
Intrarenal vascular alterations in hemodialysis patientsA semiquantitative light microscopic study
9
INTRARENAL VASCULAR ALTERATIONS IN HEMODIALYSIS PATIENTS A Semiquantitative Light Microscopic Study A. Olusegun Fayemi, M.Sc, M.D ., * and Majid Ali, M.D., F.R.G.S. t Abstract The intrar enal arteri al and arteriolar changes in the kidneys of 80 pa- tient s with chronic renal insufficiency maintained on hemodialysis were stud- ied serniquantitati vel y by light microscopy and histochemistry. Intimal prolif- eration was common and accounted for thick ening of vessel walls and luminal narrowing. Fibrocollagenous and fibroelastotic intimal changes were located predominantl y in the interlobul ar and arcuate art eries, whereas the fibrornucin- ous intimal lesion was found mainly in the interlobar arteries. Thickening of the media was encountered in 25 per cent, and adventitial fibrosis in 20 per cent of the kidneys. Necrotizing arterial or arteriolar lesions were not seen. The significance of these alterations as a possible cause of renal ischemia and their role in the perpetuation of hypertension ar e discussed. The pathologic alterati ons occurring in terminal chronic ren al disease, the 50 - called end stage kidne y disease, have been the subject of numerous investigations. I, 2 Most of these studies have been directed toward the ide nt ification of the causative primary renal di seases and their pathoge- netic mechan isms.s-:' Studies concerning the intrarenal vascular changes in chronic renal disea ses hav e dealt mainly with be- nign and malignan t hype rten sion .s" the morphology of ren al vascu lar changes has also been stud ied, albeit less inten- sively, in scleroderma, hemolytic-ure mic syndrome, and toxemia of pregnancy.8, 10-14 Th e intrarenal vascular changes in kidneys of hemolydialysis patients have received only passing attention in previ- ou s investigations. Heptinstalf described considera ble intimal changes in arteries of all calibers - from segmental to inter- lobular . Such intimal changes were cellu- lar, cellular with a mucinous background, or fibrous. It was suggested that these ch anges might be rel ated to "disuse en- darteritis." Kincaid-Smith" described *Assistan t Clinical Professor of Pathology, Mount Sinai School of Medicine of the City Univer- sity of Ne w York , New York, New York. tAssistant Prof essor of Pathology (Adj.), Colu mbia Uni versity College of Physicians an d Sur- geons, New York, New York. 685
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Intrarenal vascular alterations in hemodialysis patientsA semiquantitative light microscopic study
INTRARENAL VASCULARALTERATIONS INHEMODIALYSIS PATIENTS
A Semiquantitative Light Microscopic Study
A. Olusegun Fayemi, M.Sc, M.D .,*and Majid Ali, M.D., F.R.G.S. t
Abstract
The intrarenal arterial and ar teriolar changes in the kidneys of 80 patients with chronic renal insufficiency maintain ed on hemodialysis were studied serniquantitati vely by light microscopy and histochemistry. Intimal proliferation was common and accounted for thickening of vessel walls and luminalnarrowing. Fibrocollagenous and fibroelastotic intimal changes were locatedpredominantly in the interlobular and arcuate arteries, whereas the fibrornucinous intimal lesion was found mainly in the interlobar arteries. Thickening ofthe media was encountered in 25 pe r cent, and adventitial fibrosis in 20 percent of the kidneys. Necrotizing arterial or arteriolar lesions were not seen.The significance of these alterations as a possible cause of renal ischemia andtheir role in the perpetuation of hypertension are discussed.
The pathologic alterations occurringin terminal chronic renal disease, the 50
called end stage kidney disease, have beenth e subject of numerous investigations. I, 2
Most of these studies have been directedtoward the identification of the causativeprimary renal diseases and their pathogenetic mechanisms.s-:' Studies concerningthe intrarenal vascular ch an ges in chronicrenal disea ses have dealt mainly with ben ign and malignant hypertension .s" themorphology of renal vascu lar changeshas also been studied , albeit less inten-
sively, in scleroderma, hemolytic-ure micsyndrome, and toxemia of pregnancy.8, 10-14
The intrarenal vascular changes inkidneys of hemolydialysis patients havereceived only passing attention in previou s investigations. Heptinstalf describedconsiderable intimal changes in arteriesof all calibers - from segmental to interlobular . Such intimal changes were cellular, cellular with a mucinous background,or fibrous. It was suggested that thesechanges might be related to "disuse endarteritis." Kincaid-Smith" described
*Assistan t Clinica l Professor of Pathology, Mount Sina i School of Medicine of the City University of Ne w York, New York, New York.
tAssistant Professor of Pa thology (Adj .), Colu mbia Uni versity College of Physicians an d Sur-geons, New York, New York. 685
HUMAN PATHOLOGY-VOLUME 10, NUMBER 6 November 1979
686
marked vascular lesions in patients whohad been on hemodialysis for some timeor who had functioning transplants. Thelesions consisted of prominent reduplication of fibrous and elastic layers of arteries. This lesion was supposed to represent "disuse" atrophy and was judged tobe similar to that encountered in atrophicpyelonephritic scars. More recentlyMcManus et al." described cellular nodules in the intrarenal arteries and arterioles in 12 of 40 kidneys from hemodialysis patients. The lesions weretraceable to necrotic arteries and arterioles and were thought to representsmooth muscle proliferation.
This presentation concerns the renalvascular alterations in 80 autopsy cases inpatients who had been maintained onlong term intermittent hemodialysis. Thestudy provides a semiquantitative evaluation and discusses the significance of intimal proliferative, medial, and adventitial changes in arteries and arterioles.
MATERIALS AND METHODS
The autopsy files of Holy NameHospital for the years January 1969through December 1977 were examinedto identify patients with chronic renalfailure treated with or without hemodialysis. Ninety-six such cases were identified. Five cases were excluded because ofinsufficient clinical information or inadequate pathologic material for evaluation.The histologic slides and autopsy reportsof the remaining 91 cases were reviewed.Of these, 80 patients were maintained onhemodialysis for periods ranging fromthree weeks to seven years.
Paraffin sections of the kidneys werecut at 3 to 5 microns and stained with hematoxylin and eosin, elastica-van Gieson,trichrome, and, when indicated, alcianblue and periodic acid-Schiff stains.Three to six sections were available forstudy in all cases.
The severity of intimal alterationswas graded on a semiquantitative scaleemploying a modification of the methodof Pitcock et al." (Table 1). Similar semiquantitative grades were used for evaluating arteriolar changes except that the
TABLE 1. SEMIQUANTITATIVE GRADING OF
ARTERIOLAR THICKENING AND INTIMAL
PROLIFERATION IN INTRARENAL ARTERIES
o No significant lesions+ Small bur definite patchy intimal or
arteriolar thickening++ Intimal or arteriolar thickening exceeding
two to three times the luminal diameter++ Intimal or arteriolar thickening
approximately equal to or greaterthan the diameter of the lumen of thevessel
thickness of the entire wall of the arteriole was substituted for intimal thickness. Medial and adventitial alterationswere not quantitated.
Three main patterns of intimal proliferation were defined: fibrocollagenous,fibromucinous, and fibroelastotic. In fibrocollagenous intimal proliferation thelesion was composed predominantly offibroblasts and collagen fibrils. This waseasily demonstrable by the trichromestain and was sometimes associated withmild reduplication of the internal elasticlamina (Fig. 1). In the fibroelastotic pattern the duplication of the elastic laminawas prominent and constituted the mostconspicuous change of the intima. Thislesion usually had a minor fibrous cornponent (Fig. 2). The third type of intimalalteration, the fibromucinous type, wascharacterized by a faintly bluish hue onhematoxylin and eosin sections andsparse cellularity; the predominant cellwas stellate shaped with a few fibroblasts(Fig. 3). The lesion stained diffusely withalcian blue. The significance of the difference in the distribution of the types ofintimal proliferation in the arteries ofdifferent sizes was determined by chisquare (X2
) analysis. Additionally, the relationship of the arterial and arteriolarlesions to the duration of dialysis, thepresence and severity of hypertension,and the primary renal diseases was studied.
Other parameters that were studiedincluded the primary renal disease, thedata for which were derived from boththe gross and the microscopic features ineach case. The criteria employed for differentiating the various forms of chronicrenal disease were those described by

INTRARENAL VASCULAR ALTERATIONS-FAYEMI, ALI
Figure 1. Arcuate artery showing librocollagenous intimal thickening. There IS reduplication of theelastic lamina. (Elastica-van Gieson stain. X IDO.)
Figure 2. Fibroelastotic intimal thickening in an arcuate artery. Note luminal narrowing. (Elastica-vanGieson stain. x 100.)
687

HUM.-\:\ PATHOLOGY-VOLUME I D, ~UMBER fi Not.ember 1979
Figure 3. Longitudinal section of an arcuate artery showing fibrornucinous intimal thickening. Note theabsence of significant elastotic change. (Elastica-van Gieson stain. X 100.)
Heptinstall.v> Special attention was paidto calcification of the various histologiccomponents of the kidneys. The hospitalrecords and clinical summaries that forman integral part of the autopsy protocolprovided information regarding the agesof the patients and the duration of hemodialysis before death.
OBSERVATIONS
Age and Sex Distribution
The ages of the 80 patients in thisstudy ranged from 15 to 84 years with an
average of 55.8 years. There were 43men and 37 women. Fifteen patientswere 40 years old or younger (Fig. 4).
Etiology of Chronic Renal Failure
The underlying renal diseases inthese patients were as follows: chronicpyelonephritis (20), chronic glomerulonephritis (I3), arterio- and arteriolonephrosclerosis (14), diabetic nephropathy (I3), polycystic kidney disease (10),end stage renal disease of indeterminable etiology (4), chronic interstitialnephritis (3), focal sclerosis (1), amyloidosis (1), and medullary cystic disease (1).
20.------ - - ----------,
Figure 4. Age and sex distribution ofSO patients. Most patients were 50 years orolder.
MolesFema les
o 10-19 20-29 30-39 40-49 50-59 60-69 70·79 80-89AGE
fflI-z 15wi=Cf.~ 100:WCD~ 5::lZ
688
INTRARENAL VASCULAR ALTERATIONS-FAYEMI, ALl
NUMBER OF CASESo 10 15 20 25 30 35 40
FIBROUS
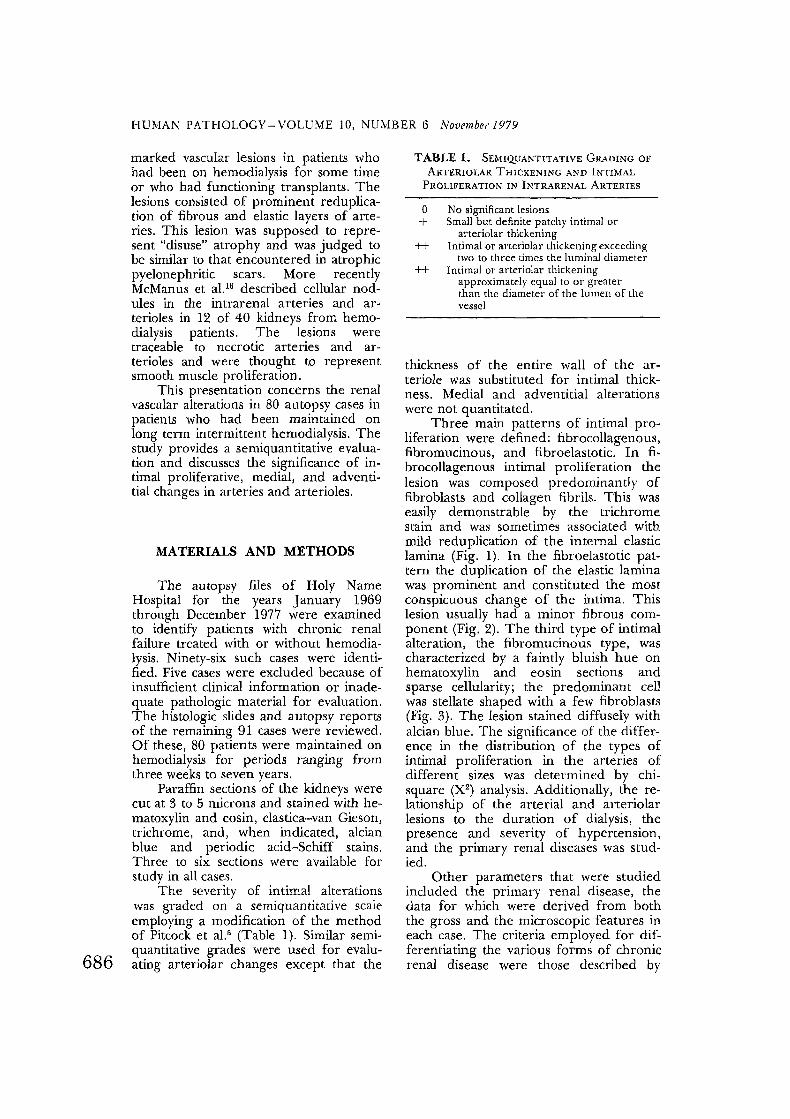
Figure 5. Pattern of intimal thickeningin intrarenal arteries of hemodialysis patients.The lesions in the interlobular and arcuate FIBROarteries are generally similar but differ sig- ELASTOTICnificantly from those in interlobar arteries(p < 0.0001).
FIBROMUCINOUS
LOBAR ( INTERLOBAR )
INTIMAL CHANGES. The pattern,frequency, and severity of intimal proliferation in the intrarenal arteries are detailed in Figures 5 and 6. Although thevarious types of lesions do not differ significantly in their incidence in the arcuateand interlobular arteries, a significant difference exists when these two types ofvessels are compared individually or incombination with the larger interlobar arteries (p< 0.0001). The predominant lesion of the interlobar arteries is fibromucinous; fibrous andfibroelastotic intimalchanges occur more frequently in theother arteries. Similarly, statistical analysis of the data shows that a predictioncould be made regarding the location ofeach type of lesion. For example, whenthe lesion is fibrous, it is more likely to befound in an arcuate or interlobular thanin a lobar artery. ~ similar conclusioncan be drawn for fibroelastotic and theopposite conclusion for fibromucinous intimal changes. The intimal changes boreno relationship to the duration of dialysistreatment, the underlying renal disease,or the hypertensive status of the patients.
MEDIAL AND ADVENTITIAL CHANGES.
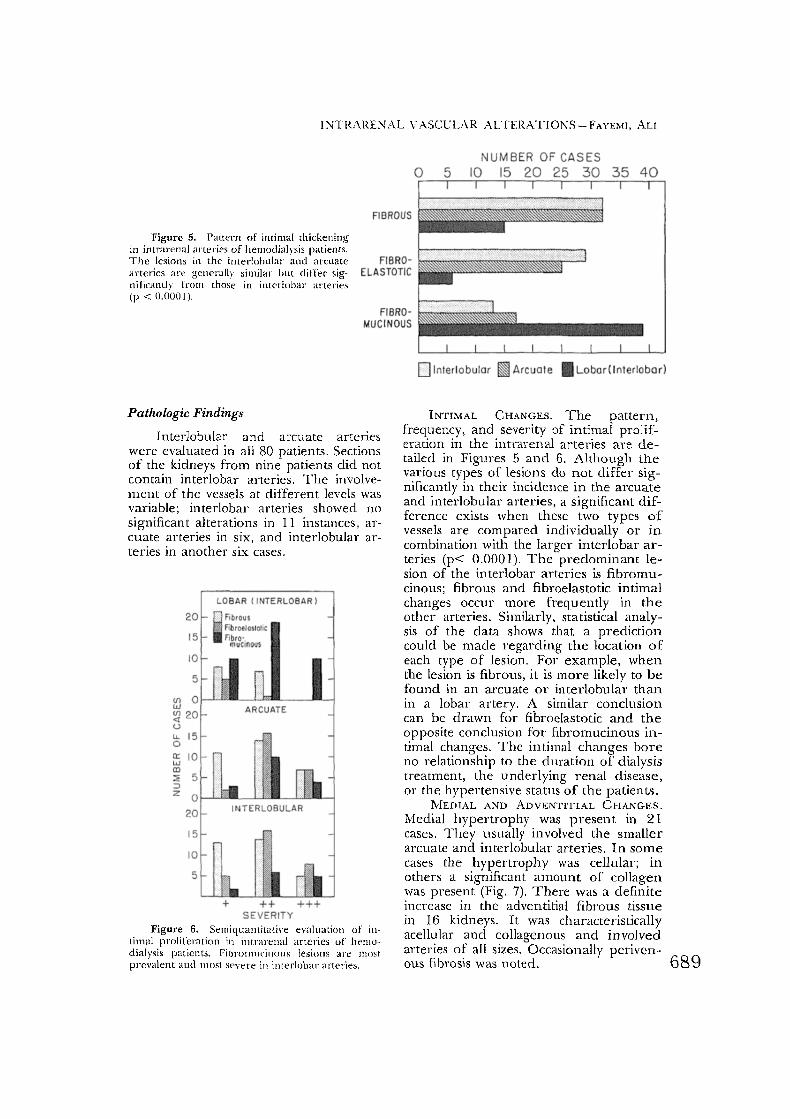
Meclial hypertrophy was p resen t in 21cases. They usually involved the smallerarcuate and interlobular arteries. In somecases the hypertrophy was cellular; inothers a significant amount of collagenwas present (Fig. 7). There was a definiteincrease in the adventitial fibrous tissuein 16 kidneys. It was characteristicallyacellular and collagenous and involvedarteries of all sizes. Occasionally periven-ous fibrosis was noted. 689
ARCUATE
INT ERLOBULAR
(/) 0wl;{l20uu, 15oa: 10wlD~ 5:JZ O t-J'-"'.-._'-J...-_..L.....L~'--i
20
15
10
5
20
15
10
5
++ +++SE VERITY
Figure 6. Semiquantitative evaluation of intimal proliferation in intrarenal arteries of hemodialysis patients. Fibrornucinous lesions are most.prevalent and most severe in interlobar arteries.
Pathologic Findings
Interlobular and arcuate arterieswere evaluated in all 80 patients. Sectionsof the kidneys from nine patients did notcontain interlobar arteries. The involvement of the vessels at different levels wasvariable; interlobar arteries showed nosignificant alterations in II instances, arcuate arteries in six, and interlobular arteries in another six cases.
HUMAN PATHOLOGY-VOLUME 10, NU~IBER 6 November 1979
Figure 7. Arterial wall showing medial thickening and mild fibromucinous intimal lesion.
ARTERIOLAR CHANGES. The ar-terioles were relatively normal in the kidneys of 10 patients. The others showedhyperplastic or hyaline arteriolosclerosis.The severity and distribution of thesechanges are detailed in Table 2. Neitherfibrinoid necrosis nor necrotizing arteriolitis was encountered.
MISCELLANEOUS OnSERVATIONS. Thedeposition of calcium in the renal parenchyma was found in 61 cases. Amongthese, vascular calcification was observedin 10 instances (six mild, four moderate).The larger vessels were more commonlyinvolved. Despite the high frequency andusually severe renal oxalosis in this study,deposition of oxalate crystals in the renalblood vessels was not seen.
TABLE 2. RENAL ARTERIOLAR LESIONS IN
80 HEMODIALYSIS PATIENTS
Type ofLesion Severity of Lesions Total
+ ++ +t+Hyaline
arteriolosclerosis 19 13 3:~
Hyperplasticarteriolosclerosis 9 }[) 12 37
No pathologic
690 alterations 10
DISCUSSION
The present study has shown the distribution and severity of intrarenal vascular lesions in patients with chronic renalfailure on hemodialysis. The entire intrarenal vascular system from the interlobar arteries t.o the arterioles were involved by t.hese pathologic changes.Although fibrous, fibroelastotic, and fibromucinous intimal proliferative lesionsmay be found in intrarenal arteries of alltypes, we have demonstrated that significant differences occur in the distributionof these lesions. Thus, fibroelastotic andfibrous lesions are more likely to be encountered in interlobular and arcuate arteries, whereas the fibromucinous varietyis most prevalent in the interlobar vessels.The duration of dialysis and the hypertensive status of the patients could not becorrelated with the type or severity of thearterial lesions. Similarly the impact ofthe underlying renal diseases on the vascular lesions could not be ascertained.This may be attributed in part to thesmall number of cases in each disease category.
The pathogenesis of intimal thickening in intrarenal arteries is obscure. Twomechanisms have been proposed. The

INTRARENAL VASCULAR ALTERATIONS-FAYEMI, ALI
'1[~i~;;~':::::~1:ng ----)"J> Endothelial >~ Increased permeabilityof vessels damage of endothelium 1
Vasoconstriction
Organization and ~(~---------___ Insudation of plasmarnyointimal proliferation components
(intimal thickening)
Figure 8. Pathogenetic mechanism for intimal thickening in intrarenal arteries.
more widely accepted view, representedschematically in Figure 8, invokes endothelial damage with a subsequent increasein permeability as the initial event. Support for this pathway is derived from experimental work and ultrastructuralstudies. 17•2o Mural thrombosis followed byorganization and endothelialization servesas the basis for the second mechanism ofintimal thickening." In this study recanalized thrombi were seen in only twocases and in these appeared to be secondary to the underlying severely thickenedintima.
The literature contains scanty information about the alterations of the vascular media in chronic renal disease. Observations that have been reported are thoseconcerning the morphology of the arterial media in hypertension. Sinclair et al."noted an "attenuated" layer of mediastretched around the intima; Pitcock eta!.5 found that the media was frequentlynormal, occasionally showed thinning,and rarely was completely absent; jones"described a thin layer of hypertrophiedmedial cells stretched over an "onionskin" type of intimal proliferation.
However, divergent data are provided by ~jungqvist,22 who in a microangiographic and histologic study of intrarenalarterial patterns in malignant hypertension found hypertrophy of the vascularmedia. The media may be thick in theearly phases of hypertension but maysubsequently become atrophic." The onlyreference to the medial alterations in theend stage kidney disease in hemodialysispatients is provided by McManus et al.,"who found a decrease in the musculaturebut an increase in the ground substanceof the media.
The findings in the present study are
at variance with this conclusion. Aboutone-quarter of our patients showed hypertrophy of the smaller arcuate and interlobular arteries. These changes wereusually associated with a hyperplastic"onion skin" type of intimal lesion in thearterioles. Unfortunately we did notquantitate the degree of medial thickening in these cases. The discrepancy inthese findings may be explained by suggesting that medial hypertrophy occursas an initial response to hypertension.Later, as the elevated blood pressure becomes more severe or chronic, secondarythinning by dilatation of the vesselsensues. This may be combined with medial atrophy resulting from external pressure exerted by the severely thickened intima. The situation would be similar tothe changes encountered in the vessels ofthe lungs in pulmonary hypertension."
The absence of necrotizing arteriolarlesions in this investigation is of some interest. The arterioles showed either hyperplastic and hyaline arteriolosclerosis inalmost equal proportions. This findingconfirms the observations of others whohave recently studied the renal vascularchanges in hypertensive kidneys." 6,11 Arteriolar fibrinoid necrosis, traditionallyconsidered the hallmark of malignant hypertension, has been encountered lessfrequently in these studies. The decreased incidence of this pathologicchange has been linked with better drugcontrol of hypertension.v !' Since hemodialysis ameliorates hypertension to aconsiderable extent through a reductionin body electrolytes and extracellularfluid, it would be expected that fibrinoidnecrosis would be less commonly encountered in hemodialysis patients.
The significance of the intrarenal 691
HUMAN PATHOLOGY- VOLUME 10, NUMBER 6 November 1979
692
vascular changes in hemodialysis patientslies in the probability of sustaining hypertension, a central problem in the management of patients with end stage renaldisease. The prevailing current opinionholds that hypertension, especially the essential type, precedes and induces intrarenal vascular disease.': 2, 7 This viewhas been vigorously challenged by Goldblatr'" and Hollenberg et al.,25-27 who inelegant studies have demonstrated theimportant role of the renal vasculature inthe pathogenesis and sustenance of hypertension. The latter have shownthrough pharmacologic and radiographicstudies that vasoconstriction of intrarenalvessels may be the primary abnormalityin renal ischemia in a large number ofhypertensive patients ,26 The presentstudy provides anatomic support for thispoint of view. The intrarenal microvascular alteration in patients maintained onhemodialysis reported herein leads tonarrowing of the vascular lumen, whichwould produce and accentuate renal ischemia. This, in turn, may adversely affect the hypertensive status of the patients.
Our observations have led us to conclude that the vascular alterations inthese patients should not be regarded aspassive lesions emanating from kidneyswhose functions have been usurped byartificial support, but as a probablesource of significant morbidity.
ACKNOWLEDGMENT
We are indebted to Dr. David Korts,Department of Biostatistics, The MountSinai School of Medicine, New York, forthe statistical analysis and to Joyce Yondolino for secretarial assistance.
REFERENCES
1. Heptinstall, R. H.: Pathology of end-stage kidney disease. Am. j. Med., 44 :656, 1968.
2. Heptinstall, R. H.: Pathology of the Kidney.Ed. 2. Boston, Little. Brown and Company,1974.
3. Schwartz, M. M., and Cotran, R. S.: Primaryrenal disease in transplant recipients. Hum.Path., 7:455, 1976.
4. Velosa, J., Miller, K., and Michael, A. F.: Im-
munopathology of the end-stage kidney. Immunoglobulin and complement componentdeposition in non-immune disease. Am. j.Path., 84:149, 1976.
5. Pitcock, J. A., johnson, J. G., Hatch, F. E., etal.: Malignant hypertension in blacks. Malignant intrarenal arterial disease as observed bylight and electron microscopy. Hum. Path.,7:333, 1976.
6. jones, D. B.: Arterial and glomerular lesions associated with severe hypertension. Light andelectron microscopic studies. Lab. Invest.,31 :303, 1974.
7. Stoddard, L. D., and Puchtler, H.: Humanrenal vascular lesions and hypertension. InSommers, S. C. (Editor): Pathology Annual.New York, Appleton-Century-Crofts, 1969,Vol. 4, p. 253.
8. Heptinstall, R. H.: Malignant hypertension: astudy of 51 cases. J. Path. Bact., 65:423,1953.
9. MacMahon, H. E.: Malignant nephrosclerosis - a reappraisal. In Sommers, S. C. (Editor): Pat11010gy Annual. New York, AppletonCentury-Crofts, 1968, Vol. 3, p. 297.
10. Cannon, P. J., Hassav, M., Case, D. B., et al.:The relationship of hypertension and renalfailure of scleroderma (progressive systemicsclerosis) to structural and functional abnormalities of the renal cortical circulation. Medicine, 53: 1, 1974.
11. Sinclair, R. A., Antonovych, T. T., and Mostofi,F. K.: Renal proliferative arteriopathies andassociated glomerular change. A light andelectron microscopic study. Hum. Path.,5 :565, 1976.
12. Pardo, V., Fisher, E. R., Perez-Stable, E., et al.:Ultrastructural studies in hypertension. II.Renal vascular changes in progressive systemic sclerosis. Lab. Invest., 15:1434,1976.
13. Vitsky, B. H., Suzuki, Y., Strauss, L., et al.: Thehemolytic-uremic syndrome: the study ofrenal pathologic alterations. Am. J. Path.,57:627, 1969.
14. Pollack, V. E., and Nettles, J. B.: The kidney intoxemia of pregnancy: a clinical and pathologic study based on renal biopsies. Medicine,39:469, 1960.
15. Kincaid-Smith, P.: The Kidney. Oxford, Blackwell Scientific Publications, 1975.
16. McManus. J. F. A., Hughson, M. D., Fitts, G.,et al.: Studies on "end-stage" kidneys. I. Nodule formation in intrarenal arteries and arterioles. Lab. Invest., 37:339, 1977.
17. Wiener, j., Spiro, D., and Lattes, R. G.: Thecellular pathology of hypertension. II. Arteriolar hyalinosis and fibrinoid change. Am.J. Path .. 47:456, 1965.
18. Esterly, J. A., and Glagov, S.: Altered permeability of the renal artery of the hypertensiverat: an electron microscopic study. Am. J.Path., 43:619,1963.
19. Allison, P. R., Bleechan, M., Brown, W., et al.:The production and resolution of hypertensive vascular lesions in the rabbit. Clin. Sci.,33:39,1967.
20. Olsen, F.: Penetration of circulating fluorescentproteins into walls of arterioles and venules
INTRARENAL VASCULAR ALTERATIONS-FAYEMI, ALI
in rats with intermittent acute angiotensinhypertension. Acta Path. Microbiol. Scand.,74 :325, 1968.
21. McGee, W. G., and Ashworth, C. T. : Finestructure of chronic hypertensive arterioparhy in human kidney. Am. J. Path., 43:273 ,1963.
22. Ljungqvist, A.: The intrarenal arterial patternin essential hypertension . A microangiographic and histologic stud y. J. Path .Bact., 84:313 ,1962.
23. Wagenvoort, C. A. , and Wagenvoort, N.: Pathology of Pulmonary Hypertension. NewYork, John Wiley & Sons, Inc., 1977, P: 62.
24. Goldblatt, H .: Hypertension due to renal ischemia. Bull. N.Y. Acad. Med., 40:745, 1964.
25. Hollenberg, N. K., Adams, D. F., Solomon, H.,et aJ.: Rena l vascular tone in essential andsecondary hypertension: hemodynamic andangiographic responses to vasodilators. Medicine (Baltimore), 54:29, 1975.
26. Hollenberg, N. K., and Adams, D. F.: Therenal circulation in hypertensive disease. Am.J . Med., 60:773, 1976.
27. Hollenberg, N. K., Borucki, L. ]., and Adams,D. F.: The renal vasculature in early essentialhypertension: evidence for a pathogeneticrole. Medicine (Baltimore), 57:167. 1978.
Department of PathologyHoly Name HospitalTeaneck, New Jersey 07666 (Dr. Fayemi)
693




















