Evaluation of Small Intestine Grafts Decellularization Methods for Corneal Tissue Engineering
Upload
independentCategory
view
1download
0
Femorofemoral bypass graft: Analysis patency and factors influencing long-term outcome
of
Enrique Criado, MD, Steven J. Burnham, MD, Ellis A. Tinsley, Jr., MD, George Johnson, Jr., MD, and Blair A. Keagy, MD, Chapel Hill, N.C.
Purpose: To evaluate the results of femorofemoral bypass graft (FFBPG), we analyzed 110 consecutive FFBPGs performed at our institution during an 11-year period. Methods: In 62 (56%) patients the indication for surgery was claudication and in 48 (44%) patients rest pain or tissue loss. In 42 patients the superficial femoral artery (SFA) was occluded. A preoperative percutaneous transluminal baUoon angioplasty (PTA) was performed in 24 (22%) patients to correct a significant donor iliac artery stenosis. In 48 (44%) patients a total of 54 arterial procedures were performed simultaneously with FFBPG. Results: After surgery 75 (68%) patients were moderately or markedly improved, whereas 20 (18%) were minimally improved, unchanged, or worse, including 7 (6%) with hemodynamic failures. The in-hospital mortality rate was 4.5%. Actuarial patient survival rate was 70%-+ 8.6% at 6 years. The actuarial primary graft patency rate was 83% + 4.2%at 1year, 71% -+ 6.9% at 3 years, 60% -+ 8.3% at 5 years, and51% -+ 9.6% at 6 years. Age, sex, and race of the patient did not influence graft patency. Grafts placed for limb-threatening ischemia or in patients with SFA occlusion had a similar patency rate compared with those placed for claudication or in patients with patent SFA. The overall limb preservation rate was 83% - 7.3% at 5 years but was only 64% for patients who underwent operation for limb-threatening ischemia. Conclusions: In conclusion, FFBPG offers moderately low long-term patency in a population with limited survival. Outflow procedures performed concomitantly with FFBPG seemed to compensate for the negative impact on graft patency rate of ipsilateral SFA occlusion and limb-threatening ischemia. Limb-threatening ischemia, however, carried a significantly higher (p < 0.05) amputation rate. The influence of preoperative donor iliac artery percutaneous transluminal balloon angioplasty on FFBPG patency remains unclear. (J VASC SURG 1993;18:495-505.)
Since the first report by Vetro 1 in 1962, femoro- femoral bypass grafting (FFBPG) has become the preferred approach for the treatment of patients with unilateral iliac lesions not amenable to percutaneous transluminal balloon angioplasty (PTA). The results o f FFBPG, however, have been shown to vary widely among the different published series, z16 This vari-
From the Vascular Surgery Section, Department of Surgery, University of North Carofina at Chapel Hill School of Medicine, Chape ! Hill.
Presented at the Seventeenth Annual Meeting of the Southern Association for Vascular Surgery Fort Lauderdale, Fla., Jan. 28-31, 1993.
Reprint requests: Enrique Criado, MD, Vascular Surgery Section, University of North Carolina Department of Surgery, 210 Burnett-Womack, CB# 7210, Chapel Hill, NC 27599-7210.
Copyright © 1993 by The Society for Vascular Surgery and International Society for Cardiovascular Surgery, North Amer- ican Chapter.
0741-5214/93/$1.00 + .10 24/6/47896
ability is likely caused by the differences among the various patient populations under study~ in terms of factors that influence graft patency. The advantages of use of FFBPG as an inflow procedure rather than aortofemoral or iliofemoral bypass, including avoid- ance of potentially hostile abdominal conditions and theoretically lower mortality and morbidity rates, are shadowed by its lower patency rate. The selection of surgical treatment for iliac artery disease should weigh operative risk and life expectancy of the patient against the durability of the different procedures under consideration. The identification of factors that favorably or adversely affect FFBPG patency would improve the treatment selection process for the patient with iliac disease. This study reviews our 11-year experience with FFBPG to obtain informa- tion on the long-term outcome of these patients and to determine which factors influence graft patency.
495

JOURNAL OF VASCULAR SURGERY 496 Criado et al. September 1993
Table I. Risk factors in 110 patients undergoing femorofemoral bypass
Risk factor No. of patients
Cigarette smoking 99 (90%) Diabetes 18 (16%) Hypertension 63 (57%) Heart disease 56 (51%) Cerebrovascular disease 39 (35%) Lung disease 35 (32%) Renal insufficiency 25 (23%) Hyperlipidemia 4 (4%)
PATIENTS AND METHODS
The hospital records, noninvasive arterial study results, and arteriograms of 110 patients who under- went FFBPG at the University of North Carolina Hospitals between July 1980 and July 1991 were reviewed. This patient population was obtained from our vascular data base by identifying all recipients of an FFBPG during the study period. Additionally, to doctnnent graft patency, those patients who were alive and whose grafts had not failed at the time of this review were evaluated with noninvasive arterial studies. Demographic features, indications for sur- gery, 30-day hospital and long-term mortality rates, complications, recipient limb superficial femoral artery (SFA) patency, and early and late primary graft patency were obtained from the review. All observa- tions were made according to the "Suggested Stan- dards for Reports Dealing with Lower Extremity Ischemia" outlined by the Society for Vascular Surgery and International Society for Cardiovascular Surgery, North American Chapter. 17 Graft patency and patient survival rates were obtained with the actuarial method described by Anderson et al.18 Statistical comparison of graft patency and survival rates between different subgroups of patients at specific intervals was made with the chi-squared method. Comparison of unpaired groups of data was made with the Student t test.
One hundred ten consecutive patients underwent FFBPG during the 11-year period from 1980 to 1991. There were 69 men and 41 women with a mean age of 59 years (11.4 +_ SD), range 15 to 84 years. Seventy-one patients were white, and 39 were black. The risk factors for these patients are shown in Table I. The average number of days of hospital stay after FFBPG was 7.8 (median of 5 days). In 95 (86%) patients the FFBPG was performed as a primary inflow operation, whereas in 15 (14%) a previous inflow procedure had failed; these included one iliofemoral, three axiUofemoral, three femoro- femoral, and eight aortobifemoral bypasses. No procedures were done because of infection of an
Table II. Preoperative degree of lower extremity ischemia in 110 patients undergoing femorofemorai bypass
No. of patients
Major tissue loss 5 (4.5%) Minor tissue loss 25 (23%) Rest pain (arterial pressure < 18 (16%)
40 mm Hg) Severe claudicafion 36 (33%) Moderate claudieafion 13 (12%) Mild clandication 11 (10%) Symptom free 0 Not specified 2
According to the "Suggested Standards for Reports Dealing with Lower Extremity Ischemia" published by the Society for Vascular Surgery/North American Chapter, International Society for Car- diovascular Surgery. 17
abdominal aortic graft. The indications for surgery are detailed in Table II. Ninety-six (87%) patients had symptoms of chronic ischemia and underwent elective surgery, whereas 14 (13%) patients had acute ischemia in addition to chronic symptoms and underwent an emergency procedure. The preop- erative mean anlde/brachial index (ABI) was 0.33 + 0.2, 0.4 + 0.2 for patients with claudication, and 0.22 -+ 0.1 for patients with limb-threatening ischemia. Twenty-four patients (22%) underwent a PTA of the donor iliac artery before the FFBPG, whereas 13 patients (12%) had failure of a recipient iliac artery PTA before surgery. Review of the preoperative arteriograms revealed that 42 (38%) patients had complete occlusion of the recipient limb SFA, although it was patent but diseased to different degrees in 43 (39%). Patency of the recipient limb SFA was not determined in 25 patients. In 57 patients the recipient limb was the right, and in 53 patients it was the left. The type of conduit used for the bypass was 8 mm Dacron in 86 (78%) cases, 8 mm polytetrafluoroethylene (PTFE) in 21 (19%) cases, saphenous vein in one case, and was not documented in 2 cases.
In addition to the FFBPG, 48 (44%) patients underwent 54 simultaneous procedures, which in- cluded 17 femoral proftmdaplasties, 9 femoral endarterectomies, 14 femoral thrombectomies, 8 femoropopliteal-distal bypasses, 3 fasciotomies, 1 excision of femoral pseudoaneurysm, 1 excision of an infected axillofemoral graft, and 1 above-the-knee amputation. There were 12 major postoperative complications (11% complication rate), 5 of which led to the death of the patient (4.5% hospital mortality rate), and 9 minor complications as pre- sented in Table III. Two patients died of early graft infection. Both were treated initially with wound debridement and antibiotics. Both patients' courses

JOURNAL OF VASCULAR SURGERY Volume 18, Number 3 Criado et al. 497
Table III. Morbidity and mortality in 110 patients undergoing FFBPG
Complication No. of patients
Graft infection 4 (2 deaths) Myocardial infarction 4 (2 deaths) Ventricular ectopy 5 Superficial wound infection 3 Deep wound infection 1 Wound seroma 1 Adult respiratory distress syn- 1 (1 death)
drome Donor SFA thrombosis 1 Deep vein thrombosis and pulmo- 1
nary embolism
Twelve complications were major and led to death in five patients, nine complications were considered minor because they did not alter the length of hospitafization.
Table IV. Initial clinical outcome in patients after femorofemoral bypass
Outcome No. of patients
Markedly improved 28 (25%) Moderately improved 47 (43%) Minimally improved 2 (2%) No change 13 (12%) Mildly worse 0 Moderately worse 0 Markedly worse 6 (5%) Not determined 5 (5%)
Five patients died after operation. In four patients the FFBPG was performed to allow healing of an above-the-knee amputation. According to the Outcome Criteria outlined in the "Suggested Standards for Reports Dealing with Lower Extremity Ischemia," by the Society for Vascular Surgery/North American Chapter, International Society for Cardiovascular Surgery. Iz
were complicated by systemic sepsis requiring graft excision, followed by a protracted septic course ending in death.
RESULTS
The initial outcome of the surviving patients after FFBPG is described in Table IV. Hemody- namic failure of the FFBPG occurred in seven patients (6%), leading to major amputation of six limbs although the graft was still patent. All he- modynamic failures occurred in patients who un- derwent surgery for tissue necrosis, had an occluded SFA, or had acute ischemia. After operation there was a mean improvement in the recipient limb ABI of 0.35 + 2.5. This improvement in ABI was greater in the group of patients who underwent surgery for claudication compared with those pa- tients who underwent surgery for limb-threatening ischemia (0.37 + 2.4 versus 0.27 + 2.6). However, the statistical significance of this difference was at the 0.058 level.
Follow-up time ranged from 1 to 132 months (mean 28 _+ 3.4). Long-term survival of these pa- tients was 89.6% + 3.4% at 1 year, 79.7% + 5.7% at 3 years, 73.7% + 7.4% at 5 years, and 69.7% + 8.6% at 6 years (Fig. 1). Primary graft patency was 83.6% + 4.2% at 1 year, 71.3% + 6.9% at 3 years, 60% + 8.3% at 5 years, and 51.4% + 9.6% at 6 years (Fig. 2). The complete life-table analysis of the primary graft patency is presented in Table V. Four FFBPGs performed to allow healing of an above-the-knee amputation remained patent during the hospital period and accomplished the intended goal; therefore they were withdrawn from the patency analysis after the ini- tial interval. The secondary patency rate was 87.8% + 3.7% at 1 year and 60.6% + 8.1% at 5 years. Limb preservation after FFBPG was
83% + 6.5% at 5 years. However, there was a significantly lower (p < 0.05) long-term limb pres- ervation rate in patients who underwent operation for limb-threatening ischemia compared with those who underwent operation for claudication (64% vs 93% at 5 years) (Fig. 3). Statistical comparison of graft patency rates between different subgroups of patients at different intervals revealed that sex, race, and age more than 60 years did not significantly influence graft patency rate. Graft patency did not improve for patients who underwent operation during the second half of the period under study compared with those who underwent operation during the first half. The patency at 2 years for PTFE grafts was significantly (p < 0.001) lower than that for Dacron grafts (44% _+ 10.4% vs 79% _+ 5.7%). However, the number of PTFE grafts was small (21), and the follow-up period was shorter than that for Dacron grafts. The presence of an occluded SFA and the need for a concomitant arterial reconstruction did not produce a significant difference in graft patency rates (Figs. 4 and 5). Patients with limb-threatening ischemia had no difference in graft patency compared with those who underwent operation for claudication (Fig. 6). We found a strikingly lower graft patency rate at 1 year for those patients who underwent preoperative donor iliac artery PTA compared with those patients who did not (78% vs 93%); however, it did not reach statistical significance (Fig. 7). Donor iliac artery PTA was performed on lesions that were suitable for angioplasty but were not necessarily ideal. The hemodynamic improvement after donor iliac PTA was documented in only a few cases. The number of patients in the subgroups having diabetes, undergoing emergency surgery, and undergoing FFBPG as a secondary procedure was not considered large enough to allow reliable statistical comparison of their graft patency rates.

JOURNAL OF VASCULAR SURGERY 498 Criado et al. September 1993
1.0
0.9
0.8
"~ 0.7
• - 0.6 - i
0,5
'~ 0.4
E 0.3 0
0.2
0.1
0.0
SURVIVAL IN 110 PATIENTS FOLLOWING FFBPG
• .
2G 1 2O
! ! i I i I
12 24 36 48 60 72
Interval in M o n t h s
Fig. 1. Life-table analysis of patient survival after FFBPG. Five-year survival rate was 74% -+ 7.4%. Survival curve starts at 95.5% because of 4.5% in-hospital mortaliv¢ rate.
0 c 0
n
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0 .2 -
0.1
0,0 0
PRIMARY PATENCY IN 110 FFBPG
5O .L 31
I
14
i i i ] i , ]
12 24 36 48 60 72
Interval in Months
Fig. 2. Life-table analysis of FFBPG primary graft patency (see Table V).
D I S C U S S I O N
Femorofemoral bypass continues to be the most widely used primary procedure for reconstruction of unilateral iliac artery disease, despite its significantly
lower patency when compared with bypasses origi- nating in the aorta) 9 The technical simplicity and expeditiousness of FFBPG and its relatively low morbidity and mortality rates, overshadow its limited

JOURNAL OF VASCULAR SURGERY Volume 18, Number 3 Criado et al. 499
LIMB SALVAGE FOR CLAUDICATION vs LIMB THREAT
1 . 0 -
I
0 . 9 -
0.8 ¸
0.7
( D
o~ 0.6 >
0.5
E 0.4 - , I
0.3
0.2
0.1
57 46 42 26 19 15 14
p<.05 ~ o
17 11 p<.01 p<.05
0 [] []
10 9 4 p<.05 p<.05
D - - - Threat Limb
- Claudicants
0.0 i I i i I I
0 12 24 36 48 60 72
I n t e r va l in M o n t h s
Fig. 3. Comparison of limb salvage rates after FFBPG in patients undergoing surgery for claudication with that in patients who underwent operation for limb-threatening ischemia. Significantly higher amputation rate was noted in patients with limb-threatening ischemia starting at 6 months.
Table V. Actuarial analysis of primary graft patency in 110 patients undergoing FFBPG
Interval patency Cumulative patency Interval (months) Grafts at r isk Failed grafts Patients withdrawn * (%) (%) SE
0-1 110 1 151- 99 99.0 0.9 1-6 94 8 20 95 90.0 3.0 6-12 66 4 12 93 83.6 4.2
12-24 50 5 14 88 73.9 5.3 24-36 31 1 6 96 71.3 6.9 36-48 24 0 3 100 71.3 7.8 48-60 21 3 4 84 60.0 8.3 60-72 14 2 0 86 51.4 9.6
*Patients were withdrawn because of death, duration of follow-up, or lost to follow-up. +Four patients undergoing FFBPG to allow healing of an above-the-knee amputation were withdrawn during the first interval with patent grafts.
durability. The 4.5% 30-day hospital mortality rate in our study is similar to the 4% mortality rate among 97 patients who underwent abdominal aortoiliac reconstructions at our institution during the same period and is comparable to those reported in recent series.3,s,2o,21
Our graft patency rate is comparable to those published in some series during recent years. 2,306,2° However, others s,/1 have reported higher graft pa- tency rates, perhaps because of the lesser severity of vascular disease present in their patient population. Our 6-year 51% graft patency rate and 70% survival
rate imply that more than one third of our patients will actually sustain graft thrombosis. This outcome compares poorly with that of inflow procedures originating in the aorta) 9 Our secondary graft patency rate was minimally improved from our primary patency rate because only four grafts were salvaged or revised. This may be explained b y our patient referral pattern, which in many cases prevents us from examining patients soon after graft throm- bosis occurs.
The selection of FFBPG for an inflow procedure tends to be mainly influenced by the anatomic
5 0 0 Criado et al. JOURNAL OF VASCULAR SURGERY September 1993
43 PATIENTS WITH PATENT SFA vs 39 WITH O C C L U D E D SFA
U
O
O >
E
o
1.04
0.9,
0.8-
0.7-
0.6-
0.5-
0.4-
0.3-
0.2-
0.1
2O
41 6
NS ~ 27 " ~ NS 17
NS
3 3 2
15 13 NS
10 NS
Patent SFA
~- Occluded SFA
0,0 i I I ] i I
0 12 24 36 48 60 72
In terva l in Mon ths
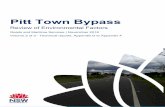
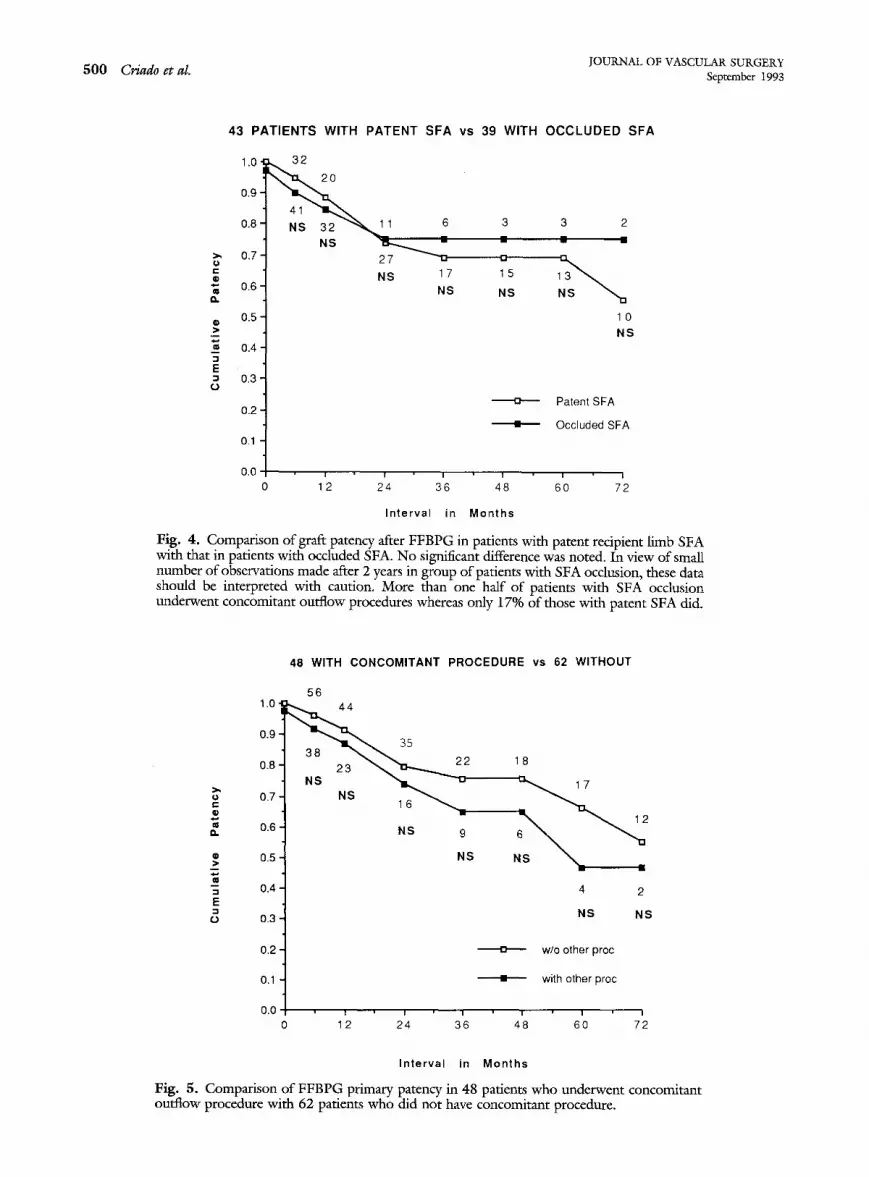
Fig. 4. Comparison of graft patency after FFBPG in patients with patent recipient limb SFA with that in patients with occluded SFA. No significant difference was noted. In view of small number of observations made after 2 years in group of patients with SFA occlusion, these data should be interpreted with caution. More than one half of patients with SFA occlusion underwent concomitant outflow procedures whereas only 17% of those with patent SFA did.
>
E
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
48 WITH CONCOMITANT PROCEDURE vs 62 WITHOUT
56
38 23 ~ 2
NS
NS 1 6 ~
NS 9
NS
18
N S ~ . _ _ m
4 2
NS NS
w/o other proc
~- with other proc
12 2 36 48 60 7
Interval in Months
Fig. 5. Comparison of FFBPG primary patency in 48 patients who underwent concomitant outflow procedure with 62 patients who did not have concomitant procedure.

JOURNAL OF VASCULAR SURGERY Volume 18, Number 3 Criado et al. 501
62 C L A U D I C A N T S vs 44 P A T I E N T S W I T H L IMB T H R E A T E N I N G I S C H E M I A
1.0
0.9
0.8
~' 0.7 O r -
"" 0.6
0.5
"~ 0.4 -,=
E 0.3
o
0.2
0.1
0.0
15 NS 10
NS
16
. s .,% 3
NS
- - u Claud Patency
-- Threat Patency
I I I I I I
12 24 36 48 60 72
Interval in Months
Fig. 6. Comparison of FFBPG primary graft patency in 62 patients who underwent operation for claudication with 44 patients who underwent operation for limb-threatening ischemia (rest pain or tissue necrosis).
24 WITH DONOR ILIAC PTA vs 82 WITHOUT PTA
o
O
n
M
- 1
E - I
O
1.0
0 . 9 "
0.8-
0.7-
0.6 [
0.5 ~
0.4 [
0.3 ]
0.2 ]
0.1
68 47
3 ~ 22
NS 18 ~ , , , , ~ .
NS 12 8
NS NS
17
1
4
NS
~- Patency c PTA
Patency w/o PTA
0.0 i i i i I i
0 12 24 36 48 60 72
Interval in Months
Fig. 7. Comparison of FFBPG primary graft patency in 24 patients who underwent preoperative donor iliac artery PTA with 82 patients who did not undergo preoperative PTA. Trend toward lower graft patency in patients with preoperative PTA did not reach significance. However, small number of grafts observed in this group does not allow tirm conclusions.
JOURNAL OF VASCULAR SURGERY 502 Criado et al. September 1993
Table VI. Primary patency rates reported for FFBPG
3-year patency 5-year patency
No. of grafls No. of graf~s Author Year No. of grafts (% +_ SE) observed (% +- SE) observed Method
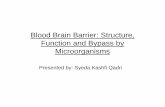
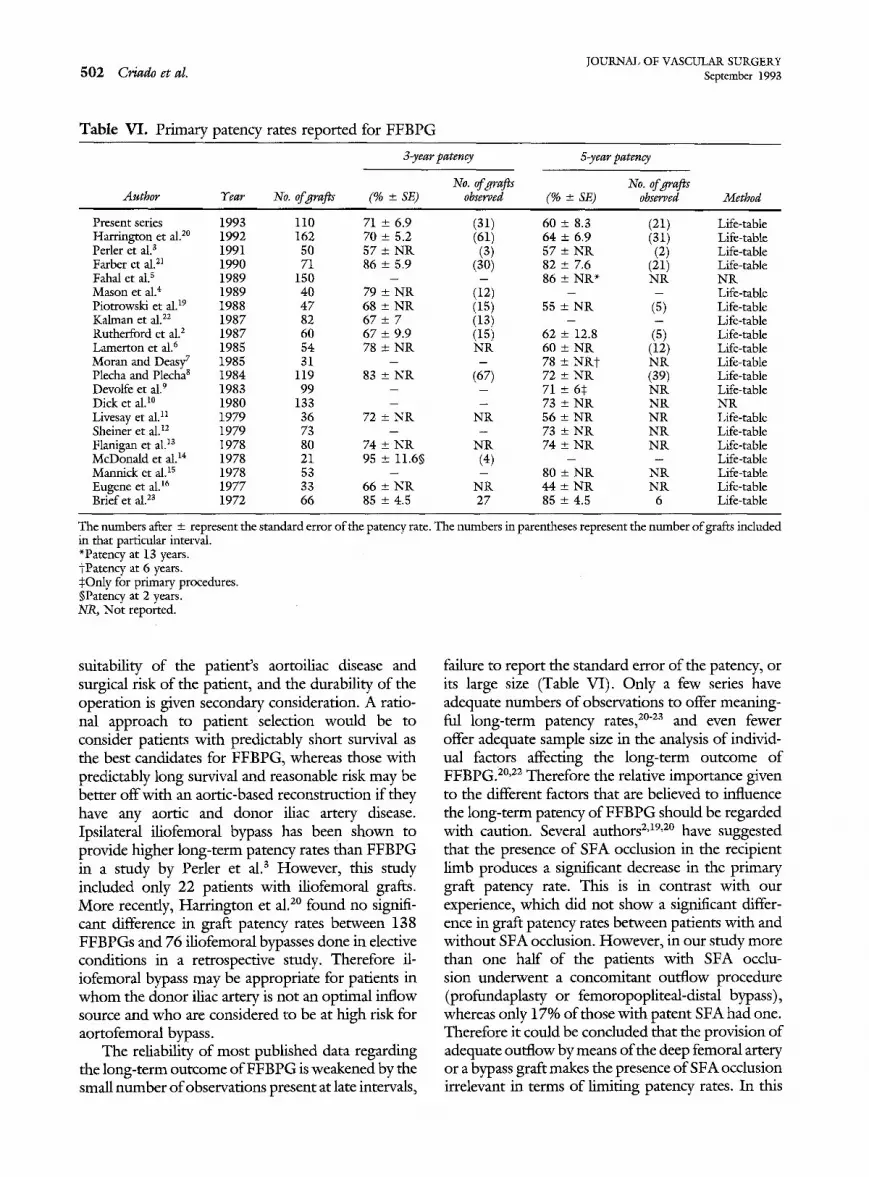
Present series 1993 110 71 + 6.9 (31) 60 + 8.3 (21) Life-table H a r r i n g t o n et al.20 1992 162 70 _+ 5.2 (61) 64 -+ 6.9 (31) Life- table Per ler e t al. s 1991 50 57 + N R (3) 57 + N K (2) Life- table Farber et al. 21 1990 71 86 + 5.9 (30) 82 + 7.6 (21) Life- table Fahal e t al.s 1989 150 - - 86 + N R ~ N R N R M a s o n et al. 4 1989 40 79 + N R (12) - - Life- table P io t rowsk i et al. 19 1988 4 7 68 -+ N R (15) 55 + N R (5) Life- table Ka lman et al. 22 1987 82 67 + 7 (13) - - Life- table Ru the r fo rd et al.2 1987 60 67 + 9.9 (15) 62 + 12.8 (5) Life- table L a m e r t o n et al. 6 1985 54 78 + N R N R 60 + N R (12) Life- table M o r a n and Deasy 7 1985 31 - - 78 + N R t N R Life- table Plecha and Plecha 8 1984 119 83 + N R (67) 72 -+ N R (39) Life- table Devol fe e t al. 9 1983 99 - - 71 -+ 65 N R Life- table D i c k et al.10 1980 133 - - 73 + N R N R N R Livesay et al. 11 1979 36 72 + N R N R 56 -+ N R N R Life- table Sheiner e t al.12 1979 73 - - 73 + N R N R Life- table F lan igan et al. ~3 1978 80 74 + N R N R 74 + N R N R Life- table M c D o n a l d et al.14 1978 21 95 + 11.6~ (4) - - Life- table M a n n i c k et al.ls 1978 53 - - 80 + N R N R Life- table E u g e n e et al. 16 1 9 7 7 33 66 -+ N R N R 44 _+ N R N R Life- table B r i e f e t al. 2s 1972 66 85 + 4.5 27 85 + 4.5 6 Life- table
The numbers after + represent the standard error of the patency rate. The numbers in parentheses represent the number of grafts included in that particular interval. *Patency at 13 years. tPatency at 6 years. $Only for primary procedures. §Patency at 2 years. N-R, Not reported.
suitability of the patient's aortoiliac disease and surgical risk of the patient, and the durability of the operation is given secondary consideration. A ratio- nal approach to patient selection would be to consider patients with predictably short survival as the best candidates for FFBPG, whereas those with predictably long survival and reasonable risk may be better off with an aortic-based reconstruction if they have any aortic and donor iliac artery disease. Ipsilateral iliofemoral bypass has been shown to provide higher long-term patency rates than FFBPG in a study by Perler et al.3 However, this study included only 22 patients with iliofemoral grafts. More recently, Harrington et al. 2° found no signifi- cant difference in graft patency rates between 138 FFBPGs and 76 iliofemoral bypasses done in elective conditions in a retrospective study. Therefore il- iofemoral bypass may be appropriate for patients in whom the donor iliac artery is not an optimal inflow source and who are considered to be at high risk for aortofemoral bypass.
The reliability of most published data regarding the long-term outcome of FFBPG is weakened by the small number of observations present at late intervals,
failure to report the standard error of the patency, or its large size (Table V-I). Only a few series have adequate numbers of observations to offer meaning- ful long-term patency rates, 2°23 and even fewer offer adequate sample size in the analysis of individ- ual factors affecting the long-term outcome of FFBPG. 2°,22 Therefore the relative importance given to the different factors that are believed to influence the long-term patency of FFBPG should be regarded with caution. Several authors 2,19,2° have suggested that the presence of SFA occlusion in the recipient limb produces a significant decrease in the primary graft patency rate. This is in contrast with our experience, which did not show a significant differ- ence in graft patency rates between patients with and without SFA occlusion. However, in our study more than one half of the patients with SFA occlu- sion underwent a concomitant outflow procedure (profundaplasty or femoropopliteal-distal bypass), whereas only 17% of those with patent SFA had one. Therefore it could be concluded that the provision of adequate outflow by means of the deep femoral artery or a bypass graft makes the presence of SFA occlusion irrelevant in terms of limiting patency rates. In this

JOURNAL OF VASCULAR SURGERY Volume 18, Number 3 Criado et al. 503
regard Brener et al.24 recently reported a series of 228 FFBPGs in which the indication for surgery and SFA occlusion had no influence on graft patency rate. It could be argued therefore that patients with multi- level disease benefit from simultaneous procedures. This is in agreement with Dalman et al.,2~ who observed that multilevel procedures can accomplish patency rates equal to single level operations, and with similar morbidity rates. On the other hand, the experience of Harrington et al. 2° showed a lower patency rate in FFBPG performed with concomitant ipsilateral endarterectomy or distal bypass.
In 1972 Porter et al. 26 first reported the combi- nation of donor iliac artery PTA with FFBPG. Since then the results of this treatment combination have not been well documented. Recently, Harrington et al. 2° reported similar patency rates for FFBPG with and without preoperative donor iliac artery PTA, but the time interval was not specified. In our experience with 24 patients who underwent donor iliac artery PTA before FFBPG there was a striking difference in patency rates at 1 year (78% vs 93%), which decreased over subsequent years. However, the difference was not statistically significant. In view of the small number of patients in this group, this observation should be taken with caution and more data are warranted before donor iliac PTA before FFBPG can be considered equivalent to FFBPG alone.
Kalman et al. 22 suggested that patients undergo- ing FFBPG for clandication had a higher graft patency rate when compared with those patients who underwent operation for limb preservation. Our experience, however, showed no difference between the two indications. Furthermore the greater post- operative improvement in ABI in our patients who underwent operation for claudication did not reach statistical significance when compared with those patients who underwent operation for limb preser- vation. The lack of difference between these two groups may be a product of the greater number of patients who had a concomitant arterial procedure in our series (26 patients with claudication and 22 patients with threatened limb). However, there was a significantly higher amputation rate in patients who underwent operation for limb-threatening ischemia compared with those who underwent operation for clandication (64% vs 93% at 5 years). This fact suggests that limb loss may be caused by progression of distal disease; however, whether insufficient inflow provided by FFBPG is also a factor responsible for limb loss is unclear. The lower early patency rate obtained With PTFE grafts compared with Dacron
grafts is likely a product of the presence of more severe disease in patients with PTFE grafts. Further- more the retrospective comparison of the patency rates for different graft materials with such small numbers of observations is not very reliable.
In summary, in view of the limited patency of FFBPG, it is most suitable for patients with predict- ably low survival and high surgical risk. Patients who are fair surgical candidates and are expected to be long-term survivors should be considered for aortoil- iac reconstruction. The negative impact on the graft patency rate of recipient limb SFA occlusion and limb-threatening ischemia as the surgical indications may be compensated by the association of concom- itant outflow procedures with FFBPG. However, the presence of limb-threatening ischemia in patients undergoing FFBPG with or without concomitant outflow procedures carries a high long-term ampu- tation rate.
We thank Ivis Reed Bohlen for her editorial assistance in the preparation of the manuscript.
REFERENCES
1. Vetto RM. The treatment of unilateral iliac artery obstruction with a transabdominal, subcutaneous, femorofemoral graft. Surgery 1962;52:342-5.
2. Rutherford RB, Patt A, Pearce WH. Extraanatomic bypass: a closer view. J VASC SURG 1987;6:437-46.
3. Perler BA, Burdick JF, Williams GM. Femoro-femoral or ilio-femoral bypass for unilateral inflow reconstruction? Am J Surg 1991;161:426-30.
4. Mason RA, Smirnov VB, Newton GB, Giron F. Alternative procedures to aortobifemoral bypass grafting. J Cardiovasc Surg 1989;30:192-7.
5. Fahal All, McDonald AM, Marston A. Femorofemoral bypass in unilateral iliac artery occlusion. Br J Surg 1989;76: 22-5.
6. Lamerton AJ, Nicolaides AN, Eastcott HHG. The femoro- femoral graft. Arch Surg 1985;120:1274-8.
7. Moran KT, Deasy JT. Extra-anatomic femoro-femoral bypass grafting for iliac artery disease. Ir Med J 1985;78:310-1.
8. Plecha FR, Plecha FM. Femorofemoral bypass grafts: ten-year experience. J VAsc SURG 1984;1:555-61.
9. Devolfe C, Adeleine P, Henrie M, Violet F, Descotes J. Ilio-femoral and femorofemoral crossover grafting. J Cardio- vasc Surg 1983;24:634-40.
10. Dick LS, Brief DK, Alpert J, Brener BJ, Goldenkranz R, Parsonnet V. A 12-year experience with femorofemoral crossover grafts. Arch Surg 1980;115:1359-65.
11. Livesay JJ, Atldnson JB, Baker JD, Busuttil RW, Barker WF, Machleder HI. Late results of extra-anatomic bypass. Arch Surg 1979;114:1260-7.
12. Sheiner NM, Ashby D, Zeltzer J. Treatment oftmilateral iliac artery disease by femorofemoral bypass grafting. Can J Surg 1979;22:474-6.
13. Flanigan DP, Pratt DG,Goodreau JJ, Burnham SJ, Yao JST, Bergan JJ. Hemodynamic and angiographic guidelines in selection of patients for femorofemoral bypass. Arch Surg 1978;113:1257-62.

1OURNAL OF VASCULAR SURGERY 504 Criado et al. September 1993
14. McDonald PT, Rich NM, CoUins Jr GJ, Anderson CA, Kozloff L. Femorofemoral grafts: the role of concomitant extended profimdaplasty. Am J Surg 1978;136:622-8.
15. Mannick JA, Maini BS. Femorofemoral grafting: indications and late results. Am J Surg 1978;136:190-2.
16. Eugene J, Goldstone J, Moore WS. Fifteen year experience with subcutaneous bypass grafts for lower extremity ischemia. Ann Surg 1977;186:177-83.
17. Ad Hoc Committee on Reporting Standards. Society for Vascular Surgery/NoR American Chapter, International Society for Cardiovascular Surgery. Suggested standards for reports dealing with lower extremity ischemia. J VAse SURG 1986;4:80-94.
18. Anderson RP, Bonchek LI, Grunkemeier GL, Lambert LE, Starr A. The analysis and presentation of surgical results by actuarial methods. J Surg Res 1974;16:224-30.
19. Piotrowski J~, Pearce WH, Jones DN, et al. Aortobifemoral bypass: the operation of choice for unilateral iliac occlusion? J VASC SURG 1988;8:211-8.
20. Harrington ME, I-Iarrington EB, Haimov M, Schanzer H, Jacobson II JH. Iliofemoral versus femorofemoral bypass: the case for an individualized approach. J VAse SURG 1992;16: 841-54.
21. Farber MA, Hollier LH, Eubanks R, Ochsner JL, Bowen JC. Femorofemoral bypass: a profile of graft failure. South Med J 1990;83:1437-43.
22. Kalman PG, Hosang M, Johnston KW, Walker PM. The current role for femorofemoral bypass. J VASC SURG 1987; 6:71-6.
23. Brief DK, Alpert J, Parsonnet V. Crossover femoro-femoral grafts. Arch Surg 1972;105:889-94.
24. Brener BJ, Brief DK, Alpter J, et al. Femorofemoral bypass: a twenty-five-year experience. In: Yao JST, Pearce WH, ed. Long-term results in vascular surgery. Norwalk, Conn.: Appleton & Lange, 1993:385-93.
25. Dalman RL, Taylor Jr LM, Moneta GL, Yeager RA, Porter JM. Simultaneous operative repair of multilevel lower extremity occlusive disease. J VAsc SURG 1991;13:211- 21.
26. Porter JM, Eidemiller LR, Dotter CT, Roesch J, Vetto RM. Combined arterial dilatation and femorofemoral by- pass for limb salvage. Surg Gynecol Obstet 1973;137: 409-12.
Submitted Feb. 2, 1993; accepted April 11, 1993.
D I S C U S S I O N
Dr. Morr is D. Kerstein (Philadelphia, Pa.). The femorofemoral crossover bypass for isolated iliac occlusive disease has gained wider acceptance in recent years and seems to be significantly superior to the iliofemoral approach in relation to ease of performance, long-term patency, survival, complications, and shorter hospital stay. This patency rate of nearly 91% is good or better than what one sees in the literature. Many patients who have femorofemoral bypass grafts have associated bilateral superficial femoral occlusion in addition to iliac occlusion. Significant improvement in recipient pressure index at rest was seen with patent grafts 6 weeks to 6 months after operation at our institution and others. Femorofemoral bypass remains a valuable operation in the treatment of these selected patients.
The issue of diversion away from a donor limb after operation either at rest or after exercise has never been totally resolved and depends on the status of the SFA on the same side. Various degrees of a steal may be incurred. I would appreciate your commentary on whether iliofemoral bypass should be used more often because of longer lasting patency.
Two prominent articles on this subject I make reference to are: one published in 1991, in the American Journal of Surgery, and the other published in the British Journal of Surgery in 1992. The clinical and hemodynamic steal that seems to be present in less than 5% of patients remains an tmsolved problem. Can you use duplex scanning or ABI as a hemodynamic measure of progression of disease?
Because your study period was nearly 11 years, I
wonder whether all the surgical techniques are actually comparable. Why were the femorofemoral bypasses per- formed in this group of patients? Did you consider this group to be a population at high risk, or did you select this procedure in preference to an iliofemoral bypass? Was the donor limb of the iliac artery evaluated through noninva- sive arteriography measures such as hemodynamic pressure measurements with and without intraarterial papaverine to document pressure gradients? You suggest that there were problems with the use of PTA to dilate the donor lliac artery. Did you document pressure gradients before and after PTA? Did the use of PTA stents in conjunction with the PTA in the long-term patency rates of those two groups really make a difference? Was the cause of graft failure the usual problem of rtm-offor was it progression of the disease in the iliac limb?
Dr. Enrique Criado. We have had very limited experience with the use of iliofemoral bypass instead of femorofemoral bypass; as a matter of fact, I believe we have had 13 such cases. Our experience has been positive, but we do not have enough data to analyze it. I t is not clear from the literature whether iliofemoral bypass is superior to femorofemoral bypass.
In terms of the comparability of surgical techniques during the l 1-year period, Drs. Johnson, Burnham, and Keagy were the operating surgeons in the first part of the study in most cases, and I have added a few to the series during the last few years. I do not believe that there were any important variations in the technique.
With regard to the possibility of steal syndrome after

JOURNAL OF VASCULAR SURGERY Volume lS, Numlx~r S Criado et al. 505
femorofemoral bypass, we found in a group of about 30 patients with synchronously patent femorofemoral bypass grafts that the donor limb ABI decreased significantly in most patients immediately after surgery. However, on follow-up, we saw that months to years later, the ABI in the donor limb returned to preoperative levels. This reduction in the ABI did not result in symptoms of claudication or rest pain in any patients. I believe that the so-called steal syndrome is rarely clinically relevant.
With regard to the evaluation of the donor iliac artery before surgery, we favored the use of duplex scanning with measurement of acceleration times. We believe that a prolonged acceleration time has good predictive value for significant aortoifiac stenosis, with arteriography used as the gold standard.
With regard to the preoperative PTA, all patients had gradients measured before and after PTA, and those gradients disappeared in most cases. There were no stents used in this group of patients because most of the PTAs were performed before the era ofstenting. In terms of how to assess these patients for progression of disease, it is difficult to assess the causes of failure in most patients; however, progression of distal occlusive disease is probably what makes these grafts fail. We use acceleration times to monitor the inflow in the donor limb, and when the acceleration time is prolonged, typically more than 122 milliseconds, that prompts us to obtain arteriograms. We have been satisfied in finding significant lesions in these situations.
Dr. Ali F. AbuRahma (Charleston, W.V.). With regard to the iliac balloon angioplasty that you performed, you indicated that there was more failure for these patients. I am curious whether you examined the length oftbe lesion and whether it might be that the longer the lesion, the worse were the patency rates.
You concluded that daudication or trophic changes were equivalent. I am curious whether it would be more objective to have studied the preoperative Doppler ABI, which might give us a better understanding of the runoff. Was there any difference between an ABI of above or below 0.5 in terms of patency rate?
Dr. Criado. All patients who underwent preoperative donor iliac artery PTA had their gradients resolved. We did not find any statistically significant difference in the patency rates in patients with preoperative donor iliac artery PTA. However, the number of patients in this group is small, and I do not believe it allows one to give a definite answer. We have examined these patients and get larger numbers to answer this question.
There was a significantly lower ABI in the recipient limb of patients with threatened ischemia compared with patients with claudication. However, although patients with claudication tended to have a greater improvement, the difference was not statistically significant after opera- tion. The reason for this is that in the group of patients with limb-threatening ischemia, there was a greater number of outflow procedures performed concomitantly with the femorofemoral bypass.
Copyright © 2022 FDOKUMEN