Patient Focused Emergency Department
11
Patient Focused Emergency Department Dr. S. A. Tabish The function of an emergency department is to evaluate and provide advice of initial treatment to anyone who comes there seeking medical assistance. In planning, a new or renovated emergency department for a hospital, it is necessary to realize that some well-defined trends are changing the character of emergency-care departments. The trends must be appreciated before specific programming for a given hospital is undertaken. It is necessary to have a clear idea of the kinds of services to be rendered, as well as projected patient loads, types of patient and son on. Analysis and development of planning factors will provide information on size, cost and functional characteristics of contemplated emergency department. The concern of the hospital planning is the quality of medical care and the improvement of its standards. The planners must be aware of continuing advances in medicine, changes in society, ideology and attitudes of the community, and economic and technological conditions. An efficient hospital requires a well-balanced organization for compassionate care within an adequate technical and environmental framework. Emergency department is the shop-window of a hospital. Adequate planning, design, management and maintenance of the facility and equipment of the Emergency Department is essential to ensure the high quality of services at a reasonable cost. Planning Consideration The concern of the hospital planning is the quality of medical care and the improvement of its standards. Continuing advances in medicine and society impose great demands on the planning and design of medical services. Community needs must form the basis for planning attitudes and aspirations must be clearly understood. Planning involves and requires understanding and evaluation of the current cultural mainstreams, the economic and technological conditions, and the goals of the community. Planning ought to be thinking in the probable terms of tomorrow. The long- term cost of operating a hospital can be greatly increased by the initial failure to plan proper systems and equipment. The objectives should be fully understood. The care needs of patients should directly dictate the character of every care function. The hospital is for the patient. The patients and their needs must always be the point of focus when planning any facility. The constructed environment is to be designed with nursing and treatment in view.
Transcript of Patient Focused Emergency Department
Patient Focused Emergency Department
Dr. S. A. Tabish
The function of an emergency department is to evaluate and provide advice of initial treatment to anyone who comes there seeking medical assistance.In planning, a new or renovated emergency department for a hospital, it isnecessary to realize that some well-defined trends are changing the character of emergency-care departments. The trends must be appreciated before specific programming for a given hospital is undertaken. It is necessary to have a clear idea of the kinds of services to be rendered, aswell as projected patient loads, types of patient and son on. Analysis anddevelopment of planning factors will provide information on size, cost andfunctional characteristics of contemplated emergency department.The concern of the hospital planning is the quality of medical care and the improvement of its standards. The planners must be aware of continuingadvances in medicine, changes in society, ideology and attitudes of the community, and economic and technological conditions. An efficient hospital requires a well-balanced organization for compassionate care within an adequate technical and environmental framework. Emergencydepartment is the shop-window of a hospital.Adequate planning, design, management and maintenance of the facility and equipment of the Emergency Department is essential to ensure the high quality of services at a reasonable cost.Planning ConsiderationThe concern of the hospital planning is the quality of medical care and the improvement of its standards. Continuing advances in medicine and society impose great demands on the planning and design of medical services. Community needs must form the basis for planning attitudes and aspirations must be clearly understood. Planning involves and requires understanding and evaluation of the current cultural mainstreams, the economic and technological conditions, and the goals of the community.Planning ought to be thinking in the probable terms of tomorrow. The long-term cost of operating a hospital can be greatly increased by the initial failure to plan proper systems and equipment. The objectives should be fully understood. The care needs of patients should directly dictate the character of every care function.The hospital is for the patient. The patients and their needs must always be the point of focus when planning any facility. The constructed environment is to be designed with nursing and treatment in view.
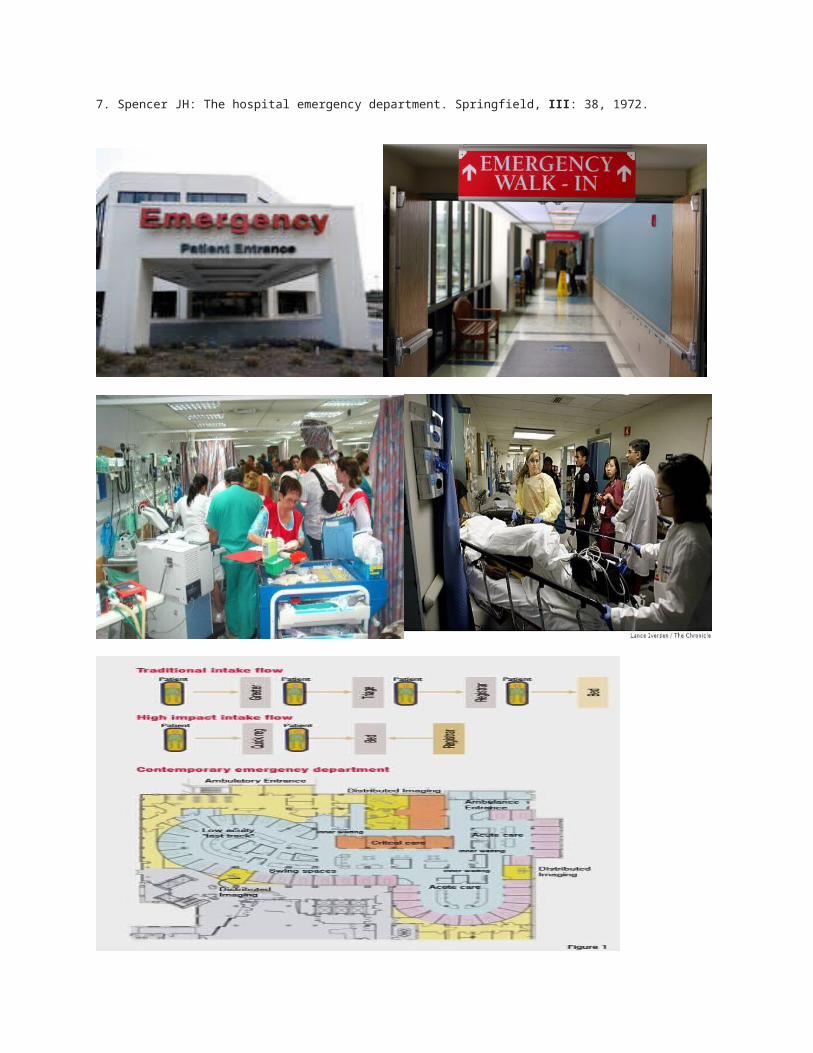
There should be recognition of the fact that an active emergency service tends to embrace more than accident and true emergency functions and oftenassumes responsibility for admitting during the evening and night shifts.Functions of Emergency DepartmentThe function of emergency department is to evaluate and provide advice or initial treatment to anyone who comes for medical assistance. The definition of an emergency has come to be determined by the needs and the perceptions of the general public. Owing to the increased specialization of medical services and the mobility of the population, the emergency department is increasingly being viewed as a place to get prompt medical attention for any condition. The emergency department must be designed andorganized to handle this widevariety of expectations.Every hospital must have a provision for receiving and dealing the “walking causalities” very simple fractures, cuts needing suturing, abscesses, and othe rminor conditons. Provision has to be made for dealingpromptly and efficiently with medical and surgical emergencies, from whatever cause.The future of the emergency may well lie in the field of automation. If automatic dispensing machines are to take the place of personal issue of supplies, and automatic analysers to take over the more painstaking diagnostic procedures, it is possible that the emergency department of thefuture will look a selfcontained, fully organised patient care service.Facility PlanningAdequate SpaceThe department should be designed to allow ready expansion of space to accommodate future changes in the volumes of the patients. It should be large and constructed of materials that ware well. Twenty to twenty-five percent must be added to the present patient volume to approach the load at completion and another 25 percent should be added to avoid overcrowdingin the first 4 or 5 years of operation.Easy AccessThe department should be located on the ground floor so that it is easily accessible to ambulances and ambulatory patients as well as to the rest ofthe hospital. There should be easy access to hospital and ambulance parking. Separate EntrancesEntrances to the department should be separate from those to the rest of the hospital so that they do notfunction as a corridor to the rest of the hospital. Directions to the Emergency should be well markedand clearly visible. The Ambulance Bay should be large enough to accommodate several ambulances
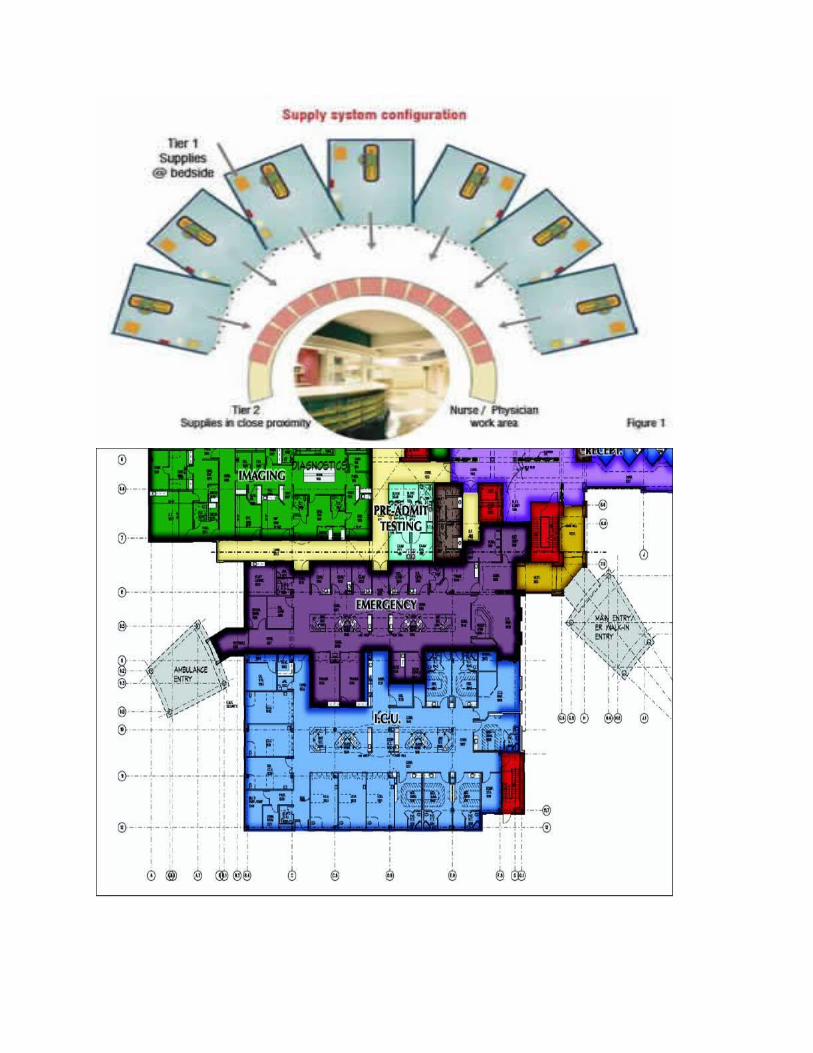
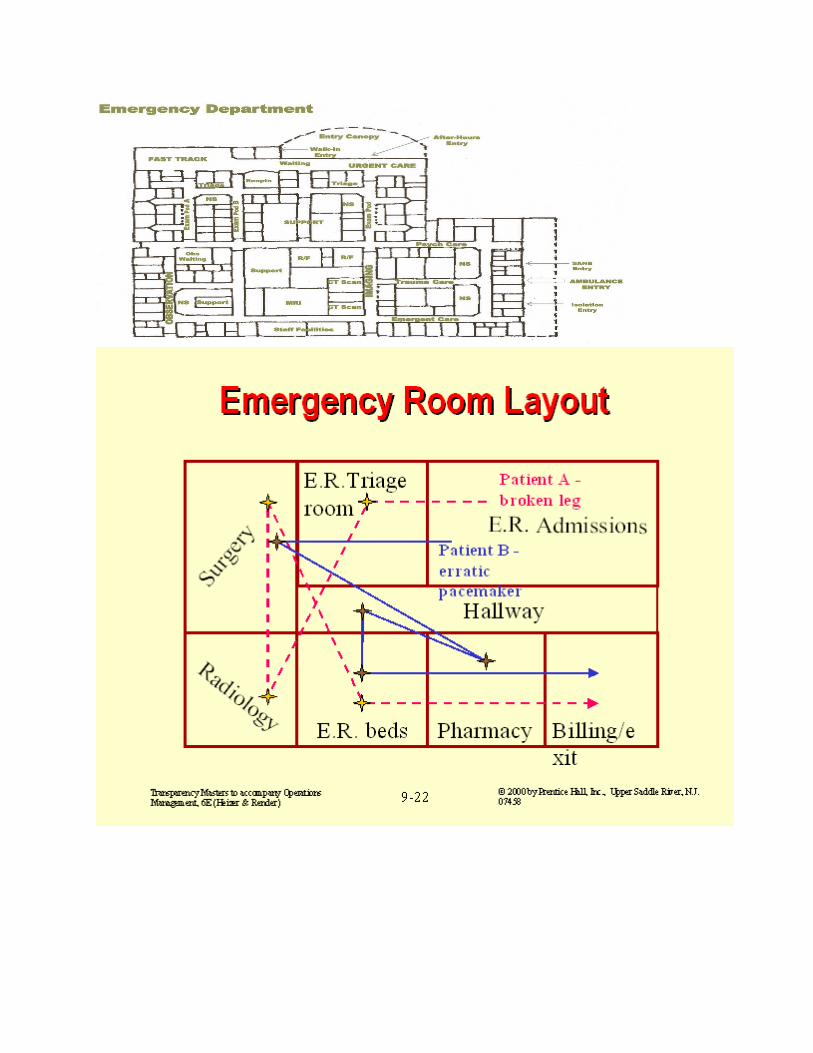
simultaneously and should be covered and protected from inclement weather.An area just inside theentrance should be allocated for the storage of wheel chairs and stretchers. There should be separateentrance for ambulatory patients whenever possible.Proximity to Other Hospital ServicesThe emergency department should have its own laboratory and Radio-diagnostic facilities, ECG room, drug counter and operation theater. Alternatively, the department should be located near the radiology services, laboratory, pharmacy and admitting office.Adaptable SpaceAll area of the department should be equipped to handle seriously ill patients if the need arises. Roomsin the emergency department should be multipurpose so that depending on need, they can be converted from use by ambulatory patients to use by gurney patients and vice versa. An adequate number of oxygen, suction, and electric outlets must be available therefore.Functional RoomsDesign of the department should make the most efficient use of staff and space while providing adequate privacy (curtained cubicles versus individual rooms).Flow of TrafficThe floor plan must consider patient flow and the volume of traffic. Unidirectional patient flow(separate ‘exit’ and ‘entrance’) is preferable to avoid chaos during busy periods.CommunicationIntercoms, paging system, telephones, and pneumatic tube systems should bewidely distributedthroughout the department.ComponentsTriage AreaIt is the reception area (14 ft × 200 ft), where incoming patients are evaluated for the degree of severity and urgency of illness. It should be very close to entrance, generous floor space should be allocated.Waiting AreaPatient’s relatives and friends should be accommodated in well appointed and comfortable waiting room. There should be shelves for literature describing the function and the rules of the department as well as other well chosen current reading material.• A television set may be an asset.• Access to a tea or coffee bar or vending machines is valuable.• For accompanying children, a separate waiting area should be provided.• Clearly marked visitors’ toilets should be provided near the main waiting space.
Admission OfficeAdmissions, discharges and record-keeping are carried out in a reception and registration room of about 15 m2 size, located immediately adjacent toentrance. This office has to be manned on 24 hrs basis.Care of BurnsA room of 20 m2 size is needed for the immediate care of burn patients.Staff RoomsThe nurses station should be adjoined by a work room for nursing personnel.Miscellaneous Facilities• Blood storage area• Room for medico-social worker• Drug dispensing facility• Room for brought dead• Room for Police personnel• Room for class IV employees.Operation RoomThe emergency operation room should be self contained. It should be provided with conducting floors. Wall suction and oxygen are indispensable.Operation theater must be connected to emergency electric supply system.Radio-diagnosis RoomThere should be two or three diagnostic rooms, a dark room, a dry film room, a radiologist room, radiographer’s room, a record office, store roomand waiting area. A large X-ray room, may be divided by partition into twoor three bays, each large enough to carry out X-ray examination of patienton a stretcher. The operator must be able to see into each bay from the central cubicle.Automatic film processing is of great advantage.In order to meet the increasing demand of trauma cases, a CT scan facilitymay be considered.High resolution ultrasonography tests should be performed in the evaluation of acute surgical emergencies. Radiology section should be connected to emergency electric system.LaboratoryIt is preferable for the emergency department to have its own laboratory and technicians, so that the priority tests can be quickly communicated.Microscopes, centrifuges and a Bunsen burner are needed. Biochemistry autoanalyser, blood gas andelectrolyte analysis facilities are desirable.Observation WardThis ward is used for patients who have been evaluated and need extended treatment, observation, re-evaluation, or other time-consuming procedures.The observation ward permits more efficient use
of treatment rooms. It is desirable to establish and absolute time limit apatient may spend in this ward.Generally, 12-48 hours is reasonable depending on the size of the ward. The need of 1-2 observationbed per 100 in-patient beds in the catchment area has been indicated. The observation ward could beused as an acute treatment facility in times of mass casualties or when the patient load is exceptional.StorageStorage space must be provided for intravenous fluid drugs, clean linen and instruments. Plaster, larger mobile equipment (X-ray and ECG machines etc.), wheel chairs and stretchers. Life-saving equipment such as resuscitation sets, tracheotomy and other procedure sets should be made available.Utility and Soiled Linen RoomUtility room for emptying, cleaning and storing of bedpans should be equipped with a bedpan washer,disinfector and cupboards. Soiled instruments and containers are rinsed and soiled linen stored in thisroom. Each room should have the size of about 7 m2.Staff-changing RoomChanging rooms for female staff should include lavatories, showers and lockers for personalpossessions. There should be a retiring room. A lounge with pantry for therecreation of staff maybe provided. Comfortable quarters for slack periods are required for doctors and nurses on duty. An oncall room of 9 m2 should be furnished.Treatment Room/Examination Cubicles• For major emergency (20’ × 20’ or 6 m × 6 m)The area should have ample floor space to accommodate several people and large piecesof equipment. Each room must be fully equipped to handle any major illness. There should beseveral wall-mounted suction units, electrical, oxygen and air outlets.• For intermediate emergency (12’ × 14’ or 12’ × 16’) Rooms set aside for patients with illnessor injury of moderate severity are used for stretcher patients (e.g., suture or fracture cases).Food lighting and wall-mounted suction and oxygen outlet facilities are required.• For minor problem (10’ × 12’) Ambulatory patients with non-life threatening problems are treated in rooms set aside for this purpose.Curtained cubicle are both more efficient and safer than single rooms.Special Treatment Rooms
• ENT, eye and dental room Equipment should include a dental chair, ENT chart, slit lamp, suction device and oxygen source.• Cast room It should have a sink for mixing plaster, a cast saw, X-ray viewboxes, and storage for orthopaedic supplies.• Obstetric room It should be equipped for pelvic examination, evaluation of patients in labour, and emergency delivery.• Psychiatric holding room• Decontamination room It should be tiled, with flexible-hose shower head forcleaning patients(radio-active decontamination, delousing) 13 m2 size.• Suture room It should be equipped for treatment of superficial wounds.• Resuscitation room The patient is to be stabilized in this room. Immediate attention is given alsoto patients who need opening or cleaning of air passages and restoring theblood volume of the body. All the equipment including ECG and medications for comprehensive cardiac area should be kept in this room so that the procedure could be immediately started. The equipment includes a treatmenttable or a patient’s trolley,an oxygen outlet and a suction point, adjustable lamps (one of them for performing minor surgical procedures), a lockup cupboard for respiratory equipment, an X-ray view box, a refrigerator for blood, a working top, shelves for balnkets, a wash basin and shelves for drugs and IV fluids.An area of 30 m2 is required. This room must be connected to the emergencyelectric supply system.• Treatment room for burn patients One airconditioned dressing-room with a stainless steel bath and mechanical hoist should be provided. Plenum-Ventilation of dressing-room with an exhaust ventilated air lock has been shown to reduce infection in a burns unit. An operation room within the burn unit is frequently favored.Other FacilitiesIf the department is large there should be a centrally located nurses station with doctors’ and nurses charting area and dictating booths. An office for the emergency department supervisor is desirable.Public telephone booths within easy reach of waiting area should be provided.General ConsiderationThe gross floor area to be assigned to the emergency department will vary from nothing to 15 sq ft per bed, according to programme requirements. Thebest test of size is to programme the department for local experience, determine the number of treatment rooms and supporting spaces and actuallycalculate the net and gross areas.Functional ProgrammeFor 500 bedded hospital, it will be as follows:• Provide an emergency department for 24 hours operation.• Include four surgical treatment-examination rooms.• Include 4 additional examination rooms.
• Provide 12 observation beds and all necessary supporting spaces.• The receiving and preparation room, 14 ft × 20 ft, shall adjoin a grade entrance with wide doors (leading immediately into the receiving corridor)and shall have facilities for taking care of at least 2 patients at a time. In a catastrophe, the adjoining space will have to be used as overflow receiving and first aid rooms.• Public waiting (partially or wholly screened) with seats for 20 persons and access to toilets is to be provided.• Provide 12 observation beds in four rooms with private toilet and showeradjoining each room, provide oxygen and suction and usual communications.Provide a nursing station for this unit.StaffingThe staffing of emergency department will depend on its size, work-load, type of hospital, and theresources available. Depending upon the scope of the servies, the following personnel are essential toman the emergency services:• General surgeon• Orthopedic surgeon• Medical specialist• Anesthetist (on call)• House surgeons/Junior residents• General duty medical officers• Obstetrician• Nurisng staff• Nursing orderlies• Sanitation staffThe department needs to be staffed in its own right. From the consultant incharge downwards by personnel whose primary concern is to run it efficiently. It is no use leaving the department (that needs to be staffedthroughout the 24 hours by specialists with a high degree of skills) in the hands-of junior doctor, as is so often done, instructing him to call the specialist in case of difficulty.The emergency department will function best if all personnel in the emergency area are directly responsible to its chief or officer in charge.The officer should be responsible to a policy committee consisting of the members of the medical staff and representative from hospital administration.Emergency PreparednessA mass casualty situation arises whenever a rapid influx of large number of critically injured people exceeds the capacity of the receiving facility to provide individualized medical care in the usual way. The objective in organising for mass causalities is to furnish care that benefits the greatest number of people. Every year many places on our
planet are struck by floods, earthquakes, landslides, house collapse, droughts, famines, vehicular accidents and other catastrophes.DisastersAny occurrence that causes damage, ecological disruption, loss of human life, deterioration of health and health services on a scale sufficient towarrant any extra-ordinary response from outside the affected community area are bound to be more frequent in the coming decades due to progressive deterioration of environment, deforestation, misuse of land, etc.Though it is not possible to prevent most of the disasters, but still their worse effects can be alleviated or mitigated in magnitude by anticipated preparedness.Disasters may be natural (earthquakes) or human (transportation accident, civil disturbance or terrorism) and the nature of injuries depends on the type of disaster.Provisions must nonetheless be made to provide everyday emergency, medicalsurgical and obstetric services if no other medical facility is available.A plan for efficient management of mass causalities in times of disaster should ensure rapid organization and expansion of community medical resources to maximum possible capacity (under emergency conditions). A plan for providing expanded medical and surgical services in disasters must be disseminated to all appropriate personnel. Emergency Medical Services is an essential element in the contribution of hsopital towards the total health care of the community. Providers of emergency services aswell as the consumers should clearly define and understand the emergency medical care needs of their population and the facilities available in thehospital so that maximum benefit can be derived within limited resources available. Emergency department must be efficient at all the times and forall the purposes for which it is meant. It must be established on right cost benefit basis. Adequate physical facilities, equipment and stores should be available. An alert well-trained and sympathetic staff that can render prompt and correct medical care to the critically ill patients is desirable.
FURTHER READING1. American college of surgeons. Committee on trauma: Advance trauma life support Course for physicians.Amercian College of Surgeons. 1996.2. Tabish SA: Planning Tomorrow’s Hospitals Today, JAHA 2: 7-14, 1990.3. Emergency medical system. In: Principles and practiceof emergency medicine. Schwartz GR et al (Eds):Suanders 1371-1494, 1978.4. Mills J et al: Current Emergency Diagnosis andTreatment (2nd edn.) USA, 1983.5. Putsep E: Modern Hospital: International planning practice. Lloyed Luke Ltd. London640-54, 1979.6. Parker S: Emergency room utilitisations at Hermann Hospital. Texas Medicine 74: 10: 62-70, 1978.
7. Spencer JH: The hospital emergency department. Springfield, III: 38, 1972.