Pain Management in Physical Rehabilitation
35
Pain Management in Physical Rehabilitation Mary Ellen Goldberg BS, LVT, CVT, SRA, CCRA July/August Issue 2014 Objective: After reading this article the reader will be able to identify behaviors that are indicative of pain, become familiarized with various pain scales, understand the roles of the credentialed rehabilitation veterinarian and the credentialed rehabilitation veterinary technician in pain management and be familiar with physical modalities and manual techniques that have been found to provide pain relief. Since the October/November 2013 issue of the NAVTA Journal, the technician members of the American Association of Rehabilitation Veterinarians (AARV) have presented articles on various aspects of Physical Rehabilitation and the part that the rehabilitation certified veterinary technician/nurse plays in this practice. It is our sincere hope to have increased awareness and interest of veterinary technicians everywhere in the practice of physical rehabilitation. If you have an interest, please go to the AARV website, http://www.rehabvets.org/ , and join us. In this issue our rehabilitation topic covers pain management of the physical rehabilitation patient, whether postoperative, post injury, because of a disease state or because of the aging process. It is beyond the scope of this article to provide in- depth information about the neurophysiology of pain, neuropharmacology, and most drug doses. Additional reading resources are provided. What are the benefits of physical rehabilitation? 1,2 : Reduce pain Increase and maintain muscle strength and flexibility Joint mobility Promote and restore normal movement patterns Increase cardiovascular fitness Combat acute and chronic inflammatory processes Improve blood perfusion and consequently tissue growth Prevent adhesions, fibrosis and tissue retraction
Transcript of Pain Management in Physical Rehabilitation
Pain Management in Physical RehabilitationMary Ellen Goldberg BS, LVT, CVT, SRA, CCRAJuly/August Issue 2014
Objective: After reading this article the reader will be able to identify behaviors that are indicative of pain, become familiarized with various pain scales, understand the roles of the credentialed rehabilitation veterinarian and the credentialedrehabilitation veterinary technician in pain management and be familiar with physical modalities and manual techniques that havebeen found to provide pain relief.
Since the October/November 2013 issue of the NAVTA Journal, the technician members of the American Association of Rehabilitation Veterinarians (AARV) have presented articles on various aspects of Physical Rehabilitation and the part that the rehabilitation certified veterinary technician/nurse plays in this practice. It is our sincere hope to have increased awareness and interest of veterinary technicians everywhere in the practice of physical rehabilitation. If you have an interest, please go to the AARV website, http://www.rehabvets.org/, and join us.
In this issue our rehabilitation topic covers pain management of the physical rehabilitation patient, whether postoperative, post injury, because of a disease state or because of the aging process. It is beyond the scope of this article to provide in-depth information about the neurophysiology of pain, neuropharmacology, and most drug doses. Additional reading resources are provided.
What are the benefits of physical rehabilitation?1,2: Reduce pain Increase and maintain muscle strength and flexibility Joint mobility Promote and restore normal movement patterns Increase cardiovascular fitness Combat acute and chronic inflammatory processes Improve blood perfusion and consequently tissue growth Prevent adhesions, fibrosis and tissue retraction

Stimulate the nervous system and prevent neurapraxia Promote the healing process
Topping off the list of benefits of physical rehabilitation is “reduce pain”. Reviewing some of the human literature in evidence-based medicine for pain reduction and physical (rehabilitation) therapy:
1. “There is platinum level evidence that land-based therapeutic exercise has at least short term benefit in terms of reduced knee pain and improved physical function for people with knee Osteoarthritis”3.
2. “Extended exercises in water and swimming have been shown toreduce edema, inflammation, and peripheral neuropathic pain in a research model”4.
3. “The most effective and strongly supported treatment modality for patients with PFPS (Patellofemoral pain syndrome) is a combined physiotherapy program, including strength training of the quadriceps and hip abductors and stretching of the quadriceps muscle group”.5
The World Health Organization’s (1992) definitions for impairmentand disability are pertinent to veterinary patients. Impairment is defined as “Any loss or abnormality of psychological, physiological, or anatomic structure or function.” Disability is defined as “Any restriction (resulting from impairment) of ability to perform an activity in the manner or within the range considered normal for the species.”6 If modified function was just a response to nociception (a painful, injurious stimulus), then analgesic medications would be enough, however, this is often not the case.6 Musculoskeletal pain can be a part of any ofthe rehabilitation conditions stated above. The causes of musculoskeletal pain are not fully understood but likely involve inflammation, fibrosis, tissue degradation, and neurotransmitter and neurosensory disturbances, and may include central and peripheral hypersensitivity and impairment of descending inhibition of incoming nociceptive impulses.7

Remember that the credentialed physical rehabilitation veterinary technician is not to diagnose, prescribe, or perform procedures that are considered to be the practice of veterinary medicine; and will obey all individual state and regional laws and regulations pertaining to the field of veterinary physical rehabilitation.8
Veterinary physical rehabilitation is a discipline that encompasses the application of physical therapeutic and rehabilitation techniques (developed in humans) to animals whose comfort and function have been compromised in some way9. Generally, patients that present for rehabilitation therapy are reluctant to move. One of the major factors contributing to this reluctance is pain. “It is absolutely necessary that pain be controlled prior to initiation of physical rehabilitation.”10 Thecredentialed rehabilitation veterinarian (CCRT/CCRP/CVMRT) will be gathering information that will influence the veterinarian’s treatment choices for individual patients. Patients experiencing acute pain following orthopedic surgery have different needs thanthe elderly dog experiencing the chronic maladaptive pain associated with long-standing osteoarthritis9. Additionally, patients may present already being administered various pain medications that the rehabilitation veterinarian may consider changing. If it is at all possible the rehabilitation veterinarian should be in contact with the surgeon before a surgical patient is referred for rehabilitation so that they are aware of the perioperative pain management plan. An excellent review of multimodal pharmaceutical management of pain can be found in Canine Sports Medicine and Rehabilitation, 2013.11
While it is important for the credentialed rehabilitation veterinary technician/nurse to know and understand pain neurophysiology, neuropharmacology, and most drug doses, what is the main job that they will have as far as pain management is concerned? As quoted from the NAVTA Journal article December/January 201412, “Pain plays a role in any patient’s willingness and motivation. A patient’s pain score should be assessed and documented in the medical record during each visit.13 A detailed history should indicate the degree of pain and the disability14. How does the patient cope with the disability? If changes in a patient’s pain level are noted, the
supervising veterinarian should be notified immediately. It is very important for the rehabilitation veterinary technician to remain in open communication with their supervisor about anythingabnormal or any changes in progress.”12
Recognition and Assessment of PainPain is an unpleasant sensory and emotional experience associatedwith actual or potential tissue damage, or described in terms of such damage15. Pain motivates us to withdraw from potentially damaging situations, protect a damaged body part while it heals, and avoid those situations in the future 16. It is initiated by stimulation of nociceptors in the peripheral nervous system, or by damage to or malfunction of the peripheral or central nervous systems 17. Most pain resolves promptly once the painful stimulus is removed and the body has healed, but sometimes pain persists despite removal of the stimulus and apparent healing of the body;and sometimes pain arises in the absence of any detectable stimulus, damage or pathology 18.Recognizing pain and assessing its intensity are both essential for its effective management. If pain is not recognized, then it is unlikely to be treated; failure to appreciate the intensity ofpain will hamper the selection of an appropriately potent analgesic, raise doubts about the effectiveness of the administered dose, and result in less than optimal treatment.19 A reliable method of pain assessment allows an appropriate analgesic regimen to be used and effectively evaluated.
Assessment of pain or distress may be based on many different criteria including:20
Decreased activity Abnormal postures, hunched back, muscle flaccidity or
rigidity Poor grooming Decreased food or water consumption Decreased fecal or urine output Weight loss (generally 20-25% of baseline), failure to grow,
or loss of body condition (cachexia) Dehydration
Decrease or increase in body temperature Decrease or increase in pulse or respiratory rate Physical response to touch (withdrawal, lameness, abnormal
aggression, vocalizing, abdominal splinting, increase in pulse or respiration)
Teeth grinding (seen in rabbits and farm animals) Self-aggression Inflammation Photophobia Vomiting or diarrhea Objective criteria of organ failure demonstrated by
hematological or blood chemistry values, imaging, biopsy, orgross dysfunction
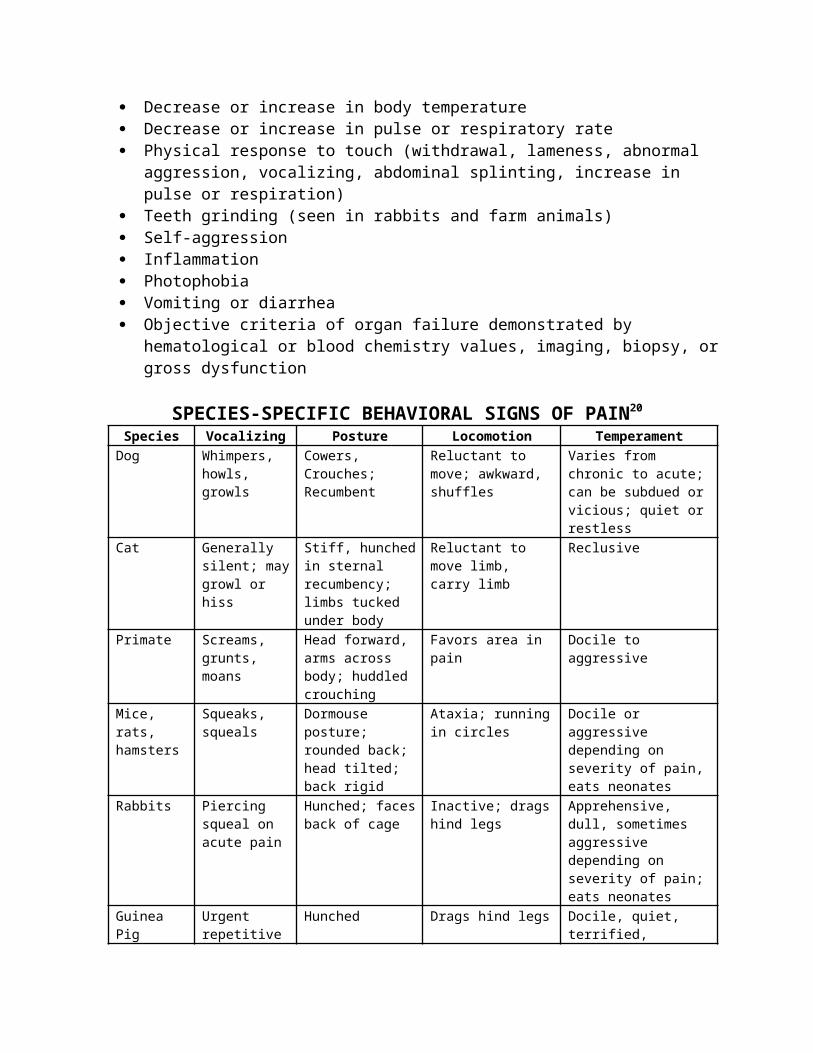
SPECIES-SPECIFIC BEHAVIORAL SIGNS OF PAIN20 Species Vocalizing Posture Locomotion Temperament Dog Whimpers,
howls, growls
Cowers, Crouches; Recumbent
Reluctant to move; awkward, shuffles
Varies from chronic to acute;can be subdued orvicious; quiet orrestless
Cat Generally silent; maygrowl or hiss
Stiff, hunchedin sternal recumbency; limbs tucked under body
Reluctant to move limb, carry limb
Reclusive
Primate Screams, grunts, moans
Head forward, arms across body; huddled crouching
Favors area in pain
Docile to aggressive
Mice, rats, hamsters
Squeaks, squeals
Dormouse posture; rounded back; head tilted; back rigid
Ataxia; runningin circles
Docile or aggressive depending on severity of pain,eats neonates
Rabbits Piercing squeal on acute pain
Hunched; facesback of cage
Inactive; dragshind legs
Apprehensive, dull, sometimes aggressive depending on severity of pain;eats neonates
Guinea Pig
Urgent repetitive
Hunched Drags hind legs Docile, quiet, terrified,

squeals agitatedHorses Grunting,
nicker Rigid; head lowered
Reluctant to move; walk in circles "up & down" movement
Restless, depressed
Chickens Gasping Stand on one foot, hunched huddled
None Lethargic, allowshandling
Cows, calves, goats
Grunting; grinding teeth
Rigid; head lowered; back humped
Limp; reluctantto move the painful area
Dull, depressed; act violent when handled
Sheep Grunting; teeth grinding
Rigid; head down
Limp; reluctantto move the painful area
Disinterested in surroundings; dull, depressed
Pigs From excessive squealing to no soundat all
All four feet close togetherunder body
Unwilling to move; unable tostand
From passive to aggressive depending on severity of pain
Birds Chirping Huddled, hunched
From excessive movement to tonic immobility depending on severity of pain
Inactive; drooping, miserable appearance
Fish None Clamped fins; pale color; hiding; anorexia
None unless forced; if a schooling fish;will separate itself from others
First sign to occur is anorexia; lethargic; stressed easily
Amphibians
None Closed eyes; color changes;rapid respirations
Immobility; lameness
Anorexia; aggressive;
Reptiles Hiss; grunting
Hunched; hiding; color change
immobility unless forced
Anorexia; aggressive; lethargic; avoidance
This chart is meant to display some of the different signs species may exhibitif in pain. Individuals may not show any of these signs or they show signs notlisted. This is meant as a general guide. Table developed by MEGoldberg
The most common approach to pain assessment is the use of charts and scales.
Are their limitations to Pain Scales21?1. Pain scales should be used in conjunction with a thorough
physical exam and history to assess every patient2. Recognize that all pain scales have limitations3. Individual patient behavior may dictate prompt pain relief,
regardless of the pain score4. Caregivers should strive for low pain scores in a
comfortable appearing patient
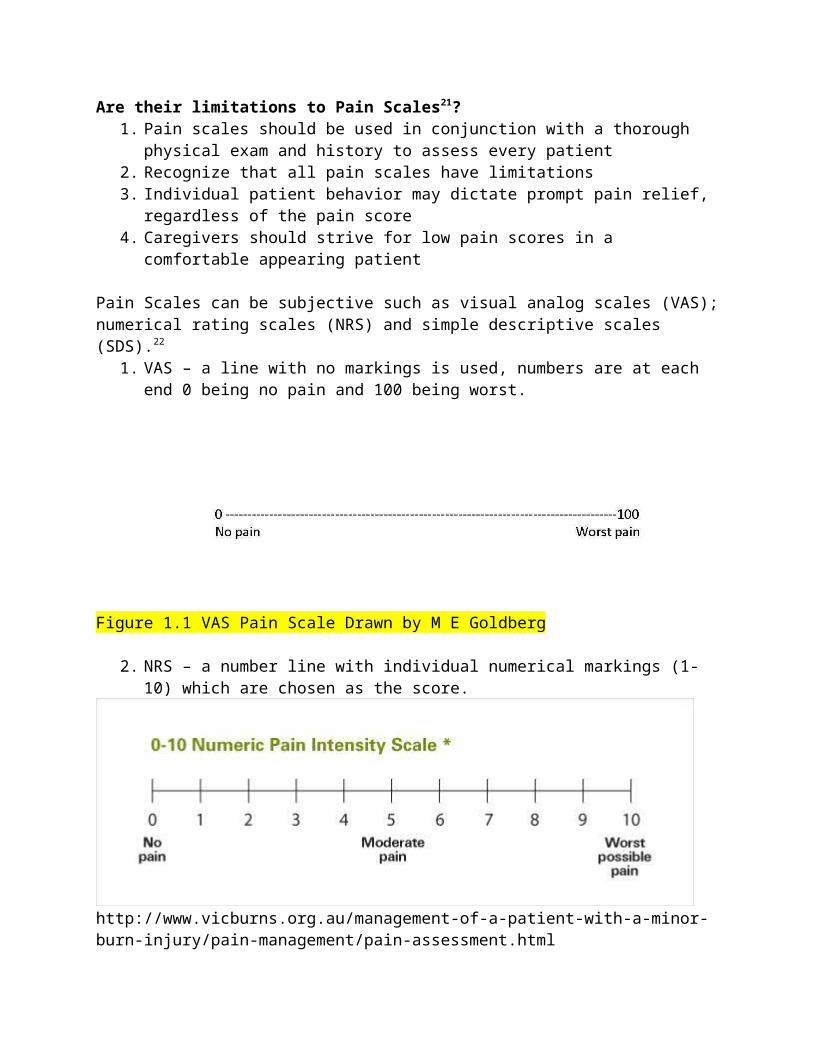
Pain Scales can be subjective such as visual analog scales (VAS);numerical rating scales (NRS) and simple descriptive scales (SDS).22
1. VAS – a line with no markings is used, numbers are at each end 0 being no pain and 100 being worst.
Figure 1.1 VAS Pain Scale Drawn by M E Goldberg
2. NRS – a number line with individual numerical markings (1-10) which are chosen as the score.
http://www.vicburns.org.au/management-of-a-patient-with-a-minor-burn-injury/pain-management/pain-assessment.html
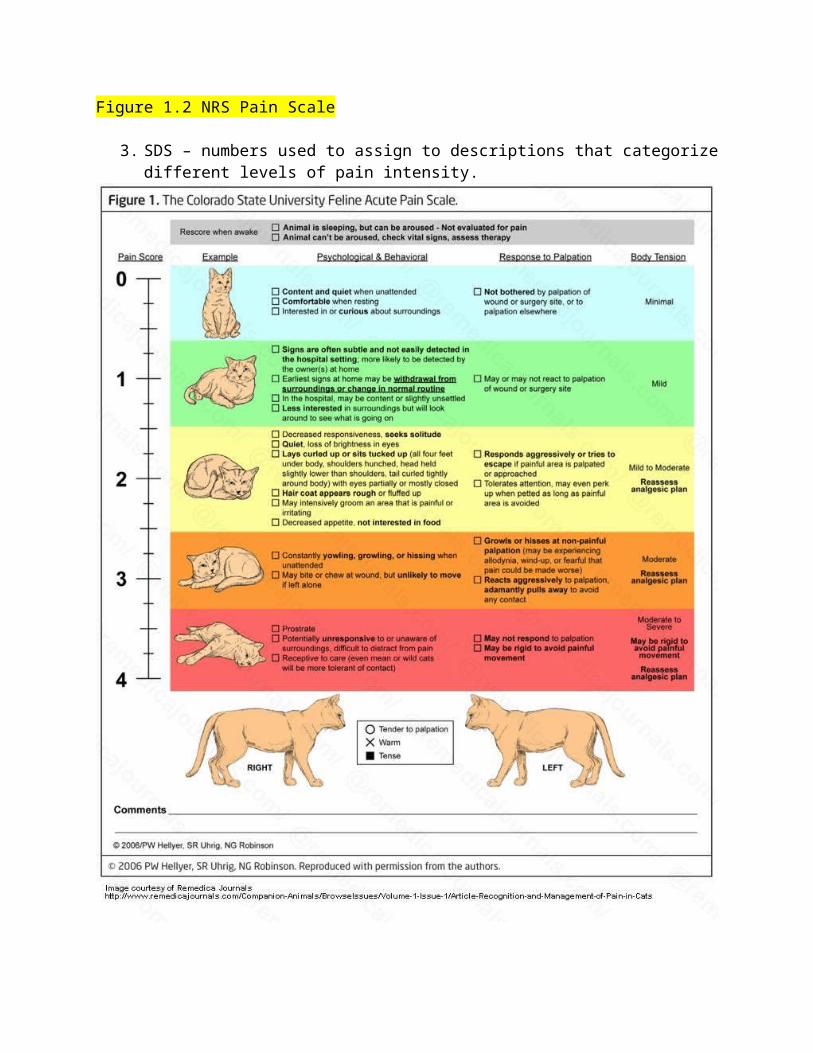
Figure 1.2 NRS Pain Scale
3. SDS – numbers used to assign to descriptions that categorizedifferent levels of pain intensity.
Figure 1.3 SDS Pain Scale - Typical feline acute pain scale used in veterinary practice With permission
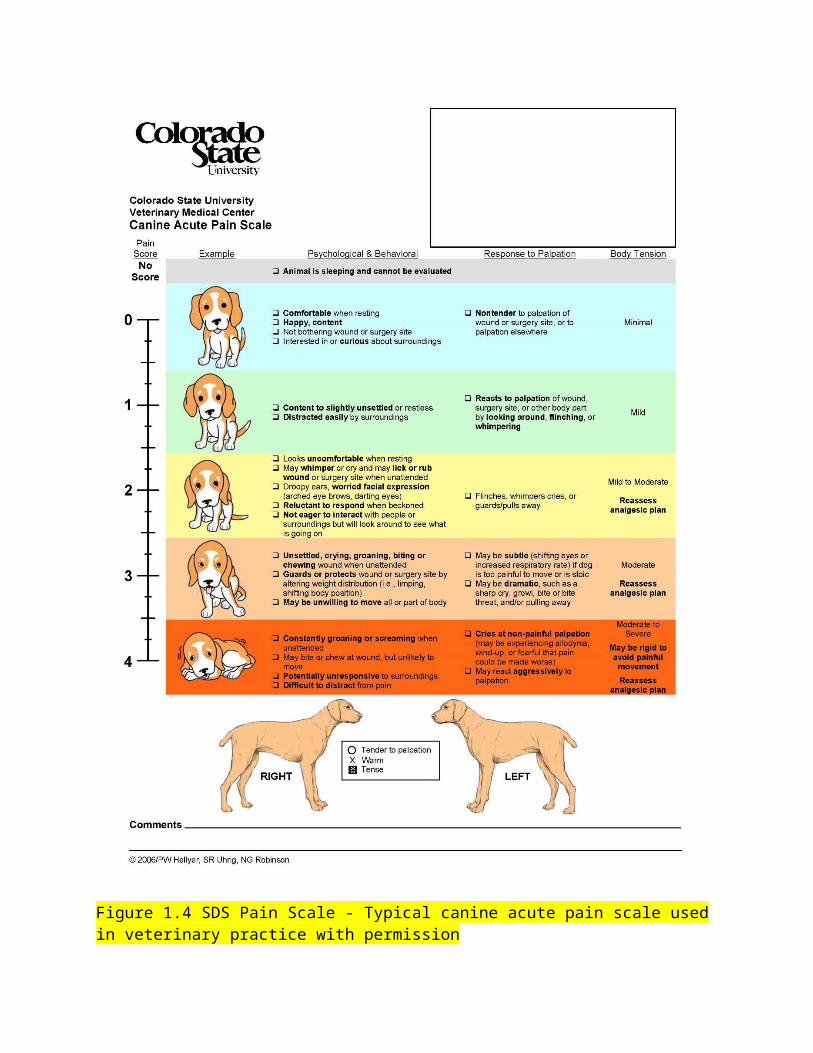
Figure 1.4 SDS Pain Scale - Typical canine acute pain scale used in veterinary practice with permission

Pain scales can be objective such as the Glasgow Composite Pain Scale. “A pain scale that takes into account the various dimensions of pain is thought to be more useful in indicating howmuch the pain "meant" to the animal, but VAS, NRS and SDS scales are unidimensional. A pain scale should ideally be multidimensional, in that several aspects of pain intensity & pain related disability are included and question especially the dynamic aspects. The Glasgow CPS is thought to be Multidimensional.”23

Figure 1.5 Glasgow Composite Pain ScalePermissions sent to [email protected].
Several Chronic Pain Scales have been developed for dogs namely:Canine Brief Pain IndexHelsinki Chronic Pain Index (HCPI)Cincinnati Orthopedic Disability Index (CODI)Liverpool Osteoarthritis in Dogs (LOAD)Instrument and Questionnaire
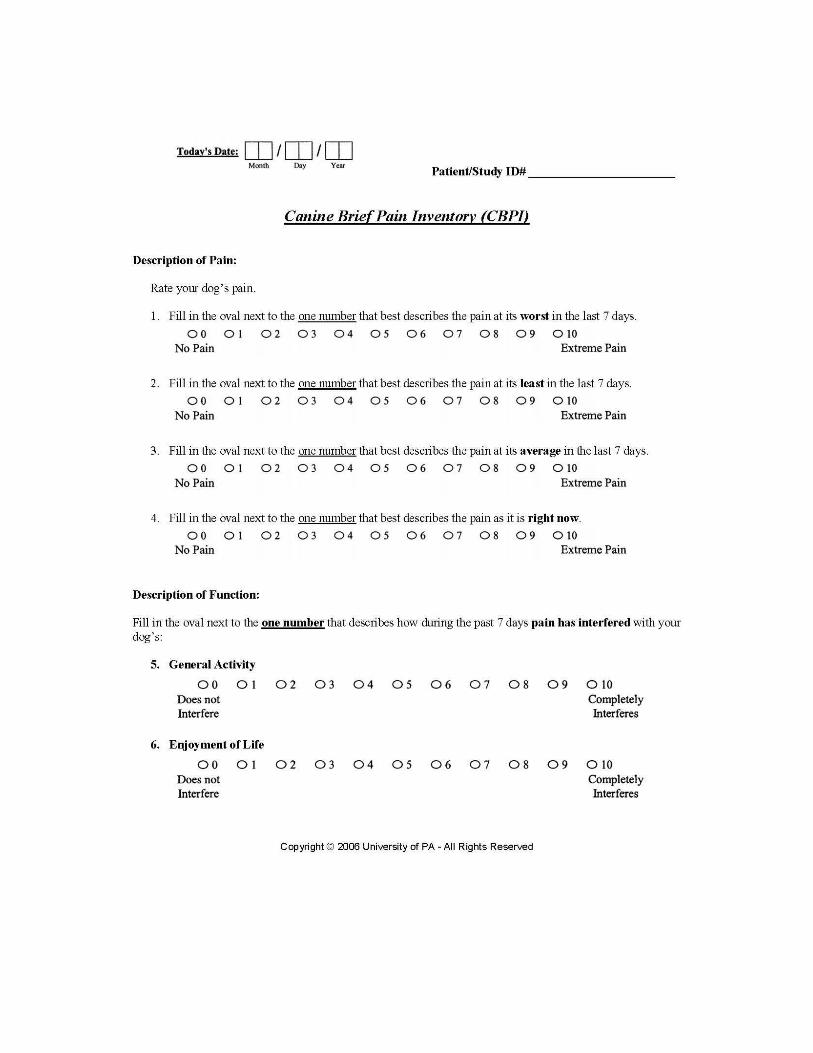
Figure 1.6 University of Pennsylvania Canine Brief Pain Inventory(CBPI)Permissions sent and receivedTo date there are no validated chronic pain scales for cats.24 There is one paper by Lascelles et al.25 that compared a client-specific outcome measure questionnaire with an activity monitor for ability to characterize impairment in 13 cats. Additional questionnaires and studies with cats have been completed, but as of now have yet to develop a validated chronic pain scale.26, 27, 28,
29
Using Pain Scoring Effectively Have same person evaluate the patient Request VAS readings as treatments Assess behavior Assess body posture, activity and position in cage Evaluate response to approach Interact with patient Palpation of Surgical Site Ask patient to ambulate, if appropriate Ask patient to eat, if appropriate
To Summarize:No single pain scoring system is right for all practices or facilities. In fact, it is not as important which system you choose as it is to simply choose one system to be used by the entire team. Once a pain scoring system is chosen, apply it! At every single visit, assess the animal for pain and record the finding in the medical record. Each individual pain assessment isimportant; for a patient with chronic pain, trends are even more important because they tell us whether the patient’s pain is improving or worsening. Similarly, surgical patients with acute pain need to be assessed at regular intervals (possibly every 2-4hours immediately postoperatively) and thereafter twice daily with the results recorded in the medical record. Trends allow theteam to understand the success of a perioperative pain managementplan. Owners should be taught how to pain score their pet. Encourage the owner to keep a chart of their pet’s pain.

When should your patient be assessed for pain?New patients should have a detailed history to correctly identifythe animal’s degree of pain and disability. Identifying how the patient copes with daily living activities creates a realistic picture of the patient’s disability. Information regarding the following should be gathered30:
Ability to ascend and descend stairs Ability to enter and exit vehicles Ability to cope with difficult surfaces such as wooden or
tiled floors Ability to remain standing while eating Willingness to exercise and exercise tolerance Ability to remain squatting while defecating Ability to posture for urination Inappropriate elimination Willingness to play Change in demeanor Response to grooming Response or lack thereof to medication Effect of exercise on the lameness/pain Effect of rest on the lameness/pain Duration and intensity of the lameness/pain Changes in sleep patterns
One of the first questions you should ask the client (whether newor long standing) is ‘has your pet appeared painful?’ If the pet is on pain medication then you should ask what medications these are and the dosages. Each time the patient is seen the client should be asked about any changes to medications or stoppage of aspecific type of medication. Good communication will improve outcome, and recent studies have shown that the relationship between the clinician and the patient and owner is of primary importance in successful management of chronic pain.31, 32 During the certified rehabilitation therapist or practitioner’s clinical evaluation, several items will be assessed33:
A. Static Assessment - assessment of muscle hypertrophy or atrophy, head and tail position, abdominal muscle tone, scarring or swelling, symmetry of the axial and appendicularskeleton, deviation in the sagittal plane of the thoracic
and lumbar spine or lordosis or kyphosis, distribution of body weight among all four limbs, and any adduction or abduction of the limbs in the animal at rest. A Gulick tape measure will be useful for atrophy measurement and this willbe a test that you can perform for your rehabilitation therapist/practitioner
Figure 1.7 Gulick Tape Measurehttp://www.shopmedvet.com/product/80461/jorgensen-laboratories
B. Dynamic Assessment - Dynamic assessment involves moving the limbs and noting reactions and resistance in the muscles as joints are flexed and extended or limbs are advanced and retracted, observing the patient as it moves from standing to sitting and vice versa, and assessing quality and controlof movement. Symmetry of the animal when sitting, and any tendency to lean or to brace with the forelimbs, is assessed.

C. Gait Assessment - This portion of the assessment allows grading of the severity of the lameness, localization of thelameness, and description of the gait in terms of cranial and caudal phases, arc of flight, and linearity of the movement.
D. Neurological Examination - A neurological examination shouldbe part of the assessment to help differentiate poor balancedue to stiffness and pain from ataxia due to a neurological lesion, as each has different rehabilitation requirements and prognosis.
E. Palpation and Range of Motion - Palpation and manipulation should occur with the patient during standing and in lateralrecumbency. It is best to develop a systematic approach: palpate muscles for their overall symmetry, texture, and tone, presence of edema, trigger point formation, and the presence of lactic acid, which confers a feeling of crackling tissue paper within the muscle.
F. Range of Motion and End Stop Assessment of Joints - Range ofmotion within a joint is the degree of motion that joint is capable of undergoing from full flexion to full extension inthe sagittal plane. It can also be used to describe the degree of abduction and adduction afforded to an individual joint. Range of motion is measured with a manual or laser goniometer.

Figure 1.8 Veterinary Goniometerhttp://www.kennelandpaddock.com/photo-gallery
The credentialed rehabilitation veterinary technician will be assisting with various aspects of all of these assessments.
Commonly used rehabilitation techniques that aid with pain management are:34
Cryotherapy Thermotherapy Therapeutic exercises Transcutaneous electrical nerve stimulation (TENS) or
Neuromuscular electrical stimulation (NMES) Low level laser therapy (LLLT) Pulsed electromagnetic field therapy (PEMF) Extracorporeal shock wave treatment (ESWT) Acupuncture Manual therapies – massage, mobilizations, manipulations
Environmental modifications35
By having a conversation with the client, you can help to determine if some simple modifications to the home environment will aid mobility and reduce pain. Slippery floors are detrimental to the aging patient. Nonskid area rugs, flooring used in children’s play areas and rubber-backed mats are examplesof how the owner can make the home more comfortable for a painfulpatient. Raising the water and food bowl off the floor and standing on a nonskid surface makes mealtime more comfortable.
Ramps can be utilized for getting into and out of vehicles. Childrestraint gates may be useful at the top and bottom of stairs. Memory foam or egg-shell foam may help make sleeping more comfortable. Slings and assistive devices may be helpful.
Painful Mobility Issues in GeriatricsDr. Julia Tomlinson BVSc, MS, PhD, DACVS, CCRP, CVSMT, DACVSMR states that in her practice she sees two types of geriatric pets with painful mobility issues: the aging, often overweight pet with little systemic disease and varying amounts of physical disability; and the extremely frail, geriatric pet with reduced
appetite, weight loss, concurrent diseases, and more extreme lossof strength and mobility.36 Pain needs to be well controlled before strengthening begins so first she works on improving pain and flexibility.36 Very simple techniques such as range of motion (ROM) exercises and stretching can be taught to clients. Handoutswith pictures are very helpful and can be referred back to when the therapist is not there to give advice.36 The exercises MUST be demonstrated for the client and then have the client repeat the exercise back to the demonstrator to ensure it is being performed properly. “Pain during the motion must be avoided as much as possible and the fine art of pushing enough but not too much is a difficult one to teach”.36 It is not until several weeks of this therapy has been completed that Dr. Tomlinson will move on to strengthening and balance exercises.
Feline Physical RehabilitationCats can benefit from appropriately planned rehabilitation techniques. Compliance with treatment is often less predictable than with dogs, and the success of therapy with cats demands a good understanding of feline behavior, coupled with excellent handling skills.37, 38 Points to remember about rehabilitation with cats39:
Physiotherapy and rehabilitation with cats requires a calm, confident approach. Treatment time should be kept to a minimum to prevent boredom and minimize handling. Competentand confident manual skills are essential to ensure effective treatment. Use a hands-off approach whenever possible.
Treatment is best carried out in a quiet, calm environment with no distractions. Owner assistance can aid effectivenessof treatment and can ensure continuation of therapy between formal treatment sessions.
Cats can be more cooperative with therapy than is often perceived. Do not disregard certain treatment modalities just because you think a cat would not accept the treatment – you may be surprised!
Ensure that pain is not a restriction to the performance of a treatment or exercise. Adequate pain relief is essential for effective therapy. Repetitive attempts to perform a treatment on a cat that is in pain are doomed to failure, and may create resistance to any further attempts at the same treatment.
Any physiotherapy and rehabilitation program should be tailored to the patient, based on the individual cat’s identified problems and needs.
Cats in pain may40, 41: Have decreased grooming Be reluctant to jump Have an inability to jump as high as before Urinate or soil outside the litter box Have increased or decreased sleep time Avoid human interaction Hide Dislike being stroked or brushed Inappropriate activity level Sitting in the back of the kennel Mental attitude/demeanor (stupor or anxiety) Changes in attitude/personality Lack of comfort when palpated Facial expression Staring, fixed gaze Dilated pupils Lack of appetite and thirst Self-mutilation Vocalizations Posture Tachycardia Tachypnea
Two excellent articles from the Journal of Feline Medicine and Surgery about feline rehabilitation can be found in the references.37, 39
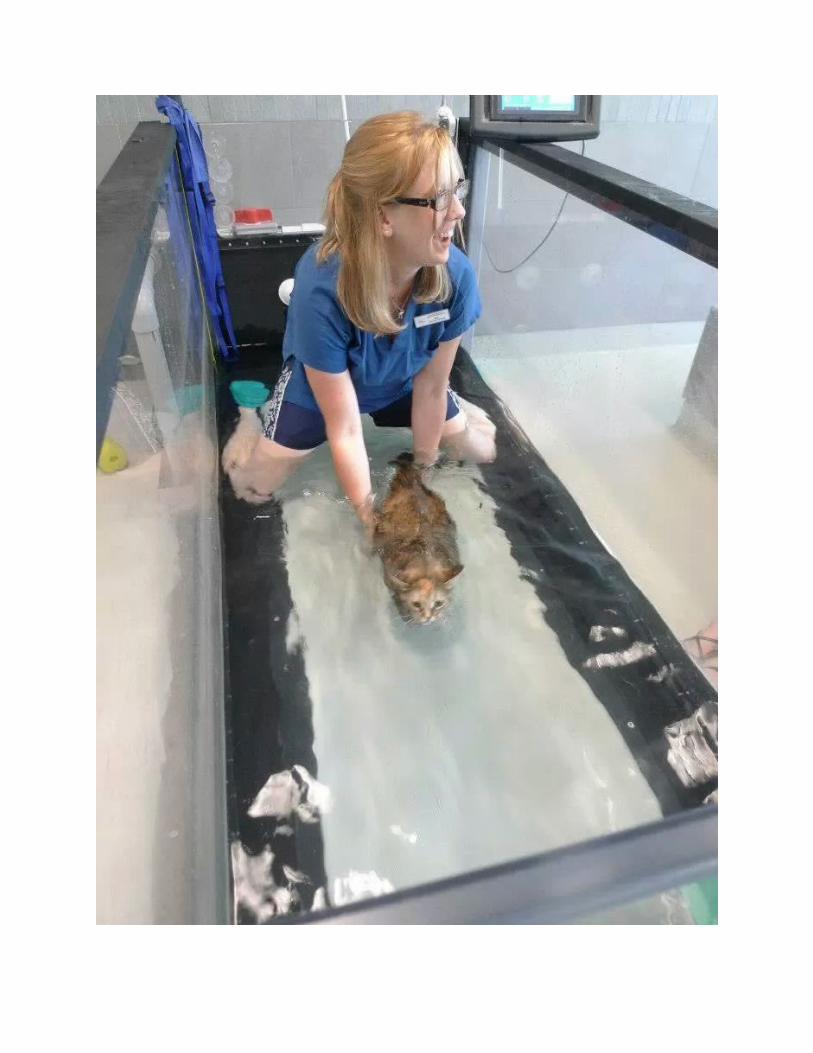
Figure 1.9 Jenn Panko RAHT, CCRP (COCM) performing underwater treadmill therapy on a cat.
Equine RehabilitationEquitation involves close contact between horse and rider. Most presenting horses are athletes of some form, thus the rider expects a full return of function. Because of this, the CertifiedEquine Rehabilitation Practitioner (CERP) must evaluate the horse, the farrier, the saddle fit and the role of the rider in causing or magnifying the lameness.42 The rider may need to undergo their own rehabilitation program if problems are caused by the rider’s posture and balance.
Pain Assessment for Horses43
Behavioral changes that are associated with pain in the horse mayinclude kicking or biting when the tender area is touched, generalized restlessness, sweating, frequent movement of the painful limb, or continuous shifting of weight from one limb to another. Changes associated with back pain, such as poor performance, poor appetite, and slight changes in demeanor may bevery subtle initially. These may progress to tail swishing or holding the tail to one side, bruxism, head shaking, resistance to saddling and grooming, loss of flexibility, stumbling, bucking, and rearing.44, 45 The horse may be withdrawn and the abdomen may have tight abdominal muscles or appear to be “tucked-up”. The horse’s breed and temperament must also be assessed.Objective measurements of pain in the horse that may be of assistance in diagnosing and treating pain include heart rate (not consistently increased in pain), respiratory rate, pressure algometry, thermography, kinematic gait analysis, and response toanalgesia (e.g. nerve blocks).43 Many times the horse is placed on analgesics (usually just NSAIDS) as a trial to see if pain is present. If the problem does not improve with this single medication, then the horse is often incorrectly declared to not be in pain. This can lead to is much more severe riding or controlling techniques (e.g. double twisted wire bit) being used on a painful horse in order to ‘control’ perceived bad behavior when the problem is actually a normal response to pain.43
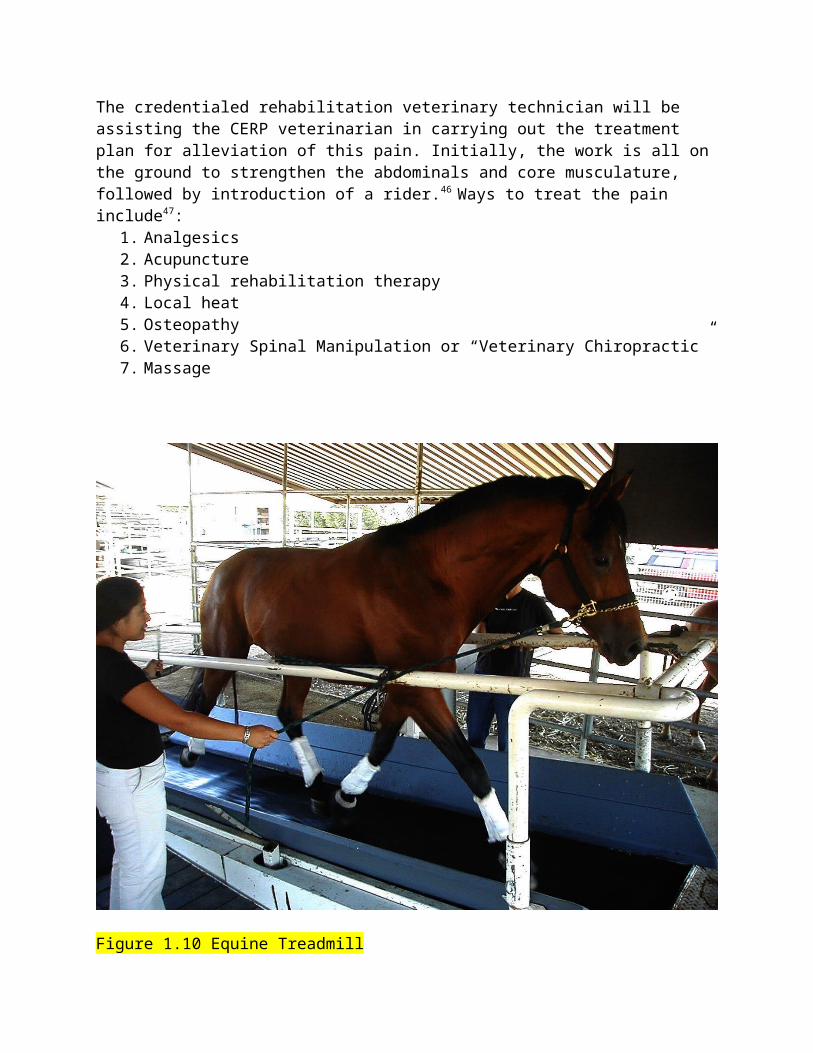
The credentialed rehabilitation veterinary technician will be assisting the CERP veterinarian in carrying out the treatment plan for alleviation of this pain. Initially, the work is all on the ground to strengthen the abdominals and core musculature, followed by introduction of a rider.46 Ways to treat the pain include47:
1. Analgesics2. Acupuncture3. Physical rehabilitation therapy4. Local heat5. Osteopathy6. Veterinary Spinal Manipulation or “Veterinary Chiropractic”7. Massage
Figure 1.10 Equine Treadmill
http://theequinecenter.com/wp-content/uploads/2010/08/treadmill1.jpg
ConclusionThe certified rehabilitation veterinarian, certified rehabilitation veterinary technician, physical therapist and owner must work as a team to have successful management of pain and restore the patient (no matter what species) to a functional life. Each animal should have its own tailored plan. Nothing should be “cook-book” in this process. The ultimate aim should beto restore the patient to an active and pain free lifestyle, whether this is in the context of a slow leisurely walk or full athletic activity.48
References
1. Sharp B. Physiotherapy in small animal practice. In Practice (2008) 30, 190-199.
2. Riviere S. Physiotherapy for cats and dogs applied to locomotor disorders of arthritic origin. Veterinary Focus 2007 17 (3) pgs: 32-36.
3. Fransen M, McConnell S. Exercise for osteoarthritis of the knee (Review) The Cochrane Library Published by JohnWiley & Sons, Ltd. 2008, Issue 4 pgs: 1-95.
4. Akyuz G, Kenis O: Physical therapy modalities and rehabilitation techniques in the management of neuropathic pain. Am J Phys Med Rehabil 2014;93:253Y259.
5. Rixe JA Glick JE Brady J Olympia RP A review of the management of patellofemoral pain syndrome The Physician and sports medicine. 2013,Vol.41(3),p.19-28.
6. Davies L. Chapter 11 Canine Rehabilitation. Pain Management inVeterinary Practice. Editors: Egger C, Love L, Doherty T. John Wiley & Sons, Inc. Ames, IA 2014 pg 133.
7. IASP (2009) Exercise in the management of musculoskeletal pain. Arendt-Nielsen, L., Barbe, M.F., Bement, M.H., et al. IASP web resource. www.iasp-pain.org.
8. Rehabilitation Veterinary Technicians: Who we are. National Association of Veterinary Technicians in America Journal, October/November2013 issue. Pg: 31.
9. Fox SM and Downing R. Chapter 14 Rehabilitating the Painful Patient: Pain Management in Physical Rehabilitation. Canine Rehabilitation and Physical Therapy 2nd Edition. Darryl L. Millis and David Levine. Saunders/Elsevier. China; 2014, pg 243-253.
10. Dr. Robin Downing – personal communication, 2013.
11. Epstein M. Chapter 19 The Prevention and Management of Pain in Dogs. Canine Sports Medicine and Rehabilitation. Editors: M. C. Zink and Janet B. Van Dyke. John Wiley & Sons, Inc. Ames,IA. 2013. Pgs: 370-388.
12. White E. Certified Veterinary Rehabilitation Technicians: What Do We Do? NAVTA Journal Dec/Jan issue 2014. Pgs: 31-36.
13. AARV Model Standards for Veterinary Physical Rehabilitation Practice http://www.rehabvets.org/model_standards.lasso (accessed 11/3/2013)
14. Davies L. Chapter 11. Canine Rehabilitation in Pain Management in Veterinary Practice, First Edition. Edited by Christine M. Egger, Lydia Love and Tom Doherty. John Wiley and Sons, INC. Ames, IA. Pg 134
15. International Association for the Study of Pain Retrieved 6 October 2009. This often quoted definition was first formulated by an IASP Subcommittee on Taxonomy Bonica,JJ (1979). "The need of a taxonomy". Pain 6 (3): 247–252.
16. 5. Lynn, B (1984) "Cutaneous nociceptors" in Holden, AV& Winlow, W The neurobiology of pain. Manchester, UK: Manchester University Press. p. 106.
17. 6. Woolf, CJ & Mannion, RJ (1999) "Neuropathic pain: aetiology, symptoms, mechanisms and management". The Lancet 353 (9168): 1959–1064.
18. 7. Raj, PP (2007) "Taxonomy and classification of pain"in Kreitler, S; Beltrutti, D; Lamberto, A et al. The handbookof chronic pain. New York: Nova Science Publishers Inc.
19. National Academy of Sciences, Chapter 3: Recognition and Assessment. Recognition and Alleviation of Pain in Laboratory Animals. National Academies Press, Washington DC. 2009. Pg 47.
20. Goldberg ME. The Fourth Vital Sign in All Creatures Great and Small. North American Veterinary Technician’s Association Journal, Winter 2010, pg 31- 54.
21. Fox SM. Chapter 3 Pain Assessment in Small Animal Medicine. Pain Management in Small Animal Medicine. Taylor and Francis Group; CRC Press, Boca Raton, FL. 2014, pg: 27-45.
22. Goldberg ME. The Fourth Vital Sign in All Creatures Great and Small. North American Veterinary Technician’s Association Journal, Winter 2010, pg 31- 54.
23. Karas A. PAIN, ANXIETY, OR DYSPHORIA - HOW TO TELL? A VIDEO ASSESSMENT LAB. https://www.acvs.org/files/proceedings/2011/data/papers/174.pdf, Proceedings from the American College of Veterinary Surgeons, 2011.
24. Sekel K. Chapter 24 The Recognition and Assessment of Pain in Cats. Pain Management in Veterinary Practice. Editors: Egger
C, Love L, Doherty T. John Wiley & Sons, Inc. Ames, IA 2014 pg 269-273.
25. Lascelles, B.D.X., Bernie, H.D., Roe, S., et al. Evaluation of client-specific outcome measures and activity monitoring to measure pain relief in cats with osteoarthritis. Journal of Veterinary Internal Medicine, 2007, 21, 410–416.
26. Bennett, D. & Morton, C.A. A study of owner observed behavioural and lifestyle changes in cats with musculoskeletal disease before and after analgesic therapy. Journal of Feline Medicine and Surgery, 2009, 11, 997–1004
27. Zamprogno, H., Hansen, B.D., Bondell, H.D., et al. Itemgeneration and design testing of a questionnaire to assess degenerative joint disease-associated pain in cats. American Journal of Veterinary Research, 2010, 71(12), 1417–1424.
28. Slingerland, L.I., Hazewinkel, H.A.W., Meij, B.P., et al. Crosssectional study of the prevalence and clinical features of osteoarthritis in 100 cats. Veterinary Journal, 2011, 187, 304–309.
29. Vainionpaa, M.H., Raekallio, M.R., Junnila, J.J.T., et al. A comparison of thermographic imaging, physical examination and modified questionnaire as an instrument to assess painful conditions in cats. Journal of Feline Medicine and Surgery, 2012 15(2) 124–131.
30. Davies L. Chapter 11. Canine Rehabilitation in Pain Management in Veterinary Practice, First Edition. Edited by Christine M. Egger, Lydia Love and Tom Doherty. John Wiley and Sons, INC. Ames, IA. Pg 134
31. Davies L. Chapter 11. Canine Rehabilitation in Pain Management in Veterinary Practice, First Edition. Edited by Christine M. Egger, Lydia Love and Tom Doherty. John Wiley and Sons, INC. Ames, IA. Pg 135
32. Jamison, R.N., 2011. Nonspecific treatment effects in pain medicine. IASP Pain Clinical Updates, XIX(2), 1–7.
33. Davies L. Chapter 11. Canine Rehabilitation in Pain Management in Veterinary Practice, First Edition. Edited by Christine M. Egger, Lydia Love and Tom Doherty. John Wiley and Sons, INC. Ames, IA. Pg 135-136
34. Fox SM. Chapter 3 Pain Assessment in Small Animal Medicine. Pain Management in Small Animal Medicine. Taylor and Francis Group; CRC Press, Boca Raton, FL. 2014, pg: 243
35. Fox SM. Chapter 3 Pain Assessment in Small Animal Medicine. Pain Management in Small Animal Medicine. Taylor and Francis Group; CRC Press, Boca Raton, FL. 2014, pg: 244
36. Tomlinson J. E. REHABILITATION AND PAIN MANAGEMENT AS AGING WELLNESS STRATEGIES. Proceedings North American Veterinary Conference 2012. 1065-1066.
37. Sharp B. FELINE PHYSIOTHERAPY AND REHABILITATION: 1. Principles and potential. Journal of Feline Medicine and Surgery (2012) 14, 622–632
38. Overall KL. Normal feline behavior. In: Clinical behavioral medicine for small animals. St Louis: Mosby, 1997, pp 45–7
39. Sharp B. Feline Physiotherapy and Rehabilitation: 2. Clinical application. Journal of Feline Medicine and Surgery (2012) 14, 633–645
40. Robertson SA. Osteoarthritis in Cats. Veterinary Medicine. Advanstar Communications, Novemeber 1, 2008. http://veterinarymedicine.dvm360.com/vetmed/Feline+Center/Osteoarthritis-in-cats-What-we-now-know/ArticleStandard/Article/detail/564437
41. Scherk M. ANALGESIA FOR FELINE ARTHRITIS, Illinois State Veterinary Medical Association (ISVMA) Annual Conference Proceedings, 2012.
42. Davies L. Chapter 12 Equine Rehabilitation. Pain Management in Veterinary Practice, First Edition. Edited by Christine M. Egger, Lydia Love and Tom Doherty. John Wiley and Sons, INC. Ames, IA. Pg 147.
43. Davies L. Chapter 12 Equine Rehabilitation. Pain Management in Veterinary Practice, First Edition. Edited by Christine M. Egger, Lydia Love and Tom Doherty. John Wiley and Sons, INC. Ames, IA. Pg 148.
44. Marks, D. Conformation and soundness. American Associationof Equine Practitioners’ proceedings, 2000. 46, 39–45.
45. Paulekas, R. & Haussler, K.K. Principles and practice of therapeutic exercises for horses. Journal of Equine Veterinary Science, 2009, 29, 870–893.
46. Davies L. Chapter 12 Equine Rehabilitation. Pain Management in Veterinary Practice, First Edition. Edited by Christine M. Egger, Lydia Love and Tom Doherty. John Wiley and Sons, INC. Ames, IA. Pg. 152
47. Davies L. Chapter 12 Equine Rehabilitation. Pain Management in Veterinary Practice, First Edition. Edited by Christine M. Egger, Lydia Love and Tom Doherty. John Wiley and Sons, INC. Ames, IA. Pg. 150
48. Davies L. Chapter 11. Canine Rehabilitation in Pain Management in Veterinary Practice, First Edition. Edited by Christine M. Egger, Lydia Love and Tom Doherty. John Wiley and Sons, INC. Ames, IA. Pg. 145
Resources for Pain Management: Additional Reading
Pain Management in Small Animal MedicineDr. Steven Foxhttp://www.crcpress.com/product/isbn/9781840761832
Pain Management in Veterinary PracticeChristine M. Egger (Editor), Lydia Love (Editor), Tom Doherty (Editor)http://www.wiley.com/WileyCDA/WileyTitl ... 12240.html
Pain Management for Veterinary Technicians and NursesMary Ellen Goldberg (Editor), Nancy Shaffran (Consulting Editor)http://www.wiley.com/WileyCDA/WileyTitl ... -VE02.html
http://www.amazon.com/Pain-Management-Veterinary-Technicians-Nurses/dp/111855552X/ref=sr_1_8?s=books&ie=UTF8&qid=1399411765&sr=1-8&keywords=Veterinary+Pain+Management
Handbook of Veterinary Pain Management, 3rd EditionJames S. Gaynor (Editor) and William W. Muir III (Editor)http://www.us.elsevierhealth.com/veteri ... 323089357/
Canine Rehabilitation and Physical Therapy 2nd Edition.Darryl L. Millis and David Levine. http://www.us.elsevierhealth.com/small-animal/canine-rehabilitation-and-physical-therapy-hardcover/9781437703092/
Canine Sports Medicine and RehabilitationM. Christine Zink (Editor), Janet B. Van Dyke (Editor)http://www.wiley.com/WileyCDA/WileyTitle/productCd-EHEP003128,subjectCd-VE0D.html

Wall & Melzack's Textbook of Pain, 6th EditionStephen McMahon, FMedSci, FSB, Martin Koltzenburg, MD, FRCP, Irene Tracey, MA (Oxon.), PhD, FRCA and Dennis C. Turk, PhDhttp://www.us.elsevierhealth.com/anesthesiology/wall-melzack-textbook-of-pain-expert-consult/9780702040597/
Anesthesia and Analgesia for Veterinary Technicians, 4th EditionJohn Thomas, DVM and Phillip Lerche, BVSc, PhD, Dipl ACVAhttp://www.us.elsevierhealth.com/veterinary-technology/anesthesia-and-analgesia-for-veterinary-technicians-paperback/9780323055048/
Small Animal Regional Anesthesia and AnalgesiaLuis Campoy (Editor), Matt Read (Editor)http://www.wiley.com/WileyCDA/WileyTitle/productCd-0813819946.html
Essentials of Small Animal Anesthesia and Analgesia, 2nd EditionKurt A. Grimm (Editor), William J. Tranquilli (Editor), Leigh A. Lamont (Editor)http://www.wiley.com/WileyCDA/WileyTitle/productCd-EHEP002353.html
Lumb and Jones' Veterinary Anesthesia and Analgesia, 4th EditionWilliam J. Tranquilli (Editor), John C. Thurmon (Editor), Kurt A.Grimm (Editor)http://www.wiley.com/WileyCDA/WileyTitle/productCd-0781754712.html
Handbook of Veterinary Pain Management, 2eJames S. Gaynor DVM MS DACVA DAAPM (Author), William W. Muir III DVM PhD (Author)http://www.amazon.com/Handbook-Veterinary-Pain-Management-2e/dp/0323046797/ref=tmm_pap_title_0?ie=UTF8&qid=1399411305&sr=1-5
Small Animal Anesthesia and Pain Management: A Color Handbook (Veterinary Color Handbook Series) by Ko, Jeff (2012)

http://www.amazon.com/Small-Animal-Anesthesia-Pain-Management/dp/B00HUBRDEI/ref=sr_1_3?s=books&ie=UTF8&qid=1399411305&sr=1-3&keywords=Small+animal+anesthesia+and+pain+management
Pain Management for the Small Animal Practitioner (Made Easy Series)by William Tranquilli, Kurt Grimm, Leigh Lamonthttp://www.amazon.com/Pain-Management-Small-Animal-Practitioner/dp/1591610249/ref=sr_1_11?s=books&ie=UTF8&qid=1399411765&sr=1-11&keywords=Veterinary+Pain+Management
Pain Management, An Issue of Veterinary Clinics: Food Animal Practice, (The Clinics: Veterinary Medicine)by Hans Coetzee BVSc PhD MRCVShttp://www.amazon.com/Pain-Management-Issue-Veterinary-Clinics/dp/1455773492/ref=tmm_hrd_title_0?ie=UTF8&qid=1399412127&sr=1-24
Update on Management of Pain, An Issue of Veterinary Clinics: Small Animal Practice, 1e (The Clinics: Veterinary Medicine)by Karol Mathewshttp://www.amazon.com/Update-Management-Issue-Veterinary-Clinics/dp/1416063757/ref=sr_1_30?s=books&ie=UTF8&qid=1399412210&sr=1-30&keywords=Veterinary+Pain+Management
Chronic Pain in Small Animal Medicine [Hardcover]Dr. Steven M. Foxhttp://www.amazon.com/Chronic-Pain-Small-Animal-Medicine/dp/1840761245/ref=sr_1_1?s=books&ie=UTF8&qid=1399412297&sr=1-1&keywords=Chronic+Pain+in+Small+Animal+Medicine
Veterinary Clinics of North America: Equine Practice: Pain in Horses: Physiology, Pathophysiology and Therapeutic ImplicationsVolume 26, Issue 3, Pages 467-680 (December 2010)http://www.vetequine.theclinics.com/issues?issue_key=S0749-0739%2810%29X0004-9
Veterinary Clinics of North America: Exotic Animal Practice Analgesia and Pain Management
Volume 14, Issue 1 Pages: 1-178Joanne Paul-Murphyhttp://www.vetexotic.theclinics.com/issues?issue_key=S1094-9194%2810%29X0004-4