
Medically unexplained chronic pain in Australia: Difficulties for rehabilitation providers and...
13
Work 36 (2010) 167–179 167 DOI 10.3233/WOR-2010-1018 IOS Press Medically unexplained chronic pain in Australia: Difficulties for rehabilitation providers and workers in pain Coralie Wales a,∗ , Lynda R. Matthews b and Michelle Donelly a a Faculty of Health Sciences, University of Sydney, Lidcombe, NSW, Australia b Ageing, Work and Health Research Unit, Faculty of Health Sciences, University of Sydney, Lidcombe, Australia Received 12 October 2008 Accepted 6 November 2009 Abstract. In Australia, evidence of an ageing population and a skills shortage are imminent challenges for employers [5,50]. A further concern arises from the work injury and motor accident compensation schemes, where many claims for soft tissue injuries result in permanent impairment depriving the community of otherwise productive workers [85]. In many cases, it is chronic pain that becomes the major barrier to a return to productive work. Objective: This study will review the operation of rehabilitation within Australian Workers’ and Motor Accidents compensation systems in order to identify values and attitudes underpinning the vocational rehabilitation ethos. The models underlying current practice will also be identified. Methods: A comprehensive review of published literature and policy documents was undertaken. Results: We identified a variety of contextual factors that influenced progress back into the workforce for people living with persistent pain. The conceptual models underpinning these factors within rehabilitation systems were explored. They were all driven by a strong focus on early return to work and at the same time the sustainability of rehabilitation as a profitable industry. Conclusions: Implications of these findings on the relationship between the rehabilitation provider and the person in pain are discussed. Rehabilitation professionals are influenced by and in turn influence the context in which chronic pain is experienced. Empirical data about the experiences of vocational rehabilitation professionals in Australian personal injury rehabilitation systems is lacking, yet the implications of the cost of chronic pain to the nation are significant. It is recommended that rehabilitation providers increase their awareness of the perhaps unforeseen traps within the various practice models they might be using on the goal of sustainable return to work for people living with pain. Keywords: Labour force participation, Cartesian dualism, medical model, biopsychosocial model, workers’ compensation, contextual factors 1. Introduction In Australia it is predicted that overall workforce par- ticipation will diminish due to important demographic factors such as an ageing population [4] and shortages of a skilled labour force [50]. Furthermore 50% of men ∗ Address for correspondence: Coralie Wales, Macarthur House, 8 Melville St, Parramatta, NSW 2150, Australia. Tel.: +61 2 9890 6988; Fax: +61 2 8580 5159; E-mail: [email protected]. and 20% of women are likely to retire early because of health issues [69]. Another influence that determines workforce partic- ipation in Australia is long-term disability due to per- sistent pain following soft tissue injuries. This phe- nomenon is noted to occur particularly within personal injury compensation systems [85]. In fact chronic pain as a barrier to returning to work is a major concern in most industrialized countries [46]. Unlike many other Western nations, Australia has incorporated the provi- 1051-9815/10/$27.50 2010 – IOS Press and the authors. All rights reserved
Transcript of Medically unexplained chronic pain in Australia: Difficulties for rehabilitation providers and...

Work 36 (2010) 167–179 167DOI 10.3233/WOR-2010-1018IOS Press
Medically unexplained chronic pain inAustralia: Difficulties for rehabilitationproviders and workers in pain
Coralie Walesa,∗, Lynda R. Matthewsb and Michelle Donellya
aFaculty of Health Sciences, University of Sydney, Lidcombe, NSW, AustraliabAgeing, Work and Health Research Unit, Faculty of Health Sciences, University of Sydney, Lidcombe, Australia
Received 12 October 2008
Accepted 6 November 2009
Abstract. In Australia, evidence of an ageing population and a skills shortage are imminent challenges for employers [5,50]. Afurther concern arises from the work injury and motor accident compensation schemes, where many claims for soft tissue injuriesresult in permanent impairment depriving the community of otherwise productive workers [85]. In many cases, it is chronic painthat becomes the major barrier to a return to productive work.Objective: This study will review the operation of rehabilitation within Australian Workers’ and Motor Accidents compensationsystems in order to identify values and attitudes underpinning the vocational rehabilitation ethos. The models underlying currentpractice will also be identified.Methods: A comprehensive review of published literature and policy documents was undertaken.Results: We identified a variety of contextual factors that influenced progress back into the workforce for people living withpersistent pain. The conceptual models underpinning these factors within rehabilitation systems were explored. They were alldriven by a strong focus on early return to work and at the same time the sustainability of rehabilitation as a profitable industry.Conclusions: Implications of these findings on the relationship between the rehabilitation provider and the person in pain arediscussed. Rehabilitation professionals are influenced by and in turn influence the context in which chronic pain is experienced.Empirical data about the experiences of vocational rehabilitation professionals in Australian personal injury rehabilitation systemsis lacking, yet the implications of the cost of chronic pain to the nation are significant. It is recommended that rehabilitationproviders increase their awareness of the perhaps unforeseen traps within the various practice models they might be using on thegoal of sustainable return to work for people living with pain.
Keywords: Labour force participation, Cartesian dualism, medical model, biopsychosocial model, workers’ compensation,contextual factors
1. Introduction
In Australia it is predicted that overall workforce par-ticipation will diminish due to important demographicfactors such as an ageing population [4] and shortagesof a skilled labour force [50]. Furthermore 50% of men
∗Address for correspondence: Coralie Wales, Macarthur House,8 Melville St, Parramatta, NSW 2150, Australia. Tel.: +61 2 98906988; Fax: +61 2 8580 5159; E-mail: [email protected].
and 20% of women are likely to retire early because ofhealth issues [69].
Another influence that determines workforce partic-ipation in Australia is long-term disability due to per-sistent pain following soft tissue injuries. This phe-nomenon is noted to occur particularly within personalinjury compensation systems [85]. In fact chronic painas a barrier to returning to work is a major concern inmost industrialized countries [46]. Unlike many otherWestern nations, Australia has incorporated the provi-
1051-9815/10/$27.50 2010 – IOS Press and the authors. All rights reserved

168 C. Wales et al. / Medically unexplained chronic pain in Australia
sion of rehabilitation into legislation governing workerscompensation and personal injury compensation sys-tems [14]. Despite this provision the annual cost ofchronic pain to work productivity is estimated to beAUD 5.1 billion, a sum that includes absenteeism andreduced effectiveness at work due to pain [78]. In NewSouth Wales (NSW) those soft tissue injury workers’compensation claims, which resulted in permanent im-pairment, were estimated to cost AUD109 million in2007 [85]. However, the full extent of the economicimpact of reduced work effectiveness due to pain is un-certain [78] and the total cost of persistent pain acrossall Australian compensation jurisdictions remains dif-ficult to quantify.
Return to work (RTW) rate is a frequently used mea-sure of success in workers’ compensation systems. In2007/2008, workers’ compensation RTW rates for sus-tained employment reduced from 80% to 75% therebycontinuing a five year trend [14]. These rates may evenbe lower for some sub-populations. In 2004, Athanasoureported that the return to work rate following episodesof upper and lower back pain was 59% [3]. In partic-ular, the population of workers who have experiencedsoft tissue or so called ‘minor injuries’, which have ledto ongoing pain, represent a significant loss of labourparticipation [57]. The phenomenon whereby ‘soft tis-sue injury’ leads to ongoing pain is often referred toas ‘medically unexplained pain’ when health profes-sionals have been unable to identify objective medi-cal markers to corroborate the reported experience ofpain [59,71].
1.1. Aim
This study examines the policy and practice of voca-tional rehabilitation in Australia in order to identify theunderlying models being used to respond to the needsof workers experiencing persistent pain.
1.2. Methodology
A search on databases including Medline, PsycIN-FO, Cinahl and AMED was undertaken using prima-ry keywords and combinations of keywords includingpain; chronic pain; persistent pain; vocational rehabili-tation; occupational rehabilitation; health professional;practitioner beliefs; beliefs; attitudes; health personnel;allied health personnel; compensation; personal injurycompensation; workers compensation; motor accidentscompensation; biopsychosocial; biomedical; medicalmodel and work stress.
The review included research articles, commen-taries, theoretical analyses, case studies, dissertationsand literature reviews published in international peerreviewed journals during the period from 1990–2008.In addition the citations listed in the publications wereinvestigated in order to identify original empirical workand seminal references. These included materials from1948 to 2008. An internet search was conducted us-ing Google and Copernic to find Government policydocuments, information resources, and other workingdocuments reflecting current policy and practice in thefield of vocational rehabilitation in Australia.
467 articles were identified and reviewed. Threemain groups of articles were selected. Firstly, thoserelevant to the experiences, attitudes and beliefs ofhealth professionals in responding to the rehabilita-tion needs of people in chronic pain; Secondly, thosethat described the development and current operation,management or practice of vocational rehabilitation inAustralia; Finally, those articles relevant to the currentmodels that explain and treat chronic pain.
Key themes were identified, and current models wereused to analyse the experiences of health professionalsand current rehabilitation practices in order to deter-mine whether these models are able to explain commonexperiences and practices.
All publications which addressed the experiences ofhealth professionals and /or current rehabilitation prac-tices and/or models which were used to explain prac-tices were retained for analysis.
2. The ‘aporia’ of chronic or persistent pain
The approach to philosophical enquiry developedby Socrates focused on uncovering puzzling questionsabout human experience rather than being satisfied withsimplistic assumptions about these phenomena. Such apuzzle is referred to as an ‘aporia’. Quintner et al. quoteDerrida when noting that the unpredictability of persis-tent pain “constitutes an aporia, a space and presencethat defies us access to its secrets” [25,66]. These the-orists acknowledge that in their attempt to understandthe experience of pain they encountered more puzzlesthan answers, and came to view persistent pain as amystery defying logical explanation [66].
Pain can be difficult to explain when it persists wellbeyond the expected healing time following an injury.While some people living with chronic pain may beable to explain their experience in terms of an underly-ing pathology such as rheumatoid arthritis or shingles,

C. Wales et al. / Medically unexplained chronic pain in Australia 169
for others medicine offers them little or no explanation.It is then that pain can become most vexatious for theperson experiencing it, and it may not be seen as ‘le-gitimate’ by significant others including their own painspecialist [45]:
“Some people actually believe what they are tellingyou. . . but you just couldn’t believe that they wereunable to do some small physical task because ofthe pain they were in” or “It stands to reason. Ifyou have done all the tests possible, and you getnothing, not a hint of a physical problem, what elsecan you conclude?” [45]
2.1. Early understanding of pain
Until the mid-20th Century it was generally believedthat a pain experienced in the body indicated an un-derlying nociceptive (i.e. tissue damaging) process andthat the underlying pathology had to be discovered andthen addressed in order to deal adequately with the pain.Scientific thought about pain had been predominant-ly framed around Descartes’ ‘specificity theory’ [56],which proposed that pain is due to specific nerve im-pulses that are produced by an injury and transmit-ted directly to a pain centre in the brain. According toDescartes, the amount of pain experienced was direct-ly proportional to the extent of the bodily injury. Thebody was seen by Descartes as a hydraulic machine –this view was consistent with contemporary philosoph-ical thought that all things in nature conformed to arith-metical models. Descartes also conceived that the mind(res cogitans) and body (res extensa) were quite sepa-rate entities [8,63]. His philosophy informed the fun-damental parameters of what has become known as the“biomedical model of disease”.
In the second half of the 20th Century, scientistsbegan to appreciate the complexity of chronic pain.For example, psychologist Ronald Melzack, a pioneer-ing pain researcher, challenged the assumptions of the‘specificity theory’ in his observation that:
“. . . pain is much more variable and modifiablethan many people have believed. Pain is not simplya function of the amount of bodily damage alone.The amount and quality of pain we feel are also de-termined by our previous experiences and how wellwe remember them, by our ability to understand thecause of the pain and to grasp its consequences.Even the significance pain has in the culture inwhich we have been brought up, plays an essentialrole in how we feel and respond to it” [53].
Melzack, together with neurobiologist Patrick Wall,formulated a new model of pain, which became knownas the ‘Gate Control’ theory, which emphasised centralneuroplasticity, the modulation of nociceptive inputsat the spinal dorsal horn and the dynamic role of thebrain in pain processing [54]. The neurophysiologicalstate known as ‘central sensitisation’ is now widelyacknowledged to be a major contributor to ‘medicallyunexplained’ chronic pain [11].
2.2. Recent developments in pain science
Beyond the nervous system, other bodily systemshave been implicated in the ‘aporia’ of chronic pain.Research into the role of the Hypothalamus – Pituitary –Adrenal (HPA) axis and the release of stress hormonesin chronic pain highlights the impact of stressors [28].The immune system is thought to modulate the ex-perience of pain through the release of various sub-stances including neuropeptides and pro-inflammatorycytokines [38] and may have a pivotal role to play in pe-ripheral neuropathic pain [48]. The feedback and feed-forward processes existing between the central nervoussystem (CNS) and the immune system have been sug-gested as mechanisms that link the ‘ancient survival–oriented circuitry’ in the CNS to the triggering of the‘sickness response’ [83].
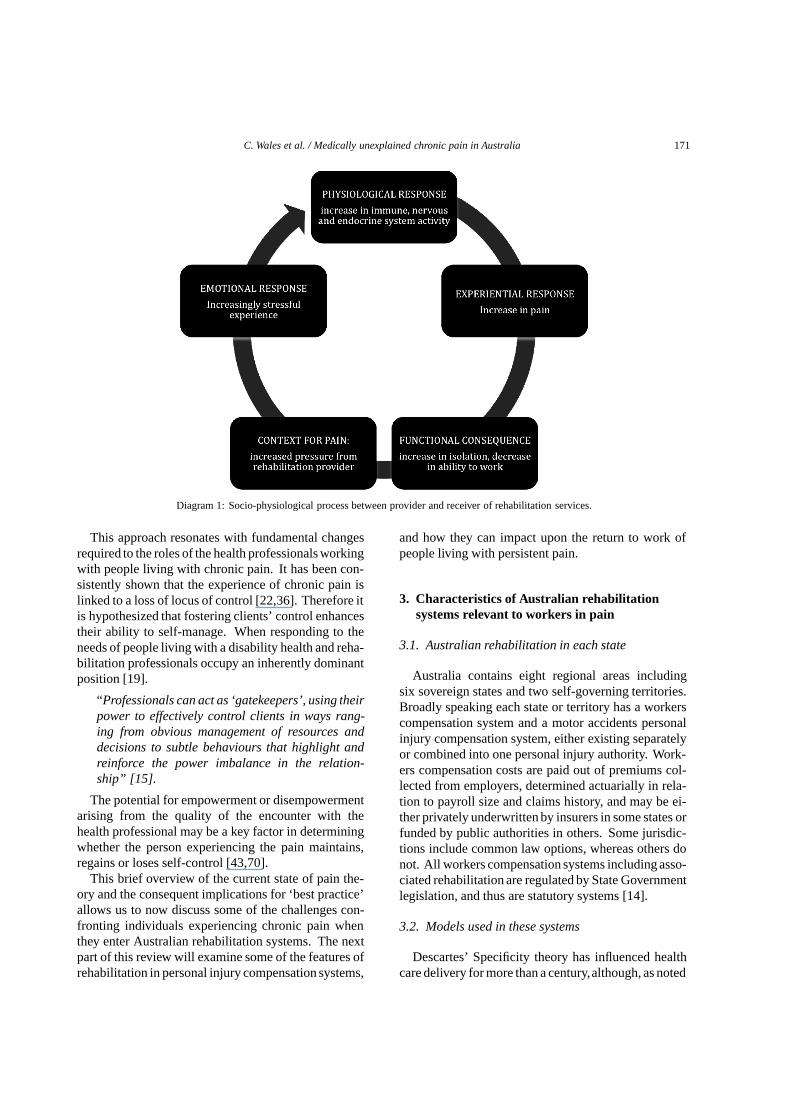
When considering the survival value of the experi-ence of pain, it is reasonable to conclude that the humanorganism has evolved to regard pain as a key element inits warning system. Pain as a response to threat com-prises contributions from many bodily systems. For ex-ample, the cells of the immune system create inflam-mation and the endocrine system produces stress hor-mones [12]. When these processes become extended intime and bodily responses consume large amounts ofenergy, the warning system becomes less helpful as anadaptive strategy. While the production of adrenaline inresponse to emergency is helpful to survival, in chron-ically stressful situations excessive production of cor-tisol has been linked to depression [51] and indirect-ly linked (through the release of pro-inflammatory cy-tokines) to the development and maintenance of centralsensitisation [24]. The stress of living with persistent‘medically unexplained’ pain can be exacerbated byuncertainty as to outcome and also by lack of valida-tion of the experience [84] creating a cycle of increas-ing pain and distress fed by further lack of validationand ultimately worsening sensitisation of the centralnervous system [55].

170 C. Wales et al. / Medically unexplained chronic pain in Australia
This cycle (shown in Diagram 1) confirms that theexperience of pain is inextricably linked to the socialcontext in which it occurs and that explanations of painwhich focus only on physiological process are incom-plete unless the effect of the external environment isalso considered.
Persistent pain has been described as ‘moulded andshaped both by the individual and their particularsocio-cultural context’ and as existing ‘at the intersec-tion between biology and culture’ [7]. Chronic paincan therefore be seen as a contextually dependent phe-nomenon. It is known that social contexts alter individ-ual physiological variables [30,77]. Studies in primateshave found increases in stress hormones in socially iso-lated situations [68,83], and human babies demonstrateincreases in H-P-A axis activity when separated fromtheir mothers [33]. Researchers have highlighted therole of stress in pain physiology [17,51,55] and it canbe argued that aspects of the environment such as fam-ily breakdown or financial disadvantage can influencethe experience of persistent pain through altering indi-vidual physiological processes. The study of such in-teractions between the body and environment has beencalled ‘socio-physiology’ [29]. Another matter worthyof consideration is the crucial interaction between theperson in pain and the rehabilitation system as embod-ied by the rehabilitation provider. Adler (2002) foundthat both parties taking part in the therapeutic encountercan impact upon each other’s health [2].
As suggested in Diagram 1, the person in pain canrespond negatively to systemic stressors such as timelimits, financial limits and support limits identified bythe rehabilitation provider culminating in pressure toquickly return to work. The person may engage defen-sive physiological processes in response to such an ad-ditional stressor, which can consequently worsen painand reduce functionality for work, thus perpetuatingthe cycle.
The shift from Descartes’ view of pain (based upon ahard-wired nervous system) to an understanding of thecomplex socio-physiological processes that may per-petuate pain has seen a major paradigm shift in pain re-search. This shift has important implications as to howpain is better understood and responded to by healthprofessionals. Consequently, although pain itself canbe thought of as an ‘aporia’,
“. . . pain may be apprehended in the clinical en-counter through the engagement of two autonomousself-referential beings in the intersubjective or so-called third space, from which new therapeutic pos-sibilities can arise” [66]
2.3. Implications of recent developments in painscience for health professionals
Recent changes in the understanding of pain presenta challenge for what is considered to be ‘best practice’in responding to the needs of people living with chronicpain. For example, the New Zealand Accident Com-pensation Corporation (ACC) has recommended thathealth professionals take a preventative approach, byaddressing within the first few weeks the biomedicalconsequences of soft tissue injuries at the same timeas addressing relevant psychosocial factors [1]. Theserecent advances in current thinking about pain, as dis-cussed above, mandate that health professionals willalso understand and respond to the contextual factorsmoulding the experience of chronic pain. Such contex-tual factors can include the personal environment, thework environment and the systemic processes involvedin the compensation environment [10,42,61].
The growing understanding of the complexity of thepain experience also has implications for the roles ofboth the health professional and the person in pain with-in the context of rehabilitation. There is concern thathealth professionals, despite advances in pain science,are not transferring this knowledge into pain rehabili-tation practice:
“. . . research projects are urgently needed to de-termine why this knowledge has not translated intopractice in order to address the indifference, lackof knowledge and the stigma that people living withchronic pain face from the professionals who aresupposed to assist them” [75]
From the perspective of the person in pain,being ableto engage meaningfully in everyday activities, includ-ing employment, ultimately involves making personalchoices about appropriate and effective strategies thatwork for them [16] and being unimpeded by social bar-riers that may contribute to disability and stigma [37].Making these choices often requires a degree of autono-my and a process of wide consultation with a variety ofhealth professionals, friends and family members [16].‘Self-management’ is a term that carries multiple mean-ings, depending on whose perspective is being consid-ered [42]. It can encompass the use of strategies by aperson living with chronic pain, and can be enhancedby concepts of social inclusion through active attemptsto reduce social barriers to disability [42]. Accordingto this view ‘self management’ would involve a personwho experiences pain choosing meaningful activitiesin an environment where a range of accommodationsand supports promote their inclusion [15].
C. Wales et al. / Medically unexplained chronic pain in Australia 171
Diagram 1: Socio-physiological process between provider and receiver of rehabilitation services.
This approach resonates with fundamental changesrequired to the roles of the health professionals workingwith people living with chronic pain. It has been con-sistently shown that the experience of chronic pain islinked to a loss of locus of control [22,36]. Therefore itis hypothesized that fostering clients’ control enhancestheir ability to self-manage. When responding to theneeds of people living with a disability health and reha-bilitation professionals occupy an inherently dominantposition [19].
“Professionals can act as ‘gatekeepers’, using theirpower to effectively control clients in ways rang-ing from obvious management of resources anddecisions to subtle behaviours that highlight andreinforce the power imbalance in the relation-ship” [15].
The potential for empowerment or disempowermentarising from the quality of the encounter with thehealth professional may be a key factor in determiningwhether the person experiencing the pain maintains,regains or loses self-control [43,70].
This brief overview of the current state of pain the-ory and the consequent implications for ‘best practice’allows us to now discuss some of the challenges con-fronting individuals experiencing chronic pain whenthey enter Australian rehabilitation systems. The nextpart of this review will examine some of the features ofrehabilitation in personal injury compensation systems,
and how they can impact upon the return to work ofpeople living with persistent pain.
3. Characteristics of Australian rehabilitationsystems relevant to workers in pain
3.1. Australian rehabilitation in each state
Australia contains eight regional areas includingsix sovereign states and two self-governing territories.Broadly speaking each state or territory has a workerscompensation system and a motor accidents personalinjury compensation system, either existing separatelyor combined into one personal injury authority. Work-ers compensation costs are paid out of premiums col-lected from employers, determined actuarially in rela-tion to payroll size and claims history, and may be ei-ther privately underwritten by insurers in some states orfunded by public authorities in others. Some jurisdic-tions include common law options, whereas others donot. All workers compensation systems including asso-ciated rehabilitation are regulated by State Governmentlegislation, and thus are statutory systems [14].
3.2. Models used in these systems
Descartes’ Specificity theory has influenced healthcare delivery for more than a century,although, as noted

172 C. Wales et al. / Medically unexplained chronic pain in Australia
above, more recent theories have challenged its dom-inance [2,66]. This section will examine the differentconceptual models used in rehabilitation and highlighttheir role in driving rehabilitation for people living withchronic pain.
3.2.1. The biomedical or ‘biogenic’ modelThis model assumes that pain is caused by an iden-
tifiable underlying pathological process, resulting in asearch for that biological abnormality in order to ‘treat’the pain [45]. Many writers comment that this has beenthe dominant model used (usually by default) whendealing with people in chronic pain [7,45,66]. Aus-tralian rehabilitation systems’ tacit acceptance of thismodel is evident in many ways not the least being theirreliance upon the primary medical contact, the GeneralPractitioner, to sign a certificate of fitness which quali-fies people for entry into and continuing participation inworkers’ compensation schemes. General Practition-ers are also the entry point for the approval and formu-lation of both treatment and rehabilitation plans [57].Another consequence of using the biomedical modelhas been that Whole Person Impairment (WPI) deter-minations are used to decide the exact amount of mon-etary compensation to be awarded to each claimant [52,86]. In effect, WPI is here being used as a surrogatemarker for disability, whereby medically unexplainedpain has been effectively excluded from the method ofcalculation. Unsurprisingly, application of this processto low back pain has been found to be unreliable be-cause “pain, functional compromise, and measurablepathoanatomic abnormality are often poorly associat-ed” [18,72]. An example of this bureaucratic sleight-of-hand can be found in the NSW Motor AccidentsScheme wherein it is affirmed that “no damages fornon-economic loss will be awarded unless the personhas a greater than 10 per cent whole-person permanentimpairment” [58,85]. Quintner (2004) argues that inthe absence of agreement that impairment and disabil-ity are causally linked, impairment ratings are merelya ‘standard means whereby medical disability determi-nations are made and legitimized’. Impairment ratingsbear little if any relationship to disability determina-tions, which are of course highly contextual as wellas pain dependent [65,49]. It may be seen from thisdiscussion that when used within Australian rehabilita-tion systems, the biomedical model excludes both pain-related disability and the socio-economic contexts inwhich it may occur, as discussed in Section 2.3 above.
3.2.2. The Psychogenic modelPsychogenic theory proposes that in the absence of
medical markers of impairment, chronic pain has psy-chological origins that play an important role in the on-set, severity, worsening and/or persistence of pain [45].There are those who argue that using the term ‘psy-chogenic’ to describe pain is not only unhelpful but al-so epistemologically flawed [45,66,73,74]. Thompsonnotes that attempts to treat pain as being a primarilypsychogenic problem inflicts
‘a great deal of damage to chronic pain patients;to the patients’ minds by telling them explicit-ly that their pain is not physical. . . and to thepatients’ financial well-being since pain resultingfrom personal injury cases is not compensable inmany jurisdictions if the pain is judged to be non-physical” [73]
However, the use of the term and the set of assump-tions that accompany it are in common practice. Forexample, a simple Google search reveals 82,100 resultsfor ‘psychogenic pain’. A typical assertion containedin one such result is:
“The diagnosis of psychogenic pain is made whenorganic (related to or affecting a bodily organ)causes of pain are ruled out. A person with a paindisorder will complain of pain that does not matchhis or her symptoms” [20].
Importantly, the use of a psychogenic model whenanalysing the experience of chronic pain at the sametime perpetuates the primacy of the biomedical model.It ascribes the experience to a psychological cause onlyin instances where there are no objective medical find-ings to account for the pain [26,66]. Kenny concludedthat doctors default to a psychogenic explanation whendealing with patients with no visible proof of pain [45]whereas other authors highlight the negative implica-tions of Cartesian (body/mind) reductionism when thepain is reduced to being either a physical or a psycho-logical problem [66]. This model is then unilaterallyimposed upon the person in pain.
3.2.3. The Biopsychosocial modelSome personal injury compensation and rehabilita-
tion systems in Australia are exploring a different ap-proach with the aim being to reduce the risk of the de-velopment of chronic pain [85]. For example, in NSW,Australia, rehabilitation professionals are advised to in-corporate a ‘biopsychosocial’ approach when dealingwith people affected by soft tissue injuries:

C. Wales et al. / Medically unexplained chronic pain in Australia 173
“The key principles align with the biopsychosocialapproach to management of a worker’s injury. Thisapproach is widely accepted as vital to improvingoutcomes when managing injured workers. Thebiopsychosocial approach recognises that pain isnot felt in accordance with the amount of injury tothe tissues. Rather, pain perception is influencedby a worker’s social environment (work, family,community and compensation systems) and theirthoughts, beliefs, attitudes and emotions. Theseother influences are often grouped together and re-ferred to as ‘psychosocial’ factors. Therefore, ap-plication of a biopsychosocial approach that con-siders the physical, social, psychosocial & emo-tional needs of the worker, underpins effective man-agement.” [85].
If these guidelines result in active interventions tominimize the disabling effect of contextual or socialfactors they may result in better outcomes for this groupof workers. It is unlikely that simply encouraging theperson in pain to better cope with these factors willaffect change [9,61,62].
However, some would argue that although the di-mensions of the social environment are encompassedby the term ‘biopsychosocial’, interventions that ac-tively seek to address the social influences that impingeupon workers in pain are lacking [9,61,62]. Address-ing ‘psychosocial aspects’ is usually limited to helpingthe individual cope with external stressors, that is bylocating the problem within the individual [49] ratherthan taking a broader view of the whole situation, in-cluding the social environment in which pain occurs orby linking ‘personal troubles and public issues’ [62].It has been well established that actively interveningto reduce the social barriers to disability leads to moreeffective worker retention as demonstrated by those or-ganisations that address the quality and nature of work-place relationships and take active steps to foster work-er support at all levels of the organization [79–81].
3.3. Conflict between these models and the effect onthe lived experience of chronic pain
Clinical practice is influenced by the theoretical as-sumptions of prevailing conceptual models, althoughfor many practitioners this is often not a conscious pro-cess [66]. The models described above underpin com-mon assumptions in clinical practice that create barri-ers for the practitioner and the person in pain. To illus-trate this point, the definition of ‘pain’ adopted by theInternational Association for the Study of Pain (IASP),
the peak body for health professionals interested in thestudy and practice of pain science, illustrates the strainbetween the models that are used in pain rehabilitation.It defines chronic pain as “an unpleasant sensory andemotional experience associated with actual or poten-tial tissue damage, or described in terms of such dam-age” [39]. As pointed out by Quintner et al. [66], thisdefinition is then qualified by a statement in the nextparagraph: “Many people report pain in the absence oftissue damage or any likely pathophysiological cause;usually this happens for psychological reasons” [39],which endorses a psychogenic explanation for the ex-perience under this circumstance [66]. This effectivelycategorises the experience as either a body or a men-tal phenomenon. The socio-cultural dimensions of thepain experience are rendered irrelevant in the formercategory and relegated to a less important status in thelatter.
Further conflict is illustrated in the operation of theNSW Motor Accidents Scheme. While rehabilitationprofessionals working in this jurisdiction are encour-aged to incorporate the biopsychosocial model in theirwork with people experiencing pain-related disability,this same group of workers in pain are routinely as-sessed for WPI, a process grounded in the biomedicalreductionist model, in order to determine their eligi-bility for compensation. For those individuals highlydisabled by pain, social withdrawal and other markersof the lived experience of chronic pain are described inthe Psychiatric Impairment Rating Scale which is themechanism used in the scheme to determine psychiatricimpairment, again as a means to quantify compensa-tion. This scheme overtly reinforces the Cartesian splitbetween body and mind, and relegates pain issues tothe province of psychiatry.
The body/mind dichotomy that fails to acknowledgeor address contextual influences that can contribute tothe phenomenon may intensify the experience of painand may leave individual sufferers with a sense thatothers do not believe them or that they are to blame insome way for their pain-related disability [23].
“They (the doctors) don’t seem to think that youmight really be in pain. They think that it is allin your mind. (Note: Variations of this statementappeared in all 20 patients’ transcripts.) They thinkthey know what is “really” happening to you. Iwas told straight out that I was putting on an act,that the pain wasn’t real. They all say, ‘Take someZoloft (an antidepressant) and go home. There isnothing wrong with you.’ You start to think, ‘AmI mad or stupid?’ I’m feeling this incredible painand they say I’m not.” (original parentheses) [45]

174 C. Wales et al. / Medically unexplained chronic pain in Australia
Return to work may be difficult if not well-nigh im-possible when people have constantly to prove to othersthat they are in pain [35]. The subtlety of underlyingassumptions about the causes of pain, and the conse-quent effects on perceptions of legitimacy may resultin workers in pain needing to defend their integrity:
“Here’s the rub. There may be much agonizing,but in the absence of impairment, society is notprepared to believe them. Rather, society is willingto go to great lengths and great expense to challengetheir perception. They are drawn into the vortex ofdisability determination. Their suffering escalates;healthfulness is rendered an abstraction. No matterwhat the outcome, healthfulness always will be anabstraction. I am certain that anyone so challengedcan only get more ill; to get well is to abandonveracity.” [35]
When applied to provide assistance for people inpain, the demonstrable deficiencies in each of thebiomedical, psychogenic and the biopsychosocial mod-els highlight the need to both consider and actively dealwith social and contextual factors. The sociophysio-logical evidence clearly shows the effect of social con-text on the experience of pain and the operation of eachperson in the therapeutic dyad as having an effect on theother [66]. However, it is unclear whether this is wellunderstood or demonstrable within current operationsof the statutory rehabilitation industry.
3.4. Vocational rehabilitation as a profitable industrywith a focus on early return to work
‘Rehabilitation’ is described as the provision of ser-vices to assist people with disabilities resume engage-ment with everyday activities in their communities [67].Health professionals from medical and allied healthfields either work in a team or individually when provid-ing rehabilitation services to people with disabilities.The two goals underpinning the profession called ‘Re-habilitation’ are firstly to provide resources for peoplewith disabilities and secondly to bring about changesin the environment – physical, social, or structural – tosatisfy the needs of such individuals and to enable themto achieve their personal goals [67]. Vocational reha-bilitation (VR) has a focus on helping people return towork. At an official level, VR has been influenced byhumanistic principles arising from emancipation move-ments such as the Independent Living Movement [41],Australian Government initiatives such as the Wood-house enquiry in 1974 [52], and the introduction of the
Australian Commonwealth Disability Services Act of1986 [21]. Humanistic principles that have influencedthe development of vocational rehabilitation includethe view that performing work is a human right:
“Everyone has the right to work, to free choiceof employment, to just and favourable condi-tions of work and to protection against unemploy-ment” [76]
Prior to the late 1980s, making a claim for per-sonal injury in Australia was embedded in commonlaw systems. Settlement of cases often took years toachieve, with a lump sum payout being made at the con-clusion of legal proceedings. It was often impossiblefor a claimant to access necessary resources to obtainrehabilitation services early after injury [52]. At thistime many Australian State Governments started mak-ing legislative changes to promote the early provisionof rehabilitation with a view to reducing the high levelsof disability and cost associated with existing commonlaw systems [47]. By the end of the decade rehabili-tation was embodied in legislated workers’ compensa-tion and motor accident systems around Australia [41].Providing access to rehabilitation soon after injury andmaking rehabilitation mandatory was meant to increasethe likelihood of an early return to work and a reductionin the total costs of injury [6].
At the same time that rehabilitation has been aim-ing to reduce the human cost of injury and disabil-ity, other significant economic forces have impingedupon rehabilitation practices. Under the influence ofconservative government in the 1990s, Australia’s old-est and largest provider of rehabilitation services, theCommonwealth Rehabilitation Service, (now knownas ‘CRS Australia’) was corporatized. Since the 1990sstatutory rehabilitation in many states has been pro-vided by numerous private companies operating in acompetitive environment using various business mod-els [41].
The vested interests of diverse stakeholder groupshave led to perhaps unforeseen difficulties for reha-bilitees whenever conflicts arise between their inter-ests and those of other stakeholders. Stakeholders in-clude the individual in chronic pain, third party insur-ers, government departments, employers, trade unionsand rehabilitation-for-profit organisations. The pres-sures on rehabilitation-for-profitorganisations are quitedifferent to those on rehabilitation services run by theGovernment several decades earlier. Whereas there wasno ambiguity about the service target in earlier ‘so-cial’ models, the introduction of a rehabilitation-for-

C. Wales et al. / Medically unexplained chronic pain in Australia 175
profit model brought a new and important customerinto the equation, the corporate funding body. Fund-ing bodies include insurers, other commercial organi-zations and individual Government departments. Ac-cording to Kendall, by the late 1990s the rehabilita-tion landscape had experienced the “end of social reha-bilitation models and the rise of a privatized businessmodel of VR” [41].
In the privatized business model of VR, the ‘cus-tomer’ always has the reasonable right to demand ser-vices from their preferred providers as defined by pre-determined key performance indicators. Such indica-tors are necessarily geared towards lowering costs andreducing the incidence and duration of claims. As sys-tems have tightened up their expenditure to limit pay-ments for pain and suffering over the last decade [31,64], so too has the pressure mounted on rehabilitationproviders to hasten their client’s journey back to work.This includes incentive payments for earlier returns towork by rehabilitees [41]. Pressure can also be appliedto rehabilitation professionals to provide confidentialinformation that could be used as evidence in litigioussituations [40]. Juggling between the competing needsof the various ‘customers’ – such as the high and cost-ly needs of the client with chronic pain and the in-centive to cut costs in order to make a profit – mayhave a decidedly negative effect on the individual per-son in pain. Maintaining humanistic health profession-al values alongside values that support the maximiza-tion of profit, the development of a competitive edgeand organizational and structural control may be ex-tremely challenging for the rehabilitation professionalas well [29].
From the point of view of the person experiencingchronic pain, return to work, while highly desirable,may not be possible before pain is adequately addressedas a health issue. Meeting the challenges associatedwith pain is a huge burden for sufferers and proba-bly constitutes a significant barrier to their return towork [44]. On the other hand, the financial viability ofthe rehabilitation provider is favourably influenced byachieving early return to work. Herein lies the poten-tial for conflict between the interests of the rehabilita-tion provider and the individual whose main barrier toreturn to work is chronic pain.
4. Health professionals working in these systems
Juggling the competing needs of stakeholders has be-come difficult for everyone but particularly so for health
professionals involved in providing rehabilitation ser-vices for people with “medically unexplained pain”.The impact of changing paradigmatic frameworks mayhave significance for the role of the health professionalin this area.
It is usual for health professionals to value the‘working alliance’ and engage empathically with theirclients [27] and it has been shown that their empath-ic engagement has significant personal consequenceswhen they witness the major losses that occur for someclients after injury [13]. However, workers in pain feelangry about their treatment by rehabilitation profes-sionals:
“There was a strong sense of grievance and dis-content among these participants regarding theirrehabilitation experience. As one injured workercommented: ‘they tried to have me go back to thesame work that caused my pain in the first place’.Indeed, such rehabilitation was seen as useless: ‘itonly made my condition worse’, and caused furtherinsult. Rehabilitation professionals were regardedas inexperienced: ‘just out of college’, and moreInterested in ‘pleasing the boss’ and ‘representingthe insurance company’ than in assisting injuredworkers. For these workers, their rehabilitation ex-periences and difficulties with insurance companiesadded to a lack of trust in, and cynicism about,what ‘the system’ and rehabilitation had to offer.Their experiences of being let down by others andof trying to work ‘despite the pain’, only intensifiedtheir anger” [34]
The nature of the relationship between the personin pain and the health professional has the potential tohelp or hinder the therapeutic process [66]. This re-lationship is the basis for facilitating the achievementof everyday-life goals identified by the worker in pain.Trust is a critical element in the relationship, especiallywhen dealing with clients experiencing medically un-explained pain, whose legitimacy is subject to continualscrutiny.
“Engaging with a person is an active process andwill not occur without trust. Trust, important inany relationship, is especially salient for a personin pain who is confronted on a daily basis by sus-piciousness. Trust implies a genuine belief that aperson experiences pain. Pain is what the personsays it is, despite any statements to the contrary byother health professionals.” [60]

176 C. Wales et al. / Medically unexplained chronic pain in Australia
Perceived distrust from health professionals may“obstruct the adjustment process, prolong sick leaveand hinder rehabilitation” [32]. However, it has beensaid that the current practice of disability determina-tion is “designed to obviate the need to trust any-one who asserts that his or her earning capacity iscompromised” [35,84]. An unfortunate consequence isthat people living with ‘medically unexplained’ chron-ic pain and making claims in personal injury compen-sation systems soon become aware that the reality oftheir pain is in question. While the usual doctor-patientrelationship is based upon the trust the patient has intheir doctor, once the validity of the patient’s pain isquestioned by the doctor, particularly in the context ofmedico-legal settings, trust gives way to anger, and therelationship enters the “disputative state”:
“The process demands that the injured litigant dem-onstrate the magnitude of illness to whomever sitsin judgment of the validity of the demonstration. . .The litigant is likely to lose the prerequisite skillsfor well-being, the abilities to discern among themorbidities, and to cope”. [35]
From a therapeutic point of view, entering a disputeabout the legitimacy of ones pain is clearly unhelp-ful given the known contribution of stress hormones tothe pain experience [83,87]. Yet rehabilitation profes-sionals who work within statutory rehabilitation sys-tems often find themselves in an environment wherebureaucratic rulings, political considerations and inter-minable litigation are common features [8] and wherethey themselves are attempting to service the needs ofa diverse and conflicting number of ‘customers’. Asdiscussed above, to respond humanely to the personin pain while navigating a maze of other stakeholders’needs and demands can be extremely challenging to thehealth and wellbeing of both parties.
The rehabilitation health professional working for aprofitable rehabilitation organisation finds him or herself required to service the needs of the customer (insur-er), as well as to provide service to his/her client, (theworker in pain). Irresolvable conflicts for the healthprofessional may take the form of undue pressure foran early return to work despite the worker’s experienceof disabling pain, and the pressure from the fundingbody to dispute the veracity of the client’s pain in orderto reduce the cost of the claim. These are some of thepotentially damaging consequences that arise from theapplication of the exclusively biogenic or psychogenicmodels that underpin these systems.
5. Conclusions
This paper set out to examine the policy and prac-tice of vocational rehabilitation in Australia in order toidentify the underlying models used to respond to theneeds of workers experiencing persistent but medicallyunexplained pain.
Reliance on the medical practitioner as being centralto rehabilitation planning, and medical determinationsof WPI occurring within the compensation jurisdic-tions, demonstrates the importance of the biomedicalmodel [57,58,86]. This model, while working well toidentify pathological determinants of illness and injury,does not address the contextual dimensions of the expe-rience of persistent pain. The biopsychosocial modelhas been propounded as an alternative model, and mayoffer some improvement on the biomedical model fromthe point of view of the person in pain however, thismodel as it is currently being applied has been shownto perpetuate a reductionist approach in response tomedically unexplained persistent pain [61,62,66].
Furthermore, the rise to prominence of businessmodels in which to frame rehabilitation discourages‘social rehabilitation’ [41] and lessens the opportunitythat people in pain will be given the time and treat-ments necessary to ensure their adequate rehabilita-tion [42]. Despite the humanistic aims of rehabilita-tion [67] the discipline has been influenced by econom-ic drivers that have tended to shift the focus of the re-habilitation provider to an early return to work in allcircumstances, most noticeably in workers’ compensa-tion jurisdictions. The wellbeing of the client has beenargued to be negatively affected:
“In the context of rehabilitation, there is little ev-idence that these economic pressures have beenanything but inimical to the well-being of individu-als with disabilities, rehabilitation counsellors andsociety in general [41].
Identifying the explanatory models that currently in-form rehabilitation responses to people experiencingpain assists us to better understand the factors con-tributing to the increasing prevalence of chronic painas a barrier to well-being and return to work. It hasalso highlighted the need for new and better modelsthat can address the contextual determinants of chronicpain. Identifying the strengths and weaknesses of thecurrent dominant models has highlighted the impact ofthe rehabilitation system itself as a contextual deter-minant of chronic pain. The application of the domi-nant models has been demonstrated to potentially ac-

C. Wales et al. / Medically unexplained chronic pain in Australia 177
centuate the chronic pain experience for injured peo-ple. In the absence of medical markers to corroboratethe experience, trust may evaporate for both the workerin pain and the health professional, leaving them bothdissatisfied with the therapeutic encounter.
Finally, the wellbeing of health professionals work-ing in statutory systems is another concern. The use ofincomplete or dysfunctional models may not only in-validate and stigmatise people living with pain but mayalso become stressful for rehabilitation professionals.This review has indicated that more research is neededto investigate the experiences of vocational rehabilita-tion professionals who work with people disabled by“medically unexplained” pain.
Rehabilitation systems that fail to take account of theaporia of pain may actually worsen pain and alienatehealth workers. The failure to acknowledge or accountfor persistent pain may result in increased costs forindividuals and organizations. It is recommended thatrehabilitation providers increase their awareness of theperhaps unforeseen implications of the various practicemodels they use on sustainable return to work for peopleliving with pain.
The literature highlights the potentially devastatingimpact of common judgments made of people who ex-perience chronic pain [23,45]. However, there is lim-ited empirically-derived understanding of the process-es being employed to discredit the person living withchronic pain. It is also important to establish if theseprocesses are evidence of intrinsic structural flaws inthe current rehabilitation system or merely examples ofpoor practice or both. Empirical research is needed tounderstand the experiences of vocational rehabilitationprofessionals in Australian personal injury rehabilita-tion systems from their perspective, including the fac-tors that influence their practice and their participationin the therapeutic encounter. As the population agesand skills shortages in Australia become more critical,the need to investigate and address these aspects ofrehabilitation practice becomes more urgent.
Acknowledgements
The corresponding author would like to thank JohnQuintner for his intellectual and moral support in re-viewing this manuscript, and the referees of WORK fortheir constructive comments on an earlier draft of thismanuscript.
References
[1] ACC, New Zealand Acute Low Back Pain Guide, Wellington2004.
[2] H. Adler, The sociophysiology of caring in the doctor-patientrelationship, Journal of General Internal Medicine 17 (2002),883–890.
[3] J. Athanasou, Return to work following whiplash and backinjury, University of Technology, Sydney, 2004.
[4] Australian Bureau of Statistics, 4102.0 – Australian SocialTrends, 2004 – the working age, 2004.
[5] Australian Bureau of Statistics, 4102.0 – Australian SocialTrends, 2007- Labour Force Participation – an InternationalComparison, 2007.
[6] Australian Government, Industry Commission: Workers’Compensation in Australia, Australian Government Publish-ing Service, Canberra, 1994.
[7] G.A. Bendelow and S.J. Williams, Transcending the dualisms:towards a sociology of pain, Sociology of Health and Illness17 (1995), 139–165.
[8] A. Benini and J.A. DeLeo, Rene Descartes’ physiology ofpain, Spine 24 (1999), 2115–2119.
[9] F.M. Blyth, G.J. Macfarlane and M.K. Nicholas, Response toMs. Nielsen’s letter to the editor of Pain, Pain 131 (2007), 349.
[10] F.M. Blyth, G.J. Macfarlane and M.K. Nicholas, The contri-bution of psychosocial factors to the development of chron-ic pain: The key to better outcomes for patients? Pain 129(2007), 8–11.
[11] D. Butler, The Sensitive Nervous System, Noigroup Publica-tions, Adelaide, 2000.
[12] D. Butler and G. Moseley, Explain Pain, Noigroup Publica-tions, Adelaide, 2003.
[13] N. Buys and E. Kendall, Stress and Burnout among rehabili-tation counsellors within the context of insurance-based reha-bilitation: an institutional-level analysis, Australian Journalof Rehabilitation Counselling 4 (1998), 1–12.
[14] Campbell Research & Consulting, 2007/08 Australia and NewZealand Return to Work Monitor, North Fitzroy, Victoria,2008.
[15] E. Catalano and K. Hardin, The Chronic Pain Control Work-book, MJF Books, New York, 1996.
[16] M. Caudill, Managing Pain Before It Manages You, GuilfordPress, New York, 2002.
[17] C. Chapman, R.P. Tuckett and C.W. Song, Pain and stressin a systems perspective: Reciprocal neural, endocrine, andimmune interactions, The Journal of Pain 9 (2008), 122–145.
[18] J. Chibnall, R. Tait and S. Merys, Disability management oflow back injuries by employer-retained physicians: ratingsand costs, American Journal of Industrial Medicine 38 (2000),529–538.
[19] J. Clapton and E. Kendall, Autonomy and participation inrehabilitation: Time for a new paradigm? Disability andRehabilitation: An International, Multidisciplinary Journal24 (2002), 987–991.
[20] Cleveland Clinic, Psychogenic pain, 2009, Available: http://my.clevelandclinic.org/services/pain management/hic psychogenic pain.aspx [Accessed: 26.7.2009, 2009].
[21] Commonwealth of Australia, Disability Services Act, 1986.[22] J.E. Crisson and F.J. Keefe, The relationship of locus of control
to pain coping strategies and psychological distress in chronicpain patients, Pain 35 (1988), 147–154.
[23] M.M. Cunningham and C. Jillings, Individuals’ descriptionsof living with fibromyalgia, Clinical Nursing Research 15(2006), 258–273.
178 C. Wales et al. / Medically unexplained chronic pain in Australia
[24] R. Dantzer and K.W. Kelley, Twenty years of research oncytokine-induced sickness behavior, Brain, Behavior, & Im-munity 21 (2007), 153–60.
[25] J. Derrida, Aporias. Translated by Thomas Dutoit, StanfordUniversity Press, Stanford, 1994.
[26] G. Duncan, Mind-body dualism and the biopsychosocial mod-el of pain: what did Descartes really say? [see comment],Journal of Medicine & Philosophy 25 (2000), 485–513.
[27] G. Egan, The Skilled Helper: A Problem-Management andOpportunity-Development Approach to Helping (8th ed.),Thomson Brooks/Cole Publishing Co, Belmont, CA, 2007.
[28] I.J. Elenkov, R.L. Wilder, G.P. Chrousos and E.S. Vizi, Thesympathetic nerve–an integrative interface between two super-systems: the brain and the immune system, PharmacologicalReviews 52 (2000), 595–638.
[29] R. Gardner, Jr., Psychiatry needs a basic science titled socio-physiology, Biological Psychiatry 39 (1996), 833–834.
[30] R. Gardner, Jr. and J.S. Price, Sociophysiology and depression.[References], in: The Interactional Nature of Depression: Ad-vances in Interpersonal Approaches, T. Joiner and J.C. Coyne,eds, American Psychological Association, Washington, DC,1999, pp. 247–268.
[31] R. Grellman, Inquiry into Workers Compensation System inNSW, NSW Government, 1997.
[32] A.-C. Gullacksen and J. Lidbeck, The life adjustment processin chronic pain: Psychosocial assessment and clinical impli-cations, Pain Research & Management 9 (2004), 145–153.
[33] M.R. Gunnar, M.C. Larson, L. Hertsgaard, M.L. Harris et al.,The stressfulness of separation among nine-month-old infants:Effects of social context variables and infant temperament,Child Development 63 (1992), 290–303.
[34] L. Guy and S.D. Short, Rehabilitation of workers with mus-culoskeletal injury and chronic pain, Health Sociology Review14 (2005), 77–83.
[35] N.M. Hadler, If you have to prove you are ill, you can’tget well. The object lesson of fibromyalgia, Spine 21 (1996),2397–2400.
[36] K. Harkapaa, Relationship of psychological distress and healthlocus of control beliefs with the use of cognitive and behavioralcoping strategies in low back pain patients, Clinical Journalof Pain 7 (1991), 275–282.
[37] I. Holloway, B. Sofaer-Bennett and J. Walker, The stigmatisa-tion of people with chronic back pain, Disability & Rehabili-tation 29 (2007), 1456–1464.
[38] F.J.P.M. Huygen, A.G.J. De Bruijn, M.T. De Bruin, J.G. Groe-neweg, J. Klein and F.J. Zijistra, Evidence for local inflamma-tion in complex regional pain syndrome type 1, Mediators ofInflammation 11 (2002), 47–51.
[39] IASP, IASP pain terminology, 2008, Available: http://www.iasp-pain.org/AM/Template.cfm?Section=General ResourceLinks&Template=/CM/HTMLDisplay.cfm&ContentID=3058#Pain [Accessed: 19 Sept 2008, 2008].
[40] E. Kendall and J. Clapton, Time for a shift in Australian reha-bilitation? Disability & Rehabilitation 28 (2006), 1097–101.
[41] E. Kendall, H. Muenchberger and J. Clapton, Trends in Aus-tralian rehabilitation: Reviving its humanitarian core, Disabil-ity and Rehabilitation 29 (2007), 817–823.
[42] E. Kendall and A. Rogers, Extinguishing the social?: Statesponsored self-care policy and the Chronic Disease Self-management Programme, Disability & Society 22 (2007),129–143.
[43] N.A. Kendall and B.F. Thompson, A pilot program for dealingwith the comorbidity of chronic pain and long-term unem-ployment, Journal of Occupational Rehabilitation 8 (1998),
5–26.[44] D. Kenny, Barriers to return to work in New South Wales:
research findings and theoretical considerations, Universityof Sydney, Sydney, 1995.
[45] D.T. Kenny, Constructions of chronic pain in doctor-patientrelationships: Bridging the communication chasm, PatientEducation and Counseling 52 (2004), 297–305.
[46] N. Krause, L. Dasinger, L. Deegan, R. Brand and L. Rudolph,Alternative approaches for measuring duration of work dis-ability after low back injury based on administrative workers’compensation data, Amercan Journal of Industrial Medicine35 (1999), 604–618.
[47] R. Madden, Woodhouse after 40 years: Observations from anAustralian Participant, University of Auckland, 2007.
[48] F. Marchand, M. Perretti and S.B. McMahon, Role of theimmune system in chronic pain, Nature Reviews Neuroscience6 (2005), 521–532.
[49] D. Marks, Models of disability, Disability and Rehabilitation:An International, Multidisciplinary Journal 19 (1997), 85–91.
[50] P. McDonald and G. Withers, Population and Australia’s Fu-ture Labour Force, The Academy of the Social Sciences inAustralia, Canberra, 2008.
[51] B. McEwen, E.N. Lasley and E. Lasley, The End of Stress asWe Know It, 2002.
[52] C. Meares and A. Woodhouse, Compensation and rehabilita-tion in Australia: report of the National Committee of Inquiry,Commonwealth of Australia, Canberra, 1974.
[53] R. Melzack, The perception of pain, Scientific American 204(1961), 41–49.
[54] R. Melzack, From the gate to the neuromatrix, Pain Suppl 6(1999), S121–S126.
[55] R. Melzack, Pain and stress: a new perspective, in: Psychoso-cial Factors in Pain, R. Gatchel and D. Turk, eds, GuildfordPress, New York, 1999.
[56] R. Melzack and P.D. Wall, Pain mechanisms: a new theory,Science 150 (1965), 971–979.
[57] Motor Accidents Authority, The NSW Motor AccidentsScheme Information for Medical Practitioners and Health Pro-fessionals (Sydney, 2002).
[58] Motor Accidents Authority, Guidelines for the assessment ofthe degree of permanent impairment, Sydney, 2007.
[59] S. Nettleton, ’I just want permission to be ill’: Towards asociology of medically unexplained symptoms, Social Science& Medicine 62 (2006), 1167–1178.
[60] A. Neville-Jan, Encounters in a World of Pain: An Au-toethnography, American Journal of Occupational Therapy 57(2003), 88–98.
[61] M. Nielsen, Comment on Blyth et al., The contribution ofpsychosocial factors to the development of chronic pain: Thekey to better outcomes for patients? Pain 131 (2007), 348–349.
[62] M. Nielsen, Explicating the Social in the Biopsychosocialmodel of pain, Australian Pain Society Annual ScientificMeeting (Perth, Australia, 2008).
[63] P. Procacci and M. Maresca, Descartes’ physiology of pain,Pain 58 (1994), 133.
[64] K. Purse, The evolution of workers’ compensation policy inAustralia, Health Sociology Review 14 (2005), 8–20.
[65] J. Quintner, Personal Injury Compensation: Lessons fromTalmudic Law, Plaintiff (2004), 54–57.
[66] J. Quintner, M. Cohen, D. Buchanan, J. Katz and O.Williamson, Pain Medicine and Its Models: Helping or Hin-dering? Pain Medicine, 2007.
[67] R. Rothwell, The Development of Rehabilitation Services and

C. Wales et al. / Medically unexplained chronic pain in Australia 179
Rehabilitation Counselling in Australia, in: RehabilitationCounselling – Profession and Practice, J.L. Sheppard, ed.,Cumberland College of Health Sciences, Sydney, 1984.
[68] W. Saltzman, S.P. Mendoza and W.A. Mason, Sociophysi-ology of relationships in squirrel monkeys: I. Formation offemale dyads, Physiology & Behavior, 50 (1991), 271–280.
[69] D.J. Schofield, M.E. Passey, A. Earnest, I.C. Gloor and R.Shrestha, Are we getting healthier as we grow older? Implica-tions for babyboomer labor force participation, Annals of theNew York Academy of Sciences 1114 (2007), 230–240.
[70] H. Skuladottir and S. Halldorsdottir, Women in chronic pain:sense of control and encounters with health professionals,Qualitative Health Research 18 (2008), 891–901.
[71] J. Stone, W. Wojcik, D. Durrance, A. Carson, S. Lewis, L.MacKenzie, C.P. Warlow and M. Sharpe, What should wesay to patients with symptoms unexplained by disease? Thenumber needed to offend [see comment], BMJ 325 (2002),1449–1450.
[72] R.C. Tait, J.T. Chibnall, E.M. Andresen and N.M. Hadler,Disability determination: validity with occupational low backpain, Journal of Pain 7 (2006), 951–957.
[73] E.N. Thompson, Psychogenic pain; in whose mind? Pain 82(1999), 109–110.
[74] K. Toda, The terms neurogenic pain and psychogenic paincomplicate clinical practice, Clinical Journal of Pain 23(2007), 380–381.
[75] J. Tollefson, I live my life according to the pain: the livedexperience of chronic pain in adults living in rural Queensland,Unpublished School of Nursing, Midwifery and Nutrition,James Cook University, 2009.
[76] United Nations, Universal Declaration of Human Rights,1948, Available: http://www.un.org/Overview/rights.html[Accessed: 11.10.08].
[77] K. Uvnas-Moberg, Physiological and endocrine effects of so-
cial contact, in: The Integrative Neurobiology of Affiliation,C.S. Carter, I.I. Lederhendler and B. Kirkpatrick, eds, NewYork Academy of Sciences, New York, NY, 1997, pp. 146–163.
[78] M.T. van Leeuwen, F.M. Blyth, L.M. March, M.K. Nicholasand M.J. Cousins, Chronic pain and reduced work effective-ness: the hidden cost to Australian employers, European Jour-nal of Pain: Ejp 10 (2006), 161–166.
[79] Victorian Government, Partnership Case Study – AustralianCatholic University, 2002.
[80] Victorian Government, Partnership Case Study – Publicis Loy-alty, Call Centre Contractor to Qantas, 2002.
[81] Victorian Government, Partnership Case Study – RACV, De-partment of Industrial Relations, Melbourne, 2002.
[82] D.T. Wade and P.W. Halligan, Do biomedical models of illnessmake for good healthcare systems? BMJ 329 (2004), 1398–1401.
[83] L.R. Watkins and S.F. Maier, Immune regulation of centralnervous system functions: from sickness responses to patho-logical pain, Journal of Internal Medicine 257 (2005), 139–155.
[84] A. Werner, L.W. Isaksen and K. Malterud, I am not the kindof woman who complains of everything: Illness stories onself and shame in women with chronic pain, Social Science &Medicine 59 (2004), 1035–1045.
[85] WorkCover NSW, Overview. Improving outcomes: Integrated,active management of workers with soft tissue injury, NSWGovernment, Gosford NSW, 2008.
[86] WorkCover NSW, Information for Injured Workers, NewSouth Wales Government, Gosford, undated.
[87] M.R. Zuccolo, Comorbidity of pain symptoms and psychoso-cial stressors in archival message data of an online pain sup-port group, Unpublished, Mark R. Zuccolo, Northcentral U,US, 2008.




















