Late Diagnosis of Breast Cancer and Associated Factors ...
18
Page 1/18 Late Diagnosis of Breast Cancer and Associated Factors Among Women Attending Hawassa University Comprehensive and Specialized Hospital Southern Ethiopia Mesay Yoseph ( [email protected] ) Hawassa University Achamyelesh Gebresadik Hawassa University Akalewold Alemayehu Hawassa University Research Article Keywords: Late breast cancer diagnosis, breast cancer, Hawassa University Specialized Hospital Posted Date: September 24th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-832493/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Late Diagnosis of Breast Cancer and Associated Factors ...
Page 1/18
Late Diagnosis of Breast Cancer and AssociatedFactors Among Women Attending HawassaUniversity Comprehensive and Specialized HospitalSouthern EthiopiaMesay Yoseph ( [email protected] )
Hawassa UniversityAchamyelesh Gebresadik
Hawassa UniversityAkalewold Alemayehu
Hawassa University
Research Article
Keywords: Late breast cancer diagnosis, breast cancer, Hawassa University Specialized Hospital
Posted Date: September 24th, 2021
DOI: https://doi.org/10.21203/rs.3.rs-832493/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License

Page 2/18
AbstractBackground; Breast cancer is a signi�cant public health issue in sub-Saharan Africa and the secondcommonest cancer overall. In Ethiopia, most women present at the late-stage presentation. This isbecause Ethiopian government gives less attention, and is not well-studied as well. Therefore, it isimportant to assess delays in diagnosis and treating breast cancer that has been associated with a moreadvanced stage of the disease and a decrease in patient survival rates.
Objective: To assess the magnitude and associated factors for late diagnosis of breast cancer amongwomen attending Hawassa University Comprehensive Specialized Hospital in Southern Ethiopia.
Methodology: A facility-based cross-sectional study was conducted from December to January 2019.Data were collected from 261 consecutively selected clients based on the arrival of their hospital visit byusing a pretested structured questionnaire and checklist. Physicians performed physical examinationsand diagnoses. Data was checked for completeness and consistency, and entered into epi data, thenexported to SPSS for analysis. Descriptive, Bivariate, and multivariable logistic regression analyses wereperformed using SPSS Version 25 Statistical Software.
Results: The magnitude of late diagnosis of breast cancer was 86.3%. The woman who had no initialadvice for breast biopsy [AOR=5.1, 95% (CI=1.4-18.9)], not sharing the problem to others [AOR=4.7, 95%(CI=1.8-12.2)] and using traditional and faith healers as a �rst treatment choice [AOR=3.3, 95% (CI=1.2 -8.8)] were associated with late diagnosis of breast cancer.
Conclusions: The majority of women having breast cancer were diagnosed at a late stage. It needsattention to provide better options of the modern health service, and providing accessible initial advice forbreast biopsy, and creating awareness about the bene�t of sharing problems with family to improve thehealth of mothers by early diagnosing and managing the breast cancer.
BackgroundBreast cancer incidence is rapidly growing in both developed and developing regions [1]. It is typicallydetected either during a screening examination, before symptoms have developed, or after a womannotices a lump [2]. Delays in cancer care are common in low-income countries, resulting in greatermorbidity, higher costs of care, a lower likelihood of survival, and disability from cancer [3].
Each year, more than 14 million people are diagnosed with cancer, the majority of whom live in low- andmiddle-income countries (LMICs) [4]. In 2015, 8.8 million died from cancer, representing one in six deathsglobally [5]. Approximately two-thirds of worldwide cancer deaths are in developing countries, where casefatality rates are higher due to late-stage diagnoses, less accessible diagnostic and treatments services[4].
Page 3/18
Breast cancer is the most common female malignancy in most African countries, being cancer with the�rst or second highest incidence and/or mortality [6]. According to the Global Action Plan for thePrevention and Control of Non-communicable Diseases (GLOBOCAN), breast cancer causes 269,000deaths in Africa. The deaths number could have risen above this if there was complete cancerregistration. The number of death from breast cancer in Africa is estimated to be double by the year 2050[4]. In sub-Saharan Africa (SSA), breast cancer survival rates are poor, diagnosis of cancer at earlierstages could prevent deaths [7].
In Ethiopia, breast cancer is the �rst frequent cancer next is cervical cancer. It is estimated that about tenthousands Ethiopian women have breast cancer with thousands of more cases unreported as womenliving in rural areas often seek treatment from traditional healers before seeking help from thegovernment health system [6, 8]. The incidence of breast cancer in Ethiopia was 30.2%, among these latediagnoses was 85% [9]. However, Ethiopia has an increasingly comprehensive set of breast cancerprevention, diagnosis, and treatment interventions available for women [10]. However, these services arelimited to certain comprehensive tertiary hospital which are very far for the most residents. Moreover,these services are mostly ineffective, and have system-related barriers. It is further worsened by thewomen’s attitudes, and lack of awareness of breast cancers symptoms also account for a slowed-downinitiation of action [13].
The magnitude of late diagnosis of breast cancer, and its determinant factors are not well studied in thearea. Therefore, conducting this study was found to be very important. This can be helpful for publichealth o�cials, clinicians, and health planners to do interventions to reduce the impacts of late diagnosisof breast cancer.
Methods
Study setting and study population The study was carried out in Hawassa University Comprehensive Specialized Hospital, Sidama region.The study area is located 275 km south of Addis Ababa, the capital of Ethiopia. It is expected to servemore than 18 million people of the Sidama, Southern region and the surrounding Oromia zones. Thehospital provides surgical and chemotherapy treatment service for breast cancer patients including thepathologic diagnostic services. The oncology unit of the hospital provides for more than 2000 clients peryear. Among these, about 600 breast cancer were diagnosed in last year, 2018.
Study design, and study populationFacility-based cross-sectional study design with quantitative data was carried out in Hawassa UniversityComprehensive Specialized Hospital, Sidama Region, Ethiopia. The study population was all women whodiagnosed for breast cancer and arrive consecutively from December to January, 2019.

Page 4/18
Eligibility CriteriaInclusion criteria: All women diagnosed with breast cancer either newly diagnosed or on follow-up wereincluded in the study.
Exclusion criteria: Those patients who had cancer from another site and disseminated to the breast,critically ill patient and patients with mental problem were excluded from study.
Sample size and sampling proceduresThe sample size (n) was calculated by using the single population proportion formula. From the similarstudy from Tikur Ambessa Specialized Hospital, Addis Ababa, the proportion of late diagnosis of breastcancer (p) was 88.89% [12]. 95% Con�dence interval (CI) (1.96), 4% margin of error (d), and adding 10%contingency was assumed.
Final sample size was (237 + 23.7) = 260.7 ≈ 261
In this study, 261 women with breast cancer were selected consecutively based on their arrival to thehospital during the study period.
Data collection tools, and proceduresData were collected by face-to-face interviews by using a pre-tested questionnaire. A clinical data of thepatient like; stage of diagnosis, methods, treatment planned and type of diagnoses were collected byusing a pre-tested checklist (from the medical records after physicians performed diagnoses). Thequestionnaire was developed by the investigators after reviewing different related literature. Thequestionnaire was �rst prepared in English, and then appropriately translated into the Amharic language.The component of the questionnaire was introductory, demographic information, socio- economicinformation, information on reasons for delay, patient’s history on diagnostic procedures, patient’s historyon help seeking, health awareness and behavioral factors of the patients. The interviews were conductedin outpatient and inpatient departments of oncology unit in the hospital. Four pre-trained nurses collecteddata under the strict supervision of principal investigator.
Data Analysis

Page 5/18
After data collection, each questionnaire was again visually checked for completeness, clarity, andaccuracy. The data were coded and entered into EPI INFO version 7, exported into the SPSS version 25Software. Descriptive, bivariate, and multivariable logistic regression analyses were performed. Selectedvariables that have a P-value of ≤0.2 at the bivariate analysis were included in the multivariable logisticregression to control all possible confounding factors simultaneously. The goodness of �t was assessedby using the Hosmer and Lemeshow goodness test. Generally, a P-value ≤ 0.05 was consideredstatistically signi�cant.
Operational de�nitionsLate diagnosis; patients diagnosed with breast cancer stage III and stage IV on their �rst diagnosis in lastsix month [2].
Early diagnosis; patients diagnosed with breast cancer stage 0, Stage I andStage II
Cancer staging; is important in diagnosis in order to give appropriate management.
Breast cancer staging based on TNM classi�cation, T stands for tumor size N for lymph nodeinvolvement depending on methods (2)
Patient delay: The period from a patient �rst becoming aware of symptoms until their �rst presentation toa health care provider (HCP). The duration of more than 60 days de�ned as “long patient delay” and 60days or less de�ned as short patient delay” [15].
Alternative therapy: Complementary alternative therapy was de�ned as any therapy using methods andproducts not included in conventional modern medicine (traditional medicine, and traditional andreligious practices [16].
Results
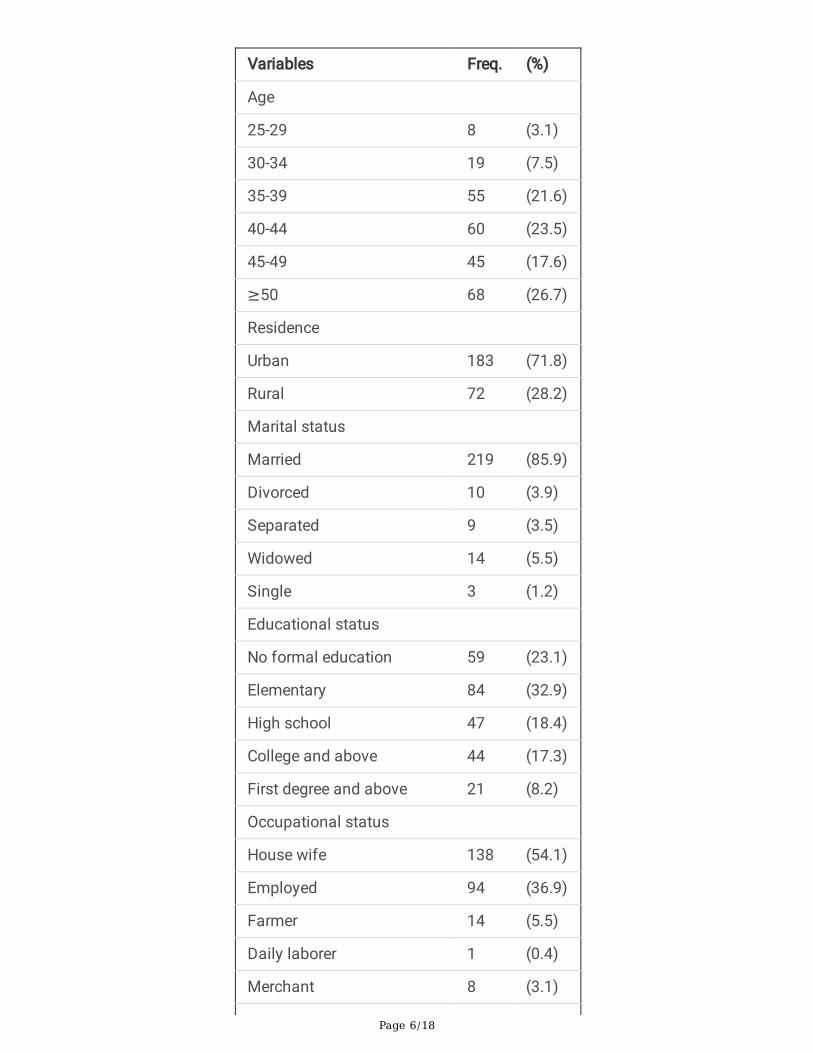
Socio-demographic characteristics A total of 255 woman who diagnosed for breast cancer participated with a response rate of 97.70%.Majority of the respondents 219 (85.9%) were married and 183 (71.8%) were urban dwellers. Fifty-nine(23.1%) had no formal education. Nearly half 138 (54.1%) of the participants were house wives and 94(36.9%) were employed (involved in government employee, private employee and private business). Theaverage of parity (±Standard Deviation) was 3.3 (±2.03), and majority 215 (84.3%) of the women weremulti-para. Sixty women (23.5%) earned below average household monthly income, (below 1050 ETB)(Table 1).
Table 1: Socio demographic characters of woman who diagnosed for breast cancer among who visitoncology department in HUCRCH in Hawassa city, Southern Ethiopia, 2020.
Page 6/18
Variables Freq. (%)
Age
25-29 8 (3.1)
30-34 19 (7.5)
35-39 55 (21.6)
40-44 60 (23.5)
45-49 45 (17.6)
≥50 68 (26.7)
Residence
Urban 183 (71.8)
Rural 72 (28.2)
Marital status
Married 219 (85.9)
Divorced 10 (3.9)
Separated 9 (3.5)
Widowed 14 (5.5)
Single 3 (1.2)
Educational status
No formal education 59 (23.1)
Elementary 84 (32.9)
High school 47 (18.4)
College and above 44 (17.3)
First degree and above 21 (8.2)
Occupational status
House wife 138 (54.1)
Employed 94 (36.9)
Farmer 14 (5.5)
Daily laborer 1 (0.4)
Merchant 8 (3.1)
Page 7/18
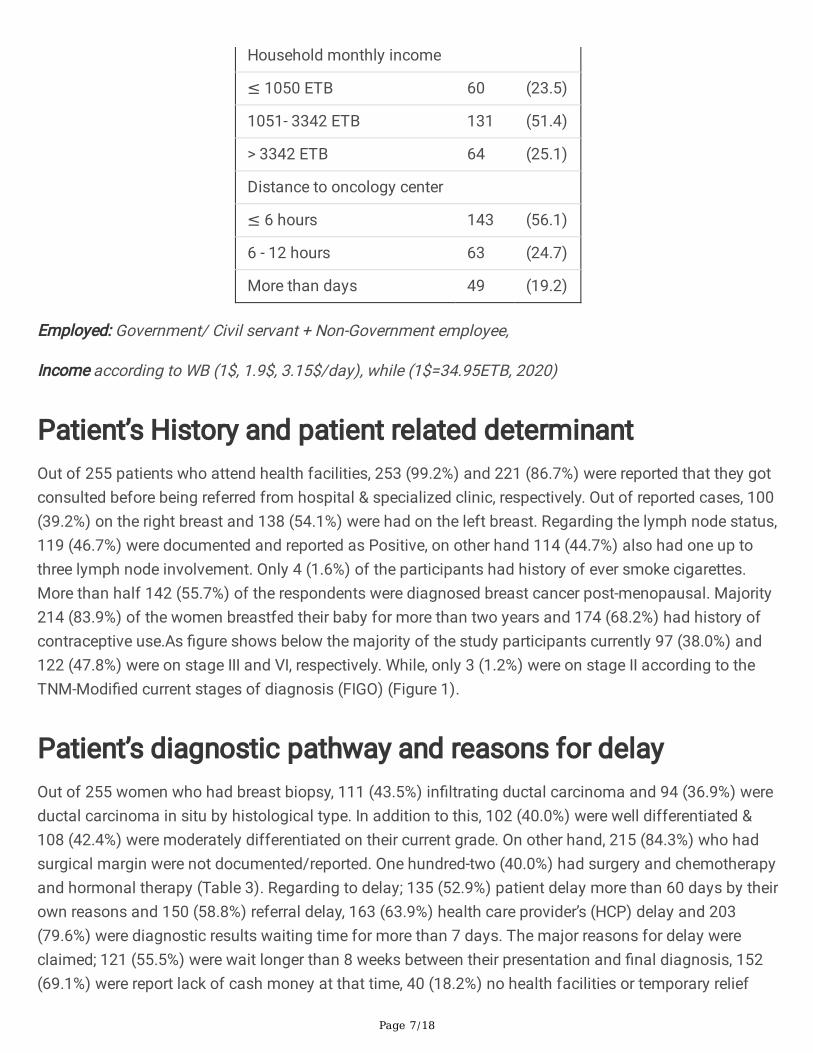
Household monthly income
≤ 1050 ETB 60 (23.5)
1051- 3342 ETB 131 (51.4)
> 3342 ETB 64 (25.1)
Distance to oncology center
≤ 6 hours 143 (56.1)
6 - 12 hours 63 (24.7)
More than days 49 (19.2)
Employed: Government/ Civil servant + Non-Government employee,
Income according to WB (1$, 1.9$, 3.15$/day), while (1$=34.95ETB, 2020)
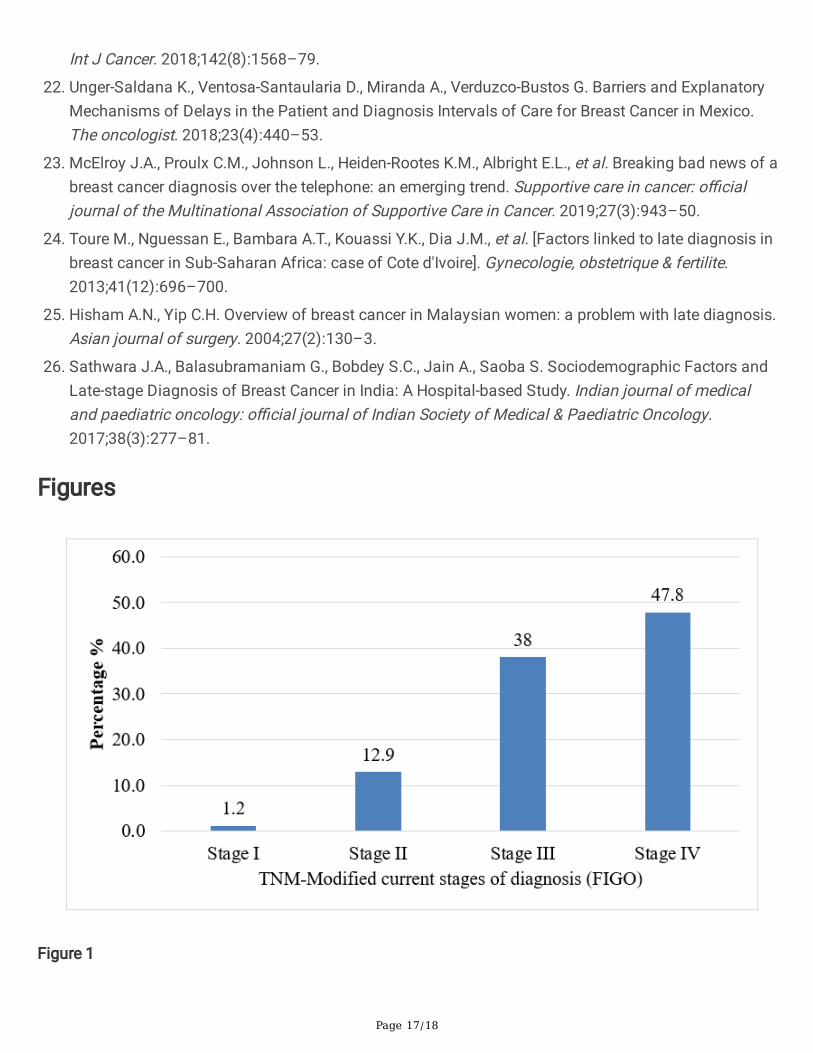
Patient’s History and patient related determinantOut of 255 patients who attend health facilities, 253 (99.2%) and 221 (86.7%) were reported that they gotconsulted before being referred from hospital & specialized clinic, respectively. Out of reported cases, 100(39.2%) on the right breast and 138 (54.1%) were had on the left breast. Regarding the lymph node status,119 (46.7%) were documented and reported as Positive, on other hand 114 (44.7%) also had one up tothree lymph node involvement. Only 4 (1.6%) of the participants had history of ever smoke cigarettes.More than half 142 (55.7%) of the respondents were diagnosed breast cancer post-menopausal. Majority214 (83.9%) of the women breastfed their baby for more than two years and 174 (68.2%) had history ofcontraceptive use.As �gure shows below the majority of the study participants currently 97 (38.0%) and122 (47.8%) were on stage III and VI, respectively. While, only 3 (1.2%) were on stage II according to theTNM-Modi�ed current stages of diagnosis (FIGO) (Figure 1).
Patient’s diagnostic pathway and reasons for delayOut of 255 women who had breast biopsy, 111 (43.5%) in�ltrating ductal carcinoma and 94 (36.9%) wereductal carcinoma in situ by histological type. In addition to this, 102 (40.0%) were well differentiated &108 (42.4%) were moderately differentiated on their current grade. On other hand, 215 (84.3%) who hadsurgical margin were not documented/reported. One hundred-two (40.0%) had surgery and chemotherapyand hormonal therapy (Table 3). Regarding to delay; 135 (52.9%) patient delay more than 60 days by theirown reasons and 150 (58.8%) referral delay, 163 (63.9%) health care provider’s (HCP) delay and 203(79.6%) were diagnostic results waiting time for more than 7 days. The major reasons for delay wereclaimed; 121 (55.5%) were wait longer than 8 weeks between their presentation and �nal diagnosis, 152(69.1%) were report lack of cash money at that time, 40 (18.2%) no health facilities or temporary relief
Page 8/18
from itself and 16 (7.3%) perceived that the cancer had no cure. On other hand regarding to the healthfacility, 179 (81.4%), 143 (65.0%) and 124 (56.4%) were complains that they delay due to the waiting timein the reception, waiting time to see a doctor and no appropriate physician, respectively (Table 2).
Table 2: Reasons for delay among the woman who diagnosed for breast cancer among who visitoncology department in HUCRCH in Hawassa city, Southern Ethiopia, 2020. (n=220)

Page 9/18
Variables Freq. (%)
Above 8wks lag b/n presentation & Dx
Yes 121 (55.5)
No 97 (44.5)
The reasons for late presentation
Lack of cash money at that time 152 (69.1)
No health facilities 16 (7.3)
Thinking that cancer was not be cured 40 (18.2)
Temporary relief by the lesion itself 12 (5.5)
Waiting time in the reception
Yes 179 (81.4)
No 41 (18.6)
Waiting time to see a doctor
Yes 143 (65.0)
No 77 (35.0)
Lack of appropriate attention
Yes 124 (56.4)
No 96 (43.6)
Being busy
Yes 132 (60.0)
No 88 (40.0)
Patient delay
≤ 60 days 120 (47.1%)
> 60 days 135 (52.9%)
Health care provider’s (HCP) delay
≤7 days 92 (36.1%)
>7 days 163 (63.9%)
Referral delay
≤7 days 105 (41.2%)
Page 10/18
>7 days 150 (58.8%)
Diagnostic waiting time
≤7 days 63 (24.7%)
>7 days 192 (75.3%)
The Prevalence of Late Diagnosis of Breast CancerThe prevalence of late diagnosis of breast cancer among woman was 220 (86.3%) [95% CI: 81.7–90.1], atvisit oncology department at HUCRCH (Figure 2).
Factors associated with late diagnosis of breast cancerIn the bivariable logistic regression model, the analysis factors that had an association with latediagnosis of breast cancer were; advice for breast biopsy, residence, educational status, ever heard aboutmammography test, immediately share the problem to others, family history of cancer, menopausalstatus, and using traditional and faith healers as �rst choice. In the multivariate logistic regressionanalysis model; having no initial advice for breast biopsy, not sharing one’s problem immediately toothers, and using traditional healers or/and faith healers as �rst choice of treatments were signi�cantlyassociated with late diagnosis of breast cancer.
Accordingly, the woman who had no initial advice for breast biopsy were 5 times more likely diagnosed atlate stage [AOR=5.1, 95% (CI=1.4-18.9)] as compared with who had initial advised for breast biopsy. Thewomen who did not share their problem immediately to others were 4.7 times more likely diagnosed atlate stage with [AOR=4.7, 95% (CI=1.8-12.2)] as compared with who could share their problem with theirfamily, husband and others. The study participants who use traditional and faith healers as �rst choicewere also about three time more likely diagnosed at late stage [AOR=3.3, 95% (CI=1.2- 8.8)] as comparedwith their counterparts (Table 3)
Table 3: Bivariable and multivariable logistic regression analysis late diagnosis of breast cancer amongwoman at HUCSH in Hawassa city, Southern Ethiopia, 2020.

Page 11/18
Late diagnosis of BCa
Yes No
Freq. (%) Freq. (%) COR (95%CI) AOR (95%CI) P-Value
Advice for breast biopsy
No 8 (57.1) 6 (42.9) 1 1
Yes 212 (88.0) 29 (12.0) 5.48(1.78,16.93)
5.13(1.39,18.90)
0.014*
Residence
Urban 153 (83.6) 30 (16.4) 1 1
Rural 67 (93.1) 5 (6.9) 2.63(0.98,7.07)
2.17(0.74,6.43)
0.160
Educational status
No formal education 53 (89.8) 6 (10.2) 2.04(0.77,5.37)
1.42(0.38,5.29)
0.601
Elementary 76 (90.5) 8 (9.5) 2.19(0.92,5.23)
1.44(0.40,5.21)
0.578
High school andabove
91 (81.3) 21 (18.8) 1 1
Ever heard about mammography test
Yes 63 (79.7) 16 (20.3) 1 1
No 157 (89.2) 19 (10.8) 2.10(1.02,4.34)
2.02(0.83,4.90)
0.122
Immediately share the problem to others
Yes 115 (81.0) 27 (19.0) 1 1
No 105 (92.9) 8 (7.1) 3.08(1.34,7.08)
4.72(1.83,12.17)
0.001*
Family history of cancer
Yes 18 (75.0) 6 (25.0) 1 1
No 202 (87.4) 29 (12.6) 2.32(0.85,6.33)
2.28(0.74,7.02)
0.153
Menopausal status
Pre-menopausal 117 (82.4) 25 (17.6) 1 1
Post-menopausal 103 (91.2) 10 (8.8) 2.20(1.01, 1.75(0.63, 0.285

Page 12/18
4.80) 4.91)
Using traditional and faith healers as �rst choice
No 138 (82.6) 29 (17.4) 1 1
Yes 82 (93.2) 6 (6.8) 2.87(1.14,7.21)
3.29(1.23,8.80)
0.017*
NB; * P-value < 0.05, was statistically signi�cant, 1= Reference, AOR= Adjusted Odds Ratio, COR= CrudeOdds Ratio, CI= Con�dence Interval.
DiscussionsThis study primarily assessed the prevalence and associated factors for late diagnosis of breast canceramong women attending Hawassa University Comprehensive Specialized Hospital in Southern Ethiopia.Accordingly, recent study showed that the prevalence of late diagnosis of breast cancer among thewoman who diagnosed for breast cancer was 86.3%, [95% CI: 81.7–90.1]. This study result wasconsistent with the study reported from Addis Ababa, Ethiopia (88.89%) [12]. The possible justi�cation forthe similarity of the �ndings is most likely due to both studies were conducted in relatively similar socio-economic, health facilities and systems related factors. The recent �nding was higher than in LMICs,between 30 and 80% are diagnosed in late stages [17, 18], 69% Tanzania [19] and 60% in Egypt [20]. Thismay be due to less education (in the study areas) on breast cancer especially who at higher risk ofdiagnosis delay, imparting adequate knowledge to its presenting signs and symptoms, also the necessityof regular self-breast examination. In addition to this majority of the rural community in the study areasstill practice traditional and religious healers’ alternatives before attending referral hospital. This alsoneeds more attention on community mobilization, community-based screening programs and providetraining for the traditional and religious healers.
This study �nding showed that having no initial advice for breast biopsy or diagnosis is associated withlate diagnosis of breast cancer. This �nding is supported by the other study report from in Addis Ababa,Ethiopia [12]. This might be due to women who had no initial advice for breast biopsy diagnosis notaware on the consequence of breast cancer so they come lately to health institutions. Moreover, inEthiopia, increasing the awareness on the breast cancer is not priority issues for the governmentsbecause government gives more priority for more very urgent health and health related issues.Furthermore, women with breast cancer have limited access to be consulted by the physicians becausegeneral hospitals are very distantly located.
Not early sharing the problem to others was also had signi�cant association with late diagnosis of breastcancer. This �nding is in line with the study conducted in Mexico [22], Columbia [23] and in Ethiopia [14].In the culture of Ethiopia, women feel ashamed of sharing the reproductive health problem to their familymembers, their husband and others because breast is taken as sensitive part of the body to expose asequal as genitalia. This affects the early presentation of the women with breast cancer and contributes

Page 13/18
to lately diagnoses of the breast cancer. In addition to this, most of the time the women in the studyarea were economically dependent and they cannot afford the cost of modern treatments and diagnosticmodalities unless they share their problems to their family members or husband.
This study �nding revealed that using traditional and faith healers as �rst choice was associatedwith late diagnosis of breast cancer. This �nding is supported by the similar study �nding conducted inCote d'Ivoire [24], Malaysia [25] and India [26]. In the study area, people who unable to afford the price ofthe modern medicine, modern radiologic diagnosis and other direct or indirect cost, are enforced to usetraditional herbal medicines and faith healers as their �rst-choice because it is the easily available andaffordable. In addition, biopsy, �ne needle cytology or a core biopsy are performed in few large tertiaryhospitals and specialized secondary level facilities which are not locally available and located muchmiles distant away. These all have a signi�cant contribution for the late diagnosis of breast cancer.
Recommendations and ConclusionsThis study has an implication to target better health practice and health seeking behavior at primaryhealth care facilities level including health education to the women attending health facilities onscreening, treatment, consequences of the late diagnosis of breast cancer. Moreover, health care systemneeds to provide training on modern health care system and the consequences of the late diagnosis ofbreast cancer for licensed traditional healers. Furthermore, health care providers need to provideconsultation service on self-breast examination techniques, breast cancer screening, and informing themearly symptoms can decrease the impact of the late diagnosis of the breast cancer. In addition, everywoman should not be ashamed to share the reproductive health problems with their family, and healthprofessionals also important to have successful treatment of the breast cancer.
In this study, we found a majority of the woman who diagnosed for breast cancer were diagnosed at latestage in my study. The woman who had no initial advice for breast biopsy, not sharing their problemimmediately to others and using traditional medicines and faith healers as their �rst choice wereassociated with late diagnosis of breast cancer.
This was a hospital-based study. It lacks generalizability to the community at large. As this study wascross-sectional, the factors do not establish temporal relationship. Recall bias was tried to reduce butseems not completely avoided. Another limitation of recent study was small number of sample size.Future investigators should study with a large sample size with both quantitative and qualitative datainquiry.
Abbreviations

Page 14/18
AOR Adjusted Odds Ratio
BCRF Breast Cancer Research Foundation
BSE Breast Self-Examination
CBE Clinical Breast Examination
CI Con�dence Interval
COR Crude Odds Ratio
FIGO International Federation of Gynecology and Obstetrics
FMOH Federal Ministry of Health
Gyn Gynecology
HCPD Health Care Provider’s Delay
IARC International Agency for Cancer Research on Cancer
IUCD Intra Uterine Device
MCH Maternal and Childhood Health
OPD Outpatient Department
OR Odds Ratio
SNNPR Southern Nation Nationality and People Region
TNM Tumor, Lymph node and Metastasis
UNICEF United Nations Children's Fund
WHO World Health Organization
CSA Central Statistical Agency
HUCSH Hawassa University Comprehensive and Specialized Hospital
DeclarationsEthics approval and consent to participate
Ethical clearance was obtained from Hawassa University College of Medicine and Health sciences andconducted in accordance with the Declaration of Helsinki and was approved by an institutional reviewboard or ethics committee. Support letter was obtained from the Hawassa University ComprehensiveSpecialized Hospital medical directory. All participants were informed about the purpose, risks, bene�tand con�dentiality issues related to the study. Participation was on voluntary basis and written informedconsent (written informed consent was obtained from legally authorized representatives of respondentfor those who cannot read and write).

Page 15/18
Consent for publication
Not applicable.
Availability of data and materials
The datasets used in this study are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no con�ict of interests.
Funding
Hawassa University provided fund for the study. The funder had no role in designing the study andconducting the analysis.
Authors’ contributions
MY, AG, and AA participated in the conceptualization, formal analysis, investigation, methodology,supervision, visualization, writing-original draft, writing-review and editing, and approving the �nal draft.All authors read and approved the manuscript.
Acknowledgments
The authors would like to thank Hawassa University for providing fund for the study. The authors aregrateful to all data collectors and study participants for their valuable contributions.
References1. Freitas A., Gabrielly Q., Weller M. Patient delays and system delays in breast cancer treatment in
developed and developing countries. Ciência & Saúde Coletiva. 2015;20:3177–89.
2. Ben Fatma L., Belaid I., Said N., Gahbiche S., Hochlef M., et al. What could be the reasons of latediagnosis of breast cancer in Tunisia? La Tunisie medicale. 2018;96(10–11):665–71.
3. Brunet J., Saunders S., Gifford W., Thomas R., Hamilton R. An exploratory qualitative study of themeaning and value of a running/walking program for women after a diagnosis of breast cancer.Disability and rehabilitation. 2018;40(9):1041-8.
4. Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, et al. Cancer Incidence and Mortality WorldwideIARC Cancer Base No. 11 [internet]. Lyon, France: International Agency for Research on Cancer,. 2013.
5. WHO. Global health observatory. Geneva: World Health Organization; 2017
�. Hadgu E., Seifu D., Tigneh W., Bokretsion Y., Bekele A., et al. Breast cancer in Ethiopia: evidence forgeographic difference in the distribution of molecular subtypes in Africa. BMC women's health.2018;18(1):40-.

Page 16/18
7. Dickens C., Joffe M., Jacobson J., Venter F., Schüz J., et al. Stage at breast cancer diagnosis anddistance from diagnostic hospital in a peri-urban setting: A South African public hospital case seriesof over 1000 women. Int J Cancer. 2014;1(135):2173–218.
�. Gemta E., Bekele A., Seifu D., Bekuretsion Y. Patterns of Breast Cancer Among Ethiopian Patients:Presentations and Histopathological Features. Journal of Cancer Science and Therapy.2019;11:038–42.
9. Federal Ministry of Health Ethiopia, Disease Prevention and Control Directorate, National CancerControl Plan, 2016–2020. 2015.
10. Biniyam T.D., Nikola C., Eugenia V.B., Alexandros T., Daniel R. Breast cancer care in northern Ethiopia:cross-sectional analysis. BMC Cancer 2019;19:393
11. Abate S., Yilma Z., Assefa M., Tigeneh W. Trends of Breast Cancer in Ethiopia. Int J Cancer Res MolMech 2016;2(1):1–5.
12. Bedada T., Teshale H., Hailu A., Mulugeta T. Prevalence and Factors Contributing to Late Diagnosis ofBreast Cancer among Women Attending Tikur Anbessa Specialized Hospital, Oncology Unit, AddisAbaba, Ethiopia, 2017. J Integr Oncol 2018;7: 214.
13. Gebremedhin A., Shamebo M. Clinical pro�le of Ethiopian patients with breast cancer. East AfricanMedical Journal. 2004;75(11): 640–3.
14. Gebremariam A., Addissie A., Worku A., Assefa M., Kantelhardt E.J., et al. Perspectives of patients,family members, and health care providers on late diagnosis of breast cancer in Ethiopia: Aqualitative study. PloS one. 2019;14(8):e0220769.
15. Shieh S.-H., Hsieh V.C.-R., Liu S.-H., Chien C.-R., Lin C.-C., et al. Delayed time from �rst medical visit todiagnosis for breast cancer patients in Taiwan. Journal of the Formosan Medical Association.2014;113(10):696–703.
1�. Norsa'adah B., Rampal K.G., Rahmah M.A., Naing N.N., Biswal B.M. Diagnosis delay of breast cancerand its associated factors in Malaysian women. BMC Cancer. 2011;11(1):141.
17. Bastiaannet E., Charman J., Johannesen T.B., Schrodi S., Siesling S., et al. A European, ObservationalStudy of Endocrine Therapy Administration in Patients With an Initial Diagnosis of HormoneReceptor-Positive Advanced Breast Cancer. Clinical breast cancer. 2018;18(4):e613-e9.
1�. Iversen J.R., Amlie E., Hagen S., Harbitz T., Karesen R., et al. [Late diagnosis of advanced breastcancer–a challenge for health services]. Tidsskrift for den Norske laegeforening: tidsskrift forpraktisk medicin, ny raekke. 2004;112(14):1821–4.
19. Yassin N.I.R., Omran S., El Houby E.M.F., Allam H. Machine learning techniques for breast cancercomputer aided diagnosis using different image modalities: A systematic review. Computer methodsand programs in biomedicine. 2018;156:25–45.
20. Harris E.E.R. Precision Medicine for Breast Cancer: The Paths to Truly Individualized Diagnosis andTreatment. International journal of breast cancer. 2018;2018:4809183.
21. McKenzie F., Zietsman A., Galukande M., Anele A., Adisa C., et al. Drivers of advanced stage at breastcancer diagnosis in the multicountry African breast cancer - disparities in outcomes (ABC-DO) study.
Page 17/18
Int J Cancer. 2018;142(8):1568–79.
22. Unger-Saldana K., Ventosa-Santaularia D., Miranda A., Verduzco-Bustos G. Barriers and ExplanatoryMechanisms of Delays in the Patient and Diagnosis Intervals of Care for Breast Cancer in Mexico.The oncologist. 2018;23(4):440–53.
23. McElroy J.A., Proulx C.M., Johnson L., Heiden-Rootes K.M., Albright E.L., et al. Breaking bad news of abreast cancer diagnosis over the telephone: an emerging trend. Supportive care in cancer: o�cialjournal of the Multinational Association of Supportive Care in Cancer. 2019;27(3):943–50.
24. Toure M., Nguessan E., Bambara A.T., Kouassi Y.K., Dia J.M., et al. [Factors linked to late diagnosis inbreast cancer in Sub-Saharan Africa: case of Cote d'Ivoire]. Gynecologie, obstetrique & fertilite.2013;41(12):696–700.
25. Hisham A.N., Yip C.H. Overview of breast cancer in Malaysian women: a problem with late diagnosis.Asian journal of surgery. 2004;27(2):130–3.
2�. Sathwara J.A., Balasubramaniam G., Bobdey S.C., Jain A., Saoba S. Sociodemographic Factors andLate-stage Diagnosis of Breast Cancer in India: A Hospital-based Study. Indian journal of medicaland paediatric oncology: o�cial journal of Indian Society of Medical & Paediatric Oncology.2017;38(3):277–81.
Figures
Figure 1

Page 18/18
TNM-Modi�ed current stages of diagnosis of woman who diagnosed for breast cancer among who visitoncology department in HUCRCH in Hawassa city, Southern Ethiopia, 2020
Figure 2
Late diagnosis of breast cancer among the woman who diagnosed for breast cancer among who visitoncology department in HUCRCH in Hawassa city, Southern Ethiopia, 2020.