Master Thesis in Cardiovascular Technology with special
33
The Scandinavian school of Cardiovascular Technology Aarhus University, Denmark Master Thesis in Cardiovascular Technology with special reference to Cardiopulmonary bypass DOES SHED MEDASTINAL BLOOD PRESENT AS FRIEND (OR) FOE FOR CARDIAC PATIENTS? Proposed to be submitted in partial fulfilment of the degree Masters of Cardiovascular Technology of the Aarhus University By Vishwanath G. Belavi RigsHospitalet, Copenhagen Thorax-Anaestesiologisk, Afd 3044 Blegdamsvej 9, 2100, Denmark Under the Supervision of Prof Dr Shivappa Anurshetru 2012- 2014 SDM Narayana Hrudayalaya Heart Centre, Hubli-Dharwar Road Manjushree Nagar Sattur Dharwar, Karnataka, India - 580005
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Master Thesis in Cardiovascular Technology with special

The Scandinavian school of Cardiovascular Technology
Aarhus University, Denmark
Master Thesis in Cardiovascular Technology with special
reference to Cardiopulmonary bypass
DOES SHED MEDASTINAL BLOOD PRESENT AS
FRIEND (OR) FOE FOR CARDIAC PATIENTS?
Proposed to be submitted in partial fulfilment of the degree Masters of
Cardiovascular Technology of the Aarhus University
By
Vishwanath G. Belavi
RigsHospitalet, Copenhagen Thorax-Anaestesiologisk, Afd 3044 Blegdamsvej 9, 2100, Denmark
Under the Supervision of Prof Dr Shivappa Anurshetru
2012- 2014
SDM Narayana Hrudayalaya Heart Centre, Hubli-Dharwar Road Manjushree Nagar Sattur Dharwar, Karnataka, India - 580005

2
Sl.No CONTENTS Page No
1 Acknowledgement 3
2 Abstract 5-6
3 Introduction 7-8
4 History of Leukocyte Filters 9-11
5 Filter Technology 12
6 Use of Cardiotomy suction blood 13
7 Hypothesis 13
8 Aim of study 14
9 Purpose 14
10 Filter characteristics 14
11 Inclusion and Exclusion criteria 15
12 Materials: Perfusion 16
13 Patients and Methods 16
14 Anesthesia and Perfusion procedures 18
15 Leukocyte filtration procedure 18-19
16 Perfusion measurements 20
17 Lung Function 20
18 Clinical effects 21
19 Results 21-26
20 Discussion 27-29
21 Summary and Conclusion 30
22 References 31-33

3
ACKNOWLEDGEMENT
This Master Thesis is my last theoretical examination paper that completes my
education and entitlement as a “Master of Cardiovascular Perfusion Technology”
in addition to my certification to practice as a “Cardiovascular Perfusionist”. At this
moment I would like to thank the following people without whom this Master thesis
would not have been possible. Special thanks to Chiefs of the departments,
particularly to Dr. Professor Shivappa Anurshetru and Dr. Shanmukh Hiremath
for the possibility to collect data for this thesis in his department.
Quite special thanks are valid at this point for my Parents, my dear wife
Dr. Manisha and my daughter Anushka for the valuable support and help during my
whole Masters study.
Also I would like to thank my colleagues of the team Perfusionist at the
Rigshospitalet, Copenhagen University hospital for their co-operation support during
my master’s course. Special thanks to Casper Seidelin, Peter Fast Nielsen, Marx
Runge, for tutoring and guiding this master thesis.
My thanks are also valid for those who are not mentioned especially, but
considerably contributed to the success and completing of this project thesis.
Student Vishwanath Ganapati Belavi
Supervisor Dr. Shivappa Anurshetru
Honorary Consultant Cardiovascular Surgeon
SDM Narayana Hrudayalaya Heart Centre,
Manjushree Nagar, Sattur
Dharwar, Hubli-Dharwad, Karnataka, India - 580005

4
Perfusionist Casper Seidelin, Chief Perfusionist, MCVT, ECCP
Supervisor Rigshospitalet, Copenhagen university hospital
Thorax-Anaestesiologisk, Afd 3044
Blegdamsvej 9, 2100, Denmark
Examiners Prof Hans Nygaard, Bsc Eng,DMsc
The faculty of health science, Aarhus University
Scandinavian school of Cardiovascular Technology
Aarhus University Hospital, Skejby Sygehus, Denmark

5
ABSTRACT
Background: During cardiac surgery using cardiopulmonary bypass (CPB),
retransfusion of shed mediastinal blood is a common practice to minimize blood loss.
Cardiopulmonary bypass induces a whole body inflammatory response that leads to
postoperative lung dysfunction (1-2)
which is largely mediated by the activation of
poly-morphonuclear leucocytes and by subsequent leukocyte deposition and
interaction within the basement membrane of lung endothelium.(3-4)
During the initial
phase of CPB, leukocytes are activated by the contact of blood with foreign materials
in the extracorporeal circuit. After release of the aortic cross clamp in the late phase of
CPB, when heart and lungs are reperfused, activation of leukocytes and leukocyte
endothelium interaction are intensified, leading to the impairment of lung function
and the induction of a post-operative inflammatory response known as the “post
perfusion syndrome”.
Methods: Cardiac surgery with CPB; Coronary artery bypass and valve patients were
randomly divided in two groups. Group I: filtration of cardiotomy suction and
residual pump blood during cardiopulmonary bypass with a fat leukocyte removal
filter (n = 14). Group II: control patients without filtration (n = 14). Filter efficacy was
evaluated in group I using biochemical markers of blood samples taken
simultaneously before and after the filter. In addition, clinical and biochemical
markers for organ injury were determined in both groups.

6
Results and Conclusion: Leukocyte filtration removed more than 95% of leucocytes,
46% free fatty acids,30% triglycerides from the re-transfused blood (p < 0.01) and
significantly reduced circulating leukocytes (p < 0.05) and granulocytes (p < 0.05)
compared with the control group. Levels of the inflammatory mediator thromboxane
B2 as determined at the end of operation were significantly lower in the depletion
group than the control group (p < 0.05), whereas no statistical differences in
interleukin-6 levels were found between the two groups. After operation, pulmonary
gas exchange function (arterial oxygen tension at a fraction of inspired oxygen of 0.4)
was significantly higher in the leukocyte-depletion group 1 hour after arrival to the
intensive care unit (p < 0.05) and after extubation (p < 0.05).
There were no statistical differences between the two groups with respect to
postoperative circulating platelet level, blood loss, and no infection was observed
during the whole period of hospitalization. Results suggest that leukocyte filtration of
the residual blood in the heart-lung machine at end of bypass and cardiotomy suction
blood during CPB,(1) improves postoperative lung gas exchange function, (2) reduces
the inflammatory response and protects the lungs against the acute injury, (3) prevents
post-operative organ injury in patients and is safe to be used for those patients who
are expected to develop severe inflammatory response after cardiac surgery. A larger
study is needed to determine clinical effects on organ damage.
Limitations: This study has small numbers of patients in the groups. Thus, results
presented here can only be considered to be preliminary value.

7
INTRODUCTION
In cardiac surgery with cardiopulmonary bypass (CPB), retransfusion of shed
mediastinal blood is common practice to minimize blood loss .The rationale for
intraoperative salvage of blood is to reduce the need for allogenic blood transfusions.
In addition to being costly, allogenic blood transfusions have been shown to increase
the risk of infection and to have a negative effect on the long term survival after
cardiac surgery (5,6)
. The reuse of salvaged blood from the mediastinum by cardiotomy
suction has however been questioned because of its potentially severe negative
effects. Not only is there a systemic inflammatory response to the reuse of cardiotomy
suction blood, but also it is contaminated with embolic material. It has been shown
that this blood is contaminated with lipids, which may act as emboli (7)
. Furthermore,
these particles pass through the CPB circuit and find their way into various organs (8)
.
Flow within the cardiotomy suction tubing differs significantly from that in
the CPB circuit. The concurrent suction of air results in highly turbulent flow with
high shear stresses at the air-fluid interface. This results in cellular damage and
activates the humoral cascades involved in the systemic inflammatory response.
Cardiotomy suction blood therefore contains an elevated level of free haemoglobin
brought about by mechanical haemolysis. High concentrations of free haemoglobin
cause platelet dysfunction and direct injury to the renal tubular cells. Similarly,
platelet numbers are reduced in cardiotomy suction blood due to rheological trauma.
Several strategies are used to prevent retransfusion of cardiotomy suction blood. Off-
pump revascularization is being increasingly performed, but is not suitable for
intracardiac surgery. In some centers the cardiotomy suction blood is completely
discarded, but this leads to increased allogenic transfusion requirements.
Retransfusion of cardiotomy suction blood, however, is still used during CPB, and
thus a novel approach with a simple and inexpensive filter for the removal of fat and
debris from cardiotomy suction blood may be an suitable alternative. Such a fat
removal filter has been developed which has a polyester 40 µm screen filter based on
a leucocyte removal filter and allows high flow transfusions.
Activated leukocytes play a key role in this process by their interaction with
the endothelium and with the cardiopulmonary bypass tubing and circuit, to form
platelet leucocyte complexes which play role in re-perfusion injury to minimize

8
postoperative tissue injury; it makes sense to target the leukocytes. This has been tried
by various methods in nearly all the stages of the inflammatory pathway. Leukocyte
activation may be prevented with heparin coated bypass circuits, which reduce contact
activation and possess an enhanced biocompatibility.
D-1 D-2
Pharmacological agents may also prevent leukocyte activation. A serine
protease inhibitor with a variety of actions, aprotinin, is frequently used. Aprotinin
and prednisolone have been found to attenuate the generation of tumor necrosis factor
and the up regulation of leucocyte adhesion molecules. Pharmacological agents are
also used to modify the inflammatory response. For this purpose corticosteroids, and
particular dexamethasone, are often used. Corticosteroids probably change the
cytokine balance from pro-inflammatory to anti-inflammatory. Corticosteroids reduce
leucocyte activation and pulmonary leukocyte sequestration although dexamethasone
has been shown to decrease the concentration of C-reactive protein on the first post-
operative day, clear clinical benefits in terms of post-operative oxygenation, time on
mechanical ventilation, or intensive care unit stay have not been demonstrated.(9)
Use
of dexamethasone may even be detrimental by delaying early postoperative tracheal
extubation, and initiating post-operative hyperglycemia. Fat also contributes to post-
operative tissue injury. Fat microemboli have been demonstrated in brain tissue after
cardiopulmonary bypass (10)
.These microemboli were related to the retransfusion of
cardiotomy suction blood, and were associated with postoperative neurocognitive
dysfunction. In addition, the role of fat on tissue injury is underestimated, because fat
microemboli have not only been demonstrated in brain tissue after cardiopulmonary
bypass, but also in lung and renal tissue.(11, 12)

9
Ultrafiltration techniques are used to restore the intraoperative fluid balance
and to reduce the inflammatory response. This approach is based on the idea that
ultrafiltration removes factors that trigger the inflammatory response. Ultrafiltration
has found a place mainly in pediatric cardiac surgery where it has been shown to
reduce body water, and to increase the haematocrit.
Cell savers are being increasingly used to process cardiotomy suction blood,
but these devices might be less than ideal for several reasons. First, fat is not
completely removed by cell savers. Second, their use is expensive and requires
attention and time to process. Third, processed cell saver blood contains increased
levels of interleukin-1 and activated leucocytes, which may aggravate the
inflammatory reaction associated with cardiopulmonary bypass.(13)
Kaza et al. found
that cell savers were not more effective than a filter after the cardiotomy reservoir for
the elimination of small and large fat emboli.(14)
Therefore leucocyte and fat depletion
by means of a filter may offers a good and practical alternative to modify the
postoperative inflammatory response in cardiac surgical patients. The aim of this
study is to demonstrate that leucocyte and fat filtration, applied in the setting of
cardiac surgery, has a beneficial effect on inflammatory markers and postoperative
organ injury.
HISTORY OF LEUKOCYTE DEPLETION FILTRATION:
In 1928, the pathologist Fleming was the first to use a cotton wool plug as a
filter for the removal of leukocytes from blood. His apparatus is shown in (fig.1), and
consisted of a bent glass tube with a constriction. Cotton wool was introduced in the
constricted limb of the tube and pressed down as tightly as possible with a cork-borer.
Blood was placed above the cotton wool and under pressure forced through the cotton
wool with a teat. We shows his apparatus, because the compressed cotton wool
closely resembles the structure of a modern depth filter and the pressure applied by
the teat is comparable to the pressure that may be generated to force blood through
modern leukocyte depletion filters. In the 1980s research was focused on what
happened in organs during ischemia and reperfusion. Engler et al demonstrated in
dogs that the myocardial stunning which was observed after occlusion of the left
anterior descending coronary artery resulted largely from reperfusion injury.
10
They observed during reperfusion an incomplete restoration of the blood flow
in the microvasculature of the heart. This so called no reflow phenomenon was
associated with capillary leukocyte plugging and endothelial cell protrusion and was
based on an acute inflammatory response, (15)
revealed a central role for leukocytes.
Engler et al hypothesized therefore that leukocyte depletion might be beneficial in the
setting of ischemia and reperfusion. They tested this hypothesis in the dog model and
found that reperfusion with leukocyte depleted blood almost completely prevented
reperfusion injury.(16)
These findings started research in the clinical application of
leukocyte depletion filters for organ protection.
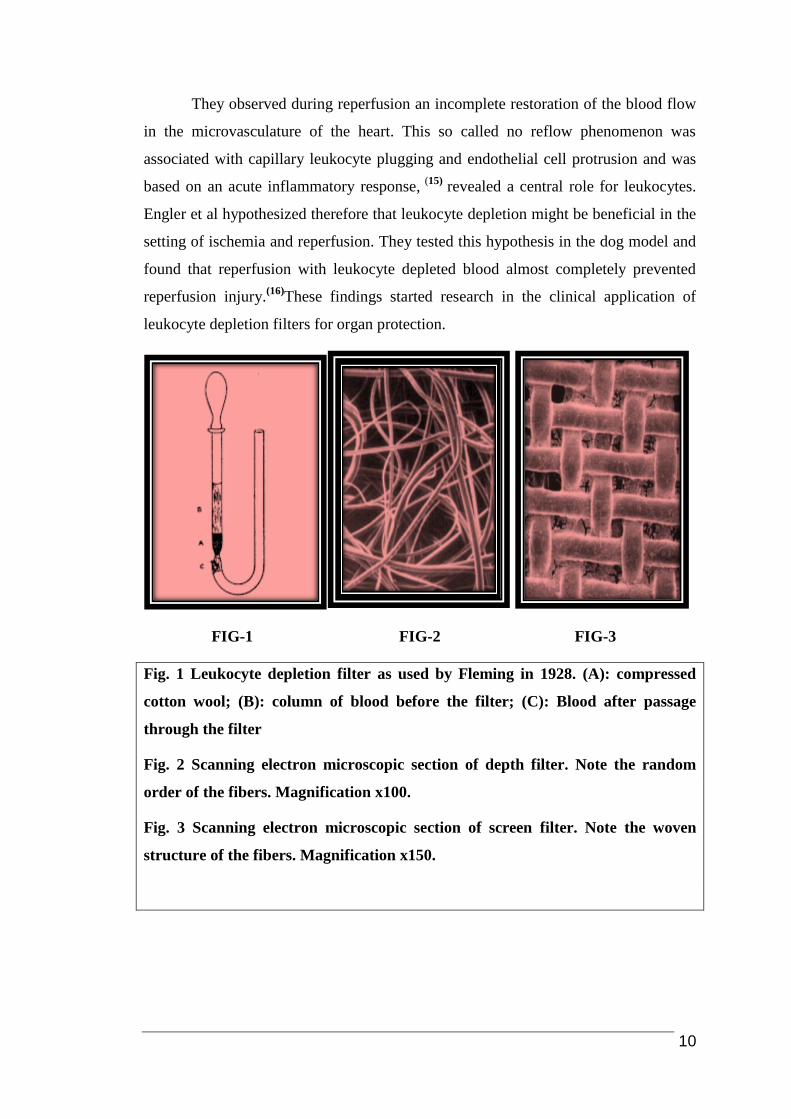
FIG-1 FIG-2 FIG-3
Fig. 1 Leukocyte depletion filter as used by Fleming in 1928. (A): compressed
cotton wool; (B): column of blood before the filter; (C): Blood after passage
through the filter
Fig. 2 Scanning electron microscopic section of depth filter. Note the random
order of the fibers. Magnification x100.
Fig. 3 Scanning electron microscopic section of screen filter. Note the woven
structure of the fibers. Magnification x150.

11
The improved flow properties allow these filters to be used in patients with
higher fluid requirements. For an explanation of these improved flow properties, some
aspects of the biomaterials and design that are used must be discussed. At this
moment depth and screen filters are used. In depth filters, the filter material has the
form of compressed wool fibers (Fig. 2) Polyester and sometimes polyurethane is
used as filter material, which promote adhesion of the leukocytes throughout the filter.
In screen filters, the filter is built up with layers of woven polyester filter material
(Fig. 3). In this type of filter, leukocytes are bound to the subsequent layers of filter
material. Most leukocytes are thus trapped at the outer most layers of the filter and
this may increase the resistance over the filter. The way leukocytes are trapped inside
the filter also influences the efficacy and capacity of the filter. At least 4 mechanisms
have been described, (18)
but the most important mechanism is adhesion. By adhesion,
the negatively charged leukocytes are attached to the filter material by Van der Waals
and electrostatic forces. This adhesion is an active process and has the advantage that
a larger pore size with subsequent higher flow rates is possible in the filter. Thus,
properties of the filter material like surface charge and hydrophilicity greatly
determine the efficacy of the filter.
To modify the surface charge of the filter, coating of the filter material is often
used to improve filter efficacy. A coating of methacrylate creates a more positive
surface charge that results in a stronger bond with the negatively charged
leukocytes.(19)
Hydrophilicity is important for optimal contact between the leukocytes
and the fibers and thus for the subsequent adhesion. This implies that optimal
leukocyte depletion can only occur if the whole filter is exposed to blood, which
means that de-airing must be carefully performed before use.
Insufficient de-airing disturbs the optimal blood flow and thus reduces filter
efficacy. Another effect of the physicochemical properties of the filter material is that
leukocytes appear predominantly to stick to the crossing points of the filter fibers.
Thus more crossing points increase the efficacy of the filter. More crossing points
require thinner fibers. However, thinner fibers also lead to an increase in resistance
and thus to flow reduction. This indicates in a nutshell the compromises that have to
be made in the design of a filter. The current generation of leukocyte depletion filters
may be pressurized up to 300mmHg. This allows rapid transfusion in a clinical
setting, but decreases the efficacy as it has been shown that a longer contact time of

12
the leukocytes in the filter increases the filter efficacy. The efficiency of the filters
also decreases over time as the filter becomes saturated with cells and debris.
Therefore, application of leukocyte depletion filters may interfere with blood
coagulation. This is a problem of all leukocyte depletion filters as generally 40% of
the platelets that pass through the filter are trapped. Allen et al demonstrated a
significant difference in platelet counts by drawing samples simultaneous up and
downstream of the filter.(20)
Nonetheless, a certain amount of platelet deposition on the
polyester fibers of the filter helps to bind the leukocytes.(21)
It appears that platelets
have a higher affinity for the filter material than leukocytes. In addition, platelets have
active surface receptors so that they rapidly establish a strong bond with leukocytes. A
beneficial aspect of the removal of platelets is that activated platelets release different
vaso-active substances. Therefore, removal of platelets could reduce thromboxane
release with a reduction in vasoconstriction but before reviewing the clinical aspects
of the application of leukocyte depletion, we will now briefly discuss some aspects of
the filter technology used.
FILTER TECHNOLOGY:
The first generation of leukocyte depletion filters designed for routine use was
made of cellulose and had a leukocyte removal rate of about 98%. Although clinically
acceptable results were achieved, these filters had two drawbacks. First, they also
appeared to activate complement C3, with a subsequent vasoconstriction and
increased capillary permeability (17)
. Second, the efficacy of leukocyte removal was
strongly dependent on the flow across the filter. Filtration was therefore a slow
process and took about 30 minutes for one unit of red blood cells. Currently, a new
generation of filters is available which combines rapid flow with an excellent
leukocyte removal rate. These new filters remove 99.995% of the leukocytes from the
blood. However, during operation this may be somewhat lower with a 96.8% removal
of leukocytes for cardiopulmonary bypass perfusate.

13
USE OF CARDIOTOMY SUCTION AND RESIDUAL PUMP BLOOD:
The reuse of mediastinal blood with cardiotomy suction is more or less
mandatory in open cardiac surgery. Not only does this enable the surgeon to visualize
the field but saves the shed blood from being discarded and thereby avoiding costly
and potentially dangerous problems associated with donor blood transfusion. In case
of profuse bleeding the use of cardiotomy suction and residual pump blood can also
be lifesaving whereas the blood can be immediately retransfused through the CPB
circuit. Filters in the cardiotomy suction are used to decrease the risk of solid emboli
making their way into the circulation. Several authors have shown that
microembolisation is a potential threat during cardiac surgery, and will influence the
outcome (22)
.Opening of the mediastinum during cardiac surgery involves trauma. The
sternum is opened with an oscillating saw and thereby exposing the marrow. Bone
marrow is relatively rich in fat and consists of 40% fat in the adult. With
electorcautery the subcutaneous and mediastinal fat is exposed. Both bone marrow
and adipocytes in the wound are a probable source of lipid which can be seen in the
shed mediastinal blood at surgery. Small and large fat droplets can be observed in the
pool of blood collecting in the surgical field. It is this contaminated blood that is
common practice to collect and reuse during surgery by means of cardiotomy suction
(Fig 4 and 5).
HYPOTHESIS:
Leukocyte filtering of cardiotomy suction and residual pump blood improves
post-operative lung gas exchange, protects lungs against the acute injury, minimizes
severe inflammatory response and prevents post-operative organ injury in patients
undergoing open heart surgeries.

14
AIM OF STUDY:
To assess the efficacy of fat removal filter during open heart surgery by
filtering residual heart lung machine and cardiotomy suction blood in patient’s
undergoing bypass surgery and its effects on post-operative organ injury. We
evaluated some of the possible filter effects on lungs, kidney and heart with clinical
and biochemical markers, using an unfiltered group of cardiac patients as controls and
its beneficial effects on inflammatory response.
PURPOSE:
To test the efficacy of a fat removal filter in patients undergoing cardiac
surgery using CPB for (1) Fat Removal, (2) Leukocyte depletion, from the cardiotomy
suction and residual heart lung machine blood at the end of CPB.
FILTER CHARACTERISTICS:
The amount of cardiotomy suction and residual pump blood was 1104 ± 152
mL on an average with a haematocrit of 19 ± 1.4%. Baseline plasma triglyceride level
in the patients was 1.02 ± 0.15 mmol.L-1
. The filter removed 30% of the triglycerides
and reduced leucocytes by 47% and platelets by 35% (table 4). Thin layer
chromatography revealed that after filtration, free fatty acids (FFA), triglycerides and
phospholipids were reduced (table 3).
The efficacy of the filter decreased slightly during the 600 mL of blood that
passed through the filter. After 600 mL of blood the filter removed 13% of the
triglycerides and reduced leucocytes by 34% and platelets by 31%.The time needed to
pass 200 Ml of blood under gravity at a height of 90 cm was 2 min 40s ± 13s, and for
600 mL this time was 7 min ± 20s. We found no adsorption of (hydrophobic) platelet
activating factor (PAF) on the filter material, excluding its effect on the preservation
of the blood platelet.

15
FIG-4 FIG-5
Figure 4.Surface of shed blood from the surgical field where lipid droplets
are easily seen.
Figure 5.Scanning Electron Micrograph of lipid particles found in shed
mediastinal blood.
INCLUSION CRITERIA:
Only patients admitted for cardiac surgery using cardiopulmonary bypass were
included. Clinical assessment of operative blood loss was done. In patients with
significant blood loss and where allogen blood replacement was needed fat filters
were used. In patients with no significant blood loss filters were not used as
significant volume is needed in the cardiotomy reservoir for circulation in the filter
and for it to be effective for filtration.
EXCLUSION CRITERIA:
Patients older than 70 years with congestive heart failure (CHF) greater than
class II(NYHA), pre-existing lung disease, cerebral vascular disease, diabetes
mellitus, body mass index (BMI) over 35 kg/m2,creatinine ≥ 1.4mg/dl, emergency
operation and re-operation were excluded.

16
MATERIALS -PERFUSION:
After institutional approval and patients consent 28 patients scheduled for
cardiac surgery were prospectively randomized to Group I: fat filtration of cardiotomy
suction and residual pump blood during CPB using LG-6(Pall Biomedical) 40µ
polyester screen filter (n = 14), and Group II: control patients without filtration
(n = 14). The extracorporeal circuit consisted of roller pumps (Stöckert, München,
Germany), a hollow fibre oxygenator (Sarns Turbo, 3M, St. Paul, MN, USA) and a
standard arterial line filter (Affinity 38μ Medtronic, Minneapolis, MN, USA). The
priming consisted of 500 mL hydroxyethylstarch 10% (Haes, Fresenius, Bad
Hamburg, Germany) and 800 mL lactated Ringer’s solution and 20% 100ml
Mannitol. Pump flow was adjusted to 2.4 L.m-2 per min. Nasopharyngeal temperature
during CPB was maintained at 35.6º degrees.
PATIENTS AND METHODS:
After getting approval by the medical committee at Narayana Hrudayalaya
cardiac research center Hospital in Hubli, Karnataka, and informed consent from
patients, 28 patients electively undergoing either coronary artery bypass grafting,
heart valve replacement or a combined procedure were randomly allocated to a
leukocyte-depletion group (n = 14) and control group (n = 14) without filtration.
Exclusion criteria were pre-existing lung disease, cerebro vascular disease, diabetes
mellitus, recurrent infection, reoperation, and emergency operation. Blood samples
were drawn from the radial artery (1) after induction of anesthesia, (2) at the end of
the operation, (3) after three hours in the ICU and (4) on the morning of the first post-
operative day. From the blood samples taken pre-operatively on day 1, 2 and 3, the
creatinine clearance was calculated to the Cockcroft formulae. Both groups were
similar with respect to age, sex, length, weight, haematocrit (p = 0.16), creatinine
clearance, CPB time (p = 0.2).The demographic data are summarized in table (1 and
2).

17
Variable Unit Mean (Range)
Age Y 64 (47-75)
Male - 14
Female - -
Height cm 175.1 (165-190)
Weight kg 75.6 (60-103)
CPB Time min 97 ( 56-165)
X-Clamp Time min 60.5 ( 38-103)
Temp(np) during CPB Degrees centigrade 35.6 ( 34.5-36.0)
Table 1: The demographic data of patients in both groups are summarized Creatinine
clearance according to the Cockroft formulae; CPB, cardiopulmonary bypass.
Group Filter (n=14) Control (n=14)
Age(Year) 62 ± 2.5 63 ± 3.2
Sex(Male) 14 14
Length(cm) 176 ± 2.6 172 ± 2
Weight( Kg) 81 ± 2.5 77 ± 2
Hematocrit (%) 33.5 ± 0.9 35.8 ± 1.3
Creatinine Cl (ml.kg-1 per min
) 101 ± 6.5 79 ± 7.9 P<0.04
CPB(min) 85 ± 7.0 61 ± 7.0
Table 2: Characteristics of patients (N=14) receiving filtration CPB. All patients that
were included completed the study. The demographic data are summarized in table 1,
which shows that both groups were similar. The post-operative clinical data are
summarized in table 6, and indicate that there were no differences between both
groups. There were no complications requiring a prolonged hospital stay.

18
ANESTHESIA AND PERFUSION PROCEDURES:
Anaesthesia was induced and maintained by intravenous infusion of sufentanil
citrate (1–3μg/kg) and midazolam (0.05-0.1mg/kg).Muscle relaxation was achieved
with pancuronium bromide (100–140μg/kg), Cefamandol 2g and dexamethasone 1
mg/kg were administered after induction. Anticoagulation was achieved by
intravenous administration of bovine lung heparin at a dose of 300 IU/kg about 5
minutes before the start of bypass. The extracorporeal circuit consisted of roller
pumps (Stöckert, Munich, Germany) and a microporous polypropylene membrane
oxygenator (CML Excel, Cobe Laboratories Inc., Lakewood, CO). Within 10 minutes
of CPB initiation at a flow rate at 2.4 L/min/m2, the aorta was cross clamped and 1 L
of St. Thomas cardioplegia solution (4°C) was infused into the aortic root to provide
myocardial preservation. During CPB, moderate hypothermia was induced to
maintain the nasopharyngeal temperature between 34.5º to 36.0º.
The mean arterial pressure was maintained between 50 to 60 mmHg during
CPB. Anticoagulation during CPB was monitored by the celite activated clotting time
(International Technidyne Co., Edison, N.J.). After CPB, heparin was neutralized by
protamine chloride (3 mg/kg).
PERFUSION PROCEDURE FOR LEUKOCYTE FILTRATION:
In this study we used a leukocyte depletion filter for Cardiotomy suction and
residual heart-lung machine blood that was retransfused in the patient after
cardiopulmonary bypass. The hypothesis being, blood that is retransfused in a vein
first passes the lungs. The lungs act as an endogenous filter and remove activated
leucocytes and debris from this blood. If these activated leucocytes and debris were
to be trapped in a filter before reaching the lungs it would result in less pulmonary
injury and improved postoperative lung function.
LeukoGard 6(LG6) leukocyte depletion filter consists of polycarbonate
housing with a polyester cartridge that has a leukocyte reduction effect. It also
includes a 40µ polyester screen filter. The priming volume is 220ml and allows flows
upto 6L/min. The main mechanism is to trap leukocytes by adhesion to the material in
the filter. The negatively charged leukocytes are attached to the positively charged
filter material by Van der Vaals and electrostatic forces. The placement of the

19
leukocyte depletion filter may be in the arterial line, the venous return line, the
cardioplegia line (or) a combination of these, and used at various times( continuous or
strategic) during cardiopulmonary bypass. In addition, to assess the qualitative effects
of filtration, modified thin layer chromatography according Folch13 was performed
on samples before and after the filter and on a patient blood sample before CPB, as
well as on the blood samples that were taken for the assessment of the filter capacity.
After CPB, the residual blood in the heart-lung machine was filtered and collected in
a transfusion bag and in both groups retransfused to the patients.
In Group I(Filtration), total amount of blood collected from cardiotomy and
residual pump blood on an average was 1104 ± 152.Here, we filtered 550ml from
residual heart lung machine using a high-flow leucocyte removal filter (LG6, Pall
Biomedical, Portsmouth, UK) incorporated in the arterial line. This procedure was
associated with intermediate flow, but high pressures. After each 600ml of
cardiotomy blood a new filter was used.
Secondly, Leukofiltration of cardiotomy suction blood was (600mL) which
was then collected in separate cardiotomy reservoir from the moment that the ACT
was > 400s. Later, this blood was transfused into the patient under gravity ≤ 100mm
Hg using a leucocyte removal filter (RS 1, Pall Biomedical,UK). At the end of CPB
using the same roller pump blood flows were adjusted to 400 mL/ min. The filtration
pressure, measured between the pump and the filter, was generally high (≥/150
mmHg), but did not exceed 300 mmHg.
The filtration procedure lasted 10 ±/0.7 minutes and, thus the total amount
of filtered blood at end of CPB from cardiotomy suction was 600 ml and 550ml
from residual heart lung machine blood. In both groups, the residual blood in the
extracorporeal circuit after CPB was collected in a transfusion bag and transfused
into the patient using a standard transfusion system. When 200 mL blood had
passed through the filter, samples were taken simultaneously before and after the
filter. From EDTA-anticoagulated blood, hematocrit, platelet and total white blood
cell counts were determined by an electronic cell counter (Cell-Dyn 610, Abbott,
Santa Clara, CA, USA). In both groups, the residual blood in the extracorporeal
circuit after CPB was collected in a transfusion bag and transfused into the patient
using a standard transfusion system. Triglyceride levels were determined with a
biochemical assay (Sigma, St. Louis, MO, USA).

20
In Group II, control group the cardiotomy suction blood was collected
directly in the same cardiotomy reservoir of the CPB circuit from the moment that
the ACT was >400s. The blood was transfused directly into patient at the end of CPB
procedure without performing any leukocyte filtration.
PERFUSION MEASUREMENTS:
For all laboratory tests and biochemical assays EDTA and citrate
anticoagulated blood was drawn from the patients’ radial artery catheter. Blood
samples were drawn (1) after induction of anaesthesia, before the start of CPB, (2) at
the end of the operation, (3) after three hours in the ICU and (4) on the morning of the
first post-operative day. For biochemical assays, plasma was obtained by
centrifugation of whole blood at 1000 RPM and immediately stored at -80°C for
further determinations. Plasma levels of glycerol and triglyceride were both
determined by routine biochemical methods (Sigma. St. Louis, MO, USA).
Haemoglobin, haematocrit and platelet, total white blood cell and granulocyte counts
were determined by an electronic cell counter (Cell-Dyn 610, Abbott, Santa Clara,
CA, USA). Levels of triglycerides, leucocyte and platelet counts were measured from
EDTA and in addition citrate anticoagulated samples taken simultaneously before and
after the filter to assess the efficacy of the fat removal filter. Thromboxane was
determined by enzyme immunoassay (Cayman Chemical Company, Ann Arbor,
Mich) in plasma anticoagulated with citrate and indomethacin. Interleukin-2 and
interleukin-6 were determined by enzyme immunoassay (Quantikine, R&D Systems
Europe, Abingdon, UK) from citrated plasma.
LUNG FUNCTION:
Pulmonary gas exchange was measured by the partial pressure of arterial
oxygen from blood samples drawn from the radial artery line and standardized at a
fraction of inspired oxygen of 0.4. Pulmonary hemodynamics exemplified by mean
pulmonary artery pressure (PAP) and pulmonary capillary wedge pressure (PCWP)
were measured through a Swan-Ganz catheter (Edwards, Baxter Healthcare Corp,
Irvine, CA) introduced percutaneously through the right internal jugular vein into the
pulmonary artery. Pulmonary vascular resistance (PVR) was calculated according to
the following formula: PVR (dyne.sec.cm-5) = (PAP - PCWP) / CO x 80.

21
CLINICAL EFFECTS:
The calculated creatinine clearance was higher in the filter group on the first
postoperative day (p = 0.04) (tables 3 and 7). The two groups were similar with
respect to fluid intake, diuresis, blood loss, lung function and myocardial injury (table
6). In the control group, one patient had a myocardial infarction (defined as new
Q-wave on the ECG and CK > 180 U/L with CK-MB > 10% of total), one patient had
major blood loss and one patient developed renal function disturbances with a serum
creatinine level of 231 mmol.L-1
. Overall hospital stay was slightly shorter in the
filter group (table 6). The PaO2 showed a time effect (p = 0.001), but there was no
difference between the groups (p = 0.25) (figure 1). The A-a gradients showed a time
effect (p < 0.001), but no difference between the groups (p = 0.25) (figure 7).
RESULTS
After operation, pulmonary gas exchange function (arterial oxygen tension at a
fraction of inspired oxygen of 0.4) was significantly higher in the leucocyte-depletion
group 1 hour after arrival to the intensive care unit (p < 0.05) and after extubation
(p < 0.05). There were no statistical differences between the two groups with respect
to post-operative circulating platelet level, blood loss, and no infection was observed
during the whole period of hospitalization. The results observed were;
1) CIRCULATING LEUCOCYTES AND PLATELETS:
Circulating leukocyte and granulocyte counts at the end of operation were
significantly less in the leucocyte-depletion group than in the control group (p < 0.05).
There were no significant differences in circulating lymphocyte and platelet counts
between the two groups. The fat filter removed triglycerides (0.9 ± 0.09 mmol.L-1
vs
0.63 ± 0.07 mmol.L-1
, p = 0.003), leucocytes (4.3 ± 0.8 x 109 vs 2.3 ± 0.6 x 10
9 .L
-1, p
= 0.03) and platelets (116 ± 26 x 109.L
-1 vs 75 ± 21 x 10
9.L
-1, p = 0.003) from the
cardiotomy suction blood (600 ± 154 mL).

22
2) LEUKOCYTE REDUCTION IN RESIDUAL MACHINE BLOOD:
The average leukocyte count determined from the residual machine blood
before filtration was 5.76 ± 0.44 x 109/L. After filtration, the count was 0.152 ± 0.01 x
109/L. More than 97% of leucocytes were removed from the residual blood in the
leucocyte depletion group. The average platelet count from the machine blood before
filtration was 107 ± 6 x 109/L, after filtration, it was 54 ± 2 x 10
9/L. About 60% of the
platelets in the machine blood were removed by the filters in the leucocyte-depletion
group.
3) INFLAMMATORY MEDIATORS:
Thromboxane B2 levels were significantly lower in the leucocyte-depletion
group than in the control group at the end of operation (p < 0.05; table 4). Interleukin-
6 levels increased in both the leucocyte-depletion and control groups during the early
postoperative period. No significant difference was found between the two groups.
Interleukin-2 was not detectable in any of the sample.
4) LUNG FUNCTION:
Pulmonary gas exchange, measured by partial oxygen pressure, was
significantly higher in the leukocyte-depletion group than that in the control group
both at one hour after arrival in the intensive care unit (118 ± 10 mmHg versus
86 ± 10 mmHg, p < 0.05) and immediately after extubation (120 ± 8 mmHg versus
89 ± 10 mmHg, p < 0.05. PAP was somewhat lower in patients receiving leukocyte
depletion than in the control group, but this difference in PAP was not significant.

23
Samples Before the filter After the filter P-Value
Biochemical Assays
Triglycerides(mmol.L-1
) 0.9 ± 0.09 0.63 ± 0.07 0.003
Leukocytes( x 109.
L-1
) 4.3 ± 0.8 2.3 ± 0.6 0.03
Platelets ( x 10 9 .
L-1
) 116 ± 26 75 ± 21 0.003
Free Fatty acids 7.6 ± 1.1 4.1 ± 0.8 0.005
Phospholipids 49.3 ± 3.4 45.3 ± 3.8 0.04
Cholesterol 9.8 ± 1.4 9.7 ± 1.7 0.91
Table 3:-The P-Value reflects the statistical analysis of the sample taken before and
after the filter by one -way student t-test.
Parameter Before
CPB
End CPB End
operation
ICU 1hr ICU 3hr POD 1
Thromboxane
(pg/ml)
Depletion ND 48 ± 15 48 ± 9 33 ± 7 23 ± 29 19 ± 26
Control ND 62 ± 95 127 ± 63 48 ± 15 89 ± 56 21 ± 34
Interleukin
6(pg/ml)
Depletion 36 ± 14 126 ± 96 ND 393 ± 116 344 ± 90 125 ± 46
Control 20 ± 24 197 ± 246 ND 208 ± 103 260 ± 38 155 ± 29
Interleukin 2
Depletion UD UD ND UD UD UD
Control UD UD ND UD UD UD
Table 4:- Values are expressed as the geometric mean and the standard error of the
mean. ICU (Intensive care unit; POD, Post -operative day; ND; not determined; UD,
undetectable (below the lowest detectable level as stated by the manufacturer (P <
0.05) compared with control.

24
5) PRE AND POST-OPERATIVE DATA:
Parameters Depletion (N= 14) Control ( N = 14)
CPB Time 88 ± 38 100 ± 24
Cross Clamp time 61 ± 29 67 ± 19
Blood loss(ml) 414 ± 68 324 ± 34
Intubation(hr) 11.7 ± 0.9 13.8 ± 1.3
ICU Stay(days) 1.0 ± 00 1.1 ± 0.1
Hospital stay(days) 4.2 ± 0.8 10.5 ± 1.5
Table 5.Values expressed as mean ± standard deviation of the mean. (ICU) Intensive
care unit.
Group Filter Control P value
Cr .CL(ml.kg-1
per min) 76 ± 4.5 72 ± 7.2 0.04
Fluid in (ml) 4040 ± 262 4079 ± 291 0.94
Blood loss(ml) 414 ± 68 324 ± 34 0.27
Diuresis(ml) 2920 ± 215 3183 ± 308 0.49
CK enzymes( IU.L-1
) 236 ± 56 169 ± 27 0.32
CK-MB( IU.L-1
) 12 ± 6.4 6 ± 1.8 0.44
Platelets(x 109. L-1
) 181 ± 13 162 ± 13 0.31
Leukocytes(x 109. L-1
) 18.6 ± 0.8 13.5 ± 1 0.13
Table 6. Clinical effects on the first, second post-operative day and hospital stay.
Cr CL, renal, creatinine clearance according to the cockroft formula.

25
Figure 6: Circulating Leukocyte and platelet counts in the filter group and in
unfiltered control group pre-operatively(Pre-op),at the end of operation(end -op),
after 3 hours in the intensive care unit (3h ICU) and on the morning of the first post
operative day 1.
OTHER CLINICAL PARAMETERS:
Duration of postoperative intubation was recorded during each patient’s stay
in the intensive care unit. Blood loss was indicated by 24-hour chest drainage. In
addition, durations of stay in the intensive care unit and of hospitalization after
operation were obtained from hospital registration records.

26
Figure 7:- Arterial oxygen tension (PaO2) and alveolar- arterial (A-a) oxygen
gradients in the fat filter group and in the unfiltered control group pre-operatively
(pre-op), at the end of operation (end-op), after 3 hours in the intensive care unit (3h
ICU) and on the morning of the first postoperative day (day 1), The PaO2 showed
time effect (p=0.0009), but no difference between the groups. The A-gradients
showed a time effect (P<0.001), but no difference between the groups.

27
DISCUSSION
From the results and observations in this project thesis it may be concluded
that leukocyte depletion has a beneficial effect on several clinical parameters in the
post-operative period of patients in group I. However, leukocyte depletion filters are
relatively less used in routine practice for several reasons. Firstly, there are no large
randomized prospective studies that demonstrate the clinical effects of leukocyte
depletion in terms of reduced organ injury and length of intensive care unit or hospital
stay. Secondly, at this moment it is not clear which level of leukocyte depletion
should be achieved during cardiac surgery to obtain a clinically useful result. The
results of the studies during organ reperfusion suggest that lower counts are more
effective, but data regarding systemic leukocyte depletion are lacking. Thirdly, the
optimal period of leukocyte depletion during cardiac surgery, during the whole
cardiopulmonary bypass period or in well aimed time spans, must be defined. Until
these problems are resolved leukocyte depletion during cardiac surgery by means of
filtration will not gain the place it deserves. This study showed that the application of
a fat removal filter reduced the fat content of cardiotomy suction blood in cardiac
surgical patients.
In the leukocyte-depletion group (n = 14), all cardiotomy suction and residual
pump blood (1104 ± 152) on an average was filtered by leukocyte-removal filters and
reinfused in patients after CPB, whereas in the control group an identical amount of
residual blood after CPB was reinfused without filtration (n = 14).There were no
significant statistical differences between the two groups with respect to duration of
CPB time, aortic cross clamp time, postoperative circulating platelet levels, blood loss
and no infection as observed during entire period of hospitalization.
The filter consists of tightly packed fibers with a porous structure of about
40µm. This may mechanically stop the larger fat globules. Such a view is supported
by a recent study on cardiotomy suction blood.23
Fat micro emboli were divided in
large (> 50 µm) and small (10-50 µm) size emboli. No large emboli were detected
after the filter. In our filter the removal of the various fat subgroups was highly
variable. This may be explained by a difference in electrostatic adhesion to the filter
material. One could therefore speculate on filter improvement by coating of the fibers
to increase the removal of the other subgroups, but clinically the free fatty acids
appear to be the most important.

28
Free fatty acids are bound to albumin. Plasma albumin is reduced by
haemodilution after CPB. For this reason we did not use a prime with albumin, but
instead used hydroxyethylstarch, which is not known to interfere with binding of free
fatty acids. Increased levels of free fatty acids have documented clinical effects. In
lung tissue free fatty acids are associated with the development of an acute respiratory
distress syndrome.24
In endothelial cells free fatty acids cause vasoconstriction and
granulocytes are activated through surface expression and activity of CD11b.25
It has
recently been shown that the composition of the cardiotomy suction blood is different,
and that a low temperature increases filter efficacy.26
With about 85 mL/min the filter appeared to have a high flow during
transfusion under gravity. However, a high flow reduces the contact time between
blood and filter medium and thus may result in lower filter efficiency. Thus, filter
efficiency may be improved by coating the fibers, or alternatively by packing more
filter materials in the housing. This latter option would reduce the flow over the filter.
However, a flow of 30 mL/min should be sufficient to filter on an average of 1.5 L
blood, which equals the amount of cardiotomy suction blood, during a cross clamp
time of 45 min. For widespread use the fat removal filter will need a larger capacity,
as our results indicated that the filter became saturated after 600 mL, requiring to
change it.
Clinical findings in this study suggest a beneficial effect of the filter. First, the
higher calculated creatinine clearance in the filter group on the first post-operative day
in view of a similar post-operative fluid balance and second, the higher post-operative
platelet counts in the filter group. Platelets and leucocytes in the cardiotomy suction
blood are activated in the presence of fat and tissue factor from the pericardium. Thus,
removal of platelets and leucocytes by the filter may be advantageous and protective
against the systemic inflammatory response and thrombus formation.
Third is post-operative oxygenation although not significant different in itself
due to the small sample size, the fact that the postoperative A-a gradients were
smaller, and the postoperative PaO2 values were higher in the filter group suggest that
in the filter group less pulmonary injury occurred. This may be explained by the fact
that the filter significantly reduced free fatty acids, known for their deleterious effects
on lung function.28
In addition; the filter also removed a significant part of the
leukocytes from the suction blood. We have previously shown that filtration of

29
leukocytes improved postoperative lung function. Several other possibilities for the
management of the cardiotomy suction blood exists. Cell savers are increasingly used,
but these devices might be less than ideal for several reasons. First, fat is not
completely removed by cell savers. Thus, as a consequence, even cell saver blood
may benefit from the application of a fat removal filter before retransfusion. Second,
their use is expensive and requires attention and time to process.
In contrast, fat removal filters are cheaper, about 25% of the cost of a cell
saver, they are very easy to operate and processed blood is immediately available.
Kaza found cell savers not more effective than the application of a filter after the
cardiotomy reservoir for the elimination of small and large fat emboli.27
Third,
processed cell saver blood contains increased levels of interleukin-1 and activated
leukocytes, which may aggravate the inflammatory reaction associated with CPB.
Based on our results, at least 35 patients in each group had to be included to
demonstrate clinical differences with a power of 0.8 and an α of 0.05. However, our
results suggest that it would be worthwhile to perform such a study. Further, we use
routinely dexamethasone for all our patients to reduce the inflammatory reaction after
CPB because the incidence of the fat embolism syndrome was decreased in a
prospective randomized clinical trial, where steroids were given to prevent the effects
of the fat embolism syndrome.28
Therefore, the effects of the fat removal filter on
organ damage could be more pronounced than demonstrated in this study. Moreover,
we speculated that fat release during the operation would mainly result from
mechanical damage through surgical manipulation and shear forces. This would result
in a direct release of the triglycerides and free fatty acids, which we measured in this
study. Platelets and leukocytes in the cardiotomy suction blood are activated in the
presence of fat and tissue factor from the pericardium. Thus, removal of platelets and
leucocytes by the filter may be advantageous and protective against the systemic
inflammatory response and thrombus formation.
The demographic of patients variables, filter and control groups data are
summarized in (table 1 and 2), which shows that both groups had similar findings.
The post-operative clinical data as summarized in (table 5), indicate that there was
very little difference between the groups. There were no complications requiring a
prolonged hospital stay and all patients recovered uneventfully after operation (Table
6).

30
Lastly, the fat filter removed triglycerides (0.9 ± 0.09 mmol.L-1
vs 0.63 ± 0.07
mmol.L-1
, p = 0.003), leukocytes (4.3 ± 0.8 x 109 vs 2.3 ± 0.6 x 10
9 .L
-1, p = 0.03) and
platelets (116 ± 26 x 109.L
-1 vs 75 ± 21 x 10
9.L
-1, p = 0.003) from the cardiotomy
suction blood (600 ± 154 mL).Use of leukocyte and fat depletion filters undoubtedly
has a place in CPB for open heart surgeries. However, many other clinical parameters
need to be studied and assessed in larger number of patients, for us to conclusively
establish the routine use of these filters in open heart procedures.
SUMMARY AND CONCLUSION
Results suggest that leukocyte filtration of the residual heart-lung machine and
cardiotomy suction blood, (1) improves postoperative lung gas exchange function, (2)
reduces the inflammatory response and protects the lungs against the acute injury, (3)
prevents post-operative organ injury in patients and is safe to be used for those
patients who are expected to develop severe inflammatory response after cardiac
surgery. Postoperative oxygenation although not significantly different in itself due to
the small sample size, the fact that the postoperative A-a gradients were smaller, and
the postoperative PaO2 values were higher in the filter group suggest that in the filter
group less pulmonary injury occurred. This may be explained by the fact that the filter
significantly reduced free fatty acids, known for their deleterious effects on lung
function.

31
REFERENCES
1. Kirklin JK, Westaby S, et al. Complement and the damaging effects of
cardiopulmonary bypass. J Thorac Cardiovasc Surg 1983; 86:845-857.
2. Taggart DP, El-Fiky MM, Respiratory dysfunction after uncomplicated
cardiopulmonary bypass. Ann Thorac Surg 1993;56:1123-28.
3. Van O everen. A prospective study of bubble versus membrane oxygenation.
J Thorac Cardiovasc Surg 1985; 89:888-899.
4. Dreyer WJ, Michael LH, Neutrophil activation and adhesion molecule expression
in a canine model of open heart surgery with cardiopulmonary bypass. 1995;
29:775-781.
5. Koch CG, Li L, Duncan AI, Mihaljevic T, Cosgrove DM, Loop FD, et al.
Morbidity and mortality risk associated with red blood cell and blood component
transfusion in isolated coronary artery bypass grafting. Crit Care Med 2006;
34(6):1608-16.
6. Kuduvalli M, Oo AY, Newall N, Effect of peri-operative red blood cell
transfusion on 30-day and 1-year mortality following coronary artery bypass
surgery. EurJ Cardiothorac Surg 2005;27(4):592-8.
7. Brooker RF, Brown WR, Moody DM, Hammon JW, Jr., Reboussin DM, Deal
DD, et al. Cardiotomy suction: a major source of brain lipid emboli during
cardiopulmonary bypass. Ann Thorac Surg 1998;65(6):1651-5.
8. Bronden B, Dencker M, Allers M, Plaza I, Jonsson H. Differential distribution of
lipid microemboli after cardiac surgery. Ann Thorac Surg 2006; 81(2):643-8.

32
9. Yared JP, Starr NJ, Torres FK, et al. Effects of single dose, post-induction
dexamethasone on recovery after cardiac surgery. Ann Thorac Surg 2000;
69:1420-1424.
10. Moody DM, Brown WR, Challa VR, et al. Brain microemboli associated with
cardiopulmonary bypass. Ann Thorac Surg 1995; 59:1304-1307.
11. De Gasparis C. Human lung fat microembolism associated with cardiopulmonary
bypass: electron microscopic evidence. Scand J Thorac Cardiovasc Surg 1968;
2:84-91.
12. Arrants JE, Gadsden RH, Huggins MB, Lee WH, Jr. Effects of extracorporeal
circulation upon blood lipids. Ann Thorac Surg 1973; 15:230-242.
13. Reents W, Babin-Ebell J, Misoph M, et al. Influence of different auto transfusion
devices on the quality of salvaged blood. Ann Thorac Surg 1999; 68:58-62.
14. Kaza AK, Cope JT, Fiser SM, et al. Elimination of fat microemboli during
cardiopulmonary bypass. Ann Thorac Surg 2003; 75:555-559.
15. Engler RL, Schmid-Schoenbein GW, Pavelec RS. Leukocyte capillary plugging in
myocardial ischemia and reperfusion in the dog. Am J Pathol1983; 111: 98-111
16. Engler RL, Dahlgren MD, Morris DD, et al. Role of leukocytes in response to
acute myocardial ischemia and reflow in dogs. Am J Physiol 1986; 251: H314-
H323.
17. Gu YJ, van Oeveren W. Activation of plasma components by leukocyte removal
filters. ASAIOJ 1994; 40: M598- M601
18. Gu YJ, deVries AJ. Clinical performance of a high-efficiency rapid flow
leucocyte removal filter for leucocyte depletion of heparinized cardiopulmonary
bypass perfusate. Perfusion1995; 10: 425-30

33
19. Bruil, A. Leukocyte filtration: Filtration mechanisms and material design. pp 8-9.
Thesis 1993.
20. Smit JJ, de Vries AJ, Gu YJ, van Oeveren W. Efficiency and safety of leukocyte
filtration during cardiopulmonary bypass for cardiac surgery.1999; 20:151-65
21. Heggie AJ, Corder. Clinical evaluation of the new Pall leucocyte-depleting blood
cardioplegia filter (BC1). Perfusion 1998; 13: 17-25.
22. Liu YH, et al. The effects of cardiopulmonary bypass on the number of cerebral
microemboli and the incidence of cognitive dysfunction after coronary artery
bypass graft surgery. Anesth Analg 2009; 109(4):1013-22.
23. Grotjohan HP, Van der Heijde RMJL, Jansen JRC, et al. A stable model of
respiratory distress by small injections of oleic acid in pigs. Intensive Care Med
1996; 22:336-244.
24. Kaza AK, Cope JT, Fiser SM, et al. Elimination of fat microemboli during
cardiopulmonary bypass. Ann Thorac Surg 2003; 75:555-559.
25. Mastrangelo AM, Jeitner TM, Eaton JW. Oleic acid increases cell surface
expression and activity of CD11b on human neutrophils. J Immunol 1998;
161:4268-4275.
26. Engström KG. The embolic potential of liquid fat in pericardial suction blood, and
its elimination. Perfusion 2003; 18:69-74.
27. Rinder HM, Murphy M, Mitchell J, et al. Progressive platelet activation with
storage: evidence for shortened survival of activated platelets following
transfusion. Transfusion 1991; 31:409-414.
28. Schonfeld SA, Ploysongsang Y, DiLisio, R et al. Fat embolism prophylaxis with
corticosteroids. Ann Int Med 1983; 99:438-443.