
PHARMACOLOGY KNOWLEDGE ACQUISITION - OhioLINK ...
151
Running head: PHARMACOLOGY KNOWLEDGE ACQUISITION i THE RELATIONSHIP OF SELECTED ACADEMIC, NONACADEMIC, AND CLINICAL VARIABLES AS FACTORS INFLUENCING PHARMACY KNOWLEDGE ACQUISITION IN ASSOCIATE DEGREE PRE-LICENSURE NURSING STUDENTS By DIANE M. STAUFFER Submitted in partial fulfillment of the requirements for the degree of Doctor of Nursing Practice Committee Chair: Marilyn Lotas, PhD, RN, FAAN Frances Payne Bolton School of Nursing CASE WESTERN RESERVE UNIVERSITY August 2016
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of PHARMACOLOGY KNOWLEDGE ACQUISITION - OhioLINK ...

Running head: PHARMACOLOGY KNOWLEDGE ACQUISITION i
THE RELATIONSHIP OF SELECTED ACADEMIC, NONACADEMIC,
AND CLINICAL VARIABLES AS FACTORS INFLUENCING
PHARMACY KNOWLEDGE ACQUISITION IN ASSOCIATE DEGREE
PRE-LICENSURE NURSING STUDENTS
By
DIANE M. STAUFFER
Submitted in partial fulfillment of the requirements for the degree of
Doctor of Nursing Practice
Committee Chair: Marilyn Lotas, PhD, RN, FAAN
Frances Payne Bolton School of Nursing
CASE WESTERN RESERVE UNIVERSITY
August 2016

ii
CASE WESTERN RESERVE UNIVERSITY
FRANCES PAYNE BOLTON SCHOOL OF NURSING
We hereby approve the scholarly written project of
Diane M. Stauffer
Committee Chair
Marilyn Lotas, PhD, RN, FAAN
Committee Member
Deborah Lindell, DNP, RN, CNE, ANEF
Committee Member
Joni Goldwasser, DNP, APRN, FNP-BC
Date of Defense
June 10, 2016
We also certify that written approval has been obtained for any proprietary material
contained therein.

iii
Abstract
Effective medication management is critical to safe practice. The Institute of
Medicine reports that medication errors are common and adversely affect patient
outcomes. In order for nurses to effectively manage medications and ensure safe
patient care, a comprehensive knowledge of pharmacology is required. However,
studies suggest nurses are inadequately prepared and do not have sufficient
knowledge. The lack of pharmacology knowledge is attributed to a variety of factors
that impact nursing education including the lack of biological sciences, ineffective
teaching, superficial learning strategies, inadequate time devoted to pharmacology,
and barriers or lack of opportunities for clinical application. Identifying factors that
contribute to academic success or failure enables educators to pinpoint high-risk
students early, provide counseling and academic support, and optimize student
performance. This study used a descriptive correlational design to examine academic,
non-academic, and clinical variables for pre-licensure nursing students in an
Associate’s degree program. The purpose of the study was to determine the
correlation between selected variables and pharmacology knowledge acquisition as
demonstrated by scores on a standardized pharmacology assessment. A second
purpose of the study was to determine any correlation between student perceptions of
clinical experience opportunities for medication management and performance on the
pharmacology assessment. Seven variables were analyzed for the nature and strength
of relationships including nursing grade point average (GPA), science GPA, previous
college credit or degree, previous health care experience in direct patient care,
working hours per week, family responsibilities, and clinical experience opportunities
for medication administration and decision-making. The study found a significant
correlation between nursing grade point average (GPA) and pharmacology test
scores, and science GPA and pharmacology test scores. These findings are consistent
with the literature that demonstrates science GPA as a predictor for academic success
in nursing, and nursing GPA as a predictor for standardized testing and NCLEX-RN
success. No other variables were found to be significant in the correlational analysis.
Further study is recommended to examine the selected variables in a larger more
heterogeneous population, and to analyze pharmacology knowledge acquisition
among programs with varying clinical experience opportunities for medication
management.

iv
Copyright© 2016 by Diane M. Stauffer, MSN, RN, CNE
v
Dedication
This scholarly project is dedicated to all students of the Good Samaritan College of
Nursing and Health Science in honor of their commitment to nursing education, and
to the class of May 2016 for their support of nursing research through participation in
this study. Throughout my career as a nurse educator, I have been overwhelmed by
the adversity students overcome to be successful in the nursing program, yet I
continue to witness a genuine compassion, caring, and advocacy for all patients. To
all nurses and nursing students, thank you for your amazing work, and for all of your
efforts to ensure safe and quality patient care in a very challenging health care
environment.
vi
Acknowledgements
I would like to acknowledge the contributions and support of the following
individuals in the completion of this research project and toward achievement of
my goal to obtain a doctoral degree in nursing practice.
Thank you to Dr. Marilyn Lotas, the chairperson of my committee for her
guidance through the research process. Her direction enabled me to focus on the
essential elements of the study, and to improve my scientific writing with clear
and concise communication. Thank you to committee members, Dr. Lindell and
Dr. Goldwasser for their time and valuable feedback for the study proposal
through the final defense. Thank you to Dr. Goldwasser for her friendship,
empathy and reassurance that I would survive this journey.
Thank you to Dr. Joy Dienger, Nurse Researcher at TriHealth, Inc. for her
guidance in developing the clinical experience survey questionnaire, and for her
invaluable assistance in obtaining IRB approval and navigating the complex
Institutional Review Board process.
Thank you to Dr. Gregory Graham and Dr. Mary Ann Heverly for their statistical
expertise and assistance in determining and conducting the statistical analyses for
the study. Dr. Heverly was especially instrumental in helping me to conduct the
analysis and interpret the results of the study.
Thank you to the Good Samaritan College of Nursing and Health Science faculty
and administration. The encouragement, accommodation, and support of
administrators and colleagues have been unwavering throughout my doctoral
education. A special thank you is extended to Dr. Teresa Getha-Eby for her
guidance and meticulous work in editing this final scholarly project.
Thank you to my sister, Debbie Young and dear friend, Randi Carnahan. Their
love and support is unconditional and means the world to me. Thank you both for
always offering a listening ear and shoulder to lean on. To my sister, I would not
have been able to devote the time necessary to complete this educational endeavor
had it not been for you.
vii
Table of Contents
Title Page i
Committee Approval Page ii
Abstract iii
Copyright Page iv
Dedication v
Acknowledgements vi
Table of Contents vii
List of Figures xi
List of Tables xii
Chapter 1: Introduction 1
Introduction/Background 1
Problem 2
Purpose 3
Significance of the Problem 4
Significance to Nursing 5
Theoretical Framework 7
Research Questions 13
Conceptual Definitions 14
Summary 15
viii
Chapter 2: Review of the Literature 17
Pharmacology Knowledge Level for Nurses, New Graduate
Nurses, and Nursing Students
18
Inadequate Pharmacology Knowledge as a Factor for
Medication Errors
28
Factors Influencing Pharmacology Knowledge
34
Strategies to Enhance Pharmacology Knowledge 45
Gaps in the Literature
50
Chapter 3: Methodology 52
Design 52
Setting 52
Study Population 53
Recruitment 55
Inclusion and Exclusion Criteria 57
Sample Size Determination 57
Measurements 59
ATI RN Pharmacology Assessment 59
Clinical Experience Survey Questionnaire 65
Demographic Information Form 66
Data Collection Procedure 67
Data Management 69
Statistical Analysis 70
Protection of Human Subjects 75
ix
Chapter 4: Data Analysis 79
Sample Demographics 79
Analyses of Research Questions 81
Research Question 1 81
Research Question 2 83
Research Question 3 89
Summary 95
Chapter 5: Discussion 97
Discussion 97
Level of Performance on ATI Pharmacology Assessment 98
Relationship between Selected Variables and ATI Performance 100
Relationship between Clinical Experiences and ATI Performance 104
Utility of the Theoretical Framework 107
Limitations 108
Implications for Nursing and Nursing Education 110
Future Research 112
Conclusion 114
References 117
Appendices
Appendix A - Script for Introduction and Description of Study 130
Appendix B – Notice of Study 131

x
Appendix C - Original Survey Questionnaire and Summary of Reviewer
Feedback
132
Appendix D - Final Revised Clinical Survey Questionnaire 136
Appendix E - Demographic Information Form 138
xi
List of Figures
Figure 1 – Differences between Pedagogy and Andragogy 8
Figure 2 - Scatter Plots for Continuous Variables 82
Figure 3 - Histogram of ATI Pharmacology Assessment Scores 83
Figure 4 - Histograms of Clinical Experience Survey Average Scores 91
xii
List of Tables
Table 1 - Perceived Factors Influencing Pharmacology Knowledge
Acquisition
36
Table 2 - Categories and Competency Areas that Establish Medication
Competence
47
Table 3 – Associate Degree Nursing Program Curriculum 55
Table 4 - ATI RN 2013 Proctored Pharmacology Assessment
Concepts and Content Areas
60
Table 5 - ATI RN 2013 Pharmacology Assessment Cut Scores
and Proficiency Level Definitions
63
Table 6 - RN CMS 2013 Test Statistics for the Pharmacology
Assessment
65
Table 7 - Study Participants’ Age, Gender, Ethnicity 80
Table 8 - Descriptive Statistics for ATI Pharmacology Assessment
Scores
84
Table 9 - Descriptive Statistics for Academic Variables 86
Table 10 - Descriptive Statistics for Non-Academic Variables 88
Table 11 - Correlations for Selected Variables and ATI Pharmacology
Assessment Score
89
Table 12 - Descriptive Statistics for Clinical Experience Survey 92
Table 13 - Frequency Distribution for Clinical Experience Survey
Responses
93
Table 14 - Correlational Statistics for Clinical Survey Questionnaire 94
PHARMACOLOGY KNOWLEDGE ACQUISITION 1
Chapter 1: Introduction
Nurses have key responsibilities in the management of medication therapy,
and fulfill a number of roles that require pharmacology knowledge. In addition to
roles and responsibilities, the importance of pharmacology knowledge for nurses is
reinforced by the magnitude of drugs on the market, the use of multiple drug
therapies, changing regimens involving new drugs, and complex fast-paced health
care environments (Adhikari, Tocher, Smith, Corcoran, & MacArthur, 2014; Ndosi &
Newell, 2008). Effective medication management is critical to safe practice; however,
in order for nurses to successfully manage the diverse roles of medication therapy and
promote safe patient care, a comprehensive knowledge of pharmacology is essential
(Adhikari et al., 2014; Dilles, Vander Stichele, Van Bortel, & Elseviers, 2011; King,
2004; Manias & Bullock, 2002a, Manias & Bullock, 2002b).
Despite the need for pharmacology knowledge and the role of nurses in
medication administration, many nurses have insufficient knowledge and are
inadequately prepared in this area (Adhikari et al., 2014; Bullock & Manias, 2002;
Dilles et al., 2011; Honey & Lim, 2008; King, 2004; Latter, Rycroft-Malone, Yerrell,
& Shaw, 2000, 2001; Ndosi & Newell, 2008; Simonsen, Daehlin, Johansson, &
Farup, 2014). Novice nurses or new graduates, in particular, have difficulty
comprehending pharmacology and applying it to practice (Adhikari et al., 2014;
Manias & Bullock, 2002; Simonsen et al., 2014). The limited understanding of
pharmacology is attributed to a variety of academic factors including the lack of
biological sciences in nursing education, difficulty understanding the biological
PHARMACOLOGY KNOWLEDGE ACQUISITION 2
sciences, dissatisfaction with teaching, a gap between theory and practice, inadequate
time devoted to pharmacology, and barriers or lack of opportunities for clinical
application (Bullock & Manias, 2002; Clancy, McVicar, & Bird, 2000; McVicar,
Clancy, & Mayes, 2010; Dilles et al., 2011; King, 2004; Morrison-Griffiths,
Snowden, & Pirmohamed, 2002). The academic issues described in the literature
reflect potential deficiencies in nursing curriculum design or teaching methodologies.
Several studies have explored the influence of course design, teaching strategies, and
other classroom factors (Adhikari et al., 2014; Dilles et al., 2011; Honey & Lim,
2008; King, 2004; Latter et al., 2001; Manias & Bullock, 2002a, 2002b); however,
few studies have examined specific variables unique to the student, or the impact of
clinical opportunities for medication management on pharmacology knowledge
acquisition.
Nursing education is responsible to ensure graduates have acquired the
knowledge and skills to provide safe and effective patient care inclusive of
medication management. Accordingly, it is imperative that nurse educators recognize
the increasing significance of pharmacology education, examine and evaluate
pharmacology curricula, identify variables that impact science comprehension, and
employ effective teaching strategies to support the acquisition of adequate
pharmacology knowledge in pre-licensure nursing students.
Problem
Nurses have a major role in medication administration; however, the knowledge
base for safe medication administration and patient education is inadequate for many
PHARMACOLOGY KNOWLEDGE ACQUISITION 3
nurses and nursing students. The complexities surrounding the acquisition of
pharmacology knowledge are well documented in the literature including, but not
limited to, the task of incorporating adequate pharmacology in nursing curricula, the
difficulty students have with the biological sciences, the lack of faculty expertise or
effective teaching strategies, the extensive amount of content to learn, and the lack of
clinical opportunities for medication administration and decision-making. In order to
improve pharmacology knowledge acquisition by nursing students, it is essential for
nurse educators to better understand the factors contributing to the current
pharmacology knowledge deficit. However, few studies exist in the literature
examining factors that influence or predict pharmacology knowledge acquisition for
nursing students.
Purpose
The purpose of this study was to examine the relationship of selected
academic and non-academic variables in pre-licensure Associate Degree nursing
students, and pharmacology knowledge acquisition as demonstrated by performance
on a final standardized pharmacology assessment. A second purpose of the study was
to evaluate the medication administration and decision-making experience as self-
reported by Associate Degree nursing students, and determine if there was any
correlation between student perceptions of clinical experience opportunities for
medication management and performance on the final pharmacology assessment.
PHARMACOLOGY KNOWLEDGE ACQUISITION 4
Significance of the Problem
Advancements in medical science and technology over the past several
decades have improved the ability to diagnose and manage complicated health
conditions. As a result, patients with chronic illnesses live longer, and are
increasingly dependent on complex therapeutic regimens (Adhikari et al., 2014).
Likewise, changing demographics reveal an aging patient population with multiple
co-morbidities, and many of these patients require more than one prescriptive
medication (Ndosi & Newell, 2008). The acuity of hospitalized patients has risen
significantly, resulting in many patients who are receiving a variety of
pharmacological therapies. These complex regimens potentially compromise safe
patient care as the risk of medication error rises in proportion to the number and
variety of drugs a patient receives (van den Bernt, Egberts, & Lenderink, 2000).
Quality care and patient safety have been targeted intensely for improvement
in health care institutions over the past decade. Reports by the Institute of Medicine
(IOM) of the National Academies have demonstrated that medical errors are common
and adversely affect patient outcomes (IOM, 1999). Current estimates for annual
deaths in the United States related to medical error are as high as 400,000, and
adverse drug events are evolving as a leading cause of death for Americans (James,
2013). Medication errors are costly to patients, families, employers, hospitals, health
care providers, and insurance companies. It has been difficult to determine reliable
estimates of cost, but the IOM suggested that each preventable adverse drug event
occurring in a hospital in 2006 added approximately $8,750.00 to the cost of the
PHARMACOLOGY KNOWLEDGE ACQUISITION 5
hospital stay; the total annual cost of adverse drug events was estimated at three to
five billion dollars (IOM, 2006). Unequivocally, medication errors potentially create
physical, emotional and economic distress for patients and families, cost human lives,
prolong hospital length of stay, and have serious financial consequences for providers
and health care institutions.
Medication management is a complex, multi-stage, multidisciplinary process.
Medication errors may occur at any stage of the medication process, but are most
frequently noted during the prescribing and administration phases (Cohen, 2006;
IOM, 2006). Of the disciplines involved in the medication process, nurses are most
frequently responsible to administer medications to patients. Medication
administration is a high-risk area, and medication errors are noted as a persistent
problem in nursing practice (Armitage & Knapman, 2003; O’Shea, 1999). There are
numerous factors associated with medication errors involving nurses and nursing
students; cited among these factors are the issues of inadequate pharmacology
knowledge and limited clinical experience opportunities for medication management
(Brady, Malone & Fleming, 2009).
Significance to Nursing
Nurses assume a primary role in the administration of medications, and are
regarded as the final link in the defense for medication safety (Adhikari et al., 2014).
It is estimated that nurses spend as much as 30-40% of their time administering
medications (Armitage & Knapman, 2003; Keohane et al., 2008). While studies
confirm that nurses do, in fact, follow the traditional “five rights” principle of
PHARMACOLOGY KNOWLEDGE ACQUISITION 6
medication administration, expertise beyond the “five rights” is needed in order to
ensure holistic medication safety (Adhikari et al., 2014; Eisenhauer, Hurley, & Dolan,
2007). In consideration of the nursing time spent on medication administration, the
high-risk nature of the process, the impact of adverse drug events, and the complexity
of the clinical environment, it is essential for nursing to develop effective strategies to
enhance pharmacology knowledge.
Ensuring that graduates are prepared to function in the current health care
environment is a priority for nurse educators; therefore, it is important that educators
examine factors that contribute to or detract from pharmacology knowledge
acquisition. Evidence reveals that medication errors are high among the prevalent
errors involving new graduate nurses (Cebeci, Karazeybek, Sucu, & Kahveci, 2015;
Smith & Crawford, 2003), and that novice nurses struggle to understand and apply
pharmacology knowledge to clinical practice (Adhikari et al., 2014; Manias &
Bullock, 2002b; Simonsen et al., 2014). Over 6000 drugs are currently approved by
the Food and Drug Administration (FDA), and 25-50 new drugs are added to the
market every year (U.S. FDA, 2013). In addition to preparing students to function as
a beginning clinician, students must also develop effective skills for lifelong learning
in a subject that is constantly changing (Lim & Honey, 2006). The incidence of errors
and the need for effective skills for ongoing learning have wide-ranging implications
for curriculum development, teaching methodologies, and transition to practice. The
findings are also important for administrators with respect to mentoring, orientation
programs, staffing levels, and continuing education.
PHARMACOLOGY KNOWLEDGE ACQUISITION 7
Factors that hinder or promote academic success in nursing and on the
NCLEX-RN examination are highly relevant for nursing education. Updates to the
NCLEX-RN blueprint in 2004 reflected an increase in content associated with
pharmacology and physiological integrity. Additionally, a very recent change in the
NCLEX-RN is the exclusive use of generic names for test items addressing
medications (National Council State Boards of Nursing, 2015). Nurse educators have
a responsibility to identify students who are at risk for failure, and implement early
interventions to promote success or counsel students for an alternative course of
action. Unsuccessful student performance in academia or on the NCLEX-RN
examination has significant consequences for students, programs of nursing and
health care institutions. These consequences include financial burden, emotional
distress, nursing shortages, hiring and training costs, and issues related to nursing
program accreditation. The volume of learning required to master the body of
knowledge necessary for safe nursing practice is overwhelming for students and
continues to rise. All of these factors are significant for nursing education and
pharmacology curricula.
Theoretical Framework
In a 2012 survey of student demographics from Schools of Nursing, the
National League for Nursing (2013) identified that fifty percent of the population of
Associate Degree students are greater than thirty years of age. The Health Resources
and Services Administration (HRSA) under the United States Department of Health
and Human Services (2010) also reports that the average age of nursing students who
PHARMACOLOGY KNOWLEDGE ACQUISITION 8
graduated from their initial nursing education program after 2004 is 31 years. Clearly,
the entry level for the majority of nursing students is well beyond adolescent years,
and therefore, most students are categorized as adult learners. For this reason, adult
learning theory was used to inform the study.
Adult Learning Theory
Andragogy is a term used to refer to the art and science of adult learning or to
the education of adults, which holds a set of assumptions about how adults learn
(Peterson & Ray, 2013). There are several explanations of the Greek origin of the
word, andragogy, which are based on the stems aner, andr or Andros (Henschke,
1998). All explanations of the stems or term, andragogy, denote a meaning of “man,
not boy” or “adult man guiding himself” versus pedagogy, which is explained as
“leader of child” (Henschke, 1998). The term, andragogy, was coined by Alexander
Knapp, a German educator, as early as 1833; however, Malcom Shepherd Knowles
(1913-1997) is primarily credited as pioneering andragogy in America and
developing andragogy into a theory of adult learning (Peterson & Ray, 2013).
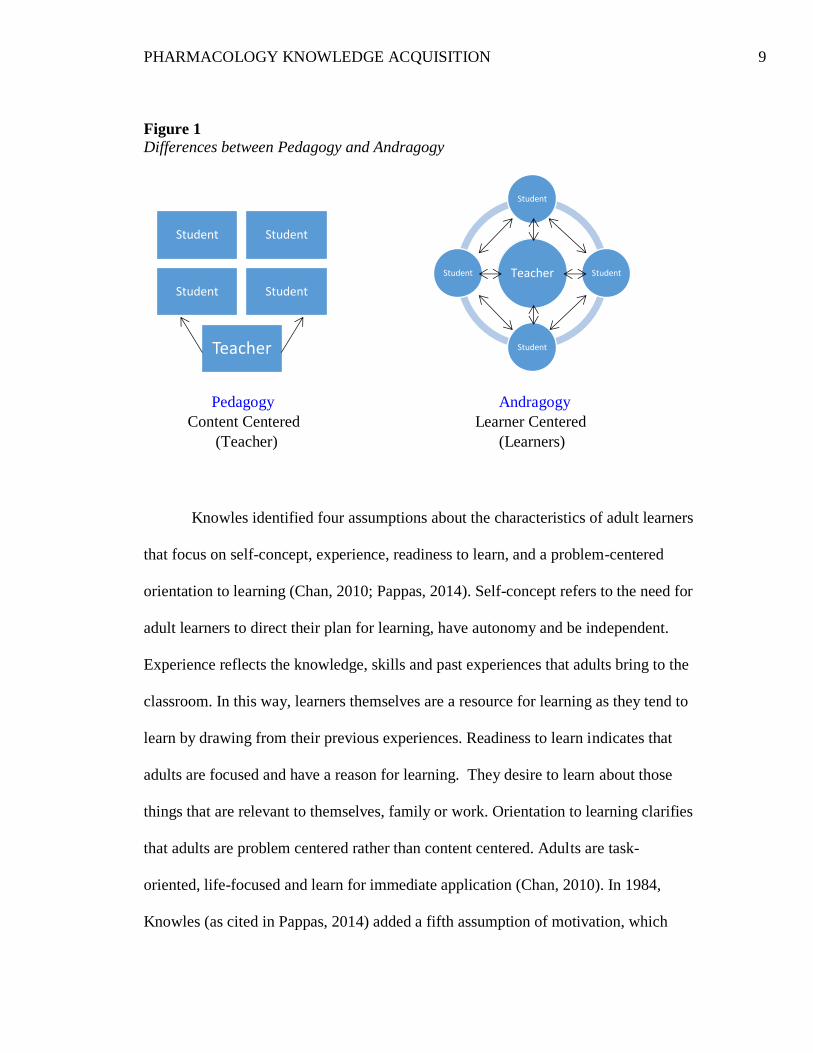
The concept of andragogy specifically focuses on differences in how adults
learn that warrant methods of teaching unlike those used in Pedagogy, the education
of children. Figure 1 demonstrates the difference in relationships between the
instructor and the student in pedagogy as compared to andragogy. In pedagogy, the
learner (child) is dependent on the teacher who controls all learning and the learning
environment. In andragogy, the learner is self-directed and involved in the learning
process, and the teacher is a facilitator of learning.
PHARMACOLOGY KNOWLEDGE ACQUISITION 9
Figure 1
Differences between Pedagogy and Andragogy
Pedagogy Andragogy
Content Centered Learner Centered
(Teacher) (Learners)
Knowles identified four assumptions about the characteristics of adult learners
that focus on self-concept, experience, readiness to learn, and a problem-centered
orientation to learning (Chan, 2010; Pappas, 2014). Self-concept refers to the need for
adult learners to direct their plan for learning, have autonomy and be independent.
Experience reflects the knowledge, skills and past experiences that adults bring to the
classroom. In this way, learners themselves are a resource for learning as they tend to
learn by drawing from their previous experiences. Readiness to learn indicates that
adults are focused and have a reason for learning. They desire to learn about those
things that are relevant to themselves, family or work. Orientation to learning clarifies
that adults are problem centered rather than content centered. Adults are task-
oriented, life-focused and learn for immediate application (Chan, 2010). In 1984,
Knowles (as cited in Pappas, 2014) added a fifth assumption of motivation, which
Student Student
Student Student
Teacher
Teacher
Student
Student
Student
Student
PHARMACOLOGY KNOWLEDGE ACQUISITION 10
recognizes that learning is internally motivated, and there is a sense of urgency about
learning. Billings and Halstead (2012) provide a contemporary and succinct
description of adult learners as “… increasingly self-directed and have experiences
that serve as a rich resource for their own and others’ learning” (p. 221).
In the 1980’s, Knowles also identified four principles that are applied to adult
learning. These principles overlap with some of the assumptions and are described as
the need for adults to be involved in their instruction, the recognition that experience
(including mistakes) provides the basis for learning activities, the need for learning
content that has immediate relevance, and the focus of learning on problems rather
than content (Pappas, 2014). Adult learners are thought to perform well when they
use their prior experience, and apply new knowledge to solve real problems. Two
additional characteristics of adult learners relevant to the theory are that adults have
preferred differences in personal learning style, and have responsibilities and life
situations that provide a social context that affects their learning (Jackson and
Caffarella as cited in Billings & Halstead, 2012). For the adult learner, school is often
secondary to other activities and responsibilities. Knowles emphasized that educators
must understand that adults return to school for specific reasons and to gain specific
knowledge. Educators must also recognize the prior knowledge that adult learners
bring and build on that knowledge.
Holton, Swanson and Naquin (2001) extended the core model of Andragogy
to develop the Andragogy in Practice Framework. This framework offers an
expanded conceptualization of andragogy that incorporates domains that influence the
PHARMACOLOGY KNOWLEDGE ACQUISITION 11
application of core principles. It applies andragogy across multiple domains of adult
learning, and identifies three dimensions in practice: goals and purposes for learning,
individual and situational differences, and core adult learning principles (Holton,
Swanson, & Naquin, 2001). The three rings of the model interact offering a process to
understand adult learning situations. The goals and purposes for learning create the
experience and may be categorized as institutional, societal or individual (Holton,
Swanson, & Naquin, 2001). Individual and situational differences represent variables
that impact adult learning and include subject matter differences, situational
differences and learner differences. The “individual differences” category
incorporates variations in cognitive ability, personality and prior knowledge.
Situational differences during learning include a full range of social, cultural, and
situation-specific factors that may impact the learning transaction (Holton, Swanson,
& Naquin, 2001). The core adult learning principles have been described in the
preceding paragraphs. The model recognizes that learning is multi-faceted, and that
individuals vary in their approaches, strategies and preferences for learning activities
(Holton, Swanson, & Naquin, 2001).
Both Andragogy, or Adult Learning Theory and the expanded Andragogy in
Practice serve as a framework for this study. In a 2012 survey of student
demographics from Schools of Nursing, the National League for Nursing (2013)
identified that fifty percent of the population of Associate Degree students are greater
than thirty years of age. The Health Resources and Services Administration (HRSA)
under the United States Department of Health and Human Services (2010) also
PHARMACOLOGY KNOWLEDGE ACQUISITION 12
reports that the average age of nursing students who graduated from their initial
nursing education program after 2004 is 31 years. Clearly, the entry level for the
majority of nursing students is well beyond adolescent years, and therefore, most
students are categorized as adult learners.
Individual and situational differences as described in the Andragogy in
Practice framework can be applied as variables that influence knowledge acquisition
for adult learners. The core principles of andragogy also incorporate factors that may
be studied as variables that contribute to or impede learning for adult students. For
example, prior experience such as health care experience, or prior knowledge as a
result of earning another degree or college credit may serve to enhance learning.
Cumulative grade point average in nursing and in the sciences reflects cognitive
abilities, which is a component of individual differences in the Andragogy in Practice
model. As adult learners and non-traditional students, employment and family
responsibilities are potential variables that interfere with academic performance and
success in nursing.
Andragogy emphasizes that adult students must find relevance in what they
are learning. This assumption may be applied in relation to the value of clinical
experiences and the opportunities for medication management. In these practical
experiences, the significance of pharmacology to nursing practice is clearly evident
and appreciated by most students. Furthermore, since andragogy emphasizes that
adults tend to learn from previous experiences, it is reasonable to infer that a potential
relationship exists between a student’s cumulative clinical experience in medication
PHARMACOLOGY KNOWLEDGE ACQUISITION 13
management and pharmacology knowledge acquisition. In consideration of the
premise of the theory, the core principles, and the expanded contextual factors, the
Theory of Adult Learning - Andragogy and Andragogy in Practice provides an
appropriate framework to structure the study. Selected academic and non-academic
variables that are especially relevant to adult learners will be evaluated in the study in
order to identify any correlation with pharmacology knowledge acquisition in
Associate Degree pre-licensure nursing students. The quality of students’ clinical
experiences in relation to medication management will also be examined as a
potential factor influencing knowledge acquisition as evaluated by the ATI
standardized pharmacology assessment.
Research Questions
The specific research questions guiding the study were as follows:
1) What is the level of performance for the study group on the final ATI
standardized pharmacology assessment?
2) What is the bivariate relationship between certain academic variables (nursing
grade point average and science grade point average) and non-academic
variables (previous college credit or degree, previous health care experience,
working hours per week, and family responsibilities) and performance on the
final ATI standardized pharmacology assessment?
3) What is the bivariate relationship between students’ self-reported perceived
clinical experiences in medication management and performance on the final
ATI standardized pharmacology assessment?
PHARMACOLOGY KNOWLEDGE ACQUISITION 14
Conceptual Definitions
The following definitions were identified in relation to the specific research
questions, the underlying theoretical framework, and selected variables in the study:
1. Andragogy – The theory of the education of adult students or adult learners.
2. Clinical Experience in Medication Management – Perceived opportunities for
experience in medication administration and decision-making as self-reported
by students.
3. Family Responsibilities – financial responsibility as head of household,
responsibility for dependent children, or responsibility as a caregiver.
4. Health Care Experience – Any current or previous work experience related to
direct patient care in a health care setting.
5. Nursing Grade Point Average - the cumulative grade point average achieved
in three prior nursing clinical courses.
6. Pharmacology Knowledge Acquisition – the acquisition of pharmacology
knowledge expected for a newly licensed, entry-level registered nurse as
demonstrated by scores on the ATI Pharmacology Assessment test that meet
the content-specific assessment benchmark.
7. Science Grade Point Average – the cumulative grade point average achieved
in three prior biological science courses.
Summary
Effective medication management is critical to safe practice, and nurses have
key roles and responsibilities in the administration of medications. In order for nurses
PHARMACOLOGY KNOWLEDGE ACQUISITION 15
to successfully manage the roles and responsibilities of medication management and
ensure safe patient care, a comprehensive knowledge of pharmacology is required.
Research indicates that nurses do not have sufficient knowledge and are inadequately
prepared in pharmacology. The limited knowledge of pharmacology by nurses and
nursing students is attributed to a variety of factors that impact educators and
academia. Nurse educators are responsible to ensure that graduates have sufficient
knowledge and skills for safe practice. Medication competence is a priority for
nursing education, and requires educators to carefully assess pharmacology curricula,
implement effective teaching methodologies, provide ample clinical opportunities for
medication decision-making, and identify variables that impact pharmacology
knowledge acquisition.
Research has identified a correlation between pharmacology course grades or
standardized assessments, and performance on the NCLEX-RN. A number of studies
have been conducted to determine variables that predict successful NCLEX-RN
performance; however, few studies have investigated variables that influence
pharmacology learning. The purpose of this study was to examine selected academic,
non-academic, and clinical variables for nontraditional second-year students in an
Associate Degree nursing program, and determine if any of these variables correlated
with successful acquisition of pharmacology knowledge. There was a large
population of nontraditional students in the selected program, and nontraditional
students are perceived as a potential group at risk for retention and academic
performance issues. Identifying valid predictors of academic success or failure
PHARMACOLOGY KNOWLEDGE ACQUISITION 16
enables nurse educators to pinpoint high-risk students, provide needed academic
support, and optimize student performance. Empirical evidence of the relationship
between standardized assessments in pharmacology and NCLEX-RN performance
also supports the need to further investigate factors that influence or predict
pharmacology knowledge acquisition.
PHARMACOLOGY KNOWLEDGE ACQUISITION 17
Chapter 2: Review of the Literature
The purpose of this study was to examine the relationship of selected
academic and non-academic variables to pharmacology knowledge acquisition by
undergraduate nursing students as demonstrated by performance on a final
standardized pharmacology assessment. A second purpose of the study was to
evaluate the medication administration and decision-making experience as self-
reported by students, and determine if there was any correlation between student
perceptions of opportunities for medication management during clinical experiences,
and performance on the final standardized pharmacology assessment. This chapter
contains a review of the current literature in relation to four primary areas: 1) studies
of pharmacology knowledge level in nurses, new graduate nurses, and nursing
students; 2) studies identifying inadequate pharmacology knowledge as a factor for
medication errors; 3) studies of factors influencing pharmacology knowledge
acquisition; and 4) strategies faculty have used to enhance pharmacology knowledge
acquisition.
The process used to review the literature was consistent for all primary areas
to be presented. Several web-based searches were conducted with a variety of
keywords or search terms through PubMed (inclusive of MEDLINE), Cumulative
Index for Nursing and Allied Health Literature (CINAHL), and Education Resources
Information Center (ERIC). Additional searches were completed through OVID, a
software available through the hospital and college library service, which
incorporates MEDLINE, Pre MEDLINE, CINAHL, Evidence Based Medicine
PHARMACOLOGY KNOWLEDGE ACQUISITION 18
(EBM) Reviews, Cochrane Database of Systematic Reviews, Cancerlit, and Excerpta
Medica Database (EMBASE). The database searches were primarily limited to the
past ten years, although some earlier key studies that have been cited frequently in the
literature were also reviewed and are included in this discussion.
Pharmacology Knowledge Level for Nurses, Graduate Nurses, Nursing Students
Effective medication management is critical to safe practice, and dependent
on adequate pharmacology knowledge of the nurse. However, a number of studies
present evidence that nurses have insufficient pharmacology knowledge, lack
confidence in their knowledge, or are inadequately prepared in this area. Twelve
research studies ranging from 1996 to 2015 were examined regarding the adequacy of
pharmacology knowledge, factors impacting this knowledge, and recommendations to
improve pharmacology education. For purposes of this study, articles solely
addressing mathematical skills and drug calculations were excluded from the review.
The research is presented in reverse chronological order and organized under the
following subject headings: inadequate pharmacology knowledge for nurses and new
graduates and inadequate pharmacology knowledge for nursing students. The
following discussion focuses on the more prominent studies that reported on the level
of pharmacology knowledge in nurses, new graduates, and nursing students.
Inadequate pharmacology knowledge for nurses, new graduate nurses.
The first study in this section addressed pharmacology knowledge level for
both nurses and nursing students. Adhikari et al. (2014) conducted an ethnography-
style observational study utilizing qualitative interviews and group discussions to
PHARMACOLOGY KNOWLEDGE ACQUISITION 19
study the medication management systems and practices of two hospital wards. This
study also sought to clarify nursing education on medication safety in three Higher
Education Institutions (HEIs) in Scotland. The researcher spent 63 hours shadowing
health care professionals, and conducted seven interviews with charge nurses and
registered nurses. Data was also collected from 21 final year nursing students in three
HEIs using peer and focus group discussions. While the authors found that nursing
staff did, in fact, follow the “five-rights” principle of medication administration, they
concluded that this principle alone is inadequate to ensure holistic medication safety.
The study reported that nursing students expressed a lack of confidence and concerns
of limited knowledge in pharmacology, and insufficient understanding of how
medications work. Furthermore, the depth of learning experiences and clinical
exposure in pharmacology during clinical placements varied among the group.
Eisenhauer et al. (2007) also emphasized that medication administration requires
professional expertise beyond the technical application of the “five-rights” principle.
This conclusion was based upon semi-structured interviews and real-time tape
recordings of 40 nurses at a large tertiary care teaching hospital. Eisenhauer et al.
(2007) analyzed nurses’ thinking processes during medication administration, and
revealed that nursing judgment was required for dosage, timing, and selection of
specific medications.
A comparative study examining medication knowledge, certainty and risk of
error between graduating Bachelor of Science in nursing (BSN) students and
experienced nurses was completed by Simonsen et al. (2014). A multiple-choice test
PHARMACOLOGY KNOWLEDGE ACQUISITION 20
in pharmacology, drug management and drug dose calculations was administered to
243 graduating students and 203 registered nurses. The participants were required to
assign a self-estimated level of certainty for accurately answering each question. The
risk of medication error was then defined based on the combination of knowledge and
certainty for each question. Medication knowledge of experienced nurses was
superior to graduating students with the largest difference in drug management and
dosage calculations. Overall, the knowledge of both experienced nurses and nursing
students was still considered insufficient as the study revealed that one out of four
(25%) answers to test questions on drug management would have led to a high risk of
error. The authors noted that the findings of their study were consistent with an
integrative review by Killam et al. (as cited in Simonsen et al., 2014), which
emphasized lack of knowledge, skill incompetence, and overconfidence as
characteristics of students who are at risk for unsafe nursing practice.
A non-experimental causal comparative and correlational design was used in a
study by Ndosi and Newell (2008) to determine if nurses had adequate knowledge of
the drugs they commonly administer. Data was collected by structured interview and
questionnaire methods from 42 nurses working in surgical wards in England.
Participants blindly selected one out of four drugs they commonly administer, and
were required to answer standard questions focusing on specific pharmacology
knowledge. Knowledge scores ranged from 20-90% with a mean score of 60%. The
majority (n=31, 74%) scored below 80%, which was considered insufficient
knowledge by the authors. The median experience of the participants was 10.87
PHARMACOLOGY KNOWLEDGE ACQUISITION 21
years, and a correlation was found between test scores and years of experience. The
study suggested that nurses have inadequate pharmacology knowledge, especially for
drug interactions and mechanism of action, and that supplementary education focused
on common drugs is needed in clinical settings to promote safer medicine
management.
A descriptive study by King (2004) attempted to identify nursing roles that
require pharmacology knowledge, and evaluate nurses’ preparation for practice
through undergraduate pharmacology education. A qualitative approach was used to
collect data from 10 staff nurses of a 30-bed emergency admissions unit in northern
England. Semi-structured interviews were audiotaped, transcribed, and analyzed
using Burnard’s 14-stage method for analysis (Burnard as cited in King, 2004).
Participants indicated that they did not have sufficient pharmacology knowledge,
were dissatisfied with their pharmacology education, and experienced anxieties
related to potential harm as a result of insufficient preparation. Lack of structure,
insufficient time spent on pharmacology, and over-emphasis of the behavioral
sciences were cited as issues in undergraduate education. The author concluded that
improved teaching might increase nurses’ confidence in performing drug
administration and patient education, and decrease anxieties related to these roles.
Manias and Bullock (2002a, 2002b) completed two separate studies to explore
the perceptions and experiences of lecturers, students, and clinical nurses regarding
the educational preparation of undergraduate nursing students in pharmacology. The
second study (Manias & Bullock, 2002b) specifically focused on the perceptions and
PHARMACOLOGY KNOWLEDGE ACQUISITION 22
experiences of clinical nurses regarding graduate nurses’ medication knowledge. In
this descriptive study, six focus group interviews were conducted with 38 nurses at
metropolitan and regional hospitals in Victoria, Australia. Four themes emerged from
the interviews including the knowledge base of graduate nurses, continuing education
needs of graduate nurses, aspects of pharmacology knowledge perceived as important
for nursing practice, and improvements for undergraduate nursing education. Clinical
nurses identified that the pharmacology knowledge base of graduate nurses was
severely inadequate. Furthermore, the study revealed that some experienced nurses
also lacked knowledge resulting in a reluctance to mentor or teach new graduate
nurses. Recommendations for pre-licensure education included the need for more
structured clinical experiences, pharmacology as a separate course, and self-directed
learning strategies for lifelong continuing education.
Ives, Hodge, Bullock, and Marriott (1996) have been cited in many articles for
their descriptive study to identify first year registered nurses’ actual and self-rated
pharmacology knowledge. A questionnaire survey was completed by 363 first year
nurses requiring participants to self-rate their knowledge in five categories of
pharmacology, and to answer questions designed to test their knowledge of the same
five categories. The survey also asked participants to rank the value of pharmacology
teaching strategies used in their undergraduate education. Test scores ranged from
16% to 92% with a mean score of 55.8%, and 35% of respondents scored less than
50% on the test. The study found that longer experience as a registered nurse
correlated with higher test scores. Respondents indicated that first year practical
PHARMACOLOGY KNOWLEDGE ACQUISITION 23
experience and undergraduate clinical experience were the most important
contributions to their current pharmacology knowledge. Overall, the authors
concluded that many new nurses have an inadequate knowledge of pharmacology.
Allocating more time to pharmacology (35.3%), teaching pharmacology as a separate
subject (30.9%), and improved teaching methods (20.6%) were cited by nurses as
factors that would have improved undergraduate pharmacology education.
Inadequate pharmacology knowledge for nursing students.
A descriptive cross-sectional study of nursing education in Flanders, Belgium
was conducted by Dilles et al. (2011), which sought to describe pharmacology
education, evaluate graduating students’ pharmacology knowledge and calculation
skills, and describe their self-rated readiness for safe medication practice. Twenty-
nine schools participated in the study, and findings showed considerable diversity in
pharmacology curricula. These differences were noted in hours of content, specific
content topics, background or profession of the instructor, and integrated versus
separate pharmacology modules. A total of 613 graduating students also participated
in a correlational survey using the Medication Knowledge and Calculations Test
(MKC test). The mean score on the knowledge component of the MKC test was 52%
for diploma students (n=404) and 55% for baccalaureate students (n=209). On a scale
of 1-10, 27% of students rated readiness perception as < 5, and only 15% rated
themselves at eight or higher. No relationships were identified with the organization
of pharmacology as a separate or integrated module, the amount of hours per study
year, or the background of the instructor. However, the authors concluded that
PHARMACOLOGY KNOWLEDGE ACQUISITION 24
graduating nursing students’ pharmacology knowledge and calculation skills are
insufficient to deliver safe medication care, and identified the need for defining a
framework with clear goals for pharmacology education.
Honey and Lim (2008) conducted a qualitative descriptive study to explore
nursing students’ perceptions of clinical practice situations and the ability to apply
pharmacology knowledge. Following completion of a final clinical rotation, 54
students in a class of 60 (90%) participated in the survey. An iterative method of
content analysis was used to identify phrases and themes from the survey responses.
The lack of time, accessible drug resources, opportunities to practice decision-
making, and role modeling by preceptors were identified as practice setting and staff-
related barriers. Lack of confidence in their depth and ability to apply pharmacology
knowledge, and information overload were two additional themes that emerged.
Some students (20%) indicated that academic preparation for pharmacology was
inadequate, and perceived the amount of information to learn as a barrier to
integrating pharmacology. Feelings of stress, lack of confidence in retaining
information, and the need to learn both trade and generic names of drugs were cited
as contributing factors to information overload. The authors emphasized the need to
explicitly link theory with clinical practice, and that students should learn
fundamental principles of pharmacology rather than attempting rote memorization of
multiple drugs.
The first study completed by Manias and Bullock (2002a) explored the
perceptions and experiences of lecturers and students regarding the educational
PHARMACOLOGY KNOWLEDGE ACQUISITION 25
preparation of undergraduate nursing students in pharmacology. This study involved
fourteen focus group interviews at ten university settings in Victoria, Australia.
Participants comprised second and third year undergraduate students, and lecturer
participants included both nursing and bioscience faculty. In relation to pharmacology
knowledge level, the study found that basic pharmacological principles were rarely
addressed, and learning was superficial as students focused on memorizing isolated
and numerous facts about individual medications without understanding
characteristics of a group of medications. In addition to superficial learning, the study
identified that fast-paced clinical practice settings precluded productive learning
experiences in medication administration and management.
A study by Latter et al. (2001) reported on findings from a national survey
conducted to evaluate the educational preparation of nurses for a medication
education role in practice. A postal questionnaire was distributed to all higher
education institutions delivering pre and post-registration education in England.
Respondents were queried regarding curriculum design, time allocated to
pharmacology, learning outcomes, teaching methods, assessment strategies, and
integration of learning. The survey revealed a general dissatisfaction with the amount
of pharmacology included in the curricula, and the predominant model for teaching
pharmacology was as an integrated subject within other courses. The study also found
a lack of clarity regarding the pre-requisite knowledge required for practice as
reflected by imprecise learning outcomes and competencies, particularly for
medication education. The authors emphasized the need to establish outcomes and
PHARMACOLOGY KNOWLEDGE ACQUISITION 26
competencies within the national policy framework for nurse education in order to
delineate knowledge and skills that should be included, and the amount of time that
should be devoted to the subject.
Summary of inadequate pharmacology knowledge and education.
In relation to a lack of pharmacology knowledge and education, the studies
reviewed primarily presented descriptive qualitative research. Two studies were
identified as comparative research designs; one of these two studies was a non-
experimental causal comparative and correlational design. One study in the review
was identified as a cross-sectional descriptive study. Sample populations were
comprised of staff registered nurses (including experienced and graduate nurses),
nursing students and nursing educators. A large percentage of the collective sample
encompassed first-year graduate nurses and final-year nursing students. In all studies
reviewed, data was collected through semi-structured peer, individual, and focus
group interviews, as well as surveys and questionnaires. One study incorporated real-
time tape recordings during medication administration, and four studies incorporated
some method of testing for pharmacology knowledge and drug calculations.
All of the studies included in this section of the review of the literature
queried subjects regarding medication safety practices and the adequacy of
pharmacology knowledge for nurses and nursing students. One study sought to
document nurses’ thinking processes during medication administration, and one study
focused on student perceptions of clinical experiences for application of
pharmacology knowledge. Many studies questioned about the perceptions of nurses,
PHARMACOLOGY KNOWLEDGE ACQUISITION 27
nursing students and nurse educators regarding pharmacology education,
pharmacology curricula, and factors that influence the quality of pharmacology
knowledge acquisition. A collective summary of the research in relation to
pharmacology knowledge and education for nurses (including new graduate nurses)
and nursing students is presented.
Registered Nurses. Many clinical nurses acknowledge a lack of confidence
and knowledge in pharmacology, particularly in relation to patient medication
education, understanding of mechanism of action, and drug interactions. The lack of
nurses’ pharmacology knowledge, combined with the complex fast-paced nature of
the clinical setting hinders mentoring and teaching for both graduate nurses and
undergraduate students. It is also suggested that inexperienced new graduates are
potentially unable to recognize high-risk situations with medications, or may not be
prepared to manage adverse events, particularly in the context of multiple distractions
in the clinical setting. The demand for multi-tasking further increases the risk of error.
Pharmacology knowledge does tend to increase with length of experience, but
seasoned nurses are also noted to have knowledge deficits. Clinical nurses and new
graduate nurses consistently express dissatisfaction with undergraduate pharmacology
education, and indicate that more time needs to be allocated to pharmacology
curricula. Nurses, educators, and researchers agree that post-licensure supplemental
education is also important to consolidate pharmacology, but nurses observe the need
for continuing education programs that focus on mechanism of action, adverse
effects, and drug interactions rather than safe administration of medication.
PHARMACOLOGY KNOWLEDGE ACQUISITION 28
Nursing Students. The research suggests that students’ pharmacology
knowledge and calculation skills are inadequate to support safe medication care.
Throughout the literature students identify that the amount of time spent on
pharmacology curricula does not match the extent of time nurses spend in practice for
managing patient medications. Overall, most students believe that academic
preparation for pharmacology is inadequate. Students lack confidence in their depth
of pharmacology knowledge and in the ability to apply that knowledge. The literature
identifies that students typically resort to superficial learning strategies as a result of
information overload, faculty expectations, and lack of guidance in self-directed
learning. Drug calculations and mathematical skills remain an ongoing problem area
for pre-licensure students, but conceptual skills in relation to extracting clinical data
and logically constructing a problem have been emphasized as a leading source of
math deficiency rather than calculation skills.
Inadequate Pharmacology Knowledge as a Factor for Medication Errors
Research studies addressing adverse drug events or medication errors in the
healthcare environment, particularly involving nurses and nursing students, were
examined to validate inadequate pharmacology knowledge as a contributing factor to
error. A total of fourteen articles published from 1999 to 2015 were reviewed, and the
sample population for each study targeted nurses or nursing students. All studies
sought to identify perceptions and factors contributing to medication errors, and data
was primarily collected by direct observation, surveys, or focus-group semi-
PHARMACOLOGY KNOWLEDGE ACQUISITION 29
structured interviews. An overview of the most prominent of these exploratory
descriptive studies is presented.
Three studies presented a review of the literature on medication error factors
based upon a comprehensive computerized data search (Armitage & Knapman, 2003;
Brady, Malone, & Fleming, 2009; O’Shea, 1999). Brady, Malone, and Fleming
(2009) completed a review of the empirical literature on factors contributing to
medication errors from 1988 to 2007. Twenty-six quantitative and qualitative studies
were selected for specific review from an initial search generating 93 papers. The
authors determined that multiple complex factors impacted medication errors
inclusive of both system and individual issues. In the category of knowledge and
skills, the literature review revealed a high percentage of drug errors related to a
nurse’s lack of knowledge and experience with either the drug or equipment.
Confusion over drug names, lack of safety knowledge (i.e. compatibility issues),
miscalculations of dosage, and inability to conceptualize clinical information to
formulate a mathematical calculation were specific subsets of knowledge and skill
factors contributing to medication errors.
Armitage and Knapman (2003) utilized the ten factors for the role of the nurse
in drug administration as identified by O’Shea (1999) as a framework for their review
of adverse events. Contributing factors to adverse events included workload, staffing
shortages, failure to follow policy, distractions or interruptions, lack of
communication, and lack of pharmacology knowledge, particularly in relation to a
lack of conceptual mathematical skills. Evidence for length of experience and
PHARMACOLOGY KNOWLEDGE ACQUISITION 30
educational level was inconclusive, but a Japanese study of 2800 errors (Kawamura,
as cited in Armitage & Knapman, 2003) did identify poor knowledge of recent
graduates as a key factor for intravenous drug errors. In addition to new graduates,
many studies reviewed by Armitage and Knapman (2003) indicated that nurses new
to the job, hospital, or clinical unit were more likely to make errors despite years of
experience.
O’Shea (1999) is cited by many authors for her literature review on factors
contributing to medication errors. She identified these factors as the following:
mathematical skills of nurses, nurses’ knowledge of medications, length of
experience, length of nursing shifts, workload, staffing levels, medication delivery
systems, single-nurse drug administration, policy and procedures, distractions and
interruptions, and quality of prescriptions. The lack of mathematical proficiency was
related to math calculations, conceptual issues, and measurement inabilities.
Three prominent studies examined factors contributing to medication errors as
perceived by nursing students (Cebeci et al., 2015; Harding & Petrick, 2008; Wolf,
Hicks, & Serembus, 2006). Cebeci et al. (2015) completed a cross-sectional survey of
324 students in Turkey over one academic year noting 402 reported errors, of which
124 (38.3%) actual errors occurred. The leading causes of error as identified by
students were performance deficit (n=141, 43.4%) and knowledge deficit (n=133,
41%). Harding and Petrick (2008) conducted a retrospective review of 77 medication
errors made by baccalaureate nursing students over a three-year period. Of the 77
errors, 28 (36.4%) were associated with limited knowledge and understanding of the
PHARMACOLOGY KNOWLEDGE ACQUISITION 31
student. Forty-two percent of omission errors were related to the inexperience of
students in reading or accurately interpreting the medication administration record
(MAR). A descriptive, retrospective, secondary analysis study by Wolf et al. (2006)
examined 1135 medication administration errors by nursing students as reported to
MEDMARX, a national voluntary, internet-accessible medication error database.
The majority of errors were omission errors, followed by errors of administering the
wrong dose of a drug. Performance deficits (51.01%) and lack of knowledge
(26.52%) were prevalent causes of error, and inexperienced staff (77.71%) was a
leading contributing factor to error.
Two studies examined factors for medication errors as perceived by nurses
(Smith & Crawford, 2003; Tang, Sheu, Yu, Wei, & Chen, 2007). Smith and Crawford
(2003) attempted to determine the degree to which newly licensed nurses are involved
in medical errors, and the challenges novice nurses experience with beginning patient
assignments. Stratified random samples of 1000 recently registered nurses (RNs) and
1000 licensed practical/vocational nurses (LPN/VNs) were selected for a survey
questionnaire. Almost all of the RNs (97%) were working for an average of 6.8
months, and 87% were employed in hospitals. Forty-nine percent of RNs had been
involved in errors, and medication errors were cited as the most frequent type of error
(75%). Inadequate staffing was identified as the most frequent factor contributing to
all errors (70%), followed by communication issues (44%) and long work hours
(23%). Approximately 20% of RNs believed that their initial and current patient
assignments were too difficult.
PHARMACOLOGY KNOWLEDGE ACQUISITION 32
Tang et al. (2007) administered a questionnaire to seventy-two registered
nurses who were required to choose from a classification of eight categories and 34
conditions when assigning contributing factors to medication errors. “Personal
neglect” (86.1%), “heavy workload” (37.5%), and “new staff” (37.5%) were the three
main factors in the eight categories. The need to “solve other problems while
administering drugs” (47%), “new graduate” (31.9%), and “advanced drug
preparation without rechecking” (29%) were ranked most frequently of the 34
conditions. Unfamiliarity with the medications, drug names, and mechanism of action
were also involved in a number of errors in the study.
Simonsen et al. (2014) conducted a study that compared the risk of medication
errors between graduating students and working registered nurses. A multiple-choice
test in pharmacology, drug management, and drug dose calculations was administered
to 243 graduating students and 203 registered nurses. Medication knowledge of
experienced nurses was superior to graduating students with the largest difference in
drug management and dose calculations. Overall, the knowledge of both experienced
nurses and nursing students was still considered insufficient as the study revealed that
one out of four (25%) answers to test questions on drug management would have led
to a high risk of error.
Summary of Inadequate Pharmacology Knowledge as a Factor for
Medication Errors.
A recurring theme in the literature is the conclusion that because many factors
and confounding variables contribute to medication errors, any attempt to clearly
PHARMACOLOGY KNOWLEDGE ACQUISITION 33
pinpoint causation is extremely difficult (Armitage & Knapman, 2003). Factors
contributing to medication errors primarily center on the following themes:
medication reconciliation, medication distribution systems, the quality of
prescriptions, deviations from policies and procedures, distractions during medication
administration, excessive workloads, staffing shortages, breakdowns in
communication, and nurses’ knowledge of medications. It was interesting to note that
some authors interpret the lack of drug knowledge as a consequence of systems
failure.
Knowledge deficits contributing to drug errors have been related to dosage
miscalculations, lack of knowledge for mechanism of action, unfamiliarity with the
medications, lack of conceptual mathematical skills, confusion with drug names, and
lack of safety knowledge such as compatibility issues, drug interactions, and drug
side effects (Adhikari et al., 2014; Bullock & Manias, 2002; Honey & Lim, 2008;
King, 2004; Latter et al. 2001; Morrison-Griffiths et al., 2002; Simonsen et al., 2014).
The findings for length of nursing experience as a contributing factor to errors have
been inconsistent; however, several studies report a higher prevalence of errors with
new staff, novice nurses, or new graduates (Armitage & Knapman, 2003; Simonsen et
al., 2014; Smith & Crawford, 2003; Tang et al., 2007).
In general, it is agreed that medication errors are relatively common in
hospitalized patients, potentially result in patient morbidity and mortality, and
increase the cost of healthcare. The literature emphasizes that the nature of
medication errors is complex, multifaceted, and involves an increasing number of
PHARMACOLOGY KNOWLEDGE ACQUISITION 34
system issues. The association of systems issues or systems failure with medication
errors is discussed at length in many studies; however, the literature also consistently
identifies knowledge deficits in pharmacology as a significant factor contributing to
the risk of error.
Factors Influencing Pharmacology Knowledge Acquisition
A number of studies in the literature address variables that influence academic
success and performance on the NCLEX-RN examination in general. However, only
one study was found that specifically evaluated factors correlating with pharmacology
knowledge acquisition. Strayer and Beitz (2010) conducted a comparative descriptive
design study to analyze the nature and strength of the relationship between academic
and nonacademic variables (including the Kolb Learning Styles Inventory III), and
final pharmacology course grades. The relationship of selected variables to
pharmacology course grades was also compared between traditional and
nontraditional students. A convenience sample of 58 traditional students and 73
nontraditional students comprised the initial study population with a final sample of
100 participants. As demonstrated in numerous studies on academic performance,
overall grade point average (GPA) showed a positive correlation with pharmacology
course grades. Lower pharmacology course grades were noted with the nontraditional
student group; the authors suggested that students with nonacademic responsibilities
such as family dependence and the need to work to support themselves do not
perform as well academically. “Program format and learning styles revealed a weak
significant negative correlation suggesting that teaching and testing methods did not
PHARMACOLOGY KNOWLEDGE ACQUISITION 35
fit the learning styles of the nontraditional students”(Strayer & Beitz, 2010, p. 305).
Also, in contrast to earlier studies in the literature, learning style did not play a
significant role in pharmacology knowledge acquisition. Regression analysis revealed
GPA and family dependence as the variables that contributed to the prediction of
pharmacology success or failure.
There is an overlap of studies that have documented inadequate pharmacology
knowledge with studies that have identified potential factors influencing
pharmacology knowledge acquisition. Several investigators report barriers to
pharmacology knowledge as perceived by students and graduate nurses, as well as
recommendations from nurses and students for enhancing pharmacology knowledge
and education. Table 1 presents a summary of the studies discussed previously in
Chapter 2 that also described factors believed to promote or impede pharmacology
knowledge acquisition. The type of study, measures used, and population sample
have been described in the previous section. The recommendations presented by
researchers were based upon data collected from nurses, students, and educators
through interviews, surveys and/or questionnaires.
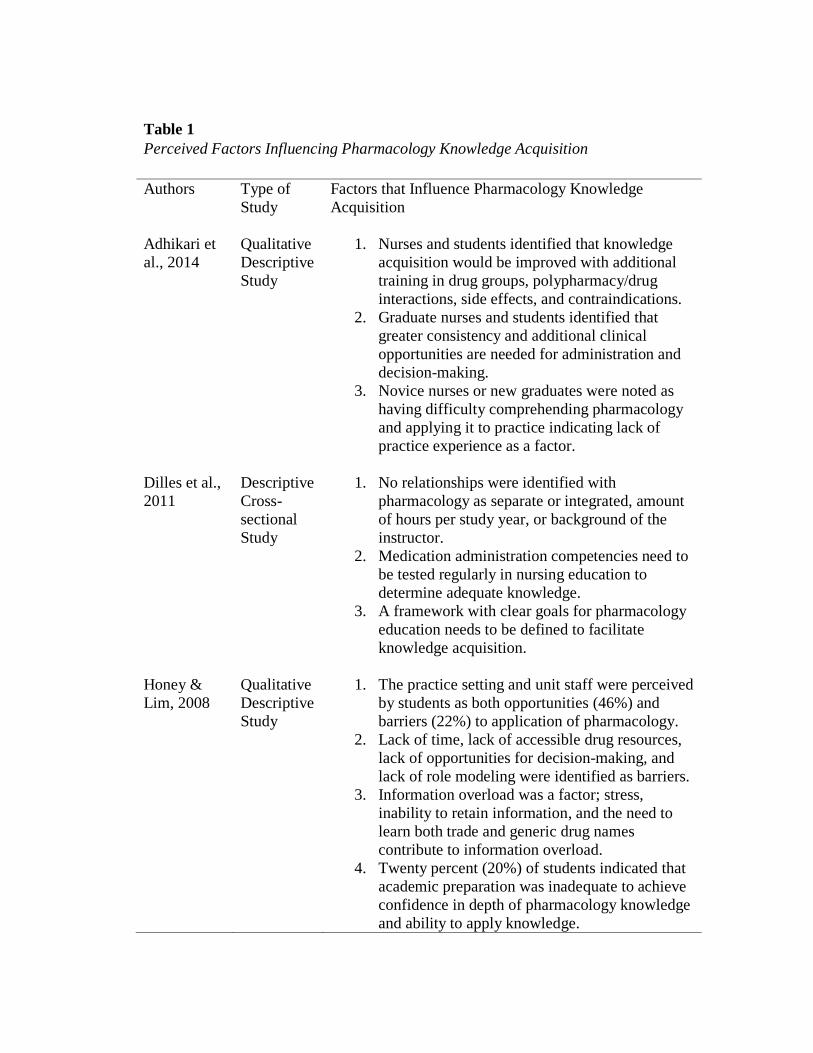
Table 1
Perceived Factors Influencing Pharmacology Knowledge Acquisition
Authors
Type of
Study
Factors that Influence Pharmacology Knowledge
Acquisition
Adhikari et
al., 2014
Dilles et al.,
2011
Honey &
Lim, 2008
Qualitative
Descriptive
Study
Descriptive
Cross-
sectional
Study
Qualitative
Descriptive
Study
1. Nurses and students identified that knowledge
acquisition would be improved with additional
training in drug groups, polypharmacy/drug
interactions, side effects, and contraindications.
2. Graduate nurses and students identified that
greater consistency and additional clinical
opportunities are needed for administration and
decision-making.
3. Novice nurses or new graduates were noted as
having difficulty comprehending pharmacology
and applying it to practice indicating lack of
practice experience as a factor.
1. No relationships were identified with
pharmacology as separate or integrated, amount
of hours per study year, or background of the
instructor.
2. Medication administration competencies need to
be tested regularly in nursing education to
determine adequate knowledge.
3. A framework with clear goals for pharmacology
education needs to be defined to facilitate
knowledge acquisition.
1. The practice setting and unit staff were perceived
by students as both opportunities (46%) and
barriers (22%) to application of pharmacology.
2. Lack of time, lack of accessible drug resources,
lack of opportunities for decision-making, and
lack of role modeling were identified as barriers.
3. Information overload was a factor; stress,
inability to retain information, and the need to
learn both trade and generic drug names
contribute to information overload.
4. Twenty percent (20%) of students indicated that
academic preparation was inadequate to achieve
confidence in depth of pharmacology knowledge
and ability to apply knowledge.
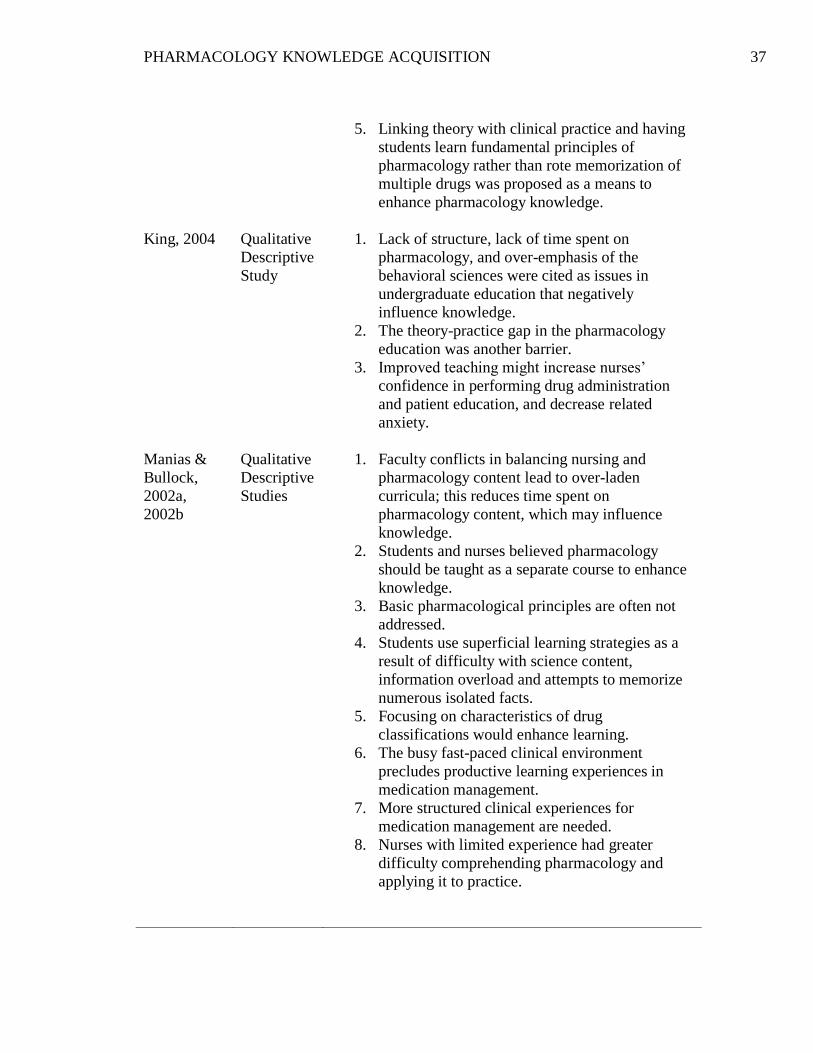
PHARMACOLOGY KNOWLEDGE ACQUISITION 37
King, 2004
Manias &
Bullock,
2002a,
2002b
Qualitative
Descriptive
Study
Qualitative
Descriptive
Studies
5. Linking theory with clinical practice and having
students learn fundamental principles of
pharmacology rather than rote memorization of
multiple drugs was proposed as a means to
enhance pharmacology knowledge.
1. Lack of structure, lack of time spent on
pharmacology, and over-emphasis of the
behavioral sciences were cited as issues in
undergraduate education that negatively
influence knowledge.
2. The theory-practice gap in the pharmacology
education was another barrier.
3. Improved teaching might increase nurses’
confidence in performing drug administration
and patient education, and decrease related
anxiety.
1. Faculty conflicts in balancing nursing and
pharmacology content lead to over-laden
curricula; this reduces time spent on
pharmacology content, which may influence
knowledge.
2. Students and nurses believed pharmacology
should be taught as a separate course to enhance
knowledge.
3. Basic pharmacological principles are often not
addressed.
4. Students use superficial learning strategies as a
result of difficulty with science content,
information overload and attempts to memorize
numerous isolated facts.
5. Focusing on characteristics of drug
classifications would enhance learning.
6. The busy fast-paced clinical environment
precludes productive learning experiences in
medication management.
7. More structured clinical experiences for
medication management are needed.
8. Nurses with limited experience had greater
difficulty comprehending pharmacology and
applying it to practice.
PHARMACOLOGY KNOWLEDGE ACQUISITION 38
Bullock &
Manias,
2002
Latter et al.,
2001
Ives et al,
1996
Qualitative
Descriptive
Analysis
Study
Qualitative
Descriptive
Study
Qualitative
Descriptive
Study
9. Self-directed learning strategies for lifelong
continuing education are needed to maintain
adequate pharmacology knowledge.
1. Inadequate time was dedicated to pharmacology;
a greater number of hours was allocated when
taught as a separate subject.
2. Additional time for pharmacology would be at
the expense of other needed curricular content.
3. Factors impeding pharmacology knowledge
included lack of reinforcement of theory in
clinical, timing of clinical opportunities with the
timing of theory content, and expectations of
students by the instructor.
4. The hectic environment of the clinical setting,
and the need for more consistent exposure in
clinical experiences were also identified as
factors influencing pharmacology
5. Educators believed that pharmacology
application is enhanced by faculty who have a
nursing background.
1. Pharmacology taught as an integrated subject
may contribute to the lack of adequate
pharmacology content.
2. There is a lack of clarity for the pre-requisite
pharmacology knowledge required for practice; a
national policy framework is needed to identify
learning outcomes, skills, and the amount of time
that should be devoted to the subject.
3. Faculty need to be able to apply theory to
practice to enhance pharmacology.
1. First year practical experience and undergraduate
clinical experience were identified as the most
important factors for pharmacology knowledge.
2. Allocating more time to pharmacology (35.3%),
teaching pharmacology as a separate subject
(30.9%), and improved teaching methods
(20.6%) were cited as factors that would have
improved undergraduate pharmacology
education.
Two studies not previously discussed that identified potential factors
influencing pharmacology knowledge included a study by Morrison-Griffiths et al.
(2002), and a study by Courtenay (1991). In 2002, Morrison-Griffiths et al.
distributed survey questionnaires to 52 university nursing departments in England to
identify the pharmacology education provided for pre-registration (pre-licensure)
nurses. Thirty-three questionnaires from three different types of programs were
completed for a 63.5% response rate. The results of the study showed wide variation
in pre-licensure pharmacology education. This variation is noted in terms of hours
allocated, specific content included, resources and teaching methodologies, and
assessment of learning outcomes. Interestingly, it was found that the least number of
hours were allocated in the program with the greatest number of students. The
majority of programs indicated that nurses were involved in the planning of
pharmacology content, and methods of teaching varied significantly, although lecture
was still the most common method.
Nurses and nursing students traditionally identify the biological sciences,
including pharmacology, as difficult subjects to understand (Caon & Treagust, 1993;
Courtenay, 1991; Clancy et al., 2000; McVicar et al. 2010; Tse & Lo, 2008). A
landmark study by Courtenay (1991) explored the teaching and learning of the
biological sciences in nursing, and found several issues related to pharmacology
education. A questionnaire was sent to 140 third-year nursing students (62% response
rate) and 43 nursing faculty (67% response rate) to evaluate the importance of
behavioral and biological sciences, level of knowledge taught, adequacy of
PHARMACOLOGY KNOWLEDGE ACQUISITION 40
preparation, and teaching methods. Both students and teachers felt themselves to be
inadequately prepared in pharmacology and microbiology, and 68.2% of students
identified the subject of pharmacology to be taught at a low level. Although self-
directed learning was the teaching method most frequently utilized by faculty (36%),
it was perceived by students as the least effective method. Problem areas identified by
faculty included lack of guidance with regard to the depth and breadth of content
(31.3%), difficulty linking theory to practice (25%), and lack of instructor knowledge
(18.8%). Only 6.3% of the faculty identified teaching methods as an issue, while most
students evaluated teaching methods to be ineffective. The author suggested that
nurse educators may lack the skills and expertise to use self-directed learning
effectively, and therefore, may be unable to facilitate an adequate knowledge base for
students if the educators themselves do not feel adequately prepared.
In addition to the issue of behavioral versus biological sciences in nursing
education, teaching pharmacology as an integrated rather than separate course has
been a source of controversy, and warrants special comment in this discussion. As
noted previously, nurses and students consistently identify the need and preference
for a separate pharmacology course. On the other hand, most faculty value integration
of pharmacology for consistency of an integrated curriculum and as a measure to
facilitate clinical application. Several studies found that students were actually
exposed to more hours of pharmacology when it was taught as an integrated subject
(Lim & Honey, 2006; Meechan, Mason, & Catling, 2011; Zellner, Boerst, & Semling,
2003). Lim and Honey (2006) described the integration of pharmacology through a
PHARMACOLOGY KNOWLEDGE ACQUISITION 41
three-year undergraduate curriculum, and indicated that students perceived the
material to be more relevant with integration. They also highlighted ways in which
integration supported other content in the curriculum such as legal and ethical issues,
communication, and physiology. Zellner et al. (2003) conducted a nonexperimental
descriptive exploratory study to retrospectively compare integrated and separate
pharmacology. Data was collected from a convenience sample of 299 students
completing a computerized adaptive pharmacology test. The study investigators
found that teaching pharmacology as a separate course did not result in an increase in
test scores.
Ninety percent (90%) of the institutions surveyed in the study by Morrison-
Griffiths et al. (2002) taught pharmacology as an integrated subject in the nursing
curriculum. Even though this is consistent with many other schools of nursing,
shortcomings of integration have also been described. These issues include dilution of
content, inadequacy of addressing the basic pharmacological principles of
pharmacokinetics and pharmacodynamics, inadequate inclusion of the biological
sciences for a true holistic approach, and lack of clear learning objectives specific to
pharmacology (Latter et al., 2001; Manias & Bullock, 2002a; Morrison-Griffiths et
al., 2002; Sulosaari, Suhonen, & Leino-Kilpi, 2011). In the descriptive cross-sectional
study by Dilles et al. (2011), 619 students participated in a correlational survey and
medication testing, which revealed no relationships between pharmacology as a
separate or integrated module and performance on the medication test. Regardless of
whether pharmacology is integrated or offered separately, the literature demonstrates
PHARMACOLOGY KNOWLEDGE ACQUISITION 42
that nurses still do not have adequate pharmacology knowledge. Some study
investigators advocate for both approaches proposing the development of a core
pharmacology module or dedicated pharmacology course in addition to integrated
pharmacology teaching (Morrison-Griffiths et al., 2002).
Summary of Factors Influencing Pharmacology Knowledge Acquisition
Fifteen studies were reviewed in the literature that addressed factors for
pharmacology knowledge acquisition, and all of these studies presented qualitative
descriptive research. Data in the studies was gathered from nurses, graduate nurses,
students, and nursing faculty through various surveys, questionnaires or interviews.
Only one study in the literature directly examined factors that correlate with
pharmacology knowledge. In this study, cumulative GPA and anatomy and
physiology GPA correlated positively with pharmacology grades. Nontraditional
students with family dependence or financial responsibilities were found to perform
at a lower level, and therefore, correlated negatively with pharmacology course
grades.
There is consensus in the literature that a more comprehensive knowledge of
pharmacology is essential for safe clinical practice, and that pharmacology education
may be inadequate or ineffective. There is a mutual perception of inadequate
pharmacology preparation and knowledge by most groups involved - clinical nurses
(both experienced and graduate nurses), students, nurse educators, and researchers.
Several themes emerged in the literature with respect to factors that influence
pharmacology knowledge as perceived by nurses and nursing students. First and
PHARMACOLOGY KNOWLEDGE ACQUISITION 43
foremost, nurses and students believe that inadequate time is devoted to
pharmacology, particularly in consideration of the nurse’s role and amount of hours
spent in clinical practice for medication management. In addition to inadequate time,
lack of clinical opportunities, integration of pharmacology, information overload,
superficial learning strategies, ineffective teaching methods, and the clinical
environment are all cited as factors that negatively influence pharmacology
knowledge acquisition. Students consistently identify that greater opportunities are
needed for medication management during clinical experiences. (Banning, 2003;
Bullock & Manias, 2002; Honey & Lim, 2008; Latter et al., 2001; Page & McKinney,
2007; Sulosaari et. al., 2011). The length of clinical practice experience for nurses
and clinical opportunities for medication decision-making are also frequently noted as
significant factors that impact pharmacology knowledge acquisition.
In addition to the desire for more pharmacology hours, students universally
insist that pharmacology should be taught as a separate course. They also believe that
an excessive emphasis on the behavioral sciences in nursing education contributes to
the lack of a solid foundation in the biological sciences. Other recommendations from
students include the need for more effective teaching strategies, a greater focus on
polypharmacy and drug interactions, and more clinical opportunities for medication
decision-making and application of pharmacology knowledge. The complexity and
pace of the clinical setting, lack of preceptor role modeling, and lack of time are cited
as barriers to clinical application.
PHARMACOLOGY KNOWLEDGE ACQUISITION 44
Many nurse educators agree that inadequate time has been allocated for
pharmacology, yet most faculty believe that students have sufficient pharmacology
knowledge for safe practice (Bullock & Manias, 2002). Faculty further identify that
existing content-laden curricula typically preclude additional time for pharmacology.
Educators emphasize the need for clinical application of pharmacology and therefore,
favor integration as opposed to pharmacology taught as a separate course. Study
investigators suggest, however, that basic pharmacological principles are not being
addressed when pharmacology is integrated, and emphasize the significance of these
principles to promote future consolidation and application of pharmacology
knowledge. Several studies also underscore the need to focus on drug groups or
medication classifications as a means to manage the scope of pharmacological
content and address the issue of information overload.
There is consensus among educators that faculty who teach pharmacology
content should be able to apply the theory component to clinical practice. Teaching
methodologies are cited as factors influencing pharmacology knowledge although to a
lesser degree than other issues that have been described. Educators continue to utilize
lecture as the primary format for teaching, but a variety of teaching strategies have
been described in the literature as a means to promote knowledge and retention of
pharmacology. A final key point in the literature focuses on the need for professional
accountability and self-directed lifelong learning in order for nurses to maintain
adequate knowledge in the wide-ranging and dynamic area of pharmacological
therapies.
PHARMACOLOGY KNOWLEDGE ACQUISITION 45
Researchers frequently conclude that nurses have inadequate pharmacology
knowledge, and the findings of almost all studies have important educational
implications. Studies examining pharmacology curricula identify wide variations in
curriculum design, content, dedicated hours, faculty, teaching strategies, and
assessment of learning. Several authors underscore the lack of clarity regarding
prerequisite pharmacology knowledge for beginning practitioners, and assert the need
for specific outcomes and competencies for pharmacology knowledge. Although
nurse prescribing is not relevant to this study, the literature also highlights the need
for adequate pharmacology knowledge and supplemental education in relation to the
expanding role of nurses in prescribing medications.
Strategies to Enhance Pharmacology Knowledge Acquisition
The need for improved pharmacology education is noted throughout the
literature. Managing the depth and breadth of pharmacology content is challenging,
and even more so in the current fast-paced clinical environment. In a review of
nursing student medication errors, Harding and Petrick (2008) assert, “There is a
paucity of literature specific to nursing education that identifies teaching strategies to
address the complex dynamic system in which students are learning to administer
medications” (p. 44). A number of studies were reviewed that examined general
elements of a nursing program that are believed to enhance pharmacology knowledge,
while other articles offered specific strategies for teaching pharmacology to promote
application and retention of content. The previous section of this chapter discussed
several components of pharmacology education that have been identified as
PHARMACOLOGY KNOWLEDGE ACQUISITION 46
approaches to enhance pharmacology knowledge. This next discussion summarizes
some of the specific strategies for teaching pharmacology that have been used online
or in the classroom.
In evaluating the effectiveness of teaching strategies, it is worthwhile to
discuss an integrative review of the literature completed in 2011 addressing registered
nurses’ medication competence (Sulosaari et al.). The objective of the study was to
describe medication competence, document the need for future studies, and utilize the
results for instrument development. The established areas for medication competence
served as a guideline for content and curricular development in nursing pharmacology
courses. The integrative review followed five stages, and twenty-one studies met the
selection criteria. See Table 2 for eleven competency areas that were determined to
constitute medication competence, and three major categories that integrated these
competencies. The authors concluded that medication competence requires a solid
knowledge base for pharmacology and the ability to apply that knowledge in complex
and dynamic real-life situations (Sulosaari et al., 2011). Furthermore, decision-
making ability was found to be an integral component of both theoretical and practice
competence.
Changes in educational standards in the United Kingdom created the need for
a greater emphasis on theoretical principles of medication management and skills for
clinical reasoning. Banning (2003) developed a generic framework in applied
pharmacology and therapeutics with the intention of providing students with basic
principles and a concrete foundation. She also identified teaching and learning

PHARMACOLOGY KNOWLEDGE ACQUISITION 47
strategies recommending that self-directed teaching strategies be avoided as students
require considerable guidance to comprehend applied pharmacology. A variety of
teaching methods were encouraged including role play, small group discussion,
video-taped vignettes, problem-solving exercises, patient simulation, and review of
clinical scenarios. Banning emphasized the need for a clinical environment that
fosters inquiry, trust, and openness. Furthermore, the environment should eliminate
threat, fear of mistakes, and judgment on performance.
Table 2
Categories and Competency Areas that Establish Medication Competence
Categories of Medication
Competence
Competency Areas for Medication Competence
1. Theoretical Competence
2. Practical Competence
3. Decision-Making
Competence
1. Anatomy and Physiology
2. Pharmacology
3. Communication
4. Interdisciplinary Collaboration
5. Information Seeking
6. Mathematical and Medication
Calculation
7. Medication Administration
8. Medication Education
9. Assessment and Evaluation
10. Documentation
11. Promoting Medication Safety
(Source: Sulosaari, V., Suhonen, R., & Leino-Kilpi, H. (2011). An integrative review
of the literature on registered nurses' medication competence. Journal of Clinical
Nursing, 20 (3-4), 464-478. )
Barry, O’Sullivan, and McCarthy (2015) implemented structured periodic
class review sessions for 89 multidisciplinary students in an undergraduate
PHARMACOLOGY KNOWLEDGE ACQUISITION 48
pharmacology course, and evaluated the efficacy of these sessions through a pre- and
post-review, multiple choice examination. The review sessions were based on various
classroom assessment techniques, where students were asked to identify topics of
difficulty following a lecture. There was a significant increase in student learning
across all disciplines following three review sessions, and 99% of the students
indicated that learning was enhanced.
Eight studies in the literature from 2007 to 2015 were reviewed that described
educational strategies for teaching pharmacology through various technological
innovations. Three studies discussed the use of mobile technologies including
personal digital assistants, mobile phones with text messaging, and smartphones
(Cibulka & Crane-Wilder, 2011; Yeu-Hui & Chiung-Wen, 2013; Wittman-Price,
Kennedy, & Goodwin, 2012). Four studies presented web-based educational
programs or software for basic pharmacology and medication safety (Fidalgo-Neto et
al., 2014; Hewitt, Tower, & Latimer, 2015; Tse & Lo, 2008; Vana & Silva, 2014).
One study evaluated the effectiveness of an audience response system for teaching
pharmacology to baccalaureate students (Vana, Silva, Muzyka, & Hirani, 2011). Of
the eight studies, four were qualitative descriptive studies, two were quasi-
experimental studies, one was experimental, and one was a mixed methods pilot
study. Pre-licensure nursing students comprised the population for seven of the
studies with sample sizes ranging from 8 to 119 students. The one experimental study
included 60 students from various biological and health-related fields. All studies
incorporating pre- and post-testing of pharmacology content identified improved
PHARMACOLOGY KNOWLEDGE ACQUISITION 49
performance in the post-test following implementation of a selected intervention.
Students completing survey questionnaires also provided positive feedback regarding
the technological innovations, and acknowledged enhanced learning of pharmacology
content.
A number of other strategies described by educators to teach pharmacology
include the use of faculty-generated videotapes, high-fidelity simulation, a
collaborative graphic organizer, interprofessional teaching, case studies, interactive
microsimulation, computer-assisted instruction, and a conceptual approach for
teaching psychopharmacology (Bonniver & Magateaux, 2012; Collins, Graves,
Gullette, & Edwards, 2010; Gee, Peterson, Martin, & Reeve, 1998; Jordan, 1997;
Manias, Bullock, & Bennett, 1999; Montenery, 2013; Powell, Canterbury, & McCoy,
1998; Sears, Goldsworthy, & Goodman, 2010; Thompson & Bonnel, 2008). Authors
of these articles indicated effectiveness of the teaching strategy based on qualitative
feedback from students or performance improvement in medication testing.
Summary of Strategies to Enhance Pharmacology Knowledge Acquisition
The literature acknowledges the challenges in teaching pharmacology as a
result of the extent of content and limited time allocated in most curricula. Educators
continuously strive for new and innovative teaching methodologies. Advances in
technology have offered various innovative electronic instruments to facilitate
learning; however, some of these devices are cost-prohibitive, and technology support
for the student is required.
PHARMACOLOGY KNOWLEDGE ACQUISITION 50
The need to supplement traditional lecture with interactive learning strategies
has been emphasized in education as a means to improve student learning, increase
knowledge retention, and apply science to practice. A variety of active learning
strategies for pharmacology have been presented that are similar to strategies utilized
in other areas of nursing education; these include role play, case studies, group
activities, videotaped vignettes, problem-based learning, and simulation. Researchers
and educators agree that even more effective and efficient methodologies are needed.
Current trends emphasize innovative techniques that will promote a more integrated
and efficient curriculum, as well as improve the quality of teaching and student
learning.
Gaps in the Literature
There is an abundance of articles in the literature that document an inadequate
level of pharmacology knowledge for nurses, and the lack of this knowledge as a
factor for medication errors. Several studies also identify the wide variation in
pharmacology curricula across nursing programs, and the fact that the level of
knowledge required by nurses to administer medications safely and monitor their
effects is not well-defined. Numerous authors have also identified various factors that
influence pharmacology knowledge acquisition as perceived by students, nurses, and
faculty. However, only one study was found in the literature that directly evaluated
the relationship between selected variables and pharmacology knowledge acquisition.
Numerous factors are involved in the context of medical errors. While many
medication errors involve novice nurses or a lack of practice experience, distractions
PHARMACOLOGY KNOWLEDGE ACQUISITION 51
and the complex dynamic nature of the clinical environment contribute significantly
to the incidence of errors. At the same time, the literature acknowledges the scarcity
of teaching strategies to address the complex clinical environment in which students
administer medications.
Several studies have presented qualitative descriptive data identifying
perceived problems in nursing education with respect to how pharmacology is taught.
Issues relate to lack of a dedicated pharmacology course, inadequate time devoted to
the subject, lack of clinical opportunities, information overload, and ineffective
teaching strategies. Some research has been completed to compare integrated versus
separate course approaches; however, few studies have addressed information
overload and the lack of clinical opportunities for medication management.
The extent of scientific information students must learn has increased
considerably with advancements in technology and drug discovery; however,
teaching all of the pharmacological facts for each drug is impossible. The
complexities of teaching and learning pharmacology are increasingly significant for
empirical study. Interestingly, several studies have specifically linked pharmacology
course grades or performance on pharmacology standard assessments to NCLEX-RN
success (Emory, 2012; Paraszczuk, 2011; Silvestri, 2010; Ukpabi, 2008). This
information is valuable for identifying students at risk academically. Nevertheless, the
literature research is limited with respect to specific factors that influence
pharmacology knowledge acquisition.
PHARMACOLOGY KNOWLEDGE ACQUISITION 52
Chapter 3: Methodology
The purpose of this study was to examine the relationship of selected
academic and non-academic variables to pharmacology knowledge acquisition by
undergraduate nursing students as demonstrated by performance on a final
standardized pharmacology assessment. A second purpose of the study was to
evaluate the medication administration and decision-making experience as self-
reported by students, and determine if there is any correlation between student
perceptions of opportunities for medication management during clinical experiences,
and performance on the final standardized pharmacology assessment. This chapter
describes the methodology for the research study.
Design
This study was a descriptive correlational design examining relationships
between selected variables and the final pharmacology assessment. Correlational
statistical analyses were used to explore any relationships between the selected
variables and performance on the standardized pharmacology assessment.
Setting
The study was conducted at a private, not-for-profit institution of higher
education located in the Midwestern area of the United States. The institution is a
subsidiary of a teaching hospital and large integrated health care delivery system, and
serves the Tri-State region of Southwestern Ohio, Northern Kentucky, and
Southeastern Indiana. The history of the institution dates to 1896 when the School of
Nursing was originally established; diplomas were granted to the first graduates of the
PHARMACOLOGY KNOWLEDGE ACQUISITION 53
program in 1899. The College transitioned from a diploma program to an associate
degree program, and was re-founded as an independent college in 2001. Three degree
programs were offered at the time of the study, including two nursing programs and
one non-nursing program.
The College admits students twice a year in January and August. Total student
enrollment in the institution averages in the range of 400-450 students. At the time of
the study, there were 332 students in the pre-licensure AASN nursing program; the
remaining students were enrolled in the BSN completion program or the non-nursing
program. Of the 332 students in the pre-licensure AASN nursing program, 232
students were registered in nursing courses; the remaining 100 students were taking
general education courses at the time. The age profile for AASN students during the
spring 2016 semester revealed an average age of 19.3 years and a range of 17-56
years. The College is approved by the Ohio Board of Nursing and Ohio Board of
Regents, and is accredited by the Higher Learning Commission North Central
Association. In 2010, the AASN program was accredited by the National League for
Nursing Accrediting Commission (NLNAC), now the Accreditation Commission for
Education in Nursing (ACEN). The BSN program is accredited by ACEN.
Study Population
The AASN nursing program encompassed four major nursing courses that
included theory and clinical hours, and one non-clinical nursing course focusing on
professional issues. Each clinical nursing course was a pre-requisite for the next
higher level course. Completion of the Nursing IV course (NUR 202) signified the
PHARMACOLOGY KNOWLEDGE ACQUISITION 54
culmination of all clinical experiences in the AASN program. The study required a
sample of students who had finished all of their clinical nursing courses with the
exception of role transition. Role transition clinical hours were excluded because the
ATI Pharmacology Assessment was conducted prior to the role transition rotation.
Therefore, the projected sixty-five students that were enrolled in the ten credit hour
Nursing IV course during the spring 2016 semester comprised the target population
from which the sample was drawn. The majority of these students were taking
Nursing V as a co-requisite, and were within five weeks of graduating from the
program at the time of the pharmacology assessment. Table 3 provides an overview
of the curriculum for the AASN program. While the General Chemistry II course
incorporated basic pharmacological principles and some drug classifications, it should
be noted that a separate pharmacology course did not exist in the curriculum.
All students in the Nursing IV course were required to complete the ATI
standardized pharmacology assessment during week ten of the semester. Five percent
of the course grade was allocated to ATI proctored and non-proctored testing.
Students who met the benchmark of a Level 2 proficiency in the ATI Pharmacology
Assessment received one point of the five potential points. Students who did not meet
the Level 2 proficiency were expected to remediate in the lower performing content
areas. The ATI pharmacology assessment was intentionally scheduled during week
ten rather than at the end of the semester in order for students to identify weak areas
in pharmacology. Students were then able to focus on these areas to prepare for the
PHARMACOLOGY KNOWLEDGE ACQUISITION 55
Nursing IV final course examination conducted at week eleven, and for the ATI RN
Comprehensive Predictor assessment during week thirteen.
Table 3
Associate Degree Nursing Program Curriculum
Course Description
Credits
Required General Education Courses - (37 Credits)
CSP 100 First Semester Experience
BIO 201 Human Anatomy and Physiology I
BIO 202 Human Anatomy and Physiology II
BIO 215 General Microbiology
CHE 101 General Chemistry I
CHE 102 General Chemistry II
ENG 101 English Composition
ETH 212 Health Care Ethics
MTH 103 Pharmacological Mathematics
PSY 103 Introduction to Psychology
PSY 205 Lifespan Development
SOC 103 An Introduction to Sociology
Required Nursing Courses - (36 Credits)
NUR 101 Nursing I - Fundamentals
NUR 102 Nursing II - Adult MS (Chronic Care)
NUR 201 Nursing III - Pediatrics, OB, Community, MS
NUR 202 Nursing IV - Adult MS (Acute Care)
NUR 260 Nursing V - Trends and Professional Issues
1
4
4
4
4
4
3
3
1
3
3
3
6
8
10
10
2
Recruitment
The study investigator reviewed the study with the course faculty and
determined a convenient day and time during class to meet with students. The
investigator introduced the study to all students enrolled in the Nursing IV course
during the tenth week of the semester. A notice for the study was distributed one
PHARMACOLOGY KNOWLEDGE ACQUISITION 56
week in advance to allow students time to contemplate participation and ask
questions. See Appendix A for a copy of the notice distributed to students via e mail
by the course faculty. To encourage participation in the study, time was allotted
during scheduled class hours for students to complete the questionnaires. The purpose
of the study, significance, data collection procedure, time commitment, informed
consent, and expectations of the participants were explained. The study investigator
emphasized that participation in the study was voluntary, and that declining to
participate would not affect any aspect of the remaining semester nor the students’
course grades. The study investigator was explicit that student records would be
reviewed, but that individual names would be removed from all documents.
Furthermore, study findings would be reported only as aggregate data. See Appendix
B for a copy of the script that was used to introduce and describe the study.
It was expected that students would be able to complete the demographic
questions and survey questionnaire within approximately ten minutes. As an
inducement for students to remain for the duration of the class and participate in the
study, refreshments were also provided. Students who did not wish to participate had
the option to leave the class, but were still able to partake of refreshments if desired.
All students who provided informed consent and completed the survey questionnaire
comprised the study sample. It was estimated that 85-90% of the class would
participate in the study since time was allotted to complete the questionnaire during
the regular class session, and minimal time was required. The investigator also
believed that students would be motivated to participate in the study as a result of
PHARMACOLOGY KNOWLEDGE ACQUISITION 57
personal interest in the focus of the research. Considering the magnitude of
pharmacology content, implications for safe practice, and numerous challenges
associated with pharmacology education, the nature of the research topic was highly
relevant for both faculty and students.
Inclusion and Exclusion Criteria.
Inclusion criteria for participants in the study were 1) students enrolled in the
Nursing IV course at week ten of the spring 2016 semester, and 2) students
completing all regular clinical rotations prior to role transition. Students meeting
these criteria were eligible members of the target population for the study sample.
The only exclusion criterion was a student who withdrew from the course prior to
completing the Nursing IV clinical rotation. However, it was not expected that such a
student would be present for the class unless special permission was granted to audit
the remaining semester.
Sample Size Determination.
There are several factors that influence sample size of a study including the
type of study, effect size, the number of variables, the sensitivity of the measurement
methods, and the data analysis techniques. The deciding factor in determining an
adequate sample size for a correlational study is power, and power is the ability to
detect differences or relationships that actually exist in the sample population (Burns
& Grove, 2009). Field (2013) defines power as “the ability of a test to detect an effect
of a particular size, with a value of .8 as a good level to aim for” (p. 881). A power of
.8 means that there is an 80% chance of detecting an effect if one does actually exist
PHARMACOLOGY KNOWLEDGE ACQUISITION 58
(Field, 2013). Effect size may be described as small, medium, or large; a large sample
size is needed for a small effect size or to detect small differences. Small sample sizes
may be used to detect large differences between groups.
Pearson’s product-moment correlation coefficient was utilized to explore
relationships between the selected variables and performance on the standardized
pharmacology assessment. When using Pearson’s correlation coefficient, the values
for the effect sizes are .10 for a small effect, .30 for a medium effect, and .50 for a
large effect (Field, 2013). Although other statistical analyses were also used in the
study, Pearson’s correlation analysis took priority as a parametric test. Parametric
testing is more sensitive to violations of statistical assumptions and therefore,
provides more robust data.
A power analysis allows the determination of a sample size needed to obtain
sufficient power and determination of the risk of a type II error. The investigator ran a
priori power analysis in G*Power with a medium effect size, alpha of .05, and beta of
.20 for a power of .80; this was based on using Pearson’s correlation two-tailed power
analysis. In order to arrive at .80 power and a medium effect size of .30 with an alpha
of .05 and beta of .20, the minimum sample size needed is 82 participants. A target
population of 65 pre-licensure nursing students was anticipated, and the investigator
expected 85-90% participation in the study. Participation by 85-90% of the class
would provide a sample of 55-59 students; even with 100% participation of the class,
the desired sample size cannot be met since the target population is limited.
Therefore, the investigator re-ran the power analysis based on the actual number of
PHARMACOLOGY KNOWLEDGE ACQUISITION 59
students who participated in the study, and then reported the effect size that could be
obtained. When solving for effect size rather than sample size, there was power to
detect up to an effect size of .35 with a sample of 60 participants, and up to .36 with a
sample of 58 participants; these were both slightly larger than a medium effect size.
Measurements
ATI RN Pharmacology Assessment.
The comprehensive assessment and review program offered by ATI provides
remediation and assessment activities to assist students throughout a nursing program.
ATI acknowledges a relationship with 2100 colleges and universities nationwide that
utilize the company’s products (Emory, 2012). The outcome and dependent variable
for the study was pharmacology knowledge acquisition as measured by the ATI 2013
RN Proctored Pharmacology Assessment. This assessment is incorporated in the ATI
2013 RN Content Mastery Series (CMS), and is a 70-item examination, which
provides an appraisal of a student’s basic comprehension and mastery of
pharmacologic principles (ATI, 2015a). Ten of the seventy items in the examination
are pilot questions and are not considered when calculating the test score.
Consequently, there are a total of sixty questions which determine the final test score
and resulting level proficiency. Students are allotted 70 minutes to complete the
examination. Table 4 provides a listing of concepts and content areas evaluated in the
ATI RN Proctored Pharmacology Assessment.
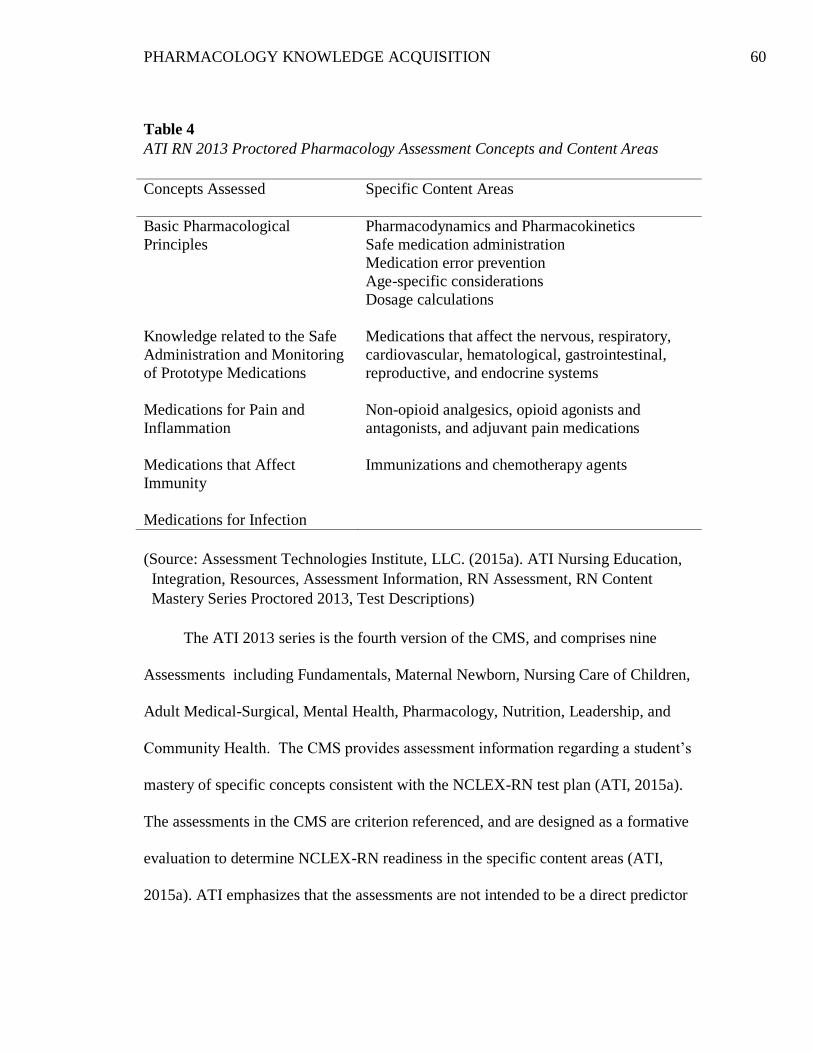
PHARMACOLOGY KNOWLEDGE ACQUISITION 60
Table 4
ATI RN 2013 Proctored Pharmacology Assessment Concepts and Content Areas
Concepts Assessed
Specific Content Areas
Basic Pharmacological
Principles
Knowledge related to the Safe
Administration and Monitoring
of Prototype Medications
Medications for Pain and
Inflammation
Medications that Affect
Immunity
Medications for Infection
Pharmacodynamics and Pharmacokinetics
Safe medication administration
Medication error prevention
Age-specific considerations
Dosage calculations
Medications that affect the nervous, respiratory,
cardiovascular, hematological, gastrointestinal,
reproductive, and endocrine systems
Non-opioid analgesics, opioid agonists and
antagonists, and adjuvant pain medications
Immunizations and chemotherapy agents
(Source: Assessment Technologies Institute, LLC. (2015a). ATI Nursing Education,
Integration, Resources, Assessment Information, RN Assessment, RN Content
Mastery Series Proctored 2013, Test Descriptions)
The ATI 2013 series is the fourth version of the CMS, and comprises nine
Assessments including Fundamentals, Maternal Newborn, Nursing Care of Children,
Adult Medical-Surgical, Mental Health, Pharmacology, Nutrition, Leadership, and
Community Health. The CMS provides assessment information regarding a student’s
mastery of specific concepts consistent with the NCLEX-RN test plan (ATI, 2015a).
The assessments in the CMS are criterion referenced, and are designed as a formative
evaluation to determine NCLEX-RN readiness in the specific content areas (ATI,
2015a). ATI emphasizes that the assessments are not intended to be a direct predictor
PHARMACOLOGY KNOWLEDGE ACQUISITION 61
of NCLEX-RN performance or future success in nursing, but rather determine the
level of proficiency the student has attained. In relation to Bloom’s taxonomy of the
cognitive domain, questions in the content-specific assessments and comprehensive
predictor tests are written at the application level or above. The intended testing
population for the RN CMS 2013 are students who are at or near completion of a
course in a selected content area (ATI, 2015a). The ATI content-specific assessments
are also designed to guide remediation efforts based on exam performance. A variety
of tools to measure academic performance enable educators to identify problem areas
early and intervene to promote student success.
ATI developed a set of recommended cut scores based on standards
established by the National Council on Measurement in Education (NCME); nursing
schools could choose to adopt these scores as benchmarks for student performance on
each of the nine RN CMS 2013 assessments (ATI, 2015a). Content expert judges
were selected to participate in a study to determine the criterion-referenced cut scores;
these judges were nurse educators from various RN programs across the United
States, typically with at least ten years of experience in teaching the content area. The
cut scores were established through a formal study in accordance with the
recommendations of the NCME standards (ATI, 2015a).
The college in the study setting utilized the recommended Level 2 proficiency
as a benchmark for all proctored ATI assessments. The recommended cut score by
ATI for the Pharmacology Assessment for a Level 2 proficiency is 71.7%-83.3%
(ATI, 2015a). The faculty rounded the low end of the range value from 71.7% to 72%
PHARMACOLOGY KNOWLEDGE ACQUISITION 62
for consistency with all ATI assessments in the Nursing IV course. It should be noted
that gaps in percentage values between the level scores reflect only a one-item
difference, and values between these percentages for each cut score are not possible
(ATI, 2015a). ATI defines the Level 2 proficiency as a performance level whereby
the student is expected to readily meet NCLEX-RN standards in the content area. ATI
clarifies that the definitions for the CMS proficiency levels are based on the expertise
of nurse educators participating in the cut score study, rather than on any empirical
research relating NCLEX-RN performance to performance on the CMS or to actual
job performance (ATI, 2015b). Table 5 identifies the ATI recommended cut score
ranges for the Pharmacology Assessment, and describes the levels of proficiency.
The ATI RN Content Mastery Series 2013 Technical Manual (2015b) presents
a comprehensive report which analyzes data from the pilot study including the first
attempt scores of examinees who completed any CMS 2013 assessment between
September 17, 2013 and April 19, 2014 (ATI, 2015b). There were 7,066 examinees
who completed the Pharmacology Assessment from October 18, 2013 through April
19, 2014 (ATI, 2015b). The findings in the technical manual report provide evidence
to support the reliability and validity of the RN CMS 2013 scores. Validity evidence
is discussed in the report, including research to support content validity and measures
to investigate construct-irrelevant variance (ATI, 2015b). In particular, analyses were
conducted to verify that test “speededness” was not a significant source of construct-
irrelevant variance. Test speededness involves the examination of the degree to which
scores include a speed component for a test that has a time limit (ATI, 2015b).
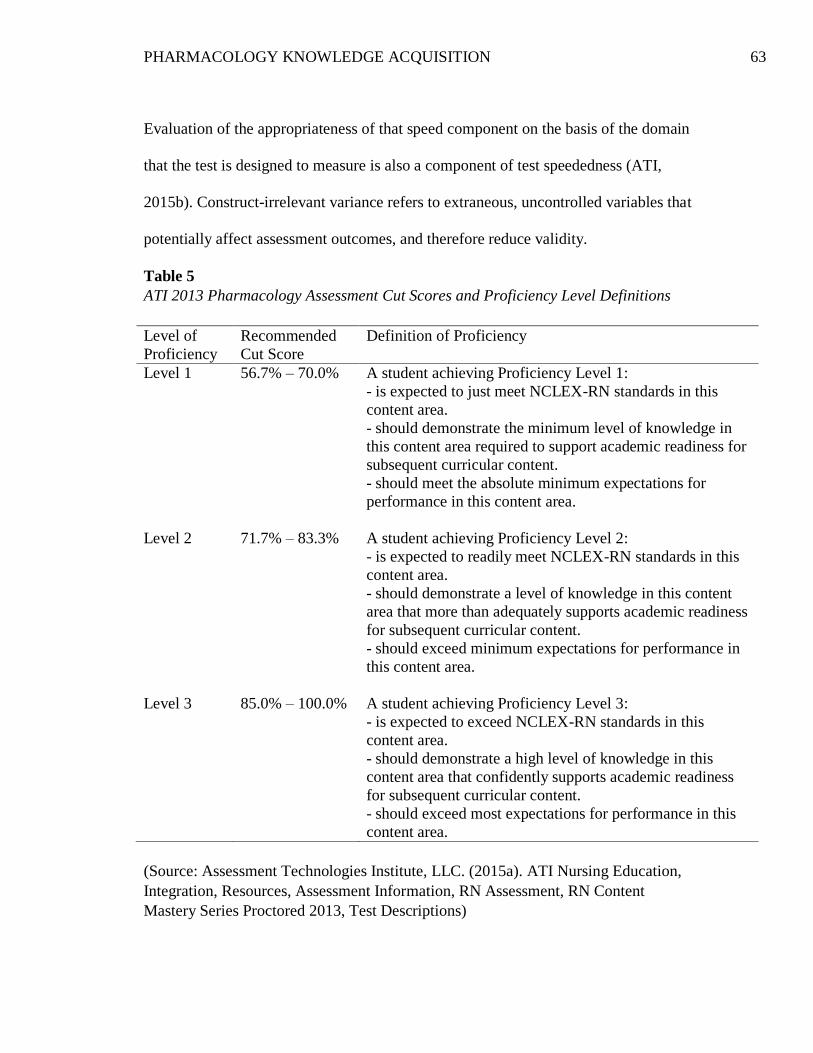
PHARMACOLOGY KNOWLEDGE ACQUISITION 63
Evaluation of the appropriateness of that speed component on the basis of the domain
that the test is designed to measure is also a component of test speededness (ATI,
2015b). Construct-irrelevant variance refers to extraneous, uncontrolled variables that
potentially affect assessment outcomes, and therefore reduce validity.
Table 5
ATI 2013 Pharmacology Assessment Cut Scores and Proficiency Level Definitions
Level of
Proficiency
Recommended
Cut Score
Definition of Proficiency
Level 1
Level 2
Level 3
56.7% – 70.0%
71.7% – 83.3%
85.0% – 100.0%
A student achieving Proficiency Level 1:
- is expected to just meet NCLEX-RN standards in this
content area.
- should demonstrate the minimum level of knowledge in
this content area required to support academic readiness for
subsequent curricular content.
- should meet the absolute minimum expectations for
performance in this content area.
A student achieving Proficiency Level 2:
- is expected to readily meet NCLEX-RN standards in this
content area.
- should demonstrate a level of knowledge in this content
area that more than adequately supports academic readiness
for subsequent curricular content.
- should exceed minimum expectations for performance in
this content area.
A student achieving Proficiency Level 3:
- is expected to exceed NCLEX-RN standards in this
content area.
- should demonstrate a high level of knowledge in this
content area that confidently supports academic readiness
for subsequent curricular content.
- should exceed most expectations for performance in this
content area.
(Source: Assessment Technologies Institute, LLC. (2015a). ATI Nursing Education,
Integration, Resources, Assessment Information, RN Assessment, RN Content
Mastery Series Proctored 2013, Test Descriptions)
PHARMACOLOGY KNOWLEDGE ACQUISITION 64
Standard 4.10 of the ATI RN Content Mastery Series 2013 Technical Manual
(2015b) specifically addresses the reliability and validity of the ATI tests. Following
the release of an assessment for use, ATI conducted additional analyses of the test
data with students taking the assessments for the first time. Table 6 presents the test
statistics, including the reliability coefficient, for scores on the pharmacology
assessments. The distribution of item difficulty (p-value) and discrimination (point
biserial correlation) were also presented in the report. The mean p values for the nine
RN CMS 2013 assessments ranged from 0.62 to 0.72, and the mean discrimination
values ranged from 0.22 to 0.28; ATI indicates that these values fall within ranges
which contribute to the overall range of scores and delineate between low and high
ability examinees (ATI, 2015b). Test items were evaluated by expert nurses and
scored according to established criteria, and cultural bias was addressed by ethnic and
gender experts. Reports presented by the scientists and psychometricians at ATI
conclude that reliability and validity of the content-specific assessments has been
established with respect to the intended use and purpose of the test.
Following administration of any content-specific assessment, students receive
a report which provides an overall raw percentage of correct items and a norm-
referenced percentile ranking. This percentile compares each student’s score to the
scores of all students in registered nursing programs nationally, and to all students
completing the assessment who are enrolled in a comparable program.
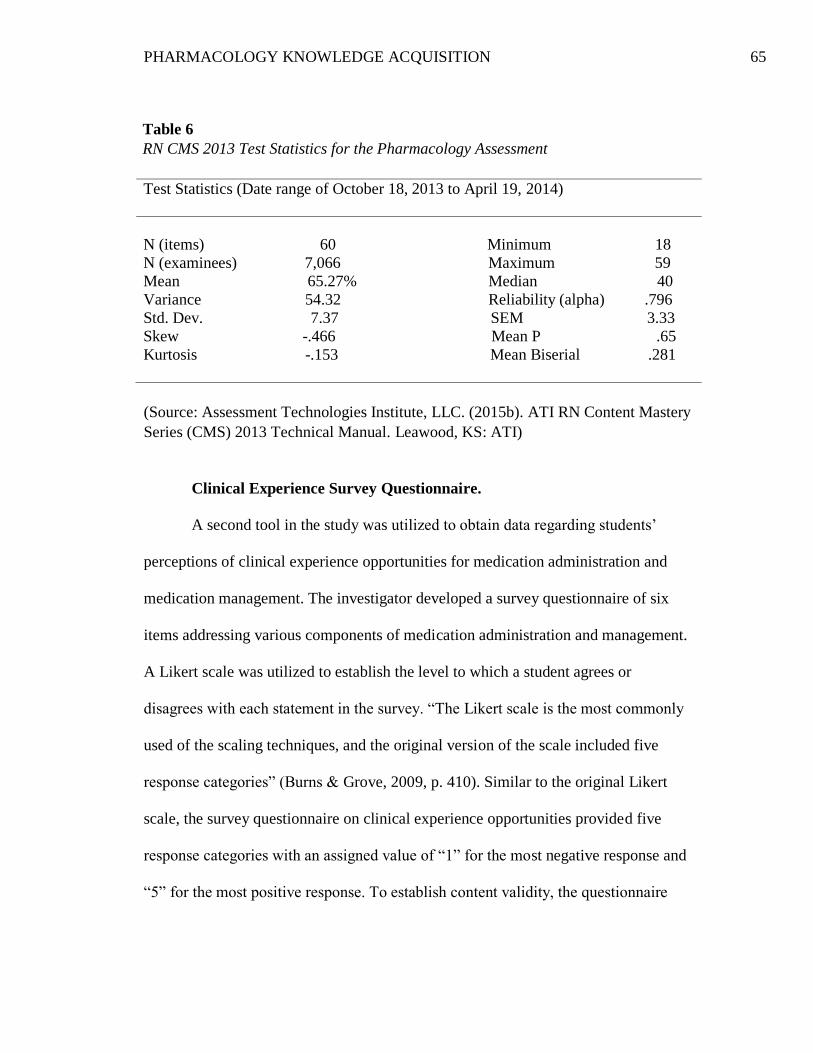
PHARMACOLOGY KNOWLEDGE ACQUISITION 65
Table 6
RN CMS 2013 Test Statistics for the Pharmacology Assessment
Test Statistics (Date range of October 18, 2013 to April 19, 2014)
N (items) 60 Minimum 18
N (examinees) 7,066 Maximum 59
Mean 65.27% Median 40
Variance 54.32 Reliability (alpha) .796
Std. Dev. 7.37 SEM 3.33
Skew -.466 Mean P .65
Kurtosis -.153 Mean Biserial .281
(Source: Assessment Technologies Institute, LLC. (2015b). ATI RN Content Mastery
Series (CMS) 2013 Technical Manual. Leawood, KS: ATI)
Clinical Experience Survey Questionnaire.
A second tool in the study was utilized to obtain data regarding students’
perceptions of clinical experience opportunities for medication administration and
medication management. The investigator developed a survey questionnaire of six
items addressing various components of medication administration and management.
A Likert scale was utilized to establish the level to which a student agrees or
disagrees with each statement in the survey. “The Likert scale is the most commonly
used of the scaling techniques, and the original version of the scale included five
response categories” (Burns & Grove, 2009, p. 410). Similar to the original Likert
scale, the survey questionnaire on clinical experience opportunities provided five
response categories with an assigned value of “1” for the most negative response and
“5” for the most positive response. To establish content validity, the questionnaire
PHARMACOLOGY KNOWLEDGE ACQUISITION 66
was distributed to six graduate nurses and six faculty members in the college.
Graduate nurses were defined as nurses with less than one year experience. None of
the individuals participating in the review of the survey tool were involved with the
study. Reviewers were asked to answer specific questions, as well as rate the
importance of each survey statement to the purpose of the study and the survey tool.
See Appendix C for a copy of the original tool and questions completed by the
reviewers.
The survey evaluations were returned by three graduate nurses and five
faculty members. Suggestions for change were identified, as well as
recommendations for additional statements. One hundred percent of the survey
statements were perceived as moderately essential or highly essential to the study.
The survey questionnaire was revised based upon feedback from the reviewers, and
was then distributed to three individuals a second time for re-evaluation of content
and terminology. See Appendix D for the final revised survey questionnaire.
Demographic Information Form
Selected variables and demographic data in the study were collected through
admission and academic records; however, three variables required direct feedback
from participants in addition to the clinical experience survey questionnaire. These
non-academic variables included previous health care experience, working hours per
week, and family responsibilities. A third form was utilized to collect this data, and
each variable was explained on the form in accordance with its conceptual definition.
See Appendix E for the demographic information form.
PHARMACOLOGY KNOWLEDGE ACQUISITION 67
Data Collection Procedure
The study investigator discussed and secured permission for the study from
the President of the College, the Dean of Academic Affairs, and the Dean of
Enrollment Management. The data collection process was initiated upon approval by
the Institutional Review Board (IRB) of both the integrated health care organization
affiliated with the college and Case Western Reserve University. Three sets of
individual data were collected. The first set of data was obtained through college
admission and registration records following IRB approval and consent by individual
students. SONISWEB was the data administration system of the college, which
allowed faculty access to grade point averages, admissions, registration, financial aid,
billing, alumni, and fundraising information.
The study investigator met with the Dean of Enrollment Management and the
Registrar who confirmed access to reports that provided data for demographics and
for the selected variables of the study. The demographic information obtained from
these reports included age, gender, and race or ethnicity. Gender is defined as male or
female, and age was presented as specific age in years. School districts and states are
required to follow federal standards for categorizing race and ethnicity for students
and staff; these standards are commonly used for data collection. Race and ethnicity
were defined according to the following federal categories: American Indian or
Alaska Native, Asian, Black or African American, Native Hawaiian, Hispanic or
Latino, and White (U.S. Office of Management and Budget, 1997). Additional data
retrieved from college records for other selected variables included nursing GPA,
PHARMACOLOGY KNOWLEDGE ACQUISITION 68
science GPA, and previous college credit or degrees. The study investigator obtained
the reports from the Registrar upon IRB approval and student consent to participate.
A second set of data was collected directly from the participants. This data
included the non-academic variables of previous health care experience, working
hours per week, family responsibilities, and student self-perceived opportunities for
medication management during clinical experiences. Participants in the study were
asked to complete the investigator-developed survey questionnaire and the
demographic information form following introduction of the study. A third set of data
was collected from the computerized testing report generated by ATI for the
proctored pharmacology assessment; this data only included the one dependent
variable of the student’s pharmacology test score.
The study investigator prepared and distributed a packet which included a
consent form, the demographic information form, and the clinical experience survey
questionnaire. Each packet and set of documents was assigned a code number. A
student identification number assigned by the registrar’s office upon entry to the
program was recorded by the student on the survey questionnaire and demographic
information form. Although specific student names would not be identified on any
documents, it was, in fact, possible to connect data to a specific student. The college-
generated identification number was necessary, however, in order to match
demographic and survey information with the corresponding ATI standardized
pharmacology assessment. Therefore, students also needed to provide informed
PHARMACOLOGY KNOWLEDGE ACQUISITION 69
consent. The written consent form was developed in accordance with IRB guidelines
and requirements of the institution.
Data Management
When all students completed the informed consent and survey questionnaire,
the documents were collected by the study investigator and maintained in a locked
file cabinet in the investigator’s office. After data was collected from academic
records, the survey questionnaire, and the assessment report from the testing
company’s password-protected electronic database, a study enrollment log was
created using Microsoft Excel. This log included the study code number, student
names, the college identification number, and demographic information.
The data was prepared for computer entry by first examining all demographic and
survey questionnaires for missing data or inaccurately recorded responses. A
computerized database was created to collect demographic information, information
for the six independent study variables, and performance on the ATI Pharmacology
Assessment. Data entry was completed using Statistical Package for the Social
Sciences (SPSS), Version 23. Both the study enrollment log and the data file in SPSS
were secured in an electronic password-protected and encrypted computer database
by the investigator.
Once the data file was created and score reports matched with the participants,
student identification numbers were removed from the data file prior to analysis. In
this way, it was not possible to connect specific data results to any participants in the
study. Only the code number assigned by the investigator was identified in order to
PHARMACOLOGY KNOWLEDGE ACQUISITION 70
maintain confidentiality, and study results were reported as aggregate data. All study
documents were boxed and submitted to the Research Council liaison to be
maintained in an IRB-designated storage area for a period of ten years. This was a
requirement of the institutional IRB.
A systematic plan for data entry was established, which served to reduce
errors and minimize interruptions during the data entry process (Burns & Grove,
2009). The labeling and organization of fields for data entry or development of a
codebook in SPSS was constructed prior to the data entry. The codebook identified
the range of possible numerical values entered in the entire computer file, and defined
each variable. Once data was entered, the data file was printed and crosschecked for
accuracy with the original data documents. An exploratory analysis was conducted to
identify any missing values and outliers, and to determine if the data was skewed or
normally distributed. There were no missing fields for essential data points and
therefore, no participants were excluded from the study.
Upon completion of data entry and cleaning, the original data was returned to
a locked cabinet in the investigators office. The data file was backed up automatically
by the institutional network on a daily basis. Computer printouts of the statistical
analysis were systematically stored by time sequence to facilitate easy access at a
later time.
Statistical Analysis
The sample population was comprised of pre-licensure nursing students in an
Associate Degree program who were enrolled in Nursing IV (NUR 202), the terminal
PHARMACOLOGY KNOWLEDGE ACQUISITION 71
clinical nursing course of the curriculum. Approximately 65 students were enrolled in
the Nursing IV course during the spring 2016 semester, and the anticipated sample
size was 55-59 participants. The demographics of the sample population were
analyzed using descriptive statistics; these variables included age, gender, and
ethnicity. Age, a continuous variable, was described by three measures of central
tendency (mean, median and mode), two measures of dispersion (range and standard
deviation), and one measure of distribution (skewness). Gender and ethnicity
reflected categorical data and were presented with frequencies. The data analysis plan
was presented for each individual research question in the study.
Research Question 1: What is the level of performance for the study group on
the final ATI standardized pharmacology assessment? The data analyzed for this
question were the specific scores that students achieved on the ATI Pharmacology
Assessment and therefore, were continuous data. Continuous variables are variables
that provide a score for each individual and can take on any value on the
measurement scale that is being used (Field, 2013). Specifically, the scores on the
ATI Pharmacology Assessment reflected interval data because there were equal
distances or differences between intervals on the scale of test scores. As continuous
data, a descriptive analysis was completed for measures of centrality and measures of
dispersion. The mean, median, mode, standard deviation, variance, and range were
reported for the test scores for the sample. A second analysis was completed by
categorizing the scores into two groups, students who met the benchmark and
students who did not meet the benchmark, using the level 2 proficiency score of 72%
PHARMACOLOGY KNOWLEDGE ACQUISITION 72
as the cutoff. This secondary analysis was done in the event that the statistical
assumptions of Pearson’s correlation coefficient could not be met. For example, the
data may not have been normally distributed, or the data may have been skewed to
one end or another. Burns and Grove (2009) identify the assumptions of Pearson’s
correlation are as follows: (a) interval measurement of both the independent and
dependent variables, (b) normal distribution of at least one variable, (c) independence
of observational pairs, and (d) homoscedasticity which is defined as data that “are
evenly dispersed above and below the regression line, which indicates a linear
relationship on a scatter diagram (plot)” (p. 479). If the assumptions of Pearson’s
correlation coefficient could not be met, non-parametric testing would have been used
to analyze the data. Non-parametric tests do not rely on the restrictive assumptions of
parametric tests; in particular, it is not assumed that the sample is normally distributed
(Field, 2013). As categorical data, the level of performance was presented by
frequencies.
Research Question 2: What is the bivariate relationship between certain
academic variables (nursing grade point average and science grade point average)
and non-academic variables (previous college credit or degree, previous health care
experience, working hours per week, and family responsibilities) and performance on
the final ATI standardized pharmacology assessment? The academic variables of
nursing GPA, science GPA, and working hours per week were continuous data, and
presented by the measures of centrality. The non-academic variables of previous
college credit, health care experience, and family responsibilities were dichotomous
PHARMACOLOGY KNOWLEDGE ACQUISITION 73
variables defined by a “Yes” or “No” answer; this data was described with
frequencies. For example, participants were asked to answer “Yes” or “No” if they
had received any credit for college courses prior to acceptance to the college. Health
care experience was defined as any current or previous work experience related to
direct patient care in a health care setting to which respondents also answered either
“Yes” or “No. When exploring family responsibilities, participants answered “Yes” if
they have assumed financial responsibility as head of household, responsibility for
dependent children, or responsibility as a caregiver during their enrollment in the
Associate Degree program.
Bivariate correlation analyses determine the direction and strength of the
relationship between two variables in a single sample, and a correlation is used when
two variables are continuous (Burns & Grove, 2009). Pearson’s correlation
coefficient examines interval data, which requires that data has equal intervals,
mutually exclusive categories, and exhaustive categories. The academic variables of
nursing GPA, science GPA, and working hours per week were continuous interval
data. The outcome variable of the ATI Pharmacology Assessment test score also
reflected continuous interval data. Therefore, Pearson’s correlation coefficient was
used to evaluate for any relationships between these independent continuous variables
and test performance.
The Chi square test is used when the independent predictor variable is
categorical or dichotomous and the dependent outcome variable is also categorical. If
performance on the ATI Pharmacology Assessment was required to be analyzed as
PHARMACOLOGY KNOWLEDGE ACQUISITION 74
categorical data, meaning that the student either met the 72% benchmark or did not
meet the benchmark, the Chi square test was to be utilized. There were three non-
academic dichotomous variables and therefore, three 2 x 2 contingency tables would
be presented showing the relationship between each of the three independent
variables and the one outcome variable. The three non-academic dichotomous
variables could also be treated as continuous variables because each of them has a
meaningful mean. For example, if the sample size is 60 and 30 participants answer
“Yes” to family responsibilities, 50% of participants have family responsibilities and
the mean for family responsibilities is .50. Therefore, Pearson’s biserial correlation
coefficient would also be used to analyze the three dichotomous variables if scores on
the ATI Pharmacology Assessment were presented as continuous data.
Research Question 3: What is the bivariate relationship between students’
self-reported perceived clinical experiences in medication management and
performance on the final ATI standardized pharmacology assessment? Students’ self-
reported perceived clinical experiences for medication management presented
continuous ordinal data that was obtained through a survey questionnaire. Students
were required to respond to specific statements about clinical experience
opportunities that were evaluated with a Likert scale. The scale ranged from
“Strongly Disagree” (a value of 1) to “Strongly Agree” (a value of 5). A positive
evaluation of clinical experiences was reflected by a higher score number for each of
the survey statements. The data was ordinal because the intervals between the ranked
categories were not equal; however, since there were more than four items in the
PHARMACOLOGY KNOWLEDGE ACQUISITION 75
questionnaire, the data was able to be powered up to interval data. Interval data
allows the magnitude of an attribute to be identified more precisely and therefore, is
considered to be more useful than ordinal data (Burns & Grove, 2009; Field, 2013).
Additionally, many statistical tests rely on having data measured at the interval level
including Pearson’s product-moment correlation; this correlational analysis was used
to answer the Research Question 3. The average score for each statement in the
survey was reported, and each statement was analyzed for any significant relationship
to performance on the ATI Pharmacology Assessment.
The study encompassed an item-level survey analysis and statistical analyses
requiring multiple correlations. Both of these circumstances may compound the error
factor or increase the probability of making a Type I error. This is sometimes referred
to as a “galloping alpha”, whereby statistically significant results simply occur by
accident when multiple correlations are performed. In order to compensate for the
number of tests that were run on the same data, the alpha was adjusted to a 0.04 level.
Trends were established at the .05 level, but statistical significance was only reported
at the .04 level.
Protection of Human Subjects
Researchers have an ethical responsibility to protect the rights of human
research subjects. The human rights that require protection include the right to self-
determination, the right to privacy, the right to anonymity and confidentiality, the
right to fair treatment, and the right to protection from discomfort and harm
(American Nurses Association and American Psychological Association as cited in
PHARMACOLOGY KNOWLEDGE ACQUISITION 76
Burns & Grove, 2009). The right to self-determination is based on respect for human
subjects and freedom to participate or not participate in research.
A number of steps were taken to ensure the protection of human subjects. First
and foremost, approval for the research study was obtained through the institutional
review boards of the health care organization affiliated with the college, and Case
Western Reserve University. These approvals were acquired prior to introducing the
study or any data collection. Second, no coercion was employed to achieve
participation. As identified previously, the study investigator emphasized that
participation in the study was voluntary, and that declining to participate carried no
consequences for the student. The investigator clarified that student grades,
progression to role transition, and graduation from the program would not be affected
in any way. The study investigator was not involved in teaching the Nursing IV
course during the spring 2016 semester, and therefore, did not know the students nor
was affiliated with the course in any way. Consequently, any student concerns
regarding a negative relationship with course faculty as a result of not participating
was avoided. Furthermore, there were no excessive rewards being offered that would
constitute undue influence for participation in the study. Finally, the investigator for
the study completed the Collaborative Institutional Training Initiative (CITI)
education as a requirement for the NUND 541 course, Practice-Focused Research II;
this certification was a requirement for human subjects’ research and was also
mandated by the affiliated health care organization’s IRB. The CITI Program mission
statement reads: "To promote the public's trust in the research enterprise by
PHARMACOLOGY KNOWLEDGE ACQUISITION 77
providing high quality, peer reviewed, web based, research education materials to
enhance the integrity and professionalism of investigators and staff conducting
research” (CITI, 2015).
A student identification number assigned by the registrar’s office was utilized
to determine demographic information and relationships between selected variables
and performance on the ATI RN Proctored Pharmacology Assessment.
Confidentiality was maintained as all data collected in the study were analyzed and
reported in aggregate form. Furthermore, all survey questionnaires, data collection
records, statistical analyses, and study results were maintained in a secure locked
cabinet in the investigator’s office, and any document with student identification
numbers was destroyed once the data file was created.
All students in the Nursing IV course were at least 18 years of age and were
informed regarding the research study and their rights as a participant. The
completion of a survey questionnaire presented no risk of harm to participants;
however, informed consent was obtained since student records were reviewed, and it
would be possible to link data to individual students through the college-generated
identification number.
All students in the Nursing IV course were eligible to participate, thereby
supporting fair selection. No potential participants in the study were considered to
have diminished autonomy. The nature of the study precluded concern regarding
freedom from discomfort or harm for human subjects as students were only
completing a demographic form and survey questionnaire. No treatment or
PHARMACOLOGY KNOWLEDGE ACQUISITION 78
intervention was implemented, and there were no physical, emotional, or social risks
involved for participants in the study. However, it was possible that some students
would be uncomfortable with a faculty member outside of the course reviewing
personal grades and test scores. Exposure to the research process might have been
considered a benefit to those students participating in the study, but any benefits with
respect to changes in the curriculum to improve pharmacology education would only
be applicable to future students in the program.
PHARMACOLOGY KNOWLEDGE ACQUISITION 79
Chapter 4: Data Analysis
This study was conducted to examine the relationship of selected academic
and non-academic variables in undergraduate nursing students’ acquisition of
pharmacology knowledge as demonstrated by performance on a final standardized
pharmacology assessment. The study also sought to evaluate the medication
administration and decision-making experience as self-reported by students, and
determine any correlation between student perceptions of clinical experience
opportunities for medication management, and performance on the final
pharmacology assessment. Chapter four presents the demographics of participants,
the descriptive statistics for seven independent study variables, the descriptive
statistics for one dependent outcome variable, and the results of the correlational
analyses conducted in the study.
Sample Demographics
Pre-licensure nursing students enrolled in the final clinical nursing course of
an AASN program during the spring 2016 semester comprised the target population
from which the sample for the study was drawn. Fifty-six students were present for
class when the research study was introduced; of these 56 students, 54 students
(96.4%) participated in the study. The demographic information for the study sample
was collected through school admission and registration records in SONISWEB, the
data administration system of the college. Reports from SONISWEB for demographic
data and selected variables were generated by the college Registrar. A data file was
created using SPSS software, and all information was entered by the study
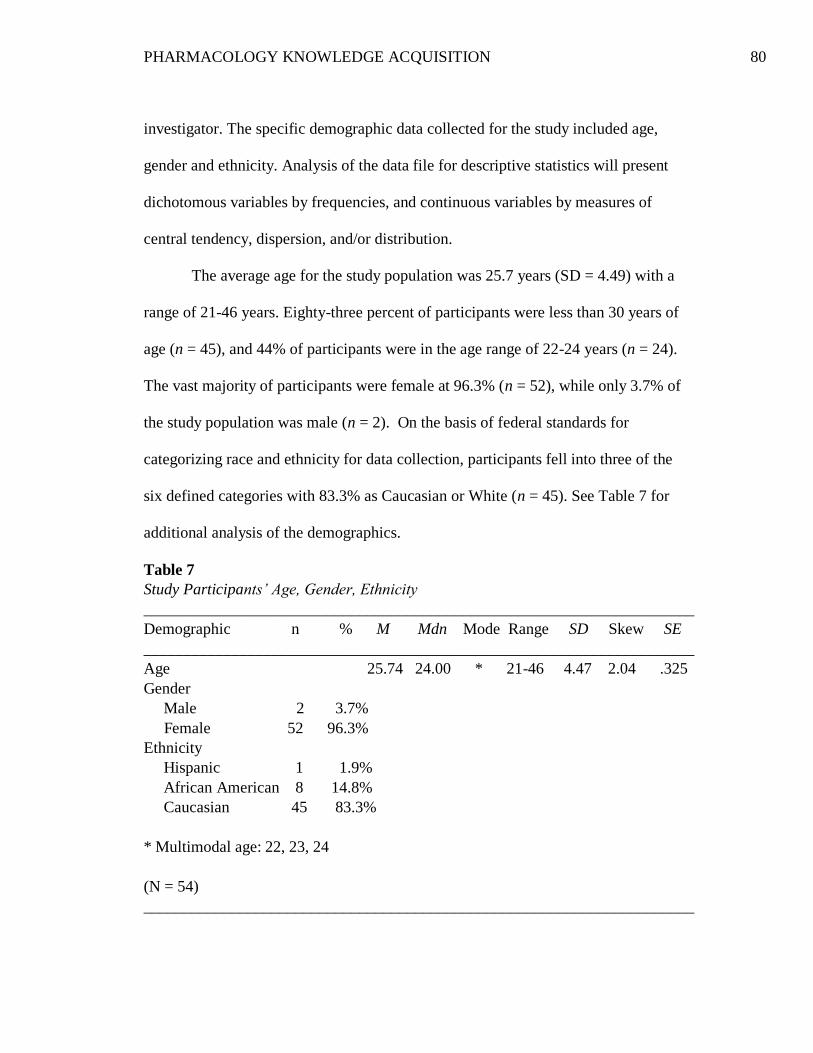
PHARMACOLOGY KNOWLEDGE ACQUISITION 80
investigator. The specific demographic data collected for the study included age,
gender and ethnicity. Analysis of the data file for descriptive statistics will present
dichotomous variables by frequencies, and continuous variables by measures of
central tendency, dispersion, and/or distribution.
The average age for the study population was 25.7 years (SD = 4.49) with a
range of 21-46 years. Eighty-three percent of participants were less than 30 years of
age (n = 45), and 44% of participants were in the age range of 22-24 years (n = 24).
The vast majority of participants were female at 96.3% (n = 52), while only 3.7% of
the study population was male (n = 2). On the basis of federal standards for
categorizing race and ethnicity for data collection, participants fell into three of the
six defined categories with 83.3% as Caucasian or White (n = 45). See Table 7 for
additional analysis of the demographics.
Table 7
Study Participants’ Age, Gender, Ethnicity
_____________________________________________________________________
Demographic n % M Mdn Mode Range SD Skew SE
_____________________________________________________________________
Age 25.74 24.00 * 21-46 4.47 2.04 .325
Gender
Male 2 3.7%
Female 52 96.3%
Ethnicity
Hispanic 1 1.9%
African American 8 14.8%
Caucasian 45 83.3%
* Multimodal age: 22, 23, 24
(N = 54)
_____________________________________________________________________
PHARMACOLOGY KNOWLEDGE ACQUISITION 81
Analyses of Research Questions
Analysis of the study data for each research question was also completed
through Statistical Package for the Social Sciences (SPSS), version 23. Pearson’s
product-moment correlation coefficient and Pearson’s biserial correlation were
utilized to explore the relationships between the selected variables and test scores on
the pharmacology assessment. The significance level for the correlational analyses in
the study was adjusted to 0.04 as previously identified in order to compensate for the
use of an item-level survey, and for the series of bivariate correlations required for the
analysis.
The assumptions of Pearson’s correlation were met as demonstrated by the
normal distribution of data and no evidence of nonlinearity. The Scatter Plots in
Figure 2 indicate a linear relationship between the continuous independent variables
and ATI pharmacology assessment scores. While the linear relationship is less
obvious in Scatter Plots b and c as a result of the weak correlation for these variables,
none of the Scatter plots revealed a curvilinear presentation, which would be a
concern with Pearson’s correlation.
Research Question 1. What is the level of performance for the study group on
the final ATI standardized pharmacology assessment? Since the assumptions of
Pearson’s correlation were met, the analysis for performance on the ATI
pharmacology assessment was completed using the ATI scores as continuous data.
Therefore, it was not necessary to categorize the scores into two groups, students who
met the benchmark and students who did not meet the benchmark, in order to
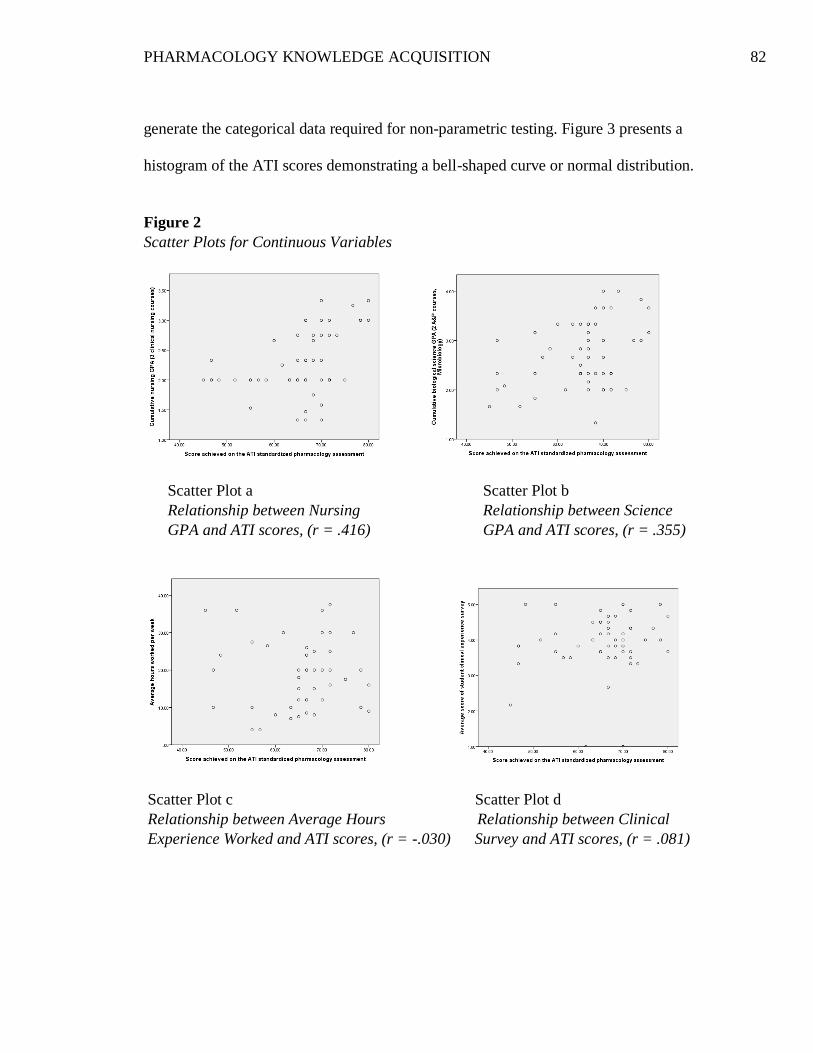
PHARMACOLOGY KNOWLEDGE ACQUISITION 82
generate the categorical data required for non-parametric testing. Figure 3 presents a
histogram of the ATI scores demonstrating a bell-shaped curve or normal distribution.
Figure 2
Scatter Plots for Continuous Variables
Scatter Plot a Scatter Plot b
Relationship between Nursing Relationship between Science
GPA and ATI scores, (r = .416) GPA and ATI scores, (r = .355)
Scatter Plot c Scatter Plot d
Relationship between Average Hours Relationship between Clinical
Experience Worked and ATI scores, (r = -.030) Survey and ATI scores, (r = .081)
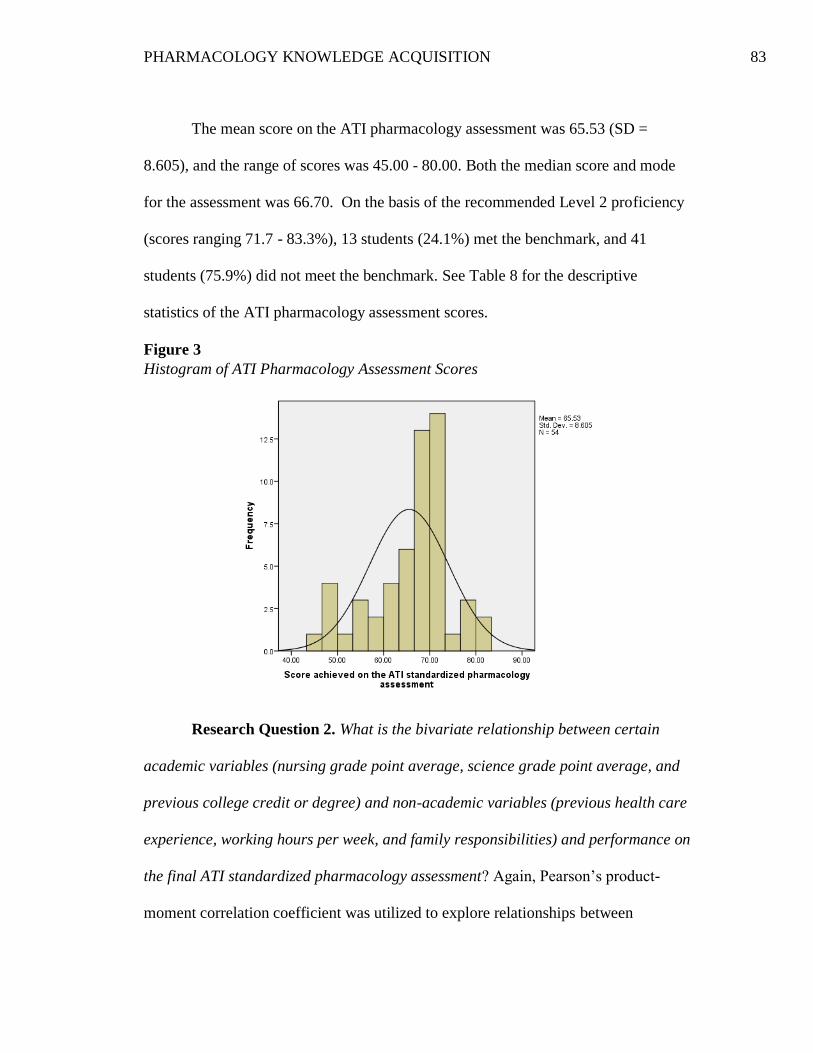
PHARMACOLOGY KNOWLEDGE ACQUISITION 83
The mean score on the ATI pharmacology assessment was 65.53 (SD =
8.605), and the range of scores was 45.00 - 80.00. Both the median score and mode
for the assessment was 66.70. On the basis of the recommended Level 2 proficiency
(scores ranging 71.7 - 83.3%), 13 students (24.1%) met the benchmark, and 41
students (75.9%) did not meet the benchmark. See Table 8 for the descriptive
statistics of the ATI pharmacology assessment scores.
Figure 3
Histogram of ATI Pharmacology Assessment Scores
Research Question 2. What is the bivariate relationship between certain
academic variables (nursing grade point average, science grade point average, and
previous college credit or degree) and non-academic variables (previous health care
experience, working hours per week, and family responsibilities) and performance on
the final ATI standardized pharmacology assessment? Again, Pearson’s product-
moment correlation coefficient was utilized to explore relationships between
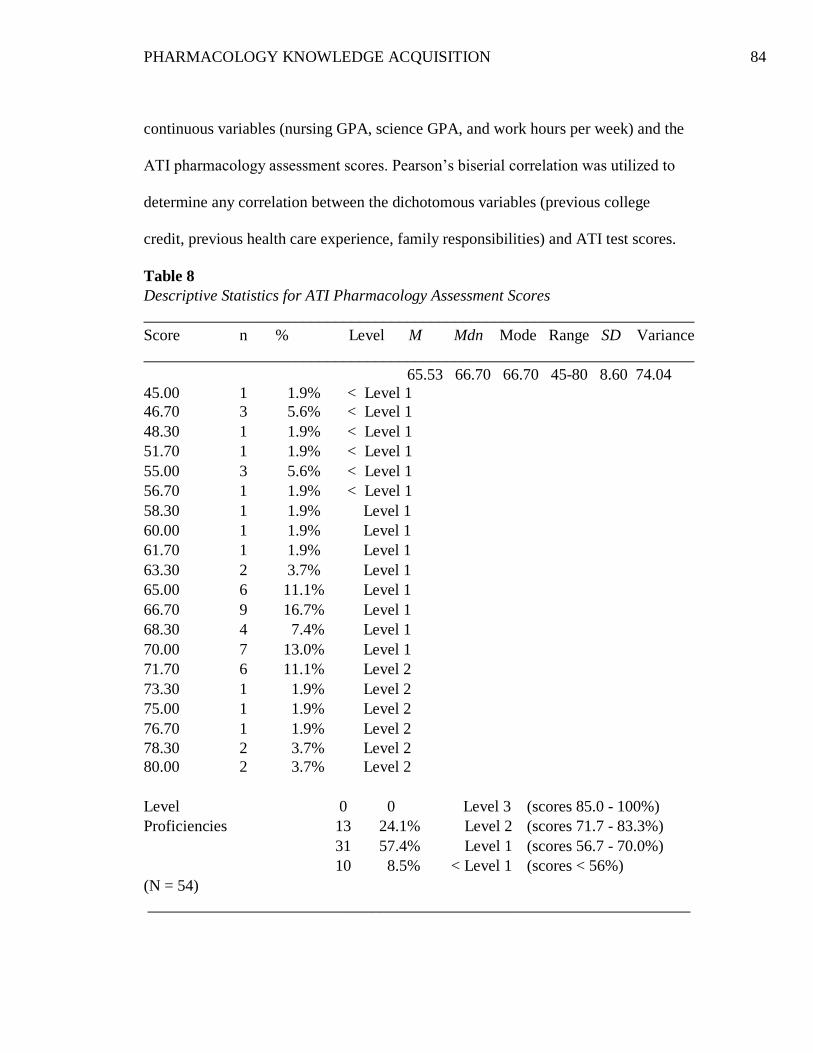
PHARMACOLOGY KNOWLEDGE ACQUISITION 84
continuous variables (nursing GPA, science GPA, and work hours per week) and the
ATI pharmacology assessment scores. Pearson’s biserial correlation was utilized to
determine any correlation between the dichotomous variables (previous college
credit, previous health care experience, family responsibilities) and ATI test scores.
Table 8
Descriptive Statistics for ATI Pharmacology Assessment Scores
_____________________________________________________________________
Score n % Level M Mdn Mode Range SD Variance
_____________________________________________________________________
65.53 66.70 66.70 45-80 8.60 74.04
45.00 1 1.9% < Level 1
46.70 3 5.6% < Level 1
48.30 1 1.9% < Level 1
51.70 1 1.9% < Level 1
55.00 3 5.6% < Level 1
56.70 1 1.9% < Level 1
58.30 1 1.9% Level 1
60.00 1 1.9% Level 1
61.70 1 1.9% Level 1
63.30 2 3.7% Level 1
65.00 6 11.1% Level 1
66.70 9 16.7% Level 1
68.30 4 7.4% Level 1
70.00 7 13.0% Level 1
71.70 6 11.1% Level 2
73.30 1 1.9% Level 2
75.00 1 1.9% Level 2
76.70 1 1.9% Level 2
78.30 2 3.7% Level 2
80.00 2 3.7% Level 2
Level 0 0 Level 3 (scores 85.0 - 100%)
Proficiencies 13 24.1% Level 2 (scores 71.7 - 83.3%)
31 57.4% Level 1 (scores 56.7 - 70.0%)
10 8.5% < Level 1 (scores < 56%)
(N = 54)
____________________________________________________________________
PHARMACOLOGY KNOWLEDGE ACQUISITION 85
Description of Independent Variables. The study encompassed data
collection for seven independent variables for each participant. These academic and
non-academic variables included nursing GPA, science GPA, previous college credit
or degree, previous health care experience, average work hours per week, family
responsibilities, and average score for the student clinical experience survey. This
section will describe all independent variables with the exception of the clinical
experience survey, which is addressed in the analysis of the third research question.
The academic variables were collected from college admission and registration
records, and the non-academic variables were obtained through direct participant
feedback on a demographic information form.
Academic variables. The cumulative nursing GPA was based on three clinical
nursing courses in the program and ranged from 1.33 to 3.33 with a mean value of
2.27 (SD = .526). It should be noted that nursing GPA was based on first-time
performance in a course; therefore, the GPA for students failing a nursing course does
not reflect the revised cumulative average based on successful completion of the
course a second time.
The cumulative science GPA was calculated based on three biological science
courses; this GPA was based on science courses conducted at the college, as well as
science credits transferred in for equivalent courses. The mean science GPA for study
participants was 2.68 (SD = .656) and ranged from 1.33 to 4.00. The number of
participants who received transfer credit for external science courses, and the specific
number of credit hours accepted were additional variables collected in order to
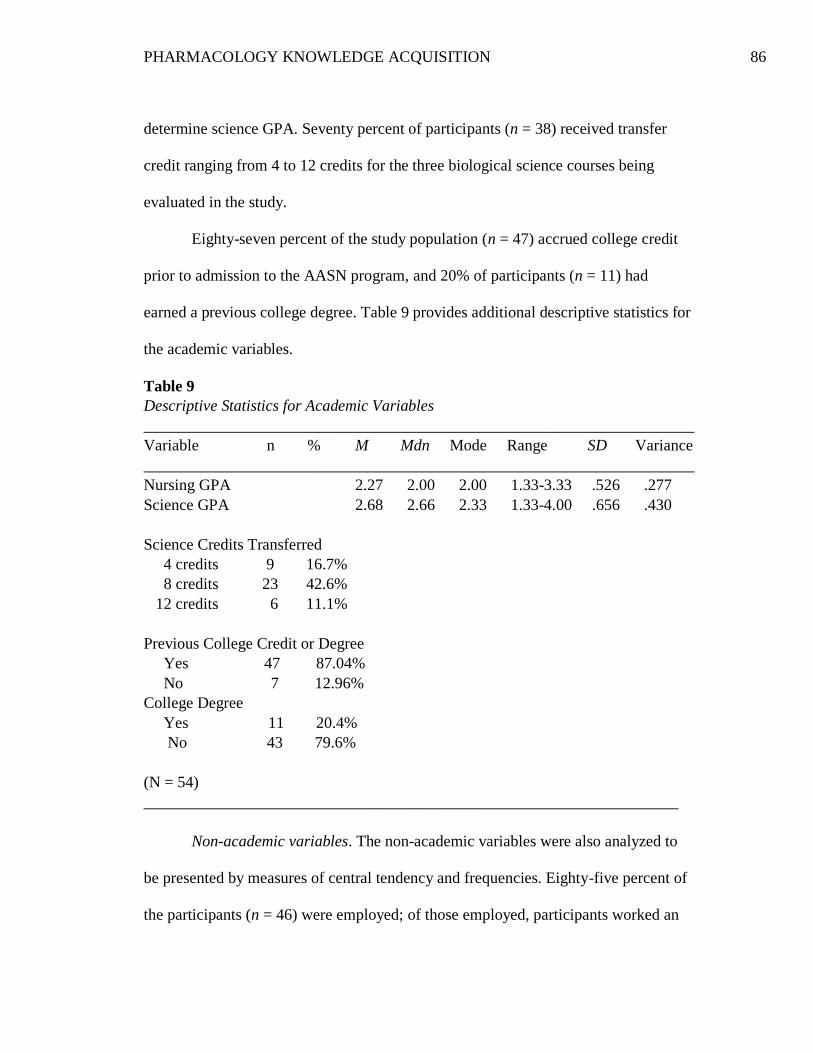
PHARMACOLOGY KNOWLEDGE ACQUISITION 86
determine science GPA. Seventy percent of participants (n = 38) received transfer
credit ranging from 4 to 12 credits for the three biological science courses being
evaluated in the study.
Eighty-seven percent of the study population (n = 47) accrued college credit
prior to admission to the AASN program, and 20% of participants (n = 11) had
earned a previous college degree. Table 9 provides additional descriptive statistics for
the academic variables.
Table 9
Descriptive Statistics for Academic Variables
_____________________________________________________________________
Variable n % M Mdn Mode Range SD Variance
_____________________________________________________________________
Nursing GPA 2.27 2.00 2.00 1.33-3.33 .526 .277
Science GPA 2.68 2.66 2.33 1.33-4.00 .656 .430
Science Credits Transferred
4 credits 9 16.7%
8 credits 23 42.6%
12 credits 6 11.1%
Previous College Credit or Degree
Yes 47 87.04%
No 7 12.96%
College Degree
Yes 11 20.4%
No 43 79.6%
(N = 54)
___________________________________________________________________
Non-academic variables. The non-academic variables were also analyzed to
be presented by measures of central tendency and frequencies. Eighty-five percent of
the participants (n = 46) were employed; of those employed, participants worked an
PHARMACOLOGY KNOWLEDGE ACQUISITION 87
average of 4 - 37.5 hours per week. When participants identified a range of hours
worked instead of a whole number, working hours per week were averaged between
the two numbers. For example, if participants identified the average number of work
hours as 8-12 hours, a value of 10 was entered for this field in the data file. The
average number of working hours per week for all employed participants was 18.89
hours (SD = 9.161).
Approximately 80% of the study population (n = 43) acknowledged previous
or current health care experience involving direct patient care other than that acquired
during nursing school. Forty-four percent of participants (n = 24) identified existing
family responsibilities; these responsibilities were further categorized by financial
responsibility as head of household (29.6%, n = 16), responsibility for dependent
children (27.8%, n = 15), and responsibility as a caregiver (13%, n = 7). Ten
participants (18.5%) answered “Yes” to more than one category of family
responsibilities, and four participants (7.4%) answered “Yes” to all three categories of
family responsibilities. See Table 10 for statistics describing the remaining non-
academic variables analyzed in the second research question.
Correlational Analysis. Pearson’s product moment correlation was used to
evaluate relationships between nursing GPA, science GPA or average work hours and
ATI test scores. The correlation between nursing GPA and ATI pharmacology
assessment scores was significant (r = .416, p = .002), and the size of the correlation
was moderate (r2 = .173). This suggests that nursing GPA explains 17.3% of the
variability of the ATI score. The correlation between science GPA and ATI
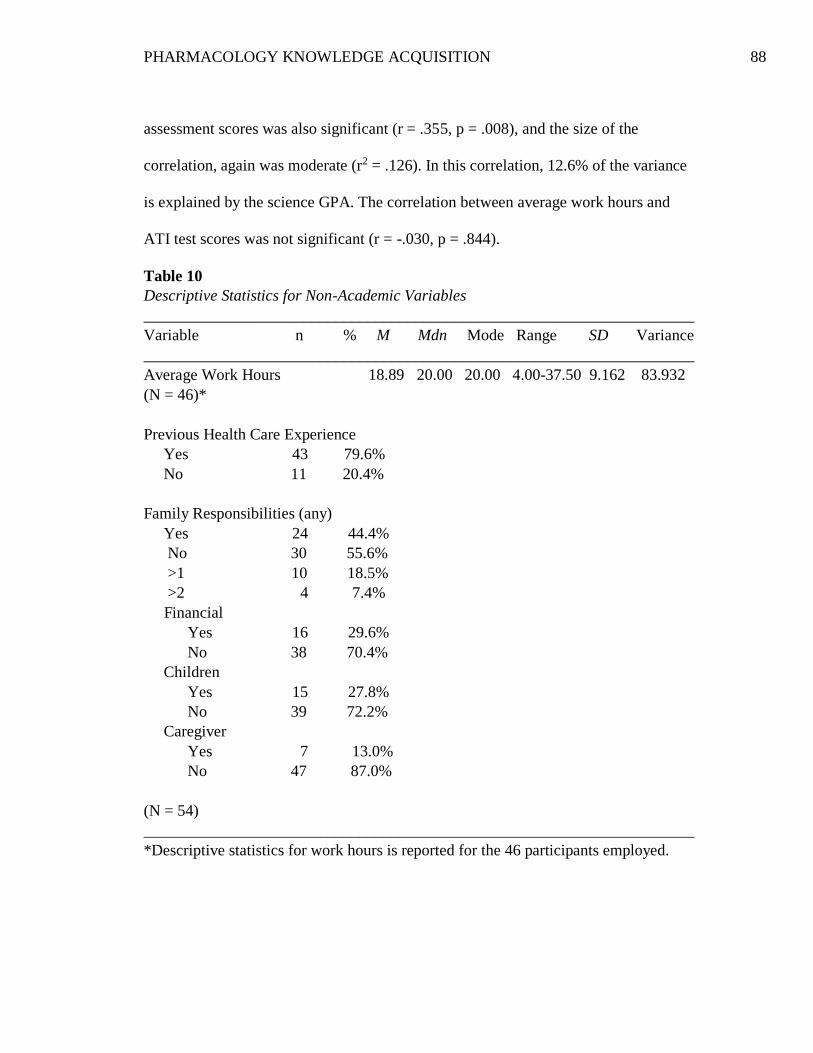
PHARMACOLOGY KNOWLEDGE ACQUISITION 88
assessment scores was also significant (r = .355, p = .008), and the size of the
correlation, again was moderate (r2 = .126). In this correlation, 12.6% of the variance
is explained by the science GPA. The correlation between average work hours and
ATI test scores was not significant (r = -.030, p = .844).
Table 10
Descriptive Statistics for Non-Academic Variables
_____________________________________________________________________
Variable n % M Mdn Mode Range SD Variance
_____________________________________________________________________
Average Work Hours 18.89 20.00 20.00 4.00-37.50 9.162 83.932
(N = 46)*
Previous Health Care Experience
Yes 43 79.6%
No 11 20.4%
Family Responsibilities (any)
Yes 24 44.4%
No 30 55.6%
>1 10 18.5%
>2 4 7.4%
Financial
Yes 16 29.6%
No 38 70.4%
Children
Yes 15 27.8%
No 39 72.2%
Caregiver
Yes 7 13.0%
No 47 87.0%
(N = 54)
_____________________________________________________________________
*Descriptive statistics for work hours is reported for the 46 participants employed.
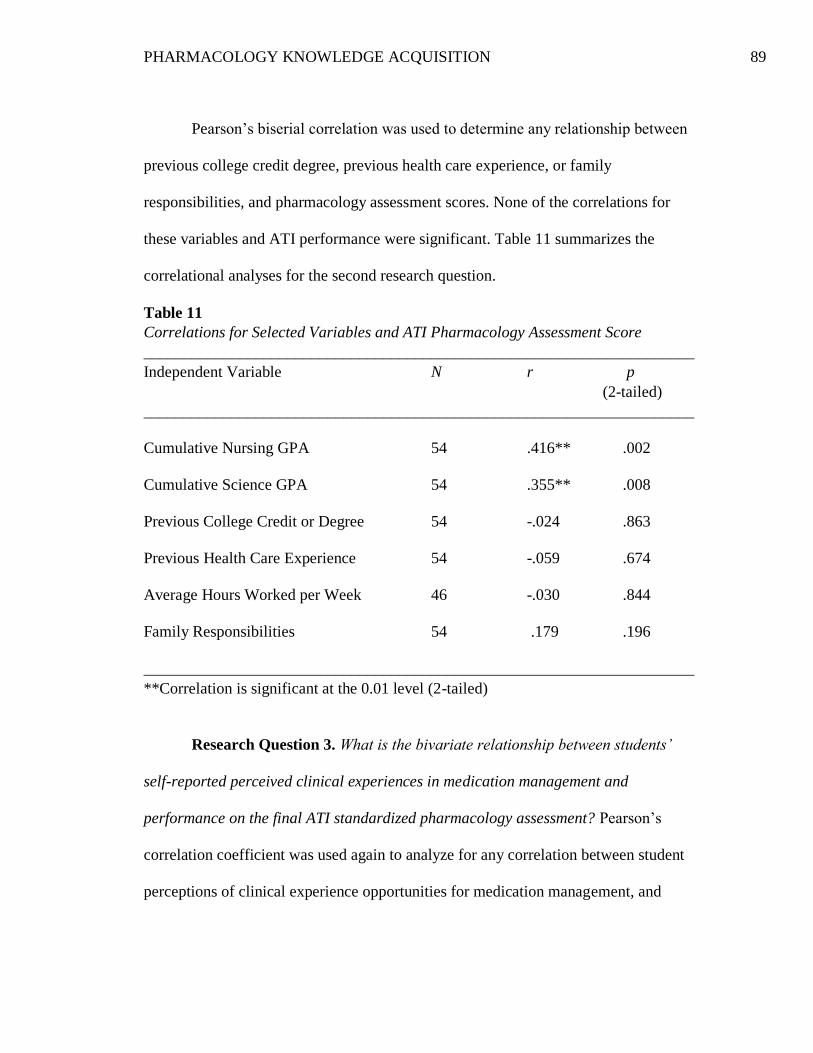
PHARMACOLOGY KNOWLEDGE ACQUISITION 89
Pearson’s biserial correlation was used to determine any relationship between
previous college credit degree, previous health care experience, or family
responsibilities, and pharmacology assessment scores. None of the correlations for
these variables and ATI performance were significant. Table 11 summarizes the
correlational analyses for the second research question.
Table 11
Correlations for Selected Variables and ATI Pharmacology Assessment Score
_____________________________________________________________________
Independent Variable N r p
(2-tailed)
_____________________________________________________________________
Cumulative Nursing GPA 54 .416** .002
Cumulative Science GPA 54 .355** .008
Previous College Credit or Degree 54 -.024 .863
Previous Health Care Experience 54 -.059 .674
Average Hours Worked per Week 46 -.030 .844
Family Responsibilities 54 .179 .196
_____________________________________________________________________
**Correlation is significant at the 0.01 level (2-tailed)
Research Question 3. What is the bivariate relationship between students’
self-reported perceived clinical experiences in medication management and
performance on the final ATI standardized pharmacology assessment? Pearson’s
correlation coefficient was used again to analyze for any correlation between student
perceptions of clinical experience opportunities for medication management, and
PHARMACOLOGY KNOWLEDGE ACQUISITION 90
performance on the final pharmacology assessment. When evaluating the distribution
of data, the histograms for three variables presented values outside of the normal
distribution. These outliers were noted on the histograms for age, the average score
on the clinical experience survey questionnaire, and the total score on the survey.
Participant age was not to be utilized in any correlation but rather only for the
descriptive statistics. Therefore, the outlier for age did not need to be removed since
there was no potential influence on the results of the study analysis. However, the
clinical experience survey was a variable being examined in the analysis for the third
research question. The clinical experience survey was analyzed by average score and
total score, but only the average score was utilized in the correlational analysis. In
order to evaluate for any distortion of significance as a result of extreme values or
values outside of the normal distribution, the correlational analyses were run before
and after removal of the outliers. The histograms in Figure 4 show the distribution of
survey scores with and without the outliers.
Description of the Clinical Experience Survey Questionnaire. The clinical
experience survey questionnaire was an investigator-developed survey comprised of
six statements, and participants responded to each item using a Likert scale. The
survey was analyzed using both the average score for each statement and the total
score for all survey items. There were no missing values for any of the survey items.
The average score of survey responses was selected for analysis to enhance clarity for
interpreting results. Prior to analyzing the overall scores of the survey, reliability of
the six-item scale was evaluated by Cronbach’s alpha statistic. Cronbach’s alpha was
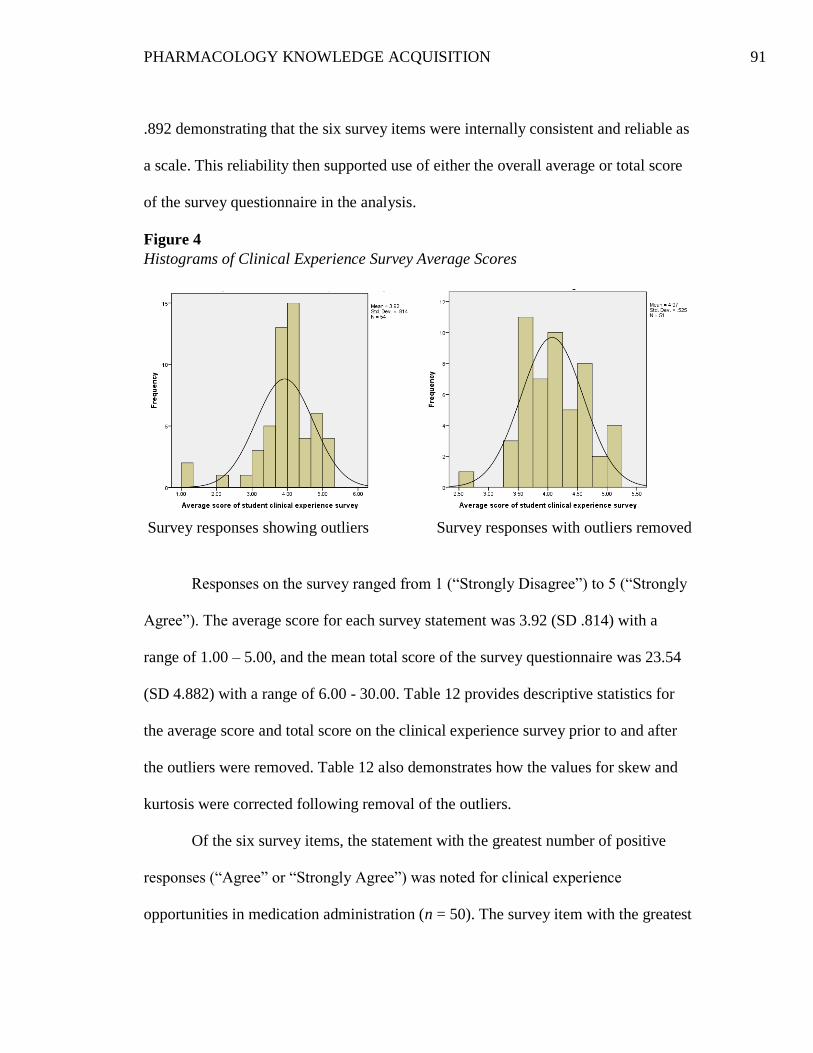
PHARMACOLOGY KNOWLEDGE ACQUISITION 91
.892 demonstrating that the six survey items were internally consistent and reliable as
a scale. This reliability then supported use of either the overall average or total score
of the survey questionnaire in the analysis.
Figure 4
Histograms of Clinical Experience Survey Average Scores
Survey responses showing outliers Survey responses with outliers removed
Responses on the survey ranged from 1 (“Strongly Disagree”) to 5 (“Strongly
Agree”). The average score for each survey statement was 3.92 (SD .814) with a
range of 1.00 – 5.00, and the mean total score of the survey questionnaire was 23.54
(SD 4.882) with a range of 6.00 - 30.00. Table 12 provides descriptive statistics for
the average score and total score on the clinical experience survey prior to and after
the outliers were removed. Table 12 also demonstrates how the values for skew and
kurtosis were corrected following removal of the outliers.
Of the six survey items, the statement with the greatest number of positive
responses (“Agree” or “Strongly Agree”) was noted for clinical experience
opportunities in medication administration (n = 50). The survey item with the greatest
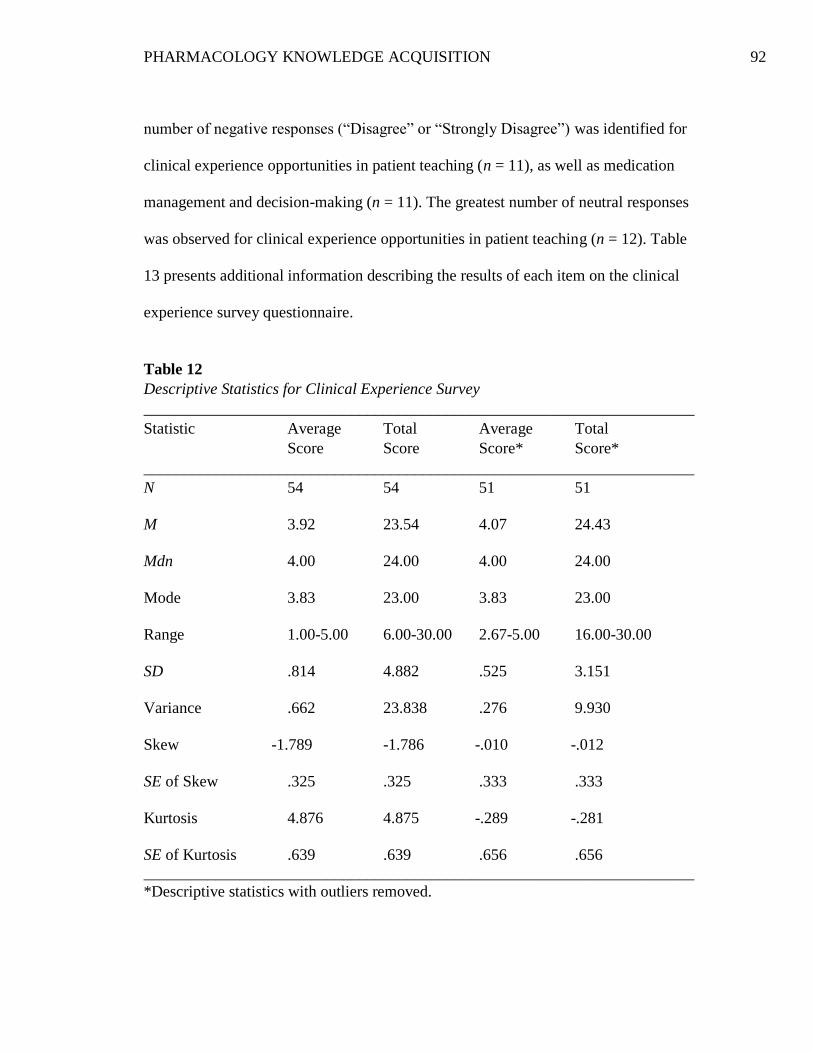
PHARMACOLOGY KNOWLEDGE ACQUISITION 92
number of negative responses (“Disagree” or “Strongly Disagree”) was identified for
clinical experience opportunities in patient teaching (n = 11), as well as medication
management and decision-making (n = 11). The greatest number of neutral responses
was observed for clinical experience opportunities in patient teaching (n = 12). Table
13 presents additional information describing the results of each item on the clinical
experience survey questionnaire.
Table 12
Descriptive Statistics for Clinical Experience Survey
_____________________________________________________________________
Statistic Average Total Average Total
Score Score Score* Score*
_____________________________________________________________________
N 54 54 51 51
M 3.92 23.54 4.07 24.43
Mdn 4.00 24.00 4.00 24.00
Mode 3.83 23.00 3.83 23.00
Range 1.00-5.00 6.00-30.00 2.67-5.00 16.00-30.00
SD .814 4.882 .525 3.151
Variance .662 23.838 .276 9.930
Skew -1.789 -1.786 -.010 -.012
SE of Skew .325 .325 .333 .333
Kurtosis 4.876 4.875 -.289 -.281
SE of Kurtosis .639 .639 .656 .656
_____________________________________________________________________
*Descriptive statistics with outliers removed.
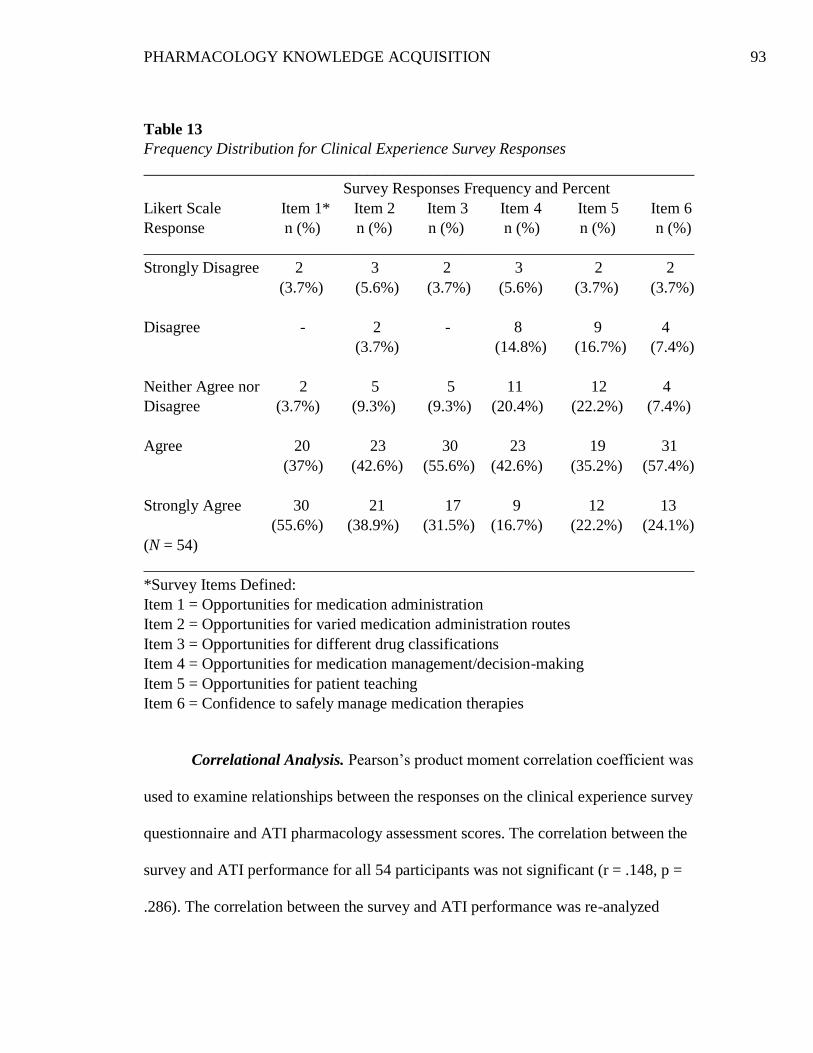
PHARMACOLOGY KNOWLEDGE ACQUISITION 93
Table 13
Frequency Distribution for Clinical Experience Survey Responses
_____________________________________________________________________
Survey Responses Frequency and Percent
Likert Scale Item 1* Item 2 Item 3 Item 4 Item 5 Item 6
Response n (%) n (%) n (%) n (%) n (%) n (%)
_____________________________________________________________________
Strongly Disagree 2 3 2 3 2 2
(3.7%) (5.6%) (3.7%) (5.6%) (3.7%) (3.7%)
Disagree - 2 - 8 9 4
(3.7%) (14.8%) (16.7%) (7.4%)
Neither Agree nor 2 5 5 11 12 4
Disagree (3.7%) (9.3%) (9.3%) (20.4%) (22.2%) (7.4%)
Agree 20 23 30 23 19 31
(37%) (42.6%) (55.6%) (42.6%) (35.2%) (57.4%)
Strongly Agree 30 21 17 9 12 13
(55.6%) (38.9%) (31.5%) (16.7%) (22.2%) (24.1%)
(N = 54)
_____________________________________________________________________
*Survey Items Defined:
Item 1 = Opportunities for medication administration
Item 2 = Opportunities for varied medication administration routes
Item 3 = Opportunities for different drug classifications
Item 4 = Opportunities for medication management/decision-making
Item 5 = Opportunities for patient teaching
Item 6 = Confidence to safely manage medication therapies
Correlational Analysis. Pearson’s product moment correlation coefficient was
used to examine relationships between the responses on the clinical experience survey
questionnaire and ATI pharmacology assessment scores. The correlation between the
survey and ATI performance for all 54 participants was not significant (r = .148, p =
.286). The correlation between the survey and ATI performance was re-analyzed
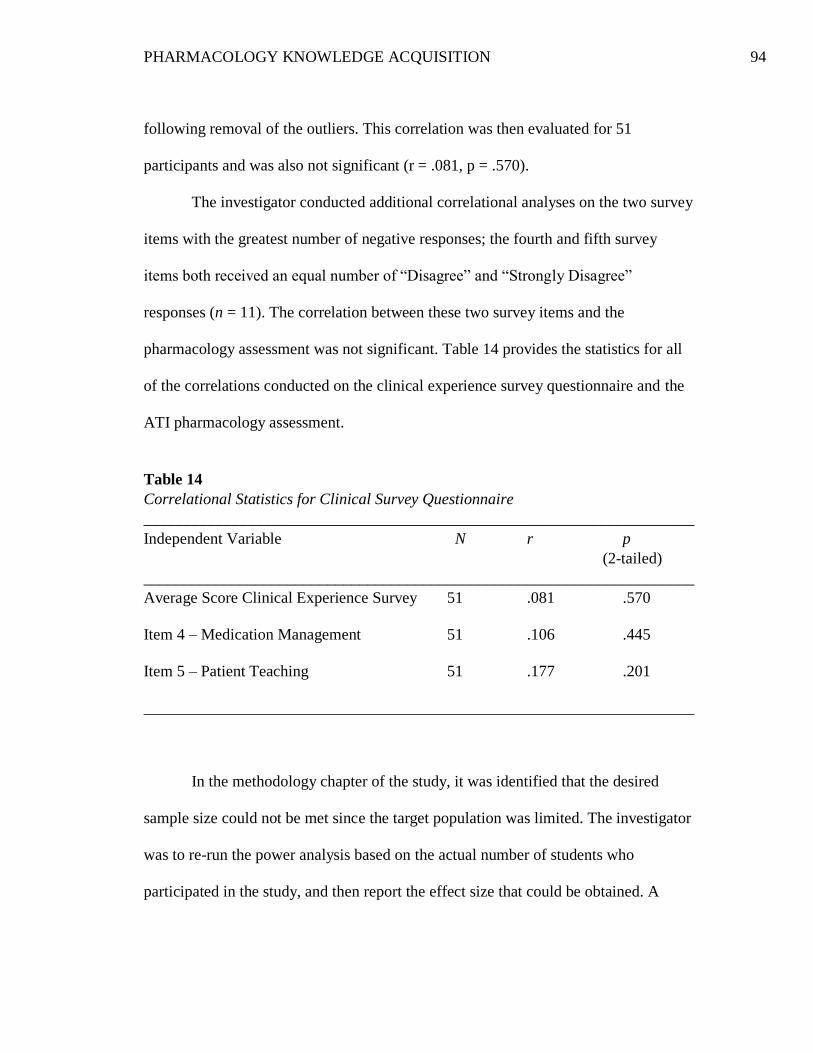
PHARMACOLOGY KNOWLEDGE ACQUISITION 94
following removal of the outliers. This correlation was then evaluated for 51
participants and was also not significant (r = .081, p = .570).
The investigator conducted additional correlational analyses on the two survey
items with the greatest number of negative responses; the fourth and fifth survey
items both received an equal number of “Disagree” and “Strongly Disagree”
responses (n = 11). The correlation between these two survey items and the
pharmacology assessment was not significant. Table 14 provides the statistics for all
of the correlations conducted on the clinical experience survey questionnaire and the
ATI pharmacology assessment.
Table 14
Correlational Statistics for Clinical Survey Questionnaire
_____________________________________________________________________
Independent Variable N r p
(2-tailed)
_____________________________________________________________________
Average Score Clinical Experience Survey 51 .081 .570
Item 4 – Medication Management 51 .106 .445
Item 5 – Patient Teaching 51 .177 .201
_____________________________________________________________________
In the methodology chapter of the study, it was identified that the desired
sample size could not be met since the target population was limited. The investigator
was to re-run the power analysis based on the actual number of students who
participated in the study, and then report the effect size that could be obtained. A
PHARMACOLOGY KNOWLEDGE ACQUISITION 95
revised power analysis was conducted for the sample size of 54 participants based on
Pearson’s correlation two-tailed power analysis. A sample size of 54 with an alpha of
.04 and beta of .20, for a power of .80 yields an effect size of .37. This is slightly
larger than a medium effect size but relatively close to the .30 correlation size initially
desired.
Summary
In summary, a total of seven academic and non-academic variables were
evaluated in this study for any relationship to pharmacology knowledge acquisition as
demonstrated by performance on a final standardized ATI pharmacology assessment.
Descriptive analysis of the variables was completed and reported using SPSS
statistical procedures. In addition to the descriptive statistics, Pearson’s product
moment correlation coefficient and Pearson’s biserial correlation were utilized to
complete a series of bivariate correlations. The assumptions for Pearson’s correlation
were met as demonstrated by the normal distribution of data and linearity of the
Scatter Plots. The correlational analysis for the variables was completed with and
without the outliers to evaluate for any misrepresentation of statistical significance.
Cronbach’s alpha coefficient revealed internal consistency of the clinical experience
survey items, thereby establishing reliability of the survey questionnaire as a scale.
The analysis of the study showed statistically significant correlations for
nursing GPA and ATI pharmacology assessment scores, and science GPA and ATI
pharmacology assessment scores. The strength of the correlation was moderate for
both variables. The correlation between clinical experience opportunities for

PHARMACOLOGY KNOWLEDGE ACQUISITION 96
medication administration and management as self-reported by students and
pharmacology test scores was not statistically significant, nor were any of the other
academic and non-academic variables in the study.
PHARMACOLOGY KNOWLEDGE ACQUISITION 97
Chapter 5: Discussion
The purpose of this study was to determine any correlation between selected
academic and non-academic variables and pharmacology knowledge acquisition as
demonstrated by performance on a cumulative pharmacology assessment. A total of
seven academic and non-academic variables were evaluated for undergraduate
nursing students. The analysis of the medication administration and decision-making
experience as self-reported by students was of particular interest to the investigator;
this variable reflected any relationship between student perceptions of clinical
experience opportunities for medication management, and performance on the final
pharmacology assessment. Chapter five provides a discussion of the major findings of
the study, limitations, and implications for nursing, nursing education, and future
research.
Discussion
Of the seven variables analyzed in the study, the analysis only showed
statistically significant correlations for nursing GPA and ATI pharmacology
assessment scores, and science GPA and ATI pharmacology assessment scores.
Pearson’s product moment correlation was used to evaluate for these relationships. A
correlation coefficient of positive or negative .1 reflects a small effect compared to .3,
which is considered a moderate effect, or .5 a large effect (Field, 2013, p. 270).
Therefore, the strength of the correlation was moderate for both of the GPA variables.
The following discussion will focus on the findings of the study for each research
question and compare these findings to the literature.
PHARMACOLOGY KNOWLEDGE ACQUISITION 98
Level of performance on the ATI pharmacology assessment. The overall
level of performance of the study group was below the established Level II
benchmark; this benchmark demonstrates the ability to readily achieve NCLEX-RN
standards and exceed expectations for performance in the content area of
pharmacological therapies. Level 1 proficiency suggests that the student has minimal
knowledge and meets the absolute minimum expectations for performance. Fifty-
seven percent of the study population achieved a Level 1 proficiency, and 18% fell
below the Level 1 proficiency. These findings are concerning for students nearing
completion of an undergraduate program. Nevertheless, they are consistent with the
literature suggesting that nurses do not have sufficient knowledge and are
inadequately prepared in pharmacology (Adhikari et al., 2014; Dilles et al., 2011;
Honey & Lim, 2008; King, 2004; Latter, et al., 2000, 2001; Morrison-Griffiths et al.,
2002; Ndosi & Newell, 2008; Simonsen et al., 2014). The literature also identified
that nursing students, novice nurses and new graduates have difficulty
comprehending pharmacology (Adhikari et al., 2014; Manias & Bullock, 2002;
Simonsen et al., 2014). The level of participant performance on the ATI
pharmacology assessment correlates with these findings in the literature.
It is possible that the timing and consequences of the ATI pharmacology
assessment influenced the level of performance. The theory content of the Nursing IV
course is front-loaded within the first ten weeks of the course resulting in eight hours
of theory content per week. The pharmacology assessment was conducted during the
tenth week of the semester and within less than one week of the final course
PHARMACOLOGY KNOWLEDGE ACQUISITION 99
examination. Although points were allocated for achieving the benchmark, the
pharmacology assessment was only worth 1% of the course grade. Fatigue during the
tenth week of the semester and minimal consequences tied to the assessment are
potential factors negatively impacting motivation for students to do well on the test.
Participants may also have been more focused on the upcoming comprehensive
examination, which was worth 30% of the course grade and therefore, significantly
influences passing or failing the course.
The computerized report generated by ATI for the pharmacology assessment
demonstrated a group score mean of 65.4% for all students in the class. The national
mean for the test was 63.2% and the program group mean was 64.1%. The program
mean reflects the average score of groups within the same program type category. It
should be noted that the group score mean was based on the entire class of 63
students who took the examination, as opposed to the 54 participants who agreed to
participate in the study. Although only 24% of the study population met the Level 2
benchmark, almost 80% of participants exceeded the national mean, and 72%
exceeded the program type mean. While it may appear that the study population
performed well in comparison to students in other programs, there are several factors
that are unknown in the group performance calculations by ATI. For example, it is
not clear whether students from the study population are compared to other students
who are at the same progression point in their respective programs. It is also uncertain
as to whether the testing for other programs was proctored or non-proctored, if the
PHARMACOLOGY KNOWLEDGE ACQUISITION 100
assessment comprised a portion of a course grade, or whether any other consequences
were tied to the examination.
Relationship between selected variables and ATI performance. Of the six
variables analyzed in the second research question, two factors correlated positively
with performance on the pharmacology assessment. A higher nursing GPA and
science GPA was associated with a higher score on the ATI assessment. These
findings were not unexpected as a number of studies have demonstrated science GPA
as a predictor for success in nursing, nursing GPA as a predictor for NCLEX-RN
success, and science GPA as a predictor of NCLEX-RN success. The literature also
presents several studies that have linked pharmacology course grades or performance
on pharmacology standardized assessments to NCLEX-RN success (Emory, 2012;
Paraszczuk, 2011; Silvestri, 2010; Ukpabi, 2008).
The study did not show any correlation between the academic variable of
previous college credit or degree and performance on the ATI assessment. This
finding was inconsistent with assertions of the theoretical framework that past
experiences serve as a rich resource for learning, or that adults tend to draw on
previous experience for learning. Eighty-seven percent of participants had completed
previous college courses. This finding is not surprising considering the increasing
number of nontraditional students who enter undergraduate nursing programs or the
number of students who are pursuing nursing as a second career. However, the
overall high percentage of students who accrued previous college credit contributes to
PHARMACOLOGY KNOWLEDGE ACQUISITION 101
the homogeneity of the sample. The lack of variability in the study population
potentially explains the lack of any impact on ATI performance.
While student admission records identify the specific courses taken or degrees
acquired prior to entry in the program, the study investigator did not collect or
analyze this information. However, when calculating the science GPA, the
investigator did ascertain that 70% of participants transferred 4-12 credits in the
biological sciences. While transferred credit was not a variable in the study, several
questions are raised in relation to the impact on science GPA, nursing GPA or
pharmacology knowledge acquisition. Theoretical competence and proficiency in
anatomy and physiology is identified as a competency area for pharmacology
knowledge and medication competence (Sulosaari et al., 2011). The rigor and
expectations of science courses completed outside of the college is not known. In
consideration of science GPA as a predictor for academic success in nursing, one
implication is that outside courses may not be comparable to those offered internally.
Conversely, another implication is that outside courses are actually more rigorous
accounting for the average science GPA of 2.68 and low range of 1.33. The teaching
methods for outside courses may be inconsistent with the conceptual approach of the
college, or the application of theory to practice may have been limited. The interval
of time that has transpired since completion of an external science course is also
unclear. The retention of basic principles of anatomy and physiology as a foundation
for nursing is a concern when large gaps of time exist between science and nursing
courses. The relationship between performance in the biological sciences and nursing
PHARMACOLOGY KNOWLEDGE ACQUISITION 102
GPA has been well documented in the literature, and therefore, the quality of
education in the biological sciences warrants close attention.
The non-academic variables of previous health care experience, working
hours per week, and family responsibilities did not reveal any significant correlations
with ATI performance. Nearly 80% of participants in the study identified previous
health care experience for direct patient care outside of clinical experiences. Similar
to college credit, this high percentage suggests a homogenous group, thereby lending
little variability to the study population. Again, the discussion of andragogy as a
theoretical framework for the study noted that adult learners perform well when they
use prior experience (Pappas, 2014, Billings & Halstead, 2012). On this principle,
prior experience such as health care experience, or prior knowledge as a result of
earning another degree or college credit would be expected to enhance learning.
Therefore, the lack of correlation for previous health care experience is inconsistent
with the literature. The fact that some schools of nursing require nursing assistant
certificates as an admission requirement had piqued interest by the investigator in the
relevance of previous health care experience; however, any previous health care
experience that may have been associated with nursing assistant certification did not
reveal any impact on test performance.
As non-licensed personnel, it is possible that previous health care experience
had little relevance for the knowledge needed to comprehend pharmacological
principles and apply them to practice. Another consideration is the age of the study
population and the length of experience in health care. Although the college has a
PHARMACOLOGY KNOWLEDGE ACQUISITION 103
high percentage of nontraditional students, the mean age of participants was 26 years
and the mode ranged from 22 to 24; students in the age range of 24 years and younger
accounted for 54% of the study population. Even though the student population is
considered nontraditional and beyond adolescent years, the average age of
participants was still fairly young. Consequently, some of the principles of andragogy
may not be as applicable in this study population as they would be to an older student
population. The study also did not analyze the length of health care experience nor
the specific type of health care setting where experience had been obtained. Students
may also have failed to recognize the aspect of the question that emphasized
experience in direct patient care. All of these are additional factors that may have
impacted the lack of correlation to ATI performance.
Eighty-five percent of study participants were employed, and worked an
average of 18-20 hours per week. Forty-four percent of participants indicated family
or financial responsibilities, and ten participants identified responsibility in two or all
three categories. It is logical to expect that as work hours or family responsibilities
increase, time available for studying decreases; decreased study time is typically
associated with decreased academic performance. Therefore, a negative correlation
was anticipated between working hours and ATI test scores, but no correlation
existed between these variables. Furthermore, even though a high percentage of
students in the college fall into one or more of the characteristics that define
nontraditional students (AACRAO, 2015), and studies have shown that nontraditional
PHARMACOLOGY KNOWLEDGE ACQUISITION 104
students may be at risk for failure, there was no correlation between this variable and
ATI test performance.
The study findings for the nonacademic variables of working hours per week
and family responsibilities were inconsistent with the literature. The study by Strayer
and Beitz (2010) evaluated pharmacology knowledge acquisition between traditional
and nontraditional students, and indicated that students with responsibilities such as
family dependence and the need to work to support themselves do not perform as well
academically. Lack of time and the use of superficial learning strategies as a result of
time constraints and information overload have also been identified as factors
influencing pharmacology knowledge (Honey & Lim, 2008; King, 2004; Manias &
Bullock, 2002a, 2002b). As with several other variables, the high percentage of
working students, and the significant number of participants with family
responsibilities resulted in a more homogenous sample. The overall performance by
the study group on the pharmacology assessment was also similar, which further
contributes to the homogeneity of the study population. The degree to which
participants were very similar is, again, a leading factor in the lack of correlation with
ATI performance.
Relationship between clinical experiences and ATI performance. There
was no correlation between student perceived clinical experience opportunities for
medication administration and management and performance on the pharmacology
assessment. The investigator further analyzed those items in the survey where
opportunities were perceived lowest; however, no correlation was noted between
PHARMACOLOGY KNOWLEDGE ACQUISITION 105
those survey items and ATI scores. These findings are not consistent with the
literature in terms of factors that have been found to influence pharmacology
knowledge acquisition. Numerous studies have identified that additional clinical
experience opportunities are needed for medication administration and decision-
making, and that undergraduate clinical experience is one of the most important
factors promoting pharmacology knowledge acquisition (Adhikari et al., 2014; Honey
& Lim, 2008; Manias & Bullock, 2002a, 2002b; Bullock & Manias, 2002; Ives et al.,
1996). The importance of clinical experience opportunities has been emphasized in
the literature by both graduate nurses and seasoned nurses, as well as undergraduate
students in nursing.
When analyzing the total clinical experience survey score and the average
survey score, the mean values are relatively high, and the majority of responses to
each survey item were positive. Of the potential 324 responses by 54 participants, 248
responses (77%) were identified as “Agree” or “Strongly Agree”. This finding
indicates that a high number of participants found the clinical experience
opportunities in the program to be sufficient. The positive evaluation of clinical
experiences may be associated with the long-time clinical emphasis of the
undergraduate program. The degree of positive responses by the vast majority of the
group is a factor for the absence of any correlation between the clinical experience
survey and ATI performance.
Other explanations for the lack of correlation with clinical experience
opportunities include survey-related issues. Students may not feel comfortable
PHARMACOLOGY KNOWLEDGE ACQUISITION 106
answering survey items in an unfavorable manner, or may feel pressured to respond
in a way they believe faculty expect them to respond. Students tend to record
responses that reflect more positively on their abilities, knowledge, or perceptions. It
is possible that survey items were interpreted differently by different participants.
Students were instructed to consider cumulative clinical experience opportunities
when responding, but were possibly influenced to a greater extent by their most
recent clinical experiences. Nursing IV clinical experiences involve the most
comprehensive patient care by students, provide multiple patient assignments and
require administration of all medications. Survey responses may have been influenced
by the clinical experiences immediately prior to administration of the survey, or
students may not have been able to recall the quality of experiences in previous
courses. It should be noted, however, that only 12% of all responses were answered
as “Neither Agree nor Disagree” suggesting that participants were confident and clear
in the majority of their answers to the survey items.
Burns and Grove identify that measurement error is inherent in any
measurement strategy and is defined as the “difference between what exists in reality
and what a research instrument measures” (2009, p. 372). Content validity for the
survey was established by the investigator through review by faculty colleagues, as
well as students who recently graduated from the program. Furthermore, the
reliability of the six-item scale was evaluated by Cronbach’s alpha statistic. A statistic
of .7 to .8 is considered an acceptable value for Cronbach’s alpha (Field, 2013). The
internal consistency reliability of the six-item survey scale was supported by a
PHARMACOLOGY KNOWLEDGE ACQUISITION 107
Cronbach’s alpha of .892. Despite efforts to establish content validity and reliability,
“an instrument that is reliable cannot be assumed to be valid for a particular study or
population” (Burns & Grove, 2009, p. 380). The survey questionnaire has not been
tested as a valid instrument from one sample population to another; therefore, the
extent to which the instrument potentially measures concepts other than what was
intended contributes to systematic error and decreased validity. Measurement error is
a final potential factor affecting the results of the analysis.
Utility of the theoretical framework. As mentioned previously, several
findings in the study were inconsistent with the theoretical framework. These findings
included the lack of correlation of previous college credit or degree and previous
health care experience with performance on the ATI pharmacology assessment. Adult
Learning Theory or Andragogy emphasizes the value of past experiences of the adult
learner as a resource for learning. Factors that may have contributed to this lack of
correlation have been presented. Another issue impacting the usefulness of the
theoretical framework was the average age of the study population. While the
majority of students in the college met criteria for nontraditional status, the mean age
of participants was 26 years, and 54% of the study population was 24 years or
younger. As a result, some of the principles or assertions of Andragogy may be less
relevant to this younger population of students. Andragogy also asserts that adult
learners are self-directed and need to be involved in the learning process or be able to
direct their learning. Pharmacology is traditionally a difficult subject for many
students to learn and encompasses an extensive amount of material; therefore, the
PHARMACOLOGY KNOWLEDGE ACQUISITION 108
need for greater direction by faculty may be warranted in this content area. Despite
some of the inconsistencies between the study results and the theoretical framework,
components of Andragogy germane to the study population included readiness to
learn, personal relevance of the learning, and employment and family responsibilities
as potential variables interfering with academic performance.
Limitations
A number of methodological limitations of the study exist which restrict the
population to which the findings can be generalized. The first primary limitation is
the use of a convenience sample, the size of the sample, and data collection from a
single setting. The original estimate of 65 students in the Nursing IV class fell to 63 at
the time of enrollment in the study due to withdrawal from the course. Attendance of
the class when the study was introduced dropped even further to 56 students.
Therefore, even though 96% of the target population participated in the study, the
sample size obtained was small. A small sample size affects the power or capacity of
the study to detect differences or relationships that actually exist in the population
(Burns & Grove, 2009, p.357). In addition to sample size, the number of variables to
be examined in the study and effect size are additional factors that impact power. The
need for a larger sample size and greater diversity within the group was a foremost
issue for the study. While the use of multiple sites would have increased the size and
diversity of the sample, differences among programs with respect to admission
standards, curriculum design, faculty, and teaching methods would present other
influencing factors to consider.
PHARMACOLOGY KNOWLEDGE ACQUISITION 109
Another limitation for the study was the use of an investigator-developed
survey instrument, and the fact that responses to this survey relied on self-reported
data by students. The lack of any tested survey instrument in the literature to evaluate
clinical experience opportunities for medication management can be considered a
limitation as well. Concerns regarding measurement error and validity were addressed
in the discussion of the survey questionnaire. The reliability of self-reported data by
participants is also questionable. Factors that influence how participants might
respond to survey items were also presented in the discussion of the survey results.
All of these elements contribute to measurement error potentially creating bias and
variable error. In turn, bias and variance affect reliability; in this way, self-reported
data is another limitation of the study.
The lack of studies in the literature with which to compare this study
constitutes a final limitation of the study. A number of studies have addressed
variables which influence academic success and performance on the NCLEX-RN
examination, and several studies exist that identified a correlation between
pharmacology grades and NCLEX-RN performance. However, only one study was
found that specifically evaluated factors correlating with pharmacology knowledge
acquisition. Strayer and Beitz (2010) examined variables influencing pharmacology
course grades comparing traditional and nontraditional students. This gap in the
literature provided support for conducting the study, but the lack of similar studies
precludes comparison of findings to revise the methodology or validate results.
PHARMACOLOGY KNOWLEDGE ACQUISITION 110
Implications for Nursing and Nursing Education
As noted under the limitations of the study, the generalizability of the study is
limited. Even so, valuable information may be garnered from the review of the
literature and study results. The review of the literature provides a comprehensive
analysis of variables influencing pharmacology knowledge acquisition. The areas
identified serve as criteria by which nursing programs can establish curricular
standards for teaching pharmacology. The review of the literature identifies specific
knowledge deficits found in new graduates and novice nurses. This information is
valuable to nursing administrators for designing orientation programs and preventing
medication errors.
The study results have implications for program admission requirements and
processing, and a number of institutional policies. Enrollment management
committees may need to reconsider standards for admission, and revise policies
establishing admission criteria in order to enhance student success. Cumulative GPA
in the biological sciences may need to be considered more carefully, emphasized to a
greater extent, or assigned a higher percentage in comparison to other criteria used for
admission rubrics. Despite educational regulations that facilitate the transfer of
college credits, students who complete the majority of science courses outside of the
admitting institution may require further scrutiny. Cut-off values for grade point
averages that warrant academic probation may need to be raised, or students may
need to be referred for counseling and remediation at an earlier time. Grading policies
PHARMACOLOGY KNOWLEDGE ACQUISITION 111
should be evaluated and revised to ensure that passing grades reflect the necessary
achievement to facilitate success in subsequent courses and the overall program.
Nontraditional students are perceived as a group potentially at risk for
retention and academic performance issues. Identifying valid predictors of academic
success or failure enables nurse educators to pinpoint high-risk students, provide
needed academic support, and optimize student performance. Evidence of the
relationship between standardized assessments in pharmacology and NCLEX-RN
performance also supports the need to further investigate factors that influence or
predict pharmacology knowledge acquisition.
Even though the variables of work hours and family responsibilities did not
show a significant correlation, these issues compete for time available to devote to
studies. Admission processing should emphasize program rigor and expectations, and
incorporate a self-assessment analysis of personal circumstances. In this way,
potential applicants understand the impact of school on work-life balance and may be
counseled to delay admission until personal situations are less demanding. Institutions
that utilize standardized testing should continue to focus on early identification of
students who are at risk for failure, whether this failure applies to higher level nursing
courses or to the NCLEX-RN examination. Remediation efforts may need to begin
earlier in the program particularly for content-specific assessments that rely heavily
on a solid foundation of the biological sciences.
PHARMACOLOGY KNOWLEDGE ACQUISITION 112
Future Research
Curricular factors that influence pharmacology knowledge acquisition and
overall student success in nursing need to be explored further. In consideration of the
limitations of the study, the principal indication for future research is to repeat the
study for additional Nursing IV groups to obtain a larger sample size and a more
diverse study population. Future research might evaluate pharmacology knowledge
upon completion of the course rather than during week ten so as to minimize some of
the influencing factors described during this time of the semester. A pharmacology
assessment at the end of the semester would also account for clinical experiences
during role transition, which often significantly impacts student confidence in clinical
skills and patient care.
Several variables in the study present possible areas for future study as result
of the descriptive analysis. The high number of transferred science credits raises
questions as to the relationship between this variable and pharmacology knowledge
acquisition and academic success in general. A future study could examine any
correlation between the number of science credits transferred and nursing GPA, or the
number of science credits transferred and pharmacology test scores. The non-
academic variables of work hours and family responsibilities could be analyzed to
determine the relationship between combined factors and performance on the
pharmacology assessment. Combined factors might examine those participants who
are working plus have a family responsibility, or participants with two and three
family responsibilities combined.
PHARMACOLOGY KNOWLEDGE ACQUISITION 113
The emphasis of the literature on clinical experience opportunities as a
significant factor in acquiring pharmacology knowledge warrants further
investigation of this variable. In addition to the number of opportunities for
medication administration and management, the context in which clinical experiences
take place is worthwhile to study as numerous factors associated with the practice
setting have been cited to impact student experiences. The survey questionnaire
regarding clinical experience opportunities could also be revised to include more than
one measure of a concept being evaluated. For example, two or three survey items
could be developed to evaluate the same concept (e.g. medication management or
patient teaching), and the results of each of the items could be compared to enhance
validity. The impact of clinical experience opportunities for medication management
and decision-making on pharmacology knowledge could also be compared among
different nursing programs with varying clinical experience hours and requirements.
The relationship that has been identified between standardized pharmacology
tests and NCLEX-RN performance warrants further investigation of the factors that
influence or predict pharmacology knowledge acquisition. Identification of valid
predictors of academic success and academic risk can enable nurse educators to
devise strategies and interventions to optimize student performance and increase the
probability of passing the NCLEX-RN (Briscoe & Anema, 1999). Determining such
factors for pharmacology knowledge acquisition may assist educators to identify
high-risk students earlier in the program, provide needed academic support, and focus
on more effective teaching methodologies.
PHARMACOLOGY KNOWLEDGE ACQUISITION 114
The level of performance on the pharmacology assessment was consistent
with studies identifying inadequate knowledge and preparation of new graduates.
Numerous studies indicate that the number of hours allocated to pharmacology
education is unbalanced with the responsibilities and time nurses spend managing
pharmacological therapies. The literature also identifies controversy regarding
separate versus integrated pharmacology education, and some authors have suggested
the need for both. The college does not offer a separate pharmacology course at this
time. Therefore, future research might also focus on the impact of a separate
pharmacology course in the curriculum or compare outcomes between programs that
offer a separate pharmacology course and those that do not. While variables
influencing knowledge assist to identify at-risk students and facilitate early
remediation, future research is also needed to explore more effective teaching
strategies for this highly complex and wide-ranging subject matter.
Conclusion
A discussion of the seven variables analyzed in the study has been presented.
The variables of nursing GPA and science GPA were found to be statistically
significant, and these study results are consistent with the literature. The remaining
five variables did not show any correlation with performance on the ATI
pharmacology assessment. These findings were inconsistent with the literature, and a
number of factors have been suggested as possible reasons for the lack of correlation.
One factor considered was the homogeneity of the study population with respect to
ATI performance, college credit, working hours, and family responsibilities.
PHARMACOLOGY KNOWLEDGE ACQUISITION 115
Additional significant factors include the size of the sample, the single-site setting,
the use of an investigator-developed survey questionnaire, and the use of student self-
reported data. The issues surrounding each of these factors have been described.
Some of the factors that potentially influenced the outcome of the study were
also recognized as limitations. Again, these elements encompassed the small sample
size, a single setting, measurement errors associated with student self-reported data,
and the use of an instrument that has not been tested. Factors influencing motivation
to perform well on the pharmacology assessment were also recognized, and may be
considered limitations of the study.
The results of this study validate the significance of nursing GPA and science
GPA in determining academic success in nursing programs. Careful scrutiny of GPA
is indicated as a standard for admission and throughout the admission process.
Admission criteria and grading policies may need to be revised to support optimal
performance and successful completion of the program.
The findings in the descriptive analysis of variables raised questions regarding
additional areas to study in future research. Potential themes include further
investigation of the impact of transferred science credits, and working hours
combined with family responsibilities. Clinical experience opportunities need to be
evaluated further for a larger sample, and incorporate aspects of the clinical
environment that influence the experience.
The Institute of Medicine (IOM) has identified a number of recommendations
for the prevention of medication errors in response to alarming statistics for adverse
PHARMACOLOGY KNOWLEDGE ACQUISITION 116
medical events in health care. These recommendations include the need to improve
patient education regarding the risks, contraindications, and possible side effects of
prescribed medications, as well as the need for additional training in medication
management practices (IOM, 2006). Implicit in the IOM recommendations is the
need for nurses to acquire more comprehensive pharmacology knowledge. The
significance of pharmacology knowledge to safety, quality patient care, and the
prevention of medication errors warrant ongoing investigation of the factors that
influence, predict, or support knowledge acquisition.
PHARMACOLOGY KNOWLEDGE ACQUISITION 117
References
Adhikari R., Tocher, J., Smith, P., Corcoran, J., & MacArthur, J. (2014). A multi-
disciplinary approach to medication safety and the implication for nursing
education and practice. Nurse Education Today, 34(2), 185-190.
American Association of Collegiate Registrars and Admissions Officers (AACRAO).
(2015). Retrieved from
http://consulting.aacrao.org/publicationsevents/publications/changing-
demographics-why-nontraditional-students-should-matter-to-enrollment-
managers-and-what-they-can-do-to-attract-them
Armitage, G., & Knapman, H. (2003). Adverse events in drug administration: A
literature review. Journal of Nursing Management, 11(2), 130-40.
Assessment Technologies Institute, LLC. (2015a). ATI Nursing Education,
Integration Resources, Assessment Information, RN Assessment, RN Content
Mastery Series Proctored 2013, Test Descriptions. Retrieved from
http://www.atitesting.com/ati_next_gen/Faculty/FacultyLanding.aspx)
Assessment Technologies Institute, LLC. (2015b). ATI RN Content Mastery Series
(CMS) 2013 Technical Manual. Leawood, KS: ATI.
Banning, M. (2003). Pharmacology education: A theoretical framework of applied
pharmacology and therapeutics. Nurse Education Today, 23(6), 459-466.
PHARMACOLOGY KNOWLEDGE ACQUISITION 118
Barry, O. P., O’Sullivan, E., & McCarthy, M. (2015). Periodic review sessions
contribute to student learning across the disciplines in pharmacology. Journal
of the Scholarship of Teaching and Learning, 15(1), 38 - 56. doi:
10.14434/josotl.v15i1.12984
Billings, D. M., & Halstead, J. A. (2012). Teaching in nursing: A guide for faculty,
(3rd ed.). St. Louis: Saunders Elsevier.
Bonnivier, J. F., & Magoteaux, A. L. (2012). Innovative teaching strategy for
pharmacology in psychiatric-mental health nursing: Moving from content to
concepts. Journal of Psychosocial Nursing, 50(12), 22-29.
Brady, A., Malone, A., & Fleming, S. (2009). A literature review of the individual
and systems factors that contribute to medication errors in nursing practice.
Journal of Nursing Management, 17(6), 679-697.
Briscoe, V. J., & Anema, M. G. (1999). The relationship of academic variables as
predictors of success on the National Council Licensure Examination for
Registered Nurses (NCLEX-RN) in a selected associate degree program.
Journal of the Association of Black Nursing Faculty in Higher Education,
10(4), 80-83.
Bullock, S., & Manias, E. (2002). The educational preparation of undergraduate
nursing students in pharmacology: A survey of lecturers' perceptions and
experiences. Journal of Advanced Nursing, 40(1), 7-16.
Burns, N., & Grove, S. K. (2009). The practice of nursing research: Appraisal,
synthesis and generation of evidence, (6th ed). St. Louis: Saunders Elsevier.
PHARMACOLOGY KNOWLEDGE ACQUISITION 119
Caon, M., & Treagust, D. (1993). Why do some nursing students find their science
courses difficult? Journal of Nursing Education, 32(6), 255–259.
Cebeci, F., Karazeybek, E., Sucu, G., & Kahveci, R. (2015). Nursing students’
medication errors and their opinions on the reasons of errors: A cross-
sectional survey. Journal of Pakistan Medical Association, 65(5), 457-62.
Chan, S. (2010). Applications of andragogy in multi-disciplined teaching and
learning. Journal of Adult Education, 39(2), 25-35.
Cibulka, N. J., & Crane-Wilder, L. (2011). Introducing personal digital assistants to
enhance nursing education in undergraduate and graduate nursing programs.
Journal of Nursing Education, 50(2), 115-118.
Clancy, J., McVicar, A., & Bird, D. (2000). Getting it right? An exploration of issues
relating to the biological sciences in nurse education and nursing practice.
Journal of Advanced Nursing, 32(6), 1522-1532.
Cohen, M. R. (2006). Medication errors. American Pharmacists Association:
Washington DC. Collaborative Institutional Training Initiative (CITI). (2015).
CITI Program, Retrieved from https://www.citiprogram.org/
Collins, A. S., Graves, B. A., Gullette, D., & Edwards, R. (2010). Developing an
interactive microsimulation method in pharmacology. Journal of Nursing
Education, 49(7), 410-413.
Courtenay, M. (1991). A study of the teaching and learning of the biological sciences
in nurse education. Journal of Advanced Nursing, 16(9), 1110–1116.
PHARMACOLOGY KNOWLEDGE ACQUISITION 120
Dilles, T., Vander Stichele, R. R., Van Bortel, L., & Elseviers, M. M. (2011). Nursing
students' pharmacological knowledge and calculation skills: ready for
practice? Nurse Education Today, 31(5), 499-505. doi:
10.1016/j.nedt.2010.08.009.
Eisenhauer, L. A., Hurley, A. C., & Dolan, N. (2007). Nurses’ reported thinking
during medication administration. Journal of Nursing Scholarship, 39(1),
82-87.
Emory, D. J. (2012). Use of standardized mastery content assessments given during
the first year of a baccalaureate nursing program for predicting NCLEX-RN
outcomes. (Doctoral Dissertation) Retrieved from ProQuest, UMI
Dissertations Publishing, 3505834.
Fidalgo-Neto, A. A., Pinto-Alberto, A.V., Calvano-Bonavita, A.G., Soares-Bezerra,
R. J., Berçot, F. F., Lopes, R. M., & Alves, L. A. (2014). PHARMAVIRTUA:
educational software for teaching and learning basic pharmacology. Advanced
Physiology Education, 38, 368-371.
Field, A. (2013). Discovering statistics using IBM SPSS statistics, (4th ed.) Los
Angeles: Sage Publications.
Gee, P. R., Peterson, G.M., Martin, J. L., & Reeve, J. F. (1998). Development and
evaluation of a computer-assisted instruction package in clinical
pharmacology for nursing students. Computers in Nursing, 16(1), 37-44.
Harding, L., & Petrick, T. (2008). Nursing student medication errors: A retrospective
review. Journal of Nursing Education 47(1), 43-47.
PHARMACOLOGY KNOWLEDGE ACQUISITION 121
Henschke J. A., (2011). Considerations regarding the future of andragogy. Adult
Learning, 22(1), 34-37.
Henschke, J. (1998, September). Historical antecedents shaping conceptions of
andragogy: A comparison of sources and roots. Paper presented at the
International Conference on Research in Comparative Andragogy, Radovljica,
Slovenia.
Hewitt, J., Tower, M., & Latimer, S. (2015). An education intervention to improve
nursing students’ understanding of medication safety. Nursing Education in
Practice, 15, 18-22.
Holton, E. F., Swanson, R. A., & Naquin, S. (2001). Andragogy in practice:
Clarifying the andragogical model of adult learning. Performance
Quarterly, 14(1), 118-143.
Honey, M., & Lim, A. G. (2008). Application of pharmacology knowledge in
Medication management by final year undergraduate nursing students.
Contemporary Nurse, 30(1), 12-19.
Institute of Medicine of the National Academies. (1999). To err is human: Building
a safer health system. L. T. Kohn, J. M. Corrigan, M. S. Donaldson, (Eds).
Washington, DC: National Academy Press.
Institute of Medicine of the National Academies (2006). Preventing medication
errors: Quality chasm series. Report Brief July 2006, Retrieved from
http://www.nationalacademies.org/hmd/Reports/2006/Preventing-Medication-
Errors-Quality-Chasm-Series.aspx
PHARMACOLOGY KNOWLEDGE ACQUISITION 122
Ives, G., Hodge, K., Bullock, S., & Marriott, J. (1996). First year RNs’ actual and
self-rated pharmacology knowledge. Australian Journal of Advanced Nursing,
14(1), 13–19.
James, J. T. (2013). A new, evidence-based estimate of patient harms associated with
hospital care. Journal of Patient Safety, 9(3), 122-128.
Jordan, S. (1997). Teaching pharmacology by case study. Nurse Education Today,
17(5), 386-393.
Keohane, C. A., Bane, A. D., Featherstone, E., Hayes, J., Woolf, S., Hurley, A.,
Bates, D. W., Gandhi, T. K., & Poon, E. G. (2008). Quantifying nursing
workflow in medication administration. Journal of Nursing Administration,
38(1), 19-26.
King, R. L. (2004). Nurses’ perceptions of their pharmacology educational needs.
Journal of Advanced Nursing, 45(4), 392-400.
Latter, S., Rycroft-Malone, J., Yerrell, P., & Shaw, D. (2000). Evaluating educational
preparation for a health education role in practice: The case of medication
education. Journal of Advanced Nursing, 32(5), 1282-1290.
Latter, S., Rycroft-Malone, J., Yerrell P., & Shaw, D. (2001). Nurses' educational
preparation for a medication education role: Findings from a national survey.
Nurse Education Today, 21(2), 143-154.
Lim, A. G., & Honey, M. (2006). Integrated undergraduate nursing curriculum for
pharmacology. Nursing Education Practice, 6(3), 163-168.
PHARMACOLOGY KNOWLEDGE ACQUISITION 123
Manias, E., Bullock, S., & Bennett, R. (2000). Formative evaluation of a computer-
Assisted learning program in pharmacology for nursing students. Computers
in Nursing, 18(6), 265-271.
Manias, E., & Bullock, S. (2002a). The educational preparation of undergraduate
nursing students in pharmacology: perceptions and experiences of lecturers
and students. International Journal of Nursing Studies, 39(7), 757-769.
Manias, E., & Bullock, S. (2002b). The educational preparation of undergraduate
Nursing students in pharmacology: clinical nurses' perceptions and
experiences of graduate nurses' medication knowledge. International Journal
of Nursing Studies, 39(8), 773-784. PubMed PMID: 12379295.
McVicar, A., & Clancy, J. (2001). The biosciences and fitness for practice: A time for
review? British Journal of Nursing, 10(21), 1415-1420.
McVicar, A., Clancy, J., & Mayes, N. (2010). An exploratory study of the application
of biosciences in practice, and implications for pre-qualifying education.
Nurse Education Today, 30 (7), 615-622
Meechan, R., Mason, V., & Catling, J. (2011). The impact of an integrated
pharmacology and medicine management curriculum for undergraduate adult
nursing students on the acquisition of applied drug/pharmacology knowledge.
Nursing Education Today, 31(4), 383-389.
Montenery, S. M. (2013). Reinforcing pharmacology content using the medication
mansion. Nurse Educator, 38(3), 96-97.
PHARMACOLOGY KNOWLEDGE ACQUISITION 124
Morrison-Griffiths, S., Snowden, M., & Pirmohamed, M. (2002). Pre-registration
nurse education in pharmacology: Is it adequate for the roles that nurses are
expected to fulfil? Nurse Education Today, 22(6), 447-456.
National Council of State Boards of Nursing (NCSBN). (2015). NCLEX and
Other Exams, FAQs, Exam Development FAQs. Retrieved from
https://www.ncsbn.org/2324.htm
National League for Nursing. (2013). Annual Survey of Schools of Nursing, Fall
2012. Nursing Student Demographics, Percentage of Students Over Age 30
by Program Type, 2012. Retrieved from
www.nln.org/research/slides/index.htm.
Ndosi, M. E., & Newell, R. (2008). Nurses’ knowledge of pharmacology behind the
drugs they commonly administer. Journal of Clinical Nursing, 18(4), 570-
580.
O’Shea, E. (1999). Factors contributing to medication errors: A literature review.
Journal of Clinical Nursing, 8, 496-504.
Page, K., & McKinney, A. A. (2007). Addressing medication errors - The role of
undergraduate nurse education. Nurse Education Today, 27(3), 219-224.
Pappas, C. (2014, April). The Adult Learning Theory Andragogy of Malcolm
Knowles. Adult Education Infographics, e- Learning Infographics: ELearning
Industry. Retrieved from http://elearninginfographics.com/adult-learning-
theory-andragogy-infographic/
PHARMACOLOGY KNOWLEDGE ACQUISITION 125
Paraszczuk, A. M. (2011). The effect of review classes on performance on
comprehensive assessments and the National Council Licensure Examination
of graduating baccalaureate nursing students. (Doctoral Dissertation)
Retrieved from ProQuest, UMI Dissertations Publishing, AAI3497100.
Peterson, C. M., & Ray, C. M. (2013). Andragogy and metagogy: The evolution of
neologisms. Journal of Adult Education, 42(2), 80-85.
Powell, S. S., Canterbury, M. A., & McCoy, D. (1998). Medication administration:
Does teaching method really matter? Journal of Nursing Education, 37(6),
281-283.
Robinson, J. E. (1987). Separate or integrated pharmacology content? Nursing
Outlook, 35(4), 185–188.
Sears, K., Goldsworthy, S., & Goodman, W. M. (2010). The relationship
between simulation in nursing education and medication safety.
Journal of Nursing Education, 49(1), 52-55.
Silvestri, L. A. (2010). Self-efficacy and the predictors for NCLEX-RN (RTM) success
for baccalaureate nursing students. (Doctoral Dissertation) Retrieved from
ProQuest, UMI Dissertations Publishing, AAI3412401.
Simonsen, B.O., Daehlin, G.K., Johansson, I., & Farup, P. G. (2014). Differences in
medication knowledge and risk of errors between graduating nursing students
and working registered nurses. BioMed Central Health Services, 21(14), 580.
doi: 10.1186/s12913-014-0580-7.
PHARMACOLOGY KNOWLEDGE ACQUISITION 126
Smith, J., & Crawford, L. (2003). Medication errors and difficulty in first patient
assignments of newly licensed nurses. Journal of Nursing Administration
Healthcare Law, Ethics and Regulation, 5(3), 65–67.
Steunkel, D. (2006). At-risk students: Do theory grades + standardized
examinations = success? Nurse Educator, 31(5), 207–212.
Strayer, R. M., & Beitz, J. M. (2010). Factors influencing pharmacology knowledge
acquisition in traditional versus nontraditional baccalaureate nursing students.
Journal of Professional Nursing, 26(5), 301-308. doi:
10.1016/j.profnurs.2010.02.001.
Sulosaari, V., Suhonen, R., & Leino-Kilpi, H. (2011). An integrative review of the
literature on registered nurses' medication competence. Journal of Clinical
Nursing, 20(3-4), 464-478.
Tang, F., Sheu, S-J., Yu, S., Wei, I-L., & Chen, C-H. (2007). Nurses relate the
contributing factors involved in medication errors. Journal of Clinical
Nursing, 16, 447-57.
Thompson, T. L., & Bonnel, W.B. (2008). Integration of high-fidelity patient
simulation in an undergraduate pharmacology course. Journal of Nursing
Education, 47(11), 518-521.
Thornton, T. (1997). Attitudes towards the relevance of biological, behavioral and
social sciences in nursing education. Journal of Advanced Nursing, 26(1),
180–186.
PHARMACOLOGY KNOWLEDGE ACQUISITION 127
Trnobranski, P. H. (1993). Biological sciences and the nursing curriculum: A
challenge for educationalists. Journal of Advanced Nursing, 18(3), 493–499.
Tse, M. M., & Lo, L. W. (2008). A web-based e-learning course: Integration of
pathophysiology into pharmacology. Telemedicine and e-Health, 14(9), 919-
924.
Ukpabi, C. (2008). Predictors of successful nursing education outcomes: A study of
the North Carolina Central University's nursing program. Educational
Research Quarterly, 32(2), 30–40.
United States Department of Education, National Center for Education Statistics
(2002). Nontraditional Undergraduates (NCES 2002–012). Retrieved from
http://nces.ed.gov/Pubs2002/2002012.pdf
United States Government, Executive Offices, Office of Management and Budget.
(1997). Revisions to the Standards for the Classification of Federal Data on
Race and Ethnicity (Report). Federal Register Notice. Retrieved from
https://www.whitehouse.gov/omb/fedreg_1997standards
United States Department of Health and Human Services, Food and Drug
Administration (FDA). (2013). Drug Approvals and Databases. Retrieved
from http://www.fda.gov/Drugs/InformationOnDrugs/default.htm.
United States Department of Health and Human Services, Health Resources and
Services Administration. (2010). The Registered Nurse Population, Findings
from the 2008 National Sample Survey of Registered Nurses, Retrieved from
hpr.hrsa.gov/healthworkforce/rnsurveys/rnsurveyfinal.pdf
PHARMACOLOGY KNOWLEDGE ACQUISITION 128
van den Bemt P. M., Egberts, A. C., & Lenderink A. W. (2000). Risk factors for the
development of adverse drug events in hospitalised patients. Pharmaceutical
World Science 22(2), 62– 66.
Vana, K. D., & Silva, G. E. (2014). Evaluating the use of a simulated electronic
health record and online drug reference in a case study to enhance nursing
students’ understanding of pharmacologic concepts and resources. Nurse
Educator, 39(4), 160-165.
Vana, K. D., Silva, G. E., Muzyka, D., & Hirani, L. M. (2011). Effectiveness of an
audience response system in teaching pharmacology to baccalaureate nursing
students. Computer Informatics Nursing, 29(6), 326-34; quiz 335-336. doi:
10.1097/NCN.0b013e3181f9dd9c.
Wittman-Price, R. A., Kennedy, L. D., & Goodwin, C. (2012). Use of personal
phones by senior nursing students to access health care information during
clinical education: Staff nurses’ and students’ perceptions. Journal of Nursing
Education, 51(11), 642-646.
Wolf, Z. R., Hicks, R., & Serembus, J. F. (2006). Characteristics of medication errors
made by students during the administration phase: A descriptive study.
Journal of Professional Nursing, 22(1), 39-51.
Yeu-Hui, C., & Chiung-Wen, T. (2013). Enhancing nursing students’ medication
knowledge: The effect of learning materials delivered by short message
service. Computers and Education, 61, 168-175.

PHARMACOLOGY KNOWLEDGE ACQUISITION 129
Zellner, K., Boerst, C., & Semling, K. (2003). Teaching separate versus integrated
pharmacology content. Western Journal of Nursing Research, 25(3), 338-348.
PHARMACOLOGY KNOWLEDGE ACQUISITION 130
Appendix A
Notice of Study
NOTICE OF A RESEARCH STUDY AT GOOD SAMARITAN COLLEGE
OF NURSING AND HEALTH SCIENCE
Nursing 202 students are invited to participate in a research study entitled:
The Relationship of Selected Academic, Nonacademic, and Clinical Variables
as Factors Influencing Pharmacy Knowledge Acquisition
in Associate Degree Pre-licensure Nursing Students
This purpose of this study is to examine the following:
What is the relationship between student academic variables and pharmacology knowledge?
What is the relationship between student non-academic variables and pharmacology
knowledge?
What is the relationship between clinical experience opportunities for medication
administration and decision-making and pharmacology knowledge?
When: Thursday, March 17, 2016 (following class)
Where: NUR 202 Classroom 869.7&8
Who: Study Investigator:
Diane M. Stauffer, MSN, RN, CNE
Associate Professor, Good Samaritan College
Please consider participating in this important study - student participation in the study is
voluntary. Completion of study questionnaires will take approximately 10 minutes. For
questions regarding this study, please contact Professor Stauffer at 513-862-3717.
REFRESHMENTS WILL BE PROVIDED
PHARMACOLOGY KNOWLEDGE ACQUISITION 131
Appendix B
Script for Participant Recruitment
Following introduction of the faculty member/principal investigator…
As a student in the process of completing a doctoral research project, I am very
interested in studying factors that may affect nursing students’ ability to learn pharmacology.
You are invited to participate in a research study entitled, “The Relationship of Selected
Academic, Nonacademic, and Clinical Variables as Factors Influencing Pharmacy
Knowledge Acquisition in Associate Degree Pre-licensure Nursing Students.” The purpose of
this study is to examine the relationship of selected student variables to pharmacology
knowledge acquisition as demonstrated by the ATI pharmacology assessment. A second
purpose of the study is to determine if there is any correlation between student perceptions of
clinical experience opportunities for medication management and scores on the ATI
pharmacology assessment.
As a senior nursing student who has successfully completed all clinical rotations
prior to role transition, you are eligible to participate in the study. Participation in this study
is voluntary and will have no effect on your course grade, progression to role transition or
graduation from the program. All students will be given a packet with three forms to
complete. The first form is an informed consent to participate in the study. The second form is
for demographic information related to selected student variables. The third form is a brief
survey questionnaire regarding your clinical experience opportunities with medication
management. It will take approximately 5-10 minutes for you to complete the forms.
Some data for the study will also be obtained through college records including age,
gender, ethnicity and grade point average. Pharmacology Assessment scores will be obtained
through ATI testing reports. In order to achieve the purpose of the study, student variables
must be matched with corresponding ATI pharmacology scores. This matching will be
completed with the use of your student identification number, but the investigator will not be
able to view any student names. Once the data has been collected and entered, all student
identification numbers will be removed from the study data file, and all study results will be
reported only as aggregate or group data.
If you agree to participate in this study, please complete all the forms in the study
packet, return them to the envelope, and place the envelope in the collection box at the front
of the room. If you do not wish to participate in the study, you may simply return the blank
forms to the envelope, and place the envelope in the same collection box.
Are there any questions about this study?
Thank you very much for your time and consideration to participate in this study.
Please help yourself to refreshments that have been provided. If you have any further
questions or concerns at a later time, this study investigator will be available to answer your
questions.
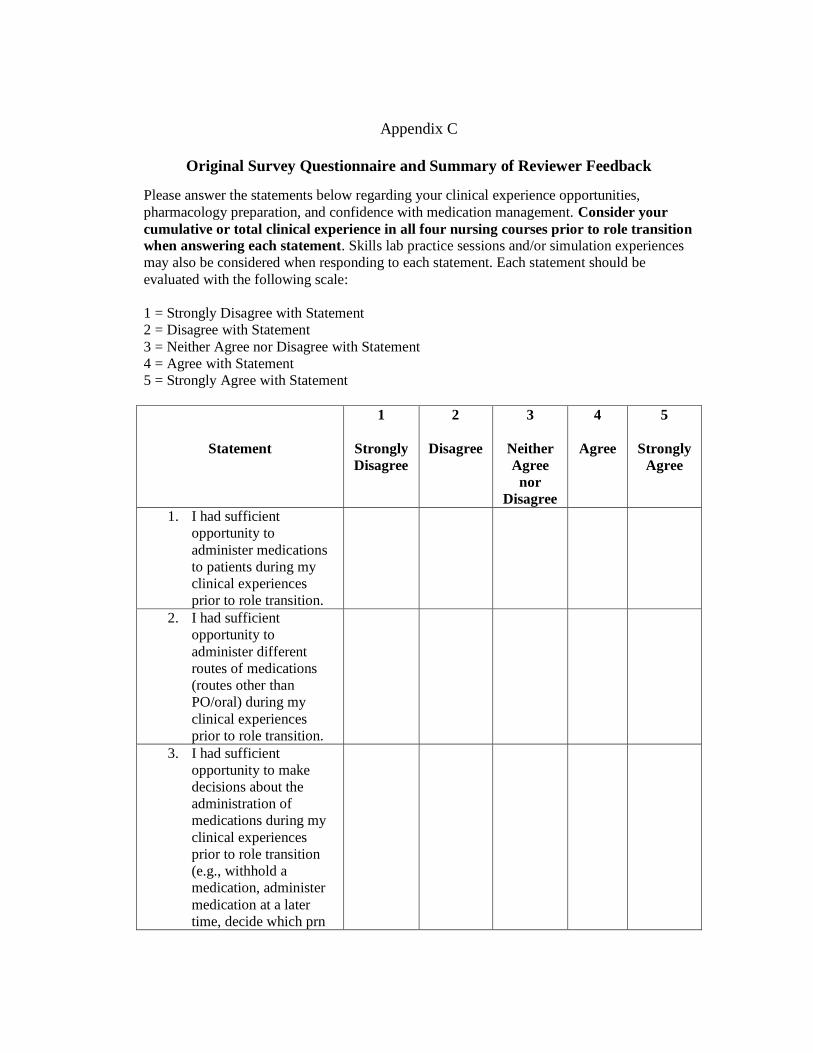
Appendix C
Original Survey Questionnaire and Summary of Reviewer Feedback
Please answer the statements below regarding your clinical experience opportunities,
pharmacology preparation, and confidence with medication management. Consider your
cumulative or total clinical experience in all four nursing courses prior to role transition
when answering each statement. Skills lab practice sessions and/or simulation experiences
may also be considered when responding to each statement. Each statement should be
evaluated with the following scale:
1 = Strongly Disagree with Statement
2 = Disagree with Statement
3 = Neither Agree nor Disagree with Statement
4 = Agree with Statement
5 = Strongly Agree with Statement
Statement
1
Strongly
Disagree
2
Disagree
3
Neither
Agree
nor
Disagree
4
Agree
5
Strongly
Agree
1. I had sufficient
opportunity to
administer medications
to patients during my
clinical experiences
prior to role transition.
2. I had sufficient
opportunity to
administer different
routes of medications
(routes other than
PO/oral) during my
clinical experiences
prior to role transition.
3. I had sufficient
opportunity to make
decisions about the
administration of
medications during my
clinical experiences
prior to role transition
(e.g., withhold a
medication, administer
medication at a later
time, decide which prn
PHARMACOLOGY KNOWLEDGE ACQUISITION 133
medication to give,
decide on the dosage
when a range is ordered,
question a medication
order, consult with the
RN/MD or Pharmacist
on an issue or concern).
4. I had sufficient
opportunity to teach
patients about their
medications during my
clinical experiences
prior to role transition.
5. I feel confident in my
ability to accurately and
safely administer
medications to patients.
6. I feel confident in my
knowledge of
pharmacology as a
beginning clinician in
terms of how drugs
work, side effects,
nursing implications,
and how to evaluate if a
medication is effective.
ORIGINAL Study Survey Tool
SUMMARY OF FEEDBACK/RESPONSES FROM SURVEY REVIEWERS
GRADUATE STUDENTS AND FACULTY: Please consider the following in your
evaluation of the statements that have been included in the tool:
1. Are the instructions for completing the survey tool well-defined/distinct/clear?
100% of responses indicated that the instructions were clear.
Comment: “Examples that are included make the statements very clear for the
reader. I am able to read these statements and know exactly what aspect of
medication administration it is referring to.”
2. Does each statement relate to the purpose of the study?
100% of responses answered “Yes” to this question
3. Is each statement applicable to current pharmacology practice/expectations during
student clinical experiences? (Consider cumulative experience.)
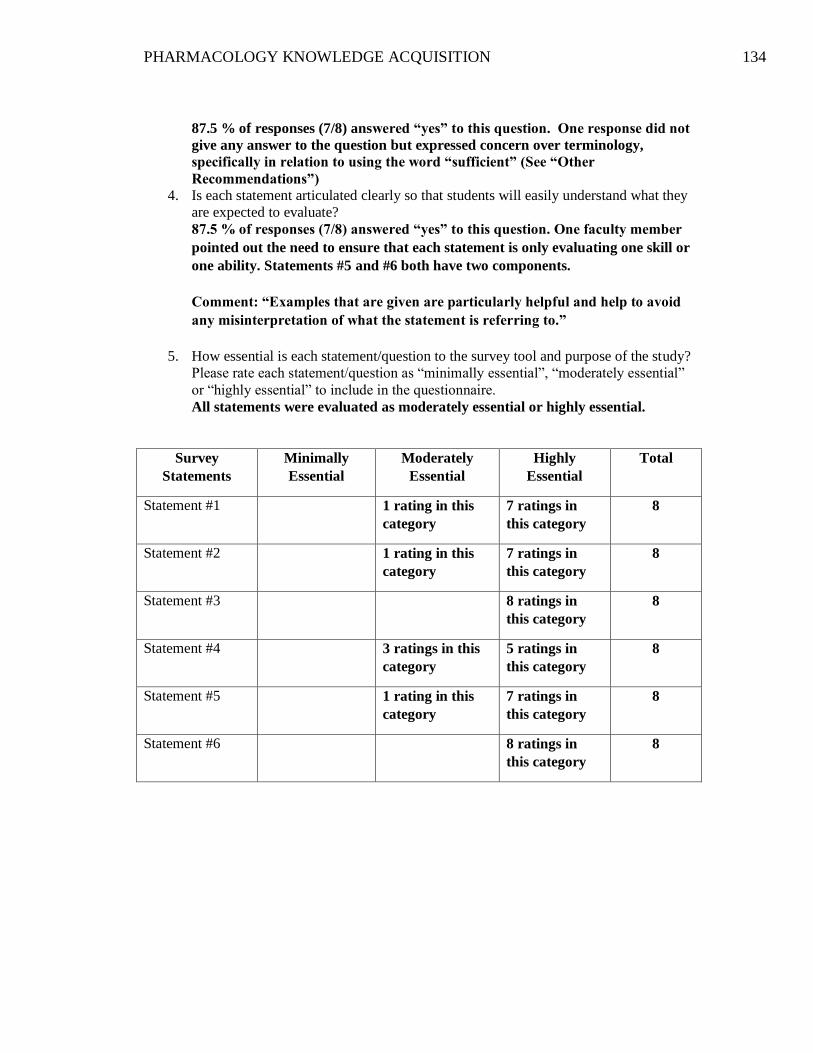
PHARMACOLOGY KNOWLEDGE ACQUISITION 134
87.5 % of responses (7/8) answered “yes” to this question. One response did not
give any answer to the question but expressed concern over terminology,
specifically in relation to using the word “sufficient” (See “Other
Recommendations”)
4. Is each statement articulated clearly so that students will easily understand what they
are expected to evaluate?
87.5 % of responses (7/8) answered “yes” to this question. One faculty member
pointed out the need to ensure that each statement is only evaluating one skill or
one ability. Statements #5 and #6 both have two components.
Comment: “Examples that are given are particularly helpful and help to avoid
any misinterpretation of what the statement is referring to.”
5. How essential is each statement/question to the survey tool and purpose of the study?
Please rate each statement/question as “minimally essential”, “moderately essential”
or “highly essential” to include in the questionnaire.
All statements were evaluated as moderately essential or highly essential.
Survey
Statements
Minimally
Essential
Moderately
Essential
Highly
Essential
Total
Statement #1 1 rating in this
category
7 ratings in
this category
8
Statement #2 1 rating in this
category
7 ratings in
this category
8
Statement #3 8 ratings in
this category
8
Statement #4 3 ratings in this
category
5 ratings in
this category
8
Statement #5 1 rating in this
category
7 ratings in
this category
8
Statement #6 8 ratings in
this category
8
PHARMACOLOGY KNOWLEDGE ACQUISITION 135
ORIGINAL Study Survey Tool
SUMMARY OF FEEDBACK/RESPONSES FROM SURVEY REVIEWERS
6. Are there statements/questions that you believe to be essential that are NOT included
in the survey tool?
Comments or suggested additional statements:
1) Consider adding a statement regarding experience with different
classifications of medications.
2) Consider asking about the impact of the Chemistry II course which
incorporates basic pharmacological principles and some drug classifications.
3) Consider asking if the student ever experienced a medication error or had
difficulty with skill competencies related to medication administration (e.g.
was required to repeat a return demonstration for a competency).
4) Should there be a statement that asks about how students perceive
consistency (or inconsistency) with faculty expectations of medication
administration? This consistency or lack of consistency may affect the
number of opportunities and confidence.
5) If pharmacology preparation is being assessed (as in the directions and
statement #5 and #6), there should be a question regarding this.
7. Other Recommendations:
1) There are a variety of definitions for the word “sufficient”. Should this be
quantified?
2) Add category of “Unsure” to Likert scale.
3) Change the word, “feel” in statements #5 and #6 to “am”.
4) Change the statement in the directions to three courses since students do not
actually give medications in the clinical area until the second nursing course.
5) Will the student understand the terminology, “sufficient”? Other options
would be “Adequate” or “Satisfactory”. Does this need to be clarified on the
tool?
6) Do you want to assess if the student feels “confident” or “competent”?
Students often feel confident about something but may not be competent.
7) Should statement #3 say RN/Health Care Provider instead of RN/MD?
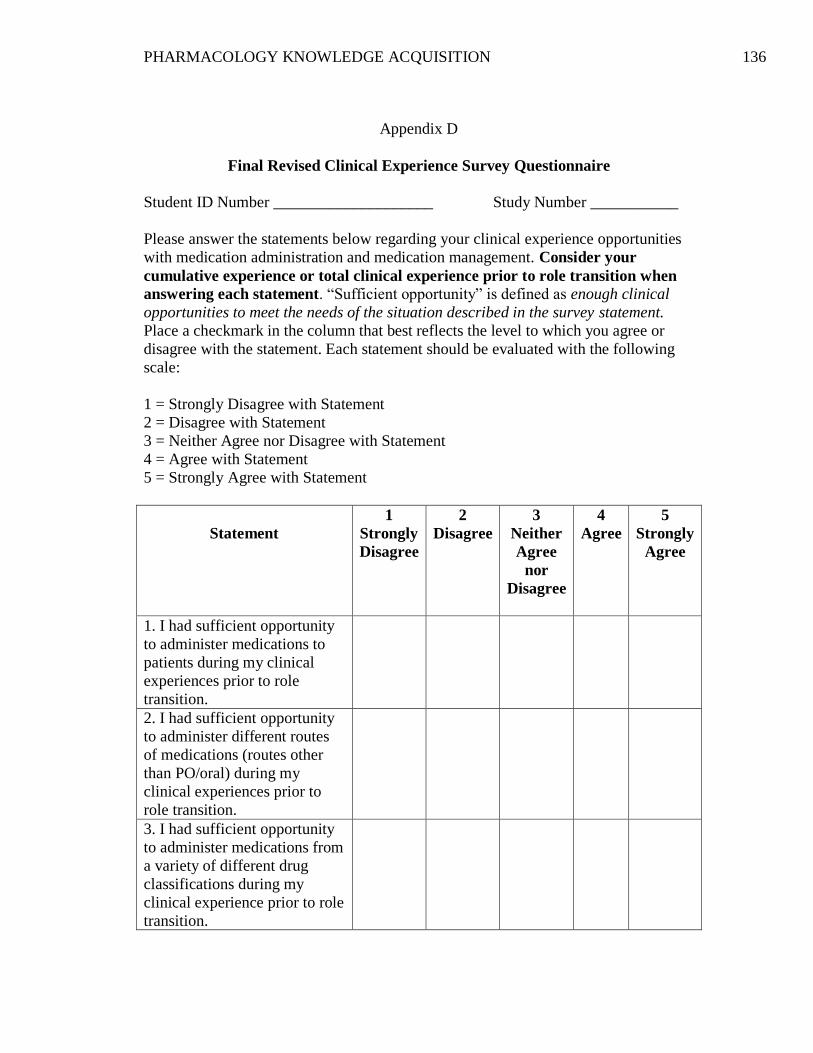
PHARMACOLOGY KNOWLEDGE ACQUISITION 136
Appendix D
Final Revised Clinical Experience Survey Questionnaire
Student ID Number ____________________ Study Number ___________
Please answer the statements below regarding your clinical experience opportunities
with medication administration and medication management. Consider your
cumulative experience or total clinical experience prior to role transition when
answering each statement. “Sufficient opportunity” is defined as enough clinical
opportunities to meet the needs of the situation described in the survey statement.
Place a checkmark in the column that best reflects the level to which you agree or
disagree with the statement. Each statement should be evaluated with the following
scale:
1 = Strongly Disagree with Statement
2 = Disagree with Statement
3 = Neither Agree nor Disagree with Statement
4 = Agree with Statement
5 = Strongly Agree with Statement
Statement
1
Strongly
Disagree
2
Disagree
3
Neither
Agree
nor
Disagree
4
Agree
5
Strongly
Agree
1. I had sufficient opportunity
to administer medications to
patients during my clinical
experiences prior to role
transition.
2. I had sufficient opportunity
to administer different routes
of medications (routes other
than PO/oral) during my
clinical experiences prior to
role transition.
3. I had sufficient opportunity
to administer medications from
a variety of different drug
classifications during my
clinical experience prior to role
transition.
PHARMACOLOGY KNOWLEDGE ACQUISITION 137
4. I had sufficient opportunity to make decisions about the
management of medications
during my clinical experiences
prior to role transition (e.g.,
withhold a medication,
administer a medication at a
different time, decide which
prn medication to give, decide
on the dosage when a range is
ordered, question a medication
order, consult with the health
care provider or pharmacist on
a concern.
5. I had sufficient opportunity
to teach patients about their
medications during my clinical
experiences prior to role
transition.
6. My clinical experience
opportunities were sufficient to
achieve confidence in my
ability to safely manage
medication therapy for
patients.
PHARMACOLOGY KNOWLEDGE ACQUISITION 138
Appendix E
Demographic Information Form
Student ID Number ____________________ Study Number ___________
Please answer the following questions. Mark an “X” beside the answer that is most
accurate.
1. Do you have any previous or current health care experience involving direct
patient care other than that acquired during nursing school as a student?
YES __________
NO __________
2. Are you currently employed? (includes any type of work for which you are
employed).
YES __________
NO __________
If YES, how many hours per week on average do you work?
__________ hours/week
3. Do you have any of the following family responsibilities?
a. Financial responsibility as head of household
YES __________
NO __________
b. Responsibility for dependent children
YES __________
NO __________
c. Responsibility as a caregiver (e.g., aging parent, family member, friend or
significant other with health care issues)
YES __________
NO _________





















