Kallikrein-related peptidase-6 (KLK6) mRNA expression is an independent prognostic tissue biomarker...
13
RESEARCH ARTICLE Kallikrein-related peptidase-6 (KLK6 ) mRNA expression is an independent prognostic tissue biomarker of poor disease-free and overall survival in colorectal adenocarcinoma Spyridon Christodoulou & Dimitra K. Alexopoulou & Christos K. Kontos & Andreas Scorilas & Iordanis N. Papadopoulos Received: 12 December 2013 /Accepted: 2 January 2014 /Published online: 16 January 2014 # International Society of Oncology and BioMarkers (ISOBM) 2014 Abstract Members of the family of tissue kallikrein and kallikrein-related peptidases possess important prognostic val- ue in cancer. Moreover, the oncogenic role of kallikrein- related peptidase-6 (KLK6) in colorectal cancer has been well documented so far. This study investigated the prognostic value of KLK6 mRNA expression as a molecular tissue bio- marker in colorectal adenocarcinoma. For this purpose, KLK6 mRNA expression was studied in 110 primary colorectal adenocarcinomas and 39 paired noncancerous colorectal spec- imens. A dramatic upregulation of KLK6 mRNA expression was observed in colorectal tumors. KLK6 mRNA overexpres- sion was associated with high depth of tumor invasion, pres- ence of distant metastases, and tumor-node-metastasis (TNM) stage of patients. Furthermore, KLK6 mRNA expression was shown to predict poor disease-free and overall survival inde- pendently of patient gender, age, tumor size, location, histo- logical subtype, grade, venous invasion, lymphatic invasion, TNM stage, radiotherapy, and chemotherapy treatment. More- over, Kaplan–Meier survival analysis revealed that colorectal adenocarcinoma patients with negative regional lymph nodes (N0) and those without distant metastases (M0) harboring KLK6 mRNA-positive colorectal tumors tended to relapse and die earlier than N0 and M0 patients with KLK 6 mRNA- negative colorectal adenocarcinoma. Thus, KLK6 mRNA ex- pression could be considered as an independent, unfavorable molecular prognostic biomarker in colorectal adenocarcino- ma, with additional prognostic value in patients without re- gional or distant metastases. Keywords Kallikreins . Tumor marker . Molecular tissue biomarker . Colorectal cancer . Colon cancer . Quantitative real-time PCR Introduction Colorectal cancer (CRC) represents the third most usually diagnosed malignancy all over the world and also the fourth most common cause of death due to cancer [1]. CRC screen- ing tests that are widely used in clinical practice can detect both primary CRC and postoperative recurrence earlier than in the past. Thus, they are critical for effective treatment and contribute to a better clinical outcome of CRC patients. The American Society of Clinical Oncology Tumor Marker Panel and the European Group on Tumor Markers recommend quantification of preoperative and postoperative circulating carcinoembryonic antigen (CEA), a biomarker with indepen- dent prognostic value in CRC. Besides that, CEA is used to monitor disease relapse after surgical resection of the colorec- tal tumor as well as the efficacy of systemic therapy (or treatment failure) of patients with metastatic CRC. However, neither CEA nor any other previously suggested tumor bio- markers such as cancer antigen 19–9 (CA19-9) possess re- markable sensitivity [2, 3]. Despite the fact that colonoscopy remains a method of choice for CRC screening [4], reliable prognostic and/or response-predictive tumor biomarkers are needed to diminish CRC burden of morbidity and mortality and to increase long-term survival. The family of tissue kallikrein and kallikrein-related pepti- dases (KLKs) comprises 15 genes (KLK1 –KLK15 ), which are closely located in the largest contiguous cluster of peptidase- encoding genes within the entire human genome, spanning ~300 kb on the chromosomal region 19q13.4 [5, 6]. KLKs are secreted trypsin- or chymotrypsin-like serine peptidases of S. Christodoulou : I. N. Papadopoulos Fourth Surgery Department, University General Hospital “Attikon”, Haidari, Athens 12462, Greece D. K. Alexopoulou : C. K. Kontos : A. Scorilas (*) Department of Biochemistry and Molecular Biology, University of Athens, Panepistimiopolis, Athens 15701, Greece e-mail: [email protected] Tumor Biol. (2014) 35:4673–4685 DOI 10.1007/s13277-014-1612-y
Transcript of Kallikrein-related peptidase-6 (KLK6) mRNA expression is an independent prognostic tissue biomarker...

RESEARCH ARTICLE
Kallikrein-related peptidase-6 (KLK6) mRNA expressionis an independent prognostic tissue biomarker of poordisease-free and overall survival in colorectal adenocarcinoma
Spyridon Christodoulou & Dimitra K. Alexopoulou &
Christos K. Kontos & Andreas Scorilas &
Iordanis N. Papadopoulos
Received: 12 December 2013 /Accepted: 2 January 2014 /Published online: 16 January 2014# International Society of Oncology and BioMarkers (ISOBM) 2014
Abstract Members of the family of tissue kallikrein andkallikrein-related peptidases possess important prognostic val-ue in cancer. Moreover, the oncogenic role of kallikrein-related peptidase-6 (KLK6) in colorectal cancer has been welldocumented so far. This study investigated the prognosticvalue of KLK6 mRNA expression as a molecular tissue bio-marker in colorectal adenocarcinoma. For this purpose, KLK6mRNA expression was studied in 110 primary colorectaladenocarcinomas and 39 paired noncancerous colorectal spec-imens. A dramatic upregulation of KLK6 mRNA expressionwas observed in colorectal tumors. KLK6mRNA overexpres-sion was associated with high depth of tumor invasion, pres-ence of distant metastases, and tumor-node-metastasis (TNM)stage of patients. Furthermore, KLK6mRNA expression wasshown to predict poor disease-free and overall survival inde-pendently of patient gender, age, tumor size, location, histo-logical subtype, grade, venous invasion, lymphatic invasion,TNM stage, radiotherapy, and chemotherapy treatment.More-over, Kaplan–Meier survival analysis revealed that colorectaladenocarcinoma patients with negative regional lymph nodes(N0) and those without distant metastases (M0) harboringKLK6 mRNA-positive colorectal tumors tended to relapseand die earlier than N0 and M0 patients with KLK6 mRNA-negative colorectal adenocarcinoma. Thus, KLK6mRNA ex-pression could be considered as an independent, unfavorablemolecular prognostic biomarker in colorectal adenocarcino-ma, with additional prognostic value in patients without re-gional or distant metastases.
Keywords Kallikreins . Tumormarker . Molecular tissuebiomarker . Colorectal cancer . Colon cancer . Quantitativereal-time PCR
Introduction
Colorectal cancer (CRC) represents the third most usuallydiagnosed malignancy all over the world and also the fourthmost common cause of death due to cancer [1]. CRC screen-ing tests that are widely used in clinical practice can detectboth primary CRC and postoperative recurrence earlier than inthe past. Thus, they are critical for effective treatment andcontribute to a better clinical outcome of CRC patients. TheAmerican Society of Clinical Oncology Tumor Marker Paneland the European Group on Tumor Markers recommendquantification of preoperative and postoperative circulatingcarcinoembryonic antigen (CEA), a biomarker with indepen-dent prognostic value in CRC. Besides that, CEA is used tomonitor disease relapse after surgical resection of the colorec-tal tumor as well as the efficacy of systemic therapy (ortreatment failure) of patients with metastatic CRC. However,neither CEA nor any other previously suggested tumor bio-markers such as cancer antigen 19–9 (CA19-9) possess re-markable sensitivity [2, 3]. Despite the fact that colonoscopyremains a method of choice for CRC screening [4], reliableprognostic and/or response-predictive tumor biomarkers areneeded to diminish CRC burden of morbidity and mortalityand to increase long-term survival.
The family of tissue kallikrein and kallikrein-related pepti-dases (KLKs) comprises 15 genes (KLK1–KLK15), which areclosely located in the largest contiguous cluster of peptidase-encoding genes within the entire human genome, spanning~300 kb on the chromosomal region 19q13.4 [5, 6]. KLKs aresecreted trypsin- or chymotrypsin-like serine peptidases of
S. Christodoulou : I. N. PapadopoulosFourth Surgery Department, University General Hospital “Attikon”,Haidari, Athens 12462, Greece
D. K. Alexopoulou : C. K. Kontos :A. Scorilas (*)Department of Biochemistry and Molecular Biology, University ofAthens, Panepistimiopolis, Athens 15701, Greecee-mail: [email protected]
Tumor Biol. (2014) 35:4673–4685DOI 10.1007/s13277-014-1612-y

~25–30 kDa, mainly synthesized in secretory epithelial cellswithin the glandular epithelia of several organs, such as thecolon, pancreas, skin, prostate, breast, and brain. These serinepeptidases act independently and/or participate in proteolyticcascades to regulate many physiological processes [7-9]. Fur-thermore, they are heavily involved in carcinogenesis, as theyare able to degrade components of the extracellular matrix(ECM) [10]. Consequently, they facilitate tumor invasion andmetastasis. KLKs regulate also the enzymatic activity of manysubstrates, such as proteinase-activated receptors (PARs) [11].The protein subfamily of PARs includes four G-protein-coupled receptors, two of which (PAR1 and PAR2) are aber-rantly expressed in gastrointestinal malignancies [12, 13].Proteolytic cleavage of these receptors leads to their couplingwith heterotrimeric G proteins, and finally to signal transduc-tion, in many different cellular contexts [14].
The prognostic value of several members of the KLKfamily in CRC has already been uncovered. Protein expres-sion of a panel of KLKs in cytosolic extracts fromCRC tissuesrevealed that KLK4, KLK6, KLK7, KLK8, KLK10, KLK11,KLK13, and KLK15 are significantly overexpressed in ma-lignant colorectal tumors, compared to adjacent noncanceroustissue specimens [7, 13, 15, 16]. Additionally, KLK5, KLK6,KLK7, KLK13, and KLK14 expression predicts poor overallsurvival (OS) for CRC patients. Most importantly, the unfa-vorable prognostic power of KLK5, KLK7, and KLK14 isindependent of patients’ age, histological grade, and tumornode metastasis (TNM) stage [15]. Regarding mRNA expres-sion of KLK genes in CRC, an upregulation has been noticedin most cases. Moreover, high mRNA levels of several mem-bers of this family display prognostic significance in thisneoplasia [17]. For instance, patients with high KLK10 ex-pression have shorter disease-free survival (DFS) and OS rates[18]. Furthermore, KLK4 mRNA expression constitutes anunfavorable prognostic biomarker in colorectal adenocarcino-ma, predicting poor DFS, independently of tumor size andpatients’ nodal status [19]. KLK11mRNA expression can alsobe regarded as a novel, molecular prognostic biomarker incolorectal adenocarcinoma, with significant prognostic valuein patients with highly invasive tumors and/or positive lymphnodes [20].
Accumulating evidence supports the oncogenic role ofKLK6 in colorectal cancer. This trypsin-like serine peptidasewas shown to mediate KRAS-dependent migration of humancolorectal cancer cells. It should be noted thatKLK6 transcrip-tion is induced by activation of the PI3K and the p42/44MAPK pathways [21]. Another inducer of KLK6 expressionand secretion is caveolin 1 (CAV1), the main structural proteinof caveolae. In HCT116 colorectal cancer cells, CAV1 in-creases the amount of phosphorylated AKT, resulting in en-hancedKLK6expression [22]. KLK6 has also been implicatedin angiogenesis, migration, and invasion through mechanismsinvolving ECM degradation [10]. KLK6 substrates include
collagen, fibrinogen, fibronectin, and laminin [10, 23-27].Furthermore, KLK6 was shown to activate PAR1 in neuronsas well as both PAR1 and PAR2 in astrocytes to induceintracellular Ca2+ flux [28], to regulate the mitogen-activatedprotein kinase (MAPK) signaling pathway [28, 29], and totrigger reactive astrogliosis [9]. Moreover, in melanoma cells,KLK6 elicited intracellular Ca2+ flux and tumor cell invasioncritically depending on the protease-activated receptor 1(PAR1) [30]. It should also be noted that activated PAR1and PAR2 have been shown to enhance the proliferation andmotility of colon cancer cells [31, 32] as well as their migra-tion potential and matrix adhesion [33]. Hence, KLK6 mayalso act through a KLK6/PAR axis to directly alter the tumormicroenvironment and to enhance the invasiveness and met-astatic potential of colorectal adenocarcinoma cells.
In the present study, we investigated the putative clinicalsignificance of KLK6mRNA expression as a novel moleculartissue biomarker in colorectal adenocarcinoma. For this pur-pose, we developed a highly accurate and cost-effective quan-titative real-time PCR (qRT-PCR) methodology, based on theSYBR Green chemistry, and analyzed KLK6mRNA expres-sion in colorectal adenocarcinoma specimens and adjacentnoncancerous colorectal mucosae. Finally, we undertook ex-tensive biostastical analysis to examine the discriminatory andprognostic potential of KLK6 mRNA expression in thisdisease.
Materials and methods
Patients
The current study included 110 adult patients submitted to acolectomy for a primary colorectal adenocarcinoma in theFourth Surgery Department of the University General Hospi-tal “Attikon” (Athens, Greece), between 2000 and 2007.Informed consent was obtained from all individuals partici-pating in the study, which was performed in accordance withthe ethical standards of the World Medical Association Dec-laration of Helsinki (version 2008) and was also approved bythe institutional Ethics Committee of the University GeneralHospital “Attikon” (Athens, Greece).
Patients’ age ranged from 35.0 to 93.0 years with a mean ±SEM of 65.5±1.2. All surgical specimens of the colectomieswere completely evaluated by a pathologist. Clinicopatholog-ical data used for comparison in the present study such as thedimensions of the colorectal tumors, histological subtype,grade, venous and lymphatic invasion, depth of tumor inva-sion (T), lymph node count and metastasis (N), distant metas-tasis (M), and TNM stage were also routinely reported ac-cording to the TNM classification system (seventh version), asdesignated by the American Joint Committee on Cancer
4674 Tumor Biol. (2014) 35:4673–4685

(AJCC) for colorectal adenocarcinoma [34]. All the aforemen-tioned data were recorded in an electronic database.
Decision for postoperative adjuvant chemoradiation wastaken by oncologists. Postoperative radiotherapy and chemo-therapy treatment data were available for 101 patients, whilefollow-up information was available for 96 patients and in-cluded disease status (disease-free or recurrence) and survivalstatus (alive or deceased), along with the dates of the eventsand the cause of death. Recurrence and death were consideredas endpoints for DFS and OS, respectively. The maximumfollow-up time was 10 years.
Colorectal tissue specimens
We collected 110 colorectal adenocarcinomas and 39 paired,adjacent noncancerous colorectal tissue specimens from pa-tients having undergone surgical treatment for primary colo-rectal adenocarcinoma. Macroscopically observed necroticareas of the tumor were avoided during the collection ofcancerous samples with the assistance of a pathologist. Fur-thermore, noncancerous samples were obtained from macro-scopically observed normal intestine at the cut end of thesurgical specimen, away from the adenocarcinoma. The non-cancerous colorectal tissue specimens were also routinelyprocessed by a pathologist to exclude tumor invasion. Allcolorectal tissue specimens were frozen in liquid nitrogenimmediately after resection.
Cancer cell line culture
The human colorectal adenocarcinoma cell line HT-29 wasmaintained in McCoy’s 5A medium, adjusted to contain 10 %fetal bovine serum (FBS), 100 kU/L penicillin, 0.1 g/L strep-tomycin, and 2 mML-glutamine. Cells were seeded at a con-centration of 5 × 105 cells/mL and subcultured at 37 °C in ahumidified atmosphere containing 5 % CO2, before theircollection for further use.
Total RNA extraction and cDNA synthesis
Reagent (Ambion (Europe) Ltd., Huntingdon, UK). TotalRNA was extracted from homogenized tumors and HT-29cells according to the manufacturer’s instructions and wasthen diluted in RNA Storage Solution (Ambion (Europe)Ltd.) and stored at −80 °C until use. Total RNA concentrationand purity were assessed spectrophotometrically at 260 and280 nm. The quantity of isolated RNA ranged from 10 to25 μg. Next to determination of RNA concentration, theintegrity of the isolated RNAwas checked by electrophoresisof 1 μg of total RNA on agarose gel. No signs of degradationwere observed among all samples that were included in thecurrent study.
First-strand cDNAwas produced from 2 μg of total RNA,using the M-MLV Reverse Transcriptase (Invitrogen, Carls-bad, CA, USA) and oligo-dT as primer, following the manu-facturer’s instructions. The final reaction volume was 20 μL.
Quantitative real-time PCR
Quantitative real-time PCR as performed using the SYBRGreen chemistry in a 7500 Real Time PCR System (AppliedBiosystems, Foster City, CA, USA). Two pairs of gene-specific primers were designed, based on the KLK6 and B2McDNA sequences. The sequences of the KLK6 real-time PCRprimers were 5′-TCTGTGGTGGGGTCCTTATCC-3′ and 5′-TAGTCAGGGTGGATCACAGCC-3′, generating a 157-bpPCR amplicon originating from all KLK6 splice variants,and those of the B2M real-time PCR primers were 5′-ACTGAATTCACCCCCACTGA-3′ and 5′-AAGCAAGCAAGCAGAATTTGG-3′, producing a PCR amplicon of 167 bp.The reaction mixture contained 20 ng of cDNA diluted in2.5 μL of RNase-free water, 5 μL Power SYBR Green PCRMaster Mix (2×) (Applied Biosystems), and 2 μL of gene-specific primers (final concentration 50 nM each), in a finalreaction volume of 10 μL. The cycling conditions were asfollows: a denaturation step at 95 °C for 10 min, followed by40 cycles of 95 °C for 15 s, 60 °C for 60 s, and a final step forthe generation of a dissociation curve, in order to distinguishbetween the major PCR product and primer-dimers.
Calculations and validation of the comparative CT (2−ΔΔCT)
method for KLK6 mRNA quantification
The comparative CT (2−ΔΔCT) method was used for all calcu-lations. Its application is based on the assumptions that thePCR amplification efficiencies of the target and the referencegenes are similar to each other and close to 1 [35]. Theprerequisites for the application of the 2−ΔΔCT method—sim-ilar PCR amplification efficiencies of the target and the refer-ence genes, and also both of them close to 100 %—werechecked in a validation experiment, in which CT values ofKLK6 and B2M were measured in a dilution series of HT-29cDNA over a 105-fold range and then plotted against logcDNA dilution. The slopes of KLK6 and B2M standard curveswere −3.468 and −3.447, respectively. Real-time PCR effi-ciency (E) for amplification of each gene was calculated usingthe following formula: E=−1+10(−1/a), where α is the slope ofthe corresponding standard curve; hence, the calculated effi-ciencies of KLK6 and B2M amplification were 94.3, and95.0 %, respectively.
In the current study, beta-2-microglobulin (B2M) was usedas an endogenous reference gene so as to normalize PCRs forthe amount of RNA added to the reverse transcription reac-tions, as this housekeeping gene presents very small variationamong colorectal tissue specimens [36, 37]. In more detail, a
Tumor Biol. (2014) 35:4673–4685 4675
Tissue specimens were pulverized and then dissolved in TRI®

previous study analyzing the stability of expression of house-keeping genes showed that B2M generated the best score as anormalizing gene for comparing human colon primary carci-nomas with their noncancerous counterparts originating fromnormal resection margins, although other housekeeping geneswere shown to constitute acceptable alternatives [37]. More-over, the colorectal adenocarcinoma cell line HT-29 was usedas a calibrator, thus rendering all PCR runs comparable [35].
Statistical analysis
As the distributions of KLK6 mRNA expression levels incolorectal adenocarcinomas and in their normal counterpartswere not Gaussian, the analysis of the differences in the twogroups of paired samples was carried out with the nonpara-metric Wilcoxon signed-rank test. Moreover, analyses of thedifferences among subgroups of patients—stratified accord-ing to clinicopathological parameters—were performed withthe Mann–Whitney U test or Jonckheere-Terpstra test, whereappropriate. Correlations between KLK6 mRNA expressionand the other continuous variables (age and tumor size) of thestudy were assessed by Spearman correlation coefficient (rs).
Next, we used the X-tile software, an algorithm that allowsdetermination of an optimal cutoff value by correcting for theuse of minimum p value statistics [38], to create the optimalcutoff point for KLK6mRNA expression in colorectal adeno-carcinoma, as there are no established cutoffs. This optimalcutoff value was 30.98 relative quantification units (RQU),equal to the 42th percentile. Based on this value, KLK6mRNA expression was categorized as positive or negative,and associations between KLK6mRNA expression status andother clinicopathological parameters, including patient genderand age, tumor size and location, histological subtype, grade,venous and lymphatic invasion, depth of tumor invasion (T),metastases in regional lymph nodes (N), distant metastases(M), and the resulting TNM stage, were analyzed using thetwo-tailed chi-square (χ2) or Fisher’s exact test, whereappropriate.
Survival analysis was performed by constructing Kaplan–Meier DFS and OS curves [39]; the differences between thesecurves were evaluated using the log-rank (Mantel–Cox) test.Additionally, Cox proportional hazard regression models [40]were developed for the assessment of the association betweenthe prognostic markers and the relative risk patients’ forrelapse and death. Multivariate Cox regression models wereadjusted for all the aforementioned clinicopathological fea-tures of colorectal adenocarcinoma plus radiotherapy andchemotherapy. Finally, Kaplan–Meier survival analysis wascarried out to evaluate the prognostic potential of KLK6mRNA expression status with regard to DFS and OS insubgroups of patients, stratified according to each of theaforementioned clinicopathological characteristics. The level
of significance was defined at a probability value of less than0.05 (p<0.05).
Results
Clinical and biological characteristics of colorectaladenocarcinoma patients
Our study included 110 colorectal adenocarcinoma specimensand 39 adjacent noncancerous colorectal tissue specimens.The cohort of patients consisted of 56 men and 54 women.The median patient age at the time of diagnosis was 67 years(range 35–93). Seventy-two (65.5 %) patients had a primaryadenocarcinoma located in the colon and 38 (34.5 %) had aprimary tumor located in the rectum. Regarding the histolog-ical subtype of the colorectal tumors, the vast majority of them(89.1 %) were adenocarcinomas (nonmucinous), and the rest(10.9 %) were mucinous adenocarcinomas. According to theWHO classification system (fourth edition), 9 (8.3 %) malig-nant tumors were histologically characterized as well differ-entiated (grade I), 83 (76.1 %) were characterized as moder-ately differentiated (grade II), and 17 (15.6 %) were poorlydifferentiated (grade III). Furthermore, 12 (10.9 %) colorectaladenocarcinomas invaded venous blood vessels and another11 (10.0 %) invaded lymphatic vessels. According to theTNM staging system (seventh edition), 14 (12.7 %) patientswere at stage I, 46 (41.8 %) at stage II, 38 (34.5 %) at stage III,and 12 (10.9 %) at stage IV. Patients’ clinical and biologicalfeatures are summarized in Table 1.
Out of the 96 patients with complete follow-up informa-tion, 30 patients (31.3 %) had a relapse during the respectivefollow-up period. The median DFS was 41.0 months (range1.0–120.0), while the estimated mean DFS time was83.8 months (95 % confidence interval [95 % CI] = 73.2–94.4). In the same subset of 96 patients for whom detailedfollow-up information was available, 27 deaths (28.1 %) wererecorded during the respective follow-up period. Causes relat-ed to colorectal adenocarcinoma account for all patient deaths.The median OSwas 51.0 months (range 5.0–120.0), while theestimated mean OS time was 87.8 months (95 % CI = 77.9–97.8).
KLK6 mRNA overexpression in colorectal adenocarcinoma
Normalized results were expressed as the ratio of KLK6 tran-scripts to B2M transcripts calculated for each colonic tissuespecimen divided by the same ratio calculated for HT-29 cellsand were finally multiplied by 1,000 and designated as RQU,standing for KLK6mRNA copies/1,000 B2MmRNA copies.Each real-time PCR reaction was performed in triplicate, inorder to obtain high data reproducibility.
4676 Tumor Biol. (2014) 35:4673–4685

KLK6 mRNA expression in colorectal adenocarcinomatissues ranged between 0.19 and 945.36 RQU with a mean ±SEM of 113.51±16.76, while KLK6 levels in 37 out of 39normal counterparts were undetectable. Comparison of KLK6mRNA levels between colorectal adenocarcinomas and theiradjacent noncancerous colorectal tissue specimens uncoveredthe profound overexpression of this molecule in all malignanttumor specimens (p<0.001). Thus, KLK6 mRNA expressionwas shown to distinguish very efficiently colorectal adenocar-cinoma from noncancerous colorectal tissue.
Table 1 Clinical and biological features of patients with colorectaladenocarcinoma
Total patients Patient subgroupa
Number of patients 110 39
Median (range)
Age (years) 67.5 (35.0–93.0) 66.0 (37.0–93.0)
Tumor size (cm) 4.8 (1.5–12.0) 4.8 (2.2–12.0)
Disease-free survival (months) 41 (1–120) 40 (1–60)
Overall survival (months) 51 (5–120) 48 (5–60)
Gender
Male 56 (50.9 %) 19 (48.7 %)
Female 54 (49.1 %) 20 (51.3 %)
Tumor location
Colon 72 (65.5 %) 31 (79.5 %)
Cecum 15 (13.6 %) 5 (12.8 %)
Ascending colon 16 (14.5 %) 9 (23.1 %)
Transverse colon 4 (3.6 %) 1 (2.6 %)
Descending colon 7 (6.4 %) 5 (12.8 %)
Sigmoid colon 30 (27.3 %) 11 (28.2 %)
Rectum 38 (34.5 %) 8 (20.5 %)
Histological subtypeb
Adenocarcinoma (nonmucinous) 98 (89.1 %) 35 (89.7 %)
Mucinous adenocarcinoma 12 (10.9 %) 4 (10.3 %)
Other subtypes 0 (0.0 %) 0 (0.0 %)
Gradeb
I 9 (8.2 %) 3 (7.7 %)
II 83 (75.5 %) 28 (71.8 %)
III 17 (15.5 %) 8 (20.5 %)
IV 0 (0.0 %) 0 (0.0 %)
xc 1 (0.9 %)
Venous invasion
No 98 (89.1 %) 37 (94.9 %)
Yes 12 (10.9 %) 2 (5.1 %)
Lymphatic invasion
No 99 (90.0 %) 35 (89.7 %)
Yes 11 (10.0 %) 4 (10.3 %)
Td
Tx 0 (0.0 %) 0 (0.0 %)
Tis 0 (0.0 %) 0 (0.0 %)
T1 1 (0.9 %) 0 (0.0 %)
T2 16 (14.6 %) 4 (10.3 %)
T3 64 (58.2 %) 22 (56.4 %)
T4 29 (26.3 %) 13 (33.3 %)
T4a 14 (12.7 %) 7 (17.9 %)
T4b 15 (13.6 %) 6 (15.4 %)
Nd
Nx 0 (0.0 %) 0 (0.0 %)
N0 63 (57.3 %) 21 (53.9 %)
N1 31 (28.2 %) 13 (33.3 %)
N1a 14 (12.7 %) 3 (7.7 %)
N1b 17 (15.5 %) 10 (25.6 %)
Table 1 (continued)
Total patients Patient subgroupa
Number of patients 110 39
N1c 0 (0.0 %) 0 (0.0 %)
N2 16 (14.5 %) 5 (12.8 %)
N2a 9 (8.3 %) 3 (7.7 %)
N2b 7 (6.4 %) 2 (5.1 %)
Md
M0 98 (89.1 %) 33 (84.6 %)
M1 12 (10.9 %) 6 (15.4 %)
M1a 9 (8.2 %) 4 (10.3 %)
M1b 3 (2.7 %) 2 (5.1 %)
TNM staged
I 14 (12.7 %) 3 (7.7 %)
II 46 (41.8 %) 17 (43.6 %)
IIA 36 (32.7 %) 14 (35.9 %)
IIB 4 (3.6 %) 2 (5.1 %)
IIC 6 (5.5 %) 1 (2.6 %)
III 38 (34.6 %) 13 (33.3 %)
IIIA 2 (1.8 %) 1 (2.6 %)
IIIB 28 (25.5 %) 10 (25.6 %)
IIIC 8 (7.3 %) 2 (5.1 %)
IV 12 (10.9 %) 6 (15.4 %)
IVA 9 (8.2 %) 4 (10.3 %)
IVB 3 (2.7 %) 2 (5.1 %)
Radiotherapy
No 85 (77.3 %) 35 (89.7 %)
Yes 16 (14.5 %) 4 (10.3 %)
xc 9 (8.2 %)
Chemotherapy
No 43 (39.1 %) 15 (38.5 %)
Yes 58 (52.7 %) 24 (61.5 %)
xc 9 (8.2 %)
Abbreviations: T depth of tumor invasion, N nodal status, M distantmetastasisa Patients for whom noncancerous colorectal tissue specimens wereavailablebWHO classification (fourth edition)c Unknownd TNM classification system (seventh edition)
Tumor Biol. (2014) 35:4673–4685 4677

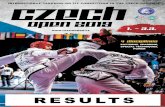
Interestingly, KLK6 mRNA expression was significantlydifferent among highly invasive tumors and those showinglow invasion (p=0.013). More specifically, colorectal adeno-carcinomas having penetrated through muscularis propria(T3) had higher KLK6 mRNA levels than tumors limited tosubmucosa (T1) or having penetrated into muscularis propriabut not through (T2). Furthermore, the KLK6 gene wasexpressed utmost in colorectal adenocarcinomas characterizedby invasion or adherence to surrounding organs/structures(T4) (Fig. 1).
Association between KLK6 mRNA expression statusand clinicopathological features of colorectal adenocarcinoma
KLK6 mRNA expression levels were next categorized intotwo subgroups (positive vs. negative), as described in the“Materials and methods” section. Therefore, 46 (41.8 %) co-lorectal adenocarcinomas were classified as KLK6-negativeand 54 (58.2 %) as KLK6-positive. KLK6mRNA expressionstatus seems to be associated with tumor invasion, distantmetastases, and TNM stage (Table 2). In more detail, highlyinvasive (T3 and T4) colorectal adenocarcinomas were morefrequently KLK6-positive, compared to tumors showing lowinvasiveness (T1 or T2) (p=0.048). Furthermore, adenocarci-nomas of the vast majority (91.7 %) of patients with metasta-ses in distant organs exhibited strong KLK6 mRNA expres-sion, whereas only 54.1 % of metastasis-free patients werecharacterized as KLK6-positive (p=0.013). Finally, the fre-quency of KLK6 mRNA positivity was shown to increaseprogressively following the TNM stage incline (p=0.019).
KLK6 mRNA expression is an independent indicator of poorsurvival in colorectal adenocarcinoma
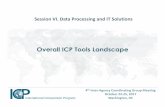
Kaplan–Meier survival curves illustrated that colorectal ade-nocarcinoma patients with KLK6-positive adenocarcinomashad significantly shorter DFS time (p=0.002), in comparisonwith those who had a KLK6-negative malignant tumor(Fig. 2a). In accordance with these findings, Cox univariatesurvival analysis revealed that besides histological grade,depth of tumor invasion, and patient nodal status, which wereconfirmed as significant predictors of DFS (p=0.048, 0.001,and 0.028, respectively),KLK6mRNA expression was shownto predict poor DFS in colorectal adenocarcinoma (Table 3),since patients with KLK6 mRNA-positive tumors were athigher risk of relapse (hazard ratio [HR]=3.67, 95 % CI=1.50–9.00, p=0.004). In multivariate Cox regression analysis,KLK6 mRNA expression added prognostic power in the de-veloped multiparametric model, as it remained an unfavorableprognosticator, which was independent of patient gender, age,tumor size, location, histological subtype, grade, venous andlymphatic invasion, depth of tumor invasion, nodal status,
radiotherapy, and/or chemotherapy treatment (HR=4.47,95 % CI=1.58–12.64, p=0.005).
Fig. 1 Comparison of the distribution of KLK6 mRNA expression incolorectal adenocarcinoma limited to submucosa (T1) or having pene-trated into muscularis propria but not through (T2), with those havingpenetrated through muscularis propria (T3), and those showing invasionor adherence to surrounding organs/structures (T4). The distributions ofKLK6mRNA levels were compared with the nonparametric Jonckheere–Terpstra test. The dark line close to the middle of each box represents the50th percentile (the median value) of each group, the bottom and top ofeach box show the 25th and 75th percentiles, respectively, and whiskersextend to 1.5 times the height of the box; the points represent outliers,while the asterisks indicate extreme outliers
Table 2 Associations between KLK6mRNA expression status and otherclinicopathological variables
Variable Total Number of patients (%) p value
KLK6-negativea KLK6-positivea
Tb
T1/T2 17 11 (64.7) 6 (35.3) 0.024c
T3 64 28 (43.8) 36 (56.2)
T4 29 7 (24.1) 22 (75.9)
Mb
M0 98 45 (45.9) 53 (54.1) 0.013d
M1 12 1 (8.3) 11 (91.7)
TNM stageb
I 14 9 (64.3) 5 (35.7) 0.019c
II 46 17 (37.0) 29 (63.0)
III 38 19 (50.0) 19 (50.0)
IV 12 1 (8.3) 11 (91.7)
Abbreviations: T depth of tumor invasion, N nodal status, M distantmetastasisa Cutoff point 30.98 RQU, equal to the 42th percentileb TNM classification system (7th edition)c Calculated by chi-square (χ2 ) testd Calculated by Fisher’s exact test
4678 Tumor Biol. (2014) 35:4673–4685

With regard to OS, Kaplan–Meier survival curves illustrat-ed that colorectal adenocarcinoma patients with KLK6-posi-tive tumors had significantly smaller survival probabilities(p=0.005) than patients with KLK6-negative colorectal ade-nocarcinoma (Fig. 2b). Univariate Cox regression analysisclearly demonstrated that KLK6 mRNA expression predictspoor OS in colorectal adenocarcinoma, as KLK6-positive pa-tients were at a 3.6-fold higher risk of death, compared toKLK6-negative patients (HR=3.63, 95 % CI=1.37–9.60, p=0.009). Furthermore, multivariate analysis demonstrated thatKLK6mRNA expression is a significant predictor of poor OS(HR=3.65, 95%CI=1.27–10.46, p=0.016), independently ofpatient gender, age, tumor size, location, histological subtype,grade, venous invasion, lymphatic invasion, TNM stage, ra-diotherapy, and/or chemotherapy treatment (Table 4).
Prognostic value of KLK6 mRNA expressionin node-negative and metastasis-free colorectaladenocarcinoma
Colorectal adenocarcinoma patients with negative regionallymph nodes (N0) as well as without metastases at distantorgans (M0) have substantially different prognosis from node-positive (N1 or N2) and metastasis-positive (M1) patients,respectively. For this purpose, we also investigated the prog-nostic significance ofKLK6mRNA expression regarding DFSand OS in subgroups of patients, stratified according to theaforementioned clinicopathological parameters. Thus,Kaplan–Meier survival analysis revealed that N0 patients withcolorectal tumors that were positive for KLK6mRNA tendedto relapse and/or die earlier than N0 patients with KLK6-negative malignant neoplasms (p=0.026 and 0.042, respec-tively, Fig. 3a, b). In addition, M0 patients withKLK6-positiveadenocarcinomas had more unfavorable DFS and OS ratesthan did M0 patients bearing KLK6-negative tumors (p=0.012and 0.011, respectively, Fig. 3c, d).
Discussion
The carcinogenesis in the colon and rectum is a multistepprocess comprising mutations and/or alterations in the meth-ylation pattern of proto-oncogenes and tumor-suppressorgenes, impaired apoptosis, and deregulated expression ofmany cancer-related genes. All these molecular changes resultin aberrant cell growth and proliferation [41]. Peptidases exertcritical actions in colorectal carcinogenesis due to their abilityto cleave ECM proteins, thus promoting tumor cell invasionand metastasis [42]. Degradation of ECM and non-ECMcomponents by peptidases such as KLK family membersconfers alterations to the tumor microenvironment, whichaffect tumor cell behavior and characteristics, including lossof differentiation, enhanced tumor aggressiveness, angiogen-esis, and metastasis [10]. In general, the expression of KLKs isderegulated in many malignancies, including colorectal can-cer [19, 43, 44], gastric adenocarcinoma [26, 45], pancreaticductal adenocarcinoma [46, 47], and esophageal cancer [48,49]. Expression patterns and levels of KLK family membershave been noticed in primary malignant tumors arising insteroid hormone-regulated tissues (prostate, breast, and ova-ry), compared to normal, benign, and premalignant specimensof the same tissue origin [50-52].
KLK6 was originally discovered in an attempt to identifynovel serine proteases with aberrant expression in ovariancarcinoma cells [53]. Thereafter, a lot of research work result-ed in the establishment of KLK6 as a very promising molec-ular biomarker in ovarian cancer, with unfavorable prognosticvalue. The significant association of elevated KLK6 levelswith aggressive phenotypes of ovarian carcinoma and poorpatient outcome has been corroborated by several studiesusing serum and/or ovarian tissue specimens and employingdistinct research strategies [23, 54-58]. Besides its clinicalimportance as a biomarker in ovarian cancer, KLK6 geneexpression has been suggested as a solid unfavorable
Fig. 2 Kaplan–Meier disease-free survival (DFS) and overallsurvival (OS) of patients withKLK6mRNA-positive andmRNA-negative colorectaladenocarcinomas. KLK6mRNAexpression was shown to have anunfavorable prognostic value forthe DFS (a) and OS (b), aspatients with KLK6-positivecolorectal tumors havesignificantly shorter DFS and OSintervals, compared to those withKLK6-negative tumors
Tumor Biol. (2014) 35:4673–4685 4679

prognostic biomarker in uterine serous papillary cancer [25],gastrointestinal cancer [26, 59], nonsmall cell lung cancer[60], renal cell carcinoma [61], and pancreatic ductal adeno-carcinoma [47].
To the best of our knowledge, the current study is the firstto show that KLK6 mRNA expression is an independentpredictor of short-term relapse in colorectal adenocarcinoma.A previously described quantitative analysis of KLK6mRNAexpression in cancerous colorectal tissue specimens from 63CRC patients had shown that KLK6 mRNA positivity couldpredict poor OS, but it had not analyzed its prognostic signif-icance in terms of DFS [24]. Furthermore, high KLK6 proteinexpression detected by IHC predicted—independently fromother clinicopathological factors—unfavorable rates ofrecurrence-free survival and OS in CRC patients [59, 62].Taking into consideration that other KLK genes too have beensuggested as molecular prognostic biomarkers in colorectal
adenocarcinoma [63], that lymph node KLK6mRNA positiv-ity has been suggested as an indicator of poor outcome inCRC [64], and that the KLK6 protein is dramaticallyoverexpressed in malignant colorectal tumors compared tonormal colorectal epithelia [15, 62], we decided to quantifyand compare the levels of KLK6mRNA present in malignantneoplasms and matched noncancerous colorectal tissuesresected from patients with colorectal adenocarcinoma, inorder to assess potential associations between KLK6 mRNAstatus and established prognostic factors in colorectal adeno-carcinoma and to assess its prognostic significance in thismalignancy. For this purpose, an accurate and sensitive qPCRmethodology was developed and used for KLK6 mRNAquantification, followed by advanced biostatistics. At thispoint, we should note that we focused on expression analysisof mRNA and not protein expression of the KLK6 gene, as35 % of the specimens included in our study were rectal
Table 3 KLK6mRNA expres-sion and disease-free survival(DFS) of patients with colorectaladenocarcinoma
Abbreviations:HRhazard ratio,CIconfidence interval, T depth oftumor invasion, N nodal statusa HR estimated from Cox propor-tional hazard regression modelb CI of the estimated HRc Multivariate Cox regressionmodels were adjusted for patientage and gender, tumor size andlocation, histological subtype andgrade, venous and lymphatic in-vasion grade, T, N, radiotherapy,and chemotherapyd WHO classification (fourthedition)e TNM classification system (sev-enth edition)
Covariate DFS
HRa 95 % CIb p value HRa 95 % CIb p valueUnivariate analysis (N=96) Multivariate analysisc (N=95)
KLK6mRNA expression
Negative 1.00 1.00
Positive 3.67 1.50–9.00 0.004 4.47 1.58–12.64 0.005
Gender
Male
Female 0.83 0.40–1.71 0.61 0.97 0.41–2.29 0.95
Age 1.01 0.98–1.04 0.57 1 0.96–1.05 0.89
Tumor size 1.01 0.84–1.22 0.91 0.93 0.72–1.21 0.60
Tumor location
Colon
Rectum 1.76 0.86–3.61 0.12 3.06 1.11–8.45 0.030
Histological subtyped
Adenocarcinoma (nonmucinous)
Mucinous adenocarcinoma 0.45 0.11–1.89 0.28 0.34 0.07–1.66 0.18
Grade (ordinal)d 2.1 1.01–4.38 0.048 1.48 0.68–3.18 0.32
Venous invasion
No
Yes 2.48 0.95–6.53 0.065 0.97 0.27–3.51 0.96
Lymphatic invasion
No
Yes 2.03 0.78–5.34 0.15 2.18 0.61–7.70 0.23
T (ordinal)e 2.84 1.53–5.29 0.001 3.16 1.42–7.03 0.005
N (ordinal)e 1.67 1.06–2.64 0.028 1.43 0.77–2.69 0.26
Radiotherapy
No
Yes 1.21 0.49–2.96 0.68 0.51 0.14–1.88 0.31
Chemotherapy
No
Yes 1.49 0.68–3.27 0.32 1.32 0.46–3.76 0.61
4680 Tumor Biol. (2014) 35:4673–4685

adenocarcinomas and KLK6 protein expression in CRC hadbeen analyzed before bymeans of immunohistochemistry [59,62]. Besides that, the objectiveness of KLK6mRNA quantifi-cation using a validated qPCR methodology described in thecurrent study is more advantageous than the immunohisto-chemical assessment of KLK6 protein expression. On theother hand, IHC can be complementary to qPCR, since thelatter is used to quantify also noncoding splice variants whichdo not encode functional protein isoforms.
In accordance with the findings of a previously publishedstudy [24], transcription of the KLK6 gene was found to bevery elevated in colorectal adenocarcinomas, compared toadjacent noncancerous colorectal tissues, similar to KLK4[65], KLK7 [43, 66, 67], KLK10 [44, 68, 69], KLK11 [20],and KLK14 [66]. Interestingly, the dramatic upregulation ofKLK6 gene expression in malignant colorectal tumors (com-pared to their noncancerous counterparts) along with its pro-gressive increase in parallel with the depth of tumor invasion
(T) indicate that KLK6 is likely to be involved in the progres-sion of colorectal adenocarcinoma. Besides its associationwith high tumor invasiveness, KLK6 mRNA overexpressionwas associated with the presence of distant metastases, likeKLK7 [43, 67]. KLK6mRNA positivity is also more frequentin advanced stage colorectal adenocarcinoma than in earlystage disease, like KLK7, KLK10, and KLK14 [66-69]. Onthe other hand, KLK11mRNA expression status did not seemto be significantly associated with tumor location and histol-ogy, venous and lymphatic invasion, and patient nodal status[20].
Despite the fact that this study cannot demonstrate a cause-and-effect relationship between KLK6mRNA expression andtumor aggressiveness, it implies that KLK6 might favor colo-rectal adenocarcinoma cell metastasis. This could be attributedto E-cadherin shedding by KLK6, an in vivo mechanismwhich has been shown to promote cell proliferation, migra-tion, and invasion [70]. Proteolytic activation of PAR2 by
Table 4 KLK6mRNA expres-sion and overall survival (OS) ofpatients with colorectaladenocarcinoma
Abbreviations: HR hazard ratio,CI confidence intervala HR estimated from Cox propor-tional hazard regression modelb CI of the estimated HRc Multivariate Cox regressionmodels were adjusted for patientage and gender, tumor size andlocation, histological subtype andgrade, venous and lymphatic in-vasion grade, TNM stage, radio-therapy, and chemotherapyd WHO classification (fourthedition)e TNM classification system (sev-enth edition)
Covariate OS
HRa 95 % CIb p value HRa 95 % CIb p valueUnivariate analysis (N=96) Multivariate analysisc (N=95)
KLK6mRNA expression
Negative 1.00 1.00
Positive 3.63 1.37–9.60 0.009 3.65 1.27–10.46 0.016
Gender
Male 1.00 1.00
Female 0.88 0.41–1.89 0.74 1.06 0.44–2.54 0.89
Age 1.03 0.99–1.06 0.14 1.04 0.99–1.08 0.13
Tumor size 0.94 0.77–1.16 0.58 0.9 0.72–1.14 0.39
Tumor location
Colon 1.00 1.00
Rectum 1.9 0.89–4.05 0.098 3.59 1.28–10.05 0.015
Histological subtyped
Adenocarcinoma (nonmucinous) 1.00 1.00
Mucinous adenocarcinoma 0.51 0.12–2.14 0.35 1.2 0.24–5.89 0.82
Grade (ordinal)d 1.85 0.82–4.20 0.14 1.38 0.58–3.30 0.47
Venous invasion
No 1.00 1.00
Yes 3.19 1.19–8.53 0.021 4.3 1.15–16.02 0.030
Lymphatic invasion
No 1.00 1.00
Yes 1.71 0.59–4.98 0.32 0.65 0.14–2.97 0.58
TNM stage (ordinal)e 2 1.22–3.30 0.006 2.76 1.44–5.30 0.002
Radiotherapy
No 1.00 1.00
Yes 1.1 0.41–2.93 0.85 0.46 0.12–1.81 0.26
Chemotherapy
No 1.00 1.00
Yes 1.13 0.51–2.46 0.77 0.56 0.17–1.91 0.36
Tumor Biol. (2014) 35:4673–4685 4681

KLK6 could also account for this apparent promotion ofmetastasis [71-73]. In line with the aforementioned results,Cox univariate regression analysis showed that high KLK6mRNA expression in this malignancy predicts an increasedrisk of recurrence and death, and Kaplan–Meier survivalanalysis revealed significantly lower DFS and OS rates forKLK6-positive patients. Interestingly, the unfavorable prog-nostic significance of KLK6 is independent of biological andclinicopathological features of colorectal adenocarcinoma pa-tients, including patient gender, age, tumor size, location,histological subtype, grade, venous and lymphatic invasion,TNM staging parameters, radiotherapy, and chemotherapytreatment, as shown by the developed multivariate regressionmodel.
In terms of DFS, our results are reminiscent of the prog-nostic potential of KLK4 and KLK11, which can predict short-term relapse in colorectal adenocarcinoma patients indepen-dently of other established prognostic factors [19, 20]. Inaddition to KLK4 and KLK11, three other members of theKLK family, namely KLK7, KLK10, and KLK14, have recent-ly been demonstrated to predict low DFS probabilities in CRC
patients, albeit not independently of any clinicopathologicalcharacteristics of the colorectal adenocarcinoma [44, 66, 67,69]. Therefore, among allKLKgenes that have been studied atthe mRNA level in colorectal adenocarcinoma, KLK4, KLK6,and KLK11mRNA positivities are the only independent pre-dictors of DFS. However, the multivariate regression analysisfor KLK4mRNA expression status did not include importantparameters such as patient age, tumor location and histologi-cal subtype, venous and lymphatic invasion, and—perhapsmost importantly—radiotherapy and chemotherapy treatmentof patients [19], in contrast with the multivariate regressionanalysis for KLK6 mRNA status presented in the currentstudy. Regarding the prognostic value of KLK11 mRNA ex-pression status, although it was independent of all these pa-rameters, its statistical significance was marginal (p=0.048)[20]. Therefore, the prognostic power of KLK6 mRNA ex-pression appears to be superior to the ones of KLK4 andKLK11.
With regard to OS, our results agree with those of Ogawaet al. [24], showing the unfavorable prognostic value of KLK6mRNA positivity in colorectal adenocarcinoma. However, our
Fig. 3 Kaplan–Meier disease-free survival (DFS) and overallsurvival (OS) curves for distinctsubgroups of colorectaladenocarcinoma patients. KLK6mRNA expression predicts poorDFS (a) and OS (b) in patientswith negative nodal status, asnode-negative patients withKLK6mRNA-positive tumors tend torelapse and/or die earlier thannode-negative patients withKLK6mRNA-negative tumors. Theprognosis of metastasis-freepatients, with regard to both DFS(c) and OS (d), was significantlyworse for those with KLK6mRNA-positiveadenocarcinomas than for thosewith KLK6mRNA-negativetumors
4682 Tumor Biol. (2014) 35:4673–4685

study shows, for the first time, that this prognostic significanceis independent of biological and clinicopathological featuresof colorectal adenocarcinoma patients, including patient gen-der and age, tumor size and location, histological subtype,grade, venous and lymphatic invasion, and TNM stage. Itshould be also noted that although other KLKs too—KLK7[43, 66, 67], KLK10 [44], KLK11 [20], and KLK14 [66]—areindependent prognosticators of OS, KLK6mRNA expressionis probably the most important prognosticator, since it doesnot depend on radiotherapy and/or chemotherapy treatment ofpatients.
In addition, KLK6 mRNA overexpression detected in co-lorectal tumors of patients with metastases either in regionallymph nodes (N0) or at distant sites (M0) was shown tostrongly predict poor DFS and OS, compared to similar (N0or M0) patients with KLK6 mRNA-negative colorectal ade-nocarcinoma. Undoubtedly, it would be very interesting tocombine KLK6 with KLK4 in a prognostic model regardingDFS, since high KLK4 mRNA levels predict short-term re-lapse in patients with negative lymph nodes and/or early stagedisease [19].
In conclusion, our study is the first to show that KLK6mRNA expression can be regarded as an independent unfa-vorable prognosticator of DFS and OS in colorectal adenocar-cinoma patients. Interestingly, KLK6 mRNA expression pre-dicts short DFS and OS intervals, independently of biologicaland clinicopathological features of patients as well as of theradiotherapy or chemotherapy treatment they may receive.Undoubtedly, further investigation in larger cohorts of patientsis needed to answer whether KLK6mRNA expression can beused in clinical practice as a molecular tissue biomarker ofunfavorable prognosis in colorectal adenocarcinoma. Our on-going work includes medium-scale analysis of mRNA expres-sion of all alternative transcripts produced by the members ofthe KLK gene family in colorectal adenocarcinoma by meansof semiconductor sequencing, validation of the most strikingdifference in the expression profiles of colorectal adenocarci-noma and noncancerous colorectal tissue, and the study oftheir combinatorial prognostic value by buildingmultiparametric panels of molecular prognostic biomarkers.
Conflicts of interest None.
References
1. Bray F, Jemal A, Grey N, Ferlay J, Forman D. Global cancertransitions according to the human development index (2008–2030): a population-based study. Lancet Oncol. 2012;13:790–801.
2. Duffy MJ. Carcinoembryonic antigen as a marker for colorectalcancer: is it clinically useful? Clin Chem. 2001;47:624–30.
3. Locker GY, Hamilton S, Harris J, et al. ASCO 2006 update ofrecommendations for the use of tumor markers in gastrointestinalcancer. J Clin Oncol. 2006;24:5313–27.
4. Selby JV, Friedman GD, Quesenberry Jr CP, Weiss NS. A case–control study of screening sigmoidoscopy and mortality from colo-rectal cancer. N Engl J Med. 1992;326:653–7.
5. Yousef GM, Chang A, Scorilas A, Diamandis EP. Genomic organi-zation of the human kallikrein gene family on chromosome 19q13.3-q13.4. Biochem Biophys Res Commun. 2000;276:125–33.
6. Puente XS, Sanchez LM, Overall CM, Lopez-Otin C. Human andmouse proteases: a comparative genomic approach. Nat Rev Genet.2003;4:544–58.
7. Kontos CK, Scorilas A. Kallikrein-related peptidases (KLKs): a genefamily of novel cancer biomarkers. Clin Chem Lab Med. 2012;50:1877–91.
8. Emami N, Diamandis EP. New insights into the functional mecha-nisms and clinical applications of the kallikrein-related peptidasefamily. Mol Oncol. 2007;1:269–87.
9. Scarisbrick IA, Radulovic M, Burda JE, et al. Kallikrein 6 is a novelmolecular trigger of reactive astrogliosis. Biol Chem. 2012;393:355–67.
10. Borgono CA, Diamandis EP. The emerging roles of human tissuekallikreins in cancer. Nat Rev Cancer. 2004;4:876–90.
11. Ramsay AJ, Reid JC, Adams MN, et al. Prostatic trypsin-likekallikrein-related peptidases (KLKs) and other prostate-expressedtryptic proteinases as regulators of signalling via proteinase-activated receptors (PARs). Biol Chem. 2008;389:653–68.
12. Nishibori M, Mori S, Takahashi HK. Physiology and pathophysiol-ogy of proteinase-activated receptors (PARs): Par-2-mediated prolif-eration of colon cancer cell. J Pharmacol Sci. 2005;97:25–30.
13. Gratio V, Beaufort N, Seiz L, et al. Kallikrein-related peptidase 4: anew activator of the aberrantly expressed protease-activated receptor1 in colon cancer cells. Am J Pathol. 2010;176:1452–61.
14. Macfarlane SR, Seatter MJ, Kanke T, Hunter GD, Plevin R.Proteinase-activated receptors. Pharmacol Rev. 2001;53:245–82.
15. Talieri M, Li L, Zheng Y, et al. The use of kallikrein-related pepti-dases as adjuvant prognostic markers in colorectal cancer. Br JCancer. 2009;100:1659–65.
16. Gratio V, Loriot C, Virca GD, et al. Kallikrein-related peptidase 14acts on proteinase-activated receptor 2 to induce signaling pathway incolon cancer cells. Am J Pathol. 2011;179:2625–36.
17. Kontos CK,Mavridis K, Talieri M, A S. Kallikrein-related peptidases(KLKs) in gastrointestinal cancer: mechanistic and clinical aspects.Thromb Haemost. 2013;109: doi: 10.1160/TH12-11-0791.
18. AlexopoulouDK, Papadopoulos IN, Scorilas A. Clinical significanceof kallikrein-related peptidase (KLK10) mRNA expression in colo-rectal cancer. Clin Biochem. 2013.
19. Kontos CK, Chantzis D, Papadopoulos IN, Scorilas A. Kallikrein-related peptidase 4 (KLK4) mRNA predicts short-term relapse incolorectal adenocarcinoma patients. Cancer Lett. 2013;330:106–12.
20. Alexopoulou DK, Kontos CK, Christodoulou S, Papadopoulos IN,Scorilas A. Kallikrein-related peptidase-11 (KLK11) mRNA expres-sion predicts poor disease-free and overall survival in colorectaladenocarcinoma patients. Biomark Med. 2014 (in press).
21. Henkhaus RS, Gerner EW, Ignatenko NA. Kallikrein 6 is a mediatorof K-RAS-dependent migration of colon carcinoma cells. Biol Chem.2008;389:757–64.
22. Henkhaus RS, Roy UK, Cavallo-Medved D, Sloane BF, Gerner EW,Ignatenko NA. Caveolin-1-mediated expression and secretion ofkallikrein 6 in colon cancer cells. Neoplasia. 2008;10:140–8.
23. Diamandis EP, Scorilas A, Fracchioli S, et al. Human kallikrein 6(hK6): a new potential serum biomarker for diagnosis and prognosisof ovarian carcinoma. J Clin Oncol. 2003;21:1035–43.
24. Ogawa K, Utsunomiya T, Mimori K, et al. Clinical significance ofhuman kallikrein gene 6 messenger RNA expression in colorectalcancer. Clin Cancer Res. 2005;11:2889–93.
Tumor Biol. (2014) 35:4673–4685 4683

25. Santin AD, Diamandis EP, Bellone S, et al. Human kallikrein 6: anew potential serum biomarker for uterine serous papillary cancer.Clin Cancer Res. 2005;11:3320–5.
26. Nagahara H, Mimori K, Utsunomiya T, et al. Clinicopathologic andbiological significance of kallikrein 6 overexpression in human gas-tric cancer. Clin Cancer Res. 2005;11:6800–6.
27. Ghosh MC, Grass L, Soosaipillai A, Sotiropoulou G, Diamandis EP.Human kallikrein 6 degrades extracellular matrix proteins and mayenhance the metastatic potential of tumour cells. Tumour Biol.2004;25:193–9.
28. Vandell AG, Larson N, Laxmikanthan G, et al. Protease-activatedreceptor dependent and independent signaling by kallikreins 1 and 6in CNS neuron and astroglial cell lines. J Neurochem. 2008;107:855–70.
29. Yoon H, RadulovicM,Wu J, et al. Kallikrein 6 signals through PAR1and PAR2 to promote neuron injury and exacerbate glutamate neu-rotoxicity. J Neurochem. 2013;127:283–98.
30. Krenzer S, Peterziel H, Mauch C, et al. Expression and function ofthe kallikrein-related peptidase 6 in the human melanoma microen-vironment. J Investig Dermatol. 2011;131:2281–8.
31. Darmoul D, Gratio V, Devaud H, Laburthe M. Protease-activatedreceptor 2 in colon cancer: trypsin-induced MAPK phosphorylationand cell proliferation are mediated by epidermal growth factor recep-tor transactivation. J Biol Chem. 2004;279:20927–34.
32. Darmoul D, Gratio V, Devaud H, Lehy T, Laburthe M. Aberrantexpression and activation of the thrombin receptor protease-activatedreceptor-1 induces cell proliferation and motility in human coloncancer cells. Am J Pathol. 2003;162:1503–13.
33. Heider I, Schulze B, Oswald E, Henklein P, Scheele J, Kaufmann R.Par1-type thrombin receptor stimulates migration and matrix adhe-sion of human colon carcinoma cells by a pkcepsilon-dependentmechanism. Oncol Res. 2004;14:475–82.
34. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL. Trotti A(eds): AJCC cancer staging manual, ed 7th. New York: Springer;2010.
35. Livak KJ, Schmittgen TD. Analysis of relative gene expression datausing real-time quantitative PCR and the 2(−Delta Delta C(T)) meth-od. Methods. 2001;25:402–8.
36. Kheirelseid EA, Chang KH, Newell J, Kerin MJ, Miller N.Identification of endogenous control genes for normalisation ofreal-time quantitative PCR data in colorectal cancer. BMC MolBiol. 2010;11:12.
37. Dydensborg AB, Herring E, Auclair J, Tremblay E, Beaulieu JF.Normalizing genes for quantitative RT-PCR in differentiating hu-man intestinal epithelial cells and adenocarcinomas of thecolon. Am J Physiol Gastrointest Liver Physiol. 2006;290:G1067–74.
38. Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res. 2004;10:7252–9.
39. Kaplan EL, Meier P. Nonparametric observation from incompleteobservations. J Am Stat Assoc. 1958;53:457–81.
40. Cox DR. Regression models and life Tables. J R Stat Soc Series BStat Methodol. 1972;34:187–202.
41. Chung DC. The genetic basis of colorectal cancer: insights intocritical pathways of tumorigenesis. Gastroenterology. 2000;119:854–65.
42. Mook OR, Frederiks WM, Van Noorden CJ. The role of gelatinasesin colorectal cancer progression and metastasis. Biochim BiophysActa. 2004;1705:69–89.
43. Inoue Y, Yokobori T, Yokoe T, et al. Clinical significance of humankallikrein7 gene expression in colorectal cancer. Ann Surg Oncol.2010;17:3037–42.
44. AlexopoulouDK, Papadopoulos IN, Scorilas A. Clinical significanceof kallikrein-related peptidase (KLK10) mRNA expression in colo-rectal cancer. Clin Biochem. 2013;46:1453–61.
45. Florou D,Mavridis K, Scorilas A. The kallikrein-related peptidase 13(KLK13) gene is substantially up-regulated after exposure of gastriccancer cells to antineoplastic agents. Tumour Biol. 2012;33:2069–78.
46. Linardoutsos D, AvgerisM, Bramis J, Zografos GC, A. S: Expressionanalysis of kallikrein-related peptidase 4 gene (KLK4) in pancreaticcancer. In: Scorilas A (ed): 4th International symposium on kalli-kreins and kallikrein-related peptidases. Rhodes, Greece, 2011.
47. Ruckert F, Hennig M, Petraki CD, et al. Co-expression of KLK6 andKLK10 as prognostic factors for survival in pancreatic ductal adeno-carcinoma. Br J Cancer. 2008;99:1484–92.
48. Dlamini Z, Bhoola KD. Upregulation of tissue kallikrein, kinin B1receptor, and kinin B2 receptor in mast and giant cells infiltratingoesophageal squamous cell carcinoma. J Clin Pathol. 2005;58:915–22.
49. Yousef GM, Borgono CA, White NM, et al. In silico analysis of thehuman kallikrein gene 6. Tumour Biol. 2004;25:282–9.
50. Avgeris M, Mavridis K, Scorilas A. Kallikrein-related peptidases inprostate, breast, and ovarian cancers: from pathobiology to clinicalrelevance. Biol Chem. 2012;393:301–17.
51. Sidiropoulos M, Pampalakis G, Sotiropoulou G, Katsaros D,Diamandis EP. Downregulation of human kallikrein 10 (KLK10/NES1) by CpG island hypermethylation in breast, ovarian and pros-tate cancers. Tumour Biol. 2005;26:324–36.
52. Pampalakis G, Sotiropoulou G. Multiple mechanisms underlie theaberrant expression of the human kallikrein 6 gene in breast cancer.Biol Chem. 2006;387:773–82.
53. Tanimoto H, Underwood LJ, Shigemasa K, Parmley TH, O’Brien TJ.Increased expression of protease m in ovarian tumors. Tumour Biol.2001;22:11–8.
54. Kountourakis P, Psyrri A, Scorilas A, et al. Prognostic value ofkallikrein-related peptidase 6 protein expression levels in advancedovarian cancer evaluated by automated quantitative analysis(AQUA). Cancer Sci. 2008;99:2224–9.
55. Hoffman BR, Katsaros D, Scorilas A, et al. Immunofluorometricquantitation and histochemical localisation of kallikrein 6 protein inovarian cancer tissue: a new independent unfavourable prognosticbiomarker. Br J Cancer. 2002;87:763–71.
56. Shan SJ, Scorilas A, Katsaros D, Diamandis EP. Transcriptionalupregulation of human tissue kallikrein 6 in ovarian cancer: clinicaland mechanistic aspects. Br J Cancer. 2007;96:362–72.
57. White NM, Mathews M, Yousef GM, Prizada A, Popadiuk C, DoreJJ. KLK6 and KLK13 predict tumor recurrence in epithelial ovariancarcinoma. Br J Cancer. 2009;101:1107–13.
58. Diamandis EP, Yousef GM, Soosaipillai AR, Bunting P. Humankallikrein 6 (zyme/protease m/neurosin): a new serum biomarker ofovarian carcinoma. Clin Biochem. 2000;33:579–83.
59. Petraki C, Dubinski W, Scorilas A, et al. Evaluation and prognosticsignificance of human tissue kallikrein-related peptidase 6 (KLK6) incolorectal cancer. Pathol Res Pract. 2012;208:104–8.
60. Nathalie HV, Chris P, Serge G, et al. High kallikrein-related peptidase6 in non-small cell lung cancer cells: an indicator of tumour prolifer-ation and poor prognosis. J Cell Mol Med. 2009;13:4014–22.
61. Petraki CD, Gregorakis AK, Vaslamatzis MM, et al. Prognosticimplications of the immunohistochemical expression of human kal-likreins 5, 6, 10 and 11 in renal cell carcinoma. Tumour Biol.2006;27:1–7.
62. Kim JT, Song EY, Chung KS, et al. Up-regulation and clinicalsignificance of serine protease kallikrein 6 in colon cancer. Cancer.2011;117:2608–19.
63. Avgeris M, Mavridis K, Scorilas A. Kallikrein-related peptidasegenes as promising biomarkers for prognosis and monitoring ofhuman malignancies. Biol Chem. 2010;391:505–11.
64. Ohlsson L, Lindmark G, Israelsson A, et al. Lymph node tissuekallikrein-related peptidase 6 mRNA: a progression marker for colo-rectal cancer. Br J Cancer. 2012;107:150–7.
4684 Tumor Biol. (2014) 35:4673–4685

65. Kontos CK, Chantzis D, Papadopoulos IN, Scorilas A. Quantitativeexpression analysis and prognostic significance of KLK4 mRNAexpression in colon cancer; in Schmitt M, Fritz H, Sommerhoff CP,Magdolen V (eds): 3rd International symposium on kallikreins andkallikrein-related peptidases Munich, Germany, Hieronymus Druckund Verlag, 2009, pp 86.
66. Devetzi M, Trangas T, Scorilas A, Xynopoulos D, Talieri M. Paralleloverexpression and clinical significance of kallikrein-related pepti-dases 7 and 14 (KLK7KLK14) in colon cancer. Thromb Haemost.2013;109:716–25.
67. Talieri M, Mathioudaki K, Prezas P, et al. Clinical significance ofkallikrein-related peptidase 7 (KLK7) in colorectal cancer. ThrombHaemost. 2009;101:741–7.
68. Feng B, Xu WB, Zheng MH, et al. Clinical significance of humankallikrein 10 gene expression in colorectal cancer and gastric cancer.J Gastroenterol Hepatol. 2006;21:1596–603.
69. Talieri M, Alexopoulou DK, Scorilas A, et al. Expression analysisand clinical evaluation of kallikrein-related peptidase 10 (KLK10) incolorectal cancer. Tumour Biol. 2011;32:737–44.
70. Klucky B, Mueller R, Vogt I, et al. Kallikrein 6 induces E-cadherinshedding and promotes cell proliferation, migration, and invasion.Cancer Res. 2007;67:8198–206.
71. Oikonomopoulou K, Hansen KK, Saifeddine M, et al. Proteinase-activated receptors, targets for kallikrein signaling. J Biol Chem.2006;281:32095–112.
72. Oikonomopoulou K, Hansen KK, Saifeddine M, et al. Proteinase-mediated cell signalling: targeting proteinase-activated recep-tors (PARS) by kallikreins and more. Biol Chem. 2006;387:677–85.
73. Angelo PF, Lima AR, Alves FM, et al. Substrate specificity of humankallikrein 6: salt and glycosaminoglycan activation effects. J BiolChem. 2006;281:3116–26.
Tumor Biol. (2014) 35:4673–4685 4685