
study of mitral annular calcification in chronic kidney disease
Upload
independentCategory
view
2download
0
THE EFFECT OF PURE MITRAL REGURGITATION ON MITRALANNULAR GEOMETRY AND 3-D SADDLE-SHAPE
Tom C. Nguyen, MDa, Akinobu Itoh, MDa, Carl J. Carlhäll, MD, PhDa,b, Wolfgang Bothe,MDa, Tomasz A. Timek, MDa, Daniel B. Ennis, PhDa, Robert A. Oakes, MDa, David Liang, MD,PhDc, George T. Daughters, MSa,d, Neil B. Ingels Jr., PhDa,d, and D. Craig Miller, MDa
aDepartment of Cardiothoracic Surgery, Stanford University School of Medicine, Stanford, California
bDepartment of Clinical Physiology, University Hospital, Linköping, Sweden
cDivision of Cardiovascular Medicine, Stanford, California
dResearch Institute, Palo Alto Medical Foundation, Palo Alto, California
AbstractObjectives—Chronic ischemic mitral regurgitation (IMR) is associated with mitral annulardilatation in the septal-lateral dimension and flattening of the annular 3-D saddle-shape. To examinewhether these perturbations are due to the ischemic insult, mitral regurgitation (MR), or both, weinvestigated the effects of pure MR (low pressure volume overload) on annular geometry and shape.
Methods—Eight radiopaque markers were sutured evenly around the mitral annulus in sheeprandomized to control (CTRL, n=8) or experimental (HOLE, n=12) groups. In HOLE, a 3.5mm to4.8mm hole was punched in the posterior leaflet to generate pure MR. 4-D marker coordinates wereobtained radiographically 1 and 12 weeks postoperatively. Mitral annular area (MAA), annularseptal-lateral (SL) and commissure-commissure (CC) dimensions, and annular height werecalculated every 16.7ms.
Results—MR grade was 0.4±0.4 in CTRL and 3.0±0.8 in HOLE (p<0.001) at 12 weeks. End-diastolic LV volume index was greater in HOLE at both 1 and 12 weeks; end-systolic volume indexwas larger in HOLE at 12 weeks. MAA increased in HOLE predominantly in the CC dimension,with no difference in annular height between HOLE vs. CTRL at 1 or 12 weeks, respectively.
Conclusions—In contrast to annular SL dilatation and flattening of annular saddle-shape observedwith chronic IMR, pure MR was associated with CC dimension annular dilatation and no change inannular shape. Thus, infarction is a more important determinant of SL dilatation and annular shapethan is MR, which reinforces the need for disease-specific designs of annuloplasty rings.
ULTRAMINI- ABSTRACT—In a chronic pure mitral regurgitation (MR) ovine model, weexamined changes in mitral annular dimensions and shape over 12 weeks to understand thecontribution of MR to annular remodeling independent of the effects of myocardial infarction. PureMR resulted in commissure-commissure annular dilatation and no change in annular saddle-shape.
Address for Correspondence: D. Craig Miller, M.D., Department of Cardiothoracic Surgery, Falk Cardiovascular Research Center,Stanford University School of Medicine, Stanford, California 94305-5247, 01.650.725.3826 FAX 01.650.725.3846, E-mail:[email protected] at the 87th Annual Meeting of the American Association for Thoracic Surgery Washington, DC, May 2007Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customerswe are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resultingproof before it is published in its final citable form. Please note that during the production process errors may be discovered which couldaffect the content, and all legal disclaimers that apply to the journal pertain.
NIH Public AccessAuthor ManuscriptJ Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
Published in final edited form as:J Thorac Cardiovasc Surg. 2008 September ; 136(3): 557–565. doi:10.1016/j.jtcvs.2007.12.087.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

INTRODUCTIONChronic ischemic mitral regurgitation (IMR) is a common sequela of ischemic heart disease,with a prevalence estimated at 1.6 million to 2.8 million patients in the United States [1]. Theclinical consequence of severe, uncorrected mitral regurgitation (MR) is excess morbidity andmortality [2]. In recent years, much has been learned about the pathophysiology of chronicIMR. We now know that chronic IMR results in mitral annular dilatation, predominantly inthe septal-lateral (SL) dimension [3], and alterations in annular 3-D saddle-shape [4,5] in sheepand man, which has guided the evolution of annuloplasty rings and novel medical devices.Whether these perturbations are catalyzed by the ischemic insult to the left ventricle (LV), thevolume overload from MR, or both, is unknown. In an effort to dissect the role of low pressurevolume overload on mitral annular geometry, dynamics, and shape, we developed a chronicovine model of pure MR and tested the hypotheses that pure MR symmetrically increases mitralannular area and flattens annular 3-D saddle-shape.
METHODSAll animals received humane care in compliance with guidelines sets forth by the NationalInstitutes of Health (US Department of Health and Human Services NIH Publ. 85-23, Revised1985). This study was approved by the Stanford Medical Center Laboratory Research AnimalReview Committee and conducted according to Stanford University policy.
Surgical PreparationSheep were premedicated with ketamine (25mg/kg, i.m.) and randomized to either control(CTRL, n=8) or experimental (HOLE, n=12) groups. Anesthesia was induced with sodiumthiopental (6.8mg/kg, i.v.) and maintained with inhalational isoflurane (1–2.5%). Epicardialechocardiography was used to qualitatively grade (0–4) mitral regurgitation (MR) at baselineon the basis of color Doppler regurgitant jet extent and width [6,7]. Through a left thoracotomy,twelve tantalum myocardial markers were inserted in the left ventricular (LV) subepicardiumand septum along four equally spaced longitudinal meridians, with one marker at the LV apex.After establishment of cardiopulmonary bypass (CPB), eight tantalum markers were suturedevenly around the circumference of the mitral annulus via an atriotomy, one near eachcommissure (#1, #5) and three along the septal (#2, #3, and #4) and lateral (#6, #7, and #8)annular perimeter (Figure 1a). In HOLE, a 3.5mm to 4.8mm hole was created in the middlescallop of the posterior mitral leaflet (PML) using an aortic hole puncher to generate MR(Figure 1b and Figure 1c). The atriotomy was closed, the heart de-aired, the cross-clampremoved, and the heart defibrillated (mean CPB time 65±5 min; mean aortic cross-clamp time30±4 min). An implantable micromanometer pressure transducer (PA4.5-X6; KonigsbergInstrument, Inc., Pasadena, Ca, USA) was placed in the LV chamber through the apex andexteriorized through the skin between the scapulae. The chest was closed and the animalrecovered.
Study GroupFifty-eight sheep were initially randomized to either control (CTRL, n=25) or experimental(HOLE, n=33) groups. Intraoperatively, 9 sheep had natural moderate-severe MR and wereexcluded. We were unable to wean 4 sheep off cardiopulmonary bypass, and 1 sheep expiredfrom technical/accidental complications. A total of 9 perioperative complications occurred(stroke [n=3] and pulmonary edema [n=6]). Four animals were excluded due to insufficientMR despite creating a hole in the PML (a smaller 2.8mm hole was used in three of the fouranimals). Three animals expired from unknown causes (necropsy results were unrevealing).Eight sheep were excluded due to either missing or poorly placed markers, leaving a remainingtotal of twenty animals (CTRL, n=8; HOLE, n=12) for analysis.
Nguyen et al. Page 2
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Experimental ProtocolAfter an acclimatization period of 7±1 days, animals were taken to the cardiac catheterizationlaboratory, sedated with ketamine, intubated, mechanically ventilated, and maintained withinhalational isoflurane. A micromanometer catheter (Millar Instruments, Inc., Houston, TX,USA) was introduced through a sheath in the left carotid artery and advanced to the aortic archfor aortic pressure measurement. Transthoracic echocardiography (TTE) and simultaneousbiplane videofluoroscopic marker data and hemodynamic data were acquired. MR was thengraded by a blinded expert echocardiographer (D.L.) on the basis of color Doppler regurgitantjet extent and width [6]. The animal was then stabilized and recovered. All animals werefollowed for clinical signs of heart failure (tachypnea, lethargy, and anorexia). TTE wasperformed by our blinded echocardiographer weekly to grade MR and to detect LV dilatation.After 12±1 weeks, the animals returned to the cardiac catheterization laboratory for recordingof hemodynamic, TTE, and marker data.
Data Acquisition and AnalysisImages were acquired with animals in the right lateral position with a biplane videofluoroscopysystem (Philips Medical Systems, North America Company, Pleasanton, Ca, USA). Data fromthe two radiographic views were digitized and merged to yield 3-D coordinates for each markerevery 16.7 ms using custom software [8]. The accuracy of 3-D reconstructions from biplanevideograms of length measurements, expressed as mean percentage error of a known marker-to-marker 3-D length has been shown to be 0.2% with a reproducibility of 1% [9]. Aorticpressure, LV pressure, and electrocardiogram voltage signals were digitized and recordedsimultaneously during marker data acquisition.
Three consecutive steady-state beats in sinus rhythm were selected for analysis from eachstudy. For each cardiac cycle, end-diastole (ED) was defined as the maximal second derivativeof LV pressure, corresponding to the upstroke of LV pressure. End-systole (ES) was definedas the videofluoroscopic frame before the time of peak negative LV rate of pressure decrease(−dP/dtmax). Instantaneous LV volume was calculated from LV markers by multiple tetrahedraconstructed from the marker coordinates and corrected for LV convexity [10]. Althoughmyocardial volume is included in the calculation of LV volume, relative changes in LVchamber size are accurately measured.
Mitral Annular GeometryMitral annular area (MAA) in 3-D space was calculated for each frame throughout the cardiaccycle as the sum of the areas of eight triangles formed by consecutive adjacent marker pairson the annulus and the annular centroid defined by markers #1 to #8 (Figure 1b). The septal-lateral (SL) diameter of the annulus was calculated as the distance in 3-D space between thetwo markers placed in the middle of the septal and lateral mitral annulus, respectively (#3 and#7, Figure 1b). The commissure-commissure (CC) diameter was calculated as the distance inthree-dimensional space between the two annular commissural markers (#1 and #5, Figure 1b).Mitral annular height was calculated as the orthogonal distance from the saddlehorn marker(#3, Figure 1b) to the least-squares mitral annular plane defined without considering thesaddlehorn marker.
Statistical AnalysisData are reported as mean ±1 SD unless otherwise specified. Hemodynamic and marker-derived data from consecutive steady-state beats from each heart were time aligned at eitherED or ES. Marker data were calculated over 20 frames before and after either ED or ES, thusallowing evaluation over a time period of 700 ms. Data were compared using two-way repeated
Nguyen et al. Page 3
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

measure ANOVA with the Bonferroni post-hoc test for multiple comparisons. (Sigmastat 3.5,Systat Software, Inc). P≤0.04 was considered statistically significant.
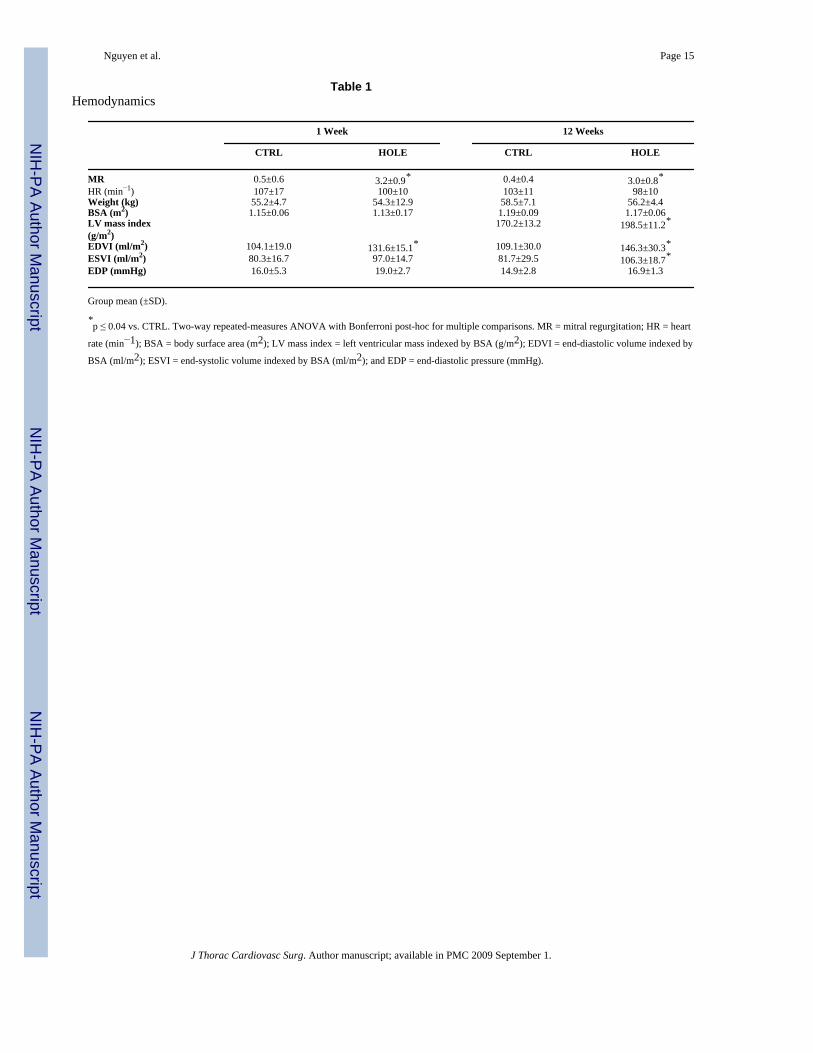
RESULTSHemodynamic data for CTRL and HOLE are shown in Table 1. There was no difference inHR, weight, and BSA between CTRL and HOLE at 1 and 12 weeks. MR was significantlygreater in HOLE versus CTRL at 1 and 12 weeks (1week: 3.2±0.9 vs. 0.5±0.6; 12 weeks: 3.0±0.8 vs. 0.4±0.4, all p < 0.001), Table 1. At 12 weeks, LV mass index, however, was greaterin HOLE than CTRL (198.5±11.2 g/m2 vs. 170.2±13.2 g/m2, p = 0.002). LV end-diastolicindex (EDVI) was larger in HOLE versus CTRL at both 1 and 12 weeks (1week: 131.6±15.1vs. 104.1±19.0, p=0.04, 2df, F=2.4; 12 weeks: 146.3±30.3 vs. 109.1±30.0, p=0.01, 2df, F=5.3),while ESVI was larger in HOLE vs. CTRL only at 12 weeks (106.3±18.7 vs. 81.7±29.5, p=0.03,2df, F=4.9). Figure 2 shows changes in MR grade between CTRL and HOLE throughout thestudy time course.
Figure 3 summarizes mitral annular dynamics time-aligned at ED while Table 2 shows annulargeometry at ED and ES at 12 weeks. There was a significant increase in MAA, CC, and SLdimensions at 12 weeks in HOLE versus CTRL, with a predominant increase in CC relativeto SL dimension.
In order to assess changes in mitral annular 3-D shape, we calculated annular height throughoutthe cardiac cycle with data time aligned at ES (Figure 4). At both 1 and 12 weeks, there wasno difference in annular height between CTRL and HOLE. To obtain a more complete pictureof 3-D geometry of the entire annulus, the displacement of each annular marker from the least-squares annular plane was calculated at ED and ES (Figure 5). There was no difference inmarker displacement from the least-square annular plane between CTRL and HOLE at ED orES.
DISCUSSIONIn order to understand the contribution of chronic pure MR to mitral annular remodelingwithout the confounding effects of LV ischemia or infarction, we developed a chronic ovinemodel of pure low pressure LV volume overload MR and examined the effects of pure MR onmitral annular geometry and dynamics. In this chronic ovine study, pure MR resulted in mitralannular dilatation predominately in the CC dimension and no change in mitral annular 3-Dshape.
Chronic Ovine Model of Mitral RegurgitationMR imposes a pure low-pressure volume overload on the LV, whereas excess volume is ejectedinto the low-impedance left atrium during systole with either normal or subnormal LV systolicpressure [11]. Increased end-diastolic stress causes replication of sarcomeres in series andcompensatory eccentric LV hypertrophy [12]. Although MR is a common phenomenon, mostprior studies of LV volume overload have utilized high-pressure experimental models whereagainst a competent mitral valve excess LV volume is ejected into the high pressure aorticsystem [13–19]. Other experimental models relied on division of chordae tendineae [20,21],which can result in deterioration of global LV systolic function [22,23]. Our chronic closed-chest ovine model of “low-pressure” volume overload does not appear to directly affect LVsystolic function. By placing a pre-defined hole in the PML (Figure 1c and Figure 2), we wereable to reproducibly create low-pressure volume overload.
Nguyen et al. Page 4
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Annular Geometry and DynamicsChronic ovine IMR remodels the mitral annulus by increasing mitral annular areapredominantly in the SL dimension [3,24]. Due to the inherent dual nature of the insult,however, it is unclear whether these changes occur from LV infarction, volume overload fromMR, or both. In this study, chronic pure MR without infarction increased mitral annular areaprimarily in the mitral CC dimension (Figure 3). These findings suggest that infarction maybe a more important determinant of increased SL annular dilatation than is LV volumeoverload, which has spawned a new generation of disease-specific “IMR/FMR” annuloplastyrings (Edwards GeoForm and IMR ETlogix rings, St. Jude Medical RSR ring).
It is widely held that MR begets MR in a self-perpetuating cycle [1], although this suppositionhas not been directly tested experimentally. Myocardial infarction distorts the LV, resulting inpapillary muscle displacement, impaired leaflet coaptation, and MR [1]. LV dilatation leadsto annular enlargement, thereby exacerbating valvular incompetence in a vicious cycle. It isinteresting to note that in this study, however, MR did not beget MR. Specifically, despite anobserved increase in mitral annular area and ventricular dilatation, there were minimal changesin MR grade throughout the study (Figures 2, Table 1). Several possible explanations exist forthis observation: (1) The time course of the study may not have been sufficient to increasemitral annular area to a large enough degree where the annular dilatation would enhance theprogression of MR; (2) The amount of MR vis-à-vis regurgitant fraction and the effectiveregurgitant orifice area were not quantitatively measured; and (3) TTE in sheep is inherentlydifficult and the image quality may not be sufficient to discern subtle differences in MR grade.Despite these limitations, we believe it is important to qualify the concept “MR begets MR”,as this situation may not necessarily hold true in the setting of pure low-pressure MR.
In this study, mitral annular area increased predominantly in the CC direction. It is thought,however, that perturbations in the mitral SL direction are more important for leaflet coaptationcompared to CC dilatation [25,26]. Annular dilatation alone may not be sufficient to supportthe “MR begets MR” supposition; understanding the regional dimensions of annular changeis equally, if not more, important. Since SL dilation is known to predominate with chronicIMR, perhaps a more accurate description might be “chronic IMR begets more MR,” althoughfurther studies are required to substantiate this possibility conclusively.
Annular 3-D Saddle-ShapeThe saddle-shape nonplanarity of the mitral annulus has been extensively described by three-dimensional echocardiography, 4-D marker videofluoroscopy, and sonomicrometry arraylocalization [27–30]. Using finite element analysis, it is believed that 3-D annular saddle-shapemay be important for maintaining leaflet curvature which pari passu minimize leaflet closingstress [30]. Annular 3-D saddle-shape, however, is not present in IMR, suggesting globalflattening of the mitral annulus and, thus, a theoretical increase in leaflet stresses at end-systole[4,24,31,32]. It has been difficult to ascertain, however, whether the culprit of annularremodeling is the LV ischemic insult, the MR, or both. To isolate these variables, mitral annularheight and the displacement of each annular marker from the mitral plane was measured in thischronic ovine model of pure MR without the confounding ischemia. There was no differencein mitral annular height throughout the cardiac cycle (Figure 4) between CTRL and HOLE at12 weeks. To obtain a more complete picture of 3-D annular geometry, the displacement ofeach annular marker from the mitral annular plane was calculated at ED and ES (Figure 5).There was no difference in marker displacement from the least-square annular plane betweenCTRL and HOLE at ED or ES. Furthermore, annular height to commissure-width ratio(AHCW) has been proposed as a normalized surrogate for annular 3-D shape, and indeed thisvariable appears to be conserved across species [4,30]. Although end-systolic AHCW wassmaller in HOLE versus CTRL at both 1 and 12 weeks, this difference was not significant
Nguyen et al. Page 5
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
(1week: 10.3±3.2 vs. 12.1±2.4; 12weeks: 10.6±3.6 vs. 13.0±4.2, respectively, both N.S.).These data, therefore, suggests that, in contrast to IMR, the 3-D saddle-shape of the mitralannulus does not flatten with pure MR. This implies that LV infarction plays the dominant rolein annular flattening seen with chronic IMR. In both clinical and experimental studies, IMR isassociated with a decrease in annular height [4,31,32], whereas in this ovine study pure MRdid not decrease annular height. It is known that the post-infarction remodeling associated withIMR results in lateral displacement of the posterior papillary muscle and LV wall [3,33].Against a relatively fixed aortic annulus, lateral displacement of the ventricle could potentially“drag” the mitral annulus in the lateral direction thereby flattening the mitral annulus (Figure6), which might also explain why with IMR, mitral annular SL dilation predominates, whilewith pure MR dilation in the SL direction does not. Lastly, because pure MR did not alter the3-D saddle-shape of the mitral annulus, theoretically, pure MR may have less of an effect onleaflet closing stress than does LV infarction, although this was not directly tested in thisexperiment.
Left Ventricular RemodelingIn this ovine experiment, there was only a minimal increase in LV EDV despite 3+ MR in theHOLE group. Mitral regurgitation is a chronic and insidious process that often takes yearsbefore substantial LV dilatation occurs; the relatively short duration of our study (12 weeks)probably accounts for the minimal increase in LVEDV. Second, we support the suppositionfirst introduced by Gorman and colleagues that infarction alone may play a more dominantrole in LV remodeling than MR [34–36]. In previous IMR experiments by our and other groups,ventricular volume increased following the insult by 30–40% by 8 weeks. It was unclear fromthese previous studies, however, whether this was due to the infarct, MR, or both. In this currentstudy, we isolated the role of MR alone (without infarction). We conclude that MR causes LVdilatation, but at a slow and gradual rate, while infarction is more likely the major driving forceresponsible for adverse LV remodeling.
LIMITATIONSConsiderable caution should be exercised when extrapolating results from this animal study tothe clinical scenario of long-standing IMR or structural MR in human patients. The sequela ofMR in patients is a chronic and insidious phenomenon that can be tolerated clinically for monthsto years. The 12 week follow-up in this study may be insufficient to capture the truepathophysiology of chronic MR. Although it is known that the amount of MR is heavilyinfluenced by ventricular loading conditions, this variable was not directly controlled in thisstudy. In future studies, however, we do plan to interrogate how alterations in loadingconditions affect annular geometry, dynamics, and annular 3-D shape. Lastly, although wereport that chronic pure MR did not alter mitral annular 3-D saddle-shape, it is possible thatthe study was not sufficiently powered to establish a statistical difference and that a Type 2(beta) error was made by incorrectly accepting the null hypothesis.
ACKNOWLEDGMENTSThis work was supported by Grants HL-29589 and HL-67025 from the National Heart, Lung and Blood Institute.Doctors Nguyen was a Leah McConnell Cardiovascular Surgical Research Fellow and recipient of the Thoracic SocietyFoundation Research Fellowship Award. Dr. Itoh received funding from the Uehara Memorial Foundation, and Dr.Carlhäll received funding from the Swedish Heart and Lung Foundation and the County Council of Östergötland,Sweden. Dr. Bothe received stipend support from the Deutsche Herzstiftung. We deeply appreciate the technicalexpertise provided by Lars Wigstrom, PhD, Frederick Tibayan, MD, Maggie Brophy, A.S., Mary K. Zasio, B.A., andKatha Gazda, B.A. Lastly, we would like to thank Simon Kimm, MD for the wonderful illustrations.
Nguyen et al. Page 6
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

REFERENCES1. Borger MA, et al. Chronic ischemic mitral regurgitation: repair, replace or rethink? Ann Thorac Surg
2006;81(3):1153–1161. [PubMed: 16488757]2. Hickey MS, et al. Current prognosis of ischemic mitral regurgitation. Implications for future
management. Circulation 1988;78(3 Pt 2):I51–I59. [PubMed: 2970346]3. Tibayan FA, et al. Geometric distortions of the mitral valvular-ventricular complex in chronic ischemic
mitral regurgitation. Circulation 2003;108:II116–II121. [PubMed: 12970219]4. Gorman JH 3rd, et al. The effect of regional ischemia on mitral valve annular saddle shape. Ann Thorac
Surg 2004;77(2):544–548. [PubMed: 14759435]5. Kaji S, et al. Annular geometry in patients with chronic ischemic mitral regurgitation: three-
dimensional magnetic resonance imaging study. Circulation 2005;112(9 Suppl):I409–I414. [PubMed:16159855]
6. Helmcke F, et al. Color Doppler assessment of mitral regurgitation with orthogonal planes. Circulation1987;75(1):175–183. [PubMed: 3791603]
7. Mele D, et al. Proximal jet size by Doppler color flow mapping predicts severity of mitral regurgitationClinical studies. Circulation 1995;91(3):746–754. [PubMed: 7828303]
8. Niczyporuk MA, Miller DC. Automatic tracking and digitization of multiple radiopaque myocardialmarkers. Comput Biomed Res 1991;24(2):129–142. [PubMed: 2036779]
9. Daughters, GT., et al. A comparison of two analytical systems for three-dimensional reconstructionfrom biplane videoradiograms; Proc Comp Cardiol (IEEE); 1988. p. 79-82.
10. DeAnda A Jr, et al. A method to assess endocardial regional longitudinal curvature of the left ventricle.Am J Physiol 1995;268(6 Pt 2):H2553–H2560. [PubMed: 7611505]
11. Wisenbaugh T, Spann JF, Carabello BA. Differences in myocardial performance and load betweenpatients with similar amounts of chronic aortic versus chronic mitral regurgitation. J Am Coll Cardiol1984;3(4):916–923. [PubMed: 6707357]
12. Ross J Jr, et al. Diastolic geometry and sarcomere lengths in the chronically dilated canine leftventricle. Circ Res 1971;28(1):49–61. [PubMed: 5539440]
13. Badke FR, Covell JW. Early changes in left ventricular regional dimensions and function duringchronic volume overloading in the conscious dog. Circ Res 1979;45(3):420–428. [PubMed: 455609]
14. Belenkie I, Baumber JS, Rademaker A. Changes in left ventricular dimensions and performanceresulting from acute and chronic volume overload in the conscious dog. Can J Physiol Pharmacol1983;61(11):1274–1280. [PubMed: 6661683]
15. LeWinter MM, Engler RL, Karliner JS. Enhanced left ventricular shortening during chronic volumeoverload in conscious dogs. Am J Physiol 1980;238(2):H126–H133. [PubMed: 7361905]
16. Newman WH. Contractile state of hypertrophied left ventricle in long-standing volume overload. AmJ Physiol 1978;234(1):H88–H93. [PubMed: 146436]
17. Ross J Jr, McCullagh WH. Nature of enhanced performance of the dilated left ventricle in the dogduring chronic volume overloading. Circ Res 1972;30(5):549–556. [PubMed: 5026757]
18. Taylor RR, Covell JW, Ross J Jr. Left ventricular function in experimental aorto-caval fistula withcirculatory congestion and fluid retention. J Clin Invest 1968;47(6):1333–1342. [PubMed: 5653213]
19. Turina M, Bussmann WD, Krayenbuhl HP. Contractility of the hypertrophied canine heart in chronicvolume overload. Cardiovasc Res 1969;3(4):486–495. [PubMed: 4243335]
20. Kleaveland JP, et al. Volume overload hypertrophy in a closed-chest model of mitral regurgitation.Am J Physiol 1988;254(6 Pt 2):H1034–H1041. [PubMed: 3381891]
21. Carabello BA, et al. Left ventricular function in experimental volume overload hypertrophy. Am JPhysiol 1989;256(4 Pt 2):H974–H981. [PubMed: 2523200]
22. Sarris GE, et al. Global and regional left ventricular systolic performance in the in situ ejecting canineheart. Importance of the mitral apparatus. Circulation 1989;80(3 Pt 1):I24–I42. [PubMed: 2766532]
23. Rodriguez F, et al. Importance of mitral valve second-order chordae for left ventricular geometry,wall thickening mechanics, and global systolic function. Circulation 2004;110:II115–II122.[PubMed: 15364849]
Nguyen et al. Page 7
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

24. Tibayan FA, et al. Annular remodeling in chronic ischemic mitral regurgitation: ring selectionimplications. Ann Thorac Surg 2003;76(5):1549–1554. [PubMed: 14602284]discussion 1554–5
25. Timek T, et al. Ring annuloplasty prevents delayed leaflet coaptation and mitral regurgitation duringacute left ventricular ischemia. J Thorac Cardiovasc Surg 2000;119(4 Pt 1):774–783. [PubMed:10733769]
26. Glasson JR, et al. Early systolic mitral leaflet "loitering" during acute ischemic mitral regurgitation.J Thorac Cardiovasc Surg 1998;116(2):193–205. [PubMed: 9699570]
27. Gorman JH 3rd, et al. Dynamic three-dimensional imaging of the mitral valve and left ventricle byrapid sonomicrometry array localization. J Thorac Cardiovasc Surg 1996;112(3):712–726. [PubMed:8800160]
28. Levine RA, et al. Three-dimensional echocardiographic reconstruction of the mitral valve, withimplications for the diagnosis of mitral valve prolapse. Circulation 1989;80(3):589–598. [PubMed:2766511]
29. Glasson JR, et al. Most ovine mitral annular three-dimensional size reduction occurs before ventricularsystole and is abolished with ventricular pacing. Circulation 1997;96(9 Suppl):II-115–II-122.discussion II-123
30. Salgo IS, et al. Effect of annular shape on leaflet curvature in reducing mitral leaflet stress. Circulation2002;106(6):711–717. [PubMed: 12163432]
31. Watanabe N, et al. Mitral annulus flattens in ischemic mitral regurgitation: geometric differencesbetween inferior and anterior myocardial infarction: a real-time 3-dimensional echocardiographicstudy. Circulation 2005;112(9 Suppl):I458–I462. [PubMed: 16159863]
32. Kaplan SR, et al. Three-dimensional echocardiographic assessment of annular shape changes in thenormal and regurgitant mitral valve. Am Heart J 2000;139(3):378–387. [PubMed: 10689248]
33. Messas E, et al. Paradoxic decrease in ischemic mitral regurgitation with papillary muscledysfunction: insights from three-dimensional and contrast echocardiography with strain ratemeasurement. Circulation 2001;104(16):1952–1957. [PubMed: 11602500]
34. Guy, TSt, et al. Prevention of ischemic mitral regurgitation does not influence the outcome ofremodeling after posterolateral myocardial infarction. J Am Coll Cardiol 2004;43(3):377–383.[PubMed: 15013117]
35. Enomoto Y, et al. Surgical treatment of ischemic mitral regurgitation might not influence ventricularremodeling. J Thorac Cardiovasc Surg 2005;129(3):504–511. [PubMed: 15746731]
36. Enomoto Y, et al. Early ventricular restraint after myocardial infarction: extent of the wrap determinesthe outcome of remodeling. Ann Thorac Surg 2005;79(3):881–887. [PubMed: 15734399]discussion881–7
Nguyen et al. Page 8
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.a: Locations of LV epicardial markers (shaded circles) surgically implanted to silhouette theLV chamber along four equally spaced longitudinal meridians.b: Schematic representation of the eight marker array on the mitral annulus, as viewed fromthe left atrium. Marker numbers (1–8) are shown. The location of the hole in the middle scallopof the posterior mitral leaflet is shown as a shaded circle.c: Intra-operative photograph as viewed from the left atrium of mitral annular markers with a4.8mm hole in the middle scallop of the posterior mitral leaflet.
Nguyen et al. Page 9
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
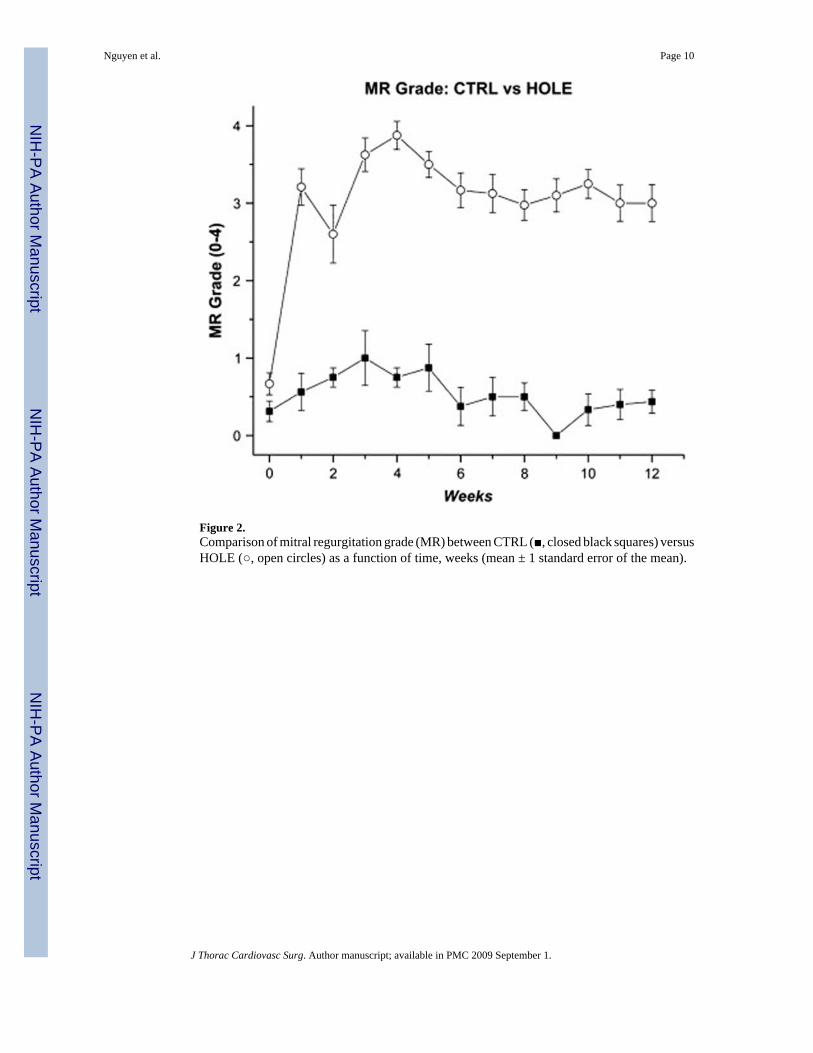
Figure 2.Comparison of mitral regurgitation grade (MR) between CTRL (■, closed black squares) versusHOLE (○, open circles) as a function of time, weeks (mean ± 1 standard error of the mean).
Nguyen et al. Page 10
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
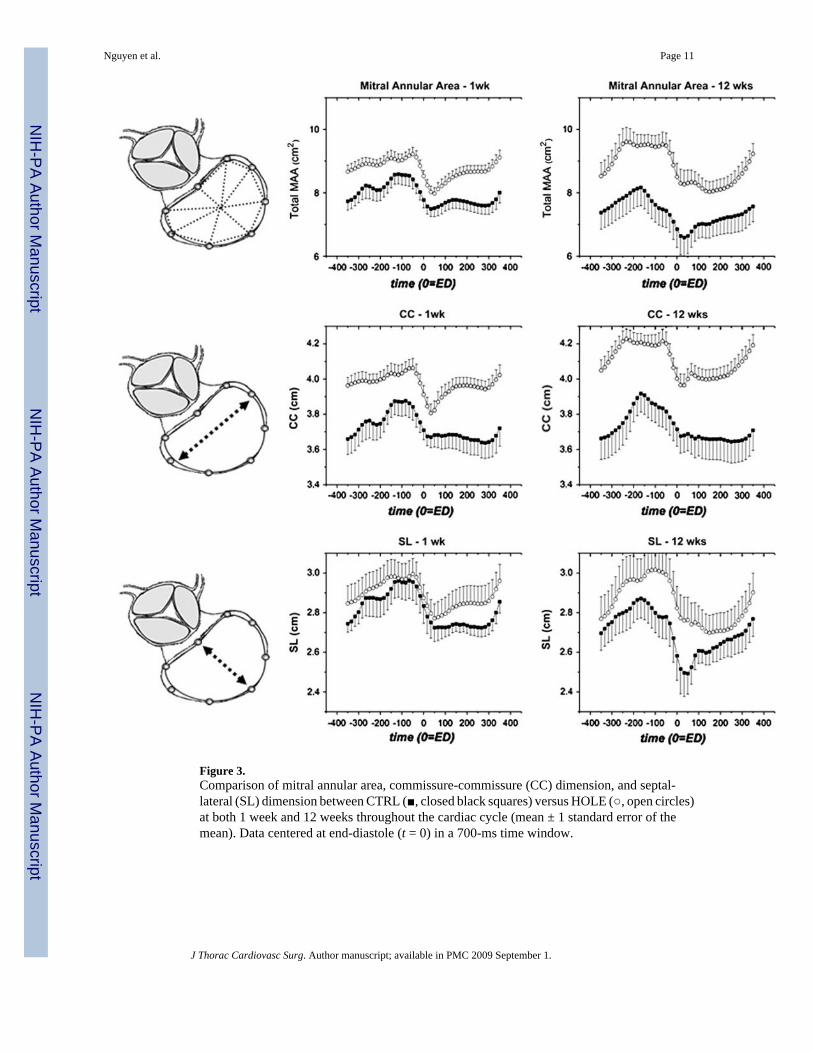
Figure 3.Comparison of mitral annular area, commissure-commissure (CC) dimension, and septal-lateral (SL) dimension between CTRL (■, closed black squares) versus HOLE (○, open circles)at both 1 week and 12 weeks throughout the cardiac cycle (mean ± 1 standard error of themean). Data centered at end-diastole (t = 0) in a 700-ms time window.
Nguyen et al. Page 11
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 4.Mitral annular height (AH) between CTRL (■, closed black squares) versus HOLE (○, opencircles) at both 1 week and 12 weeks throughout the cardiac cycle (mean ± 1 standard error ofthe mean). Data centered at end-systole (t = 0) in a 700-ms time window.
Nguyen et al. Page 12
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
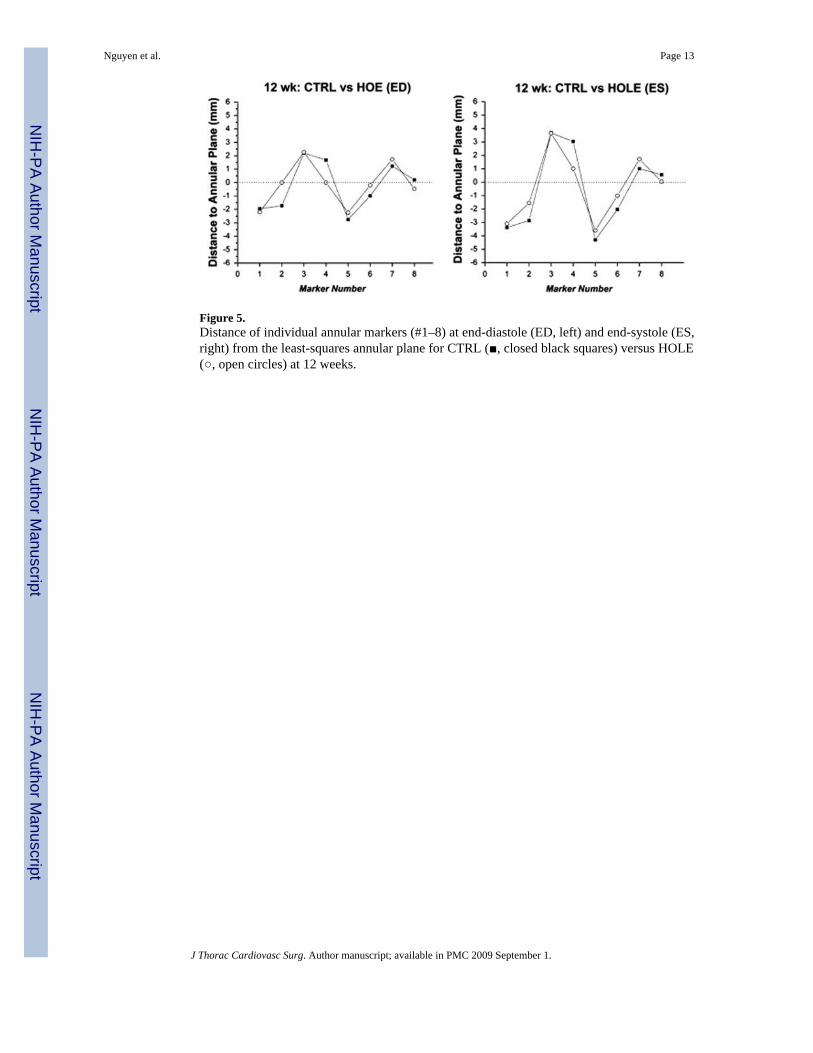
Figure 5.Distance of individual annular markers (#1–8) at end-diastole (ED, left) and end-systole (ES,right) from the least-squares annular plane for CTRL (■, closed black squares) versus HOLE(○, open circles) at 12 weeks.
Nguyen et al. Page 13
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 6.Cross section of a normal (Figure 6a) and chronic ischemic mitral regurgitation (IMR) heart(Figure 6b) with schematic of the mitral annulus magnified on the right. Note that the mitralannulus (red dotted line) in the normal heart resembles the shape of saddle (Figure 6a).Following a posterior infarction, remodeling results in lateral displacement of the papillarymuscle and ventricular wall (dotted blue line). Against a relatively fixed aortic annulus, thismay “drag” the mitral annulus in the lateral direction thereby flattening the mitral annulus(solid blue line). This is also consistent with the predominant septal-lateral dilation seen withchronic IMR.
Nguyen et al. Page 14
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Nguyen et al. Page 15
Table 1Hemodynamics
1 Week 12 Weeks
CTRL HOLE CTRL HOLE
MR 0.5±0.6 3.2±0.9* 0.4±0.4 3.0±0.8*HR (min−1) 107±17 100±10 103±11 98±10Weight (kg) 55.2±4.7 54.3±12.9 58.5±7.1 56.2±4.4BSA (m2) 1.15±0.06 1.13±0.17 1.19±0.09 1.17±0.06LV mass index 170.2±13.2 198.5±11.2*(g/m2)EDVI (ml/m2) 104.1±19.0 131.6±15.1* 109.1±30.0 146.3±30.3*ESVI (ml/m2) 80.3±16.7 97.0±14.7 81.7±29.5 106.3±18.7*EDP (mmHg) 16.0±5.3 19.0±2.7 14.9±2.8 16.9±1.3
Group mean (±SD).
*p ≤ 0.04 vs. CTRL. Two-way repeated-measures ANOVA with Bonferroni post-hoc for multiple comparisons. MR = mitral regurgitation; HR = heart
rate (min−1); BSA = body surface area (m2); LV mass index = left ventricular mass indexed by BSA (g/m2); EDVI = end-diastolic volume indexed by
BSA (ml/m2); ESVI = end-systolic volume indexed by BSA (ml/m2); and EDP = end-diastolic pressure (mmHg).
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Nguyen et al. Page 16
Table 2Annular Geometry and Shape
1 Week
End-Diastole End-Systole
CTRL HOLE CTRL HOLE
MAA(i), cm2/m2 7.1±0.8 8.1±0.7* 5.8±1.0 6.6±0.9CC(i), cm/m2 3.2±0.3 3.5±0.4 2.9±0.3 3.2±0.4SL(i), cm/m2 2.4±0.4 2.7±0.3 2.3±0.3 2.4±0.3
12 Weeks
End-Diastole End-Systole
CTRL HOLE CTRL HOLE
MAA(i), cm2/m2 6.8±2.1 8.8±1.3* 4.9±1.8† 6.4±1.1*CC(i), cm/m2 3.1±0.5 3.8±0.3† * 2.8±0.5 3.4±0.3*SL(i), cm/m2 2.2±0.5 2.5±0.4* 1.8±0.4 2.1±0.3*
Group mean (±SD).
*p ≤ 0.01 vs. CTRL.
†p ≤ 0.04 vs. 1 Week; Two-way repeated-measures ANOVA with Bonferroni post-hoc for multiple comparisons. MAA(i) = mitral annular area indexed
by BSA (cm2/m2); CC(i) = commissure-commissure dimension indexed by BSA (cm/m2); and SL(i) = septal-lateral dimension indexed by BSA (cm/
m2).
J Thorac Cardiovasc Surg. Author manuscript; available in PMC 2009 September 1.
Copyright © 2022 FDOKUMEN



















