majority of noninterpretable stentswere located in distal arterial locations (56.2%). By ICA,24 stents were occluded (22 in the interpretable groupand 2 in the noninterpretable group).
Stent characteristics for the 106 interpretable stentsamong patients with and without stent patency are shownin Table 1. Patients with patent stents tended to be older
19 December 2009 � 2:13 am
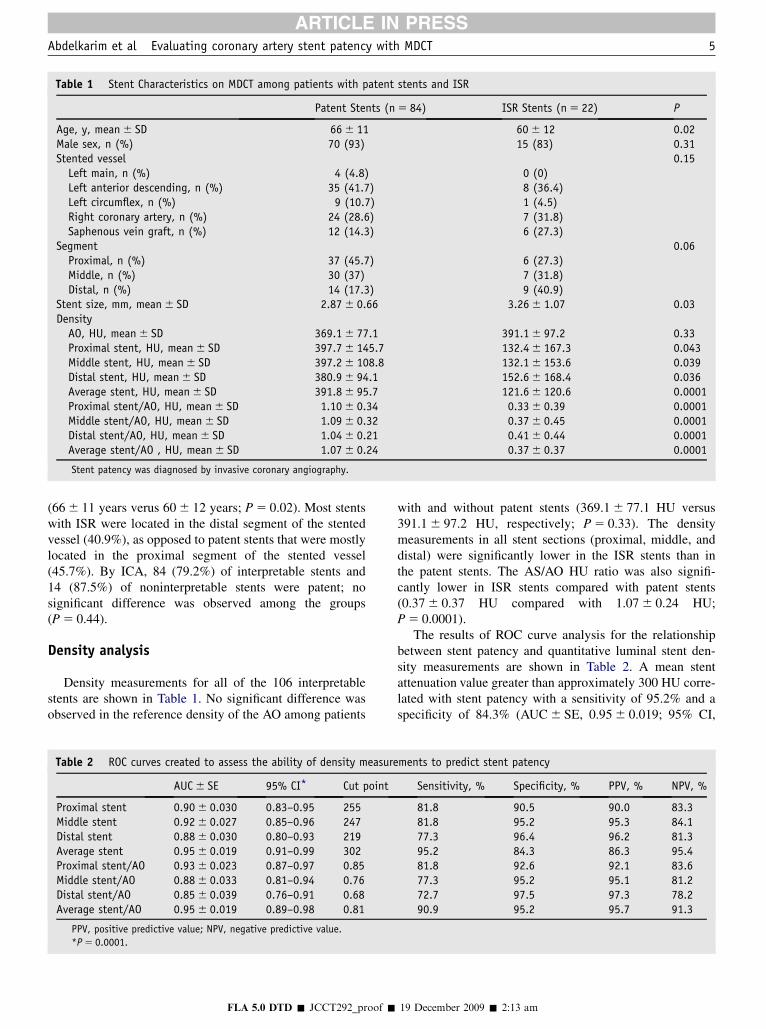
Table 1 Stent Characteristics on MDCT among patients with patent stents and ISR
Patent Stents (n 5 84) ISR Stents (n 5 22) P
Age, y, mean 6 SD 66 6 11 60 6 12 0.02Male sex, n (%) 70 (93) 15 (83) 0.31Stented vessel 0.15
Left main, n (%) 4 (4.8) 0 (0)Left anterior descending, n (%) 35 (41.7) 8 (36.4)Left circumflex, n (%) 9 (10.7) 1 (4.5)Right coronary artery, n (%) 24 (28.6) 7 (31.8)Saphenous vein graft, n (%) 12 (14.3) 6 (27.3)
Segment 0.06Proximal, n (%) 37 (45.7) 6 (27.3)Middle, n (%) 30 (37) 7 (31.8)Distal, n (%) 14 (17.3) 9 (40.9)
Stent size, mm, mean 6 SD 2.87 6 0.66 3.26 6 1.07 0.03Density
AO, HU, mean 6 SD 369.1 6 77.1 391.1 6 97.2 0.33Proximal stent, HU, mean 6 SD 397.7 6 145.7 132.4 6 167.3 0.043Middle stent, HU, mean 6 SD 397.2 6 108.8 132.1 6 153.6 0.039Distal stent, HU, mean 6 SD 380.9 6 94.1 152.6 6 168.4 0.036Average stent, HU, mean 6 SD 391.8 6 95.7 121.6 6 120.6 0.0001Proximal stent/AO, HU, mean 6 SD 1.10 6 0.34 0.33 6 0.39 0.0001Middle stent/AO, HU, mean 6 SD 1.09 6 0.32 0.37 6 0.45 0.0001Distal stent/AO, HU, mean 6 SD 1.04 6 0.21 0.41 6 0.44 0.0001Average stent/AO , HU, mean 6 SD 1.07 6 0.24 0.37 6 0.37 0.0001
Stent patency was diagnosed by invasive coronary angiography.
Abdelkarim et al Evaluating coronary artery stent patency with MDCT 5
ARTICLE IN PRESS
(66 6 11 years verus 60 6 12 years; P 5 0.02). Most stentswith ISR were located in the distal segment of the stentedvessel (40.9%), as opposed to patent stents that were mostlylocated in the proximal segment of the stented vessel(45.7%). By ICA, 84 (79.2%) of interpretable stents and14 (87.5%) of noninterpretable stents were patent; nosignificant difference was observed among the groups(P 5 0.44).
Density analysis
Density measurements for all of the 106 interpretablestents are shown in Table 1. No significant difference wasobserved in the reference density of the AO among patients
Table 2 ROC curves created to assess the ability of density measure
AUC 6 SE 95% CI* Cut point
Proximal stent 0.90 6 0.030 0.83–0.95 255Middle stent 0.92 6 0.027 0.85–0.96 247Distal stent 0.88 6 0.030 0.80–0.93 219Average stent 0.95 6 0.019 0.91–0.99 302Proximal stent/AO 0.93 6 0.023 0.87–0.97 0.85Middle stent/AO 0.88 6 0.033 0.81–0.94 0.76Distal stent/AO 0.85 6 0.039 0.76–0.91 0.68Average stent/AO 0.95 6 0.019 0.89–0.98 0.81
PPV, positive predictive value; NPV, negative predictive value.
*P 5 0.0001.
FLA 5.0 DTD � JCCT292_proof �
with and without patent stents (369.1 6 77.1 HU versus391.1 6 97.2 HU, respectively; P 5 0.33). The densitymeasurements in all stent sections (proximal, middle, anddistal) were significantly lower in the ISR stents than inthe patent stents. The AS/AO HU ratio was also signifi-cantly lower in ISR stents compared with patent stents(0.37 6 0.37 HU compared with 1.07 6 0.24 HU;P 5 0.0001).
The results of ROC curve analysis for the relationshipbetween stent patency and quantitative luminal stent den-sity measurements are shown in Table 2. A mean stentattenuation value greater than approximately 300 HU corre-lated with stent patency with a sensitivity of 95.2% and aspecificity of 84.3% (AUC 6 SE, 0.95 6 0.019; 95% CI,
ments to predict stent patency
Sensitivity, % Specificity, % PPV, % NPV, %
81.8 90.5 90.0 83.381.8 95.2 95.3 84.177.3 96.4 96.2 81.395.2 84.3 86.3 95.481.8 92.6 92.1 83.677.3 95.2 95.1 81.272.7 97.5 97.3 78.290.9 95.2 95.7 91.3
19 December 2009 � 2:13 am

web
4C/FPO
web
4C/FPO
6 Journal of Cardiovascular Computed Tomography, Vol -, No -, -/- 2010
ARTICLE IN PRESS
0.91–0.99; P , 0.0001). The optimal AS/AO HU ratio forthe diagnosis of stent patency was 0.81 with sensitivity of90.9%, specificity of 95.2%, positive predictive value of95.7%, and negative predictive value of 91.3% (AUC 6 SE,0.95 6 0.019; 95% CI, 0.89–0.98: P , 0.0001) (Fig. 4).
Stent size threshold analysis
The optimal stent diameter needed to evaluate stentpatency on MDCT angiography was R2.5 mm (Fig. 5). Atthis threshold, stent patency was detected with a sensitivityof 93.8%, specificity of 91.8%, positive predictive value of92.1%, and negative predictive value of 93.8% (AUC 6 SE,0.97 6 0.01; 95% CI, 0.93–0.99; P , 0.0001).
Figure 5 ROC curve of stent size and interpretable stentpatency.
Discussion
The current literature available on the use of MDCT forthe qualitative evaluation of coronary artery stent patencyshows a range of sensitivity from 86% to 100% andspecificity from 91% to 98%.8–14 Despite this apparentaccuracy, concerns exist over the ability to translate thesefindings to daily practice, given the need for qualitativeassessment and a requirement for advanced reconstructionand postprocessing techniques. As such, an objective andquantitative method of evaluating stent patency with64-row MDCT would potentially enable greater confidencein evaluation of stent patency.
In this study, we have shown that a mean stent densityR300 HU and a difference in CT density from thereference vessel (AO) to the coronary stent lumen of%19% correlated with a patent stent with a high sensitivity
Figure 4 ROC curve of average stent/AO HU ratio. PPV, posi-tive predictive value; NPV, negative predictive value.
FLA 5.0 DTD � JCCT292_proof �
and specificity. With the use of this method, the evaluationof coronary stents R 2.5 mm in diameter appears feasible.Advantages of this method include its quantitative natureand the ability to apply it without special reconstructiontechniques. Furthermore, display parameters such as win-dow width and display levels do not affect Hounsfieldunit measures, so this is independent of reader preferenceand workstation settings. This study marks the onset ofan era in which MDCT angiography has emerged as a via-ble and effective option in the noninvasive evaluation ofpatients with coronary stents after PCI (Fig. 6).
Prior studies have applied densitometric analysis for theanalysis of coronary stents. In a study evaluating a com-plicated method that compared density measurements in theproximal, mid, and distal regions inside each stent, 60%ISR was detected with a sensitivity of 54.5% and specificityof 94.7%.8 An alternative method, proposed by Kitagawaet al,15 evaluated ISR with the use of quantitative densityanalysis in 16-row MDCT angiography. A density measure-ment of R5 region of interest (area %1 mm2) positioned ina low-density area of the stent, compared with referencevessels (sites proximal and distal to stent), suggested ISRin the present of high variability of density values(75 6 10 HU to 270 6 7 HU). These initial studies led toa subsequent study by Kitagawa et al,16 in which regionsof interest were assessed in a reference segment 5–10 mmproximal to the stented segment and compared with regionswithin the stent. The study found that the accuracy for de-tection of ISR was high with the use of either a mean CTdensity cutoff value of 280 HU (sensitivity of 83% andspecificity of 83%) or a DCT density cutoff value of 75HU (sensitivity of 100% and specificity of 96%).
As in the study by Kitagawa et al,16 we found that amean in-stent attenuation value of 300 HU was highly
19 December 2009 � 2:13 am

Figure 6 Cardiac CT Angiography of a proximal left anterior descending (LAD) stent with ISR. (A) Long-axis and (B) cross-sectionalimages showing a dark center in the proximal portion of the stent measuring 216/239 HU, far below the aortic comparison of 414 HU in thisstudy. (C) This evidence of ISR correlated well with the invasive coronary angiogram.
Abdelkarim et al Evaluating coronary artery stent patency with MDCT 7
ARTICLE IN PRESS
accurate for the exclusion of ISR. In addition, the evalua-tion of relative attenuation within the stent compared withan aortic reference segment avoided the confounding effectof interpatient variability of cardiac output and volume ofdistribution of intracoronary contrast. We chose to useaortic attenuation as a reference segment because thisregion is less influenced by various artifacts (partial volumeeffects, beam hardening from nearby stent struts, banding,and vessel calcification) that may result in either an overes-timation or underestimation of D CT density. With the useof this method, we have shown that quantitative assessmentof ISR can enable the evaluation of stent diameters of%2.5 mm.
Despite the superiority of 64-row MDCT compared witholder generation scanners, limitations in coronary stent
FLA 5.0 DTD � JCCT292_proof �
evaluation include inferior spatial resolution compared withICA, relatively low temporal resolution, and increasedfalse-positive rates for detection of ISR in smaller stents.Stent design (diameter, length, strut thickness, and mate-rial) is the main limiting factor for the application ofMDCT in the detection of ISR. Smaller diameter stentsremain a challenge. In one recent study evaluating long-term outcomes of drug-eluting compared with bare-metalstent diameter data in 13,890 stents, 30% of implantedstents were ,3.0 mm in diameter and 4.8% were ,2.5 mmin diameter.17 Trends in stent design and size will have aneffect on MDCT stent assessability. In a study by Schuijfet al,18 90% of stents . 3.0 mm were interpretable, com-pared with only 72% of stents , 3.0 mm. In addition, 89%of stents with strut thickness , 140 mm were interpretable,
19 December 2009 � 2:13 am

Figure 7 A high-definition cardiac CT angiogram showing pa-tency of multiple stents with good distal filling. This new technol-ogy applying thinner slice thickness with specializedreconstruction techniques may allow better visualization of stentswith fewer artifacts.
8 Journal of Cardiovascular Computed Tomography, Vol -, No -, -/- 2010
ARTICLE IN PRESS
compared with only 41% of thicker strutted stents. The futuremay see refinements in MDCT scanner (Fig. 7) or stenttechnology that further enhances the accuracy of non-invasive stent patency evaluations.
Our study has several limitations. This was a retrospec-tive study; therefore, complete information was not avail-able on stent design and the time between stentimplantation and MDCT angiography acquisition. Thelack of established criteria for quantitatively evaluatingstent patency and the overall small size of our patientpopulation make it difficult to draw generalized conclu-sions for the application of our method to all patients withcoronary stents receiving MDCT angiography. Finally,inherent problems or limitations in the MDCT angiographytechnique exist such as radiation exposure, use of iodinatedcontrast, and the absence of functional or perfusion data.
Conclusion
The use of 64-row MDCT angiography coronary arterystent patency can be evaluated quantitatively with highsensitivity and specificity and with improved diagnosticpredictability in stents R 2.5 mm.
References
1. Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N,
Hailpern SM, Ho M, Howard V, Kissela B, Kittner S, Lloyd-Jones D,
McDrmott M, Meigs J, Moy C, Nichol G, O’Donnell C, Roger V,
FLA 5.0 DTD � JCCT292_proof �
Sorlie P, Steinberger J, Thorn T, Wilson M, Hong: American Heart
Association Statistics Committee and Stroke Statistics Subcommittee:
Heart disease and stroke statistics–2008 update: a report from the
American Heart Association Statistics Committee and Stroke Statistics
Subcommittee. Circulation. 2008;117:e25–146.
2. Fischman DL, Leon MB, Baim DS, Bairn DS, Schatz RA, Savage MP,
Penn I, Detre K, Veltri L, Ricci D, Nobuyoshi M, et al: A randomized
comparison of coronary-stent placement and balloon angioplasty in
the treatment of coronary artery disease. Stent Restenosis Study Inves-
tigators. N Engl J Med. 1994;331:496–501.
3. Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W,
Heyndrickx G, Emanuelsson H, Marco J, Legrand V, Materne P,
et al: A comparison of balloon-expandable-stent implantation with
balloon angioplasty in patients with coronary artery disease. Benestent
Study Group. N Engl J Med. 1994;331:489–95.
4. Holmes DR Jr., Leon MB, Moses JW, Popma JJ, Cutlip D, Fitzgeral PJ,
Brown C, Fischell T, Wong SC, Midei M, Snead D, Kruntz RE: Analysis
of 1-year clinical outcomes in the SIRIUS trial: a randomized trial of a
sirolimus-eluting stent versus a standard stent in patients at high risk
for coronary restenosis. Circulation. 2004;109:634–40.
5. Morice MC, Colombo A, Meire B, Serruys P, Tamburino C,
Guagliumi G, Sousa E, Stoll HP: REALITY Trial Investigators: Siro-
limus-vs paclitaxel-eluting stents in de novo coronary artery lesions:
the REALITY trial: a randomized controlled trial. JAMA. 2006;295:
895–904.
6. Stone GW, Ellis SG, Cox DA, Hermiller J, O’Shaughnessy C,
Mann JT, Turco M, Caputo R, Bergin P, Greenberg J, Popma JJ,
Russell ME: TASUX-IV Investigators: A polymer-based, paclitaxel-
eluting stent in patients with coronary artery disease. N Engl J Med.
2004;350:221–31.
7. Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR,
O’Shaughnessy C, Caputo RP, Kereiakes DJ, Williams DO,
Teirstein PS, Jaeger JL, Kuntz RE: SIRIUS Investigators: Sirolimus-
eluting stents versus standard stents in patients with stenosis in a native
coronary artery. N Engl J Med. 2003;349:1315–23.
8. Gaspar T, Halon DA, Lewis BS, Adawi S, Schliamser JE,
Rubinshtein R, Flugelman MY, Peled N: Diagnosis of coronary in-
stent restenosis with multidetector row spiral computed tomography.
J Am Coll Cardiol. 2005;46:1573–9.
9. Van Mieghem CA, Cademartiri F, Mollet NR, Malagutti P,
Valgimigli M, Meijboom WB, Pugliese F, McFadden EP, Lightart J,
Runza G, Bruining N, Smits PC, Regar E, van der Giessen WJ,
Sianos G, van Dombrug R, de Jaegere P, Krestin GP, Serruys PW,
de Feyter PJ: Multislice spiral computed tomography for the evalua-
tion of stent patency after left main coronary artery stenting: a compar-
ison with conventional coronary angiography and intravascular
ultrasound. Circulation. 2006;114:645–53.
10. Rixe J, Achenbach S, Ropers D, Baum U, Kuettner A, obers U,
Bautz W, Daniel WG, Anders K: Assessment of coronary artery stent
restenosis by 64-slice multi-detector computed tomography. Eur Heart
J. 2006;27:2567–72.
11. Rist C, von Zeigler F, Nikolaou K, Kirchin MA, Wintersperger BJ,
Johnson TR, Knez A, Lebert AW, Reiser MF, Becker CR: Assessment
of coronary artery stent patency and restenosis using 64-slice com-
puted tomography. Acad Radiol. 2006;13:1465–73.
12. Ehara M, Surmely JF, Kawai M, Katoh O, Matsubara T, Terashima M,
Tsuchikane E, Kinoshita Y, Suzuki T, Ito T, Takeda Y, Nasu K,
Tanaka N, Murata A, Suzuki Y, Sato K, Suzuki T: Diagnostic accuracy
of 64-slice computed tomography for detecting angiographically sig-
nificant coronary artery stenosis in an unselected consecutive patient
population: comparison with conventional invasive angiography.
Circ J. 2006;70:564–71.
13. Cademartiri F, Schuijf JD, Pugliese F, Mollet NR, Jukema JW,
Maffei E, Kroft LJ, Palumbo A, Ardissino D, Serruys PW,
Krestin GP, Van der Wall EE, de Feyter PJ, Bax JJ: Usefulness of
64-slice multislice computed tomography coronary angiography to
assess in-stent restenosis. J Am Coll Cardiol. 2007;49:2204–10.
19 December 2009 � 2:13 am

Abdelkarim et al Evaluating coronary artery stent patency with MDCT 9
ARTICLE IN PRESS
14. Oncel D, Oncel G, Karaca M: Coronary stent patency and in--
stent restenosis: determination with 64-section multi detector
CT coronary angiography-initial experience. Radiology. 2007;
242:403–9.
15. Kitagawa T, Fujii T, Tomohiro Y, Maeda K, Kobayashi M,
Kunita E, Sekiguchi Y: Noninvasive assessment of coronary stents
in patients by 16-slice computed tomography. Int J Cardiol. 2006;
109:188–94.
16. Kitagawa T, Yamamoto H, Horiguchi J, Hirai N, Fujii T, Ito K,
Kohno N: Usefulness of measuring coronary lumen density with
FLA 5.0 DTD � JCCT292_proof �
multi-slice computed tomography to detect in-stent restenosis. Int
J Cardiol. 2008;124:239–43.
17. Lagerqvist B, Stefan JK, Stenestrand U, Lindback J, Nilsson T,
Wallentin L: SCAAR Study Group: Long-term outcomes with drug-
eluting stents versus bare-metal stents in Sweden. N Engl J Med.
2007;356:1009–19.
18. Schuijf JD, Bax JJ, Jukema JW, Lamb HJ, Warda HM, Viegen HW, de
Roos A, van der Wall EE: Feasibility of assessment of coronary stent
patency using 16-slice computed tomography. Am J Cardiol. 2004;94:
427–30.
19 December 2009 � 2:13 am




















