
Ser-estar no sertão: capítulos da vida como filosofia visceral
Upload
uam-xochimilcoCategory
view
0download
0
|l | l _l _ s * 111 1|#w } s * s r _ _ ji 1t & sl - _ _ E __ A iW n iL w ^ J - J ] t JI | _ - - _ 1 - Z d | tX = a s _s w _ - A 1 i s| | _ * * _ s ;_I n _ _ - l - _Intestinal Transplantation in CompositeVisceral Grafts or Alone
SATORU TODO, M.D.,*tt ANDREAS G. TZAKIS, M.D.,*tt KAREEM ABU-ELMAGD, M.D.,*t JORGE REYES, M.D.,*tKENJIRO NAKAMURA, M.D.,*t ADRIAN CASAVILLA, M.D.,*t RICK SELBY, M.D.,* BAKR M. NOUR, M.D.,*t
HARLAN WRIGHT, M.D.,*t JOHN J. FUNG, MD, PH.D.,*tt ANTHONY J. DEMETRIS, M.D.,t§DAVID H. VAN THIEL, M.D.,*t and THOMAS E. STARZL, M.D., PH.D.*tt
Under FK 506-based immunosuppression, the entire cadaversmall bowel except for a few proximal and distal centimeterswas translated to 17 randomly matched patients, of whom twohad antigraft cytotoxic antibodies (positive cross-match). Eightpatients received the intestine only, eight had intestine in con-tinuity with the liver, and one received a full multivisceral graftthat included the liver, stomach, and pancreas. One liver-intestinerecipient died after an intestinal anastomotic leak, sepsis, andgraft-versus-host disease. The other 16 patients are alive after1 to 23 months, in one case after chronic rejection, graft removal,and retransplantation. Twelve of the patients have been liberatedfrom total parenteral nutrition, including all whose transplan-tation was 2 months or longer ago. The grafts have supportedgood nutrition, and in children, have allowed growth and weightgain. Management of these patients has been difficult and oftencomplicated, but the end result has been satisfactory in mostcases, justifying further clinical trials. The convalescence of theeight patients receiving intestine only has been faster and moretrouble free than after liver-intestine or multivisceral transplan-tation, with no greater difficulty in the control of rejection.
Tn HE INTESTINE was one of the first organs to betransplanted experimentally," 2 but the last to beengrafted successfully in humans. In spite of nu-
merous attempts between 1964 and 1987,3 there were noclinical examples of a functioning intestinal graft untilNovember 1987. Then, a 3-year-old girl began a 6-monthperiod of enterally supported survival after receiving amultivisceral abdominal graft that contained all of thehollow abdominal organs plus the liver and pancreas.4 Ina similar operation 1 year later, Grant et al.' transplantedthe small bowel in continuity with the liver to a recipient
Presented at the I 12th Annual Meeting of the American Surgical As-sociation, April 6-8, 1992, Palm Desert, California.
Supported by Research Grants from the Veterans Administration andProject grant No. DK 29961 from the National Institutes of Health,Bethesda, Maryland.
Address reprint requests to Thomas E. Starzl, M.D., Ph.D., Departmentof Surgery, 3601 Fifth Avenue, Falk Clinic 5C, Pittsburgh, PA 15213.
Accepted for publication April 10, 1992.
From the Departments of Surgery* and Pathology,§University of Pittsburgh School of Medicine,t and the
Veterans Administration Medical Center,*Pittsburgh, Pennsylvania
who is still alive and eating along with a handful of otherpatients treated with variations of the multivisceral pro-cedure.6'7 In contrast, there have been only two examplesoflong survival and function ofcadaveric intestinal graftswhen these were transplanted alone.6'8The prospects for progress in this difficult field were
improved with the demonstration in rat intestinal andmultivisceral transplant models ofthe superior therapeuticindex of the new immunosuppressive drug FK 506.9-2We report here our experience using this drug for onerecipient ofthe originally described full multivisceral graft,eight recipients of liver-intestine grafts, and eight patientswho were given small intestine only. Sixteen of these 17patients are alive after 1 to 23 months, and most ofthemare eating. This experience has opened up new optionsfor the treatment of end-stage intestinal disease with orwithout liver involvement and seems certain to greatlyinfluence the future development and practice of gastro-enterology.
Methods
Case Material
Recipients. The intestinal diagnosis in 15 of the 17 pa-tients was short-gut syndrome in which the intestine hadbeen resected for a variety of reasons; the intestine in theother two recipients had uncorrectable disease (Table 1).All ofthe patients were on total parenteral nutrition (TPN)before transplantation for 1 to 132 (40.9 ± 41.9 [standarddeviation]) months (Table 1) and all had experienced morethan one episode of sepsis, liver damage, or other TPN-related complications.
223

TODO AND OTHERS
C)
Cs
: - u -;>
.a! e a! CZ
=no e:,1
) 0
Ann. Surg. - September 1992
CZcr 0ct
QC OCO*c* CO
U U. a a.L~ LC)J L L L4.JLJ L L~ JL L L PuC
o al enen; 6 0 1 0Cl
l C _ _ _
A A A A A
-6r-oc n o-n r- r--- r- V~
AAA A
I I o
° 1 1 °
ON
oo QN6l o6~ r-2c:: j6O 00r "C
- - I- -
en)rJ #Cf) #)
0000l
1-
It r- oo .rCE
o " -o ONoo r-66e e Ci O 6
A A A A A A A
o o
wo o o
Cl -C
00 00 C4 rn00
I--
.-I
cl
cl6 e
ri) rA rJ (I
o l toR_1tr. aT T o- 00 O0 0 - - -0 0
0 Cl 00" ~ ON£ o - oCl 10en Cl -CC1 el,) en
C~~~~~~~~~~C
-o CO CO0.~~~~~~~~~~~~.. 0
0A7 oCO .-OO0>H
CA C _C o oe e -
Itt t) 'IC -00 (ON ol _ t_ (I0v
C.
ct
._
ctC)
CZ
.-
0
C;
E
CA
C)m
cli
-o
00-.
C)
0..
COeC)3
-oc, O0
>
C)c)0F
_ .0
oQQ
* ~
0-
224
C)E
E0
u
Cl
s0
COr.
o oCZO0
-CO
*.CO r
>. O
CO-1 Ek1 ).
0
CO0
z
HL.
C)
au
O
C-)
C4
ZC)
LLz
Hz
20
C)
U.c
0.
o 0-0z
2
2
O
CZ
-L E
_
Hco _CLO
._o0t
*- ._0
0
-o
C)
r- e 00
CIA
I
INTESTINAL TRANSPLANTATION IN CON
Eight of the 17 patients were 21- to 50-year-old adults(mean age, 31.9 ± 9), and nine were children who were0.6 to 4.3 years of age (Table 1). The full multivisceralprocedure was in a 32-year-old man with protein S defi-ciency whose clotting abnormality had caused thrombosisof his superior mesenteric artery and celiac axis, with con-sequent intestinal gangrene. Because the liver is the sourceof protein S,'3 its inclusion in the graft was obligatoryeven though hepatic failure was not present. All eight pa-tients undergoing liver-intestine transplantation (twoadults, six children) had advanced hepatic disease withserum total bilirubin concentration from 6.3 to 50 mg/dL. The eight patients (five adults, three children) givenisolated small bowel grafts were jaundice free, althoughmost had minor liver function abnormalities.
Transplantation Procedures
Donors. Cadaveric donors ofsimilar or smaller size wereselected, all being ABO blood group identical with therespective recipients. Human leukocyte antigen matchingwas random and uniformly poor. The lymphocytotoxiccross-match was positive in two patients.The principles'4 as well as details'5 of the donor oper-
ations have been described elsewhere and included aneffort at selective bacterial and fungal decontamination.The contents of the intestinal lumen were not mechani-cally washed during the donor operation or afterward.Instead, the proximal and distal ends ofthe intestine weresealed with a stapling machine, carrying and transplantingthe succus entericus to the recipient. Initial cooling ofthegraft was by infusion with cold University of Wisconsin(UW) solution, the volume of which was limited to 1 Lin adult donors to prevent infusion injury.'5 Cold ischemiatimes were 2.8 to 10.6 hours (Table 1). For reasons dis-cussed elsewhere,'4 no effort was made to alter the lym-phoreticular (immunologic) component of the graft withantilymphoid agents, irradiation, or other means.
PYA SMA
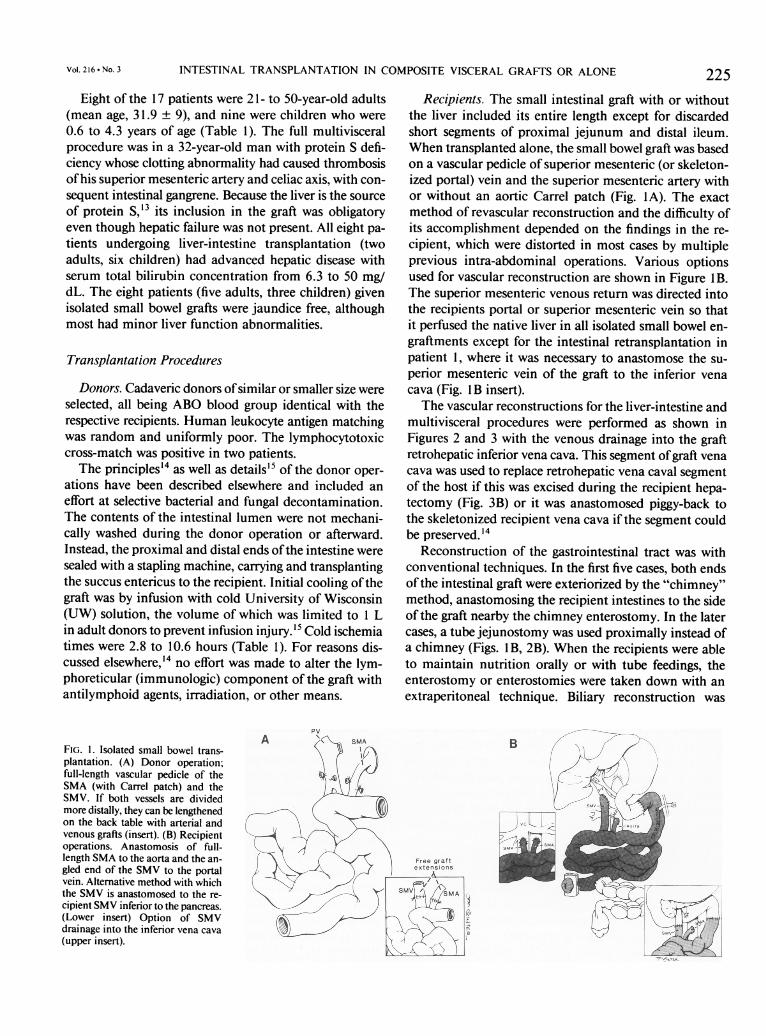
FIG. 1. Isolated small bowel trans-plantation. (A) Donor operation;full-length vascular pedicle of theSMA (with Carrel patch) and theSMV. If both vessels are divided
more distally, they can be lengthenedon the back table with arterial andvenous grafts (insert). (B) Recipient
operations. Anastomosis of full-length SMA to the aorta and the an-
gled end of the SMV to the portalvein. Alternative method with which
the SMV is anastomosed to the re-
cipient SMV inferior to the pancreas.(Lower insert) Option of SMV
drainage into the inferior vena cava(upper insert).
4POSITE VISCERAL GRAFTS OR ALONE 225
Recipients. The small intestinal graft with or withoutthe liver included its entire length except for discardedshort segments of proximal jejunum and distal ileum.When transplanted alone, the small bowel graft was basedon a vascular pedicle of superior mesenteric (or skeleton-ized portal) vein and the superior mesenteric artery withor without an aortic Carrel patch (Fig. 1A). The exactmethod of revascular reconstruction and the difficulty ofits accomplishment depended on the findings in the re-cipient, which were distorted in most cases by multipleprevious intra-abdominal operations. Various optionsused for vascular reconstruction are shown in Figure l B.The superior mesenteric venous return was directed intothe recipients portal or superior mesenteric vein so thatit perfused the native liver in all isolated small bowel en-graftments except for the intestinal retransplantation inpatient 1, where it was necessary to anastomose the su-perior mesenteric vein of the graft to the inferior venacava (Fig. lB insert).The vascular reconstructions for the liver-intestine and
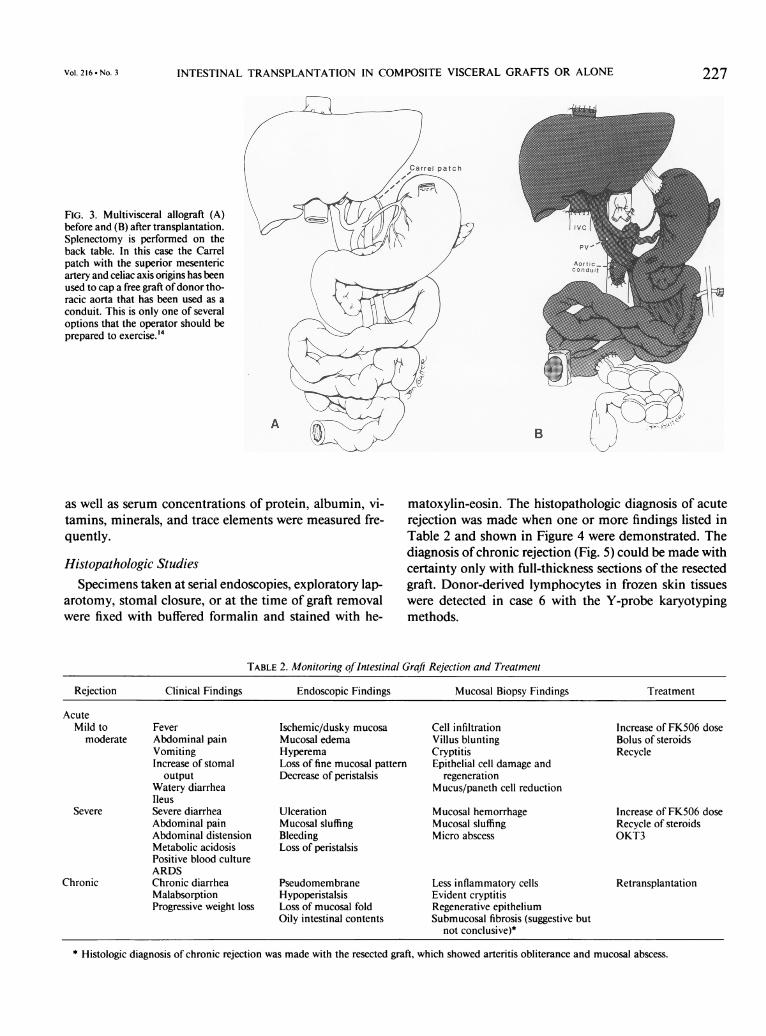
multivisceral procedures were performed as shown inFigures 2 and 3 with the venous drainage into the graftretrohepatic inferior vena cava. This segment ofgraft venacava was used to replace retrohepatic vena caval segmentof the host if this was excised during the recipient hepa-tectomy (Fig. 3B) or it was anastomosed piggy-back tothe skeletonized recipient vena cava if the segment couldbe preserved.'4
Reconstruction of the gastrointestinal tract was withconventional techniques. In the first five cases, both endsofthe intestinal graft were exteriorized by the "chimney"method, anastomosing the recipient intestines to the sideof the graft nearby the chimney enterostomy. In the latercases, a tube jejunostomy was used proximally instead ofa chimney (Figs. 1 B, 2B). When the recipients were ableto maintain nutrition orally or with tube feedings, theenterostomy or enterostomies were taken down with anextraperitoneal technique. Biliary reconstruction was
Vol. 216 - No. 3

TODO AND OTHERS
FIG. 2. (A) Small bowel-liver allo-graft. Note the continuity of donorportal vein. (B) Recipient operation.Carrel patch containing the origin ofthe SMA and the celiac axis is anas-tomosed to the aorta. Ideally, thevenous return from residualsplanchnic viscera ofthe recipient isrouted by vascular anastomosis intothe graft portal vein. Numerous op-tions of graft rearterialization andvenous drainage have been describedelsewhere. 14
B
performed by Roux-en-y choledochojejunostomy in theliver-intestine recipients (Fig. 2B). Cholecystectomy was
carried out in all native (Fig. 1) or allograft livers (Figs. 2and 3).
Management
Immunosuppression. FK 506 (0.1 to 0.15 mg/kg/day)by continuous intravenous infusion was begun immedi-ately after graft revascularization. When enteral feedingwas started, FK 506 was switched to a twice-daily oralformulation with several days of overlap. Plasma levelsofFK 506 (trough target, ng/mL) were measured dailyduring the hospital stay, 2 or 3 times/week for the first 3months, and at longer intervals thereafter.
Methylprednisolone also was started intraoperatively(first dose of 200-mg bolus) and rapidly weaned by dec-rements of40 mg/day over the next 5 days to 20 mg/day.Prostaglandin El (prostin) at 0.6 to 0.8 ,ug/kg/hour, was
began intraoperatively in the last nine patients and con-
tinued for 7 to 14 days. The FK 506-prednisone-prosta-glandin cocktail has given superior results in liver trans-plant patients, including those with positive cytotoxiccross-matches. 16
Rejection was treated with an upward dose adjustmentofFK 506 when this was possible without nephrotoxicity,augmentation of steroids, and OKT3 when necessary.'7
Infection. The same kind of selective decontaminationused in the donor was begun before operation in the re-
cipient and continued for 4 weeks after transplantation.Systemic antibiotics were given for the first 5 days ac-
cording to the results of frequent cultures of the blood,stool, urine, sputum, wound exudate, and peritoneal dis-charge. Chronic virus and protozoal prophylaxis was withacyclovir (for cytomegalovirus) and Bactrim (Roche Lab-oratories, Nutley, NJ; for Pneumocystis carinii).
Nutrition. Total parenteral nutrition was tapered grad-ually when enteral feeding with a jejunal tube was com-
menced with Peptamen (Clintec Nutrition Co., Deerfield,IL), an isotonic elemental diet that contains peptide-basedprotein, medium-chain triglycerides, and glutamine.Later, Peptamen was converted in children to Compleat(Sandoz, East Hanover, NJ), a lactose- and gluten-freediet that contains dietary fibers to promote normalizationof intestinal motility function.
MonitoringRejection. When the diagnosis was suspected clinically,
endoscopy was performed and mucosal biopsies were ob-tained for histopathologic analysis. Adjustments in im-munosuppression were dependent mainly on the biospyfindings in a decision-making process summarized in Ta-ble 2.
Graft Function. Standard liver and pancreas functiontests were used to follow the function ofthese solid organs.
The transplanted and host hollow viscera were studiedwith repeated endoscopy. Upper gastrointestinal serieswith barium meal were performed periodically to deter-mine changes of mucosal foldings and the duration ofgastric emptying and intestinal transit time. Absorptionof d-xylose and fat was measured with the methods ofBreiter et al.'8 and Amenta,'9 respectively. Body weight
226 Ann. Surg. * September 1992
Vol. 216 * No. 3 INTESTINAL TRANSPLANTATION IN COMPOSITE VISCERAL GRAFTS OR ALONE
FIG. 3. Multivisceral allograft (A)before and (B) after transplantation.Splenectomy is performed on theback table. In this case the Carrelpatch with the superior mesentericartery and celiac axis origins has beenused to cap a free graft ofdonor tho-racic aorta that has been used as aconduit. This is only one of severaloptions that the operator should beprepared to exercise.'4
as well as serum concentrations of protein, albumin, vi-tamins, minerals, and trace elements were measured fre-quently.
Histopathologic Studies
Specimens taken at serial endoscopies, exploratory lap-arotomy, stomal closure, or at the time of graft removalwere fixed with buffered formalin and stained with he-
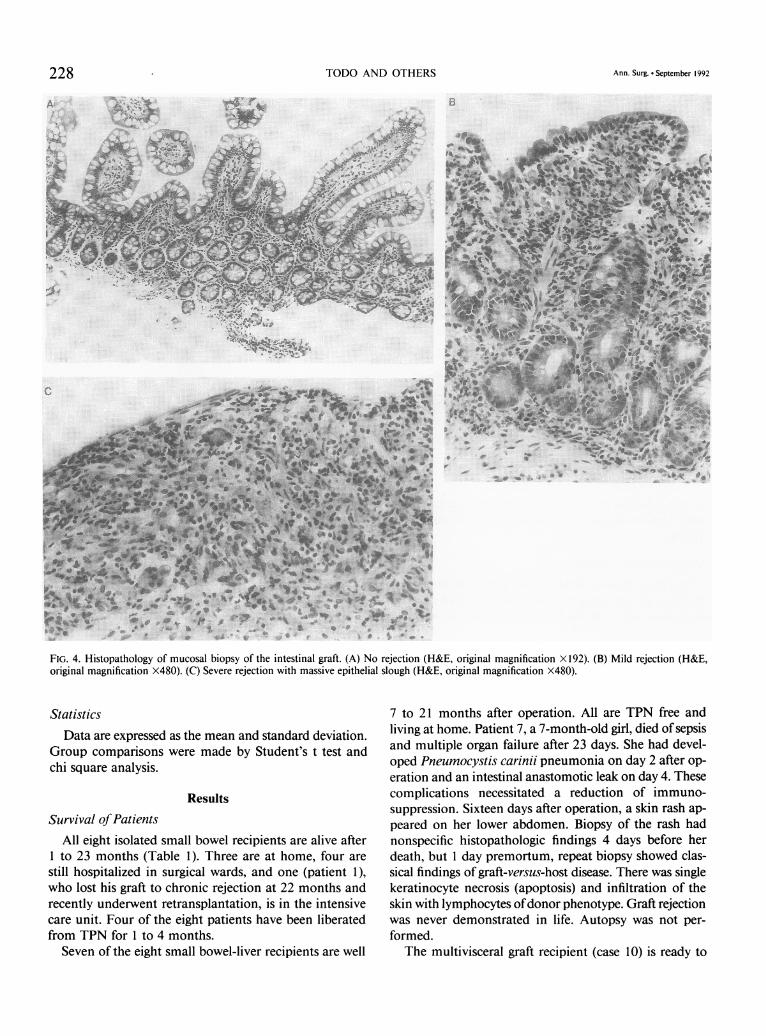
matoxylin-eosin. The histopathologic diagnosis of acuterejection was made when one or more findings listed inTable 2 and shown in Figure 4 were demonstrated. Thediagnosis ofchronic rejection (Fig. 5) could be made withcertainty only with full-thickness sections of the resectedgraft. Donor-derived lymphocytes in frozen skin tissueswere detected in case 6 with the Y-probe karyotypingmethods.
TABLE 2. Monitoring ofIntestinal Graft Rejection and Treatment
Rejection Clinical Findings Endoscopic Findings Mucosal Biopsy Findings Treatment
AcuteMild to Fever Ischemic/dusky mucosa Cell infiltration Increase of FK506 dose
moderate Abdominal pain Mucosal edema Villus blunting Bolus of steroidsVomiting Hyperema Cryptitis RecycleIncrease of stomal Loss of fine mucosal pattern Epithelial cell damage and
output Decrease of peristalsis regenerationWatery diarrhea Mucus/paneth cell reductionIleus
Severe Severe diarrhea Ulceration Mucosal hemorrhage Increase of FK506 doseAbdominal pain Mucosal sluffing Mucosal sluffing Recycle of steroidsAbdominal distension Bleeding Micro abscess OKT3Metabolic acidosis Loss of peristalsisPositive blood cultureARDS
Chronic Chronic diarrhea Pseudomembrane Less inflammatory cells RetransplantationMalabsorption Hypoperistalsis Evident cryptitisProgressive weight loss Loss of mucosal fold Regenerative epithelium
Oily intestinal contents Submucosal fibrosis (suggestive butnot conclusive)*
* Histologic diagnosis of chronic rejection was made with the resected graft, which showed arteritis obliterance and mucosal abscess.
227
TODO AND OTHERS Ann. Surg. * September 1992
B
FIG. 4. Histopathology of mucosal biopsy of the intestinal graft. (A) No rejection (H&E, original magnification X 192). (B) Mild rejection (H&E,original magnification X480). (C) Severe rejection with massive epithelial slough (H&E, original magnification X480).
Statistics
Data are expressed as the mean and standard deviation.Group comparisons were made by Student's t test andchi square analysis.
Results
Survival ofPatientsAll eight isolated small bowel recipients are alive afterto 23 months (Table 1). Three are at home, four are
still hospitalized in surgical wards, and one (patient 1),who lost his graft to chronic rejection at 22 months andrecently underwent retransplantation, is in the intensivecare unit. Four of the eight patients have been liberatedfrom TPN for to 4 months.
Seven of the eight small bowel-liver recipients are well
7 to 21 months after operation. All are TPN free andliving at home. Patient 7, a 7-month-old girl, died of sepsisand multiple organ failure after 23 days. She had devel-oped Pneumocystis carinii pneumonia on day 2 after op-eration and an intestinal anastomotic leak on day 4. Thesecomplications necessitated a reduction of immuno-suppression. Sixteen days after operation, a skin rash ap-peared on her lower abdomen. Biopsy of the rash hadnonspecific histopathologic findings 4 days before herdeath, but day premortum, repeat biopsy showed clas-sical findings of graft-versus-host disease. There was singlekeratinocyte necrosis (apoptosis) and infiltration of theskin with lymphocytes ofdonor phenotype. Graft rejectionwas never demonstrated in life. Autopsy was not per-
formed.The multivisceral graft recipient (case 10) is ready to
228

INTESTINAL TRANSPLANTATION IN COMPOSITE VISCERAL GRAFTS OR ALONE
FIG. 5. Histopathology of chronicrejection of the removed intestinalgraft. (A) Apoptosis of crypt cells(insert, H&E, original magnificationX480) with sparse inflammatory cellinfiltration (H&E, original magnifi-cation X192). (B) Arteritis obliter-ance seen at the subserosal layer(H&E, X480).
be discharged on full oral nutrition after staying in theintensive care unit for 2 months because of postoperativepulmonary insufficiency requiring ventilation.
Survival ofGrafts
Fifteen of the 17 original grafts remain in place. Inaddition to the liver-intestinal transplant lost by death(case 6), an isolated intestinal graft was resected after 22months (case 1) and replaced by retransplantation 3 weekslater. Recovery from the primary transplantation wasstormy, with bouts of severe rejection, sepsis, and renalfailure, and several later episodes of graft rejection asso-ciated with drug noncompliance. Serial intestinal biopsiesshowed apoptoses of crypt cells with sparse inflammatorycell infiltration, suggesting chronic rejection of the graft(Fig. 4A). An angiogram performed at 19 months dem-onstrated narrowing ofthe peripheral mesenteric arteries,which was worse on a repeat study at 22 months, leadingto the decision for graft enterectomy. The resected grafthad mucosal ulceration, abscesses, and arteritis obliterance(Fig. 4B).
Nongastrointestinal Morbidity
The early convalescence of most of the recipients wasprolonged and complicated. Irreversible renal failure de-veloped in patient 1, necessitating cadaver renal trans-plantation 19 months later, and in patient 10, whose pro-tein S deficiency already had been responsible for renalartery thrombosis and loss of one kidney. A third patient(case 9), who had undergone earlier nephrectomy after a
V
IIs
i,
..~~~~~~~~~~~~~~~~~~~~~e
]: . __ o '}~~o
traffic accident, required temporary hemodialysis aftertransplantation.
Because of paralysis of the right hemidiaphragm, anintestine-liver recipient (patient 5) required respiratorysupport for 300 days. Another child (case 4) with the sameoperation became permanently paraplegic after a lumberpuncture. An adult (patient 3) underwent femoral arterialgrafting for treatment of a pseudoaneurysm caused by afemoral arterial puncture.
Gastrointestinal Morbidity
Rejection. Three patients (cases 6, 7, and 12) had nohistopathologic evidence of rejection during their follow-up of23, 234, and 97 days. In the other 14, some evidenceof acute rejection was first demonstrated with mucosalbiopsy at a mean postoperative time of 15.5 ± 7.8 days(range, 7 to 55). This usually was mild or moderate. Nearlytotal denudation of the mucosa by severe graft rejection,however, developed on four occasions in three patients(case 1, days 14 and 167; case 4, day 74; case 5, day 137).This was reversed with complete healing within 1 to 2weeks after a management adjustment. Two courses ofOKT3 were given each to patients 1 and 10.
Unexpectedly, the incidence of graft rejection in thefirst 2 months after isolated small bowel transplantationwas lower than after combined liver-intestine or multior-gan transplantation (Table 3). In six of the nine graftscontaining liver and intestine (eight liver-intestine andone multivisceral), the incidence of rejection was similarin both organs. Rejection was more prevalent in the liver
229VOl. 216.- NO. 3

TODO AND OTHERS
TABLE 3. Comparison ofEarly Postoperative Course* in Recipients After Small Bowel Versus Small Bowel/Liver Transplantation
Graft Small Bowel Small Bowel/Liver
Caset 5 7Pediatric 3 5Adult 2 2
ICU stay (days) 7.6 (5-14) 63 (3-300)Hospital stay (mo) 3.9 (1-12) 5.2 (3-10)ImmunosuppressiontFK506 (mg/kg/day)
IV dose 0.09 (0.06-0.12) 0.07 (0.05-0.13)Oral dose 0.4 (0.2-0.70) 0.2 (0.1-0.5)Plasma level (ng/ml) 3.0 (1.7-6.2) 1.9 (1.5-2.6)
Steroid (mg/kg/day)IV dose 0.6 (0.3-1.0) 0.4 (0-1.0)Oral dose 0.2 (0-0.3) 0.3 (0-1.2)
Imurane (mg/kg/day) 1.0 (0-0.3) 0.2 (0-1.3)PGE, 4 patients 1 patient
No. of patients requiring adjuvant therapySteroid
Bolus 4 (80%) 7 (100%)Recycle 4 (80%) 1 (14%)
OKT3 1 (20%) 0 (0%)Small bowel rejection
No. of biopsies 30 29Histologic rejectionNone 26 (87%) 17 (59%)Mild to moderate 3 (10%) 12 (41%)Severe 1 (3%) 0 (0%)
NutritionEnteral feeding, started (days)§ 8.8 (5-14) 27.7 (11-37)TPN, stopped§ 30.5 (14-49) 123.1 (45-210)
Infectious episodes"l IViral 1 4Bacterial (translocation) 3 (2) 7 (3)Fungal (translocation) 2 (1) 2
* Findings within 2 months after transplantation.t Includes only patients with data for longer than 2 months (small
bowel cases 1, 11, 12, 13, and 14; small bowel-liver cases 2, 3, 4, 5, 7,8, and 9).
than in the intestine in the other three patients, however(case 2, 83% versus 27%; case 4, 53% versus 21%; case 5,85% versus 57%). On the 38 occasions on which both liverand small bowel biopsies were taken simultaneously or
closely together, 16 (42%) of the dual specimens had no
sign of rejection in either organs, nine (24%) had rejectionin both, nine (23%) had rejection only in the liver, andfour (1 1%) had rejection in the intestine only.
Infection. Microorganisms were detected in the bloodin eight patients at 21 occasions: Candida albicans (oneexample), enterococcus fecium/fecalis (six examples), co-
agulase-negative Streptococcus (four), cytomegalovirus(three), influenza hemophilus (one), and gram-positivecocci (six). Bacterial translocation was proven in four pa-
tients on six occasions, half ofwhich were associated withrejection: case 1 at day 57; case 2 at days 18 and 30; case
4 at days 7 and 21, and case 11 at day 15. Recipients ofisolated small bowel were neither more nor less prone toinfectious complications than the recipients of the com-
plex grafts (Table 3).
t Mean value (range).§ Statistically significant (p < 0.05).11 Number of episodes in each group of patients.
Small Bowel Function
Nutrition. Total parenteral nutrition was discontinuedafter 14 to 210 days (89.5 ± 69.7), the average periodbeing much shorter in isolated small bowel recipients thanin those with organ combinations (Table 3). All nine pe-
diatric patients had failed to learn (or had forgotten) toeat. Oral feeding had to be taught, and patients 5 and 7still prefer tube feeding to eating in spite of intensive re-
habilitation.Except for patient 6 (who died) or patients 1, 15, 16,
and 17, who were operated on recently, the other 12 re-
cipients are supported nutritionally solely with their func-tioning grafts. All recipients followed for more than 3months have maintained or gained body weight after 3months, with the exception of patient 1, who eventuallycame to retransplantation (Fig. 6).
Gastrointestinal motility. Gastric emptying in the earlypostoperative period was delayed from 3 to 12 hours inhalf of the recipients studied (7/14), but recovered spon-
230 Ann. Surg. September 1992

INTESTINAL TRANSPLANTATION IN COMPOSITE VISCERAL GRAFTS OR ALONE
Small Bowel
73t
Small Bowel / Liver 100
Time in months
FIG. 6. Body weight changes of the recipients after small bowel trans-plantation. Numbers indicate cases listed in Table 1. The seemingly poorerweight gain in the isolated small bowel recipients reflects the more recentcase accrual and consequent shorter follow-ups. Weight gain in eitherthe isolated small bowel or bowel-liver patients did not start until 2 or3 months.
00-
c
0).)L-xw
coLL.
C.)0)U.
90
80
70
60
50
40
30
20
10
0
231
0
0
0
+
0
A
A
0
.
aRange/ ///>/ -K ... ." .. .
0
I . I I. . I . . I I I I .
3 6 9 12 1 5 18 21
Months After SB Transplant
taneously after 4 to 6 months. Tan abnormality of the intestinalwas markedly accelerated (less*prolonged (more than 3 hours)studied later, these abnormalitic
Absorption. D-xylose absorpt12 patients 1 to 22 months aftein six, slightly abnormal in five,The amount of the total fecal liearly postoperative period, andnormal in some patients as longtation (Fig. 8).
Discussic
There are metabolic and imnin planning the transplantationorgans. At one time, it was suspe
Small Bowel
TIME IN M
FIG. 7. D-Xylose absorption test in the reiplantation. Most recent data are shown (study).
en ofthese recipients hadIgraft transit time, whichfhn'n 1 h..ill-I ;i r%*vt-
FIG. 8. Fecal fat excretion of the recipients after small bowel transplan-tation. Multiplication symbols indicate data from the same patient.
iLnanI i nouUr) inI sVCeve U1 be ameliorated with primary delivery of a graft's venousin the other three. When return through the liver through the portal vein.20 Evi--s were improved. dence supporting this hypothesis it applies to the in-
ion tests performed with testine, however, has not been obtained by direct testingr operation were normal in rats.21-23 Thus, efforts to drain the transplanted intestine
ipids was usually high at
transportally for immunologic reasons have little justifi-fatabsorption
ws
usu ill abt cation.fat absorption is still ab- There are significant metabolic reasons, however, to
,as a year after transplan- try to have transportal venous drainage. Either the nativeor the transplanted liver is subject to adverse Eck fistula(portaprival) effects to the extent that the so-called he-
Dn patotrophic factors in the venous effluent from the pan-
nunologic considerations creas (principally insulin) and intestine (nutrients and en-of the intra-abdominal teric hormones) are diverted from it.24-26 Consequently,
cted that rejection would the ability to use techniques that drain the intestinal ve-nous return transportally was noteworthy. In cases inwhich the intestine was transplanted alone, it was routinely
Small Bowel/Liver possible to its through the native liver
instead of resorting to the technically more expedient op-
io tion of mesocaval drainage.27 Similarly, when the intestine4, 191) and liver were transplanted together, the metabolic ob-
,0- / jective was systematically met of draining the venous re-
5) turn from the recipient's pancreas and other residuale (5, 253) splanchnic organs, through the transplanted liver.
An important additional question ofbasic immunologic/7, 1111 as well as practical surgical interest is how protective (to-
lerogenic) a concomitantly transplanted liver is of other
organ allografts from the same donor. 10,28.29 Hepatic to-
138, 73) lerogenicity has been confirmed in numerous experimen-0 tal models and could be used as an argument to replace0 30 60 90 120 the liver as an "expediter" for the intestine even thoughIINUTES it is normal.5'7 The persuasiveness of this proposition hascipients after smallboweltr been enhanced by the rejection in the past of almost allcipients after small bowel trans-
(case, postoperative days of the reported isolated cadaveric small bowel transplants in hu-mans.
Vol. 216 * No. 3
a
I

232 TODO AND OTHERS
Our experience suggests on the contrary that the lessdraconian procedure of isolated small bowel transplan-tation is the procedure of choice if the only need is forthe intestine. This would reserve the multivisceral or liver-intestinal operations, as has been our policy, for specificindications such as coexisting liver failure or a hepaticinborn error (exemplified by the protein S deficiency inour case 10). Although in no way interdicting the hepatictolerogenicity concept, our results indicate that the im-munologic advantage of a coexisting liver graft is not anobligatory condition for successful intestinal transplan-tation. In fact, the greater ease, lower expense, and aboveall greater safety of the isolated intestinal procedureemerged clearly from our series, which is the first that hasbecome available for such analysis. Realization of thepracticality of isolated intestinal transplantation shouldbe an incentive to intervene earlier in selected cases beforethe advent of the poorly understood secondary hepaticinjury that is associated with TPN.The list of indications for isolated intestinal transplan-
tation in addition to the short gut syndrome already isemerging and so far in our series has included inflam-matory bowel (Crohn's) disease, microvillus inclusiondisease, intestinal pseudo-obstruction, and a nonresectabledesmoid tumor in a patient with Gardner's syndrome. Itis too early to predict how good the function will be ofthe chronically tolerated intestinal graft, whether it istransplanted alone or as part ofan organ complex. Nearlynormal intestinal allograft function, however, has beendescribed in rats'0 and pigs.30 Dogs had the subnormalfat and d-xylose absorption detected in some of our pa-tients,3' but in spite of the imperfect laboratory tests, mostof the human recipients have had satisfactory nutrition,which improved with time.The ability to move forward with intestinal transplan-
tation has been facilitated by FK 506, not only becausethis drug has been shown by direct testing to provide morepotent immunosuppression than cyclosporine for protec-tion ofthe intestinal graft,9'-2 but also because its absorp-tion characteristics after oral administration are less in-fluenced by the presence or absence of bile, bile acids32and by the motility and function of the intestine itself.The oral doses of FK 506 in long-surviving patients nec-essary to maintain adequate plasma levels were very littledifferent (Table 3) from that in recipients of livers, hearts,or kidney.As these and previous trials proceeded, some of the
assumptions have come into question on which earlierclinical trials of intestinal transplantation were based. Forone thing, the monitoring of rejection has proven to be astraightforward exercise, depending on clinical judgmentand biopsy studies rather than on any kind of special test.Our procurement procedures also have evolved towardsimplicity. Past practices that were omitted included ex-
Ann. Surg. * September 1992
tensive infusion of cold preservation fluids during pro-curement, cleaning the lumen of its contents, and ma-neuvers to weaken the immunologic reactivity of thebowel's large lymphoreticular cell population. This lastpolicy has not resulted in a high incidence ofgraft-versus-host disease, as some had predicted.
Study of the intestinal graft may help to better under-stand graft-versus-host disease and its prevention. In ratsurvivors of intestinal or multivisceral transplantationunder FK 506, it was shown that the lymphoid and den-dritic cells of the graft were rapidly replaced with similarrecipient cells,'0 whereas the donor cells migrated to andnested in recipient lymphoid and other tissues.33 Appar-ently these cells are nonreactive in their new locations tothe alien tissues in which they reside, and cause neitherrejection nor graft-versus-host disease, providing there iseffective immunosuppression. The same kind of cell trafficand repopulation has been documented in our humanintestinal and multivisceral recipients6'34 and probably isa generic phenomenon with the successful allotransplan-tation and xenotransplantation of all tissues and organs.35Ifthis latter concept is validated, it will change many con-cepts and dogmas of transplantation immunology.
References
1. Lillehei RC, Goott B, Miller FA. The physiologic response of thesmall bowel of the dog to ischemia including prolonged in vitropreservation of the bowel with successful replacement and sur-vival. Ann Surg 1959; 150:543.
2. Starzl TE, Kaupp HA Jr. Mass homotransplantation of abdominalorgans in dogs. Surg Forum 1960; 11:28-30.
3. Grant D. Intestinal transplantation: current status. Transplant Proc1989; 21:2869-2871.
4. Starzl TE, Rowe M, Todo S, et al. Transplantation of multiple ab-dominal viscera. JAMA 1989; 261:1449-1457.
5. Grant D, Wall W, Mimeault R, et al. Successful small-bowel/livertransplantation. Lancet 1990; 335:181-184.
6. Todo S, Tzakis AG, Abu-Elmagd K, et al. Cadaveric small boweland small bowel-liver transplantation in humans. Transplantation1992; 53:369-376.
7. McAlister V, Wall W, Ghent C, et al. Successful small intestinetransplantation. Transplant Proc 1992; 24:1236-1237.
8. Goulet 0, Revillon Y, Brousse N, et al. Successful small boweltransplantation in an infant. Transplantation 1992; 53:940-943.
9. Murase N, Kim D, Todo S, et al. Induction of liver, heart, andmultivisceral graft acceptance with a short course of FK 506.Transplant Proc 1990; 22:74-75.
10. Murase N, Demetris Aj, Matsuzaki T, et al. Long survival in ratsafter multivisceral versus isolated small bowel allotransplantationunder FK 506. Surgery 1991; 110:87-98.
11. Hoffman AL, Makowka L, Banner B, et al. The use of FK 506 forsmall intestine allotransplantation: inhibition of acute rejectionand prevention of fatal graft versus host disease. Transplantation1990; 49:483-490.
12. Lee K, Stangl MJ, Todo S, et al. Successful orthotopic small boweltransplantation with short term FK 506 immunosuppressivetherapy. Transplant Proc 1990; 22:78-79.
13. Stern DM, Brett J, Harris K, Nawroth PP. Participation ofendothelialcells in the protein C-protein S anticoagulant pathway: the syn-thesis and release of protein S. J Cell Biol 1986; 102:1971-1978.
14. Starzl TE, Todo S, Tzakis A, et al. The many faces of multivisceraltransplantation. Surg Gynecol Obstet 1991; 172:335-344.

INTESTINAL TRANSPLANTATION IN COMPOSITE VISCERAL GRAFTS OR ALONE
15. Casavilla A, Selby R, Abu-Elmagd K, et al. Logistics and techniquefor combined hepatic-intestinal retreival. Ann Surg (in press).
16. Takaya S, Iwaki Y, Starzl TE. Liver transplantation in positive cy-totoxic crossmatch cases using FK 506, high dose steroids, andprostaglandin El. Transplantation (in press).
17. Todo S, Fung JJ, Starzl TE, et al. Liver, kidney, and thoracic organtransplantation under FK 506. Ann Surg 1990; 212:295.
18. Breiter HC, Craig RM, Levee G, Atkinson AJ: Use ofkinetic methodsto evaluate d-xylose malabsorption in patients. J Lab Clin Med1988; 112:533.
19. Amenta JS. Lipiodol absorption and urinary lodide excretion as ascreening test for steatorrhea. Clin Chem 1969; 15(4):295-306.
20. Mazzoni G, Benichous J, Porter KA, Starzl TE. Renal homotrans-plantation with venous outflow or infusion of antigen into theportal vein of dogs or pigs. Transplantation 1977; 24:268-273.
21. Murase N, Demetris AJ, Furuya T, Todo S, Fung JJ, Starzl TE.Comparison of the small intestine after multivisceral transplan-tation with the small intestine transplanted with portal or cavaldrainage. Transplant Proc 1992; 24:1143-1144.
22. Gorczynski RM, Cohen Z, Levy G, Koh I. Comparison of functionalactivity in host and graft mesenteric lymphoid tissue of rats re-ceiving syngeneic heterotopic small bowel allografts with portalor systemic drainage. Transplant Proc 1992; 24:1133-1144.
23. Shaffer D, Diflo T, Love W, et al. Immunologic and metabolic effectsof caval versus portal venous drainage in small-bowel transplan-tation. Surgery 1988; 104:518-524.
24. Starzl TE, Porter KA, Francavilla A. The Eck fistula in animals andhumans. Curr Probl Surg 1982; 20:687-752.
23325. Koltun WA, Kirkman RL. Nutritional and metabolic aspects of
total small bowel transplantation in inbred rats. Transplant Proc1987; 19:1120-1122.
26. Schraut WH, Abraham VS, Lee KW. Portal versus caval venousdrainage of small bowel allografts: technical and metabolic con-sequences. Surgery 1986; 99:193-198.
27. Tzakis AG, Todo S, Reyes J, et al. Piggyback orthotopic intestinaltransplantation. Surg Gynecol Obstet (in press).
28. Calne RY, Sells RA, Pena JR, et al. Induction of immunologicaltolerance by porcine liver allografts. Nature 1969; 223:472-476.
29. Kamada N. The immunology of experimental liver transplantationin the rat. Immunology 1985; 55:369-389.
30. Grant D, Duff J, Zhong R, et al. Successful intestinal transplantationin pgis treated with cyclosporine. Transplantation 1988; 45:279-284.
31. Diliz-Perez HS, McClure J, Bedetti C, et al. Successful small bowelallotransplantation in dogs with cyclosporine and prednisone.Transplantation 1984; 37:126-129.
32. Furukawa H, Imventarza 0, Venkataramanan R, et al. The effectof bile duct ligation and bile diversion on FK 506 pharmacoki-netics in dogs. Transplantation 1992; 53:722-725.
33. Murase N, Demetris AJ, Woo J, et al. Lymphocyte traffic and graft-versus-host disease after fully allogeneic small bowel transplan-tation. Transplant Proc 1991; 23:3246-3247.
34. Iwaki Y, Starzl TE, Yagihashi A, et al. Replacement of donor lym-phoid tissue in human small transplant under FK 506 immu-nosuppression. Lancet 1991; 337:818-820.
35. Starzl TE, Demetris AJ, Murase N, et al. Cell migration, chimerism,and graft acceptance. Lancet 1992; 339:1579-1582.
DISCUSSION
DR. RONALD W. BuSUTTIL (Los Angeles, California): This presen-tation represents a major advance in small intestinal transplantation andaffirms the pioneering position in transplantation of Dr. Starzl and hiscolleagues.We also have been interested in small intestinal transplantation at
UCLA and initiated a program in July of 1991. Our first case that Iwould like to share with you has many similarities to the series reportedhere. Our recipient was a 19-year-old man with a short gut syndromesecondary to a stab wound to the superior mesenteric artery. A combinedliver-small bowel transplant using an ABO-matched, HLA-mismatchedallograft was performed under quadruple immunosuppression includingOKT-3, cyclosporine, low-dose Imuran, and steroids.
The graft was placed orthotopically with portal drainage ofthe recipientdirected into the donor's portal vein. Severe rejection of both the liverand the intestine occurred on postoperative day 26. Within 24 hours,severe mucosal ulcerations developed that went on to sloughing of theentire mucosa.
[Slide] This shows you the upper gastrointestinal tract during the boutof severe rejection. And you can see there is loss of the feathered edgeof the mucosa with a pseudomembrane formation. The episode wasrefractory to steroids and anti-lymphocyte preparations but reversed withFK506.
His recovery after this episode of rejection was uneventful and he wasdischarged after 21/2 months on total oral feedings and is now under thecare of our recorder, Dr. Clyde Barker.
In the interim, we found it very useful to have a jejunal feeding tubeas was described by Dr. Todo and his colleagues and also to place a
gastrostomy tube. We encountered a very difficult 2-month period ofunexplained and refractory gastric paresis, which was also seen, I believe,by the Pittsburgh group. This fortunately subsequently resolved. The J-tubes and the G-tubes, however, were invaluable during this critical periodfor enteral feedings to bypass the stomach.
Dr. Todo, I would like to ask you three questions. We have also usedprostaglandin El in our liver patients, the benefits of which may beachieved from its vasodilatory properties, smooth muscle relaxation, andmild immunosuppressive properties. Could you expand on how the
FK506 prostaglandin cocktail has given superior results and if this spe-cifically applies only to small bowel grafts?
Secondly, there are numerous experimental studies confirming thedifficulty of diagnosing small intestinal rejection given the segmentalnature of the rejection process. Could you comment on the adequacyof mucosal biopsies in your series for diagnosing small intestinal rejection,and did you find any instances of clinical rejection in the presence ofnormal biopsies?
Third, what is your explanation of the gastric paresis that you saw inyour patients, and was it related to abnormalities in the jejunal pace-makers?And finally, it is generally acknowledged that the liver provides an
immunologically favorable environment for other organs transplantedfrom the same donor. In your paper, however, you note that the incidenceof graft rejection in the first 2 months was lower in isolated intestinalgrafts versus multivisceral transplants and combined liver-small intestinalgrafts. Additionally, in three of the nine liver-small bowel grafts, therejection was more severe in the liver than it was in the small intestine.Do you have any theory to explain this, and do you think that it isprobably related to the use of FK506?
DR. FELIX T. RAPAPORT (Long Island, New York): President Thomp-son, members, and guests: I enjoyed both papers, and I want to congra-tulate Dr. Todo on his outstanding presentation of what may well be anhistoric paper.
Until recently, cluster and intestinal transplants were considered rel-atively futile. In fact, I remember many years ago, when Tom Starzl firstpresented his cluster procedures here, one ofour great leaders, Dr. Long-mire, arose to question why he bothered. Why did he not just wheel thepatient from the donor room to the recipient room, and then trade places?Well, we have now come full swing around. With the advent of newimmunosuppressants, we have gradually seen the so-called "forbiddenorgans" come into the fold and within the range ofclinical transplantation.This applies to the cluster procedures, to small intestinal transplants,and to many other procedures to come. To a large extent, this is due toexplosive development in our understanding of the immunologic reactionat the efferent and afferent arcs, and to the use of increasingly specific
Vol. 216 No. 3
Copyright © 2022 FDOKUMEN




















