Intracerebral quinolinic acid injection in the rat: Effects on dopaminergic neurons

320Neuro-Oncology■JULY 2006
Neuro-oNcology
The purpose of this study is to determine the maximum tolerated dose (MTD), dose-limiting toxicity (DLT), and intracerebral distribution of a recombinant toxin (TP-38) targeting the epidermal growth factor receptor in patients with recurrent malignant brain tumors using the intracerebral infusion technique of convection-enhanced delivery (CED). Twenty patients were enrolled and strati-fied for dose escalation by the presence of residual tumor from 25 to 100 ng/ml in a 40-ml infusion volume. In the last eight patients, coinfusion of 123I-albumin was performed to monitor distribution within the brain. The MTD was not reached in this study. Dose escalation was stopped at 100 ng/ml due to inconsistent drug delivery as evidenced by imaging the coinfused 123I-albumin. Two DLTs were seen, and both were neurologic. Median sur-vival after TP-38 was 28 weeks (95% confidence inter-val, 26.5–102.8). Of 15 patients treated with residual dis-ease, two (13.3%) demonstrated radiographic responses, including one patient with glioblastoma multiforme who had a nearly complete response and remains alive .260
Intracerebral infusion of an EGFR-targeted toxin in recurrent malignant brain tumors
John H. Sampson, Gamal Akabani, Gerald E. Archer, Mitchel S. Berger, R. Edward Coleman, Allan H. Friedman, Henry S. Friedman, Kim Greer, James E. Herndon II, Sandeep Kunwar, Roger E. McLendon, Alison Paolino, Neil A. Petry, James M. Provenzale, David A. Reardon, Terence Z. Wong, Michael R. Zalutsky, Ira Pastan, and Darell D. BignerDivision of Neurosurgery, Department of Surgery (J.H.S., G.E.A., A.H.F., H.S.F., D.A.R.), Department of Pathology (J.H.S., R.E.M., D.D.B.), Department of Radiology (G.A., R.E.C., K.G., N.A.P., J.M.P., T.Z.W., M.R.Z.), and Department of Biostatistics and Bioinformatics (J.E.H.), Duke University Medical Center, Durham, NC; Department of Neurosurgery, University of California, San Francisco, San Francisco, CA (M.S.B., S.K.); Department of Neurological Surgery, Emory University, Atlanta, GA (A.P.); and Laboratory of Molecular Biology, National Cancer Institute, Bethesda, MD (I.P.); USA
Received May 30, 2007; accepted September 19, 2007.
Address correspondence to John H. Sampson, Division of Neurosurgery, Department of Surgery, Box 3050, Room 220 Sands Building, Duke University Medical Center, Durham, NC 27710, USA ([email protected]).
weeks after therapy. Coinfusion of 123I-albumin demon-strated that high concentrations of the infusate could be delivered .4 cm from the catheter tip. However, only 3 of 16 (19%) catheters produced intraparenchymal infusate distribution, while the majority leaked infusate into the cerebrospinal fluid spaces. Intracerebral CED of TP-38 was well tolerated and produced some durable radio-graphic responses at doses <100 ng/ml. CED has signifi-cant potential for enhancing delivery of therapeutic mac-romolecules throughout the human brain. However, the potential efficacy of drugs delivered by this technique may be severely constrained by ineffective infusion in many patients. Neuro-Oncology 10, 320–329, 2008 (Posted to Neuro-Oncology [serial online], Doc. D07-00107, April 10, 2008. URL http://neuro-oncology.dukejournals.org; DOI: 10.1215/15228517-2008-012)
Keywords: brain neoplasms, convection, drug delivery sys-tems, epidermal growth factor receptor, immunotoxins
The prognosis for patients with malignant primary or metastatic brain tumors remains poor.1 Fail-ure of conventional therapies can be attributed,
at least in part, to their lack of specificity for neoplastic tissue, which results in dose-limiting systemic or neuro-logic toxicity.2 Protein cytotoxins produced by bacteria and plants represent a novel class of therapeutic agents
Copyright 2008 by the Society for Neuro-Oncology

Sampson et al.: Intracerebral infusion of an EGFR-targeted toxin
Neuro-oNcology • J U N E 2 0 0 8 321
that can be conjugated to specific ligands and deliv-ered regionally to target tumors more specifically.3–6 These targeted toxins have produced dramatic clinical responses in therapeutically refractory patients with leu-kemia7–9 and lymphoma.10,11 The efficacy of these agents is likely related to their potency, specificity, immunity to resistance mechanisms, and lack of dependence on cell-cycle kinetics. Results in solid tumors, however, have been less encouraging, possibly because these large molecules have difficulty penetrating solid tumors.12–15 The surface expression of targeted antigens may also be lower and the heterogeneity of antigen expression may be greater in solid neoplasms; as a result, a single anti-body is less likely to target all neoplastic cells.
Delivery of high-molecular-weight agents, such as targeted toxins, to tumors within the intracerebral com-partment is even more challenging because these tumors are further isolated from the systemic circulation by the restrictive blood-brain barrier (BBB).13,14,16–19 Regional intracerebral drug delivery, however, bypasses the BBB and has the potential to deliver high concentrations of the therapeutic agent directly to the site of the tumor, thereby reducing the risk of systemic toxicity. The inno-vative regional drug delivery technique of convection-enhanced delivery (CED) uses a fluid pressure gradient to infuse therapeutic molecules directly into the interstitial spaces of the brain that are infiltrated with tumor.20–23 The potential of this simple approach has been clearly demonstrated in preclinical studies by others, especially Lonser and Oldfield’s group, and more recently by our-selves.19,20,22–37 The results of early clinical studies21,38–47 have also shown some potential efficacy, but they have not attempted to assess the adequacy of drug distribu-tion in humans.
TP-38 is a 43.5-kDa recombinant chimeric protein containing a genetically engineered form of the cytotoxic Pseudomonas exotoxin (PE). By replacing the native binding domain of PE with transforming growth factor-a (TGF-a), the TP-38 construct has been specifically tar-geted to the epidermal growth factor receptor (EGFR). EGFR is frequently overexpressed in malignant gliomas and metastatic tumors of the brain,48 but is expressed at only very low levels within normal human brain.49,50 In this phase I study we sought to determine the maximum tolerated dose (MTD), dose-limiting toxicity (DLT), and intracerebral distribution of TP-38 using the intracere-bral infusion technique of CED. We show that CED of TP-38 is well tolerated at effective doses and provides some encouraging radiographic responses. However, we also show that the potential efficacy of agents delivered by CED may be severely constrained by inconsistent and ineffective infusion in many patients.
Materials and Methods
TP-38
TP-38 is a recombinant protein consisting of a genetic fusion of TGF-a and a modified PE, PE-38, formed by the deletion of domain Ia/Ib. This deletion results in a
toxin (containing amino acids 253–364 and 381–604) with intact adenosine diphosphate-ribosylating activity but negligible cytotoxicity because of its inability to bind cells. Replacing the native binding domain with TGF-a selectively targets the toxin to cells expressing the EGFR. Prior to delivery, TP-38 was diluted with 0.2% human albumin (Plasbumin-25; Bayer Corporation, Elkhart, IN, USA) in 0.9% saline.
Patient Selection, Study Design, and Toxicity Monitoring
Twenty adult patients with a KPS score >60 with recur-rent or progressive malignant primary or metastatic brain tumors were enrolled at Duke University (19 patients) or the University of California, San Francisco (1 patient). Patients were excluded if they had a tumor >5 cm in maximum diameter, midline brain shift >0.5 cm, evidence of cerebral uncal herniation, or diffuse subependymal disease. An interval of at least 4 weeks between prior radiation or chemotherapy and enroll-ment was required. The Duke University and Univer-sity of California at San Francisco institutional review boards (0344-01) and the U.S. Food and Drug Adminis-tration (BB-IND-9184) approved the protocol. Informed consent was obtained from the patients after the nature of all procedures was explained.
Two barium-impregnated catheters (PS Medical cere-brospinal fluid [CSF]-ventricular catheter no. 41207; Medtronic, Inc., Minneapolis, MN, USA) with an outer diameter of 2.1 mm were placed in each patient with stereotactic guidance. These standard ventricular cath-eters had perforations extending proximally from the catheter tip for 17 mm. The tip of each catheter was positioned to target either residual contrast-enhancing tumor or deep white matter adjacent to areas of pre-viously resected tumor. All patients underwent radio-graphic imaging to confirm catheter placement prior to infusion. Corticosteroids were administered every 6 h and continued for at least 72 h after the completion of the TP-38 infusion. TP-38 was infused over 50 h at a flow rate from each catheter of 0.4 ml/h for a total vol-ume of 40 ml. Intracranial pressure (ICP) was monitored throughout the infusion.
Toxicity and Response Evaluation
Patients were treated on a dose-escalation protocol to determine the MTD and DLT. Patients were stratified by the presence or absence of residual disease for dose escalation but not for toxicity assessment. Three escalat-ing concentrations of TP-38 were selected for study as follows: 25 ng/ml, 50 ng/ml, and 100 ng/ml. The volume of infusate and flow rate were kept constant at each con-centration. At least three patients were entered at each dose level in each stratum. If one of the three patients developed a DLT, as described below, an additional three patients were entered at that dose level. The MTD was defined as the highest dose level at which fewer than two subjects developed DLT. DLT was defined by the NCI Common Toxicity Criteria as a grade 3 or greater

Sampson et al.: Intracerebral infusion of an EGFR-targeted toxin
322 Neuro-oNcology • J U N E 2 0 0 8
lution) fanbeam collimators and a Precise (Precise Corp., Caryville, TN, USA) pinhole collimator. The volume of distribution was subsequently determined by a threshold pixel method that has proved to be accurate at our insti-tution for calculating the volume of small spheres rang-ing in size from 1.3 cm3 to 5.3 cm3 in a brain phantom model with a resolution of 3 mm. Isodose contours were calculated using a three-dimensional discrete Fourier transform convolution. Fiduciary markers were used to co-register these SPECT images with MR with a spatial margin of error of less than 1 mm.
Results
Patient Characteristics
Demographic and treatment information for all partici-pants is given in Table 1. All patients had recurrent dis-ease in the brain except for the patient with the spindle cell metastasis (patient 7). In the strata without residual disease, three patients received TP-38 at the initial dose level of 25 ng/ml (1 mg total dose), and two received 50 ng/ml (2 mg). In the strata with residual disease at the time of TP-38 treatment, three patients received TP-38 at the initial dose level of 25 ng/ml (1 mg total dose); six received 50 ng/ml (2 mg); and six received 100 ng/ml (4 mg). Eighteen of the 20 patients received no further therapy after TP-38 until progressive disease was identi-fied pathologically, and two patients received systemic chemotherapy after TP-38 before evidence of tumor recurrence. One of these two patients (patient 7) received chemotherapy after voluntarily withdrawing from the protocol. The other patient (patient 19) had never been treated with chemotherapy and so elected to do so after TP-38 therapy but before tumor recurrence.
Toxicity
All toxicities encountered have been neurologic, and no hepatic, renal, or hematologic toxicities have occurred. Five patients, all with preexisting seizure disorder, had a seizure during the TP-38 infusion, but all seizures resolved following anticonvulsant medication adjust-ments. Other adverse events are shown in Table 2.
DLTs were identified in two patients (Table 3). One patient (patient 8) with residual disease, treated at the 50-ng/ml dose level, developed a grade 3 hemiparesis. Although this was considered to be a DLT, it may also have been related to tumor recurrence, which was diag-nosed 3 weeks later. Three more patients with residual disease were treated at the 50-ng/ml dose level as a precaution, but no DLTs were identified in these sub-sequent three patients. In addition, during this interval, two patients without residual disease were also treated at this dose level without incident. However, one patient (patient 15), also with residual disease, treated at the 100-ng/ml dose level developed grade 4 constitutional symptoms (fatigue) possibly related to TP-38. This patient had a substantial leak of the infusate intraven-tricularly, which may have been the cause of this toxic-
hematologic or grade 4 or greater nonhematologic toxic-ity, although seizures that were not different in character or increased in frequency were not considered DLTs. In addition, an ICP of >30 mmHg for greater than 30 min, a decrease in the Glasgow Coma Scale (GCS) score of >2 points, and development of a new focal neurologic deficit that did not resolve within 2 weeks with medical management were also considered DLTs.
Patients underwent physical and neurologic examina-tions, and MR imaging upon completion of the TP-38 infusion and at 4, 8, 16, 24, 36, and 48 weeks postinfu-sion. Radiographic responses were defined as previously outlined51 on consecutive contrast-enhanced MR or CT scans at least 4 weeks apart, combined with clinical neu-rologic stability or improvement and no increase in ste-roid dose. All adverse events were recorded, whether or not they were thought to be drug related. Corticosteroids must have been at a stable dose for at least 1 week prior to entry. Thereafter, they were allowed to be increased if necessary, but episodes of acute cerebral edema requir-ing emergent intervention were considered DLTs.
Imaging
For the first 48 h of each infusion in the last eight patients treated at Duke University, 123I-labeled albumin was coinfused with TP-38 in the same infusion volume. The radiolabeled albumin was used for imaging the distribu-tion of the infusion instead of the unlabeled albumin routinely used as a carrier protein for these infusions. This was done because the protein doses of TP-38 used were too low to be radiolabeled with sufficient radioac-tivity to be imaged directly and because the radiolabel-ing procedure has the potential to damage the EGFR binding site of the toxin. The goal of this approach was to determine which infusions provided effective distri-bution of the infusate intraparenchymally and which leaked into the subarachnoid space or ventricle. The albumin was purified to homogeneity by ion-exchange high-pressure liquid chromatography and radiolabeled with 123I (MDS Nordion International, Vancouver, BC, Canada) using a modified iodogen method with a target dosage of 80 mCi on 10 mg of albumin. 123I-labeled albu-min was chosen because its size, shape, and molecular weight (66.5 kDa) are similar to those of TP-38 (44 kDa) and albumin forms an otherwise essential component of cytotoxin drug formulations. In addition, recent work by Murad et al.52 has shown in well-controlled animal studies that labeled albumin does precisely track the dis-tribution of a similar targeted toxin. Although the use of albumin as a surrogate for imaging drug distribution does not allow evaluation of the potential influence of drug-binding kinetics on distribution, it should be noted that TP-38 was used at a concentration in this study predicted to exceed that needed to saturate all potential binding sites.
Single-photon emission computed tomography (SPECT) scans of the head were obtained at 24 h and at the completion of the infusion with a three-head SPECT scanner (Trionix Research Labs, Twinsburg, OH, USA) fitted with two Triad LESR (low-energy super-high reso-

Sampson et al.: Intracerebral infusion of an EGFR-targeted toxin
Neuro-oNcology • J U N E 2 0 0 8 323
ity. Three additional patients with residual disease were treated at the 100-ng/ml dose level and experienced no DLTs. In addition to these events, one patient devel-oped a subdural hygroma, and one patient had an intra-cerebral hemorrhage after catheter placement but before TP-38 therapy.
Response, Progression, and Survival
Overall, 2 of 15 (13.3%) patients with residual tumor at the time of therapy have demonstrated radiographic responses. One patient (patient 2), also described above, who was treated for a multirecurrent bifrontal glioblas-toma multiforme (GBM) at the 25-ng/ml dose level, had a nearly complete response that was sustained for 198 weeks, but ultimately developed tumor recurrence (Fig. 1).46 Another patient (patient 18) treated at the 100-ng/ml dose, had a partial response with .50%
shrinkage of tumor diameter 24 weeks after TP-38 therapy but then died 34 weeks after TP-38 therapy of unrelated infectious complications (Fig. 2). In addition, a third patient (patient 12), without residual disease at the time of treatment, developed a large area of con-trast enhancement 9 weeks after treatment that was never biopsied but has subsequently regressed without additional treatment (Fig. 3). It remains unclear whether this enhancing area represented a tumor recurrence with spontaneous remission or an asymptomatic inflamma-tory reaction to infusion or the drug.53 This patient with GBM remains alive and without evidence of tumor pro-gression .211 weeks after initial diagnosis.
All but two patients in this study have died from progressive disease. One patient (patient 12) with GBM remains alive and without progression .211 weeks after TP-38 therapy, and another patient (patient 2) with GBM went 198 weeks without progressive disease after
Table 1. Patient demographic summary
Histologic TP-38 Therapy after No. Age KPS Diagnosis Therapy Prior to TP-38 (ng/ml) TP-38
Residual tumor
2 59 80 GBM OR, EBRT, carmustine, cisplatin, etoposide, carmustine 25 None wafers/temozolomide, irinotecan, cyclophosphamide, tamoxifen
3 40 80 GBM OR, EBRT, carmustine/mercaptopurine 3 1, EBRT, lomustine 3 6, 25 None temozolomide 3 6
4 55 60 GBM OR 3 2, 131I-monoclonal antibody, EBRT, temozolomide 3 2, 25 Thalidomide lomustine 3 4, etoposide, irinotecan/temozolomide
5 55 60 GBM OR, EBRT, procarbazine/lomustine/vincristine 3 6, 50 None temozolomide/tamoxifen 3 4, OR
6 51 90 GBM OR 3 2 EBRT, lomustine 3 6 50 Temozolomide
8 55 90 GBM OR, EBRT, lomustine 3 2, radiosurgery, temozolomide 3 5, OR 50 None
9 58 90 GSC OR, OR, EBRT, carmustine/irinotecan 3 1, temozolomide 3 4, 50 Etoposide tamoxifen 3 4
10 45 90 GBM OR, EBRT, OR, 131I-monoclonal antibody, EBRT, temozolomide 3 4, 50 None lomustine 3 4, etoposide 3 2, temozolomide 3 1, lomustine 3 4
13 52 90 GBM OR, EBRT, lomustine 3 2, temozolomide 3 2, irofulven 3 3 50 Irinotecan
15 62 70 GBM OR, 125I brachytherapy, EBRT, Cu21 chelation, temozolomide 3 9, 100 None irinotecan 3 8
16 49 90 GBM OR, EBRT, temozolomide 100 None
17 50 90 AO OR, EBRT, procarbazine/lomustine/vincristine 3 6, OR 100 Temozolomide/ irinotecan 3 5
18 48 90 GBM OR, EBRT 100 None
19 31 90 GBM OR, EBRT 100 Irinotecan
20 21 90 GBM OR 3 2, EBRT 100 None
No residual tumor
1 59 90 GBM OR, EBRT, lomustine 3 2, etoposide/tamoxifen 3 2, irinotecan 3 2, 25 None lomustine 3 1, temozolomide 3 3, thalidomide, radiosurgery, topotecan
7 23 90 Metastatic None for brain metastasis 25 Temozolomide/ spindle cell imatinib mesylate
11 56 90 GBM OR, EBRT, carmustine 3 2, OR 25 Temozolomide/ O6-benzylguanine
12 55 90 GBM OR, EBRT, lomustine 3 2, temozolomide 3 2, OR 50 None
14 68 100 GBM OR, radiosurgery, EBRT, temozolomide 3 1 50 OSI-774
Abbreviations: GBM, glioblastoma multiforme; OR, operative resection; EBRT, external beam radiation therapy; GSC, gliosarcoma; AO, anaplastic oligodendroglioma.

Sampson et al.: Intracerebral infusion of an EGFR-targeted toxin
324 Neuro-oNcology • J U N E 2 0 0 8
a nearly complete response to TP-38 and remains alive .260 weeks from TP-38 therapy.46 Overall median time to progression (TTP) was 14.9 weeks (95% confidence interval [CI], 4.1–45.1; range, ,1–210.57 weeks) in this mostly heavily pretreated group. Median TTP was slightly longer in patients without residual disease at the time of treatment (17.1 weeks; 95% CI, 9.6–129.3) when compared to those with residual disease (14.1 weeks; 95% CI, 3.9–42.1), but this difference was not statisti-cally significant (p 5 0.32). The study, however, was not powered to detect such differences.
Overall median survival after TP-38 therapy for all patients was 28 weeks (95% CI, 26.5–102.8; range, 1.1 to .260 weeks). For patients with residual disease at the time of TP-38 therapy, median survival was only 20.1 weeks (95% CI, 16.7–110.0), whereas for those without radiographic evidence of residual disease, median sur-
vival was 33.0 weeks (95% CI, 0–170.4), but again this difference was not statistically significant (p 5 0.60). However, the study was not powered to detect such dif-ferences.
Drug Distribution Imaging
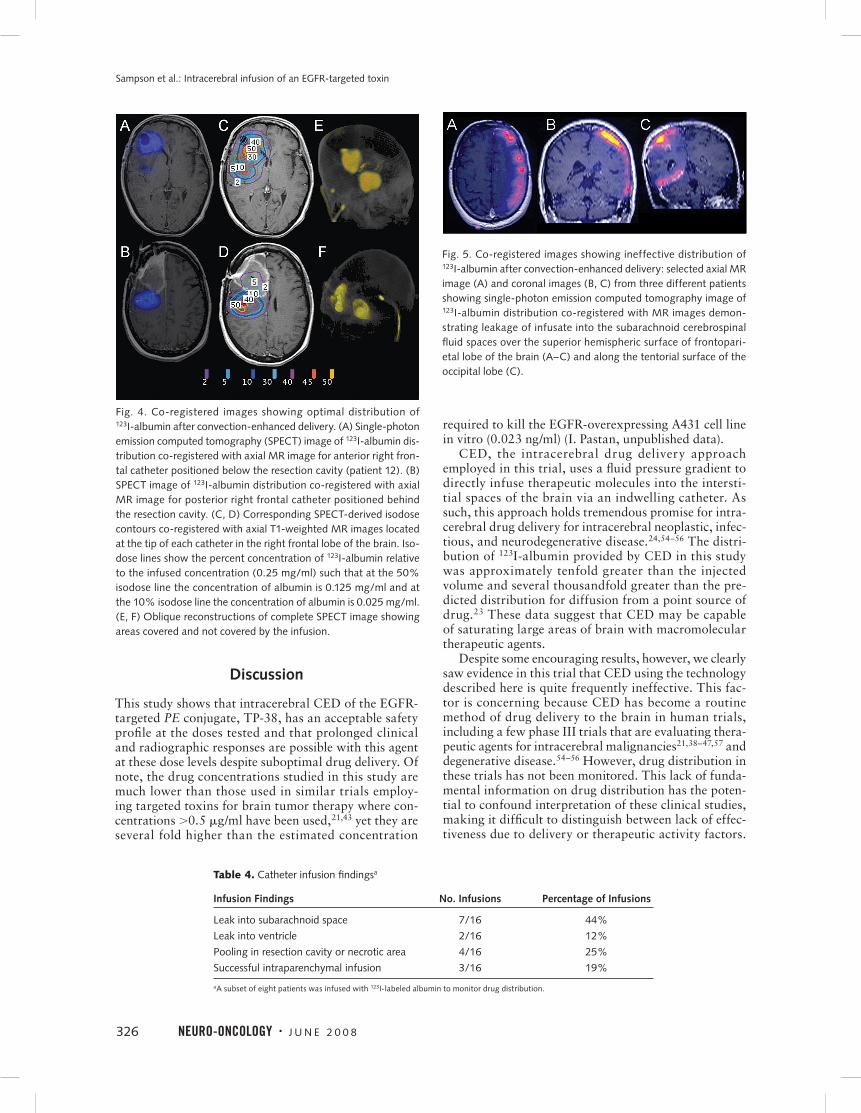
SPECT imaging of coinfused 123I-labeled albumin dur-ing and immediately after infusion demonstrated that the intracerebral delivery technique of CED is capable of producing extensive and relatively homogeneous dis-tribution of high-molecular-weight molecules within the human brain in some patients (Fig. 4). For example, in patient 12, after 24 h of infusion (9.6 ml), the volumes of distribution from each catheter at the 10% isodose level relative to infused dose were found to be 54 ml and 60 ml, respectively. Similarly, at the end of the 50-h infu-sion, the volumes of distribution at a 10% isodose level were found to be 174 ml and 292 ml, respectively. Thus, this novel technique for bypassing the BBB allowed for distribution of at least 10% of the injected concentration of this macromolecule within a nearly spherical radius of 3.5 cm and 4.1 cm (patient 12).
Although in some cases CED did provide dramatic distributions of the infusate, very concerning was the number of catheters for which imaging identified signifi-cant leaks of infusate into the subarachnoid or intraven-tricular CSF spaces (Table 4; Fig. 5). We imaged infu-sions from eight patients with a total of 16 catheters. In all but three patients (19%) infusate distributions were significantly influenced by such leaks and failed to pro-duce any significant intraparenchymal distribution. Typ-ically, these leaks were thought to be due to the catheter trajectory perforating a deep pial or ependymal border that allowed a path of least resistance for the infusate away from the interstitial space. In one specific example, the catheter trajectory traversed the deep portions of the Sylvian fissure (Fig. 6). Based on the imaging studies, which failed to show adequate delivery of the drug in the majority of patients, the study was halted at a dose of 100 ng/ml without reaching an MTD.
Table 2. Summary of adverse eventsa
Grade 1 Grade 2 Grade 3 Grade 4
Summary by dose
25 ng/ml 2
50 ng/ml 1 9 1 (8)b,c
100 ng/ml 1 5 1 1 (15)b
Summary by type
Neuropathy—motor (hemiparesis) 2 1 (8)b,c
Headache 1 5 1
Ocular/visual 2
Speech 3
Seizured 1
Constitutional 1 1 1 (15)b
aEvents that were related to catheter placement (before TP-38 delivery) are not
included. All adverse events resolved with the exception of the grade 3 and 4 events
shown. For events occurring more than once, only the highest grade event for each
patient is recorded. Some patients had more than one event.
bDose-limiting toxicities; patient numbers are shown in parentheses.
cMay have been related to recurrent tumor.
dOverall, 5 of 20 patients (25%) had seizures prior to TP-38 therapy. These were not
included as adverse events unless there was an increase in frequency.
Table 3. Dose-limiting toxicities
Grade 3 or 4 Grade 4 Decrease in GCS Dose No. Hematologic Nonhematologic Increased or New Focal Percent Level Patients Toxicity Toxicity ICP Neurologic Deficit DLT
Residual tumor
25 ng/ml 3 0 0 0 0 0%
50 ng/ml 6 0 0 0 1a 16.7%
100 ng/ml 6 0 1b 0 0 16.7%
No residual tumor
25 ng/ml 3 0 0 0 0 0%
50 ng/ml 2 0 0 0 0 0%
100 ng/ml 0 0 0 0 0 0%
Abbreviations: ICP, intracranial pressure; GCS, Glasgow Coma Scale score; DLT, dose-limiting toxicity.
aHemiparesis that may have been related to recurrent tumor.
bConstitutional.
Sampson et al.: Intracerebral infusion of an EGFR-targeted toxin
Neuro-oNcology • J U N E 2 0 0 8 325
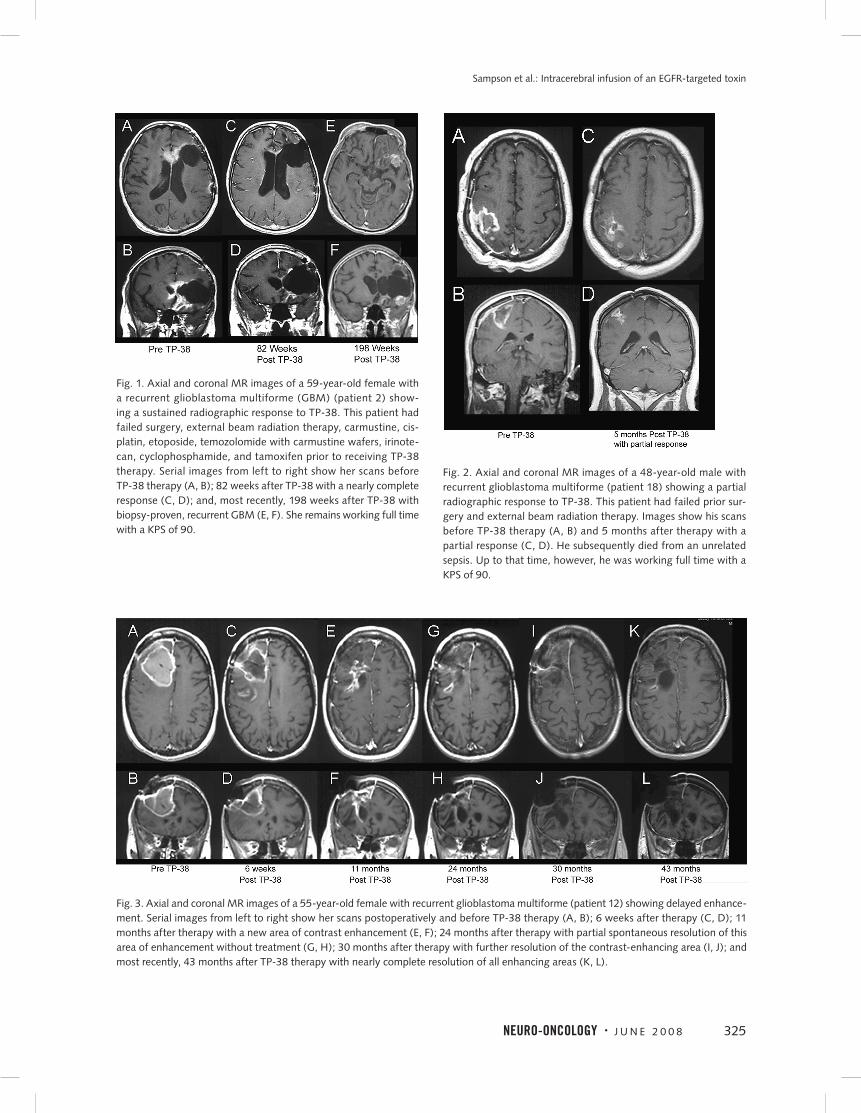
Fig. 1. Axial and coronal MR images of a 59-year-old female with a recurrent glioblastoma multiforme (GBM) (patient 2) show-ing a sustained radiographic response to TP-38. This patient had failed surgery, external beam radiation therapy, carmustine, cis-platin, etoposide, temozolomide with carmustine wafers, irinote-can, cyclophosphamide, and tamoxifen prior to receiving TP-38 therapy. Serial images from left to right show her scans before TP-38 therapy (A, B); 82 weeks after TP-38 with a nearly complete response (C, D); and, most recently, 198 weeks after TP-38 with biopsy-proven, recurrent GBM (E, F). She remains working full time with a KPS of 90.
Fig. 2. Axial and coronal MR images of a 48-year-old male with recurrent glioblastoma multiforme (patient 18) showing a partial radiographic response to TP-38. This patient had failed prior sur-gery and external beam radiation therapy. Images show his scans before TP-38 therapy (A, B) and 5 months after therapy with a partial response (C, D). He subsequently died from an unrelated sepsis. Up to that time, however, he was working full time with a KPS of 90.
Fig. 3. Axial and coronal MR images of a 55-year-old female with recurrent glioblastoma multiforme (patient 12) showing delayed enhance-ment. Serial images from left to right show her scans postoperatively and before TP-38 therapy (A, B); 6 weeks after therapy (C, D); 11 months after therapy with a new area of contrast enhancement (E, F); 24 months after therapy with partial spontaneous resolution of this area of enhancement without treatment (G, H); 30 months after therapy with further resolution of the contrast-enhancing area (I, J); and most recently, 43 months after TP-38 therapy with nearly complete resolution of all enhancing areas (K, L).
Sampson et al.: Intracerebral infusion of an EGFR-targeted toxin
326 Neuro-oNcology • J U N E 2 0 0 8
Discussion
This study shows that intracerebral CED of the EGFR-targeted PE conjugate, TP-38, has an acceptable safety profile at the doses tested and that prolonged clinical and radiographic responses are possible with this agent at these dose levels despite suboptimal drug delivery. Of note, the drug concentrations studied in this study are much lower than those used in similar trials employ-ing targeted toxins for brain tumor therapy where con-centrations .0.5 mg/ml have been used,21,43 yet they are several fold higher than the estimated concentration
required to kill the EGFR-overexpressing A431 cell line in vitro (0.023 ng/ml) (I. Pastan, unpublished data).
CED, the intracerebral drug delivery approach employed in this trial, uses a fluid pressure gradient to directly infuse therapeutic molecules into the intersti-tial spaces of the brain via an indwelling catheter. As such, this approach holds tremendous promise for intra-cerebral drug delivery for intracerebral neoplastic, infec-tious, and neurodegenerative disease.24,54–56 The distri-bution of 123I-albumin provided by CED in this study was approximately tenfold greater than the injected volume and several thousandfold greater than the pre-dicted distribution for diffusion from a point source of drug.23 These data suggest that CED may be capable of saturating large areas of brain with macromolecular therapeutic agents.
Despite some encouraging results, however, we clearly saw evidence in this trial that CED using the technology described here is quite frequently ineffective. This fac-tor is concerning because CED has become a routine method of drug delivery to the brain in human trials, including a few phase III trials that are evaluating thera-peutic agents for intracerebral malignancies21,38–47,57 and degenerative disease.54–56 However, drug distribution in these trials has not been monitored. This lack of funda-mental information on drug distribution has the poten-tial to confound interpretation of these clinical studies, making it difficult to distinguish between lack of effec-tiveness due to delivery or therapeutic activity factors.
Fig. 4. Co-registered images showing optimal distribution of 123I-albumin after convection-enhanced delivery. (A) Single-photon emission computed tomography (SPECT) image of 123I-albumin dis-tribution co-registered with axial MR image for anterior right fron-tal catheter positioned below the resection cavity (patient 12). (B) SPECT image of 123I-albumin distribution co-registered with axial MR image for posterior right frontal catheter positioned behind the resection cavity. (C, D) Corresponding SPECT-derived isodose contours co-registered with axial T1-weighted MR images located at the tip of each catheter in the right frontal lobe of the brain. Iso-dose lines show the percent concentration of 123I-albumin relative to the infused concentration (0.25 mg/ml) such that at the 50% isodose line the concentration of albumin is 0.125 mg/ml and at the 10% isodose line the concentration of albumin is 0.025 mg/ml. (E, F) Oblique reconstructions of complete SPECT image showing areas covered and not covered by the infusion.
Table 4. Catheter infusion findingsa
Infusion Findings No. Infusions Percentage of Infusions
Leak into subarachnoid space 7/16 44%
Leak into ventricle 2/16 12%
Pooling in resection cavity or necrotic area 4/16 25%
Successful intraparenchymal infusion 3/16 19%
aA subset of eight patients was infused with 123I-labeled albumin to monitor drug distribution.
Fig. 5. Co-registered images showing ineffective distribution of 123I-albumin after convection-enhanced delivery: selected axial MR image (A) and coronal images (B, C) from three different patients showing single-photon emission computed tomography image of 123I-albumin distribution co-registered with MR images demon-strating leakage of infusate into the subarachnoid cerebrospinal fluid spaces over the superior hemispheric surface of frontopari-etal lobe of the brain (A–C) and along the tentorial surface of the occipital lobe (C).
Sampson et al.: Intracerebral infusion of an EGFR-targeted toxin
Neuro-oNcology • J U N E 2 0 0 8 327
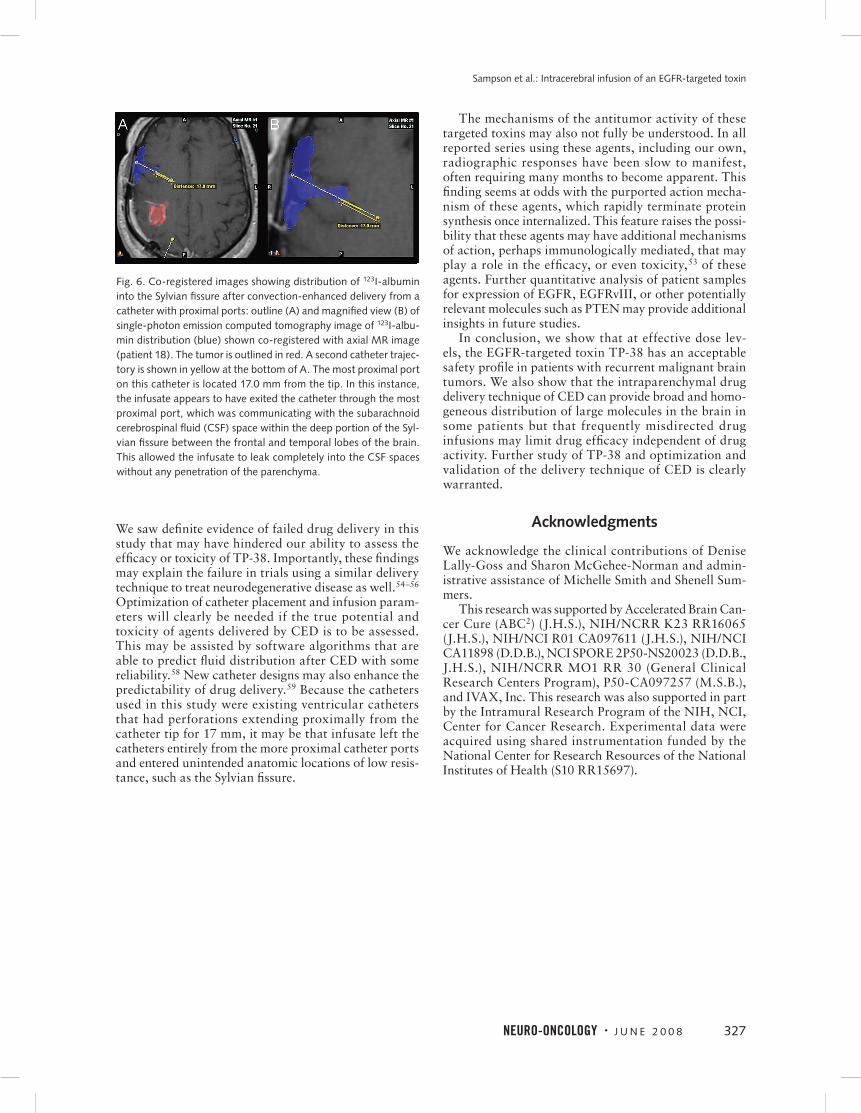
We saw definite evidence of failed drug delivery in this study that may have hindered our ability to assess the efficacy or toxicity of TP-38. Importantly, these findings may explain the failure in trials using a similar delivery technique to treat neurodegenerative disease as well.54–56 Optimization of catheter placement and infusion param-eters will clearly be needed if the true potential and toxicity of agents delivered by CED is to be assessed. This may be assisted by software algorithms that are able to predict fluid distribution after CED with some reliability.58 New catheter designs may also enhance the predictability of drug delivery.59 Because the catheters used in this study were existing ventricular catheters that had perforations extending proximally from the catheter tip for 17 mm, it may be that infusate left the catheters entirely from the more proximal catheter ports and entered unintended anatomic locations of low resis-tance, such as the Sylvian fissure.
The mechanisms of the antitumor activity of these targeted toxins may also not fully be understood. In all reported series using these agents, including our own, radiographic responses have been slow to manifest, often requiring many months to become apparent. This finding seems at odds with the purported action mecha-nism of these agents, which rapidly terminate protein synthesis once internalized. This feature raises the possi-bility that these agents may have additional mechanisms of action, perhaps immunologically mediated, that may play a role in the efficacy, or even toxicity,53 of these agents. Further quantitative analysis of patient samples for expression of EGFR, EGFRvIII, or other potentially relevant molecules such as PTEN may provide additional insights in future studies.
In conclusion, we show that at effective dose lev-els, the EGFR-targeted toxin TP-38 has an acceptable safety profile in patients with recurrent malignant brain tumors. We also show that the intraparenchymal drug delivery technique of CED can provide broad and homo-geneous distribution of large molecules in the brain in some patients but that frequently misdirected drug infusions may limit drug efficacy independent of drug activity. Further study of TP-38 and optimization and validation of the delivery technique of CED is clearly warranted.
Acknowledgments
We acknowledge the clinical contributions of Denise Lally-Goss and Sharon McGehee-Norman and admin-istrative assistance of Michelle Smith and Shenell Sum-mers.
This research was supported by Accelerated Brain Can-cer Cure (ABC2) (J.H.S.), NIH/NCRR K23 RR16065 (J.H.S.), NIH/NCI R01 CA097611 (J.H.S.), NIH/NCI CA11898 (D.D.B.), NCI SPORE 2P50-NS20023 (D.D.B., J.H.S.), NIH/NCRR MO1 RR 30 (General Clinical Research Centers Program), P50-CA097257 (M.S.B.), and IVAX, Inc. This research was also supported in part by the Intramural Research Program of the NIH, NCI, Center for Cancer Research. Experimental data were acquired using shared instrumentation funded by the National Center for Research Resources of the National Institutes of Health (S10 RR15697).
Fig. 6. Co-registered images showing distribution of 123I-albumin into the Sylvian fissure after convection-enhanced delivery from a catheter with proximal ports: outline (A) and magnified view (B) of single-photon emission computed tomography image of 123I-albu-min distribution (blue) shown co-registered with axial MR image (patient 18). The tumor is outlined in red. A second catheter trajec-tory is shown in yellow at the bottom of A. The most proximal port on this catheter is located 17.0 mm from the tip. In this instance, the infusate appears to have exited the catheter through the most proximal port, which was communicating with the subarachnoid cerebrospinal fluid (CSF) space within the deep portion of the Syl-vian fissure between the frontal and temporal lobes of the brain. This allowed the infusate to leak completely into the CSF spaces without any penetration of the parenchyma.
Sampson et al.: Intracerebral infusion of an EGFR-targeted toxin
328 Neuro-oNcology • J U N E 2 0 0 8
1. CBTRUS, Central Brain Tumor Registry of the United States. Statisti-
cal Report: Primary Brain Tumors in the United States, 1997–2001.
Chicago: CBTRUS; 2004.
2. Imperato JP, Paleologos NA, Vick NA. Effects of treatment on long-
term survivors with malignant astrocytomas. Ann Neurol. 1990;28:
818–822.
3. Pai LH, Pastan I. Immunotoxins and recombinant toxins. In: DeVita VT
Jr, Hellman S, Rosenberg SA, eds. Biologic Therapy of Cancer. Phila-
delphia: J.B. Lippincott; 1995:521–533.
4. Phillips PC, Levow C, Catterall M, et al. Transforming growth fac-
tor-alpha-Pseudomonas exotoxin fusion protein (TGF-alpha-PE38)
treatment of subcutaneous and intracranial human glioma and
medulloblastoma xenografts in athymic mice. Cancer Res. 1994;54:
1008–1015.
5. Pastan I. Targeted therapy of cancer with recombinant immunotoxins.
Biochimica et Biophysica Acta. 1997;1333:C1–C6.
6. Pastan I, FitzGerald D. Recombinant toxins for cancer treatment. Sci-
ence. 1991;254:1173–1177.
7. Kreitman RJ, Wilson WH, White JD, et al. Phase I trial of recombinant
immunotoxin anti-Tac(Fv)-PE38 (LMB-2) in patients with hemato-
logic malignancies. J Clin Oncol. 2000;18:1622–1636.
8. Kreitman RJ, Wilson WH, Bergeron K, et al. Efficacy of the anti-CD22
recombinant immunotoxin BL22 in chemotherapy-resistant hairy-cell
leukemia. N Engl J Med. 2001;345:241–247.
9. Frankel AE, McCubrey JA, Miller MS, et al. Diphtheria toxin fused to
human interleukin-3 is toxic to blasts from patients with myeloid leu-
kemias. Leukemia. 2000;14:576–585.
10. Frankel AE, Kreitman RJ, Sausville EA. Targeted toxins. Clin Cancer
Res. 2000;6:326–334.
11. Olsen E, Duvic M, Frankel A, et al. Pivotal phase III trial of two dose
levels of denileukin diftitox for the treatment of cutaneous T-cell lym-
phoma. J Clin Oncol. 2001;19:376–388.
12. Jain RK. Transport of molecules in the tumor interstitium: a review.
Cancer Res. 1987;47:3039–3051.
13. Jain RK. Vascular and interstitial barriers to delivery of therapeutic
agents in tumors. Cancer Metastasis Rev. 1990;9:253–266.
14. Jain RK. Tumor physiology and antibody delivery. Front Radiat Ther
Oncol. 1990;24:32–46.
15. Jain RK. Physiological barriers to delivery of monoclonal antibodies
and other macromolecules in tumors. Cancer Res. 1990;50:1.
16. Jain RK. Transport of molecules across tumor vasculature. Cancer
Metastasis Rev. 1987;6:559–593.
17. Groothuis DR. The blood-brain and blood-tumor barriers: a review
of strategies for increasing drug delivery. Neuro-Oncology. 2000;2:
45–59.
18. Zalutsky MR, Moseley RP, Coakham HB, Coleman RE, Bigner DD.
Pharmacokinetics and tumor localization of 131I-labeled anti-tenascin
monoclonal antibody 81C6 in patients with gliomas and other intra-
cranial malignancies. Cancer Res. 1989;49:2807–2813.
19. Grossi PM, Ochiai H, Archer GE, et al. Efficacy of intracerebral micro-
infusion of trastuzumab in an athymic rat model of intracerebral met-
astatic breast cancer. Clin Cancer Res. 2003;9:5514–5520.
20. Laske DW, Morrison PF, Lieberman DM, et al. Chronic interstitial infu-
sion of protein to primate brain: determination of drug distribution
and clearance with single-photon emission computerized tomography
imaging. J Neurosurg. 1997;87:586–594.
References
21. Laske DW, Youle RJ, Oldfield EH. Tumor regression with regional dis-
tribution of the targeted toxin TF-CRM107 in patients with malignant
brain tumors. Nat Med. 1997;3:1362–1368.
22. Lieberman DM, Laske DW, Morrison PF, Bankiewicz KS, Oldfield EH.
Convection-enhanced distribution of large molecules in gray matter
during interstitial drug infusion. J Neurosurg. 1995;82:1021–1029.
23. Morrison PF, Laske DW, Bobo H, Oldfield EH, Dedrick RL. High-flow
microinfusion: tissue penetration and pharmacodynamics. Am J Phys-
iol. 1994;266(1 pt 2):R292–R305.
24. Hamilton JF, Morrison PF, Chen MY, et al. Heparin coinfusion during
convection-enhanced delivery (CED) increases the distribution of the
glial-derived neurotrophic factor (GDNF) ligand family in rat striatum
and enhances the pharmacological activity of neurturin. Exp Neurol.
2001;168:155–161.
25. Morrison PF, Chen MY, Chadwick RS, Lonser RR, Oldfield EH. Focal
delivery during direct infusion to brain: role of flow rate, catheter
diameter, and tissue mechanics. Am J Physiol. 1999;277(4 pt 2):
R1218–R1229.
26. Bobo RH, Laske DW, Akbasak A, et al. Convection-enhanced delivery
of macromolecules in the brain. Proc Natl Acad Sci U S A. 1994;91:
2076–2080.
27. Laske DW, Ilercil O, Akbasak A, Youle RJ, Oldfield EH. Efficacy of
direct intratumoral therapy with targeted protein toxins for solid
human gliomas in nude mice. J Neurosurg. 1994;80:520–526.
28. Heimberger AB, Archer GE, McLendon RE, et al. Temozolomide deliv-
ered by intracerebral microinfusion is safe and efficacious against
malignant gliomas in rats. Clin Cancer Res. 2000;6:4148–4153.
29. Sanftner LM, Sommer JM, Suzuki BM, et al. AAV2-mediated gene
delivery to monkey putamen: evaluation of an infusion device and
delivery parameters. Exp Neurol. 2005;194:476–483.
30. Saito R, Bringas JR, Panner A, et al. Convection-enhanced delivery of
tumor necrosis factor-related apoptosis-inducing ligand with systemic
administration of temozolomide prolongs survival in an intracranial
glioblastoma xenograft model. Cancer Res. 2004;64:6858–6862.
31. Saito R, Bringas JR, McKnight TR, et al. Distribution of liposomes
into brain and rat brain tumor models by convection-enhanced
delivery monitored with magnetic resonance imaging. Cancer Res.
2004;64:2572–2579.
32. Mamot C, Nguyen JB, Pourdehnad M, et al. Extensive distribution of
liposomes in rodent brains and brain tumors following convection-
enhanced delivery. J Neurooncol. 2004;68:1–9.
33. Cunningham J, Oiwa Y, Nagy D, et al. Distribution of AAV-TK fol-
lowing intracranial convection-enhanced delivery into rats. Cell Trans-
plant. 2000;9:585–594.
34. Kawakami K, Kawakami M, Kioi M, Husain SR, Puri RK. Distribu-
tion kinetics of targeted cytotoxin in glioma by bolus or convection-
enhanced delivery in a murine model. J Neurosurg. 2004;101:1004–
1011.
35. Degen JW, Walbridge S, Vortmeyer AO, Oldfield EH, Lonser RR.
Safety and efficacy of convection-enhanced delivery of gemcitabine
or carboplatin in a malignant glioma model in rats. J Neurosurg.
2003;99:893–898.
36. Groothuis DR, Ward S, Itskovich AC, et al. Comparison of 14C-sucrose
delivery to the brain by intravenous, intraventricular, and convection-
enhanced intracerebral infusion. J Neurosurg. 1999;90:321–331.
37. Puri RK, Hoon DS, Leland P, et al. Preclinical development of a recom-
binant toxin containing circularly permuted interleukin 4 and trun-
Sampson et al.: Intracerebral infusion of an EGFR-targeted toxin
Neuro-oNcology • J U N E 2 0 0 8 329
cated Pseudomonas exotoxin for therapy of malignant astrocytoma.
Cancer Res. 1996;56:5631–5637.
38. Patel SJ, Shapiro WR, Laske DW, et al. Safety and feasibility of con-
vection-enhanced delivery of Cotara for the treatment of malignant
glioma: Initial experience in 51 patients. Neurosurgery. 2005;56 :
1243–1253.
39. Rainov NG, Heidecke V. Long term survival in a patient with recur-
rent malignant glioma treated with intratumoral infusion of an IL4-
targeted toxin (NBI-3001). J Neurooncol. 2004;66:197–201.
40. Kunwar S. Convection enhanced delivery of IL13-PE38QQR for
treatment of recurrent malignant glioma: presentation of interim
findings from ongoing phase 1 studies. Acta Neurochir Suppl.
2003;88:105–111.
41. Weber FW, Floeth F, Asher A, et al. Local convection enhanced
delivery of IL4-Pseudomonas exotoxin (NBI-3001) for treatment
of patients with recurrent malignant glioma. Acta Neurochir Suppl.
2003;88:93–103.
42. Weber F, Asher A, Bucholz R, et al. Safety, tolerability, and tumor
response of IL4-Pseudomonas exotoxin (NBI-3001) in patients with
recurrent malignant glioma. J Neurooncol. 2003;64:125–137.
43. Rand RW, Kreitman RJ, Patronas N, et al. Intratumoral administra-
tion of recombinant circularly permuted interleukin-4-Pseudomonas
exotoxin in patients with high-grade glioma. Clin Cancer Res.
2000;6:2157–2165.
44. Oldfield EH, Youle RJ. Immunotoxins for brain tumor therapy. Curr
Top Microbiol Immunol. 1998;234:97–114.
45. Lidar Z, Mardor Y, Jonas T, et al. Convection-enhanced delivery of
paclitaxel for the treatment of recurrent malignant glioma: a phase I/
II clinical study. J Neurosurg. 2004;100:472–479.
46. Sampson JH, Reardon DA, Friedman AH, et al. Sustained radiographic
and clinical response in patient with bifrontal recurrent glioblastoma
multiforme with intracerebral infusion of the recombinant targeted
toxin TP-38: case study. Neuro-Oncology. 2005;7:90–96.
47. Sampson JH, Reardon DA, Akabani G, et al. A phase I study of intra-
tumoral infusion of a recombinant chimeric protein composed of
transforming growth factor (TGF)-alpha and a mutated form of the
Pseudomonas exotoxin (TP-38) for the treatment of malignant brain
tumors [abstract]. Proc Am Assoc Cancer Res. 2002;43:746.
48. Torp SH, Helseth E, Ryan L, et al. Expression of the epidermal
growth factor receptor gene in human brain metastases. APMIS.
1992;100:713–719.
49. Libermann TA, Razon N, Bartal AD, et al. Expression of epidermal
growth factor receptors in human brain tumors. Cancer Res. 1984;44:
753–760.
50. Torp SH, Helseth E, Dalen A, Unsgaard G. Epidermal growth factor
receptor expression in human gliomas. Cancer Immunol Immunother.
1991;33:61–64.
51. Macdonald DR, Cascino TL, Schold SC Jr, Cairncross JG. Response
criteria for phase II studies of supratentorial malignant glioma. J Clin
Oncol. 1990;8:1277–1280.
52. Murad G, Walbridge S, Morrison PF, et al. Real-time, image-guided,
convection-enhanced delivery of interleukin 13 bound to pseudo-
monas exotoxin. Clin Cancer Res. 2006;12:3145–3151.
53. Parney IF, Kunwar S, McDermott M, et al. Neuroradiographic changes
following convection-enhanced delivery of the recombinant cytotoxin
interleukin 13-PE38QQR for recurrent malignant glioma. J Neurosurg.
2005;102:267–275.
54. Gill SS, Patel NK, Hotton GR, et al. Direct brain infusion of glial cell
line-derived neurotrophic factor in Parkinson disease. Nat Med.
2003;9:589–595.
55. Love S, Plaha P, Patel NK, et al. Glial cell line-derived neurotrophic
factor induces neuronal sprouting in human brain. Nat Med. 2005;11:
703–704.
56. Patel NK, Bunnage M, Plaha P, et al. Intraputamenal infusion of glial
cell line-derived neurotrophic factor in PD: a two-year outcome study.
Ann Neurol. 2005;57:298–302.
57. Sampson JH, Akabani G, Archer GE, et al. Progress report of a Phase
I study of the intracerebral microinfusion of a recombinant chime-
ric protein composed of transforming growth factor (TGF)-alpha
and a mutated form of the Pseudomonas exotoxin termed PE-38
(TP-38) for the treatment of malignant brain tumors. J Neurooncol.
2003;65:27–35.
58. Sampson JH, Raghavan R, Brady ML, et al. Clinical utility of a patient-
specific algorithm for simulating intracerebal drug infusions. Neuro-
Oncology. 2007;9:343–353.
59. Krauze MT, Saito R, Noble C, et al. Reflux-free cannula for convec-
tion-enhanced high-speed delivery of therapeutic agents. J Neuro-
surg. 2005;103:923–929.
Copyright © 2022 FDOKUMEN