
Reduction of myocardial infarct size by human mesenchymal stem cell conditioned medium

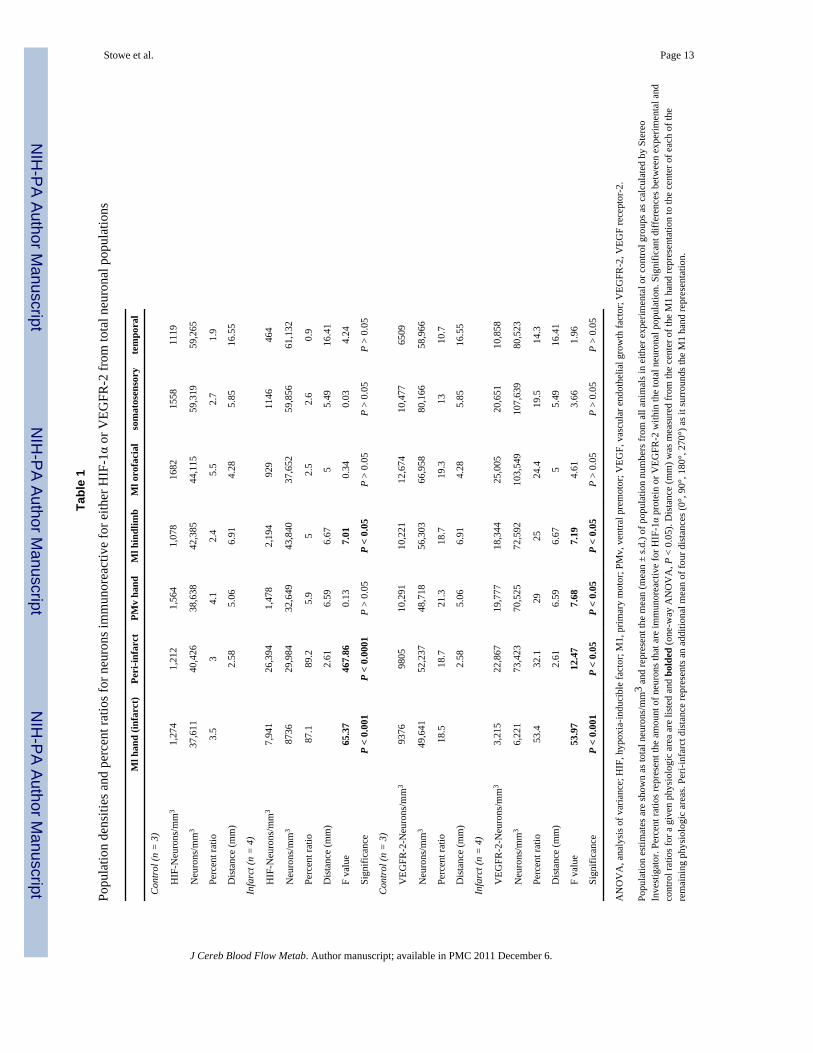
Neuronal HIF-1α protein and VEGFR-2 immunoreactivity infunctionally related motor areas following a focal M1 infarct
Ann M Stowe1, Erik J Plautz2, Phuong Nguyen3, Shawn B Frost2, Ines Eisner-Janowicz2,Scott Barbay2, Numa Dancause4, Anirban Sensarma2, Michael D Taylor5, Elena VZoubina2, and Randolph J Nudo2
1Department of Neurological Surgery, Washington University in St Louis, Missouri, USA2Department of Molecular and Integrative Physiology, and Landon Center on Aging, University ofKansas Medical Center, Kansas City, Kansas, USA3Department of Cytopathology, University of Nebraska Medical Center, Omaha, Nebraska, USA4Department of Neurology, University of Rochester Medical Center, Rochester, New York, USA5Center for Structural and Functional Neuroscience, University of Montana, Missoula, Montana,USA
AbstractClinical and experimental data support a role for the intact cortex in recovery of function afterstroke, particularly ipsilesional areas interconnected to the infarct. There is, however, littleunderstanding of molecular events in the intact cortex, as most studies focus on the infarct andperi-infarct regions. This study investigated neuronal immunoreactivity for hypoxia-induciblefactor-1α (HIF-1α) and vascular endothelial growth factor (VEGF) receptor-2 (VEGFR-2) inremote cortical areas 3 days after a focal ischemic infarct, as both HIF-1α and VEGFR-2 havebeen implicated in peri-infarct neuroprotection. For this study, intracortical microstimulationtechniques defined primary motor (M1) and premotor areas in squirrel monkeys (genus Saimiri).An infarct was induced in the M1 hand representation, and immunohistochemical techniquesidentified neurons, HIF-1α and VEGFR-2. Stereologic techniques quantified the total neuronalpopulations and the neurons immunoreactive for HIF-1α or VEGFR-2. The results indicate thatHIF-1α upregulation is confined to the infarct and peri-infarct regions. Increases in VEGFR-2immunoreactivity occurred; however, in two remote regions: the ventral premotor handrepresentation and the M1 hindlimb representation. Neurons in these representations werepreviously shown to undergo significant increases in VEGF protein immunoreactivity, andcomparison of the two data sets showed a significant correlation between levels of VEGF andVEGFR-2 immunoreactivity. Thus, while remote areas undergo a molecular response to theinfarct, we hypothesize that there is a delay in the initiation of the response, which ultimately mayincrease the ‘window of opportunity’ for neuroprotective interventions in the intact cortex.
KeywordsVEGF (vascular endothelial growth factor); VEGF receptor-2 (VEGFR-2); HIF-1α (hypoxiainducible factor-1α); stroke; neuron; stereology
© 2008 ISCBFM All rights reservedCorrespondence: Dr AM Stowe, Department of Neurological Surgery, Box 8057, Washington University School of Medicine, 660 SEuclid Ave, St Louis, Missouri 63110, USA. [email protected].
NIH Public AccessAuthor ManuscriptJ Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
Published in final edited form as:J Cereb Blood Flow Metab. 2008 March ; 28(3): 612–620. doi:10.1038/sj.jcbfm.9600560.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

IntroductionAfter stroke, peri-infarct regions have reduced oxygen delivery as a result of a reduction inblood flow surrounding the infarct (Marti et al, 2000; Wei et al, 2001). This lack of oxygen(i.e., hypoxia) places peri-infarct neurons at risk of apoptotic or necrotic cell death. Thisstudy investigated the neuronal patterns of immunoreactivity for hypoxia-induciblefactor-1α (HIF-1α) protein and vascular endothelial growth factor (VEGF) receptor-2(VEGFR-2) to address how hypoxia affects neurons in a non-human primate model of focalcortical ischemia. The neuronal immunoreactivity of HIF-1α and VEGFR-2 is expected toincrease in areas of cortex that become hypoxic, due to injuries such as stroke, based onprevious findings (Bergeron et al, 1999; Chavez and LaManna, 2002). Unique to thisinvestigation was the evaluation of both HIF-1α and VEGFR-2 in presumably non-hypoxicneurons interconnected to and functionally associated with the infarct. Neurons projecting toan area of infarct may be at risk of cell death due to a loss of retrograde neurotrophintransport (Skaper and Walsh, 1998), whereas neurons receiving projections from an infarctare at risk of death because of lost excitatory input (Stein, 1998). The survival of theseinterconnected neurons may be critical, however, as clinical and experimental evidencesuggests that intact ipsilesional regions of the brain undergo molecular, anatomic, andphysiologic changes in response to the infarct and can aid functional recovery (Dancause etal, 2005; Frost et al, 2003; Liu and Rouiller, 1999; Seitz et al, 1998).
The HIF-1α subunit functions as the main regulator for oxygen homeostasis and is stabilizedunder hypoxic conditions in the peri-infarct region, but not in contralateral or controlcortices, after stroke (Bergeron et al, 1999; Marti et al, 2000). One transcriptional target ofpost-stroke HIF-1α is the gene encoding VEGF, which has been implicated in the post-stroke recovery processes of angiogenesis and neuroprotection (Sun et al, 2003; Wang,2003; Zhang et al, 2000). Neurons express one of four receptors for VEGF, VEGFR-2,throughout adulthood in both the cortex and hippocampus (Yang et al, 2003). After stroke,VEGFR-2 is the main receptor for the action of VEGF, though the receptor does not have apromoter region to allow for upregulation by HIF-1α. Instead, VEGF directly upregulatesVEGFR-2 mRNA through either increased mRNA stability or gene transcription (Shen et al,1998). Experimental data show that neurons can upregulate VEGFR-2 expression as soon as1 h post-infarct (Hayashi et al, 2003), and clinical data suggests that upregulation can bemaintained through 150 days post-stroke in the infarct and peri-infarct regions, but not in thecontralateral cortex (Issa et al, 1999).
We previously examined neuronal VEGF protein expression levels in infarct, peri-infarct,and remote cortical regions at 3 days after a focal ischemic infarct in motor cortex (Stowe etal, 2007). Neurons in both the ventral premotor (PMv) hand representation, a remote regionaxonally interconnected to the infarct, and the primary motor (M1) hindlimb representation,significantly increased immunoreactivity for VEGF protein. This study continues theinvestigation into remote molecular events in these functionally defined motor areas byexamining neuronal immunoreactivity for HIF-1α protein and VEGFR-2 in adjacent corticalsections within the same animals.
Materials and methodsSurgical and Mapping Procedures
All surgical procedures were conducted under aseptic conditions and in accordance withprotocols approved by the University of Kansas Animal Care and Use Committee (KUIACUC protocol no. 2004-1470). Seven adult squirrel monkeys (genus Saimiri) were usedin this study. Briefly, we utilized intracortical microstimulation (ICMS) mapping techniquesto define the motor representations of the primary motor cortex (M1) and ventral premotor
Stowe et al. Page 2
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

cortex (PMv; Figure 1). Then, four monkeys received an experimental ischemic infarct inthe M1 hand area (experimental group), whereas three monkeys underwent motor mappingprocedures in the absence of infarct (control group). At 3 days post-surgery, all monkeyswere killed and histologic procedures conducted.
Methods are identical to previous published methods (Stowe et al, 2007). Briefly, acraniotomy contralateral to the preferred hand exposed areas of primary and secondarymotor cortices, as well as primary somatosensory cortex. Intracortical microstimulationmapping techniques were used to identify the borders of the M1 hand, the PMv hand, andthe lateral extent of the M1 hindlimb representations. One-micron polystyrene beads(Polysciences Inc., Warrington, PA, USA) were injected around each of these movementrepresentations to identify during further processing and analysis. Microforceps connected toa bipolar electrocoagulator induced an infarct through permanent occlusion of corticalvessels supplying the M1 hand area in the experimental groups (animals 601, 563A, 602,and 653). This technique consistently produces infarcts throughout the gray but not theunderlying white matter (Nudo et al, 1996). Control animals (animals 155, 597, and 598) didnot undergo the infarct procedure.
Histologic ProceduresThree days after the surgical procedures, animals were deeply anesthetized and perfusedthrough the left ventricle (0.1 mol/L PBS, pH 7.25; 3% paraformaldehyde). The cerebralcortex was dissected from surrounding tissue, flattened between glass slides, and kept in 3%paraformaldehyde/0.1 mol/L PBS for 72 h (Dancause et al, 2006b). Each hemisphere wasdehydrated, paraffin-embedded, and sectioned tangential to the cortical surface at a 12-µmthickness on a rotary microtome. Sections were exposed to primary antibodies to stain for(a) neurons (mouse anti-NeuN; 1:100; Chemicon); (b) HIF-1α protein (mouse anti-HIF-1α;1:200; Chemicon); and (c) VEGFR-2 (mouse anti-VEGFR-2; 1:200; Chemicon). Proceduresfor blocking and secondary labeling followed the Rapid Antibody Procedure in the mouseVectastain ABC Elite kits (Vector labs, Burlingame, CA, USA).
StereologyIn each animal, five serial sections, each 10 sections apart, were randomly selected foranalysis and visualized on an Axioplan 2 Microscope (Zeiss, Jena, Germany). Borders of themotor areas were identified in every section using the polystyrene bead injection sites(Stowe et al, 2007) or by topographical references based on criteria established in priorstudies in this laboratory and others (Dancause et al, 2006b; Huang et al, 1988). Cellnumbers were estimated using the Optical Fractionator (West et al, 1991). One marker wasplaced on every neuron with an intact cell membrane, and another marker on each neuronthat also had positive staining for HIF-1α protein or VEGFR-2 expression. The coefficientof error (CE); (Gundersen et al, 1999) for total neuron counts was between 0.03 to 0.08 forall areas in either control or experimental animals for both HIF-1α and VEGFR-2estimations, excluding the M1 hand infarct in the experimental animals. This area had a CErange of 0.08 to 0.16, due to the low number of cells counted in the infarct region. Wedetermined the ratio of the mean CE2 to the coefficient of variance (CV)2 to establish thecontribution of stereological analysis to the observed group variance (Gundersen et al, 1999;Slomianka and West, 2005). The CE2/CV2 for all cortical regions was between 0.01 and0.25 for both the HIF-1α and the VEGFR-2 data sets, indicating that stereologicalprocedures contributed little to the observed group variances.
Statistical AnalysisAs each physiologic region varied in surface area both within and between animals, rawneuronal population estimates were converted to neurons per unit volume (total neuron
Stowe et al. Page 3
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

estimation/region of interest in cubic mm) to facilitate comparison. One-way analysis ofvariance compared the neurons/mm3 between groups (experimental and control; arcsin-transformed) for each physiologic region (JMP statistical software, Cary, NC, USA). Theratio of neurons that were immunoreactive for the antigen of the protein or receptor ofinterest to total neuronal population was calculated for each physiologic region in eachgroup. Values are reported as mean ± standard deviation (s.d.). The correlation betweenestimates of neuron numbers immunoreactive for VEGF and VEGFR-2 within eachphysiologic area was assessed using linear regression analysis on the ratios of arcsin-transformed neuronal densities of VEGF or VEGFR-2 to total neurons. Statistical outcomeswere considered significant for P < 0.05.
ResultsIdentification of Intracortical Microstimulation-Defined Representations and the Area ofInfarct
Intracortical microstimulation mapping procedures identified the M1 hand, PMv hand, andM1 hindlimb representations (Figure 1A). Examination of the tissue showed that the area ofinfarct was almost exclusively confined to the M1 hand representation in all experimentalcases. The infarct was readily distinguished from surrounding tissue based on blood-filledvessels, an artifact of the electrocoagulation method employed. Neuronal staining within theinfarct was markedly reduced, and most neurons that did stain positive for NeuN hadshrunken and irregularly shaped cell bodies. NeuN staining patterns were identical topreviously published results (Sondell et al, 2000; Stowe et al, 2007). Staining patterns forHIF-1α protein in neurons were similar to previous results in rodents (Jin et al, 2000).Hypoxia-inducible factor-1α protein was confined to a peri-cytoplasmic location in cells thatalso positively stained for NeuN (Figure 1F–I). Staining of VEGFR-2 resulted in intensestaining patterns in the cell body and occasional dendrites, predominantly in cells that alsopositively stain for NeuN (Figure 1B–E). Sections processed without primary antibodies didnot show discernable staining (data not shown). The M1 orofacial region was used to controlfor motor cortex plasticity and proximity to the infarct, as it was the closest remote area tothe peri-infarct region. Because of previous evidence of a lack of penumbra using the bipolarelectrocoagulation method (Frost et al, 2003), and analysis of the M1 orofacial region as acontrol, we are confident that changes in ‘remote’ ipsilesional areas were not a result of peri-infarct hypoxia or diffusion of growth factors from the peri-infarct region into thesurrounding cortex.
Significant Neuronal Loss Was Confined to the Primary Motor Hand Area InfarctDesign-based stereological analysis yielded two population estimates, one for total neurons(NeuN-positive cells) and another for neurons that associated with either HIF-1α (NeuN-positive cells that were immunoreactive for HIF-1α protein; Table 1) or VEGFR-2 (NeuN-positive cells that were immunoreactive for VEGFR-2; Table 1). Although only neuronswere investigated in this series of experiments, the results do not preclude significantchanges occurring in other cell types within the cortex. Estimates for neuronal populationswere similar to previous results (Stowe et al, 2007). Conversion of the estimates to neuronaldensities (neurons/mm3) in each region of interest facilitated comparison across corticalregions and between animals.
In the HIF-1α data set, the mean neuronal density within the M1 hand representation wassignificantly reduced in experimental versus control conditions (P < 0.01; Figure 2). Themean density of neurons in the M1 hand representation in control animals was 37,611 ±6,902 neurons/mm3. The mean density of M1 hand area neurons in experimental animalswas 8,736 ± 4,525 neurons/mm3. The experimental mean reflected a 76.8% reduction of
Stowe et al. Page 4
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

neurons in the M1 hand region at 3 days post-infarct in this set of serial sections. There wasno significant difference in neuronal densities between control and experimental groups inany of the remaining cortical regions: peri-infarct, PMv hand, M1 hindlimb, M1 orofacial,somatosensory, and temporal regions (P > 0.05).
Similarly, in the VEGFR-2 data set, the only significant decrease in mean neuronal densitiesbetween control and experimental conditions again occurred within the M1 handrepresentation (P < 0.01; Figure 2). The mean (± s.d.) density of neurons in the M1 handrepresentation in control animals was 49, 641 ± 21,723 neurons/mm3, whereas the meandensity in experimental animals was 6,221 ± 2,040 neurons/mm3. The experimental densityin this series of sections reflected an 87.4% reduction in neurons in the M1 handrepresentation at 3 days after an infarct. Again, there was no significant difference betweencontrol and experimental neuronal densities in any of the remaining cortical regions (P >0.05).
Neurons Under Control Conditions were Immunoreactive for Both Hypoxia-InducibleFactor-1α and Vascular Endothelial Growth Factor Receptor-2 in All Examined Areas of theCortex
The ratio of neurons immunoreactive for either HIF-1α or VEGFR-2 was derived frompopulation estimates described above and found in Table 1. In general, fewer than 5% ofneurons were immunoreactive for HIF-1α protein under control conditions, regardless ofcortical region. Approximately 19% of the total neurons in the primary and secondary motorcortices were immunoreactive for VEGFR-2 under control conditions. The somatosensory(13.0%) and the temporal (10.7%) regions each had fewer neurons immunoreactive forVEGFR-2 compared with motor cortex.
Neurons Have Significantly Greater Immunoreactivity for Hypoxia-inducible factor-1αProtein at 3 Days After an Infarct
After the M1 hand area infarct, the mean proportion of neurons immunoreactive for HIF-1αprotein was significantly greater in three cortical areas: the M1 hand, the peri-infarct, andthe M1 hindlimb regions (Table 1 and Figure 2). Although there was a significant reductionin total neurons in the M1 hand representation after infarct, neurons increasedimmunoreactivity for HIF-1α from 3.5 ± 0.8% in the control group to 87.1 ± 16.3% in theneurons remaining at 3 days post-infarct (P < 0.001). Peri-infarct neurons increasedimmunoreactivity for HIF-1α, from 3.0 ± 0.7% in the control group to 89.2 ± 4.5% in theexperimental group (P < 0.0001). One remote cortical area, the M1 hindlimb representation,also significantly increased neuronal immunoreactivity for HIF-1α from 2.4 ± 1.2% in thecontrol group to 5.0 ± 1.4% in the experimental group (P < 0.05). There were no significantdifferences between experimental and control groups in any of the remaining cortical areas(P > 0.05).
Neurons Significantly Increased Vascular Endothelial Growth Factor Receptor-2Immunoreactivity After an Infarct
After an M1 hand representation infarct, the mean proportion of neurons immunoreactive forVEGFR-2 significantly increased in four cortical areas: the M1 hand, the peri-infarct, thePMv hand, and the M1 hindlimb regions (Table 1 and Figure 2). The significant increase inVEGFR-2 immunoreactivity in the M1 hand representation was in a significantly reducedtotal neuron population. The percentage of neurons in the M1 hand area that wereimmunoreactive for VEGFR-2 increased from 18.5 ± 3.3% in the control group to 53.4 ±7.9% in the experimental group (P < 0.001). Peri-infarct neurons significantly increasedVEGFR-2 immunoreactivity from 18.7 ± 2.5% expressing VEGFR-2 in the control group to32.1 ± 6.5% in the experimental group (P < 0.05). VEGFR-2 immunoreactivity in neurons
Stowe et al. Page 5
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

also significantly increased in two remote areas. The PMv hand representation increasedfrom 21.3 ± 1.1% in control to 29.0 ± 4.8% in experimental condition (P < 0.05). Neurons inthe M1 hindlimb representation significantly increased VEGFR-2 immunoreactivity from18.7 ± 4.3 to 25.0 ± 1.6% (P < 0.05). There were no significant differences betweenexperimental and control groups in three cortical areas: the M1 orofacial, somatosensory,and temporal regions (P > 0.05), though there appeared to be a trend toward increasedimmunoreactivity of VEGFR-2 on neurons in these cortical areas as well.
Vascular Endothelial Growth Factor Receptor-2 Immunoreactivity Significantly Correlatedto Neuronal Vascular Endothelial Growth Factor Receptor Protein Levels
Under both experimental and control conditions, there was a significant correlation betweenthe ratio of neurons immunoreactive for VEGFR-2 (present results) to the ratio of neuronsimmunoreactive for VEGF protein (Stowe et al, 2007). Under control conditions and acrossall cortical areas, the correlation between VEGF and VEGFR-2 was significant, with an R2
of 0.80 (P < 0.0001; Figure 3). At 3 days after an M1 hand representation infarct, there stillremained a significant correlation between VEGF and VEGFR-2, with an R2 of 0.74 (P <0.0001; Figure 3). The overall variance in the slope of the linear fit between experimentaland control conditions are addressed in the Discussion.
DiscussionThe Role of hypoxia-inducible factor-1α in Neuroprotection After Stroke
In this study in non-human primates, neurons significantly increased immunoreactivity forHIF-1α in both the peri-infarct and infarct (i.e., M1 hand representation) regions, inagreement with previous rodent studies (Chavez and LaManna, 2002; Jin et al, 2000).Although the neuronal densities in the M1 hand infarct reflect a 77% loss of neurons, nearly9 out of every 10 (87%) viable neurons remaining stained for HIF-1α protein, versus only4% in the control M1 hand area. This ratio represented more than a 20-fold increase inHIF-1α immunoreactivity. Evidence supports a role for HIF-1α in the upregulation of genespromoting both neuroprotection (Jin et al, 2000; Semenza, 2004) as well as apoptosis(Carmeliet et al, 1998; Helton et al, 2005). Despite evidence that increased activation ofHIF-1α reduces infarct volume (Siddiq et al, 2005), Helton et al (2005) suggest that thepredominant role of HIF-1α during hypoxia/ischemia is proapoptotic, and that the loss ofHIF-1α function is neuroprotective. The present data conflicts with this idea, however, as themajority of peri-infarct neurons (89%) were immunoreactive for HIF-1α in the absence ofsignificant neuronal death at this time point. Perhaps the type and severity of hypoxic injurydetermines the exact role that HIF-1α takes in post-infarct neurons, and this role may not beexclusively determined during the initial stabilization of the HIF-1α subunit. NeuronalHIF-1α immunoreactivity in the M1 hindlimb region also increased at 3 days post-infarct.Although statistically significant, the magnitude of this increase (5%) was so modest,relative to the increases noted in the infarct and peri-infarct regions, that its physiologicsignificance is questionable.
Neuronal Vascular Endothelial Growth Factor Receptor-2 Expression Occurred inFunctionally Related Remote Areas
This study investigated neuronal immunoreactivity for VEGFR-2 in remote ipsilesionalphysiologic areas that may be involved in recovery of function. Previous studies in thesquirrel monkey showed that the PMv hand representation is heavily interconnected to theM1 hand representation (Dancause et al, 2006a) and, at 3 months after an M1 hand areainfarct, PMv hand neurons undergo neuroanatomic and neurophysiologic plasticity(Dancause et al, 2005; Frost et al, 2003). Despite verification of PMv plasticity in both non-
Stowe et al. Page 6
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

human primate and clinical data (Seitz et al, 1998), the understanding of molecular events,in response to an infarct, in this or other remote regions of the intact cortex, is minimal.
There was a significant increase in the proportion of neurons immunoreactive for VEGFR-2in the PMv hand representation by 3 days post-infarct. Because VEGFR-2 is not under thetranscriptional regulation of HIF-1α, but instead upregulated by VEGF itself (Kremer et al,1997; Shen et al, 1998), it is possible that the increased VEGFR-2 immunoreactivity in PMvwas a result of a VEGF-induced neuroprotective cascade initiated by interconnectedneurons. Neuronal levels of VEGFR-2 in the M1 hindlimb representation also underwent asignificant increase in neuronal immunoreactivity after infarct. It is doubtful, however, that asignificant number of M1 hindlimb neurons were at risk of neuronal death due to theischemic injury, as neurons in this region are not heavily interconnected to the area of infarct(Hatanaka et al, 2001). Instead, increases in collateral blood flow from the anterior cerebralartery may have upregulated VEGF, and thus VEGFR-2 production, in this area (Milkiewiczet al, 2001).
Vascular Endothelial Growth Factor Receptor-2 Expression Highly Correlated to NeuronalVascular Endothelial Growth Factor Levels Throughout the Cortex
The level of neuronal VEGF protein immunoreactivity (Stowe et al, 2007) correlated toVEGFR-2 expression levels in neurons in both motor and non-motor cortices under eithercontrol and experimental conditions. During control conditions, there was a 1:2 ratio ofVEGF/VEGFR-2 in neurons. At 3 days after an M1 hand area infarct, however, the linear fitevolved into a ratio of 2:3 for VEGF/VEGFR-2. The results suggest that increased VEGFprotein levels can drive increased VEGFR-2 expression on neurons, albeit in a time-delayedmanner. The data seem to reflect a time point where the VEGF protein is still promotingupregulation of VEGFR-2. Despite the uniformity of VEGF/VEGFR-2 ratios when allregions are pooled, there are differences in the magnitude of increases when consideringspecific regions. In the infarct and peri-infarct regions, the overall magnitude of percentagechange increased over control values by 35 and 13%, respectively, for VEGFR-2immunoreactivity and 26 and 9%, respectively, for VEGF immunoreactivity. In both ofthese areas, there was a greater magnitude increase of neuronal VEGFR-2 expression overVEGF protein immunoreactivity.
Within the PMv hand representation, however, both VEGFR-2 and VEGF proteinimmunoreactivity increased 8% over control values, and in the M1 hindlimb, neuronalimmunoreactivity for VEGFR-2 actually increased 2% less than the magnitude increase ofVEGF immunoreactivity in neurons. The equality of magnitude in the PMv region suggestsa delayed response to the infarct, a reasonable hypothesis if the stimulus driving themolecular response in this region is not due to the direct insult of hypoxia/ischemia, butinstead due to neurons interconnected to the infarct. These comparisons reveal a lack ofuniformity in the magnitude of upregulation in the ipsilesional cortex. In conclusion, ouranalyses of molecular plasticity in neurons from interconnected ipsilesional regions, remotefrom the ischemic injury but still at risk for cell death, suggest that a uniquely prolonged‘window of opportunity’ may exist during the subacute stage of recovery for directedcytoprotective therapies in the intact cortex.
AcknowledgmentsWe thank Erica Blumberg and Robert Cross for assistance in data acquisition and analysis. We also thank Dr LutzSlomianka, University of Zurich, Switzerland, for continued guidance with the stereological protocols and analysis.
This work was supported by American Heart Association Predoctoral Fellowship (Stowe, PI) and NIH/NINDS R01NS 30853-10 (Nudo, PI)
Stowe et al. Page 7
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

ReferencesBergeron M, Yu AY, Solway KE, Semenza GL, Sharp FR. Induction of hypoxia-inducible factor-1
(HIF-1) and its target genes following focal ischaemia in rat brain. Eur J Neurosci. 1999; 11:4159–4170. [PubMed: 10594641]
Carmeliet P, Dor Y, Herbert JM, Fukumura D, Brusselmans K, Dewerchin M, Neeman M, Bono F,Abramovitch R, Maxwell P, Koch CJ, Ratcliffe P, Moons L, Jain RK, Collen D, Keshert E. Role ofHIF-1alpha in hypoxia-mediated apoptosis, cell proliferation and tumour angiogenesis. Nature.1998; 394:485–490. [PubMed: 9697772]
Chavez JC, LaManna JC. Activation of hypoxia-inducible factor-1 in the rat cerebral cortex aftertransient global ischemia: potential role of insulin-like growth factor-1. J Neurosci. 2002; 22:8922–8931. [PubMed: 12388599]
Dancause N, Barbay S, Frost SB, Plautz EJ, Chen D, Zoubina EV, Stowe AM, Nudo RJ. Extensivecortical rewiring after brain injury. J Neurosci. 2005; 25:10167–10179. [PubMed: 16267224]
Dancause N, Barbay S, Frost SB, Plautz EJ, Popescu M, Dixon PM, Stowe AM, Friel KM, Nudo RJ.Topographically divergent and convergent connectivity between premotor and primary motorcortex. Cereb Cortex. 2006a; 16:1057–1068. [PubMed: 16221929]
Dancause N, Barbay S, Frost SB, Plautz EJ, Stowe AM, Friel KM, Nudo RJ. Ipsilateral connections ofthe ventral premotor cortex in a new world primate. J Comp Neurol. 2006b; 495:374–390.[PubMed: 16485282]
Frost SB, Barbay S, Friel KM, Plautz EJ, Nudo RJ. Reorganization of remote cortical regions afterischemic brain injury: a potential substrate for stroke recovery. J Neurophysiol. 2003; 89:3205–3214. [PubMed: 12783955]
Gundersen HJ, Jensen EB, Kieu K, Nielsen J. The efficiency of systematic sampling in stereology—reconsidered. J Microsc. 1999; 193:199–211. [PubMed: 10348656]
Hatanaka N, Nambu A, Yamashita A, Takada M, Tokuno H. Somatotopic arrangement andcorticocortical inputs of the hindlimb region of the primary motor cortex in the macaque monkey.Neurosci Res. 2001; 40:9–22. [PubMed: 11311401]
Hayashi T, Noshita N, Sugawara T, Chan PH. Temporal profile of angiogenesis and expression ofrelated genes in the brain after ischemia. J Cereb Blood Flow Metab. 2003; 23:166–180. [PubMed:12571448]
Helton R, Cui J, Scheel JR, Ellison JA, Ames C, Gibson C, Blouw B, Ouyang L, Dragatsis I, Zeitlin S,Johnson RS, Lipton SA, Barlow C. Brain-specific knock-out of hypoxia-inducible factor-1alphareduces rather than increases hypoxic-ischemic damage. J Neurosci. 2005; 25:4099–4107.[PubMed: 15843612]
Huang CS, Sirisko MA, Hiraba H, Murray GM, Sessle BJ. Organization of the primate face motorcortex as revealed by intracortical microstimulation and electrophysiological identification ofafferent inputs and corticobulbar projections. J Neurophysiol. 1988; 59:796–818. [PubMed:2835448]
Issa R, Krupinski J, Bujny T, Kumar S, Kaluza J, Kumar P. Vascular endothelial growth factor and itsreceptor, KDR, in human brain tissue after ischemic stroke. Lab Invest. 1999; 79:417–425.[PubMed: 10211994]
Jin KL, Mao XO, Nagayama T, Goldsmith PC, Greenberg DA. Induction of vascular endothelialgrowth factor and hypoxia-inducible factor-1alpha by global ischemia in rat brain. Neuroscience.2000; 99:577–585. [PubMed: 11029549]
Kremer C, Breier G, Risau W, Plate KH. Up-regulation of flk-1/vascular endothelial growth factorreceptor 2 by its ligand in a cerebral slice culture system. Cancer Res. 1997; 57:3852–3859.[PubMed: 9288799]
Liu Y, Rouiller EM. Mechanisms of recovery of dexterity following unilateral lesion of thesensorimotor cortex in adult monkeys. Exp Brain Res. 1999; 128:149–159. [PubMed: 10473753]
Marti HJ, Bernaudin M, Bellail A, Schoch H, Euler M, Petit E, Risau W. Hypoxia-induced vascularendothelial growth factor expression precedes neovascularization after cerebral ischemia. Am JPathol. 2000; 156:965–976. [PubMed: 10702412]
Stowe et al. Page 8
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Milkiewicz M, Brown MD, Egginton S, Hudlicka O. Association between shear stress, angiogenesis,and VEGF in skeletal muscles in vivo. Microcirculation. 2001; 8:229–241. [PubMed: 11528531]
Nudo RJ, Wise BM, SiFuentes F, Milliken GW. Neural substrates for the effects of rehabilitativetraining on motor recovery after ischemic infarct. Science. 1996; 272:1791–1794. [PubMed:8650578]
Seitz RJ, Hoflich P, Binkofski F, Tellmann L, Herzog H, Freund HJ. Role of the premotor cortex inrecovery from middle cerebral artery infarction. Arch Neurol. 1998; 55:1081–1088. [PubMed:9708958]
Semenza GL. Hydroxylation of HIF-1:oxygen sensing at the molecular level. Physiology. 2004;19:176–182. [PubMed: 15304631]
Shen BQ, Lee DY, Gerber HP, Keyt BA, Ferrara N, Zioncheck TF. Homologous up-regulation ofKDR/Flk-1 receptor expression by vascular endothelial growth factor in vitro. J Biol Chem. 1998;273:29979–29985. [PubMed: 9792718]
Siddiq A, Ayoub IA, Chavez JC, Aminova L, Shah S, LaManna JC, Patton SM, Connor JR, ChernyRA, Volitakis I, Bush AI, Langsetmo I, Seeley T, Gunzler V, Ratan RR. Hypoxia-inducible factorprolyl 4-hydroxylase inhibition. A target for neuroprotection in the central nervous system. J BiolChem. 2005; 280:41732–41743. [PubMed: 16227210]
Skaper SD, Walsh FS. Neurotrophic molecules: strategies for designing effective therapeuticmolecules in neurodegeneration. Mol Cell Neurosci. 1998; 12:179–193. [PubMed: 9828084]
Slomianka L, West MJ. Estimators of the precision of stereological estimates: an example based on theCA1 pyramidal cell layer of rats. Neuroscience. 2005; 136:757–767. [PubMed: 16344149]
Sondell M, Sundler F, Kanje M. Vascular endothelial growth factor is a neurotrophic factor whichstimulates axonal outgrowth through the flk-1 receptor. Eur J Neurosci. 2000; 12:4243–4254.[PubMed: 11122336]
Stein, DG. Brain injury and theories of recovery. In: Goldstein, LB., editor. Restorative neurology:advances in pharmacotherapy for recovery after stroke. Armonk, NY: Futura Publishing Co., Inc.;1998. p. 1-34.
Stowe AM, Plautz EJ, Eisner-Janowicz I, Frost SB, Barbay S, Zoubina EV, Dancause N, Taylor MD,Nudo RJ. VEGF protein associates to neurons in remote regions following cortical infarct. J CerebBlood Flow Metab. 2007; 27:76–85. [PubMed: 16639424]
Sun Y, Jin K, Xie L, Childs J, Mao XO, Logvinova A, Greenberg DA. VEGF-inducedneuroprotection, neurogenesis, and angiogenesis after focal cerebral ischemia. J Clin Invest. 2003;111:1843–1851. [PubMed: 12813020]
Wang JH. Short-term cerebral ischemia causes the dysfunction of interneurons and more excitation ofpyramidal neurons in rats. Brain Res Bull. 2003; 60:53–58. [PubMed: 12725892]
Wei L, Erinjeri JP, Rovainen CM, Woolsey TA. Collateral growth and angiogenesis around corticalstroke. Stroke. 2001; 32:2179–2184. [PubMed: 11546914]
West MJ, Slomianka L, Gundersen HJ. Unbiased stereological estimation of the total number ofneurons in the subdivisions of the rat hippocampus using the optical fractionator. Anat Rec. 1991;231:482–497. [PubMed: 1793176]
Yang SZ, Zhang LM, Huang YL, Sun FY. Distribution of Flk-1 and Flt-1 receptors in neonatal andadult rat brains. Anat Rec A Discov Mol Cell Evol Biol. 2003; 274:851–856. [PubMed: 12923895]
Zhang ZG, Zhang L, Jiang Q, Zhang R, Davies K, Powers C, Bruggen N, Chopp M. VEGF enhancesangiogenesis and promotes blood-brain barrier leakage in the ischemic brain. J Clin Invest. 2000;106:829–838. [PubMed: 11018070]
Stowe et al. Page 9
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.(A) Flattened cortex was tangentially sectioned at 12-µm thickness. Note the presence ofcingulate (C), parietal (P), frontal (F), and temporal (T) cortices. Central sulcus (CS) isoutlined in white. The surface vascular photograph and the ICMS data for this animal issuperimposed and aligned. White dots mark the bead injection sites around each ICMS-defined representation. All representations are outlined according to the color legend at theright. The M1 hand area (infarct) lies in the middle of the peri-infarct region. Intracorticalconnections between the M1 hand representation and both PMv hand and somatosensoryregions are identified by arrows. (B–I) Representative photomicrographs of tangentialhistologic sections through the cerebral cortex in experimental and control animals.Immunohistochemical staining identifies (B–E) VEGFR-2 (DAB; brown), (F–I) HIF-1αprotein (DAB; brown), and NeuN (Vector SG, gray; Vector VIP, purple). Representativeneurons immunoreactive for VEGFR-2 or HIF-1α are designated by black arrows,representative pathologic neurons are designated by asterisks. (B and C) M1 hand areainfarct for VEGFR-2 data set. (D) Magnification of VEGFR-2 peri-infarct region. Nucleiappear more robust and similar to M1 hand regions controls. (E) Note the non-neuronalVEGFR-2 staining (gray arrow). (F and H) Peri-infarct region from HIF-1α data set. (G)Magnification of the M1 hand infarct region. (I) Control M1 hand region for HIF-1α. Notethe non-neuronal HIF-1α staining (gray arrow). Bars: (B, F) 100 µm and (C–E, G–I) 25 µm.
Stowe et al. Page 10
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.(A and C) Population estimates are shown as total neurons/mm3 and represent the mean(mean ± s.d.) of population numbers from all animals in either experimental or controlgroups as calculated by Stereo Investigator. Significant variation between experimental andcontrol populations was identified only in M1 hand area for both data sets, as identified byasterisk (one-way analysis of variance, P < 0.05). (B and D) Percentage ratios are based oncell populations derived from stereological analysis of neurons. The ratio represents theamount of neurons that associate with either HIF-1α protein or VEGFR-2 to total neuronestimations. Exact ratios are given in Table 1. Note that, although there is a significantincrease within the M1 hand representation infarct, the total neuronal populations for thisarea were significantly reduced versus all other areas depicted (one-way analysis ofvariance, P < 0.05).
Stowe et al. Page 11
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 3.Linear regression analysis based on arcsin-transformed population densities for neuronsimmunoreactive for VEGF and VEGFR-2 in all physiologic areas of the cortex for eitherexperimental or control conditions for each animal. The R2 for both the experimental group(0.74) and the control group (0.80) were significant (one-way analysis of variance; P <0.0001).
Stowe et al. Page 12
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Stowe et al. Page 13
Tabl
e 1
Popu
latio
n de
nsiti
es a
nd p
erce
nt ra
tios f
or n
euro
ns im
mun
orea
ctiv
e fo
r eith
er H
IF-1α
or V
EGFR
-2 fr
om to
tal n
euro
nal p
opul
atio
ns
Ml h
and
(infa
rct)
Peri
-infa
rct
PMv
hand
Ml h
indl
imb
Ml o
rofa
cial
som
atos
enso
ryte
mpo
ral
Con
trol
(n =
3)
H
IF-N
euro
ns/m
m3
1,27
41,
212
1,56
41,
078
1682
1558
1119
N
euro
ns/m
m3
37,6
1140
,426
38,6
3842
,385
44,1
1559
,319
59,2
65
P
erce
nt ra
tio3.
53
4.1
2.4
5.5
2.7
1.9
D
ista
nce
(mm
)2.
585.
066.
914.
285.
8516
.55
Infa
rct (
n =
4)
H
IF-N
euro
ns/m
m3
7,94
126
,394
1,47
82,
194
929
1146
464
N
euro
ns/m
m3
8736
29,9
8432
,649
43,8
4037
,652
59,8
5661
,132
P
erce
nt ra
tio87
.189
.25.
95
2.5
2.6
0.9
D
ista
nce
(mm
)2.
616.
596.
675
5.49
16.4
1
F
val
ue65
.37
467.
860.
137.
010.
340.
034.
24
S
igni
fican
ceP
< 0.
001
P <
0.00
01P
> 0.
05P
< 0.
05P
> 0.
05P
> 0.
05P
> 0.
05
Con
trol
(n =
3)
V
EGFR
-2-N
euro
ns/m
m3
9376
9805
10,2
9110
,221
12,6
7410
,477
6509
N
euro
ns/m
m3
49,6
4152
,237
48,7
1856
,303
66,9
5880
,166
58,9
66
P
erce
nt ra
tio18
.518
.721
.318
.719
.313
10.7
D
ista
nce
(mm
)2.
585.
066.
914.
285.
8516
.55
Infa
rct (
n =
4)
V
EGFR
-2-N
euro
ns/m
m3
3,21
522
,867
19,7
7718
,344
25,0
0520
,651
10,8
58
N
euro
ns/m
m3
6,22
173
,423
70,5
2572
,592
103,
549
107,
639
80,5
23
P
erce
nt ra
tio53
.432
.129
2524
.419
.514
.3
D
ista
nce
(mm
)2.
616.
596.
675
5.49
16.4
1
F
val
ue53
.97
12.4
77.
687.
194.
613.
661.
96
S
igni
fican
ceP
< 0.
001
P <
0.05
P <
0.05
P <
0.05
P >
0.05
P >
0.05
P >
0.05
AN
OV
A, a
naly
sis o
f var
ianc
e; H
IF, h
ypox
ia-in
duci
ble
fact
or; M
1, p
rimar
y m
otor
; PM
v, v
entra
l pre
mot
or; V
EGF,
vas
cula
r end
othe
lial g
row
th fa
ctor
; VEG
FR-2
, VEG
F re
cept
or-2
.
Popu
latio
n es
timat
es a
re sh
own
as to
tal n
euro
ns/m
m3
and
repr
esen
t the
mea
n (m
ean
± s.d
.) of
pop
ulat
ion
num
bers
from
all
anim
als i
n ei
ther
exp
erim
enta
l or c
ontro
l gro
ups a
s cal
cula
ted
by S
tere
oIn
vest
igat
or. P
erce
nt ra
tios r
epre
sent
the
amou
nt o
f neu
rons
that
are
imm
unor
eact
ive
for H
IF-1α
prot
ein
or V
EGFR
-2 w
ithin
the
tota
l neu
rona
l pop
ulat
ion.
Sig
nific
ant d
iffer
ence
s bet
wee
n ex
perim
enta
l and
cont
rol r
atio
s for
a g
iven
phy
siol
ogic
are
a ar
e lis
ted
and
bold
ed (o
ne-w
ay A
NO
VA
, P <
0.0
5). D
ista
nce
(mm
) was
mea
sure
d fr
om th
e ce
nter
of t
he M
1 ha
nd re
pres
enta
tion
to th
e ce
nter
of e
ach
of th
ere
mai
ning
phy
siol
ogic
are
as. P
eri-i
nfar
ct d
ista
nce
repr
esen
ts a
n ad
ditio
nal m
ean
of fo
ur d
ista
nces
(0°,
90°,
180°
, 270
°) a
s it s
urro
unds
the
M1
hand
repr
esen
tatio
n.
J Cereb Blood Flow Metab. Author manuscript; available in PMC 2011 December 6.
Copyright © 2022 FDOKUMEN









![Synthesis, in silico, in vitro, and in vivo investigation of 5-[11C]methoxy-substituted sunitinib, a tyrosine kinase inhibitor of VEGFR-2](https://static.fdokumen.com/doc/165x107/6333b54176a7ca221d0858ae/synthesis-in-silico-invitro-and-invivo-investigation-of-5-11cmethoxy-substituted.jpg)










