Mutations at coding mononucleotide repeats in gastric cancer with the microsatellite mutator...
6
Mutations at coding mononucleotide repeats in gastric cancer with the microsatellite mutator phenotype Laura Ottini 1 , Mario Falchetti 1 , Cristina D’Amico 1 , Andrea Amorosi 3 , Calogero Saieva 2 , Giovanna Masala 4 , Luigi Frati 1,5 , Alessandro Cama 6 , Domenico Palli 2 and Renato Mariani-Costantini 6 1 Department of Experimental Medicine and Pathology, University ‘La Sapienza’, Rome; 2 Epidemiology Unit, CSPO, Careggi Hospital, Florence; 3 Department of Pathology, University of Florence; 4 Epidemiology Satellite Unit, IST-CSPO, Florence; 5 IMNS, Pozzilli, Isernia; 6 Department of Oncology and Neurosciences, University ‘Gabriele D’Annunzio’, 66013 Chieti, Italy We analysed 50 gastric carcinomas (GCs) to verify whether mutations at coding repeats were associated with microsatellite instability (MSI). The tumors included: ten cases with no MSI, 14 cases with MSI=1 locus, 13 cases with MSI=two loci and 13 cases with MSI53 loci. We investigated coding repeats within the TGF-b RII, IGFIIR, BAX, hMSH6, hMSH3 and BRCA2 genes. The TGF-b RII, IGFIIR, BAX, hMSH6 and hMSH3 repeats were altered in 11 (22%), five (10%), four (8%), 16 (32%) and five (10%) cases respectively. Mutations occurred only in MSI-positive (MSI+) tumors and correlated with increasing MSI levels. No alterations of the BRCA2 repeat were found. Mutations in genes other than hMSH6 were strongly associated to hMSH6 mutations, suggesting a key role of this gene. The non-coding BAT-26 and E-Cadherin 3’ UTR poly(A)8/(T)15 repeats were analysed in 44 of the 50 cases. Novel tumor-associated alleles were observed only in MSI-positive GCs and were in most cases associated with mutations at coding repeats. Further investigations with BAT-40 confirmed that four cases manifested mononucleotide repeat alterations restricted to hMSH6 and one case to TGF-b RII. A subset of tumors with MSI at two or more dinucleotide loci resulted negative for mutations at coding and non-coding mononucleotide repeats. Keywords: gastric cancer; microsatellite instability; TGFb-RII; IGFIIR; BAX; hMSH3; hMSH6; BRCA2; mutation Introduction The mechanism(s) by which microsatellite instability (MSI) contributes to cancer are not fully elucidated, but it has been assumed that mismatch repair (MMR) deficiencies underlying MSI result in mutations of cancer-related genes, and that such mutations are responsible for carcinogenesis and/or tumor progres- sion (Arnheim and Shibata, 1997 and citations therein). Genes with proven or potential tumor-suppressor function(s) containing mononucleotide runs in their coding sequence are candidates for mutational inactivation in MSI-positive (MSI+) tumors. The first gene targeted by MMR deficiencies to be identified in MSI+ gastrointestinal and, more rarely, endometrial cancers, was the transforming growth factor-b type II receptor (TGF-b RII) gene (Marko- witz et al., 1995; Myero et al., 1995; Chung et al., 1996, 1997). MSI-associated TGF-b RII frameshift mutations tend to occur at a poly(A)10 in the 5’ half of the cDNA (codons 125 – 128). Mutations in coding monotonic runs within the IGFIIR and BAX genes were also detected in MSI+ cancers. The IGFIIR is a multifunctional protein, involved in the intracellular tracking of lysosomal enzymes, in the activation of TGFb1, and in the degradation of the insulin-like growth factor II (IGFII) (Dahms et al., 1989; Dennis et al., 1991; Kornfeld et al., 1992). Mutations in a coding IGFIIR poly(G)8 tract (nucleotides 4089 – 4096) were identified in MSI+ gastrointestinal and endometrial cancers (Souza et al., 1996; Chung et al., 1997; Ouyang et al., 1997). BAX, a member of the BCL2 gene family transactivated by p53 in response to DNA damage (Miyashita and Reed, 1995), encodes a protein that competes with the BCL2 protein in the regulation of cellular responses to death signals. BAX deficiencies may result in a diminished ability to trigger apoptosis (Oltvai et al., 1993). Mutations targeting a BAX poly(G)8 at codons 38 – 41 were found to be frequent in MSI+ gastrointestinal cancers (Rampino et al., 1997; Chung et al., 1997). In MSI+ gastrointestinal tumors, additional coding mutational targets were identified in a poly(C)8 within the hMSH6 gene at codons 1116 – 1118 and in a poly(A)8 within the hMSH3 gene at codons 381 – 383 (Malkhosyan et al., 1996; Chung et al., 1997). The products of these two MMR genes interact with the hMSH2 protein to form heterodimers with partially redundant functions (Prolla et al., 1996) and it has been suggested that hMSH6 and/or hMSH3 inactivation in cells already deficient in MMR may accelerate the accumulation of mutations at mononucleotide runs (Perucho, 1996). The objective of this study, which analyses GCs of known MSI status identified in an epidemiological case-control study (Buiatti et al., 1991; Ottini et al., 1997), was to verify associations between MSI at dinucleotide repeats and mutations at coding mono- nucleotide runs within the TGF-b RII, IGFIIR, BAX, hMSH6 and hMSH3 genes. In addition, we analysed a coding repeat within BRCA2, a tumor-suppressor gene not specifically involved in gastric carcinogenesis (Stratton and Wooster, 1996; Casey, 1997) for which inactivation at mononucleotide runs has been docu- mented (Takahashi et al., 1996). In most tumors we Correspondence: R Mariani-Costantini Received 14 August 1997; revised 2 January 1998; accepted 2 January 1998 Oncogene (1998) 16, 2767 – 2772 1998 Stockton Press All rights reserved 0950 – 9232/98 $12.00 http://www.stockton-press.co.uk/onc
Transcript of Mutations at coding mononucleotide repeats in gastric cancer with the microsatellite mutator...

Mutations at coding mononucleotide repeats in gastric cancer with themicrosatellite mutator phenotype
Laura Ottini1, Mario Falchetti1, Cristina D'Amico1, Andrea Amorosi3, Calogero Saieva2,Giovanna Masala4, Luigi Frati1,5, Alessandro Cama6, Domenico Palli2 andRenato Mariani-Costantini6
1Department of Experimental Medicine and Pathology, University `La Sapienza', Rome; 2Epidemiology Unit, CSPO, CareggiHospital, Florence; 3Department of Pathology, University of Florence; 4Epidemiology Satellite Unit, IST-CSPO, Florence; 5IMNS,Pozzilli, Isernia; 6Department of Oncology and Neurosciences, University `Gabriele D'Annunzio', 66013 Chieti, Italy
We analysed 50 gastric carcinomas (GCs) to verifywhether mutations at coding repeats were associated withmicrosatellite instability (MSI). The tumors included: tencases with no MSI, 14 cases with MSI=1 locus, 13cases with MSI=two loci and 13 cases with MSI53loci. We investigated coding repeats within the TGF-bRII, IGFIIR, BAX, hMSH6, hMSH3 and BRCA2genes. The TGF-b RII, IGFIIR, BAX, hMSH6 andhMSH3 repeats were altered in 11 (22%), ®ve (10%),four (8%), 16 (32%) and ®ve (10%) cases respectively.Mutations occurred only in MSI-positive (MSI+)tumors and correlated with increasing MSI levels. Noalterations of the BRCA2 repeat were found. Mutationsin genes other than hMSH6 were strongly associated tohMSH6 mutations, suggesting a key role of this gene.The non-coding BAT-26 and E-Cadherin 3' UTRpoly(A)8/(T)15 repeats were analysed in 44 of the 50cases. Novel tumor-associated alleles were observed onlyin MSI-positive GCs and were in most cases associatedwith mutations at coding repeats. Further investigationswith BAT-40 con®rmed that four cases manifestedmononucleotide repeat alterations restricted to hMSH6and one case to TGF-b RII. A subset of tumors withMSI at two or more dinucleotide loci resulted negativefor mutations at coding and non-coding mononucleotiderepeats.
Keywords: gastric cancer; microsatellite instability;TGFb-RII; IGFIIR; BAX; hMSH3; hMSH6; BRCA2;mutation
Introduction
The mechanism(s) by which microsatellite instability(MSI) contributes to cancer are not fully elucidated,but it has been assumed that mismatch repair (MMR)de®ciencies underlying MSI result in mutations ofcancer-related genes, and that such mutations areresponsible for carcinogenesis and/or tumor progres-sion (Arnheim and Shibata, 1997 and citations therein).Genes with proven or potential tumor-suppressorfunction(s) containing mononucleotide runs in theircoding sequence are candidates for mutationalinactivation in MSI-positive (MSI+) tumors.
The ®rst gene targeted by MMR de®ciencies to beidenti®ed in MSI+ gastrointestinal and, more rarely,endometrial cancers, was the transforming growthfactor-b type II receptor (TGF-b RII) gene (Marko-witz et al., 1995; Myero� et al., 1995; Chung et al.,1996, 1997). MSI-associated TGF-b RII frameshiftmutations tend to occur at a poly(A)10 in the 5' halfof the cDNA (codons 125 ± 128). Mutations in codingmonotonic runs within the IGFIIR and BAX geneswere also detected in MSI+ cancers. The IGFIIR is amultifunctional protein, involved in the intracellulartra�cking of lysosomal enzymes, in the activation ofTGFb1, and in the degradation of the insulin-likegrowth factor II (IGFII) (Dahms et al., 1989; Dennis etal., 1991; Kornfeld et al., 1992). Mutations in a codingIGFIIR poly(G)8 tract (nucleotides 4089 ± 4096) wereidenti®ed in MSI+ gastrointestinal and endometrialcancers (Souza et al., 1996; Chung et al., 1997; Ouyanget al., 1997). BAX, a member of the BCL2 gene familytransactivated by p53 in response to DNA damage(Miyashita and Reed, 1995), encodes a protein thatcompetes with the BCL2 protein in the regulation ofcellular responses to death signals. BAX de®cienciesmay result in a diminished ability to trigger apoptosis(Oltvai et al., 1993). Mutations targeting a BAXpoly(G)8 at codons 38 ± 41 were found to be frequentin MSI+ gastrointestinal cancers (Rampino et al.,1997; Chung et al., 1997). In MSI+ gastrointestinaltumors, additional coding mutational targets wereidenti®ed in a poly(C)8 within the hMSH6 gene atcodons 1116 ± 1118 and in a poly(A)8 within thehMSH3 gene at codons 381 ± 383 (Malkhosyan et al.,1996; Chung et al., 1997). The products of these twoMMR genes interact with the hMSH2 protein to formheterodimers with partially redundant functions (Prollaet al., 1996) and it has been suggested that hMSH6and/or hMSH3 inactivation in cells already de®cient inMMR may accelerate the accumulation of mutationsat mononucleotide runs (Perucho, 1996).The objective of this study, which analyses GCs of
known MSI status identi®ed in an epidemiologicalcase-control study (Buiatti et al., 1991; Ottini et al.,1997), was to verify associations between MSI atdinucleotide repeats and mutations at coding mono-nucleotide runs within the TGF-b RII, IGFIIR, BAX,hMSH6 and hMSH3 genes. In addition, we analysed acoding repeat within BRCA2, a tumor-suppressor genenot speci®cally involved in gastric carcinogenesis(Stratton and Wooster, 1996; Casey, 1997) for whichinactivation at mononucleotide runs has been docu-mented (Takahashi et al., 1996). In most tumors we
Correspondence: R Mariani-CostantiniReceived 14 August 1997; revised 2 January 1998; accepted 2 January1998
Oncogene (1998) 16, 2767 ± 2772 1998 Stockton Press All rights reserved 0950 ± 9232/98 $12.00
http://www.stockton-press.co.uk/onc

examined the status of BAT-26, a sensitive indicator ofinstability at sequence repeats (Myero� et al., 1995;Parsons et al., 1995; Hoang et al., 1997), and of apoly(A)8/(T)15 repeat wihin the 3' UTR of the E-Cadherin gene. Cases negative for instability at BAT-26and at the E-Cadherin 3' UTR repeat, but positive formutations at two or more dinucleotide microsatellitesand/or at coding mononucleotide repeats, were furtheranalysed using BAT-40.
Results
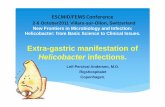
To investigate associations between MSI and muta-tions at coding repeats, we selected 50 primary GCswhose status had been previously assessed at sixdinucleotide loci (Ottini et al., 1997). The seriesanalysed included ten cases with no evidence of MSI,14 cases with MSI at one locus, and 26 cases with MSIat two or more loci. Coding mononucleotide repeatswithin the TGF-b RII (codons 125 ± 128), IGFIIR(nucleotides 4089 ± 4096), BAX (codons 38 ± 41),hMSH6 (codons 1116 ± 1118), hMSH3 (codons 381 ±383) and BRCA2 (nucleotides 1443 ± 1450) genes wereampli®ed by PCR from paired normal and tumorDNAs obtained by microdissection of a single para�n-embedded section and the sizes of PCR products werecompared. Mutations, exempli®ed in Figure 1 (arrows)and reported in Table 1, were identi®ed by the presenceof abnormal bands in tumor DNAs that were notpresent in normal DNAs (Myero� et al., 1995; Souzaet al., 1996; Malkhosyan et al., 1996; Chung et al.,1997). Paired genotypings of cases positive foralterations were always con®rmed in triplicate experi-ments.No mutations in the poly(A)8 repeat within the
BRCA2 gene were observed in the 50 GCs analysed.Mutations in the poly(A)10 repeat of the TGF-b RIIgene were found in 11/50 cases (22%) and were
associated with the presence of MSI at increasingnumber of dinucleotide loci: in fact, mutations weredetected in 2/14 (14%) cases with MSI at one locus, 3/13 (23%) cases with MSI at two loci and 6/13 (46%)cases with MSI at three or more loci. Overall, TGF-bRII mutations were observed in 9/26 (35%) of the GCswith MSI at two or more loci, while no mutations wereidenti®ed in the ten cases with no evidence of MSI.Mutations of the IGFIIR poly(G)8 were found in 5/
50 cases (10%), including 2/13 (15%) cases with MSIat two loci and 3/13 (23%) cases with MSI at three ormore loci. The analysis of the BAX poly(G)8 revealedmutations in 4/50 cases (8%), including 1/13 (8%)cases with MSI at two loci and 3/13 (23%) cases withMSI at three or more loci. Mutations of the poly(G)8tracts within the IGFIIR and BAX genes were observedonly in GCs with MSI at two or more dinucleotideloci: in fact, 19% (5/26) and 15% (4/26) of the GCswith multiple MSI respectively showed IGFIIR andBAX mutations.We further investigated the mononucleotide runs
within the hMSH6 and hMSH3 genes. The hMSH6poly(C)8 appeared to be much more frequentlymutated than the hMSH3 poly(A)8, resulting themost frequently altered among the coding mutationaltargets. In fact, hMSH6 was mutated in 16/50 cases(32%), including 4/14 (29%) cases with MSI at onelocus, 4/13 (31%) cases with MSI at two loci and 8/13(61%) cases with MSI at three or more loci. Mutationsof hMSH3 were detected in 5/50 cases (10%),respectively with MSI at two loci (1/13 cases, 8%)and three or more loci (4/13 cases, 31%). Overall,among GCs with MSI at two or more loci, 46% (12/26) and 19% (5/26) respectively showed hMSH6 andhMSH3 mutations. Mutations in target genes otherthan hMSH6 were strongly associated with thepresence of hMSH6 mutations: in fact, hMSH6resulted mutated in 9/11 cases with TGF-b RIImutations, in 4/5 cases with IGFIIR mutations, and
N T N T N T N T N T N TN T
TGF-β RII poly(A)10
IGFIIR poly(G)8
BAX poly(G)8
hMSH3 poly(A)8
hMSH6 poly(C)8
E-CAD poly(A)8/(T)15
BAT-26 poly(A)26
case #5
case #58
case #60
case #70
case #75
Figure 1 Examples of mutations at coding sequence repeats within the TGFb-RII, IGFIIR, BAX, hMSH6, hMSH3 and BRCA2genes and at the non coding BAT-26 and E-Cadherin poly(A)8/(T)15 repeats. Mutations are identi®ed by the presence of bands(arrows) in tumor DNA (T) that are not present in the corresponding normal DNA (N)
Mutations at coding repeats in gastric cancerL Ottini et al
2768

in all four cases with BAX mutations. Cases withmutations at three or more coding repeats occurredonly in the category of cases with MSI at two or moreloci.With regard to clinicopathologic parameters, TGF-b
RII mutations were associated with antral tumorlocation (P50.01), while IGFIIR mutations wereassociated with female gender (P=0.03). There wereno signi®cant associations between mutations at targetgenes and patients' age, gastric cancer family history,histologic classi®cation and tumor stage.Mutations in coding mononucleotide repeats con-
sisted in allele contractions, with the exception of case#70, which harbored an expanded IGFIIR allele andbiallelic hMSH6 alterations, respectively resulting inallele expansion and allele contraction (Figure 1). Inthe case of TGF-b RII mutations the signal of theupper wild-type allele was markedly diminished relativeto that of the matching normal tissue, suggestingdouble-hit inactivation. With the exception of theabove mentioned biallelic inactivation of hMSH6,which was con®rmed by sequence analysis (data notshown), the comparable intensities of the wild-type andmutant alleles suggested that the mutations in the othercoding repeats were heterozygous.
BAT-26 and the E-Cadherin 3'UTR poly(A)8/(T)15repeat could be analysed in 44 of the 50 GCs (Table1). Mutations were observed only in MSI+ GCs and,as shown in Figure 1 (arrows), were always allelecontractions. Fourteen of the 37 MSI+ cases tested(38%) manifested BAT-26 allele shifts, including 3/14cases (21%) with MSI at one locus, 3/10 cases (30%)with MSI at two loci, 7/10 cases (70%) with MSI atthree loci and the single case with MSI at ®ve out ofsix loci. Notably, 12/14 cases (86%) with BAT-26contractions resulted also positive for mutations atcoding repeats, including 11 of 14 cases with hMSH6mutations. Ten of the 37 MSI+ cases tested (27%)manifested allele shifts of the E-Cadherin 3' UTRrepeat, including 3/10 cases (30%) with MSI at twoloci, 6/10 cases (60%) with MSI at three loci and thesingle case with MSI at ®ve out of six loci.Sequencing analysis of the cases positive for E-Cadherin 3' UTR repeat alterations revealed short-ening from 2 ± 5 bp in the poly(T)15 run examined(data not shown). The ten cases with mutations of theE-Cadherin 3' UTR repeat were always positive forBAT-26 alterations. Nine of these cases (90%)resulted also positive for mutations at codingrepeats, always including hMSH6.
Table 1 Status of coding mononucleotide repeats within the TGF-b RII, IGFIIR, BAX, hMSH6, hMSH3 and BRCA2 genes and of the non-coding BAT-26 and E-Cadherin repeats in the 40 gastric carcinomas positive for MSI at dinucleotide loci
MSI E-Cad(unstable loci) BAT-26 TGF-b RII IGFIIR BAX hMSH6 hMSH3 BRCA2 poly
Case # # poly(A)26 poly(A)10 poly(G)8 poly(G)8 poly(C)8 poly(A)8 poly(A)8 (A)8/(T)15
1224303138414657a
6979a
85971001093a
581026a
29a
357075a
105116a
117a
12125405355608898102106a
113b
108110a
58
1111111111111122222222222223333333333445
77+7+7+77777777+ndnd77++7777nd7+++++++7777+
77+777+77777777+77777+777+777++7+7+7+77+
777777777777777+77777+7777777777++77777+
777777777777777777777+777777+77777+7777+
77+777++7+77777+77777++777+7+++++7++777+
777777777777777+7777777777777+77+7+7777+
7777777777777777777777777777777777777777
777777777777777+ndnd77++7777nd7+++++7+7777+
aCases negative for BAT-40 mutations; bCase positive for BAT-40 mutation; nd: not determined
Mutations at coding repeats in gastric cancerL Ottini et al
2769

The four cases with hMSH6 mutations that werenegative for mutations of the non-coding BAT-26, andE-Cadherin repeats and of the other coding repeats (i.e.#57, #75, #79 and #106, Table 1) were furtherevaluated with BAT-40, resulting negative. Case #121,that manifested only hMSH6 mutations, could not betested for alterations at non-coding mononucleotiderepeats because of lack of DNA. The two tumors withTGF-b RII mutations that were negative for mutationsof BAT-26, of the E-Cadherin repeat and of the othercoding repeats (i.e. #113 and #117, Table 1) weresimilarly reevaluated with BAT-40. Case #113 waspositive for a BAT-40 allele contraction, whereas case#117 was con®rmed as negative.Five of the eight cases that were MSI+ at two or
more dinucleotide loci but negative for mutations atthe BAT-26 and E-Cadherin repeats and at codingmononucleotide runs (cases #3, #26, #29, #110 and#116, Table 1) were also reevaluated with BAT-40,resulting negative for mutations. The other three cases(#25, #105 and #108) could not be tested becausepara�n-embedded blocks were exhausted.
Discussion
We studied 50 GCs selected on the basis of MSI statusat dinucleotide loci (Ottini et al., 1997) for mutationsat coding repeats within the TGF-b RII, IGFIIR, BAX,hMSH6, hMSH3 and BRCA2 genes, and at non-coding repeats, including BAT-26, the poly(A)8/(T)15at the 3' UTR of the E-Cadherin gene, and, in speci®ccases, BAT-40.While a somatic BRCA2 mutation within the
poly(A)8 at codons 602 ± 605 was reported to beassociated with a somatic hMSH2 mutation in anMSI+ ovarian cancer (Takahashi et al., 1996), noBRCA2 mutations in the same poly(A)8 were observedin the presently studied GC series. In general, nomononucleotide mutations were identi®ed among the 10cases with no evidence of MSI at dinucleotide repeats.The TGF-b RII, IGFIIR, BAX, hMSH6 and hMSH3repeats were altered in 22%, 10%, 8%, 32% and 10%of the 50 cases respectively. Among GCs with MSI attwo or more loci, we observed mutations of the TGF-bRII poly(A)10 in 35% of the cases, of the IGFIIR andBAX poly(G)8 runs respectively in 17% and 14% of thecases, and of the hMSH6 poly(C)8 and hMSH3poly(A)8 respectively in 46% and 21% of the cases.With the exception of seven cases, of which two withmutations limited to TGF-b RII and ®ve to hMSH6,multiple target genes were simultaneously mutated.In agreement with other recent reports (Zhou et al.,
1997; Chung et al., 1997), we did not observeanticorrespondences between mutations of genesinsisting, at least in part, on the same molecularpathway. In particular, mutations in the TGF-b RIIand IGFIIR repeats occurred in the same cases,together with alterations at other mononucleotiderepeats. With regard to clinico-pathologic parameters,the association of TGF-b RII mutations with antralGC location may re¯ect the association between MSIand antral tumors described in our previous study(Ottini et al., 1997). The association of IGFIIRmutations with female gender is intriguing but ofobscure signi®cance.
Di�erently from colorectal cancer (Markowitz et al.,1995; Myero� et al., 1995; Rampino et al., 1997), thepresently studied GC series showed a high percentageof mutations in the hMSH6 gene relative to the othergenes, including IGFIIR and BAX. Indeed, thefrequency of TGF-b RII mutations was rather lowcompared to other studies that examined smaller seriesof MSI+ gastric cancers, reporting percentages ofmutated cases ranging from 50% (3/6) to 91% (10/11)(Ohue et al., 1996; Myero� et al., 1995; Chung et al.,1996, 1997). In particular, the recent study of Chung etal. (1997) suggested a primary responsibility of TGF-bRII and BAX mutations in driving the growth of MSI-positive gastric cancers, followed by a secondaryinvolvement of hMSH6. Our results, deriving from apopulation with di�erent epidemiological risk factors(Buiatti et al., 1991; Ottini et al., 1997), rather suggesta key role of hMSH6 in the mutational cascade leadingto the progression of MSI+ GCs. In this respect, thereport of Akiyama et al. (1997), implicating an hMSH6germline mutations in an atypical hereditary nonpoly-posis colorectal cancer kindred also suggests a primaryrole of hMSH6 in gastric carcinogenesis.Both hMSH3 and hMSH6 contribute to the
stabilization of microsatellite sequences and hMSH6is particularly involved in repairing single base mispairswithin mononucleotide runs (Papadopoulos et al.,1995). In this study, double hMSH3/hMSH6 mutantswere relatively frequent and it may be relevant to notethat these cases showed MSI at two or moredinucleotide loci and also tended to manifest muta-tions at other target genes, as well as BAT-26 and E-Cadherin 3' UTR repeat contractions. Interestingly,case #70, which manifested biallelic hMSH6 inactiva-tion, was positive for mutations of all coding and non-coding mononucleotide repeats analysed, except thehMSH3 and BRCA2 repeats.These observations are consistent with the model of
progressive mutator mutations that drives a cascade ofgenomic alterations at sequence repeats. Intriguingly,BAT-26 is located just downstream of the GT splicedonor site of intron ®ve of the hMSH2 gene and isalmost monomorphic in the population, which suggeststhat variations in its length might interfere withhMSH2 splicing (Hoang et al., 1997). However, bothcoding and non-coding mononucleotide repeats,including BAT-26, the E-Cadherin 3' UTR repeat andBAT-40 were negative for mutations in a subset ofcases with MSI at two or more dinucleotide loci,suggesting the possible existence of independent path-ways controlling mono- and dinucleotide stability ingastric cancer.
Materials and methods
Subjects
Fifty GCs were selected from a series of 108 cases in whichthe presence of MSI had been assessed at six dinucleotideloci (Ottini et al., 1997). The criteria for selection mainlytook into account MSI-positive status and availability oftissue sections for multiple DNA extractions. We selectedmost of the cases with MSI at two or more loci, including13/16 cases with MSI at two loci, 10/11 with MSI at threeloci, 2/4 with MSI at four loci and 1/2 with MSI at ®veloci. We also included a sample of the cases with MSI at
Mutations at coding repeats in gastric cancerL Ottini et al
2770

one locus (14/19) and of the MSI-negative cases (10/56).The series analysed consisted of 34 male and 16 female GCpatients with a mean age of 64.2 years at diagnosis (5 aged555 years, eight between 55 and 64 years and 26465years). A ®rst-degree family history positive for gastriccancer was veri®ed for 18 cases.
Pathology
Twenty-eight tumors were localized in the antrum and 22 inother regions of the stomach. The cases were classi®edaccording to Lauren's classi®cation (Buiatti et al., 1991). Theseries consisted of 21 GC cases of di�use and unclassi®edhistotype and 29 cases of intestinal hystotype. Twenty caseswere staged pT1-2 and 30 pT3-4, 12 were pN negative and 38pN positive. Formalin-®xed, para�n-embedded sampleswere retrieved from the ®les of the Pathology Department,Florence University. Several 5 mm step sections were cutfrom one representative block for each patient; only onesection was stained with hema-toxylin-eosin.
Analyses of mononucleotide repeats
Tumor and normal tissue DNA was extracted frompara�n-embedded sections as previously described (Ottiniet al., 1995, 1997). DNA extractions and set-up of PCRreactions were performed in a laboratory distinct from thatin which ampli®ed DNAs were manipulated. Mutations inmononucleotides runs were analysed using a PCR-basedassay, as previously described (Ottini et al., 1995, 1997).The 73-base pair region encompassing the TGF-b RIIpoly(A)10 repeat at codons 125 ± 128 was ampli®ed asreported by Parsons et al. (1995). The IGFIIR poly(G)8 atnucleotides 4089 ± 4096 was analysed by ampli®cation of a110-base pair region as reported by Souza et al. (1996). A94-base pair region encompassing the BAX poly(G)8 atcodons 38 ± 41 was ampli®ed as described by Rampino et
al. (1997). The poly(C)8 and poly(A)8 repeats, respectivelyat codons 1116 ± 1118 of the hMSH6 gene and at codons381 ± 383 of the hMSH3 gene were ampli®ed as reported byMalkhosyan et al. (1996). The BRCA2 poly(A)8 atnucleotides 1443 ± 1450 was ampli®ed using the followingprimers: forward 5'-TCTGTAGCTTTGAAGAATGCAG-3', backward 5'-TGCAAATGTAAGTGGTGCTTC-3'. A205-base pair region encompassing the E-Cadherinpoly(A)8/(T)15 at nucleotides 3153 ± 3160/3205 ± 3219 wasampli®ed using the following primers: forward 5'-ATCA-GAAGGTTCACCCAGCACC-3', backward 5'-CCGATA-GAATGAGACCCTGTC-3'. The primers used forampli®cation of BAT-26 and BAT-40 were reported byParsons et al. (1995). Analyses of mononucleotide repeatswere always consistent from at least two di�erent DNAextracts, including one extract that had been used for typingsat dinucleotide repeats, as previously reported (Ottini et al.,1997). Direct sequencing of PCR products was performedby using the Sequenase PCR sequencing kit (USB).
AcknowledgementsThis work was supported by grants from the `AssociazioneItaliana per la Ricerca sul Cancro' (AIRC) to RM-C (`Roleof BRCA1 mutations and of genomic instability in breastcancer') and AC (special project `Hereditary ColorectalTumors') and by CNR-ACRO grant 95.00325.PF39(®nalized project: `Molecular Epidemiology of GastricCancer'). LO is the recipient of an AIRC fellowship. Wethank Dr Angelo del Nero, Department of ExperimentalMedicine and Pathology, University of Rome `La Sapien-za', for his kind support. We wish to dedicate the study tothe memory of Gaetano (`Nino') Salvatore, late Professorof General Pathology at the University `Federico II' ofNaples, who was one of the founding fathers of molecularoncology in Italy.
References
Akiyama Y, Sato H, Yamada T, Nagasaki H, Tsuchiya A,Abe R and Yuasa Y. (1997). Cancer Res., 57, 3920 ± 3923.
Arnheim N and Shibata D. (1997). Curr. Opin. Genet. Dev.,7, 364 ± 370.
Buiatti E, Palli D, Bianchi S, Decarli A, Amadori D, AvelliniC, Cipriani F, Cocco P, Giacosa A, Lorenzini L, MarubiniE, Puntoni R, Saragoni A, Fraumeni JF Jr and Blot WJ.(1991). Int. J. Cancer, 48, 369 ± 374.
Chung Y-J, Song J-M, Lee J-Y, Jung Y-T, Seo E-J, Choi S-Wand Rhyu M-G. (1996). Cancer Res., 56, 4662 ± 4665.
Chung Y-J, Park S-W, Song J-M, Lee K-Y, Seo E-J, Choi S-W and Rhyu M-G. (1997). Oncogene, 15, 1719 ± 1726.
Dahms NM, Lobel P and Kornfeld S. (1989). J. Biol. Chem.,264, 12115 ± 12118.
Dennis PA and Rifkin DB. (1991). Proc. Natl. Acad. Sci.USA, 88, 580 ± 584.
Casey G. (1997). Curr. Opin. Oncol., 9, 88 ± 93.Hoang JM, Cottu PH, Thuille B, Salmon RJ, Thomas G andHamelin R. (1997). Cancer Res., 57, 300 ± 303.
Kornfeld S. (1992). Annu. Rev. Biochem., 61, 307 ± 330.Malkhosyan S, Rampino N, Yamamoto H and Perucho M.(1996). Nature, 382, 499 ± 500.
Markowitz S, Wang S, Myero� L, Parsons R, Sun LZ,Lutterbaugh J, Fan RS, Zborowska E, Kinzler KW,Vogelstein B, Brattain M and Willson JKV. (1995).Science, 268, 1336 ± 1338.
Miyashita T and Reed JC. (1995). Cell, 80, 293 ± 299.Myero� LL, Parsons R, Kim SJ, Hedrick L, ChoKR, OrthK,Mathis M, Kinzler KW, Lutterbaugh J, Park K, Bang YJ,Lee HY, Park JG, Lynch HT, Roberts AB, Vogelstein Band Markowitz SD. (1995). Cancer Res., 55, 5545 ± 5547.
Ohue M, Tomita N, Monden T, Miyoshi Y, Ohnishi T,Izawa H, Kawabata Y, Sasaki M, Sekimoto M, NishishoI, Shiozaki H and Monden M. (1996). Int. J. Cancer, 68,203 ± 206.
Oltvai ZN, Milliman CL and Korsmeyer SJ. (1993). Cell, 74,609 ± 619.
Ottini L, Esposito DL, Richetta A, Carlesimo M, PalmirottaR, VerõÁ MC, Battista P, Frati L, Caramia FG, Calvieri S,Cama A and Mariani-Costantini R. (1995). Cancer Res.,55, 5677 ± 5680.
Ottini L, Palli D, Falchetti M, D'Amico C, Amorosi A,Saieva C, Calzolari A, Cimoli F, Tatarelli C, De MarchisL, Masala G, Mariani-Costantini R and Cama A. (1997).Cancer Res., 57, 4523 ± 4529.
Ouyang H, Shiwaku HO, Hagiwara H, Miura K, Abe T,Kato Y, Ohtani H, Shiiba K, Souza RF, Meltzer SJ andHorii A. (1997). Cancer Res., 57, 1851 ± 1854.
Papadopoulos N, Nicoladeis NC, Liu B, Parsons R,Lengauer C, Palombo F, D'Arrigo A, Markowitz S,Willson JKV, Kinzler KW, Jiricny J and Vogelstein B.(1995). Science, 268, 1915 ± 1917.
Parsons R, Myero� LL, Liu B, Willson JKV, Markowitz SD,Kinzler KW and Vogelstein B. (1995). Cancer Res., 55,5548 ± 5550.
Perucho M. (1996). Nat. Med., 2, 630 ± 631.Prolla TA, Abuin A and Bradley A. (1996). Semin. Cancer
Biol., 7, 241 ± 247.Rampino N, Yamamoto H, Ionov Y, Li Y, Sawai H, ReedJC and Perucho M. (1997). Science, 275, 967 ± 969.
Mutations at coding repeats in gastric cancerL Ottini et al
2771

Souza RF, Appel R, Yin J, Wang SN, Smolinski KN,Abraham JM, Zou TT, Shi YQ, Lei JY, Cottrell J, CymesK, Biden K, Simms L, Leggett B, Lynch PM, Frazier M,Powell SM, Harpaz N, Sugimura H, Young J and MeltzerSJ. (1996). Nat. Genet., 14, 255 ± 257.
Stratton MR and Wooster R. (1996). Curr. Opin. Genet.Dev., 6, 93 ± 97.
Takahashi H, Chiu H-S, Bandera CA, Behbakht K, Liu PC,Couch FJ, Weber BL, LiVolsi VA, Furusato M, RebaneBA, Cardonick A, Benjami M, Morgan MA, King SA,Mikuta JJ, Rubin SC and Boyd J. (1996). Cancer Res., 50,2738 ± 2741.
Zhou X-P, Hoang J-M, Cottu P, Thomas G and Hamelin R.(1997). Oncogene, 15, 1713 ± 1718.
Mutations at coding repeats in gastric cancerL Ottini et al
2772