
Mannosylated nanoparticulate carriers of rifabutin for alveolar targeting
Upload
chu-besanconCategory
view
0download
0
M A J O R A R T I C L E
Increased Incidence and Characteristics ofAlveolar Echinococcosis in Patients WithImmunosuppression-Associated Conditions
Adrien Chauchet,1,2 Frédéric Grenouillet,1,5,a Jenny Knapp,1,5,a Carine Richou,1 Eric Delabrousse,1 Charlotte Dentan,3
Laurence Millon,1,5 Vincent Di Martino,1,6 Remy Contreras,4 Eric Deconinck,2,7 Oleg Blagosklonov,1,8
Dominique A. Vuitton,1,9 and Solange Bresson-Hadni1,5; for the FrancEchino Networkb
1WHO Collaborating Centre for Prevention and Treatment of Human Echinococcosis, and French National Reference Centre on Alveolar Echinococcosis,Franche-Comté University and University Hospital, and 2Department of Hematology, University Hospital, Besançon; 3Department of Internal Medicine,University Hospital, Grenoble; 4Department of Pharmacy, Hospital of Belfort-Montbéliard, Belfort; 5UMR 6249 ‘Chrono-environment,’ 6EA 4266 ‘Pathogensand inflammation,’ 7UMR 1098 ‘Graft-tumor-host interactions and cell and tissue engineering,’ 8EA 4662 ‘Nanomedicine, imagery, therapeutics,’ and9EA 3181 ‘Epithelial carcinogenesis; preventive and predictive factors,’ Franche-Comté University, Besançon, France
Background. An increased incidence of alveolar echinococcosis (AE) in patients with immunosuppression (IS)has been observed; our aim was to study this association and its characteristics.
Methods. Fifty AE cases with IS-associated conditions (ISCs) before or at AE diagnosis were collected from theFrench AE registry (1982–2012, 509 cases). There were 30 cancers, 9 malignant hematological disorders, 14 chronicinflammatory diseases, 5 transplants, and 1 case of AIDS; 9 patients had ≥2 ISCs. Characteristics of the 42 IS/AEcases and the 187 non-IS/AE cases diagnosed during the period 2002–2012 were statistically compared.
Results. There was a significant increase in IS/AE cases over time. Risk factors did not differ between IS/AE andnon-IS/AE patients. However, AE was more frequently an incidental finding (78% vs 42%) and was diagnosed at earlierstages (41% vs 23%) in IS/AE than in non-IS/AE patients. Serology was more often negative (14% vs 1%) and treatmentefficacy was better (51% regression after 1-year treatment vs 27%) in IS/AE patients. All IS/AE patients but 7 took ISdrugs; 7 received biotherapeutic agents. When not concomitant, AE occurred in IS patients within a 48-month mediantime period. Atypical presentation and abscess-, hemangioma-, and metastasis-like images delayed AE diagnosis in 50%of IS/AE patients, resulting in inappropriate treatment. Liver images obtained for 15 patients 1–5 years before diagnosisshowed no AE lesions. Albendazole efficacy was good, but 19 of 48 treated patients experienced side effects.
Conclusions. Patients with immunosuppression are at increased risk for occurrence, delayed diagnosis, and pro-gression of AE.
Keywords. Echinococcus multilocularis; cancer; biotherapy; liver abscess; liver metastases.
Alveolar echinococcosis (AE), a zoonosis caused by thegrowth of the Echinococcus multilocularis metacestode,mimics slow-growing liver cancer. The curative treat-ment is surgical resection associated with a 2-year
administration of albendazole (ABZ). Patients who arenot eligible for surgery must take ABZ for life, riskingsevere side effects [1].AE occurs inWestern and CentralEurope, Central Asia, western and central China, Alaska,and Japan [2]. It is a rare disease in Europe, but its yearlyincidence has more than doubled over the last 10 years[2–5]. Cases are now being found in Central Europeand the Baltic region [4, 6], and the emergence of animalinfection has been reported in the United States andCanada [7–9].
The influence of immunosuppression (IS) on E. mul-tilocularis development has been demonstrated in ex-perimental hosts [10], in liver-transplanted patientswith AE, and in patients with AIDS [3, 11, 12]. Cases
Received 16 December 2013; accepted 30 June 2014; electronically published 16July 2014.
aF. G. and J. K. contributed equally to this work.bThe FrancEchino network members are listed in the Acknowledgments.Correspondence: Dominique A. Vuitton, MD, PhD, WHO Collaborating Centre for
Prevention and Treatment of Human Echinococcosis, Department of Parasitology,Jean Minjoz University Hospital, 25030 Besançon, France ([email protected]).Clinical Infectious Diseases 2014;59(8):1095–104© The Author 2014. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/cid/ciu520
Echinococcosis and Immune Suppression • CID 2014:59 (15 October) • 1095
at INSE
RM
on June 7, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

of AE have also been reported in patients receiving immuno-suppressive therapy for malignant and inflammatory diseasesor after transplant [13–18]. Data on the incidence and clinicalpresentation of AE in immunosuppressed patients are limited.We accessed the French AE registry, a population-based, case-recording system with the highest number of well-documentedcases ever recorded over the last 3 decades [19], to collect AEcases diagnosed in patients with IS-associated conditions(ISCs), labeled here “IS/AE,” and compare them with non-IS/AE patients.
MATERIALS AND METHODS
Patient SelectionThe FrancEchino Registry [3], approved by French ethical com-mittees, has recorded all French AE cases since 1982 [19, 20],following the recommendations of the World Health Organiza-tion (WHO) Informal Working Group on Echinococcosis(IWGE) [21]. All patients gave us their informed consent.
We collected AE cases recorded from 1 July 1982 to 30 June2012 in patients who, before or at time of AE diagnosis, present-ed with chronic (>6 months’ duration) inflammatory/autoim-mune diseases (CIDs), AIDS, solid organ or hematopoieticstem cell transplant, solid organ cancer, and malignant hemato-logical disorders. Patients with liver transplant for AE or ISCdiagnosed >6 months after AE diagnosis were excluded. Datawere compared using χ2 and Fisher exact tests.
Comparison of Epidemiological DataMedian age, sex ratio, agricultural activity/occupation, numberof at-risk activities (hunting, contact with foxes, consumption ofraw berries and vegetables, ownership of a garden/dogs), andresidence in at-risk areas [22], recorded from 1982 to 2012,were compared in IS/AE and non-IS/AE patients.
Comparison of Clinical DataTo guarantee data reliability, given that 84% of IS/AE patients(42 patients) were observed during this period, we comparedthe following parameters recorded prospectively in IS/AE andnon-IS/AE patients from 1 July 2002 to 30 June 2012: (1) Echi-nococcus species serology at diagnosis—positive if at least 1of the following tests was above the threshold: indirect hemag-glutination (IHA) (Fumouze Diagnostics, Levallois-Perret,France), and/or enzyme-linked immunosorbent assay (ELISA)using crude Echinococcus species extracts, Em2plus ELISA (Bor-dier Affinity Products, Crissier, Switzerland), and/or Westernblotting (EmWB) (LD BIO Diagnostics, Lyon, France) [23].(2) PNM (P: parasite location, N: neighboring structure in-volvement, M: metastases) staging according to WHO-IWGE [24], and presence/absence of liver calcifications.Liver lesion sizes are not recorded in the database and thus
were not compared. Ultrasound (US) and computed tomogra-phy (CT) were performed in all patients annually. Magneticresonance imaging (MRI) was performed on selected patientsdepending on diagnostic or therapeutic difficulties. (3) Courseof AE lesions on conventional imaging, assessed as follows:“recurrence/no recurrence,” after radical resection, “regres-sion” (decreased size and increased percentage of calcifica-tion), “progression” (increase in size and/or extension toneighboring organs and/or metastases), “stabilization” (nochange in lesions) [24]. (4) Number of IS/AE patients who un-derwent surgery and, among them, those with complete lesionresection. Because benzimidazole side effects are not system-atically recorded in the database, they were not statisticallycompared.
Data Collected on IS/AE Patients OnlyAdditional data were collected from patients’ physicians. Bloodliver tests, serum C-reactive protein (CRP), blood count, andserology were recorded for IS/AE patients at diagnosis, 3 and6 months after diagnosis, then every 6 months. When diagno-sis was difficult, polymerase chain reaction (PCR) was per-formed on lesion samples using E. multilocularis–specificDNA probes [25]. Retrospective serology was performed onsera sampled before AE diagnosis whenever available in a bio-bank. Retrospective imaging was reviewed by a radiologist withexpertise in AE.
After 2003, 18F-fluorodeoxyglucose positron emission to-mography (FDG-PET) combined with CT was performed1 hour after FDG injection for 26 IS/AE patients to assess AE“metabolic activity.” After July 2007, for 17 patients, it includeddelayed image acquisition [26]. Yearly evaluation categories ofFDG uptake were “increased,” “unchanged,” “decreased,” and“absent.”
Patients received ABZ (10–15 mg/kg/day, continuously), ormebendazole (4.5 g/day) when ABZ side effects occurred.Whenever difficulties in patient management appeared, ABZsulfoxide plasma levels were measured 4 hours after morningdrug intake. Benzimidazole side effects were recorded for allIS/AE patients.
ISC Diagnosis and Follow-upData on diagnosis, follow-up, and treatment of the underlyingdisease(s), including IS drugs administered, were carefullyrecorded.
RESULTS
Epidemiological CharacteristicsOf the 509 AE cases recorded from 1 July 1982 to 30 June 2012,50 IS/AE cases were observed (first case in 1988). There was asignificant increase in AE incidence in IS/AE patients. From
1096 • CID 2014:59 (15 October) • Chauchet et al
at INSE
RM
on June 7, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

1992 to 2012 the progression rate was higher than in non-IS/AEcases (Figure 1; P < .001). There was no overall significant
difference between IS/AE and non-IS/AE patients regardingage (65.5 years vs 60.0 years; P = .86), sex (P = .90), risk factors(P = .90), or geographical area of residence (P = .90) (Supple-mentary Figure 1).
Comparison of IS/AE and Non-IS/AE Patient ClinicalCharacteristics From 2002 to 2012In the 42 IS/AE patients, compared with the 187 non-IS/AE pa-tients, AE was more frequently an incidental finding (78% vs42%, P < .001), specific serology was more often negative(14% vs 1%, P = .001), and PNM localized stages (stages I–II)more frequent (41% vs 23%, P < .035). Prevalence of metastaseswas not significantly different. Liver calcifications were observedin 52% of IS/AE vs 61% of non-IS/AE patients. The differencewas not significant (P = .36). Thirty-three percent of IS/AE pa-tients underwent operations vs 40% of non-IS/AE patients(P = .46). The percentage was the same in both groups for rad-ical resection (85%). Remarkably, regression under benzimida-zole therapy after 1 year of follow-up was significantly moreoften observed in IS/AE patients (51% vs 27%, P < .004). All 8deaths in IS/AE patients were due to ISCs, and none to AE; 3 of
Figure 1. Significant increase in the incidence of alveolar echinococco-sis in patients with immunosuppression (IS/AE) compared with non-IS/AEpatients from the FrancEchino database over the last 3 decades (1982–1992 vs 1992–2002, P < .05; 1982–1992 vs 2002–2012, P < .01; 1992–2002 vs 2002–2012, P < .01). Abbreviation: AE, alveolar echinococcosis.
Figure 2. Characteristics of immunosuppression-associated conditions (ISCs) in 50 patients with alveolar echinococcosis from the FrancEchino registry.Number of patients with ISCs are shown. Stripes indicate associated ISC in the same patients. In addition, 1 patient had myeloma + prostate cancer, 1 hadlymphoma + colorectal cancer, and 1 had Hodgkin disease + colorectal cancer. Abbreviations: IgA, immunoglobulin A; ISC, immunosuppression-associatedconditions; MHD, malignant hematological disorder.
Echinococcosis and Immune Suppression • CID 2014:59 (15 October) • 1097
at INSE
RM
on June 7, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

187 non-IS/AE patients (1.6%) died from AE complications.The difference was not significant.
Clinical Characteristics of IS/AE PatientsAssociated ISCs were mostly cancer, followed by CIDs; 2 ISCswere diagnosed in 9 cases (Figure 2). Diagnosis of ISC and AEwas concomitant in 16 patients (mainly with cancer). When notconcomitant, median time between ISC diagnosis and AE was48 months (range: 0–288) (Table 1). It was longer for CIDs (88months [range: 54–288]) than for cancer (30 months [range: 0–204]). Of 49 non-AIDS patients, only 7 had no IS therapy: 5 hadcancer surgery only, and 2 had advanced stages of cancer. Me-dian duration of IS therapy was 54 months. Combined chemo-therapy was most frequent, followed by corticosteroids andother IS drugs (Supplementary Figure 2). Twenty patients re-ceived ≥2 IS drugs; 7 received biotherapeutic agents.
AE diagnosis was an incidental finding in abdominal imagingin 26 patients, in liver tests in 8, on both in 4, and during lap-arotomy in 4 (Table 1); incidental diagnosis was more frequentin cancer patients. Four patients presented with unusual acuteliver abscess–like symptoms with acute pain and fever (Table 1),2 presented with pulmonary symptoms, and 1 AIDS patient hadprolonged cholestasis. At diagnosis, liver tests were abnormal in22 patients (cholestasis in 18, cytolysis in 10), C-reactive proteinwas high in 16 patients (9 with CID), lymphopenia <1500 cells/µL was observed in 14 patients, and <700 cells/µL in 5. All 4 pa-tients with abscess-like presentations were lymphopenic. Therewas no significant difference in PNM stages between patientswith and without lymphopenia.
Hepatic lesions (median size, 53 mm [range: 15–210]) werein the right lobe in 21 patients, left lobe in 7, and in bothlobes in 22; 50% of patients had 2–5 lesions. Lesion size was sig-nificantly larger (P = .03) in symptomatic patients. Regional in-vasion was observed in 5 patients and distant AE metastases (inthe lung, spleen, sacroiliac bone, retroperitoneal space, andmuscles) in 9 (Table 1). When comparing ISC types, no diffe-rence was found for PNM stage or size or number of lesions(P = .9). Increased FDG uptake was observed in the liver in allbut 1 patient who underwent PET/CT.
Delayed AE Diagnosis in IS/AE PatientsAfter the first AE symptom/image, diagnosis was delayed in 25of 50 IS/AE patients, more often in symptomatic (80%) than inasymptomatic patients (43%), due to unusual presentation, me-tastasis- or lymphoma-like lesions, negative serology and/orpathological exam, or concomitant opportunistic infection (as-pergillosis in 2 patients). Median delay was 5 months (2–72),and longer for transplant and CID patients (Table 1). IHA se-rology was negative in 65% of IS/AE patients at the 1:320 “diag-nostic” cutoff, and in 10% at the 1:80 “screening” cutoff [23].Em2plus ELISA was negative in 25%, and EmWB showed a Ta
ble1.
Clinical
Characteris
ticsof
50Pa
tients(1982–2012)W
ithAlveolar
Echinococcosis
andImmunosuppression-AssociatedCo
nditions
Type
ofISC,
No.
(%)
PNM
Class
ificatio
n,No.
(%)
Med
ianTime
Betwee
nISCan
dAE,m
o(Extreme
Values
)
Med
ianTimeof
Delay
toDiagn
osis,
mob
(Extreme
Values
)
Fortuitous
Diagn
osisa ,No.
(%)
Diagn
osis
onSigns
andSym
ptom
sa,N
o.(%
)
Stage 1
Stage 2
Stage 3
Stage 4
Type
ofISC,
No.
(%)
Surge
ryIm
aging
Biology
cTy
peof
ISC,
No.
(%)
Abs
cess/
Cho
lang
itis
LD/Jau
ndice,
Pruritus
,and
/or
PH
Abd
ominal
Pain
Impa
ired
Clinical
Status
Hep
atom
egaly
Solid
canc
er,3
0(60)
20(67)
1(3)
3(10)
6(20)
5(0–20
4)5(2–72
)Solid
canc
er,2
5(83)
4(16)
20(80)
2(8)
Solid
canc
er,5
(17)
2(40)
5(100
)3(60)
3(60)
2(40)
Maligna
nthe
matolog
ical
diso
rders,
9(18)
8(89)
1(11)
00
54(0–18
0)6(3–72
)Maligna
nthe
matolog
ical
diso
rders,
5(55)
04(80)
1(20)
Maligna
nthe
matolog
ical
diso
rders,
4(45)
1(25)
1(25)
1(25)
2(50)
2(50)
Chron
icinfla
mmatory
dise
ases
,14(28)
8(58)
1(7)
2(14)
3(21)
96(54–
288)
8(2–8)
Chron
icinfla
mmatory
dise
ases
,9(64)
06(67)
5(55)
Chron
icinfla
mmatory
dise
ases
,5(36)
2(40)
2(40)
1(20)
4(80)
1(20)
Tran
splant,5
(10)
4(80)
1(20)
00
84(12–
180)
11(3–19
)Tran
splant,5
(100
)0
4(80)
1(20)
Tran
splant,0
...
...
...
...
...
AIDS,1
(2)
1(100
)0
00
120
0AIDS,1
(100
)0
01(100
)AIDS,0
...
...
...
...
...
2as
sociated
ISCs,
9(18)
9(100
)0
00
78(12–
180)
6(3–72
)2as
sociated
ISCs,
7(78)
06(86)
2(29)
2as
sociated
ISCs,
2(22)
1(50)
1(50)
1(50)
1(50)
0
Total,50
(100
)31
(62)
5(10)
5(10)
9(18)
48(0–28
8)5(2–72
)To
tal,38
(76)
4(10)
26(68)
8(22)
Total,12
(24)
4(30)
7(55)
5(42)
8(60)
4(30)
Abb
reviations
:AE,alve
olar
echino
cocc
osis;ISC,im
mun
osup
pres
sion
-ass
ociatedco
ndition
;LD
,liver
dysfun
ction,
PH,po
rtal
hype
rten
sion
;PNM,P:pa
rasite
locatio
n,N:ne
ighb
oringstructureinvo
lvem
ent,M:
metastase
s.aAEdiag
nosismight
beba
sedon
imag
ingan
dbiolog
y.bWhe
neve
rAEan
dISCdiag
nose
swereno
tco
ncom
itant.
cAbn
ormal
liver
tests.
1098 • CID 2014:59 (15 October) • Chauchet et al
at INSE
RM
on June 7, 2015http://cid.oxfordjournals.org/
Dow
nloaded from
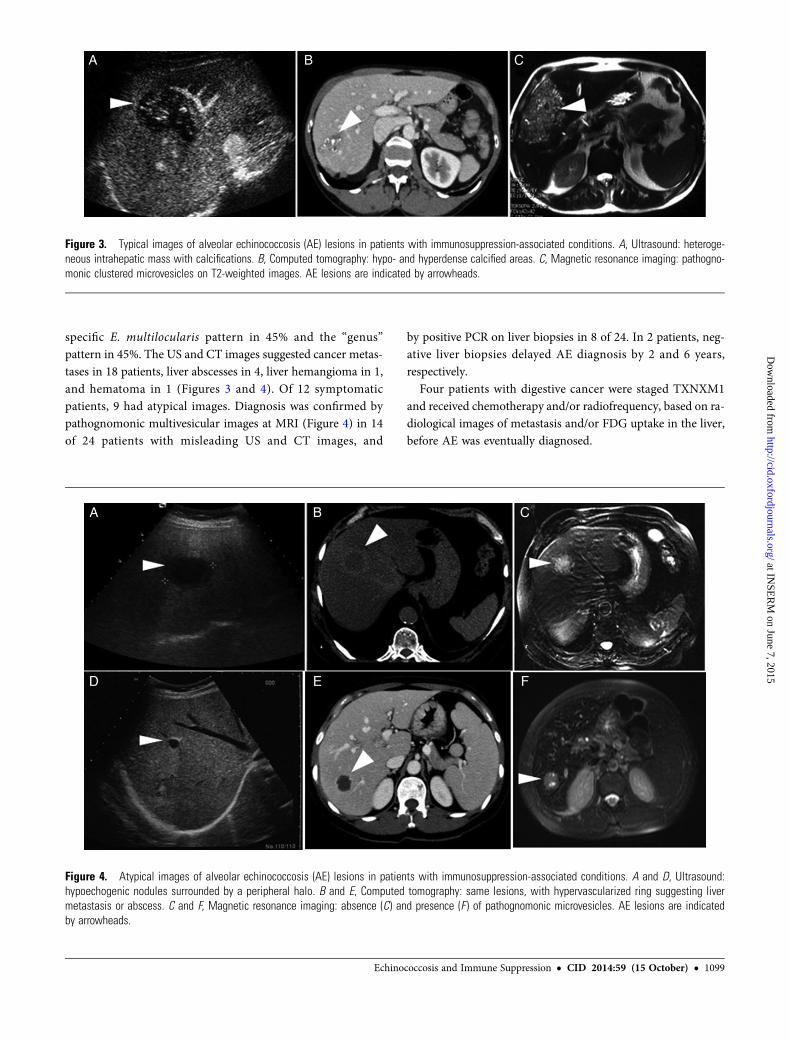
specific E. multilocularis pattern in 45% and the “genus”pattern in 45%. The US and CT images suggested cancer metas-tases in 18 patients, liver abscesses in 4, liver hemangioma in 1,and hematoma in 1 (Figures 3 and 4). Of 12 symptomaticpatients, 9 had atypical images. Diagnosis was confirmed bypathognomonic multivesicular images at MRI (Figure 4) in 14of 24 patients with misleading US and CT images, and
by positive PCR on liver biopsies in 8 of 24. In 2 patients, neg-ative liver biopsies delayed AE diagnosis by 2 and 6 years,respectively.
Four patients with digestive cancer were staged TXNXM1and received chemotherapy and/or radiofrequency, based on ra-diological images of metastasis and/or FDG uptake in the liver,before AE was eventually diagnosed.
Figure 3. Typical images of alveolar echinococcosis (AE) lesions in patients with immunosuppression-associated conditions. A, Ultrasound: heteroge-neous intrahepatic mass with calcifications. B, Computed tomography: hypo- and hyperdense calcified areas. C, Magnetic resonance imaging: pathogno-monic clustered microvesicles on T2-weighted images. AE lesions are indicated by arrowheads.
Figure 4. Atypical images of alveolar echinococcosis (AE) lesions in patients with immunosuppression-associated conditions. A and D, Ultrasound:hypoechogenic nodules surrounded by a peripheral halo. B and E, Computed tomography: same lesions, with hypervascularized ring suggesting livermetastasis or abscess. C and F, Magnetic resonance imaging: absence (C) and presence (F ) of pathognomonic microvesicles. AE lesions are indicatedby arrowheads.
Echinococcosis and Immune Suppression • CID 2014:59 (15 October) • 1099
at INSE
RM
on June 7, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

Table 2. Type of Treatment, Imaging, and Serological Evolution After Treatment Including Albendazole Administration, in 48 Patients (1982–2012) With Alveolar Echinococcosisa andImmunosuppression-Associated Conditions
Type of AETreatment Imaging Serologyd
Type of ISC, No.
ABZ WithoutSurgery/
Surgerya + ABZ
18-FDG Uptake at PET/CTb Abdominal Imagingc (US, CT, MRI) Indirect Hemagglutination (Cutoff ≥80) Em2plus ELISA (Cutoff 0.6)
Unchanged Decreased Absent Increased Stabilization RegressionNo
Recurrence Progression Stable Decreased Negative Increased Stable Decreased Negative Increased
Solid cancer, 28 15/28/13/28
6/15 3/15 6/15 0/15 16/29 4/29 9/29 0/29 10/23 9/23 3/23 2/23 4/20 8/20 5/20 3/20
Malignanthematologicaldisorder, 9
9/9/0/9
2/4 1/4 1/4 0/4 4/9 5/9 0/9 0/9 2/7 5/7 0 0 1/8 4/8 2/8 1/8
Chronicinflammatorydisease, 14
9/14/5/14
4/8 1/8 3/8 0/8 8/14 4/14 2/14 0/14 2/11 9/11 0 0 0/12 3/12 7/12 2/12
Transplant, 5 3/5/2/5
1/1 0/1 0/1 0/1 0/5 0/5 5/5 0/5 . . . . . . . . . . . . 0/3 1/3 2/3 1/3
AIDS, 1 0/1/1/1
0/1 0/1 1/1 0/1 1/1 0/1 0/1 0/1 0/1 1/1 0/1 0/1 0/1 0/1 1/1 0/1
2 associated ISCs, 9 7/9/2/9
3/6 1/6 2/6 0/6 5/9 3/9 1/9 0/9 1/7 6/7 0/7 0/7 0/6 2/6 3/6 1/6
No. of patients/totalNo.c
32/48/16/48
12/26 5/26 9/26 0/26 25/47 11/47 12/47 0/47 13/36 20/36 2/36 1/36 5/37 13/37 12/37 7/37
Type of presentation, No. (%)
AE symptomaticpresentation,12 (24)
9/12 /3/12
3/10 3/10 4/10 0/10 6/12 3/12 3/12 0/12 3/8 3/8 1/8 1/8 1/9 2/9 5/9 1/9
AE asymptomaticpresentation,38 (76)
19/36/15/36
9/16 3/16 4/16 0/16 20/35 8/35 7/35 0/35 11/28 17/28 0/28 0/28 4/28 13/28 7/28 4/28
Type of AE treatment, No. (%)
Surgerya + ABZ,16 (32)
. . . 0/5 1/5 4/5 0/5 4/16 1/16 11/16 0/16 3/10 4/10 3/10 0/10 0/13 5/13 8/13 0
ABZ withoutsurgery, 32(64)
. . . 14/21 4/21 3/21 0/21 21/31 10/31 0/31 0/31 8/26 17/26 0/26 1/26 3/24 7/24 7/24 7/24
Abbreviations: 18-FDG, 18F-fluorodeoxyglucose; ABZ, albendazole; AE, alveolar echinococcosis; CT, computed tomography; ELISA, enzyme-linked immunosorbent assay; ISC, immunosuppression-associatedconditions; MRI, magnetic resonance imaging; PET, positron emission tomography; US, ultrasound.a Two patients with cancer and surgery alone, without ABZ treatment, are not shown in this table (the total number of patients is thus 48).b FDG-PET/CT was performed in 26 of the 50 patients with AE and ISC.c Because of the presence of patients with associated ISCs, the number of cases with each ISC is higher than the total number of patients.c Radiological follow-up was not available in 1 patient with cancer.d Serological follow-up is shown for those patients with positive serology at diagnosis, ie, 36 patients using indirect hemagglutination (follow-up using indirect hemagglutination was not performed in all 5 patients withtransplant), and 37 patients using Em2plus ELISA.
1100•
CID
2014:59(15
October)
•Chauchet
etal
at INSERM on June 7, 2015 http://cid.oxfordjournals.org/ Downloaded from

Retrospective Findings in IS/AE PatientsIn 7 seropositive patients, on sera sampled 1–5 years before AEdiagnosis, IHA and ELISA were negative, with a weak 7-kDaband for 3 sera collected 2 years before diagnosis.
All US, CT, and MRI liver images obtained for 15 patientswithin the 5 years before AE diagnosis were normal.
Treatment and Follow-up of IS/AE PatientsABZ was given to all patients but 2 with advanced cancer. Sur-gery was more frequently performed in patients with cancer(47%) or transplantation (40%) (Table 2). Response to treat-ment was favorable in 46 of 48 ABZ-treated patients (averagefollow-up, 44 months [range: 5–245]). FDG-PET images (42%vs 28%) and Em2plus serology (56% vs 25%) tested negativemore frequently in these patients (Table 2 and Figure 5). Imag-ing showed stabilization in 53%, regression in 23%, and no re-currence in 24%. Among nonoperated patients, stabilization orregression was observed in 68% and 32% of cases, respectively.If initially positive, FDG uptake at PET/CT did not change(67%), decreased (17%), or was absent (16%), but it never in-creased. Em2plus serology became negative in 1 of 3 cases(Table 2). ABZ side effects occurred in 19 of 48 patients: abdom-inal pain (n = 2), alopecia (n = 5), skin rash (n = 2), pruritus(n = 1), neutropenia (n = 3); alanine/aspartate aminotransferas-es increased by 2- to 10-fold (n = 14) compared with normal
values. Eleven patients with side effects had excessive ABZsulfoxide levels. ABZ dosage was consequently decreased in10 patients, replaced by mebendazole in 3 with subsequentswitching to ABZ at lower dosages, and interrupted in 1 patientwith neutropenia.
DISCUSSION
This report on 50 IS/AE patients from a population-based, na-tionwide registry of >500 patients argues strongly for the “oppor-tunistic” status of AE. It shows that ISCs affect AE presentation,make diagnosis more problematic, and lead to inappropriatetherapeutic interventions. ABZ rapidly stabilized AE, but thehigh side effect rate made patient care management moredifficult.
There was a significant increase in IS/AE case incidence after2000, and the difference was highly significant during the peri-od 1992–2012. There was no change in our prospective case-retrieval process, and we find it highly unlikely that this increasecould be related to earlier detection of AE cases because ofchanges in diagnosis procedures and follow-up of cancer orCID patients. US and CT exams have been widely availablethroughout France for the last 4 decades, and thanks to theFrench health insurance system, they are free of charge forall the above-mentioned patient types. Patient follow-up
Figure 5. Course of 18F-fluorodeoxyglucose (FDG) positron emission tomography combined with computed tomography imaging and Em2plusenyzme-linked immunosorbent assay serology in patients with immunosuppression-associated conditions and alveolar echinococcosis (AE) after albendazole treat-ment. A–C, Patient with systemic lupus and Burkitt lymphoma: abscess-like presentation. A, FDG uptake at presentation by 2 AE lesions. B, Dramaticdecrease of FDG uptake after 3 months of treatment. C, Concomitant decrease of serology. D–F, Patient with lymphoma in remission: fortuitous AE discoveryat follow-up. D, FDG uptake by segment VII AE lesion. E, Persistent FDG uptake after 4 years of treatment. F, No decrease of serology. AE lesions areindicated by arrowheads. Abbreviation: ABZ, albendazole.
Echinococcosis and Immune Suppression • CID 2014:59 (15 October) • 1101
at INSE
RM
on June 7, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

recommendations by the scientific/public health bodies havenot changed for the last 2 decades. We suggest that the increasewas most likely provoked by changes in therapeutic options inEurope. In France, the “First Cancer Plan,” launched in 2003[27], contained new therapeutic recommendations, includingintensified chemotherapy for patients with malignant disorders.This factor, plus the availability of biotherapeutic agents fortreatment of both cancer and CIDs, may have reinforced thetrend also observed in other European countries [16]. In ourstudy, 86% of IS/AE patients took IS drugs, 38 of 42 in thelast decade. The prolonged survival, and follow-up of cancer pa-tients using new imaging procedures, may also have played arole: 2 cases were found by FDG-PET/CT. Our inclusion criteriawere conservative. We excluded occurrence of ISCs after AE di-agnosis [12, 28], and we could have included conditions such askidney and liver dysfunction, diabetes, or malnutrition. Howev-er, the variety of IS levels would have hampered data analysisand posed the risk of overestimation. Immunosuppression cov-ers a broad spectrum, and further studies will enable AE referralcenters to better characterize AE courses for each type of con-dition in the future. Epidemiological characteristics were similarto those observed in non-IS/AE patients. This is not surprising,as E. multilocularis infection is linked to geographical, environ-mental, and behavioral factors. Also, the median age at diagno-sis of ISCs and AE is similar [3, 22]. More severe AE wasobserved in patients with lymphopenia, combined IS drug reg-imens, and/or biological agents. AE is the first cestode infectionever reported to be associated with tumor necrosis factor (TNF)inhibitors [17, 18]. TNF control of E. multilocularis by its hostshas been solidly demonstrated [10]. Clinicians should thus bealerted to AE occurrence, and E. multilocularis should beadded to the list of biotherapy-associated opportunistic organ-isms [29]. Rituximab-induced B-cell depletion may have con-tributed to the patient’s negative serology, as reported in arenal transplant recipient [16]. Our 5 cases confirm AE occur-rence after any allotransplant: not just in liver-transplanted AEpatients [30].
In immunocompetent hosts, the specific date of infection isnearly always unknown, but a 10- to 15-year interval is assumedbetween infection and symptoms [1]. Absence of AE lesions atimaging and negative serology during the 5 years before diagno-sis are suggestive of accelerated parasite growth and/or recentinfection. However, presence of an “Echinococcus” band at7 kDa in 3 of our “retrospective” sera suggests, as described inAIDS for a variety of opportunistic diseases [31], a prolonged,latent, lesion-free period between infection and diagnosis.Low PNM stages, “acute” presentation, and atypical imagesmay indicate rapid metacestode growth and/or its early diagno-sis in IS/AE patients. We previously described hemangioma-likelesions as “early” AE [11, 32]. The already reported [17] unusualabscess-like presentation and images, never described before
for AE, could also indicate rapid growth, with limited cellularimmune response and fibrosis [16]. Our 4 cases were observedin patients with severe IS. Metastasis-like lesions, also unusual,delayed AE diagnosis and led to erroneous, anticancer treat-ment. The variety of clinical presentations, atypical images,and negative serology definitely made AE diagnosis difficultin IS patients. IHA serology with a screening cutoff of 1:80[23] combined with EmWB, which takes all Echinococcus spe-cies bands into account, may improve diagnosis efficiency. Thecurrent recommendations for diagnostic serology should thusbe modified to take this situation into account [21]. In specificcases, when MRIs are not pathognomonic and pathologicalexams are inconclusive, specific immunostaining [33] and/orPCR performed on lesion biopsies should be used to rapidly as-certain diagnosis and avoid incorrect and potentially damagingtreatment.
The similar percentages and high rates of success in IS/AEand non-IS/AE patients who underwent surgery show that thecombination of surgery plus ABZ is feasible and efficient. IStherapy should be decreased whenever possible; this was suc-cessfully done in 7 cases. All studies on AE patient series haveshown that clinical improvement and changes in AE lesionswith ABZ alone are usually slow [1, 34]. In our series of IS/AE patients, clinical improvement was fast and impressive,with rapid disappearance of FDG uptake. This could be relatedto enhanced local ABZ bioavailability due to fast-developing,nonfibrotic AE lesions, but should be assessed by drug measure-ment and pathology studies. Given the structure of the FrancEchino database, we were unable to statistically compare ABZside effects in IS and non-IS/AE patients. However, comparedwith our clinical practice and to the literature [1, 21], an unusu-ally high percentage of side effects was observed in our IS/AEpatients, including systemic hypersensitivity to ABZ. Severeleukopenia was probably partly due to associated malignanthematological disorders, and/or to the combined side effectsof IS drugs. Pharmacological interactions may explain frequ-ent ABZ overdosage: ABZ-sulfoxide monitoring would preventthis.
Because the proportion of patients with treatment-inducedimmunosuppression is increasing, along with E. multilocularisinfection risks [4–9], it is likely that the number of IS/AE pa-tients will also increase. There thus may be concern about theburden of AE in the general population, which may be higherthan assumed. All physicians in endemic areas should be madeaware of this new situation. Our data, which stress early AE de-tection and good response to ABZ, could easily lead to overop-timism regarding the management and prognosis of IS/AEpatients. However, in those patients with side effects, the cur-rent situation, with only 2 similar drugs to treat AE, is farfrom ideal, and the increased number of IS/AE patients maylead to therapeutic cul-de-sacs in the future. Long-term
1102 • CID 2014:59 (15 October) • Chauchet et al
at INSE
RM
on June 7, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

concomitant treatment of AE and the underlying disease(s)may be hazardous because of possible interference and cumula-tive side effects. For these reasons, proposing surgery whenevercomplete lesion resection is possible, to avoid long-term use ofABZ, seems a sensible option. Furthermore, intensified researchon the treatment of this still deadly, albeit orphan, disease isnecessary.
Supplementary Data
Supplementary materials are available at Clinical Infectious Diseases online(http://cid.oxfordjournals.org). Supplementary materials consist of dataprovided by the author that are published to benefit the reader. The postedmaterials are not copyedited. The contents of all supplementary data are thesole responsibility of the authors. Questions or messages regarding errorsshould be addressed to the author.
Notes
Acknowledgments. The FrancEchino network includes the followingmembers: Annecy: Virginie Vitrat. Besançon: Karine Bardonnet, BrigitteBartholomot, Isabelle Beurton-Chataigner, Oleg Blagosklonov, SolangeBresson-Hadni, Marie Pascale Brientini; Sylvie Cappelle, Remy Contreras,Eric Delabrousse, Vincent Di Martino, Philippe Evrard, Sophie Felix,Patrick Giraudoux, Frédéric Grenouillet, Bruno Heyd, Séverine Valmary-Degano, Jenny Knapp, Stéphane Koch, Georges Mantion, Laurence Millon,Francis Raoul, Carine Richou, Claire Vanlemmens, Dominique A. Vuitton,Lucine Vuitton. Bourg-en-Bresse: Patricia Prost. Charleville-Mézière:Claire Godet. Clermont-Ferrand: Armand Abergel, Jean Beytout, MoniqueCambon. Dijon: Jean François Besancenot, Bernadette Cusenier, PatrickHillon, Anne Minello. Grenoble: Odile Faure, Christian Letoublon.Lyon: Jérôme Dumortier, Olivier Guillaud, Christian Partensky, MejaRabodonirina, Martine Wallon. Marseille: Martine Piarroux. Metz: EricChatelain, Marc Johann, Jean-Jacques Raabe. Mulhouse: Daniel Sondag.Nancy: Alain Gerard, Lorraine Letranchant, Marie Machouart, JérômeWatelet. Paris: Olivier Farges, Didier Samuel. Reims: Cathy Chemla, JeanFrancois Delattre. Rodez: Bruno Guerin. Saint Ouen l’Aumône: MoniqueDebruyne. Strasbourg: Ahmed Abou-Bacar, Maxime Audet, Yves Hansmann,Nicolas Lefebvre. Thonon: Véronique Li. Vesoul: Blandine Alby-Lepresle.The authors gratefully acknowledge the invaluable help of Ms Lois Rose
for the revision of the manuscript; the help of Dr Sylvie Capelle and PhilippeEvrard in the collection of IS/AE cases from the database; and the efforts anddedication of all the health professionals involved in the diagnosis, follow-up, and treatment of the ISCs of the patients included in this study, and whoprovided the authors with complementary data on their patients: UniversityHospital, Besançon: Dr Etienne Daguindau and Dr Annie Brion, Depart-ment of Hematology; Prof. Xavier Pivot, Dr Laurent Cals, Departmentof Oncology; Prof. Daniel Wendling, Department of Rheumatology;Dr François Clément, Department of Thoracic Surgery; Prof. NadineMagy, Prof. Jean-Louis Dupond, and Dr Helder Gil, Department of InternalMedicine; Dr Nicolas Sailley, Department of Radiology; Dr Damien Mon-tange, Department of Clinical Pharmacology. University Hospital, Dijon:Prof. François Ghiringhelli, Department of Oncology. University Hospital,Strasbourg: Prof. Philippe Bachelier. University Hospital, Lyon: Prof.Emmanuel Morelon, Department of Kidney Transplantation; Dr Françoisand Pierre Biron, Department of Infectious Diseases and Oncology; Prof.Christian Ducerf, Department of Abdominal Surgery and Liver Transplan-tation. University Hospital Grenoble: Prof. Philippe Gaudin and RoselineMazet, Department of Rheumatology and Pharmaceuticals; Dr PatriciaPavese, Department of Infectious Diseases; Dr Danièle Maubon, Dr AntoinePrijent, Dr Nancy Sauvage, and Jean-Cyril Bourre, Departments of Imaging,Parasitology and Immunology; Vesoul Hospital: Dr Mathieu Miguet. BelfortHospital: Dr Francis Duchene; Besancon: Dr Benoit Auge and Dr Brigitte
Bartholomot; Annecy: Dr Bernadette Corront; and Epinal: Dr Aussedat.We also thank Florence Skana and Marie-Pierre Faivre for the retrospectiveanalysis of serology; Karine Bardonnet and Martine Piarroux for theirdedication in the maintenance of the FrancEchino Registry during the1997–2005 period; Prof. Patrick Giraudoux and Dr Francis Raoul for theirconstant support; and the members of the patients’ association, AIREA(Association pour l’information et la recherche sur l’échinococcose alvéolaire).Financial support. This work was supported by the French National
Institute for Disease Surveillance, which provides financial support to theFrancEchino network and the French Registry of Alveolar Echinococcosis.Potential conflicts of interest. All authors: No potential conflicts of
interest.All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to the con-tent of the manuscript have been disclosed.
References
1. Kern P. Clinical features and treatment of alveolar echinococcosis. CurrOpin Infect Dis 2010; 23:505–12.
2. Vuitton DA,Wang Q, Zhou HX, et al. A historical view of alveolar echi-nococcosis, 160 years after the discovery of the first case in humans:part 1. What have we learnt on the distribution of the disease and onits parasitic agent? Chin Med J (Engl) 2011; 124:2943–53.
3. Kern P, Bardonnet K, Renner E, et al. European echinococcosis registry:human alveolar echinococcosis, Europe, 1982–2000. Emerg Infect Dis2003; 9:343–9.
4. Romig T. Echinococcus multilocularis in Europe—state of the art. VetRes Commun 2009; 33(suppl 1):31–4.
5. Torgerson PR, Keller K, Magnotta M, Ragland N. The global burden ofalveolar echinococcosis. PLoS Negl Trop Dis 2010; 4:e722.
6. Bruzinskaite R, Marcinkute A, Strupas K, et al. Alveolar echinococcosis,Lithuania. Emerg Infect Dis 2007; 13:1618–9.
7. Catalano S, Lejeune M, Liccioli S, et al. Echinococcus multilocularis inurban coyotes, Alberta, Canada. Emerg Infect Dis 2012; 18:1625–8.
8. Peregrine AS, Jenkins EJ, Barnes B, et al. Alveolar hydatid disease (Echi-nococcus multilocularis) in the liver of a Canadian dog in British Co-lumbia, a newly endemic region. Can Vet J 2012; 53:870–4.
9. Storandt ST, Kazacos KR. Echinococcus multilocularis identified inMichigan with additional records from Ohio. J Parasitol 2012; 98:891–3.
10. Vuitton DA, Gottstein B. Echinococcus multilocularis and its intermedi-ate host: a model of parasite-host interplay. J Biomed Biotechnol 2010;2010:923193.
11. Koch S, Bresson-Hadni S, Miguet JP, et al. Experience of liver transplan-tation for incurable alveolar echinococcosis: a 45-case European collab-orative report. Transplantation 2003; 75:856–63.
12. Kaplan JE, Benson C, Holmes KK, Brooks JT, Pau A, Masur H. Guide-lines for prevention and treatment of opportunistic infections inHIV-infected adults and adolescents: recommendations from CDC,the National Institutes of Health, and the HIV Medicine Associationof the Infectious Diseases Society of America. MMWR Recomm Rep2009; 58:1–207; quiz CE1–4.
13. Gruener B, Cretu C, Brunetti E, et al. Accelerated larval growth of Echi-nococcus spp. in the immunodeficient host? [abstract]. Am J Trop MedHyg 2008; 6:118.
14. Kayacan SM, Vatansever S, Temiz S, et al. Alveolar echinococcosis lo-calized in the liver, lung and brain. Chin Med J (Engl) 2008; 121:90–2.
15. Gaultier JB, Hot A, Mauservey C, Dumortier J, Coppere B, Ninet J.Granulomatous liver disease as the presenting feature of alveolarechinococcosis in an hepatitis C infected cardiac transplant patient[in French]. Rev Med Interne 2009; 30:812–5.
16. Geyer M, Wilpert J, Wiech T, et al. Rapidly progressive hepatic alveolarechinococcosis in an ABO-incompatible renal transplant recipient.Transpl Infect Dis 2011; 13:278–84.
17. Weiner SM, Krenn V, Koelbel C, Hoffmann HG, Hinkeldey K, Ockert D.Echinococcus multilocularis infection and TNF inhibitor treatment in
Echinococcosis and Immune Suppression • CID 2014:59 (15 October) • 1103
at INSE
RM
on June 7, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

a patient with rheumatoid arthritis. Rheumatol Int 2011; 31:1399–400.
18. Dentan C, Mazet R, Gilson M, Marchou-Lopez S, Gaudin P. Rheuma-toid arthritis, alveolar echinococcosis, and rituximab: a case report. JointBone Spine 2012; 79:325–7.
19. Piarroux M, Piarroux R, Giorgi R, et al. Clinical features and evolutionof alveolar echinococcosis in France from 1982 to 2007: results of a sur-vey in 387 patients. J Hepatol 2011; 55:1025–33.
20. Bresson-Hadni S, Vuitton DA, Bartholomot B, et al. A twenty-year his-tory of alveolar echinococcosis: analysis of a series of 117 patients fromeastern France. Eur J Gastroenterol Hepatol 2000; 12:327–36.
21. Brunetti E, Kern P, Vuitton DA. Expert consensus for the diagnosis andtreatment of cystic and alveolar echinococcosis in humans. Acta Trop2010; 114:1–16.
22. Piarroux M, Piarroux R, Knapp J, et al. Populations at risk for alveolarechinococcosis, France. Emerg Infect Dis 2013; 19:721–8.
23. Bart JM, Piarroux M, Sako Y, et al. Comparison of several commercialserologic kits and Em18 serology for detection of human alveolar echi-nococcosis. Diagn Microbiol Infect Dis 2007; 59:93–5.
24. Kern P, Wen H, Sato N, et al. WHO classification of alveolar echinococ-cosis: principles and application. Parasitol Int 2006; 55(suppl):S283–7.
25. Georges S, Villard O, Filisetti D, et al. Usefulness of PCR analysis fordiagnosis of alveolar echinococcosis with unusual localizations: twocase studies. J Clin Microbiol 2004; 42:5954–6.
26. Caoduro C, Porot C, Vuitton DA, et al. The role of delayed 18F-FDGPET imaging in the follow-up of patients with alveolar echinococcosis.J Nucl Med 2013; 54:358–63.
27. French National Cancer Plan 2003–2007. Available at: http://www.plan-cancer.gouv.fr/images/stories/fichiers/Historique/Plan_cancer_2003-2007_MILC.pdf. Accessed 21 February 2014.
28. Dunn GP, Bruce AT, Ikeda H, Old LJ, Schreiber RD. Cancer immunoe-diting: from immunosurveillance to tumor escape. Nat Immunol 2002;3:991–8.
29. Nam JL, Winthrop KL, van Vollenhoven RF, et al. Current evidence forthe management of rheumatoid arthritis with biological disease-modifying antirheumatic drugs: a systematic literature review informingthe EULAR recommendations for the management of RA. Ann RheumDis 2010; 69:976–86.
30. Kern P, Gruner B, Wahlers K. Diagnosis and course of echinococ-cocal diseases in the transplant setting. Transpl Infect Dis 2011;13:217–21.
31. Brooks JT, Kaplan JE, Holmes KK, Benson C, Pau A, Masur H. HIV-associated opportunistic infections—going, going, but not gone: thecontinued need for prevention and treatment guidelines. Clin InfectDis 2009; 48:609–11.
32. Bresson-Hadni S, Delabrousse E, Blagosklonov O, et al. Imaging aspectsand non-surgical interventional treatment in human alveolar echino-coccosis. Parasitol Int 2006; 55(suppl):S267–72.
33. Barth TF, Herrmann TS, Tappe D, et al. Sensitive and specific immuno-histochemical diagnosis of human alveolar echinococcosis with themonoclonal antibody Em2G11. PLoS Negl Trop Dis 2012; 6:e1877.
34. Kadry Z, Renner EC, Bachmann LM, et al. Evaluation of treatment andlong-term follow-up in patients with hepatic alveolar echinococcosis.Br J Surg 2005; 92:1110–6.
1104 • CID 2014:59 (15 October) • Chauchet et al
at INSE
RM
on June 7, 2015http://cid.oxfordjournals.org/
Dow
nloaded from
Copyright © 2022 FDOKUMEN




















