The anatomical base of unilateral external fixation in the upper limb
Upload
independentCategory
view
4download
0
RESEARCH PAPER
Mental health and satisfaction with life among upper limb amputees:a Norwegian population-based survey comparing adult acquired majorupper limb amputees with a control group
KRISTIN ØSTLIE1, PER MAGNUS2, OLA H. SKJELDAL3, BEATE GARFELT1 &
KRISTIAN TAMBS4
1Innlandet Hospital Trust, Department of Physical Medicine and Rehabilitation Ottestad, Jørgen Jensens vei, 2312,
Norway, 2Norwegian Institute of Public Health, Division of Epidemiology, Oslo, Norway, 3Innlandet Hospital Trust,
Department of Research, Brumunddal, Norway, and 4Norwegian Institute of Public Health, Division of Mental Health, Oslo,
Norway
Accepted November 2010
AbstractPurpose. To assess how upper limb amputation affects mental health and life satisfaction.Method. Cross-sectional study comparing the mental health and perceived satisfaction with life among adult acquired majorupper limb amputees in Norway with a control group drawn from the Norwegian general population. The scales used werethe Satisfaction With Life Scale (SWLS) and the Hopkins Symptom Check List 25-item (SCL-25). The groups werecompared using multiple linear regression analyses.Results. The amputees scored significantly lower on life satisfaction than the control group. A tendency to poorer mentalhealth in the amputee group was observed, but there was no clear evidence of such a difference. The amputation effect on lifesatisfaction seemed to be mediated mainly by changes in occupational status and by the occurrence of short- or long-termcomplications related to the amputation.Conclusions. Our findings imply that rehabilitation of upper limb amputees should emphasise facilitating return to work aswell as the prevention of short- and long-term complications, and that this will be of importance not only for the amputees’physical function, but for the maintenance of acceptable life satisfaction. Further studies on the effect of upper limbamputation on mental health are recommended.
Keywords: Amputees, upper limb, anxiety, depression, quality of life, social support
Introduction
Arms and hands are used for most activities of daily
living, and are also important for expression, com-
munication and affection [1,2]. Thus, loss of an
upper limb has an extensive effect on people’s lives,
resulting in major restrictions of function, sensation
and appearance [3]. According to Fitzpatrick [4], the
loss of a limb phenomenologically parallels the death
of a loved one, and it is known that both upper and
lower limb amputees frequently manifest emotional
reactions such as shock, grief, denial, anxiety and
depression [5]. Traumatic amputation may also cause
post-traumatic stress syndrome and other personality
and adjustment disorders [6]. Furthermore, limb loss
has been found to dramatically change a person’s
sense of body image and consequently self image, in
turn affecting the person’s satisfaction with life [1].
Knowledge about these mental and psychosocial
aspects of amputation is important if one is to
succeed with amputee rehabilitation.
In existing literature, there are several reports on
amputee mental health and psychosocial issues
following amputation, as well as specific articles on
the quality of life following lower limb amputation,
and on lower limb amputee mental health. Recent
Correspondence: Kristin Østlie, Innlandet Hospital Trust, Department of Physical Medicine and Rehabilitation Ottestad, Jørgen Jensens vei, 2312 Ottestad
Norway. E-mail: [email protected]
Disability and Rehabilitation, 2011; 33(17–18): 1594–1607
ISSN 0963-8288 print/ISSN 1464-5165 online ª 2011 Informa UK, Ltd.
DOI: 10.3109/09638288.2010.540293
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

reviews have been given by Desmond and
MacLachlan [7] and Horgan and MacLachlan [8].
Emotional aspects of amputation in children have
also been described [9,10], as well as psychiatric
aspects of replantation surgery [11]. Persons with
limb loss have been shown to have poor health-
related quality of life (HRQL) compared to other
illness groups, lower limb loss affecting HRQL more
than upper limb loss [12]. Regarding mental health,
there is inconclusive evidence regarding the long-
term association between amputation and increased
risk for depression, whereas research does not
suggest elevated long-term levels of anxiety among
amputees compared to the general population [7,8].
There are, however, considerable inconsistencies
and ambiguities in terms of both methodology and
sampling in the existing literature, severely limiting
generalisability [7]. Moreover, literature specifically
addressing upper limb amputee quality of life and
mental health is scarce. Some articles are published in
other languages than English: Spikowska analyses the
quality of life after upper limb amputation in Polish
[13], Engelhardt et al. [14] in German and Chevrier
et al. [15] describe psychosocial aspects of rehabilita-
tion in upper limb amputations in French. Other
publications are case studies [16], or address satisfac-
tion with prostheses and functional abilities [17,18]
or the treatment of post-traumatic stress disorder
[19]. One article discusses the team approach in
dealing with the psychosocial aspects of traumatic
upper limb loss [6]. A few recent studies using the
Hospital Anxiety and Depression Scale (HADS)
suggest rates of borderline or significant depression
scores between 18% and 28% and rates of borderline
or significant anxiety scores between 30% and 35% in
samples of upper limb amputees [20,21]. To the
authors’ knowledge, no study specifically comparing
upper limb amputee life satisfaction and mental
health with a control group has been performed.
Given the unique nature and functions of the hand
and the upper limb, the mental and psychosocial
effects of losing an upper limb is likely to be different
from those of lower limb loss. Furthermore, upper
limb amputees differ from lower limb amputees in
several important aspects such as mean age at
amputation, average number and pattern of co-
morbidities and cause of amputation. Upper limb
loss typically results from traumatic injury in
relatively young adults otherwise in good health,
whereas the majority of lower limb amputations are
performed secondary to peripheral vascular disease
in elderly adults commonly experiencing several
concurrent medical conditions [20,22,23]. Thus,
pooled knowledge on both groups or knowledge on
lower limb amputees alone may not be applicable on
upper limb amputees. The need for further informa-
tion is evident.
Purpose of study
The aim of this study was to assess how upper limb
amputation affects mental health and life satisfaction
by comparing the mental health and perceived life
satisfaction among adult acquired major upper limb
amputees in Norway with a control group drawn
from the Norwegian general population.
Method
Design and subjects
We performed a cross-sectional study. Inclusion of
amputees started 1 October 2006 and was termi-
nated 30 May 2008. The control group was
randomly drawn from the National Population
Register (DSP) on 3 November 2006. Inclusion
criteria for both groups were as follows: adult (�18
years of age at 1 October 2006, i.e. born 1 October
1988 or before), resident in Norway at the time of the
survey, and mastering spoken and written Norwe-
gian. An exclusion criterion was severely reduced
cognitive function or general condition (impairing
the ability to give the information called for in the
study). For the amputees, two extra inclusion criteria
were as follows: acquired upper limb loss (congenital
excluded) and level of amputation through the radio
carpal joint or proximal of this level (major ULA).
We identified eligible upper limb amputees
(ULAs) through a search of the databases of the
two companies in Norway that make upper limb
prostheses: Norwegian Technical Orthopaedics AS
(NTO AS) and Sophies Minde Orthopaedics AS
(SMO AS). Amputees not wearing a prosthesis
(‘non-users’) were searched for in the electronic
and manual medical records of three large Norwe-
gian hospitals: Oslo University Hospital Rikshospita-
let (Oslo), St. Olav’s Hospital (Trondheim) and
Haukeland University Hospital (Bergen). Lists of
potential participants from the different sources were
pooled and duplicates removed sequencially. The
final list was checked against the DSP to exclude
patients who had died or emigrated, and against the
inclusion and exclusion criteria listed above.
We identified 390 eligible amputees. 224 filled in
questionnaires. After imputation, 201 had valid
SWLS data and 158 had valid SCL data. 1002
controls were randomly drawn from the DSP. 962
were eligible according to our inclusion- and exclu-
sion criteria. 318 filled in questionnaires. After
imputation, 296 had valid SWLS data and 224 had
valid SCL data.
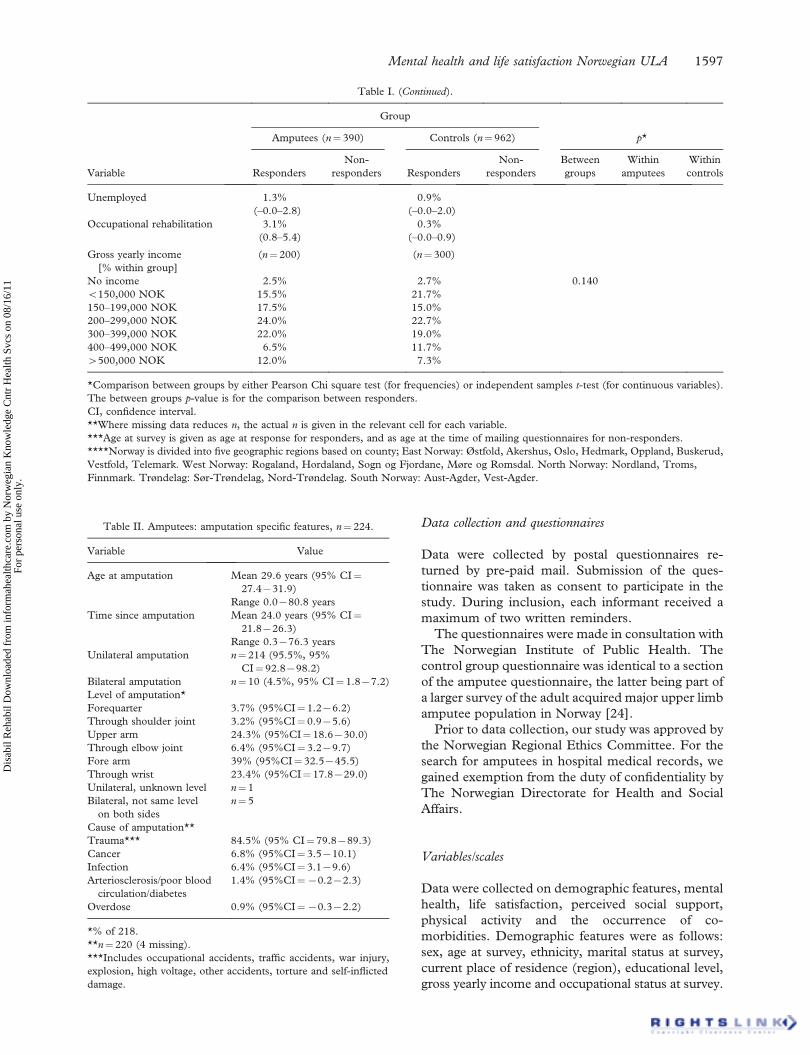
Demographic features of amputees and controls
are given in Table I. Amputation-specific features are
given in Table II.
Mental health and life satisfaction Norwegian ULA 1595
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

Table I. Demographic data.
Group
Amputees (n¼ 390) Controls (n¼962) p*
Variable Responders
Non-
responders Responders
Non-
responders
Between
groups
Within
amputees
Within
controls
n** 224 166 318 644
Sex [% male (95% CI)] 83.5%
(78.6–88.3)
84.3%
(78.8–89.9)
46.5%
(41.1–52.0)
45.5%
(41.7–49.3)
50.001 0.821 0.760
Age at survey***
[mean (95% CI)]
53.7 years
(51.6–55.8)
53.7 years
(50.9–56.4)
55.9 years
(53.6–58.1)
60.0 years
(58.1–61.8)
50.001 0.967 0.009
Place of residence (region)****
[number (% within group)]
East Norway 109
(48.7%)
83
(50.0%)
168
(52.8%)
313
(48.6%)
0.891 0.826 0.237
West Norway 54
(24.1%)
44
(26.5%)
72
(22.6%)
188
(29.2%)
North Norway 24
(10.7%)
16
(9.6%)
28
(8.8%)
56
(8.7%)
Trøndelag 20
(8.9%)
15
(9.0%)
27
(8.5%)
53
(8.2%)
South Norway 17
(7.6%)
8
(4.8%)
23
(7.2%)
34
(5.3%)
Ethnicity (native country)
[number (% within group)]
(n¼311)
Norway 202
(90.2%)
291
(93.6%)
0.150
Other 22
(9.8%)
20
(6.4%)
Marital status at survey
[% within group (95% CI)]
(n¼222) (n¼316)
Married, cohabitant or partner 70.7%
(64.7–76.7)
67.1%
(61.9–72.3)
50.001
Separated or divorced 7.2%
(3.8–10.6)
5.7%
(3.1–8.3)
Single 18.9%
(13.8–24.1)
13.6%
(9.8–17.4)
Widow/widower 3.2%
(0.9–5.5)
13.6%
(9.8–17.4)
Educational level
[% within group]
(n¼222) (n¼308)
No education 2.7% 4.2% 0.100
Primary school 20.7% 14.0%
Comprehensive school,
vocational training 29.7% 25.3%
Comprehensive school,
general education 10.4% 9.7%
College or university �4 years 19.8% 25.0%
College or university 44 years 12.6% 13.3%
Other education 4.1% 8.4%
Occupational status at survey
[% within group (95% CI)]
Working at home 1.8%
(0.1–3.5)
3.1%
(1.2–5.1)
50.001
Student 3.6%
(1.1–6.0)
5.0%
(2.6–7.4)
Employed 30.4%
(24.3–36.4)
44.0%
(38.6–49.5)
Self-employed 7.6%
(4.1–11.1)
4.7%
(2.4–7.0)
Disability pension 32.1%
(26.0–38.3)
4.7%
(2.4–7.0)
Retired 20.1%
(14.8–25.3)
37.1%
(31.8–42.4)
(continued)
1596 K. Østlie et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.
Data collection and questionnaires
Data were collected by postal questionnaires re-
turned by pre-paid mail. Submission of the ques-
tionnaire was taken as consent to participate in the
study. During inclusion, each informant received a
maximum of two written reminders.
The questionnaires were made in consultation with
The Norwegian Institute of Public Health. The
control group questionnaire was identical to a section
of the amputee questionnaire, the latter being part of
a larger survey of the adult acquired major upper limb
amputee population in Norway [24].
Prior to data collection, our study was approved by
the Norwegian Regional Ethics Committee. For the
search for amputees in hospital medical records, we
gained exemption from the duty of confidentiality by
The Norwegian Directorate for Health and Social
Affairs.
Variables/scales
Data were collected on demographic features, mental
health, life satisfaction, perceived social support,
physical activity and the occurrence of co-
morbidities. Demographic features were as follows:
sex, age at survey, ethnicity, marital status at survey,
current place of residence (region), educational level,
gross yearly income and occupational status at survey.
Table I. (Continued).
Group
Amputees (n¼ 390) Controls (n¼962) p*
Variable Responders
Non-
responders Responders
Non-
responders
Between
groups
Within
amputees
Within
controls
Unemployed 1.3%
(–0.0–2.8)
0.9%
(–0.0–2.0)
Occupational rehabilitation 3.1%
(0.8–5.4)
0.3%
(–0.0–0.9)
Gross yearly income
[% within group]
(n¼200) (n¼300)
No income 2.5% 2.7% 0.140
5150,000 NOK 15.5% 21.7%
150–199,000 NOK 17.5% 15.0%
200–299,000 NOK 24.0% 22.7%
300–399,000 NOK 22.0% 19.0%
400–499,000 NOK 6.5% 11.7%
4500,000 NOK 12.0% 7.3%
*Comparison between groups by either Pearson Chi square test (for frequencies) or independent samples t-test (for continuous variables).
The between groups p-value is for the comparison between responders.
CI, confidence interval.
**Where missing data reduces n, the actual n is given in the relevant cell for each variable.
***Age at survey is given as age at response for responders, and as age at the time of mailing questionnaires for non-responders.
****Norway is divided into five geographic regions based on county; East Norway: Østfold, Akershus, Oslo, Hedmark, Oppland, Buskerud,
Vestfold, Telemark. West Norway: Rogaland, Hordaland, Sogn og Fjordane, Møre og Romsdal. North Norway: Nordland, Troms,
Finnmark. Trøndelag: Sør-Trøndelag, Nord-Trøndelag. South Norway: Aust-Agder, Vest-Agder.
Table II. Amputees: amputation specific features, n¼224.
Variable Value
Age at amputation Mean 29.6 years (95% CI¼27.4731.9)
Range 0.0780.8 years
Time since amputation Mean 24.0 years (95% CI¼21.8726.3)
Range 0.3776.3 years
Unilateral amputation n¼ 214 (95.5%, 95%
CI¼ 92.8798.2)
Bilateral amputation n¼ 10 (4.5%, 95% CI¼ 1.877.2)
Level of amputation*
Forequarter 3.7% (95%CI¼ 1.276.2)
Through shoulder joint 3.2% (95%CI¼ 0.975.6)
Upper arm 24.3% (95%CI¼ 18.6730.0)
Through elbow joint 6.4% (95%CI¼ 3.279.7)
Fore arm 39% (95%CI¼ 32.5745.5)
Through wrist 23.4% (95%CI¼ 17.8729.0)
Unilateral, unknown level n¼ 1
Bilateral, not same level
on both sides
n¼ 5
Cause of amputation**
Trauma*** 84.5% (95% CI¼79.8789.3)
Cancer 6.8% (95%CI¼ 3.5710.1)
Infection 6.4% (95%CI¼ 3.179.6)
Arteriosclerosis/poor blood
circulation/diabetes
1.4% (95%CI¼70.272.3)
Overdose 0.9% (95%CI¼70.372.2)
*% of 218.
**n¼ 220 (4 missing).
***Includes occupational accidents, traffic accidents, war injury,
explosion, high voltage, other accidents, torture and self-inflicted
damage.
Mental health and life satisfaction Norwegian ULA 1597
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

Ethnicity was recorded as native country, Norway or
other. For marital status, the categories in the
questionnaire were: Married, cohabitant, partner,
separated, divorced, single, widow/widower. The
categories married, cohabitant and partner were
combined in the analyses, and so were the categories
separated and divorced. Educational level was re-
corded as: No education, primary school, comprehen-
sive school, vocational training, comprehensive school,
general education, college or university �4 years,
college or university 44 years, other education. In the
analyses, the category ‘other education’ was combined
with the category ‘primary school’. The categories for
the variables ‘Occupational status at survey’ and
‘Gross yearly income’ are displayed in Table I.
Mental health was assessed by the Hopkins
Symptom Check List 25-item (SCL-25), a 25-item
self-report symptom rating scale that measures
current anxiety and depression [25,26]. We also
obtained a report describing SCL-25 data from the
Statistics Norway population survey ‘Health in Nor-
way’. ‘Health in Norway’ describes the Norwegian
general population aged 16–79 years, and conven-
tionally divides the SCL-25 scores into three groups,
where scores 1.00–1.54 indicate good mental health,
scores 1.55–1.74 indicate a risk of mental illness and
scores �1.75 may be considered a high probability of
mental illness [27].
Satisfaction with life was assessed by the Satisfac-
tion With Life Scale (SWLS) [28–30]. The SWLS is
a 5-item measure asking respondents to rate their
agreement to statements such as ‘In most ways my
life is close to my ideal’ on a 7-point Likert scale. The
SWLS measures global life satisfaction, which can be
defined as ‘a global assessment of a person’s quality
of life according to his chosen criteria’. How satisfied
people are with their lives is based on a comparison
with a standard each individual sets for him or
herself, it is not externally imposed. The SWLS is
narrowly focussed on life satisfaction, not tapping
related constructs of subjective well-being such as
positive affect or loneliness [28].
Four yes/no questions assessed the extent of
support from the informants’ social network. Per-
ceived social support was estimated as a sum score
based on the number of yes-answers. The questions
were: ‘Have you in the last 14 days talked to (a)
Someone inside the family about joys and sorrows?
(b) Someone inside the family about health-related
matters? (c) Someone outside the family about joys
and sorrows? d) Someone outside the family about
health-related matters?’.
The informants were asked whether during the last
12 months they had been exercising on a regular
basis, more than 30 min each time and so intensely
that they were sweating. The alternative answers
were ‘Yes’ and ‘No’.
The informants gave information on the present
and/or past occurrence of the following diseases/
complaints: musculoskeletal pain, lower limb ampu-
tation and upper limb trauma other than amputation.
There was also a space for comments on this in the
questionnaire.
Data analysis
Data were processed using the Statistical Package for
the Social Sciences (SPSS1) version 14.0. For hypo-
thesis testing, the significance level was set at 0.05.
For SCL-25 data, missing data analyses were
performed, and missing values replaced by imputed
values calculated by EM (expectation-maximisation)
analyses for cases missing �10 of 25 answers. For
SWLS data, imputation based on EM analyses was
performed for cases missing �two of five answers.
The effect of upper limb amputation on the SCL-
25 and SWLS scores (between group differences) was
studied with multiple linear regression analyses. The
imputed SWLS- and SCL-scores were z-scaled before
the regression analyses. The SCL scores were
logarithm (ln) transformed in order to remove a
strong skewness of the distribution, and then z-scaled.
The variables age, educational level and perceived
social support showed nonsignificant non-linear ef-
fects and were entered in the analyses as continuous
variables. The variable gross yearly income showed
significant non-linear effects on the SWLS and on the
SCL depression scores and was included in the anal-
yses of all outcome variables as a categorical variable.
First, multiple linear regression was performed
with possible confounders in the model. Confoun-
ders included were as follows: sex, age, marital
status, birth country, place of residence, educational
level and the occurrence of leg amputation.
Second, possible mediator variables were included
in the model one at a time. Possible mediators
included were as follows: occupational status at
survey, gross yearly income last year before survey,
physical activity, social support, the occurrence of
upper limb trauma other than amputation and the
occurrence of musculoskeletal pain.
Finally, possible interaction effects between upper
limb amputation and the variables sex, age, marital
status, physical activity and perceived social support
were tested. New variables were computed as the
products between amputation and each of the other
variables. New regression analyses were run con-
secutively with all the covariates and one of the
product variables at a time.
To assess the representativeness of our control
group, we also compared the report describing SCL-
25 data from the Statistics Norway population survey
‘Health in Norway’ [27] with our data on the control
1598 K. Østlie et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

group responders. For completeness, our amputee
responder SCL-25 scores were also compared with
our control-group scores and with the Statistics
Norway survey scores, as a supplement to the
regression analyses described above.
Results
Response rates
In sum, we identified 390 eligible ULAs. 224
returned questionnaires (responders), yielding a
57.4% response rate. This amputee population is
described elsewhere [24].
From a list of 1002 randomly drawn control group
subjects, 962 were found eligible according to our
inclusion- and exclusion criteria. 318 returned ques-
tionnaires (responders), yielding a 33.1% response rate.
Demographic data
Demographic data for the whole sample of amputees
and controls are shown in Table I and described
below.
Demographic data: differences between responders and
non-responders. There were no significant differences
within the groups regarding gender distribution or
place of residence. Within the amputee group there
was no significant difference in mean age. The non-
responder controls, however, had a slightly higher
mean age than the responder controls. The mean
difference was 4.1 years (55.9 vs. 60.0 years).
Demographic data: between group differences: responders
only. There were significant differences between
amputees and controls regarding gender distribution
and age at survey. The number of males was
considerably larger in the amputee group, whereas
the control group had a slightly higher mean age at
survey than the amputees (mean difference 2.2
years). There were no significant differences regard-
ing place of residence or birth country. All Norwegian
regions were represented. The pattern of residence
was concurrent with the number of residents in each
region [31]. Most responders in both groups were
born in Norway. There were significantly more
widow/widowers in the control group. The amputees’
educational level and gross yearly income did not
differ significantly from that in the control group, but
there were significant differences in occupational
status at the time of the survey between amputees and
controls. A considerably larger proportion of ampu-
tees received disability pension, whereas the number
of employed controls exceeded that of employed
amputees. Furthermore, significantly more controls
than amputees were retired.
Other between group differences: responders only
The amputees had a significantly higher occurrence
of lower limb amputation and of upper limb trauma
other than amputation than the control group. The
occurrence of lower limb amputation in the amputee
group was 4.5%, in the control group 0.6%,
p¼ 0.003. The occurrence of upper limb trauma
other than amputation in the amputee group was
43.3%, in the control group 3.8%, p5 0.001. There
were no significant between group differences
regarding social-support score (p¼ 0.261), physical
activity (p¼ 0.820) or the occurrence of musculos-
keletal pain (p¼ 0.109). 50.9% of amputees reported
to be exercising regularly (controls 51.9%) and
43.3% of amputees reported musculoskeletal pain
(controls 36.5%). The average social-support score
among amputees was 2.03 (controls 2.18).
SCL-25: comparison with statistics Norway’s population
survey ‘Health in Norway’
SCL-25 scores in the Health in Norway sample, our
control responder group and our amputee responder
group were compared. There were no significant
differences between either of the groups in any of the
score categories. In the Health in Norway sample
(n¼ 6192), 10% scored �1.75 [27]. In our control
group (n¼ 224), 8.9% scored �1.75 (95% CI¼ 5.2–
12.7). The CI shows that the difference is not
significant at the 5% level, indicating that our control
group responders do not differ significantly from the
general population. In our amputee group (n¼ 158)
14.6% scored �1.75 (95% CI¼ 9.1–20.1). Although
the difference from the control group or the
population sample is not significant at the 5% level,
there is a non-significant trend towards higher scores
in the amputee group.
Missing data analyses
There were 29.5% missing or incomplete SCL data
after imputation. Because of the high percentage of
missing SCL data, the group with missing SCL data
was compared with the remaining sample regarding
sociodemographic and amputation specific features.
For the SWLS scores, 91.7% had valid data after
imputation, and missing data analyses were not
performed.
Looking at amputees and controls separately,
there were no significant differences between SCL
Mental health and life satisfaction Norwegian ULA 1599
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

responders and SCL non-responders regarding sex,
place of residence, native country, marital status,
gross yearly income, time since the amputation, level
of amputation or cause of amputation. There were
significant differences regarding age at survey,
educational level and occupational status at survey.
Details on these variables are shown in Table III.
Differences between amputees and controls in satisfaction
with life and mental health
SWLS. In sum, 33 amputees and 39 controls were
missing one or more SWLS answers. For 10
amputees and 17 controls imputation was performed,
leaving 201 amputees and 296 controls eligible for
SWLS analyses. Mean standardised SWLS score
(zSWLS) for amputees was 70.20 (95% CI¼70.35
to 70.05). Mean zSWLS for the control group was
0.14 (95% CI¼ 0.03–0.24). Controlling for age and
gender, there was still a significant difference between
amputees and controls, p5 0.001. The mean differ-
ence in zSWLS in this model was 70.381 (95%
CI¼70.574 to 70.188). Controlling for age,
gender, marital status, birth country, place of resid-
ence, educational level and the occurrence of leg
amputation, the mean difference between amputees
and controls in zSWLS was 70.333 (95%
CI¼70.488 to 70.104), p¼ 0.001. Detailed effects
in this model are shown in Table IV.
Introducing possible mediator variables in the
model one at a time (Table V), it appears that the
effect of upper limb amputation on life satisfaction is
mediated mainly by changes in occupational status
and by the occurrence of short- or long-term
complications noted by the amputees as ‘other upper
limb trauma’. Based on the amputees’ comments in
the questionnaire, ‘other upper limb trauma’ include
various stump complaints, various overuse com-
plaints on the non-amputated side and sequelae of
other traumas concurrent with the amputation such
as nerve damage affecting stump function, extensive
scarring and contra lateral finger amputations. The
effect seems to a lesser extent also to be mediated by
effect on gross yearly income, a variable strongly
correlated with present occupational status.
Including all confounder and mediator variables
simultaneously, the effect of group was in the
opposite of the expected direction and no longer
significant, B¼ 0.046, p¼ 0.687. No significant
interaction effects were detected.
SCL-25. In sum, 80 amputees and 112 controls were
missing one or more SCL-25 answers. For 14
Table III. SCL responders and SCL non-responders: significant differences.
Group
Amputee responders
(n¼224)
Control responders
(n¼318) p*
Variable SCLþ SCL7 SCLþ SCL7Within
amputees
Within
controls
n** 158 66 224 94
Age at survey [mean, in years] 52.5 56.8 52.5 63.9 0.063 50.001
Educational level [% within group] (n¼ 157) (n¼65) (n¼ 220) (n¼88)
No education 0.6% 7.7% 2.7% 8.0% 0.020 0.045
Primary school or other education 17.8% 27.7% 11.8% 19.3%
Comprehensive school, vocational training 30.6% 27.7% 24.5% 27.3%
Comprehensive school, general education 11.5% 7.7% 10.5% 8.0%
College or university �4 years 21.7% 15.4% 29.1% 14.8%
College or university 44 years 14.6% 7.7% 13.6% 12.5%
Other education 3.2% 6.2% 7.7% 10.2%
Occupational status at survey [% within group (95% CI)]
Working at home 1.9% 1.5% 2.7% 4.3% 0.068 0.001
Student 4.4% 1.5% 6.7% 1.1%
Employed 34.2% 21.2% 50.0% 29.8%
Self-employed 7.6% 7.6% 5.4% 3.2%
Disability pension 28.5% 40.9% 4.0% 6.4%
Retired 20.3% 19.7% 30.4% 53.2%
Unemployed 0% 4.5% 0.9% 1.1%
Occupational rehabilitation 3.2% 3.0% 0% 1.1%
SCLþ : SCL responders (after imputation) SCL7: SCL non-responders (missing or incomplete data).
*Comparison between groups by either Pearson Chi square test (for frequencies) or independent samples t-test (for continuous variables).
**Where missing data reduces n, the actual n is given in the relevant cell for each variable.
There were no significant differences detected for the variables sex, place of residence, birth country, marital status, gross yearly income,
time since amputation, level of amputation and cause of amputation.
1600 K. Østlie et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

amputees and 18 controls imputation was per-
formed, leaving 158 amputees and 224 controls
eligible for SCL-25 analyses.
SCL-25 anxiety score. Mean logarithm transformed
and z-scaled SCL anxiety score (zANX) for ampu-
tees was 0.040 (95% CI¼70.120 to 0.199). Mean
zANX for the control group was 70.028 (95%
CI¼70.158 to 0.102). Controlling for age and
gender, there was a significant difference between
amputees and controls, p¼ 0.040. The mean differ-
ence for zANX in this model was 0.226 (95%
CI¼ 0.01170.442). Controlling for age, gender,
marital status, birth country, place of residence,
educational level and the occurrence of leg amputa-
tion, the difference between amputees and controls
in zANX was not statistically significant, p¼ 0.177,
B¼ 0.148. Detailed results from this model are
shown in Table VI.
Introducing mediator variables one at a time in
the model (Table VII) to a greater or lesser degree
reduced the estimated B for group, suggesting
mediator effects. Including all confounder and
mediator variables simultaneously, the effect of
group remained nonsignificant, p¼ 0.201, and the
trend of the effect was in the opposite of the
expected direction, B¼70.153 (95% CI¼70.389
to 0.082). No significant interaction effects were
detected.
SCL-25 depression score. Mean logarithm transformed
and z-scaled SCL depression score (zDEP) for
amputees was 0.026 (95% CI¼70.135 to 0.186).
Mean zDEP score for the control group was 70.018
(95% CI¼70.148 to 0.112). Controlling for age
and gender, the difference between amputees and
controls was not statistically significant, p¼ 0.063,
B¼ 0.206 (95% CI¼70.011 to 0.423). Controlling
for the other confounders, the difference was clearly
not significant, p¼ 0.199, B¼ 0.143. Detailed results
from this model are shown in Table VI.
Introducing mediator variables one at a time in the
model (Table VII) to a greater or lesser degree
reduced estimated B for group, suggesting mediator
effects. Including all confounder and mediator
variables simultaneously, the trend of the effect, just
Table V. Effect of arm amputation on standardised SWLS score (zSWLS) when introducing possible mediator variables one at a time in the
model.
Mediator B for group (unstandardised) 95% CI for B p
None (model as in Table IV) 70.333 70.525 to 70.142 0.001
Occupational status at survey 70.116 70.319 to 0.086 0.260
Gross yearly income last year before survey 70.244 70.438 to 70.050 0.014
Physical activity (yes vs. no) 70.334 70.525 to 70.143 0.001
Social support 70.334 70.530 to 70.137 0.001
Occurrence of upper limb traumaother than amputation* 70.205 70.410 to 70.001 0.049
Musculoskeletal pain 70.304 70.495 to 70.112 0.002
*Many amputees noted in the questionnaires that by this they mean short- or long-term complications to the amputation such as stump
complaints and overuse complaints on the non-amputated side.
Table IV. Effects on standardised SWLS score (zSWLS), all confounders in the model.
Independent variable
B
(unstandardised) 95% CI for B Beta p
Group (amputee vs. control) 70.333 70.525 to 70.142 70.164 0.001
Gender (male vs. female) 0.037 70.158 to 0.231 0.018 0.709
Age at survey 0.003 70.003 to 0.008 0.051 0.323
Native country (other vs. Norway) 70.466 70.799 to 70.133 70.121 0.006
Place of residence:* West Norway 0.188 70.025 to 0.402 0.080 0.084
Place of residence: North Norway 70.098 70.389 to 0.193 70.030 0.508
Place of residence: Trøndelag 0.055 70.251 to 0.362 0.016 0.723
Place of residence: South Norway 0.268 70.073 to 0.609 0.069 0.124
Educational level 0.102 0.039 to 0.164 0.146 0.002
Occurrence of leg amputation 70.362 70.935 to 0.210 70.054 0.214
Marital status:** separated or divorced 70.493 70.844 to 70.142 70.121 0.006
Marital status: single 70.445 70.692 to 70.197 70.161 50.001
Marital status: Widow/widower 70.561 70.902 to 70.220 70.163 0.001
*Reference category: East Norway.
**Reference category: married, cohabitant or partner.
Mental health and life satisfaction Norwegian ULA 1601
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

Tab
leV
I.E
ffec
tso
nlo
gar
ith
mtr
ansf
orm
edan
dz-
scal
edS
CL
anxie
tysc
ore
(zA
NX
)an
dlo
gar
ith
mtr
ansf
orm
edan
dz-
scal
edS
CL
dep
ress
ion
sco
re(z
DE
P),
all
con
fou
nd
ers
inth
em
od
el.
Dep
end
ent
vari
able
zAN
XzD
EP
Ind
epen
den
tva
riab
le
B
(un
stan
dar
dis
ed)
95
%C
Ifo
rB
Bet
ap
B
(un
stan
dar
dis
ed)
95
%C
Ifo
rB
Bet
ap
Gro
up
(am
pu
tee
vs.
con
tro
l)0
.14
87
0.0
67
to0
.36
20
.07
30.1
77
0.1
43
70
.07
6to
0.3
62
0.0
71
0.1
99
Gen
der
(mal
evs
.fe
mal
e)7
0.3
66
70
.58
4to
70
.14
77
0.1
79
0.0
01
70
.36
27
0.5
85
to7
0.1
40
70
.17
80
.00
1
Age
atsu
rvey
70
.00
67
0.0
12
to0
.00
07
0.1
11
0.0
63
0.0
03
70
.00
4to
0.0
09
0.0
54
0.3
73
Nat
ive
cou
ntr
y(o
ther
vs.
No
rway
)0
.75
70
.36
7to
1.1
48
0.1
89
50.0
01
0.7
51
0.3
53
to1
.14
90
.18
95
0.0
01
Pla
ceof
resi
den
ce:*
Wes
tN
orw
ay7
0.3
01
70
.54
6to
70
.05
67
0.1
25
0.0
16
70
.11
07
0.3
60
to0
.13
97
0.0
46
0.3
86
Pla
ceof
resi
den
ce:
No
rth
No
rway
70
.26
87
0.6
36
to0
.09
97
0.0
72
0.1
52
70
.31
07
0.6
84
to0
.06
57
0.0
83
0.1
05
Pla
ceof
resi
den
ce:
Trø
nd
elag
70
.08
07
0.4
52
to0
.29
27
0.0
21
0.6
72
70
.08
67
0.4
65
to0
.29
37
0.0
23
0.6
56
Pla
ceof
resi
den
ce:
So
uth
No
rway
70
.30
47
0.6
66
to0
.05
87
0.0
83
0.0
99
70
.18
37
0.5
52
to0
.18
57
0.0
50
0.3
29
Ed
uca
tio
nal
leve
l7
0.1
31
70
.20
1to
70
.06
07
0.1
85
50.0
01
70
.07
87
0.1
50
to7
0.0
06
70
.11
10
.03
4
Occ
urr
ence
of
leg
amp
uta
tio
n0
.57
07
0.1
00
to1
.24
00
.08
30.0
95
0.2
14
70
.46
9to
0.8
96
0.0
31
0.5
38
Mar
ital
stat
us:
**
sep
arat
edo
rd
ivo
rced
0.2
36
70
.20
4to
0.6
75
0.0
52
0.2
93
0.1
36
70
.31
2to
0.5
84
0.0
30
0.5
50
Mar
ital
stat
us:
sin
gle
0.1
78
70
.10
3to
0.4
59
0.0
66
0.2
14
0.3
79
0.0
93
to0
.66
50
.14
10
.01
0
Mar
ital
stat
us:
wid
ow
/wid
ow
er0
.09
17
0.3
08
to0
.49
10
.02
60.6
52
0.2
00
70
.20
7to
0.6
06
0.0
57
0.3
35
*R
efer
ence
cate
go
ry:
Eas
tN
orw
ay.
**R
efer
ence
cate
go
ry:
mar
ried
,co
hab
itan
to
rp
artn
er.
1602 K. Østlie et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

like for the anxiety score, was in the opposite of the
expected direction, B¼70.160 (95% CI¼70.400
to 0.080), p¼ 0.190. No significant interaction
effects were detected.
Discussion
Main findings
In our material, a tendency to poorer mental health
in the amputee group was observed, but there was no
clear evidence of such a difference. However, the
amputees scored significantly lower on life satisfac-
tion than the control group. The effect on life
satisfaction seemed to be mediated mainly by
changes in occupational status and by the occurrence
of short- or long-term complications related to the
amputation such as stump complaints and overuse
complaints on the non-amputated side.
Strength and weaknesses
A relatively low response rate in both groups is a
weakness of our study. This may have led to selection
bias in our sample. However, Table I shows that
there were no large differences between responders
and non-responders. The percentage of missing data
was also high, especially for the SCL-data, even after
imputation. This may have led to information bias.
Comparing the groups, however, such a bias may not
have seriously affected the results, as long as the bias
has the same direction in both groups. Our missing
data analyses suggest that this is the case for the
majority of sociodemographic variables and for all
amputation specific variables compared. Further-
more, comparison to SCL-25 data from Statistics
Norway indicates that our control group responders
may be considered as representative of the Norwe-
gian general population.
However, the high proportion of missing data in
the SCL analyses has reduced the statistical power to
detect systematic differences between the groups.
The sample size with valid anxiety and depression
data permits mean differences higher than approxi-
mately 0.2 SD to be detected with 85% probability,
implying that moderate effects on mental health may
have been left undetected.
Differences between amputees and controls re-
garding the possible confounders sex, age and
marital status were controlled for in the multiple
regression analyses. We did not control for current
occupational status in the initial regression analyses,
because this variable was assumed to be a mediator
of the amputation effect. To the extent that occupa-
tional status was a cause, rather than a result of
amputation, the results from these analyses are not
fully controlled for. The same might be argued for
the other assumed mediators, though a causal link to
the amputation in these cases is considered more
unlikely. On the other hand, including educational
level as a confounder may have obscured a possible
mediator effect of this variable.
Strengths of the study include comparison to a
control group, use of standardised measures and
inclusion of possible mediators as well as the
population-based sample including amputees from
the entire country, and including both prosthetic
users and non-users.
Confounders and mediators: the rationale behind
classification of some variables
Educational level was considered a possible con-
founder as the risk of occupational accidents is
higher in ‘blue collar jobs’ than in ‘white collar jobs’.
Table VII. Effect of arm amputation on logarithm transformed and z-scaled SCL anxiety score (zANX) and logarithm transformed and z-
scaled SCL depression score (zDEP) when introducing possible mediator variables one at a time in the model.
Mediator
Dependent variable
zANX zDEP
B for group
(unstandardised) 95% CI for B p
B for group
(unstandardised) 95% CI for B p
None (model as in Table VI) 0.148 70.067 to 0.362 0.177 0.143 70.076 to 0.362 0.199
Occupational status at survey 70.061 70.284 to 0.162 0.591 70.044 70.270 to 0.183 0.706
Gross yearly income last year before survey 0.116 70.101 to 0.332 0.295 0.090 70.126 to 0.305 0.414
Physical activity (yes vs. no) 0.139 70.072 to 0.350 0.196 0.135 70.081 to 0.350 0.219
Social support 0.140 70.077 to 0.357 0.205 0.160 70.060 to 0.380 0.154
Upper limb trauma other than amputation* 0.012 70.218 to 0.241 0.920 70.029 70.261 to 0.203 0.806
Musculoskeletal pain 0.117 70.094 to 0.327 0.276 0.123 70.094 to 0.340 0.267
*Many amputees noted in the questionnaires that by this they mean short- or long-term complications to the amputation such as stump
complaints and overuse complaints on the non-amputated side.
Mental health and life satisfaction Norwegian ULA 1603
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

The possible mediator effect of this variable –
amputees may undertake further education to qualify
for less physically demanding jobs – was considered
to be of less importance. In our material, there was a
strong correlation between arm amputation and leg
amputation, 10 of totally 12 leg amputees were also
arm amputees. Leg amputation is known to affect
mental health and life satisfaction [32], and we
therefore included the occurrence of leg amputation
in the analyses as a possible confounder.
Present occupational status is likely to be a
mediator of the effect of arm amputation, as upper
limb loss in many cases leads to either occupational
rehabilitation or disability pension [24]. Present
occupational status was not considered a confoun-
der, as would indeed be the case for occupational
status at the time of the amputation, occupational
accidents accounting for many arm amputations.
However, amputation in our material on average
occurred 24 years ago. Gross yearly income may be
associated with present occupational status and was
therefore also considered a possible mediator of
amputation effect. Physical activity was analysed as a
possible mediator bearing in mind that arm ampu-
tees often exercise as a part of their rehabilitation,
especially amputees with musculoskeletal pain or
difficulties with their prostheses (factors with a
potentially negative impact on life satisfaction).
Social support was considered a possible mediator
rather than a confounder, possibly affected by the
amputation but not likely to be linked to the risk of
amputation. The variable ‘upper limb trauma other
than amputation’ was considered a possible mediator
variable as many amputees noted in their question-
naires that this was directly related to the amputation
either as trauma caused by the same incident as the
amputation or as a short- or long-term complications
to the amputation.
Earlier findings
Existing literature is characterised by considerable
inconsistencies regarding methodology and sam-
pling. In many cases, pooling of upper- and lower-
limb amputees limit generalisability. In a review of
the literature, Desmond and MacLachlan concluded
that whereas research to date does not suggest
elevated levels of anxiety among people with
amputations compared to the general public or
compared to patients with chronic musculoskeletal
pain, there is little consensus regarding whether
amputees face an elevated risk of depressive symp-
toms. According to this review, the prevalence of
depressive symptoms among amputees in some
studies has been reported between 18% and 28% –
higher than the general population, but similar to the
35% prevalence reported for individuals with a
variety of physical disabilities, and to a 24%
prevalence found among individuals with chronic
pain. Other studies have failed to show increased
prevalence of depression compared to the general
population. The Medical Outcomes Study Short
Form (SF-36) scores have in several studies on lower
limb amputees been found to be poorer than in the
general population, with most prominent differences
in physical functioning, role limitation due to
physical health and bodily pain dimensions. How-
ever, mental health was in many cases not found to
be significantly reduced compared to age- and
gender-matched norm groups [7].
Studies specifically addressing upper limb ampu-
tee mental health are scarce. The findings of recent
studies are mainly in accordance with Desmond and
MacLachlan’s review. In a cross-sectional study of
British male amputees with traumatic upper limb
loss, Desmond found a prevalence of clinically
significant anxiety symptoms of 34.6%, broadly
consistent with the general population rates. The
prevalence of depressive symptomatology in this
study, using the HADS to define caseness, was
28.3%, almost three times higher than rates reported
in a non-clinical sample broadly representative of
UK adults [20]. All amputees in Desmond’s sample
had lost their limb serving in Her Majesty’s Forces or
Auxiliary Forces. The prevalence of anxiety in
Desmond’s sample was of the same magnitude as
found by Datta, who studied British patients with
proximal upper limb deficiency (acquired and con-
genital). The prevalence of depression in Datta’s
sample – also using the HADS – was however
considerably lower (18.3%) [21]. Datta’s sample was
recruited from a subregional prosthetic and amputee
rehabilitation unit. Neither compared their sample to
a control group.
In 2003, Demet et al. studied health-related
quality of life (HRQL) in French upper- and lower-
limb amputees using the Nottingham Health Profile
(NHP). The study population consisted of war
victims as well as self-employed people living in the
eastern area of France. The NHP indicated a
relatively poor HRQL for persons with limb loss
compared to other illness groups, mostly for physical
disability, pain and energy level scores. Upper limb
amputees had a better HRQL than lower limb
amputees [12]. In 2008, Saradjian et al. performed
a qualitative study of 11 male upper limb amputees,
looking at psychosocial adjustment, physical/func-
tional adaptation, coping style and the use of
prostheses. The areas of people’s lives found to be
most affected by the amputation were occupational
status, social relationships and activities of daily
living [1]. This has also been noted elsewhere
[17,18].
1604 K. Østlie et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

Relating our findings to the literature
Regarding anxiety, our findings are undoubtedly in
accordance with the literature. Regarding depression,
our findings are indicative, but not statistically signi-
ficant 7 illustrative of Desmond and MacLachlan’s
review [7]. Our data indicate a somewhat lower
occurrence of depression among upper limb ampu-
tees than found by Desmond [20] and Datta [21],
though the observed tendency to poorer mental
health in our amputee group may be considered
consistent with their findings. Neither of these
samples was population-based or compared to a
control group. On the other hand, our findings of
relatively good mental health among upper limb
amputees may be considered consistent with what
was noted by Saradijan et al., where the amputees
were found to display ‘a positive and accepting
attitude, exhibiting an engagement in life and an
openness and embracement of new experiences
within their rehabilitation and life in general. As a
result, participants’ lives appeared minimally re-
stricted, with all describing the fulfilment of person-
ally meaningful roles, activities and relationships’ [1].
Our findings on life satisfaction are consistent with
earlier literature. Whereas the NHP used by Demet
et al. [12] measures quality of life as a sum of defined
categories including pain and physical disability, the
SWLS used in our study measures global life
satisfaction, which leaves the respondent free to
weight various domains and feeling states in what-
ever way he or she chooses [28]. Our statistical
analyses however indicate that the effect of upper
limb amputation in our sample to a large extent is
mediated by impact on occupational status and by
the occurrence of short- or long-term complications
related to the amputation (noted as ‘other upper limb
trauma’). This is in accordance with earlier studies
demonstrating severe consequences in terms of
employment [17,33] and with earlier studies using
both the SF-36 and the NHP, where reduced
physical functioning, pain and role limitation due
to physical health problems have been noted as the
most affected domains of HRQL among amputees
[7,12]. It is interesting that though the effect of upper
limb amputation on mental health in our material
was nonsignificant, the mediators significantly redu-
cing B for anxiety and depression were the same
variables that showed significant mediator effects on
life satisfaction.
The correlation between occupational status and
mental health and life satisfaction is well known, also
from population studies not including amputees
[34,35]. An important effect of falling out of the
labour market might be a feeling of not coping,
known to affect life satisfaction negatively [1,30].
This was demonstrated in Saradijan’s qualitative
study, emphasising the importance of positive coping
among upper limb amputees. High self-worth was
related to successful functional and social adjustment
[1]. The overall differences in occupational status in
our material probably reflect effects of the amputa-
tion, with a high occurrence of disability pension in
the amputee group and a high occurrence of
employed/self-employed and retired (as opposed to
disability pension) in the control group.
The correlation between pain and mental health
and/or quality of life in amputees is well established
[5,36,37], and has also been described in the general
population [38]. In a recent cross-sectional study of
104 upper limb amputees, Hanley et al. [36] found
that self-reported quality of life measured with the
SWLS was significantly lower for individuals experi-
encing each type of: Phantom limb pain, residual
limb pain, back-, neck- and non-amputated-limb
pain compared to those without any pain. A high
occurrence of pain in and problems with the
remaining arm in upper limb amputees has also
been noted [39]. We therefore tested for possible
mediator effects of the occurrence of musculoskeletal
pain in addition to the occurrence of ‘other upper
limb trauma’. Musculoskeletal pain had surprisingly
little effect measured as B-change, probably due to
the many amputees coding amputation-related pain
and problems as ‘other upper limb trauma’ rather
than musculoskeletal pain. This may in part be
explained by the phrasing of the question: ‘muscu-
loskeletal pain (for instance long-lasting back pain)’,
which may have caused the respondents to state the
occurrence of arm or shoulder pain under ‘other
upper limb trauma’ instead.
There is accumulating evidence of the associations
between physical activity and mental health and well-
being [40,41]. However, the lack of experimental
evidence for a causal link between physical activity
and improved psychological well-being has been
noted [41]. Although habitual exercise may improve
psychological well-being, a strong sense of well-being
may also be necessary to comply with a habitual and
intensive exercise programme. However, an increas-
ing number of outcome studies provide evidence for
the efficacy of exercise interventions for clinical
samples. For instance, a meta-analysis examining
data from 36 studies linking physical activity to well-
being in older adults without clinical disorders
showed a small but significant effect of exercise on
well-being [41], and a recent review concluded that
exercise can be a powerful intervention for clinical
depression [40]. In our material, physical activity did
not have a significant mediator effect on the SWLS
or the SCL scores and it was not a significant
interaction variable. Interpreting these results, one
should remember that the low statistical power in our
study does not permit other than quite strong
Mental health and life satisfaction Norwegian ULA 1605
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

interaction effects to be detected. Also, the relation-
ship between exercise and mental health in amputees
might be more complex than in the samples of
clinical depression and healthy older adults referred
above.
Social support is known to be associated with
mental health and well-being [1,42]. Studying social
support in lower limb amputees, Williams et al. [42]
found that the Multidimensional Scale of Perceived
Social Support (MSPSS) was an important predictor
of pain interference, life satisfaction and mobility,
controlling for demographic and amputation-related
factors. In the light of these findings, perceived social
support was analysed both as a possible mediator and
as a possible effect modificator in our material. No
significant between-group differences in social sup-
port were detected, and no significant effects were
found in the regression analyses. This may be
explained by different scales of measurement in
Williams et al.’s and our study, and also by our lack
of statistical power as discussed above.
Conclusions
Knowledge of the mental and psychosocial aspects of
upper limb amputation is important if one is to
succeed with amputee rehabilitation.
According to our data, upper limb loss signifi-
cantly lowers life satisfaction compared to a control
group from the general population. The effect on life
satisfaction appears mainly to be mediated by
reduced ability to work and by the occurrence of
post-amputation arm complications. A tendency to
poorer mental health in the amputee group was
observed, but there was no clear evidence of such a
difference. Further studies are recommended.
Emphasising measures that facilitate return to
work in upper limb amputee rehabilitation is likely
to be of importance for the amputees’ well-being as
well as for their physical function. Furthermore,
focus in amputee rehabilitation should be kept on
preventing complications shown to have an impact
on life satisfaction, such as stump and overuse pain
and prosthetic- and musculoskeletal dysfunction.
Within amputee group factors that may affect
mental health and quality of life such as amputation
level, cause of amputation, time since amputation,
the use of and satisfaction with prostheses, rehabili-
tation experiences and details on pain and physical
function will be addressed in subsequent papers.
Acknowledgements
We thank Espen Røysamb, Professor Dr. Psychol.
for his advices regarding choice of scales for the
assessment of mental health and life satisfaction. We
also thank Nina Gunnes, statistician PhD, for her
statistical advices.
Declaration of interest
The authors report no declarations of interest. Our
work was funded in part by Innlandet Hospital Trust
and in part by The Norwegian Extra Foundation for
Health and Rehabilitation.
References
1. Saradjian A, Thompson AR, Datta D. The experience of men
using an upper limb prosthesis following amputation: positive
coping and minimizing feeling different. Disabil Rehabil
2008;30:871–883.
2. Roeschlein RA, Domholdt E. Factors related to successful
upper extremity prosthetic use. Prosthet Orthot Int 1989;
13:14–18.
3. Kejlaa GH. The social and economic outcome after upper
limb amputation. Prosthet Orthot Int 1992;16:25–31.
4. Fitzpatrick MC. The psychologic assessment and psychosocial
recovery of the patient with an amputation. [Review]. Clin
Orthop Relat Res 1999;361:98–107.
5. Gallagher P, Maclachlan M. Psychological adjustment and
coping in adults with prosthetic limbs. Behav Med 1999;25:
117–124.
6. Mendelson RL, Burech JG, Polack EP, Kappel DA. The
psychological impact of traumatic amputations. A team
approach: physician, therapist, and psychologist. Hand Clin
1986;2:577–583.
7. Desmond DM, Maclachlan M. Psychosocial perspectives on
postamputation rehabilitation: a review of disease, trauma,
and war related literature. Crit Rev Phys Rehabil Med
2004;16:77–93.
8. Horgan O, Maclachlan M. Psychosocial adjustment to
lower-limb amputation: a review. Disabil Rehabil 2004;26:
837–850.
9. Turgay A, Sonuvar B. Emotional aspects of arm or leg
amputation in children. Can J Psychiatr-Revue Canadienne de
Psychiatrie 1983;28:294–297.
10. Varni JW, Setoguchi Y, Rappaport LR, Talbot D. Effects of
stress, social support, and self-esteem on depression in
children with limb deficiencies. Arch Phys Med Rehabil
1991;72:1053–1058.
11. Schweitzer I, Rosenbaum MB. Psychiatric aspects of replan-
tation surgery. Gen Hospital Psychiatry 1982;4:271–279.
12. Demet K, Martinet N, Guillemin F, Paysant J, Andre JM.
Health related quality of life and related factors in 539 persons
with amputation of upper and lower limb. Disabil Rehabil
2003;25:480–486.
13. Spikowska A, Stryla W. [Analysis of quality of life in persons
after arm amputations]. [Polish]. Chirurgia Narzadow Ruchu
i Ortopedia Polska 2000;65:665–673.
14. Engelhardt TO, Jeschke J, Piza-Katzer H. [About the self-
reported quality of life after amputation of the hand in patients
with upper extremity tumors]. [German]. Handchirurgie,
Mikrochirurgie, Plastische Chirurgie 2008;40:23–30.
15. Chevrier JM, Gingras G, Lemieux R, Mongeau M, Susset V,
Voyer R. [Psychosocial aspect of rehabilitation in upper arm
amputations.]. [French]. Union Medicale du Canada 1956;
85:1245–1250.
1606 K. Østlie et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.

16. Paterson MC, Burke FD. Psychosocial consequences of upper
limb injury. J Hand Surg Br 1995;20:776–781.
17. Davidson J. A survey of the satisfaction of upper limb
amputees with their prostheses, their lifestyles, and their
abilities. J Hand Ther 2002;15:62–70.
18. Jones LE, Davidson JH. The long-term outcome of upper
limb amputees treated at a rehabilitation centre in Sydney,
Australia. Disabil Rehabil 1995;17:437–442.
19. Grunert BK, Matloub HS, Sanger JR, Yousif NJ. Treatment
of posttraumatic stress disorder after work-related hand
trauma. J Hand Surg Am 1990;15:511–515.
20. Desmond DM. Coping, affective distress, and psychosocial
adjustment among people with traumatic upper limb amputa-
tions. J Psychosom Res 2007;62:15–21.
21. Datta D, Selvarajah K, Davey N. Functional outcome of
patients with proximal upper limb deficiency – acquired and
congenital. Clin Rehabil 2004;18:172–177.
22. Durance JP, O’Shea BJ. Upper limb amputees: a clinic profile.
Int Disabil Stud 1988;10:68–72.
23. Schoppen T, Boonstra A, Groothoff JW, de V, Goeken LN,
Eisma WH. Physical, mental, and social predictors of
functional outcome in unilateral lower-limb amputees. Arch
Phys Med Rehabil 2003;84:803–811.
24. Østlie K, Skjeldal OH, Garfelt B, Magnus P. Adult acquired
major upper limb amputation in Norway: prevalence, demo-
graphic features and amputation specific features. A popula-
tion based survey. Disabil Rehabil, in press.
25. Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L.
The Hopkins Symptom Checklist (HSCL). A measure of
primary symptom dimensions. [Review] [76 refs]. Modern
Problems of Pharmacopsychiatry 1974;7:79–110.
26. Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L.
The Hopkins Symptom Checklist (HSCL): a self-report
symptom inventory. Behav Sci 2001;19:1–15.
27. Statistics Norway. [Health in Norway. II. Health and disease.]
[Norwegian]. 1998. pp. 49–62. http://www.ssb.no/emner/03/
00/sa41/helseogsyk.pdf. Last accessed March 2010.
28. Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction
with life scale. J Pers Assess 1985;49:71–75.
29. Pavot W, Diener E. Review of the satisfaction with life scale.
PsycholAssess1993;5:164–172.
30. Diener E. Understanding scores on the satisfaction with life
scale. http://www.psych.uiuc.edu/*ediener/Documents/Under
standing%20SWLS%20Scores.pdf. Last accessed March 2010.
31. [Norwegian regions] [Norwegian] [Internet]. http://no.
wikipedia.org/wiki/Distrikter_i_Norge#Landsdelstabell. Last
accessed February 2010.
32. Pezzin LE, Dillingham TR, Mackenzie EJ. Rehabilitation and
the long-term outcomes of persons with trauma-related
amputations. Arch Phys Med Rehabil 2000;81:292–300.
33. Whyte AS, Carroll LJ. A preliminary examination of the
relationship between employment, pain and disability in an
amputee population. Disabil Rehabil 2002;24:462–470.
34. Kessler RC, Berglund P, Demler O, Jin R, Koretz D,
Merikangas KR, Rush AJ, Walters EE, Wang PS, National
C. The epidemiology of major depressive disorder: results
from the National Comorbidity Survey Replication (NCS-R).
JAMA 2003;289:3095–3105.
35. Kessler RC, Zhao S, Blazer DG, Swartz M. Prevalence,
correlates, and course of minor depression and major
depression in the National Comorbidity Survey. J Affective
Disord 1997;45:19–30.
36. Hanley MA, Ehde DM, Jensen M, Czerniecki J, Smith DG,
Robinson LR. Chronic pain associated with upper-limb loss.
Am J Phys Med Rehabil 2009;88:742–751.
37. Ephraim PL, Wegener ST, Mackenzie EJ, Dillingham TR,
Pezzin LE. Phantom pain, residual limb pain, and back pain in
amputees: results of a national survey. Arch Phys Med Rehabil
2005;86:1910–1919.
38. Penny KI, Purves AM, Smith BH, Chambers WA, Smith
WC. Relationship between the chronic pain grade and
measures of physical, social and psychological well-being.
Pain 1999;79:275–279.
39. Jones LE, Davidson JH. Save that arm: a study of problems in
the remaining arm of unilateral upper limb amputees. Prosthet
Orthot Int 1999;23:55–58.
40. Stathopoulou G, Powers MB, Berry AC, Smits JAJ, Otto
MW. Exercise interventions for mental health: a quantitative
and qualitative review. Clin Psychol: Sci Pract 2006;13:179–
193.
41. Netz Y, Wu M-J, Becker BJ, Tenenbaum G. Physical
activity and psychological well-being in advanced age: a
meta-analysis of intervention studies. Psychol Aging
2005;20:272–284.
42. Williams RM, Ehde DM, Smith DG, Czerniecki JM,
Hoffman AJ, Robinson LR. A two-year longitudinal study of
social support following amputation. Disabil Rehabil
2004;26:862–874.
Mental health and life satisfaction Norwegian ULA 1607
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
weg
ian
Kno
wle
dge
Cnt
r H
ealth
Svc
s on
08/
16/1
1Fo
r pe
rson
al u
se o
nly.
Copyright © 2022 FDOKUMEN