Mind-Body Medicine: Stress and Its Impact on Overall Health and Longevity
14
492 Ann. N.Y. Acad. Sci. 1057: 492–505 (2005). © 2005 New York Academy of Sciences. doi: 10.1196/annals.1322.038 Mind–Body Medicine Stress and Its Impact on Overall Health and Longevity L. VITETTA, a B. ANTON, b F. CORTIZO, c AND A. SALI c a Centre for Molecular Biology and Medicine, Epworth Hospital Medical Centre, Melbourne, Australia b PathLab, Melbourne, Australia c National Institute of Integrative Medicine, Swinburne University, Melbourne, Australia ABSTRACT: The belief that adverse life stressors and the emotional states that can lead to major negative impacts on an individual’s body functions and hence health has been held since antiquity. Adverse health outcomes such as coronary heart disease, gastrointestinal distress, and cancer have been linked to unre- solved lifestyle stresses that can be expressed as a negative impact on human survival and ultimately a decrease of the human life span. Psychological mod- ulation of immune function is now a well-established phenomenon, with much of the relevant literature published within the last 50 years. Psychoneuroimmu- nology and psychoneuroendocrinology embrace the scientific evidence of re- search of the mind with that of endocrinology, neurology and immunology, whereby the brain and body communicate with each other in a multidirectional flow of information that consists of hormones, neurotransmitters/neuropep- tides, and cytokines. Advances in mind–body medicine research together with healthy nutrition and lifestyle choices can have a significant impact on health maintenance and disease prevention and hence the prolongation of the human life span. KEYWORDS: mind–body medicine; psychoneuroimmunology; psychoneuro- endocrinology; psychosocial stress; longevity MIND–BODY MEDICINE The concept of the mind and human thought is not a novel one. Many tentative explanations have been advanced, even in the form of art—notably in Michelange- lo’s Creation of Adam, in which man’s mind and thought are depicted by a sagittal section of the brain that is strikingly similar to current anatomical drawings of the brain (FIG. 1). The most important factor in why a person becomes ill lies in the brain. Stress and pleasure play a critical role in wellness and disease, with stress contributing Address for correspondence: Dr. Luis Vitetta, Associate Professor and Senior Research Fel- low, Centre for Molecular Biology and Medicine, Epworth Medical Centre, 185-187 Hoddle St. Richmond, Melbourne, Victoria, Australia 3121. Voice: +61 3 9426 4200; fax: +61 3 9426 4201. [email protected]
Transcript of Mind-Body Medicine: Stress and Its Impact on Overall Health and Longevity

492
Ann. N.Y. Acad. Sci. 1057: 492–505 (2005). © 2005 New York Academy of Sciences.doi: 10.1196/annals.1322.038
Mind–Body Medicine
Stress and Its Impact on OverallHealth and Longevity
L. VITETTA,a B. ANTON,b F. CORTIZO,c AND A. SALIc
aCentre for Molecular Biology and Medicine, Epworth Hospital Medical Centre, Melbourne, AustraliabPathLab, Melbourne, AustraliacNational Institute of Integrative Medicine, Swinburne University, Melbourne, Australia
ABSTRACT: The belief that adverse life stressors and the emotional states thatcan lead to major negative impacts on an individual’s body functions and hencehealth has been held since antiquity. Adverse health outcomes such as coronaryheart disease, gastrointestinal distress, and cancer have been linked to unre-solved lifestyle stresses that can be expressed as a negative impact on humansurvival and ultimately a decrease of the human life span. Psychological mod-ulation of immune function is now a well-established phenomenon, with muchof the relevant literature published within the last 50 years. Psychoneuroimmu-nology and psychoneuroendocrinology embrace the scientific evidence of re-search of the mind with that of endocrinology, neurology and immunology,whereby the brain and body communicate with each other in a multidirectionalflow of information that consists of hormones, neurotransmitters/neuropep-tides, and cytokines. Advances in mind–body medicine research together withhealthy nutrition and lifestyle choices can have a significant impact on healthmaintenance and disease prevention and hence the prolongation of the humanlife span.
KEYWORDS: mind–body medicine; psychoneuroimmunology; psychoneuro-endocrinology; psychosocial stress; longevity
MIND–BODY MEDICINE
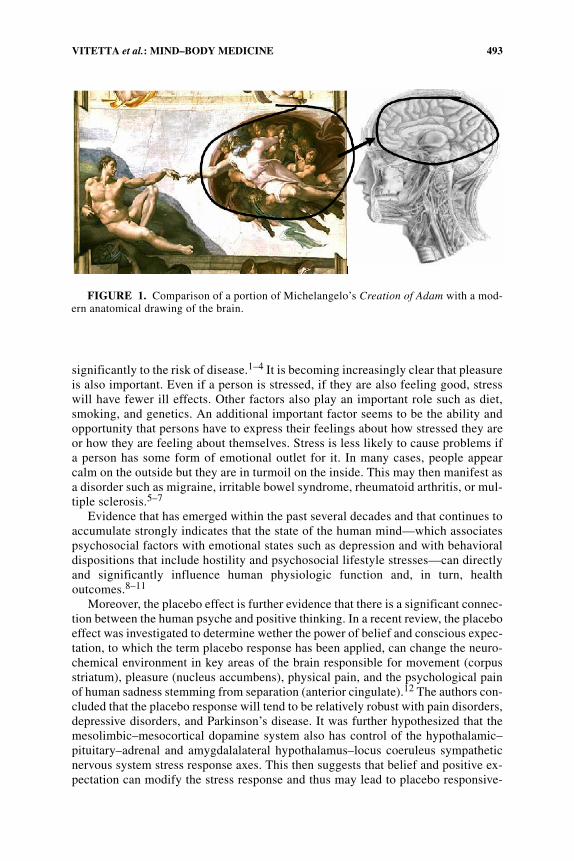
The concept of the mind and human thought is not a novel one. Many tentativeexplanations have been advanced, even in the form of art—notably in Michelange-lo’s Creation of Adam, in which man’s mind and thought are depicted by a sagittalsection of the brain that is strikingly similar to current anatomical drawings of thebrain (FIG. 1).
The most important factor in why a person becomes ill lies in the brain. Stressand pleasure play a critical role in wellness and disease, with stress contributing
Address for correspondence: Dr. Luis Vitetta, Associate Professor and Senior Research Fel-low, Centre for Molecular Biology and Medicine, Epworth Medical Centre, 185-187 Hoddle St.Richmond, Melbourne, Victoria, Australia 3121. Voice: +61 3 9426 4200; fax: +61 3 9426 4201.
493VITETTA et al.: MIND–BODY MEDICINE
significantly to the risk of disease.1–4 It is becoming increasingly clear that pleasureis also important. Even if a person is stressed, if they are also feeling good, stresswill have fewer ill effects. Other factors also play an important role such as diet,smoking, and genetics. An additional important factor seems to be the ability andopportunity that persons have to express their feelings about how stressed they areor how they are feeling about themselves. Stress is less likely to cause problems ifa person has some form of emotional outlet for it. In many cases, people appearcalm on the outside but they are in turmoil on the inside. This may then manifest asa disorder such as migraine, irritable bowel syndrome, rheumatoid arthritis, or mul-tiple sclerosis.5–7
Evidence that has emerged within the past several decades and that continues toaccumulate strongly indicates that the state of the human mind—which associatespsychosocial factors with emotional states such as depression and with behavioraldispositions that include hostility and psychosocial lifestyle stresses—can directlyand significantly influence human physiologic function and, in turn, healthoutcomes.8–11
Moreover, the placebo effect is further evidence that there is a significant connec-tion between the human psyche and positive thinking. In a recent review, the placeboeffect was investigated to determine wether the power of belief and conscious expec-tation, to which the term placebo response has been applied, can change the neuro-chemical environment in key areas of the brain responsible for movement (corpusstriatum), pleasure (nucleus accumbens), physical pain, and the psychological painof human sadness stemming from separation (anterior cingulate).12 The authors con-cluded that the placebo response will tend to be relatively robust with pain disorders,depressive disorders, and Parkinson’s disease. It was further hypothesized that themesolimbic–mesocortical dopamine system also has control of the hypothalamic–pituitary–adrenal and amygdalalateral hypothalamus–locus coeruleus sympatheticnervous system stress response axes. This then suggests that belief and positive ex-pectation can modify the stress response and thus may lead to placebo responsive-
FIGURE 1. Comparison of a portion of Michelangelo’s Creation of Adam with a mod-ern anatomical drawing of the brain.

494 ANNALS NEW YORK ACADEMY OF SCIENCES
ness of many psychophysiological disorders such as hypertension, angina,inflammatory bowel disease, and asthma.12
There is now clear scientific evidence that indicates that the brain regulates im-mune function through efferent autonomic and neuroendocrine pathways.1 More-over, there are numerous afferent pathways by which the immune system modulatesbrain function. Psychoneuroimmunology, a term first coined by Robert Ader in the1980s, refers to these connections between the psyche, the nervous system, and theimmune system.1,2 The development of the science of psychoneuroimmunologyprovides an enormous opportunity to understand the role of the mind in the cause ofdisease. Psychoneuroendocrinology, which refers to the connections between thepsyche and the endocrine system, is equally important. Thus, behavior, the nervoussystem, and the endocrine system all influence the immune system. A feedback sys-tem also exists by which it is able to connect with all aspects of the brain. The detailsof the mechanisms involved in psychoneuroimmunology are the subject of much ofthe current research.
STRESS AND HEALTH
The history of the concept of stress in relation to disease processes reaches backto the nineteenth century and through to the twentieth century and beyond. It hasbeen and continues to be the subject of intense debate and research with reports thatstress may have ameliorating or detrimental capacities. The pioneering work of HansSelye is often credited with establishing the scientific fact that there is a significantrelationship between pathophysiological processes and the onset of chronic diseas-es.13,14 Selye successfully advanced the concept that stress was critically importantin physiology and medicine, and that today we recognize that many contemporarytheories relating to the etiology of chronic diseases have a stress component as a sig-nificant precipitating variable. Moreover, recently it has been shown that stressfullife events can have a significant negative impact on longevity, by playing an impor-tant role in the onset of cardiovascular disease, immunological disorders, and patho-physiological consequences of normal aging.
Stress describes the effects of psychosocial and environmental factors on physicalor mental well being. Stressors and stress-related reactions have been documentedand recognized and exposure to chronic social stress has been associated with manysystemic and mental disorders. Hypotheses from different research groups supportthe notion that health consequences are more likely to occur when unpredictablestressors of a social nature chronically induce physiological and behavioral adjust-ments that may create wear and tear on the underlying physiological functions.15
When stressors challenge an organism’s integrity, a set of physiological reactions iselicited to counteract the possible threat and adjust the physiological setting of theorganism to the new situation. This has become known as the stress response.16
The stress response that initiates the neuroendocrine system has been extensivelystudied in the sympathetic–adreno–medullary system, which is under the control ofthe central nervous system.16 A further component of the stress response is the hy-pothalamic–pituitary–adrenal axis, which is diagrammatically illustrated in FIGURE
2, and is an important modulator of the brain–immune–endocrine–neurotransmitterinterconnection cycle.

495VITETTA et al.: MIND–BODY MEDICINE
These two systems are normally operating within a fine-tuned state of balanceknown as homeostasis, which is established in order to maintain the organism’s in-tegrity even under extremely challenging conditions. Further, these two systemshave a dependence on chemical transmitters for effective communication. This is ob-served when electrical signals along nerve pathways are converted to chemical sig-nals at the site of synaptic junctions between neurons. The chemical message that isproduced by the activity of immune-system cells can communicate not only withother parts of the immune system but also with the brain and nerves. Alternatively,chemicals released by nerve cells can act as signals to immune cells.
There is also an important endocrine component to these systems, where the brainhas a central and prolific role as an endocrine organ in the body and produces manyhormones that act both on the brain and on tissues throughout the body. In particular,a key hormone shared by the central nervous and immune systems is corticotropin-releasing hormone (CRH). CRH is produced in the hypothalamus and other brain ar-eas and is essential in uniting the stress and immune response. Specifically, the hy-pothalamus releases CRH into a specialized bloodstream circuit that conveys thehormone to the pituitary gland. CRH causes the pituitary gland to release adrenocor-ticotropin hormone (ACTH) into the bloodstream, which stimulates the adrenalglands to produce cortisol, an extensively studied stress hormone.16,17
FIGURE 2. Diagrammatic representation of the inter-relationships between the hypo-thalamic–pituitary–adrenal axis and the immune–endrocrine responses. Ach = acetylcho-line; 5HT = 5 hydroxytryptamine; CRF = corticotrophin-releasing factor; GABA = gamma-aminobutyric acid; A = adrenaline; NA = noradrenaline; IL = interleukin; TNF = tumornecrosis factor. (Modified from Song and Leonard.1)

496 ANNALS NEW YORK ACADEMY OF SCIENCES
Cortisol is a steroid hormone that has many actions that include: increasing therate and strength of heart contractions and sensitizing blood vessels to the actions ofnorepinephrine; it has effects on many metabolic functions as well. These actions as-sist the body in coping with stressful situations. Moreover, cortisol is a potent immu-noregulator and anti-inflammatory agent. Cortisol also has a crucial role inpreventing the immune system from overreacting to injuries and damaging tissues.Cortisol inhibits the release of CRH by the hypothalamus, thus keeping this compo-nent of the stress response under a fine control. Hence the body’s brain-regulatedstress response and its associated immune response directly link the activity of CRHand cortisol.There are CRH-secreting neurons of the hypothalamus that send fibersto regions in the brain stem that help regulate the sympathetic nervous system, aswell as to other brain stem areas such as the locus coeruleus. The sympathetic ner-vous system, which mobilizes the body during stress, also innervates immune-activetissue, such as the thymus, lymph nodes, and the spleen, and further assists to controlinflammatory responses throughout the body. Stimulation of the locus coeruleusleads to behavioral arousal, fear, and enhanced vigilance. Other brain CRH-secretingneurons are present in the central nucleus of the amygdala and send fibers to the hy-pothalamus, the locus coeruleus, and other parts of the brain stem. These CRH-se-creting neurons are targets of messengers released by immune cells during animmune response. The additional recruitment of these CRH-secreting neurons al-lows immune signals not only to activate cortisol-mediated restraint of the immuneresponse, but also to induce behaviors that assist in recovery from illness or traumat-ic injury. Further, chemical transmitters are also involved in tensing muscles. Thusthe tenser a muscle becomes, the more alert and stressed the brain becomes and thetenser the muscles become, which creates further stress. An additional and importantconnection is that CRH-secreting neurons also have connections with hypothalamicregions that regulate food intake and reproductive behavior.16,17
The immune response is an elegant surveillance mechanism that is finely tunedin a series of cascade cellular events whose ultimate goal is to protect the organismfrom foreign substances, such as bacteria and viruses. The discovery of small proteinmolecules known as cytokines (e.g., interleukin-1 and interleukin-2), which areelaborated by different types of white blood cells, allowed for further understandingof how the immune response is structured and coordinated. Cytokines from thebody’s immune system can send signals to the brain via several mechanisms, includ-ing crossing the brain–blood barrier via the bloodstream. This permeability is essen-tial for communication with brain areas. Cytokines can attach to their receptors inthe lining of blood vessels in the brain and stimulate the release of secondary chem-ical signals in the brain tissue around the blood vessels. Cytokines can also signalthe brain via direct nerve routes, (e.g., the vagus nerve) and a multitude of connec-tions with abdominal organs result. The activation of the brain by cytokines from theperipheral parts of the body induces the behaviors of anxiety and cautious avoidanceassociated with the stress response’s principle activity—maintaining the organism’sintegrity during recovery from stressful activities or from traumatic injury.18
The disruption of communication between the brain and the immune system leadsto greater susceptibility to inflammatory disease and, frequently, to increased im-mune complications.18,19 Laboratory animals whose brain-immune communica-tions have been disrupted (through surgery or pharmaceuticals) are highlyvulnerable to lethal complications of inflammatory diseases and infectious diseases.
497VITETTA et al.: MIND–BODY MEDICINE
Further, in studies with laboratory animals and in human pharmacological and sur-gical trials there has been evidence of a causal link between an impaired stress re-sponse and susceptibility to inflammatory disease.
The stress response hence represents a complex effector system that is susceptibleto pathophysiological factors and conditions and has an input into many biologicalprocesses. Therefore the stress response can exert ameliorating or detrimental ef-fects, where mediators of stress physiology can have both protective and harmful ef-fects in organs such as the heart, the immune system, or the brain. Adverse effectson such organs may well have significant negative shifts in overall survival.16–19
Humans living in the 21st century are subject to an ever-increasing degree of ho-meostatic control between the interrelationships of external/environmental and in-ternal (behavioral, cognitive, emotional) stressors, the physiological responses tothese challenges, and the prevalence of disease/illness. This dynamic balance of con-tinual adjustment to stressors maintains stability. Also, the cascade of adaptive re-sponses imprinted within the human genetic makeup may themselves turn intostressors capable of triggering and maintaining disease processes.
MIND–BODY MEDICINE: THE CONNECTION TO DISEASE
Social stressors and lifestyle choices can be a significant trigger for disease,which can then affect longevity. Psychosocial stress is a personal response perceivedthrough the complexities of social interactions. These interactions can either be neg-ative and increase or be positive and lessen psychological stress. These interactionscan affect the hormonal responses that are elicited as a result, which can then signif-icantly alter immune responses. Moreover, stress can significantly reduce physicaland mental tolerances (immune potential) of humans and it can induce the progres-sion of existing illnesses or it can cause latent disorders to become active. Therefore,the control and suppression of stress is very important in the improvement of qualityof life and the prevention of diseases. The physiological changes that ensue with un-manageable stress may then have a negative impact on health.20 The social-psycho-logical network of stressors that we experience can affect our susceptibility toinflammatory and infectious diseases as well as the course of these and other diseas-es and in so doing affect the human life span.20–23
In humans, loneliness is associated with a threat, or an epinephrine-like patternof activation of the stress response that results in an elevation of blood pressure,whereas exercising is associated with a challenge pattern of high blood flow and car-diac output. Studies have shown that people exposed to chronic social stresses formore than two months have increased susceptibility to the common cold.24
It is of significant interest that in Australia there is a disparity in the rate of suicidedeaths between rural and city areas.25–27 Australia has one of the highest per capitayoung male youth suicide rate as well as one of the highest rates of antidepressantuse.25,26 Young males are experiencing grave difficulties with life changes that oc-cur, whether in the work or home environments. In rural areas unemployment andisolation play major roles in the rate of suicide. Further a recent study evaluated theassociation of glycemic control and major depression in type 1 and 2 diabetes mel-litus.28 Type 1 insulin–dependent diabetes mellitus patients with a lifetime historyof depression showed a significantly worse glycemic control, whereas patients with

498 ANNALS NEW YORK ACADEMY OF SCIENCES
type 2 non-insulin–dependent diabetes mellitus with a similar history did not have asignificantly worse glycemic control.28 Hence depression can be a significant mark-er for increased risk of ill health and a decrease in the human life span.29
This link between depression and ill health is further strengthened in studies be-tween depression and idiopathic urinary incontinence. It has been shown that this as-sociation may be due to altered serotonin functioning and may help explain theefficacy of serotogenic-based antidepressants in the treatment of urge inconti-nence.30 Also, depression has been associated with functional disability in patientswith coronary artery disease (CAD). Depressive symptoms are highly prevalent inpatients with CAD and have been shown to increase their rate of cardiac-associateddeath and rate of mortality due to all causes. Depressed CAD patients have beenshown to have an 84% greater risk of cardiac death 5–10 years later when comparedto nondepressed CAD patients.31
Evidence continues to support the fact the physical disease results from emotion-al distress. School examination–induced stresses increase viral infection susceptibil-ity in adolescents.32,33 Stress from lack of control in the workplace or from lifeevents increases susceptibility to cardiovascular disease.34 A recent meta-analysis ofbiofeedback and pelvic floor exercises for female stress incontinence has been re-ported.35 The results showed that biofeedback may be an important adjunct to pelvicfloor muscle exercises. Further, interstitial cystitis, which causes bladder symptoms,has been shown to be stress related and these patients significantly have an elevatedlevel of norepinephrine in urine.36
Other studies have shown that the immune responses of long-term caregivers,such as spouses of Alzheimer’s patients, become blunted.37 Immune responses dur-ing marital discord are also blunted in the spouse (usually the wife) who experiencesthe greatest amount of stress and feelings of helplessness.38 In such studies the levelsof stress hormones are elevated in the affected spouse.37,38 Conversely, a positivesupportive environment of extensive social networks or group psychotherapy can en-hance immune response and resistance to disease—even cancer.39,40 Studies haveshown that women with breast cancer, for instance, who receive strong, positive so-cial support during their illness have significantly longer life spans than womenwithout such support.41
Moreover, recently our group has shown in preliminary data that psychosocialtreatment programs for cancer patients annexed to traditional approaches offered bymainstream medical institutions in less orthodox approaches, such as that deliveredby The Gawler Foundation in Melbourne, Australia, may constitute the holistic careprovision that active cancer support programs should provide. With a design focusto improve quality of life and, if possible, to affect length of life, this holistic healthapproach, which is complementary to mainstream medical treatment, adjusts the pa-tient’s focus on mind–body medicine modalities, such as relaxation and meditation,that then are combined with low-fat vegetarian diets, positive thinking, and drawingon effective support. This approach provides a positive environment that significant-ly contributes to enhancing the quality of life of chronically ill patients and couldsignificantly affect longevity.
Certainly, our preliminary data showed that a significant reduction in scores de-termined by the Profile of Mood States (POMS) for total mood disturbance, tension-anxiety, depression-dejection, anger-hostility, fatigue, and confusion-bewildermentscores and showed increase scores for vigor (all P < 0.01). Scores on the helpless-

499VITETTA et al.: MIND–BODY MEDICINE
ness-hopelessness subscale of the mini-Mental Adjustment to Cancer (mini-MAC)were significantly reduced and scores on the fighting spirit subscale were signifi-cantly increased (P < 0.01). Total scores on the Functional Assessment of ChronicIllness Therapy-Spirituality (FACIT-Sp) scale were significantly increased as werescores on the physical, emotional, functional, and spiritual subscales (all P < 0.01).Salivary cortisol levels were significantly decreased (P < 0.05).42
Several epidemiological studies have shown that social and emotional supportcan protect against premature mortality, prevent illness, and assist recovery from ill-ness.43,44 A recent report found that smokers treated with nortriptyline and cognitivebehavioral therapy were significantly aided in smoking cessation. It is not surprisingthat this treatment was successful, as other research has demonstrated that smokersare more likely to be depressed.45 Vigorous exercise facilitates smoking cessationwhen combined with a cognitive behavioral program. Moreover, exercise has beenshown to work as an antidepressant.46
Nutrition is an important factor that significantly contributes to how long a personwill live. Decisions about poor dietary choices, in addition to smoking, lack of exer-cise, and excessive drinking are known to be important causes of disease.47 The sizeand frequency of meals are fundamental aspects of nutrition that can have profoundeffects on the health and longevity of laboratory animals. Moreover, caloric restric-tion is the most potent and reproducible environmental variable capable of extendingthe life span in a variety of animals from worms to rats. In humans, excessive caloricintake is associated with increased incidence of cardiovascular disease, diabetes, andcertain types of cancer. It is a major cause of disability and death in industrializedcountries.48 The type of nutrients consumed also have significant correlations to nu-merous kinds of cancer (TABLE 1).49–51
The worsening global epidemic of obesity has increased the urgency of researchaimed at understanding the mechanisms of appetite regulation. An important aspectof the complex pathways involved in modulating energy intake is the interaction be-tween hormonal signals of energy status released from the gut in response to a meal,and appetite centers in the brain and brainstem. The challenges of the obesity epi-demic are not limited to concerns about bulk and weight. The disabilities caused byobesity are physiologic and psychosocial. The increased waist-to-hip girth is associ-ated with increased risk of cardiovascular disease, hyperlipidemia, hypertension,and diabetes.52 Obesity also has been related directly to increased risk of sleep ap-nea, cancer, gallbladder disease, musculoskeletal disorders, severe pancreatitis, bac-terial panniculitis, diverticulitis, infertility, urinary incontinence, and idiopathicintracranial hypertension. The psychosocial factors and quality of life in the obesepopulation also have been documented. Although there is some debate, the obesehave been found to be twice as likely to suffer from anxiety, impaired social interac-tion, and depression when compared with the nonobese population.52
Several studies indicate that adherence to a Mediterranean diet is associated witha reduction in total and cardiovascular mortality.53–56 High intake of olive oil is con-sidered a hallmark of the traditional Mediterranean diet, resulting in high intake ofmonounsaturated fatty acids and lower intake of saturated fatty acids. The replace-ment of saturated with monounsaturated lipids is strongly associated with a signifi-cant reduction in coronary heart disease risk, through a mechanism involvingreduction of LDL cholesterol, without a reduction of HDL cholesterol or an increasein triacylglycerols.57

500 ANNALS NEW YORK ACADEMY OF SCIENCES
THE PSYCHE AND ITS LINK TO HEALTH/DISEASEAND PREMATURE DEATH/LONGEVITY
Characteristics of an unhealthy lifestyle, such as too little physical activity, smok-ing, irregular and unbalanced diet, and excessive consumption of alcohol and coffeeare assumed to have relationships with major health problems such as cardiovasculardisease, cancer, and osteoporosis58 and thus significantly reduce the human life
TABLE 1. Specific cancer relationships based on epidemiological studiesa
Cancer site Incidence association
Pancreatic smokingpossibly meatcholesterol
Esophageal alcoholtobaccocombined use
Stomach salt-preserved foodspossibly BBQgrilling
Colorectal saturated fatpossibly eggsgrillingsugar
Liver hepatitis Baflatoxinsalcohol
Lung smokingpossibly alcoholsaturated fatscholesterol
Breast obesityearly-puberty alcohol consumptionpossibly meatsaturated fats
Endometrial obesityestrogen therapysaturated fats
Cervical folate deficiencysmoking
Bladder smokingpossibly artificial sweetenerscoffeealcohol
Prostate high saturated fat intake
aAdapted from Cummings49 and Bingham and Willett.50,51

501VITETTA et al.: MIND–BODY MEDICINE
span. Moreover, hostility, anger, and aggressive behavior play a central role in thecenturies-old hypothesis that emotions and aspects of personality influence physicalhealth.59
The idea of personality traits may be as old as human communication and lan-guage itself. In Aristotle’s (384–322 B.C.) Ethics, character traits such as vanity,modesty, and cowardice are described as key determinants of human moral and im-moral behavior. He also described individual variations in these traits, often referringto excessive, defective, and intermediate levels of each. The role of personalities forthe development of chronic diseases has received much attention and the role of be-havioral medicine in the area of cardiovascular disease has successfully introducedthe type A or coronary-prone behavior pattern evident from large epidemiologicstudies.59 This pattern of chronic disease development was shown to be marked byboth psychologic and physiologic hyper responsiveness. Type A individuals appearto be hostile, easily angered, competitive, and hard-driving. More recently, oncolo-gists who study human behavior have similarly attempted at hypothesizing a type Cor biopsychosocial cancer risk pattern: it was noted these individuals have a profileconsistent with denial and suppression of emotions, in particular anger. Further, ad-ditional features of this pattern are a sense of too much niceness that borders on apathological problem, avoidance of conflicts, exaggerated social desirability, harmo-nizing behavior, over-compliance, over-patience, as well as high rationality and arigid control of emotional expression. It is further conceptualized that this patterncould be usually concealed behind a facade of pleasantness that appears to be effec-tive as long as environmental and psychological homeostasis is maintained. Howev-er the facade can collapse in the course of time under the impact of accumulatedstrains and stressors, especially those evoking feelings of depression and reactionsof helplessness and hopelessness as encountered during everyday life. As a promi-nent feature of this particular coping style, excessive denial, avoidance, suppression,and repression of emotions and basic needs appears to weaken the human organism’snatural resistance to carcinogenic influences.59,60 Yet conflicting data fail to conclu-sively elucidate the causal role of the Type C personality on cancer development.61
As a general view of mechanisms that link an individual’s personality to health,the constitutional vulnerability model suggests that basic, possibly genetically deter-mined, biological, individual differences are responsible both for the personalityphenotype and the increased risk of disease.
Recent clinical reviews present cumulative clinical evidence that lends strongsupport to the notion that medicine should indeed adopt a biopsychosocial ratherthan an exclusively biologic–genetic model of health.62,63 This is the domain that in-cludes mind–body medicine, which is at the center of the provision of holistic health.However, this may be only a modern version of an already-practiced art that seemedlost in history.
Throughout history, spa and sanatorium mountain resorts have played an impor-tant role in the history of medicine; in almost every culture there have been archae-ological discoveries of the existence of hot springs and spa treatment.64 In Homerictimes (1000–700 B.C.), bathing was used primarily for cleansing and hygienic pur-poses. By the time of Hippocrates (460–370 B.C.), bathing was considered more thana simple hygienic mesasure; it was a healthy practice considered beneficial for mostdiseases. The hypothesis then elaborated by Hippocrates proposed that the cause ofall diseases lay in an imbalance of bodily fluids. Hence, to regain the balance, a

502 ANNALS NEW YORK ACADEMY OF SCIENCES
change of habits and environment was advised, which included bathing, perspira-tion, exercise/walking, and bodily massage. The baths were often combined withsports and education, the precursors of modern gymnasiums and meditation centers.
The scientific evidence emerging within the past several decades strongly sug-gests that psychosocial factors from emotional states that include depression and be-havioral dispositions that range from hositlity to psychosocial stress can directlyinfluence both physiologic function and health outcomes. It then follows that inflam-matory responses are modulated by a bidirectional communication flow between theneuroendocrine and immune systems and the brain. Also, many lines of researchhave established multiple pathways by which the immune system and the centralnervous system communicate. Hormonal and neuronal mechanisms by which thebrain regulates the function of the immune system and, conversely, cytokines, whichallow the immune system to regulate the brain provide the basis for mind–body med-icine modalities such as relaxation and meditation that impart a positive influence onhomeostatic balance. In a healthy individual this bidirectional regulatory syustemforms a negative feedback loop that keeps the immune system and contral nervoussystem in homeostatic balance. Changes to these regulatory systems have been pos-tulated to potentially lead to either overactive immune response, inducing inflamma-tory disease, or oversuppression of the immune system and increased susceptibilityto infectious disease.62–65 Relaxation and meditation in daily recreatrional activitiesmay consititute the requisite trigger for a regularizatrion of homeostatic balance.
Practices that link the mind through brain-guided activites to physiological func-tioning extend our understanding of the biopsychological model and the role emo-tional well-being has in the brain, immune system, and endocrine organs. Hence, alink is established between psychological and lifestyle-induced stressors and a broadarray of adverse health outcomes that can be traced to hypothalamic–pituitary–im-mune system–endocrine mediators. It may well be feasible to view attendance at spaand sanatorium mountain resorts as reversal programs of deleterious health out-comes in which the ultimate aim is to revitalize the body. The physiological under-pinnings of this relationship comprises an exciting area of medicine that aims atrestoring the disrupted communication system, whether through pharmacotherapyalone or, more importantly, in conjunction with the relaxing effects of a spa and med-itation in an integrative approach, the framework of mind–body medicine.
As evidence continues to accumulate within the field of psychoneuroendocrinol-ogy and psychoneuroimmunology, the brain has truly an overarching role in healthand disease1–3 and may hence be viewed as the conductor of the body orchestra.Clinical research in health and in disease prevention as well as diseases associatedwith chronic inflammations that significantly affect an individual’s mood or level ofanxiety and depression will further crystallize the role of the brain and the mind inhuman health. When the body is working well, nutrition and mental health are alsogood. If one then feels good about oneself, quality of life is enhanced, and a long lifeis made possible.
Finally, the plethora of scientific evidence that is currently available overrides theboundaries that have restricted the elucidation of the interrelationships between themind, brain, and body and that will be looked back upon as artifacts.
[Competing interests: The authors declare that they have no competing financialinterests.]
503VITETTA et al.: MIND–BODY MEDICINE
REFERENCES
1. SONG, C. & B.E. LEONARD. 2001. Fundamentals of Psychoneuroimmunology. Wiley.New York.
2. KIECOLT-GLASER, J.K., L. MCGUIRE, T.F. ROBLES & R. GLASER. 2002. Psychoneuroim-munology and psychosomatic medicine: back to the future. Psychosom. Med. 64:15–28.
3. YOUNG, E. et al. 1998. Psychoneuroendocrinology of depression: hypothalamic–pitu-itary–gonadal axis. In Psychoneuroendocrinology. C.B. Nemeroff, Ed.: 309–324.The Psychiatric Clinic of North America. Saunders. Philadelphia.
4. PLOTSKY, P.M. et al. 1998. Psychoneuroendocrinology of depression: hypothalamic–pituitary–gonadal axis. In Psychoneuroendocrinology. C.B. Nemeroff, Ed.: 293–308.The Psychiatric Clinic of North America. Saunders. Philadelphia.
5. ERNST, E. et al. 1998. Complementary therapies for depression: an overview. Arch.Gen. Psychiatry 55: 1026–1032.
6. MUFSON, L. et al. 1999. Efficacy of interpersonal psychotherapy for depressed adoles-cents. Arch. Gen. Psychiatry 56: 573–579.
7. FABA, G.A. et al. 1998. Prevention of recurrent depression with cognitive behavioraltherapy. Arch. Gen. Psychiatry 55: 816–820.
8. ROZANSKI, A., J.A. BLUMENTHAL & J. KAPLAN. 1999. Impact of psychological factorson the pathogenesis of cardiovascular disease and implications for therapy. Circula-tion 99: 2192–2217.
9. KIECOLT-GLASER, J.K. 1999. Norman Cousins Memorial Lecture. Stress, personal rela-tionships, and immune function: health implications. Brain Behav. Immun. 13: 61–72.
10. SALOVEY, P., A.J. ROTHMAN, J.B. DETWEILER & W.T. STEWARD. 2000. Emotional statesand physical health. Am. Psychol. 55: 110–121.
11. BAUM, A. & D.M. POSLUSZNY. 1999. Health psychology: mapping biobehavioral con-tributions to health and illness. Annu. Rev. Psychol. 50: 137–163.
12. FRICCHIONE, G. & G.B. STEFANO. 2005. Placebo neural systems: nitric oxide, mor-phine, and the dopamine brain reward and motivation circuitries. Med. Sci. Monit.11: 54–65.
13. SEYLE, H. 1973. The evolution of the stress concept. Am. Sci. 61: 692–699.14. ESCH, T. 2002. Health in stress: change in the stress concept and its significance for
prevention health and lifestyle. Gesundheitswesen 64: 73–81.15. TAMASHIRO, KL, M.M. NGUYEN & R.R. SAKAI. 2005. Social stress: from rodents to pri-
mates. Front. Neuroendocrinol. 26: 27–40.16. LEONARD, B. 2000. Stress, depression, and the activation of the immune system. World
J. Biol. Psychiatry 1: 17–25.17. HARBUZ, M.S. & S.L. LIGHTMAN. 1992. Stress and the hypothalamo–pituitary–adrenal
axis: acute, chronic, and immunological activation. J. Endocrinol. 134: 327–339.18. CHROUSOS, G.P. 1995. The hypothalamic–pituitary–adrenal axis and immune-mediated
inflammation. N. Engl. J. Med. 332: 1351–1362.19. BAILEY, M., H. ENGLER, J. HUNZEKER & J.F. SHERIDAN. 2003. The hypothalamic–pitu-
itary–adrenal axis and viral infection. Viral Immunol. 16: 141–157.20. BROADHEAD, W.E. et al. 1983. The epidemiologic evidence for a relationship between
social support and health. Am. J. Epidemiol. 117: 521–537.21. CHROUSOS, G.P. & P.W. GOLD. 1992. The concepts of stress and stress system disor-
ders. Overview of physical and behavioral homeostasis. J. Am. Med. Assoc. 267:1244–1252.
22. ROSENGREN, A. et al. 1993. Stressful life events, social support, and mortality in menborn in 1933. Br. Med. J. 307: 1102–1105.
23. MAUNDER, R.G. & J.J. HUNTER. 2001. Attachment and psychosomatic medicine: devel-opmental contributions to stress and disease. Psychosom. Med. 63: 556–567.
24. TAKKOUCHE, B., C. REGUEIRA & J.J. GESTAL-OTERO. 2001. A cohort study of stress andthe common cold. Epidemiology 12: 345–349.
25. AGUGLIA, E. et al. 2004. Stress in the caregivers of Alzheimer’s patients: an experi-mental investigation in Italy. Am. J. Alzheimers Dis. Other Demen. 19: 248–252.

504 ANNALS NEW YORK ACADEMY OF SCIENCES
26. KIECOLT-GLASER, J.K. et al. 1993. Negative behavior during marital conflict is associ-ated with immunological downregulation. Psychosom. Med. 55: 395–409.
27. CANTOR, C.H. et al. 1999. Australian suicide trends 1964–1997: youth and beyond?Med. J. Aust. 171: 137–141.
28. CALDWELL, T.M., A.F. JORM & K.B. DEAR. 2004. Suicide and mental health in rural,remote, and metropolitan areas in Australia. Med. J. Aust. 181: 10–14.
29. LESTER, D., P. WOOD, C. WILLIAMS & J. HAINES. 2004. Motives for suicide: a study ofAustralian suicide notes. Crisis 25: 33–34.
30. DE GROOT, M. et al. 1999. Glycaemic control and major depression in diabetes withtype 1 and type 2 diabetes mellitus. J. Psychosom. Res. 46: 425–435.
31. TSUTSUMI, A. 2005. Psychosocial factors and health: community and workplace study.J. Epidemiol. 15: 65–69.
32. ZORN, B.H. 1999. Urinary incontinence and depression. J. Urol. 162: 82–84.33. STEFFESN, B.C. et al. 1999. The effect of major depression on functional status in
patients with coronary artery disease. J. Am. Ger. Soc. 47: 319–322.34. SIVONOVA, M. et al. 2004. Oxidative stress in university students during examinations.
Stress 7: 183–188.35. CHIU, A., S.Y. CHON & A.B. KIMBALL. 2003. The response of skin disease to stress:
changes in the severity of acne vulgaris as affected by examination stress. Arch. Der-matol. 139: 897–900.
36. MÖLLER, J. et al. 2005. Work related stressful life events and the risk of myocardialinfarction. Case-control and case-crossover analyses within the Stockholm heart epi-demiology programme (SHEEP). J. Epidemiol. Comm. Health 59: 23–30.
37. WEATHERALL, M. 1999. Biofeedback or pelvic floor muscle exercises for female genu-ine stress incontinence: a meta analysis of trials identified in a systematic review. Br.J. Urol. Int. 83: 1015–1016.
38. STEIN, P.C. et al. 1999. Elevated urinary norepinephrine in interstitial cystitis. Urol. J.53: 1140–1143
39. DAVIS, L.L. et al. 2004. Biopsychological markers of distress in informal caregivers.Biol. Res. Nurs. 6: 90–99.
40. DE KLOET, E.R. 2004. Hormones and the stressed brain. Ann. N.Y. Acad. Sci. 1018: 1–15.
41. KISSANE, D.W. et al. 1998. Psychological morbidity and quality of life in Australianwomen with early-stage breast cancer: a cross-sectional survey. Med. J. Aust. 169:192–196.
42. REAVLEY, N., L. VITETTA, F. CORTIZO & A. SALI. 2004. A preliminary report of theeffect of psychosocial support on the psychological and physical wellbeing of a het-erogeneous group of cancer patients. Psycho-Oncology 13: 51.
43. YATES, B.C. 1995. The relationships among social support and short- and long-termrecovery outcomes in men with coronary heart disease. Res. Nurs. Health 18: 193–203.
44. FROST, M.H. et al. 2000. Long-term satisfaction and psychological and social functionfollowing bilateral prophylactic mastectomy. J. Am. Med. Assoc. 284: 319–324.
45. HALL, S.M. et al. 1998. Nortriptyline and cognitive behavioural therapy in the treat-ment of cigarette smoking. Arch. Gen. Psychiatry 55: 683–690.
46. MARCUS, B.H. et al. 1999. The efficacy of exercise as an aid for smoking cessation inwomen. Arch. Int. Med. 159: 1229–1234.
47. MYINT, P.K. et al. 2005. Relation between self-reported physical functional health andchronic disease mortality in men and women in the european prospective investiga-tion into cancer (EPIC-Norfolk): a prospective population study. Ann. Epidemiol.Epub ahead of print Jul. 6, 2005.
48. MATTSON, M.P. 2005. Energy intake, meal frequency, and health: a neurobiologicalperspective. Annu. Rev. Nutr. 25: 237–260.
49. CUMMINGS, J.A. & S.A. BINGHAM. 1998. Diet and the prevention of cancer. Br. Med. J.317: 1636–1640. Review.
50. WILLETT, W.C. 1999. Goals for nutrition in the year 2000. CA Cancer J. Clin. 49: 331–352.
51. WILLETT, W.C. 2000. Diet and cancer. Oncologist 5: 393–404.

505VITETTA et al.: MIND–BODY MEDICINE
52. PENDER, J.R. & W.J. PORIES. 2005. Epidemiology of obesity in the United States. Gas-troenterol. Clin. North Am. 34: 1–7.
53. TRICHOPOULOU, A. et al. 2005. Modified Mediterranean diet and survival: EPIC-elderlyprospective cohort study. Br. Med. J. 330: 991. Epub Apr 8, 2005.
54. PSALTOPOULOU, T. et al. 2004. Olive oil, the Mediterranean diet, and arterial bloodpressure: the Greek European prospective investigation into cancer and nutrition(EPIC) study. Am. J. Clin. Nutr. 80: 1012–1018.
55. TRICHOPOULOU, A., T. COSTACOU, C. BAMIA & D. TRICHOPOULOS. 2003. Adherence to aMediterranean diet and survival in a Greek population. N. Engl. J. Med. 348: 2599–2608.
56. LASHERRAS, C., S. FERNANDEZ & A.M. PATTERSON. 2000. Mediterranean diet and agewith respect to overall survival in institutionalized, nonsmoking elderly people. Am.J. Clin. Nutr. 71: 987–992.
57. ASCHERIO, A. 2002. Epidemiologic studies on dietary fats and coronary heart disease.Am. J. Med. 113: 9–12.
58. HAVEMAN-NIES, A. et al. 2002. Dietary quality and lifestyle factors in relation to 10-year mortality in older Europeans: the SENECA study. Am. J. Epidemiol. 156: 962–968.
59. SMITH, T.W. & L.C. GALLO. 2001. Personality traits as risk factors for physical illness.In Handbook of Health Psychology. A. Baum, T. Revenson & J. Singer, Eds.: 139–172. Lawrence Erlbaum. Hillsdale, NJ.
60. SMITH, T.W., K. GLAZER, J.M. RUIZ & L.C. GALLO. 2004. Hostility, anger, aggressive-ness, and coronary heart disease: an interpersonal perspective on personality, emo-tion, and health. J. Pers. 72: 1217–1270.
61. NAKAYA, N. et al. 2003. Personality and the risk of cancer. J. Natl. Cancer Inst. 95:799–795.
62. SMITH, A. & K. NICHOLSON. 2001. Psychosocial factors, respiratory viruses, and exac-erbation of asthma. Psychoneuroendocrinology 26: 411–420.
63. ASTIN, J.A. et al. 2003. Mind-body medicine: state of the science, implications forpractice. J. Am. Board Fam. Pract. 16: 131–147.
64. VAN TUBERGEN, A. & S. VAN DER LINDEN. 2002. A brief history of spa therapy. Ann.Rheum. Dis. 61: 273–275.
65. ESKANDARI, F., J.I. WEBSTER & E.M. STERNBERG. 2003. Neural immune pathways andtheir connection to inflammatory diseases. Arthritis Res. Ther. 5: 251–265.
All in-text references underlined in blue are linked to publications on ResearchGate, letting you access and read them immediately.