Current Trends in Cardiovascular Pharmacology
17
Current Trends in Cardiovascular Pharmacology To help resolve abnori~lalities in cardiovascular function, many differ- ent types of drugs have been developed. Only recently, however, has there been increased emphasis on determining how these agents decrease morbidity and mortality. In some cases, standard drug therapy has been challenged somewhat by newer drugs or new applications of existing drugs that seem to provide better outcomes in terms of disease progression and survival. The purpose of this article is to provide an update on contemporary pharmacologic management of three common conditions: hypertension, congestive heart failure, and myocardial ischemia/infarction. Physical therapists should be aware of the rationale for using specific drugs in each condition and that these medications can have positive therapeutic effects and adverse side effects that can influence the patient's response to physical therapy. [Ciccone CD. Current trends in cardiovascular pharmacology. Phy~ 7'/1n: 1996;'76:481-49'7.1 Key Words: Cardiovascz~lar system, Drug therapy, Pharmacology. Charles D Ciccone Physical Therapy . Volume 76 . Number 5 . May 1996 Downloaded from https://academic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Current Trends in Cardiovascular Pharmacology
Current Trends in Cardiovascular Pharmacology
To help resolve abnori~lalities in cardiovascular function, many differ- ent types of drugs have been developed. Only recently, however, has there been increased emphasis on determining how these agents decrease morbidity and mortality. In some cases, standard drug therapy has been challenged somewhat by newer drugs or new applications of existing drugs that seem to provide better outcomes in terms of disease progression and survival. The purpose of this article is to provide an update on contemporary pharmacologic management of three common conditions: hypertension, congestive heart failure, and myocardial ischemia/infarction. Physical therapists should be aware of the rationale for using specific drugs in each condition and that these medications can have positive therapeutic effects and adverse side effects that can influence the patient's response to physical therapy. [Ciccone CD. Current trends in cardiovascular pharmacology. Phy~ 7'/1n: 1996;'76:481-49'7.1
Key Words: Cardiovascz~lar system, Drug therapy, Pharmacology.
Charles D Ciccone
Physical Therapy . Volume 76 . Number 5 . M a y 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

ardiovascular nledications represent onc of the largest and most frequently prescribed groups of drugs, and nlany patients receiving physical therapy also are taking medications fbr cardio-
vascular prohlerns. Because cardiovascular disease is so common in industriali~ed societies, development of new cardiovascular drugs is an obvious priority in pharmaco- logic research. There has, however, also been an empha- sis on examining how effective drugs are in actually improving morbidity and mortality associated with car- diovascular problems. Likewise, medications that are typically used for one form of cardiovascular disease are contiriually being studied to determine how effective they are in treating other cardiovascular problems.
The purpose of this article is to provide an update on the pharmacologic strategies currently used for three com- mon types of cardiovascular disease: hypertension, con- gestive heart failure, and myocardial ischemia/infarc- tion. Special emphasis will be placed on newer drugs and new applications of existing medications. This informa- tion will provide physical therapists with knowledge about the effects of these drugs and the rationale for why various medications are c~lrrently used.
Hypertension Hypertension, a chronic sustained increase in blood pressure, is a cornrnorl cardiovascillar condition that can lead to other problerrls such as myocardial infarction (MI), renal failure, and cerebrovascular accident. Cer- tain genetic or familial factors combined with lifestyle issues (poor diet, physical inactivity, levels of stress, and so forth) can contribute to a hypertensive state.'.' The exact cause of hypertension, however, is unknown in most patients.
Although a definitive cause of hypertension is usually not apparent, i t is known that the heart and peripheral vasculature typically undergo structural changes (remod- eling) that help sustain the elevated blood pressure and potentiate filrther increases in hypertension.:'-Vn par- ticular, vascular remodeling that causes thickening of arteriolar walls and a decrease in the internal diameter of arterioles and capillaries seems to be especially harm- ful in patients with hyper te t~s ion .~-~~ Likewise, hyperten- sion is associated with certain metabolic abnormalities such as glucose intolerance and inslllin resistance.7-I' That is, people with hypertension may have metabolic problems similar to those seen in the early stages of type I1 diabetes mellitus, where glucose metabolism is impaired because of reclllced sensitivity of peripheral tissues to insu1in.l' Patients with hypertension also are more prone to lipid abnormalities such as increased
serum triglycerides and cholesterol, and the atheroscle- rotic effects of increased blood lipids also may be exaggerated in h y p e r t e n s i ~ n . ~ : ~ , ~ ~
Drugs that traditionally have been used to reduce blood pressure are being reexamined to determine whether these agents have additional properties that favorably influence vascular remodeling and the metabolic abnor- malities associated with h y p e r t e n s i o ~ ~ . ~ ~ , ~ ~ Likewise, drugs that merely reduce blood pressure but do not favoriibly affect the other features of hypertension may not be the most adva~ltageous agents. The primary antihypertensive drugs categories are listed in Table 1, and the pharmacology of each category is addressed here.
Angiotensin-Converting Enzyme Inhibitors Development of drugs that inhibit angiotensin-convert- ing enLyine (ACE) is among the most important advar~cements in thc treatment of cardiovascular disease. Arlgiotensin-converting enzyme inhibitors were devel- oped during the 1980s to control activity of the systemic renin-angiotensin system in hypertension. This system is characterized by the interaction between renin, an enzyme released from the kidney, and angiotensinogen, a peptide circulating in the blood stream.17 A fall in blood pressure causes renin to he released from the kidneys, which catalyzes the conversion of angiotensino- gcn to angiotensin I. Angiotensin I i \ then converted to angiotcnsin I1 by ACE, which is located in the lungs and many other tissues. Angiotensin I1 is a very powerful vasoconstrictor that helps elevate blood pressure. Angio- tensin I1 (or its by-product, angiotensin 111) also pro- motes aldosterone release from the adrenal cortex, thus adding to the antihypotensive effect by increasing sodium and water retention.
Angiotensin-converting enzyme inhibitors decrease vas- cular resistance by limiting excessive production of angiotensin I1 in the bloodstream. Their actual role in hypertension, however, is probably much more com- plex. There is, for example, a fully functioning renin- angiotensin system located in many tissues in the body, including the brain, heart, and peripheral vascular tis- sues.l7,'8 Angiotensin-converting enzyme inhibitors, therefore, affect local production of angioterlsin I1 in these tissues as well as in the general circulation. Like- wise, angiotensin I1 produces effects other than just vasoconstriction and stimulation of aldosterone release. In particular, angiotensin I1 stimulates growth and pro- liferation of vascular smooth Thus, ACE inhibitors can influence vascular resistance directly by limiting the production of a powerful vasoconstrictor,
(:D (:icconr. I'hl), YI', is Associ;ltr Professor, Llepal-tment of Physical Therapy, School o f Health Science anrl Hu111all Per-fi)srnancr, lthaca (:ollegr, Ithaca, NY 14850 (USA) ([email protected]~).
482 . Ciccone Physical Therapy . Volume 76 . Number 5 . May 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022
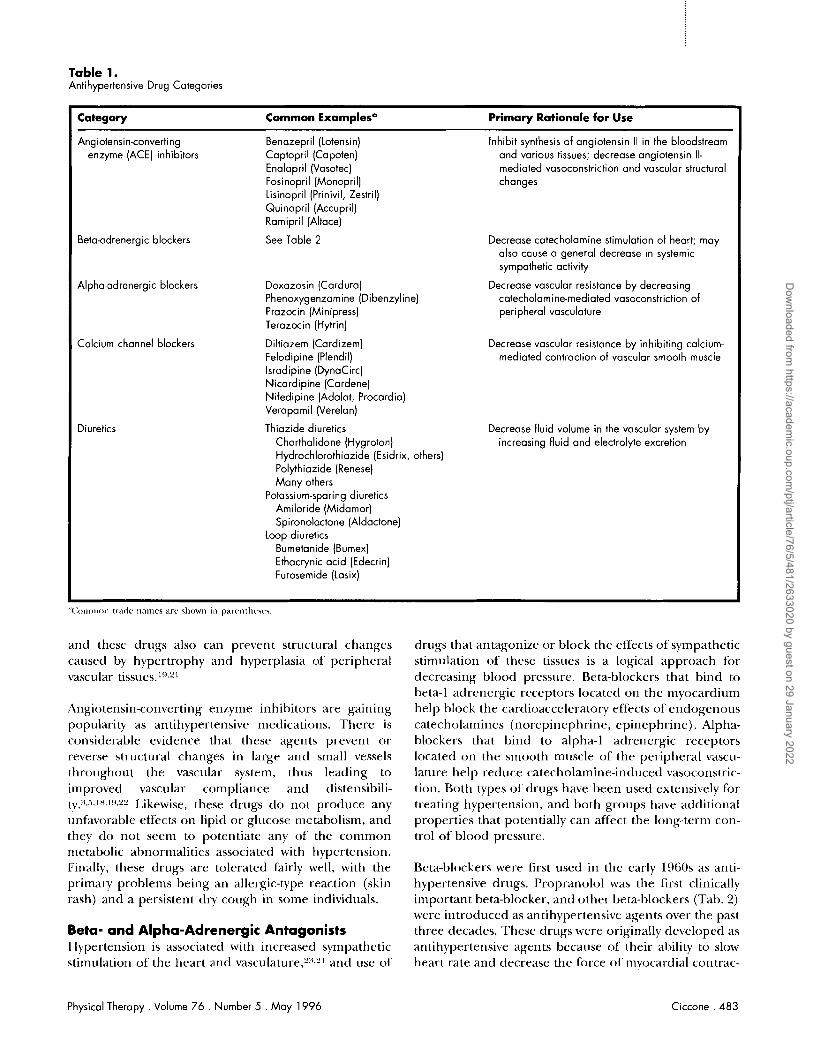
Table 1. Antihypertensive Drug Categories
Category Common Examplesa Primary Rationale for Use
Angiotensin-converting Benazepril (Lotensin) Inhibit synthesis of angiotensin II in the bloodstream enzyme (ACE) inhibitors Captopril (Capoten) and various tissues; decrease angiotensin II-
Enalapril (Vasotec) mediated vasoconstriction and vascular structural Fosinopril (Monopril) changes Lisinopril (Prinivil, Zestril) Quinapril (Accupril) Ramipril (Altace)
Beta-adrenergic blockers See Table 2 Decrease catecholamine stimulation of heart; may also cause a general decrease in systemic sympathetic activity
Alpha-adrenergic blockers Doxazosin (Cardura) Decrease vascular resistance by decreasing Phenoxygenzamine (Dibenzyline) catecholaminemediated vasoconstriction of Prazocin (Minipress) peripheral vasculature Terazocin (Hytrin)
Calcium channel blockers Diltiazem (Cardizem) Decrease vascular resistance by inhibiting calcium- Felodipine (Plendil) mediated contraction of vascular smooth muscle lsradipine (DynaCirc) Nicardipine (Cardene) Nifedipine (Adalat, Procardia) Verapamil (Verelan)
Diuretics Thiazide diuretics Decrease fluid volume in the vascular system by Chorthalidone (Hygroton) increasing fluid and electrolyte excretion Hydrochlorothiazide (Esidrix, others) Polythiazide (Renese) Many others
Potassium-sparing diuretics Amiloride (Midamor) Spironolactone (Aldactone)
Loop diuretics Burnetanide (Bumex) Ethacrynic acid (Edecrin) Furosemide (Lasix)
and these drugs also can prevent structural changes caused by hypertrophy and hyperplasia of peripheral vascular
Angiotensin-converting enzyme inhibitors are gaining popularity as antihypertensive medications. There is considerable evidence that these agents prevent or reverse structural changes in large and small vessels throughout the vascular system, thus leading to improved vascular compliance and distensibili- t ~ . ~ ~ , ~ , l ~ . l ! ~ , n ! ~ Likewise, these drugs do not produce any unfavorable effects on lipid or glucose metabolism, and they do not seem to potentiate any of' the common nletabolic abnormalities associated with hypertension. Finally, these drugs are tolerated fairly well, with the primary problems being an allergic-type reaction (skin rash) and a persistent dry cough in some individuals.
Beta- and Alpha-Adrenergic Antagonists Hypertension is associated with increased sympathetic stimulation of the heart and v a ~ c u l a t u r e , ~ : ~ , ~ ~ and use of
dnigs that antagonize or block the effects of sympathetic stimulation of these tissues is a logical approach for decreasing blood pressure. Beta-blockers that bind to beta-1 adrenergic receptors located on the myocardium help block the cardioaccelerato~ effects of endogenous catecholamines (norepinephrine, epinephrine). Alpha- blockers that bind to alpha-] adrenergic receptors located on the smooth muscle of the peripheral vascu- lature help reduce catecholamine-induced vasoconstric- tion. Both types of drugs have been used extensively for treating hypertension, and both groups have additional properties that potentially can affect the long-tern) con- trol of blood pressure.
Beta-blockers were first used in the early 1960s as anti- hypertensive drugs. Propranolol was the first clinically important beta-blocker, and other beta-blockers (Tab. 2) were introduced as antihypertensive agents over the past three decades. These drugs were originally developed as antihypertensive agents because of their ability to slow heart rate and decrease the force of myocardial contrac-
Physical Therapy . Volume 76 . Number 5 . May 1996 Ciccone . 483
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

Table 2. Betacldrenergic Blockers
shown inconsistent effects in their ability to reduce small-vessel h y p r r t r ~ p h y . ~
Intrinsic Generic Trade Beta Sympathomimetic 1 Name Name Sensitivity" Activity (ISA)
Acebutolol Atenolol Betaxolol Bisoprolol Carteolol Labetolol
Metoprolol Nadolol Penbutolol Pindolol Propranolol Sotalol Timolol
Sectral Tenormin Kerlone Zebeta Cartrol Normodyne,
Trandate Lopressor Corgard Levatol Visken lnderal Betapace Blocadren
Beta- 1 Beta-l Beta-1 Beta- 1 Nonselective Nonselectiveb
Beta-1 Nonselective Nonselective Nonselective Nonselective Nonselective Nonselective
Mild-moderate None None None Moderate None
None None Moderate High None None None
tion." Beta-t)lockers also have a general ability to decrease sy~npathetic activity throughout the body; that is, their antihypertenqive effects are not rnecliated exclu- sively by ;In inhibitory effect on the heart.-
There are approximately 13 beta-blockers that ar-c com- monly used as antihypertensive agents (Tab. 2) . These drugs are disting~iished f'rom one another by variotrs additional properties such as how well they bind to beta-1 receptors versus other beta-receptors (beta sensi- tivity) and whether they can prodlice low background levels of sympathetic stimulation while blocking exces- sive catecholamine effects (intrinsic sympathomimetic activity) ."5,'7 Certain beta-blockers such as labetolol have received a great deal of attention because these drugs have beta-blocking and alpha-blocking proper tie^.'^,") These drugs will decrease heart rate and contr;~ctility (beta-1 effect) while simultaneously decreasing periph- eral vascular resistance (alpha-l etf'ect). The conlbined cardiac and peripheral vascular effects should act syner- gistically to produce an optimal antihyperte~~sive effect.
The primary problem associated with beta-blockers is that these agents may produce excessive slowir~g of heart rate and contractility, resulting in depressed cardiac function. Beta-blockers, however, are generally well- tolerated, and serious adverse effects are infrequent. As a result, beta-blocker therapy has been one of the most common forms of' antihypertensive drug treatment. Nonetheless, there has been some criticisrrr of beta- l~lockers l,eca~~se these di.ugs do 1101 appreciably a k c t vascrilar remodeling in hypertension. That is, beta- blockers d o not seem to drcrcasc hypertrophy in large vessels such as the aorta, and specific beta-blockers have
Concern also has been raised because certain beta- blockers may perpetuate some of the metabolic prob- lerns associated with hypertension. Beta-blockers that lack intrinsic sympathomimetic activity can cause adverse changes in blood lipid profiles, including increased serum triglycerides and decreased high- density lipoprotein^.",'^' Patients with hypertension who receive beta-blockers also tend to have elevated plasma insulin and glucose levels tbllowing a glucose load, suggesting that these drugs promote glucose intolerance and insulin resist;~nce.:'" The reasons for these effects are not fully understood but are probably related to block- ade of beta-adrenergic receptors located on fat cells, liver cells, and other tissues, thus causing disruption of catecholamine-mediated control of lipid and carbohy- drate metabolism in these tissues. I,ikewise, certain beta- blockers such as the relatively nor~selective drugs (see Tab. 2) seem to have ;I greater tendency to produce adverse metabolic changes as compared with cardio- selective agents and beta-blockers with intrinsic sympa- thomimetic activity.
Beta-blockers produce Favorable hemodynamic changes in the heart and peripheral vasculatur-e that mediate a decrease in blood presstrre. The routine, long-term use of these medications in patients with hypertension has becn q~iestioned, however, because these drugs do not scem to produce distinct improvements in peripheral vascular structure and because some of these drugs may act~ially potentiate the metabolic problems associated with hypertension. The use of beta-blockers in hyperten- sion continues to be debated, and additional research will be needed to determine whether the beneficial 1 effects of these d r ~ ~ g s are outweighed by potential limi- tations such as increased metabolic abnormalities ill
certain patients.
Alpha-blockers were first used 21s antihypertensive agents in the 1970s. The lise of these agents in treating hyper: tension, however, has bee11 somewhat limited over the years because they tend to prodlice a fairly dramatic decrease i r ~ blood pressure that can cxtrse side effects such ;IS hypotension, orthostatic hypotension, and reflex tachycardia (ie, heart rate increases to compensate for the hypotensive effect). Thus, alpha-blockers often were reserved for more severe, advanced cases of hypertension.
Alpha-blockers co~ild be beneficial on a wider basis because these drugs lower blood pressure while produc- ing positive effects or1 glucose and lipid metabolism. Alpha-blockers seem t o decrease insulin resistance and improve glucose tolei-ance as well as decrease serum
484 . Ciccone Physical Therapy . Volume 76 . Number 5 . May 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

triglycerides and produce other beneficial effects on serum lipid profiles.'{'-t44 It follows that these drugs may be a usefill addition to the antihypertensive regimen for many patients, and it will be interesting to see whether alpha-blockers will be used more often in the future.
Calcium Channel Blockers Calcium channel blockers limit the entry of calcium into vascular tissues, thus limiting contraction of vascular smooth n iu~cle . '~These drugs were originally developed during the 1960s to prevent coronary artery constriction during vasospastic angina, but they gained widespread use as antihypertensive agents during the 1980~.:'"."~ Calcium channel blockers exert their antihypertensive effects primarily by decreasing calcium entry into peripheral vascular tiss~res, thus decreasing peripheral vascular constriction and resi~tance.:",~"
Calcium channel blockers may prevent or resolve some of the cardiovascular remodeling associated with hyper- tension. Long-term (6 rrionths) administratio~l of cal- cium channel blockers may help reduce structural changes in the left ventricle as well as small resistance vessels.'+x '"' These drugs seem to inhibit structural changes in the vasculature primarily through inhibition of vascular smooth-muscle cell proliferation and qecond- arily through inhibition of atherosclerotic plaque forma- tion in the vascular cell wall.40
Calciurri channel blockers have been used in an expanded role in treating various stages of hypertension, including cases of early or borderline hypertension. These drugs are associated with several side effects, including swelling in the feet and ankles, orthostatic hypotension, headache, and nausea.4' These agents also can influence heart rate, and certain calcium channel blockers (verapamil, diltiazem) are used routinely to manage certain cardiac arrhythmias. Recently, however, investigators reported that certain patients taking short- acting calcium channel blockers for treatment of hyper- tension had a 60% greater risk of MI compared with patients taking other antihypertensive medication^.^?,^:^
This finding has obviously caused concern about the use of these medications, and additional research is needed to clarify whether these medications should continue to be used in the treatment of hypertension.
Diuretics Diuretics increase renal sodium and water excretion.44 These drugs have been a mainstay in the treatment of hypertension since the 1950s because they reduce the amount of fluid in the vascular system, thus reducing intravascular pressure. Diuretics are often used as the first drug (monotherapy) in early or mild stages of hypertension, and these drugs also can be combined with other antihypertensive agents if blood pressure
continues to i n c r e a ~ e . ~ T h e primary adverse effects associated with these drugs are, predictably, fluid and electrolyte imbalances that are caused by excessive sodium, potassium, and water e x c r e t i ~ n . ~ ~ ~ , ~ ~ Severe adverse reactions are relatively rare, however, and diuret- ics are often advocated because they are generally safe and well-tolerated in most patient^.^^,^"
Diuretics continue to be used extensively as antihyper- tensive agent~.~"hese drugs do not, however, have any appreciable effect on vascular compliance or distensibil- ity."51Wore importantly, there is evidence that certain diuretics such as the thiazide and thiazide-like diuretics (Tab. 1) are associated with glucose intolerance and insulin resistance, and these drugs may increase serum triglyceride and cholesterol level^.".'^'^'^'^^^ These drugs, therefore, do not make any additional contribution to resolving the vascular consequences of hypertension, and certain types of diuretics may exaggerate the meta- bolic problems associated with high blood pressure. There has been a growing trend to use other drugs such as the ACE inhibitors or calcium channel blockers as initial therapy instead of the diuretic drugs.
Effects of Antihypertensive Agents on Morbidity and Mortality Traditional antihypertensive therapy using beta-blockers and diuretics is predicted to reduce the incidence of stroke by 33% to 50% and the incidence of MI and other events related to coronary heart disease by 4% to 22% in patients with mild to moderate h y p e r t e n ~ i o n . ~ ~ This effect seems true for middle-aged people with hyperten- sion, and these benefits may be even greater in elderly individuals with hype r t en~ ion .~ ' .~~
The major controversy currently surrounding antihyper- tensive drug therapy is whether or not the newer types of antihypertensive drugs (ACE inhibitors, calcium chan- nel blockers) can provide even greater benefits than traditional medications, especially with regard to coro- nary heart disease. The classic antihypertensive drugs (beta-blockers, diuretics) are very successf~~l in reducing the incidence of stroke and other problems, but these drugs are not as successful in preventing coronary heart disease and MI related to high blood p r e ~ s u r e . " ' ~ ~ ~ Diuretics and beta-blockers often produce unfavorable effects on serum lipids and glucose metabolis~n.~~) Drugs such as the ACE inhibitors, calcium channel blockers, and alpha-adrenergic blockers may be superior because they reduce blood pressure without causing u~ldesirable metabolic effects.
Over the last 10 years, there has been a clear reductioil in the use of beta-blockers and diuretics, with a concom- itant increase in the use of alternative agents such as ACE inhibitors and ca l c i~~m channel blocker^.'^,^^ These
Physical Therapy . Volume 76 . Number 5 . May 1996 Ciccone . 485
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

trends have occurred despite a paucity of evidence that these expensive newer drugs actually produce more favorable effects on morbidity and mortality than d o the less expensive drugs traditionally used to lower blood pressure. Several large clinical trials are currently in progress to compare conventional regirnens that priniar- ily use beta-blockers and diuretics with newer regimens that use ACE illhihitors, calcium channel blockers, and alpha-adrrnergic blockers.
Congestive Heart Failure Congestive heart failure (CHF) is characterized by a decrease in cardiac pumping ability that leads to inade- quate tissue perfusion and accunlulation of fluid (con- gestion) in the lungs and other organs.""."' Although the causes of'this condition may vary from patient to patient, it appears that some type of injury to the myocardium often initiates a progressive decline in myocardial f ~ ~ n c - tion."' As the heart fails, several compensatory neuro- humoral mechanisnis occur, irlcl~~cling increased syrnpa- thetic nervous systertl activation and increased activation of the renin-angioterlsil~ syste~n.~'.~:' Rather than helping alleviate heart failure, these compensatory changes nlay actually exacerbate myocardial dysfilnction by increasing cardiac work load. The prognosis for patients with heart failure often is rather poor, with 5-year mortality rates estimated at 60% and 45% fbr men and women, re~pectively.":~
Drug therapy for heart failure traditionally has focused on two primary goals: increasing cardiac pumping ability (positive inotropic effect) and decreasing cardiac work load by reducing vascular resistance or the amount of' fluid in the vascular system.64 More recently, ernphasis has been placed on selecting drugs that also help resolve the nellrohumoral compensations that contribute to the progressiori of myocardial dysfunction in heart failure. Attempts also have been made to use drugs or drug combinations that not only decrease the symptoms of CHF but act~lally decrease the rather high mortality rate associated with this disease.
Drugs Used to Improve Cardiac Pumping Abiliiy in CHF
Digitalis glycosides. Digitalis glycosides such as digoxin ([,anoxin) and digitoxin (Crystodigin) have been used to treat heart failure for over 'LOO years, and these agents continue to be one of the most commonly prescribed medications in the United These drugs increase cardiac pumping ability through a complex mechanism that ultimately results in increased intracel- lular ralciurn in myocardial Increased intracel- lular calcium improves the inechanical pumping ability of myocardial cells by facilitating increased interaction of contractile filaments. Digitalis drugs also exert elec- trophysiologic effects that slow heart rate and iiornialize
autonomic influence on the heart by decreasing sympa- thetic influence and increasing parasympathetic activi- ty."!' This combination of digitalis' mechanical and elec- trophysiologic effects improves myocardial contractility and filnctiorl, thus helping to improve the symptoms of heart f ' a i l~re .~"
Despite their comnion use, these dr-ugs have a relatively small rnargin of safety, and accumulation of digitalis in the body can lead to serious problems with digitalis toxicity." Digitalis toxicity is characterizecl by symptoms such as fatigue, confusion, gastrointestirlal problems, and cardiac arrhythmia^.^^ Questiorls about the efficacy of' digitalis also have been raised because the prognosis of patients with heart failure often remains poor even when these patients are treated with digitalis. Digitalis can decrease symptoms of heart Failure and provide short-tern1 improvements in cardiac function but does not seem to stop the progression of' heart failure or decrease the high nlortality rate."5."' 7y As a result, con- siderable effort has been made to find other agents that are safer and mor-e effective than digitalis. Alternatively, the combination of digitalis with other agents such as ACE inhibitors has been investigated as a means of providing optirrial survival in patients with CHF.70
Other positive inotropic agents. Agents such as phos- phodiesterase (PDE) inhibitors and dobutamine have been used on a limited basis in certain cases of CHF because these drugs produce an increase i r ~ cardiac pumping ability (positive inotropic effect) .79 Phospho- diesterase inhibitors such as amrillone (Inocor) and rnilrinone (Prirnacor) have been developed over the last 10 year^.^-*-^" These agents inhibit the PDE enzyme located in cardiac cells, thus allowing cyclic adenosine monophosphate (CAMP) to i nc rea~e .~" Increased CAMP fncilitates calcium influx into the myocardial cells, and increased intracellular calcium facilitates myocardial coritractility because of increased interaction of contrac- tile These medications also produce moder- ate levels of peripheral vasodilation, which enhances their beneficial effects by decreasing the amount of blood returning to the heart (cardiac preload) and by decreasing the pressure the heart. must pump against (cardiac afterload) .75,7"
Phosphodiesterase inhibitors were developecl as a possi- ble alternative to digitalis drugs. There is rlo conclusive eviclence, however, that these agents are more effective than digitalis drugs in the long-term management of CHF. More importantly, evidence exists that PDE inhih itors may actually have a greater risk of adverse effects, including an increased nior~ality rate, as compared with digitalis.7%75 Currently, PDE inhibitors are administered
intravenously for the short-term ( < 5 days) treatment of severe CHF,74 but these drugs do not seem to play an
4 8 6 . Ciccone Physical Therapy . Volume 7 6 . Number 5 . May 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

import an^ role in the long-term management of heart failure.
Dobutamine (Dobutrex) has traditionally been used for the short-term management of acute heart f a i l ~ r r e . ~ ~ . ~ ~ This drug increases myocardial contractility by directly stim~rlating beta-1 receptors on the heart.7" Dobutamine ;rlso reduces cardiac afterload by blocking the effects of catecholamines on vascular alpha-1 receptors.77 The combinecl effects of increased cardiac contl-actility and decreased cardiac afterload make this drug especially va1u;ible in the short-term treatment of cardiac decom- pensation following heart surgery and MI."
Use of dobutamine in the long-term management of CHF has been somewhat limited, however, because of side effects such as cardiac a r r h y t h r n i a ~ ~ ~ ~ ~ ~ and because patients often become tolerant to dobutamine during continuous administration of this agent.77 Likewise, dobutamine must be administered by intravenous infu- sion, thus making routine use of this drug somewhat impractical for community-dwelling patient~.~Z Portable infusion pumps, however, may enable certain patients to receive continuous dobutamine infusion at home for prolonged Problems with drug toler-ance can be minimizecl by instituting dobutamine-free inter- vals on ;i periodic basis.H5 It does not appear that dob~itamine therapy increases survival, but this drug may temporarily improve symptoms in some patients with advanced CHF who are refractory to more conventional forms of treatment.x"~s7
Beta-blockers. Beta-adrenergic blockers decrease cate- cholaniine-induced stimulation of the myocardium, thereby decreasing heart rate and myocardial contrac- tion. It may seem odd, therefore, that these drugs would be helpful in heart hilure, a condition in which pump- ing ability is already compromised. Heart failure is characterized, however, by an increase in sympathetic stimulation of the myocardium through the local release of norepinephrine from sympathetic neive terminals and from circiilating catecholamines from the adrenal r r ~ e d i r l l a . ~ ~ ~ ~ ~ ~ Excessive sympathetic stimulation reslilts in a rapid but ineffective heart rate (tachycardia), which furtiler compromises the pumping ability of the heart. Beta-blockers inhibit sympathetic stimulation of the myocardium, which improves ventricular function by prolongir~g diastolic filling time and promoting more complete emptying during s y s t ~ l e . ~ ~ - ! ~ ~
Beta-blockers are currently being considered a way of enhancing cardiac function in certain types of heart f'ailure. In particular, drugs that have combined beta- blocking and alpha-blocking effects (rg, labetolol; see 'I'ab. 2) may be especially advantageous because these agents will help normalile cardiac sympathetic effects
through beta-1 blockade and decrease carcliac preload and afterload through alpha-1 blockade.Hx Investigations currently in progress will help determine the optimal way that beta-blockers can be used with other medica- tions and whether the addition of beta-blocker therapy will help decrease the morbidity and mortality com- monly seen in patients with CHF.H".'"l
Drugs Used to Reduce Vascular Resistance or Fluid Volume in CHF
Diuretics. Diuretics increase sodium and water excre- tion, thus reducing the amount of fluid in the vascular system. This effect is beneficial in patients with heart failure because diuretics help reduce excess fluicl that has accun~~ilated in the lungs and other organs.'" Diuret- ics seem especially helpful when combined with other agents such as digitalis or ACE inhibitors.":' As a result, these agents have been used on a widespread basis for several decades to treat patients with heart failure, and these drugs will probably continue to play a principal role in the management of heart failure in the futlire.
ACE inhibitors. Angiotensin-convertirlg enzyme inhibi- tors have been used increasingly to treat patients who have heart failure because the renin-angiotensin system is activated in heart failure, resulting in increased vascu- lar resistance through the vasoconstrictive efftcts of angiotensin I1 and through the str-uctural/ren~odeling effects inducecl by angiotensin I1 on vascular tissues. Increased vascular resistance increases the pressure that the heart must pump against (afterload), and this increase in cardiac afterload is extremely detrimental to the failing heart. Angiotensin-converting enzyme inhib- itors block the synthesis of circulating levels of angioten- sin 11, thus decreasing vascular resistance ancl cardiac afterload. Some of the beneficial effects also are medi- ated through local inhibition of the renin-angiotensin system located directly within the myocardi~im and vas- cular walls.!'2
Angiotensin-converting enzyme inhibitors improve car- diac function ancl decrease the symptoms associated with CHF, especially poor exercise t ~ l e r a n c e . " ~ J ' ~ These drugs also may produce more long-term improvement in car- diac function than traditional CHF medications (diuret- ics, digitalis), and there is considerable evidence that ACE inhibitors sttbstantially reduce the morbidity and mortality associated with this disease.'" The effects of ACE inhibitors on morbidity and mortality i l l people with CHF is addressed later in this article.
Other vasodilators. Various vasodilating drugs have been used to decrease vascular resistance and cardiac preload and afterload in patients with CHF. These agents typically cause relaxation of vascular tissues by
Physical Therapy . Volume 7 6 . Number 5 . M a y 1996 Ciccone . 4 8 7
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

directly inhibiting smooth-muscle contraction (eg, hydralazine, ~ninoxidil, organic nitrates) or by decreas- ing sympathetic stirnulation of' the peripheral vascula- ture (eg, pra~osin) . !)~~."~ Regardless of the drug mecha- nism, reduction in vascular resistance helps decrease the work load on the failing heart.
Various vasodilators have been introduced over the past 30 years that have been helpfill for pa~ients with CHF. These vasodilators typically have been used in combina- tion with other drugs such as digoxin and diuretic^.'^>"^ Continued use of these vasodilators may diminish some- what in the filture, however, because ACE inhibitors seem to provide more effective and longer-lasting con- trol of peripheral resistance in patients with CHF.!)"
Effects of Pharmacotherapy on Morbidity and Mortality in CHF (:onventional treatment of CHF with drugs such as digitalis, diuretics, and vasodilators may produce short- term benefits that help decrease the symptoms of this disease, but there is little evidence that these drugs clelay the progression of heart failure and reduce the risk of death from CHF.!)!' In contrast, ACE inhibitors appar- ently provide rnore long-term improvement in cardiac function ant1 help decrease morbidity and mortality of patients with CHF. ""J-loMeta-analysis of recent clinical trials of patients with C:HF indicated that total mortality was reduced by 28% and that the combined incidence of death and hospitalizatioii was reduced by 31% when ACE inhibitors were administered instead of a placebo.?'"
As a result, there is an indication that pharmacologic treatment may help improve the prognosis of patients with CMF. Current treatment of many patients consists of' ACE inhibitors used alone or in combination with other more convel~tional drugs (diuretics, digitalis, other vasodilators). Nonetheless, the mortality rate con- tinues to be rather high for people with CHF, and additional research is needed to determine the optimal use of ACE inhibitors and other drilgs in treating specific types of CHF.IO''
Myocardial Ischemia and Infarction l'roblems related to myocardial ischemia and inf:arction remaill the leading cause of death in the United States and other industrialized nations."" Factors contributing to myocardial ischerrlia are complex, but ischemia is caused primarily by coronary artery atherosclerosis that decreases the ability o f the coronary arteries to supply adequate oxygen to rneet the demands of the myocardi- um."" An imbalance between niyocardial oxygen supply and demand causes the characteristic symptoms of' pain associated with angina pectoris. Progressive atheroscle- rosis also leads to the development of coronary artery thrombosis, resulting in vessel occlusion and
Drug therapy for ischemic heart disease has focused on resolving an acute irnhalance between myocarclial oxy- gen supply and myocardial oxygen delnancl; that is, drugs are often used to treat the syinptolnh of ischemic heart disease (angina pt-ctoris) and restore myocardial oxygen balance before additional damage occurs to the heart. More recently, however, attention also has been directed toward preventing ischemia ancl infarction by controlling the factors that lead to coronary occlusion or by resolving thrombus forn~ation in the coronary arteries.
Drugs Used to Treat Symptoms of Ischemia: Antiangina/ Medications
Nitrates. Organic nitrates such as nitroglycerin have 1,eeri used since the mid-1800s to prevent or decrease symptoms of angina pectoris. Nitrates are potent vasodi- lators because they are metaholizecl in vascular tissues to form nitrous oxide, a po~verf'ul inhibitor of vascular smooth-nii~scle c o n t r a c t i ~ n . ~ ~ ) ~ - ' ~ ) ~ It was originally held that nitrates decrease anginal symptoms by increasing coronary artery dilation, thus increasing myocardial blood flow and oxygen supply. It is now understood, however, that these agents decrease angina primarily by increasing peripheral venous dilation. thus reducing cardiac preload, and, to a lesser extent, by increasing arterial dilation, thus decreasing cardiac afterload.")" Nitrates, therefore, act primarily as peripheral vasodila- tors, decreasir~g myocardial oxygen demand ancl reduc- ing or relieving angi~ial
Nitrate tablets are traditionally administered suhlin- gually at the onset of' an anginal episode to resolve symptoms. Sublingual administration allows the drug to be absorbed rapidly into the systeinic circulatio~i without first being metabolized and destroyed in the liver, as would occur if these drugs were taken orally and absorbed from the gastrointestinal tract (a phenornenoll known as the first-pass effect).I0" An alternative method of' nitrate administration is through transderrnal patches. Patch administration provides a slow, steady infusion of the drug into the systemic circulation, and this type of drug delivery seems to prevent the onset of arigiria better than conventional sublingual tablets.
Many anginal episodes are asymptomatic or "silent" and can only be detected through electrocardiographic inon- itoring.lo"-lll Patch administration may help control episodes of silent ischemia that would not be treated through sublingual administration because the person would be unaware that an anginal episode was occurring.
The primary side effects of nitrates are clue to the drugs' vasodilating properties. Headache, dizziness, and ortho-
488 . Ciccone Physical Therapy . Volume 76 . Number 5 . May 1995
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

static hypotension are fairly common, especially imme- diately after administration of a sublingual dose.-" Tol- erance, or a decrease in drug effectiveness, also may develop during continuous nitrate use, especially when transderrnal patches are used to deliver these drugs on a daily basis.Iofj Nitrate tolerance can be prevented, how- ever, by instituting daily nitrate-free periods when the patch is not worn. A person can wear the patch, for example, for 12 hours and take the patch off for 12
The daily period when the patch is worn should correspond to the part of the day when each person experiences the majority of anginal episodes, thus providing optimal benefits while still instituting nitrate-free intervals to prevent tolerance.
Calcium channel blockers. Calcium channel blockers were developed in the 1960s to treat angina pectoris, and the number of calcium channel blockers and their use for angina as well as for other conditions (hypertension, arrhythmias) has grown over the past 30 years. The primary role of calcium channel blockers in ischemic heart disease is to increase coronary artery dilation and provide increased perfusion and oxygen delivery,Il4 which reduces symptoms of effort (classic angina) as well as angina caused by coronary artery vasospasm (Prinz- metal's i ~ c h e m i a ) . ~ ' ~ . ~ ] ~ Calcium channel blocker drugs cause coronary vasodilation by limiting calcium entry into coronary artery smooth-muscle cells and by limiting calcium release from intracellular storage site^.^^^,^^^
Decreased cytosolic calcium in the vascular smooth- muscle cells results in less interaction of contractile filaments, thus promoting vascular relaxation and dilation.
Selection of a particular agent for treatment of angina depends on each patient's symptoms and concomitant problems (common calcium channel blockers are listed in Tab. 1). Agents such as diltiazem and verapamil, for example, also have antiarrhythmic effects, and some of their beneficial effects in preventing ischemia and infarction are undoubtedly related to their ability to stabilize heart rate in certain individuals.llb Calcium channel hlockers may cause side effects such as periph- eral edema (ankle swelling), and there may be serious concerns about the fact that these drugs may actually increase the risk of infarction in some patients. In particular, moderate to high doses sf the short-acting form of nifedipine have been associated with a signifi- cant increase in the risk of mortality in patients with coronary heart disease.42 Research is under way to determine the reason for this increased risk and to determine whether other calcium channel blockers pose similar risks to patients who have coronary heart disease.
Beta-blockers. The effectiveness of beta-blockers in treating patients who have ischemic heart disease was
realized soon after these drugs were introduced as antihypertensive agents.l17 These drugs have been used for more than 20 years to decrease cardiac work load and oxygen demand, thus preventing symptoms of angina pectoris in certain individuals. Likewise, beta-blockers have antiarrhythmogenic effects, and some of their benefits in myocardial ischemia are related to their ability to stabilize heart rate and prevent some of the more serious types of rhythm disturbance^."^
Perhaps one of the most important effects of beta- blockers is their ability to help prevent reinfarction following MI. These drugs apparently reduce cardiac work load and prevent postinfarction arrhythmias, thus allowing the damaged heart to recover more complete- ly.1151-122 Use of beta-blockers and other agents (throm- bolytic drugs, aspirin) should enable patients to survive infarction as well as limit cardiac damage, thus allowing them to begin earlier and more aggressive cardiac rehabilitation programs.
Drugs Used to Prevent or Resolve Coronary Thrombosis and Infarction
Thrombolytic agents. Perhaps the most exciting phar- macologic advancement for treating acute MI has been the development of thrombolytic drugs. These agents are relatively new, having appeared on the market only within the last 5 to 10 years. Thrombolytic drugs facili- tate the breakdown of clots that have already formed in the coronary arteries, thus reestablishing myocardial perfusion and oxygenation.'" This effect can limit infarct size and help restore function to the myocar- dium, thus reducing mortality and improving recovery in patients who have sustained an acute i n f a r ~ t i o n . ~ ~ ~ - ~ ~ " Thrombolytic agents originally were thought to be effec- tive only if administered directly into the blocked coro- nary artery via cardiac ~a the ter iza t i0n . l~~ These drugs can be administered intravenously into the systemic circulation, where they will activate specific clot- dissolution factors that eventually act at the site of thrombosis (ie, the coronary artery) .lY4 There also seems to be a fairly large window of opportunity (3-6 hours) for administering these agents following the onset of
It is undoubtedly best, however, to begin thrombolytic treatment as soon as possible follow- ing the onset of
Thrombolytic agents that are currently used to treat acute MI are listed in Table 3. These agents initiate clot breakdown by directly or indirectly converting plasmin- ogen (profibrinolysin) to plasmin (fibrinolysin).12:' There has been considerable debate about which type of thrombolytic agent is safest and most effective.'^ Tissue plasminogen activator (t-PA), a substance that is identi- cal to the body's endogenous thrombolytic activating
Physical Therapy . Volume 76 . Number 5 . M a y 1996 Ciccone . 489
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022
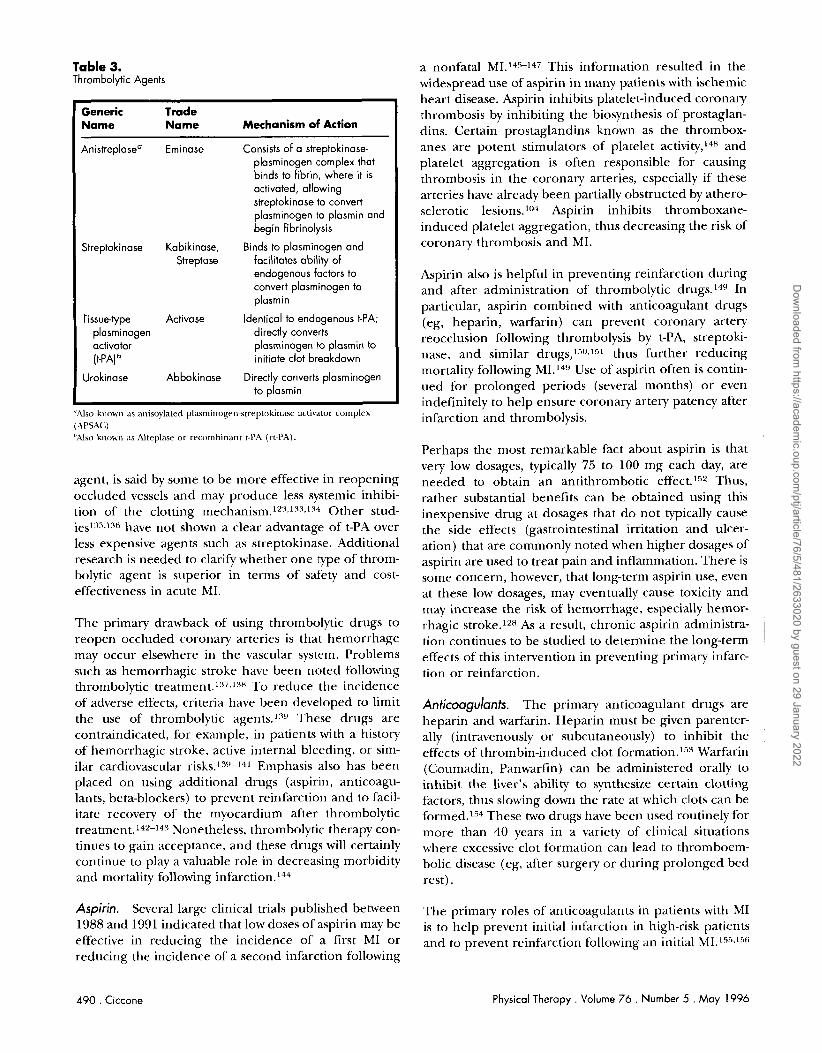
Table 3. Thrombolytic Agents
Generic Trade Name Name Mechanism of Action
Anistreplasea Eminase Consists of a streptokinase- plasminogen complex that binds to fibrin, where it is activated, allowing streptokinase to convert plasminogen to plasmin and begin fibrinolysis
Streptokinase Kabikinase, Binds to plasminogen and Streptase facilitates ability of
endogenous factors to convert plasminogen to plasmin
Tissuetype Activase Identical to endogenous t-PA; plasminogen directly converts aclivator plasminogen to plasmin to (t-PA] initiate clot breakdown
Urokinase Abbokinase Directly converts plasminogen to plasrnin
a nonfatal MI.I4"-" This information resulted in the widespread use of aspirin in many patients with ischemic heart disease. Aspirin inhibits platelet-induced coronary thrombosis by inhibiting the biosynthesis of prostaglan- dins. Certain prostaglandins known as the thrombox- anes are potent stimulators of platelet and platelet aggregation is often responsible for causing thrombosis in the coronary arteries, especially if these arteries have already been partially obstructed by athero- sclerotic lesions.104 Aspirin inhibits thromboxane- induced platelet aggregation, thus decreasing the risk of coronary thrombosis and MI.
':%lso known as Alteplasr or- r-rcombiriarit t-PA (r-t-PA)
".4lso kllow11 as anisovlated plasminogrn-str-eptoki~lasr activator- complex
agent, is said by some to be more effective in reopening occluded vessels and may produce less systemic inhibi- tion of the clotting mechan i~m.~z :~> l - l~ ,~~* Other stud- ie~l:~"l-l%ave not shown a clear advantage of t-PA over less expensive agents such as streptokinase. Additional research is needed to clarify whether one type of throm- bolytic agent is superior in terms of safety and cost- effectiveness in acute MI.
Aspirin also is helpful in preventing reinfarction during and after administration of thrombolytic In particular, aspirin combined with anticoagulant drugs (eg, heparin, warfarin) can prevent coronary artery reocclusion following thrombolysis by t-PA, streptoki- nase, and similar drugs,'"sl" thus further reducing mortality following MI.'" Use of aspirin often is contin- ued for prolonged periods (several months) or even indefinitely to help ensure coronary artery patency after
The primary drawback of using thrombolytic drugs to reopen occluded coronary arteries is that hemorrhage may occur elsewhere in the vascular system. Problems such as hemorrhagic stroke have been noted following thrombolytic treatment.l:".l:'* To reduce the incidence of adverse effects, criteria have been developed to limit the use of thrombolytic agents.':'" These drugs are contraindicated, for example, in patients with a history of hemorrhagic stroke, active internal bleeding, or sim- ilar cardiovascular ri~ks.~""-141 Emphasis also has been placed on using additional drugs (aspirin, anticoagu- lants, beta-blockers) to prevent reinfarction and to facil- itate recovery of the myocardium after thrombolytic treatment.14'-1" Nonetheless, thrombolytic therapy con- tinues to gain acceptance, and these drugs will certainly continue to play a valuable role in decreasing morbidity and mortality following i n f a r ~ t i 0 n . I ~ ~
(hPSAC) infarction and thrombolysis.
Aspirin. Several large clinical trials published between 1988 and 1991 indicated that low doses of aspirin may be effective in reducing the incidence of a first MI or reducing the incidence of a second infarction following
Perhaps the most remarkable fact about aspirin is that very low dosages, typically 75 to 100 mg each day, are needed to obtain an antithrombotic effect.l5z Thus, rather substantial benefits can be obtained using this inexpensive drug at dosages that do not typically cause the side effects (gastrointestinal irritation and ulcer- ation) that are commonly noted when higher dosages of aspirin are used to treat pain and inflammation. There is some concern, however, that long-term aspirin use, even at these low dosages, may eventually cause toxicity and twny increase the risk of hemorrhage, especially hemor- rhagic stroke.IzH As a result, chronic aspirin administra- tion continues to be studied to determine the long-term I effects of this intervention in preventing primary infarc- tion or reinfarction.
Anticoagulants. The primary anticoagulant drugs are heparin and warfarin. Heparin must be given parenter- ally (intravenously or subcutaneously) to inhibit the effects of thrombin-induced clot formation.lm Warfarin (Coumadin, Panwarfin) can be administered orally to inhibit the liver's ability to synthesize certain clotting factors, thus slowing down the rate at which clots can be formed.'" These two drugs have been used routinely for more than 40 years in a variety of clinical situations where excessive clot formation can lead to thromboem- bolic disease (eg, after surgery or during prolonged bed rest).
The primary roles of anticoagulants in patients with MI is to help prevent initial infarction in high-risk patients and to prevent reinfarction following an initial MI.155.156
490 . Ciccone Physical Therapy . Volume 76 . Number 5 . May 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022
Warfarin and heparin often are combined with aspirin to provide maximal protection against coronary occlusion or r e o c c l ~ s i o n . ~ ~ ~ There is consensus that use of an anticoagillant (heparin or warfarin) combined with an antiplatelet drug (aspirin) provides greater benefit than either type of drug given separately.12:This fact makes sense considering that each type of drug affects different aspects of the clotting mechanism, thus providing a synergistic and additive effect.
Predictably, the primary concern with anticoagulant use is the risk of hemorrhage.'",lfl This risk can be mini- mized, however, by using fairly low dosages of each type of agent and by routinely monitoring blood coagulation levels to ensure that hemostasis is not excessively inhibited.151
Lipid-lowering drug therapy. Lipid-lowering agents have been used for more than 30 years to help improve serum lipid profiles and decrease coronary atherosclerosis, the primary underlying factor in coronary artery disease (CAD) .1(J4,1m Various forms of hyperlipidemias and dys- lipidemias contribute to atherosclerotic plaque forma- tion in the coronary arteries, thus causing narrowing of the coronary artery lumen and subsequent thrombo- sis.'" Some serum lipid abnormalities that are associated with CAD include high triglyceride levels, high total cholesterol levels, increased low-density lipoprotein (LDL)-cholesterol levels, reduced high-density lipopro- tein (HDL)-cholesterol levels, or various combinations of these and other abnormalities.'"-1ti1 Lipid-lowering drug therapy may be helpful in many patients to help provide optimal control over abnormal lipid profiles, especially when nonpharmacologic interventions (diet, exercise) are unsuccessful.162
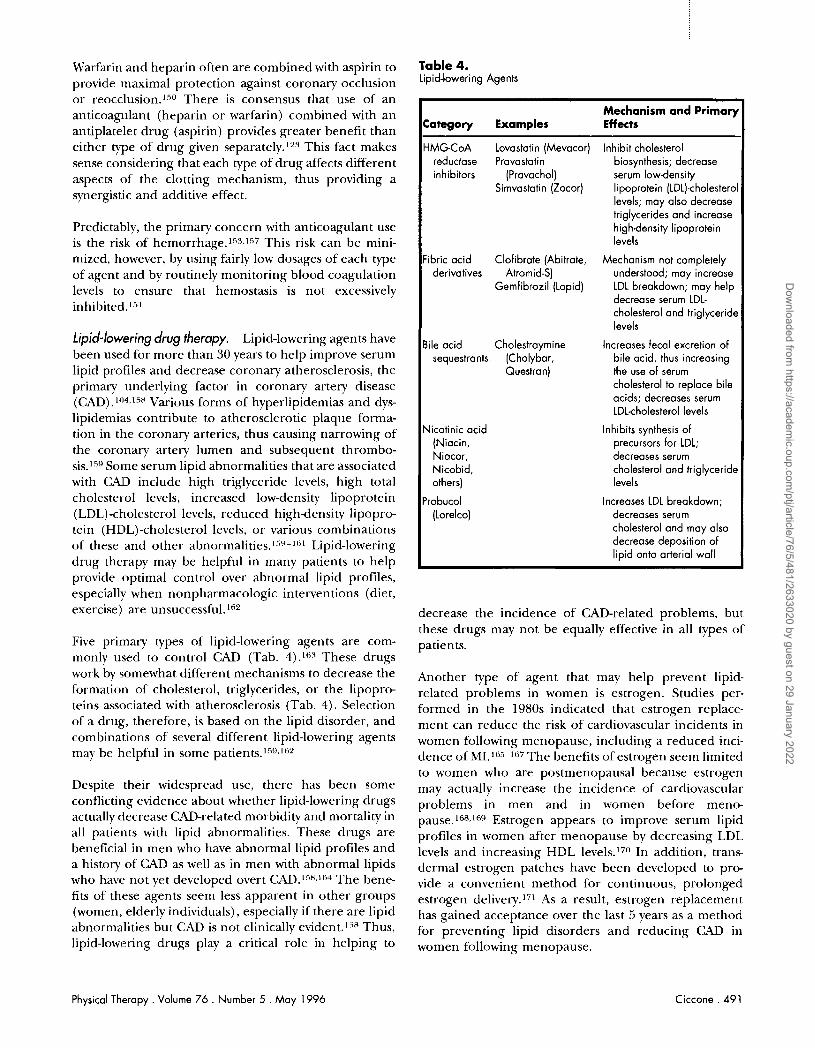
Five prirnary types of lipid-lowering agents are com- monly used to control CAD (Tab. 4).IK4 These drugs work by somewhat different mechanisms to decrease the formation of cholesterol, triglycerides, or the lipopro- teins associated with atherosclerosis (Tab. 4). Selection of a drug, therefore, is based on the lipid disorder, and combinations of several different lipid-lowering agents may be helpful in some p a t i e n t ~ . ~ ~ ~ J ~ z
Despite their widespread use, there has been some conflicting evidence about whether lipid-lowering drugs actually decrease CAD-related morbidity and mortality in all patients with lipid abnormalities. These drugs are beneficial in men who have abnormal lipid profiles and a history of CAD as well as in men with abnormal lipids who have not yet developed overt CAD.15H.1M The bene- fits of these agents seem less apparent in other groups (women, elderly individuals), especially if there are lipid abnormalities but CAD is not clinically evident.15H Thus, lipid-lowering drugs play a critical role in helping to
Table 4. Lipid-lowering Agents
Mechanism and Primary Category Examples Effects
HMG-CoA Lovastatin (Mevacor) Inhibit cholesterol reductase Pravastatin biosynthesis; decrease inhibitors (Pravachol) serum lowdensity
Simvastatin (Zocor) lipoprotein (LDL)-cholesterol levels; may also decrease triglycerides and increase highdensity lipoprotein levels
Fibric acid Clofibrate (Abitrate, Mechanism not completely derivatives Atromid-S) understood; may increase
Gemfibrozil (Lopid) LDL breakdown; may help decrease serum LDL- cholesterol and triglyceride levels
Bile acid Cholestraymine Increases fecal excretion of sequestrants (Cholybar, bile acid, thus increasing
Questran) the use of serum cholesterol to replace bile acids; decreases serum LDL-cholesterol levels
Nicotinic acid Inhibits synthesis of (Niacin, precursors for LDL; Niacor, decreases serum Nicobid, cholesterol and triglyceride others) levels
Probucol Increases LDL breakdown; (Lorelco) decreases serum
cholesterol and may also decrease deposition of lipid onto arterial wall
decrease the incidence of CAD-related problems, but these drugs may not be equally effective in all types of patients.
Another type of agent that may help prevent lipid- related problems in women is estrogen. Studies per- formed in the 1980s indicated that estrogen replace- ment can reduce the risk of cardiovascular incidents in women following menopause, including a reduced inci- dence of MI.165167 The benefits of estrogen seem limited to women who are postmenopausal because estrogen may actually increase the incidence of cardiovascular problems in men and in women before meno- pause.16H,1E"strogen appears to improve serum lipid profiles in women after menopause by decreasing LDL levels and increasing HDL 1e~e l s . l~~) In addition, trans dermal estrogen patches have been developed to pro- vide a convenient method for continuous, prolonged estrogen de1 i~e ry . I~~ As a result, estrogen replacement has gained acceptance over the last 5 years as a method for preventing lipid disorders and reducing CAD in women following menopause.
Physical Therapy . Volume 76 . Number 5 . May 1996 Ciccone . 491
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

Effects of Pharmacotherapy on Morbidiv and Mortaliv in Myocardial Ischemia and Infarction In contrast to drugs that merely decrease symptoms of angina (nitrates), agents that prevent or resolve coro- nary thrombosis may help reduce illness and death associated with coronary heart disease. In particular, early administration of thrombolytic agents following acute MI is associated with reduced mortality.17' Two large clinical trials that compared thrombolytic treat- ment using streptokinase with no thrombolytic treat- ment demonstrated that in-hospital mortality was reduced by 15%'7.i and 23%.174 Results of subsequent studies suggested that these benefits were even greater when acute thrombolytic treatment (streptokinase, t-PA) was combined with other agents such as aspirin and heparin. 1'",1",13",l74
Mortality and morbidity also are substantially reduced when certain drugs are administered for prolonged periods to prevent reinfarct~on following MI. Angioten- sin-converting enzyme inhibitors, for example, may be helpful in patients who survive MI but have decreased left ventricular fun~tion.~75,17" The risk of developing a recurrent MI was reduced by 25% and the risk of death from recurrent MI was reduced by 32% when the ACE inhibitor captopril was administered instead of a place- b0.~7"imilarly, administration of ramipril (another ACE inhibitor) versus a placebo resulted in a 27% reduction in the risk of death in a population of high- risk patients who had sustained an infar~tion.l7~
Drugs such as aspirin, beta-blockers, anticoagulants, and lipid-lowering agents also can be administered to reduce morbidity and mortality postinfarction or to prevent infarction in specific high-risk patients. As a result, in studies that are currently in progress, attempts are being made to compare various combinations of these agents to determine which drugs are most effective in prevent- ing infarction or reinfarction.
Clinical Implications Cardiovascular medications affect cardiovascular adapta- tions to an acute bout of exercise and to exercise training.l77 For example, cardiovascular responses to exercise are attenuated somewhat in patients who are taking beta-blockers because these drugs limit the increase in heart rate and myocardial contractility that typically occurs as exercise work load increases. Some patients, however, may actually have an improved ability to exercise because cardiovascular medications help control symptoms that limit an exercise bout. The patient who is limited by symptoms of angina pectoris or CHF, for example, may actually have an improved ability to exercise if these symptoms are controlled by the appropriate medications. In this article, it is not possible to review all the potential ways that cardiovascular drugs
can influence exercise responses, and this topic has been addressed e l ~ e w h e r e . ' ~ ~ , ~ ~ ~ Therapists should be aware, however, that these drugs often have profound effects that can affect both short-term and long-term responses to exercise.
Many of the side effects of cardiovascular drugs also can have an effect on physical therapy. Medications that cause peripheral vasodilation often can produce hypotension, dizziness, and syncope, especially if these medications are combined with physical therapy inter- ventions that also produce extensive peripheral vasodi- lation. For example, systemic heat (large whirlpool, Hubbard tank, therapeutic pool) or aerobic exercise can produce vasodilation that exaggerates the effect of the vasodilating drugs, thus producing a profound decrease in vascular resistance and blood pressure. Procedures that increase systemic vasodilation should be used very cautiously in patients who are taking any antihyperten- sive medication or any other medication that produces systemic vasodilation.
Clinicians should recognize that they can play a critical role in implementing various nonpharmacologic inter- ventions that act synergistically with pharmacotherapy to provide optimal management of cardiovascular dis- ease.17g,1x0 Exercise, proper diet, weight loss, and other lifestyle modifications are essential in decreasing the risk of almost all types of cardiovascular d i s e a ~ e . l ~ l - ~ ~ These nonpharmacologic interventions also can decrease the need for specific medications, thus decreasing the risk of drug-related side effects.'" Physical therapists can imple- ment exercise programs as well as educate patients for the need to adjust their lifestyle to obtain the best results and possibly even decrease the need for long-term administration of cardiovascular medications.
Summary Cardiovascular drugs continue to be a mainstay in the treatment of cardiovascular disease. There is no question that these drugs are critical in improving cardiac func- tion and decreasing the effects of conditions such as hypertension, CHF, and myocardial ischemia/infarc- tion. Increased emphasis, however, has been placed on determining the most effective use of traditional medi- cations in these cardiovascular problems. In many cases, standard drug therapy has been challenged somewhat by newer drugs or new uses of existing medications that seem to provide better outcomes in terms of disease progression and survival.
Physical therapists should be aware that many patients will be taking cardiovascular medications and that these drugs can have a favorable impact on the patients' ability to participate in virtually all aspects of the rehabilitation program. Likewise, these drugs have side effects that may
492 . Ciccone Physical Therapy . Volume 76 . Number 5 . May 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

adversely affect a patient's response to specific physical therapy interventions. Finally, therapists should be aware that the use of cardiovascular drugs is constantly being reexamined to assess optimal drug use and effectiveness. Strategies for preventing and treating cardiovascular disease will undoubtedly continue to be an area of interest and research for some time.
References 1 Benditt EP, Schwartz SM. Blood vessels. In: Rubin E, Farber JL, eds. I'utholop~. 2nd ed. Philadelphia, Pa: JB Lippincott Co; 1994:454-501.
2 Friedrnan GD, Selby ,JV, Quesenberry CP, et al. Precursors of essen- tial hypertension: body weight, alcohol and salt use, and parental history of hypertension. Prm hled. 1988;17:387-402.
3 Buhler FR. Cardiovascular remodeling and its correction: toward a comprehensive strategy. Am J Med. 1993;94(suppl 4A) : 1 S-3s.
4 Dzau VJ, Gibbons GH. Vascular remodeling: mechanisms and impli- cations.,] Corcliot~asc Phannacol. 1993;21 (suppl 1):Sl-S5.
5 Struyker-Iioudier HA, van Bortel LM, De Mey JG. Remodeling of the vascular tree in hypertension: drug effects. Trends Phannacol Sci. 1990; 1 I :240-245.
6 Schachter M. Drug-induced modification of vascular structure: effects of antihypertensive drugs. Am Head J. 1991;122:316-323.
7 Morris Al3, Connell JM. Insulin resistance and essential hyperten- sion: mechanisms and clinical implications. Am J Med Sn. 1994; 307(suppl 11 ):S47-S52.
8 Reaven GM. Treatment of hypertension: focus on prevention of coronary heart disease. J Clin Endooinol Metab. 1993;76:537-540.
9 Sowers JK. Is hypertension an insulin-resistant state? Metabolic rhanges asltociated with hypertension and antihypertensive therapy. Am Fletrrl J. 199 I; l?2:932-935.
10 Wridmann P, d r Courten M, Ferrari P. Bohlen L. Serum lipopro- tcins tlurirl:q treatmrnt with antihypel-tensive drugs. J Cnrdiovasc Phnr- mnml. 1993;22(suppl 6):S98-S10.5.
11 Wchrr MA. The evolutiol~ of antihypertensive therapy: current throretical conditions and individualized treatment options. Am J M t d . 1992;9:l(suppl 2A): 1 6 3 s .
12 Pwsa P. Insulin resistance and hypertension. Cli7i Exp Hypmms. 3993;15:1047-3059.
13 Fchrr MD, L,ant AF. Management choices fol- hypertension with coexistent hyprrcholesterolaemia. J Royal Soc Med. 1991;84:?0.34205.
14 M'rber MA. Hypertension as a risk factor syndrome: therapeutic implications. Am J iWd. 1993;94(wlppl 4A):24631S.
15 F~rrherg CD. Berglund G, Manolio TA, Psaty BM. Overtreatment and under~reatrnent of hypertension. J h / a n Mrd. 1994;?35:387-397.
16 Scu~npe KO. Antihypertensive therapy: new strategies beyond blood prrssurr control. J (.'izrdiovasc. Phnnnacol. 1992;?O(suppl 6):Sl-S4.
17 Frl.lario CM. The renin-angiotensin system: importance in physiol- o p and pathology. J (,'c~rdiovasc Phanncol. 1990;15(suppl 3):Sl-S5.
18 Unger TU, (;ohlke P. Tissue renin-angiotensin systems in the heart and vasculature: possible involvement in the cardiovascular actions of converting enzyme inhibitors. Am J Cardiol. 1990;65:3-10.
19 Schelling P, Fischer H, Ganten D. Angiotensin and cell growth: a link to cartliovascular hypel-trophy? J Hypertens. 1991;9:3-15.
20 Unger T, Gohlke P. Converting enzyme inhibitors in cardiovascular therapy: current status and future potential. Cardiovn\c RPs. 1994;?8: 146-158.
21 Gohlke P, Lamberty V, Kuwer 1, et al. Vascular remodeling in systemic hypertension. Am J Cardiol. 1993;71:?E-7E.
22 Levy B1, Michel JB, Salzmann JL, et al. Long-term effects of angiotensinconverting enzyme inhibition on the arterial wall of adult spontaneously hypertensive rats. A m J Cardiol. 1993;71:8E-16E.
23 Abboud FM. The sympathetic nervous system in hypertension: state-of-the-art review. Hypertension. 1982;4(suppl ?):208-225.
24 Julius S. Autonomic nervous system dysl-egulation in human hyper- tension. Am J Cardiol. 1991;67:3B-7B.
25 Scriabine A. Beta-adrenoceptor blocking drugs in hypertension. Annu Rev Phannacol Toxicol. 1979;19:269-284.
26 DeBono G, Kaye CM, Roland E, Summers AJH. Acebutolol: 10 years of experience. Am HeadJ 1985;109:1211-1224.
27 Turner P. Which ancillary properties of beta-adrenoceptor blocking drugs influence their therapeutic or adverse effects: a review.,] Royal Sor hied. 1991;84:672-674.
28 Frohlich ED. Vasodilating beta-blockers: systemic and regional hemodynamic effects. Am Heatt J. 1991;1?1: 1012-101 7.
29 Prichard BNC. Beta-blocking agents with vasodilating action. J Cardiovasc Phanacol. 1992;19(suppl 1 ) 51-S4.
30 Swislocki ALM, Hoffman BB, Reaven GM. Insulin resistance, glu- cose intolerance, and hyperinsulinemia in patients with hypertension. Am J Hypotens. 1989;2:419-423.
31 Carruthers SG. The place of alpha blockers in the antihypertensive arniamentarium. J Clin Phanacol. 1993;33:260-263.
32 Horky K. Alpha(1)-blockade in the management of hypertension. J Clin Phnnnacol. 1993;33:874-878.
33 Symposium (various authors). Management of coronary heart dis- ease risk factors in hypertensive patients: clinical experience with doxazosin. Am HeadJ 1991;121:245-406.
34 Tavlor SH. New developments in the role of alpha-1 adrenergic receptors in cardiovascular disease. Am Head J. 1990;l 19:655-662.
35 Frishman WH, Landau A, (:I-etkovic A. Combination drug therapy with calcium-channel blockers in the treatment of systrn~ic hyperten- sion. J Clin Phannaml. 1993;33:75?-755.
36 Klaus D. The role of calcium antagonists in the treatment o f hypertension. J (;ardiovasc Phnnacol. 1992;?0(suppl 6 ) :S5-S14.
37 Symposium (various authors). Expanding the role of calcium antagonists in hypertension. J Cnrdiovasc Phnnnc~col. 1991 ; l7 (suppl 4) 51-S99.
38 Agabiti-Rosei E, Muiesan ML, Rizzoni D, et al. Regression of cardio- vascular structural changes after long-term antihypertensive treatmrnt with the calcium antagonist nitrendipine. J Cnrdiovasc Plznrrnacol. 1991;18(suppl 5):S5-S9.
39 Symposium (various authors). Calcium, calcium antagonism, and structural changes in hypertension. J Cr~rdlountc Phanacol. 1992; 19(suppl 2):Sl-S62.
40 Pauletto P, Sartore S, Giuriato L, et al. Calcium antagonists and vascular smooth muscle cells in atherogenesis. J Cnrdiovasc Phannrol. 1992;19(suppl ?):S8-S16.
41 Robertson RM, Robertson D. Drugs used for the treatment of myocardial ischemia. In: Hardman JG. Limbird LE, eds. 7'ht Phano- cological Basis of Therapeutics. 9th ed. New York, NY McGraw-Hill Book Co: 1996:759-779.
Physical Therapy. Volume 76 . Number 5 . May 1996 Ciccone . 493
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022
42 Furberg CD, Psaty BM, Meyer JV. Nifedipine: dose-related increase 65 Kulick DL, Rahirntoola SH. Current role of digitalis therapy in in mortality in patients with coronary heart disease. Cinul(~lion. 1995; patients with congestive heart failure. J.4MA. 1991;265:2995-2997. 92:1326-1331.
43 Psaty BM, Heckbert SR, Koepsell TD, et al. The risk of myocardial infarction associated with antihypertensive drug therapies. JAhf.4. 1995;274:620-625,
44 Kokko JP. Site and mechanism of action of diuretics. Am, / Ale(/. 1984;77(suppl 4A):ll-17.
45 Ogilvie RI, Burgess ED, ( : ~ l s s o ~ ~ JR, et al. Report of the Canadian- Hypertension-Society Consensus Conference: Pharmacologic treat- ment of essential hypertension. Can hfed Assoc J. 1993;149:575-584.
46 Mende CW. Current issues in diuretic therapy. lfosp Pracl. 1990; 25 (suppl 1) : 15-2 1.
47 Sonnenblick M, Friedlander Y, Rosin AJ. Diuretic-induced hypona- trernia: review and analysis of 129 reported patients. C i ~ c ~ l . 19'33; 3 03: 60 1 - 606.
48 Freis ED. The cardiovascular risks of thiazide diuretics. Clin l ' h n ~ macol ?'hrr. 1986;39:239-244.
66 Yt~sef S, Garg R, Held P, Gorlin R. Nerd for a large randomized trial to evaluate the effects of digitalis on morbidity and mortalih in congestive heart failure. A m J Cardiol. 1992;69:64G70G.
67 Noble D. Mechanism of action of therapeutic levels of cardiac glycosides. C(~rdio71nsc Rcs. 1980; 14:49.5-514.
68 Siegl PIG. Overview of cardiac inotropic mechanisms. J (:flrd2071nc P\~armacol. 1 YXfi;X(suppl 9):Sl-S10.
69 Ferguson DW. Digitalis and neurohormonal abnormalities in heart fail~rre and implications fbr therapy. Ain J Crrrtliol. 1992;69:24G33G.
70 Gheorghiade M. Zarowitr BJ. Review of rar~domized trials of digoxin therapy in patients with chronic heart failure. A m J C(rrdio1. 1992;69: 4 8 G 63G.
71 Kelly RA, Smith TW. Recognition and managenlent of digitalis toxiciv. .4n1,/ Cardiol. 1992;69:108G-1 IYG.
72 Swan HJC. Can heart failure be prevented, delayed, or reversed? Am Hrartl. 1990;120: 1540-1546.
49 (;ifford RW. The role of diuretics in the treatment of hypertension. 73 Leier CV. Current status of non-digitalis positive inotropic drugs.
Am J k l ~ ~ i . 1984;77(suppl 4A):102-106. Am / Cardiol. 1992;69: 120G12XG.
50 Bennett WM, McDonald WJ, Kuehnel E, e t al. Do tli~lretics have antihypertensive properties independent of natriuresis? Clin Phamn~urol 7'ht-r. 1937;22:499-504.
51 Ames RI'. The effects of antihypertensive drugs on serun~ lipids and lipoproteins, I: diuretics. Diugr. 1986;32:260-278.
52 Woskins B,Jackson CM. The mechanism of chlorothiazide-induced carbohydrate intolerance. J l'i~annaml Exp Thm. 3978;206:423-430.
53 Wilson MD. Weart CW. Hypertension: Are beta-blockers and diuret- ics appropriate first-line therapies? Ann Phannaco!hrr. 1994;28:617-6 25.
54 Hansson I.. Treatment of hypertension in the elderly. J C(rrdio71asc Pl~nnnncol. 1994;23(suppl 5):S59 -Sf?].
74 Anderson JL. IIemodynamic and clinical benefits with ir~traveno~ls milrinone in severe congestive heart faill~re: results of a multicenter st~tdy in the United States. A m Hm?l,/. 1991;121:1!)56-1964.
75 Fisher Th. Erhel R, Tresse N. Current status of phosphodiesterasr inhibitors in [he treatment of congestive heart failure. I)nrg. 1992;44: 928-945.
76 Honerjagel. P. Pharmacology of bipyridine phosphodiesterase I11 inhibitors. Am Hear! J 19'31;121:1939-1944.
77 Krlly RA, Smith TW. Pharn~acological treatment of heart failure. In: Hardman JG, Li~nhird LE, eds. ?'he Pha~mucolopcal Basis of7Rerapmtics. 9th ed. New York, NY McGraw-Hill Book Co; 1996:809-838.
55 Dahlof B, Hansson L, Lindholm LH, et al. Swedish trial in old 78 McGhie AI, Golstein RA. Pathogenesis and management of acute patients with hypertension (STOP-hypertension) analyses performed heart fail~rre and cardiogenic shock: roIe of inotropic therapy. Chert. LIP to 1992. Clin EX!] HypPl;'m~. 1993;15:925-939. 1992; 102(s1lppl 2) :626.%632S.
56 McVeigh GE, FlackJ, Grimm R. Goals of antihypertensive therapy. 79 Deighton NM, Motomura S. Bals S, et al. Characterization of the Drugs. 191)5;49:161-175. beta-adrenoceptor subtype(s) mediating the positive inotropic effect4
of epinine, dopamine, dohutamine, denopamine, and xamoterol in 57 Moan A, 0 s 1, Hjermann 1, Fjeldsen SE. Hypertension therapy and
isolated human right atrium. J Phn~macol h'xp 7'hrr: 1!)92;262:532-538. risk of coronary heart disease: How do antihypertensives affect meta- bolic tictors? (:ardioloL~. l995;86:89-93. 80 Rich hlW, Woods MiL. Davila-Roman VG, et al. A randomized
con1p;rrison of intravenous arnrinone versus dohutamine in older 58 Manolio TA, CutlerJA, Furberg CD, e t al. Trends in pharrnacologic
patients with decompensated congestive heart failure. J A m (:m:a!r Sot.. management of hypertension in the United States. Arch Inlrrr~ Mrtl.
1995;43:271-274. 199.5;155:829-837.
81 Tisdale JE, Pate1 R, Webb CR, et al. Electrophysiologic and prcr 59 Weidmann P. Differential effects of antihypertensive drugs on
arrhythmic effects of intravenous inotropic agents. Prog Cartliovm.sc L)i.c. hypertension: associated risk factors. Cardiology. 1994;85(suppl 1):78-
1995;38: 167-180. 83.
60 Jennings KB, Steenbergen <:, Hackel DB. The heart. In: Ruben E, Farber JI., eds. P(l/holo,q. 2nd ed. Philadelphia, Pa: JB Lippincott Co; 199452 1-532.
61 Symposium (various authors). Heart failure: adaptive and maladap- tivtr processes. Circulalion. 1993;87 ( s ~ ~ p p l 7) :1-12 1.
62 Ferguson DW. Sympathetic mechanisms in heart failure: pathophys- iological and pharmarological implications. (~irculalion. 1993;87(suppl 7):68-75.
63 Ventura HO. Murgo JP, Srnart FW, et al. Current i ss~~es in advanced heart failure. Mpd Clin. 1992;76: 1057-1082.
82 Scrima DA. Managing dobutamine infilsions. Mr(l.surg Ni~,rs. 1993;2: 459-465.
83 Kdtaoka T. Keteyian SJ, hlarks CRC, et al. Exercise training in a patient with congestive heart failr~re on continuous dohutamine. hfed Sri S/>ort.s ~,'XPIC. 1994:26:678- 68 I.
84 Sherman A. Critical care management of the heart failure patient in the home. Cril Carp Nurs Q. 1995;18:77-87.
85 Erlemeier HH, Kupper W, Bleifeld W. Intermittant infusion of dohutamine in the therapy of severe congestive heart failure: long- term effects and lack of tolerance. (;<~rdiot~a.tc ,!hugs Thn: 1992;6:391- 398.
64 Hohhs RE, Crerska B. Congestive heart failure: current and future btrategies to decrease mortality. Postgrad Mpd. 1994;1)6:167-172.
4 9 4 . Ciccone Physical Therapy . Volume 76 . Number 5 . May 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

86 Om A, Hess ML. Inotropic therapy of the failing nlyocardiun~. Clin (:(~rr/iol. 1993;16:5-14.
87 Pickwor~h KK. Long-term dobutamine therapy for refractory con- gestive heart failure. Clin Phorm. 1992;11:618-624.
88 Bristow MR. Pathophysiologic and pharmacologic rationales for clinical management of chronic heart hilure with beta-blocking agents. Am J C ~ d i o l . 1993;7 1: 12C-22<1.
89 Dought). RN, Machlahon S, Sharpe N. Beta-blockers in heart hilure: promising or proved? J A m Coil (;arr/iol. 1994:23:834-821.
90 Eichhorn El. The paradox of beta-adrenergic blockade f i r the management of congestive hedrt failure. Am J M P ~ . 1992;'32:5'17-5.18.
91 Taylor SH. Dillretics in cardiovascular therapy: perusing the past, ~ -
practicing in the present, preparing for the future. % Kordiol. 1985; 74(suppl 2) 2-12,
92 J o h n s t o ~ ~ C1, Fabris B, Yoshida K. The cardiac renin-angiotensin system In heart hilure. Am Htnri J. 1993;126:756-760.
93 Giles T. Enalapril in the treatment of congestive heart failure. (d'i~r~lr~ivosr I'hormncol. 1990; 15(suppl S):S6-SlO.
94 Kibner HS, Sagar KB, Glasser SP, et al. Long-terrr~ therapy with benalepril in patients with congestive heart failure: effects on clinical s t a t ~ ~ s and exercise tolerance. J Clin Phormorol. l9!~0:30:1 106-1 11 1.
95 Garg R. Yusef S. Ovelview of randomized trials of angiotensin- converting enzyme inhibitors on mortality and morbidity in patients with heart failure: collaborative group on ACE inhibitor trials. JAMA. 1995;273: 1450-1156.
96 Cohn JN , ,]ohnson G, Ziesche S, et al. A comparison of enalapril with hydralazine-isosorl,ide dinitrate in the treatment of chronic congestive heart failure. N I : 'n~ l ] Med. 199 1 ;525:303-3 10.
97 Tisdale,]E, Gheorghiade M. Acute hemodynamic effects of digoxin alone or in combination with other vasoactive agens in patients with congestive heart failure. Arn,/ Cnrdiol. 1992;69:34G-47G.
98,lennisor~ SH, Miller LW. What to try while congestive heart hilure patients are still ambulatory. Po.~tg.md Med. 1993;94:66-78.
99 Kamahi TM, Lee FA. Medical therapy and prognosis in chronic heart failnre: lessons from clinical trials. Cnrdiol (,'/in. 1995;13:5-26.
100 SOLVE1 Investigators. Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricl~lar ejection fractions. N Engl.1 Mtd. 1992:327:685-691.
101 SOLVD Investigators. Effect of en;ilapril on sulvival in patients with reduced left ventrictllar ejection fractions and congestive heart failure. N I..:11gl J M P ~ . 1991;325:293-302.
102 Swt-dberg K. Reduction in mortality by pharmacological therapy in congestive heart failnre. Czrculniion. 1993;87: 126-1 29,
103 Eriksson H. Heart failure: a growing public concel-n. JInicrn M P ~ . 1'395:237: 13-141.
104 Clark L.T. Atherogenesis and thrombosis: mechanisms, pathogen- esis, and therapeutic implications. Am H ~ o r i J. 1992;12:3:3 106-1 109.
105 Chhn IN. Phar~nacologic mechanisn~s of nitrates in myocardial ischemia. Am J (:nrdiol. 1992:70:38G42G.
106 Fung HL. Clinical ph;~r~nacology of the organic nitrates. Am J (:urdiol. 1993;72:9(:-1.5(;.
107 ParkerJO. Nitrates and angina pectoris. Am J (:rlrd~ol. 1993;72:3<:- 8C.
108 Henet LZ, Kroetz DL, Sheiner LB. Pharmacokinetics: t l ~ e dynamics of drug absorption, distribution, and elimination. In: Hardman JC;, Lirnbird LE:, eds. Tht Ph(~rmnrological Basis of l l~~r (~~)cu i i r : s . 9th ed. New York. NY hlcGraw-Hill Book (10; 1996:S-27.
109 ACIP Investigators. Asymptomatic cardiac ischen~ia pilot study (ACIP). Am J (;aldiol. 1992;70:744-747.
110 Cohn PF. Silent myocardial ischemia: classification, prevalence. and prognosis. Am J Mtd. 1985;79 (suppl 3A) 2-6.
111 Pepine C]. Clinical aspects of silent myocardial ischerr~ia in patients with angina and other forms of coronary heart disease. A m , / h f ~ d . 1986;80(suppl 4C):25-34.
112 Paciaroni E, Luca C. Discontinuous transdermal nitroglycerin a treatment for stable angina in thr elderly: a double-blind rnulticentre study. Eur Htari,]. 1991;12:1076-1080.
113 Scheidt S. Angina: evolution of the role of nitrates. Am I f t n ~ i J. l990;120(suppl) :757-761.
114Ant1nan E, Muller J , Goldberg S, et al. Nifedipine therapy for coronaly-artery spasm: experience in 127 patients. N Engl J Med. 1980;302: 1269-1273.
115 Mehta JL. En~erging options in the management of ~nyocardial ischemia. A m J (;r~rdrol. 1994;73: 18A-27A.
116 Hansson 1.. Calcium antagonists: an overview. Am H(,rrr% J. 1991; 122:308-31 1.
117 dehluinck ED, Lie KI. Safety and efficacy of beta-l,lockers in the treatment of stable angina pectoris. J Cor(li~iou(~.\r. 1'lirrlrnrrc.ol. 1990: 16(suppl 5):S123-S128.
118 Scheidt S. Beta blockade for angina and arrhythmias: an c~velview. Drugs. 1983;25(suppl 2): 153-1 59.
119 Cruickshank JM. Beta-blockers: primary and seconda~y preven- tion. J Cnrdiour~.sr P l~orm~~ro l . I992;20(suppl 1 1):S55-S65.
120 Hansson L. Review of state-of-the-art beta-blockcr therapy. Am , ] OY(lrdiol. 199 1 ;67:43%46B.
121 Levy S. Secondary prevention after myocardial infarction: in Savor of beta-blockers. ,/ C(irdiovncr Pharmncol. 1990;16(suppl 6):S50-S54.
122Viskin S, Kitzis I, Lev E, et al. Treatment with beta-adrenergic blocking agents after myocardial infarction: from randomi~ed trials to clinical practice. J A m (;ull (;(lrdiol. 1995;25:1327-1332.
123 (;ollen D, Stump DC:, Gold HK. Thrombolytic therapy. Annzc KPII hfcd. 1988;39:405-423.
124 Becker RC, Harrington R. Recombinant tissue-type plasminogen activator: current concepts and guidelines fi,r clinical use in acute myocardial infarction. Am Htari J. 199 1 ;12 1:627-640.
125 Bell WR. Thrombolytic therapy: agents, indications, and labora- tory monitoring. MI^ (:/in. 1994;78:745-764.
126 GUSTO Angiographic Investigators. The effects of tissue plasmin- ogen activator, streptokinase, or both, on coronary-artery patency. ventricular fi~nction, and sulvival after acnte n~yocardial inhrction. N i:?lgI J h,ftd. l9Y3;329:1615-1622.
127 Anderson JL. Marshall HW, Bray BE, et al. A randorni~ed trial of intracoronary streptokinase in the treatment of acute ~nyocardial infarction. N fig1 J M P ~ . 1983;308: 131 2-1318.
128 Schreiber T. Review of clinical studies of thronlbolytic agents in acute myocardial infarction. A m J Med. 1987;83(suppl 2A):20-25.
129 Bett N, Aroney G, Thompson P. Delays preceding adn~ission to hospital and treatment with thrombolytic agents of patients with possible heart attack. Azcsl N%,/ Mtd. 1993;23:312-313.
130 C:ollen D, Lijnen HR. On the t u t ~ ~ r e of thrombolytic therapy for acute myocardial infarction. AIII , / (;(~rdiol. 1993;72:46(;-50G.
131 1)oorcy AJ, Michelson EL, Topol El. Thrombolytic therapy of acute myocardial infarction: keeping the unfulfilled pron~ises. JAMA. 1992; 268:3108-3114.
Physical Therapy . Volume 7 6 . Number 5 . May 1996 Ciccone . 495
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022

132 Habib GB. Current status of thrombolysis in acute myocardial 151 Meade TW, Miller GJ. Combined use of aspirin and warfarin in infarction, I: optimal selection and delivery of a thrombolytic drug, primary prevention of ischemic heart disease in men at high risk. Am (:hest. 1995; 107:225-232, J Cardiol. 1995;75:23B-26B.
133 TlMI S t ~ ~ d y Group. The thrombolysis in myocardial infarction 152 Patrono C. Drug therapy: aspirin a.r an antiplatelet drug. NEnglJ (TlMl) trial. N Engl J Mrd. 1985;312:932-936. Mrd. 1994;330:1287-1294.
134 White HD, Rivers JT, Maslowski AH, et al. Effect of intravenous 153 Hirsh J. Drug therapy: heparin. NEnglJMrd. l991;324:1565-1574. slrepiokinase as compared with that of tissue plasminogen activator on
154 Suttie JW. The biochemical basis ofwarfarin therapy. AdnLxp Mrd left ventricular function after first myocardial infarction. N Engl J Med.
Biol. 1987;24:3-16. 1989;320:817-821.
155 Schreiber TL, Miller DH, Silvasi D, et al. Superiority of warfarin 135 GISSl-2 Investigators. GlSSI-2: a factorial randomized trial of
over aspirin long-term after ihrombolytic therapy for acute myocardial alteplace versus streptokinase and heparin versus no heparin among
infarction. Am Hmrt J. 1990;119: 1238-1244. 12,490 patients with acute myocardial infarction. Lancrt. 1990;336:65- 71. 156 Smith P, Arnesen H, Holme 1. The effect of warfarin on mortality
and reinfarction after myocardial infarction. N Engl J Mrd. 1990;323: 136 lSlS-3 Investigators. 1SlS-3: a randomized coniparison of streptoki-
147-152. nase vs tissue plasminogen activator vs anistreplase and of aspirin plus heparin vs aspirin alone among 41,299 cases of suspected myocardial 157 Launhjerg J, Egeblad H, Heaf~j , et al. Bleeding complications to infarction. Lancrt. 19Y'L;339:753-770. oral anticoagulant therapy: multivariate analysis of 1,010 treatment
years in 551 outpatients. J I n t m Mrd. 1991;229:351-3.55. 137 Maggioni AP, Franzosi MG, Santoro E, et al. The risk of stroke in patients with acute myocardial infarction after thrombolytic and anti- 158 Howes LG, Simons LA. Efficacy of drug interventions for lipids in thrombotic treatment. N Eng1.J Mrd. 1992;327:1-6. the prevention of coronary artery disease. Aust NZJMed. 1994;24:107-
112. 138 O'Connor CM, Califf RM, Massey EW, et al. Stroke and acute myocardial infarction in the thrombolytic era: clinical correlates and 159 Grundy SM. Atherogenic dyslipidemia: lipoprotein abnormalities long-term prognosis. J A m Coll Cardiol. 1990;16:533-540. and implications for therapy. Am J Cardiol. 1995;75:45B-52B.
139 Handlin LR, Vacek JL. Thrombolytic therapy for acute myocardial 160 Spinler SA, Cziraky MJ. Lipoprotein(A): physiologic function, infarction: Are inclusion criteria too stringent? Postgrad Med. 1994;95: association with atherosclerosis, and effects of lipid-lowering drug 77-82. therapy. Ann Pharmacother. 1994;28:343-351.
140 Mueller HS, <:ohen LS, Braunwald E, et al. Predictors of early 161 Vega GL, Grundy SM. Primary hypertriglyceridemia with border- morbidity and mortality after thrombolytic therapy of acute myocardial line high cholesterol and elevated apolipoprotein B concenuations: infarction: analysis of patient subgroups in the Thrombolysis in Mytr comparison of grn~fihrozil versus lovastatin therapy. ,JAMA. 1990;264: cardial Infarction (TIMI) trial, phase 11. Ci~culation. 1992;85: 1254- 2759 -2763. 1264.
141 Kutherford ,ID, Braunwald E. Thrornholytic therapy for acute myocardial infarction. C a t . 10'3O;I~7(suppl 4) :136Sl45S.
142 Hahib GB. Current status of ilironibolysis in acute myocardial infarction, part 111: optimization 01 adjunctive therapy after thrornhtr lytic thel-apy. ( :I&~A/ . 1995; 107:809 -8 1 (i.
143 1,eFeuvre C, Yusuf S, Flather M, Farkouh M. Maximiring benefits of therapies in acute rnyocardial infarction. Am J Caldiol. 1993;72: 145cr3 55G.
144 Fendr-ick AM, Kidker PM, Bloom BS. Improved health benefits of inrrc.asc.d usr of thromholytic therapy. Arch Intern Mrrl. 1994;154: 1605-
162 Grundy SM. Cholesterol-lowering drugs as cardioprotective agents. A m J (;rl~diol. 1992;70:271-321.
163 Gotto AM. Dyslipidemia and athrrosclrrosis: a forecast of pharma- ce~~tical approaches. Czrculalion. 1993;87(suppl 4):.54-59.
164 Brown CX, Alhers Jj, Fisher LD, et al. Kegrrssion of coronary arteryclisease as a result of intensive lipid-lowering thcl-apy in mrn with high levels of apolipoprotein B. N Kngl J Mrd. 1990;323: 1289-1298.
165 Colditz (;A, Stampfer MJ. Cardiovascular effects ofmenopa~~se and estrogen replacernent: the epidemiological evidence. In: Schwart7. DP, ed. Honnonr Kpl,lncrmm/ Y'hm(~py. Baltimore, Md: Williams & Wilkins; 1992:lOY-137.
1609. 166 Gruchow HW, Anderson Aj, Barboriak J, Sobocinski KA. Post-
145 Antiplatrlet Trialists' Collaboration. Secondary prevention of vas- menopausal use of estrogen and occlusion of coronary arteries. Am cular disease by prolonged antiplatelet treatment. Mr Mrd J. 1988;296: HrarfJ. 1988;115:954-963. 320-33 1.
146 Goodnight SH, Coull BM, McAnulty Jl3, Taylor LM. Antiplatelet therapy: part 1. WrstJ bled. 1993; 158:385-392.
147 Steering Committee of the Physician's Health Research Group. Final report o n the aspirin component of the ongoing physicians' health scudy. N b,'ngI,JMrrl. 1989;321:129-13.5.
148 (>allus AS. Aspirin and other platelet-aggregation inhibiting drugs. MrdJAust . 1985;142:41-47.
149 de Bono D. Management of thrombosis in coronary heart disease. Bt. M d Bull. 1994;.50:904-910.
167 Manolio TA, Furberg CD, Shemanski L, et al. Associations of postmenopausal estrogen use with cardiovascular disease and its risk factors i n older women: the CHS Collaborative Research Group. Cirrulation. 1993;88:2 163-2171.
168 Coronary Drug Project Research Group. The coronary d n ~ g project: findings leading to discontinuation of the 2.5 mg/day estro- gen group. J A M . 1973;226:652-657.
169 Meade TW. Risks and mechanisms of cardiovascular events in users of oral contraceptives. Am J Ohstet f+nrrol. 1988;158:1646-1652.
170 Godsland IF, Wynn V, Crook D, Miller NE. Sex, plasma lipopro- - -
teins and atherosclerosis: prevailing assumptions and outstanding 150 Chesehro JH, Badimon L, Fuster V. New approaches to treatment
questions. Am Hmrt J. 1987;114:1467-1503. of myocardial infarction. A m J f;~t.dio/. 1990;65:12C-19C.
171 Coson SL. A decade of experience with transdermal estrogen replacement thcrapy: overview of key pharmacologic and clinical findings. Int,JFntility. 1993;38:79-9 1.
496 . Ciccone Physical Therapy . Volume 76 . Number 5 . M a y 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022
172 Mickley H, Junker A. Miller M. Elr'ect of thrombolytic therapy on postinfarction myocardial ischeniia. (;crrrliolqq. 1994;84:121-125.
173 GISSI Investigators. Effectiveness of intravenous thrombolytic trratment in acute myocardial infarction. L/lnrr/. 1986;l :997-402.
174 ISIS2 Investigators. Rando~nized trial of intravmous strrptoki- nase. oral aspirin, both, or neither among 17,187 cases o f suspected acute myocardial infarction. Lci~lrrl. l988;2:349-360.
175 Rutherford JD, Pfeffer MA, Moye LA, et al. EfTects of captopril on ischemic events after myocardial infarction: results of the Sumival and \'rntricular Enlargement (SALT) trial. I.'irr71/rr/inn . 1994;90:17.11-I 738.
176 Thr Acutr Infarction Ramipril Efticacy (.-\IRE) Study Investigators. Effect of lamipril 011 mortality and morbidity vf si~rvivors of acute myocardial infarction with clinical evidence of heart failure. Lnnrel. 1993::342:821-828.
177 Peel C, hlossherg M. Effects of cardio\,ascular medications on rxer-rise responsrs. Phv.7 Thn. 1995;7.5:387-396.
179 Iangford HG. Davis BR, Blaufox D, et al. Effect of drug and diet treatment of mild hypertension on diastolic blood pressure. Hypmtm- sinn. 1991;17:210-217.
180 Keaton JD, Grimm RH. Prineas RJ, et al. Treatment of mild hypertension study final results. J A M . 1993;270:71:3-724.
181 Cutler J . The effects of nonpharmacologic interventions on blood pressure of persons with high normal levels: results of the trials of hypertension prevention, phase I. JAhfA. 1992;267: I? 1.%1220.
182 Schotte DE, Stunkard AJ. The effects of weight reduction on blood pressure in 301 obese patients. Arrh Intern Med. 1990;150:1701-1704.
183 Symposium (various authors). New vlstas on nonpharmacologic approaches to hypertension. j Cardionarr Pharmarol. 1990;16(suppl 8):Sl-S83.
184 Kaplan NM. Use of nonilrug therapy in treating hypertension. Am jibfed. I984;77(suppl 4A):96-101.
178 Cahalin LP. (:ardiovascular medications. In: .\lalnne T, rcl. I ' / l~~irnl
o ~ r d Orrup~~t iar~ol 771rmpy: Dnrg Implirn/ionsfir If-nrlir~. Philadelphia. Pa: IB Lippincott (:o; 1989:58-tiX.
The 1 995 Directory of Certified linical Specialists
The American Physical Therapy I TOORDER: I Association is proud to offer a By Phone: 1800!999 APTA. w t 3395. between 830am and 5.30 pm. Eastern trme. I comprehensive directory of the I Monday through Fnday. Pea% have your MasteCard or USA ready For TDD access, dral I
1,351 individuals who have been t 703'683-6748 I
certified by The American Board of By Maii Return thrs order f o n w~th your payment (payable to APTA] to. Amencan Physrcal I Physical Therapy Specialties I Theravy ksoc~ation, 1 l I I N hrrfax St. Alexandria, VA 2231 4 ! 4 8 8 I
(ABpTS]. These individuals have I By Fax: 703fl0b3396.24 houn a day Please provide credit card and membership I I
been certified for their advanced I i"ormatrmand daflrne phone number. I I
clinical knowledge and skills in I By EMail: Send your crfdrt card and mernbershrp nforrnat~on -- wa Internet to. [email protected] - I cardiopulmonary, clinical electrophysiologic, geriatric, ( I Mmkdiuount pridNmmemk price T S U ~ L ~ M I
neurologic, orthopaedic, pediatric, and sports physical therapy. S201S28 I s u m r - l I I Md $4.00 (shippis & handlid --il I I
PTs, ~hysic~ans, and other health care prov~ders will find this d~rectory invaiu 1 Mania msi~enb add 4.5% sales tar
able fgr patient referrals and consultations Students and researchers will be I ,C7! L- -
armed with a priceless k t of name5 to consult h r research questions. And I Name -- Member # I I
everyone will find this an indispensable networking too/. I Address -_ I I
I City,State,Zlp - I I
This easy-to-use directory lists certified specialists by specialty area, I Dayt~me Telephme I ___ I I
0 Mastercard 0 VISA by alphabetic order, by state, and by area code. For each certified specialist, I n hecke enclosed pay able to^^^^ I I
I Cred~t 4rM - E\F you'll find information on facility address and phone number, I
&Mk"L< &H I .",.,'., ."C.A*
year 3f certification, and practice focus. A,.,7., An.. ; s , g n a l u r e _ I
I
p q j 1 -----------------------------------------A
Physical Therapy . Volume 76 . Number 5 . May 1996 Ciccone . 497
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/5/481/2633020 by guest on 29 January 2022