Effects of training on upper limb function after cervical spinal cord injury: a systematic review
12
Clinical Rehabilitation 2015, Vol. 29(1) 3–13 © The Author(s) 2014 Reprints and permissions: sagepub.co.uk/journalsPermissions.nav DOI: 10.1177/0269215514536411 cre.sagepub.com CLINICAL REHABILITATION Introduction Over the last few decades, various interventions have evolved in an attempt to improve arm and hand function in individuals with spinal cord injury. 1–3 Loss of arm and hand function is one of the most devastating consequences of tetraplegia and it has been shown to be the priority of recovery for this population. Even a small improvement in Effects of training on upper limb function after cervical spinal cord injury: a systematic review Xiao Lu 1 , Camilla R Battistuzzo 2 , Maryam Zoghi 2 and Mary P Galea 2 Abstract Objective: To summarize the evidence for the effectiveness of exercise training in promoting recovery of upper extremity function after cervical spinal cord injury. Data sources: Medline, Cochrane, CINAHL, EMBASE and PEDro were used to search the literature. Review methods: Two reviewers independently selected and summarized the included studies. Methodological quality of the selected articles was scored using the Downs and Black checklist. Results: A total of 16 studies were included, representing a total of 426 participants. Overall, the internal validity and reporting of the studies was fair to good, while power and external validity were poor. Interventions included exercise therapy, electrical stimulation, functional electrical stimulation, robotic training and repetitive transcranial magnetic stimulation. Most of the studies reported improvements in muscle strength, arm and hand function, activity of daily living or quality of life after intervention. Conclusions: Training including exercise therapy, electrical stimulation, functional electrical stimulation of the upper limb following cervical spinal cord injury leads to improvements in muscle strength, upper limb function and activity of daily living or quality of life. Further research is needed into the effects of repetitive transcranial magnetic stimulation and robotic training on upper limb function. Keywords Spinal cord injury, systematic review, training, upper limb Received: 24 March 2013; accepted: 27 April 2014 1 Department of Rehabilitation, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China 2 Physiotherapy Department, The University of Melbourne, Parkville, Victoria 3010, Australia Corresponding author: Xiao Lu, Department of Rehabilitation, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China. Email: [email protected] 536411CRE 0 0 10.1177/0269215514536411Clinical RehabilitationLu et al. research-article 2014 Article
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Effects of training on upper limb function after cervical spinal cord injury: a systematic review

Clinical Rehabilitation2015, Vol. 29(1) 3 –13© The Author(s) 2014Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/0269215514536411cre.sagepub.com
CLINICALREHABILITATION
IntroductionOver the last few decades, various interventions have evolved in an attempt to improve arm and hand function in individuals with spinal cord injury.1–3 Loss of arm and hand function is one of the most devastating consequences of tetraplegia and it has been shown to be the priority of recovery for this population. Even a small improvement in
Effects of training on upper limb function after cervical spinal cord injury: a systematic review
Xiao Lu1, Camilla R Battistuzzo2, Maryam Zoghi2 and Mary P Galea2
AbstractObjective: To summarize the evidence for the effectiveness of exercise training in promoting recovery of upper extremity function after cervical spinal cord injury.Data sources: Medline, Cochrane, CINAHL, EMBASE and PEDro were used to search the literature.Review methods: Two reviewers independently selected and summarized the included studies. Methodological quality of the selected articles was scored using the Downs and Black checklist.Results: A total of 16 studies were included, representing a total of 426 participants. Overall, the internal validity and reporting of the studies was fair to good, while power and external validity were poor. Interventions included exercise therapy, electrical stimulation, functional electrical stimulation, robotic training and repetitive transcranial magnetic stimulation. Most of the studies reported improvements in muscle strength, arm and hand function, activity of daily living or quality of life after intervention.Conclusions: Training including exercise therapy, electrical stimulation, functional electrical stimulation of the upper limb following cervical spinal cord injury leads to improvements in muscle strength, upper limb function and activity of daily living or quality of life. Further research is needed into the effects of repetitive transcranial magnetic stimulation and robotic training on upper limb function.
KeywordsSpinal cord injury, systematic review, training, upper limb
Received: 24 March 2013; accepted: 27 April 2014
1 Department of Rehabilitation, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
2 Physiotherapy Department, The University of Melbourne, Parkville, Victoria 3010, Australia
Corresponding author:Xiao Lu, Department of Rehabilitation, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China. Email: [email protected]
536411 CRE0010.1177/0269215514536411Clinical RehabilitationLu et al.research-article2014
Article

4 Clinical Rehabilitation 29(1)
arm and hand function may lead to increased inde-pendence in daily activities, improving independ-ence and quality of life.4,5
Interventions, such as tendon transfer surgery, implanted neuroprostheses and re-training of arm and hand function, are currently used to improve upper limb function.6,7 Among these methods, re-training is the most common as it is non-invasive and relatively inexpensive. However, studies assessing the effects of training on upper limb or hand function following cervical spinal cord injury are scarce and results are somewhat diverse.8 Identifying the value and efficacy of these inter-ventions can help clinicians and also future clinical trials, and there are few existing systematic reviews of this topic. Thus, the aim of this review was to summarize the evidence for the effectiveness of training aimed at promoting recovery of upper limb/hand function from clinical trials involving people with cervical spinal cord injury.
MethodsA systematic literature search of studies published from January 1950 to November 2013 was con-ducted using Medline, Web of Science, EMBASE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Physiotherapy Evidence Database (PEDro) databases. In the search strat-egy, MeSH-terms and text words for participants (tetraplegia, quadriplegia, spinal cord injury, spinal cord lesion), interventions (exercise, strength, robotic, repetitive transcranial magnetic stimula-tion, electric* stimulation, task specific training, virtual reality, biofeedback) and outcomes (hand function, arm function, upper limb function, upper extremity function) were combined (Appendix I). Reference lists of all selected trials were also screened to identify additional studies.
Randomized controlled trials, quasi-randomized controlled trials, crossover and controlled trials published in peer-reviewed journals were included if they compared therapy intervention to a control group in patients with complete or incomplete cer-vical spinal cord injury and hand function or upper limb function were an outcome measured. The fol-lowing therapy interventions were included in this
study: robotic training, repetitive transcranial mag-netic stimulation, functional electrical stimulation, electrical stimulation, resistance training task- specific repetitive functional training, virtual real-ity and biofeedback. Case studies, reviews, book chapters and letters were excluded, as well as studies using surgery, orthoses, splints, implants or drugs. All searches were limited to English language articles.
Two investigators (XL and CRB) independently evaluated the title and abstract of indentified stud-ies according to selection criteria. Thereafter, the full-text articles of all eligible studies were obtained and evaluated for in/exclusion by the two investi-gators. In case of disagreement, consensus was reached by discussion between all the authors.
The following data were extracted from each included study: (1) patient characteristics (group, number of participants, time since injury, American Spinal Injury Association (ASIA) grade, level of injury, age); (2) intervention(s) implemented in the study (type of therapy, intensity, duration and fre-quency); (3) outcome measures (strength, hand or arm function, activities of daily living and quality of life); and (4) conclusions. For studies that included paraplegic and tetraplegic patients, only data about tetraplegic participants were extracted.
A 27-item checklist developed by Downs and Black was used to assess the methodological qual-ity of included studies. This checklist contains items for reporting (10 items), external validity (three items), internal validity (bias and confound-ing 13 items) and power (one items). Answers are scored 0 or 1, except for one single item on power, which was scored 0 to 5. The total maximum score was therefore 31.9
Agreement between investigators on inclusion of studies was assessed using the Kappa statistic and percentage agreement (SPSS software version 17.0, Chicago, Illinois, USA). Findings were sum-marized using descriptive statistics.
ResultsA total of 15 eligible studies were identified after searching the databases. After full text screening, one article was excluded because no intervention

Lu et al. 5
was provided and two further articles were added after checking the references of relevant publica-tions, resulting in 16 studies being included in this systematic review10–25 (Figure 1). A 99% (Kappa 0.73) inter-rater agreement was found for the study selection.
Out of 16 included studies, 13 (81%) were ran-domized controlled trials, two (12%) were cohort studies and one (6%) was a cross-over study. The results of quality assessment of these studies are listed in Table 1. Overall, scores for reporting and
internal validity, which includes bias and con-founding, were good, however the scores for exter-nal validity and power were poor. Five studies included blinded outcome measures (Table 1).
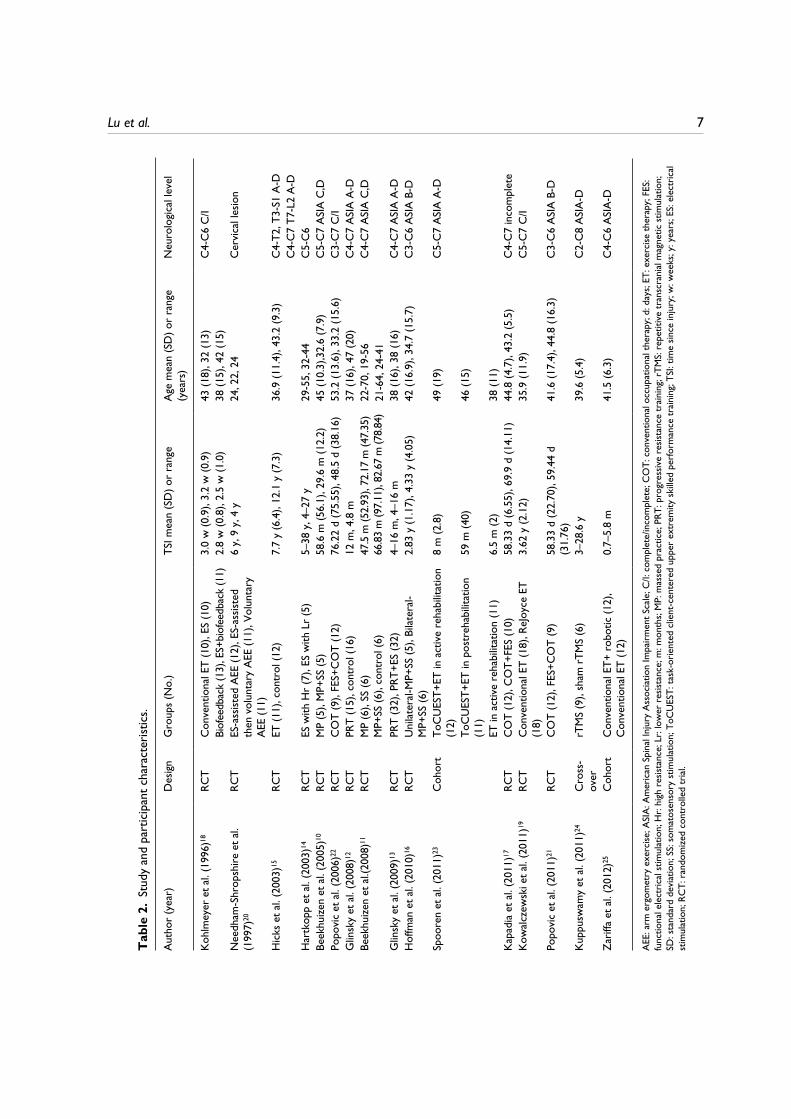
The sizes of the experimental and control groups were comparable in the selected studies ranging from five to 32 participants in each group.10–25 There was a wide range of time between injury of participants included (2.5 weeks to 28.5 years). The ASIA classification ranging from grades A to D (Table 2).
Figure 1. Flowchart of screened, excluded and analyzed articles.

6 Clinical Rehabilitation 29(1)
Table 1. Methodological quality assessment of included studies.
Number of studiesmedian (quartile range)
Reporting (10 items) 8 (2)External validity (3 items) 2 (2)Bias (7 items) 6 (1)Confounding (6 items) 3 (3)Power (1 item) 0 (1)
In terms of the type of therapy investigated, the effects of aerobic ergometry, resistance training, massed practice training, task-oriented training, somatosensory stimulation, electrical stimulation and functional electrical stimulation were studied in 14 studies.10–23 The two most recent published studies24–25 focused on the effect of more advanced technology, such as robotic training and repetitive transcranial magnetic stimulation. The length of the training programs ranged from two weeks to nine months, with the majority (56%) lasting between 6–8 weeks (Table 3).
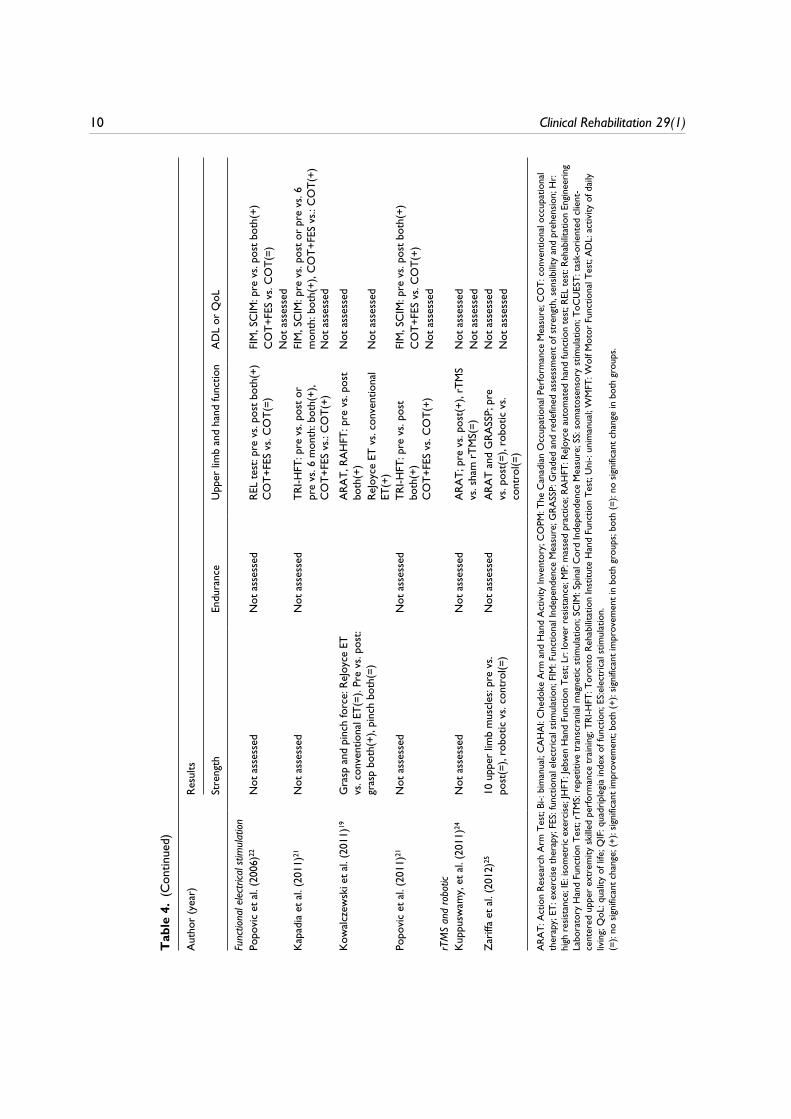
Six studies focused on the effect of exercise ther-apy10–12,15,16,23 (Table 4). The overall results of exer-cise therapy on muscle strength and upper limb/hand function seemed positive. Three studies12,15,23 observed the impact of exercise therapy on activities of daily living or quality of life. Only one study15 assessed quality of life and reported positive results. A positive change in activities of daily living meas-ured by the Quadriplegia Index of Function and the Functional Independence Measure was reported by one study,23 whereas no change was observed in activities of daily living when assessed using the Canadian Occupational Performance Measure.12
Four studies investigating the effect of electrical stimulation13,14,18,20 focused on the change in upper limb muscle strength. Most studies13,14,18 measured change in wrist extensor strength and showed signifi-cant improvement after electrical stimulation (ES) therapy. None of these four studies reported changes in upper limb function and only one study18 evalu-ated self-feeding abilities, but showed no positive results (Table 4).
All four studies investigating functional electri-cal stimulation17,19,21,22 showed positive results on
upper limb function. Among them two studies17,21 showed that compared with conventional therapy alone, conventional therapy combined with func-tional electrical stimulation was more effective in improving upper limb function, while one study22 showed no extra benefit. One of the four studies19 showed a significant increase in grasp force after functional electrical stimulation combined with exercise therapy, but there was no improvement of pinch force. A combination of functional electrical stimulation and conventional therapy resulted in significant improvement in activities of daily living17,19,21and the gains were maintained at six months follow-up.17
Robotic training combined with conventional therapy had no significant effect on muscle strength and functional task performance in the patients with partial hand function.25 Compared with sham stimulation, repetitive transcranial magnetic stimu-lation for five days increased upper extremity func-tion assessed by the Action Research Arm Test, but that was not significantly different from control group24 (Table 4).
DiscussionIn general, the results of this systematic review demonstrate that there are a limited number of studies investigating effects of training on arm and hand function in people with cervical spinal cord injury. The studies included in this review had a wide range of functional levels of participants, training, methodology and outcome parameters. Interestingly, these studies revealed that improve-ment in arm and hand muscle strength and function was possible with training in both the acute and chronic phases.
According to the checklist developed by Down and Black,9 studies included in this systematic review showed fair to good results for reporting and internal validity, but external validity and power was poor. Most studies did not include a sample size calculation and the sample sizes were small, which impacted on the power of the studies. The limited sample sizes might be explained by several factors. First, cervical spinal cord injury have low incidence. Second, patients with cervical
Lu et al. 7T
able
2.
Stud
y an
d pa
rtic
ipan
t cha
ract
erist
ics.
Aut
hor
(yea
r)D
esig
nG
roup
s (N
o.)
TSI m
ean
(SD
) or
rang
eA
ge m
ean
(SD
) or
rang
e (y
ears
)N
euro
logi
cal l
evel
Koh
lmey
er e
t al.
(199
6)18
RCT
Con
vent
iona
l ET
(10)
, ES
(10)
3.0
w (0
.9),
3.2
w (0
.9)
43 (1
8), 3
2 (1
3)C
4-C
6 C
/I
Biof
eedb
ack
(13)
, ES+
biof
eedb
ack
(11)
2.8
w (0
.8),
2.5
w (1
.0)
38 (1
5), 4
2 (1
5)
Nee
dham
-Shr
opsh
ire
et a
l. (1
997)
20RC
TES
-ass
isted
AEE
(12)
, ES-
assis
ted
then
vol
unta
ry A
EE (1
1), V
olun
tary
A
EE (1
1)
6 y,
9 y
, 4 y
24, 2
2, 2
4C
ervi
cal l
esio
n
Hic
ks e
t al.
(200
3)15
RCT
ET (1
1), c
ontr
ol (1
2)7.
7 y
(6.4
), 12
.1 y
(7.3
)36
.9 (1
1.4)
, 43.
2 (9
.3)
C4-
T2, T
3-S1
A-D
C
4-C
7 T7
-L2
A-D
Har
tkop
p et
al.
(200
3)14
RCT
ES w
ith H
r (7
), ES
with
Lr
(5)
5–38
y, 4
–27
y29
-55,
32-
44C
5-C
6Be
ekhu
izen
et a
l. (2
005)
10RC
TM
P (5
), M
P+SS
(5)
58.6
m (5
6.1)
, 29.
6 m
(12.
2)45
(10.
3),3
2.6
(7.9
)C
5-C
7 A
SIA
C,D
Popo
vic
et a
l. (2
006)
22RC
TC
OT
(9),
FES+
CO
T (1
2)76
.22
d (7
5.55
), 48
.5 d
(38.
16)
53.2
(13.
6), 3
3.2
(15.
6)C
3-C
7 C
/IG
linsk
y et
al.
(200
8)12
RCT
PRT
(15)
, con
trol
(16)
12 m
, 4.8
m37
(16)
, 47
(20)
C4-
C7
ASI
A A
-DBe
ekhu
izen
et a
l.(20
08)1
1 RC
TM
P (6
), SS
(6)
MP+
SS (6
), co
ntro
l (6)
47.5
m (5
2.93
), 72
.17
m (4
7.35
)66
.83
m (9
7.11
), 82
.67
m (7
8.84
)22
-70,
19-
56C
4-C
7 A
SIA
C,D
21-6
4, 2
4-41
G
linsk
y et
al.
(200
9)13
RCT
PRT
(32)
, PRT
+ES
(32)
4–16
m, 4
–16
m38
(16)
, 38
(16)
C4-
C7
ASI
A A
-DH
offm
an e
t al.
(201
0)16
RCT
Uni
late
ral-M
P+SS
(5),
Bila
tera
l-M
P+SS
(6)
2.83
y (1
.17)
, 4.3
3 y
(4.0
5)42
(16.
9), 3
4.7
(15.
7)C
3-C
6 A
SIA
B-D
Spoo
ren
et a
l. (2
011)
23
Coh
ort
ToC
UES
T+ET
in a
ctiv
e re
habi
litat
ion
(12)
8 m
(2.8
)49
(19)
C5-
C7
ASI
A A
-D
ToC
UES
T+ET
in p
ostr
ehab
ilita
tion
(11)
59 m
(40)
46 (1
5)
ET in
act
ive
reha
bilit
atio
n (1
1)6.
5 m
(2)
38 (1
1)K
apad
ia e
t al.
(201
1)17
RCT
CO
T (1
2), C
OT+
FES
(10)
58.3
3 d
(6.5
5), 6
9.9
d (1
4.11
)44
.8 (4
.7),
43.2
(5.5
)C
4-C
7 in
com
plet
eK
owal
czew
ski e
t al.
(201
1)19
RCT
Con
vent
iona
l ET
(18)
, ReJ
oyce
ET
(18)
3.62
y (2
.12)
35.9
(11.
9)C
5-C
7 C
/I
Popo
vic
et a
l. (2
011)
21RC
TC
OT
(12)
, FES
+CO
T (9
)58
.33
d (2
2.70
), 59
.44
d (3
1.76
)41
.6 (1
7.4)
, 44.
8 (1
6.3)
C3-
C6
ASI
A B
-D
Kup
pusw
amy
et a
l. (2
011)
24C
ross
-ov
errT
MS
(9),
sham
rTM
S (6
)3–
28.6
y39
.6 (5
.4)
C2-
C8
ASI
A-D
Zar
iffa
et a
l. (2
012)
25C
ohor
tC
onve
ntio
nal E
T+ r
obot
ic (1
2),
Con
vent
iona
l ET
(12)
0.7–
5.8
m41
.5 (6
.3)
C4-
C6
ASI
A-D
AEE
: arm
erg
omet
ry e
xerc
ise; A
SIA
: Am
eric
an S
pina
l Inj
ury
Ass
ocia
tion
Impa
irm
ent S
cale
; C/I:
com
plet
e/in
com
plet
e; C
OT:
con
vent
iona
l occ
upat
iona
l the
rapy
; d: d
ays;
ET: e
xerc
ise th
erap
y; F
ES:
func
tiona
l ele
ctri
cal s
timul
atio
n; H
r: h
igh
resis
tanc
e; L
r: lo
wer
res
istan
ce; m
: mon
ths;
MP:
mas
sed
prac
tice;
PRT
: pro
gres
sive
resis
tanc
e tr
aini
ng; r
TMS:
rep
etiti
ve tr
ansc
rani
al m
agne
tic s
timul
atio
n;
SD: s
tand
ard
devi
atio
n; S
S: s
omat
osen
sory
stim
ulat
ion;
ToC
UES
T: ta
sk-o
rien
ted
clie
nt-c
ente
red
uppe
r ex
trem
ity s
kille
d pe
rfor
man
ce tr
aini
ng; T
SI: t
ime
since
inju
ry; w
: wee
ks; y
: yea
rs; E
S: e
lect
rica
l st
imul
atio
n; R
CT:
ran
dom
ized
con
trol
led
tria
l.

8 Clinical Rehabilitation 29(1)
Tab
le 3
. Tr
aini
ng c
hara
cter
istic
s of
incl
uded
stu
dies
.
Aut
hor
(yea
r)Tr
aini
ng fr
eque
ncy/
dura
tion
Type
of e
xerc
ise th
erap
y
Koh
lmey
er e
t al.
(199
6)18
20 m
in/d
, 5/w
, 5–6
wC
onve
ntio
nal t
reat
men
t: pa
ssiv
e RO
M, s
tren
gthe
ning
of a
vaila
ble
mus
cles
by
exer
cise
and
func
tiona
l tra
inin
g of
teno
desis
gra
sp. E
S an
d EM
G b
iofe
edba
ck o
n w
rist
ext
enso
r.N
eedh
am-S
hrop
shir
e et
al.
(199
7)20
20 m
in/d
, 3/w
, 8 w
Volu
ntar
y ar
m e
rgom
etry
trai
ning
. Neu
rom
uscu
lar
stim
ulat
ion-
assis
ted
arm
erg
omet
ry tr
aini
ngH
icks
et a
l. (2
003)
1590
–120
min
/d, 2
/w, 9
mA
erob
ic tr
aini
ng (a
rm e
rgom
etry
, 70%
of H
R m
ax.)
and
resis
tanc
e ci
rcui
t tra
inin
g (7
0%–8
0% o
f 1RM
)H
artk
opp
et a
l. (2
003)
1430
min
/d, 5
/w, 1
2 w
Elec
tric
al s
timul
atio
n on
Hr
30-H
z st
imul
atio
n ag
ains
t max
imum
load
El
ectr
ical
stim
ulat
ion
on L
r 15
-Hz
stim
ulat
ion
agai
nst 5
0% m
axim
um
load
Beek
huiz
en e
t al.
(200
5, 2
008)
10,1
112
0 m
in/d
, 5/w
, 3 w
Mas
sed
prac
tice:
con
tinuo
us r
epet
ition
s of
task
s: gr
oss
uppe
r ex
trem
ity
mov
emen
t, gr
ip, g
rip
with
rot
atio
n, p
inch
and
pin
ch w
ith r
otat
ion.
So
mat
osen
sory
stim
ulat
ion:
Med
ian
nerv
e st
imul
atio
n at
wri
stPo
povi
c et
al.
(200
6)22
45 m
in/d
, 5/w
, 12
wC
onve
ntio
nal o
ccup
atio
nal t
hera
py: m
uscl
e fa
cilit
atio
n ex
erci
ses,
task
-spe
cific
trai
ning
; str
engt
heni
ng a
nd s
tret
chin
g ex
erci
ses;
elec
tric
al
stim
ulat
ion,
AD
L tr
aini
ng. F
ES-a
ssist
ed r
each
ing
and
gras
ping
Glin
sky
et a
l. (2
008)
123
sets
of 1
0RM
3/w
, 8 w
Prog
ress
ive
resis
tanc
e ex
erci
se p
rogr
am fo
r w
rist
flex
ors
or e
xten
sors
Glin
sky
et a
l. (2
009)
136
sets
of 1
0 re
petit
ion
max
imum
3/w
,8 w
Prog
ress
ive
resis
tanc
e ex
erci
se p
rogr
am fo
r w
rist
flex
ors
or e
xten
sors
El
ectr
ical
stim
ulat
ion
Hof
fman
et a
l. (2
010)
1612
0 m
in/d
, 5/w
, 3 w
Uni
man
ual o
r bi
man
ual m
asse
d pr
actic
e pl
us s
omat
osen
sory
stim
ulat
ion
(as
per
Beek
huiz
en e
t al.
2005
)10
Spoo
ren
et a
l. (2
011)
2390
min
/d, 3
/w, 8
wTa
sk-o
rien
ted
clie
nt-c
ente
red
uppe
r ex
trem
ity s
kille
d pe
rfor
man
ce
trai
ning
mod
ule
Kap
adia
et a
l. (2
011)
1760
min
/d, 5
/w, 8
wC
onve
ntio
nal t
hera
py: s
tren
gthe
ning
and
str
etch
ing
exer
cise
s an
d A
DL
prac
tice.
FE
S: p
erfo
rmin
g A
DL
assis
ted
by e
lect
rica
l stim
ulat
ion
Kow
alcz
ewsk
i et a
l. (2
011)
1960
min
/d, 5
/w, 6
wC
onve
ntio
nal e
xerc
ise th
erap
y: 2
0 m
in s
tren
gth
trai
ning
, 20
min
ac
cura
cy tr
aini
ng, 2
0 m
in e
lect
rica
l stim
ulat
ion;
FES
-ass
isted
exe
rcise
on
the
ReJo
yce
wor
ksta
tion.
Popo
vic
et a
l. (2
011)
2112
0 m
in/d
, 5/w
, 8 w
As
per
Popo
vic
et a
l. (2
006)
Kup
pusw
amy,
et a
l. (2
011)
2415
min
/d, 5
d, a
nd c
ross
-ov
erSt
imul
atio
n:5H
z as
2s
trai
ns s
epar
ated
by
8s 8
0% o
f the
act
ive
mot
or
thre
shol
d,Z
ariff
a et
al.
(201
2)25
60 m
in/d
, 3–5
/w, 6
wC
onve
ntio
nal t
hera
py: s
tren
gthe
ning
and
str
etch
ing
exer
cise
s an
d A
DL
prac
tice,
rob
otic
:Arm
eo S
prin
g
d: d
ay(s
); FE
S: fu
nctio
nal e
lect
rica
l stim
ulat
ion;
Hr:
hig
h re
sista
nce;
Lr:
low
er r
esist
ance
; m: m
onth
s; m
in: m
inut
e(s)
; w: w
eeks
; RO
M: r
ange
of m
otio
n; E
S: e
lect
rica
l stim
ula-
tion;
EM
G: e
lect
rom
yogr
aphy
; AD
L: a
ctiv
ity o
f dai
ly li
ving
; RM
: rep
etiti
on m
axim
um.

Lu et al. 9T
able
4.
Out
com
e pa
ram
eter
s of
incl
uded
stu
dies
.
Aut
hor
(yea
r)Re
sults
Stre
ngth
Endu
ranc
eU
pper
lim
b an
d ha
nd fu
nctio
nA
DL
or Q
oL
Exer
cise
ther
apy
Hic
ks e
t al.
(200
3)15
IE
of c
hest
, bic
eps,
ante
rior
del
toid
pr
e vs
. pos
t(+)
Arm
erg
omet
ry
perf
orm
ance
pre
vs.
post
(+)
Not
ass
esse
dQ
oLET
vs.
cont
rol(+
)N
ot a
sses
sed
Beek
huiz
en e
t al.
(200
5)10
M
axim
al p
inch
gri
p fo
rce
: MP+
SS(+
)N
ot a
sses
sed
WM
FT: M
P+SS
(+)
Not
ass
esse
dJH
FT: M
P+SS
(+),
MP(
+)N
ot a
sses
sed
Glin
sky
et a
l. (2
008)
12IE
of w
rist
ext
enso
rET
vs.
cont
rol(=
)Fa
tigue
res
istan
ce o
f w
rist
ext
enso
r: E
T vs
. con
trol
(=)
Not
ass
esse
dC
OPM
: ET
vs. c
ontr
o(=)
Not
ass
esse
d
Beek
huiz
en e
t al.
(200
8)11
M
axim
al p
inch
gri
p fo
rce
: M
P+SS
(+),
SS(+
)N
ot a
sses
sed
WM
FT: M
P+SS
(+),
SS(+
)N
ot a
sses
sed
JHFT
: MP+
SS(+
), M
P(+)
, SS
(+)
Not
ass
esse
d
Hof
fman
et a
l. (2
010)
16
pinc
h gr
ip s
tren
gth
Bi-M
P+SS
(=),
Uni
-MP+
SS(=
)N
ot a
sses
sed
JHFT
, CA
HA
I: Bi
-MP+
SS(+
), U
ni-M
P+SS
(+)
Not
ass
esse
d
Not
ass
esse
dSp
oore
n et
al.
(201
1)23
N
ot a
sses
sed
Not
ass
esse
dVa
n Li
esho
ut T
est:
pre
vs.
post
or
pre
vs. 3
mon
th: (
+),
ToC
UES
T vs
. sta
ndar
d(=)
QIF
, FIM
: pre
vs.
post
or
pre
vs. 3
m
onth
(+),
ToC
UES
T vs
. sta
ndar
d(=)
, C
OPM
: pre
vs.
post
or
pre
vs. 3
mon
th(+
)N
ot a
sses
sed
Elec
trica
l stim
ulat
ion
Koh
lmey
er e
t al.
(199
6)18
W
rist
ext
enso
r, d
elto
id a
nd b
icep
s: am
ong
4 gr
oups
(=),
pre
vs. p
ost(
+)
(4 g
roup
s to
geth
er)
Not
ass
esse
dN
ot a
sses
sed
Self-
feed
ing
abili
ties:
amon
g fo
ur g
roup
s (=
). Pr
e vs
. pos
t(+)
(fou
r gr
oups
to
geth
er)
Not
ass
esse
dN
eedh
am e
t al.
(199
7)20
Tr
icep
s m
uscl
e gr
ades
ES+v
olun
tary
vs.
volu
ntar
y(+)
Not
ass
esse
dN
ot a
sses
sed
Not
ass
esse
dN
ot a
sses
sed
Har
tkop
p et
al.
(200
3)14
St
reng
th o
f wri
st e
xten
sors
Hr(
+), L
r(=)
Fatig
ue r
esist
ance
of
wri
st e
xten
sor:
H
r(+)
, Lr(
+)
Not
ass
esse
dN
ot a
sses
sed
Not
ass
esse
d
Glin
sky
et a
l. (2
009)
13
W
rist
ext
enso
r IE
: Pre
vs.
post
bo
th(+
), ES
+ET
vs. E
T(=)
Fatig
ue r
esist
ance
: pr
e vs
. pos
t bot
h(=)
, ES
+ E
T vs
. ET(
=)
Not
ass
esse
dN
ot a
sses
sed
Not
ass
esse
d
(Con
tinue
d)
10 Clinical Rehabilitation 29(1)
Aut
hor
(yea
r)Re
sults
Stre
ngth
Endu
ranc
eU
pper
lim
b an
d ha
nd fu
nctio
nA
DL
or Q
oL
Func
tiona
l ele
ctric
al s
timul
atio
nPo
povi
c et
al.
(200
6)22
N
ot a
sses
sed
Not
ass
esse
dRE
L te
st: p
re v
s. po
st b
oth(
+)C
OT+
FES
vs. C
OT(
=)FI
M, S
CIM
: pre
vs.
post
bot
h(+)
CO
T+FE
S vs
. CO
T(=)
Not
ass
esse
dK
apad
ia e
t al.
(201
1)21
N
ot a
sses
sed
Not
ass
esse
dTR
I-HFT
: pre
vs.
post
or
pre
vs. 6
mon
th: b
oth(
+),
CO
T+FE
S vs
.: C
OT(
+)
FIM
, SC
IM: p
re v
s. po
st o
r pr
e vs
. 6
mon
th: b
oth(
+), C
OT+
FES
vs.:
CO
T(+)
Not
ass
esse
d
Kow
alcz
ewsk
i et a
l. (2
011)
19
G
rasp
and
pin
ch fo
rce:
ReJ
oyce
ET
vs. c
onve
ntio
nal E
T(=)
. Pre
vs.
post
: gr
asp
both
(+),
pinc
h bo
th(=
)
ARA
T, R
AH
FT: p
re v
s. po
st
both
(+)
Not
ass
esse
d
ReJo
yce
ET v
s. co
nven
tiona
l ET
(+)
Not
ass
esse
d
Popo
vic
et a
l. (2
011)
21
Not
ass
esse
dN
ot a
sses
sed
TRI-H
FT: p
re v
s. po
st
both
(+)
CO
T+FE
S vs
. CO
T(+)
FIM
, SC
IM: p
re v
s. po
st b
oth(
+)C
OT+
FES
vs. C
OT(
+)N
ot a
sses
sed
rTM
S an
d ro
botic
Kup
pusw
amy,
et a
l. (2
011)
24
Not
ass
esse
dN
ot a
sses
sed
ARA
T; p
re v
s. po
st(+
), rT
MS
vs. s
ham
rTM
S(=)
Not
ass
esse
dN
ot a
sses
sed
Zar
iffa
et a
l. (2
012)
25
10
upp
er li
mb
mus
cles
: pre
vs.
post
(=),
robo
tic v
s. co
ntro
l(=)
Not
ass
esse
dA
RAT
and
GRA
SSP;
pre
vs
. pos
t(=)
, rob
otic
vs.
cont
rol(=
)
Not
ass
esse
dN
ot a
sses
sed
ARA
T: A
ctio
n Re
sear
ch A
rm T
est;
Bi-:
bim
anua
l; C
AH
AI:
Che
doke
Arm
and
Han
d A
ctiv
ity In
vent
ory;
CO
PM: T
he C
anad
ian
Occ
upat
iona
l Per
form
ance
Mea
sure
; CO
T: c
onve
ntio
nal o
ccup
atio
nal
ther
apy;
ET:
exe
rcise
ther
apy;
FES
: fun
ctio
nal e
lect
rica
l stim
ulat
ion;
FIM
: Fun
ctio
nal I
ndep
ende
nce
Mea
sure
; GRA
SSP:
Gra
ded
and
rede
fined
ass
essm
ent o
f str
engt
h, s
ensib
ility
and
pre
hens
ion;
Hr:
hi
gh r
esist
ance
; IE:
isom
etric
exe
rcise
; JH
FT: J
ebse
n H
and
Func
tion
Test
; Lr:
low
er r
esist
ance
; MP:
mas
sed
prac
tice;
RA
HFT
: ReJ
oyce
aut
omat
ed h
and
func
tion
test
; REL
test
: Reh
abili
tatio
n En
gine
erin
g La
bora
tory
Han
d Fu
nctio
n Te
st; r
TMS:
rep
etiti
ve tr
ansc
rani
al m
agne
tic s
timul
atio
n; S
CIM
: Spi
nal C
ord
Inde
pend
ence
Mea
sure
; SS:
som
atos
enso
ry s
timul
atio
n; T
oCU
EST:
task
-ori
ente
d cl
ient
- ce
nter
ed u
pper
ext
rem
ity s
kille
d pe
rfor
man
ce tr
aini
ng; T
RI-H
FT: T
oron
to R
ehab
ilita
tion
Inst
itute
Han
d Fu
nctio
n Te
st; U
ni-:
unim
anua
l; W
MFT
: Wol
f Mot
or F
unct
iona
l Tes
t; A
DL:
act
ivity
of d
aily
liv
ing;
QoL
: qua
lity
of li
fe; Q
IF: q
uadr
iple
gia
inde
x of
func
tion;
ES:
elec
tric
al s
timul
atio
n.
(=):
no s
igni
fican
t cha
nge;
(+):
signi
fican
t im
prov
emen
t; bo
th (+
): sig
nific
ant i
mpr
ovem
ent i
n bo
th g
roup
s; bo
th (=
): no
sig
nific
ant c
hang
e in
bot
h gr
oups
.
Tab
le 4
. (C
ontin
ued)

Lu et al. 11
spinal cord injury have, among the total population with spinal cord injury, the most secondary compli-cations, leading to frequent drop-outs and poorer adherence to trial training specifications. Third, these patients are difficult to match owing to the complexity of their pathology. Fourth, both in spi-nal cord injury and non-spinal cord injury patients, arm and hand function is a complex issue. It encompasses a wide variety of highly non-cyclic movements, which are not always easy to measure objectively, especially at the activity level.26
Some studies in the literature indicate that early initiation of spinal cord injury-specific rehabilita-tion is extremely important. A delay in starting these interventions may negatively influence ulti-mate functional capability.27,28 However, studies included in this review showed that training initi-ated in the chronic stage still resulted in improve-ment of muscle strength, hand function and activities of daily living or quality of life. These findings indicated that improvement in arm and hand muscle strength and function was possible with training in both the acute and chronic phases.
The outcome of included studies showed that exer-cise therapy and functional electrical stimulation improved muscle strength, arm and hand function, activities of daily living or quality of life in patients with cervical spinal cord injury. Studies that focused on electrical stimulation showed improvements in muscle strength of upper extremity, but there were few reports about whether it could improve arm and hand function, activities of daily living or quality of life. New techno-logical innovations, such as repetitive transcranial stimulation, robotic training and virtual reality, have been introduced in rehabilitation in recent years. But most studies were case series, with only two studies on repetitive transcranial stimulation and robotic training, which were included in this review, including a control group.24,25 Neither of the two studies reported muscle strength improvement after training, only repetitive transcranial magnetic stimulation (rTMS) showed an arm function increase after training. The negative results be owing to the small sample size.
In this review, we only included English-language articles, which may cause bias owing to missing some published studies in this area in another language. Most of the studies did not include a sample size
calculation. The small sample size means that the power of the studies to detect an effect, if the effect actually exists, is compromised. Therefore, conclu-sions drawn from these studies should be made with caution. A meta-analysis was not possible because of the variety of outcome measures. Comparison of results across studies would be improved by stand-ardization of outcome measures. There are initiatives in the field of spinal cord injury rehabilitation to develop international standards and data sets for spi-nal cord injury. The Functional Independence Measure and the Spinal Cord Independence Measure are recommended in these guidelines to assess activi-ties of daily living in patients with spinal cord injury.29,30 Other tests, such as the Jebsen test and the Sollerman test have also been suggested in these guidelines. However, at the present time, there is a lack of consensus on what might be the most useful tests of arm and hand function after spinal cord injury.
In conclusion, the results of this systematic review suggest that training of the upper limb following spinal cord injury, including exercise therapy, electrical stim-ulation and functional electrical stimulation, leads to improvements in muscle strength, upper limb function and activities of daily living or quality of life. Further research is needed on the use of new technology, such as repetitive transcranial stimulation in improving upper limb function. Future studies should be carefully designed to increase trial power and external validity. The routine use of a series of standardized objective tests would allow future meta-analyses of the effective-ness of exercise interventions on upper limb function from a number of smaller studies.
Clinical messages
x� Training, including exercise therapy, elec-trical stimulation and functional electrical stimulation, could improve arm and hand muscle strength and function after spinal cord injury.
x� The use of standardized outcome meas-ures of upper limb function in future clini-cal trials would facilitate meta-analyses on the effectiveness of training interven-tions on upper limb function.

12 Clinical Rehabilitation 29(1)
Conflict of interestThe authors declare that there is no conflict of interest.
FundingThis research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References 1. Wyndaele M and Wyndaele JJ. Incidence, prevalence and
epidemiology of spinal cord injury: what learns a world-wide literature survey? Spinal Cord 2006; 44: 523–529.
2. Nussbaum SB. Epidemiology of cervical spinal cord injury. Top Spinal Cord Inj Rehabil 2004; 9: 1–10.
3. DeVivo MJ. Epidemiology of traumatic spinal cord injury. In: Kirshblum S, Campagnolo DI and DeLisa JS (eds) Spinal cord medicine. Philadelphia, PA: Lippincott Williams & Wilkins, 2002, pp.69–81.
4. Snoek GJ, Ijzerman MJ, Hermens HJ, Maxwell D and Biering-Sorensen F. Survey of the needs of patients with spinal cord injury: impact and priority for improvement in hand function in tetraplegics. Spinal Cord 2004; 42: 526–532.
5. Ginis KA and Hicks AL. Exercise research issues in the spinal cord injured population. Exerc Sport Sci Rev 2005; 33: 49–53.
6. Murray WM, Hentz VR, Friden J and Lieber RL. Variability in surgical technique for brachioradialis ten-don transfer. Evidence and implications. J Bone Joint Surg Am 2006; 88: 2009–2016.
7. Rupp R and Gerner HJ. Neuroprosthetics of the upper extremity – clinical application in spinal cord injury and challenges for the future. Acta Neurochir Suppl 2007; 97: 419–426.
8. Kloosterman MG, Snoek GJ and Jannink MJ. Systematic review of the effects of exercise therapy on the upper extremity of patients with spinal-cord injury. Spinal Cord 2009; 47: 196–203.
9. Downs SH and Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health 1998; 52: 377–384.
10. Beekhuizen KS and Field-Fote EC. Massed practice ver-sus massed practice with stimulation: Effects on upper extremity function and cortical plasticity in individuals with incomplete cervical spinal cord injury. Neurorehabil Neural Repair 2005; 19: 33–45.
11. Beekhuizen KS and Field-Fote EC. Sensory stimulation augments the effects of massed practice training in per-sons with tetraplegia. Arch Phys Med Rehabil 2008; 89: 602–608.
12. Glinsky J, Harvey L, Korten M, Drury C, Chee S and Gandevia SC. Short-term progressive resistance exer-cise may not be effective at increasing wrist strength in
people with tetraplegia: a randomised controlled trial. Austr J Physiother 2008; 54: 103–108.
13. Glinsky JHL, van Es P, Chee S and Gandevia SC. The addition of electrical stimulation to progressive resistance training does not enhance the wrist strength of people with tetraplegia: a randomized controlled trial. Clin Rehabil 2009; 23: 696–704.
14. Hartkopp AHS, Mizuno M, Ratkevicius A, Quistorff B, Kjaer M and Biering-Sorensen F. Effect of training on contractile and metabolic properties of wrist extensors in spinal cord-injured individuals. Muscle Nerve 2003; 27: 72–80.
15. Hicks AL, Martin KA, Ditor DS, et al. Long-term exer-cise training in persons with spinal cord injury: effects on strength, arm ergometry performance and psychological well-being. Spinal Cord 2003; 41: 34–43.
16. Hoffman LR and Field-Fote EC. Functional and cortico-motor changes in individuals with tetraplegia following unimanual or bimanual massed practice training with somatosensory stimulation: a pilot study. J Neurol Phys Ther 2010; 34: 193–201.
17. Kapadia NM, Zivanovic V, Furlan JC, Craven BC, McGillivray C and Popovic MR. Functional electrical stimulation therapy for grasping in traumatic incomplete spinal cord injury: randomized control trial. Artif Organs 2011; 35: 212–216.
18. Kohlmeyer KM, Hill JP, Yarkony GM and Jaeger RJ. Electrical stimulation and biofeedback effect on recovery of tenodesis grasp: a controlled study. Arch Phys Med Rehabil 1996; 77: 702–706.
19. Kowalczewski J, Chong SL, Galea M and Prochazka A. In-home tele-rehabilitation improves tetraplegic hand function. Neurorehabil Neural Repair 2011; 25: 412–422.
20. Needham-Shropshire BM, Broton JG, Cameron TL and Klose KJ. Improved motor function in tetraplegics follow-ing neuromuscular stimulation-assisted arm ergometry. J Spinal Cord Med 1997; 20: 49–55.
21. Popovic MR, Kapadia N, Zivanovic V, Furlan JC, Craven BC and McGillivray C. Functional electrical stimulation therapy of voluntary grasping versus only conventional rehabilitation for patients with subacute incomplete tetra-plegia: a randomized clinical trial. Neurorehabil Neural Repair 2011; 25: 433–442.
22. Popovic MR, Thrasher TA, Adams ME, Takes V, Zivanovic V and Tonack MI. Functional electrical ther-apy: retraining grasping in spinal cord injury. Spinal Cord 2006; 44: 143–151.
23. Spooren AI, Janssen-Potten YJ, Kerckhofs E, Bongers HM and Seelen HA. Evaluation of a task-oriented client-centered upper extremity skilled performance training module in persons with tetraplegia. Spinal Cord 2011; 49: 1049–1054.
24. Kuppuswamy A, Balasubramaniam AV, Maksimovic R, et al. Action of 5 Hz repetitive transcranial magnetic stimulation on sensory, motor and autonomic function in human spinal cord injury. Clin Neurophysiol 2011; 122: 2452–2461.

Lu et al. 13
25. Zariffa J, Kapadia N, Kramer JL, et al. Feasibility and efficacy of upper limb robotic rehabilitation in a subacute cervical spi-nal cord injury population. Spinal Cord 2012; 50: 220–226.
26. Spooren AI, Janssen-Potten YJ, Kerckhofs E and Seelen HA. Outcome of motor training programmes on arm and hand functioning in patients with cervical spinal cord injury according to different levels of the ICF: a system-atic review. J Rehabil Med 2009; 41: 497–505.
27. Norrie BA, Nevett-Duchcherer JM and Gorassini MA. Reduced functional recovery by delaying motor training after spinal cord injury. J Neurophysiol 2005; 94: 255–264.
28. Kirshblum SC, Priebe MM, Ho CH, Scelza WM, Chiodo AE and Wuermser LA. Spinal cord injury medicine. 3. Rehabilitation phase after acute spinal cord injury. Arch Phys Med Rehabil 2007; 88: S62–70.
29. Steeves JD, Lammertse D, Curt A, et al. Guidelines for the conduct of clinical trials for spinal cord injury (SCI) as developed by the ICCP panel: clinical trial outcome meas-ures. Spinal Cord 2007; 45: 206–221.
30. Biering-Sørensen F, Charlifue S, DeVivo M, et al. International spinal cord injury data sets. Spinal Cord 2006; 44: 530–534.
Appendix 1
Search strategyMEDLINE search strategy (the search strategy uses MeSH terms unless indicated otherwise): Set A terms (combined by OR) tetraplegia quadriplegia spinal cord injury spinal cord lesion; Set B terms (combined by OR) hand function arm function upper limb function upper extremity function; Set C (combined by OR) exercise strength robotic electric* stimulation task specific training repetitive transcranial magnetic stimu-lation virtual reality.

Copyright of Clinical Rehabilitation is the property of Sage Publications, Ltd. and its contentmay not be copied or emailed to multiple sites or posted to a listserv without the copyrightholder's express written permission. However, users may print, download, or email articles forindividual use.