Feasibility and Limits of Split Liver Transplantation From Pediatric Donors
10
ORIGINAL ARTICLES Feasibility and Limits of Split Liver Transplantation From Pediatric Donors An Italian Multicenter Experience Matteo Cescon, MD,* Marco Spada, MD, PhD,† Michele Colledan, MD,* Giuliano Torre, MD,‡ Enzo Andorno, MD,§ Umberto Valente, MD,§ Giorgio Rossi, MD,¶ Paolo Reggiani, MD,¶ Umberto Cillo, MD, Umberto Baccarani, MD,** Gian Luca Grazi, MD,†† Giuseppe Tisone, MD,‡‡ Franco Filipponi, MD,§§ Massimo Rossi, MD,¶¶ Giuseppe Maria Ettorre, MD, Mauro Salizzoni, MD,*** Oreste Cuomo, MD,††† Tullia De Feo, MD,‡‡‡ and Bruno Gridelli, MD† Objective: To report the results of a multicenter experience of split liver transplantation (SLT) with pediatric donors. Summary Background Data: There are no reports in the literature regarding pediatric liver splitting; further; the use of donors weigh- ing 40 kg for SLT is currently not recommended. Methods: From 1997 to 2004, 43 conventional split liver procedures from donors aged 15 years were performed. Nineteen donors weighing 40 kg and 24 weighing 40 kg were used. Dimensional matching was based on donor-to-recipient weight ratio (DRWR) for left lateral segment (LLS) and on estimated graft-to-recipient weight ratio (eGRWR) for extended right grafts (ERG). In 3 cases, no recipient was found for an ERG. The celiac trunk was retained with the LLS in all but 1 case. Forty LLSs were transplanted into 39 children, while 39 ERGs were transplanted into 11 children and 28 adults. Results: Two-year patient and graft survival rates were not signif- icantly different between recipients of donors 40 kg and 40 kg, between pediatric and adult recipients, and between recipients of LLSs and ERGs. Vascular complication rates were 12% in the 40 kg donor group and 6% in the 40 kg donor group (P not significant). There were no differences in the incidence of other complications. Donor ICU stay 3 days and the use of an interpo- sition arterial graft were associated with an increased risk of graft loss and arterial complications, respectively. Conclusions: Splitting of pediatric liver grafts is an effective strat- egy to increase organ availability, but a cautious evaluation of the use of donors 40 kg is necessary. Prolonged donor ICU stay is associated with poorer outcomes. The maintenance of the celiac trunk with LLS does not seem detrimental for right-sided grafts, whereas the use of interposition grafts for arterial reconstruction should be avoided. (Ann Surg 2006;244: 805– 814) D espite the worldwide acceptance of split liver transplan- tation (SLT) as a strategy to expand a limited donor pool, problems still exist in its widespread application. 1 The technique of “conventional” SLT divides the liver of a heart- beating donor into an extended right graft (ERG) and a left lateral segment graft (LLS), including Couinaud segments I, IV–VIII, and segments II–III, respectively. 2,3 Recent single- center series of either in situ or ex situ SLT reported results comparable to whole liver transplantation (WLT). 3–16 The ideal split liver donor should be between 14 and 50 years of age, with good liver function, serum sodium level 160 mmol/L, short intensive care unit (ICU) stay, stable hemodynamics, and with a grossly normal liver. 15,17,18 It has been shown that conventional splitting can yield a 15% increase in the number of grafts when donors within the From the *Liver and Lung Transplantation Unit, Azienda Ospedaliera “Ospedali Riuniti,” Bergamo, Italy; †Department of Surgery, Abdominal Transplantation Unit, Istituto Mediterraneo per i Trapianti e Terapie ad Alta Specializzazione (IsMeTT), University of Pittsburgh Medical Cen- ter (UPMC), Palermo, Italy; ‡Department of Pediatrics, Azienda Osped- aliera “Ospedali Riuniti,” Bergamo, Italy; §Department of Transplant Surgery, Ospedale San Martino, University of Genoa, Genoa, Italy; ¶Department of General and Transplantation Surgery, Liver and Lung Transplantation Unit, IRCCS Ospedale Maggiore, University of Milan, Italy; Department of General and Transplantation Surgery, General Surgery Unit I, University of Padua, Italy; **Department of Surgery, Transplantation Unit, University Hospital, Udine, Italy; ††Liver and Multiorgan Transplant Unit, Department of Surgery and Transplantation, University of Bologna, Bologna, Italy; ‡‡Department of Surgery, Trans- plantation Unit, Ospedale Sant’Eugenio, Tor Vergata University, Rome, Italy; §§Liver Transplantation Unit, Azienda Ospedaliera Universitaria Pisana, University of Pisa, Italy; ¶¶Department of Surgery, Transplanta- tion Unit, Policlinico Umberto I, La Sapienza University of Rome, Italy; Department of Digestive Surgery and Liver Transplantation, Regina Elena Cancer Institute, Rome, Italy; ***Liver Transplantation Center, Ospedale San Giovanni Battista, Turin, Italy; †††Laparoscopic and Liver and Transplantation Surgery Unit, Ospedale Cardarelli, Naples, Italy; ‡‡‡Organ and Tissue Transplant Immunology Unit, IRCCS Ospedale Maggiore, Milan, Italy. Reprints: Marco Spada, MD, PhD, Department of Surgery, Abdominal Transplantation Unit, Istituto Mediterraneo per i Trapianti e Terapie ad Alta Specializzazione (IsMeTT), UPMC Italy, Via E. Tricomi, 1, 90127 Palermo, Italy. E-mail: [email protected]. Copyright © 2006 by Lippincott Williams & Wilkins ISSN: 0003-4932/06/24405-0805 DOI: 10.1097/01.sla.0000218076.85213.60 Annals of Surgery • Volume 244, Number 5, November 2006 805
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Feasibility and Limits of Split Liver Transplantation From Pediatric Donors

ORIGINAL ARTICLES
Feasibility and Limits of Split Liver Transplantation FromPediatric Donors
An Italian Multicenter Experience
Matteo Cescon, MD,* Marco Spada, MD, PhD,† Michele Colledan, MD,* Giuliano Torre, MD,‡Enzo Andorno, MD,§ Umberto Valente, MD,§ Giorgio Rossi, MD,¶ Paolo Reggiani, MD,¶
Umberto Cillo, MD,� Umberto Baccarani, MD,** Gian Luca Grazi, MD,†† Giuseppe Tisone, MD,‡‡Franco Filipponi, MD,§§ Massimo Rossi, MD,¶¶ Giuseppe Maria Ettorre, MD,��
Mauro Salizzoni, MD,*** Oreste Cuomo, MD,††† Tullia De Feo, MD,‡‡‡ and Bruno Gridelli, MD†
Objective: To report the results of a multicenter experience of splitliver transplantation (SLT) with pediatric donors.Summary Background Data: There are no reports in the literatureregarding pediatric liver splitting; further; the use of donors weigh-ing �40 kg for SLT is currently not recommended.Methods: From 1997 to 2004, 43 conventional split liver proceduresfrom donors aged �15 years were performed. Nineteen donorsweighing �40 kg and 24 weighing �40 kg were used. Dimensionalmatching was based on donor-to-recipient weight ratio (DRWR) forleft lateral segment (LLS) and on estimated graft-to-recipient weightratio (eGRWR) for extended right grafts (ERG). In 3 cases, norecipient was found for an ERG. The celiac trunk was retained with
the LLS in all but 1 case. Forty LLSs were transplanted into 39children, while 39 ERGs were transplanted into 11 children and 28adults.Results: Two-year patient and graft survival rates were not signif-icantly different between recipients of donors �40 kg and �40 kg,between pediatric and adult recipients, and between recipients ofLLSs and ERGs. Vascular complication rates were 12% in the �40kg donor group and 6% in the �40 kg donor group (P � notsignificant). There were no differences in the incidence of othercomplications. Donor ICU stay �3 days and the use of an interpo-sition arterial graft were associated with an increased risk of graftloss and arterial complications, respectively.Conclusions: Splitting of pediatric liver grafts is an effective strat-egy to increase organ availability, but a cautious evaluation of theuse of donors �40 kg is necessary. Prolonged donor ICU stay isassociated with poorer outcomes. The maintenance of the celiactrunk with LLS does not seem detrimental for right-sided grafts,whereas the use of interposition grafts for arterial reconstructionshould be avoided.
(Ann Surg 2006;244: 805–814)
Despite the worldwide acceptance of split liver transplan-tation (SLT) as a strategy to expand a limited donor
pool, problems still exist in its widespread application.1 Thetechnique of “conventional” SLT divides the liver of a heart-beating donor into an extended right graft (ERG) and a leftlateral segment graft (LLS), including Couinaud segments I,IV–VIII, and segments II–III, respectively.2,3 Recent single-center series of either in situ or ex situ SLT reported resultscomparable to whole liver transplantation (WLT).3–16
The ideal split liver donor should be between 14 and 50years of age, with good liver function, serum sodium level�160 mmol/L, short intensive care unit (ICU) stay, stablehemodynamics, and with a grossly normal liver.15,17,18
It has been shown that conventional splitting can yield a15% increase in the number of grafts when donors within the
From the *Liver and Lung Transplantation Unit, Azienda Ospedaliera“Ospedali Riuniti,” Bergamo, Italy; †Department of Surgery, AbdominalTransplantation Unit, Istituto Mediterraneo per i Trapianti e Terapie adAlta Specializzazione (IsMeTT), University of Pittsburgh Medical Cen-ter (UPMC), Palermo, Italy; ‡Department of Pediatrics, Azienda Osped-aliera “Ospedali Riuniti,” Bergamo, Italy; §Department of TransplantSurgery, Ospedale San Martino, University of Genoa, Genoa, Italy;¶Department of General and Transplantation Surgery, Liver and LungTransplantation Unit, IRCCS Ospedale Maggiore, University of Milan,Italy; �Department of General and Transplantation Surgery, GeneralSurgery Unit I, University of Padua, Italy; **Department of Surgery,Transplantation Unit, University Hospital, Udine, Italy; ††Liver andMultiorgan Transplant Unit, Department of Surgery and Transplantation,University of Bologna, Bologna, Italy; ‡‡Department of Surgery, Trans-plantation Unit, Ospedale Sant’Eugenio, Tor Vergata University, Rome,Italy; §§Liver Transplantation Unit, Azienda Ospedaliera UniversitariaPisana, University of Pisa, Italy; ¶¶Department of Surgery, Transplanta-tion Unit, Policlinico Umberto I, La Sapienza University of Rome, Italy;��Department of Digestive Surgery and Liver Transplantation, ReginaElena Cancer Institute, Rome, Italy; ***Liver Transplantation Center,Ospedale San Giovanni Battista, Turin, Italy; †††Laparoscopic and Liverand Transplantation Surgery Unit, Ospedale Cardarelli, Naples, Italy;‡‡‡Organ and Tissue Transplant Immunology Unit, IRCCS OspedaleMaggiore, Milan, Italy.
Reprints: Marco Spada, MD, PhD, Department of Surgery, AbdominalTransplantation Unit, Istituto Mediterraneo per i Trapianti e Terapie adAlta Specializzazione (IsMeTT), UPMC Italy, Via E. Tricomi, 1, 90127Palermo, Italy. E-mail: [email protected].
Copyright © 2006 by Lippincott Williams & WilkinsISSN: 0003-4932/06/24405-0805DOI: 10.1097/01.sla.0000218076.85213.60
Annals of Surgery • Volume 244, Number 5, November 2006 805

above criteria are selected, and a 43% increase if donors withonly one missing criterion are included.18 We had satisfactoryresults by extending the donor age beyond 50 years;19 while thelower age limit is still unclear, the splitting of donors youngerthan 10 years,17,20 or weighing less than 40 to 45 kg15,18 remainquestionable.
The recipients of LLSs are usually pediatric patients,while ERGs are transplanted into adolescents or adults. In thecase of children less than 5 to 6 kg, SLT from an adult donoroften means the transplantation of a large-for-size graft caus-ing a number of complications, including graft dysfunction.21
The use of a single liver segment or of the LLS from apediatric donor can circumvent this problem. The success ofthe former strategy has already been reported.22 Conversely,there are no data specifically addressing SLT from pediatricdonors, particularly from those aged less than 10 years orweighing less than 40 kg. A corollary of this limitation is theunknown fate of the right-sided graft.
Since 1997, an extensive application of SLT began inthe Northern Italian Transplant (NITp) area with the intentionof satisfying the shortage of organs for pediatric recipients8
and pediatric donors are considered for splitting when smallchildren are on the waiting list. We report herein the resultsof a prospective multicenter study evaluating the outcome ofSLT from donors younger than 15 years.
METHODSFrom October 1997 to July 2004, 43 split liver proce-
dures were carried out in donors younger than 15 years. In allcases, an LLS and an ERG were procured. In 7 cases (16%),both LLS and ERG were transplanted at the same center; in33 cases (77%), the grafts were transplanted in 2 differentcenters. In 3 cases (7%) in which the donor weight was �40kg (20, 20, and 30 kg, respectively), no recipient could befound for the ERG, and only the LLS was transplanted. In 7cases the grafts were shared with a European liver transplantcenter. Only AB0-compatible donors were used.
One child was excluded from the analysis having receiveda combined split liver (LLS) and kidney transplant. Anotherpediatric recipient of a combined split liver (LLS) and smallbowel transplant, subsequently retransplantated for hepatic ar-tery thrombosis (HAT) with an LLS from another pediatricdonor, was also excluded from the analysis. Overall, 80 isolatedSLTs with grafts from pediatric donors were performed. The73 SLTs performed by Italian Centers represented 16% of the453 SLTs performed in Italy during the same period.
Data on demographic and clinical profiles of recipients,procurement and transplant technique, postoperative compli-cations, causes of death, and retransplantation and actualpatient and graft status recorded by the transplant centerswere collected by completion of appropriate forms. A fullresponse was obtained for 79 of 80 transplants (99%), withdata available for 40 of 40 LLSs (100%) and 39 of 40 ERGs(97%). A 1-month-old girl with neonatal hemochromatosiswith subacute liver failure had a primary transplant with anLLS from a donor �40 kg; she subsequently developedchronic rejection and was retransplantated with an LLS froma donor �40 kg. The patient population therefore included 78
recipients: 50 children, who received 40 LLSs and 11 ERGs,and 28 ERG adult recipients. The pediatric population in-cluded 25 males and 25 females, with a mean age of 3.2 � 4.0years (median, 1.0 year; range, 1 month to 12 years). Theadult population included 5 males and 23 females, with amean age of 46.1 � 13.8 years (median, 50 years; range,17–66 years).
Criteria for SplittingThe following donor characteristics were considered
ideal for splitting: 1) no past history of liver dysfunction/damage, 2) liver function tests within 5-fold normal values, 3)normal macroscopic appearance of the graft, and 4) hemody-namic stability.8 In some cases, criteria were liberally ex-tended by agreement between centers.
In the NITp area, liver grafts from pediatric donors(�15 years) are offered to pediatric recipients (listed fortransplant before the age of 15 years). Donors are allocated tocenters with pediatric liver transplant programs according torotation criteria, with the exception of UNOS status 1 patientsto whom the first available donor is assigned. The assignedcenter allocates the graft to the most urgent recipient with anadequate dimensional matching. Dimensional matching isusually established as follows: 1) If donor-to-recipient weightratio (DRWR) is �2, a WLT is performed; 2) if DRWR isbetween 2 and 12, and donor characteristics satisfy criteriafor splitting, the patient is a potential recipient of an LLS, anda split procedure is considered. The volume of the ERGobtainable from that donor, assumed to be 75% of the wholedonor liver mass, is estimated using the formula proposed byUrata et al.23 An ERG is offered to a pediatric recipient withan estimated graft-to-recipient weight ratio (eGRWR) �1%and �5%. If no pediatric recipients of ERG are found, theERG is offered to an adult recipient.
Surgical TechniquesThe splitting procedure was performed in situ, without
special surgical equipment and according to the techniquedescribed by Rogiers et al,4 except in 1 case where theparenchymal division was carried out ex situ for logisticalreasons. Briefly, the operation started with the identificationof the full course of the left hepatic artery and of the portalvein, as well as the origin of the right hepatic artery. Thepresence of aberrant arterial branch(es) was carefullychecked. When the arterial branch to segment IV originatedfrom the right hepatic artery, it was usually preserved, whilewhen it originated from the left, proper or common hepaticartery it was usually interrupted. The liver was divided so asto obtain an ERG (including segments IV–VIII, plus thecaudate lobe) and an LLS (including segments II and III).The LLS included the left hepatic vein, the left branch of theportal vein and, in all but 1 case, the left hepatic artery incontinuity with the celiac trunk. The ERG included the venacava, the portal trunk, the right hepatic artery, and thecommon bile duct. The LLS had an accessory left hepaticartery in 3 cases (7%), and a replaced one originating fromthe left gastric artery in 5 (12%). The ERG had a replacedright hepatic artery in 2 cases (5%), an accessory right hepaticartery in 3 cases (8%), and a hepato-mesenteric trunk in 1
Cescon et al Annals of Surgery • Volume 244, Number 5, November 2006
© 2006 Lippincott Williams & Wilkins806
case (3%). In no case did the split procedure jeopardize theviability of other organs.
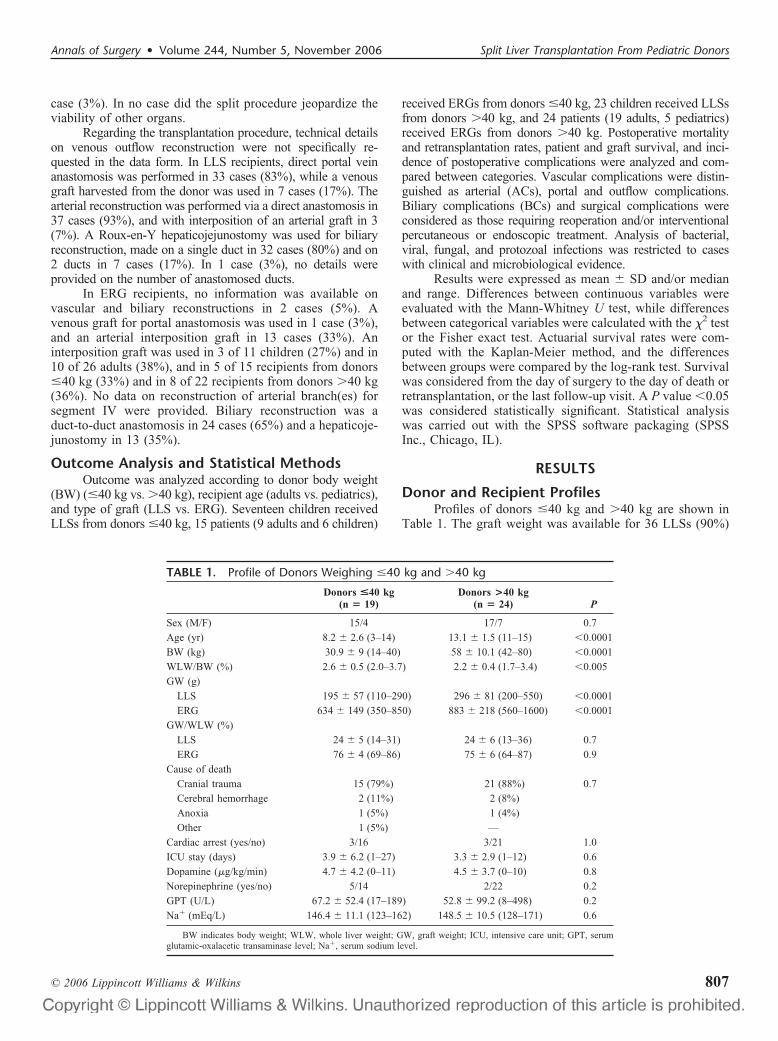
Regarding the transplantation procedure, technical detailson venous outflow reconstruction were not specifically re-quested in the data form. In LLS recipients, direct portal veinanastomosis was performed in 33 cases (83%), while a venousgraft harvested from the donor was used in 7 cases (17%). Thearterial reconstruction was performed via a direct anastomosis in37 cases (93%), and with interposition of an arterial graft in 3(7%). A Roux-en-Y hepaticojejunostomy was used for biliaryreconstruction, made on a single duct in 32 cases (80%) and on2 ducts in 7 cases (17%). In 1 case (3%), no details wereprovided on the number of anastomosed ducts.
In ERG recipients, no information was available onvascular and biliary reconstructions in 2 cases (5%). Avenous graft for portal anastomosis was used in 1 case (3%),and an arterial interposition graft in 13 cases (33%). Aninterposition graft was used in 3 of 11 children (27%) and in10 of 26 adults (38%), and in 5 of 15 recipients from donors�40 kg (33%) and in 8 of 22 recipients from donors �40 kg(36%). No data on reconstruction of arterial branch(es) forsegment IV were provided. Biliary reconstruction was aduct-to-duct anastomosis in 24 cases (65%) and a hepaticoje-junostomy in 13 (35%).
Outcome Analysis and Statistical MethodsOutcome was analyzed according to donor body weight
(BW) (�40 kg vs. �40 kg), recipient age (adults vs. pediatrics),and type of graft (LLS vs. ERG). Seventeen children receivedLLSs from donors �40 kg, 15 patients (9 adults and 6 children)
received ERGs from donors �40 kg, 23 children received LLSsfrom donors �40 kg, and 24 patients (19 adults, 5 pediatrics)received ERGs from donors �40 kg. Postoperative mortalityand retransplantation rates, patient and graft survival, and inci-dence of postoperative complications were analyzed and com-pared between categories. Vascular complications were distin-guished as arterial (ACs), portal and outflow complications.Biliary complications (BCs) and surgical complications wereconsidered as those requiring reoperation and/or interventionalpercutaneous or endoscopic treatment. Analysis of bacterial,viral, fungal, and protozoal infections was restricted to caseswith clinical and microbiological evidence.
Results were expressed as mean � SD and/or medianand range. Differences between continuous variables wereevaluated with the Mann-Whitney U test, while differencesbetween categorical variables were calculated with the �2 testor the Fisher exact test. Actuarial survival rates were com-puted with the Kaplan-Meier method, and the differencesbetween groups were compared by the log-rank test. Survivalwas considered from the day of surgery to the day of death orretransplantation, or the last follow-up visit. A P value �0.05was considered statistically significant. Statistical analysiswas carried out with the SPSS software packaging (SPSSInc., Chicago, IL).
RESULTS
Donor and Recipient ProfilesProfiles of donors �40 kg and �40 kg are shown in
Table 1. The graft weight was available for 36 LLSs (90%)
TABLE 1. Profile of Donors Weighing �40 kg and �40 kg
Donors <40 kg(n � 19)
Donors >40 kg(n � 24) P
Sex (M/F) 15/4 17/7 0.7
Age (yr) 8.2 � 2.6 (3–14) 13.1 � 1.5 (11–15) �0.0001
BW (kg) 30.9 � 9 (14–40) 58 � 10.1 (42–80) �0.0001
WLW/BW (%) 2.6 � 0.5 (2.0–3.7) 2.2 � 0.4 (1.7–3.4) �0.005
GW (g)
LLS 195 � 57 (110–290) 296 � 81 (200–550) �0.0001
ERG 634 � 149 (350–850) 883 � 218 (560–1600) �0.0001
GW/WLW (%)
LLS 24 � 5 (14–31) 24 � 6 (13–36) 0.7
ERG 76 � 4 (69–86) 75 � 6 (64–87) 0.9
Cause of death
Cranial trauma 15 (79%) 21 (88%) 0.7
Cerebral hemorrhage 2 (11%) 2 (8%)
Anoxia 1 (5%) 1 (4%)
Other 1 (5%) —
Cardiac arrest (yes/no) 3/16 3/21 1.0
ICU stay (days) 3.9 � 6.2 (1–27) 3.3 � 2.9 (1–12) 0.6
Dopamine (�g/kg/min) 4.7 � 4.2 (0–11) 4.5 � 3.7 (0–10) 0.8
Norepinephrine (yes/no) 5/14 2/22 0.2
GPT (U/L) 67.2 � 52.4 (17–189) 52.8 � 99.2 (8–498) 0.2
Na� (mEq/L) 146.4 � 11.1 (123–162) 148.5 � 10.5 (128–171) 0.6
BW indicates body weight; WLW, whole liver weight; GW, graft weight; ICU, intensive care unit; GPT, serumglutamic-oxalacetic transaminase level; Na�, serum sodium level.
Annals of Surgery • Volume 244, Number 5, November 2006 Split Liver Transplantation From Pediatric Donors
© 2006 Lippincott Williams & Wilkins 807
and 33 ERGs (85%). Mean age, BW, and mean graft weightof both LLSs and ERGs were significantly lower in donors�40 kg. The mean whole liver weight to BW ratio wassignificantly higher in donors �40 kg. In both categories,LLS and ERG represented approximately 25% and 75% ofthe whole liver mass, respectively. Causes of death, occur-rence of cardiac arrest, length of stay in the ICU, use ofvasopressors, serum GPT, and sodium levels did not differbetween groups.
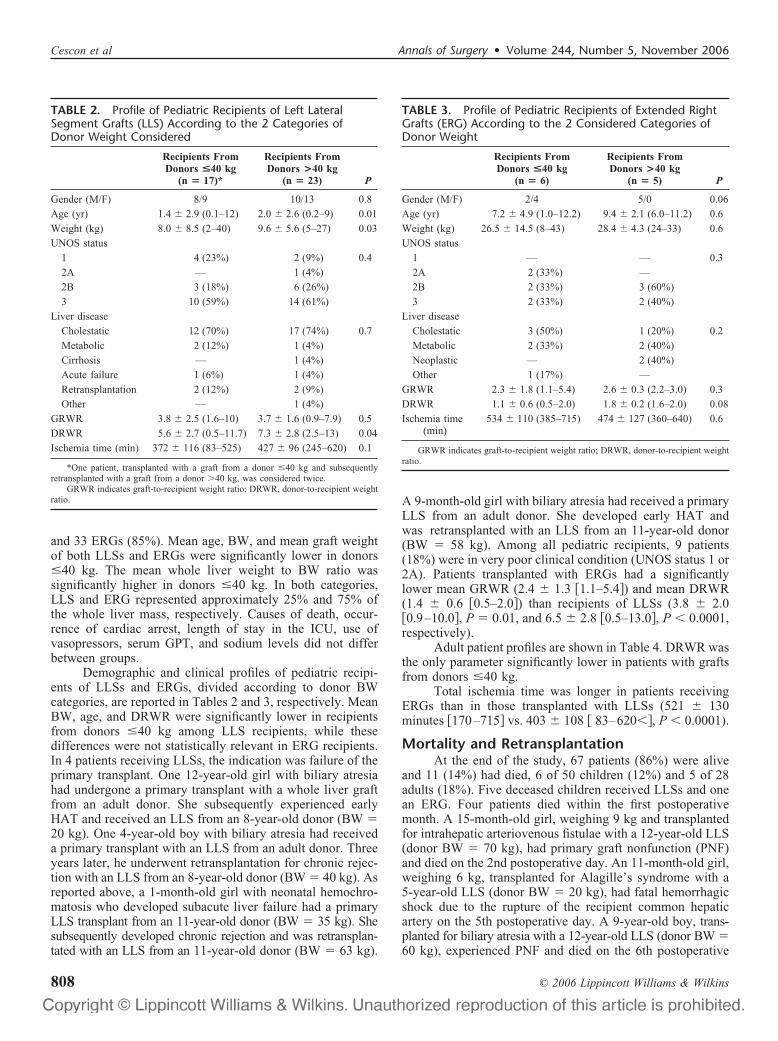
Demographic and clinical profiles of pediatric recipi-ents of LLSs and ERGs, divided according to donor BWcategories, are reported in Tables 2 and 3, respectively. MeanBW, age, and DRWR were significantly lower in recipientsfrom donors �40 kg among LLS recipients, while thesedifferences were not statistically relevant in ERG recipients.In 4 patients receiving LLSs, the indication was failure of theprimary transplant. One 12-year-old girl with biliary atresiahad undergone a primary transplant with a whole liver graftfrom an adult donor. She subsequently experienced earlyHAT and received an LLS from an 8-year-old donor (BW �20 kg). One 4-year-old boy with biliary atresia had receiveda primary transplant with an LLS from an adult donor. Threeyears later, he underwent retransplantation for chronic rejec-tion with an LLS from an 8-year-old donor (BW � 40 kg). Asreported above, a 1-month-old girl with neonatal hemochro-matosis who developed subacute liver failure had a primaryLLS transplant from an 11-year-old donor (BW � 35 kg). Shesubsequently developed chronic rejection and was retransplan-tated with an LLS from an 11-year-old donor (BW � 63 kg).
A 9-month-old girl with biliary atresia had received a primaryLLS from an adult donor. She developed early HAT andwas retransplanted with an LLS from an 11-year-old donor(BW � 58 kg). Among all pediatric recipients, 9 patients(18%) were in very poor clinical condition (UNOS status 1 or2A). Patients transplanted with ERGs had a significantlylower mean GRWR (2.4 � 1.3 �1.1–5.4�) and mean DRWR(1.4 � 0.6 �0.5–2.0�) than recipients of LLSs (3.8 � 2.0�0.9–10.0�, P � 0.01, and 6.5 � 2.8 �0.5–13.0�, P � 0.0001,respectively).
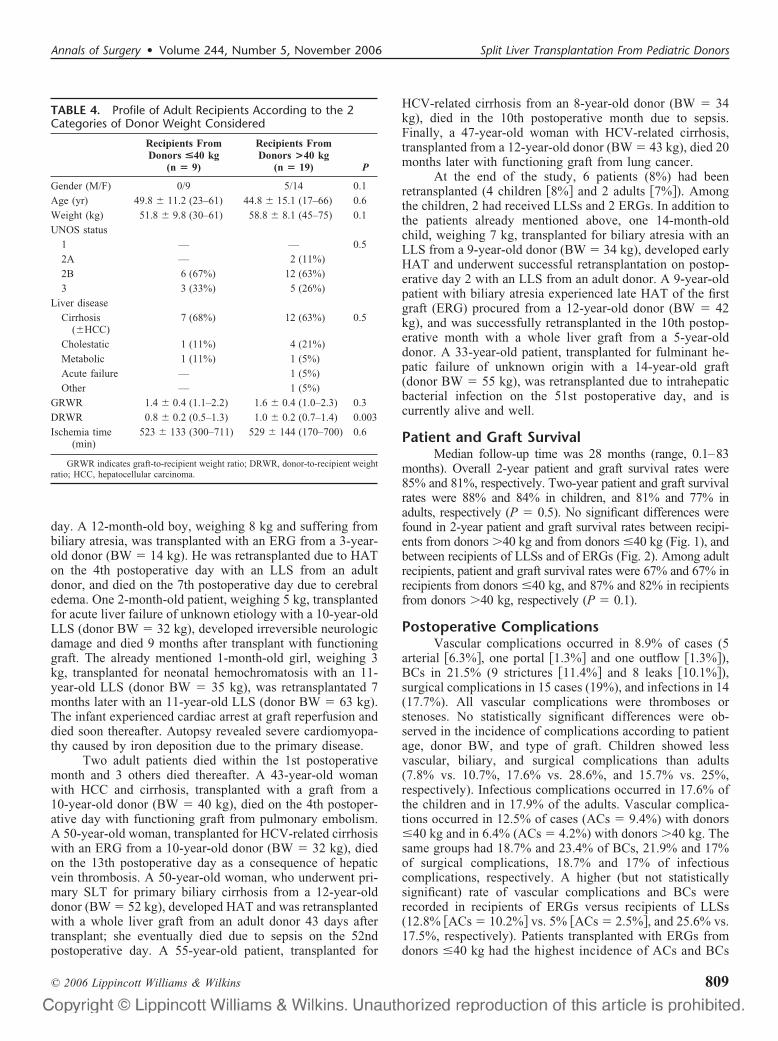
Adult patient profiles are shown in Table 4. DRWR wasthe only parameter significantly lower in patients with graftsfrom donors �40 kg.
Total ischemia time was longer in patients receivingERGs than in those transplanted with LLSs (521 � 130minutes �170–715� vs. 403 � 108 � 83–620��, P � 0.0001).
Mortality and RetransplantationAt the end of the study, 67 patients (86%) were alive
and 11 (14%) had died, 6 of 50 children (12%) and 5 of 28adults (18%). Five deceased children received LLSs and onean ERG. Four patients died within the first postoperativemonth. A 15-month-old girl, weighing 9 kg and transplantedfor intrahepatic arteriovenous fistulae with a 12-year-old LLS(donor BW � 70 kg), had primary graft nonfunction (PNF)and died on the 2nd postoperative day. An 11-month-old girl,weighing 6 kg, transplanted for Alagille’s syndrome with a5-year-old LLS (donor BW � 20 kg), had fatal hemorrhagicshock due to the rupture of the recipient common hepaticartery on the 5th postoperative day. A 9-year-old boy, trans-planted for biliary atresia with a 12-year-old LLS (donor BW �60 kg), experienced PNF and died on the 6th postoperative
TABLE 2. Profile of Pediatric Recipients of Left LateralSegment Grafts (LLS) According to the 2 Categories ofDonor Weight Considered
Recipients FromDonors <40 kg
(n � 17)*
Recipients FromDonors >40 kg
(n � 23) P
Gender (M/F) 8/9 10/13 0.8
Age (yr) 1.4 � 2.9 (0.1–12) 2.0 � 2.6 (0.2–9) 0.01
Weight (kg) 8.0 � 8.5 (2–40) 9.6 � 5.6 (5–27) 0.03
UNOS status
1 4 (23%) 2 (9%) 0.4
2A — 1 (4%)
2B 3 (18%) 6 (26%)
3 10 (59%) 14 (61%)
Liver disease
Cholestatic 12 (70%) 17 (74%) 0.7
Metabolic 2 (12%) 1 (4%)
Cirrhosis — 1 (4%)
Acute failure 1 (6%) 1 (4%)
Retransplantation 2 (12%) 2 (9%)
Other — 1 (4%)
GRWR 3.8 � 2.5 (1.6–10) 3.7 � 1.6 (0.9–7.9) 0.5
DRWR 5.6 � 2.7 (0.5–11.7) 7.3 � 2.8 (2.5–13) 0.04
Ischemia time (min) 372 � 116 (83–525) 427 � 96 (245–620) 0.1
*One patient, transplanted with a graft from a donor �40 kg and subsequentlyretransplanted with a graft from a donor �40 kg, was considered twice.
GRWR indicates graft-to-recipient weight ratio; DRWR, donor-to-recipient weightratio.
TABLE 3. Profile of Pediatric Recipients of Extended RightGrafts (ERG) According to the 2 Considered Categories ofDonor Weight
Recipients FromDonors <40 kg
(n � 6)
Recipients FromDonors >40 kg
(n � 5) P
Gender (M/F) 2/4 5/0 0.06
Age (yr) 7.2 � 4.9 (1.0–12.2) 9.4 � 2.1 (6.0–11.2) 0.6
Weight (kg) 26.5 � 14.5 (8–43) 28.4 � 4.3 (24–33) 0.6
UNOS status
1 — — 0.3
2A 2 (33%) —
2B 2 (33%) 3 (60%)
3 2 (33%) 2 (40%)
Liver disease
Cholestatic 3 (50%) 1 (20%) 0.2
Metabolic 2 (33%) 2 (40%)
Neoplastic — 2 (40%)
Other 1 (17%) —
GRWR 2.3 � 1.8 (1.1–5.4) 2.6 � 0.3 (2.2–3.0) 0.3
DRWR 1.1 � 0.6 (0.5–2.0) 1.8 � 0.2 (1.6–2.0) 0.08
Ischemia time(min)
534 � 110 (385–715) 474 � 127 (360–640) 0.6
GRWR indicates graft-to-recipient weight ratio; DRWR, donor-to-recipient weightratio.
Cescon et al Annals of Surgery • Volume 244, Number 5, November 2006
© 2006 Lippincott Williams & Wilkins808
day. A 12-month-old boy, weighing 8 kg and suffering frombiliary atresia, was transplanted with an ERG from a 3-year-old donor (BW � 14 kg). He was retransplanted due to HATon the 4th postoperative day with an LLS from an adultdonor, and died on the 7th postoperative day due to cerebraledema. One 2-month-old patient, weighing 5 kg, transplantedfor acute liver failure of unknown etiology with a 10-year-oldLLS (donor BW � 32 kg), developed irreversible neurologicdamage and died 9 months after transplant with functioninggraft. The already mentioned 1-month-old girl, weighing 3kg, transplanted for neonatal hemochromatosis with an 11-year-old LLS (donor BW � 35 kg), was retransplantated 7months later with an 11-year-old LLS (donor BW � 63 kg).The infant experienced cardiac arrest at graft reperfusion anddied soon thereafter. Autopsy revealed severe cardiomyopa-thy caused by iron deposition due to the primary disease.
Two adult patients died within the 1st postoperativemonth and 3 others died thereafter. A 43-year-old womanwith HCC and cirrhosis, transplanted with a graft from a10-year-old donor (BW � 40 kg), died on the 4th postoper-ative day with functioning graft from pulmonary embolism.A 50-year-old woman, transplanted for HCV-related cirrhosiswith an ERG from a 10-year-old donor (BW � 32 kg), diedon the 13th postoperative day as a consequence of hepaticvein thrombosis. A 50-year-old woman, who underwent pri-mary SLT for primary biliary cirrhosis from a 12-year-olddonor (BW � 52 kg), developed HAT and was retransplantedwith a whole liver graft from an adult donor 43 days aftertransplant; she eventually died due to sepsis on the 52ndpostoperative day. A 55-year-old patient, transplanted for
HCV-related cirrhosis from an 8-year-old donor (BW � 34kg), died in the 10th postoperative month due to sepsis.Finally, a 47-year-old woman with HCV-related cirrhosis,transplanted from a 12-year-old donor (BW � 43 kg), died 20months later with functioning graft from lung cancer.
At the end of the study, 6 patients (8%) had beenretransplanted (4 children �8%� and 2 adults �7%�). Amongthe children, 2 had received LLSs and 2 ERGs. In addition tothe patients already mentioned above, one 14-month-oldchild, weighing 7 kg, transplanted for biliary atresia with anLLS from a 9-year-old donor (BW � 34 kg), developed earlyHAT and underwent successful retransplantation on postop-erative day 2 with an LLS from an adult donor. A 9-year-oldpatient with biliary atresia experienced late HAT of the firstgraft (ERG) procured from a 12-year-old donor (BW � 42kg), and was successfully retransplanted in the 10th postop-erative month with a whole liver graft from a 5-year-olddonor. A 33-year-old patient, transplanted for fulminant he-patic failure of unknown origin with a 14-year-old graft(donor BW � 55 kg), was retransplanted due to intrahepaticbacterial infection on the 51st postoperative day, and iscurrently alive and well.
Patient and Graft SurvivalMedian follow-up time was 28 months (range, 0.1–83
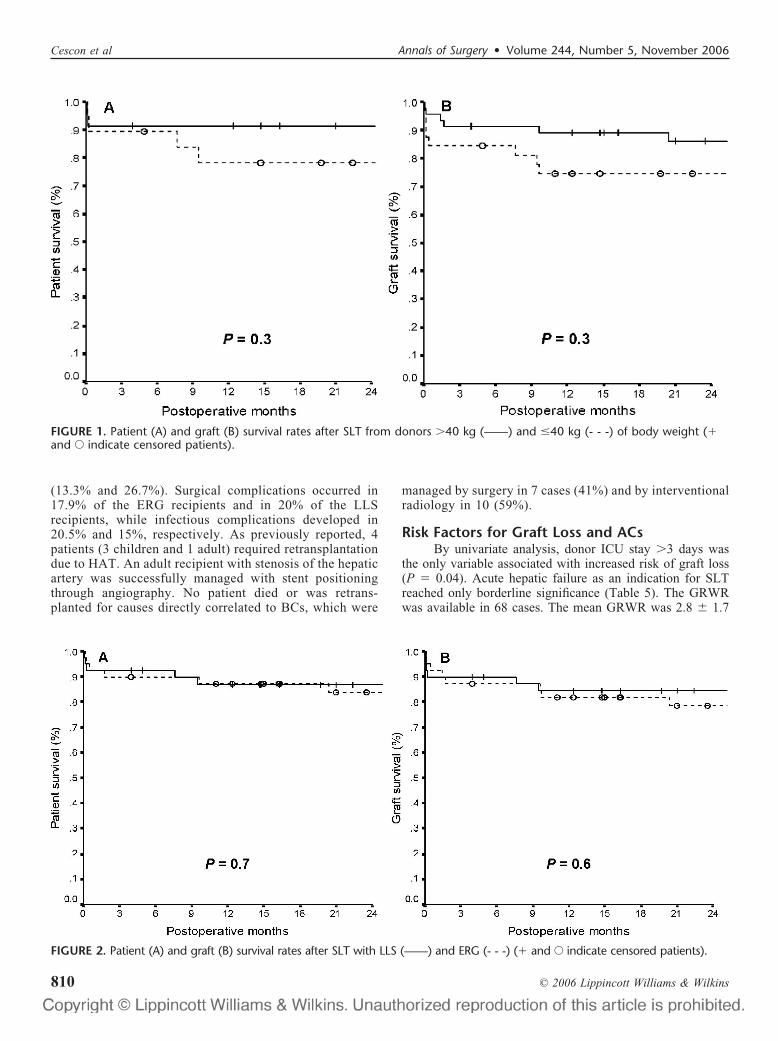
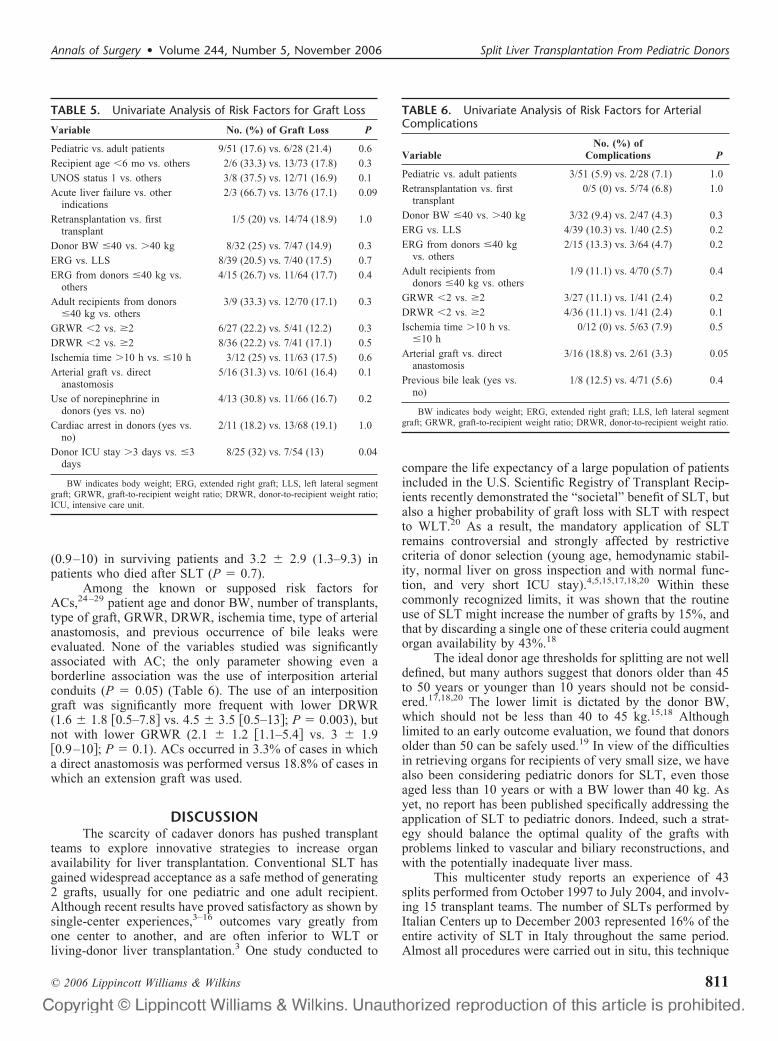
months). Overall 2-year patient and graft survival rates were85% and 81%, respectively. Two-year patient and graft survivalrates were 88% and 84% in children, and 81% and 77% inadults, respectively (P � 0.5). No significant differences werefound in 2-year patient and graft survival rates between recipi-ents from donors �40 kg and from donors �40 kg (Fig. 1), andbetween recipients of LLSs and of ERGs (Fig. 2). Among adultrecipients, patient and graft survival rates were 67% and 67% inrecipients from donors �40 kg, and 87% and 82% in recipientsfrom donors �40 kg, respectively (P � 0.1).
Postoperative ComplicationsVascular complications occurred in 8.9% of cases (5
arterial �6.3%�, one portal �1.3%� and one outflow �1.3%�),BCs in 21.5% (9 strictures �11.4%� and 8 leaks �10.1%�),surgical complications in 15 cases (19%), and infections in 14(17.7%). All vascular complications were thromboses orstenoses. No statistically significant differences were ob-served in the incidence of complications according to patientage, donor BW, and type of graft. Children showed lessvascular, biliary, and surgical complications than adults(7.8% vs. 10.7%, 17.6% vs. 28.6%, and 15.7% vs. 25%,respectively). Infectious complications occurred in 17.6% ofthe children and in 17.9% of the adults. Vascular complica-tions occurred in 12.5% of cases (ACs � 9.4%) with donors�40 kg and in 6.4% (ACs � 4.2%) with donors �40 kg. Thesame groups had 18.7% and 23.4% of BCs, 21.9% and 17%of surgical complications, 18.7% and 17% of infectiouscomplications, respectively. A higher (but not statisticallysignificant) rate of vascular complications and BCs wererecorded in recipients of ERGs versus recipients of LLSs(12.8% �ACs � 10.2%� vs. 5% �ACs � 2.5%�, and 25.6% vs.17.5%, respectively). Patients transplanted with ERGs fromdonors �40 kg had the highest incidence of ACs and BCs
TABLE 4. Profile of Adult Recipients According to the 2Categories of Donor Weight Considered
Recipients FromDonors <40 kg
(n � 9)
Recipients FromDonors >40 kg
(n � 19) P
Gender (M/F) 0/9 5/14 0.1
Age (yr) 49.8 � 11.2 (23–61) 44.8 � 15.1 (17–66) 0.6
Weight (kg) 51.8 � 9.8 (30–61) 58.8 � 8.1 (45–75) 0.1
UNOS status
1 — — 0.5
2A — 2 (11%)
2B 6 (67%) 12 (63%)
3 3 (33%) 5 (26%)
Liver disease
Cirrhosis(�HCC)
7 (68%) 12 (63%) 0.5
Cholestatic 1 (11%) 4 (21%)
Metabolic 1 (11%) 1 (5%)
Acute failure — 1 (5%)
Other — 1 (5%)
GRWR 1.4 � 0.4 (1.1–2.2) 1.6 � 0.4 (1.0–2.3) 0.3
DRWR 0.8 � 0.2 (0.5–1.3) 1.0 � 0.2 (0.7–1.4) 0.003
Ischemia time(min)
523 � 133 (300–711) 529 � 144 (170–700) 0.6
GRWR indicates graft-to-recipient weight ratio; DRWR, donor-to-recipient weightratio; HCC, hepatocellular carcinoma.
Annals of Surgery • Volume 244, Number 5, November 2006 Split Liver Transplantation From Pediatric Donors
© 2006 Lippincott Williams & Wilkins 809
(13.3% and 26.7%). Surgical complications occurred in17.9% of the ERG recipients and in 20% of the LLSrecipients, while infectious complications developed in20.5% and 15%, respectively. As previously reported, 4patients (3 children and 1 adult) required retransplantationdue to HAT. An adult recipient with stenosis of the hepaticartery was successfully managed with stent positioningthrough angiography. No patient died or was retrans-planted for causes directly correlated to BCs, which were
managed by surgery in 7 cases (41%) and by interventionalradiology in 10 (59%).
Risk Factors for Graft Loss and ACsBy univariate analysis, donor ICU stay �3 days was
the only variable associated with increased risk of graft loss(P � 0.04). Acute hepatic failure as an indication for SLTreached only borderline significance (Table 5). The GRWRwas available in 68 cases. The mean GRWR was 2.8 � 1.7
FIGURE 2. Patient (A) and graft (B) survival rates after SLT with LLS (——) and ERG (- - -) (� and E indicate censored patients).
FIGURE 1. Patient (A) and graft (B) survival rates after SLT from donors �40 kg (——) and �40 kg (- - -) of body weight (�and E indicate censored patients).
Cescon et al Annals of Surgery • Volume 244, Number 5, November 2006
© 2006 Lippincott Williams & Wilkins810
(0.9–10) in surviving patients and 3.2 � 2.9 (1.3–9.3) inpatients who died after SLT (P � 0.7).
Among the known or supposed risk factors forACs,24–29 patient age and donor BW, number of transplants,type of graft, GRWR, DRWR, ischemia time, type of arterialanastomosis, and previous occurrence of bile leaks wereevaluated. None of the variables studied was significantlyassociated with AC; the only parameter showing even aborderline association was the use of interposition arterialconduits (P � 0.05) (Table 6). The use of an interpositiongraft was significantly more frequent with lower DRWR(1.6 � 1.8 �0.5–7.8� vs. 4.5 � 3.5 �0.5–13�; P � 0.003), butnot with lower GRWR (2.1 � 1.2 �1.1–5.4� vs. 3 � 1.9�0.9–10�; P � 0.1). ACs occurred in 3.3% of cases in whicha direct anastomosis was performed versus 18.8% of cases inwhich an extension graft was used.
DISCUSSIONThe scarcity of cadaver donors has pushed transplant
teams to explore innovative strategies to increase organavailability for liver transplantation. Conventional SLT hasgained widespread acceptance as a safe method of generating2 grafts, usually for one pediatric and one adult recipient.Although recent results have proved satisfactory as shown bysingle-center experiences,3–16 outcomes vary greatly fromone center to another, and are often inferior to WLT orliving-donor liver transplantation.3 One study conducted to
compare the life expectancy of a large population of patientsincluded in the U.S. Scientific Registry of Transplant Recip-ients recently demonstrated the “societal” benefit of SLT, butalso a higher probability of graft loss with SLT with respectto WLT.20 As a result, the mandatory application of SLTremains controversial and strongly affected by restrictivecriteria of donor selection (young age, hemodynamic stabil-ity, normal liver on gross inspection and with normal func-tion, and very short ICU stay).4,5,15,17,18,20 Within thesecommonly recognized limits, it was shown that the routineuse of SLT might increase the number of grafts by 15%, andthat by discarding a single one of these criteria could augmentorgan availability by 43%.18
The ideal donor age thresholds for splitting are not welldefined, but many authors suggest that donors older than 45to 50 years or younger than 10 years should not be consid-ered.17,18,20 The lower limit is dictated by the donor BW,which should not be less than 40 to 45 kg.15,18 Althoughlimited to an early outcome evaluation, we found that donorsolder than 50 can be safely used.19 In view of the difficultiesin retrieving organs for recipients of very small size, we havealso been considering pediatric donors for SLT, even thoseaged less than 10 years or with a BW lower than 40 kg. Asyet, no report has been published specifically addressing theapplication of SLT to pediatric donors. Indeed, such a strat-egy should balance the optimal quality of the grafts withproblems linked to vascular and biliary reconstructions, andwith the potentially inadequate liver mass.
This multicenter study reports an experience of 43splits performed from October 1997 to July 2004, and involv-ing 15 transplant teams. The number of SLTs performed byItalian Centers up to December 2003 represented 16% of theentire activity of SLT in Italy throughout the same period.Almost all procedures were carried out in situ, this technique
TABLE 5. Univariate Analysis of Risk Factors for Graft Loss
Variable No. (%) of Graft Loss P
Pediatric vs. adult patients 9/51 (17.6) vs. 6/28 (21.4) 0.6
Recipient age �6 mo vs. others 2/6 (33.3) vs. 13/73 (17.8) 0.3
UNOS status 1 vs. others 3/8 (37.5) vs. 12/71 (16.9) 0.1
Acute liver failure vs. otherindications
2/3 (66.7) vs. 13/76 (17.1) 0.09
Retransplantation vs. firsttransplant
1/5 (20) vs. 14/74 (18.9) 1.0
Donor BW �40 vs. �40 kg 8/32 (25) vs. 7/47 (14.9) 0.3
ERG vs. LLS 8/39 (20.5) vs. 7/40 (17.5) 0.7
ERG from donors �40 kg vs.others
4/15 (26.7) vs. 11/64 (17.7) 0.4
Adult recipients from donors�40 kg vs. others
3/9 (33.3) vs. 12/70 (17.1) 0.3
GRWR �2 vs. �2 6/27 (22.2) vs. 5/41 (12.2) 0.3
DRWR �2 vs. �2 8/36 (22.2) vs. 7/41 (17.1) 0.5
Ischemia time �10 h vs. �10 h 3/12 (25) vs. 11/63 (17.5) 0.6
Arterial graft vs. directanastomosis
5/16 (31.3) vs. 10/61 (16.4) 0.1
Use of norepinephrine indonors (yes vs. no)
4/13 (30.8) vs. 11/66 (16.7) 0.2
Cardiac arrest in donors (yes vs.no)
2/11 (18.2) vs. 13/68 (19.1) 1.0
Donor ICU stay �3 days vs. �3days
8/25 (32) vs. 7/54 (13) 0.04
BW indicates body weight; ERG, extended right graft; LLS, left lateral segmentgraft; GRWR, graft-to-recipient weight ratio; DRWR, donor-to-recipient weight ratio;ICU, intensive care unit.
TABLE 6. Univariate Analysis of Risk Factors for ArterialComplications
VariableNo. (%) of
Complications P
Pediatric vs. adult patients 3/51 (5.9) vs. 2/28 (7.1) 1.0
Retransplantation vs. firsttransplant
0/5 (0) vs. 5/74 (6.8) 1.0
Donor BW �40 vs. �40 kg 3/32 (9.4) vs. 2/47 (4.3) 0.3
ERG vs. LLS 4/39 (10.3) vs. 1/40 (2.5) 0.2
ERG from donors �40 kgvs. others
2/15 (13.3) vs. 3/64 (4.7) 0.2
Adult recipients fromdonors �40 kg vs. others
1/9 (11.1) vs. 4/70 (5.7) 0.4
GRWR �2 vs. �2 3/27 (11.1) vs. 1/41 (2.4) 0.2
DRWR �2 vs. �2 4/36 (11.1) vs. 1/41 (2.4) 0.1
Ischemia time �10 h vs.�10 h
0/12 (0) vs. 5/63 (7.9) 0.5
Arterial graft vs. directanastomosis
3/16 (18.8) vs. 2/61 (3.3) 0.05
Previous bile leak (yes vs.no)
1/8 (12.5) vs. 4/71 (5.6) 0.4
BW indicates body weight; ERG, extended right graft; LLS, left lateral segmentgraft; GRWR, graft-to-recipient weight ratio; DRWR, donor-to-recipient weight ratio.
Annals of Surgery • Volume 244, Number 5, November 2006 Split Liver Transplantation From Pediatric Donors
© 2006 Lippincott Williams & Wilkins 811

allowing maximization of organ sharing in Italy as well as inother countries.1,8,11
This study shows that the use of donors aged �15 yearsis safe (85% patient and 81% graft survival). The splitting oflivers from donors between 11 and 15 years seems justifiedbecause their body size approaches that of an adult, as shownby our data on BW in this category.
Our analysis revealed that survival and complicationrates were not significantly different between the 3 stratifi-cations considered (donors �40 kg vs. �40 kg, adult vs.pediatric recipients, and recipients of LLSs vs. ERGs). Over-all, they were similar to those reported in the largest single-center series of conventional SLT, without distinction be-tween donor age categories,3–16 and to those obtained withother techniques (ie, cadaveric WLT and living-donor trans-plantation).11,16 Recipients from donors weighing �40 kg,adult recipients, and recipients of ERG had less favorableoutcomes than recipients from donors �40 kg, pediatricrecipients, and recipients of LLS, respectively. The lownumber of patients might not support definitive conclusionson a strategy of using grafts from donors �40 kg for adultrecipients. The use of too small donors could be a possibleexplanation for these different outcomes. Dismal results havebeen reported when using pediatric whole grafts in adultpatients,24–28 with an increased incidence of HAT, cholesta-sis and sepsis, and reduced survival in cases of inadequatedimensional matching.27,28
In our experience, the application of Urata’s formula23
for estimation of whole liver weight, and the approximationof 25% and 75% of whole hepatic mass for LLSs and ERGs,respectively, were both correct as emerging from the actualgraft weights, whereas GRWR remained above the safetylimit of �1%21 in all cases. Interestingly, and again inaccordance with previous findings,23 the GW/donor BW ratiowas significantly higher in donors �40 kg versus �40 kg.These data confirmed that our criteria for donor/recipient sizematching were appropriate, resulting in no occurrence ofsmall-for-size syndromes. The proportionally higher livermass in younger donors seems to be an argument in favor ofa “downward” expansion of criteria of donor age. The prob-lems relative to the small vasculature and biliary tract, ratherthan a low liver mass, seem responsible for the increasedincidence of postoperative complications. Nevertheless, thegraft loss was due to technical or graft dysfunction-relatedcauses in 16% of recipients from donors �40 kg, in 13% ofERG recipients, in 11% of adult patients, and in 11% of adultrecipients from donors �40 kg, with corresponding 2-yearunrelated-death censored graft survival21 rates of 84%, 86%,88%, and 88% in these categories.
Except for our early experience of transplanting apediatric patient with an ERG from a 3-year-old donor, withsubsequent retransplantation for HAT, the use of right-sidedgrafts from donors �40 kg in children appears reasonable.On the other hand, the slightly less than 80% graft survivalrate in recipients of LLSs from donors �40 kg might havebeen adversely affected by the 25% of patients requiringurgent SLT, UNOS status 1 and 2A being recognized asnegative prognostic factors.7 This experience confirmed that
good donor selection is able to guarantee an excellent func-tional recovery in all paired grafts. Our selection criteria areslightly broader than those adopted by others.15–18
Donor ICU stay �3 days was the only factor able topredict graft loss by univariate analysis. However, we hadonly 2 cases of PNF (2.5%), whereas others reported PNFranging from 4% to 8%17 or even higher than 10%.11,16 Weobserved an ischemia time significantly longer with ERGsthan with LLSs. This could be explained by the fact that in16% of cases both grafts were transplanted at the same center,in which the LLS transplant usually starts before ERG.Moreover, the back table of ERG is longer than LLS, givenalso the more frequent use of an arterial interposition graft.Apparently, this different ischemia time had no impact on theoutcome, and especially on the incidence of PNF.
Concerning the separation of the hepatic vessels, thepolicy shared by the NITp Centers is to retain the celiac trunkwith the LLS, which is dictated by the smaller caliber andpossible multiplicity of the left hepatic artery. The overallincidence of vascular complications (9%) was almost entirelydue to the ACs rate, lower in recipients of LLSs (2%) andhigher in recipients of ERGs (10%), with an average of 6%.This complication was especially pronounced, as expected, inrecipients of ERGs from donors �40 kg.
Which partial graft, right or left, should retain the celiactrunk remains controversial. Most groups demonstratedthat by maintaining the entire length of the celiac axis incontinuity with the right grafts organ sharing among centersis improved without worsening patient and graft out-comes.3,11,16,30 Other authors6,31 showed that maintenance ofthe celiac trunk with the left-sided allograft does not increasethe overall incidence of HAT and avoids the need for a lefthepatic artery microvascular anastomosis. The recent litera-ture reports an incidence of vascular complications of around10%.3–16 Transplant centers performing SLT with mainte-nance of the celiac axis with the ERG frequently had anincidence of vascular complications above 10% with the“disadvantaged” LLS, whereas our overall data are within therange of 3% to 15% more commonly observed.3–16 Althoughsome caution is needed when evaluating the use of ERGsfrom very small pediatric donors, we think that the imple-mentation of organ sharing probably remains the only funda-mental issue favoring the preservation of the celiac trunk withright grafts.
Many surgical and nonsurgical risk factors for ACshave been previously elucidated.24–29 Compared with livertransplantation with adult donors, additional risk factors withpediatric grafts are the small diameter of vessels, the frequentuse of cytomegalovirus-positive donors for cytomegalovirus-negative recipients, and the greater postoperative fluctuationof coagulative state of pediatric recipients.24–26 Dealing withpartial and small-sized grafts, the low GRWR and the needfor interposition arterial grafts seem to be critical vari-ables.24–28 In particular, when transplanting pediatric liversinto adult recipients, it has been argued that, even though thesize discrepancy of vessels can be managed by a wideningplasty or an interposition graft, the entire hepatic vascular bedand the arterial flow through it will not change, and might be
Cescon et al Annals of Surgery • Volume 244, Number 5, November 2006
© 2006 Lippincott Williams & Wilkins812

very low with small-sized livers, especially with a significantportal flow.27 Among the available factors investigated in ourstudy, univariate analysis showed that the use of an arterialinterposition graft for arterial anastomosis was the only oneassociated with ACs. We found a correlation between lowDRWR and the use of arterial grafts, whose use probablyreflected either surgeon’s choice or necessity due to a graft/recipient size discrepancy. However, neither DRWR norGRWR was associated with ACs. Our findings are supportedby considerable evidence from both pediatric and adult livertransplantation24–26,29 but are in contrast with observationsthat the use of interposition grafts may improve results ofliving-donor and pediatric liver transplantation.32,33
Furthermore, the small diameter of arteries of ERGs inour series could justify the more frequent use of arterialinterposition grafts compared with adult-to-adult right lobetransplantation.
The incidence of BCs was 21%, higher than that usu-ally reported in SLTs.3–16 However, otherwise excellent se-ries of partial graft transplantation showed a BC rate ofaround 30%,34,35 whereas a BC rate of approximately 22% isreported in adult-to-adult right lobe living-donor transplanta-tion.36 The reason for the discrepancy is probably due to thesmaller size of pediatric grafts. BCs were more frequent, withprevalence of leaks (data not reported), in recipients of ERGsthan in recipients of LLSs. LLS bile ducts were very small,and their vascularization might have been impaired despitethe “in situ” division of the hilar plate. On the other hand, ajeopardized blood supply to segment IV might be responsiblefor the higher prevalence of leaks in recipients of ERGs.However, no graft was lost as a direct consequence of BCs,which shows the ability of experienced liver transplant cen-ters to treat the most common technical challenge in SLTconservatively.
CONCLUSIONThis multicenter experience shows that SLT with pe-
diatric donors should be considered a valid tool in limiting thepersisting organ shortage. These results are probably relatedto the implementation of a SLT program in the NITp areawith involvement of all cooperating centers and with a largenumber of cases, leading to sharing of the learning curve.Both small pediatric and adult patients might benefit from thisstrategy, although the use of donors �40 kg in larger recip-ients remains debatable. In this particular setting of SLT, thepolicy of maintaining the celiac trunk with left-sided graftsseems acceptable, while the use of vascular interpositiongrafts should be avoided due to the increased risk of arterialthrombosis.
ACKNOWLEDGMENTSThe authors thank the following contributors to this
multicenter study: Dr. Pietro Majno, Clinics of VisceralSurgery and Transplantation, University Hospitals of Ge-neva, Geneva, Switzerland; Dr. Xavier Rogiers, Departmentof Hepatobiliary Surgery, University Hospital Eppendorf,Hamburg, Germany; and Dr. Manuel Lopez Santamaria,
Unit of Liver Transplantation, Department of Pediatric Sur-gery, Hospital Universitario La Paz, Madrid, Spain; as wellas Wallis Marsh, MD, for reviewing the manuscript.
REFERENCES1. Renz JF, Emond JC, Yersiz H, et al. Split-liver transplantation in the United
States: outcomes of a Nation survey. Ann Surg. 2004;239:172–181.2. Couinaud C. Le Foie, Etudes anatomiques et chirurgicales. Paris:
Masson, 1957.3. Renz JF, Yersiz H, Reichert PR, et al. Split-liver transplantation: a
review. Am J Transplant. 2003;3:1323–1335.4. Rogiers X, Malago M, Gawad K, et al. In situ splitting of cadaveric
livers: the ultimate expansion of a limited donor pool. Ann Surg.1996;224:331–341.
5. Goss JA, Yersiz H, Shackleton CR, et al. In situ splitting of the cadavericliver for transplantation. Transplantation. 1997;64:871–877.
6. Rela M, Vougas V, Muiesan P, et al. Split liver transplantation: King’sCollege Hospital experience. Ann Surg. 1998;227:282–288.
7. Ghobrial RM, Yersiz H, Farmer DG, et al. Predictors of survival after invivo split liver transplantation: analysis of 110 consecutive patients. AnnSurg. 2000;232:312–323.
8. Spada M, Gridelli B, Colledan M, et al. Extensive use of split liver forpediatric transplantation: a single center experience. Liver Transpl.2000;6:415–428.
9. Sauer IM, Pascher A, Steinmuller T, et al. Split liver and living donation:the Berlin experience. Transplant Proc. 2001;33:1459–1460.
10. Nashan B, Lueck R, Becker T, et al. Outcome of split liver transplan-tation using ex-situ or in-situ splits from cadaver donors �abstract�. JointMeeting of the International Liver Transplantation Society, EuropeanLiver Transplantation Association, and Liver Intensive Care Group ofEurope. Berlin, Germany, July 11–13, 2001. Liver Transpl. 2001;7:C94.
11. Broering DC, Mueller L, Ganschow R, et al. Is there still a need for living-related liver transplantation in children? Ann Surg. 2001;234:713–722.
12. Otte JB. History of split liver transplantation. In: Rogiers X, Bismuth H,Busuttil RW, et al, eds. Split Liver Transplantation: Theoretical andPractical Aspects. Steinkopff-Darmstadt: Springer, 2002:3–9.
13. Deshpande RR, Bowles MJ, Vilca-Melendez H, et al. Results of splitliver transplantation in children. Ann Surg. 2002;236:248–253.
14. Gridelli B, Spada M, Petz W, et al. Split-liver transplantation eliminatesthe need for living-donor liver transplantation in children with end-stagecholestatic liver disease. Transplantation. 2003;75:1197–1203.
15. Noujaim HM, Gunson B, Mayer DA, et al. Worth continuing doing ex situliver graft splitting? A single-center analysis. Am J Transpl. 2003;3:318–323.
16. Yersiz H, Renz JF, Farmer DG, et al. One hundred in situ split-livertransplantation: a single-center experience. Ann Surg. 2003;238:496–507.
17. Emond JC, Freeman RB, Renz JF, et al. Optimizing the use of donatedcadaver livers: analysis and policy development to increase the applica-tion of split-liver transplantation. Liver Transpl. 2002;8:863–872.
18. Toso C, Ris F, Mentha G, et al. Potential impact of in situ liver splittingon the number of available grafts. Transplantation. 2002;74:222–226.
19. Petz W, Spada M, Sonzogni A, et al. Pediatric split liver transplantationusing elderly donors. Transplant Proc. 2001;33:1361.
20. Merion RM, Rush SH, Dykstra DM, et al. Predicted lifetimes for adultand pediatric split liver versus adult whole liver transplant recipients.Am J Transplant. 2004;4:1792–1797.
21. Kiuchi T, Kasahara M, Uryuhara K, et al. Impact of graft size mismatch-ing on graft prognosis in liver transplantation from living-donor. Trans-plantation. 1999;67:321–327.
22. Srinivasan P, Vilca-Melendez H, Muiesan P, et al. Liver transplantationwith monosegments. Surgery. 1999;126:10–12.
23. Urata K, Kawasaki S, Matsunami H, et al. Calculation of child and adultstandard volume for liver transplantation. Hepatology. 1995;21:1317–1321.
24. Mazzaferro V, Esquivel CO, Makowka L, et al. Hepatic artery throm-bosis after pediatric liver transplantation: a medical or surgical event?Transplantation. 1989;47:971–977.
25. Oh CK, Pelletier SJ, Sawyer RG, et al. Uni- and multi-variate analysisof risk factors for early and late hepatic artery thrombosis after livertransplantation. Transplantation. 2001;71:767–772.
26. Pastacaldi S, Teixeira R, Montalto P, et al. Hepatic artery thrombosis
Annals of Surgery • Volume 244, Number 5, November 2006 Split Liver Transplantation From Pediatric Donors
© 2006 Lippincott Williams & Wilkins 813

after orthotopic liver transplantation: a review of nonsurgical causes.Liver Transpl. 2001;7:75–81.
27. Yasutomi M, Harmsmen S, Innocenti F, et al. Outcome of pediatricdonor livers in adult recipients. Liver Transpl. 2001;7:38–40.
28. Emre S, Soejima Y, Altaca G, et al. Safety and risk of using pediatricdonor livers in adult liver transplantation. Liver Transpl. 2001;7:41–47.
29. Stange BJ, Glanemann M, Nuessler NC, et al. Hepatic artery thrombosisafter adult liver transplantation. Liver Transpl. 2003;9:612–620.
30. Noujaim HM, Gunson B, Mirza DF, et al. Ex situ preparation of leftsplit-liver grafts with left vascular pedicle only: is it safe? A comparativesingle-center study. Transplantation. 2002;74:1386–1390.
31. Kilic M, Seu P, Goss JA. Maintenance of the celiac trunk with theleft-sided liver allograft for in situ split-liver transplantation. Transplan-tation. 2002;73:1252–1257.
32. Rela M, Muiesan P, Bhatnagar V, et al. Hepatic artery thrombosis afterliver transplantation in children under 5 years of age. Transplantation.1996;61:1355–1357.
33. Marcos A, Killackey M, Orloff MS, et al. Hepatic arterial reconstructionin 95 adult right lobe living-donor liver transplants: evolution of anas-tomotic technique. Liver Transpl. 2003;6:570–574.
34. Sieders E, Peeters PM, TenVergert EM, et al. Analysis of survival andmorbidity after pediatric liver transplantation with full-size and techni-cal-variant grafts. Transplantation. 1999;68:471–472.
35. Wallot MA, Mathot M, Janssen M, et al. Long-term survival and lategraft loss in pediatric liver transplant recipients: a 15-year single-centerexperience. Liver Transpl. 2002;8:615–622.
36. Pascher A, Neuhaus P. Bile duct complications after liver transplanta-tion. Transpl Int. 2005;18:627–642.
Cescon et al Annals of Surgery • Volume 244, Number 5, November 2006
© 2006 Lippincott Williams & Wilkins814