Stem-Cell Transplantation in Children With Acute Lymphoblastic Leukemia: A Prospective International...
12
Stem-Cell Transplantation in Children With Acute Lymphoblastic Leukemia: A Prospective International Multicenter Trial Comparing Sibling Donors With Matched Unrelated Donors—The ALL-SCT-BFM-2003 Trial Christina Peters, Martin Schrappe, Arend von Stackelberg, André Schrauder, Peter Bader, Wolfram Ebell, Peter Lang, Karl-Walter Sykora, Johanna Schrum, Bernhard Kremens, Karoline Ehlert, Michael H. Albert, Roland Meisel, Susanne Matthes-Martin, Tayfun Gungor, Wolfgang Holter, Brigitte Strahm, Bernd Gruhn, Ansgar Schulz, Wilhelm Woessmann, Ulrike Poetschger, Martin Zimmermann, and Thomas Klingebiel See accompanying article doi: 10.1200/JCO.2014.58.4631; listen to the podcast by Dr Bunin at www.jco.org/podcasts Author affiliations appear at the end of this article. Published online ahead of print at www.jco.org on March 9, 2015. Written on behalf of the Berlin- Frankfurt-Muenster (BFM) Study Group, the International BFM Study Group, the Children’s Cancer Research Institute, and the European Society for Blood and Marrow Transplantation Paediatric Diseases Working Party. Supported by the Children’s Cancer Research Institute, Vienna, Austria; Deutsche Krebshilfe, Bonn, Germany; Deutsche Knochenmarkspenderdatei, Tübingen, Germany; Orphan Pharma- ceuticals and Amomed Pharma, Vienna, Austria; Fresenius Biotech, Gräfelfing, Germany; Gilead Sciences, Vienna, Austria; and Medac, Wedel, Germany. Authors’ disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article. The supporting institutes and compa- nies had no role in study design, data collection, data analysis, data interpreta- tion, or writing of the report. All data were maintained by the Berlin- Frankfurt-Muenster statistics and data center and were reviewed by an inde- pendent data safety monitoring committee. Clinical trial information: NC01423747. Corresponding author: Christina Peters, MD, St Anna Children’s Hospital, Kinderspitalgasse 6, A-1090 Vienna, Austria; e-mail: [email protected]. © 2015 by American Society of Clinical Oncology 0732-183X/14/3399-1/$20.00 DOI: 10.1200/JCO.2014.58.9747 A B S T R A C T Purpose Although hematopoietic stem-cell transplantation is widely performed in children with high-risk acute lymphoblastic leukemia (ALL), the influence of donor types is poorly understood. Thus, transplantation outcomes were compared in the prospective multinational Berlin-Frankfurt- Muenster (BFM) study group trial: ALL-SCT-BFM 2003 (Allogeneic Stem Cell Transplantation in Children and Adolescents with Acute Lymphoblastic Leukemia). Patients and Methods After conditioning with total-body irradiation and etoposide, 411 children with high-risk ALL received highly standardized stem-cell transplantations during the first or later remissions. Depending on donor availability, grafts originated from HLA-genoidentical siblings or from HLA-matched unrelated donors who were identified and matched by high-resolution allelic typing and were compatible in at least 9 of 10 HLA loci. Results Four-year event-free survival ( standard deviation [SD]) did not differ between patients with transplanta- tions from unrelated or sibling donors (0.67 0.03 v 0.71 0.05; P .405), with cumulative incidences of nonrelapse mortality ( SD) of 0.10 0.02 and 0.03 0.02 ( P .017) and relapse rates ( SD) of 0.22 0.02 and 0.24 0.04 ( P .732), respectively. Among recipients of transplantations from unrelated donors, no significant differences in event-free survival, overall survival, or nonrelapse mortality were observed between 9/10 and 10/10 matched grafts or between peripheral blood stem cells and bone marrow. The absence of chronic graft-versus-host disease had no effect on event-free survival. Engraftment was faster after bone marrow transplantation from siblings and was associated with fewer severe infections and pulmonary complications. Conclusion Outcome among high-risk pediatric patients with ALL after hematopoietic stem-cell transplanta- tion was not affected by donor type. Standardized myeloablative conditioning produced a low incidence of treatment-related mortality and effective control of leukemia. J Clin Oncol 33. © 2015 by American Society of Clinical Oncology INTRODUCTION Although the majority of children and adolescents with acute lymphoblastic leukemia (ALL) are cur- able with current chemotherapy regimens, poor outcomes persist in some individuals. 1,2 These high-risk patients require additional therapeutic ap- proaches after achieving remission. Allogeneic he- matopoietic stem-cell transplantation (HSCT) can effectively induce immunologic antileukemic con- trol in children with ALL by means of the graft- versus-leukemia effect. 3 HSCT from allogeneic donors has become the standard of care for such high-risk patients. Only 20% to 25% of children with indications for allogeneic HSCT have HLA- matched sibling donors (MSDs), but the availability JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T © 2015 by American Society of Clinical Oncology 1 http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2014.58.9747 The latest version is at Published Ahead of Print on March 9, 2015 as 10.1200/JCO.2014.58.9747 Copyright 2015 by American Society of Clinical Oncology Zurich) on March 27, 2015 from 130.60.58.2 Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Stem-Cell Transplantation in Children With Acute Lymphoblastic Leukemia: A Prospective International...

Stem-Cell Transplantation in Children With AcuteLymphoblastic Leukemia: A Prospective InternationalMulticenter Trial Comparing Sibling Donors With MatchedUnrelated Donors—The ALL-SCT-BFM-2003 Trial
Christina Peters, Martin Schrappe, Arend von Stackelberg, André Schrauder, Peter Bader, Wolfram Ebell,Peter Lang, Karl-Walter Sykora, Johanna Schrum, Bernhard Kremens, Karoline Ehlert, Michael H. Albert,Roland Meisel, Susanne Matthes-Martin, Tayfun Gungor, Wolfgang Holter, Brigitte Strahm, Bernd Gruhn,Ansgar Schulz, Wilhelm Woessmann, Ulrike Poetschger, Martin Zimmermann, and Thomas Klingebiel
See accompanying article doi: 10.1200/JCO.2014.58.4631; listen to the podcast by Dr Bunin atwww.jco.org/podcasts
Author affiliations appear at the end ofthis article.
Published online ahead of print atwww.jco.org on March 9, 2015.
Written on behalf of the Berlin-Frankfurt-Muenster (BFM) Study Group,the International BFM Study Group, theChildren’s Cancer Research Institute,and the European Society for Blood andMarrow Transplantation PaediatricDiseases Working Party.
Supported by the Children’s CancerResearch Institute, Vienna, Austria;Deutsche Krebshilfe, Bonn, Germany;Deutsche Knochenmarkspenderdatei,Tübingen, Germany; Orphan Pharma-ceuticals and Amomed Pharma, Vienna,Austria; Fresenius Biotech, Gräfelfing,Germany; Gilead Sciences, Vienna,Austria; and Medac, Wedel, Germany.
Authors’ disclosures of potentialconflicts of interest are found in thearticle online at www.jco.org. Authorcontributions are found at the end ofthis article.
The supporting institutes and compa-nies had no role in study design, datacollection, data analysis, data interpreta-tion, or writing of the report. All datawere maintained by the Berlin-Frankfurt-Muenster statistics and datacenter and were reviewed by an inde-pendent data safety monitoringcommittee.
Clinical trial information: NC01423747.
Corresponding author: Christina Peters,MD, St Anna Children’s Hospital,Kinderspitalgasse 6, A-1090 Vienna,Austria; e-mail: [email protected].
© 2015 by American Society of ClinicalOncology
0732-183X/14/3399-1/$20.00
DOI: 10.1200/JCO.2014.58.9747
A B S T R A C T
PurposeAlthough hematopoietic stem-cell transplantation is widely performed in children with high-riskacute lymphoblastic leukemia (ALL), the influence of donor types is poorly understood. Thus,transplantation outcomes were compared in the prospective multinational Berlin-Frankfurt-Muenster (BFM) study group trial: ALL-SCT-BFM 2003 (Allogeneic Stem Cell Transplantation inChildren and Adolescents with Acute Lymphoblastic Leukemia).
Patients and MethodsAfter conditioning with total-body irradiation and etoposide, 411 children with high-risk ALLreceived highly standardized stem-cell transplantations during the first or later remissions.Depending on donor availability, grafts originated from HLA-genoidentical siblings or fromHLA-matched unrelated donors who were identified and matched by high-resolution allelic typingand were compatible in at least 9 of 10 HLA loci.
ResultsFour-year event-free survival (� standard deviation [SD]) did not differ between patients with transplanta-tions from unrelated or sibling donors (0.67 � 0.03 v 0.71 � 0.05; P � .405), with cumulative incidences ofnonrelapse mortality (� SD) of 0.10 � 0.02 and 0.03 � 0.02 (P � .017) and relapse rates (� SD) of 0.22 �0.02 and 0.24 � 0.04 (P � .732), respectively. Among recipients of transplantations from unrelated donors,no significant differences in event-free survival, overall survival, or nonrelapse mortality were observedbetween 9/10 and 10/10 matched grafts or between peripheral blood stem cells and bone marrow. Theabsence of chronic graft-versus-host disease had no effect on event-free survival. Engraftment was fasterafter bone marrow transplantation from siblings and was associated with fewer severe infections andpulmonary complications.
ConclusionOutcome among high-risk pediatric patients with ALL after hematopoietic stem-cell transplanta-tion was not affected by donor type. Standardized myeloablative conditioning produced a lowincidence of treatment-related mortality and effective control of leukemia.
J Clin Oncol 33. © 2015 by American Society of Clinical Oncology
INTRODUCTION
Although the majority of children and adolescentswith acute lymphoblastic leukemia (ALL) are cur-able with current chemotherapy regimens, pooroutcomes persist in some individuals.1,2 Thesehigh-risk patients require additional therapeutic ap-proaches after achieving remission. Allogeneic he-
matopoietic stem-cell transplantation (HSCT) caneffectively induce immunologic antileukemic con-trol in children with ALL by means of the graft-versus-leukemia effect.3 HSCT from allogeneicdonors has become the standard of care for suchhigh-risk patients. Only 20% to 25% of childrenwith indications for allogeneic HSCT have HLA-matched sibling donors (MSDs), but the availability
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
© 2015 by American Society of Clinical Oncology 1
http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2014.58.9747The latest version is at Published Ahead of Print on March 9, 2015 as 10.1200/JCO.2014.58.9747
Copyright 2015 by American Society of Clinical OncologyZurich) on March 27, 2015 from 130.60.58.2
Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek UniversitatCopyright © 2015 American Society of Clinical Oncology. All rights reserved.
of volunteer HLA-matched unrelated donors (MUDs) has increasedtransplantation rates over recent decades.4,5
Previous retrospective analyses demonstrated that some high-riskpatients with ALL benefitted from unrelated donor HSCT, but they hadnonrelapsemortality(NRM)ratesof25%.6,7 Inaddition,heterogeneityofavailabledataregardingpatientselection,qualityofHLAtyping,degreeofmatching, transplantation procedures, and study end points have ham-pered comparisons of different HSCT approaches. 8,9 Thus, in 2003, theBerlin-Frankfurt-Muenster (BFM) study group initiated the prospectiveinternational multicenter ALL-SCT-BFM 2003 (Allogeneic Stem CellTransplantation in Children and Adolescents with Acute LymphoblasticLeukemia)trialofallogeneicHSCTforchildrenwithALLandindicationsfor HSCT according to first-line and relapse chemotherapy protocolsduring first, second, or subsequent complete remissions (CRs). In thesestudies, all patients received pretransplantation treatments according to
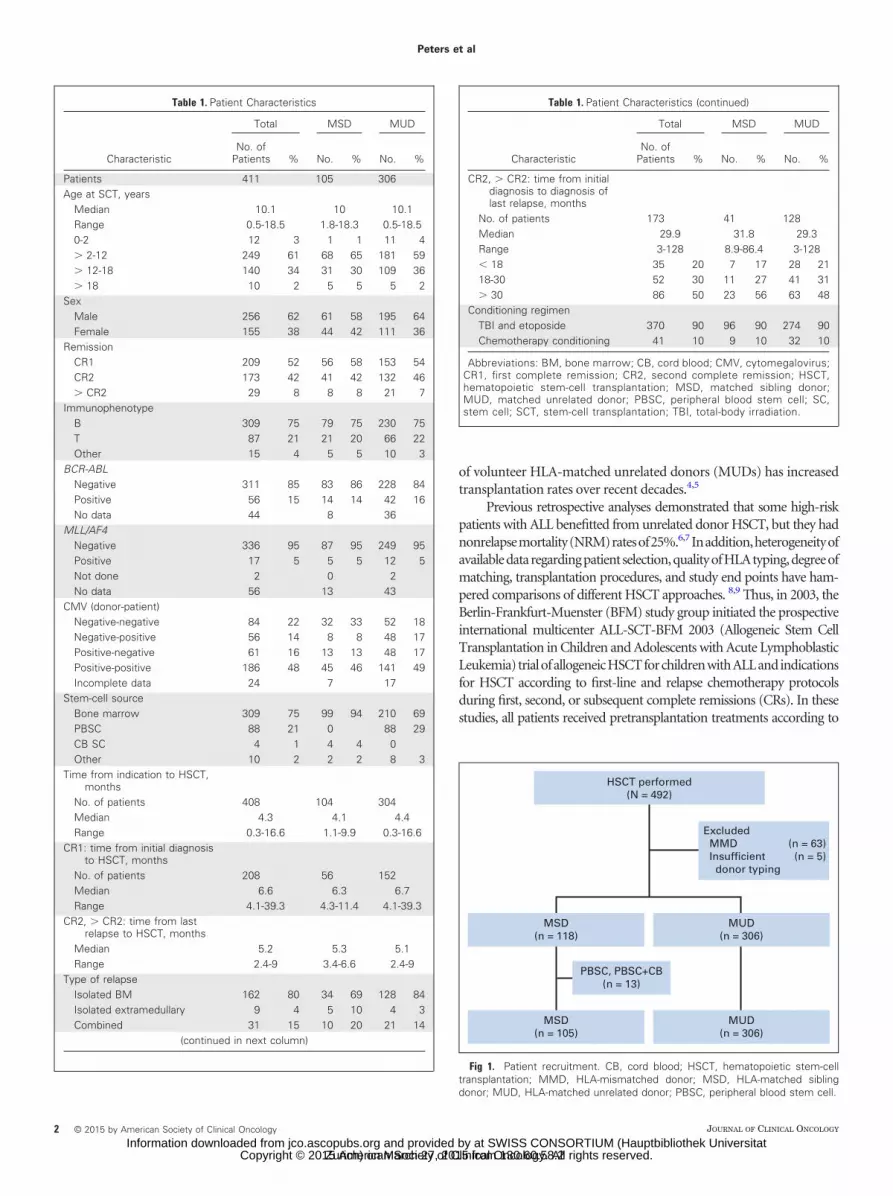
Table 1. Patient Characteristics
Characteristic
Total MSD MUD
No. ofPatients % No. % No. %
Patients 411 105 306Age at SCT, years
Median 10.1 10 10.1Range 0.5-18.5 1.8-18.3 0.5-18.50-2 12 3 1 1 11 4� 2-12 249 61 68 65 181 59� 12-18 140 34 31 30 109 36� 18 10 2 5 5 5 2
SexMale 256 62 61 58 195 64Female 155 38 44 42 111 36
RemissionCR1 209 52 56 58 153 54CR2 173 42 41 42 132 46� CR2 29 8 8 8 21 7
ImmunophenotypeB 309 75 79 75 230 75T 87 21 21 20 66 22Other 15 4 5 5 10 3
BCR-ABLNegative 311 85 83 86 228 84Positive 56 15 14 14 42 16No data 44 8 36
MLL/AF4Negative 336 95 87 95 249 95Positive 17 5 5 5 12 5Not done 2 0 2No data 56 13 43
CMV (donor-patient)Negative-negative 84 22 32 33 52 18Negative-positive 56 14 8 8 48 17Positive-negative 61 16 13 13 48 17Positive-positive 186 48 45 46 141 49Incomplete data 24 7 17
Stem-cell sourceBone marrow 309 75 99 94 210 69PBSC 88 21 0 88 29CB SC 4 1 4 4 0Other 10 2 2 2 8 3
Time from indication to HSCT,months
No. of patients 408 104 304Median 4.3 4.1 4.4Range 0.3-16.6 1.1-9.9 0.3-16.6
CR1: time from initial diagnosisto HSCT, months
No. of patients 208 56 152Median 6.6 6.3 6.7Range 4.1-39.3 4.3-11.4 4.1-39.3
CR2, � CR2: time from lastrelapse to HSCT, months
Median 5.2 5.3 5.1Range 2.4-9 3.4-6.6 2.4-9
Type of relapseIsolated BM 162 80 34 69 128 84Isolated extramedullary 9 4 5 10 4 3Combined 31 15 10 20 21 14
(continued in next column)
Table 1. Patient Characteristics (continued)
Characteristic
Total MSD MUD
No. ofPatients % No. % No. %
CR2, � CR2: time from initialdiagnosis to diagnosis oflast relapse, months
No. of patients 173 41 128Median 29.9 31.8 29.3Range 3-128 8.9-86.4 3-128� 18 35 20 7 17 28 2118-30 52 30 11 27 41 31� 30 86 50 23 56 63 48
Conditioning regimenTBI and etoposide 370 90 96 90 274 90Chemotherapy conditioning 41 10 9 10 32 10
Abbreviations: BM, bone marrow; CB, cord blood; CMV, cytomegalovirus;CR1, first complete remission; CR2, second complete remission; HSCT,hematopoietic stem-cell transplantation; MSD, matched sibling donor;MUD, matched unrelated donor; PBSC, peripheral blood stem cell; SC,stem cell; SCT, stem-cell transplantation; TBI, total-body irradiation.
HSCT performed(N = 492)
MSD(n = 105)
MUD(n = 306)
MSD(n = 118)
MUD(n = 306)
Excluded MMD (n = 63) Insufficient (n = 5) donor typing
PBSC, PBSC+CB(n = 13)
Fig 1. Patient recruitment. CB, cord blood; HSCT, hematopoietic stem-celltransplantation; MMD, HLA-mismatched donor; MSD, HLA-matched siblingdonor; MUD, HLA-matched unrelated donor; PBSC, peripheral blood stem cell.
Peters et al
2 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
the ALL-BFM 2000 (Combination Chemotherapy Based on Risk of Re-lapse in Treating Young Patients With Acute Lymphoblastic Leuke-mia), the COALL (Multicenter Therapy Study of the Co-OperativeStudy Group for Childhood ALL), or the ALL-REZ BFM 2002(ALL-REZ BFM 2002: Multi-Center Study for Children With Re-lapsed Acute Lymphoblastic Leukemia) protocols.10,11 Patientswere allocated to receive HSCT from MSDs when they were avail-able or allogeneic HSCT from 9/10 or 10/10 MUDs when no MSDswere available. Hence treatment assignments were biologicallyrandomized according to the availability of donors.
Outcomes after HSCT are influenced by patient’s remission sta-tus, age, conditioning regimens, graft-versus-host disease (GVHD)prophylaxis, and supportive care and are also influenced by donorselections and stem-cell sources.12-16 Therefore, this trial aimed tostratify patients according to their remission status and age to harmo-nize the transplantation procedures (which were clearly defined ac-cording to standardized protocols) and to include patients from 29centers in Austria, Germany, and Switzerland (Data Supplement).
PATIENTS AND METHODS
Study Design
Outcomes of HSCTs from MSDs and MUDs in children with ALL whohad poor prognoses after treatment with a consistent remission inductionprotocol were prospectively compared.17,18
Patients were allocated to receive HSCT from MSDs when they wereavailable or from 9/10 or 10/10 HLA-matched MUDs. Conditioning wasperformed with total-body irradiation (TBI) and etoposide in patients olderthan age 2 years and in the absence of contraindications for TBI. Patients willbe observed indefinitely, and the median follow-up time at the time of thisanalysis was 4.2 years (see the Data Supplement for protocol outlines). Thisstudy was performed in accordance with the Declaration of Helsinki and GoodClinical Practice and was approved by the local institutional review board ateach participating site. Patients and/or their legal guardians provided writteninformed consent before enrollment.
Patient Selection
Eligible patients were treated with remission induction therapy accord-ing to the BFM or COALL trial protocol; were identified as high-risk by usingthe risk-adapted stratification criteria defined by BFM, including leukemiaphenotype, response to induction chemotherapy, and time and site of re-lapse19; had morphologic remission (� 5% bone marrow blasts) at the time ofHSCT; were age 18 years or younger at the time of initial diagnosis or relapse;and had no pregnancy, no secondary malignancy, and no previous HSCT.
Donor Selection
HLA typing was performed by using allelic typing, with a resolution offour digits per allele at HLA-A, -B, -C, -DRB1, and -DQB1 loci. Matchedsibling donors were defined as genotypically or phenotypically identical sib-lings. No 9/10 or 10/10 HLA-matched nonsibling donors were identified.Thus, in the absence of MSDs, 9/10 or 10/10 MUDs were recruited fromnational and international donor registries. The assignment to a donor group
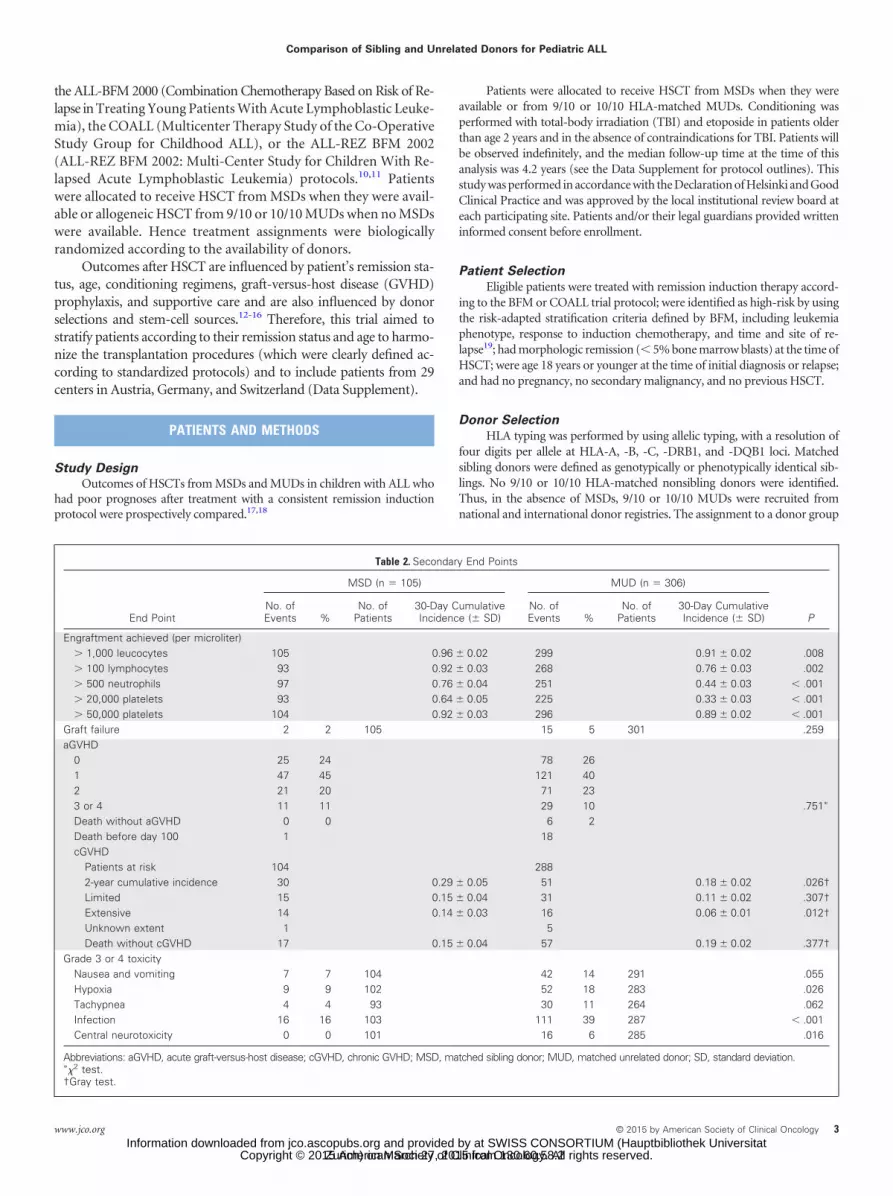
Table 2. Secondary End Points
End Point
MSD (n � 105) MUD (n � 306)
PNo. ofEvents %
No. ofPatients
30-Day CumulativeIncidence (� SD)
No. ofEvents %
No. ofPatients
30-Day CumulativeIncidence (� SD)
Engraftment achieved (per microliter)� 1,000 leucocytes 105 0.96 � 0.02 299 0.91 � 0.02 .008� 100 lymphocytes 93 0.92 � 0.03 268 0.76 � 0.03 .002� 500 neutrophils 97 0.76 � 0.04 251 0.44 � 0.03 � .001� 20,000 platelets 93 0.64 � 0.05 225 0.33 � 0.03 � .001� 50,000 platelets 104 0.92 � 0.03 296 0.89 � 0.02 � .001
Graft failure 2 2 105 15 5 301 .259aGVHD
0 25 24 78 261 47 45 121 402 21 20 71 233 or 4 11 11 29 10 .751�
Death without aGVHD 0 0 6 2Death before day 100 1 18cGVHD
Patients at risk 104 2882-year cumulative incidence 30 0.29 � 0.05 51 0.18 � 0.02 .026†Limited 15 0.15 � 0.04 31 0.11 � 0.02 .307†Extensive 14 0.14 � 0.03 16 0.06 � 0.01 .012†Unknown extent 1 5Death without cGVHD 17 0.15 � 0.04 57 0.19 � 0.02 .377†
Grade 3 or 4 toxicityNausea and vomiting 7 7 104 42 14 291 .055Hypoxia 9 9 102 52 18 283 .026Tachypnea 4 4 93 30 11 264 .062Infection 16 16 103 111 39 287 � .001Central neurotoxicity 0 0 101 16 6 285 .016
Abbreviations: aGVHD, acute graft-versus-host disease; cGVHD, chronic GVHD; MSD, matched sibling donor; MUD, matched unrelated donor; SD, standard deviation.��2 test.†Gray test.
Comparison of Sibling and Unrelated Donors for Pediatric ALL
www.jco.org © 2015 by American Society of Clinical Oncology 3
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
determined the transplantation regimen (ie, stem-cell source, stem-cell ma-nipulation, conditioning protocol, and GVHD prophylaxis; details are pro-vided in the Protocol [online only]).
In the absence of matched donors, patients continued with conventionalchemotherapy, or other transplantation approaches were performed by usingmismatched cord blood (CB) or haploidentical HSCTs. These patients will bedescribed in a separate report.
Stem-Cell Source
For children, the preferred stem-cell source was bone marrow (BM)from either MSDs or MUDs, as indicated by a large retrospective analysis that
showed a higher incidence of chronic GVHD (cGVHD) and lower overallsurvival (OS) after peripheral blood stem cell (PBSC) transplantation.20 Re-cipients of unrelated grafts received BM or PBSCs according to donor choices.CB from MSDs or MUDs was used when sufficient cell numbers were available(� 2.5 � 107 cells per kilogram of recipient body weight).21
Conditioning Regimen
The conditioning regimen for patients older than age 2 years comprisedfractionated TBI (12 Gy in six fractions over 3 days with lung shielding at 10Gy) and intravenous etoposide 60 mg/kg (upper total dose, 3,600 mg). Chil-dren younger than age 2 years and older children with contraindications for
cGVH
D
Time (years)
1.0
0.8
0.6
0.4
0.2
BA
0 42 6 8 1031 5 7 9
cGVH
D
Time (years)
1.0
0.8
0.6
0.4
0.2
0 42 6 8 1031 5 7 9
Exte
nsiv
e cGVH
D
Time (years)
1.0
0.8
0.6
0.4
0.2
DC
0 42 6 8 1031 5 7 9
Exte
nsiv
e cGVH
D
Time (years)
1.0
0.8
0.6
0.4
0.2
0 42 6 8 1031 5 7 9
Lim
ited
cGVH
D
Time (years)
1.0
0.8
0.6
0.4
0.2
FE
0 42 6 8 1031 5 7 9
Lim
ited
cGVH
D
Time (years)
1.0
0.8
0.6
0.4
0.2
0 42 6 8 1031 5 7 9
10/10 HLA matches9/10 HLA matches
Peripheral-blood stem cellsBone marrow
10/10 HLA matches9/10 HLA matches
Peripheral-blood stem cellsBone marrow
10/10 HLA matches9/10 HLA matches
Peripheral-blood stem cellsBone marrow
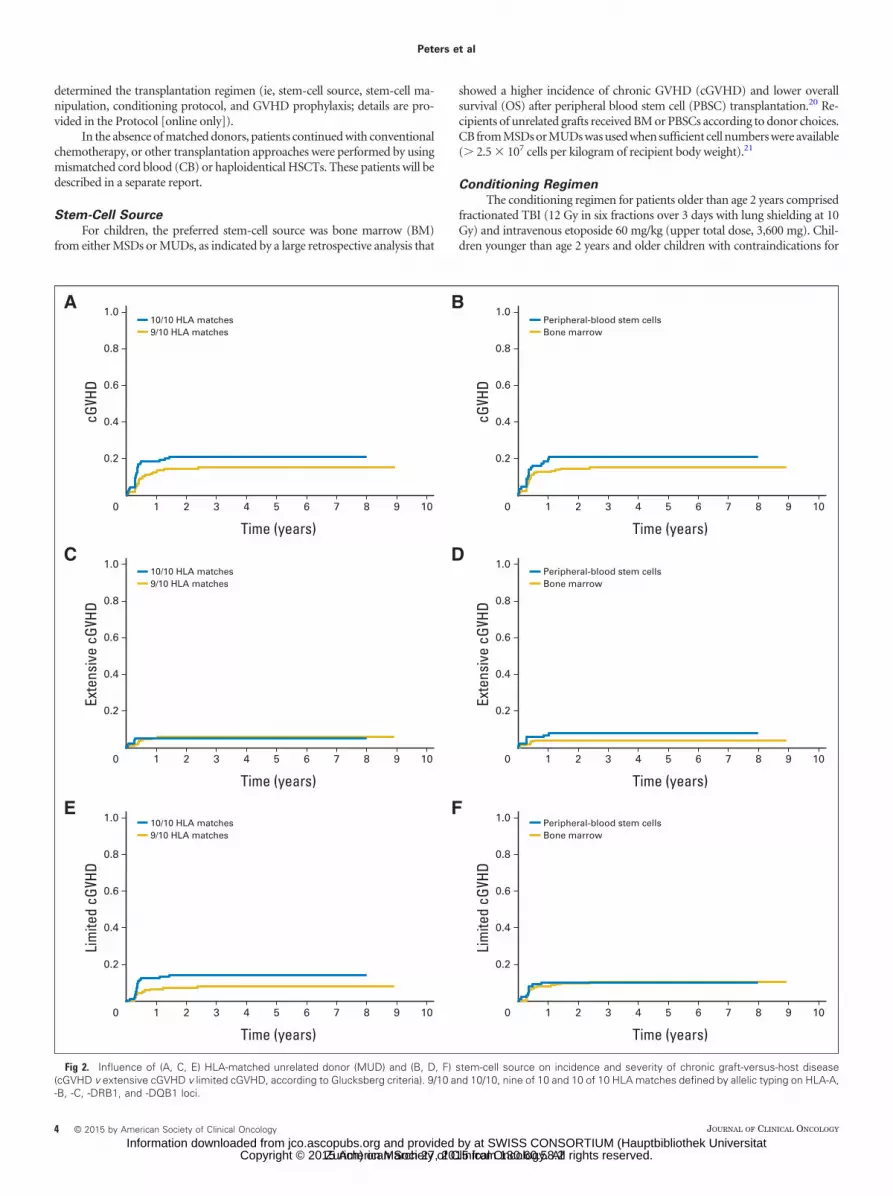
Fig 2. Influence of (A, C, E) HLA-matched unrelated donor (MUD) and (B, D, F) stem-cell source on incidence and severity of chronic graft-versus-host disease(cGVHD v extensive cGVHD v limited cGVHD, according to Glucksberg criteria). 9/10 and 10/10, nine of 10 and 10 of 10 HLA matches defined by allelic typing on HLA-A,-B, -C, -DRB1, and -DQB1 loci.
Peters et al
4 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.

TBI (eg, CNS irradiation before HSCT, history of CNS toxicities, signs ofleukoencephalopathy) were treated with chemotherapy consisting of intrave-nous busulfan without therapeutic drug monitoring according to the manu-facturer’s brochure and as described elsewhere,22 in combination withcyclophosphamide (120 mg/kg total dose) and etoposide (40 mg/kg totaldose). Details of conditioning regimens are provided in the Protocol.
GVHD Prophylaxis
GVHD prophylaxis for MSD bone marrow transplantation consisted ofinitial intravenous cyclosporine 1.5 mg/kg twice per day followed by oralcyclosporine when appropriate. MUD-HSCT patients were administered cy-closporine at the same dosage with methotrexate 10 mg/m2 on days �1, �3,and �6 after HSCT, followed by folinic acid 15 mg/m2 24 hours after eachdose. Antithymocyte globulin (ATG) was administered on days �3, �2, and�1 (ATG Fresenius 60 mg/kg total dose).
Statistics
Event-free survival (EFS) was the primary end point, taking the date ofHSCT as the starting point, and the date of first event or of the last follow-up asthe end of the interval. An event was defined as relapse, secondary malignancy,or death as a result of any cause. The null hypothesis is that MUD-HSCT isinferior to MSD-HSCT. To determine whether there was any difference in EFSbetween MSD-HSCT and MUD-HSCT, the cumulative incidence approachwas used, with a one-sided CI for the difference of the Kaplan-Meier estimateof the 4-year EFS. With the initially planned sample size of 84 MSD patientsand 228 MUD patients, 80% power can be achieved to show that MUD-HSCTis noninferior if a lower limit of the CI of 16% is used as the margin.23
Secondary end points were OS, relapse incidence (RI), NRM, engraft-ment, incidence and severity of acute GVHD (aGVHD) and cGVHD, andtoxicity. For OS, death as a result of any cause was used as an event, andsurvivors were censored at the date of the last follow-up information. For RI,NRM, engraftment, and cGVHD, cumulative incidences were estimated byusing the approach of Kalbfleisch and Prentice.24 Competing events weredefined as follows: for RI, deaths from any cause and secondary malignancies;for engraftment and cGVHD, deaths from any cause; and for NRM, relapsesand secondary malignancies.25 For the evaluation of risk factors and donortype, the comparison of cumulative incidences was done with Gray’s test andan approach based on pseudovalues,26 respectively. The pseudovalue ap-proach was also used to assess the impact of donor type on the 4-year proba-bility of EFS and probability of OS in subgroups of patients because theproportional hazard assumption was violated. The incidences of aGVHD andgrade 3 or 4 toxicity were compared by using the �2 test.
The impact of prognostic factors on EFS and OS was evaluated by usingCox regression analyses, and pseudovalue regression analyses were used toseparately evaluate the impact of donor type and of remission status on long-term event rates and survival times.
RESULTS
Characteristics of Study Patients
Between September 2003 and September 2011, 411 patientsreceived HSCT according to the protocol (105 MSDs and 306
EFS
Time (years)
1.0
0.8
0.6
0.4
0.2
BA
0 42 6 8 1031 5 7 9
OS
Time (years)
1.0
0.8
0.6
0.4
0.2
0 42 6 8 1031 5 7 9
RI
Time (years)
1.0
0.8
0.6
0.4
0.2
DC
0 42 6 8 1031 5 7 9
NRM
Time (years)
1.0
0.8
0.6
0.4
0.2
0 42 6 8 1031 5 7 9
Patients Events 4-yr. EFS P*MSD 105 30 0.71±0.05 .405MUD 306 100 0.67±0.03
Difference in 4-year EFS 5%Upper limit of one-sided 95% CI 13%
Patients Events 4-yr. OS P*MSD 105 22 0.79±0.04 .230MUD 306 81 0.73±0.03
Patients Events 4-yr. CI P*MSD 105 24 0.24±0.04 .732MUD 306 65 0.22±0.02
Patients Events 4-yr. CI P*MSD 105 3 0.03±0.02 .017MUD 306 30 0.10±0.02
Fig 3. Four-year (A) event-free survival (EFS), (B) overall survival (OS), (C) relapse incidence (RI), and (D) nonrelapse mortality (NRM). MSD, HLA-matched siblingdonor; MUD, HLA-matched unrelated donor. (*) Based on pseudovalues at 4 years.
Comparison of Sibling and Unrelated Donors for Pediatric ALL
www.jco.org © 2015 by American Society of Clinical Oncology 5
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
MUDs). Patient characteristics are provided in Table 1. In additionto these patients, 81 patients were given transplantations by usingapproaches that are beyond the scope of this article (Fig 1) andwere excluded from analyses.
Patient groups had comparable proportions of patients in first orlater remissions and had similar times from initial diagnosis or relapseto HSCT (median, 4.3 months) and phenotypical risk factors. In all,90% of patients in both groups received conditioning regimens con-taining TBI and etoposide.
Among 105 patients who received MSD-HSCT, 99 received BMalone, four received CB, and two received BM and CB. The majority ofpatients with MUD transplantations (210 patients; 69%) received BM,whereas 88 patients (29%) received PBSCs and the remaining eightpatients received CB or a combination of CB and BM or PBSCs afterdelayed engraftment. At the time of analysis in November 2013, themedian follow-up from time of diagnosis until last follow-up evalua-tion was 4.2 years (range, 0.27 to 9.1 years).
Engraftment
Engraftment was significantly faster after MSD-HSCT (Table 2).The median time to neutrophil engraftment (ie, absolute neutrophilcount � 500/�L) was 17 days after MSD-HSCT and 22 days afterMUD-HSCT with a 30-day cumulative incidence of 76% versus 44%(P � .001). Lymphocyte count � 100/�L was observed in the MSD
group on day 14 compared with day 23 after MUD-HSCT with 30-daycumulative incidences of 92% versus 76% (P � .001).
Transfusion-independent platelet count � 20,000/�L wasreached on day 22 after MSD-HSCT and on day 32 after MUD-HSCTwith 30-day cumulative incidences of 64% versus 33% (P � .001).Although graft failure was generally rare, it was more frequent amongpatients who received MUD-HSCT (n � 2 v n � 15; P � .259).
aGVHD and cGVHD
No differences in incidence or severity of aGVHD were observedbetween MSD-HSCT and MUD-HSCT patients; in contrast, exten-sive cGVHD occurred more frequently after MSD-HSCT (Table 2).For the MUD group, in which more intensive immunosuppressionwas used, the 2-year cumulative incidence of extensive cGVHD wasonly 0.06 � 0.01 and did not vary between BM and PBSCs or withHLA disparities (9/10 or 10/10 matches; Fig 2). Fourteen patients(14%) developed extensive cGVHD after MSD-HSCT; 16 patients(6%) developed extensive cGVHD after MUD-HSCT. Five of thosepatients had a Karnovsky/Lansky performance status below 80% 2years after MSD-HSCT and only six of 16 MUD-HSCT patientsreached a performance status of 80% to 100%, reflecting the reducedquality of life with such complications.
After MSD-HSCT, patients older than age 12 years had a higherincidence of extensive cGVHD compared with younger patients (25%
EFS
Time (years)
1.0
0.8
0.6
0.4
0.2
BA
0 42 6 8 1031 5 7 9
OS
Time (years)
1.0
0.8
0.6
0.4
0.2
0 42 6 8 1031 5 7 9
RI
Time (years)
1.0
0.8
0.6
0.4
0.2
DC
0 42 6 8 1031 5 7 9
NRM
Time (years)
1.0
0.8
0.6
0.4
0.2
0 42 6 8 1031 5 7 9
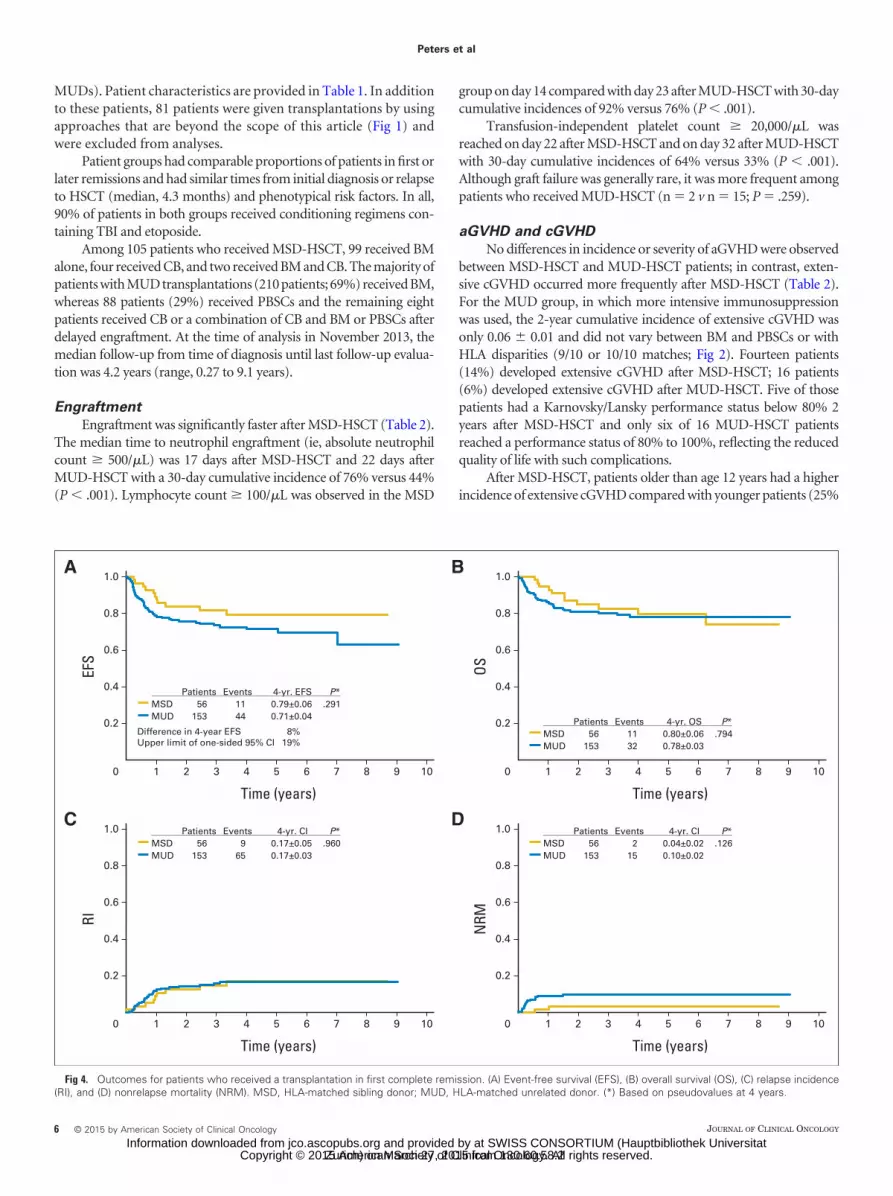
Patients Events 4-yr. EFS P*MSD 56 11 0.79±0.06 .291MUD 153 44 0.71±0.04
Difference in 4-year EFS 8%Upper limit of one-sided 95% CI 19%
Patients Events 4-yr. OS P*MSD 56 11 0.80±0.06 .794MUD 153 32 0.78±0.03
Patients Events 4-yr. CI P*MSD 56 9 0.17±0.05 .960MUD 153 65 0.17±0.03
Patients Events 4-yr. CI P*MSD 56 2 0.04±0.02 .126MUD 153 15 0.10±0.02
Fig 4. Outcomes for patients who received a transplantation in first complete remission. (A) Event-free survival (EFS), (B) overall survival (OS), (C) relapse incidence(RI), and (D) nonrelapse mortality (NRM). MSD, HLA-matched sibling donor; MUD, HLA-matched unrelated donor. (*) Based on pseudovalues at 4 years.
Peters et al
6 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
v 48%). Sex match of donor and recipient, year of HSCT, phenotype,and cytomegalovirus status did not influence the incidence and sever-ity of cGVHD after MSD-HSCT.
Toxicity
The incidenceofgrade3to4 infectionwassignificantlyhigher in theMUD group and was associated with a tendency toward pulmonarycomplications (Table 2). Other extramedullary toxicities of grade � 2were rare and were predominantly associated with oral mucositis. Thirty-threepatientsdiedasaresultofnonrelapsecomplications, includingthreeof 105 from the MSD-HSCT group and 30 of 306 from the MUD-HSCTgroup (P � .017). The main causes of death were bacterial (n � 6) andviral(n�6)infections,Epstein-Barrvirus–lymphoproliferativedisease(n�3),multiorganfailure(n�6), toxicity(n�4),andaGVHD(n�2)orcGVHD (n � 6). A total of nine patients developed secondary malignan-cies at a median of 5 years (range, 26 to 84 months) after HSCT: fivethyroid cancers, one myelodysplastic syndrome, one osteosarcoma, onerhabdomyosarcoma, and one colon carcinoma. Among these patients,three were in the MSD-HSCT group and six were in the MUD-HSCTgroup. All patients received TBI.
Outcomes
The 4-year EFS rate after MUD-HSCT was similar to that afterMSD-HSCT (0.67�0.03 v 0.71�0.05; P� .405). The upper limit of the
95% CI for the difference in 4-year EFS was 13% (Fig 3A). No significantdifferences in OS or RI were observed (4-year cumulative incidence,0.22 � 0.02 after MUD-HSCT and 0.24 � 0.02 after MSD-HSCT).
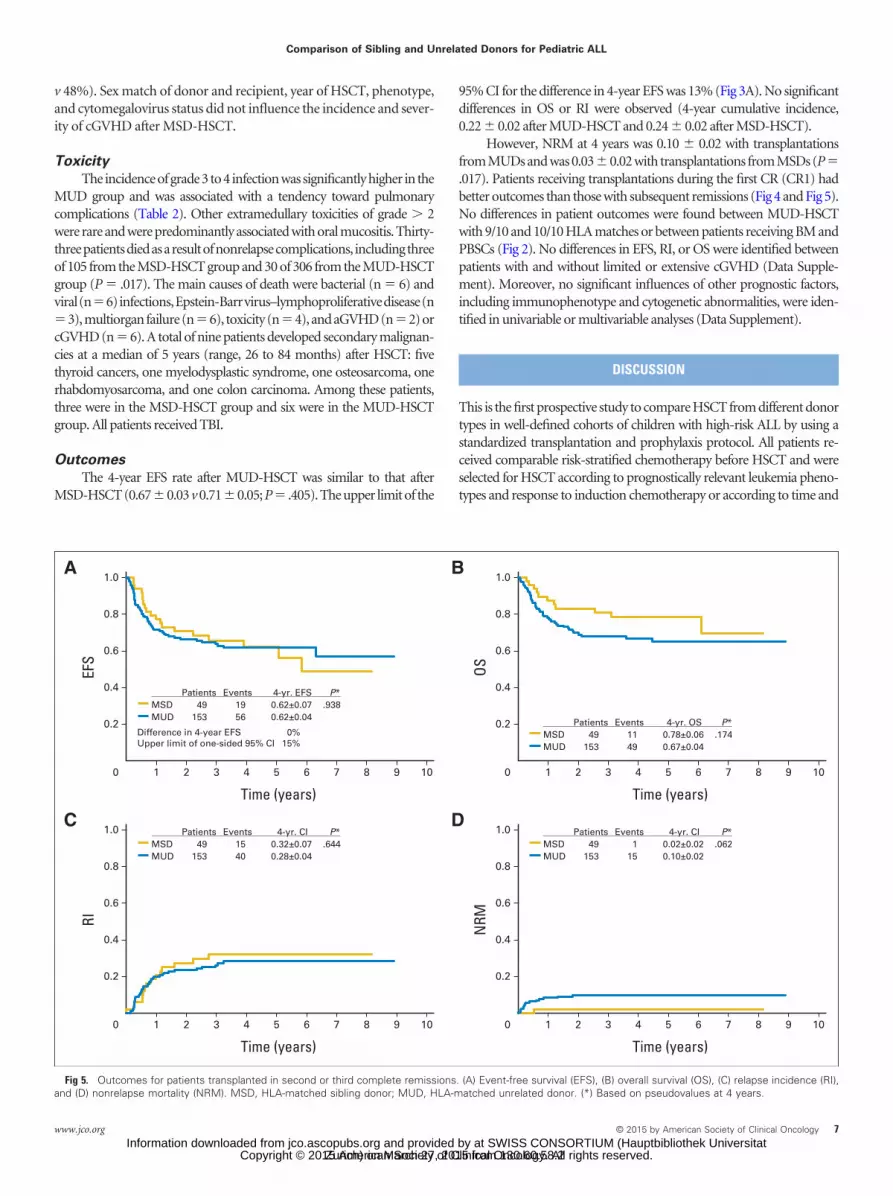
However, NRM at 4 years was 0.10 � 0.02 with transplantationsfrom MUDs and was 0.03�0.02 with transplantations from MSDs (P�.017). Patients receiving transplantations during the first CR (CR1) hadbetter outcomes than those with subsequent remissions (Fig 4 and Fig 5).No differences in patient outcomes were found between MUD-HSCTwith 9/10 and 10/10 HLA matches or between patients receiving BM andPBSCs (Fig 2). No differences in EFS, RI, or OS were identified betweenpatients with and without limited or extensive cGVHD (Data Supple-ment). Moreover, no significant influences of other prognostic factors,including immunophenotype and cytogenetic abnormalities, were iden-tified in univariable or multivariable analyses (Data Supplement).
DISCUSSION
This is the first prospective study to compare HSCT from different donortypes in well-defined cohorts of children with high-risk ALL by using astandardized transplantation and prophylaxis protocol. All patients re-ceived comparable risk-stratified chemotherapy before HSCT and wereselected for HSCT according to prognostically relevant leukemia pheno-types and response to induction chemotherapy or according to time and
EFS
Time (years)
1.0
0.8
0.6
0.4
0.2
BA
0 42 6 8 1031 5 7 9
OS
Time (years)
1.0
0.8
0.6
0.4
0.2
0 42 6 8 1031 5 7 9
RI
Time (years)
1.0
0.8
0.6
0.4
0.2
DC
0 42 6 8 1031 5 7 9
NRM
Time (years)
1.0
0.8
0.6
0.4
0.2
0 42 6 8 1031 5 7 9
Patients Events 4-yr. EFS P*MSD 49 19 0.62±0.07 .938MUD 153 56 0.62±0.04
Difference in 4-year EFS 0%Upper limit of one-sided 95% CI 15%
Patients Events 4-yr. OS P*MSD 49 11 0.78±0.06 .174MUD 153 49 0.67±0.04
Patients Events 4-yr. CI P*MSD 49 15 0.32±0.07 .644MUD 153 40 0.28±0.04
Patients Events 4-yr. CI P*MSD 49 1 0.02±0.02 .062MUD 153 15 0.10±0.02
Fig 5. Outcomes for patients transplanted in second or third complete remissions. (A) Event-free survival (EFS), (B) overall survival (OS), (C) relapse incidence (RI),and (D) nonrelapse mortality (NRM). MSD, HLA-matched sibling donor; MUD, HLA-matched unrelated donor. (*) Based on pseudovalues at 4 years.
Comparison of Sibling and Unrelated Donors for Pediatric ALL
www.jco.org © 2015 by American Society of Clinical Oncology 7
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.

site of relapse. Donor selections were determined according to the avail-ability of suitable siblings, which produced biologically randomized treat-ment groups. The close cooperation and compliance of study centers, theprospectiveevaluation,andqualityassurancefromregularpatientconfer-ences about complications led to noticeable treatment improvementscompared with those of some previous retrospective studies.27-29 More-over, multicenter cooperation allowed stringent alignment of selectioncriteria for allogeneic HSCT according to predictions of contemporarychemotherapy outcomes. Patients with a long-term survival prognosis ofless than 50% after validated chemotherapy were selected for HSCT. Incontrast with previous trials, these criteria were defined in first-line pro-tocols and did not differ for MSD or MUD indications. Specifically,known risk factors, such as phenotype, response to prednisone, age atdiagnosis, relapse, duration of first remission, and site of relapse,were defined in the indication for allogeneic HSCT. For patientswith CR1 and second CR (CR2) HSCT indications, the minimalresidual disease level at 4 and 12 weeks after initial treatmentbecame a major selection criteria.10,12,30
EFS and OS of patients in the MUD group were superior to thosein previously published data from children with high-risk ALL whowere treated with MUD transplantations,31,32 and the quality of HLAtyping and the degree of matching may have played an important role.
When this study was designed, it was still common practice to useunrelated donors with 7/8 HLA matches, as determined by medium-resolution typing. However, the drawback of this procedure has beena high rate of transplantation-associated complications, especiallyaGVHD and cGVHD, which particularly affects the growing organs ofchildren. Petersdorf et al33 and Flomenberg et al34 demonstrated strik-ing prognostic efficacy of high-resolution typing and, consequently,only donors with 9/10 or 10/10 HLA matches (four digits per allele)were used in this study. MUDs were identified for more than 70% ofpatients who lacked MSDs, and the search for donors did not delayHSCT. Moreover, no differences in outcomes were identified betweenpatients receiving transplantations from 9/10 or 10/10 matches.
Among patients with MUD transplantations, no differences inOS were observed between recipients of BM or PBSC, probably re-flecting the protective effect of intensive GVHD prophylaxis withcyclosporine, methotrexate, and ATG Fresenius.35,36 Furthermore, nosignificant differences in outcomes were observed between patientswith various degrees of aGVHD or cGVHD. These data demonstratethat long-term relapse-free survival after MUD-HSCT can beachieved without a high incidence of cGVHD, which is a devastatingdisease for children and adolescents.37,38
Despite excellent outcomes of MUD-HSCT, our data indicate thatMSD BM transplantation remains superior, which is possibly a result offaster engraftment and more rapid immune reconstitution resulting infewer severe infections. We speculate that this is influenced by the shortand limited GVHD prophylaxis in this setting. This investigator-initiated,multicenter studyhas limitations.Becauseonly10%ofchildrenwithALLqualifyforanallogeneicHSCT,therecruitmentdurationwasmorethan7years. Although no striking differences in supportive care were observed,
some new techniques developed over time and possibly influenced thetreatment intensity of aGVHD and cGVHD; extracorporeal photophere-sis and mesenchymal stem-cell infusion were increasingly used to reducepharmacologic immunosuppression. One of the most important tools isthe evaluation of minimal residual disease before and after HSCT. Theresultsof this investigationinourstudygroupwererecentlyreported,andadditional analyses are under way.39,39a
The risk of secondary malignancies is a major concern,40-42 and ourdata demonstrate this risk with nine secondary malignancies in patientswho received TBI, with the expectation of more with longer follow-up.The long-term effects of TBI in children and adolescents also includeorgandysfunction,growthretardation,andhormonalinsufficiencies.43-45
Thus, future studies are required to develop effective alternatives to TBI.In conclusion, our data demonstrate excellent EFS and OS, and low
incidence of relapse in children with high-risk ALL after treatment withTBI and etoposide before allogeneic HSCT from HLA-matched siblingsor well-matched unrelated donors. This large, prospective, multicentertrial suggests that MUD-HSCT could be a standard of care for patientswith ALL who have a high risk of relapse and who lack MSDs.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTSOF INTEREST
Disclosures provided by the authors are available with this article atwww.jco.org.
AUTHOR CONTRIBUTIONS
Conception and design: Christina Peters, Martin Schrappe, Arend vonStackelberg, André Schrauder, Peter Bader, Wolfram Ebell, Peter Lang,Johanna Schrum, Bernhard Kremens, Michael H. Albert, Roland Meisel,Susanne Matthes-Martin, Tayfun Gungor, Wolfgang Holter, BrigitteStrahm, Bernd Gruhn, Ansgar Schulz, Wilhelm Woessmann, UlrikePoetschger, Martin Zimmermann, Thomas KlingebielProvision of study materials or patients: Christina Peters, Martin Schrappe,Arend von Stackelberg, André Schrauder, Peter Bader, Wolfram Ebell, PeterLang, Johanna Schrum, Bernhard Kremens, Michael H. Albert, Roland Meisel,Susanne Matthes-Martin, Tayfun Gungor, Wolfgang Holter, Brigitte Strahm,Bernd Gruhn, Ansgar Schulz, Wilhelm Woessmann, Ulrike Poetschger, MartinZimmermann, Thomas KlingebielCollection and assembly of data: Christina Peters, Martin Schrappe, Arend vonStackelberg, André Schrauder, Peter Bader, Wolfram Ebell, Peter Lang, JohannaSchrum, Bernhard Kremens, Michael H. Albert, Roland Meisel, SusanneMatthes Martin, Tayfun Gungor, Wolfgang Holter, Brigitte Strahm, BerndGruhn, Ansgar Schulz, Wilhelm Woessmann, Ulrike Poetschger, MartinZimmermann, Thomas KlingebielData analysis and interpretation: Christina Peters, Martin Schrappe, Arend vonStackelberg, Peter Bader, Peter Lang, Karl-Walter Sykora, Johanna Schrum,Bernhard Kremens, Karoline Ehlert, Michael H. Albert, Roland Meisel, SusanneMatthes-Martin, Tayfun Gungor, Wolfgang Holter, Brigitte Strahm, BerndGruhn, Ansgar Schulz, Wilhelm Woessmann, Ulrike Poetschger, MartinZimmermann, Thomas KlingebielManuscript writing: All authorsFinal approval of manuscript: All authors
REFERENCES
1. Schrappe M, Hunger SP, Pui CH, et al: Out-comes after induction failure in childhood acutelymphoblastic leukemia. N Engl J Med 366:1371-1381, 2012
2. von Stackelberg A, Völzke E, Kühl JS, et al: Out-come of children and adolescents with relapsed acutelymphoblastic leukaemia and non-response to salvageprotocol therapy: A retrospective analysis of the ALL-REZBFM Study Group. Eur J Cancer 47:90-97, 2011
3. Ishaqi MK, Afzal S, Dupuis A, et al: Earlylymphocyte recovery post-allogeneic hematopoietic
stem cell transplantation is associated with signifi-cant graft-versus-leukemia effect without increasein graft-versus-host disease in pediatric acute lym-phoblastic leukemia. Bone Marrow Transplant 41:245-252, 2008
4. Walker T, Milford E, Chell J, et al: The NationalMarrow Donor Program: Improving access to
Peters et al
8 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.

hematopoietic cell transplantation. Clin Transpl2011:55-62, 2011
5. Harvey J, Green A, Cornish J, et al: Improvedsurvival in matched unrelated donor transplant forchildhood ALL since the introduction of high-resolution matching at HLA class I and II. BoneMarrow Transplant 47:1294-1300, 2012
6. Zhang MJ, Davies SM, Camitta BM, et al:Comparison of outcomes after HLA-matched siblingand unrelated donor transplantation for children withhigh-risk acute lymphoblastic leukemia. Biol BloodMarrow Transplant 18:1204-1210, 2012
7. Smith AR, Baker KS, Defor TE, et al: Hema-topoietic cell transplantation for children with acutelymphoblastic leukemia in second complete remis-sion: Similar outcomes in recipients of unrelatedmarrow and umbilical cord blood versus marrowfrom HLA matched sibling donors. Biol Blood Mar-row Transplant 15:1086-1093, 2009
8. Pinkel D: ‘Allogeneic marrow transplantationin children with acute leukemia: A practice whosetime has gone’: twenty years later. Leukemia 23:2189-2196, 2009
9. Hahn T, Wall D, Camitta B, et al: The role ofcytotoxic therapy with hematopoietic stem celltransplantation in the therapy of acute lymphoblasticleukemia in children: An evidence-based review.Biol Blood Marrow Transplant 11:823-861, 2005
10. Conter V, Bartram CR, Valsecchi MG, et al:Molecular response to treatment redefines all prog-nostic factors in children and adolescents with B-cellprecursor acute lymphoblastic leukemia: Results in3184 patients of the AIEOP-BFM ALL 2000 study.Blood 115:3206-3214, 2010
11. Krentz S, Hof J, Mendioroz A, et al: Prognosticvalue of genetic alterations in children with first bonemarrow relapse of childhood B-cell precursor acute lym-phoblastic leukemia. Leukemia 27:295-304, 2013
12. Pulsipher MA, Peters C, Pui CH: High-riskpediatric acute lymphoblastic leukemia: To trans-plant or not to transplant? Biol Blood Marrow Trans-plant 17:S137-S148, 2011
13. Mann G, Attarbaschi A, Schrappe M, et al: Im-proved outcome with hematopoietic stem cell transplan-tation in a poor prognostic subgroup of infants withmixed-lineage-leukemia (MLL)-rearranged acute lympho-blastic leukemia: Results from the Interfant-99 Study.Blood 116:2644-2650, 2010
14. Dopfer R, Henze G, Bender-Götze C, et al: Alloge-neic bone marrow transplantation for childhood acutelymphoblastic leukemia in second remission afterintensive primary and relapse therapy according to theBFM- and CoALL-protocols: Results of the German Co-operative Study. Blood 78:2780-2784, 1991
15. Matthes-Martin S, Lion T, Aberle SW, et al:Pre-emptive treatment of CMV DNAemia in paedi-atric stem cell transplantation: The impact of recipi-ent and donor CMV serostatus on the incidence ofCMV disease and CMV-related mortality. Bone Mar-row Transplant 31:803-808, 2003
16. Locatelli F, Zecca M, Rondelli R, et al: Graftversus host disease prophylaxis with low-dosecyclosporine-A reduces the risk of relapse in chil-dren with acute leukemia given HLA-identical siblingbone marrow transplantation: Results of a random-ized trial. Blood 95:1572-1579, 2000
17. Möricke A, Zimmermann M, Reiter A, et al:Long-term results of five consecutive trials in child-hood acute lymphoblastic leukemia performed bythe ALL-BFM study group from 1981 to 2000.Leukemia 24:265-284, 2010
18. Tallen G, Ratei R, Mann G, et al: Long-termoutcome in children with relapsed acute lympho-blastic leukemia after time-point and site-of-relapsestratification and intensified short-course multidrugchemotherapy: Results of trial ALL-REZ BFM 90.J Clin Oncol 28:2339-2347, 2010
19. Schrauder A, von Stackelberg A, Schrappe M,et al: Allogeneic hematopoietic SCT in children withALL: Current concepts of ongoing prospective SCTtrials. Bone Marrow Transplant 41:S71-S74, 2008
20. Eapen M, Horowitz MM, Klein JP, et al:Higher mortality after allogeneic peripheral-bloodtransplantation compared with bone marrow in chil-dren and adolescents: The Histocompatibility andAlternate Stem Cell Source Working Committee ofthe International Bone Marrow Transplant Registry.J Clin Oncol 22:4872-4880, 2004
21. Peters C, Cornish JM, Parikh SH, et al: Stemcell source and outcome after hematopoietic stemcell transplantation (HSCT) in children and adoles-cents with acute leukemia. Pediatr Clin North Am57:27-46, 2010
22. Shimoni A, Bielorai B, Toren A, et al: Intravenousbusulfan-based conditioning prior to allogeneic hemato-poietic stem cell transplantation: Myeloablation with re-duced toxicity. Exp Hematol 31:428-434, 2003
23. Altman DG, Machin D, Bryant TN, et al: Sta-tistics With Confidence: Confidence Intervals andStatistical Guidelines (ed 2). London, United King-dom, BMJ Books
24. Prentice RL, Kalbfleisch JD, Peterson AV Jr,et al: The analysis of failure times in the presence ofcompeting risks. Biometrics 34:541-554, 1978
25. Gray RJ: A class of K-sample tests for com-paring the cumulative incidence of a competing risk.Ann Stat 16:1141-1154, 1988
26. Andersen PK, Perme MP: Pseudo-observations insurvival analysis. Stat Methods Med Res 19:71-99, 2010
27. Dini G, Zecca M, Balduzzi A, et al: No differ-ence in outcome between children and adolescentstransplanted for acute lymphoblastic leukemia insecond remission. Blood 118:6683-6690, 2011
28. Shaw PJ, Kan F, Woo Ahn K, et al: Outcomesof pediatric bone marrow transplantation for leuke-mia and myelodysplasia using matched sibling, mis-matched related, or matched unrelated donors.Blood 116:4007-4015, 2010
29. Tracey J, Zhang MJ, Thiel E, et al: Transplantationconditioning regimens and outcomes after allogeneichematopoietic cell transplantation in children and adoles-cents with acute lymphoblastic leukemia. Biol BloodMarrow Transplant 19:255-259, 2013
30. Eckert C, von Stackelberg A, Seeger K, et al:Minimal residual disease after induction is the stron-gest predictor of prognosis in intermediate riskrelapsed acute lymphoblastic leukaemia: Long-termresults of trial ALL-REZ BFM P95/96. Eur J Cancer49:1346-1355, 2013
31. Davies SM, Wang D, Wang T, et al: Recentdecrease in acute graft-versus-host disease in chil-dren with leukemia receiving unrelated donor bonemarrow transplants. Biol Blood Marrow Transplant15:360-366, 2009
32. Mateos MK, O’Brien TA, Oswald C, et al:Transplant-related mortality following allogeneic he-matopoietic stem cell transplantation for pediatricacute lymphoblastic leukemia: 25-year retrospectivereview. Pediatr Blood Cancer 60:1520-1527, 2013
33. Petersdorf EW, Hansen JA, Martin PJ, et al:Major-histocompatibility-complex class I alleles and anti-
gens in hematopoietic-cell transplantation. N Engl J Med345:1794-1800, 2001
34. Flomenberg N, Baxter-Lowe LA, Confer D, etal: Impact of HLA class I and class II high-resolutionmatching on outcomes of unrelated donor bonemarrow transplantation: HLA-C mismatching is as-sociated with a strong adverse effect on transplan-tation outcome. Blood 104:1923-1930, 2004
35. Veys P, Wynn RF, Ahn KW, et al: Impact ofimmune modulation with in vivo T-cell depletion andmyeloablative total body irradiation conditioning onoutcomes after unrelated donor transplantation forchildhood acute lymphoblastic leukemia. Blood 119:6155-6161, 2012
36. MacMillan ML, Davies SM, Nelson GO, et al:Twenty years of unrelated donor bone marrowtransplantation for pediatric acute leukemia facili-tated by the National Marrow Donor Program. BiolBlood Marrow Transplant 14:16-22, 2008
37. Remberger M, Mattsson J, Hentschke P, etal: The graft-versus-leukaemia effect in haematopoi-etic stem cell transplantation using unrelated do-nors. Bone Marrow Transplant 30:761-768, 2002
38. Gassas A, Sung L, Saunders EF, et al: Graft-versus-leukemia effect in hematopoietic stem celltransplantation for pediatric acute lymphoblastic leu-kemia: Significantly lower relapse rate in unrelatedtransplantations. Bone Marrow Transplant 40:951-955, 2007
39. Eckert C, Henze G, Seeger K, et al: Use ofallogeneic hematopoietic stem-cell transplantationbased on minimal residual disease response im-proves outcomes for children with relapsed acutelymphoblastic leukemia in the intermediate-riskgroup. J Clin Oncol 31:2736-2742, 2013
39a. Bader P, Kreyenberg H, von Stackelberg A,et al: Monitoring of minimal residual disease afterallogeneic stem-cell transplantation in relapsedchildhood acute lymphoblastic leukemia allows forthe identification of impending relapse: Results ofthe ALL-BFM-SCT 2003 trial. J Clin Oncol doi:10.1200/JCO.2014.58.4631
40. Baker KS, Ness KK, Weisdorf D, et al: Lateeffects in survivors of acute leukemia treated withhematopoietic cell transplantation: A report from theBone Marrow Transplant Survivor Study. Leukemia24:2039-2047, 2010
41. Rizzo JD, Curtis RE, Socié G, et al: Solidcancers after allogeneic hematopoietic cell trans-plantation. Blood 113:1175-1183, 2009
42. Socié G, Baker KS, Bhatia S: Subsequentmalignant neoplasms after hematopoietic cell trans-plantation. Biol Blood Marrow Transplant 18:S139-S150, 2012
43. Felicetti F, Manicone R, Corrias A, et al: Endocrinelate effects after total body irradiation in patients whoreceived hematopoietic cell transplantation during child-hood: A retrospective study from a single institution. JCancer Res Clin Oncol 137:1343-1348, 2011
44. Ricardi U, Filippi AR, Biasin E, et al: Latetoxicity in children undergoing hematopoietic stemcell transplantation with TBI-containing conditioningregimens for hematological malignancies. Strahlen-ther Onkol 185:17-20, 2009
45. Bailey HK, Kappy MS, Giller RH, et al: Time-courseand risk factors of hypothyroidism following allogeneichematopoietic stem cell transplantation (HSCT) in chil-dren conditioned with fractionated total body irradiation.Pediatr Blood Cancer 51:405-409, 2008
Comparison of Sibling and Unrelated Donors for Pediatric ALL
www.jco.org © 2015 by American Society of Clinical Oncology 9
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
Affiliations
Christina Peters, Susanne Matthes-Martin, and Ulrike Poetschger, St Anna Children’s Hospital, Vienna, Austria; Martin Schrappe,University Medical Center Schleswig-Holstein and Christian-Albrechts-University Kiel; André Schrauder, Kinderarztpraxis am Aalborgring,Kiel; Arend von Stackelberg and Wolfram Ebell, Charité–Children’s Hospital Berlin, Berlin; Peter Bader and Thomas Klingebiel, JohannWolfgang Goethe University, Frankfurt; Peter Lang, University Hospital Tübingen, Tübingen; Karl-Walter Sykora and Martin Zimmerman,Hannover Medical School, Hannover; Johanna Schrum, University Medical Center Hamburg-Eppendorf, Hamburg; Bernhard Kremens,University Hospital Essen, Essen; Karoline Ehlert, University Clinic Greifswald, Greifswald; Michael H. Albert, Dr. von Hauner UniversityChildren’s Hospital, München; Roland Meisel, University Hospital Düsseldorf, Düsseldorf; Wolfgang Holter, Children’s University HospitalErlangen, Erlangen; Brigitte Strahm, University Hospital Freiburg, Freiburg; Bernd Gruhn, University Hospital Jena, Jena; Ansgar Schulz,University Hospital Ulm, Ulm; Wilhelm Woessmann, University Clinic Giessen, Giessen, Germany; and Tayfun Gungor, UniversityChildren’s Hospital Zürich, Zürich, Switzerland.
■ ■ ■
Peters et al
10 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Stem-Cell Transplantation in Children With Acute Lymphoblastic Leukemia: A Prospective International Multicenter Trial Comparing SiblingDonors With Matched Unrelated Donors—The ALL-SCT-BFM-2003 Trial
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships areself-held unless noted. I � Immediate Family Member, Inst � My Institution. Relationships may not relate to the subject matter of this manuscript. For moreinformation about ASCO’s conflict of interest policy, please refer to www.asco.org/rwc or jco.ascopubs.org/site/ifc.
Christina PetersHonoraria: EUSA Pharma, Medac PharmaConsulting or Advisory Role: Medac Pharma, EUSA Pharma, PfizerSpeakers’ Bureau: Amgen, Novartis, Medac Pharma, Fresenius BiotechResearch Funding: Amgen (Inst), Fresenius Biotech (Inst), Genzyme(Inst), Medac (Inst), RIEMSER Pharma (Inst)Travel, Accommodations, Expenses: Pierre Fabre
Martin SchrappeNo relationship to disclose
Arend von StackelbergHonoraria: AmgenConsulting or Advisory Role: Amgen (Inst)Research Funding: EUSA Pharma (Inst)
André SchrauderNo relationship to disclose
Peter BaderTravel, Accommodations, Expenses: Medac Pharma, Novartis
Wolfram EbellNo relationship to disclose
Peter LangNo relationship to disclose
Karl-Walter SykoraTravel, Accommodations, Expenses: Medac Pharma
Johanna SchrumNo relationship to disclose
Bernhard KremensNo relationship to disclose
Karoline EhlertNo relationship to disclose
Michael H. AlbertStock or Other Ownership: Amgen, Biogen IdecTravel, Accommodations, Expenses: Neovii Biotech, Astellas Pharma
Roland MeiselNo relationship to disclose
Susanne Matthes-MartinNo relationship to disclose
Tayfun GungorNo relationship to disclose
Wolfgang HolterNo relationship to disclose
Brigitte StrahmNo relationship to disclose
Bernd GruhnConsulting or Advisory Role: Amgen, EUSA PharmaTravel, Accommodations, Expenses: EUSA Pharma, Neovii Biotech
Ansgar SchulzNo relationship to disclose
Wilhelm WoessmannNo relationship to disclose
Ulrike PoetschgerNo relationship to disclose
Martin ZimmermannNo relationship to disclose
Thomas KlingebielExpert Testimony: NovartisTravel, Accommodations, Expenses: EUSA Pharma, Medac Pharma
Comparison of Sibling and Unrelated Donors for Pediatric ALL
www.jco.org © 2015 by American Society of Clinical Oncology
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.

Acknowledgment
Presented in part at the 52nd Annual Meeting of the American Society of Hematology, Orlando, FL, December 4-7, 2010; at the 7th BiannualChildhood Leukemia Symposium, Antalya, Turkey, October 4-6, 2010; and at the International European Society for Blood and Marrow
Transplantation Annual Meeting, Geneva, Switzerland, April 1-4, 2012.
Peters et al
© 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Zurich) on March 27, 2015 from 130.60.58.2Information downloaded from jco.ascopubs.org and provided by at SWISS CONSORTIUM (Hauptbibliothek Universitat
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.