
Ischemia in three left ventricular regions: Insights into the pathogenesis of acute ischemic mitral...
13
2003;125:559-569 J Thorac Cardiovasc Surg and D. Craig Miller Daughters, Paul Dagum, Mary K. Zasio, Sidney Lo, Trevor Hastie, Neil B. Ingels, Jr Tomasz A. Timek, David T. Lai, Frederick Tibayan, David Liang, George T. ischemic mitral regurgitation Ischemia in three left ventricular regions: Insights into the pathogenesis of acute http://jtcs.ctsnetjournals.org/cgi/content/full/125/3/559 located on the World Wide Web at: The online version of this article, along with updated information and services, is 2003 American Association for Thoracic Surgery Association for Thoracic Surgery and the Western Thoracic Surgical Association. Copyright © is the official publication of the American The Journal of Thoracic and Cardiovascular Surgery on June 6, 2013 jtcs.ctsnetjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Ischemia in three left ventricular regions: Insights into the pathogenesis of acute ischemic mitral...

2003;125:559-569 J Thorac Cardiovasc Surgand D. Craig Miller
Daughters, Paul Dagum, Mary K. Zasio, Sidney Lo, Trevor Hastie, Neil B. Ingels, Jr Tomasz A. Timek, David T. Lai, Frederick Tibayan, David Liang, George T.
ischemic mitral regurgitationIschemia in three left ventricular regions: Insights into the pathogenesis of acute
http://jtcs.ctsnetjournals.org/cgi/content/full/125/3/559located on the World Wide Web at:
The online version of this article, along with updated information and services, is
2003 American Association for Thoracic Surgery Association for Thoracic Surgery and the Western Thoracic Surgical Association. Copyright ©
is the official publication of the AmericanThe Journal of Thoracic and Cardiovascular Surgery
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from
Ischemia in three left ventricular regions: Insights into thepathogenesis of acute ischemic mitral regurgitationTomasz A. Timek, MDa,b
David T. Lai, FRACSa
Frederick Tibayan, MDa
David Liang, MD, PhDc
George T. Daughters, MSa,d
Paul Dagum, MD, PhDa
Mary K. Zasio, BAa
Sidney Lo, MDc
Trevor Hastie, PhDe
Neil B. Ingels, Jr, PhDa,d
D. Craig Miller, MDa
Background: Acute posterolateral left ventricular ischemia in sheep results inischemic mitral regurgitation, but the effects of ischemia in other left ventricularregions on ischemic mitral regurgitation is unknown.
Methods: Six adult sheep had radiopaque markers placed on the left ventricle, mitralannulus, and anterior and posterior mitral leaflets at the valve center and near theanterior and posterior commissures. After 6 to 8 days, animals were studied withbiplane videofluoroscopy and transesophageal echocardiography before and duringsequential balloon occlusion of the left anterior descending, distal left circumflex,and proximal left circumflex coronary arteries. Time of valve closure was defined asthe time when the distance between leaflet edge markers reached its minimumplateau, and systolic leaflet edge separation distance was calculated on the basis ofleft ventricular ejection.
Results: Only proximal left circumflex coronary artery occlusion resulted inischemic mitral regurgitation, which was central and holosystolic. Delayed valveclosure (anterior commissure, 58 � 29 vs 92 � 24 ms; valve center, 52 � 26 vs92 � 23 ms; posterior commissure, 60 � 30 vs 94 � 14 ms; all P � .05) andincreased leaflet edge separation distance during ejection (mean increase, 2.2 �1.5 mm, 2.1 � 1.9 mm, and 2.1 � 1.5 mm at the anterior commissure, valvecenter, and posterior commissure, respectively; P � .05 for all) was seen duringproximal left circumflex coronary artery occlusion but not during left anteriordescending or distal left circumflex coronary artery occlusion. Ischemic mitralregurgitation was associated with a 19% � 10% increase in mitral annular area,and displacement of both papillary muscle tips away from the septal annulus atend systole.
Conclusions: Acute ischemic mitral regurgitation in sheep occurred only afterproximal left circumflex coronary artery occlusion along with delayed valve closurein early systole and increased leaflet edge separation throughout ejection in all 3leaflet coaptation sites. The degree of left ventricular systolic dysfunction induceddid not correlate with ischemic mitral regurgitation, but both altered valvular andsubvalvular 3-dimensional geometry were necessary to produce ischemic mitralregurgitation during acute left ventricular ischemia.
From the Department of Cardiovascularand Thoracic Surgery,a Division of Cardio-vascular Medicine,c and the Department ofBiostatistics,e Stanford University Schoolof Medicine, Stanford; the Department ofSurgery,b Loma Linda University MedicalCenter, Loma Linda; and the Laboratory ofCardiovascular Physiology and Biophys-ics,d Research Institute of the Palo AltoMedical Foundation, Palo Alto, Calif.
Supported by grants HL-29589 and HL-67025 from the National Heart, Lung, andBlood Institute. Drs Timek, Tibayan, Da-gum, and Lai are Carl and Leah McConnellCardiovascular Surgical Research Fellows.Drs Timek, Dagum, and Tibayan were alsosupported by NHLBI Individual ResearchService Awards HL-10452, HL-10000, andHL-67563, respectively. Dr Timek is also arecipient of the Thoracic Surgery Founda-tion Research Fellowship Award. Dr Laiwas supported by a fellowship from theAmerican Heart Association, WesternStates Affiliate.
Read at the Eighty-second Annual Meetingof The American Association for ThoracicSurgery, Washington, DC, May 5-8, 2002.
Received for publication April 29, 2002;revisions requested July 8, 2002; revisionsreceived Aug 4, 2002; accepted for publi-cation Aug 15, 2002.
Address for reprints: D. Craig Miller, MD,Department of Cardiothoracic Surgery,Falk Cardiovascular Research Center, Stan-ford University School of Medicine, Stan-ford, CA 94305-5247 (E-mail:[email protected]).
J Thorac Cardiovasc Surg 2003;125:559-69
Copyright © 2003 by The American Asso-ciation for Thoracic Surgery
0022-5223/2003 $30.00�0
doi:10.1067/mtc.2003.43
Timek et al Surgery for Acquired Cardiovascular Disease
The Journal of Thoracic and Cardiovascular Surgery ● Volume 125, Number 3 559
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from

Ischemic mitral regurgitation (IMR) presents a chal-lenging clinical problem associated with subopti-mal surgical results and poor prognosis caused bythe underlying left ventricular (LV) dysfunctioncaused by myocardial ischemia and infarction.1-3
Mitral valve repair might offer better outcomes inthis patient population than valve replacement,4 but nostandardized repair methods exist on the basis of the variousleaflet-motion abnormalities seen. Despite a plethora ofexperimental and clinical studies investigating the 3-dimen-sional (3-D) valvular and subvalvular geometric perturba-tions associated with IMR, knowledge of the precise mech-anisms responsible for valvular incompetence remainselusive. Mitral annular changes,5,6 systolic leaflet apicaltethering,6-10 more spherical LV shape,11,12 and impairedLV systolic function13 have all been suggested as contrib-uting factors, but a more detailed understanding of theunderlying mechanisms is needed to guide better surgicaltreatment.
In prior studies with radiopaque marker methods insheep, we showed that proximal left circumflex (LCx) cor-onary artery occlusion results in acute posterolateral LVischemia and IMR caused by delayed valve closure duringvery early systole5 and perturbed leaflet 3-D geometrythroughout ejection.14 Others have attributed acute IMR insimilar animal models to papillary muscle discoordinationat end systole.10 These and related studies had limitations,one of which was that neither the timing nor the location ofthe regurgitant jet could be determined from transthorac-ic5,14 or subdiaphragmatic10 echocardiography. Thereforethe observed 3-D perturbations in valvular and subvalvulardynamic geometry arising during acute ischemia could notbe correlated either spatially or temporally with the echo-cardiographic regurgitant leak nor could the pathogenesis ofIMR as a function of ischemia in other LV regions beexamined. Our previous experiments examined leaflet dy-namics only at the central edge of the leaflets not allowingdetection of possible changes occurring near the commis-sures; also, the effects of ischemia in other LV regions onmitral competence and valvular dynamics was not exam-ined. To gain more insight into the mechanistic pathogen-esis of IMR, we used transesophageal Doppler echocardi-ography and biplane videofluoroscopy of multiple leafletmarkers to study the effects of posterolateral LV ischemiacaused by proximal LCx (pLCx) coronary artery occlusionand acute ischemia in other LV regions (ie, occlusion of theleft anterior descending [LAD] coronary artery or distalLCx [dLCx] coronary artery) on mitral valve 3-D dynamicgeometry and competence.
MethodsSurgical PreparationThe surgical preparation has previously been described15 and willbe presented only in abbreviated form. Six adult sheep (71 � 13
kg) were premedicated with ketamine (25 mg/kg administeredintramuscularly), and anesthesia was induced with sodium thio-pental (6.8 mg/kg administered intravenously) and maintainedwith inhalational isoflurane (1%-2.5%). Through a left thoracot-omy, 8 tantalum myocardial markers (inner diameter, 0.8 mm;outer diameter, 1.3 mm; length, 1.5-3.0 mm) were inserted in theLV epicardial layer along 4 equally spaced longitudinal meridians,as shown in Figure 1. After establishment of cardiopulmonarybypass with the heart arrested, a single tantalum marker was placedat the tip and base of both papillary muscles (Figure 1), and 8tantalum markers were sutured around the circumference of themitral annulus (one near each commissure and 3 along the septaland lateral annulus, Figure 2). Two miniature gold markers weresutured at the central edge of each leaflet, and 4 additional markerswere sewn on each leaflet edge halfway between the central leafletedge marker and the anterior and posterior commissures (Figure2). After completion of marker placement, the animal was re-warmed, the atriotomy was closed, the crossclamp was removed,the heart was resuscitated, and the animal was weaned frombypass. Cardiopulmonary bypass time was 81 � 6 minutes, withan aortic crossclamp time of 61 � 3 minutes. A micromanometerpressure transducer (PA4.5-X6, Konigsberg Instruments, Inc) wasplaced in the LV chamber through the apex. Proper myocardialmarker position was confirmed in all animals on postmortemexamination.
Experimental ProtocolAfter 7 � 1 (mean �1 SD) days, each animal was taken to thecardiac catheterization laboratory, sedated with ketamine (1-4 mg� kg�1 � h�1 administered intravenously) and diazepam (5 mgintravenous bolus as needed), intubated, and mechanically venti-lated (veterinary anesthesia ventilator 2000, Halowell EMC). Anesmolol intravenous infusion (20-50 �g � kg�1 � min�1) mini-mized reflex sympathetic responses. Coronary artery balloon oc-clusion (1-4 minutes), as described previously,5 was performed at3 locations in sequential fashion: proximal LAD coronary artery(proximal to the first diagonal), dLCx coronary artery (distal to thesecond obtuse marginal), and pLCx coronary artery (proximal tothe first obtuse marginal).
Videofluoroscopic marker image recordings were acquired be-fore and during induction of ischemia at each location with simul-taneous transesophageal color Doppler echocardiography to assessmitral regurgitation (MR). After each data-acquisition run, a 3- to5-minute period of stabilization was allowed before data acquisi-tions were repeated. MR was graded on the basis of regurgitant jetextent and width as none (0), mild (�1), moderate (�2), moderateto severe (�3), or severe (�4) by an experienced echocardiogra-pher (D.L.).
All animals received humane care in compliance with the“Principles of Laboratory Animal Care” formulated by the Na-tional Society for Medical Research and the “Guide for Care andUse of Laboratory Animals” prepared by the National Academy ofSciences and published by the National Institutes of Health(DHEW NIHG publication no. 85-23, revised 1985). This studywas approved by the Stanford University Medical School Labora-tory Research Animal Review committee and conducted accordingto Stanford University policy.
Surgery for Acquired Cardiovascular Disease Timek et al
560 The Journal of Thoracic and Cardiovascular Surgery ● March 2003
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from

Data AcquisitionImages were acquired with the animal in the right lateral decubitusposition with a Philips Optimus 2000 biplane Lateral ARC 2/PolyDIAGNOST C2 system (Philips Medical Systems), with the imageintensifier in the 9-inch fluoroscopic mode. Data from 2 radio-graphic views were digitized and merged to yield 3-D coordinatesfor each of the radiopaque markers every 16.7 ms by usingcustom-designed software.16 Ascending aortic pressure, LV pres-sure, and electrocardiographic voltage signals were digitized andrecorded simultaneously during marker data acquisition.
Data AnalysisHemodynamics and cardiac cycle timing markers. Two to 3
consecutive steady-state beats immediately before occlusion ofany coronary artery were averaged and defined as preischemia datafor each animal. Similarly, 2 to 3 beats during occlusion of theLAD, dLCx, and pLCx coronary arteries were averaged and de-fined as ischemia data. During each cardiac cycle, end systole wasdefined as the time of the videofluoroscopic frame containing thepoint of peak negative rate of LV pressure decrease (�dP/dt),whereas end diastole was defined as the videofluoroscopic framecontaining the peak of the electrocardiographic R wave. Instanta-neous LV volume was calculated from the positions of the epicar-dial LV markers and annular markers by using a space-fillingmultiple tetrahedral volume method for each frame (ie, every 16.7ms).17 Although myocardial volume is included in calculation ofLV volume, relative changes in LV chamber size are accuratelymeasured by using the epicardial marker coordinates.
Mitral leaflet and annular dynamics. Mitral valve-closuretime was defined as the time at which leaflet edge separationreached its minimum plateau. Leaflet separation was measured asdistance in 3-D space between the 2 leaflet edge markers at thecenter of the valve and toward the anterior and posterior commis-sures (Figure 2). Leaflet edge separation throughout the cardiaccycle for each animal was represented by a unique continuousfunction generated by spline-fitting computer software (S-Plus,Mathsoft, Inc) to identify objectively the time of valve closure.Valve closure for each leaflet region (anterior commissure, valvecenter, and posterior commissure) was defined as the time after enddiastole at which the first time derivative with respect to time ofthe associated spline function decreased to less than 0.002 cm/s (avalue reflecting the beginning of the leaflet edge distance mini-mum plateau). Leaflet edge separation at each leaflet edge markerpair was determined for each experimental condition at 25%, 50%,75%, and 100% of LV ejected LV stroke volume to assess leafletseparation during systole. Mitral annular area was calculated as thesum of the areas of 8 triangles formed by consecutive adjacentmarker pairs on the annulus and the annular centroid. The septal-lateral (S-L) diameter of the annulus (clinically referred to as theanterior-posterior dimension) was calculated as the distance in 3-Dspace between the 2 markers placed in the middle of the septal andlateral mitral annulus, respectively. The commissure-commissure(C-C) diameter was calculated as the distance between the 2annular commissural markers. Papillary muscle percentage short-ening was determined as the change from end diastole to endsystole in distance between the papillary muscle tip and basemarkers divided by the distance at end diastole.
Statistical analysis. All data are reported as means � 1 SD.Hemodynamic and marker-derived data from 2 to 3 consecutivesteady-state beats that were time aligned at end diastole and datafrom these beats were averaged for each animal. The data wereanalyzed over 20 frames before and 20 frames after end diastole(total time of 667 ms), thereby allowing assessment of variablesover the entire cardiac cycle. Data were compared by using theStudent t test for paired comparisons and repeated-measures anal-ysis of variance (ANOVA) when appropriate.
Figure 1. Miniature radiopaque marker array (filled circles, myo-cardial; filled squares, papillary) used for the left ventricle in thisexperimental study. PPM, Posterior papillary muscle; APM, an-terior papillary muscle.
Figure 2. Schematic diagram of the implanted mitral annular(filled squares) and mitral leaflet (filled circles) markers. Leafletedge marker pairs were implanted at the valve center (CENT),halfway between the center and the anterior commissure(ACOM), and halfway between the center and the posterior com-missure (PCOM). AML, Anterior mitral leaflet; PML, posteriormitral leaflet.
Timek et al Surgery for Acquired Cardiovascular Disease
The Journal of Thoracic and Cardiovascular Surgery ● Volume 125, Number 3 561
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from
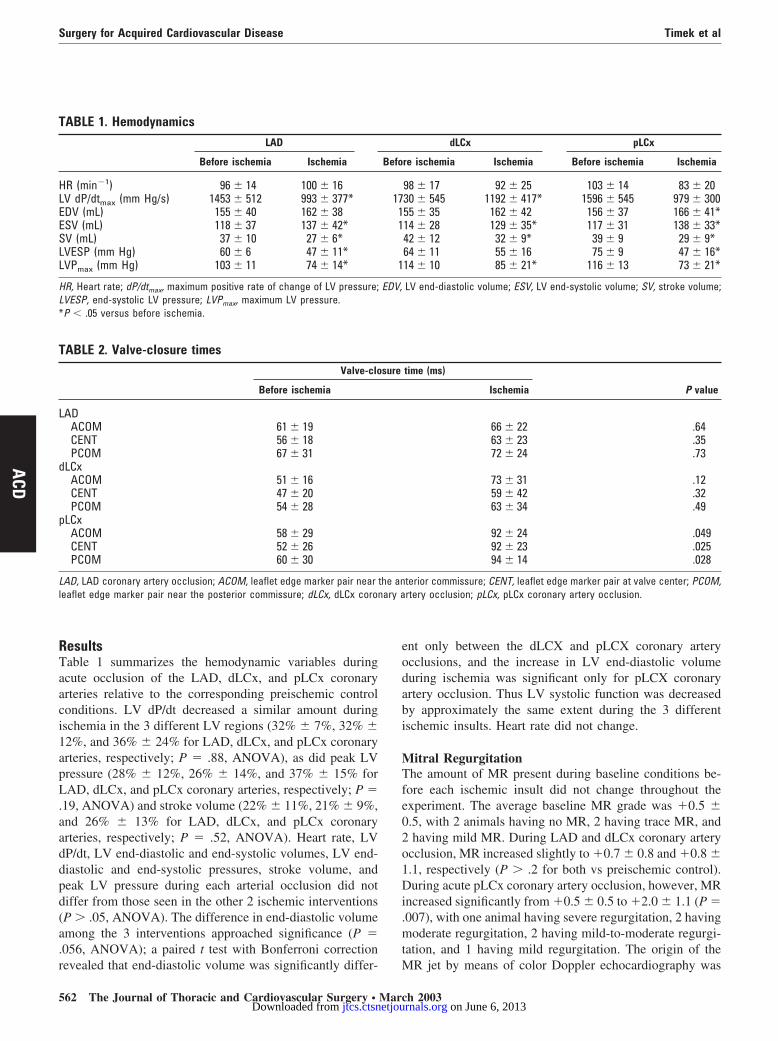
ResultsTable 1 summarizes the hemodynamic variables duringacute occlusion of the LAD, dLCx, and pLCx coronaryarteries relative to the corresponding preischemic controlconditions. LV dP/dt decreased a similar amount duringischemia in the 3 different LV regions (32% � 7%, 32% �12%, and 36% � 24% for LAD, dLCx, and pLCx coronaryarteries, respectively; P � .88, ANOVA), as did peak LVpressure (28% � 12%, 26% � 14%, and 37% � 15% forLAD, dLCx, and pLCx coronary arteries, respectively; P �.19, ANOVA) and stroke volume (22% � 11%, 21% � 9%,and 26% � 13% for LAD, dLCx, and pLCx coronaryarteries, respectively; P � .52, ANOVA). Heart rate, LVdP/dt, LV end-diastolic and end-systolic volumes, LV end-diastolic and end-systolic pressures, stroke volume, andpeak LV pressure during each arterial occlusion did notdiffer from those seen in the other 2 ischemic interventions(P � .05, ANOVA). The difference in end-diastolic volumeamong the 3 interventions approached significance (P �.056, ANOVA); a paired t test with Bonferroni correctionrevealed that end-diastolic volume was significantly differ-
ent only between the dLCX and pLCX coronary arteryocclusions, and the increase in LV end-diastolic volumeduring ischemia was significant only for pLCX coronaryartery occlusion. Thus LV systolic function was decreasedby approximately the same extent during the 3 differentischemic insults. Heart rate did not change.
Mitral RegurgitationThe amount of MR present during baseline conditions be-fore each ischemic insult did not change throughout theexperiment. The average baseline MR grade was �0.5 �0.5, with 2 animals having no MR, 2 having trace MR, and2 having mild MR. During LAD and dLCx coronary arteryocclusion, MR increased slightly to �0.7 � 0.8 and �0.8 �1.1, respectively (P � .2 for both vs preischemic control).During acute pLCx coronary artery occlusion, however, MRincreased significantly from �0.5 � 0.5 to �2.0 � 1.1 (P �.007), with one animal having severe regurgitation, 2 havingmoderate regurgitation, 2 having mild-to-moderate regurgi-tation, and 1 having mild regurgitation. The origin of theMR jet by means of color Doppler echocardiography was
TABLE 1. HemodynamicsLAD dLCx pLCx
Before ischemia Ischemia Before ischemia Ischemia Before ischemia Ischemia
HR (min�1) 96 � 14 100 � 16 98 � 17 92 � 25 103 � 14 83 � 20LV dP/dtmax (mm Hg/s) 1453 � 512 993 � 377* 1730 � 545 1192 � 417* 1596 � 545 979 � 300EDV (mL) 155 � 40 162 � 38 155 � 35 162 � 42 156 � 37 166 � 41*ESV (mL) 118 � 37 137 � 42* 114 � 28 129 � 35* 117 � 31 138 � 33*SV (mL) 37 � 10 27 � 6* 42 � 12 32 � 9* 39 � 9 29 � 9*LVESP (mm Hg) 60 � 6 47 � 11* 64 � 11 55 � 16 75 � 9 47 � 16*LVPmax (mm Hg) 103 � 11 74 � 14* 114 � 10 85 � 21* 116 � 13 73 � 21*
HR, Heart rate; dP/dtmax, maximum positive rate of change of LV pressure; EDV, LV end-diastolic volume; ESV, LV end-systolic volume; SV, stroke volume;LVESP, end-systolic LV pressure; LVPmax, maximum LV pressure.*P � .05 versus before ischemia.
TABLE 2. Valve-closure timesValve-closure time (ms)
P valueBefore ischemia Ischemia
LADACOM 61 � 19 66 � 22 .64CENT 56 � 18 63 � 23 .35PCOM 67 � 31 72 � 24 .73
dLCxACOM 51 � 16 73 � 31 .12CENT 47 � 20 59 � 42 .32PCOM 54 � 28 63 � 34 .49
pLCxACOM 58 � 29 92 � 24 .049CENT 52 � 26 92 � 23 .025PCOM 60 � 30 94 � 14 .028
LAD, LAD coronary artery occlusion; ACOM, leaflet edge marker pair near the anterior commissure; CENT, leaflet edge marker pair at valve center; PCOM,leaflet edge marker pair near the posterior commissure; dLCx, dLCx coronary artery occlusion; pLCx, pLCx coronary artery occlusion.
Surgery for Acquired Cardiovascular Disease Timek et al
562 The Journal of Thoracic and Cardiovascular Surgery ● March 2003
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from
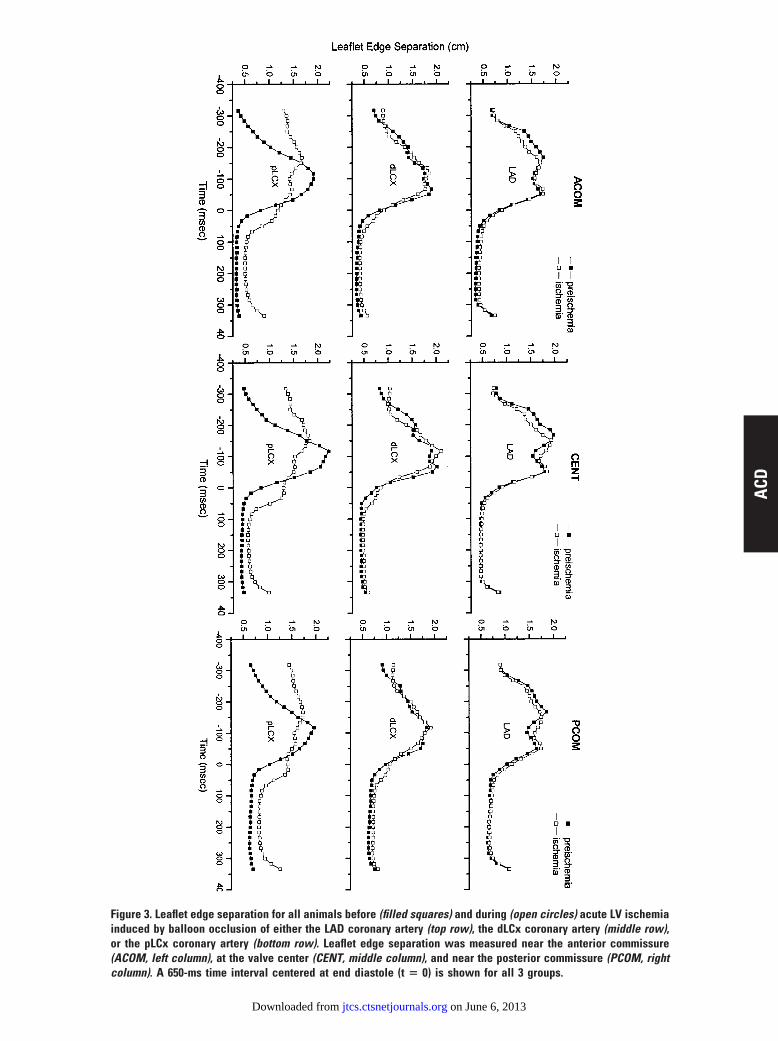
Figure 3. Leaflet edge separation for all animals before (filled squares) and during (open circles) acute LV ischemiainduced by balloon occlusion of either the LAD coronary artery (top row), the dLCx coronary artery (middle row),or the pLCx coronary artery (bottom row). Leaflet edge separation was measured near the anterior commissure(ACOM, left column), at the valve center (CENT, middle column), and near the posterior commissure (PCOM, rightcolumn). A 650-ms time interval centered at end diastole (t � 0) is shown for all 3 groups.
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from
central in 5 of the 6 animals and posterolateral in 1 of theanimals. Evaluation of the timing of the regurgitant jet wasfeasible in 4 animals: all 4 had holosystolic MR.
Mitral Valve Closure and Leaflet Edge SeparationValve-closure times with respect to end diastole for eachischemic intervention and at each leaflet edge marker pairlocation (anterior commissure, valve center, and posteriorcommissure) are summarized in Table 2. Neither LAD nordLCx coronary artery occlusion altered valve-closure time,but pLCx coronary artery occlusion significantly delayedvalve closure at all 3 leaflet locations. Leaflet edge separa-tion throughout the cardiac cycle for each leaflet edgemarker pair during the 3 ischemic interventions is shown inFigure 3. Delayed early systolic valve closure (leaflet loi-tering) was observed during pLCx coronary artery occlusionbut not during LAD or dLCx coronary artery occlusion.Leaflet edge separation was greater during systole versuspreischemic control conditions during pLCx coronary arteryocclusion, but this was not observed during the other 2ischemic interventions (Figure 3). Leaflet edge separationdistance was calculated at 25%, 50%, 75%, and 100% of LV
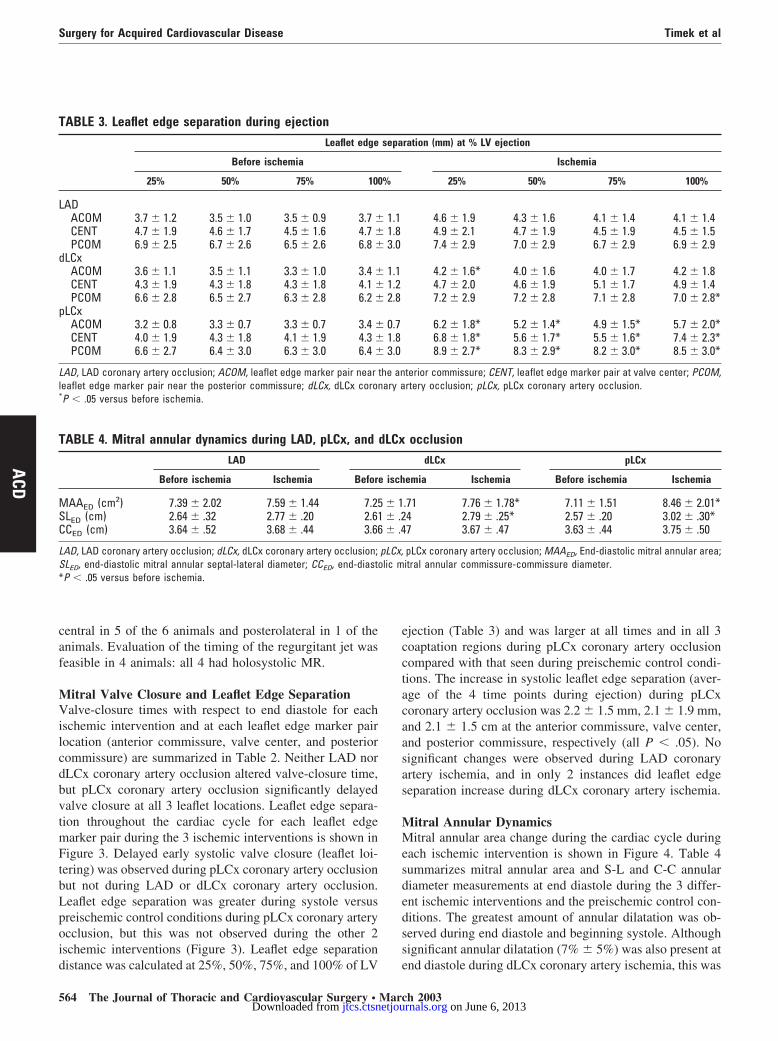
ejection (Table 3) and was larger at all times and in all 3coaptation regions during pLCx coronary artery occlusioncompared with that seen during preischemic control condi-tions. The increase in systolic leaflet edge separation (aver-age of the 4 time points during ejection) during pLCxcoronary artery occlusion was 2.2 � 1.5 mm, 2.1 � 1.9 mm,and 2.1 � 1.5 cm at the anterior commissure, valve center,and posterior commissure, respectively (all P � .05). Nosignificant changes were observed during LAD coronaryartery ischemia, and in only 2 instances did leaflet edgeseparation increase during dLCx coronary artery ischemia.
Mitral Annular DynamicsMitral annular area change during the cardiac cycle duringeach ischemic intervention is shown in Figure 4. Table 4summarizes mitral annular area and S-L and C-C annulardiameter measurements at end diastole during the 3 differ-ent ischemic interventions and the preischemic control con-ditions. The greatest amount of annular dilatation was ob-served during end diastole and beginning systole. Althoughsignificant annular dilatation (7% � 5%) was also present atend diastole during dLCx coronary artery ischemia, this was
TABLE 3. Leaflet edge separation during ejectionLeaflet edge separation (mm) at % LV ejection
Before ischemia Ischemia
25% 50% 75% 100% 25% 50% 75% 100%
LADACOM 3.7 � 1.2 3.5 � 1.0 3.5 � 0.9 3.7 � 1.1 4.6 � 1.9 4.3 � 1.6 4.1 � 1.4 4.1 � 1.4CENT 4.7 � 1.9 4.6 � 1.7 4.5 � 1.6 4.7 � 1.8 4.9 � 2.1 4.7 � 1.9 4.5 � 1.9 4.5 � 1.5PCOM 6.9 � 2.5 6.7 � 2.6 6.5 � 2.6 6.8 � 3.0 7.4 � 2.9 7.0 � 2.9 6.7 � 2.9 6.9 � 2.9
dLCxACOM 3.6 � 1.1 3.5 � 1.1 3.3 � 1.0 3.4 � 1.1 4.2 � 1.6* 4.0 � 1.6 4.0 � 1.7 4.2 � 1.8CENT 4.3 � 1.9 4.3 � 1.8 4.3 � 1.8 4.1 � 1.2 4.7 � 2.0 4.6 � 1.9 5.1 � 1.7 4.9 � 1.4PCOM 6.6 � 2.8 6.5 � 2.7 6.3 � 2.8 6.2 � 2.8 7.2 � 2.9 7.2 � 2.8 7.1 � 2.8 7.0 � 2.8*
pLCxACOM 3.2 � 0.8 3.3 � 0.7 3.3 � 0.7 3.4 � 0.7 6.2 � 1.8* 5.2 � 1.4* 4.9 � 1.5* 5.7 � 2.0*CENT 4.0 � 1.9 4.3 � 1.8 4.1 � 1.9 4.3 � 1.8 6.8 � 1.8* 5.6 � 1.7* 5.5 � 1.6* 7.4 � 2.3*PCOM 6.6 � 2.7 6.4 � 3.0 6.3 � 3.0 6.4 � 3.0 8.9 � 2.7* 8.3 � 2.9* 8.2 � 3.0* 8.5 � 3.0*
LAD, LAD coronary artery occlusion; ACOM, leaflet edge marker pair near the anterior commissure; CENT, leaflet edge marker pair at valve center; PCOM,leaflet edge marker pair near the posterior commissure; dLCx, dLCx coronary artery occlusion; pLCx, pLCx coronary artery occlusion.*P � .05 versus before ischemia.
TABLE 4. Mitral annular dynamics during LAD, pLCx, and dLCx occlusionLAD dLCx pLCx
Before ischemia Ischemia Before ischemia Ischemia Before ischemia Ischemia
MAAED (cm2) 7.39 � 2.02 7.59 � 1.44 7.25 � 1.71 7.76 � 1.78* 7.11 � 1.51 8.46 � 2.01*SLED (cm) 2.64 � .32 2.77 � .20 2.61 � .24 2.79 � .25* 2.57 � .20 3.02 � .30*CCED (cm) 3.64 � .52 3.68 � .44 3.66 � .47 3.67 � .47 3.63 � .44 3.75 � .50
LAD, LAD coronary artery occlusion; dLCx, dLCx coronary artery occlusion; pLCx, pLCx coronary artery occlusion; MAAED, End-diastolic mitral annular area;SLED, end-diastolic mitral annular septal-lateral diameter; CCED, end-diastolic mitral annular commissure-commissure diameter.*P � .05 versus before ischemia.
Surgery for Acquired Cardiovascular Disease Timek et al
564 The Journal of Thoracic and Cardiovascular Surgery ● March 2003
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from
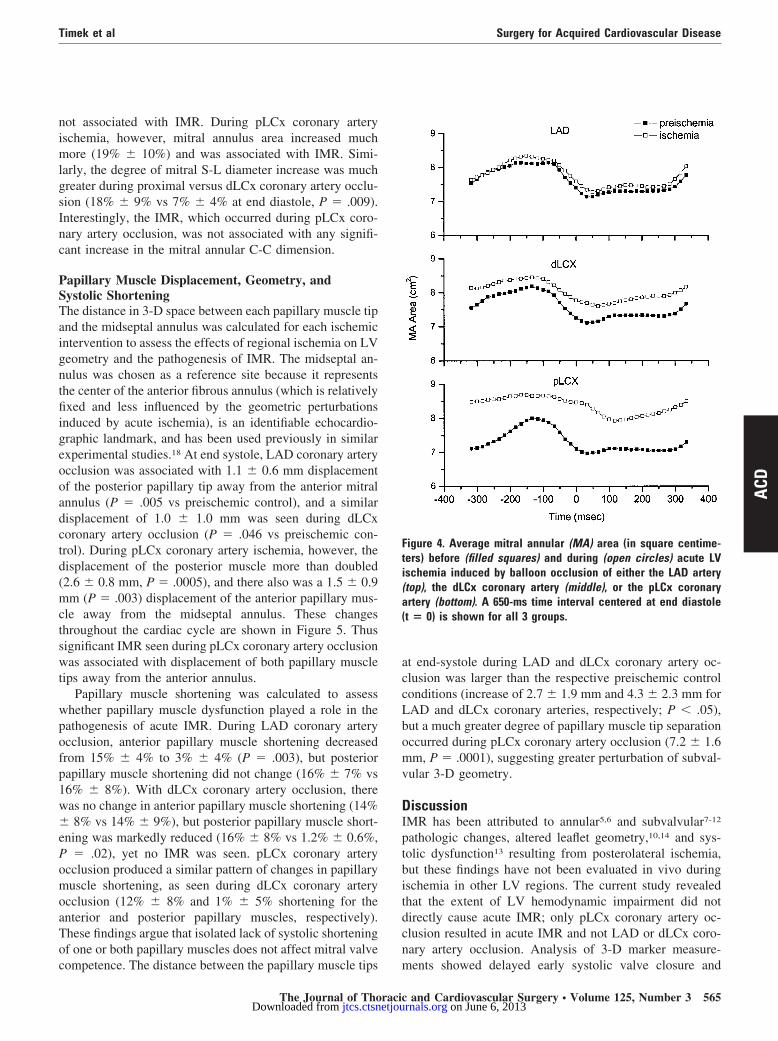
not associated with IMR. During pLCx coronary arteryischemia, however, mitral annulus area increased muchmore (19% � 10%) and was associated with IMR. Simi-larly, the degree of mitral S-L diameter increase was muchgreater during proximal versus dLCx coronary artery occlu-sion (18% � 9% vs 7% � 4% at end diastole, P � .009).Interestingly, the IMR, which occurred during pLCx coro-nary artery occlusion, was not associated with any signifi-cant increase in the mitral annular C-C dimension.
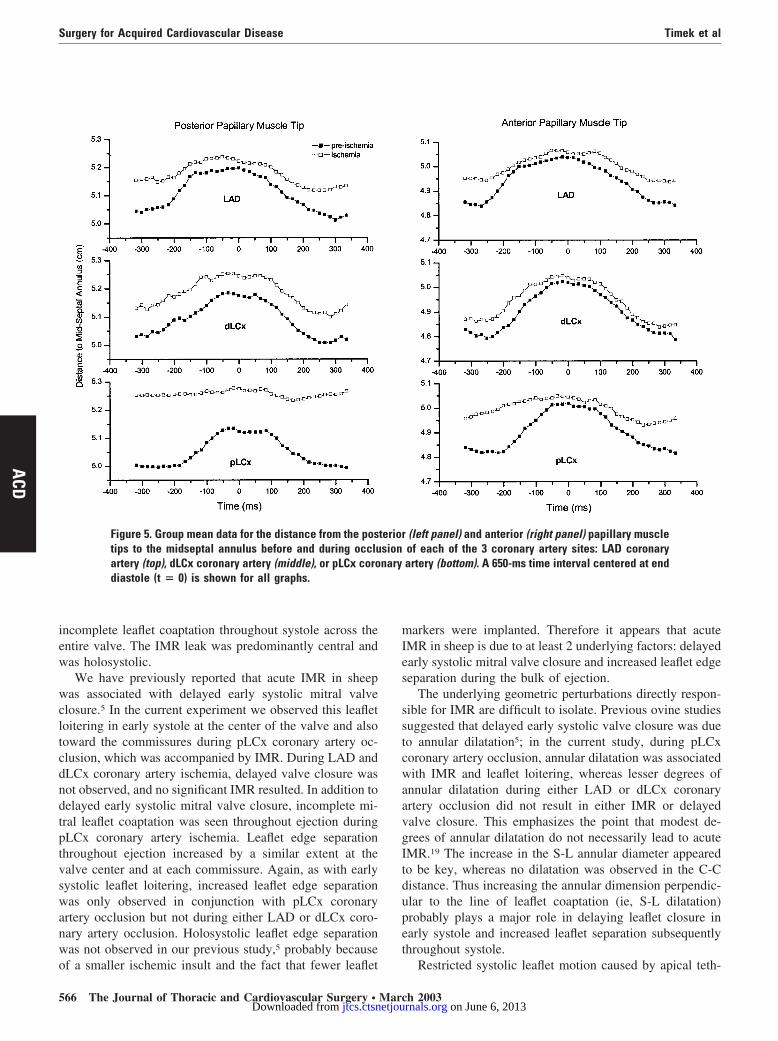
Papillary Muscle Displacement, Geometry, andSystolic ShorteningThe distance in 3-D space between each papillary muscle tipand the midseptal annulus was calculated for each ischemicintervention to assess the effects of regional ischemia on LVgeometry and the pathogenesis of IMR. The midseptal an-nulus was chosen as a reference site because it representsthe center of the anterior fibrous annulus (which is relativelyfixed and less influenced by the geometric perturbationsinduced by acute ischemia), is an identifiable echocardio-graphic landmark, and has been used previously in similarexperimental studies.18 At end systole, LAD coronary arteryocclusion was associated with 1.1 � 0.6 mm displacementof the posterior papillary tip away from the anterior mitralannulus (P � .005 vs preischemic control), and a similardisplacement of 1.0 � 1.0 mm was seen during dLCxcoronary artery occlusion (P � .046 vs preischemic con-trol). During pLCx coronary artery ischemia, however, thedisplacement of the posterior muscle more than doubled(2.6 � 0.8 mm, P � .0005), and there also was a 1.5 � 0.9mm (P � .003) displacement of the anterior papillary mus-cle away from the midseptal annulus. These changesthroughout the cardiac cycle are shown in Figure 5. Thussignificant IMR seen during pLCx coronary artery occlusionwas associated with displacement of both papillary muscletips away from the anterior annulus.
Papillary muscle shortening was calculated to assesswhether papillary muscle dysfunction played a role in thepathogenesis of acute IMR. During LAD coronary arteryocclusion, anterior papillary muscle shortening decreasedfrom 15% � 4% to 3% � 4% (P � .003), but posteriorpapillary muscle shortening did not change (16% � 7% vs16% � 8%). With dLCx coronary artery occlusion, therewas no change in anterior papillary muscle shortening (14%� 8% vs 14% � 9%), but posterior papillary muscle short-ening was markedly reduced (16% � 8% vs 1.2% � 0.6%,P � .02), yet no IMR was seen. pLCx coronary arteryocclusion produced a similar pattern of changes in papillarymuscle shortening, as seen during dLCx coronary arteryocclusion (12% � 8% and 1% � 5% shortening for theanterior and posterior papillary muscles, respectively).These findings argue that isolated lack of systolic shorteningof one or both papillary muscles does not affect mitral valvecompetence. The distance between the papillary muscle tips
at end-systole during LAD and dLCx coronary artery oc-clusion was larger than the respective preischemic controlconditions (increase of 2.7 � 1.9 mm and 4.3 � 2.3 mm forLAD and dLCx coronary arteries, respectively; P � .05),but a much greater degree of papillary muscle tip separationoccurred during pLCx coronary artery occlusion (7.2 � 1.6mm, P � .0001), suggesting greater perturbation of subval-vular 3-D geometry.
DiscussionIMR has been attributed to annular5,6 and subvalvular7-12
pathologic changes, altered leaflet geometry,10,14 and sys-tolic dysfunction13 resulting from posterolateral ischemia,but these findings have not been evaluated in vivo duringischemia in other LV regions. The current study revealedthat the extent of LV hemodynamic impairment did notdirectly cause acute IMR; only pLCx coronary artery oc-clusion resulted in acute IMR and not LAD or dLCx coro-nary artery occlusion. Analysis of 3-D marker measure-ments showed delayed early systolic valve closure and
Figure 4. Average mitral annular (MA) area (in square centime-ters) before (filled squares) and during (open circles) acute LVischemia induced by balloon occlusion of either the LAD artery(top), the dLCx coronary artery (middle), or the pLCx coronaryartery (bottom). A 650-ms time interval centered at end diastole(t � 0) is shown for all 3 groups.
Timek et al Surgery for Acquired Cardiovascular Disease
The Journal of Thoracic and Cardiovascular Surgery ● Volume 125, Number 3 565
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from
incomplete leaflet coaptation throughout systole across theentire valve. The IMR leak was predominantly central andwas holosystolic.
We have previously reported that acute IMR in sheepwas associated with delayed early systolic mitral valveclosure.5 In the current experiment we observed this leafletloitering in early systole at the center of the valve and alsotoward the commissures during pLCx coronary artery oc-clusion, which was accompanied by IMR. During LAD anddLCx coronary artery ischemia, delayed valve closure wasnot observed, and no significant IMR resulted. In addition todelayed early systolic mitral valve closure, incomplete mi-tral leaflet coaptation was seen throughout ejection duringpLCx coronary artery ischemia. Leaflet edge separationthroughout ejection increased by a similar extent at thevalve center and at each commissure. Again, as with earlysystolic leaflet loitering, increased leaflet edge separationwas only observed in conjunction with pLCx coronaryartery occlusion but not during either LAD or dLCx coro-nary artery occlusion. Holosystolic leaflet edge separationwas not observed in our previous study,5 probably becauseof a smaller ischemic insult and the fact that fewer leaflet
markers were implanted. Therefore it appears that acuteIMR in sheep is due to at least 2 underlying factors: delayedearly systolic mitral valve closure and increased leaflet edgeseparation during the bulk of ejection.
The underlying geometric perturbations directly respon-sible for IMR are difficult to isolate. Previous ovine studiessuggested that delayed early systolic valve closure was dueto annular dilatation5; in the current study, during pLCxcoronary artery occlusion, annular dilatation was associatedwith IMR and leaflet loitering, whereas lesser degrees ofannular dilatation during either LAD or dLCx coronaryartery occlusion did not result in either IMR or delayedvalve closure. This emphasizes the point that modest de-grees of annular dilatation do not necessarily lead to acuteIMR.19 The increase in the S-L annular diameter appearedto be key, whereas no dilatation was observed in the C-Cdistance. Thus increasing the annular dimension perpendic-ular to the line of leaflet coaptation (ie, S-L dilatation)probably plays a major role in delaying leaflet closure inearly systole and increased leaflet separation subsequentlythroughout systole.
Restricted systolic leaflet motion caused by apical teth-
Figure 5. Group mean data for the distance from the posterior (left panel) and anterior (right panel) papillary muscletips to the midseptal annulus before and during occlusion of each of the 3 coronary artery sites: LAD coronaryartery (top), dLCx coronary artery (middle), or pLCx coronary artery (bottom). A 650-ms time interval centered at enddiastole (t � 0) is shown for all graphs.
Surgery for Acquired Cardiovascular Disease Timek et al
566 The Journal of Thoracic and Cardiovascular Surgery ● March 2003
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from

ering or tenting, presumably from papillary muscle dis-placement, has also been observed in ovine acute IMR.14
Several investigators have postulated that perturbation ofpapillary muscle geometry prevents competent leaflet clo-sure and results in IMR.6-8 The current analysis revealedthat acute IMR requires displacement of both (but predom-inately the posterior) papillary muscle tips away from theseptal annulus throughout ejection and at end systole, as wasseen during pLCx coronary artery occlusion (Figure 5).Such papillary muscle displacement has been found in ex-perimental8 and clinical6 studies to correlate with the pres-ence of MR. In animal models of acute20 and chronic18
posterolateral ischemia, a larger distance from the papillarymuscle tips to the midseptal annulus, measured by using3-D echocardiography, was the only determinant of mitralregurgitant volume. Mitral annular dilatation was observedin both studies, being more prominent in the acute model.Indeed, during acute LCx coronary artery occlusion in dogs,displacement of the posteromedial papillary muscle tipaway from the midseptal annulus was not sufficient toproduce significant MR when the ventricle was kept small(intact pericardium and reduced LV preload), and mitralannular area remained unchanged.20 When the ventricle wasallowed to dilate (open pericardium and increased LV vol-ume) in this acute canine model, displacement of both (butparticularly the ischemic posteromedial) papillary musclestips away from the septal annulus was accompanied byapproximately 22% annular dilatation and substantial MR.A similar degree of annular dilatation with papillary muscledisplacement during IMR was observed in our experiment.Whether annular dilatation, papillary muscle displacement,or both is the mechanism primarily responsible for in-creased systolic leaflet separation cannot readily be distin-guished in this model of acute IMR.
Decreased systolic shortening of either papillary muscledid not result in MR, which corroborates the findings ofothers21 and is an additional demonstration that the oldbelief of papillary muscle dysfunction being responsible forIMR is invalid. Indeed, papillary muscle dysfunction hasactually been demonstrated to ameliorate the severity ofIMR.22 As suggested in the clinical literature,23,24 an addi-tional insult to the LV wall underlying the papillary musclesis needed before valvular incompetence occurs. This notionis supported by the increased interpapillary distance andlarger LV end-diastolic volume associated with IMR duringpLCx coronary artery occlusion but not during dLCx coro-nary artery occlusion. This implies that a mild degree of LVchamber dilatation per se does not necessarily lead to IMR,as suggested by the very small and insignificant increase inLV end-diastolic volume seen with LAD occlusion (P �.065); instead, the specific regional site and size of ischemicinsult are actually more important. On the basis of ovinecoronary artery anatomy and blood supply to the papillary
muscles,25 one would expect that both proximal and dLCxcoronary artery ischemia would result in posterior papillarymuscle dysfunction, whereas LAD occlusion would affectanterior papillary muscle shortening. This was indeed ob-served in our study, yet IMR occurred only with pLCxcoronary artery occlusion, probably because of the largearea of underlying ischemic myocardium, which is associ-ated with such an ischemic insult.25 IMR in this experimentwas not associated with reduced LV dP/dt, as previouslysuggested.13 Although a similar degree of LV systolic dys-function was induced by the 3 ischemic interventions (Table1), only pLCx coronary artery occlusion caused IMR. Oth-ers have also reported that the presence of IMR is notdependent on the degree of LV systolic dysfunction.6,8
These data further support the hypothesis that regionalalterations in valvular and subvalvular geometry play animportant role in the pathogenesis of IMR.
There is a paucity of in vivo experimental data in theliterature reporting the timing and location of IMR, buttransesophageal echocardiography clinically is accurate inlocalizing the origin of the mitral regurgitant jets,26 includ-ing those of ischemic cause.27 Reports of in vitro studies ofisolated porcine mitral valves are concordant with the echo-cardiographic and marker-derived findings reported herein.In an isolated in vitro beating heart preparation, He andcolleagues7 found that with annular dilatation and apical-posterolateral papillary muscle displacement, as can be seenin patients with IMR, MR occurred and was holosystolic,with prominent early and late systolic peaks. Using a similarexperimental preparation, Nielsen and coworkers9 observedthat displacement of both papillary muscles resulted incentral MR. Annular dilatation as a consequence of previousmyocardial infarction and LV dilatation in patients is com-monly associated with central functional MR.28 Becauseboth annular dilatation and displacement of both papillarymuscle tips were observed in this acute experiment, thefinding of holosystolic, central MR during pLCx coronaryartery occlusion is consistent with these clinical observa-tions. During pLCX coronary artery occlusion, leaflet sep-aration distance was increased throughout systole at thevalve center and also near each commissure, again demon-strating the occurrence of a broad central origin for theregurgitant jet. Not all patients with clinically significantIMR, however, have an echocardiographically demon-strated central regurgitant jet29; thus acute ovine IMR prob-ably does not completely simulate the chronic IMR condi-tion observed in human subjects.
The IMR during pLCx coronary artery occlusion in thisexperiment was accompanied by delayed early systolicvalve closure and increased leaflet edge separation through-out ejection symmetrically around the valve center. AcuteLV ischemic insults in other regions (ie, during LAD anddLCx coronary artery occlusion) did not lead to IMR, de-
Timek et al Surgery for Acquired Cardiovascular Disease
The Journal of Thoracic and Cardiovascular Surgery ● Volume 125, Number 3 567
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from

layed leaflet closure, or increased leaflet edge separation.We conjecture that annular dilatation was the key factorleading to delayed leaflet closure, whereas annular dilata-tion plus papillary muscle displacement during ejectioncaused increased leaflet edge separation. The individualcontributions of these multiple mechanisms to the patho-genesis of IMR are difficult to isolate, but it is clear that thecombination of valvular and ventricular geometric changesleads to central, holosystolic acute IMR in sheep.
Although this study overcomes some limitations of pre-vious experiments, one must be circumspect in interpretingthe results. These findings pertain only to the context ofacute LV ischemia in the otherwise normal sheep hearts andshould not be extrapolated to chronic human IMR, whereLV dilatation, subvalvular geometric perturbations inducedby previous infarction and ischemia, and LV remodelingmost likely play a bigger role. This type of experimentneeds to be conducted in chronic animal preparations aftermyocardial infarction with resultant LV remodeling andchronic LV volume overload to simulate more accuratelythe clinical problem. The present experiment, however,offers a unique opportunity to study the effects of annularand subvalvular geometric changes during 3 different re-gional LV ischemic insults in the same hearts, which cannotbe done in a chronic model. Although the degree of systolicdysfunction induced by each ischemic intervention wassimilar, LV dP/dt (an isovolumic index) during pLCx cor-onary artery ischemia might have been artificially highbecause this was the only group with significant mitralinsufficiency. Although this raises the possibility that themagnitude of the acute ischemic injury was greater duringpLCx coronary artery occlusion, other indices of LV func-tion decreased to a similar extent, suggesting equivalenthemodynamic insults.
The timing of IMR could be determined reliably in only4 animals, and not all 6 animals had a central regurgitant jet;perhaps with more animals greater heterogeneity of regur-gitant jets would have been observed. The differences incoronary anatomy between sheep and human subjects mustalso be considered because sheep left ventricles are moredependent on their dominant LCx coronary artery thanhuman ventricles, in which right coronary artery dominanceis most common. Several reliable models of human cardiacdisease, however, have been established in ovine mod-els.25,30 The radiopaque marker method provides reproduc-ible determination of 3-D marker position with submillime-ter spatial resolution every 16.7 ms but requires suturingsmall metal markers to the intracardiac structures. It isunlikely that the markers interfere with mitral leaflet motionbecause they are very small (aggregate mass, 20 � 6 mg);even when we grossly overloaded the anterior leaflet with alarger number of excessively heavy markers (total mass,184 mg) in other animals, the peak anterior leaflet opening
velocity by means of epicardial pulsed wave Doppler echo-cardiography was unchanged (0.47 � 0.05 m/s comparedwith 0.45 � 0.06 m/s for leaflets without any markersimplanted), as was the peak E-wave velocity (0.55 to 0.60m/s, unpublished data).
We acknowledge the superb technical assistance provided byCarol W. Mead, BA, and Maggie Brophy, RVT.
References
1. Czer LSC, Gray RI, DeRobertis MA, Bateman TM, Stewart ME,Chaux A, et al. Mitral valve replacement: impact of coronary arterydisease and determinants of prognosis after revascularization. Circu-lation. 1984;70(suppl I):I198-207.
2. Connolly MW, Gelbfish JS, Jacobowitz IJ, Rose DM, Mendelsohn A,Cappabianca PM, et al. Surgical results for mitral regurgitation fromcoronary artery disease. J Thorac Cardiovasc Surg. 1986;91:379-88.
3. Replogle RL, Campbell CD. Surgery for mitral regurgitation associ-ated with ischemic heart disease. Circulation. 1989;79(suppl I):I122-5.
4. Dion R. Ischemic mitral regurgitation: when and how should it becorrected? J Heart Dis. 1993;2:536-43.
5. Glasson JR, Komeda M, Daughters GT, Bolger AF, Karlsson MO,Foppiano LE, et al. Early systolic mitral leaflet “loitering” duringacute ischemic mitral regurgitation. J Thorac Cardiovasc Surg. 1998;116:193-205.
6. Yiu SF, Enriquez-Sarano M, Tribouilloy C, Seward JB, Tajik AJ.Determinants of the degree of functional mitral regurgitation in pa-tients with systolic left ventricular dysfunction. Circulation. 2000;102:1400-6.
7. He S, Fontaine AA, Schwammenthal E, Yoganathan AP, Levine RA.Integrated mechanism for functional mitral regurgitation. Circulation.1997;96:1826-34.
8. Otsuji Y, Handschumacher MD, Schwammenthal E, Jiang L, Song JK,Guerrero JL, et al. Insights from three-dimensional echocardiographyinto the mechanism of functional mitral regurgitation. Circulation.1997;96:1999-2008.
9. Nielsen SL, Nygaard H, Fontaine AA, Hasenkam JH, He S, Yoga-nathan AP. Papillary muscle misalignment causes multiple mitralregurgitant jets: an ambiguous mechanism for functional mitral regur-gitation. J Heart Valve Dis. 1999;8:551-64.
10. Gorman JH, Jackson BM, Gorman RC, Kelley ST, Gikakis N, Ed-monds LH Jr. Papillary muscle discoordination rather than increasedannular area facilitates mitral regurgitation after acute posterior myo-cardial infarction. Circulation. 1997;96(suppl II):II124-7.
11. Kono T, Sabbah HN, Rosman H, Alam M, Jafari S, Goldstein S. Leftventricular shape is the primary determinant of functional mitralregurgitation in heart failure. J Am Coll Cardiol. 1992;7:1594-8.
12. Sabbah HN, Kono T, Stein PD, Mancini GBJ, Goldstein S. Leftventricular shape changes during the course of evolving heart failure.Am J Physiol. 1992;263:H266-70.
13. Kaul S, Spotnitz WD, Glasheen PW, Touchstone DA. Mechanism ofischemic mitral regurgitation. Circulation. 1991;84:2167-80.
14. Lai DTM, Timek TA, Dagum P, Green GR, Glasson JR, DaughtersGT, et al. The effect of ring annuloplasty on mitral leaflet geometryduring acute left ventricular ischemia. J Thorac Cardiovasc Surg.2000;120:966-75.
15. Glasson JR, Komeda M, Daughters GT, Foppiano LE, Bolger AF, TyeTL, et al. Most ovine mitral annular three-dimensional size reductionoccurs before ventricular systole and is abolished with ventricularpacing. Circulation. 1997;96(suppl II):II115-23.
16. Daughters GT, Sanders WJ, Miller DC, Schwarzkopf A, Mead CW,and Ingels NB. A comparison of two analytical systems for 3-Dreconstruction from biplane videoradiograms. Comput Cardiol. 1988;15:79-82.
17. Moon MR, DeAnda A, Daughters GT, Ingels NB, Miller DC. Exper-imental evaluation of different chordal preservation methods duringmitral valve replacement. Ann Thorac Surg. 1994;58:931-44.
Surgery for Acquired Cardiovascular Disease Timek et al
568 The Journal of Thoracic and Cardiovascular Surgery ● March 2003
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from

18. Liel-Cohen N, Guerrero JL, Otsuji Y, Handschumacher MD, RudskiLG, Hunziker PR, et al. Design of a new surgical approach forventricular remodeling to relieve ischemic mitral regurgitation: insightfrom 3-dimensional echocardiography. Circulation. 2000;101:2756-63.
19. Green GR, Dagum P, Glasson JR, Daughters GT, Bolger AF, Foppi-ano LE, et al. Mitral annular dilatation and papillary muscle disloca-tion without mitral regurgitation in sheep. Circulation. 1999;100(Suppl II):II95-102.
20. Otsuji Y, Handschumacher MD, Liel-Cohn N, Tanabe H, Jiang L,Schwammenthal E, et al. Mechanism of ischemic mitral regurgitationwith segmental left ventricular dysfunction: Three dimensional echo-cardiographic studies in models of acute and chronic progressiveregurgitation. J Am Coll Cardiol. 2001;37:641-8.
21. Tsakiris AG, Rastelli GC, Amorim D, Titus JL, Wood EH. Effect ofexperimental papillary muscle damage on mitral valve closure inintact anesthetized dogs. Mayo Clin Proc. 1970;42:132-9.
22. Messas E, Guerrero JL, Handschumacher MD, Chow CM, Sullivan S,Schwammenthal E, et al. Paradoxic decrease in ischemic mitral re-gurgitation with papillary muscle dysfunction: insights form three-dimensional and contrast echocardiography with strain rate measure-ment. Circulation. 2001;104:844-50.
23. Godley RW, Wann LS, Rogers EW, Feigenbaum H, Weyman AE.Incomplete leaflet closure in patients with papillary muscle dysfunc-tion. Circulation. 1982;61:565-71.
24. Van Dantzig J, Delemarre BJ, Koster RW, Bot H, Visser CA. Patho-genesis of mitral regurgitation in acute myocardial infarction: impor-tance of changes in left ventricular shape and regional function. AmHeart J. 1996;131:865-71.
25. Llaneras MR, Nance ML, Streicher JT, Lima JA, Savino JS, BogenDK, et al. Large animal model of ischemic mitral regurgitation. AnnThorac Surg. 1994;57:432-9.
26. Foster GP, Isselbacher EM, Rose GA, Torchiana DF, Akins CW,Picard MH. Accurate localization of mitral regurgitation defects usingmultiplane transesophageal echocardiography. Ann Thorac Surg.1998;65:1025-31.
27. Enriquez-Sarano M, Freeman WK, Tribouilloy CM, Orszulak TA,Khandheria BK, Seward JB, et al. Functional anatomy of mitralregurgitation: accuracy and outcome implications of transesophagealechocardiography. J Am Coll Cardiol. 1999;34:1129-36.
28. Izumi S, Miyatake K, Beppu S, Park YD, Nagata S, Kinoshita N, et al.Mechanism of mitral regurgitation in patients with myocardial infarc-tion: a study using real-time two-dimensional Doppler flow imagingand echocardiography. Circulation. 1987;76:777-85.
29. Gillinov AM, Wierup PN, Blackstone EH, Bishay ES, Cosgrove DM,White J, et al. Is repair preferable to replacement for ischemic mitralregurgitation? J Thorac Cardiovasc Surg. 2001;122:1125-41.
30. Markovitz SE, Ratcliffe MB, Bavaria JE, Kreiner G, Iozzo RV,Hargrove WC, et al. Large animal model of left ventricular aneurysm.Ann Thorac Surg. 1989;48:838-45.
DiscussionDr Henry M. Spotnitz (New York, NY). This is a very nice articleand a very good use of the marker technique that was pioneered atStanford. I would like to ask you a methodologic question. It is abit unusual not to randomize a sequence of interventions. How didyou arrive at that particular sequence of interventions, why didn’tyou randomize the order in which you did the various occlusions,and how do you know that your observations are not a function ofthe sequence in which you did this, especially because the appear-ance of many of the control tracings change over time and thecontrols clearly are not identical, particularly in the leaflet sepa-ration tracing that you showed?
Dr Timek. That is an excellent question. Our initial sequenceof doing the occlusions really came from previous experiments.What we have noticed is that in sheep that undergo a pLCx
coronary artery occlusion there is a very high frequency of ven-tricular fibrillation, and in a closed-chest preparation, once theseanimals go into ventricular fibrillation, the experiment is basicallyover. Therefore the way we proceeded was to induce the ischemicevent, which is less likely to produce ventricular fibrillation first,that being LAD ischemia, dLCx, and then, at the end, pLCx.
Between each of these interventions, the animals were allowedto come to baseline as far as hemodynamics were concerned;however, you are correct, we cannot fully exclude that the se-quence of the experiments somehow did not contribute to this. Weare considering repeating this in an open-chest model in whichventricular fibrillation, when it does occur, can be treated muchmore easily.
Dr David H. Adams (New York, NY). I really enjoyed yourtalk. In the clinical setting ischemia in any circulatory territory canresult in the phenomena of IMR, presumably on the basis ofassociated ventricular dilatation and papillary muscle displace-ment. Would you please comment on the mechanism of IMR in thesetting of LAD occlusion or posterior descending artery occlusion,as opposed to pLCx occlusion?
Dr Timek. I think that one of the major limitations of thismodel is that this is acute IMR. We believe that some new datafrom our laboratory with chronic IMR, which has just been com-pleted by my colleague, Dr Tibayan, shows that these changes inthe chronic model are actually pretty similar to what we see in theacute model as far as pLCx coronary artery occlusion is concerned.We did not do any LAD ischemia in the chronic model, and thatwill be forthcoming.
As far as translating this into the clinical arena, the feeling is thatclinical IMR is related to LCx ischemia and papillary muscle dis-placement. From our chronic and acute models, we believe that youreally need both annular changes and you also need displacement ofpapillary muscles, and this really gets into how one should addressIMR clinically. Is a ring sufficient, addressing basically the annularproblem, or should there be some subvalvular interventions also? Wehave been working on some experimental surgical techniques toaddress these problems; however, this is still in its infancy.
Dr Adams. Just to follow up, I have one quick question aboutthe research you just mentioned. Are you and Dr Miller’s labora-tory able to give us at least some insight into your comment? Whatgeometric parameter might suggest that reduction annuloplasty isgoing to work, and would not further displacement or measure-ment of the papillary muscles suggest that we need to think aboutsome papillary remodeling as well?
Dr Timek. If I may be allowed to give a prelude to mycolleague’s research, it is annular dilatation, at least in our models,which is really the key, particularly septal lateral dilatation. Wepresented an article last year just with isolated septal lateral re-duction by a single suture that an acute model of IMR in sheep willabolish IMR. As far as the papillary muscle displacement isconcerned, what we have found, surprisingly, is that there isdisplacement of the posterior papillary muscle, which is lateral andposterior but not apical. The muscle is not actually apically dis-placed, it is posterior and lateral, and in fact, it seems to movecloser to the annular plane. There have been some suggestions ofperhaps pulling the muscle up closer to the annulus. Whether thatwill work is difficult to say.
Timek et al Surgery for Acquired Cardiovascular Disease
The Journal of Thoracic and Cardiovascular Surgery ● Volume 125, Number 3 569
ACD
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from

2003;125:559-569 J Thorac Cardiovasc Surgand D. Craig Miller
Daughters, Paul Dagum, Mary K. Zasio, Sidney Lo, Trevor Hastie, Neil B. Ingels, Jr Tomasz A. Timek, David T. Lai, Frederick Tibayan, David Liang, George T.
ischemic mitral regurgitationIschemia in three left ventricular regions: Insights into the pathogenesis of acute
Continuing Medical Education Activities
http://cme.ctsnetjournals.org/cgi/hierarchy/ctsnetcme_node;JTCSSubscribers to the Journal can earn continuing medical education credits via the Web at
Subscription Information
http://jtcs.ctsnetjournals.org/cgi/content/full/125/3/559#BIBLThis article cites 25 articles, 15 of which you can access for free at:
Citations
http://jtcs.ctsnetjournals.org/cgi/content/full/125/3/559#otherarticlesThis article has been cited by 8 HighWire-hosted articles:
Subspecialty Collections
http://jtcs.ctsnetjournals.org/cgi/collection/extracorporeal_circulation Extracorporeal circulation http://jtcs.ctsnetjournals.org/cgi/collection/coronary_disease
Coronary disease http://jtcs.ctsnetjournals.org/cgi/collection/cardiac_physiology Cardiac - physiology
This article, along with others on similar topics, appears in the following collection(s):
Permissions and Licensing
http://www.elsevier.com/wps/find/obtainpermissionform.cws_home/obtainpermissionformreceipt, is available at: An on-line permission request form, which should be fulfilled within 10 working days of
. http://www.elsevier.com/wps/find/supportfaq.cws_home/permissionusematerialcan be found online at: General information about reproducing this article in parts (figures, tables) or in its entirety
on June 6, 2013 jtcs.ctsnetjournals.orgDownloaded from




















