
Islet-Specific Glucose6Phosphatase Catalytic Subunit-Related Protein-Reactive CD4 T Cells in Human...
10
of March 3, 2014. This information is current as T Cells in Human Subjects + CD4 Catalytic Subunit-Related Protein-Reactive Islet-Specific Glucose-6-Phosphatase Pihoker, Eddie A. James and William W. Kwok Reichstetter, Helena Reijonen, Carla Greenbaum, Catherine Junbao Yang, Nancy A. Danke, DeAnna Berger, Sandra http://www.jimmunol.org/content/176/5/2781 2006; 176:2781-2789; ; J Immunol References http://www.jimmunol.org/content/176/5/2781.full#ref-list-1 , 20 of which you can access for free at: cites 43 articles This article Subscriptions http://jimmunol.org/subscriptions is online at: The Journal of Immunology Information about subscribing to Permissions http://www.aai.org/ji/copyright.html Submit copyright permission requests at: Email Alerts http://jimmunol.org/cgi/alerts/etoc Receive free email-alerts when new articles cite this article. Sign up at: Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists All rights reserved. Copyright © 2006 by The American Association of 9650 Rockville Pike, Bethesda, MD 20814-3994. The American Association of Immunologists, Inc., is published twice each month by The Journal of Immunology by guest on March 3, 2014 http://www.jimmunol.org/ Downloaded from by guest on March 3, 2014 http://www.jimmunol.org/ Downloaded from
-
Upload
washington -
Category
Documents
-
view
3 -
download
0
Transcript of Islet-Specific Glucose6Phosphatase Catalytic Subunit-Related Protein-Reactive CD4 T Cells in Human...

of March 3, 2014.This information is current as
T Cells in Human Subjects+CD4Catalytic Subunit-Related Protein-Reactive Islet-Specific Glucose-6-Phosphatase
Pihoker, Eddie A. James and William W. KwokReichstetter, Helena Reijonen, Carla Greenbaum, Catherine Junbao Yang, Nancy A. Danke, DeAnna Berger, Sandra
http://www.jimmunol.org/content/176/5/27812006; 176:2781-2789; ;J Immunol
Referenceshttp://www.jimmunol.org/content/176/5/2781.full#ref-list-1
, 20 of which you can access for free at: cites 43 articlesThis article
Subscriptionshttp://jimmunol.org/subscriptions
is online at: The Journal of ImmunologyInformation about subscribing to
Permissionshttp://www.aai.org/ji/copyright.htmlSubmit copyright permission requests at:
Email Alertshttp://jimmunol.org/cgi/alerts/etocReceive free email-alerts when new articles cite this article. Sign up at:
Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists All rights reserved.Copyright © 2006 by The American Association of9650 Rockville Pike, Bethesda, MD 20814-3994.The American Association of Immunologists, Inc.,
is published twice each month byThe Journal of Immunology
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from

Islet-Specific Glucose-6-Phosphatase Catalytic Subunit-RelatedProtein-Reactive CD4� T Cells in Human Subjects1
Junbao Yang,* Nancy A. Danke,* DeAnna Berger,* Sandra Reichstetter,* Helena Reijonen,*Carla Greenbaum,* Catherine Pihoker,† Eddie A. James,* and William W. Kwok2*‡
Islet-specific glucose-6-phosphatase catalytic subunit-related protein (IGRP) is recognized as a major autoantigen for autoimmunetype 1 diabetes (T1D) in the NOD mouse model. This study was undertaken to examine CD4� T cell responses toward IGRP in humansubjects. The tetramer-guided epitope mapping approach was used to identify IGRP-specific CD4� T cell epitopes. IGRP23–35 andIGRP247–259 were identified as DRA1*0101/DRB1*0401-restricted epitopes. IGRP13–25 and IGRP226–238 were identified as DRA1*0101/DRB1*0301-restricted epitopes. IGRP-specific tetramers were used to evaluate the prevalence of IGRP-reactive T cells in healthy andT1D subjects. More than 80% of subjects with either DRB1*0401 or DRB1*0301 haplotype have IGRP-specific CD4� T cell responsesfor at least one IGRP epitope. IGRP-specific T cells from both healthy and T1D groups produce both �-IFN and IL-10. DRA1*0101/DRB1*0401 IGRP247–259-restricted T cells also show cross-reactivity to an epitope derived from liver/kidney glucose-6-phosphatase. Thedetection of IGRP-reactive T cells in both type 1 diabetic subjects and healthy subjects and recent reports of other autoreactive T cellsdetected in healthy subjects underscore the prevalence of potentially autoreactive T cells in the peripheral immune system of the generalpopulation. The Journal of Immunology, 2006, 176: 2781–2789.
T ype 1 diabetes (T1D)3 is an autoimmune disease in whichT cell-mediated autoimmune responses eventually lead tothe destruction of insulin-producing � cells in the pancre-
atic islets (1). Susceptibility to T1D in humans is strongly associ-ated with the HLA class II loci. The DRB1*0401 (DR0401)-DQB1*0302 and DRB1*0301(DR0301)-DQB1*0201 haplotypesare disease susceptible, whereas the DRB1*1501-DQB1*0602haplotype offers disease protection (2). The NOD mouse (NOD)develops autoimmune diabetes spontaneously, and has been wellestablished as a model for studying diabetes (3). Studies in NODmice have suggested that both CD4� and CD8� T cells are in-volved in the pathogenesis of autoimmune diabetes (4). A highpercentage of islet-infiltrating CD8� T cells in NOD mice are spe-cific for a peptide mimotope NRP (5). In subsequent reports, theNRP mimotope was revealed to be an epitope derived from islet-specific glucose-6-phosphatase catalytic subunit-related protein(IGRP) (6). Progression of autoimmune diabetes in NOD mice isalso correlated with an increase in the avidity of NRP/IGRP-reactiveT cells, and administration of NRP/IGRP peptides has an antidiabe-togenic effect (7, 8). These results suggest that IGRP is a majorautoantigen and plays a role in islet destruction in the NOD model.More recently, CD4� T cells specific for IGRP were also identified in
NOD mice (9). In adoptive T cell transfer experiments, IGRP-specificCD4� T cells delayed the onset of diabetes, implying that IGRP-specific CD4� T cells acted as regulatory T cells (Treg).
IGRP is a member of the glucose-6-phosphatase (G6Pase) fam-ily of proteins. Other members of this family include G6Pase-�and ubiquitously expressed G6Pase catalytic subunit-related pro-tein (UGRP or G6Pase-�). Expression of IGRP is restricted to theislet. G6Pase-� is found in all gluconeogenic tissues, including theliver, kidney, and intestine, whereas UGRP is widely expressed(10, 11). IGRP shows 50% sequence homology to G6Pase-� and35% sequence homology to UGRP. The G6Pase catalytic subunitcouples with glucose-6-phosphate transporter to form a G6Pasecomplex that hydrolyzes glucose-6-phosphate to glucose. Thiscomplex is involved in both the glycogenolysis and gluconeogen-esis pathways and plays a major role in the control of blood glucosehomeostasis (12). Recently, the enzymatic function of the IGRP hasalso been demonstrated. Membrane fractions from cells that overex-pressed IGRP converted glucose-6-phosphate to glucose (13). It isspeculated that IGRP is the major enzyme that is responsible forG6Pase activity in the islet. Like other G6Pases, IGRP is a glyco-protein anchored in the endoplasmic reticulum by multiple trans-membrane helices. The major portion of the protein is embeddedin the membrane, with short lumens and cytoplasmic loops (14).
The precise role of IGRP in human T1D is unclear. The T1Dsusceptibility locus IDDM7 was mapped within the IGRP locus (11,15), suggesting the possibility that IGRP is a disease susceptibilitygene. Studies in human subjects have identified GAD65, insulin, andIA-2 as the major T1D autoantigens, and CD4� T cells that aredirected against each of these proteins have been described (16–21).However, the presence of IGRP-specific CD4� T or CD8� T cells inhuman subjects has not yet been reported. In this study, we examinedCD4� T cell responses to IGRP in both healthy and T1D subjectsusing MHC class II tetramers. The tetramer-guided epitope mapping(TGEM) approach (22) was used to identify human IGRP epitopes.The prevalence of these IGRP epitopes in healthy and T1D subjectswas also examined.
*Benaroya Research Institute at Virginia Mason, Seattle, WA 98101; †Children’sHospital and Regional Medical Center, Seattle, WA 98105; and ‡Department of Im-munology, University of Washington, Seattle, WA 98195
Received for publication September 15, 2005. Accepted for publication December30, 2005.
The costs of publication of this article were defrayed in part by the payment of pagecharges. This article must therefore be hereby marked advertisement in accordancewith 18 U.S.C. Section 1734 solely to indicate this fact.1 This work was supported by Juvenile Diabetes Foundation International and theImmune Tolerance Network.2 Address correspondence and reprint requests to Dr. William W. Kwok, BenaroyaResearch Institute at Virginia Mason, 1201 9th Avenue, Seattle, WA 98101. E-mailaddress: [email protected] Abbreviations used in this paper: T1D, type 1 diabetes; IGRP, islet-specific glucose-6-phosphatase catalytic subunit-related protein; Treg, regulatory T cells; G6Pase, glu-cose-6-phosphatase; UGRP, ubiquitously expressed glucose-6-phosphatase catalyticsubunit-related protein; TGEM, tetramer-guided epitope mapping.
The Journal of Immunology
Copyright © 2006 by The American Association of Immunologists, Inc. 0022-1767/06/$02.00
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from

Materials and MethodsHealthy and T1D subjects
DR0301 and/or DR0401 T1D subjects �3.5 years after diagnosis wererecruited at the Diabetes Clinical Research Unit at Benaroya ResearchInstitute (Seattle, WA). Healthy DR0301 and/or DR0401 donors were re-cruited from normal volunteers with consent. A total of 10 T1D subjectsand 10 healthy subjects were recruited for this study. The HLA status ofthese groups is shown in Table I. The mean age of the patient group was22 � 9 years, whereas the mean age of the healthy group was 30 � 10 years.
Peptides and tetramers
A panel of 43 overlapping IGRP peptides (p1 to p43) were synthesized onpolyethylene pins with 9-fluorenylmethoxycarbonyl chemistry by MIMO-TOPES. These peptides, each 20-aa in length with a 12-aa overlap betweenadjacent peptides covered the entire IGRP protein. Peptides were dissolvedin DMSO, and peptide pools were generated by mixing five consecutive pep-tides. There were a total of nine IGRP peptide pools. The individual pep-tides—IGRP13–25 QHLQKDYRAYYTF, IGRP23–35 YTFLNFMSNVGDP,IGRP226–238 RVLNIDLLWSVPI, IGRP247–259 DWIHIDTTPFAGL, G6Pase-�228–240 KGLGVDLLWTLEK, G6Pase-�249–261 EWVHIDTTPFASL,UGRP218–230 FTLGLDLSWSISL, and UGRP239–251 EWIHVDSRPFASL—were synthesized with an Applied Biosystems 433A Peptide Synthesizer.
Soluble DR0401 molecules were produced as described previously (23).Soluble DR0301 molecules were produced from Schneider cells using asimilar approach. Empty biotinylated HLA-DR0401 or DR0301 monomerwas loaded with 0.2 mg/ml of either pooled IGRP peptides or individualIGRP peptides. Loadings were conducted at 37°C for 72 h in the presenceof 2.5 mg/ml (0.25%) n-octyl-�-D-glucopyranoside and 1 mM Pefabloc SC(Sigma-Aldrich). Peptide-loaded HLA-DR monomers were tetramerizedwith PE- or allophycocyanin-conjugated streptavidin (BioSource Interna-tional) at a molar ratio of 8:1, respectively.
DR0301/Flu MP169–181 and DR0401/Flu HA306–318 were used as con-trol tetramers in staining. The sequence of Flu MP169–181 is PLIRHEN-RMVLAS and Flu HA306–318 is PRYVKQNTLKLAT.
Validation of tetramer reagents
Each individual preparation of class II protein was loaded with a referencepeptide (Flu MP169 –181 for DR0301 or Flu HA306 –318 for DR0401),assembled as a tetramer, and used to stain a defined reference T cellclone (DR0301-restricted MP169 –181-specific clone or DR0401-re-stricted HA306 –318-specific clone). Only preparations that give accept-able staining of the reference clone and low background staining whenloaded with an irrelevant peptide were used for experiments.
TGEM and tetramer staining
The TGEM approach for epitope identification has been described in detailpreviously (22). Briefly, CD4� T cells were isolated from donor PBMCsby no-touch CD4� isolation kit (Miltenyi Biotec). To augment T cell re-sponses, CD4�CD25� T cells were removed from total CD4� T cells byFACS sorting (24). Two million purified CD4�CD25� T cells were seededinto wells of a 48-well plate, which had been coated with adherent cells (tobe used as APCs) from the same donor. Cells were stimulated with 10�g/ml of pooled peptides in RPMI 1640 supplemented with 10% pooledhuman AB serum, 1 mM sodium pyruvate, 50 U/ml penicillin, and 50
�g/ml streptomycin (T cell medium). Each well of cells was stimulatedwith a different pooled peptide (a total of nine different wells for the ninedifferent IGRP-pooled peptides). After 7 days, the cells were split into twowells with addition of fresh medium containing 5% of natural human IL-2(Hemagen). The culture was maintained by changing half volume of cul-ture supernatant every 3 days with fresh medium and IL-2. On day 14, thecultured cells were stained with pooled tetramers. Cells that gave positivestaining with pooled tetramers were identified and subsequently stainedwith a corresponding set of individual peptide tetramers.
For other experiments in detecting IGRP-reactive T cells, 2 � 106 un-fractionated CD4� T cells or 3 � 106 PBMC were plated out per well ontoa 48-well plate. Cells were stimulated with either one or two IGRP peptidesper well (10 �g/ml per peptide). Cells were cultured as indicated above.
Tetramer staining was conducted with 2 � 105 cells and 10 �g/mltetramers in 100 �l of T cell medium at 37°C for 2 h followed by anti-CD4staining at 4°C for 15 min. Cells were analyzed on a FACSCalibur (BDBiosciences). In most experiments, the background tetramer staining was�0.2%, and a staining of 0.4% or higher was considered to be positive. Insome experiments, cells that were positive for a particular tetramer weresingle-cell sorted by using a BD Biosciences FACSVantage. Sorted cellswere expanded with 1.5 � 105 unmatched, irradiated PBMC per well asfeeders with 2.5 �g/ml PHA and IL-2.
Cytokine assay
CD4� T cells were stimulated with IGRP peptides as described above andassayed on day 14. For the cytokine assay, 1 � 106 T cells were incubatedwith 10 �g/ml tetramers, 10 U/ml IL-2, and 10 �g/ml anti-CD28. After 3 h ofincubation, IFN-� and IL-10 secretions were determined by use of a cytokinesecretion capture assay (Miltenyi Biotec). Briefly, cells were washed twice inPBS and incubated in 100 �l of medium on ice for 5 min with an Ab-Abconjugate directed against both CD45 and the cytokine (i.e., IFN-� or IL-10).Prewarmed medium was added to a final volume of 2 ml, and cells wereincubated at 37°C for 45 min under gentle rotation to allow cell surface captureof secreted cytokines. Cells were washed once in PBS and then stained for 15min on ice with allophycocyanin-conjugated Ab directed against the cytokineof interest and PerCP-conjugated anti-CD4 Ab.
T cell proliferation assay
T cells were plated in 96-well plates at a concentration of 104/well. Irra-diated DR0301 or DR0401-expressing BLS-1 lines were used as APCs andplated at 2.5 � 104/well (25). Peptides were added at various concentra-tions. Assays were performed in triplicate wells in 150 �l of T cell me-dium. After a 3-day incubation at 37°C, 1 �Ci [3H]thymidine/well wasadded. Cells were harvested, and tritium uptake was measured after 15 h offurther incubation.
ResultsDetection of IGRP-specific CD4 T cells and identification ofDR0301- and DR0401-restricted IGRP T cell epitopes
The TGEM approach was used to detect IGRP-specific T cells forthe identification of DR0301 and DR0401-restricted IGRP T cellepitopes. A set of 43 overlapping peptides spanning the entireIGRP protein, each 20 residues in length with an offset of 8 resi-dues, was synthesized. The peptides were divided up into 9 pools.
Table I. DR0301 and DR0401 donors
Subjectno.
T1D Healthy
HLA-DR genotypeDuration of disease in
monthsSubject
no. HLA-DR genotype
1 0301/0404 31 11 0301/07012 0301/0401 35 12 0301/12013 0301/0404 28 13 0301/01014 0301/1301 13 14 0301/13015 0301/0101 15 15 0301/1101
6 0401/0101 5 16 0301/04017 0401/0901 27 17 0401/15018 0401/1301 39 18 0401/04- -9 0401/04- - 1 19 0401/0701
10 0401/0301 7 20 0401/1401
2782 IGRP CD4� T CELLS IN HUMAN T1D
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from

Pools 1–8 consisted of 5 peptides each, whereas pool 9 consistedof 3 peptides. These pooled peptides were used to stimulateCD4�CD25� T cells from a DR0301 healthy subject and aDR0401 healthy subject. As described in Materials and Methods,CD4�CD25� T cells were used as responder cells. CD4�CD25�
T cells were depleted because CD4� T cells are more responsiveto antigenic challenge when these regulatory cells are absent (24).Fourteen to 16 days after the peptide stimulation, cells were ex-amined by staining with DR0301 or DR0401-pooled IGRP peptidetetramers. Results of tetramer staining of cells from the DR0301subject are shown in Fig. 1A, and results of staining cells from theDR0401 subject are shown in Fig. 1B. For the DR0301 subject,
positive tetramer staining was observed with DR0301 pool 1 andpool 6 tetramers (Fig. 1A). For the DR0401 subject, positive stainingwas observed with DR0401 pool 1 and pool 7 tetramers (Fig. 1B).Single peptide tetramers were generated with individual peptides fromthe positive pools, and the staining was repeated. For the DR0301subject, tetramers with peptide p2 from pool 1 and peptide p29 frompool 6 gave positive staining (Fig. 2A) (peptide p30 gave a stainingabove background; however, the result was irreproducible), and forthe DR0401 subject, tetramers with peptide p3 from pool 1 and pep-tide p31 from pool 7 gave positive staining (Fig. 2B). These experi-ments were repeated with two additional DR0301 T1D subjects (sam-ples were obtained within 16 mo after disease onset) and one DR0401
FIGURE 1. Mapping of IGRP T cell epitopes. A,CD4�CD25� T cells were isolated from PBMC of ahealthy DR0301 subject and were stimulated withIGRP-pooled peptides. Fourteen days poststimulation,cells were stained with PE-conjugated DR0301/pooledIGRP peptide tetramers, and anti-CD4 and anti-CD3mAbs. Cells were gated on light scattering and anti-CD3 positivity. Fifty thousand events were analyzed. B,CD4�CD25� T cells were isolated from PBMC of ahealthy DR0401 subject and were stimulated withIGRP-pooled peptides. Fourteen days poststimulation,cells were stained with PE-conjugated DR0401/pooledIGRP peptide tetramers, and anti-CD4 and anti-CD3mAbs. Cells were gated on scattering and anti-CD3positivity.
FIGURE 2. Fine mapping of DR0301 and DR0401-restricted IGRP epitopes. A, The positive wells shownin Fig. 1A were stained with DR0301 tetramers gener-ated with individual peptides p1, p2, p3, p4, and p5from pool 1 and peptides p26, p27, p28, p29, and p30from pool 6. B, The positive wells shown in Fig. 1Bwere stained with DR0401 tetramers generated with in-dividual peptides p1, p2, p3, p4, and p5 from pool 1 andpeptides p31, p32, p33, p34, and p35 from pool 7.
2783The Journal of Immunology
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from
T1D subject (sample was obtained within 7 mo after disease onset).Although not all of the epitopes were detected in the repeated exper-iments, no new additional IGRP epitopes were identified (data notshown). These experiments indicated IGRP p2 and p29 as the majorDR0301-restricted epitopes and IGRP p3 and p31 as the majorDR0401-restricted epitopes. DR0301-restricted T cells specific for p2and p29, respectively, were single-cell cloned by sorting for tetramer-positive T cells. Similarly, DR0401-restricted T cells that were spe-cific for p31 were also cloned. Attempts to clone DR0401/p3-specificT cells failed.
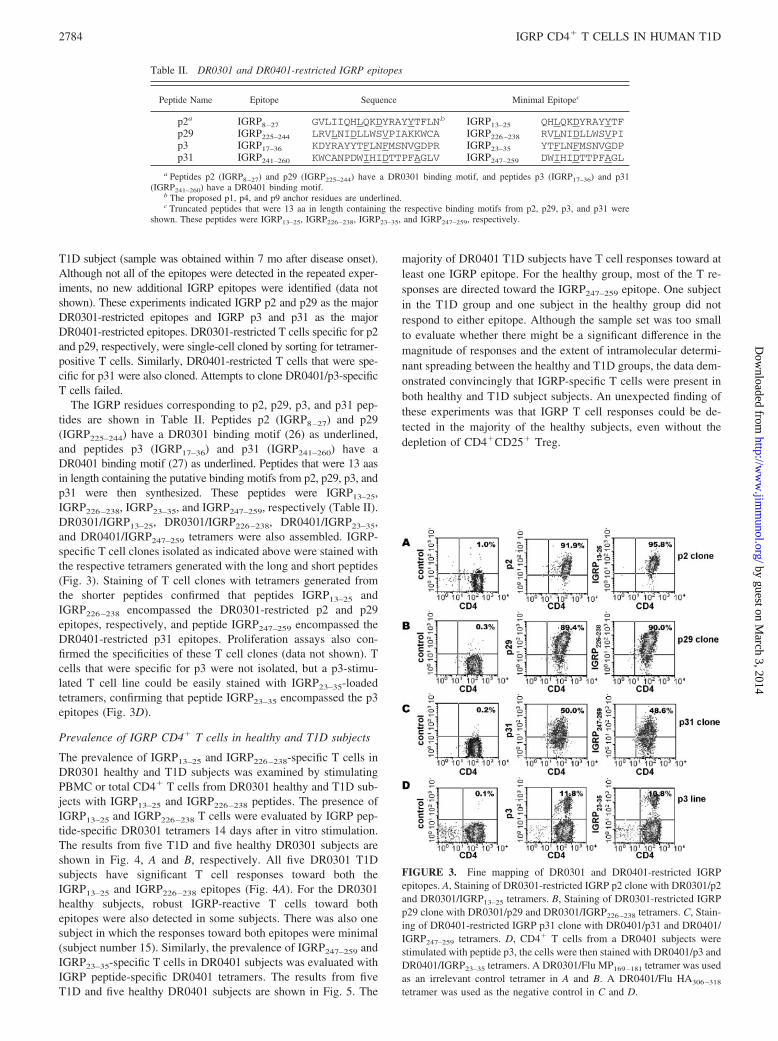
The IGRP residues corresponding to p2, p29, p3, and p31 pep-tides are shown in Table II. Peptides p2 (IGRP8–27) and p29(IGRP225–244) have a DR0301 binding motif (26) as underlined,and peptides p3 (IGRP17–36) and p31 (IGRP241–260) have aDR0401 binding motif (27) as underlined. Peptides that were 13 aasin length containing the putative binding motifs from p2, p29, p3, andp31 were then synthesized. These peptides were IGRP13–25,IGRP226–238, IGRP23–35, and IGRP247–259, respectively (Table II).DR0301/IGRP13–25, DR0301/IGRP226–238, DR0401/IGRP23–35,and DR0401/IGRP247–259 tetramers were also assembled. IGRP-specific T cell clones isolated as indicated above were stained withthe respective tetramers generated with the long and short peptides(Fig. 3). Staining of T cell clones with tetramers generated fromthe shorter peptides confirmed that peptides IGRP13–25 andIGRP226–238 encompassed the DR0301-restricted p2 and p29epitopes, respectively, and peptide IGRP247–259 encompassed theDR0401-restricted p31 epitopes. Proliferation assays also con-firmed the specificities of these T cell clones (data not shown). Tcells that were specific for p3 were not isolated, but a p3-stimu-lated T cell line could be easily stained with IGRP23–35-loadedtetramers, confirming that peptide IGRP23–35 encompassed the p3epitopes (Fig. 3D).
Prevalence of IGRP CD4� T cells in healthy and T1D subjects
The prevalence of IGRP13–25 and IGRP226–238-specific T cells inDR0301 healthy and T1D subjects was examined by stimulatingPBMC or total CD4� T cells from DR0301 healthy and T1D sub-jects with IGRP13–25 and IGRP226–238 peptides. The presence ofIGRP13–25 and IGRP226–238 T cells were evaluated by IGRP pep-tide-specific DR0301 tetramers 14 days after in vitro stimulation.The results from five T1D and five healthy DR0301 subjects areshown in Fig. 4, A and B, respectively. All five DR0301 T1Dsubjects have significant T cell responses toward both theIGRP13–25 and IGRP226–238 epitopes (Fig. 4A). For the DR0301healthy subjects, robust IGRP-reactive T cells toward bothepitopes were also detected in some subjects. There was also onesubject in which the responses toward both epitopes were minimal(subject number 15). Similarly, the prevalence of IGRP247–259 andIGRP23–35-specific T cells in DR0401 subjects was evaluated withIGRP peptide-specific DR0401 tetramers. The results from fiveT1D and five healthy DR0401 subjects are shown in Fig. 5. The
majority of DR0401 T1D subjects have T cell responses toward atleast one IGRP epitope. For the healthy group, most of the T re-sponses are directed toward the IGRP247–259 epitope. One subjectin the T1D group and one subject in the healthy group did notrespond to either epitope. Although the sample set was too smallto evaluate whether there might be a significant difference in themagnitude of responses and the extent of intramolecular determi-nant spreading between the healthy and T1D groups, the data dem-onstrated convincingly that IGRP-specific T cells were present inboth healthy and T1D subject subjects. An unexpected finding ofthese experiments was that IGRP T cell responses could be de-tected in the majority of the healthy subjects, even without thedepletion of CD4�CD25� Treg.
Table II. DR0301 and DR0401-restricted IGRP epitopes
Peptide Name Epitope Sequence Minimal Epitopec
p2a IGRP8–27 GVLIIQHLQKDYRAYYTFLNb IGRP13–25 QHLQKDYRAYYTFp29 IGRP225–244 LRVLNIDLLWSVPIAKKWCA IGRP226–238 RVLNIDLLWSVPIp3 IGRP17–36 KDYRAYYTFLNFMSNVGDPR IGRP23–35 YTFLNFMSNVGDPp31 IGRP241–260 KWCANPDWIHIDTTPFAGLV IGRP247–259 DWIHIDTTPFAGL
a Peptides p2 (IGRP8–27) and p29 (IGRP225–244) have a DR0301 binding motif, and peptides p3 (IGRP17–36) and p31(IGRP241–260) have a DR0401 binding motif.
b The proposed p1, p4, and p9 anchor residues are underlined.c Truncated peptides that were 13 aa in length containing the respective binding motifs from p2, p29, p3, and p31 were
shown. These peptides were IGRP13–25, IGRP226–238, IGRP23–35, and IGRP247–259, respectively.
FIGURE 3. Fine mapping of DR0301 and DR0401-restricted IGRPepitopes. A, Staining of DR0301-restricted IGRP p2 clone with DR0301/p2and DR0301/IGRP13–25 tetramers. B, Staining of DR0301-restricted IGRPp29 clone with DR0301/p29 and DR0301/IGRP226–238 tetramers. C, Stain-ing of DR0401-restricted IGRP p31 clone with DR0401/p31 and DR0401/IGRP247–259 tetramers. D, CD4� T cells from a DR0401 subjects werestimulated with peptide p3, the cells were then stained with DR0401/p3 andDR0401/IGRP23–35 tetramers. A DR0301/Flu MP169–181 tetramer was usedas an irrelevant control tetramer in A and B. A DR0401/Flu HA306–318
tetramer was used as the negative control in C and D.
2784 IGRP CD4� T CELLS IN HUMAN T1D
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from

Cytokine profiles of IGRP-reactive T cells in healthy and T1Dsubjects
Because frequencies of autoreactive T cells are usually very low,we have not attempted to assay for the cytokine profiles of CD4�
IGRP-reactive T cells directly ex vivo. We did compare the cyto-
kine profiles of DR0401/IGRP247–259-reactive T cells after in vitroexpansion in both healthy and T1D subjects. IGRP-reactive T cellsfrom both groups produced both �-IFN and IL-10. Examples ofthese assays are shown in Fig. 6. For T1D subjects, the percentageof �-IFN-positive cells within the tetramer-positive population
FIGURE 5. Detection of IGRP au-toreactive T cells in DR0401 T1D andhealthy subjects. A, PBMC or CD4� Tcells from DR0401 T1D subjects werestimulated with peptides IGRP247–259
and IGRP23–35. Cells were analyzed byflow cytometry 14 days poststimulationwith anti-CD3 and anti-CD4 mAbs,DR0401/IGRP247–259, and DR0401/IGRP23–35 tetramers. Results fromfive T1D subjects (numbers 6–10) areshown. B, PBMC or CD4� T cellsfrom DR0401 healthy subjects werestimulated with peptides IGRP247–259
and IGRP23–35. Cells were analyzedby flow cytometry 14 days poststimu-lation with anti-CD3 and anti-CD4mAbs, DR0401/IGRP247–259, andDR0401/IGRP23–35 tetramers. Resultsfrom five healthy subjects (numbers16–20) are shown. DR0401/FluHA306–318 was used as irrelevant con-trol tetramers in both A and B.
FIGURE 4. Detection of IGRP autoreactive T cells in DR0301 T1D and healthy subjects. A, PBMC or CD4� T cells from DR0301 T1D subjects werestimulated with peptides IGRP13–25 and IGRP226–238. Cells were analyzed by flow cytometry 14 days poststimulation with anti-CD3 and anti-CD4 mAbs,DR0301/IGRP13–25, and DR0301/IGRP226–238 tetramers. Results from five T1D subjects (numbers 1–5) are shown. B, PBMC or CD4� T cells fromDR0301 healthy subjects were stimulated with peptides IGRP13–25 and IGRP226–238. Cells were analyzed by flow cytometry 14 days poststimulation withanti-CD3 and anti-CD4 mAbs, DR0301/IGRP13–25, and DR0301/IGRP226–238 tetramers. Results from five healthy subjects (numbers 11–15) are shown.DR0301/Flu MP169–181 tetramers were used as irrelevant control tetramers in both A and B.
2785The Journal of Immunology
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from

ranged from 33 to 40%, with an average of 36 � 4%, and thepercentage of IL-10-positive cells within the tetramer-positivepopulation ranged from 14 to 33%, with an average of 26 � 8% forfour subjects. For healthy subjects, the percentage of �-IFN-pos-itive cells ranged from 11 to 41%, with an average of 25 � 14%,and the percentage of IL-10-positive cells ranged from 5 to 16%,with an average of 11 � 5% for three subjects. Although the sam-ple size was too small to conclude any significant difference incytokine profiles between the two groups, it is notable that thetetramer-positive T cells from healthy subjects and T1D produceboth �-IFN (suggesting an effector phenotype) and IL-10 (suggest-ing a regulatory phenotype).
Cross-reactivity between IGRP epitopes and G6Pase epitopes
IGRP is one member of the G6Pase family. The other members ofthis family of proteins are G6Pase-� and UGRP. IGRP proteinshows roughly 50% aa sequence homology to other G6Pases.Amino acid alignment indicated that the homology betweenIGRP23–35 and the corresponding region in G6Pase-� and UGRPis minimal. In contrast, amino acid alignment indicated IGRP247–
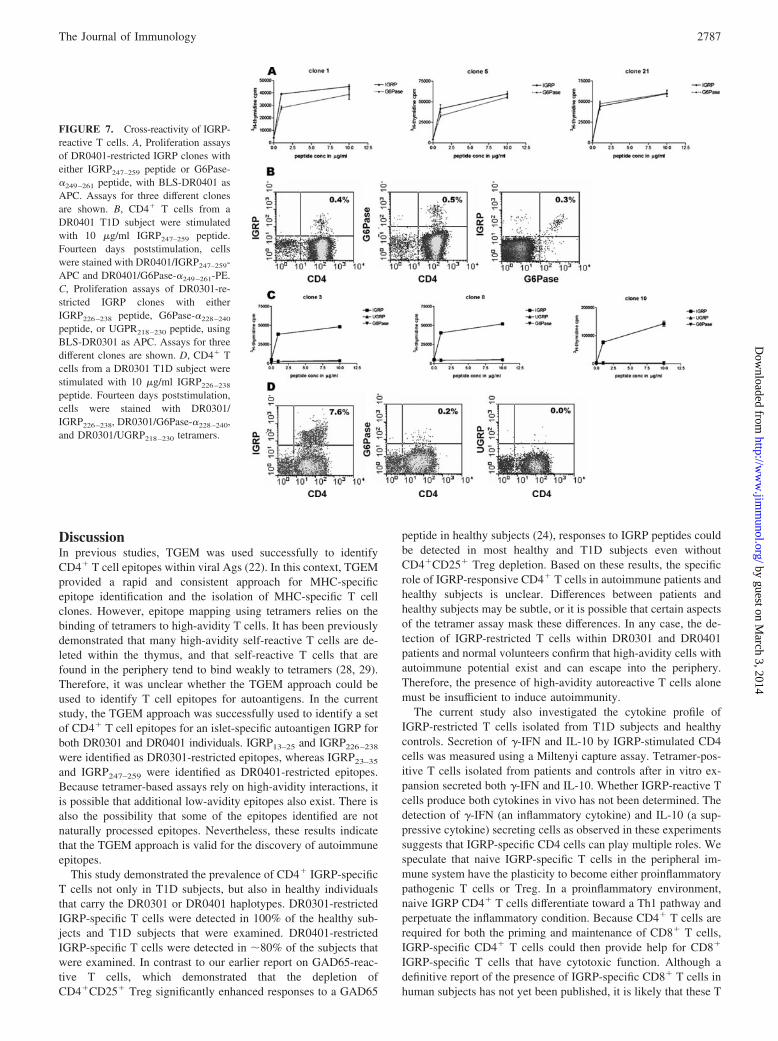
259 sequence has extensive homology to the corresponding se-quences with the other G6Pases. The IGRP247–259 sequence isDWIHIDTTPFAGL, whereas the corresponding sequence forG6Pase-�249–261 and UGRP239–251 are EWVHIDTTPFASL andEWIHVDSRPFASL, respectively (Table III). IGRP247–259 andG6Pase-�249–261 bound to DR0401 with an IC50 of 0.1 �Mand 0.3 �M, respectively, in an in vitro peptide binding assay (datanot shown). Because UGRP239–251 did not bind to DR0401 in thesame assay, this peptide was not investigated further. To examinewhether T cells that responded to IGRP247–259 could cross-reactwith G6Pase-�249–261, IGRP247–259 clones were stimulated witheither IGRP247–259 or G6Pase�249–261 peptide using BLS-DR0401transfectants as APC. Strong proliferation was observed in all ofthe 10 clones examined. Representative results from three differentclones are shown in Fig. 7A. In addition, DR0401-restricted CD4�
T cells stimulated with IGRP247–259 could be stained with bothDR0401/IGRP247–259 and DR0401/G6Pase-�249–261 tetramers(Fig. 7B).
Similarly, we examined whether DR0301-restricted T cells thatresponded to IGRP epitopes could cross-react with homologousG6Pase epitopes. No homology occurs between IGRP13–25 and thecorresponding regions of both G6Pase-� and UGRP, but limited
homology was observed between IGRP226–238 and the correspond-ing regions in G6Pase-� and UGRP. The peptide sequence forIGRP226–238 is RVLNIDLLWSVPI. The corresponding sequencesin G6Pase-�228–240 and UGRP218–230 are KGLGVDLLWTLEKand FTLGLDLSWSISL, respectively (see Table III). Five differentDR0301-restricted IGRP226–228-specific T cells were tested fortheir reactivity toward IGRP226–238, G6Pase-�228–240, andUGRP218–230 peptides in proliferation assays using BLS-DR0301as APC. Although all clones proliferated upon stimulation with thecognate IGRP peptide, no cross-reactivity was observed with theother two peptides. Representative results from three of theseclones are shown in Fig. 7C. In another series of experiments,CD4� T cells from a DR0301 subject were stimulated withIGRP226–238. Fourteen days poststimulation, these cells werestained with DR0301/IGRP226–238, DR0301/G6Pase-�228–240,and DR0301/UGRP218–230 tetramers. A strong staining signal wasobserved with the DR0301/IGRP226–228 tetramers; however, nostaining signal was observed with DR0301/G6Pase-�228–240 tet-ramers and DR0301/UGRP218–230 tetramers (Fig. 7D).
In summary, cross-reactivity was observed between IGRP247–
259 and G6Pase-�249–261 for T cells from DR0401 subjects, but nohomology or cross-reactivity was observed between other corre-sponding epitopes within IGRP and UGRP. Limited homologywas observed between IGRP226–238, G6Pase-�228–240, andUGRP218–230. However, cross-reactivity was not observed witheither of these homologous epitopes for T cells from DR0301subjects.
Table III. Homology between IGRP, G6Pase-�, and UGRP
Peptide Sequence
IGRP247–259 DWIHIDTTPFAGLa
G6Pase-�249–261 EWVHIDTTPFASLb
UGRP239–251 EWIHVDSRPFASL
IGRP226–238 RVLNIDLLWSVPIG6Pase-�228–240 KGLGVDLLWTLEKUGRP218–230 FTLGLDLSWSISL
a The proposed p1, p4, and p9 anchor residues for IGRP are underlined.b Residues of G6Pase-� and UGRP sequences that are identical to the correspond-
ing sequence in IGRP are in bold italics.
FIGURE 6. Cytokine profiles of IGRP-reactive T cells in healthy and T1D subjects. CD4� T cells were isolated from PBMC of DR0401 subjects andstimulated with 10 �g/ml IGRP247–259 peptide. Fourteen days poststimulation, cells were incubated with 10 �g/ml DR0401/IGRP247–259 tetramers for 3 h.Cells were then assayed for cytokine secretion with the Miltenyi Biotec cytokine capturing reagents. For analyses, cells were gated on light scattering andCD4�. The figure shows the profiles of two T1D subjects, and two healthy subjects. For the two T1D subjects as shown, the percentages of �-IFN cellswithin the tetramer-positive populations were 40 and 38%, the percentages of IL-10 cells were 30 and 14%. For the two healthy subjects as shown, thepercentages of �-IFN cells within the tetramer-positive populations were 11 and 41%, the percentages of IL-10 cells were 16 and 14%.
2786 IGRP CD4� T CELLS IN HUMAN T1D
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from
DiscussionIn previous studies, TGEM was used successfully to identifyCD4� T cell epitopes within viral Ags (22). In this context, TGEMprovided a rapid and consistent approach for MHC-specificepitope identification and the isolation of MHC-specific T cellclones. However, epitope mapping using tetramers relies on thebinding of tetramers to high-avidity T cells. It has been previouslydemonstrated that many high-avidity self-reactive T cells are de-leted within the thymus, and that self-reactive T cells that arefound in the periphery tend to bind weakly to tetramers (28, 29).Therefore, it was unclear whether the TGEM approach could beused to identify T cell epitopes for autoantigens. In the currentstudy, the TGEM approach was successfully used to identify a setof CD4� T cell epitopes for an islet-specific autoantigen IGRP forboth DR0301 and DR0401 individuals. IGRP13–25 and IGRP226–238
were identified as DR0301-restricted epitopes, whereas IGRP23–35
and IGRP247–259 were identified as DR0401-restricted epitopes.Because tetramer-based assays rely on high-avidity interactions, itis possible that additional low-avidity epitopes also exist. There isalso the possibility that some of the epitopes identified are notnaturally processed epitopes. Nevertheless, these results indicatethat the TGEM approach is valid for the discovery of autoimmuneepitopes.
This study demonstrated the prevalence of CD4� IGRP-specificT cells not only in T1D subjects, but also in healthy individualsthat carry the DR0301 or DR0401 haplotypes. DR0301-restrictedIGRP-specific T cells were detected in 100% of the healthy sub-jects and T1D subjects that were examined. DR0401-restrictedIGRP-specific T cells were detected in �80% of the subjects thatwere examined. In contrast to our earlier report on GAD65-reac-tive T cells, which demonstrated that the depletion ofCD4�CD25� Treg significantly enhanced responses to a GAD65
peptide in healthy subjects (24), responses to IGRP peptides couldbe detected in most healthy and T1D subjects even withoutCD4�CD25� Treg depletion. Based on these results, the specificrole of IGRP-responsive CD4� T cells in autoimmune patients andhealthy subjects is unclear. Differences between patients andhealthy subjects may be subtle, or it is possible that certain aspectsof the tetramer assay mask these differences. In any case, the de-tection of IGRP-restricted T cells within DR0301 and DR0401patients and normal volunteers confirm that high-avidity cells withautoimmune potential exist and can escape into the periphery.Therefore, the presence of high-avidity autoreactive T cells alonemust be insufficient to induce autoimmunity.
The current study also investigated the cytokine profile ofIGRP-restricted T cells isolated from T1D subjects and healthycontrols. Secretion of �-IFN and IL-10 by IGRP-stimulated CD4cells was measured using a Miltenyi capture assay. Tetramer-pos-itive T cells isolated from patients and controls after in vitro ex-pansion secreted both �-IFN and IL-10. Whether IGRP-reactive Tcells produce both cytokines in vivo has not been determined. Thedetection of �-IFN (an inflammatory cytokine) and IL-10 (a sup-pressive cytokine) secreting cells as observed in these experimentssuggests that IGRP-specific CD4 cells can play multiple roles. Wespeculate that naive IGRP-specific T cells in the peripheral im-mune system have the plasticity to become either proinflammatorypathogenic T cells or Treg. In a proinflammatory environment,naive IGRP CD4� T cells differentiate toward a Th1 pathway andperpetuate the inflammatory condition. Because CD4� T cells arerequired for both the priming and maintenance of CD8� T cells,IGRP-specific CD4� T cells could then provide help for CD8�
IGRP-specific T cells that have cytotoxic function. Although adefinitive report of the presence of IGRP-specific CD8� T cells inhuman subjects has not yet been published, it is likely that these T
FIGURE 7. Cross-reactivity of IGRP-reactive T cells. A, Proliferation assaysof DR0401-restricted IGRP clones witheither IGRP247–259 peptide or G6Pase-�249–261 peptide, with BLS-DR0401 asAPC. Assays for three different clonesare shown. B, CD4� T cells from aDR0401 T1D subject were stimulatedwith 10 �g/ml IGRP247–259 peptide.Fourteen days poststimulation, cellswere stained with DR0401/IGRP247–259-APC and DR0401/G6Pase-�249–261-PE.C, Proliferation assays of DR0301-re-stricted IGRP clones with eitherIGRP226–238 peptide, G6Pase-�228–240
peptide, or UGPR218–230 peptide, usingBLS-DR0301 as APC. Assays for threedifferent clones are shown. D, CD4� Tcells from a DR0301 T1D subject werestimulated with 10 �g/ml IGRP226–238
peptide. Fourteen days poststimulation,cells were stained with DR0301/IGRP226–238, DR0301/G6Pase-�228–240,and DR0301/UGRP218–230 tetramers.
2787The Journal of Immunology
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from

cells will be identified in the near future. In a noninflammatorystate, CD4� IGRP T cells have a more regulatory function. Inter-actions between immature DC and IGRP-specific T cells couldcause the IGRP-reactive T cells to exhibit suppressive function,which would inhibit the activity of effector T cells.
IGRP is one member of a family of homologous G6Pase pro-teins. Extensive homology between IGRP and other family mem-bers of the G6Pase proteins led us to investigate T cell cross-reactivity between homologous regions of the G6Pase proteinfamily members. The homologous epitopes for G6Pase-� andUGRP are summarized in the Results. For the DR0401-restricted Tcells, cross-reactivity between the IGRP epitope and G6Pase-�epitope was observed. However, no cross-reactivity was observedfor UGRP. Cross-reactivity for the DR0301-reactive T cells wasnot detected for either protein. The cross-reactivity of IGRP andG6Pase-�-specific T cells in DR0401 subjects raises the possibilitythat G6Pase-�-expressing tissues could become the target ofIGRP-specific (and, by cross-reaction, G6Pase-�-specific) T cells.
The identities of the primary autoantigens in T1D pathogenesisare still being defined. In mouse models, the most extensively stud-ied Ags include insulin and GAD65. For example, it has beenshown in NOD mice that the presence of a specific insulin epitopeis essential for the development of disease (30). Recent experi-ments in NOD mice indicated that CD8� T cells from the isletinfiltrates of NOD mice can recognize IGRP, and that an increasein the avidity of these T cells is associated with progression ofdisease (5–7). Others described the presence of CD4� IGRP-spe-cific T cells in mice (9). Thus, IGRP could be a major target forislet cell destruction in the NOD model. T cells from the peripheralblood of human T1D subjects have also been studied extensively,implicating GAD65, IA-2, phogrin, insulin, and islet amyloidpolypeptide as autoantigens (16–20, 31–33). A recent report alsodescribed the detection of insulin-specific T cells in pancreaticlymph nodes of T1D subjects (34). The detection of CD4� IGRP-specific T cells in peripheral blood of human subjects in this studyadds IGRP to the list of autoantigens implicated in T1D.
The role of IGRP-specific T cells in T1D is an active area ofresearch. Recent experiments in mice demonstrated that IGRP-specific CD4� T cells in NOD mice delay the onset of autoimmunediabetes in an adoptive T cell transfer animal model (9). The de-tection of IGRP-specific T cells in both healthy and T1D subjectsand the secretion of IL-10 by these cells in this study suggest thatIGRP-specific T cells could have a similar regulatory role in hu-mans. However, it should be noted that CD4� GAD65-reactive Tcells have been demonstrated to have both pathogenic and regu-latory roles in T cell transfer experiments in murine models (35–37). Our group and others (24, 38) have detected GAD65-reactiveT cells in both healthy and T1D subjects. The presence of auto-reactive T cells toward both insulin and IA-2 in both healthy andT1D subjects have also been reported (21). Thus, it is likely thatantigenic-specific effector and Treg are present in the periphery fora variety of autoantigens, and that it is the interplay of these twopopulations that will determine whether clinical autoimmunity ortolerance is the outcome. It should also be noted that the observa-tion of autoantigen-specific T cells in healthy individuals is notconfined to T1D. For example, T cells specific for desmoglein-3have been detected in both healthy subjects and patients with pem-phigus vulgaris (39). Similarly, T cells specific for myelin basicprotein and myelin oligodendrocyte glycoprotein can be detectedin healthy subjects and patients with multiple sclerosis (40–42).All of these observations attest to the prevalence of autoreactive Tcells both in healthy subjects and in patients with a variety ofdifferent autoimmune diseases. Hauben et al. (43) have suggestedthat although a prolonged autoimmune response is pathogenic, a
transient autoimmune response could actually be beneficial to thehost. They also suggested that such a “benign” autoimmune re-sponse may be an essential step for the induction of adaptive Tregto control autoimmunity. The current findings demonstrating thepresence of IGRP-autoreactive T cells in healthy subjects appear tosupport this benign autoimmunity hypothesis. Clearly, more in-vestigation is needed to determine whether IGRP-specific CD4� Tcells are primarily effector cells that accelerate or trigger disease,or regulatory cells that down-regulate the inflammatory processassociated with disease progression.
In summary, we reported in this study the identification andisolation of tetramer-positive IGRP-specific CD4� T cells fromhuman subjects for the first time. IGRP epitopes could be readilymapped using the TGEM approach, even without the removal ofCD25� Tregs. Cross-reactivity was observed between IGRP andG6Pase-� epitopes for DR0401-restricted T cells. The equal prev-alence of autoreactive T cells in healthy subjects and T1D subjectsand their production of both IL-10 and �-IFN support the hypoth-esis that autoreactive T cells with different functional roles coexist.Additional studies aimed at understanding the significance of Ag-specific effector and Treg and the differences between transientbenign autoimmunity and prolonged autoimmunity will be crucial.
AcknowledgmentsWe thank Aru Arumuganathan and Kelly Geubtner for technical assistanceand Matt Warren for secretarial assistance.
DisclosuresThe authors have no financial conflict of interest.
References1. Gianani, R., and G. S. Eisenbarth. 2005. The stages of type 1A diabetes: 2005.
Immunol. Rev. 204: 232–249.2. Noble, J. A., A. M. Valdes, M. Cook, W. Klitz, G. Thomson, and H. A. Erlich.
1996. The role of HLA class II genes in insulin-dependent diabetes mellitus:molecular analysis of 180 Caucasian, multiplex families. Am. J. Hum. Genet. 59:1134–1148.
3. Anderson, M. S., and J. A. Bluestone. 2005. The NOD mouse: a model of im-mune dysregulation. Annu. Rev. Immunol. 23: 447–485.
4. Wong, F. S., and C. A. Janeway, Jr. 1999. The role of CD4 vs. CD8 T cells inIDDM. J. Autoimmun. 13: 290–295.
5. Anderson, B., B. J. Park, J. Verdaguer, A. Amrani, and P. Santamaria. 1999.Prevalent CD8� T cell response against one peptide/MHC complex in autoim-mune diabetes. Proc. Natl. Acad. Sci. USA 96: 9311–9316.
6. Lieberman, S. M., A. M. Evans, B. Han, T. Takaki, Y. Vinnitskaya,J. A. Caldwell, D. V. Serreze, J. Shabanowitz, D. F. Hunt, S. G. Nathenson, et al.2003. Identification of the � cell antigen targeted by a prevalent population ofpathogenic CD8� T cells in autoimmune diabetes. Proc. Natl. Acad. Sci. USA100: 8384–8388.
7. Han, B., P. Serra, J. Yamanouchi, A. Amrani, J. F. Elliott, P. Dickie,T. P. DiLorenzo, and P. Santamaria. 2005. Developmental control of CD8 Tcell-avidity maturation in autoimmune diabetes. J. Clin. Invest. 115: 1879–1887.
8. Han, B., P. Serra, A. Amrani, J. Yamanouchi, A. F. Maree, L. Edelstein-Keshet,and P. Santamaria. 2005. Prevention of diabetes by manipulation of anti-IGRPautoimmunity: high efficiency of a low-affinity peptide. Nat. Med. 11: 645–652.
9. Mukherjee, R., D. Wagar, T. A. Stephens, E. Lee-Chan, and B. Singh. 2005.Identification of CD4� T cell-specific epitopes of islet-specific glucose-6-phos-phatase catalytic subunit-related protein: a novel � cell autoantigen in type 1diabetes. J. Immunol. 174: 5306–5315.
10. Arden, S. D., T. Zahn, S. Steegers, S. Webb, B. Bergman, R. M. O’Brien, andJ. C. Hutton. 1999. Molecular cloning of a pancreatic islet-specific glucose-6-phosphatase catalytic subunit-related protein. Diabetes 48: 531–542.
11. Martin, C. C., L. J. Bischof, B. Bergman, L. A. Hornbuckle, C. Hilliker,C. Frigeri, D. Wahl, C. A. Svitek, R. Wong, J. K. Goldman, et al. 2001. Cloningand characterization of the human and rat islet-specific glucose-6-phosphatasecatalytic subunit-related protein (IGRP) genes. J. Biol. Chem. 276: 25197–25207.
12. Foster, J. D., and R. C. Nordlie. 2002. The biochemistry and molecular biologyof the glucose-6-phosphatase system. Exp. Biol. Med. 227: 601–608.
13. Petrolonis, A. J., Q. Yang, P. J. Tummino, S. M. Fish, A. E. Prack, S. Jain,T. F. Parsons, P. Li, N. A. Dales, L. Ge, et al. 2004. Enzymatic characterizationof the pancreatic islet-specific glucose-6-phosphatase-related protein (IGRP).J. Biol. Chem. 279: 13976–13983.
14. Shieh, J. J., C. J. Pan, B. C. Mansfield, and J. Y. Chou. 2004. The islet-specificglucose-6-phosphatase-related protein, implicated in diabetes, is a glycoproteinembedded in the endoplasmic reticulum membrane. FEBS Lett. 562: 160–164.
15. Copeman, J. B., F. Cucca, C. M. Hearne, R. J. Cornall, P. W. Reed,K. S. Ronningen, D. E. Undlien, L. Nistico, R. Buzzetti, R. Tosi, et al. 1995.
2788 IGRP CD4� T CELLS IN HUMAN T1D
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from

Linkage disequilibrium mapping of a type 1 diabetes susceptibility gene(IDDM7) to chromosome 2q31–q33. Nat. Genet. 9: 80–85.
16. Atkinson, M. A., D. L. Kaufman, L. Campbell, K. A. Gibbs, S. C. Shah, D. F. Bu,M. G. Erlander, A. J. Tobin, and N. K. Maclaren. 1992. Response of peripheral-blood mononuclear cells to glutamate decarboxylase in insulin-dependent diabe-tes. Lancet 339: 458–459.
17. Durinovic-Bello, I., M. Hummel, and A. G. Ziegler. 1996. Cellular immune re-sponse to diverse islet cell antigens in IDDM. Diabetes 45: 795–800.
18. Durinovic-Bello, I., M. Schlosser, M. Riedl, N. Maisel, S. Rosinger,H. Kalbacher, M. Deeg, M. Ziegler, J. Elliott, B. O. Roep, et al. 2004. Pro- andanti-inflammatory cytokine production by autoimmune T cells against preproin-sulin in HLA-DRB1*04, DQ8 Type 1 diabetes. Diabetologia 47: 439–450.
19. Peakman, M., E. J. Stevens, T. Lohmann, P. Narendran, J. Dromey,A. Alexander, A. J. Tomlinson, M. Trucco, J. C. Gorga, and R. M. Chicz. 1999.Naturally processed and presented epitopes of the islet cell autoantigen IA-2eluted from HLA-DR4. J. Clin. Invest. 104: 1449–1457.
20. Herzog, B. A., P. A. Ott, M. T. Dittrich, S. Quast, A. Y. Karulin, H. Kalbacher,W. Karges, M. Tary-Lehmann, P. V. Lehmann, B. O. Boehm, andI. Durinovic-Bello. 2004. Increased in vivo frequency of IA-2 peptide-reactiveIFN��/IL-4� T cells in type 1 diabetic subjects. J. Autoimmun. 23: 45–54.
21. Arif, S., T. I. Tree, T. P. Astill, J. M. Tremble, A. J. Bishop, C. M. Dayan,B. O. Roep, and M. Peakman. 2004. Autoreactive T cell responses show proin-flammatory polarization in diabetes but a regulatory phenotype in health. J. Clin.Invest. 113: 451–463.
22. Novak, E. J., A. W. Liu, J. A. Gebe, B. Falk, G. T. Nepom, D. M. Koelle, andW. W. Kwok. 2001. Tetramer guided epitope mapping: rapid identification andcharacterization of immunodominant CD4� T cell epitopes from complex anti-gens. J. Immunol. 166: 6665–6670.
23. Novak, E. J., A. W. Liu, G. T. Nepom, and W. W. Kwok. 1999. MHC class IItetramers identify peptide-specific human CD4� T cells proliferating in responseto influenza A antigen. J. Clin. Invest. 104: R63–R67.
24. Danke, N. A., D. M. Koelle, C. Yee, S. Beheray, and W. W. Kwok. 2004.Autoreactive T cells in healthy individuals. J. Immunol. 172: 5967–5972.
25. Kovats, S., S. Drover, W. H. Marshall, D. Freed, P. E. Whiteley, G. T. Nepom,and J. S. Blum. 1994. Coordinate defects in human histocompatibility leukocyteantigen class II expression and antigen presentation in bare lymphocyte syn-drome. J. Exp. Med. 179: 2017–2022.
26. Geluk, A., K. E. van Meijgaarden, S. Southwood, C. Oseroff, J. W. Drijfhout,R. R. de Vries, T. H. Ottenhoff, and A. Sette. 1994. HLA-DR3 molecules canbind peptides carrying two alternative specific submotifs. J. Immunol. 152:5742–5748.
27. Sette, A., J. Sidney, C. Oseroff, M. F. Del Guercio, S. Southwood, T. Arrhenius,M. F. Powell, S. M. Colon, F. C. Gaeta, and H. M. Grey. 1993. HLA DR4w4-binding motifs illustrate the biochemical basis of degeneracy and specificity inpeptide-DR interactions. J. Immunol. 151: 3163–3170.
28. de Visser, K. E., T. A. Cordaro, D. Kioussis, J. B. Haanen, T. N. Schumacher, andA. M. Kruisbeek. 2000. Tracing and characterization of the low-avidity self-specific T cell repertoire. Eur. J. Immunol. 30: 1458–1468.
29. Gebe, J. A., B. A. Falk, K. A. Rock, S. A. Kochik, A. K. Heninger, H. Reijonen,W. W. Kwok, and G. T. Nepom. 2003. Low-avidity recognition by CD4� T cellsdirected to self-antigens. Eur. J. Immunol. 33: 1409–1417.
30. Nakayama, M., N. Abiru, H. Moriyama, N. Babaya, E. Liu, D. Miao, L. Yu,D. R. Wegmann, J. C. Hutton, J. F. Elliott, and G. S. Eisenbarth. 2005. Prime rolefor an insulin epitope in the development of type 1 diabetes in NOD mice. Nature435: 220–223.
31. Kelemen, K., P. A. Gottlieb, A. L. Putnam, H. W. Davidson, D. R. Wegmann,and J. C. Hutton. 2004. HLA-DQ8-associated T cell responses to the diabetesautoantigen phogrin (IA-2�) in human prediabetes. J. Immunol. 172: 3955–3962.
32. Panagiotopoulos, C., H. Qin, R. Tan, and C. B. Verchere. 2003. Identification ofa �-cell-specific HLA class I restricted epitope in type 1 diabetes. Diabetes 52:2647–2651.
33. Toma, A., S. Haddouk, J. P. Briand, L. Camoin, H. Gahery, F. Connan,D. Dubois-Laforgue, S. Caillat-Zucman, J. G. Guillet, J. C. Carel, et al. 2005.Recognition of a subregion of human proinsulin by class I-restricted T cells intype 1 diabetic patients. Proc. Natl. Acad. Sci. USA 102: 10581–10586.
34. Kent, S. C., Y. Chen, L. Bregoli, S. M. Clemmings, N. S. Kenyon, C. Ricordi,B. J. Hering, and D. A. Hafler. 2005. Expanded T cells from pancreatic lymphnodes of type 1 diabetic subjects recognize an insulin epitope. Nature 435:224–228.
35. Zekzer, D., F. S. Wong, O. Ayalon, I. Millet, M. Altieri, S. Shintani,M. Solimena, and R. S. Sherwin. 1998. GAD-reactive CD4� Th1 cells inducediabetes in NOD/SCID mice. J. Clin. Invest. 101: 68–73.
36. Kim, S. K., K. V. Tarbell, M. Sanna, M. Vadeboncoeur, T. Warganich, M. Lee,M. Davis, and H. O. McDevitt. 2004. Prevention of type I diabetes transfer byglutamic acid decarboxylase 65 peptide 206–220-specific T cells. Proc. Natl.Acad. Sci. USA 101: 14204–14209.
37. You, S., C. Chen, W. H. Lee, T. Brusko, M. Atkinson, and C. P. Liu. 2004.Presence of diabetes-inhibiting, glutamic acid decarboxylase-specific, IL-10-de-pendent, regulatory T cells in naive nonobese diabetic mice. J. Immunol. 173:6777–6785.
38. Viglietta, V., S. C. Kent, T. Orban, and D. A. Hafler. 2002. GAD65-reactive Tcells are activated in patients with autoimmune type 1a diabetes. J. Clin. Invest.109: 895–903.
39. Veldman, C. M., K. L. Gebhard, W. Uter, R. Wassmuth, J. Grotzinger,E. Schultz, and M. Hertl. 2004. T cell recognition of desmoglein 3 peptides inpatients with pemphigus vulgaris and healthy individuals. J. Immunol. 172:3883–3892.
40. Martin, R., R. Voskuhl, M. Flerlage, D. E. McFarlin, and H. F. McFarland. 1993.Myelin basic protein-specific T-cell responses in identical twins discordant orconcordant for multiple sclerosis. Ann. Neurol. 34: 524–535.
41. Van der, A. A., N. Hellings, C. C. Bernard, J. Raus, and P. Stinissen. 2003.Functional properties of myelin oligodendrocyte glycoprotein-reactive T cells inmultiple sclerosis patients and controls. J. Neuroimmunol. 137: 164–176.
42. Scholz, C., K. T. Patton, D. E. Anderson, G. J. Freeman, and D. A. Hafler. 1998.Expansion of autoreactive T cells in multiple sclerosis is independent of exoge-nous B7 costimulation. J. Immunol. 160: 1532–1538.
43. Hauben, E., M. G. Roncarolo, U. Nevo, and M. Schwartz. 2005. Beneficial au-toimmunity in Type 1 diabetes mellitus. Trends Immunol. 26: 248–253.
2789The Journal of Immunology
by guest on March 3, 2014
http://ww
w.jim
munol.org/
Dow
nloaded from




















