
Three-dimensional cartilage tissue engineering using adult stem cells from osteoarthritis patients
Upload
umcutrechtCategory
view
3download
0
435ISSN 1750-743XImmunotherapy (2009) 1(3), 435–44510.2217/IMT.09.14 © 2009 Future Medicine Ltd
Review
Joint injury and osteoarthritis: soluble mediators in the course and treatment of cartilage pathology
Cytokines provide a network controlling both innate and specific immune responses [1]. In addi-tion, they may be involved in tissue degradation, for example, during remodeling of the periodontal ligament [2,3], wound healing [4], corneal destruc-tion following keratitis [5] or bone loss during osteolytic pathologies [6]. In cartilage pathology, the relatively low turnover and remodeling of car-tilage matrix components [7] is disturbed, result-ing in a net loss of cartilage matrix components and deterioration of structural and functional properties of the cartilage [8]. Cytokines contrib-ute to this process by stimulation and produc-tion of proteolytic enzymes and other catabolic cytokines [9], or by inhibiting proteoglycan [10] or collagen synthesis [11]. In rheumatoid arthritis (RA), increased levels of proinflammatory cyto-kines in synovial fluid (SF) as compared with healthy SF [12,13] correlated with disease sever-ity [14]. Several cytokine-modulating therapies proved effective in reducing RA symptoms and disease progression [15–17]. Cytokines are also c onsidered to play an important part in the pathogenesis and progression of osteoarthritis (OA) [18–20]. In contrast with RA, which is con-sidered a chronic autoimmune disease [21], OA is more a ‘wear-related’ degenerative disorder. Moreover, the onset of OA can be accelerated after previous injury to the joint [22–25].
This review aims to discuss the role of cyto-kines in OA, and in traumatic joint injuries that predispose to development of early OA.
Players in the intra-articular environment � Cytokines
Cytokines are a category of soluble or cell surface molecules that play a role in cellular communica-tion through paracrine, autocrine and endocrine signaling [1]. In the intra-articular environment, cytokines and growth factors may diffuse from the SF towards chondrocytes, where they may bind to the cell surface and stimulate or inhibit the release of other proteins. Vice versa, chondro-cytes release cytokines and growth factors into the surrounding matrix, which are transferred into the SF in part through fluid flow generated by hydrostatic pressure in the course of load-ing the joint [9]. Although the majority of cyto-kines exert multiple effects on cartilage and are involved in a balance of stimulatory as well as inhibitory effects, a division can be made between cartilage-degrading, proinflammatory cytokines (catabolic, or ‘chondrodestructive’), cytokines with both destructive as well as protective func-tions (‘chondro modulatory’) [7] and cartilage-pro-tecting, anti-inflammatory cytokines (anabolic, a nticatabolic or ‘chondroprotective’) (Table 1).
Of the chondrodestructive cytokines, IL-1b
[26,27], TNF-a [28] and their synergistic inter-action have been studied most thoroughly [29,30]. These cytokines stimulate upregulation of vari-ous cartilage-degrading matrix-metalloprotein-ases (MMPs) [31], a process that leads to cleavage and subsequent loss of proteoglycans from the
Osteoarthritis is a disabling disease of the aging generation, which results in loss of quality of life and increased healthcare costs. Cytokines appear to play an important role in the cartilaginous degeneration characterizing the pathological process. Increasing experience is being gained with cytokine-modulating therapies aimed at interfering with effects of chondrodegradative cytokines in the synovial fluid. Although in vitro and in vivo effectiveness of several of these therapies has been demonstrated, clinical effectiveness remains disputable, which may be related to the low levels of inflammatory cytokines found in osteoarthritic joints. By contrast, directly after joint trauma, which has been shown to predipose to early osteoarthritis, synovial fluid cytokine levels are strongly increased. Cytokine-modulating therapies, however, have hardly been considered for this indication. Increased knowledge of intra-articular soluble mediators correlating with cartilage pathology will lead to further development of cytokine-modulating products and, eventually, to effective inhibition of cartilage degeneration, in both the osteoarthritic as well as injured joints.
Keywords: cartilage � cytokine � intra-articular trauma � osteoarthritis � synovial fluid
Marijn Rutgers1, Daniël BF Saris1, Kiem Gie Auw Yang1, Wouter JA Dhert1,2 & Laura B Creemers1† †Author for correspondence: 1University Medical Center Utrecht, Department of Orthopaedics, Heidelberglaan 100, 3584 CX Utrecht, The NetherlandsTel.: +31 887 558 077Fax: +31 302 510 [email protected] of Veterinary Medicine, Utrecht University, The Netherlands
For reprint orders, please contact: [email protected]

Immunotherapy (2009) 1(3)436 future science group
Review Rutgers, Saris, Auw Yang, Dhert & Creemers
extracellular matrix (ECM), while on the other hand, proteoglycan synthesis is inhibited [9,32]. IL-1a and IL-1b exhibit an amino acid homology of 22% and both bind to the biologically active IL-1 receptor (IL-1R), which leads to transcrip-tion of many proinflammatory genes, including IL‑6 and IL‑8 [33]. Although not as frequently studied as IL-1b, IL-1a is also present in OA SF, albeit at low concentrations [34]. Both cytokines are thought to exert more or less similar effects in cartilage degeneration [35] and are used inter-changeably in research. In this review, IL-1 may refer to either.
Other cytokines with chondrodestructive effects in the intra-articular environment are IFN-g [36], IL-17 [37] and oncostatin-M [38], which were shown to act synergistically with IL-1 in stimulation of production of MMPs and aggre-canases [39]. IL-7 production by osteo arthritic chondrocytes is higher in comparison with healthy chondrocytes [40] and may be involved in fibronectin fragment (Fn-f)-mediated osteo-arthritic degeneration. IL-8 has been shown to promote release of IL-6 [29] and promotes hyper-trophic differentiation [41]. Leukocyte-inhibitory factor (LIF), produced by activated T cells in the synovium, has been shown to enhance IL-1b and IL-8 production in chondrocytes [42].
Chondrodestructive [43] as well as chon-droprotective [29] actions have been described of IL-6. Its ‘chondromodulatory’ effects are mediated through increased production and attraction of inflammatory cells [44] on the one hand, and through stimulation of production of TGF-b [45] and tissue inhibitor of metallo-proteinases (TIMP)-1 [46] on the other hand. IL-6 production is stimulated by IL-1b [29,44]. Basic FGF (bFGF) may inhibit IGF-1-mediated proteoglycan production [47] and induce MMP expression [48], although it may also stimulate chondrocyte proliferation [49] as well as TIMP-1 production [48].
Anti-inflammatory cytokines, such as IL-4, -10 and -13 [50], were shown to have various effects, including inhibition of IL-1 and TNF-a secretion and stimulation of IL-1 receptor antag-onist (IL-1RA/IRAP) expression. IL-1RA com-petes with IL-1 in binding to the IL-1 receptor, and prevention of IL-1 binding inhibits activa-tion of target cells [33], thus inhibiting cartilage degradation (Table 1) [51–54]. Growth factors may also mediate proliferation or differentiation of chondrocytes. TGF-b, a so-called cysteine-knot cytokine [55], stimulates IL-1RA expression and proliferation and differentiation of chondrocytes
[56,57]; however, only few studies report on the presence of TGF-b in the intra-articular envi-ronment [12,58]. At high concentrations, TGF-b may lead to osteophyte formation [59]. IGF is considered as an important mediator in the repair of cartilage defects [60,61] as it is a potent mitogen and differentiation factor steering progenitor cells towards a cartilaginous path-way [62,63]. Osteoprotegerin [64,65] was found to stimulate IL-1RA expression, and increased levels have been reported in OA [66].
extracellular cartilage matrixIn addition to chondrocytes, cartilage consists of water, collagens and proteoglycans (the major constituents of the ECM) [67]. Proteoglycans are composed of a protein core with covalently bound glycosaminoglycan side chains, of which the most important are chondroitin sulfate and keratan sulfate [68]. Hyaluronic acid (HA) is an unsulfated glycosaminoglycan and, although it is not covalently bound to the protein core and thus not part of a proteoglycan, it is involved in forma-tion of proteoglycan aggregates through aggre-can–HA-link protein complexes [9]. Exchange of low-molecular-weight components (<20 kDa) between the cartilage matrix and SF is dependent on biomechanical loading [68]. However, proteo-lytic activity (observed in normal and in degen-erative cartilage) enables other, larger matrix components, such as proteoglycans and HA, to be cleaved into smaller fragments and released into the SF [9]. Fn-fs released following proteolytic activity play a direct role in cartilage turnover by either enhancing cartilage anabolic activity (at low concentrations) or stimulation of catabolic c ytokine release [40], upregulation of MMP e xpression and enhancing degradation of proteo-glycans [69]. Increased levels of Fn-fs in SF may be considered as a ‘signal’ of increased catabolism, and have been observed in patients with RA as well as OA [70]. In addition to cytokine-mediated car-tilage degeneration, it was recently demonstrated
Table 1. Chondrodestructive (proinflammatory), chondromodulatory and chondroprotective (anti-inflammatory, anabolic or anticatabolic) cytokines in the intra-articular environment.
Chondrodestructive Chondromodulatory Chondroprotective
IL-1a, IL-1b IL-6 IL-1RA
TNF-a Basic FGF IL-4
IL-7 IL-10
IL-8 IL-13
IL-17 TGF-bOncostatin M IGF-1
IFN-g Osteoprotegerin
Leukocyte-inhibitory factor
www.futuremedicine.com 437future science group
Joint injury & osteoarthritis Review
that activation of the discoidin domain receptor (DDR)-2 by native collagen plays a role through increased expression of the cartilage-degrading MMP-13 in cultured chondrocytes [71]. In addi-tion, DDR-2 protein was increased at the immu-nohistochemical level in the femoral heads of OA patients [72]. Of course, it cannot be excluded as yet that this activation of MMP-13 expression is mediated through autocrine cytokine signaling.
synoviumSynovial tissue consists of a synovial membrane (facing the joint capsule) and a fibrous layer con-taining loose connective tissue [9] and is the main contributor to changes in SF composition [73]. The synovial membrane consists of one or more layers of epitheloid cells, which covers a layer of fibrous tissue containing type A and type B cells [74]. The A cells resemble macrophages and can be released from the synovial membrane into the SF. The majority of the cells in the synovial membrane, however, are ‘B’ cells, which resem-ble fibroblasts and secrete proteins, glycoproteins and hyaluronic acid into the SF [75]. The fibrous tissue layer contains adipocytes, mast cells, nerve fibres, vascular endothelial cells and, occasion-ally, lymphocytes. Capillaries in the fibrous t issue layer enable exchange of nutrients.
synovial fluidThe composition and volume of SF varies between individuals and between different joints within an individual. The average healthy human knee con-tains between 1.1 and 6.7 ml [76,77] of SF, which is distributed over the surfaces of femoral and tib-ial articulating surfaces in a layer just 10–20 µm thick [9], throughout the joint cavity. Although leukocytes are usually only present at low con-centrations in SF, they have also been mentioned to contribute to intra-articular cytokine and growth factor levels [78]. Traumatic changes to the joint, for example rupture of an anterior cru-ciate ligament, meniscal tears or dis location of a cartilage or osteochondritis dissecans fragment, may change SF composition, either gradually following increased SF production by type B synovial cells, or rapidly through intra-articular hemorrhaging. In contrast to the relatively acel-lular healthy SF, blood contains high amounts of leukocytes, as well as erythrocytes and throm-bocytes. Breaching of the blood–SF barrier may affect SF composition, not only through entrance of erythrocytes, leukocytes and monocytes into the joint and subsequent cartilaginous damage
[79], but also through the presence of proinflam-matory cytokines in blood (Table 2).
synovial fluid content in oA The osteoarthritic joint demonstrates changes in cartilage, synovium, subchondral bone and SF [9,80]. Expression of IL-1 in chondrocytes is increased at the mRNA [81] level as well at the immunohistochemical level [82], but expression in the synovial membrane does not seem higher than in healthy individuals [80,83]. Although IL-1b is usually considered an important medi-ator for the OA development, low (<10 pg/ml) or undetectable IL-1b levels were found in sev-eral studies focusing on cytokine levels in SF of OA patients [12,78,84,85].
In general, the role of IL-1 in OA may have been overstated. Although it is commonly sug-gested that IL-1 exerts its effects at very low concentrations, either or not by synergy with other proinflammatory cytokines, there is not much support for this assumption. While there are studies that mention IL-1b concentrations of as low as 10 pg/ml to be capable of inhib-iting proteoglycan synthesis in vitro [86,87], commonly, IL-1b concentrations of at least 1000 pg/ml were necessary to induce c artilage damage. Studies demonstrating synergistic effects of IL-1b with IFN-g [36], TNF-a [30], IL-17 [88] or oncostatin-M [38] also depart from
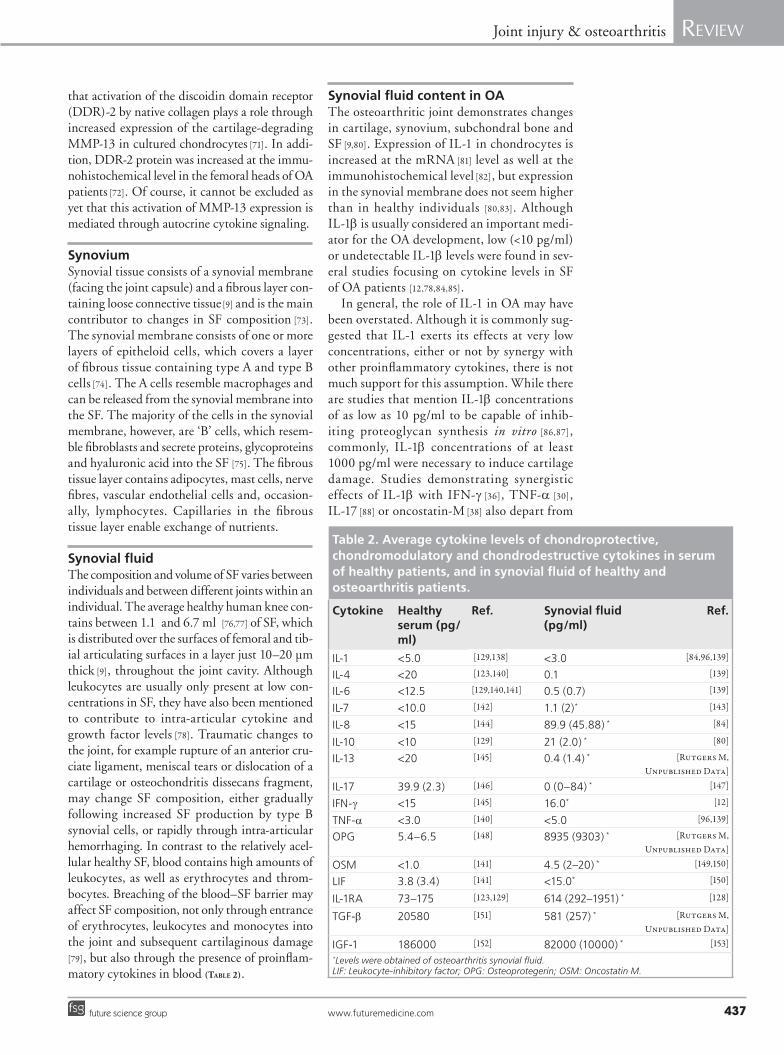
Table 2. Average cytokine levels of chondroprotective, chondromodulatory and chondrodestructive cytokines in serum of healthy patients, and in synovial fluid of healthy and osteoarthritis patients.
Cytokine Healthy serum (pg/ml)
ref. synovial fluid (pg/ml)
ref.
IL-1 <5.0 [129,138] <3.0 [84,96,139]
IL-4 <20 [123,140] 0.1 [139]
IL-6 <12.5 [129,140,141] 0.5 (0.7) [139]
IL-7 <10.0 [142] 1.1 (2)* [143]
IL-8 <15 [144] 89.9 (45.88) * [84]
IL-10 <10 [129] 21 (2.0) * [80]
IL-13 <20 [145] 0.4 (1.4) * [Rutgers M, Unpublished Data]
IL-17 39.9 (2.3) [146] 0 (0–84) * [147]
IFN-g <15 [145] 16.0* [12]
TNF-a <3.0 [140] <5.0 [96,139]
OPG 5.4–6.5 [148] 8935 (9303) * [Rutgers M, Unpublished Data]
OSM <1.0 [141] 4.5 (2–20) * [149,150]
LIF 3.8 (3.4) [141] <15.0* [150]
IL-1RA 73–175 [123,129] 614 (292–1951) * [128]
TGF-b 20580 [151] 581 (257) * [Rutgers M, Unpublished Data]
IGF-1 186000 [152] 82000 (10000) * [153]*Levels were obtained of osteoarthritis synovial fluid.LIF: Leukocyte-inhibitory factor; OPG: Osteoprotegerin; OSM: Oncostatin M.

Immunotherapy (2009) 1(3)438 future science group
Review Rutgers, Saris, Auw Yang, Dhert & Creemers
much higher IL-1b concentrations (100 pg/ml and higher) than in OA SF, which does not support a synergistic effect at low IL-1b levels. Animal models using IL-1b to induce OA also depart from concentrations 1000-fold higher than those found in OA SF [89,90], further supporting the need for high levels to induce intra-articular effects. In addition, study of OA in animals usually involves OA models in which onset of OA is ‘accelerated’, based on surgical [91] or biochemical [92] destruction of part of the cartilage, complete or incomplete meniscectomy [93] or transsection of a cruciate ligament [94,95]. Depending on the time after ‘induction’ of OA, this ‘OA model’ may, in fact, resemble a post-trauma situation rather than an OA s etting. Thus, the in vitro and in vivo models used for OA may not adequately simu-late human OA and overstate the importance of IL-1b. Similar remarks can be made regarding TNF-a, which is also low in OA SF [78].
In addition to IL-1a, increased production of IL-8 and IL-10 was observed in synovial membranes as well as in the cartilage and sub-chondral bone of patients with OA, while sub-chondral bone also expressed TNF-a, MMP-3, MMP-9 and TIMP-1 [80]. However, major increases in SF cytokine levels, as observed in patients with RA, are not observed in OA
[12,34,78,96]. It may, therefore, be that other SF components are responsible for cartilage degen-eration in OA, either alone or in combination with earlier mentioned cytokines. Although the OA SF concentrations of IL-1b and TNF-a alone do not seem high enough to induce cartilage degeneration, SF of patients with c hronically injured knees inhibited chondro-genesis in a chick limb bud bioassay, while SF of patients with acutely injured knees s timulated chondrogenesis [97].
synovial fluid content in acute traumaAcute trauma is associated with higher SF cytokine levels than the low levels found in OA patients. In vivo, intra-articular cytokine level changes following trauma have been studied following naturally acquired articular injuries [98–100], immobilization of a joint [101], biochemically induced injury [102], or mechani-cally induced intra-articular trauma [61,103]. In patients, cytokine levels after trauma have often been studied following rupture of the anterior cruciate ligament [25,104,105] or following menis-cus or cartilage trauma [97]. In both in vivo and clinical studies, high levels of a variety of cytokines were seen following intra-articular
trauma, often followed by a gradual decrease. In animals, IL-6 levels most frequently increased [98,100] as well as IL-1b, TNF-a, MMP-3 [98] and TGF-b [103]. In humans, IL-6 [25,104,105], IL-1RA [25,104,106], IL-1b [104,106], IL-8 [25,104], IL-10 and TNF-a [104] have been reported to increase following injury. It is unclear whether these acute post-traumatic changes affect car-tilage turnover in a positive [97] or negative way [107], or whether this implicates an initial repair response followed by a ‘turning point’, after which the environment of the chronically injured joint becomes u nfavorable for cartilage integrity (Figure 1) [97].
Therapies � Current treatments for OA
When a patient with OA seeks treatment, symp-tomatic treatment will be attempted first. Of the oral symptomatic therapies, nonsteroidal anti-inflammatory drugs (NSAIDs) [108] and cyclo-oxygenase (COX)-2-specific inhibitors have proven to be effective in reduction of OA symp-toms, while COX-2 inhibitors also demonstrate chondroprotective actions [109,110]. Although COX-2-specific inhibitors are associated with a lower incidence of gastrointestinal complaints than NSAIDs [111], they are associated with a higher cardiovascular morbidity [112] and, thus, are currently prescribed less frequently.
When unsuccessful, disease-modifying OA drugs may be applied in specific patient popu-lations. In OA patients, the combination of oral glucosamine and chondroitin sulfate was more effective in reduction of OA symptoms than placebo, in patients with moderate-to-severe knee pain [113]. Although the evidence for clinical effectiveness of HA treatment in OA is conflicting [114,115], it currently seems that intra-articular HA supplementation is compa-rable in efficacy to systemic forms of active intervention (NSAIDs and physical therapy) but with more prolonged effects than intra-articular corticosteroids for patients with OA of the knee [116]. Although each intra-articular injection of course poses a risk of infection, this risk is considered extremely low (4.6 per 100,000 injections) [117]. In the acute post-trauma setting, improved rehabilitation after ACL reconstruction was demonstrated after intra-articular administration of HA [118].
When symptomatic treatments or treat-ments aiming to restore SF viscosity or supple-ment ECM components are unsuccessful in reduction of OA symptoms, the final ‘golden s tandard’ is surgical joint replacement.

www.futuremedicine.com 439future science group
Joint injury & osteoarthritis Review
Future therapies: cytokine-modulating therapiesIn RA, targeting of IL-1 and TNF-a proved s uccessful for reduction of disease-related symptoms [15,16]. In OA, inhibition of cartilage degradation was most frequently attempted by targeting IL-1 [119–121]. In vivo, this did seem successful as reduction of OA symptoms, histo-logical parameters and preservation of articular cartilage quality were demonstrated after intra-articular injection of synoviocytes transduced with the IL‑1RA gene in equine and canine OA models [52,122], and IL‑1RA plasmids into a rabbit knee joint with OA induced by meniscectomy. However, in the only clinical OA trial carried out until now, intra-articular injection of recom-binant IL-1RA did not lead to improvement of OA symptoms [121]. Thus far, no compelling evi-dence exists that IL-1RA therapy is effective for treatment of OA in human patients.
A more complex treatment based on intra-articular IL-1RA administration is Orthokine®. Autologous conditioned serum (ACS) is pre-pared by in vitro incubation of the patient’s whole blood in the presence of glass beads, and the resulting product, containing increased lev-els of IL-1RA as well as IL-4 and IL-10 [123], is injected into the joint. Although infrequently investigated, in vivo studies [52,124] examining the effect of Orthokine on OA, and clinical stud-ies [120,125] comparing Orthokine with HA or
placebo demonstrate either little or moderate improvement of OA symptoms. On the other hand, in the study demonstrating the greatest improvement of OA symptoms, the Orthokine-treated cohort was injected with ACS six-times while the placebo and HA cohort were injected only three-times [120]. In this particular study, more frequent injections may have led to a greater improvement in OA symptoms for two reasons. First, a regession ana lysis of 174 ran-domized, controlled OA trials demonstrated that placebo effects increase significantly with increased invasiveness of a treatment procedure (i.e., ‘injection’ in contrast to, for example, an oral therapy) [126]. Thus, the additional injec-tions during ACS treatment may have caused an improvement in OA symptoms merely due to the ‘invasiveness’ of the treatment. Second, as joint lavage proved successful for reduction of OA symptoms in rabbits with surgically induced OA [127], the three additional injec-tions may have been responsible for a ‘lavaging’ effect, thus also resulting in improvement of OA symptoms. The exact composition of the intra-articular injected Orthokine, and thus the basis for the in vivo mechanisms responsible for clinically observed effects, is unknown [119,124].
Although several IL-1RA-based therapies focus on the role of IL-1, their therapeutical relevance may be discussed. IL-1RA levels in OA SF (614 pg/ml [128]) may already be high
Synovium
Synovial fluid
Extracellular cartilage matrix
Activated T cells
Cartilage degradation
Chondrocyte
Fibronectin fragments
IL-17, OSM, OPG, IFN-γ
NOMMP
TIMP
IL-1β, TNF-α, IL-6, IL-7, IL-8, LIF
TGF-β, IGF-β, FGFIL-1RA, IL-4, IL-10, IL-13
IL-1RA, IL-4, IL-10, IL-13, OPG, bFGFIL-1β, TNF-α, IL-6, IL-7, IL-8, LIF
Synovial fibroblasts
Immunotherapy © Future Science Group (2009)
Figure 1. Cytokines in the intra-articular environment. LIF: Leukocyte-inhibitory factor; MMP: Matrix metalloproteinase; NO: Nitric oxide; OPG: Osteoprotegerin; OSM: Oncostatin M; TIMP: Tissue inhibitor of matrix metalloproteinase.

Immunotherapy (2009) 1(3)440 future science group
Review Rutgers, Saris, Auw Yang, Dhert & Creemers
enough to block endogenous IL-1b [51], and it may not therefore be necessary to elevate this baseline level exogenously, as for example by using ACS (2015 pg/ml [129] and 10254 pg/ml [123]) IL-1RA. Moreover, exogenously added IL-1RA may hardly be available to the cartilage due to fast clearance from the joint. Although the theory behind ACS preparation and its effects seem interesting, the lack of knowledge on exact composition of the product or in vivo clinical effects demands for further investigation before broad clinical application.
Although TNF-a inhibition has gained a definite place in RA treatment [130], only a few reports exist on successful improvement of OA symptoms in patients treated with TNF-a inhibitors [131,132]. Osteoarthitic SF and osteo-arthitic synovium supernatants upregulated p55 TNF-a receptors in human chondrocytes
[133]. TNF-a antagonists decreased production of TNF-a by rabbit synovial cells in vitro, and suppressed TNF-a-mediated nitric oxide (NO) production while stimulating IL-1RA synthesis
[134]. As TNF-a levels are strongly elevated in SF after trauma, TNF-a therapy in orthopedics may be promising for intra-articular trauma. However, TNF-a therapy may increase the risk of infections and malignancies [135].
Future perspectiveThere is very little evidence regarding effective-ness of the few existing cytokine-modulating therapies for treatment of OA. This may, in part, be due to the ability of the intra-articular injected substances to in fact reach the target cells and thus mediate their protective effects, or may implicate that chondrodestructive cytokines in accordance with their low levels of in osteo-arthritic SF do not play a major role in main-tenance of the degenerative process. However, as cytokine-modulating therapies may inhibit
further disease progression, it is desirable that further knowledge is gained. Until that time, one may still consider NSAIDs, the combina-tion of glucosamine and chondroitin sulfate, or HA, as therapy.
Current cytokine-modulating therapies may be considered for application after an intra-articular injury in addition to their application for OA, as a ‘normal’ protective intra-articular environment may turn into a chondrodestructive environment with high levels of chondroprotective as well as chondrodegradative cytokines, predisposing to early onset OA after trauma. Studies evaluating the effectiveness of, and determining the medical indication for, these therapies for ‘post-trauma’ may be facilitated by noninvasive methods to depict cartilage qualitative characteristics. An important development in this field has been the introduction of the delayed gadolinium-enhanced MRI of cartilage, which depicts intra-articular proteoglycan distribution without having to per-form an invasive procedure such as a biopsy or arthroscopy [136,137].
The panel of cytokines present in the joint as well as knowledge of their effects is currently expanding. More knowledge on the character-istics of SF will finally optimize effectiveness of cartilage-preserving therapies.
Financial & competing interests disclosureMarijn Rutgers is supported by the Anna Foundation for Musculoskeletal Research in The Netherlands. Daniel BF Saris is supported by The Netherlands Organisation for Health Research and Development. Laura B Creemers is supported by the Dutch Arthritic Association (Reumafonds). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
executive summary
� Combined chondroitin sulfate in combination with glucosamine, hyaluronic acid or cyclooxygenase-2 inhibitors are the current treatment options available for osteoarthritis (OA); however, effectiveness is limited.
� Although promising for the future, current cytokine-modulating therapies for OA yield variable clinical results, and compelling in vivo mechanistic evidence is sparsely available.
� In OA synovial fluid, most cytokines, including IL-1b, are present at low levels whereas, after trauma, chondrodestructive as well as chondroprotective cytokines are present at increased levels.
� The increase in IL-6, IL-1b and TNF-a levels after trauma potentially provides a target for intra-articular intervention. The low chondrodestructive cytokine levels in OA synovial fluid may require a different approach for the OA joint.
� More knowledge on intra-articular processes and synovial fluid composition is required to optimize effectiveness of cytokine-modulating therapies for treatment of cartilage pathologies.

www.futuremedicine.com 441future science group
Joint injury & osteoarthritis Review
BibliographyPapers of special note have been highlighted as:� of interest�� of considerable interest
1 Roitt IM, Brostoff J, Male DK: Cell-mediated immune reactions. In: Immunology. Crowe L (Ed.). Mosby, London, UK 121–138 (2001).
2 Garlet TP, Coelho U, Silva JS, Garlet GP: Cytokine expression pattern in compression and tension sides of the periodontal ligament during orthodontic tooth movement in humans. Eur. J. Oral Sci. 115(5), 355–362 (2007).
3 Graves D: Cytokines that promote periodontal tissue destruction. J. Periodontol. 79(Suppl. 8), 1585–1591 (2008).
4 Gharaee-Kermani M, Phan SH: Role of cytokines and cytokine therapy in wound healing and fibrotic diseases. Curr. Pharm. Des. 7(11), 1083–1103 (2001).
5 Matsumoto K, Ikema K, Tanihara H: Role of cytokines and chemokines in pseudomonal keratitis. Cornea 24(Suppl. 8), S43–S49 (2005).
6 Blanchard F, Duplomb L, Baud’huin M, Brounais B: The dual role of IL-6-type cytokines on bone remodeling and bone tumors. Cytokine Growth Factor Rev. (2008).
7 Goldring MB, Berenbaum F: The regulation of chondrocyte function by proinflammatory mediators: prostaglandins and nitric oxide. Clin. Orthop. Relat. Res. (Suppl 427), S37–S46 (2004).
8 Goldring SR, Goldring MB: The role of cytokines in cartilage matrix degeneration in osteoarthritis. Clin. Orthop. Relat. Res. (Suppl. 427), S27–36 (2004).
�� Excellent review on the role of a variety of cytokines in cartilage damage and repair.
9 Buckwalter JA, Einhorn TA, Simon SB: Articular cartilage structure, composition, and function. In: Orthopaedic Basic Science. American Academy of Orthopaedic Surgeons, Rosemont, IL, USA 444–451 (1999).
� Comprehensive reference work on composition and biomechanical properties of cartilage.
10 Yaron I, Meyer FA, Dayer JM, Bleiberg I, Yaron M: Some recombinant human cytokines stimulate glycosaminoglycan synthesis in human synovial fibroblast cultures and inhibit it in human articular cartilage cultures. Arthritis Rheum. 32(2), 173–180 (1989).
11 Goldring MB, Birkhead J, Sandell LJ, Kimura T, Krane SM: Interleukin 1 suppresses expression of cartilage-specific types II and IX collagens and increases types I and III collagens in human chondrocytes. J. Clin. Invest. 82(6), 2026–2037 (1988).
12 Schlaak JF, Pfers I, Meyer Zum Buschenfelde KH, Marker-Hermann E: Different cytokine profiles in the synovial fluid of patients with osteoarthritis, rheumatoid arthritis and seronegative spondylarthropathies. Clin. Exp. Rheumatol. 14(2), 155–162 (1996).
13 Westacott CI, Whicher JT, Barnes IC et al.: Synovial fluid concentration of five different cytokines in rheumatic diseases. Ann. Rheum. Dis. 49(9), 676–681 (1990).
14 Rooney M, Symons JA, Duff GW: Interleukin 1 b in synovial fluid is related to local disease activity in rheumatoid arthritis. Rheumatol. Int. 10(5), 217–219 (1990).
15 Cohen SB, Moreland LW, Cush JJ et al.: A multicentre, double blind, randomised, placebo controlled trial of anakinra (Kineret®), a recombinant interleukin 1 receptor antagonist, in patients with rheumatoid arthritis treated with background methotrexate. Ann. Rheum. Dis. 63(9), 1062–1068 (2004).
16 Moreland LW, Weinblatt ME, Keystone EC et al.: Etanercept treatment in adults with established rheumatoid arthritis: 7 years of clinical experience. J. Rheumatol. 33(5), 854–861 (2006).
17 Nishimoto N, Hashimoto J, Miyasaka N et al.: Study of active controlled monotherapy used for rheumatoid arthritis, an IL-6 inhibitor (SAMURAI): evidence of clinical and radiographic benefit from an x ray reader-blinded randomised controlled trial of tocilizumab. Ann. Rheum. Dis. 66(9), 1162–1167 (2007).
18 Blom AB, van der Kraan PM, van den Berg WB: Cytokine targeting in osteoarthritis. Curr. Drug Targets 8(2), 283–292 (2007).
19 Loyau G, Pujol JP: The role of cytokines in the development of osteoarthritis. Scand. J. Rheumatol. (Suppl. 81) 8–12 (1990).
20 Furuzawa-Carballeda J, Macip-Rodriguez PM, Cabral AR: Osteoarthritis and rheumatoid arthritis pannus have similar qualitative metabolic characteristics and pro-inflammatory cytokine response. Clin. Exp. Rheumatol. 26(4), 554–560 (2008).
21 Cope AP: T cells in rheumatoid arthritis. Arthritis Res. Ther. (10 Suppl. 1) S1 (2008).
22 Gelber AC, Hochberg MC, Mead LA et al.: Joint injury in young adults and risk for subsequent knee and hip osteoarthritis. Ann. Intern. Med. 133(5), 321–328 (2000).
23 Sherman MF, Warren RF, Marshall JL, Savatsky GJ: A clinical and radiographical ana lysis of 127 anterior cruciate insufficient knees. Clin. Orthop. Relat. Res. 227, 229–237 (1988).
24 Rangger C, Kathrein A, Klestil T, Glotzer W: Partial meniscectomy and osteoarthritis. Implications for treatment of athletes. Sports Med. 23(1), 61–68 (1997).
25 Cameron ml , Fu FH, Paessler HH, Schneider M, Evans CH: Synovial fluid cytokine concentrations as possible prognostic indicators in the ACL-deficient knee. Knee Surg. Sports Traumatol. Arthrosc. 2(1), 38–44 (1994).
26 Smith RL, Allison AC, Schurman DJ: Induction of articular cartilage degradation by recombinant interleukin 1 a and 1 b. Connect Tissue Res. 18(4), 307–316 (1989).
27 Pettipher ER, Higgs GA, Henderson B: Interleukin 1 induces leukocyte infiltration and cartilage proteoglycan degradation in the synovial joint. Proc. Natl. Acad. Sci. U.S.A. 83(22), 8749–8753 (1986).
28 Westacott CI, Barakat AF, Wood L et al.: Tumor necrosis factor a can contribute to focal loss of cartilage in osteoarthritis. Osteoarthr. Cartil. 8(3), 213–221 (2000).
29 Henrotin YE, De Groote DD, Labasse AH et al.: Effects of exogenous IL-1 b, TNF a, IL-6, IL-8 and LIF on cytokine production by human articular chondrocytes. Osteoarthr. Cartil. 4(3), 163–173 (1996).
30 Henderson B, Pettipher ER: Arthritogenic actions of recombinant IL-1 and tumour necrosis factor a in the rabbit: evidence for synergistic interactions between cytokines in vivo. Clin. Exp. Immunol. 75(2), 306–310 (1989).
31 Stove J, Huch K, Gunther KP, Scharf HP: Interleukin-1b induces different gene expression of stromelysin, aggrecan and tumor-necrosis-factor-stimulated gene 6 in human osteoarthritic chondrocytes in vitro. Pathobiology 68(3), 144–149 (2000).
32 Fernandes JC, Martel-Pelletier J, Pelletier JP: The role of cytokines in osteoarthritis pathophysiology. Biorheology, 39(1–2), 237–246 (2002).
33 Arend WP: The balance between IL-1 and IL-1RA in disease. Cytokine Growth Factor Rev. 13(4–5), 323–340 (2002).
� In addition to this specific review on the role of IL-1 and its receptor, earlier work by Arend is very constructive in explaining mechanisms of action of IL-1.
34 de Jager W, Prakken BJ, Bijlsma JW, Kuis W, Rijkers GT: Improved multiplex immunoassay performance in human plasma and synovial fluid following removal of interfering heterophilic antibodies. J. Immunol. Methods 300(1–2), 124–135 (2005).
35 Arend WP, Dayer JM: Inhibition of the production and effects of interleukin-1 and tumor necrosis factor a in rheumatoid arthritis. Arthritis Rheum. 38(2), 151–160 (1995).

Immunotherapy (2009) 1(3)442 future science group
Review Rutgers, Saris, Auw Yang, Dhert & Creemers
36 Henrotin YE, Zheng SX, Labasse AH et al.: Modulation of human chondrocyte metabolism by recombinant human interferon. Osteoarthr. Cartil. 8(6), 474–482 (2000).
37 Jovanovic DV, Di Battista JA, Martel-Pelletier J et al.: IL-17 stimulates the production and expression of proinflammatory cytokines, IL-b and TNF-a, by human macrophages. J. Immunol. 160(7), 3513–3521 (1998).
38 Durigova M, Roughley PJ, Mort JS: Mechanism of proteoglycan aggregate degradation in cartilage stimulated with oncostatin M. Osteoarthr. Cartil. 16(1), 98–104 (2008).
39 Koshy PJ, Lundy CJ, Rowan AD et al.: The modulation of matrix metalloproteinase and ADAM gene expression in human chondrocytes by interleukin-1 and oncostatin M: a time-course study using real-time quantitative reverse transcription-polymerase chain reaction. Arthritis Rheum. 46(4), 961–967 (2002).
40 Long D, Blake S, Song XY, Lark M, Loeser RF: Human articular chondrocytes produce IL-7 and respond to IL-7 with increased production of matrix metalloproteinase-13. Arthritis Res. Ther. 10(1), R23 (2008).
41 Merz D, Liu R, Johnson K, Terkeltaub R: IL-8/CXCL8 and growth-related oncogene a/CXCL1 induce chondrocyte hypertrophic differentiation. J. Immunol. 171(8), 4406–4415 (2003).
42 Lotz M, Moats T, Villiger PM: Leukemia inhibitory factor is expressed in cartilage and synovium and can contribute to the pathogenesis of arthritis. J. Clin. Invest. 90(3), 888–896 (1992).
43 Flannery CR, Little CB, Hughes CE et al.: IL-6 and its soluble receptor augment aggrecanase-mediated proteoglycan catabolism in articular cartilage. Matrix Biol. 19(6), 549–553 (2000).
44 Nietfeld JJ, Wilbrink B, Helle M et al.: Interleukin-1-induced interleukin-6 is required for the inhibition of proteoglycan synthesis by interleukin-1 in human articular cartilage. Arthritis Rheum. 33(11), 1695–1701 (1990).
45 Villiger PM, Kusari AB, ten Dijke P, Lotz M: IL-1 b and IL-6 selectively induce transforming growth factor-b isoforms in human articular chondrocytes. J. Immunol. 151(6), 3337–3344 (1993).
46 Lotz M, Guerne PA: Interleukin-6 induces the synthesis of tissue inhibitor of metalloproteinases-1/erythroid potentiating activity (TIMP-1/EPA). J. Biol. Chem. 266(4), 2017–2020 (1991).
47 Loeser RF, Chubinskaya S, Pacione C, Im HJ: Basic fibroblast growth factor inhibits the anabolic activity of insulin-like growth factor 1 and osteogenic protein 1 in adult human articular chondrocytes. Arthritis Rheum. 52(12), 3910–3917 (2005).
48 Vincent T, Hermansson M, Bolton M, Wait R, Saklatvala J: Basic FGF mediates an immediate response of articular cartilage to mechanical injury. Proc. Natl Acad. Sci. U.S.A. 99(12), 8259–8264 (2002).
49 Guerne PA, Sublet A, Lotz M: Growth factor responsiveness of human articular chondrocytes: distinct profiles in primary chondrocytes, subcultured chondrocytes, and fibroblasts. J. Cell Physiol. 158(3), 476–484 (1994).
50 Alaaeddine N, Di Battista JA, Pelletier JP et al.: Inhibition of tumor necrosis factor a-induced prostaglandin E2 production by the antiinflammatory cytokines interleukin-4, interleukin-10, and interleukin-13 in osteoarthritic synovial fibroblasts: distinct targeting in the signaling pathways. Arthritis Rheum. 42(4), 710–718 (1999).
51 Arend WP, Welgus HG, Thompson RC, Eisenberg SP: Biological properties of recombinant human monocyte-derived interleukin 1 receptor antagonist. J. Clin. Invest. 85(5), 1694–1697 (1990).
52 Frisbie DD, Ghivizzani SC, Robbins PD, Evans CH, McIlwraith CW: Treatment of experimental equine osteoarthritis by in vivo delivery of the equine interleukin-1 receptor antagonist gene. Gene Ther. 9(1), 12–20 (2002).
53 Granowitz EV, Clark BD, Mancilla J, Dinarello CA: Interleukin-1 receptor antagonist competitively inhibits the binding of interleukin-1 to the type II interleukin-1 receptor. J. Biol. Chem. 266(22), 14147–14150 (1991).
54 Smith RJ, Chin JE, Sam LM, Justen JM: Biologic effects of an interleukin-1 receptor antagonist protein on interleukin-1-stimulated cartilage erosion and chondrocyte responsiveness. Arthritis Rheum. 34(1), 78–83 (1991).
55 Secombes C, Zou J, Daniels G et al.: Rainbow trout cytokine and cytokine receptor genes. Immunol. Rev. 166, 333–340 (1998).
56 van Osch GJ, van den Berg WB, Hunziker EB, Hauselmann HJ: Differential effects of IGF-1 and TGF b-2 on the assembly of proteoglycans in pericellular and territorial matrix by cultured bovine articular chondrocytes. Osteoarthr. Cartil. 6(3), 187–195 (1998).
57 Lafeber FP, van Roy HL, van der Kraan PM, van den Berg WB, Bijlsma JW: Transforming growth factor-b predominantly stimulates phenotypically changed chondrocytes in osteoarthritic human cartilage. J. Rheumatol. 24(3), 536–542 (1997).
58 Regan EA, Bowler RP, Crapo JD: Joint fluid antioxidants are decreased in osteoarthritic joints compared with joints with macroscopically intact cartilage and subacute injury. Osteoarthr. Cartil. 16(4), 515–521 (2008).
59 Scharstuhl A, Glansbeek HL, van Beuningen HM et al.: Inhibition of endogenous TGF-b during experimental osteoarthritis prevents osteophyte formation and impairs cartilage repair. J. Immunol. 169(1), 507–514 (2002).
60 Goodrich LR, Hidaka C, Robbins PD, Evans CH, Nixon AJ: Genetic modification of chondrocytes with insulin-like growth factor-1 enhances cartilage healing in an equine model. J. Bone Joint Surg. Br. 89(5), 672–685 (2007).
61 Fortier LA, Mohammed HO, Lust G, Nixon AJ: Insulin-like growth factor-I enhances cell-based repair of articular cartilage. J. Bone Joint Surg. Br. 84(2), 276–288 (2002).
62 Fukumoto T, Sperling JW, Sanyal A et al.: Combined effects of insulin-like growth factor-1 and transforming growth factor-b1 on periosteal mesenchymal cells during chondrogenesis in vitro. Osteoarthr. Cartil. 11(1), 55–64 (2003).
63 Tsukazaki T, Matsumoto T, Enomoto H et al.: Growth hormone directly and indirectly stimulates articular chondrocyte cell growth. Osteoarthr. Cartil. 2(4), 259–267 (1994).
64 Kong YY, Feige U, Sarosi I et al.: ActivatedT cells regulate bone loss and joint destruction in adjuvant arthritis through osteoprotegerin ligand. Nature 402(6759), 304–309 (1999).
65 Shimizu S, Asou Y, Itoh S et al.: Prevention of cartilage destruction with intraarticular osteoclastogenesis inhibitory factor/osteoprotegerin in a murine model of osteoarthritis. Arthritis Rheum. 56(10), 3358–3365 (2007).
66 Takemura M, Harada A, Mizuno M, Yano K, Yamada Y: Relationship between osteoprotegerin/osteoclastogenesis inhibitory factor concentration in synovial fluid and disease severity in individuals with osteoarthritis of the knee. Metabolism 50(1), 1–2 (2001).
67 Cohen NP, Foster RJ, Mow VC: Composition and dynamics of articular cartilage: structure, function, and maintaining healthy state. J. Orthop. Sports Phys. Ther. 28(4), 203–215 (1998).

www.futuremedicine.com 443future science group
Joint injury & osteoarthritis Review
68 Junqueira LC, Carneiro J, Kelley RO: Cartilage. In: Basic Histology. Elsevier, Maarssen, The Netherlands, 126–136 (1996)
69 Homandberg GA: Potential regulation of cartilage metabolism in osteoarthritis by fibronectin fragments. Front Biosci. 4, D713–D730 (1999).
70 Carnemolla B, Cutolo M, Castellani P et al.: Characterization of synovial fluid fibronectin from patients with rheumatic inflammatory diseases and healthy subjects. Arthritis Rheum. 27(8), 913–921 (1984).
71 Xu L, Peng H, Wu D et al.: Activation of the discoidin domain receptor 2 induces expression of matrix metalloproteinase 13 associated with osteoarthritis in mice. J. Biol. Chem. 280(1), 548–555 (2005).
72 Xu L, Peng H, Glasson S et al.: Increased expression of the collagen receptor discoidin domain receptor 2 in articular cartilage as a key event in the pathogenesis of osteoarthritis. Arthritis Rheum. 56(8), 2663–2673 (2007).
73 Iwanaga T, Shikichi M, Kitamura H, Yanase H, Nozawa-Inoue K: Morphology and functional roles of synoviocytes in the joint. Arch. Histol. Cytol. 63(1), 17–31 (2000).
74 Junqueira LC, Carneiro J, Kelley RO: Bone tissue. In: Basic Histology. Elsevier, Maarssen, The Netherlands, 137–162 (1996).
75 Henderson B, Edwards JCW (Eds): Structure of synovial lining. In: The Synovial Lining in Health and Disease. Chapman and Hall Medical, Cambridge, UK 17–40 (1987).
76 Ropes MW, Rossmeisl EC, Bauer W: The origin and nature of normal human synovial fluid. J. Clin. Invest. 19(6), 795–799 (1940).
77 Heilmann HH, Lindenhayn K, Walther HU: [Synovial volume of healthy and arthrotic human knee joints]. Z. Orthop. Ihre Grenzgeb. 134(2), 144–148 (1996).
78 Vignon E, Balblanc JC, Mathieu P, Louisot P, Richard M: Metalloprotease activity, phospholipase A2 activity and cytokine concentration in osteoarthritis synovial fluids. Osteoarthr. Cartil. 1(2), 115–120 (1993).
79 Roosendaal G, Vianen ME, Marx JJ et al.: Blood-induced joint damage: a human in vitro study. Arthritis Rheum. 42(5), 1025–1032 (1999).
80 Hulejova H, Baresova V, Klezl Z et al.: Increased level of cytokines and matrix metalloproteinases in osteoarthritic subchondral bone. Cytokine 38(3), 151–156 (2007).
81 Stoop R, Albrecht D, Gaissmaier C et al.: Comparison of marker gene expression in chondrocytes from patients receiving autologous chondrocyte transplantation versus osteoarthritis patients. Arthritis Res. Ther. 9(3), R60 (2007).
82 Moos V, Fickert S, Muller B, Weber U, Sieper J: Immunohistological ana lysis of cytokine expression in human osteoarthritic and healthy cartilage. J. Rheumatol. 26(4), 870–879 (1999).
83 Smith MD, Triantafillou S, Parker A, Youssef PP, Coleman M: Synovial membrane inflammation and cytokine production in patients with early osteoarthritis. J. Rheumatol. 24(2), 365–371 (1997).
84 Bertazzolo N, Punzi L, Stefani MP et al.: Interrelationships between interleukin (IL)-1, IL-6 and IL-8 in synovial fluid of various arthropathies. Agents Actions 41(1–2), 90–92 (1994).
85 Neidel J, Schulze M, Sova L, Lindschau J: Practical significance of cytokine determination in joint fluid in patients with arthroses or rheumatoid arthritis. Z. Orthop. Ihre Grenzgeb. 134(4), 381–385 (1996).
86 Benton HP, Tyler JA: Inhibition of cartilage proteoglycan synthesis by interleukin I. Biochem. Biophys. Res. Commun. 154(1), 421–428 (1988).
87 Huch K, Wilbrink B, Flechtenmacher J et al.: Effects of recombinant human osteogenic protein 1 on the production of proteoglycan, prostaglandin E2, and interleukin-1 receptor antagonist by human articular chondrocytes cultured in the presence of interleukin-1b. Arthritis Rheum. 40(12), 2157–2161 (1997).
88 Chabaud M, Lubberts E, Joosten L, van Den Berg W, Miossec P. IL-17 derived from juxta-articular bone and synovium contributes to joint degradation in rheumatoid arthritis. Arthritis Res. 3(3), 168–177 (2001).
89 Lippiello L. Glucosamine and chondroitin sulfate: biological response modifiers of chondrocytes under simulated conditions of joint stress. Osteoarthr. Cartil. 11(5), 335–342 (2003).
90 Shakibaei M, John T, Seifarth C, Mobasheri A: Resveratrol inhibits IL-1 b-induced stimulation of caspase-3 and cleavage of PARP in human articular chondrocytes in vitro. Ann. N. Y. Acad. Sci. 1095, 554–563 (2007).
91 Intema F, DeGroot J, Elshof B et al.: The canine bilateral groove model of osteoarthritis. J. Orthop. Res. 26(11), 1471–1477 (2008).
92 van der Kraan PM, Vitters EL, van Beuningen HM, van de Putte LB, van den Berg WB: Degenerative knee joint lesions in mice after a single intra-articular collagenase injection. A new model of osteoarthritis. J. Exp. Pathol. (Oxford) 71(1), 19–31 (1990).
93 Moskowitz RW, Davis W, Sammarco J et al.: Experimentally induced degenerative joint lesions following partial meniscectomy in the rabbit. Arthritis Rheum. 16(3), 397–405 (1973).
94 Chen LX, Lin L, Wang HJ et al.: Suppression of early experimental osteoarthritis by in vivo delivery of the adenoviral vector-mediated NF-kBp65-specific siRNA. Osteoarthr. Cartil. 16(2), 174–184 (2008).
95 Pond MJ, Nuki G. Experimentally-induced osteoarthritis in the dog. Ann. Rheum. Dis. 32(4), 387–388 (1973).
96 Horiuchi T, Yoshida T, Koshihara Y et al.: The increase of parathyroid hormone-related peptide and cytokine levels in synovial fluid of elderly rheumatoid arthritis and osteoarthritis. Endocr. J. 46(5), 643–649 (1999).
97 Rodrigo JJ, Steadman JR, Syftestad G, Benton H, Silliman J: Effects of human knee synovial fluid on chondrogenesis in vitro. Am. J. Knee Surg. 8(4), 124–129 (1995).
� One of the earlier studies in which the role of intra-articular injury and subsequent changes in synovial fluid composition on cartilage metabolism were recognized.
98 Fujita Y, Hara Y, Nezu Y, Schulz KS, Tagawa M: Proinflammatory cytokine activities, matrix metalloproteinase-3 activity, and sulfated glycosaminoglycan content in synovial fluid of dogs with naturally acquired cranial cruciate ligament rupture. Vet. Surg. 35(4), 369–376 (2006).
99 Innes JF, Sharif M, Barr AR: Changes in concentrations of biochemical markers of osteoarthritis following surgical repair of ruptured cranial cruciate ligaments in dogs. Am. J. Vet. Res. 60(9), 1164–1168 (1999).
100 Ley C, Ekman S, Elmen A, Nilsson G, Eloranta ml : Interleukin-6 and tumour necrosis factor in synovial fluid from horses with carpal joint pathology. J. Vet. Med. A. Physiol. Pathol. Clin. Med. 54(7), 346–351 (2007).
101 Fu LL, Maffulli N, Chan KM: Intra-articular hyaluronic acid following knee immobilisation for 6 weeks in rabbits. Clin. Rheumatol. 20(2), 98–103 (2001).
102 Williams JM, Ongchi DR, Thonar EJ: Repair of articular cartilage injury following intra-articular chymopapain-induced matrix proteoglycan loss. J. Orthop. Res. 11(5), 705–716 (1993).
103 Wei X, Messner K: Age- and injury-dependent concentrations of transforming growth factor-b 1 and proteoglycan fragments in rabbit knee joint fluid. Osteoarthr. Cartil. 6(1), 10–18 (1998).
104 Irie K, Uchiyama E, Iwaso H: Intraarticular inflammatory cytokines in acute anterior cruciate ligament injured knee. Knee 10(1), 93–96 (2003).

Immunotherapy (2009) 1(3)444 future science group
Review Rutgers, Saris, Auw Yang, Dhert & Creemers
105 Higuchi H, Shirakura K, Kimura M et al.: Changes in biochemical parameters after anterior cruciate ligament injury. Int. Orthop. 30(1), 43–47 (2006).
106 Marks PH, Donaldson ml : Inflammatory cytokine profiles associated with chondral damage in the anterior cruciate ligament-deficient knee. Arthroscopy 21(11), 1342–1347 (2005).
107 Yang KG, Saris DB, Verbout AJ, Creemers LB, Dhert WJ: The effect of synovial fluid from injured knee joints on in vitro chondrogenesis. Tissue Eng. 12(10), 2957–2964 (2006).
108 Schiff M, Minic M: Comparison of the analgesic efficacy and safety of nonprescription doses of naproxen sodium and Ibuprofen in the treatment of osteoarthritis of the knee. J. Rheumatol. 31(7), 1373–1383 (2004).
109 Mastbergen SC, Lafeber FP, Bijlsma JW: Selective COX-2 inhibition prevents proinflammatory cytokine-induced cartilage damage. Rheumatology (Oxford) 41(7), 801–808 (2002).
110 de Boer TN, Huisman AM, Polak AA et al.: The chondroprotective effect of selective COX-2 inhibition in osteoarthritis: ex vivo evaluation of human cartilage tissue after in vivo treatment. Osteoarthr. Cartil. 17(4), 482–488 (2008).
111 Curtis SP, Bockow B, Fisher C et al.: Etoricoxib in the treatment of osteoarthritis over 52-weeks: a double-blind, active-comparator controlled trial [NCT00242489]. BMC Musculoskelet. Disord. 6, 58 (2005).
112 Solomon SD, McMurray JJ, Pfeffer MA et al.: Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. N. Engl. J. Med. 352(11), 1071–1080 (2005).
113 Clegg DO, Reda DJ, Harris CL et al.: Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N. Engl. J. Med. 354(8), 795–808 (2006).
114 Arrich J, Piribauer F, Mad P et al.: Intra-articular hyaluronic acid for the treatment of osteoarthritis of the knee: systematic review and meta-ana lysis. CMAJ. 172(8), 1039–1043 (2005).
115 Modawal A, Ferrer M, Choi HK, Castle JA: Hyaluronic acid injections relieve knee pain. J. Fam. Pract. 54(9), 758–767 (2005).
116 Bellamy N, Campbell J, Robinson V et al.: Viscosupplementation for the treatment of osteoarthritis of the knee. Cochrane Database Syst. Rev. (2), CD005321 (2006).
117 Pal B, Morris J: Perceived risks of joint infection following intra-articular corticosteroid injections: a survey of rheumatologists. Clin. Rheumatol. 18(3), 264–265 (1999).
118 Huang MH, Yang RC, Chou PH: Preliminary effects of hyaluronic acid on early rehabilitation of patients with isolated anterior cruciate ligament reconstruction. Clin. J. Sport Med. 17(4), 242–250 (2007).
119 Yang KG, Raijmakers NJ, van Arkel ER et al.: Autologous interleukin-1 receptor antagonist improves function and symptoms in osteoarthritis when compared with placebo in a prospective randomized controlled trial. Osteoarthr. Cartil. 16(4), 498–505 (2008).
120 Baltzer AW, Moser C, Jansen SA, Krauspe R: Autologous conditioned serum (Orthokine) is an effective treatment for knee osteoarthritis. Osteoarthr. Cartil. (2008).
121 Chevalier X, Goupille P, Beaulieu AD et al.: Results from a double blind, placebo-controlled, multicenter trial of a single intra-articular injection of anakinra (Kineret®) in patients with osteoarthritis of the knee. Arthritis Rheum. 52(9), S507-S507 (2005).
122 Pelletier JP, Caron JP, Evans C et al.: In vivo suppression of early experimental osteoarthritis by interleukin-1 receptor antagonist using gene therapy. Arthritis Rheum. 40(6), 1012–1019 (1997).
123 Meijer H, Reinecke J, Becker C, Tholen G, Wehling P: The production of anti-inflammatory cytokines in whole blood by physico-chemical induction. Inflamm. Res. 52(10), 404–407 (2003).
124 Frisbie DD, Kawcak CE, Werpy NM, Park RD, McIlwraith CW: Clinical, biochemical, and histologic effects of intra-articular administration of autologous conditioned serum in horses with experimentally induced osteoarthritis. Am. J. Vet. Res. 68(3), 290–296 (2007).
125 Yang KG, Raijmakers NJ, van Arkel ER et al.: Autologous interleukin-1 receptor antagonist improves function and symptoms in osteoarthritis when compared with placebo in a prospective randomized controlled trial. Osteoarthr. Cartil. 16(4), 498–505 (2008).
126 Zhang W, Robertson J, Jones AC, Dieppe PA, Doherty M: The placebo effect and its determinants in osteoarthritis – meta-ana lysis of randomised controlled trials. Ann. Rheum. Dis. 67(12), 1716–1723 (2008).
127 Fu X, Lin L, Zhang J, Yu C: Assessment of the efficacy of joint lavage in rabbits with osteoarthritis of the knee. J. Orthop. Res. 27(1), 91–96 (2009).
128 Richette P, Francois M, Vicaut E et al.: A high interleukin 1 receptor antagonist/IL-1b ratio occurs naturally in knee osteoarthritis. J. Rheumatol. 35(8), 1650–1654 (2008).
129 Wehling P, Moser C, Frisbie D et al.: Autologous conditioned serum in the treatment of orthopedic diseases: the orthokine therapy. BioDrugs 21(5), 323–332 (2007).
130 Blumenauer B, Judd M, Cranney A et al.: Etanercept for the treatment of rheumatoid arthritis. Cochrane Database Syst. Rev. (4), CD004525 (2003).
131 Grunke M, Schulze-Koops H: Successful treatment of inflammatory knee osteoarthritis with tumour necrosis factor blockade. Ann. Rheum. Dis. 65(4), 555–556 (2006).
132 Cytokines induce inflammation and cartilage degradation. Oral TNF-a blocker against arthrosis. MMW Fortschr. Med. 144(15), 64 (2002).
133 Webb GR, Westacott CI,Elson CJ: Osteoarthritic synovial fluid and synovium supernatants up-regulate tumor necrosis factor receptors on human articular chondrocytes. Osteoarthr. Cartil. 6(3), 167–176 (1998).
134 Vuolteenaho K, Moilanen T, Hamalainen M, Moilanen E: Effects of TNFa-antagonists on nitric oxide production in human cartilage. Osteoarthr. Cartil. 10(4), 327–332 (2002).
135 Bongartz T, Sutton AJ, Sweeting MJ et al.: Anti-TNF antibody therapy in rheumatoid arthritis and the risk of serious infections and malignancies: systematic review and meta-ana lysis of rare harmful effects in randomized controlled trials. JAMA 295(19), 2275–2285 (2006).
136 Burstein D, Velyvis J, Scott KT et al.: Protocol issues for delayed Gd(DTPA)(2-)-enhanced MRI (dGEMRIC) for clinical evaluation of articular cartilage. Magn. Reson. Med. 45(1), 36–41 (2001).
� Clear explanation of a promising and currently broadly recognized technique for the noninvasive imaging of cartilage by delayed gadolinium-enhanced MRI of cartilage (dGEMRIC).
137 Young AA, Stanwell P, Williams A et al.: Glycosaminoglycan content of knee cartilage following posterior cruciate ligament rupture demonstrated by delayed gadolinium-enhanced magnetic resonance imaging of cartilage (dGEMRIC). A case report. J. Bone Joint Surg. Am. 87(12), 2763–2767 (2005).
138 Azuma J, Ogura M, Yamamoto I et al.: The effect of Y-25510 injection on the serum levels of some cytokines in healthy adult volunteers. Eur. J. Clin. Pharmacol. 53(6), 411–419 (1998).
139 Kutukculer N, Caglayan S, Aydogdu F: Study of pro-inflammatory (TNF-a, IL-1a, IL-6) and T-cell-derived (IL-2, IL-4) cytokines in plasma and synovial fluid of patients with juvenile chronic arthritis: correlations with clinical and laboratory parameters. Clin. Rheumatol. 17(4), 288–292 (1998).

www.futuremedicine.com 445future science group
Joint injury & osteoarthritis Review
140 Matsuzaki T, Nakajima A, Ishigami S, Tanno M, Yoshino S: Mirthful laughter differentially affects serum pro- and anti-inflammatory cytokine levels depending on the level of disease activity in patients with rheumatoid arthritis. Rheumatology (Oxford) 45(2), 182–186 (2006).
141 Robak T, Wierzbowska A, Blasinska-Morawiec M, Korycka A, Blonski JZ: Serum levels of IL-6 type cytokines and soluble IL-6 receptors in active B-cell chronic lymphocytic leukemia and in cladribine induced remission. Mediators Inflamm. 8(6), 277–286 (1999).
142 Darcissac EC, Vidal V, De La Tribonniere X, Mouton Y, Bahr GM: Variations in serum IL-7 and 90K/Mac-2 binding protein (Mac-2 BP) levels analysed in cohorts of HIV-1 patients and correlated with clinical changes following antiretroviral therapy. Clin. Exp. Immunol. 126(2), 287–294 (2001).
143 van Roon JA, Verweij MC, Wijk MW et al.: Increased intraarticular interleukin-7 in rheumatoid arthritis patients stimulates cell contact-dependent activation of CD4+
T cells and macrophages. Arthritis Rheum. 52(6), 1700–1710 (2005).
144 Rysz J, Banach M, Cialkowska-Rysz A et al.: Blood serum levels of IL-2, IL-6,IL-8, TNF-a and IL-1b in patients on maintenance hemodialysis. Cell Mol. Immunol. 3(2), 151–154 (2006).
145 Lee YC, Lee KH, Lee HB, Rhee YK: Serum levels of interleukins (IL)-4, IL-5, IL-13, and interferon-g in acute asthma. J. Asthma 38(8), 665–671 (2001).
146 Haznedaroglu S, Ozturk MA, Sancak B et al.: Serum interleukin 17 and interleukin 18 levels in familial Mediterranean fever. Clin. Exp. Rheumatol. 23(4 Suppl 38), S77–80 (2005).
147 Agarwal S, Misra R, Aggarwal A: Interleukin 17 levels are increased in juvenile idiopathic arthritis synovial fluid and induce synovial fibroblasts to produce proinflammatory cytokines and matrix metalloproteinases. J. Rheumatol. 35(3), 515–519 (2008).
148 Martini G, Gennari L, Merlotti D et al.: Serum OPG and RANKL levels before and after intravenous bisphosphonate treatment in Paget’s disease of bone. Bone 40(2), 457–463 (2007).
149 Manicourt DH, Poilvache P, Van Egeren A et al.: Synovial fluid levels of tumor necrosis factor a and oncostatin M correlate with levels of markers of the degradation of crosslinked collagen and cartilage aggrecan in rheumatoid arthritis but not in osteoarthritis. Arthritis Rheum. 43(2), 281–288 (2000).
150 Okamoto H, Yamamura M, Morita Y et al.: The synovial expression and serum levels of interleukin-6, interleukin-11, leukemia inhibitory factor, and oncostatin M in rheumatoid arthritis. Arthritis Rheum. 40(6), 1096–1105 (1997).
151 Czarkowska-Paczek B, Bartlomiejczyk I, Przybylski J: The serum levels of growth factors: PDGF, TGF-b and VEGF are increased after strenuous physical exercise. J. Physiol. Pharmacol. 57(2), 189–197 (2006).
152 Colangelo LA, Chiu B, Kopp P, Liu K, Gapstur SM: Serum IGF-I and C-reactive protein in healthy black and white young men: The CARDIA male hormone study. Growth Horm. IGF Res. (2009).
153 Tavera C, Abribat T, Reboul P et al.: IGF and IGF-binding protein system in the synovial fluid of osteoarthritic and rheumatoid arthritic patients. Osteoarthr. Cartil. 4(4),
263–274 (1996).
Copyright © 2022 FDOKUMEN




















