Emergency Department Control of Blood Pressure in Intracerebral Hemorrhage
7
doi:10.1016/j.jemermed.2009.02.001 Original Contributions EMERGENCY DEPARTMENT CONTROL OF BLOOD PRESSURE IN INTRACEREBRAL HEMORRHAGE Samantha K. Honner, MD,* Amandeep Singh, MD,* Paul T. Cheung, MPH,* Harrison J. Alter, MD,* Claudine G. Dutaret, MD,† Atul K. Patel, MD,‡ and Ananth Acharya, MD† *Department of Emergency Medicine, †Division of Neurology, Department of Medicine, and ‡Division of Neurosurgery, Department of Surgery, Alameda County Medical Center, Oakland, California Reprint Address: Amandeep Singh, MD, Department of Emergency Medicine, Alameda County Medical Center, 1411 East 31 st Street, Oakland, CA 94611 e Abstract—Background: Early treatment of elevated blood pressure (BP) in patients presenting with spontane- ous intracerebral hemorrhage (ICH) may decrease hema- toma enlargement and lead to better neurologic outcome. Study Objective: To determine whether early BP control in patients with spontaneous ICH is both feasible and tol- erated when initiated in the Emergency Department (ED). Methods: A single-center, prospective observa- tional study in patients with spontaneous ICH was per- formed to evaluate a protocol to lower, and maintain for 24 h, the mean arterial pressure (MAP) to a range of 100–110 mm Hg within 120 min of arrival to the ED. An additional goal of placing a functional arterial line within 90 min was specified in our protocol. Hematoma volume, neurologic disability, adverse events, and in-hospital mortality were recorded. Results: A total of 22 patients were enrolled over a 1-year study period. The average time to achieve our target MAP after implementation of our protocol was 123 min (range 19 –297 min). The av- erage time to arterial line placement was 84 min (range 36 –160 min). Overall, 77% of the patients tolerated the 24-h protocol. The in-hospital mortality rate in this group of patients was 41%. Conclusions: Adopting a protocol to reduce and maintain the MAP to a target of 100 –110 mm Hg within 120 min of ED arrival was safe and well tolerated in patients presenting with spontane- ous ICH. If future trials demonstrate a clinical benefit of early BP control in spontaneous ICH, EDs should imple- ment similar protocols. © 2011 Published by Elsevier Inc. e Keywords—intracerebral hemorrhage; hypertension; therapy INTRODUCTION Spontaneous intracerebral hemorrhage (ICH) is seen in more than 67,000 patients per year in the United States and results in unacceptably high mortality and neuro- logic morbidity. The 30-day reported mortality rate of these patients is between 35% and 52%, with half of all deaths occurring within the first 2 days. The majority of surviving patients are left with severe disability, with only 20% of individuals returning to a level of functional independence at 6 months (1). Contemporary theory regarding the pathogenesis of the initiation and propagation of ICH focuses on the role of intravascular fibrinoid necrosis creating “vulnerable” rupture sites at or near the bifurcation of susceptible intracranial arterioles. Chronic hypertension further re- duces vascular compliance and increases the likelihood of spontaneous rupture (2). Persistently elevated blood pressure (BP) is thought to contribute to the propaga- tion of ICH through early hematoma expansion and rebleeding. Early hematoma growth is seen in nearly one-third of all patients, most commonly in the first several hours from symptom onset, and is a poor prognostic indicator (3–9). RECEIVED: 26 August 2008; FINAL SUBMISSION RECEIVED: 7 November 2008; ACCEPTED: 5 February 2009 The Journal of Emergency Medicine, Vol. 41, No. 4, pp. 355–361, 2011 Copyright © 2011 Published by Elsevier Inc. Printed in the USA 0736-4679/$–see front matter 355
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Emergency Department Control of Blood Pressure in Intracerebral Hemorrhage

A
The Journal of Emergency Medicine, Vol. 41, No. 4, pp. 355–361, 2011Copyright © 2011 Published by Elsevier Inc.
Printed in the USA0736-4679/$–see front matter
doi:10.1016/j.jemermed.2009.02.001
OriginalContributions
EMERGENCY DEPARTMENT CONTROL OF BLOOD PRESSURE ININTRACEREBRAL HEMORRHAGE
Samantha K. Honner, MD,* Amandeep Singh, MD,* Paul T. Cheung, MPH,* Harrison J. Alter, MD,*Claudine G. Dutaret, MD,† Atul K. Patel, MD,‡ and Ananth Acharya, MD†
*Department of Emergency Medicine, †Division of Neurology, Department of Medicine, and ‡Division of Neurosurgery, Department ofSurgery, Alameda County Medical Center, Oakland, California
Reprint Address: Amandeep Singh, MD, Department of Emergency Medicine, Alameda County Medical Center, 1411 East 31st Street,
Oakland, CA 94611e Abstract—Background: Early treatment of elevatedblood pressure (BP) in patients presenting with spontane-ous intracerebral hemorrhage (ICH) may decrease hema-toma enlargement and lead to better neurologic outcome.Study Objective: To determine whether early BP control inpatients with spontaneous ICH is both feasible and tol-erated when initiated in the Emergency Department(ED). Methods: A single-center, prospective observa-tional study in patients with spontaneous ICH was per-formed to evaluate a protocol to lower, and maintain for24 h, the mean arterial pressure (MAP) to a range of100 –110 mm Hg within 120 min of arrival to the ED. Anadditional goal of placing a functional arterial line within90 min was specified in our protocol. Hematoma volume,neurologic disability, adverse events, and in-hospitalmortality were recorded. Results: A total of 22 patientswere enrolled over a 1-year study period. The averagetime to achieve our target MAP after implementation ofour protocol was 123 min (range 19 –297 min). The av-erage time to arterial line placement was 84 min (range36 –160 min). Overall, 77% of the patients tolerated the24-h protocol. The in-hospital mortality rate in thisgroup of patients was 41%. Conclusions: Adopting aprotocol to reduce and maintain the MAP to a target of100 –110 mm Hg within 120 min of ED arrival was safeand well tolerated in patients presenting with spontane-ous ICH. If future trials demonstrate a clinical benefit ofearly BP control in spontaneous ICH, EDs should imple-ment similar protocols. © 2011 Published by ElsevierInc.
RECEIVED: 26 August 2008; FINAL SUBMISSION RECEIVED: 7
CCEPTED: 5 February 2009355
e Keywords—intracerebral hemorrhage; hypertension;therapy
INTRODUCTION
Spontaneous intracerebral hemorrhage (ICH) is seen inmore than 67,000 patients per year in the United Statesand results in unacceptably high mortality and neuro-logic morbidity. The 30-day reported mortality rate ofthese patients is between 35% and 52%, with half of alldeaths occurring within the first 2 days. The majority ofsurviving patients are left with severe disability, withonly 20% of individuals returning to a level of functionalindependence at 6 months (1).
Contemporary theory regarding the pathogenesis ofthe initiation and propagation of ICH focuses on the roleof intravascular fibrinoid necrosis creating “vulnerable”rupture sites at or near the bifurcation of susceptibleintracranial arterioles. Chronic hypertension further re-duces vascular compliance and increases the likelihoodof spontaneous rupture (2). Persistently elevated bloodpressure (BP) is thought to contribute to the propaga-tion of ICH through early hematoma expansion andrebleeding. Early hematoma growth is seen in nearlyone-third of all patients, most commonly in the firstseveral hours from symptom onset, and is a poorprognostic indicator (3–9).
mber 2008;
Nove
E
m
ssapww
S
OthwtWrtl
dtmph
tdCn5
M
WTpndtSStsrcsse
356 S. K. Honner et al.
Despite increasing data suggesting that elevated BP inpatients with ICH is associated with early hematomagrowth, poor neurologic outcome, and death, there are noevidence-based guidelines supporting a specific treat-ment algorithm for managing the elevated BP in thesepatients. The 2007 American Stroke Association/AmericanHeart Association guidelines on the management of ICHgive a class IIb recommendation (i.e., usefulness/efficacyless well established by evidence or opinion) with a levelof evidence C (i.e., consensus opinion of experts) to“consider a modest reduction of blood pressure” if themean arterial pressure (MAP) is elevated � 130 mm Hgand to “consider aggressive reduction of blood pressure”if the MAP is � 150 mm Hg (1).
The goal of our study was to assess the feasibility andtolerability of early BP reduction in patients with ele-vated BP and spontaneous ICH in an Emergency Depart-ment (ED) setting. Secondary goals evaluated the fol-lowing outcomes: change in hematoma volume at 24 h,in-hospital mortality, and functional neurologic outcomeat 24 h and 3 months.
MATERIALS AND METHODS
Study Design
This was a prospective observational study conductedat a single hospital from January 15, 2007 to January15, 2008 using a multidisciplinary protocol developedjointly by the Department of Emergency Medicine andthe Divisions of Neurology, Neurosurgery, and CriticalCare. The study was approved by the hospital institu-tional review board committee. Informed consent waswaived, as this was a feasibility and safety study regard-ing an intervention that was routinely recommended bythe Divisions of Neurology and Neurosurgery at ourhospital.
Study Setting and Patients
Alameda County Medical Center, Highland Campus inOakland, California, is an urban teaching hospital withan affiliated emergency medicine residency-training pro-gram that treats approximately 72,000 patients per yearin the ED.
All adult patients with a spontaneous ICH, determinedby non-contrast head computed tomography (CT) scan,who presented during the study period and who had atriage MAP � 120 mm Hg were eligible for inclusion.
xclusion criteria included age � 18 years, pregnancy,coagulopathy (bleeding disorder, low-molecular weight
heparin or warfarin therapy, platelet count � 50,000/ nm3, or international normalized ratio � 2.0), pre-existingneurologic disability (e.g., requiring assistance for activ-ities of daily living), symptom onset � 48 h before beingeen in the ED, or a history (e.g., trauma) or CT scanuggesting secondary ICH (e.g., vascular malformation,neurysm, tumor). Patients who had a head CT scanerformed more than 90 min after ED arrival or whoere transferred from another facility to our hospitalere also excluded.
tudy Protocol
ur management protocol specified that patients judgedo be eligible by the treating emergency physician shouldave their MAP lowered to a target of 100–110 mm Hgithin 120 min of presentation to the ED and maintain
his target MAP at this level for a minimum of 24 h.e also specified a goal of placing a functional arte-
ial line within 90 min of patient arrival. Antihyper-ensive treatment before the placement of the arterialine was recommended.
The choice of antihypertensive agent was left to theiscretion of the treating emergency physician. Doses forhe hospital-preferred hypertensive medications (es-olol, fenoldapam, labetalol, nicardipine) and the hos-
ital protocols for use of recombinant factor VIIa anduman coagulation factor IX complex were provided.
All patients were monitored in a critical care room inhe ED and admitted to the intensive care unit for car-iovascular and neurologic monitoring. A repeat headT scan was obtained at 24 h, or sooner in cases ofeurologic deterioration. CT scans were performed on a12 � 512 matrix with a 5-mm slice thickness.
easurements
e collected data using standardized collection forms.he ED data were collected by the treating emergencyhysician or, if present, the consulting neurologist oreurosurgeon. The initial data collection included patientemographic information, past medical history, risk fac-ors for ICH, time of symptom onset, Glasgow Comacale (GCS) score, and National Institute of Healthtroke Scale (NIHSS) score. Time to obtain target MAP,
ime to functional arterial line placement, antihyperten-ive agent(s) used, and 24-h complications were alsoecorded. The consulting neurologist or neurosurgeonollected the inpatient data. This included antihyperten-ive agent(s) used or discontinued, GCS and NIHSScores at 24 h and discharge, and in-hospital unexpectedvents. After the enrollment period, a board-certified
eurologist, adept in the ability to measure intracranial
ED Control of BP in Intracerebral Hemorrhage 357
hematoma volume, interpreted the initial and subsequenthead CT scans. One of the authors (SH) contacted eachpatient at 3 months to determine the modified Rankinscore (mRS).
Outcomes
The primary goal of our study was to address the feasi-bility and tolerability of early aggressive BP manage-ment for patients with spontaneous ICH who present tothe ED. Secondary goals evaluated the following out-comes: change in hematoma volume at 24 h, in-hospitalmortality, and functional neurologic outcome at 24 h and3 months.
Feasibility was evaluated through the ability to obtainthe target MAP of 100–110 mm Hg within 120 min fromED presentation and to maintain the target MAP at 100–110 mm Hg for 24 h. Patients that did not incur any adverseeffects requiring termination of therapy within the first 24 hwere considered to have tolerated the protocol.
Hematoma volume was calculated using the maxi-mum CT diameter measurements inserted into this for-mula: [0.5 * (length [cm]) * (width [cm]) * (height[cm])]. This method has been found to correlate highlywith volumes calculated by planimetric methods for allhemorrhagic locations (10). The change in hematomasize was calculated as a percentage using the formula:[(final volume � initial volume)/initial volume] * 100.Significant hematoma expansion was defined as an in-crease in the volume of intraparenchymal hemorrhage bymore than 33% on the repeat head CT scan compared tothe baseline CT scan (11).
Neurologic outcomes at 24 h and hospital dischargewere evaluated using the GCS and NIHSS scales (12,13).Functional neurologic outcome at 3 months was assessedwith the mRS (14).
Data Analysis
Descriptive statistics were derived using SPSS (version11; SPSS, Inc., Chicago, IL). Statistical significance wasset at a level of 0.05 and determined using the Student’st-test for paired comparisons.
RESULTS
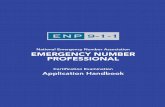
During the 1-year study period, a total of 60 patients withICH were screened for enrollment. After exclusion cri-teria were applied, 23 patients were eligible for patientenrollment (Figure 1). Twenty-two of these patients were
successfully enrolled and comprise the study population.Clinical and demographic information regarding thestudy population is listed in Table 1. Patients ranged inage from 33 to 83 years (mean age 54.7 years). Half of
Figure 1. Patient enrollment.
Table 1. Clinical and Demographic Characteristics (n � 22)
Characteristics n (%)
Age in years, Mean (SD) 54.7 (11.3)Female gender 11 (50.0)Race
African-American 10 (45.5)Hispanic 6 (27.3)Asian 5 (22.7)Caucasian 1 (4.5)
Past medical historyHypertension 17 (77.3)Cocaine* 9 (40.9)Diabetes 6 (27.3)Prior stroke 5 (22.7)Cardiac disease† 3 (13.6)Tobacco 2 (9.1)Hyperlipidemia 1 (4.5)
Hematoma location‡Basal ganglia 8 (33.3)Thalamus 8 (33.3)Pons/midbrain 4 (16.7)Lobar 3 (12.5)Cerebellum 1 (4.2)
* Per history or urine toxicology.† Prior myocardial infarction or congestive heart failure.
‡ Two patients had two hematomas giving a total number of 24hematomas.
c
pm4o
1sspts
N
*†‡M
N
*sINm
358 S. K. Honner et al.
the enrolled patients were female. A history of hyperten-sion was seen in over 75% of enrolled patients, with 41%identifying positive for cocaine use. Two-thirds of theintracranial hemorrhages were located in the basal gan-glia and thalamus. There was CT evidence of hemor-rhage extension into the ventricles in 11 cases (50%), andhydrocephalus present in 6 cases (27%).
Patients arrived, on average, 50 min (range 23–78min) from the time of symptom onset. Nearly 80% of thepatients received a CT scan within 60 min of arrival tothe ED. The median initial intracranial hematoma vol-ume was 17.9 cm3 (interquartile ratio [IQR] 10.5–29.6m3). Emergent ventriculostomy in the first 24 h was
performed in 1 patient. Three patients received factorVIIa in the ED.
The average time from arrival in the ED to targetMAP was 123 min (range 19–297 min) (Table 2). Thetarget of reducing the MAP to a level between 100 and110 mm Hg within 120 min of arrival to the ED wasobtained in 11 of the 22 cases (50%). Seventeen patients(77%) achieved the MAP target within 170 min, and 20patients (91%) achieved the target within 200 min. Four-teen of the 22 patients (68%) required multiple agents toreach the target MAP. The most commonly used regimenincluded an initial bolus therapy with labetalol followedby a nicardipine drip. A total of 16 patients receivedcontinuous nicardipine (73%) and 12 patients receivedintermittent or continuous labetalol (55%). One patienthad spontaneous regression of their MAP to the targetrange and did not require any antihypertensive therapy.
The mean time to functional arterial line placement
Table 2. Outcome Data (n � 22)
Emergency Department Data Mean (SD)Initial MAP in mm Hg 152.4 (24.9)Time from symptoms to arrival*† 49.6 (29.7)Time from ED arrival to CT scan† 41.1 (19.3)Time from arrival to arterial line† 84.7 (36.7)Time from arrival to target MAP† 123.4 (72.9)
Median (IQR)Initial hematoma volume in cm3 17.9 (10.5–29.6)Initial GCS 11 (7–15)Initial NIHSS 19 (15–26)eurologic outcome data‡24-h GCS 10 (3–14)24-h NIHSS 26 (13–38)3-month mRS 5 (3–6)
Unknown for 5 patients.Times are given in minutes.Data available for 21 patients.AP � mean arterial pressure; ED � Emergency Department;
CT � computed tomography; GCS � Glasgow Coma Scalescore; NIHSS � National Institute of Health Stroke Scale score;mRS � modified Rankin score.
was 84 min (range 36–160 min). The goal of placing a t
functional arterial line within 90 min of arrival wasobtained in 12 of the 22 cases (55%). Eighteen patients(82%) received a functional arterial line within 110 min.Reasons for delay in achieving our target MAP andarterial line included: difficult intravenous (i.v.) access (4patients), resistant hypertension (4 patients), difficulty inobtaining a definitive airway (3 patients), pharmacy de-lay in delivering antihypertensive medications (3 pa-tients), and a delay in obtaining the CT scan (2 patients).
The median initial hematoma volume, GCS and NIHSSscores, and 24-h neurological outcomes are outlined inTable 2. The median 3-month mRS was 5 (IQR 3–6).
The median initial hematoma volume of survivingpatients was 11.0 cm3 (IQR 7.5–19 cm3) compared to31.7 cm3 (IQR 22.3–40.5 cm3) in non-survivors (p �0.02). Surviving patients had a lower percentage ofintraventricular extension (38%) compared with non-survivors (67%). The median initial GCS of survivingpatients was 15 (IQR 11–15), compared to 6 (IQR 4–8)in non-survivors (p � 0.00).
The median 24-h repeat hematoma volume for survi-vors was 11.5 cm3 (IQR 9.1–16 cm3) (p � 0.35 com-ared to initial hematoma volume) (Table 3). The 24-hedian proportional hematoma growth in survivors was
.5%. Significant 24-h intracranial hematoma expansionccurred in 2 patients (17%).
Our protocol for BP management was well tolerated in7 of the 22 cases (77%). Five patients required vasopres-ors in the first 24 h for hypotension after the antihyperten-ive therapy was weaned off (Table 4). Two additionalatients experienced in-hospital adverse events. In one pa-ient, pneumonia was recognized on hospital day 2. In theecond patient, hydrocephalus requiring a ventriculostomy,
Table 3. Radiologic and Neurologic Data of Survivors(n � 13)
Median (IQR)
Radiologic data*Initial hematoma volume in cm3 11.0 (7.5–19)Repeat hematoma volume in cm3 11.5 (9.1–16)eurologic dataInitial GCS 15 (11–15)Initial NIHSS 16 (10–18)24-hour GCS 14 (12–15)24-hour NIHSS 13 (12–21)Discharge GCS 15 (15)Discharge NIHSS 10 (6–11)3-month mRS 3 (2–4)
One survivor did not have a repeat computed tomographycan.QR � interquartile range; GCS � Glasgow Coma Scale score;IHSS � National Institute of Health Stroke Scale score; mRS �odified Rankin score.
ransient renal insufficiency, and an ileus developed during

*†‡B
ED Control of BP in Intracerebral Hemorrhage 359
the first week of hospitalization. Both of these patientssurvived.
Nine patients died during hospitalization (in-hospitalmortality 41%), with a majority occurring within 48 h ofpresentation. A tenth patient died 2 months after studyenrollment.
DISCUSSION
In 2007, the American Stroke Association/AmericanHeart Association updated their recommendations forBP control in patients with spontaneous ICH (1). A classIIb recommendation, based mainly on consensus opin-ion, concludes that “aggressive reduction” of the BP withcontinuous i.v. antihypertensive infusion should be con-sidered in patients with MAP � 150 mm Hg and that a“modest reduction” of the BP with continuous or inter-mittent i.v. antihypertensive medication should be con-sidered in patients with MAP � 130 mm Hg. Theserecommendations are based on a handful of studies thathave shown a correlation between elevated initial BP inICH and early intracranial hematoma expansion, neuro-logic morbidity, and mortality (3–9). Unlike acute isch-emic stroke, pharmacologic regulation of MAP does notadversely affect regional cerebral blood flow or intracra-nial pressure in experimental models (15,16).
The recent results of the INTERACT (Intensive BloodPressure Reduction in Acute Cerebral Hemorrhage) trialsupport the notion that early BP control in patients withelevated BP and spontaneous ICH is warranted (17). Inthis prospective multicenter trial, patients were enrolledwithin 6 h of symptom onset and randomized to receiveearly intensive lowering of BP (target systolic BP 140mm Hg) vs. standard care (target systolic BP 180 mmHg). Patients in the intensive lowering of BP group had
Table 4. Timing of BP Control and Pressors forNon-Survivors (n � 9)
Case Goal MAP*Vasopressors in the First
24 h (Time of Onset)†Time ofDeath†
1 1:50 No 262 1:40 No 605‡ 0:36 Yes (2) 246 2:50 Yes (16) 21
12 2:24 Yes (14) 2513 4:57 No 2917 3:07 No 10321 0:19 Yes (14; stopped at 19) 4422 1:34 Yes (20) 36
Time in hours:minutes from ED presentation.Time in hours from ED presentation.This patient did not receive any antihypertensive agents.P � blood pressure; MAP � mean arterial pressure.
smaller volume of hematoma growth compared to pa-
tients receiving usual care (13.7% mean proportionalhematoma growth in intensive care group compared to36.3% in the standard care group; p � 0.04) at 24 h. Anon-significant trend favoring mortality was seen in theintensive care group (overall mortality 10% vs. 13% inthe standard care group).
Several additional studies support the notion of earlyBP management in the treatment of spontaneous ICH inthe ED. A retrospective chart review by Burke et al.found that patients with spontaneous ICH treated withantihypertensives in the first 6 h from initial presentationhad a significant reduction in mortality compared topatients not treated in this time frame (18). A study byQureshi et al. observed that patients with spontaneousICH treated within 6 h of symptom onset were morelikely to be functionally independent as judged by themRS, compared to patients who were treated between 6and 24 h (19).
In our prospective series of 22 patients with sponta-neous ICH presenting to a single institution, an EDprotocol with aims to place an arterial line within 90 minof presentation and to reduce the MAP to 100–110 mmHg within 120 min of presentation was feasible in only50% of patients. The average time from patient arrival inthe ED to successful arterial line placement and targetMAP was 84 min and 123 min, respectively. Althoughonly 50% of our patients achieved a target MAP of100–110 mm Hg using our pre-specified goal of 120min, over 90% of our patients reached this goal with anadditional 80 min of therapy. A prior study by Koch et al.has shown that the MAP can be safely lowered to a levelof � 110 mm Hg in patients with spontaneous ICH (20).The average time to target MAP in our study comparesfavorably to this study (123 min � 73 min compared to163 min � 164 min in the Koch et al. study) (20). Themajority of delays to achieving our target MAP andfunctional arterial line were due to delays in obtainingi.v. access, definitive airway control, and head CT scan,as well as delays in pharmacy delivery of antihyperten-sive medication.
Our protocol was tolerated in over three-quarters ofour patients per our study definition, as 5 patients re-quired vasopressor therapy in the first 24 h. In all but oneof these patients, vasopressors were started more than14 h after initial ED presentation, long after the goalMAP was obtained. The one patient who required vaso-pressors within 2 h of presentation never received anyantihypertensive medication (Table 4). Although all ofthese patients died, their mortality is unlikely to berelated to rapid blood pressure lowering in the ED. It ismore likely to be related to their larger hematoma vol-umes, higher rates of intraventricular extension, andlower GCS scores than the survivors, as these are the
most important predictors of mortality from ICH (21).
gtso3
L
GcrctHEsp
paso2t(
gssrnrs
OEauacuHBr
bcc
360 S. K. Honner et al.
The observed mortality of 41%, with most deaths occur-ring the first 2 days, is consistent with prior studies(1,2,6,18,19,22).
The 24-h median proportional hematoma growth inpatients that survived was 4.5%. This impressive result issimilar to results seen with intensive BP reduction
roup from the INTERACT trial (13.7% mean propor-ional hematoma growth compared to 36.3% in thetandard care group, p � 0.04) (17). Neurologicalutcome in this group was also favorable, with a-month mRS of 3 (IQR 2– 4).
imitations
iven the observational nature of our study, we cannotonclude that aggressive BP control in the ED leads toeduced hematoma growth or improved clinical out-omes. Our design was to assess the feasibility andolerability of achieving a MAP target of 100–110 mmg in patients with spontaneous ICH who present to theD with a MAP � 120 mm Hg. To this end, we havehown that these goals are possible in over 90% ofatients in under 3½ hours.
Although we successfully enrolled � 95% of eligibleatients who presented in a 1-year study period, we wereble to test our hypothesis in only 22 patients. Thisample size of 22 patients is slightly smaller than thosef two prospective studies by Qureshi et al. that enrolled7 and 35 patients, respectively, and significantly smallerhan the 404 patients enrolled in the INTERACT trail17,19,22).
Other limitations include interobserver bias, as emer-ency physicians obtained the initial GCS and NIHSScores, and a neurologist or neurosurgeon obtained theubsequent scores. There was no assessment of inter-ater reliability between the different physicians. Fi-ally, the physicians collecting the data and the neu-ologist reading the CT scan were not blinded to thetudy objectives.
CONCLUSION
ur study shows that a protocol of early BP control in theD for patients with spontaneous ICH is both feasiblend safe. The observational nature of our study preventss from definitively concluding that our protocol led ton improvement in hematoma volume or neurologic out-ome compared to standard therapy. The results from thepcoming Antihypertensive Treatment of Acute Cerebralemorrhage trial and the follow-up to the Intensivelood Pressure Reduction in Acute Cerebral Hemor-
hage (INTERACT-2) trial should give us an evidence-
ased answer to the question of whether aggressive BPontrol in patients with spontaneous ICH leads to betterlinical outcome.
REFERENCES
1. Broderick J, Connolly S, Feldmann E, et al. Guidelines for themanagement of spontaneous intracerebral hemorrhage in adults:2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood PressureInterdisciplinary Working Group: the American Academy of Neu-rology affirms the value of this guideline as an education tool forneurologists. Stroke 2007;38:2001–23.
2. Qureshi AI, Tuhrim S, Broderick JP, Batjer HH, Hondo H, HanleyDF. Spontaneous inracerebral hemorrhage. N Engl J Med 2001;344:1450–60.
3. Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaghuchi T.Enlargement of spontaneous intracerebral hemorrhage: incidenceand time course. Stroke 1996;26:1783–7.
4. Ohwaki K, Yano E, Nagashima H, Hirata M, Nakagomi T, TamuraA. Blood pressure management in acute intracerebral hemorrhage:Relationship between elevated blood pressure and hematoma en-largement. Stroke 2004;35:1364–7.
5. Brott T, Broderick J, Kothari R, et al. Early hemorrhage growth inpatients with intracerebral hemorrhage. Stroke 1997;28:1–5.
6. Dandapani BK, Suzuki S, Kelley RE, Iglesias YR, Duncan RC.Relation between blood pressure and outcome in intracerebralhemorrhage. Stroke 1995;26:21–4.
7. Leira R, Davalos A, Silva Y, et al. Early neurologic deteriorationin intracrerebral hemorrhage: predictors and associated factors.Neurology 2004;63:461–7.
8. Barton CW, Hemphill JC. Cumulative dose of hypertensionpredicts outcome in intracranial hemorrhage better than Amer-ican Heart Association guidelines. Acad Emerg Med 2007;14:695–701.
9. Willmot M, Leonardi-Bee J, Bath PMW. High blood pressure inacute stroke and subsequent outcome: a systematic review. Hyper-tension 2004;43:18–24.
10. Kothari R, Brott T, Broderick J, et al. The ABCs of measuringintracerebral hemorrhage volumes. Stroke 1996;27:1304–5.
11. Leira R, Davalos A, Silva Y, et al. Early neurologic deteriorationin intracrerebral hemorrhage: predictors and associated factors.Neurology 2004;63:461–7.
12. Teasdale G, Jannett B. Assessment of coma and impaired con-sciousness: a practical scale. Lancet 1974;2:81–4.
13. Brott T, Adams HP Jr, Olinger CP, et al. Measurements of acutecerebral infarction: a clinical examination scale. Stroke 1989;20:864–70.
14. Bamford JM, Sandercock PA, Warlow CP, Slattery J. Interob-server agreement for the assessment of handicap in stroke patients.Stroke 1989;20:828.
15. Qureshi AI, Wilson DA, Hanley DF, Traystman RJ. Pharmaco-logic reduction of mean arterial pressure does not adverselyeffect regional cerebral blood flow and intracranial pressure inexperimental intracerebral hemorrhage. Crit Care Med 1999;27:965–71.
16. Powers WJ, Adams RE, Yundt KD, et al. Acute pharmacologicalhypotension after intracerebral hemorrhage does not change cere-bral blood flow. Stroke 1999;30:242.
17. Anderson CS, Huang Y, Wang JG, et al. Intensive blood pressurereduction in acute cerebral haemorrhage trial (INTERACT): arandomized pilot study. Lancet Neurol 2008;7:391–9.
18. Burke RE, Dorfman M, Chan SB. Is emergent antihypertensivetreatment beneficial in intracranial hemorrhage? J Emerg Med2005;29:9 –13.
19. Qureshi A, Mohammad Y, Yahia A, Suarez J, et al. A prospec-tive multicenter study to evaluate the feasibility and safety
of aggressive antihypertensive treatment in patients with
ED Control of BP in Intracerebral Hemorrhage 361
acute intracerebral hemorrhage. J Intensive Care Med 2005;20:34 – 42.
20. Koch S, Romano JG, Forteza AM, Otero CM, Rabinstein AA.
Rapid blood pressure reduction in acute intracerebral hemorrhage:feasibility and safety. Neurocrit Care 2008;8:316–21.21. Subramaniam S. Controversies in medical management of intrace-rebral hemorrhage. Can J Neurol Sci 2005;S2:S13–21.
22. Qureshi A, Harris-Lane P, Kirmani J, et al. Treatment of acute
hypertension in patients with intracerebral hemorrhage using Ameri-can Heart Association guidelines. Crit Care Med 2006;34:1975–81.ARTICLE SUMMARY1. Why is this topic important?
Hypertension is associated with early hematoma ex-pansion, poor neurological outcome, and death in intra-cerebral hemorrhage. Recent studies have shown thatearly blood pressure control reduces hematoma growthand may decrease mortality.2. What does this study attempt to show?
This was a prospective observational trial testing thefeasibility and tolerability of lowering mean arterial pres-sure to a range of 100–110 mm Hg within 120 min ofarrival in patients with spontaneous intracerebral hemor-rhage in the Emergency Department (ED) setting.3. What are the key findings?
The average time for reaching our target mean arterialpressure was 123 min and for placing an arterial line was84 min. The protocol was tolerated in 77% of patients,and our in-hospital mortality rate was 41%.4. How is patient care impacted?
If future trials demonstrate a clinical benefit of earlyblood pressure control in intracerebral hemorrhage, EDscould successfully implement similar protocols.