A Patient-Focused Framework Integrating Self-Management and Informatics
16
SELFMANAGEMENT & INFORMATICS 1 This is the pre-peer reviewed version of the following article: Knight, E. P. and Shea, K. (2014), A Patient-Focused Framework Integrating Self-Management and Informatics. Journal of Nursing Scholarship, 46: 91–97. doi: 10.1111/jnu.12059, which has been published in final form at http://onlinelibrary.wiley.com/doi/10.1111/jnu.12059/abstract A Patient-Focused Framework Integrating Self-Management and Informatics Elizabeth P. Knight, BSN, RN (corresponding author) Beta Mu Chapter, STTI PhD/DNP Student University of Arizona College of Nursing Tucson, Arizona [email protected] Kimberly Shea, PhD, RN Beta Mu Chapter, STTI Assistant Professor University of Arizona College of Nursing Tucson, AZ [email protected]
Transcript of A Patient-Focused Framework Integrating Self-Management and Informatics

SELF-‐MANAGEMENT & INFORMATICS 1
This is the pre-peer reviewed version of the following article: Knight, E. P. and Shea, K. (2014), A Patient-Focused Framework Integrating Self-Management and Informatics. Journal of Nursing Scholarship, 46: 91–97. doi: 10.1111/jnu.12059, which has been published in final form at http://onlinelibrary.wiley.com/doi/10.1111/jnu.12059/abstract
A Patient-Focused Framework Integrating Self-Management and Informatics
Elizabeth P. Knight, BSN, RN (corresponding author) Beta Mu Chapter, STTI
PhD/DNP Student University of Arizona College of Nursing
Tucson, Arizona [email protected]
Kimberly Shea, PhD, RN Beta Mu Chapter, STTI
Assistant Professor University of Arizona College of Nursing
Tucson, AZ [email protected]

SELF-‐MANAGEMENT & INFORMATICS 2
Abstract
Purpose: This paper introduces a framework to 1) guide chronic illness self-management interventions through the integration of self-management and nursing informatics, 2) focus self-management research, and 3) promote ethical, patient-empowering technology use by practicing nurses. Method: Existing theory and research focusing on chronic illness, self-management, health-enabling technology, and nursing informatics was reviewed and examined and key concepts were identified. A care paradigm focusing on concordance, rather than compliance, served as the overall guiding principle. Findings: This framework identifies key relationships among self-management (patient behaviors), health force (patient characteristics) and patient-defined goals. The role of health-enabling technology supporting these relationships is explored in the context of nursing informatics. Conclusions: The Empowerment Informatics framework can guide intervention design and evaluation and support practicing nurses’ ethical use of technology as part of self-management support. Clinical Relevance: Nurses worldwide provide support to patients who are living with chronic illnesses. As pressures related to cost and access to care increase, technology-enabled self-management interventions will become increasingly common. This patient-focused framework can guide nursing practice using technology that prioritizes patient needs.
Key words: Chronic illness, chronic disease, self-management, informatics, technology, framework, theory, patient-focused
SELF-‐MANAGEMENT & INFORMATICS 3
A Patient-Focused Framework Integrating Self-Management & Informatics
Chronic illness is a leading cause of death and disability globally (World Health
Organization, 2011). Nearly one in two U.S. adults lives with a chronic illness, such as
diabetes, heart disease, or arthritis, and prevalence is rising (National Center for Chronic
Disease Prevention and Health Promotion, 2009). Unlike acute illnesses which can be
managed in a healthcare setting, chronic illness is managed largely by individuals and
families at home as part of their daily lives. Although the U.S. healthcare system
prioritizes acute care, rising costs and patient preferences for aging in place are driving
demand for different approaches to care, including self-management support (Wiles,
Leibing, Guberman, Reeve, & Allen, 2012).
Technology-enabled self-management interventions are ubiquitous; however,
there is limited evidence of lasting improvements in patient outcomes or cost savings.
The root of this problem may be a lack of theoretical guidance: interventions are 1)
convenience-based use of available technologies in existing disease-management plans,
and/or 2) compliance-based, designed to help patients meet the goals defined by
healthcare providers within a structured, acute-care based health system.
While existing nursing theory examines how patients self-manage, and existing
informatics theory explores nurses’ technology use, there is currently no framework
addressing the intersection of these ideas. This paper will introduce a framework to guide
the integration of self-management and informatics research and to promote ethical,
patient-empowering technology use by practicing nurses.
Understanding Self-Management
Self-management typically refers to a core set of behaviors undertaken by patients

SELF-‐MANAGEMENT & INFORMATICS 4
living with chronic illness: medical management, role management, and emotional
management (Corbin & Strauss, 1988; Lorig & Holman, 2003). A considerable body of
theory and research explores patients’ experiences of self-management (Corbin &
Strauss, 1988; Grey, Knafl, & McCorkle, 2006; Lorig & Holman, 2003; Ryan & Sawin,
2009; Schulman-Green et al., 2012). The nurse’s approach to supporting patients’ self-
management behaviors, informed by this work, is the basis of a patient-focused self-
management intervention.
Self-Management Interventions and Technology
Many existing technology-based interventions rely on a compliance-based
approach to self-management that aims to increase patient adherence to provider-defined
plans and goals. Such interventions focus on medical management, but often ignore the
other aspects of self-management. Telemonitoring devices that collect and send
physiologic data to a home health nurse are an example of technology designed to
improve compliance with prescribed medical regimens (LaFramboise, Woster, Yager, &
Yates, 2009; Woodend et al., 2008; Woods & Snow, 2013). Electronic and web-based
tools that enable the patient to track patterns in their vital signs and adjust management
according to an algorithm are also compliance-based (Brennan et al., 2010; Seto et al.,
2012).
Concordance and Self-Management
Alternatively, in a concordance-based approach, the patient learns how to live
with a chronic health condition and is empowered and motivated by relevant knowledge,
practical skill, and personal experience (Schermer, 2009). A concordance approach can
better address all core behaviors of self-management, including medical, role, and

SELF-‐MANAGEMENT & INFORMATICS 5
emotional management. While each health-related action may not be the most medically
appropriate from the provider’s perspective, the patient makes choices in accordance with
his personal goals and values (Schermer, 2009). The concordance approach requires
collaboration between nurse and patient and is the focus of the framework described in
this paper. The collaborative nurse offers information and guidance, but also recognizes
that consideration of the patient’s unique characteristics, rather than standardized clinical
targets, are the ultimate priority in self-management.
Unique Patient Characteristics
Supporting individual patient goals requires an understanding of the contexts in
which patients live with and manage their chronic illnesses, both internally (cognition
and emotion) and externally (environment and resources) (Forbes & While, 2009).
Health Force
Health force is the strength of the patient’s belief that he can actualize his own
unique concept of health. It is influenced by sociocultural and contextual factors
combined with aspects of individual experience, knowledge, values, and motivation.
Health force is personal and dynamic and may shift with the patient’s education, access
to resources, health status, and life experiences. Thus, health force is a patient
characteristic which contributes to the patient’s desire and ability to engage in self-
management behaviors.
Others have suggested that self-management is mediated by self-efficacy (Lorig
et al., 2010). Determinants of self-efficacy defined by Bandura, including social
persuasion, vicarious experience, and personal mastery, may also influence health force
(Bandura, 1998). However, the concept of health force extends the situation-specific

SELF-‐MANAGEMENT & INFORMATICS 6
nature of self-efficacy beyond individual tasks to the patient’s personal concept of health.
Understanding health force will help the nurse identify patient-focused mediators and
moderators of successful self-management, and ultimately empower the patient to pursue
self-defined goals.
Patient-Defined Goals
Self-management (patient behaviors) and health force (patient characteristics)
together contribute to the achievement of meaningful goals. Individually meaningful
goals promote patient autonomy, empowerment, and motivation (Holm, 2005). These
goals are not terminal outcomes, but rather part of the ongoing, dynamic process of self-
management (McWilliam et al., 1999). Goals may shift over time with patients’ health
status, knowledge, and circumstances. They may be objective and measureable or
subjective and personal. By supporting patient empowerment through individualized
goal-setting, nurses can help patients focus on health as they themselves experience it,
rather than on illness as measured by healthcare providers.
Individuals may choose to use empirical measurements of health directly in their
goals, or nurses may use objective data to assist patients in achieving their subjective
goals. For instance, nurses may help patients identify patterns and relationships among
their goals, such as symptom control, measurable indicators, such as vital signs, and
behaviors, such as exercise. Empirical measurements can also assist with medical
management, which is one of the behaviors of self-management. Ultimately, however,
empirical health indicators are useful primarily as a support for patient-defined goals.
Health-Enabling Technologies
Health-enabling technologies (HET) are information and communication

SELF-‐MANAGEMENT & INFORMATICS 7
technologies which create conditions for sustainable, patient-empowering health choices
(Haux et al., 2009). Patients’ direct interaction with HET increases their access to and
control over information, removes barriers to empowerment, and assists them to sustain
their self-management behaviors after professional intervention has ended. HET-enabled
self-management has the potential to address high healthcare burdens worldwide by
enhancing chronic disease management, regardless of accessibility to local healthcare
resources (Dacso, Knightly, & Dacso, 2011).
Strengths of current HET include personalizability, portability, adaptability, data
collection and management, and multimodal communication (Arsand & Demiris, 2008;
Forbes & While, 2009). HET functions useful for self-management include monitoring,
education, feedback, social support, and procedural response.
HET is deliberately defined broadly to allow ongoing integration of new
innovations. However, interventions driven by available technology rather than by
identified needs of users and theoretical guidance often fail to produce meaningful
outcomes (Vicente, 2003). Thus, a framework guiding the use of HET needs theoretical
structure to facilitate the appropriate and efficient integration, implementation, and
evaluation of new technologies. The field of nursing informatics is one potential source
of this needed theoretical structure.
Nursing Informatics
Nursing informatics is defined as the integration of data, information, and
knowledge to support patients and nurses in decision making across roles and settings,
using information structures, processes, and technology (Staggers & Thompson, 2002).
Nursing informatics frameworks have been used primarily in reference to nurses in

SELF-‐MANAGEMENT & INFORMATICS 8
hospital settings, but some may also be useful to guide community-based self-
management. The Informatics Research Organizing Model (Effken, 2003) can guide the
development of community-based HET interventions within a nursing worldview. The
explicit inclusion of the four concepts of the nursing metaparadigm (person, environment,
health, and nursing) promotes interventions that are context-aware and patient-focused
(Fawcett, 1996), characteristics necessary to support a concordance approach. The Data,
Information, Knowledge and Wisdom informatics framework provides a nursing process
approach to understanding technology’s role in self-management (Gee et al., 2012).
While previously this framework has been applied to nurses’ technology use, it may also
guide the collaboration of patient and nurse using HET by focusing on the role of
patients’ unique self-knowledge in self-management (Gee et al., 2012).
Human-Computer Interaction
Effective technology use requires not only knowledge of hardware and software
capabilities, but also an understanding how people cognitively and physically interact
with interfaces. Potential sources of theory to explicate these relationships include the
field of human factors, which explores how technology is both useful and usable (Czaja
& Lee, 2002; Demiris et al., 2010; Vicente, 2003), and sociotechnical theory, which
explores the influence of complex contextual factors on information technology tools
(Fox, 1995; Westbrook et al., 2007). A framework integrating theory that examines the
intersection of man and machine will promote theory-driven interventions rather than
one-sided, technology-driven interventions.
The Empowerment Informatics Framework
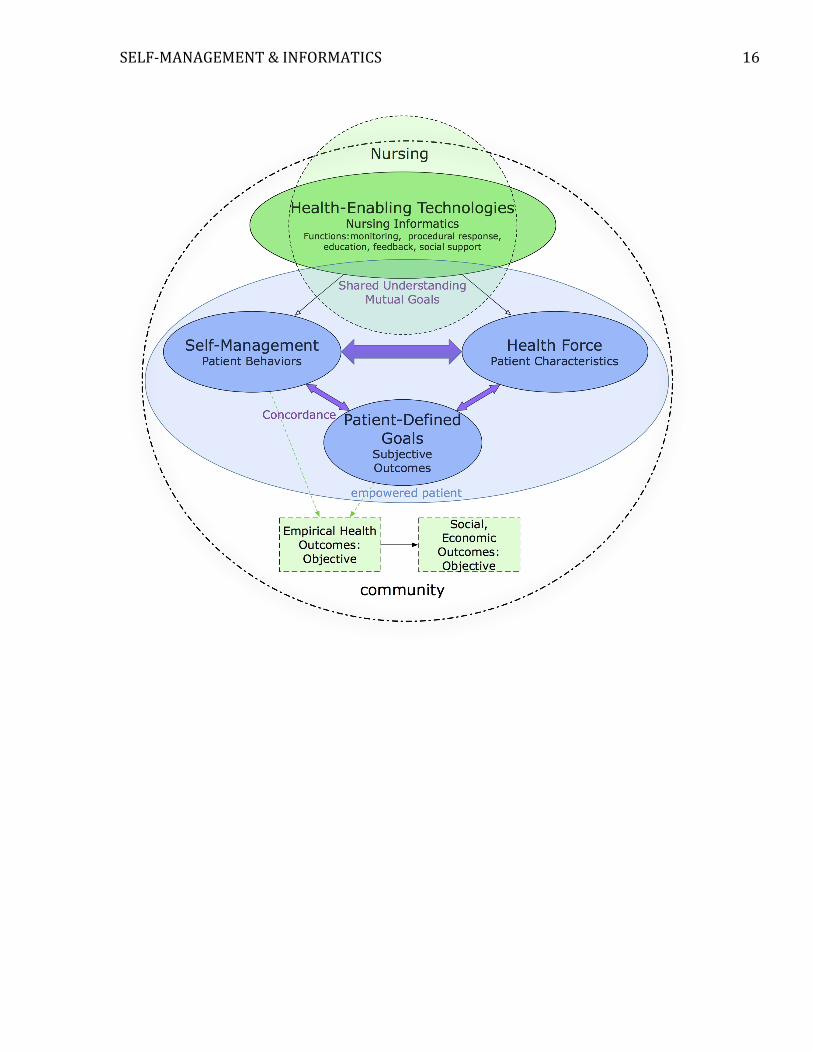
The empowerment informatics (EI) framework (Figure 1) suggests that patients

SELF-‐MANAGEMENT & INFORMATICS 9
living with chronic illnesses and collaborating nurses can use HET to support the
relationships among patients’ behaviors (self-management), patients’ unique
characteristics and context (health force), and patients’ individual goals. Self-
management plans informed by patient values, needs, and strengths can promote shared
understanding and mutual goals as part of a concordance, rather than compliance,
approach (Gunson & Chawngthu, 2012). The patient is empowered and motivated
through this focus on his own concept of health rather than on externally specified targets
enforced by healthcare providers. Patients’ behaviors directed at individual goals still
affect empirical indicators of their health and their use of resources; however, these
effects are secondary.
Existing theories related to self-management, technology, nursing, and
informatics can be integrated and tested within the EI framework. This theoretical
grounding, combined with a focus on patients’ individual goals, can begin to address the
weaknesses in current self-management interventions and drive truly innovative
approaches to managing chronic illness in the community.
Implications for Research
The EI framework aids in the identification of the goals of self-management
interventions, and consequently, the outcomes of interest. The outcomes of interest for EI
interventions are twofold: both the patient’s subjective perception of his health and
objective individual and systems-level effects are essential parts of evaluation. Most
studies to date have looked at only one of these aspects and have thus failed to capture
and communicate the overall potential impact of the interventions.
Evaluating Patient Perspectives

SELF-‐MANAGEMENT & INFORMATICS 10
The patient’s perspective on his own health is reflected in individual goals that
may shift over time in response to changes in health, environment, knowledge, and other
factors. Qualitative evaluation is most conceptually appropriate to evaluating these
subjective individual perspectives (Rahimpour, Lovell, Celler, & McCormick, 2008;
Sanders et al., 2012). Alternatively, researchers may use self-report tools to measure
constructs related to individual perception of health. Although the nurse cannot truly
measure the patient’s individual experience in a standardized fashion, in practice,
measurable constructs such as quality of life, self-perception of health, or satisfaction
with care may be useful in describing overall trends and common experiences among
groups of patients (Brennan et al., 2010; Lorig et al., 2012).
Evaluating Empirical Outcomes
The EI framework also supports quantitative research. While it is essential to
demonstrate that an intervention is subjectively valuable to patients, healthcare systems
that focus on evidence-based practice and cost control demand evidence of the
intervention’s objective clinical and economic benefit. Empirical, quantitative data can
communicate both individual-level and systems-level results in terms that will be widely
understood and will facilitate adoption. Objective evaluation in self-management
intervention studies may include process outcomes, functional outcomes, or clinical and
systems-level outcomes (Stellefson et al., 2013). Process outcomes include self-efficacy,
perceived usefulness, and frequency of communication with healthcare providers.
Functional outcomes quantify behaviors such as physical activity and medication
adherence. Clinical and systems-level outcomes include symptoms, physiologic data,

SELF-‐MANAGEMENT & INFORMATICS 11
laboratory values, mortality and hospital readmissions (Lorig et al., 2012; Woodend et
al., 2008;. Radhakrishnan & Jacelon, 2012; Stellefson et al., 2013).
Future Research
Research is needed to test the relationships between the concepts in this
framework, thereby leading to a better understanding of the unique contributions of HET
to the processes of self-management. Previously hypothesized determinants of successful
self-management (e.g., self-efficacy, self-confidence) need to be reevaluated in the
context of the EI framework. Understanding the mechanisms by which an intervention
works offers valuable direction for further research (Pingree et al., 2010). Research is
needed identify or confirm key mediators and moderators of the relationships proposed in
this framework.
Implications for Nursing Practice
Nurses working in diverse settings worldwide provide support to patients who are
living with chronic illnesses. HET self-management interventions are widely used, but
many are driven by economic and technological factors rather than patient factors
(Kaplan & Litewka, 2008). Consequently, the degree to which they meet patients’ needs,
in addition to healthcare providers’ or organizations’ needs, varies widely. Concerns
surrounding the use of HET by nurses include privacy, intrusiveness, autonomy, and
patient-centeredness (Demiris, Doorenbos, & Towle, 2009; Kaplan & Litewka, 2008).
The EI framework addresses many of these issues; it is driven by and focused on patient
goals, characteristics, and contexts and can help guide nurses in an ethical, patient-
focused approach to these issues.
SELF-‐MANAGEMENT & INFORMATICS 12
Nurses may be unaware of the paradigm underlying their care and despite
professing to promote patient empowerment, they may continue to practice in a way that
perpetuates medical dominance (Wilkinson & Whitehead, 2009). The use of this
explicitly patient-focused framework ensures emphasis on concordance, which empowers
patients, rather than compliance, which perpetuates medical dominance. Nursing values
espoused in the EI framework include focusing on quality of life, freedom of choice,
dignity, and personal health patterns based on values (Gunson & Chawngthu, 2012).
Conclusions
The growing worldwide burden of chronic illness and the imperative to reduce
healthcare costs will continue to create demand for technology-based self-management
interventions. The EI framework introduced in this paper suggests a patient-focused
approach to the integration of theory and evidence surrounding self-management and
nursing informatics. Research is needed to test these proposed relationships. This
introduction will serve to guide the use of the EI framework in nursing research and
practice.

SELF-‐MANAGEMENT & INFORMATICS 13
Clinical Resources Internet self-management programs: http://patienteducation.stanford.edu/internet/ Nursing informatics resources: http://www.amia.org/programs/working-groups/nursing-informatics Nursing theory: http://currentnursing.com/nursing_theory/
References
Arsand, E., & Demiris, G. (2008). User-centered methods for designing patient-centric self-help tools. Informatics for Health & Social Care, 33(3), 158–169. doi:10.1080/17538150802457562
Bandura, A. (1998). Health promotion from the perspective of social cognitive theory. Psychology & Health, 13(4), 623–649. doi:10.1080/08870449808407422
Bowles, K. H., Riegel, B., Weiner, M. G., Glick, H., & Naylor, M. D. (2010). The effect of telehomecare on heart failure self care. AMIA Annual Symposium Proceedings / AMIA Symposium, 2010, 71–75.
Brennan, P. F., Casper, G. R., Burke, L. J., Johnson, K. A., Brown, R., Valdez, R. S., et al. (2010). Technology-enhanced practice for patients with chronic cardiac disease: Home implementation and evaluation. Heart & Lung : The Journal of Critical Care, 39(S), S34–S46. doi:10.1016/j.hrtlng.2010.09.003
Corbin, J. M., & Strauss, A. (1988). Unending work and care: Managing chronic illness at home. San Francisco, CA: Jossey-Bass.
Czaja, S. J., & Lee, C. C. (2002). Designing computer systems for older adults. In J. A. Jacko & A. Sears (Eds.), The Human-computer interaction handbook (pp. 413–427). Mahwah, NJ: L. Erlbaum Associates Inc.
Dacso, C. C., Knightly, E., & Dacso, M. (2011). Technology-enabled chronic disease management in under-resourced environments. Proceedings of the 1st International Conference on Wireless Technologies for Humanitarian Relief, 365–369.
Demiris, G., Charness, N., Krupinski, E., Ben-Arieh, D., Washington, K., Wu, J., & Farberow, B. (2010). The role of human factors in telehealth. Telemedicine and e-Health, 16(4), 446–453. doi:10.1089/tmj.2009.0114
Demiris, G., Doorenbos, A. Z., & Towle, C. (2009). Ethical considerations regarding the use of technology for older adults: The case of telehealth. Research in Gerontological Nursing, 2(2), 128–136. doi:10.3928/19404921-20090401-02
Effken, J. A. (2003). An organizing framework for nursing informatics research. CIN: Computers, Informatics, Nursing, 21(6), 316–25.
Fawcett, J. (1996). On the requirements for a metaparadigm: an invitation to dialogue. Nursing Science Quarterly, 9(3), 94–106.
Forbes, A., & While, A. (2009). The nursing contribution to chronic disease management: A discussion paper. International Journal of Nursing Studies, 46(1), 120–131. doi:10.1016/j.ijnurstu.2008.06.010
Fox, W. M. (1995). Sociotechnical system principles and guidelines: past and present. The Journal of Applied Behavioral Science, 31(1), 91–105.
Gee, P., Greenwood, D., Kim, K., Perez, S., Staggers, N., & DeVon, H. (2012). Exploration of the e-patient phenomenon in nursing informatics. Nursing Outlook, 60(4), e9–e16. doi:10.1016/j.outlook.2011.11.005

SELF-‐MANAGEMENT & INFORMATICS 14
Grey, M., Knafl, K., & McCorkle, R. (2006). A framework for the study of self- and family management of chronic conditions. Nursing Outlook, 54(5), 278–286. doi:10.1016/j.outlook.2006.06.004
Gunson, J., & Chawngthu, L. (2012). Health Economics and Informatics: The gap-fit of current healthcare and Parse practice. Nursing Science Quarterly, 25(2), 176–181. doi:10.1177/0894318412437948
Haux, R., Gietzelt, M., Hellrung, N., Ludwig, W., Marschollek, M., Song, B., & Wolf, K. (2009). Health-enabling technologies for pervasive health care: a pivotal field for future medical informatics research education? Studies in Health Technology and Informatics, 150, 14–16.
Holm, S. (2005). Justifying patient self-management--evidence based medicine or the primacy of the first person perspective. Medicine, Health Care, and Philosophy, 8(2), 159–164. doi:10.1007/s11019-005-2280-x
Kaplan, B., & Litewka, S. (2008). Ethical challenges of telemedicine and telehealth. Cambridge Quarterly of Healthcare Ethics, 17(4). doi:10.1017/S0963180108080535
LaFramboise, L. M., Woster, J., Yager, A., & Yates, B. C. (2009). A technological life buoy: Patient perceptions of the Health Buddy. The Journal of Cardiovascular Nursing, 24(3), 216–224.
Lorig, K. R., & Holman, H. R. (2003). Self-management education: history, definition, outcomes, and mechanism. Annals of Behavioral Medicine, 26(1), 1–7.
Lorig, K., Ritter, P. L., Laurent, D. D., Plant, K., Green, M., Jernigan, V. B. B., & Case, S. (2010). Online diabetes self-management program: A randomized study. Diabetes Care, 33(6), 1275–1281. doi:10.2337/dc09-2153
Lorig, K., Ritter, P. L., Plant, K., Laurent, D. D., Kelly, P., & Rowe, S. (2012). The South Australia health chronic disease self-management internet trial. Health Education & Behavior. doi:10.1177/1090198112436969
McWilliam, C. L., Stewart, M., Brown, J. B., McNair, S., Donner, A., Desai, K., et al. (1999). Home-based health promotion for chronically ill older persons: Results of a randomized controlled trial of a critical reflection approach. Health Promotion International, 14(1), 27–41.
National Center for Chronic Disease Prevention and Health Promotion. (2009). Chronic disease: The power to prevent, the call to control. Retrieved from: http://www.cdc.gov/chronicdisease/resources/publications/aag/pdf/chronic.pdf
Nguyen, H. Q., Donesky-Cuenco, D., Wolpin, S., Reinke, L. F., Benditt, J. O., Paul, S. M., & Carrieri-Kohlman, V. (2008). Randomized controlled trial of an internet-based versus face-to-face dyspnea self-management program for patients with chronic obstructive pulmonary disease: Pilot study. Journal of Medical Internet Research, 10(2). doi:{10.2196/jmir.990}
Pingree, S., Hawkins, R., Baker, T., duBenske, L., Roberts, L. J., & Gustafson, D. H. (2010). The value of theory for enhancing and understanding e-health interventions. American Journal of Preventive Medicine, 38(1), 103–109. doi:10.1016/j.amepre.2009.09.035
Radhakrishnan, K., & Jacelon, C. (2012). Impact of telehealth on patient self-management of heart failure: a review of literature. Journal of Cardiovascular Nursing, 27(1), 33–43. doi:10.1097/JCN.0b013e318216a6e9
Rahimpour, M., Lovell, N. H., Celler, B. G., & McCormick, J. (2008). Patients'
SELF-‐MANAGEMENT & INFORMATICS 15
perceptions of a home telecare system. International Journal of Medical Informatics, 77(7), 486–498. doi:10.1016/j.ijmedinf.2007.10.006
Ryan, P., & Sawin, K. J. (2009). The Individual and family self-management theory: Background and perspectives on context, process, and outcomes. Nursing Outlook, 57(4), 217–225.e6. doi:10.1016/j.outlook.2008.10.004
Sanders, C., Rogers, A., Bowen, R., Bower, P., Hirani, S., Cartwright, M., et al. (2012). Exploring barriers to participation and adoption of telehealth and telecare within the Whole System Demonstrator trial: A qualitative study. BMC Health Services Research, 12. doi:10.1186/1472-6963-12-220
Schermer, M. (2009). Telecare and self-management: opportunity to change the paradigm? Journal of Medical Ethics, 35(11), 688–691. doi:10.1136/jme.2009.030973
Schulman-Green, D., Jaser, S., Martin, F., Alonzo, A., Grey, M., McCorkle, R., et al. (2012). Processes of self-management in chronic illness. Journal of Nursing Scholarship, 44(2), 136–144. doi:10.1111/j.1547-5069.2012.01444.x
Seto, E., Leonard, K. J., Cafazzo, J. A., Barnsley, J., Masino, C., & Ross, H. J. (2012). Perceptions and experiences of heart failure patients and clinicians on the use of mobile phone-based telemonitoring. Journal of Medical Internet research, 14(1). doi:10.2196/jmir.1912
Staggers, N., & Thompson, C. B. (2002). The evolution of definitions for nursing informatics: a critical analysis and revised definition. AMIA, 9(3), 255–261.
Stellefson, M., Chaney, B., Barry, A. E., Chavarria, E., Tennant, B., Walsh-Childers, K., et al. (2013). Web 2.0 chronic disease self-management for older adults: a systematic review. Journal of Medical Internet Research, 15(2), e35. doi:10.2196/jmir.2439
Vicente, K. (2003). The Human Factor: Revolutionizing the Way People Live With Technology. New York: Routeledge.
Westbrook, J. I., Braithwaite, J., Georgiou, A., Ampt, A., Creswick, N., Coiera, E., & Iedema, R. (2007). Multimethod evaluation of information and communication technologies in health in the context of wicked problems and sociotechnical theory. Journal of the American Medical Informatics Association, 14(6), 746–755. doi:10.1197/jamia.M2462
Wiles, J. L., Leibing, A., Guberman, N., Reeve, J., & Allen, R. E. S. (2012). The meaning of “aging in place” to older people. The Gerontologist, 52(3), 357–366. doi:10.1093/geront/gnr098
Woodend, A. K., Sherrard, H., Fraser, M., Stuewe, L., Cheung, T., & Struthers, C. (2008). Telehome monitoring in patients with cardiac disease who are at high risk of readmission. Heart & Lung : the Journal of Critical Care, 37(1), 36–45. doi:10.1016/j.hrtlng.2007.04.004
Woods, L. W., & Snow, S. W. (2013). The impact of telehealth monitoring on acute care hospitalization rates and emergency department visit rates for patients using home health skilled nursing care. Home Healthcare Nurse, 31(1), 39–45. doi:10.1097/NHH.0b013e3182778dd3
World Health Organization. (2011). Global status report on noncommunicable diseases 2010. Retrieved from: http://apps.who.int/iris/bitstream/10665/44579/1/9789240686458_eng.pdf
SELF-‐MANAGEMENT & INFORMATICS 16