Mucosal-incision assisted biopsy for suspected gastric gastrointestinal stromal tumors
Upload
independentCategory
view
0download
0
www.elsevier.com/locate/jhep
Journal of Hepatology 50 (2009) 501–510
Liver biopsy findings from healthy potential living liver donors: Reasonsfor disqualification, silent diseases and correlation with liver injury testsq
Marta I. Minervini1,*, Kristine Ruppert6, Paulo Fontes5, Riccardo Volpes2,Giovanni Vizzini2, Michael E. de Vera5, Salvatore Gruttadauria3,
Roberto Miraglia7, Loredana Pipitone1, J. Wallis Marsh5,Amadeo Marcos5, Bruno Gridelli3, Anthony J. Demetris4
1Department of Pathology, University of Pittsburgh Medical Center-ISMETT, Italy2Department of Hepatology, University of Pittsburgh Medical Center-ISMETT, Italy
3Department of Surgery, University of Pittsburgh Medical Center-ISMETT, Italy4Department of Pathology, University of Pittsburgh Medical Center, Pittsburgh, PA, USA
5Department of Surgery, University of Pittsburgh Medical Center, Pittsburgh, PA, USA6Diabetes Institute, University of Pittsburgh Medical Center, Pittsburgh, PA, USA
7Department of Radiology, University of Pittsburgh Medical Center-ISMETT, Italy
Background/Aims: Liver biopsies detect silent donor disease in potential living liver donors and provide material for stud-
ies of subclinical non-alcoholic fatty liver disease (NAFLD).
Our primary goal was to determine the contribution of biopsy findings to potential donor evaluation. Factors contrib-
uting to pre-clinical NAFLD and correlations between liver injury tests and histopathology have been also determined.
Methods: Patient records, laboratory tests and results of the histopathologic examination and diagnoses of 284 patients
from 2001 to 2005 were retrospectively extracted from the EDIT database. Hepatic histology was correlated with liver
injury tests and with general demographic characteristics in an otherwise normal healthy population.Results: A minority (n = 119; 42%) of biopsies from this population of 143 males /141 females (average age = 36.8 -
years; mean BMI = 26.6) were completely normal. The remainder showed steatosis (n = 107; 37%), steatohepatitis
(n = 44; 15%), or unexplained low-grade/early stage chronic hepatitis, primary biliary cirrhosis, or nodular regenerative
hyperplasia (n = 16; 6%). Biopsy findings disqualified 29/56 donors. Independent risk factors for NAFLD by multivariate
modeling, which differed by sex, included: BMI (p = 0.0001), age (p = 0.003), iron (p = 0.01), and ALT (p = 0.004).
Conclusions: Liver biopsies provide valuable information about otherwise undetectable liver disease in potential liver
donors. Obesity, age and iron, which are influenced by sex, contribute to NAFLD pathogenesis. Blood tests other than
standard liver profiles are needed to detect early NAFLD.� 2008 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Keywords: Living donor liver biopsy; Non-alcoholic fatty liver disease; Liver injury tests; Steatohepatitis; Transplantation
0168-8278/$34.00 � 2008 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
doi:10.1016/j.jhep.2008.10.030
Received 28 April 2008; received in revised form 26 August 2008; accepted 4 October 2008; available online 29 December 2008
Associate Editor: P.-A. Clavienq The authors declare that they do not have anything to disclose regarding funding from industries or conflict of interest with respect to this paper.* Corresponding author. Tel.: +11 091 2192 449; fax: +11 091 2192 430.
E-mail address: [email protected] (M.I. Minervini).Abbreviations: BMI, body mass index; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; ALP, alkaline phosp-
hatase; ALT, alanineaminotransferase; GGTP, gamma glutamyl transferase; TBIL, total bilirubin; H&E, hematoxilin & eosin; PAS-D, periodic-acid-Schiff with diastase digestion; IsMeTT, Mediterranean Institute for Transplantation and Advanced Specialized Therapies; UPMC, University ofPittsburgh Medical Center.

502 M.I. Minervini et al. / Journal of Hepatology 50 (2009) 501–510
1. Introduction
Liver biopsies obtained during the evaluation ofpotential living liver donors attempt to minimize donorand recipient risk by disqualifying suboptimal organsthat might not recover properly after partial hepatec-tomy and/or transplantation [1–5]. Obtaining biopsiesin this circumstance is generally considered to be safe,a useful screening tool, and most diseases uncoveredhave been mild/early stage and within the spectrum ofnon-alcoholic fatty liver disease (NAFLD) [1–5]. Otherdiseases have also been discovered and up to 12% ofpotential donors are disqualified on the basis of biopsyfindings alone [1–4].
Living donor biopsies [1–5] also provide a uniquesource of ‘‘normal” liver tissue and an opportunity tostudy the prevalence and identify risk factors for hepaticsteatosis and steatohepatitis in the general population.Correlating hepatic histology with liver injury testsand with demographic characteristics in an otherwisenormal healthy population has the potential: (1) to pro-vide insights into pre-clinical disease pathogenesis and(2) to serve as a quality control measure to determineif the normal range for liver injury tests accuratelyreflects histologically normal liver.
This study was based on an analysis of biopsies frompotential living liver donors obtained at one Italian andone American site. Our primary goal was to determinethe contribution of biopsy findings to potential donorevaluation. However, correlations among biopsyfindings, liver injury tests, and patient demographiccharacteristics enabled us to study factors contributingto pre-clinical NAFLD and to examine correlationsbetween liver injury tests and histopathology.
Table 1
Protocol used to evaluate potential living donors before transplantation.
Evaluation protocol Testing/procedure
Day 1 Laboratory evaluation including blood typingElectrocardiogram and echocardiogramChest X-ray and pulmonary function testsAbdominal ultrasound
Day 2 Abdominal computerized tomography (CT)scan with maximum intensity projections*
and liver volume measurementsCholangio magnetic resonance imagingCardiology and anesthesiology consults
Day 3 Liver biopsySocial worker consult
Day 4 Complete blood count and liver ultrasound
*Maximum Intensity Projection (MIP) is commonly used to extractvascular structures from medical CT data sets (i.e., angiography) byconnecting high intensity dots of blood vessels in three dimensions andproviding an angiogram that can be viewed from any projection.
2. Patients and methods
After informed consent, 284 potential living liver donors evaluatedbetween January 2001 and June 2006 underwent a three-phase evalua-tion protocol at the University of Pittsburgh Medical Center, Pittsburghand Palermo (Mediterranean Institute for Transplantation andAdvanced Specialized Therapies (IsMeTT). The protocol included aphysical examination, laboratory studies, radiological imaging andprotocol liver biopsy (Table 1). The first seven potential donors atUPMC-Palermo were not subjected to a liver biopsy, but after internaldiscussions about the risk–benefit ratio of detecting clinically and sero-logically silent donor diseases, the protocol was changed to include a rou-tine liver biopsy. A Menghini needle obtained right lobe biopsies atUPMC-Palermo between 2003 and 2005, but two bleeding complica-tions prompted a switch to an ultrasound-guided 18-gauge needle per-formed by a radiologist, which was routinely used at UPMC-Pittsburgh.
All donors were screened by history for alcohol consumption. Mostconsumed less than 14 U of alcohol per week and all were instructed todiscontinue all alcohol consumption after starting evaluation. Liverbiopsies were used to evaluate liver pathology after 3–4 months ofabstinence in the few potential donors consuming >14 U/week. Rou-tine screening for insulin resistance or lipid profiles was not performed.
Liver injury tests at UPMC-Palermo are generated on a Dade Beh-ring – Dimension RL Max using FLEX reagents cartridges for alkalinephosphatase (ALP), aspartate aminotransferase (AST), alanine amino-transferase (ALT), gamma glutamyl transferase (GGTP), and direct
and total bilirubin (TB). The normal ranges for these tests atUPMC-Palermo are: ALT: 30–65 U/L; AST: 15–37 U/L; ALP: 50–136 U/L; TBIL: 0–1 mg/dl; direct bilirubin: 0.00–0.30 mg/dl. AtUPMC-Pittsburgh, the liver tests are measured in Johnson & JohnsonVitros 950. Normal values for adults are: ALT and AST (640 IU/L);ALP (40–125 IU/L) and total bilirubin (0.3–1.5 mg/dl).
2.1. Routine histopathologic analyses
All specimens were formalin-fixed, paraffin-embedded, and sec-tioned at 4 lm. Two Hematoxilin & Eosin stain (H&E), one peri-odic-acid-Schiff with diastase digestion (PAS-D), one Prussian blueiron, and one Masson’s trichrome stain were routinely prepared. Retic-ulin and rhodanine stains were used in cases where either nodularregenerative hyperplasia or an unexplained ductular reaction wasdetected on the H&E stains. All biopsies were examined and inter-preted by experienced members of the Division of Liver and Trans-plantation Pathology. Each member has at least 4 years of specialtytraining and/or experience in hepatic pathology. Reviews were com-pleted without knowledge of liver injury tests.
Severity of macrovesicular steatosis was estimated and reported aspercent of involved hepatocytes to the nearest 5% using the 20� objec-tive. NAFLD was defined as P5% macrovesicular steatosis; biopsieswith <5% macrovesicular steatosis were not included in the steatosiscategory. When present, the percentage of microvesicular steatosiswas separately stated. Criteria for steatohepatitis (NASH) includedsteatosis associated with hepatocyte swelling/degeneration and lobularinflammation and hepatocyte injury marked by PAS/D+ ceroid-ladenmacrophages [6,7]. No ancillary stains were used for either quantitativeand/or qualitative assessment of steatosis.
Other histopathologic findings such as portal and lobular inflam-mation, portal/periportal fibrosis, iron deposition; and vascular or bileduct abnormalities were described as mild, moderate to severe. Patientrecords, laboratory tests and histopathologic readings were prospec-tively entered into the EDIT database [8] and then extracted for thisstudy. All ISMETT biopsies (MM and AJD) and any biopsy fromUPMC showing significant pathology were reviewed by at least twopathologists, who agreed on the findings. Finally, at least 20 randomcases were reviewed at quality assurance conferences to periodicallycheck the level of agreement. In general, biopsies showing >25% macr-ovesicular steatosis disqualified potential donors, although mitigatingcircumstances, such as co-existent steatohepatitis, were also considered.
2.2. Statistical analyses
Basic demographics were described using measures of central ten-dency (means and medians) and spread (standard deviation and range)

M.I. Minervini et al. / Journal of Hepatology 50 (2009) 501–510 503
for continuous data and frequencies and percentages for categoricaldata. Comparisons between groups were performed using Kruskill–Wallis, Chi-square, Analysis of Variance, Rank sum, and t-tests. Livertests, age and BMI were transformed where appropriate. Spearmancorrelation was performed. Logistic regression was used to examinepredictors of NAFLD to examine correlations between the percentof steatosis and various demographic factors. Mixed models wereemployed to compare histology between males and females. Sensitivityand specificity analysis was used to examine if ALT and AST couldcorrectly identify those patients with NAFLD. All analyses were per-formed using SAS 9.1 and STATA 8.0.
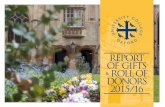
Fig. 1. Composite of a typical case of steatohepatitis. Note at low power
the mild mononuclear portal inflammation, significant, predominantly
macrovesicular steatosis involving about 30% of hepatocytes, and
lymphohistiocytic inflammation within the lobules surrounding steatotic
hepatocytes (inset).
3. Results
3.1. General demographic characteristics of population
and histopathologic diagnoses on biopsy
There were 284 potential donors, comprising 143(50.4%) males and 141 (49.6%) females, 190 Americans(66.9%), 82 Italians (28.9%) and 12 patients for whichnationality was unknown. Two hundred and sixty-two(262) patients were Caucasian (92.3%), 10 non-Cauca-sian (3.5%), and 12 (4.2%) of unknown race. The aver-age age was 36.8 ± 10.6 years (median = 36; range18.1–61.0 years).
The primary or most important histopathologic diag-nosis is shown in Table 2. A majority of biopsies(n = 224; 78.9%) was either normal or showed very mild,nonspecific, portal and/or lobular inflammation ormacro or microvesicular steatosis ranging from 5% to60% without steatohepatitis (NAFLD) (n = 107/284;37.7%). Steatohepatitis (Fig. 1) was the primaryhistopathologic diagnosis in 44/284 (15.5%) biopsies.Low-grade nodular regenerative hyperplasia was presentin 6/284 (2.1%) patients and early stage primary biliarycirrhosis was fortuitously detected in one patient(Fig. 2). The 9 (3.2%) remaining biopsies showed miscel-laneous changes such as unexplained low-grade chronichepatitis characterized by focal mild portal chronicinflammation and focal interface activity (Fig. 3); mod-erate portal/periportal fibrosis; unexplained ductularreaction; abundant mega-mitochondria associated withan initially concealed history of binge drinking; 2+ iron
Table 2
Distribution of primary, or most important, histopathologic diagnoses.
Number Percent
Final primary histopathologic diagnosis
Non-specific changes 193 68.0Non-specific inflammation 31 10.9Steatohepatitis, NOS 44 15.5Nodular regenerative hyperplasia 6 2.1Primary biliary cirrhosis 1 0.4Miscellaneous 9 3.2
Miscellaneous includes chronic portal inflammation, ductular reaction,moderate portal/periportal fibrosis, abundant mega-mitochondria,and 2–3+ iron deposition.
deposits in periportal hepatocytes (Fig. 4), and portaleosinophilia of unknown cause or significance.
In our opinion, the two most unexpected and unex-plained findings in this series of patients were portaleosinophilia of unknown cause or significance (n = 2)and periportal hepatocyte iron deposits. Despite anextensive clinical, historical, and serological evaluationfor the common causes of eosinophilia, no underlyingcause was detected in these two Italian patients. The liv-ers were used for transplantation without incident. Ironis stored in the liver, but stainable iron present predom-inantly in periportal hepatocytes from 44/284 (15.5%)potential donors was also an unexpected finding. Anoutcome study of recipient complications after livertransplant in this series of patients showed no statistical
Fig. 2. Liver biopsy showing the early stages of primary biliary cirrhosis.
Note the patchy, but significant, lymphoplasmacytic and granulomatoid
portal inflammation on low magnification in the upper inset. The involved
portal tract is shown at higher magnification in the bottom insets. This
potential female donor showed only a slightly elevated alkaline
phosphatase of 106 IU/L, and the AST = 41 IU/L, ALT = 31 IU/L,
and total bilirubin 0.4 mg/dl were within normal limits. This donor was
disqualified on the basis of the biopsy findings.

Fig. 3. An example of very low-grade, but unexplained, chronic hepatitis.
Note the mild mononuclear portal inflammation involving several portal
tracts in this biopsy. No inflammatory bile duct damage was detected and
there was only minimal interface activity. Nevertheless, this donor was
disqualified because of the biopsy findings.
504 M.I. Minervini et al. / Journal of Hepatology 50 (2009) 501–510
effect of stainable hepatic iron on recipient or graft sur-vival or the incidence or severity of complications aftertransplantation (J.W. Marsh, manuscript in prepara-tion, personnel communication).
3.2. Reasons for donor disqualification
A total of 228/284 (80.3%) of the donors proceededwith donation. The most common biopsy findings thatled to donor disqualification included steatosis and/orsteatohepatitis with macrovesicular steatosis involving>25% of hepatocytes (n = 20/56; 35.7%), unexplainedhepatitis or moderate portal/periportal fibrosis (n = 7/56; 12.5%), early primary biliary cirrhosis (n = 1/56;
Fig. 4. Stainable hepatocellular iron deposits were an unexpected finding
in nearly 20% of all donor biopsies. The deposits were scored as 1+, on a
scale of 0–4, in 90% of the biopsies with iron. But 10% showed at least
2+ deposits all of which were used for transplantation without significant
problems after transplantation.
1.8%), and nodular regenerative hyperplasia particularlywhen associated with changes suspicious for portal ven-opathy (n = 1/56; 1.8%). Other donor-related reasonsfor disqualification included an anatomy incompatiblewith the recipient (n = 8/56; 14.3%); non-hepatic medi-cal problems, and unsuitable psychological profile and/or ‘‘second thoughts” about donation (n = 11/56;19.6%). Other donors were not used because the recipi-ent was disqualified (n = 3/56; 5.3%) or received acadaveric organ (n = 5/56, 8.9%).
3.3. Analysis of livers with NAFLD
One hundred and thirty-eight patients (138/268;51.5%) showed no significant steatosis (<5%); theremaining 130 (48.5%) patients showed macrovesicularranging from 5% to 90%; 44 (15.5%) also showed ste-atohepatitis (Fig. 1). When normal livers were com-pared with NAFLD the following factors weresignificant in univariate analyses: ethnicity (Italians34% vs. Americans 54% with NAFLD; p = 0.004),more stainable hepatic iron (p = 0.001), older age(40.1 vs. 33.7 years; p = 0.0001), BMI (28.2 vs. 25.0;p = 0.0001), ALP (81.7 vs. 74.1 U/L; p = 0.003), ALT(43.1 vs. 33.4; p = 0.0008), and AST (28.2 vs. 24.0 U/L). Multivariate modeling showed BMI (p = 0.0001),age (p = 0.003), ALT (p = 0.004), and iron (p = 0.01)independently increased NAFLD risk. Americans weresignificantly heavier than the Italians and it was theBMI and not the ethnicity that increased the risk ofNAFLD.
Quantitative correlations between percent steatosisand various demographic factors (Fig. 5) showed thefollowing correlation coefficients: BMI (0.44; p =0.0001), age (0.29; p = 0.0001), ALT (0.26; p = 0.0001),and AST (0.21; p = 0.0006).
A more detailed analysis of liver biopsies stratifiedaccording to the absence of fat (<5%), >5% fat withoutsteatohepatitis, and steatohepatitis (Table 3) enabled usto examine some factors that might precipitate steato-hepatitis. No significant difference was found for genderor race. Steatotic biopsies, however, showed more stain-able iron (p = 0.0001), and were obtained more oftenfrom Americans (p < 0.0009) and older individuals(38.4 vs. 33.7 years; p = 0.001) with a higher BMI(27.6 vs. 25.0; p < 0.0001) and higher ALP levels (79.8vs. 74.1 IU/ml; p = 0.02). ALT (37.5 vs. 33.4 IU/L;p = 0.15) and AST (26.3 vs. 24.0; p = 0.06) were higherin those with steatosis, but the differences were not sta-tistically significant.
After adjusting for age and ethnicity, males weremore likely to develop hepatic steatosis than females(p = 0.03) and male donors with a BMI 6 25 are morelikely to show fat on biopsy (p = 0.02). In addition,male NAFLD donors showed significantly higher liverinjury tests than female NAFLD donors (Table 4).

020
4060
80%
Ste
atos
is
20 25 30 35 40 45BMI
P=0.0001
020
4060
80%
Ste
atos
is
20 30 40 50 60Age
P=0.0001
020
4060
80%
Ste
atos
is
0 100 200 300ALT
P=0.0001
020
4060
80%
Ste
atos
is0 50 100 150
AST
P=0.0006
Fig. 5. Scatter plot showing correlation between the percent steatosis in the biopsy and various demographic and laboratory parameters.
M.I. Minervini et al. / Journal of Hepatology 50 (2009) 501–510 505
Since sex influenced the presence of fat and extent ofliver test elevations, multivariate models comparingnormal to NAFLD was done separately for malesand females. In females (n = 135) multivariate model-ing showed that BMI (p = 0.0001) and age (p = 0.02)independently increased the risk of NAFLD, whereasin males (n = 133) the independent risk factors wereelevated ALT (p = 0.0001, BMI (p = 0.003) and iron(p = 0.006).
Univariate analysis comparing steatotic livers tothose with steatohepatitis showed that American ethnic-ity (p = 0.06), Caucasian race (p = 0.01), less stainableiron (p = 0.006), older age (43.3 vs. 38.4 years;p = 0.006), and higher BMI (29.2 vs. 27.6; p = 0.03),ALT (54.0 vs. 37.5 IU/L; p = 0.0007), and AST (31.9vs. 26.3 IU/L; p = 0.01) were associated with steatohep-atitis. Significantly elevated ALT and AST in steatohep-atitis independently substantiates the validity of thehistopathologic criteria and diagnosis. In a multivariatemodel (n = 151), older age (p = 0.002), less stainableiron (p = 0.002), and higher ALT (p = 0.0001) wereassociated with steatohepatitis.
3.4. Iron analyses
Intrigued with the above results, we undertook amore detailed analysis of the predominantly periportalhepatocellular iron deposits found in 49/284 (17.2%)biopsies. Five showed 2+ deposits, on a scale of 0–4,and the remaining donors showed 1+ deposits. Twocases with 2+ deposits also showed mild subsinusoidal
fibrosis. Interestingly, 41/49 (84%) biopsies with stain-able iron were obtained from male potential donors(p = 0.0001). Livers without iron and without fat werecompared to livers with iron alone, with fat alone, andwith iron and fat (Table 5). Biopsies with other histo-pathologic findings/diagnoses were excluded. Resultsshowed that iron alone did not significantly increaseliver injury tests, but fat alone significantly increasedserum ALT (41.6 vs. 33.7 U/L; p 6 0.04), AST (27.3vs. 24.0; p 6 0.04), and ALP (82.1 vs. 73.4 U/L;p = 0.004) compared to normal livers with neither ironnor fat. ALT and AST increases were even more signif-icant when iron and fat were found together (see Table5) suggesting that iron and fat act together to causehepatocyte injury and enzyme release. The effect is morepronounced in males, probably because females excreteiron during or before menopause.
3.5. Correlation between liver histopathology and liver
injury tests
Sex and BMI significantly influence ‘‘normal”ranges for liver injury test when values are determinedwithout liver biopsies [9,10], significant liver NAFLDcan occur with normal liver injury tests [11], andabove we showed that sex affects deposition of iron,fat and liver injury tests. Therefore, we conductedreceiver operator characteristics/area under the curve,sensitivity, specificity, positive and negative predictivevalue analyses to determine the correlation betweenliver injury tests and liver histology (Table 6). Once

Table 3
Stratification of biopsies according to the presence or absence of steatosis and steatohepatitis. Patients whose biopsies received other histopathologic
diagnosis were excluded.
Variable Neg. steatosis <5% Steatosis alone Steatohepatitis Total p-value
N = 138 (%) N = 86 (%) N = 44 (%) N = 268 (%)
Gender 0.53a 0.22b
Male 63 45.7 43 50.0 27 61.4 133 49.6Female 75 54.3 43 50.0 17 38.6 135 50.4
Ethnicity 0.0009a 0.06b
Italian 49 35.5 13 15.1 12 27.3 74 27.6Non-Italian 85 61.6 70 81.4 28 63.6 183 68.3Missing 4 2.9 3 3.5 4 9.1 11 4.1
Race 0.40a 0.01b
White 130 94.2 82 95.3 35 79.5 247 92.2Non-White 4 2.9 1 1.2 5 11.4 10 3.7Missing 4 2.9 3 3.5 4 9.1 11 4.1
Iron 0.0001a 0.006b
No 123 89.1 57 66.3 39 88.6 219 81.7Yes 15 10.9 29 33.7 5 11.4 49 18.3
Age 0.001a 0.006b
Mean [SD] 33.7 [10.7] 38.4 [9.7] 43.3 [8.6] 36.8 [10.6]Median 31 37.7 43.7 35.7Range 18.1–61.0 19.8–57.4 25.9–57 18.1–61.0
BMI <0.0001a 0.03b
Mean [SD] 25.0 [4.3] 27.6 [4.5] 29.2 [4.1] 26.6 [4.7]Median 23.8 26.4 29.3 25.6Range 19.5–43.5 20.1–42.2 22.2–39.9 19.5–43.5
ALKP 0.02a 0.38b
Mean [SD] 74.1 [21.0] 79.8 [19.6] 85.2 [26.9] 77.8 [22.0]Median 71 78 80 75Range 39–215 44–171 40–172 39–215
ALT 0.15a 0.0007b
Mean [SD] 33.4 [14.2] 37.5 [20.7] 54.0 [42.9] 38.2 [24.5]Median 31 31 42.5 32Range 12–89 14–125 19–286 12–286
AST 0.06a 0.03b
Mean [SD] 24.0 [10.2] 26.3 [10.2] 31.9 [18.1] 26.1 [12.2]Median 23 24 27 24Range 10–110 11–72 12–118 10.0–118.0
Abbreviations: ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index.a Comparing normal livers to those with steatosis.b Comparing steatosis to steatohepatitis.
506 M.I. Minervini et al. / Journal of Hepatology 50 (2009) 501–510
the ROC curve was calculated, cutoff values weredetermined that maximized sensitivity and specificity.Then the ratio of those with NAFLD to those whowere combined true- and false-positives was used tocalculate positive predictive values. Conversely, nega-tive predictive values were obtained by calculatingthe ratio of those without NAFLD to those withcombined true and false positive results.
Current ALT and AST upper normal limits (40 U/L)are relatively insensitive for detecting NAFLD, espe-cially in females (Table 6), consistent with the abovefinding that females show lower liver injury tests in thepresence of steatosis compared to males with steatosis.This, in turn, is probably partially attributable to co-
existent iron deposition. Unfortunately, lowering theupper limit of normal increased sensitivity in malesand females, but this occurred at the expense of decreas-ing specificity. Some other blood biochemical test thatreflects NAFLD pathophysiology should be developedfor non-invasive screening programs.
4. Discussion
Obtaining liver biopsies from otherwise healthy peo-ple from the general population who are being consid-ered for living liver donation provides several uniqueopportunities [1–5]. First, the role of liver biopsy in

Table 4
The effect of sex on liver injury tests in patients with steatosis alone on
liver biopsy.
Variable Males(N = 70)
Females(N = 60)
Total(N = 130)
p-value
ALKP 0.62Mean [SD] 80.5 [21.5] 83.1 [23.6] 81.7 [22.4]Median 78 80 78Range 44–171 40–172 40–172Missing 2 1 3
ALT 0.0001Mean [SD] 49.7 [21.5] 35.5 [38.2] 43.1 [31.1]Median 45 28 37Range 22–125 14–286 14–286Missing 1 1 2
AST 0.0001Mean [SD] 31.1 [11.3] 25.0 [15.3] 28.2 [13.6]Median 28 21 24Range 11–72 12–118 11–118Missing 1 0 1
M.I. Minervini et al. / Journal of Hepatology 50 (2009) 501–510 507
exclusion of potential living liver donors can be deter-mined. Second, because of the obesity epidemic in theWestern World, the prevalence of steatosis and steato-hepatitis in the general population can also be studied.Third, these biopsies provide valuable baseline/controlmaterial to determine the accuracy of the normal rangesfor liver injury tests as a monitor of hepatic injury. Thissource of ‘‘control” liver tissue is vastly superior to thatobtained from other sources such as autopsies, non-dis-eased portion of resected livers, back-table and/or pre-reperfusion liver allograft biopsies, and incidental liverbiopsies obtained at the time of laparoscopic surgery.No previous study has closely correlated liver injurytests with hepatic histology in a large, otherwise healthy,general population in Western countries.
Table 5
Comparison of liver injury tests with respect to the presence or absence of iron
Variable Normal Neg. fat,Neg. iron (N = 123)
Neg. fat, Pos.iron (N = 15)
ALTMean [SD] 33.7 [14.5] 30.4 [10.4]Median 31 26.6Range 12–89 17–58Missing 3 1
ASTMean [SD] 24.0 [10.7] 24.3 [3.6]Median 22 24Range 10–110 19–31Missing 2 1
ALKPMean [SD] 73.4 [21.3] 80.4 [18.5]Median 70 79Range 39–215 48–113Missing 2 1
*p 6 0.04 vs. normal; **p = 0.0001 vs. normal; *** p = 0.004 vs. normal.
Biopsy findings alone contributed to the disqualifica-tion of 29/284 (10%) donors, a rate that compares favor-ably with other studies (Table 7) [1–5]. Macrovesicularsteatosis involving >25% of hepatocytes with/out steato-hepatitis accounted for 20/29 biopsy-based disqualifica-tions. Other significant liver diseases were alsouncovered in this and other studies and led to exclusionof potential donors [1–5]. Included were primary biliarycirrhosis, granulomatosis, and schistosomiasis, diseasesthat would not have been discovered using other screen-ing tests/tools. Although the underlying donor liver dis-eases were discovered at an early stage, as might beexpected [1–4], the significant negative impact unex-pected donor deaths or significant complicationsbecause of pre-existing and undetected donor diseasecan be used to justify routine biopsy sampling [12,13].
The baseline prevalence of NAFLD in this study was53% in an otherwise healthy typical Western World pop-ulation. This compared favorably with our literaturereview of similar potential living liver donors (n = 631)who showed an equal sex distribution, a mean BMI of26.3, and a biopsy-proven NAFLD prevalence of 39%(Table 7). Interestingly, however, a male-predominantAsian population (Table 7) showed a similar NAFLDprevalence (53%), but a significantly lower BMI (23.3vs. 26.3) [5]. Asian NAFLD patients reportedly have sig-nificantly lower BMI [5,14] and more visceral adiposity[15] and subcutaneous fat [16] than Caucasians.
Multivariate modeling showed BMI (p = 0.0001), age(p = 0.003), ALT (p = 0.004), and iron (p = 0.01) inde-pendently increased the NAFLD risk. All of these fac-tors have been mentioned in one or more previousstudies and/or reviews [11,14,17–19]. However, a moredetailed analysis of the affect of sex and iron and corre-lation with liver test enabled us to uncovered some novel
and fat in the liver biopsy.
Pos. fat, Neg.iron (N = 96)
Pos. fat, Pos.iron (N = 34)
Total(N = 268)
41.6 [33.6]* 47.5 [22.4]** 38.2 [24.5]32 43 3214–286 24–110 12–2864 0 8
27.3 [14.6]* 30.9 [10.0]** 26.1 [12.2]24 30 2411–118 18.0–63.0 10–1183 0 6
82.1 [25.0]*** 80.6 [13.4]* 77.8 [22.0]78 79.5 7540–172 56–109 39–2153 0 6

Table 6
Receiver operator characteristics, sensitivity, specificity positive predictive value (PPV), and negative predictive values (NPV) for various different cutoffs
for normal AST and ALT values.
Variable ROC/AUC Cutoff Sensitivity (%) Specificity (%) PPV (%) NPV (%)
ALT
All males 0.72 40 64.0 74.0 71.0 78.0All males 0.72 37 72.0 71.0 71.0 82.0Males BMI </= 23** 0.69 37 78.0 72.0 73.0 85.0Males BMI > 23 0.76 36 78.0 72.0 73.0 85.0All females 0.47 40 14.0 86.0 50.0 57.0All females 0.47 24 61.0 34.0 48.0 81.0Females BMI 6 23* 0.85 23 80.0 87.0 86.0 84.0Females BMI > 23 0.52 26 58.0 44.0 51.0 79.0
AST
All males 0.53 40 17.0 100.0 100.0 55.0All males 0.67 25 65.0 62.0 63.0 80.0Males BMI 6 23** 0.81 24 89.0 61.0 70.0 93.0Males BMI > 23 0.65 25 64.0 61.0 62.0 79.0All females 0.67 40 7.0 95.0 58.0 53.0All females 0.53 20 58.0 47.0 52.0 78.0Females BMI 6 23* 0.55 22 60.0 55.0 57.0 78.0Females BMI > 23 0.56 19 67.0 47.0 59.0 82.0
*Sample size N = 36; events = 5.**Sample size N = 27; events = 9.
508 M.I. Minervini et al. / Journal of Hepatology 50 (2009) 501–510
insights into NAFLD pathogenesis. For example, infemales, multi-variant modeling showed that BMI andage were independent risk factors, whereas in males,BMI and iron were independent risk factors. In addi-tion, male livers with steatosis show higher liver injurytests thin female livers with steatosis.
Thirty-four percent (34%) of our NAFLD donorsdeveloped steatohepatitis, which is somewhat higherthan in other studies. This is probably attributable toour sensitive criteria for steatohepatitis [20]. The validity,however, of these histopathological criteria to diagnosesteatohepatitis and distinguish among groups showingnormal liver, steatosis, and steatohepatitis is validatedby the statistically significant segregation of graduallyincreasing liver injury tests among these groups.
Sex also influenced hepatic steatosis and steatohepa-titis. Males with a BMI 6 25 were more likely to have
Table 7
Comparison of findings among previous studies of living donor liver biopsies.
Ref. Rinellaet al. [1]
Ryanet al. [2]
Nadalinet al. [3]
Tot. No. Pts/Biopsies 33 100 144Average Age 32.8 35.6 39Male:Female 19:14 46:54 NAMean BMI NA 26.6 26.0NAFLD 16 (48%) 33 (33%) 21 (14.5Steatohepatitis:steatosis NA 6:27 (18%) 4:17 (19Non-specific inflammation/hepatitis NA 19 (19%) 10 (7%)Granulomas/Misc NA 12 (12%) 4 (3%)Increased iron NA 8 (8%) N/ADisqualified by biopsy NA 3 (3%) 31 (21%Correlation with liver injury tests No No No
NA, not available; *Asian population.
hepatic steatosis on biopsy and males with steatosisshowed significantly higher liver injury tests. Whetherthe difference in liver injury tests between female andmale steatotic livers is a cause or consequence of knownsex differences in the normal ranges for aminotransfer-ase levels [21,22] is uncertain. Since the potential femaledonors in this study were premenopausal, estrogensmight exert some hepatic protective effects against thedevelopment and consequences of hepatic steatosis.
Iron is a controversial, and incompletely understood,risk factor for the development of steatohepatitis(reviewed in [19]). We found that males more frequentlyshow stainable liver iron and there is a direct correlationbetween fat and iron in the liver biopsy (coeffi-cient = 0.19; p = 0.003). And fat and iron togetherincreased liver injury tests more than either fat or ironalone. But it was the fat, and not the iron, that exerted
Tranet al. [4]
Leeet Al* [5]
Currentstudy
Total
70 589 284 122040 31.1 36.8 34.234:36 408:181 143:141 650:42625.9 23.3 26.6 24.8
%) 27 (38.5%) 303 (51.4%) 130 (53%) 530/1220 (43%)%) 5:22 (19%) 13:303 (4%) 44:86 (34%) 72/476 (15%)
5 (7%) 45 (8%) 31 (10.9%) 110/1187 (9.3%)21 (7%) 17 (3%) 16 (6%) 70/1187 (6%)N/A NA 49 (17.3%) 57/384 (15%)
) 9 (13%) NA 29 (10%) 72/598 (12%)No Partial Yes NA

M.I. Minervini et al. / Journal of Hepatology 50 (2009) 501–510 509
the most significant influence. Interestingly, however,fatty livers showed more iron than either normal liversor livers with steatohepatitis. We were initially some-what perplexed by these observations. But the findingssuggest that iron probably does contribute to the devel-opment of steatohepatitis, possibly by functioning as apro-oxidant and/or mitochondrial toxin as previouslysuggested (reviewed in [19]). Once livers evolve, how-ever, from steatosis to steatohepatitis, the increasedhepatocyte injury and turnover probably releases ferritininto the peripheral circulation and dilutes the stainableiron within the liver. Other studies have shown thatapproximately 30% of patients with NAFLD have ele-vated ferritin and there is an association between insulinresistance and hepatic iron (reviewed in [19]). Based onour observations it is reasonable to speculate that ironacts as a pro-oxidative risk factor for steatohepatitisand the effect is observed more often in males becauseof female menstruation during pre-menopausal years(re-viewed in [19]).
Age was also an independent risk factor for the devel-opment of steatohepatitis, as described in other studies[5,11,14,17–19,23]. This might be related to age-relatedchanges in the immune system or the liver, or both. Ageneral tendency for the development of chronic inflam-matory and autoimmune disorders with age [24,25]might more easily trigger an inflammatory response tosteatotic hepatocytes. Or, the gradual loss of hepato-cytes that normally occurs with age [26] might more eas-ily trigger inflammatory response because the dyinghepatocytes contain fat. Both mechanisms might alsocontribute because they are not mutually exclusive.
Individuals with a histopathologic diagnosis of eitherNAFLD or even steatohepatitis showed significantlyhigher liver injury tests than those without steatohepati-tis, but the differences between these groups and patientswith histologically normal biopsies were small and stillwithin the normal range. Therefore, the current ‘‘nor-mal” range for liver injury tests is relatively insensitivefor the detection of either steatosis or steatohepatitis.We believe this data can be used to reinforce the needfor a liver biopsy to accurately quantify hepatic fat con-tent and to detect steatohepatitis in otherwise healthypotential living donors. In addition, we attempted tolower the upper level of ‘‘normal” for ALT and ASTin various subgroups to improve sensitivity for liverinjury tests detection of NAFLD. Unfortunately, theseattempts met with limited success because of decreasedspecificity. Therefore, other biochemical tests on bloodare needed to detect early NAFLD.
References
[1] Rinella ME, Alonso E, Rao S, Whitington P, Fryer J, AbecassisM, et al. Body mass index as a predictor of hepatic steatosis inliving liver donors. Liver Transplant 2001;7:409–414.
[2] Ryan CK, Johnson LA, Germin BI, Marcos A. One hundredconsecutive hepatic biopsies in the workup of living donors forright lobe liver transplantation. Liver Transplant2002;8:1114–1122.
[3] Nadalin S, Malago M, Valentin-Gamazo C, Testa G, Baba HA,Liu C, et al. Preoperative donor liver biopsy for adult living donorliver transplantation: risks and benefits. Liver Transplant2005;11:980–986.
[4] Tran TT, Changsri C, Shackleton CR, Poordad FF, Nissen NN,Colquhoun S, et al. Living donor liver transplantation: histolog-ical abnormalities found on liver biopsies of apparently healthypotential donors. J Gastroenterol Hepatol 2006;21:381–383.
[5] Lee JY, Kim KM, Lee SG, Yu E, Lim YS, Lee HC, et al.Prevalence and risk factors of non-alcoholic fatty liver disease inpotential living liver donors in Korea: a review of 589 consecutiveliver biopsies in a single center. J Hepatol 2007;47:239–244.
[6] Brunt EM, Janney CG, Di Bisceglie AM, Neuschwander-TetriBA, Bacon BR. Nonalcoholic steatohepatitis: a proposal forgrading and staging the histological lesions. Am J Gastroenterol1999;94:2467–2474.
[7] Neuschwander-Tetri BA, Caldwell SH. Nonalcoholic steatohep-atitis: summary of an AASLD Single topic conference. Hepatol-ogy 2003;37:1202–1219.
[8] Demetris AJ, Ruppert K, Dvorchik I, Jain A, Minervini M, NalesnikMA, et al. Real-time monitoring of acute liver-allograft rejectionusing the Banff schema. Transplantation 2002;74:1290–1296.
[9] Giannini EG, Testa R, Savarino V. Liver enzyme alteration: aguide for clinicians. CMAJ 2005;172:367–379.
[10] Piton A, Poynard T, Imbert-Bismut F, Khalil L, Delattre J,Pelissier E, et al. Factors associated with serum alanine transam-inase activity in healthy subjects: consequences for the definitionof normal values, for selection of blood donors, and for patientswith chronic hepatitis C. Hepatology 1998;27:1213–1219.
[11] Mofrad P, Contos MJ, Haque M, Sargeant C, Fisher RA, LuketicVA, et al. Clinical and histologic spectrum of nonalcoholic fattyliver disease associated with normal ALT values. Hepatology2003;37:1286–1292.
[12] Ringe B, Strong RW. The dilemma of living liver donor death: toreport or not to report? Transplantation 2008;85:790–793.
[13] Ringe B, Xiao G, Sass DA, Karam J, Shang S, Maroney TP, et al.Rescue of a living donor with liver transplantation. Am JTransplant 2008;8:1557–1561.
[14] Weston SR, Leyden W, Murphy R, Bass NM, Bell BP, ManosMM, et al. Hepatology 2005;41:372–379.
[15] Park YW, Allison DB, Heymsfield SB, Gallagher D. Largeramounts of visceral adipose tissue in Asian Americans. Obes Res2001;9:381–387.
[16] Wang J, Thornton JC, Russell M, Burastero S, Heymsfield S,Pierson RN, et al. Asians have lower body mass index (BMI) buthigher percent body fat than do whites: comparisons of anthro-pometric measurements. Am J Clin Nutr 1994;60:23–28.
[17] Clark JM. The epidemiology of nonalcoholic fatty liver disease inadults. J Clin Gastroenterol 2006;40:S5–S10.
[18] Liou I, Kowdley KV. Natural history of nonalcoholic steatohep-atitis. J Clin Gastroenterol 2006;40:S11–S16.
[19] McCullough AJ. Pathophysiology of nonalcoholic steatohepatitis.J Clin Gastroenterol 2006;40:S17–S29.
[20] Brunt EM. Nonalcoholic steatohepatitis: pathologic featuresand differential diagnosis. Semin Diagn Pathol 2005;22:330–338.
[21] Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB.Diagnosis and monitoring of hepatic injury. II. Recommendationsfor use of laboratory tests in screening, diagnosis, and monitoring.Clin Chem 2000;46:2050–2068.
[22] Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB.Diagnosis and monitoring of hepatic injury. I. Performancecharacteristics of laboratory tests. Clin Chem 2000;46:2027–2049.

510 M.I. Minervini et al. / Journal of Hepatology 50 (2009) 501–510
[23] Merriman RB, Aouizerat BE, Bass NM. Genetic influences innonalcoholic fatty liver disease. J Clin Gastroenterol2006;40:S30–S33.
[24] Vasto S, Candore G, Balistreri CR, Caruso M, Colonna-Romano G, Grimaldi MP, et al. Inflammatory networks inageing, age-related diseases and longevity. Mech Ageing Dev2007;128:83–91.
[25] Franceschi C, Capri M, Monti D, Giunta S, Olivieri F, Sevini F,et al. Inflammaging and anti-inflammaging: a systemic perspectiveon aging and longevity emerged from studies in humans. MechAgeing Dev 2007;128:92–105.
[26] Zeeh J, Platt D. The aging liver: structural and functional changesand their consequences for drug treatment in old age. Gerontol-ogy 2002;48:121–127.
Copyright © 2022 FDOKUMEN