PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS
16
Br. J. Anaesth. (1986), 58, 701-716 PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS B. G. COVINO Local anaesthetic drugs are chemical compounds the primary pharmacological activity of which involves inhibition of the excitation—conduction process in peripheral nerves. In common with many of the early therapeutic agents, the first local anaesthetic agent, cocaine, was a naturally occurring alkaloid that had been isolated from the leaves of the Erythroxylin coca bush which was indigenous to South America. The introduction of cocaine to clinical practice has been attributed to Roller, who described the topical anaesthetic properties of this agent for ophthalmological use in 1884. However, both the anaesthetic and QMS stimulant activities of cocaine were recognized by the South American natives for many years before Roller's presentation. Procaine was synthesized by Einhorn in 1905 and represented the first injectable agent of clinical value for the production of local anaesthesia. Following the introduction of procaine, numerous compounds of similar chemi- cal structure were developed. Amethocaine (tetra- caine, USP) and chloroprocaine are the procaine- like agents which have persisted to this day, as clinically useful local anaesthetics. In 1943, Lofgren synthesized lignocaine (lido- caine, USP) which represented a new chemical class of local anaesthetic compounds. Whereas the procaine-like drugs are ester derivatives of para-aminobenzoic acid, lignocaine is an amide derivative of diethylamino acetic acid. Since the advent of lignocaine, many other amide substances such as mepivacaine, prilocaine, bupivacaine and etidocaine have been introduced to clinical practice as local anaesthetic agents each with its own pharmacological profile. STRUCTURE-ACTIVITY RELATIONSHIP OF LOCAL ANAESTHETIC AGENTS Chemical compounds that demonstrate local anaesthetic activity usually possess an aromatic BENJAMIN G. COVINO, PH.D. , MJ)., Departments of Anesthesia, Harvard Medical School and Brigham and Women's Hospital, 75 Francis Street, Boston, Massachusetts 02115, U.S.A. and an amine group separated by an intermediate chain (table I). The clinically useful local anaesthetic agents fall essentially into one of two chemically distinct groups. Those agents which possess an ester link between the aromatic portion and the intermediate chain are referred to as amino esters and include procaine, chloroprocaine and amethocaine. Local anaesthetics with an amide link between the aromatic end and the intermediate chain are referred to as amino amides and include lignocaine, mepivacaine, prilocaine, bupivacaine and etidocaine. The basic difference between the ester and amide compounds resides in their chemical stability. Esters are hydrolysed easily and are relatively unstable in solution. On the other hand, amides are much more stable. In the body, the amino esters are hydrolysed in plasma by the enzyme cholinesterase, whereas the amide com- pounds undergo enzymatic degradation in the liver. Para-aminobenzoic acid is one of the metabolites formed from the hydrolysis of ester type compounds, and this substance is capable of inducing allergic type reactions in a small percentage of patients. The amino amides, how- ever, are not metabolized to para-aminobenzoic acid and reports of allergic reactions to these agents are extremely rare. The properties of the various local anaesthetic agents which are clinically important include potency, speed of onset and duration of anaesthetic activity. The clinical profile of the individual agents is essentially determined by the physico- chemical characteristics of the various compounds, which in turn are dependent on their chemical structure. The physicochemical properties which influence anaesthetic activity are lipid solubility, protein binding, and pK a . Minor changes in molecular structure have dramatic effects on these properties (table I). Potency Lipid solubility appears to be the primary determinant of intrinsic anaesthetic potency. Consideration of the biochemical composition of the nerve membrane provides a logical explanation Downloaded from https://academic.oup.com/bja/article/58/7/701/279293 by guest on 27 May 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS

Br. J. Anaesth. (1986), 58, 701-716
PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS
B. G. COVINO
Local anaesthetic drugs are chemical compoundsthe primary pharmacological activity of whichinvolves inhibition of the excitation—conductionprocess in peripheral nerves. In common withmany of the early therapeutic agents, the first localanaesthetic agent, cocaine, was a naturallyoccurring alkaloid that had been isolated from theleaves of the Erythroxylin coca bush which wasindigenous to South America. The introduction ofcocaine to clinical practice has been attributed toRoller, who described the topical anaestheticproperties of this agent for ophthalmological usein 1884. However, both the anaesthetic and QMSstimulant activities of cocaine were recognized bythe South American natives for many years beforeRoller's presentation. Procaine was synthesizedby Einhorn in 1905 and represented the firstinjectable agent of clinical value for the productionof local anaesthesia. Following the introduction ofprocaine, numerous compounds of similar chemi-cal structure were developed. Amethocaine (tetra-caine, USP) and chloroprocaine are the procaine-like agents which have persisted to this day, asclinically useful local anaesthetics.
In 1943, Lofgren synthesized lignocaine (lido-caine, USP) which represented a new chemicalclass of local anaesthetic compounds. Whereas theprocaine-like drugs are ester derivatives ofpara-aminobenzoic acid, lignocaine is an amidederivative of diethylamino acetic acid. Since theadvent of lignocaine, many other amide substancessuch as mepivacaine, prilocaine, bupivacaine andetidocaine have been introduced to clinicalpractice as local anaesthetic agents each with itsown pharmacological profile.
STRUCTURE-ACTIVITY RELATIONSHIP OF LOCALANAESTHETIC AGENTS
Chemical compounds that demonstrate localanaesthetic activity usually possess an aromatic
BENJAMIN G. COVINO, PH.D. , MJ). , Departments of Anesthesia,Harvard Medical School and Brigham and Women's Hospital,75 Francis Street, Boston, Massachusetts 02115, U.S.A.
and an amine group separated by an intermediatechain (table I). The clinically useful localanaesthetic agents fall essentially into one of twochemically distinct groups. Those agents whichpossess an ester link between the aromatic portionand the intermediate chain are referred to as aminoesters and include procaine, chloroprocaine andamethocaine. Local anaesthetics with an amidelink between the aromatic end and the intermediatechain are referred to as amino amides and includelignocaine, mepivacaine, prilocaine, bupivacaineand etidocaine. The basic difference between theester and amide compounds resides in theirchemical stability. Esters are hydrolysed easily andare relatively unstable in solution. On the otherhand, amides are much more stable. In the body,the amino esters are hydrolysed in plasma by theenzyme cholinesterase, whereas the amide com-pounds undergo enzymatic degradation in theliver. Para-aminobenzoic acid is one of themetabolites formed from the hydrolysis of estertype compounds, and this substance is capable ofinducing allergic type reactions in a smallpercentage of patients. The amino amides, how-ever, are not metabolized to para-aminobenzoicacid and reports of allergic reactions to theseagents are extremely rare.
The properties of the various local anaestheticagents which are clinically important includepotency, speed of onset and duration of anaestheticactivity. The clinical profile of the individualagents is essentially determined by the physico-chemical characteristics of the various compounds,which in turn are dependent on their chemicalstructure. The physicochemical properties whichinfluence anaesthetic activity are lipid solubility,protein binding, and pKa. Minor changes inmolecular structure have dramatic effects on theseproperties (table I).
Potency
Lipid solubility appears to be the primarydeterminant of intrinsic anaesthetic potency.Consideration of the biochemical composition ofthe nerve membrane provides a logical explanation
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
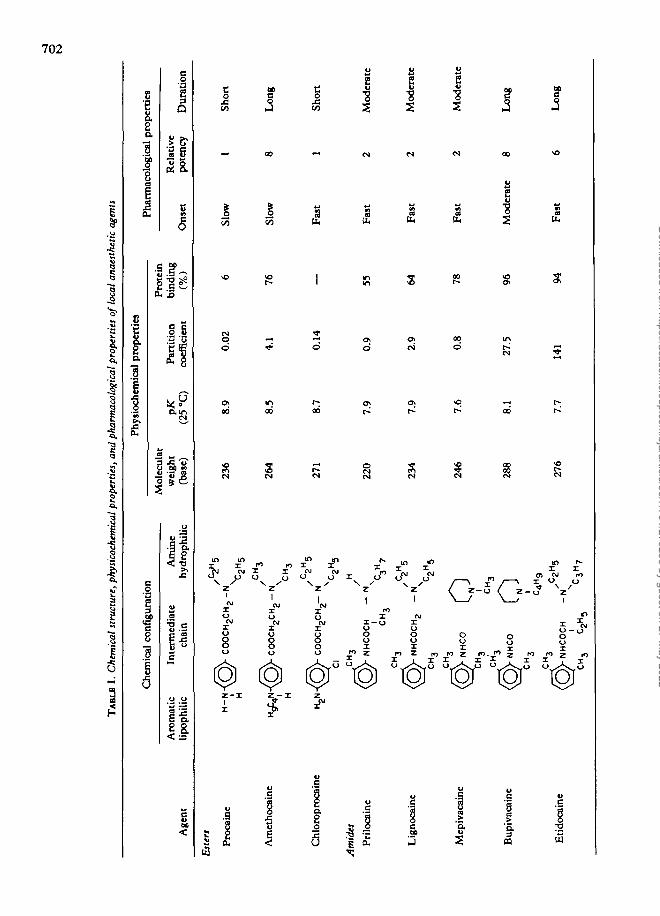
TABL
E I.
Che
mic
al s
truc
ture
, phy
sico
chem
ical
pro
pert
ies,
and
pha
rmac
olog
ical
pro
pert
ies
of l
ocal
ana
esth
etic
age
nts
Age
nt
Che
mic
al c
onfi
gura
tion
Phy
gioc
hem
icaJ
pro
pert
ies
Pha
rmac
olog
ical
pro
pert
ies
Mol
ecul
ar
Pro
tein
Aro
mat
ic
Inte
rmed
iate
A
min
e w
eigh
t pK
P
arti
tion
bi
ndin
g R
elat
ive
lipop
hilic
ch
ain
hydr
ophi
lic
(bas
e)
(25
°C)
coef
fici
ent
(%)
Ons
et
pote
ncy
Dur
atio
n
Est
ers
Pro
cain
e
Am
etho
cain
e
Chl
orop
roca
ine
Am
ides
Pri
loca
ine
Lig
noca
ine
Mep
ivac
aine
Bup
ivac
aine
Eti
doca
ine
H-N
- i H
CO
OC
H2C
H2
-N
CH
,
•CO
OC
Hg
CH
g-N
CH
3
• C
OO
CH
,CH
--
N
Cl
.CH
,
•NH
CO
CH
—
NI
VC
H,
^C
2Hg
H C,H
,
CH
,
(Q)-
NH
CO
CH
., -N
CH
3
CH
,
CH
,
C2
H5
• N
HC
O
o CH
, oC
H,
CH
,
N C4H
9
•NH
CO
CH
-
N
236
264
271
220
234
246
288
276
8.9
8.5
8.7
7.9
7.9
7.6
0.02
4.1
0.14
0.9
2.9
0.8
8.1
27.5
7.7
141
76 55 64 78 96 94
Slow
Fas
t
Fas
t
Fas
t
Fas
t
1 Sh
ort
Slow
8
Lon
g
1 Sh
ort
Mod
erat
e
Mod
erat
e
Mod
erat
e
Mod
erat
e 8
Lon
g
Fas
t6
Lon
g
CH
,C
3H
3n7
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS 703
141D
27.5
2.9
0.9
0.8
Etidocaine
Bupivacaine
Lignocaine
PrUocaine
Mepivacaine
141.0
27.5
2.9
0.9
0.8
2 4in vitro Relative
Etidocaine
Bupivacaine
| Lignocaine
I Pribcaine
| Mepivacainei i
6 8potency
1 - 2 3 4in vivo Relative potency
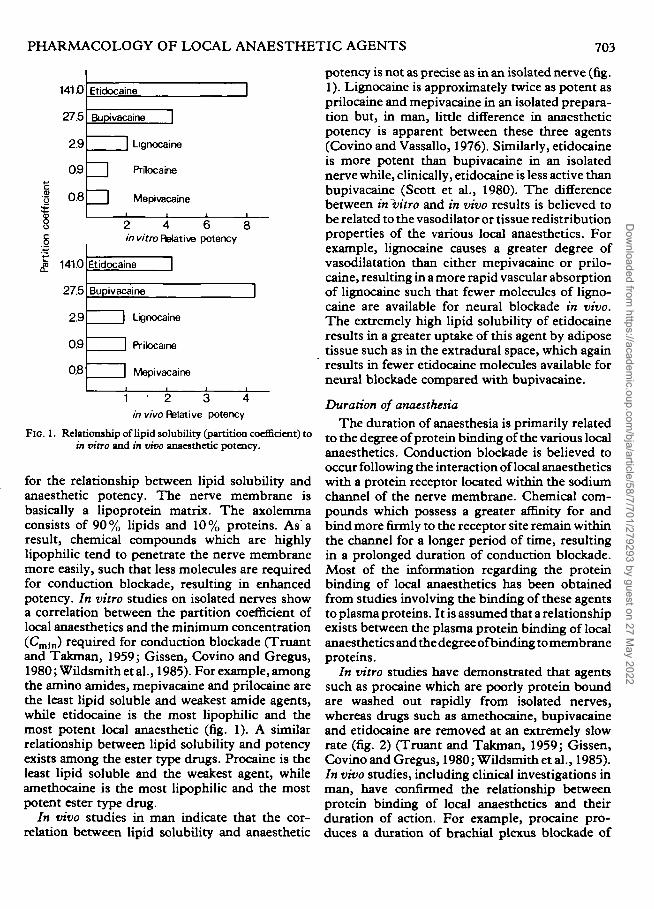
FIG. 1. Relationship of lipid solubility (partition coefficient) toin vitro and in vivo anaesthetic potency.
for the relationship between lipid solubility andanaesthetic potency. The nerve membrane isbasically a lipoprotein matrix. The axolemmaconsists of 90% lipids and 10% proteins. As aresult, chemical compounds which are highlylipophilic tend to penetrate the nerve membranemore easily, such that less molecules are requiredfor conduction blockade, resulting in enhancedpotency. In vitro studies on isolated nerves showa correlation between the partition coefficient oflocal anaesthetics and the minimum concentration(Cmln) required for conduction blockade (Truantand Takman, 1959; Gissen, Covino and Gregus,1980; Wildsmith et al., 1985). For example, amongthe amino amides, mepivacaine and prilocaine arethe least lipid soluble and weakest amide agents,while etidocaine is the most lipophilic and themost potent local anaesthetic (fig. 1). A similarrelationship between lipid solubility and potencyexists among the ester type drugs. Procaine is theleast lipid soluble and the weakest agent, whileamethocaine is the most lipophilic and the mostpotent ester type drug.
In vivo studies in man indicate that the cor-relation between lipid solubility and anaesthetic
potency is not as precise as in an isolated nerve (fig.1). Lignocaine is approximately twice as potent asprilocaine and mepivacaine in an isolated prepara-tion but, in man, little difference in anaestheticpotency is apparent between these three agents(Covino and Vassallo, 1976). Similarly, etidocaineis more potent than bupivacaine in an isolatednerve while, clinically, etidocaine is less active thanbupivacaine (Scott et al., 1980). The differencebetween in vitro and in vivo results is believed tobe related to the vasodilator or tissue redistributionproperties of the various local anaesthetics. Forexample, lignocaine causes a greater degree ofvasodilatation than either mepivacaine or prilo-caine, resulting in a more rapid vascular absorptionof lignocaine such that fewer molecules of ligno-caine are available for neural blockade in vivo.The extremely high lipid solubility of etidocaineresults in a greater uptake of this agent by adiposetissue such as in the extradural space, which againresults in fewer etidocaine molecules available forneural blockade compared with bupivacaine.
Duration of anaesthesia
The duration of anaesthesia is primarily relatedto the degree of protein binding of the various localanaesthetics. Conduction blockade is believed tooccur following the interaction of local anaestheticswith a protein receptor located within the sodiumchannel of the nerve membrane. Chemical com-pounds which possess a greater affinity for andbind more firmly to the receptor site remain withinthe channel for a longer period of time, resultingin a prolonged duration of conduction blockade.Most of the information regarding the proteinbinding of local anaesthetics has been obtainedfrom studies involving the binding of these agentsto plasma proteins. It is assumed that a relationshipexists between the plasma protein binding of localanaesthetics and the degree ofbinding to membraneproteins.
In vitro studies have demonstrated that agentssuch as procaine which are poorly protein boundare washed out rapidly from isolated nerves,whereas drugs such as amethocaine, bupivacaineand etidocaine are removed at an extremely slowrate (fig. 2) (Truant and Takman, 1959; Gissen,Covino and Gregus, 1980; Wildsmith et al., 1985).In vivo studies, including clinical investigations inman, have confirmed the relationship betweenprotein binding of local anaesthetics and theirduration of action. For example, procaine pro-duces a duration of brachial plexus blockade of
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
704 BRITISH JOURNAL OF ANAESTHESIA
120r
E 80•o
15c
sI 4°
20
0
©•Pnxane® •Prilocaino
•Amethocane• Buptvacaine
20 40 60
Washout (min)
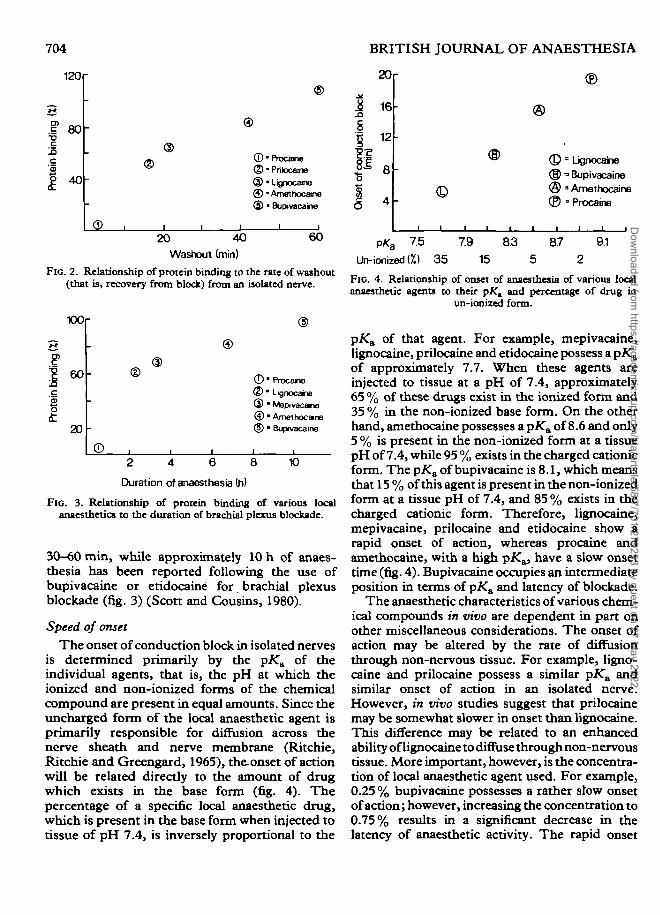
FIG. 2. Relationship of protein binding to the rate of washout(that is, recovery from block) from an isolated nerve.
100r
60
20
©
©<D
©•Procame©•LignocaiTe® • Mepivacane©•Amethocane(?) • Bupivacaine
©2 4 6 8
Duration of anaesthesia (h)
10
FIG. 3. Relationship of protein binding of various localanaesthetics to the duration of brachial plexus blockade.
30-60 min, while approximately 10 h of anaes-thesia has been reported following the use ofbupivacaine or etidocaine for brachial plexusblockade (fig. 3) (Scott and Cousins, 1980).
Speed of onset
The onset of conduction block in isolated nervesis determined primarily by the pK& of theindividual agents, that is, the pH at which theionized and non-ionized forms of the chemicalcompound are present in equal amounts. Since theuncharged form of the local anaesthetic agent isprimarily responsible for diffusion across thenerve sheath and nerve membrane (Ritchie,Ritchie and Greengard, 1965), th& onset of actionwill be related directly to the amount of drugwhich exists in the base form (fig. 4). Thepercentage of a specific local anaesthetic drug,which is present in the base form when injected totissue of pH 7.4, is inversely proportional to the
®
© = Lignocaine® "Bupivacaine@ ' Amethocane® ° Procaine
p*a 75 7.9
Un-tonized {%) 35 15
8.7 9.1
5 2
FIG. 4. Relationship of onset of anaesthesia of various localanaesthetic agents to their pAT, and percentage of drug in
un-ionized form.
pKa of that agent. For example, mepivacaine,lignocaine, prilocaine and etidocaine possess a pK&of approximately 7.7. When these agents areinjected to tissue at a pH of 7.4, approximately65 % of these drugs exist in the ionized form and35 % in the non-ionized base form. On the otherhand, amethocaine possesses a pKa of 8.6 and only5 % is present in the non-ionized form at a tissuepH of 7.4, while 95 % exists in the charged cationicform. The pKa of bupivacaine is 8.1, which meansthat 15 % of this agent is present in the non-ionizedform at a tissue pH of 7.4, and 85 % exists in thecharged cationic form. Therefore, lignocaine,mepivacaine, prilocaine and etidocaine show arapid onset of action, whereas procaine andamethocaine, with a high pK^, have a slow onsettime (fig. 4). Bupivacaine occupies an intermediateposition in terms of pKa and latency of blockade:
The anaesthetic characteristics of various chem-ical compounds in vivo are dependent in part onother miscellaneous considerations. The onset ofaction may be altered by the rate of diffusionthrough non-nervous tissue. For example, ligno-caine and prilocaine possess a similar pK& andsimilar onset of action in an isolated nerve.However, in vivo studies suggest that prilocainemay be somewhat slower in onset than lignocaine.This difference may be related to an enhancedability of lignocaine to diffuse through non-nervoustissue. More important, however, is the concentra-tion of local anaesthetic agent used. For example,0.25 % bupivacaine possesses a rather slow onsetof action; however, increasing the concentration to0.75% results in a significant decrease in thelatency of anaesthetic activity. The rapid onset
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS 705
time of chloroprocaine in vivo may be related inpart to improved diffusion through non-nervoustissue, but also to the use of a 3 % concentrationof this agent. The p/Ca of chloroprocaine isapproximately 9 and its onset of action in isolatednerves is relatively slow. However, the lowsystemic toxicity of this agent allows the use ofhigh concentrations. Therefore, the rapid onsettime in vivo of chloroprocaine may be relatedsimply to the large number of molecules placedin the vicinity of peripheral nerves.
The effect of local anaesthetic agents on thevasculature at the site of injection also influencesthe in vivo potency and duration of action of thesecompounds. Absorption of local anaestheticagents from the region of injection decreases thenumber of molecules available for diffusion to thereceptor site in the nerve membrane. Factorswhich increase the absorption decrease theapparent anaesthetic potency and duration ofaction of a specific compound. All local anaes-thetics, with the exception of cocaine, exhibit a 'biphasic effect on vascular smooth muscle. Atextremely low concentrations they cause enhancedactivity of vascular smooth muscle, leading tovasoconstriction, while, in the concentrationscommonly used for regional anaesthesia, they tendto be vasodilators. The relative degree of vasodila-tation produced by different local anaestheticdrugs can affect their potency and duration ofaction. This can be demonstrated by comparingthe in vitro and in vivo activity of different agents.For example, in vitro studies of lignocaine andmepivacaine have shown that lignocaine is signi-ficantly more potent than the latter on an isolatednerve, while the duration of conduction blockadeis similar. However, in vivo studies have shownlittle difference in their relative anaestheticpotency and, indeed, the duration of action ofmepivacaine is somewhat longer than that oflignocaine. These differences appear to be relatedto a greater degree of vasodilatation produced bylignocaine. Addition of a vasoconstrictor agentsuch as adrenaline (epinephrine, USP) to solutionsof both lignocaine and mepivacaine eliminates thedifference in duration of the two compounds,which again suggests that the greater vasodilatoractivity of lignocaine is responsible for thedifference in anaesthetic duration observed be-tween the plain solutions. The only agent whichproduces a state of vasoconstriction at clinicallyuseful concentrations is cocaine, the vasoconstric-
tor action of which is not directly related to theagent itself, but is an indirect action. Cocainepossesses the ability to prevent the re-uptake ofnoradrenaline (norepinephrine, USP) by storagegranules, which results in a state of vaso-constriction.
In summary, the pharmacological activity oflocal anaesthetic agents is related primarily to theirphysicochemical properties. However, the activityof these agents in vivo may be altered by otheractions which are essentially unrelated to theirphysicochemical properties. On the basis ofanaesthetic activity in man, the various agents maybe classified as follows: (1) Agents of lowanaesthetic potency and short duration of action:procaine and chloroprocaine. (2) Agents ofintermediate anaesthetic potency and duration ofaction: lignocaine, mepivacaine and prilocaine. (3)Agents of high anaesthetic potency and prolongedduration of action: amethocaine, bupivacaine andetidocaine. In terms of latency, chloroprocaine,lignocaine, mepivacaine, prilocaine and etidocainepossess a relatively rapid onset of action. Bupiva-caine is intermediate in terms of onset ofanaesthesia, while procaine and amethocainedemonstrate a long latency period.
Differential blockade
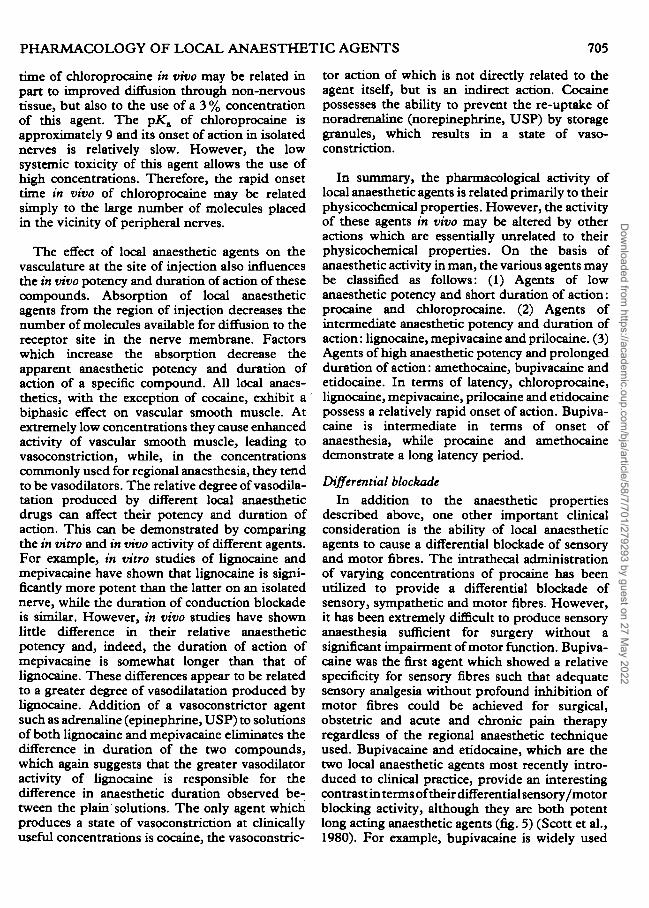
In addition to the anaesthetic propertiesdescribed above, one other important clinicalconsideration is the ability of local anaestheticagents to cause a differential blockade of sensoryand motor fibres. The intrathecal administrationof varying concentrations of procaine has beenutilized to provide a differential blockade ofsensory, sympathetic and motor fibres. However,it has been extremely difficult to produce sensoryanaesthesia sufficient for surgery without asignificant impairment of motor function. Bupiva-caine was the first agent which showed a relativespecificity for sensory fibres such that adequatesensory analgesia without profound inhibition ofmotor fibres could be achieved for surgical,obstetric and acute and chronic pain therapyregardless of the regional anaesthetic techniqueused. Bupivacaine and etidocaine, which are thetwo local anaesthetic agents most recently intro-duced to clinical practice, provide an interestingcontrast in terms of their differential sensory/motorblocking activity, although they are both potentlong acting anaesthetic agents (fig. 5) (Scott et al.,1980). For example, bupivacaine is widely used
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
706
Bupivacaine
BRITISH JOURNAL OF ANAESTHESIA
Etidocaine
100
75
50
25
025 0.5
•Sensory block0 Motor block
0.75 05Concentration (%)
1.0 1.5
FIG. 5. Comparative sensory/motor blockade of bupivacaine and etidocaine following extraduraladministration.
extradurally for both surgical and obstetricprocedures and relief of pain after operation as aresult of its ability to provide adequate sensoryanalgesia with minimal blockade of motor fibres,particularly when used as a 0.25% or 0.5%solution. Thus, the patient in labour can berendered pain free and still be able to move herlegs, which is one of the primary reasons why thisagent has enjoyed popularity for continuousextradural blockade during labour. Increasing theconcentration of bupivacaine to 0.75 % increasesthe depth of both sensory and motor blockade,while also shortening latency and producing amore prolonged duration of anaesthesia. On theother hand, etidocaine shows little separationbetween sensory and motor blockade. In order toachieve adequate extradural sensory anaesthesia,1.5% concentrations of etidocaine are usuallyrequired. At these concentrations, etidocaine hasan extremely rapid onset of action and a prolongedduration of anaesthesia. However, sensory anaes-thesia is associated with a profound degree ofmotor blockade. Thus, etidocaine is a valuableagent, particularly for extradural blockade in sur-gical situations where maximum neuromuscularblockade is desirable, since it combines a rapidonset, prolonged duration, and satisfactory qualityof anaesthesia, with profound motor blockade.However, this marked effect on motor functionrenders etidocaine of limited value for obstetricanalgesia and postoperative pain relief.
The factors responsible for the differentialsensory/motor separation associated with bupiva-
caine are not precisely known. Studies on isolatednerves have shown that, at low concentrations,bupivacaine initially blocks unmyelinated C fibresfollowed, at a later time, by a block of myelinatedA fibres (Gissen, Covino and Gregus, 1982). Onthe other hand, etidocaine blocks both A and Cfibres at approximately the same rate. The slowblockade of A fibres by bupivacaine is believed tobe attributable to the relatively high pKa of thisagent, such that fewer uncharged molecules areavailable to penetrate the diffusion barriers sur-rounding large A fibres. In vivo, the combinationof the slow diffusion of bupivacaine and itsabsorption by the vasculature in the region of drugadministration may result in a situation in whichthe number of bupivacaine molecules whichultimately penetrate the membrane of the largemotor A fibres is insufficient to cause conductionblockade. The lack of diffusion barriers around thesmall sensory C fibres allows a sufficient numberof bupivacaine molecules to reach the receptorsites in the C fibre membrane to cause sensoryanaesthesia. Thus, bupivacaine may possess theoptimal pKa and lipid solubility characteristicsrequired for differential sensory/motor blockade.
FACTORS INFLUENCING ANAESTHETIC ACTIVITY
Although the inherent pharmacological propertiesof the various local anaesthetic agents basicallydetermine their anaesthetic profile, other factorsmay also influence the quality of regionalanaesthesia. These include dose of local anaesthetic
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS 707
350
300
T 250
1= 200
to
^100
50
250 300XX) 150 200
Dose (mg)
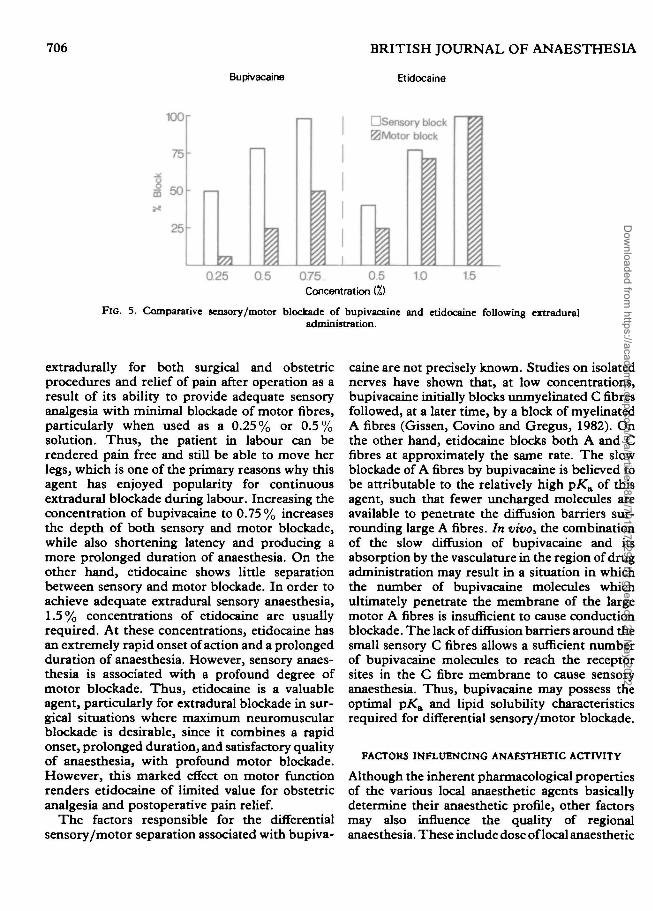
FIG. 6. Effect of dose of extradural eudocaine on onset, frequency and duration of anaesthesia.
administered; addition of a vasoconstrictor to thelocal anaesthetic solution; site of administration;carbonation of local anaesthetics; addition ofdextran; mixtures of local anaesthetics.
Dosage of local anaesthetic solutions
The mass of drug administered influences theonset, depth and duration of anaesthesia (fig. 6).As the dose of local anaesthetic is increased, thefrequency of satisfactory anaesthesia and theduration of anaesthesia increase and the time toonset of anaesthesia decreases. In general, thedose of local anaesthetic administered can beincreased by administering either a larger volumeof a less concentrated solution, or a smaller volumeof a more concentrated solution. However, inclinical practice, an increase in dose is achievedusually by using a more concentrated solution ofthe specific agent. For example, a dose-responsestudy involving the use of bupivacaine forextradural analgesia in obstetrics has shown thatincreasing the concentration from 0.125% to0.5% while maintaining the same volume ofinjectate (10 ml) resulted in a decreased latency,improved incidence of satisfactory analgesia andan increased duration of sensory analgesia (Little-wood et al., 1979). A similar study involving theuse of bupivacaine for surgical anaesthesia has alsodemonstrated that increasing the concentrationfrom 0.5 % to 0.75 % with a concomitant increasein dose from approximately 100 mg to 150 mgproduced a more rapid onset and prolongedduration of sensory anaesthesia (Scott et al., 1980).In addition, the frequency of satisfactory sensoryanaesthesia was increased and the depth of motor
blockade was enhanced. The relative influence ofvolume, concentration and dose was demonstratedin a study in which prilocaine 600 mg administeredextradurally either as 30 ml of a 2 % solution or20 ml of 3 % solution, was evaluated (Crawford,1964). No difference in onset, adequacy orduration of anaesthesia and onset, depth andduration of motor blockade was observed, despitedifferences in volume and concentration ofanaesthetic solution used, since the dose wasmaintained constant. The volume of anaestheticsolution administered may influence the spread ofanaesthesia. For example, 30 ml of 1 % lignocaineadministered to the extradural space was shown toproduce a level of anaesthesia which was 4.3dermatomes higher than that achieved when 10 mlof 3 % lignocaine was used (Erdimir, Soper andSweet, 1965). Thus, except for the possible effecton the spread of anaesthesia, the primary qualitiesof regional anaesthesia—namely, onset, depth andduration of blockade—are related to the mass ofdrug injected, that is, the product of volume andconcentration.
Addition of a vasoconstrictor to local anaestheticsolutions
Vasoconstrictors, particularly adrenaline, arefrequently added to local anaesthetic solutions.The decrease in the rate of vascular absorptionwhich results from the addition of adrenalineallows more anaesthetic molecules to reach thenerve membrane and thereby improves the depthand duration of anaesthesia. Local anaestheticsolutions usually contain a 1:200 000 (5 ug ml"1)concentration of adrenaline. This concentration
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
708 BRITISH JOURNAL OF ANAESTHESIA
250
200
I 100
0
T
Ametho Ametha Ametho.
adrenO.2mg phen. 2.0mg
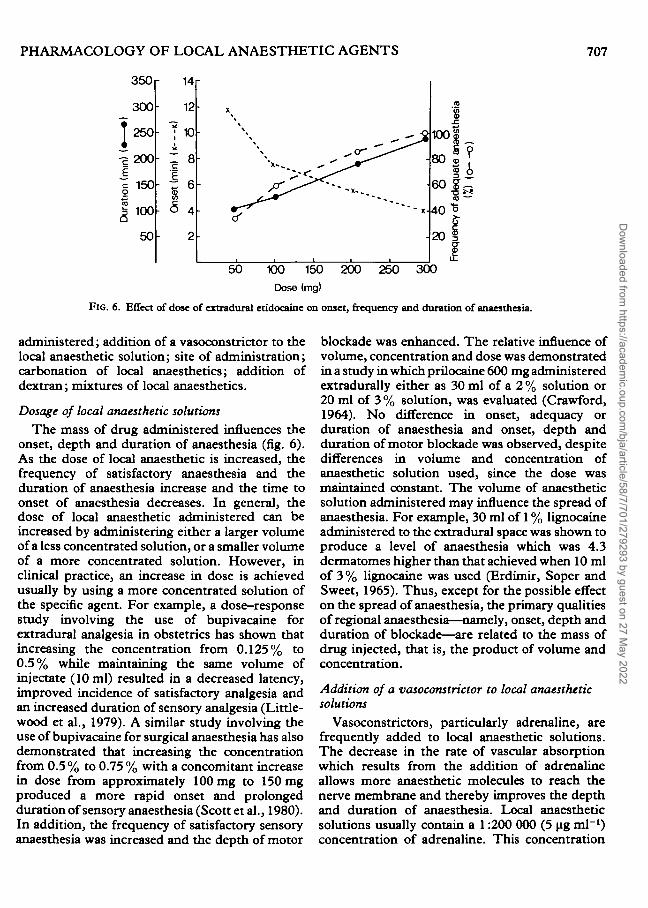
FIG. 7. Effect of adrenaline (adren.) (epinephrine, USP) andphenylephrine (phen.) on the duration of spinal anaesthesia
produced by amethocaine (Ametho.) (tetracaine, USP).
has been reported to provide an optimal degree ofvasoconstriction when used with lignocaine forextradural or intercostal use (Braid and Scott,1965). Little information is available concerningthe optimum concentration of adrenaline when itis used with other local anaesthetic agents. Othervasoconstrictor agents such as noradrenaline andphenylephrine have also been used as additives tosolutions of local anaesthetics. Regional blood nowstudies indicate that adrenaline is more effective asa vasoconstrictor than noradrenaline when com-bined with local anaesthetic agents (Dhuner andLewis, 1966). Phenylephrine has been reported toproduce the greatest prolongation of spinalanaesthesia when combined with amethocaine(Meagher, Moore and DeVries, 1966). However,more recent studies conducted under double-blindconditions indicated that, at equipment doses, nodifferences existed between the ability of adrenalineand phenylephrine to prolong the duration ofspinal anaesthesia produced by amethocaine (fig.7) (Conception et al., 1984).
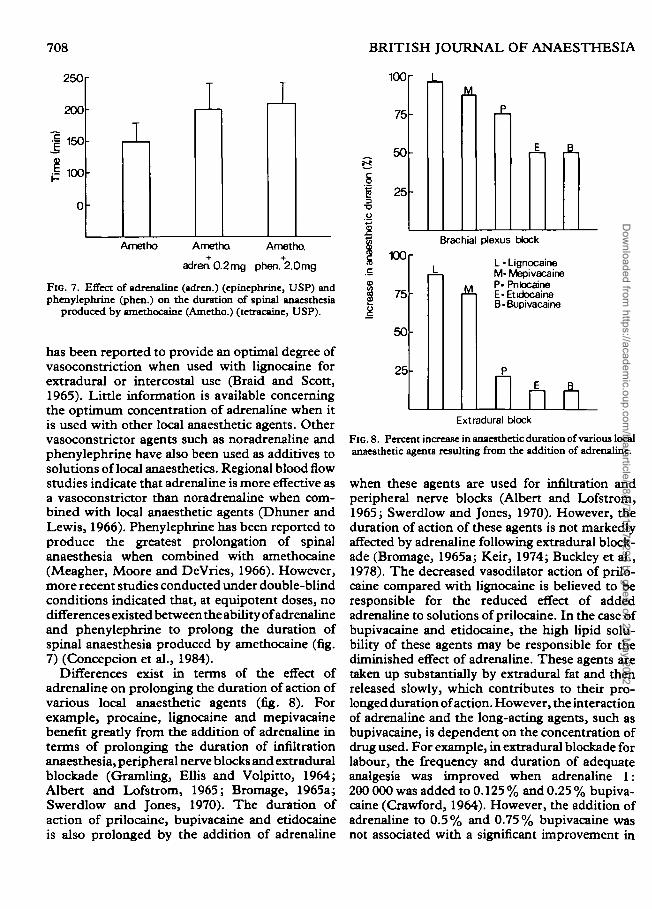
Differences exist in terms of the effect ofadrenaline on prolonging the duration of action ofvarious local anaesthetic agents (fig. 8). Forexample, procaine, lignocaine and mepivacainebenefit greatly from the addition of adrenaline interms of prolonging the duration of infiltrationanaesthesia, peripheral nerve blocks and extraduralblockade (Gramling, Ellis and Volpitto, 1964;Albert and Lofstrom, 1965; Bromage, 1965a;Swerdlow and Jones, 1970). The duration ofaction of prilocaine, bupivacaine and etidocaineis also prolonged by the addition of adrenaline
100
75
50
25
100
75
50
25
Brachial plexus block
L • LignocaineM- MepivacaineP- PnlocaineE-EtidocaineB-Bupivacaine
Extradural block
FIG. 8. Percent increase in anaesthetic duration of various localanaesthetic agents resulting from the addition of adrenaline.
when these agents are used for infiltration andperipheral nerve blocks (Albert and Lofstrom,1965; Swerdlow and Jones, 1970). However, theduration of action of these agents is not markedlyaffected by adrenaline following extradural block-ade (Bromage, 1965a; Keir, 1974; Buckley et al.,1978). The decreased vasodilator action of prilo-caine compared with lignocaine is believed to beresponsible for the reduced effect of addedadrenaline to solutions of prilocaine. In the case ofbupivacaine and etidocaine, the high lipid solu-bility of these agents may be responsible for thediminished effect of adrenaline. These agents aretaken up substantially by extradural fat and thenreleased slowly, which contributes to their pro-longed duration of action. However, the interactionof adrenaline and the long-acting agents, such asbupivacaine, is dependent on the concentration ofdrug used. For example, in extradural blockade forlabour, the frequency and duration of adequateanalgesia was improved when adrenaline 1:200 000 was added to 0.125 % and 0.25 % bupiva-caine (Crawford, 1964). However, the addition ofadrenaline to 0.5% and 0.75% bupivacaine wasnot associated with a significant improvement in
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS 709
the frequency of satisfactory extradural blockadein obstetric or surgical patients (Littlewood et al.,1979; Sinclair and Scott, 1984). The profoundnessof motor blockade is enhanced following the extra-dural administration of adrenaline-containingsolutions of bupivacaine and etidocaine (Sinclairand Scott, 1984). The differential effect ofadrenaline in terms of prolonging the duration ofaction of local anaesthetic agents is most apparentin the subarachnoid space. Adrenaline significantlyextends the duration of spinal anaesthesia whencombined with amethocaine (Armstrong, Little-wood and Chambers, 1983; Conception et al.,1984). However, the duration of effective surgicalanaesthesia is not markedly enhanced whensolutions of lignocaine or bupivacaine withadrenaline are administered intrathecally (Cham-bers et al., 1981; Chambers, Littlewood and Scott,1982).
Site of injection
The site of administration of local anaestheticagents influences their anaesthetic profile. Al-though local anaesthetics are frequently classifiedas agents of short, moderate or long duration witha slow or rapid onset of action, these generalproperties are influenced by the type of procedureperformed. For example, amethocaine is usuallvconsidered an agent of slow onset and longduration. However, the onset of action of this drugis quite rapid (approximately 3 min) whenadministered intrathecally, while the duration ofspinal anaesthesia with amethocaine is only 2-3 h(Concepcion et al., 1984). In terms of latency, themost rapid onset of action occurs following theintrathecal or subcutaneous administration oflocal anaesthetics, while the slowest onset timesare observed during the performance of brachialplexus blocks (Covino and Bush, 1975). Withregard to the duration of anaesthesia, an agent suchas bupivacaine possesses a duration of surgicalanaesthesia of approximately 4 h when adminis-tered to the extradural space. However, whenbupivacaine is administered for brachial plexusblockade, the duration of anaesthesia averages10 h. Differences in the onset and duration ofanaesthesia depending on the site of injectionresult in part from the particular anatomy of thearea of injection, the variation in the rate ofvascular absorption, and the amount of drug usedfor various types of regional anaesthesia. In thecase of spinal anaesthesia, the lack of a nerve sheatharound the spinal cord and the deposition of the
local anaesthetic solution in the immediatevicinity of the spinal cord are responsible for therapid onset of action. On the other hand, therelatively small amount of drug used for spinalanaesthesia probably accounts for the relativelyshort duration of action associated with thisparticular technique. In the case of brachial plexusblockade, the onset of anaesthesia is slow as a resultof the fact that the anaesthetic agent is usuallydeposited at some distance from the nerve roots,and therefore time for diffusion to the nervemembrane is required before signs of anaesthesiaare apparent. The long duration of brachial plexusblockade observed with most local anaesthetics,but in particular the longer acting agents, isprobably related to the decreased rate of vascularabsorption from that site, and also the larger dosesof drug commonly used for this regional anaesthetictechnique.
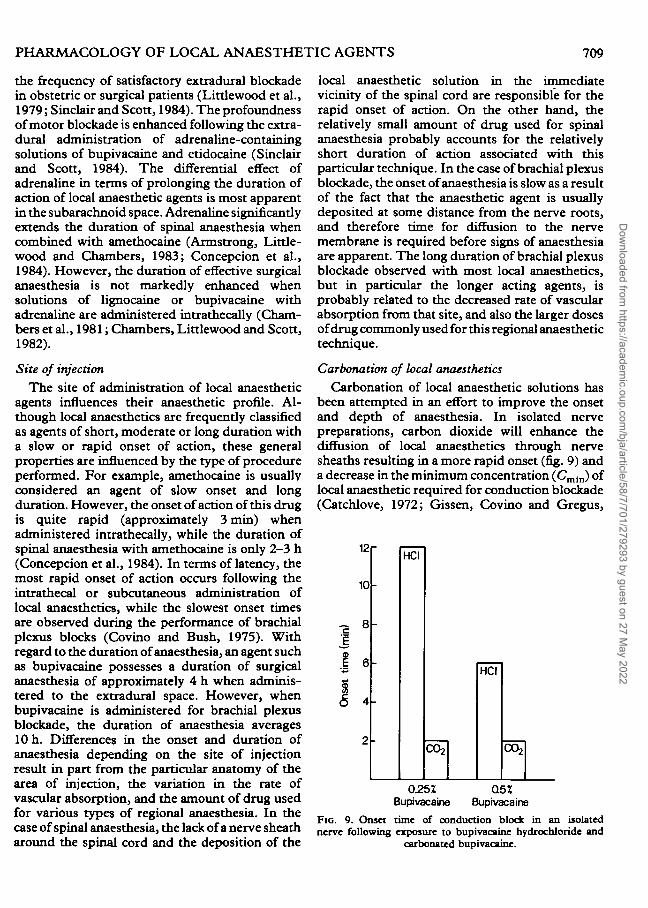
Carbonation of local anaesthetics
Carbonation of local anaesthetic solutions hasbeen attempted in an effort to improve the onsetand depth of anaesthesia. In isolated nervepreparations, carbon dioxide will enhance thediffusion of local anaesthetics through nervesheaths resulting in a more rapid onset (fig. 9) anda decrease in the minimum concentration (Cmln) oflocal anaesthetic required for conduction blockade(Catchlove, 1972; Gissen, Covino and Gregus,
10
(min
) CD
1 64-*
o
-
-
•
-
HCI
CO2
HCI
CO2
0.25Z Q5ZBupivacaine Bupivacaine
FIG. 9. Onset time of conduction block in an isolatednerve following exposure to bupivacaine hydrochloride and
carbonated bupivacaine.
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
710 BRITISH JOURNAL OF ANAESTHESIA
1985). The diffusion of carbon dioxide through thenerve membrane decreases the axoplasmic pH.The lower pH increases the intracellular concen-tration of the cationic form of the local anaesthetic,which represents the active form that binds to areceptor in the sodium channel. In addition, thelocal anaesthetic cation does not readily diffusethrough membranes, so that the drug remainsentrapped within the axoplasm, a situationreferred to as ion trapping. The enhancedformation of the local anaesthetic cation and theprocess of ion trapping are believed responsiblefor the more rapid onset and more profound degreeof conduction block. A number of clinical studieshave been carried out with carbonated solutions oflignocaine. The initial investigations in manreported that lignocaine carbonate solutionsdemonstrated a more rapid onset of brachialplexus and extradural blockade compared with theuse of lignocaine hydrochloride solutions (Bro-mage, 1965b, 1970). However, more recentdouble-blind studies have failed to demonstrate asignificantly more rapid onset of action whenlignocaine carbonate was compared with lignocainehydrochloride for extradural blockade (Morrison,1981; Cole et al., 1985). In theory an agent suchas bupivacaine which has a relatively slow onset ofaction should benefit greatly from the use of acarbonated solution and it has been reported thatbupivacaine-carbon dioxide is associated with amore rapid onset of action in man (Eckstein et al.,1978). However, double-blind studies in whichbupivacaine carbonate was compared with bupiva-caine hydrochloride for brachial plexus or extra-dural blockade, have failed to confirm these earlierreports of a significantly shorter onset of action ofthe carbonated solution (Brown et al., 1980;McClure and Scon, 1981). Thus, at the presenttime, it is not certain whether carbonation of localanaesthetic solutions imparts any advantage to thevarious local anaesthetic agents in terms of onsetof block when used under clinical conditions,although the depth of anaesthesia may beimproved.
The discrepancy between in vitro and in vivostudies suggests that the injected carbon dioxideis rapidly buffered in vivo such that the intracellularpH is not sufficiently altered and significantlyincreased concentrations of the cationic form ofthe local anaesthetic are not achieved to producea more rapid onset of anaesthesia.
Attempts have been made to improve the onset
of conduction blockade by the addition of sodiumbicarbonate to local anaesthetic solutions immedi-ately before injection (Galindo, Schou andWitcher, 1981; Hilgier, 1985). Theoretically,sodium bicarbonate may increase the pH of thelocal anaesthetic solution, which in turn increasesthe amount of drug in the uncharged base form.Thus, the rate of diffusion across the nerve sheathand nerve membrane should be enhanced, resultingin a more rapid onset of anaesthesia. Severalclinical studies have been carried out in which theaddition of sodium bicarbonate to solutions ofbupivacaine did appear to produce a significantdecrease in the latency of brachial plexus blockade +(Galindo, Schou and Witcher, 1981, Hilgier,1985). In addition, it has also been reported that *the duration of anaesthesia was prolonged byincreasing the pH of the local anaesthetic solution(Hilgier, 1985).
Addition of dextranVarious attempts have been made to prolong the
duration of anaesthesia by incorporating dextraninto local anaesthetic solutions (Loder, 1960;Rosenblatt and Fung, 1979). Discrepancies existwith regard to the effectiveness of dextran inprolonging the duration of regional anaesthesia. Inone controlled clinical study, prolonged durationsof anaesthesia were observed in some individualpatients, but the mean duration of intercostalnerve blockade was not significantly altered whensolutions of bupivacaine with and without dextranwere compared (Bridenbaugh, 1978).
It has been suggested that the difference inresults obtained by various investigators may berelated to the pH of the dextran solution used.Dextran solutions with a pH of 8.0 significantlyprolonged the duration of bupivacaine-inducedcoccygeal nerve blocks in rats, whereas theduration of block was not altered when dextranwith a pH of 4.5-5.5 was added to bupivacaine(Rosenblatt and Fung, 1980). These results v
indicate that alkalinization of the anaestheticsolution may be responsible for prolonged conduc-tion blockade, rather than the dextran itself.
Mixtures of local anaestheticsThe use of mixtures of local anaesthetics for K
regional anaesthesia has become relatively popularin recent years. The basis for this practice is tocompensate for the short duration of action of
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS 711
certain agents such as chloroprocaine or lignocaineand the long latency of other agents such asamethocaine and bupivacaine. The combination oflignocaine or mepivacaine and amethocaine wascommonly used in some centres before the adventof bupivacaine and etidocaine as long durationanaesthetics. Since the slow onset of amethocaine
* for peripheral nerve blocks and extradural anaes-thesia was clinically unacceptable, the addition oflignocaine or mepivacaine provided a localanaesthetic solution which afforded a relativelyrapid onset of action and prolonged duration ofanaesthesia. Recently, mixtures of chloroprocaine
x and bupivacaine have been used in an effort toproduce a local anaesthetic solution with a rapid
4 onset and long duration of action. The lowsystemic toxicity of chloroprocaine afforded anadditional advantage to such a mixture. However,the use of a chloroprocaine-bupivacaine mixturehas produced contradictory results. It was origi-nally reported that a mixture of chloroprocaineand bupivacaine did result in a short latency andprolonged duration of bracbial plexus blockade(Cunningham and Kaplan, 1974). However,subsequent studies indicated that the duration ofextradural anaesthesia produced by a mixtureof chloroprocaine-bupivacaine was significantlyshorter than that obtained with solutions of bupi-vacaine alone (Cohen and Thurlow, 1979). Thisreduced duration has been attributed in part to adecrease in pH, since chloroprocaine solutionshave a pH of approximately 3.0 (Galindo andWitcher, 1980). Reduction in pH decreases theamount of bupivacaine available in the unchargedbase form, which may reduce the number ofmolecules able to penetrate the nerve sheath. Inaddition, data from isolated nerve studies suggestthat a metabolite of chloroprocaine may inhibitthe binding of bupivacaine to membrane receptorsites (Corke, Carlson and Dettbarn, 1984). Atthe present time there do not appear to be anyclinically significant advantages to the use ofmixtures of local anaesthetic agents. Etidocaine
' and bupivacaine provide clinically acceptableonsets of action and prolonged durations ofanaesthesia. In addition, the use of cathetertechniques for extradural anaesthesia and also forbrachial plexus blockade make it possible to
' administer repeated injection of the rapidly actingagents such as chloroprocaine or lignocaine whichprovide an anaesthetic duration of indefinitelength.
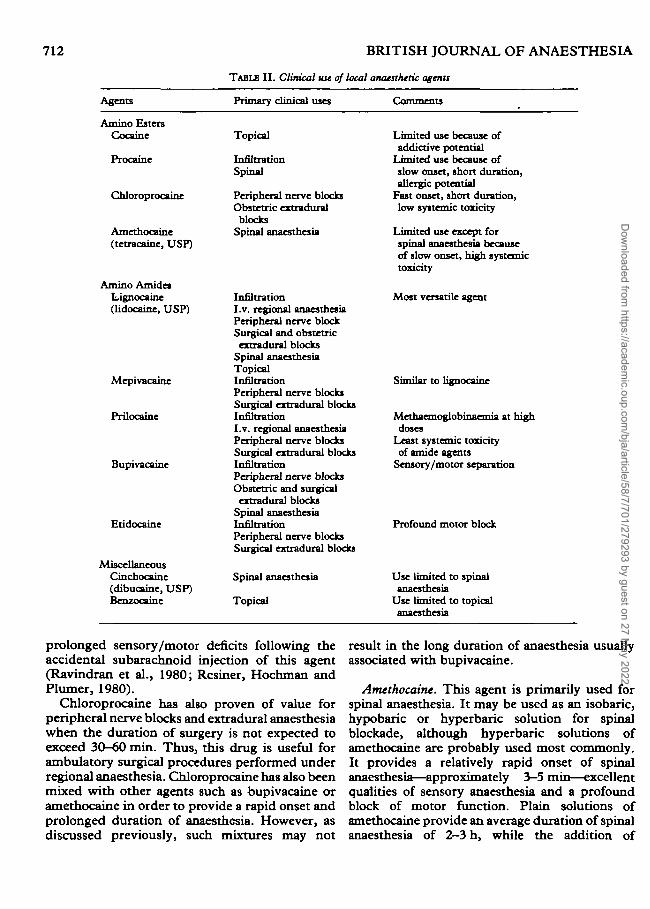
SPECIFIC LOCAL ANAESTHETIC AGENTS (table I I )
Amino ester agents
Cocaine. This compound, which was isolatedfrom the Erythroxylin coca bush, was the firstagent successfully used for the production ofclinical local anaesthesia. The relatively highpotential for systemic toxicity and the addictionliabilities associated with its use resulted in theabandonment of this agent for most regionalanaesthetic techniques. However, cocaine is anexcellent topical anaesthetic agent and is the onlylocal anaesthetic that produces vasoconstriction atclinically useful concentrations. As a result, it isstill used to anaesthetize and constrict the nasalmucosa before nasotracheal intubation. It is alsoused frequently by otolaryngologists during nasalsurgery because of its topical anaesthetic andvasoconstrictor properties.
Procaine. This was the first synthetic compoundsuccessfully used for regional anaesthesia. How-ever, procaine is a relatively weak local anaestheticwith a slow onset and short duration of action. Therelatively low potency and rapid hydrolysis of thisagent is responsible for the low systemic toxicityof procaine. On the other hand, procaine ishydrolysed to para-aminobenzoic acid, which isresponsible for the allergic reactions associatedwith the repeated use of this drug. At present,procaine is primarily used for infiltration anaes-thesia and diagnostic differential spinal blocks.Recently, a combination of procaine and ametho-caine has been used for spinal anaesthesia inobstetric patients (Chantigian et al., 1984).
Chloroprocaine. Chloroprocaine is characterizedby a rapid onset of action, a short duration, and lowsystemic toxicity. Although the potency of thisagent is relatively low, it may be used in aconcentration of 3%, because of its systemicsafety. The duration of action of chloroprocaine isapproximately 30-60 min. This agent is usedprimarily for extradural analgesia and anaesthesiain obstetrics because of its rapid onset and lowsystemic toxicity in mother and fetus. However,frequent injections are required in order toprovide adequate pain relief during labour. Often,extradural analgesia is established in the pregnantpatient with chloroprocaine, following which alonger acting agent such as bupivacaine is used.The extradural use of chloroprocaine may havedeclined somewhat as a result of reports of
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
712 BRITISH JOURNAL OF ANAESTHESIA
TABLE II. Clinical use of local anaesthetic agents
Agents
Amino EstersCocaine
Procaine
Chloroprocaine
Amethocaine(tetracaine, USP)
Amino AmidesLignocaine(lidocaine, USP)
Mepivacaine
Prilocaine
Bupivacaine
Etidocaine
MiscellaneousCinchocaine(dibucaine, USP)Benzocaine
Primary clinicnl uses
Topical
InfiltrationSpinal
Peripheral nerve blocksObstetric extradural
blocksSpinal anaesthesia
InfiltrationI.v. regional anaesthesiaPeripheral nerve blockSurgical and obstetricextradural blocks
Spinal anaesthesiaTopicalInfiltrationPeripheral nerve blocksSurgical extradural blocksInfiltrationI.v. regional anaesthesiaPeripheral nerve blocksSurgical extradural blocksInfiltrationPeripheral nerve blocksObstetric and surgical
extradural blocksSpinal anaesthesiaInfiltrationPeripheral nerve blocksSurgical extradural blocks
Spinal anaesthesia
Topical
Comments
Limited use because ofaddictive potential
T .imitrd use because ofslow onset, short duration,allergic potential
Fast onset, short duration,low systemic toxicity
I .imitrd use except forspinal anaesthesia becauseof slow onset, high systemictoxicity
Most versatile agent
Similar to lignocaine
Methaemoglobinaemia at highdoses
Least systemic toxicityof amide agents
Sensory/motor separation
Profound motor block
Use limited to spinalanaesthesia
Use limited to topicalanaesthesia
prolonged sensory/motor deficits following theaccidental subarachnoid injection of this agent(Ravindran et al., 1980; Resiner, Hochman andPlumer, 1980).
Chloroprocaine has also proven of value forperipheral nerve blocks and extradural anaesthesiawhen the duration of surgery is not expected toexceed 30-60 min. Thus, this drug is useful forambulatory surgical procedures performed underregional anaesthesia. Chloroprocaine has also beenmixed with other agents such as bupivacaine oramethocaine in order to provide a rapid onset andprolonged duration of anaesthesia. However, asdiscussed previously, such mixtures may not
result in the long duration of anaesthesia usuallyassociated with bupivacaine.
Amethocaine. This agent is primarily used forspinal anaesthesia. It may be used as an isobaric,hypobaric or hyperbaric solution for spinalblockade, although hyperbaric solutions ofamethocaine are probably used most commonly.It provides a relatively rapid onset of spinalanaesthesia—approximately 3—5 min—excellentqualities of sensory anaesthesia and a profoundblock of motor function. Plain solutions ofamethocaine provide an average duration of spinalanaesthesia of 2—3 h, while the addition of
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS 713
adrenaline can extend the duration of anaesthesiato 4-6 h.
Amethocaine is rarely used for other forms ofregional anaesthesia as a result of its extremelyslow onset of action and the potential for systemictoxic reactions when the larger doses required forother types of regional blockade are used.Amethocaine does possess excellent topical anaes-thetic properties and solutions of this agent werecommonly used for endotracheal surface anaes-thesia. However, the absorption of amethocainefrom the tracheo-bronchial area is extremelyrapid, and several fatalities have been reportedfollowing the use of an endotracheal aerosol ofamethocaine.
Amino amide agents
Lignocaim. Lignocaine was the first drug of theamino amide type to be introduced to clinicalpractice. This agent remains the most versatile andmost commonly used local anaesthetic by virtue ofits inherent potency, rapid onset, moderateduration of action and topical anaesthetic activity.Solutions of 0.5%, 1.0%, 1.5% and 2.0%lignocaine are available for infiltration, peripheralnerve blocks and extradural anaesthesia. Inaddition, 5% lignocaine with 7.5% glucose iswidely used for spinal anaesthesia of 30-60 minduration. Lignocaine is also used in ointment,jelly, viscous and aerosol preparations for a varietyof topical anaesthetic procedures.
Although the duration of action of lignocaine isapproximately 1-2 h for various regional anaes-thetic procedures, the addition of adrenalinesignificantly prolongs the duration of this agent. Inaddition, adrenaline decreases the rate of absorp-tion of lignocaine which significantly decreases itspotential for producing systemic toxic reactions.
Mepivacaine. This agent is similar to lignocainein terms of its anaesthetic profile. Mepivacainemay produce a profound depth of anaesthesia,with a relatively rapid onset and a moderateduration of action. This agent may be used forinfiltration, peripheral nerve blocks and extraduralanaesthesia in concentrations varying from 0.5 to2.0 %. In some countries, 4 % hyperbaric solutionsof mepivacaine are also available for spinalanaesthesia.
Differences do exist between mepivacaine andlignocaine. Mepivacaine is not effective as a topicalanaesthetic agent and so is less versatile thanlignocaine. In addition, the metabolism of mepiva-
caine is markedly prolonged in the fetus andnewborn, such that this agent is not usually usedfor obstetric anaesthesia. However, in adults,mepivacaine appears to be somewhat less toxicthan lignocaine. In addition, the vasodilatoractivity of mepivacaine is less than that oflignocaine. Thus, mepivacaine provides a some-what longer duration of anaesthesia than lignocainewhen the two agents are used without adrenaline.The duration of action of mepivacaine may beprolonged significantly by the addition of avasoconstrictor such as adrenaline.
Prilocaine. The clinical profile of prilocaine isalso similar to that of lignocaine. Prilocaine has arelatively rapid onset of action, while providing amoderate duration of anaesthesia and a profounddepth of conduction blockade. This agent causessignificantly less vasodilatation than lignocaineand so may be used without adrenaline. In general,the duration of prilocaine without adrenaline issimilar to that of lignocaine with adrenaline. Thus,prilocaine is particularly useful in patients inwhom adrenaline may be contraindicated. Prilo-caine is useful for infiltration, peripheral nerveblockade, and extradural anaesthesia. Althoughprilocaine possesses topical anaesthetic activity,and can induce spinal anaesthesia of shortduration, no specific formulations of this agent areavailable for topical or spinal anaesthesia.
Prilocaine is the least toxic of the amino amidelocal anaesthetics. Thus, this agent is particularlyuseful for i.v. regional anaesthesia, since CNStoxic effects are rarely seen following tourniquetdeflation, even when early accidental release of thetourniquet may occur. Forty millilitre of 0.5%prilocaine (200 mg) provides effective anaesthesiafor hand surgery using the i.v. regional anaesthetictechnique.
The major deterrent to the use of prilocaine isrelated to the formation of methaemoglobinaemiawith this drug (Lund and Cwik, 1965). Thisunusual side effect of prilocaine has essentiallyeliminated the use of this drug in obstetrics,although prilocaine has not been reported to causeany significant adverse effects in mother, fetus ornewborn. However, the cyanotic appearance ofnewborns delivered of mothers who have receivedprilocaine for extradural anaesthesia during labourhas resulted in sufficient confusion concerning theaetiology of the cyanosis, such that the obstetricuse of this potentially valuable drug has beenvirtually abandoned.
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022

714 BRITISH JOURNAL OF ANAESTHESIA
Bupivacaine. This agent has probably had thegreatest influence on the practice of regionalanaesthesia since the introduction of lignocaine.Bupivacaine was the first local anaesthetic thatcombined the properties of an acceptable onset,long duration of action, profound conductionblockade, and significant separation of sensoryanaesthesia and motor blockade. This agent is usedin concentrations of 0.125 %, 0.25%, 0.5%, and0.75 % for various regional anaesthetic procedures,including infiltration, peripheral nerve blocks,extradural and spinal anaesthesia. Bupivacaine hasnot been used for topical anaesthesia. The averageduration of surgical anaesthesia of bupivacainevaries approximately from 3 to 10 h. Its longestduration of action occurs when major peripheralnerve blocks such as brachial plexus blockade areperformed. In these situations, average durationsof effective surgical anaesthesia of 10—12 h havebeen reported. In some patients, durations ofbrachial plexus block of 24 h have been observed,with complete recovery of sensation.
The major advantage of bupivacaine appears tobe in the area of obstetric analgesia for labour. Inthis situation, bupivacaine administered extra-durally in concentrations varying from 0.125 % to0.5 % provides satisfactory pain relief for 2-3 hwhich significantly decreases the need for repeatedinjections in the pregnant patient. More import-antly, adequate analgesia is usually achievedwithout significant motor blockade, so that thepatient in labour is able to move her legs. Thisdifferential blockade of sensory and motor fibresis also the basis for the widespread use ofbupivacaine for postoperative extradural analgesiaand for certain chronic pain states.
In recent years, bupivacaine has been usedextensively for spinal anaesthesia (Chambers,Edstrom and Scott, 1981; Sheskey et al., 1983;Rocco et al., 1984). Isobaric and hyperbaricsolutions of 0.5 % and 0.75 % bupivacaine havebeen investigated for a variety of surgical pro-cedures performed under subarachnoid block-ade. Onset of spinal anaesthesia with bupivacaineusually occurs within 5 min while the duration ofsurgical anaesthesia persists for 3-4 h. Compara-tive studies of bupivacaine and amethocaine sug-gest little difference between the two agents interms of onset, spread and duration of spinalblockade. Several investigations have suggestedthat the frequency of satisfactory anaesthesiamay be greater with bupivacaine compared withamethocaine. In addition, less hypotension is
apparent following the intrathecal administrationof bupivacaine, even in patients with an exag-gerated spread of sensory anaesthesia. The degreeof motor blockade is greater when isobaric solu-tions of bupivacaine are used in comparison withthe use of the hyperbaric formulation.
Etidocaine. Etidocaine, which is chemicallyrelated to lignocaine, is the latest local anaestheticintroduced for clinical use. This agent is charac-terized by very rapid onset, prolonged duration ofaction, and profound sensory and motor blockade.Etidocaine may be used for infiltration, peripheralnerve blockade and extradural anaesthesia. Al-though etidocaine and bupivacaine provide pro-longed durations of anaesthesia, significantdifferences exist with regard to the anaestheticprofile of these two local anaesthetics. Etidocainehas a significantly more rapid onset of action thanbupivacaine. In addition, concentrations of etido-caine which are required for adequate sensoryanaesthesia produce profound motor blockade. Asa result, etidocaine is primarily useful as ananaesthetic for surgical procedures in whichneuromuscular blockade is required. Thus, thisagent is of limited use for obstetric extraduralanalgesia and for postoperative pain relief, since itdoes not provide a differential blockade of sensoryand motor fibres. It is possible to take advantageof the different pharmacological profiles ofetidocaine and bupivacaine in certain clinicalsituations. For example, it is possible to initiateextradural blockade with 1.5% etidocaine forlower limb orthopaedic procedures, such as totalhip replacements, and abdominal surgical pro-cedures. Under these conditions etidocaine pro-vides a rapid onset of action and a profound depthof anaesthesia and neuromuscular blockade.Supplementary intraoperative and postoperativeanaesthesia is then provided by 0.5 % bupivacaine,which produces excellent sensory anaesthesia withminimal motor blockade.
Miscellaneous
Cinchocaine (dibucaine, USF). This agent isessentially used for spinal anaesthesia. It is mostwidely used as a spinal anaesthetic drug outside theU.S.A., while its use is rather limited within theU.S.A. Comparative studies of cinchocaine andamethocaine indicate that the former is morepotent: 0.25% cinchocaine provides a depth ofanaesthesia similar to that produced by 0.5%amethocaine (Rocco et al., 1982). The onset of
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
PHARMACOLOGY OF LOCAL ANAESTHETIC AGENTS 715
action of the two agents is similar, while theduration of anaesthesia is slightly longer withcinchocaine. In addition, the degree of hypotensionand the profoundness of motor blockade was lessin patients receiving intrathecal cinchocaine,compared with subjects in whom amethocaine wasadministered to the subarachnoid space, althoughthe spread of sensory anaesthesia was similar in thetwo groups.
Hyperbaric solutions of 0.25% and 0.5%cinchocaine with 5% glucose are commonlyavailable in most countries. In addition, apre-formulated hypobaric solution of 0.0667%cinchocaine is also available.
Benzocaine. This local anaesthetic is usedexclusively for topical anaesthesia. It is availablein a variety of proprietary and non-proprietarypreparations. The most common forms used in anoperating room setting are as aerosol solutions forendotracheal administration and an ointment forlubrication of endotracheal tubes.
SUMMARY
The most important clinical properties of localanaesthetic agents are potency, onset, duration ofaction and relative blockade of sensory and motorfibres. These qualities are related primarily to thephysicochemical properties of the various com-pounds. In general, lipid solubility determines therelative intrinsic potency of the various agents,while protein binding influences the duration ofanaesthesia and pKa is correlated with the onset ofaction. In general, the local anaesthetics forinfiltration, peripheral nerve blockade, and extra-dural anaesthesia can be classified into threegroups: (1) agents of low potency and short dura-tion, for example procaine and chloroprocaine;(2) agents of moderate potency and duration, forexample lignocaine, mepivacaine and prilocaine;and (3) agents of high potency and long duration,for example amethocaine, bupivacaine and etido-caine. These local anaesthetics also vary in termsof onset: chloroprocaine, lignocaine, mepivacaine,prilocaine and etidocaine have a rapid onset, whileprocaine, amethocaine and bupivacaine are charac-terized by a longer latency period.
REFERENCES
Albert, J., and Lofstrom, B. (1965). Bilateral ulnar nerve blocksfor the evaluation of local anaesthetic agents. ActaAnatsthtsiol. Scand., 9, 203.
Armstrong, I. R., Littlewood, D. G., and Chambers, W. A.(1983). Spinal anesthesia with tetracaine—effect of addedvasoconstrictor. Anesth. Analg., 62, 793.
Braid, D. P., and Scott, D. B. (1965). The systemic absorptionof local analgesic drugs. Br. J. Anaesth., 37, 394.
Bridenbaugh, L. D. (1978). Does the addition of low molecularweight dextran prolong the duration of action of bupivacaine ?Rig. Anesth., 3, 6.
Bromage, P. R. (1965a). A comparison of the hydrochloridesalts of Lignocaine and prilocaine for epidural analgesia. Br.J. Anaesth., 37, 753.
(1965b). A comparison of the hydrochloride and carbondioxide salts of lidocaine and prilocaine in epidural analgesia.Acta Anaesthesiol. Scand. (Suppl.), 16, 55.
(1970). An evaluation of two new local anaesthetics formajor conduction blockade. Can. Anaesth. Soc. J., 17, 557.
Brown, D. T., Morrison, D. H., Covino, B. G., and Scon,D. B. (1980). Comparison of carbonated bupivacaine andbupivacaine hydrochloride for extradural anaesthesia. Br. J.Anaesth., 52, 419.
Buckley, F. P., Littlewood, D. G., Covino, B. G., and Scott,D. B. (1978). Effects of adrenaline and the concentration ofsolution on extradural block with etidocaine. Br.J. Anaesth.,50, 171.
Catchlove, R. F. H. (1972). The influence of CO, and pH onlocal anesthetic action. J. Pharmacol. Exp. Ther., 181, 291.
Chambers, W. A., Edstrom, H. H., and Scott, D. B. (1981).Effect of baricity on spinal anesthesia with bupivacaine. Br.J. Anaesth., 53, 279.
Littlewood, D. G., Logan, M. R., and Scott, D. B.(1981). Effect of added epinephrine on spinal anesthesia withlidocaine. Anesth. Analg., 60, 417.
Scott, D. B. (1982). Spinal anaesthesia withhyperbaric bupivacaine: effect of added vasoconstrictors.Anesth. Analg., 61, 49.
Chantigian, R. C , Datta, S., Berger, G. A., Naulty, J. S.,Lambert, D. H., and Ostheimer, G. W. (1984). Anesthesiafor Cesarean delivery utilizing spinal anesthesia: tetracaineversus tetracaine and procaine. Reg. Antsth., 9, 195.
Cohen, S. E., and Thurlow, A. (1979). Comparison of achloroprocaine-bupivacaine mixture with chlorprocaine andbupivacaine used individually for obstetric epidural anal-gesia. Anesthesiology, 51, 288.
Cole, C. O., McMorland, G. H., Axelson, J. E., and Jenkins,L. C. (1985). Epidural blockade for Cesarean sectioncomparing lidocaine hydrocarbonate and lidocaine hydro-chloride. Anesthesiology, 62, 348.
Conception, M., Maddi, R., Francis, D., Rocco, A. G.,Murray, E., and Covino, B. G. (1984). Vasoconstrictors inspinal anesthesia with tetracaine. A comparison of epine-phrine and phenylephrine. Anesth. Analg., 63, 134.
Corke.B. G., Carlson, C. G.,andDettbam,W. D. (1984). Theinfluence of 2-chloroprocaine on the subsequent analgesicpotency of bupivacaine. Anesthesiology, 60, 25.
Covino, B. G., and Bush, D. F. (1975). Clinical evaluation oflocal anaesthetic agents. Br. J. Anaesth., 47, 289.
Covino, B. G., and Vassallo, H. G. (1976). Mechanisms ofaction and clinical use; in Local Anesthetics. Grune &Stratton.
Crawford, O. B. (1964). Comparative evaluation in periduralanesthesia of lidocaine, mepivacaine and L-67, a new localanesthetic agent. Anesthesiology, 25, 321.
Cunningham, N. L., and Kaplan, J. A. (1974). A rapid onsetlong acting regional anesthetic technique. Anesthesiology, 41,509.
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022
716 BRITISH JOURNAL OF ANAESTHESIA
Dhuner, K. G., and Lewis, D. (1966). Effect of localanaesthetics and vasoconstrictors upon regional blood flow.Ada Anaetthesiol Scand., 23, 347.
Eckstein, K. L., Vincente-Eckstein, A., Steiner, R., andMissler, V. (1978). Klinische erprobung von bupivacaineCO,. Anaesthetist, 27, 1.
Erdimir, H. A., Soper, L. E., and Sweet, R. B. (1965). Studiesof factors affecting peridural anesthesia. Anesth. Analg., 44,400.
Galindo, A., Schou, M., and Witcher, T. (1981). pH-Adjustedlocal anesthetics; in Proceedings of the American Society ofRegional Anesthesia, p. 50.
Witcher, T. (1980). Mixtures of local anesthetics:bupivacaine-chloroprocaine. Anesth. Analg., 59, 683.
Gissen,A. J.,Covino,B. G., and Gregus.J. (1980). Differentialsensitivity of mammalian nerves to local anesthetic drugs.Anesthesiology, 53, 467.
(1982). Differential sensitivity of fast and slowfibres in mammalian nerve. I l l Effect of etidocaine andbupivacaine on fast/slow fibres. Anesth. Analg., 61, 370.
(1985). Differential sensitivity of fast and slowfibres in mammalian nerve. IV Effect of carbonatkm of localanesthetics. Reg. Anesth., 10, 68.
Gramling, Z. W., Ellis, R. G., and Volpitto, P. P. (1964).Clinical experiences with mepivacaine (Carbocaine). J.M.A.Georgia, 53, 16.
Hilgier, M. (1985). Alkalinizarjon of bupivacaine for brachialplexus block. Reg. Anesth., 10, 59.
Keir, L. (1974). Continuous epidural analgesia in prostatec-tomy: comparison of bupivacaine with and withoutadrenaline. Ada Anaesthesiol. Scand., 18, 1.
Littlewood, D. G., Buckley, P., Covino, B. G., Scott, D. B.,and Wilson, J. (1979). Comparative study of various localanaesthetic solutions in extradural block in labour, fir. J.Anaesth., 51, 47.
Loder, R. E. (1960). A local anaesthetic solution with longeraction. Lancet, 2, 346.
Lund, P. C , and Cwik, J. C. (1965). Propitocaine (Citanest)and methemoglobinemia. Anesthesiology, 26, 569.
McClure, J. H., and Scott, D. B. (1981). Comparison ofbupivacaine hydrochloride and carbonated bupivacaine inbrachial plexus block by the inter-scalen technique, fir. J.Anaesth., 53, 523.
Meagher, R. P., Moore, D. C , and DeVries, J. C. (1966). Themost effective potentiator of tetracaine spinal anesthesia.Anesth. Analg., 45, 134.
Morrison, D. H. (1981). A double-blind comparison ofcarbonated lidocaine and lidocaine hydrochloride in epiduralanaesthesia. Can. Anaesth. Soc. J., 28, 387.
Ravindran, R. S., Bond, V. K., Tasch, M. D., Gupta, C. D.,and Luerssen, T. G. (1980). Prolonged neural blockadefollowing regional analgesia with 2-chloroprocaine. Anesth.Analg., 58, 447.
Resiner, L. S., Hochman, B. N., and Plumer, M. H. (1980).Persistent neuralgia deficit and adhesive arachnoiditisfollowing intrathecal 2-chloroprocaine injection. Anesth.Analg., 58, 452.
Ritchie, J. M., Ritchie, B., and Greengard, P. (1965). Theactive structure of local anesthetics. J. Pharmacol. Exp. Ther.,150, 152.
Rocco, A. G., Concepcion, M., Sheskey, M. C , Murray, E.,Edstrom, H., and Covino, B. G. (1984). A double-blindevaluation of intrathecal bupivacaine without glucose and astandard solution of hyperbaric tetracaine. Reg. Anesth., 9,1.
Francis, D. M., Wark, J. A., Concepcion, M. A., andCovino, B. G. (1982). A clinical double-blind study ofdibucaine and tetracaine in spinal anesthesia. Anesth. Analg.,61, 133.
Rosenblatt, VL M., and Fung, D. L. (1979). Optional ratio ofbupivacaine and dextran for regional anesthesia. Reg.Anesth., 4, 2.
(1980). Mechanism of action of dextran prolongingregional anesthesia. Reg. Anesth., 5, 3.
Scon, D. B., and Cousins, M. J. (1980). Clinical pharmacologyof local anesthetic agents; in Neural Blockade (edsM. J. Cousins and P. O. Bridenbaugh), p. 80. Philadelphia:J. B. Lippincott.
McClure, J. H., Giasi, R. M , See, J., and Covino, B. G.(1980). Effects of concentration of local anaesthetic drugs inextradural block. Br. J. Anaesth., 52, 1033.
Sheskey, M. C , Rocco, A. G., Bizzarri-Schmid, M., Francis,D. M., Estrom, H., and Covino, B. G. (1983). A dose-response study of bupivacaine for spinal anesthesia. Anesth.Analg., 62,391.
Sinclair, C. J., and Scott, D. B. (1984). Comparison ofbupivacaine and etidocaine in extradural blockade. Br. J.Anaesth., 56, 147.
Swerdlow, M., and Jones, R. (1970). The duration of actionof bupivacaine, prilocaine and lignocaine. Br. J. Anaesth., 42,335.
Truant, A. P., and Takman, B. (1959). Differential physical-chemical and neuropharmacologic properties of localanesthetic agents. Anesth. Analg., 38, 478.
Wildsmith, J. A. W., Gissen, A, J., Gregus, J., and Covino,B. G. (1985). Differential nerve blocking activity ofamino-ester local anaesthetics. Br. J. Anaesth., 57, 612.
Dow
nloaded from https://academ
ic.oup.com/bja/article/58/7/701/279293 by guest on 27 M
ay 2022