
Sirolimus for Treatment of β-Thalassemia: From Pre-Clinical ...
Upload
independentCategory
view
1download
0
Sirolimus-Based Immunosuppression for LiverTransplantation in the Presence of Extended Criteria for
Hepatocellular CarcinomaNorman M. Kneteman,1 Jose Oberholzer,1 Mohammed Al Saghier,1
Glenda A. Meeberg,1 Maurice Blitz,1 Mang M. Ma,2 Winnie W.S. Wong,2
Klaus Gutfreund,2 Andrew L. Mason,2 Larry D. Jewell,3 A.M. James Shapiro,1
Vincent G. Bain,2 and David L. Bigam1
An increasing number of patients with hepatocellular car-cinoma (HCC) are undergoing evaluation for listing forliver transplantation. Criteria for selection require ongo-ing review for suitability. A consecutive series of 40patients with HCC within the standard Milan criteria(single tumors n � 19 <5 cm, or up to 3 tumors <3 cm)and beyond (Extended Criteria; single tumors n � 21<7.5 cm, multiple tumors <5 cm) underwent liver trans-plant with a sirolimus-based immunosuppressive protocoldesigned to minimize exposure to calcineurin inhibitorsand steroids. At 44.3 � 19.3 months (mean � standarddeviation) follow-up, 1- and 4-year survivals (Kaplan-Meier) are 94.1 � 5.7% and 87.4 � 9.3%, in the Milangroup, respectively, and 90.5 � 6.4% and 82.9 � 9.3% inthe Extended Criteria group, respectively. Five patientsdied during follow-up, only 1 from recurrent HCC. Fivetumor recurrences have occurred at median 17 (mean22 � 17) months posttransplant, 1 in the Milan groupand 4 in the Extended Criteria group. Median survival inthe patients with recurrent tumor is 42 months (mean45 � 25), and the median postrecurrence survival is 15.5months (mean 23 � 16). The rate of patients who werealive and free of tumor at 1 and 4 years is 94.1 � 5.7% and81.1 � 9.9%, respectively, in the Milan group and is90.5 � 6.4% and 76.8 � 10.5%, respectively, in theExtended Criteria group. Five patients had sirolimus dis-continued for toxicity, while 24 of 35 surviving patientshave sirolimus monotherapy immunosuppression. Inconclusion, the Milan criteria for liver transplantationin the presence of HCC can be carefully extended with-out compromising outcomes. This sirolimus basedimmunosuppression protocol appears to have benefi-cial effects on tumor recurrence and survival with anacceptable rate of rejection and toxicity. (Liver Transpl2004;10:1301–1311.)
Early enthusiasm for liver transplantation as therapyfor patients with malignancy was tempered by high
rates of tumor recurrence, particularly in patients withadvanced tumors.1–3 Survival lagged behind that oftransplantation for other indications and led to concernthat malignancy may not be a suitable indication forliver transplantation.1
The experience of the Milan Tumor Institute with livertransplantation of patients with hepatocellular carcinoma(HCC) demonstrated that excellent long-term survival and
low rates of tumor recurrence could be achieved by strictcandidacy criteria. Mazzaferro et al.4 reported in 1996 thatpatients undergoing liver transplantation with a single HCCof 5 cm or less in diameter or up to 3 tumors of 3 cm or less indiameter who were immunosuppressed with standard cyclo-sporine / steroid immunosuppression could achieve long-term survival equal to other liver transplant patient groups.The Milan criteria have become guidelines for transplan-tation of patients with HCC in many countries, includingCanada. Excellent outcomes after liver transplantation forpatients with HCC within the Milan criteria have subse-quently been reported from other centers.5–8
Our initial experience with 9 consecutive patientstransplanted with HCC, in whom no recurrences wereseen, suggested that the criteria may be too restrictiveand that patients with more advanced disease may alsobenefit from liver transplantation. Other groups havefurther investigated the impact of tumor characteristicson tumor recurrence and patient survival.5,9,10 Amongvarious parameters that influence tumor-free survivalafter liver transplantation, steroid and calcineurin-inhibitor based immunosuppression has been shown tohave an adverse effect on recurrence of hepatic malig-nancies.6,11,12 In contrast, sirolimus had been reportedto have antitumor activity in malignant cell lines and inanimal models carrying human tumors.13–16
Abbreviations: HCC, hepatocellular carcinoma; CT, computedtomography.
From the 1Department of Surgery, Section of Hepatobiliary, Pancre-atic and Transplantation Surgery, 2Department of Medicine, Division ofGastroenterology, 3Department of Laboratory Medicine and Pathology,University of Alberta, Edmonton, Canada.
Supported solely by the University of Alberta and the Alberta LiverTransplant Program.
Address reprint requests to N.M. Kneteman, Department of Surgery,2D4.44 Walter C. Mackenzie Centre, Edmonton, Alberta T6G 2B7,Canada. Telephone: 1 780 407 6168; FAX: 1 780 407 7374; E-mail:[email protected]
Copyright © 2004 by the American Association for the Study ofLiver Diseases
Published online in Wiley InterScience (www.interscience.wiley.com).DOI 10.1002/lt.20237
1301Liver Transplantation, Vol 10, No 10 (October), 2004: pp 1301–1311

In December 1996, we initiated a prospective cohortevaluation of liver transplantation in patients withtumors meeting and extending beyond the Milan crite-ria in the context of a sirolimus-based immunosuppres-sive protocol (Tumor Protocol) that sought to mini-mize exposure to calcineurin inhibitors and steroids.
Patients and Methods
We carried out a pilot evaluation of outcomes for a consecutiveseries of 40 patients transplanted in the presence of HCC andimmunosuppressed with a sirolimus-based protocol. All patientstransplanted after December 1996 and documented to haveHCC were enrolled. Standard patient safety data were tracked,and specific attention was paid to laboratory evidence of toxicitypredicted to be associated with high-level sirolimus administra-tion. Tumor recurrence was evaluated with computed tomogra-phy (CT) (preferred) or ultrasound imaging and alpha-fetopro-tein levels on a semiannual basis during follow-up.
Outcome data on this consecutive cohort of patientstransplanted with HCC were entered prospectively into anelectronic patient record database (OTTR, Hickman-KenyonSystems, Omaha, NE) and analyzed retrospectively.
Inclusion Criteria
Guidelines for liver transplantation in the presence of HCC inCanada follow the Milan criteria of single tumors 5 cm or less in
diameter, or no more than 3 tumors of 3 cm or less in diameter.This pilot evaluation of transplantation in patients with HCCwith Extended Criteria was initiated with the support of theCanadian Liver Transplant Study Group. Inclusion criteria werebroadened to include patients with single tumors up to 7.5 cm indiameter or multiple tumors (no numerical restriction) up to 5cm in diameter. Diagnosis of HCC was made pretransplant byimaging studies, with biopsy performed in selected cases only.Standard screening of patients during evaluation was with ultra-sound and / or augmented CT and serum alpha-fetoprotein.Radiological confirmation of suspected malignancy was by typi-cal findings of arterial phase enhancement on triphasic CT withcontrast enhanced magnetic resonance imaging in selectedpatients. Metastatic work-up included chest X-ray or CT. Imag-ing was repeated at 3-month intervals while on the waiting list.All patients with tumors �5 cm in diameter underwent biopsy.The presence of grade III (poorly differentiated) tumors of morethan 5 cm in diameter led to exclusion of candidacy for trans-
Table 1. Demographics
Milan(n � 19)
ExtendedCriteria
(n � 21)
Mean age � SD (years) 53.67 � 7.42 52.97 � 7.24Gender (women/men) 4 / 15 2 / 19Race
Caucasian 12 17Oriental 5 3Asian Indian 1 0N. Am. Indian 1 0Other 0 1
Cause of liver disease:Hepatocellular liver disease
HCV(�EtOH/�HBV) 8 9HBV 6 6Alcoholic cirrhosis 3 5Cryptogenic cirrhosis 1 0
Cholestatic liver diseasePBC 1 0PSC 0 1
Abbreviations: HCV, hepatitis C virus infection; EtOH,alcoholic liver disease; HBV, hepatitis B virus infection; PBC,primary biliary cirrhosis; PSC, primary sclerosing cholangitis.
Table 2. Tumor Status at the Time of Transplantation
Milan(n � 19)
ExtendedCriteria
(n � 21)
StageI 3 0II 11 2III 2 6IV 3 13
Grade (WHO)I 4 7II 9 10III 6 4
Microvascular invasion 8 12Incidental tumor 9 4MELD (raw) 13.3 � 8.8 13.3 � 11.4MELD (tumor adjusted) 23.1 � 6.2 25.5 � 4.2Alpha-fetoprotein (ng/mL) 650 � 1121 265 � 542
(3–3300) (1–1800)Previous tumor treatment
Alcohol ablation 3 2Chemoembolization 0 2Liver resection 0 2
Abbreviations: WHO, World Health Organization; MELD,model for end-stage liver disease.Stage according to pTNM classification:17 Stage 1 �T1N0M0; Stage 2 � T2N0M0; Stage 3 � T1/2N1M0 or T3;Stage 4 � T4, any N, M0; T1 �2 cm without vascularinvasion; T2 � solitary �2 cm � vascular invasion or mul-tiple, one lobe, �2 cm without vascular invasion or solitary;T3 � solitary, �2 cm with vascular invasion or multiple, onelobe �2 cm with vascular invasion or multiple, one lobe, �2cm with or without vascular invasion; T4 � multiple, � onelobe or invasion of major branch of portal or hepatic vein;grade according to WHO definition (Grade I, well differen-tiated; Grade II moderately differentiated; Grade III, poorlydifferentiated).
1302 Kneteman et al.

plant, as did extrahepatic disease, nodal metastases, or evidence ofinvasion of major branches of the portal venous system or theinferior vena cava. Candidates found at laparotomy (when adonor liver became available) to have extrahepatic or nodalmetastases or disease beyond the extended criteria were excludedfrom transplantation and the cadaveric liver was utilized fortransplant of a backup candidate.
Histopathology
Explanted livers of recipients and in selected cases intraoper-ative biopsy material were examined by an experienced his-topathologist with documentation of tumor number, diame-
ter, grade, and presence or absence of microvascular /lymphatic invasion. Histology was reviewed by the senior liverpathologist (L.J.), blinded to the patient’s identity. Stagingwas assigned by the surgical / pathological team (J.O., G.M,L.J., and N.K.) on review of all available data according to the5th edition of the Tumor, Node, Metastasis / InternationalUnion Against Cancer criteria.17
Patient Characteristics and Groups
After histopathological review, patients presenting withtumors meeting the Milan criteria were assigned to the Milan
Figure 1. Box-plot of the number (A) and maximal size of tumors (B) found in the explanted liver of patients transplantedfor hepatocellular carcinoma within the Milan criteria or the Extended Criteria. C, D: The number and size of tumorsdetected by pretransplant imaging (CT-Scan) and the corresponding histopathology review of the explanted liver(Pathology). There was a mean time period of 78 � 49 days (range 6-181 days) between the CT scan and livertransplantation. The top, bottom, and line through the middle of the box correspond to the 75th percentile, 25thpercentile, and 50th percentile, respectively. The whiskers on the bottom extend from the 10th percentile and top 90thpercentile; ■ represents the arithmetic mean. Groups were compared with the Mann-Whitney U test (Milan vs. ExtendedCriteria) and the Wilcoxon signed ranks test (CT scan vs. Pathology), P < .05 indicates significant difference.
1303Sirolimus and Extended Criteria for HCC

group, patients presenting with tumors beyond the Milancriteria were assigned to the Extended Criteria group.
Between October 1989 and June 2003, 568 patientsreceived a total of 603 liver transplants at the University ofAlberta Hospital in Edmonton. A total of 51 of these patientswere confirmed to have HCC in their explanted livers. Thirty-two patients were found to have liver tumors during evalua-tion, which were confirmed on explant pathology to be HCC.An additional 19 patients were diagnosed only at explanthistopathology to have HCC (incidental tumors). Ninetumor patients were transplanted before initiation of this pilottrial.
Forty-two patients were transplanted between expansionof candidacy criteria in December 1996 and December 2002and were to receive the Tumor Protocol postoperatively. Onepatient with an incidental tumor was inadvertently excludedfrom the modified immunosuppressive protocol. One patientwas deemed to have a tumor of no significance by the attend-ing physicians and was entered into a separate multicentertrial of immunosuppression. One patient was noted to have atumor beyond the extended criteria on CT scan (tumor diam-eter of 7.8 cm) while on the waiting list, but proceeded totransplant.
Median follow-up of the 40 included patients (Table 1)was 42 months (mean 44.3 � 19.6 [standard deviation]months; range 17-88 months). No patient required retrans-plantation. No perioperative deaths (within 60 days)occurred.
Waiting Time
Tumor Protocol patients waited a median of 56 days fortransplant (mean 86 � 109 days). One patient with atumor � 5 cm in diameter was found to have a grade IIItumor on biopsy and was delisted. Three patients wereremoved from the transplant list due to tumor progression; nopatients died on the waiting list. One patient was found tohave metastatic tumor at laparotomy (despite negative preop-erative imaging) and did not undergo transplantation. Tumordirected therapy while awaiting transplantation (in Table 2)was utilized for 9 patients judged to be at risk of importanttumor advancement during the relatively short anticipatedwaiting period. As waiting time has increased in recent years(and especially so since this cohort was closed), an increasingproportion of patients have been so treated while waiting.
Transplant Procedure
At laparotomy, careful examination of the abdominal cavitywas performed to rule out extrahepatic tumor. All patientsunderwent complete hepatectomy and removal of the retro-hepatic inferior vena cava and orthotopic liver transplantationwith a cadaver donor organ. Mean transfusion was 3.6 � .7units of packed red blood cells (median 2 units). A total of 12patients did not require blood transfusion.
Immunosuppression
The protocol was approved by the University of AlbertaHealth Sciences Ethics Committee and the Canadian LiverTransplant Study Group. Individual patient consent wasobtained for transplantation and immunosuppressive ther-apy. Posttransplant immunosuppression was structured toreduce exposure to steroids and calcineurin inhibitors, and toachieve high target levels (12-20 �g/L) of sirolimus (Rapam-une, Wyeth Research Laval, Quebec, Canada). Initial accessto sirolimus was by compassionate release under specialapproval of the Health Protection Branch of Health Canada(Ottawa, Canada) and the manufacturer. Reduction of ste-roid and calcineurin inhibitors became more aggressive asexperience with the protocol grew. The first 10 patients weretreated with cyclosporine (Neoral, Novartis, Laval, Quebec,Canada) with a target level of 150 �g/L, while the latter 30patients received tacrolimus (Prograf, Fujisawa, Markham,Ontario, Canada) with a target whole blood level of 3–6�g/L. For the first 18 patients, solumedrol was administeredintravenously at a dose of 500 mg intraoperatively, with rapidtapering postoperatively to 20 mg/day by day 5 and completetapering by month 3 as tolerated. Calcineurin inhibitors weretapered to 0 as tolerated once steroid tapering was complete.The last 22 patients received a single dose of 2 mg/kg Dacli-zumab (Zenapax, Hoffman-LaRoche, Mississauga, Ontario,Canada) intraoperatively, with no protocol steroids at anypoint, and with tapering of calcineurin inhibitor beginning atmonth 2. The protocol aimed to achieve maintenance treat-ment with monotherapy sirolimus by month 3 to 6 posttrans-plant.
Antiviral Treatment
Patients with hepatitis B virus received posttransplant pro-phylaxis with lamivudine � hepatitis B immune globulin. Noroutine prophylaxis for hepatitis C virus was administered.
Statistical Analysis
Where appropriate, data were expressed as mean � standarddeviation. Overall survival and rate of survival in the absenceof tumor were calculated by the Kaplan-Meier method andfurther analyzed by log-rank tests. Disease-free survival wasdefined as the absence of recurrence of tumor or death of therecipient (related or unrelated to tumor recurrence). Tumorsize and number were compared between the Milan and theExtended Criteria group by means of the Mann-Whitney Utest. CT findings were compared to histopathology by theWilcoxon signed ranks test. Statistical significance wasdefined as a P value � .05. The SPSS 10.0 software package(SPSS, Chicago, IL) was used for the statistical analyses. Box-plots were generated with Delta-Graph 4.0.5 software (SPSS,Chicago, IL).
1304 Kneteman et al.

ResultsPatient demographics are summarized in Table 1. Atotal of 40 patients were enrolled into the cohort study;19 patients had tumors within the Milan guidelines(Milan group) while 21 patients were beyond the Milanguidelines (Extended Criteria group). Tumor extensionand histopathological evaluation is summarized in Fig-ure 1 and Table 2. All patients had at least 17 monthsfollow-up.
Pretransplant evaluation underestimated thenumber of patients having HCC; in 13 patients, the
tumor was found incidentally at the time of trans-plant or at histopathological evaluation. As indicatedin Figure 1c and d, histopathology of the explantrevealed more and larger tumors than found on thepretransplant CT. Seven of 17 patients (41%) pre-senting with tumors on CT within the Milan criteriawere found on histopathology of the explant to havetumors beyond the Milan criteria, but within theExtended Criteria, and were so analyzed initially. Asecond analysis was then performed using stagingfrom pretransplant imaging studies.
Figure 2. Kaplan-Meier survivalcurves after liver transplantation. A:Comparing the overall Edmontonseries with patients transplantedwith HCC and treated with steroid-free, sirolimus-based immunosup-pression, either within the Milancriteria or beyond the Milan criteria(Extended Criteria). P � .73 Milanvs. Extended. B: Rate of patientsthat were alive and free of tumorafter liver transplantation in thepresence of HCC within the Milancriteria or beyond (Extended Crite-ria) (events were defined as death ortumor recurrence) in comparison topatients presenting with fulminanthepatic failure and requiring venti-latory support. Differences in sur-vival curves were analyzed by log-rank test, P < .05 was consideredsignificant. P � .50 Milan vs.Extended. Status 4F, patient who isintubated and ventilated in ICU foracute liver failure.
1305Sirolimus and Extended Criteria for HCC

Nine patients received pretransplant antitumortherapy, as shown in Table 2. Two patients had under-gone previous surgical resection and presented withnew HCC in the remaining cirrhotic liver. Patientsselected for pretransplant therapy were those felt to beat high risk for early tumor progression and therefore athigh risk of being delisted.
Survival and Tumor Recurrence
One-year and 4-year survival for the Milan groupwere 94.1% � 5.7% (mean � standard error) and87.4 � 9.3%, respectively; for the Extended Criteriagroup these values were 90.5 � 6.4% and 82.9 �9.3%, respectively (log-rank test, P � .68) (Fig. 2).Five patients died during follow-up. The causes ofdeath are summarized in Table 3. Two patients hadrecurrent tumor at the time of death, 1 of whom diedfrom recurrent HCC. This patient presented withearly and extensive liver and lung metastasis 3months after transplantation. A CT scan, performed8 days before transplantation, had revealed a singletumor, 7.8 cm in diameter, despite interval alcoholablation. The patient was inadvertently left on thetransplant waiting list. The explant liver showed amoderately differentiated (grade II) tumor, 12.5 cmin diameter, without signs of vascular invasion orlymph node metastasis. The second patient withtumor recurrence at the time of death died of a myo-cardial infarction (sudden cardiac arrest). He hadbeen discovered to have several lung nodules of up to1 cm in diameter on CT of the chest at 17 monthsposttransplant. These tumors remained stable in sizeand number up to the time of his death in the com-munity 9 months later. Alpha-fetoprotein remainedin the normal range despite suspicion of tumor recur-rence. Alpha-fetoprotein had fallen from a preoper-ative value of 259 to 1 after transplant.
The rate of patients alive and free of tumor at 1
and 4 years for the Milan group were 94.1 � 5.7%(mean � standard error) and 81.1 � 9.9%, respec-tively; for the Extended Criteria group these valueswere 90.5 � 6.4% and 76.8 � 10.5%, respectively(log-rank test, P � .48). Five patients developedtumor recurrence during follow-up. One patient wasin the Milan group, but had microvascular invasionon explant histopathology; the other 4 patients werein the Extended Criteria group.
Tumors recurred at 3, 13, 17, 27, and 51 monthsposttransplant. Two patients died at 6 and 26 monthsposttransplant and are described above. The mediansurvival for the 5 patients with tumor recurrence iscurrently 42 months (mean 45.0 � 25.9 months; range6-88 months). The median survival time after tumorrecurrence is presently 15.5 months (mean 23.2 � 15.6months; range 3-51 months). One patient underwentresection of a 2.5 cm tumor in segments 2 and 3 of theliver at 13 months posttransplant and remains tumor-free at 63 months posttransplant, 50 months postresec-tion. A second patient underwent resection of recur-rence in a suprapancreatic lymph node at 27 monthsposttransplant and remains tumor-free 15 months later.The final patient developed multifocal hepatic and pul-monary recurrence at 51 months posttransplant. Whileno additional therapy beyond sirolimus was given, hehas survived his tumor recurrence for 37 months and isalive at 88 months posttransplant.
Microvascular Invasion, Grading, and TumorRecurrence
The only patient in the Milan group that developedtumor recurrence had evidence of microvascular inva-sion on histopathology. Although the study was notpowered for this, microvascular invasion did not influ-ence disease-free survival in patients in the ExtendedCriteria group (log-rank test, P � .23).
Table 3. Cause of Death
Cause of Death Time (mo) Tumor Status at Death Group
Recurrent HCV 4.5 Tumor-free MilanMetastatic HCC 6.5 HCC in lung and liver since 3 months post-tx Extended criteriaAsphyxia (choked on food) 10.1 Tumor-free Extended criteriaIntracerebral bleed 19.1 Tumor-free MilanMyocardial infarction 26.3 Lung nodules since 17 months post-tx Extended criteria
Abbreviations: HCV, hepatitis C virus infection; M, months; HCC, hepatocellular carcinoma; time, months after transplantation;post-tx, after transplantation; time, indicates time after transplantation.
1306 Kneteman et al.
Tumor grading is subjective and the final, blindedreview changed the grading performed by the initialpathologists in 12 of the 40 cases (30%). The tumorgrade did not significantly influence disease-freesurvival in the Milan group (log-rank test, P � .17)or the Extended Criteria group (log-rank test, P �.93).
Outcome Analysis by Pretransplant Stagingwith Imaging Studies
All patients were reclassified into the Milan or ExtendedCriteria groups on the basis of imaging studies availablepreoperatively. As such, all patients with incidentaltumors were excluded from this analysis. Of 27 patientsknown to have hepatoma before transplant, 18 werestaged as within the Milan criteria, and 9 patients asExtended Criteria patients. Survival at 1 and 4 years was100% and 92% for Milan patients, and 77.8% and77.8% for Extended Criteria patients. The rate ofpatients alive and free of tumor at 1 and 4 years was100% and 87.1% for Milan criteria patients, and77.8% and 62.2% for Extended Criteria patients,respectively.
Immunosuppressive Efficacy and Toxicity
A total of 18 episodes of acute rejection (all biopsyproven) occurred in 12 patients (30%) during the fol-low-up period (Table 4); 11 had a Banff criteria rejec-tion activity index of 3, with 3, 3, and 1 rejections eachat a rejection activity index of 4, 5, and 6, respectively.Increase in baseline immunosuppression reversed 9
rejection episodes. Steroid boluses were given in 10rejection episodes as directed by the attending clinician,typically for higher Banff gradings and / or during theearlier years of the study. There were no steroid-resis-tant rejections and no graft losses.
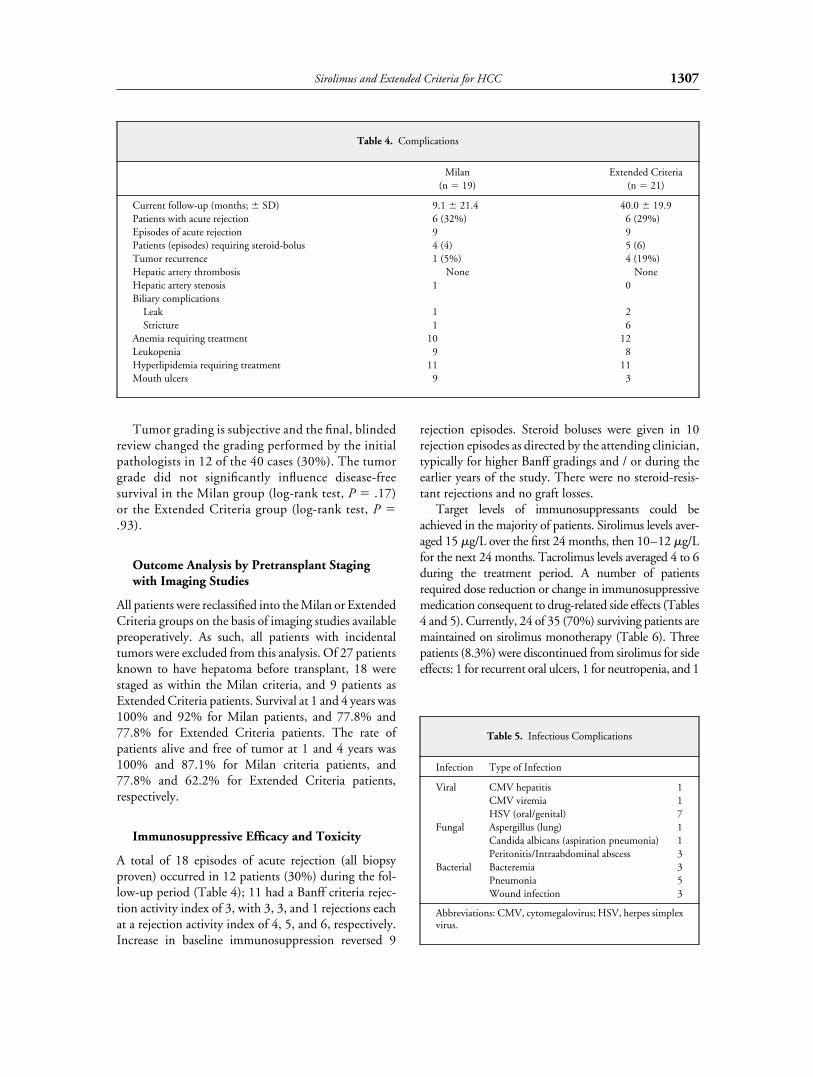
Target levels of immunosuppressants could beachieved in the majority of patients. Sirolimus levels aver-aged 15 �g/L over the first 24 months, then 10–12 �g/Lfor the next 24 months. Tacrolimus levels averaged 4 to 6during the treatment period. A number of patientsrequired dose reduction or change in immunosuppressivemedication consequent to drug-related side effects (Tables4 and 5). Currently, 24 of 35 (70%) surviving patients aremaintained on sirolimus monotherapy (Table 6). Threepatients (8.3%) were discontinued from sirolimus for sideeffects: 1 for recurrent oral ulcers, 1 for neutropenia, and 1
Table 4. Complications
Milan(n � 19)
Extended Criteria(n � 21)
Current follow-up (months; � SD) 9.1 � 21.4 40.0 � 19.9Patients with acute rejection 6 (32%) 6 (29%)Episodes of acute rejection 9 9Patients (episodes) requiring steroid-bolus 4 (4) 5 (6)Tumor recurrence 1 (5%) 4 (19%)Hepatic artery thrombosis None NoneHepatic artery stenosis 1 0Biliary complications
Leak 1 2Stricture 1 6
Anemia requiring treatment 10 12Leukopenia 9 8Hyperlipidemia requiring treatment 11 11Mouth ulcers 9 3
Table 5. Infectious Complications
Infection Type of Infection
Viral CMV hepatitis 1CMV viremia 1HSV (oral/genital) 7
Fungal Aspergillus (lung) 1Candida albicans (aspiration pneumonia) 1Peritonitis/Intraabdominal abscess 3
Bacterial Bacteremia 3Pneumonia 5Wound infection 3
Abbreviations: CMV, cytomegalovirus; HSV, herpes simplexvirus.
1307Sirolimus and Extended Criteria for HCC

for refractory hyperlipidemia. Two patients were discon-tinued for other reasons (i.e., access, cost).
Sirolimus dose reduction was necessary in 2 patientsbecause of mouth ulcers, in 6 patients because of per-sistent leukopenia, and in 6 patients because of anemia.Three patients had refractory leukopenia and requiredgranulocyte colony stimulating factor therapy. Erythro-poietin was given to 7 patients with persistent anemia;another 6 patients required blood transfusion; in 17patients iron supplementation was given. While notvery responsive to therapies such as erythropoietin, withtime, anemia resolved in all but 1 patient. A total of 22patients (55%) developed hyperlipidemia requiringtreatment with a lipid-lowering drug.
No patient developed hepatic artery thrombosis.
Discussion
Our series of 40 patients undergoing liver transplantwith or for HCC since 1996 provides insight into sev-eral ongoing controversies regarding the candidacy ofsuch patients for transplant and the influence of immu-nosuppression on tumor recurrence.
In our study, 19 patients had tumors within theMilan criteria; only 1 tumor recurrence was seen in thisgroup. Four of 21 patients transplanted with extendedtumor criteria presented with tumor recurrence. One-and 4-year overall and disease-free survival were notdifferent between the groups. Recent publications havequestioned the utility of the Milan criteria in stratifyingfor risk of posttransplant recurrence of HCC.6,18 Theoriginal Milan series4 contains a group of patients withmore advanced tumors. A total of 13 of their originalpatients qualified for transplantation by initial imagingstudies, but were found on examination of theexplanted liver to have more extensive disease. The4-year actuarial survival of these 13 patients was only50%. Three of their four tumor recurrences occurred inthese 13 advanced criteria tumor patients.
Molmenti et al.7 described the outcomes of 790patients with HCC reported to the InternationalTumor Registry in Liver Transplantation, and included23% of patients with tumors � 5 cm in diameter, and21% with vascular invasion. Four-year survival was47%, with approximately one-half of reported deathsassociated with tumor recurrence. In this registry anal-ysis, recurrence-free survival showed an inverse correla-tion with tumor size �5 cm, positive nodes, bilobarspread, and vascular invasion.7 In our study, the 1patient with recurrence in the Milan group had micro-vascular invasion.
We found a low sensitivity of pretransplant screen-ing with 13 patients diagnosed only on explant histo-pathology to have HCC. CT underestimated the num-ber and size of tumors; 7 of the 17 patients with CTfindings within the Milan criteria were found on histo-pathology to have Extended Criteria tumors. The dis-crepancy between CT and pathology findings are likelyrelated to low sensitivity and specificity of CT in thepresence of cirrhosis (especially in the earlier years ofthis study), as well as to tumor progression in the timebetween scanning and transplant. While no patientswith unrecognized disease beyond the extended criteriawere transplanted, we would recommend triphasic CTor augmented magnetic resonance imaging at 3-monthintervals while awaiting transplant with known HCCand at 6-month intervals for others at risk. Such at riskpatients include those with hepatitis B virus, hepatitis Cvirus, alcohol-associated cirrhosis, hemochromatosis,and cryptogenic cirrhosis.
Understaging of tumors of patients undergoing evalu-ation challenges the decision to offer liver transplant. Asimaging modalities have improved with advances in bothhardware and software, the accuracy of staging hasimproved significantly. Our initial experience with sub-stantial numbers of incidental tumors led to a requirementfor high quality triphasic CT (or magnetic resonanceimaging) for diagnosis and staging during evaluation andto greater attention to screening of patients awaiting trans-plant. These changes have been associated with a reduc-tion in the rate of undiagnosed (incidental) tumors from45% (5 / 11 tumors) during the period 1998–1999, to arate of 16% (4 / 25 tumors) since 2002.
Should patients whose livers contain tumors beyondthe Milan criteria be offered liver transplant with theongoing shortage of organs? These prospective candi-dates should be evaluated by the same criteria as others:the presence of life-threatening complications ofadvanced liver disease, and / or advanced symptomsthat reduce quality of life to the extent that the risk ofmortality and morbidity post– liver transplant is justi-
Table 6. Current Immunosuppression ofSurviving Patients
ImmunosuppressionMilan
(n � 17)
ExtendedCriteria
(n � 18)
Sirolimus monotherapy 11 13Sirolimus, tacrolimus 3 3Cyclosporine, mycophenolate mofetil 1 1Cyclosporine monotherapy 2 0Tacrolimus monotherapy 0 1
1308 Kneteman et al.

fied. Given the high rates of new tumor developmentafter successful local tumor treatment by resection19 orablation therapies,20,21 HCC certainly qualifies as a life-threatening complication of cirrhosis, equally as dan-gerous, while perhaps not as urgent, as variceal bleedingor spontaneous bacterial peritonitis. Given the presenceof a life-threatening complication, cirrhotic patientswith tumors beyond the Milan criteria should be eval-uated for candidacy on the likelihood that their short-and long-term outcomes will reach acceptable stan-dards. Our experience suggests many such patients canachieve long-term survival with liver transplantation.Four-year survival in our Extended Criteria tumorgroup was 82.9 � 9.3%, with a 4-year survival rate inthe absence of tumor of 76.8 � 10.5%. Both values arewell above our own and other published results withpatients transplanted for acute liver failure, a well-ac-cepted indication for liver transplantation.22 The sur-vival of the Extended Criteria tumor patients was sim-ilar to the overall survival of the 568 patientstransplanted since 1989 at our center. The presence ofunresectable tumor brought some of these patients totransplant before they developed major liver decom-pensation that might have been associated with lowerposttransplant survival and likely balances the adverseimpact of tumor recurrence on survival.
Such conclusions based on postresection histologicalstaging of patients has been criticized given that deci-sions on candidacy for transplantation must be made byimaging studies available during work-up. As such, wereanalyzed our outcomes according to staging assignedby review of imaging available before transplant. Bydefinition, all incidental tumors were excluded. Out-comes for the patients staged as within the Milan crite-ria by imaging (n � 18) were again excellent, with 1-and 4-year survivals of 100% and 92%, respectively.The number of patients with known tumor beyond theMilan criteria fell substantially (from 21 to 9), but 1-and 4-year survival remained in an acceptable range at77.8% at both time periods. One extended criteriapatient died of HCC recurrence and 1 from unrelatedissues. Additionally, we have found that the discrepancybetween imaging and explant histological staging hasdecreased progressively over the last several years.
Does an immunosuppressive protocol tailored to avoidtumor recurrence make a difference in long-term out-comes in this patient group after liver transplantation? Our“Tumor Protocol” was planned to minimize the potentialimpact of steroids12 and calcineurin-inhibitors6 on HCCrecurrence, and to allow for benefits of the previouslyreported antitumor activity of sirolimus.13–15
In the absence of a control group, we cannot con-
clude that our protocol prevented tumor recurrence orprolonged survival in cases with tumor recurrence.Comparison of the fate of our 5 patients with tumorrecurrence on sirolimus therapy and the 8 patientsreported by Yao et al.18 with HCC recurrence on main-tenance immunosuppression with cyclosporine ortacrolimus and prednisone supports a benefit of ourtailored immunosuppressive protocol. Yao et al.18
reported recurrences from 2 to 22 months (mean 8months) posttransplant, with no patient survivingbeyond 10 months postrecurrence. We observed only 1early recurrence, in a patient transplanted with a tumorbeyond even our extended criteria. The other 4 recur-rences occurred at 12, 17, 27, and 51 months (overallmean 22.2 � 16.8 months). None of these 4 patientsdied consequent to tumor recurrence, with patients cur-rently surviving their tumor recurrences for 15, 37, and51 months, and 1 patient dying of unrelated causes. Assuch, recurrence was later (mean 22 vs. 8 months) andmore indolent (survival after recurrence mean 23.2months vs. none �10 months) in our cohort.
This immunosuppressive protocol achieved satisfac-tory control of immune-mediated graft rejection. Dur-ing the mean follow-up period of 44.3 months, only 12of 40 patients (30%) presented with acute rejectionepisodes, no patient had steroid resistant rejection, andno grafts were lost. All patients were weaned off steroids(the majority never received steroids) and 24 of 35surviving patients (69%) are on sirolimus mono-therapy.
Side effects (mainly leukopenia, anemia, and mouthulcers) were generally related to the high levels of siroli-mus23–27 from which 5 of the 40 patients were with-drawn. No patient died of opportunistic infection andthe number of infections was not higher than observedin other immunosuppressive protocols (Table 5).Importantly, we did not observe any hepatic arterythrombosis with this protocol.
Suppression of the immune system by antirejectiontherapy has long been linked to increased rates of cancerin transplant recipients. Such logic predicts increasedrisk of HCC recurrence after transplantation. Advancesin basic science have strengthened the association withcalcineurin inhibition and increased risk of malignantdisease recurrence.28,29 Since initiation of our pilotseries, much stronger evidence of the impact of cal-cineurin inhibitors and sirolimus on tumor biology hasbeen reported. Hojo et al.29 reported that cyclosporinetransformed a noninvasive lung cancer cell line into aninvasive phenotype. They further demonstrated thatcyclosporine treatment of mice inoculated with murineor human cancers developed a significant increase in the
1309Sirolimus and Extended Criteria for HCC

number of metastatic nodules in the lung. Cyclosporinewas noted to increase transforming growth factor–betaproduction by tumor cell lines in vitro. Treatment withanti– transforming growth factor–beta monoclonalantibody blocked the development of the invasive phe-notype, the increase in cell motility in vitro, and pre-vented the increase in metastases in mice. These resultsindicate that cyclosporine could exacerbate tumorgrowth in patients with existing tumors.30 Vivarelli etal.6 reported that patients with HCC receiving a highdosage of cyclosporine A during post– liver transplantmonths 3 to 12 experienced a significantly lower recur-rence-free survival. A cutoff in the cumulative cyclo-sporine A dosage was determined by applying a receiv-er-operating characteristic curve. When using a cutoffof 116,834 mg of cumulative dosage of cyclosporine Aadministered in the first 12 postoperative months,recurrence-free survival at 5 years was 76% for patientsreceiving higher and 93% for patients receiving lowercumulative cyclosporine A doses.
Guba et al.31 reported that sirolimus inhibited, but thatcyclosporine promoted, the growth of lung metastases inmice given murine colon cancer cells. They furtherreported decreased tumor growth and tumor neovascular-ization in sirolimus-treated mice, but early neovasculariza-tion and accelerated tumor growth with cyclosporine.Guba et al.31 reported that sirolimus inhibited vascularendothelial growth factor secretion by tumor cell lines invitro and in vivo. Sirolimus markedly inhibited vascularendothelial growth factor–dependent human umbilicalvein endothelial cell proliferation and completely abro-gated tubule formation, a crucial component of angiogen-esis, with the potential for important impact on cancerrecurrence and progression.32,33
Schumacher et al.16 recently reported in vitro suppres-sion of human hepatoma cells by sirolimus, in contrast totacrolimus, which promoted hepatoma growth. Theimpact of sirolimus on angiogenesis may theoretically altertumor progression and so overall survival more so than therate of tumor recurrence. Although our results support thishypothesis, a controlled trial is required to assess theimpact of sirolimus on tumor outcome.
Use of sirolimus immunosuppression during the earlyperiod after liver transplantation is currently challenged bya U.S. Food and Drug Administration “black-box” rec-ommending against utilization of sirolimus for immuno-suppression after liver transplant. A trend to increased ratesof hepatic artery thrombosis, and an increase in rate ofgraft loss and death were reported from a recent clinicaltrial (unpublished results; Wiesner R, American Trans-plant Congress, Washington D.C., June 2, 2003). Wehave found that high-dose sirolimus, when combined
within a steroid-free protocol with low tacrolimus targetlevels that were tapered within the first few months post-transplant, has not been associated with high rates of infec-tion (Table 5) nor graft loss from hepatic artery thrombo-sis. Our practice has been to run heparin at a fixed rate of300 IU/hour (once PT INR falls below 1.6) in the post-operative period in any patients felt at increased risk ofhepatic artery thrombosis. Such patients include thosewith multiple-donor hepatic arteries or those requiringarterial or venous jump grafts for vascular reconstruction,or for any other such concern on the part of the operatingsurgeon. Low-dose ASA is substituted by day 7. With thisapproach, we have seen no episodes of hepatic arterythrombosis in �125 patients (including the 40 reportedhere) treated with sirolimus-based immunosuppression inthe immediate period post–liver transplant. Since thereport of increased hepatic artery thrombosis, we have runlow-dose heparin on all patients receiving induction-phasetreatment with sirolimus, and have obtained a specificinformed consent for use of our “Tumor Protocol.”
In conclusion, our study demonstrates that theMilan criteria can be carefully extended without com-promising the outcome of liver transplantation for hep-atocellular carcinoma. The “Tumor Protocol” pre-sented herein appears to have beneficial effects ontumor recurrence and patient survival with an accept-able rate of rejection and toxicity.
Acknowledgments
We thank Cathy Asano for assistance with manuscript prepara-tion and Christie Kneteman for data review. This study wasinvestigator initiated and designed, and funded solely by theUniversity of Alberta and the Alberta Liver Transplant Program.
References1. Ringe B, Pichlmayr R, Wittekind C, Tusch G. Surgical treatment of
hepatocellular carcinoma: experience with liver resection and trans-plantation in 198 patients. World J Surg 1991;15:270–285.
2. Bismuth H, Chiche L, Adam R, Castaing D, Diamond T, Den-nison A. Liver resection versus transplantation for hepatocellularcarcinoma in cirrhotic patients. Ann Surg 1993;218:145–151.
3. Dmitrewski J, El-Gazzaz G, McMaster P. Hepatocellular cancer:resection or transplantation. J Hepatobiliary Pancreat Surg1998;5:18–23.
4. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A,Bozzetti F, et al. Liver transplantation for the treatment of smallhepatocellular carcinomas in patients with cirrhosis. N EnglJ Med 1996;334:693–699.
5. Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook A,et al. Liver transplantation for hepatocellular carcinoma: expan-sion of the tumor size limits does not adversely impact survival.Hepatology 2001;33:1394–1403.
6. Vivarelli M, Bellusci R, Cucchetti A, Cavrini G, De Ruvo N,
1310 Kneteman et al.

Aden AA, et al. Low recurrence rate of hepatocellular carcinomaafter liver transplantation: better patient selection or lowerimmunosuppression? Transplantation 2002;74:1746–1751.
7. Molmenti EP, Klintmalm GB. Liver transplantation in associa-tion with hepatocellular carcinoma: an update of the Interna-tional Tumor Registry. Liver Transpl 2002;8:736–748.
8. Bechstein WO, Guckelberger O, Kling N, Rayes N, Tullius SG,Lobeck H, et al. Recurrence-free survival after liver transplanta-tion for small hepatocellular carcinoma. Transpl Int 1998;11(Suppl 1):S189–S192.
9. Klintmalm GB. Liver transplantation for hepatocellular carci-noma: a registry report of the impact of tumor characteristics onoutcome. Ann Surg 1998;228:479–490.
10. Esnaola NF, Lauwers GY, Mirza NQ, Nagorney DM, DohertyD, Ikai I, et al. Predictors of microvascular invasion in patientswith hepatocellular carcinoma who are candidates for orthotopicliver transplantation. J Gastrointest Surg 2002;6:224–232; dis-cussion 232.
11. Yokoyama I, Carr B, Saitsu H, Iwatsuki S, Starzl TE. Acceleratedgrowth rates of recurrent hepatocellular carcinoma after livertransplantation. Cancer 1991;68:2095–2100.
12. Mazzaferro V, Rondinara GF, Rossi G, Regalia E, De Carlis L,Caccamo L, et al. Milan multicenter experience in liver trans-plantation for hepatocellular carcinoma. Transplant Proc 1994;26:3557–3560.
13. Majewski M, Korecka M, Kossev P, Li S, Goldman J, Moore J, etal. The immunosuppressive macrolide RAD inhibits growth ofhuman Epstein-Barr virus-transformed B lymphocytes in vitroand in vivo: a potential approach to prevention and treatment ofposttransplant lymphoproliferative disorders. Proc Natl Acad SciUSA 2000;97:4285–4290.
14. Hidalgo M, Rowinsky EK. The rapamycin-sensitive signal trans-duction pathway as a target for cancer therapy. Oncogene 2000;19:6680–6686.
15. Eng CP, Sehgal SN, Vezina C. Activity of rapamycin(AY-22,989) against transplanted tumors. J Antibiot (Tokyo)1984;37:1231–1237.
16. Schumacher G, Oidtmann M, Rosewicz S, Langrehr J, Jonas S,Mueller AR, et al. Sirolimus inhibits growth of human hepatomacells in contrast to tacrolimus which promotes cell growth.Transplant Proc 2002;34:1392–1393.
17. Sobin LH, Wittekind CH. TNM classification of malignanttumours. New York: Wiley-Liss, Inc., 2002, 6th ed. pp. 81–83.
18. Yao FY, Ferrell L, Bass NM, Bacchetti P, Ascher NL, Roberts JP.Liver transplantation for hepatocellular carcinoma: comparison ofthe proposed UCSF criteria with the Milan criteria and the Pitts-burgh modified TNM criteria. Liver Transpl 2002;8:765–774.
19. Poon RT, Fan ST, Lo CM, Ng IO, Liu CL, Lam CM, et al.Improving survival results after resection of hepatocellular carci-noma: a prospective study of 377 patients over 10 years. AnnSurg 2001;234:63–70.
20. Transcatheter arterial chemoembolization of hepatic tumors.Tecnologica MAP Suppl 2000;13–18.
21. Llovet JM, Bruix J. Systematic review of randomized trials forunresectable hepatocellular carcinoma: chemoembolizationimproves survival. Hepatology 2003;37:429–442.
22. Farmer DG, Anselmo DM, Ghobrial RM, Yersiz H, McDiarmidSV, Cao C, et al. Liver transplantation for fulminant hepaticfailure: experience with more than 200 patients over a 17-yearperiod. Ann Surg 2003;237:666–675; discussion 675–666.
23. Brattstrom C, Wilczek H, Tyden G, Bottiger Y, Sawe J, GrothCG. Hyperlipidemia in renal transplant recipients treated withsirolimus (rapamycin). Transplantation 1998;65:1272–1274.
24. Watson CJ, Friend PJ, Jamieson NV, Frick TW, Alexander G,Gimson AE, et al. Sirolimus: a potent new immunosuppressantfor liver transplantation. Transplantation 1999;67:505–509.
25. Hong JC, Kahan BD. Sirolimus-induced thrombocytopenia and leu-kopenia in renal transplant recipients: risk factors, incidence, progres-sion, and management. Transplantation 2000;69:2085–2090.
26. Ryan EA, Lakey JR, Rajotte RV, Korbutt GS, Kin T, Imes S, et al.Clinical outcomes and insulin secretion after islet transplantationwith the Edmonton protocol. Diabetes 2001;50:710–719.
27. McAlister VC, Gao Z, Peltekian K, Domingues J, Mahalati K,MacDonald AS. Sirolimus-tacrolimus combination immuno-suppression [letter]. Lancet 2000;355:376–377.
28. Freise CE, Ferrell L, Liu T, Ascher NL, Roberts JP. Effect ofsystemic cyclosporine on tumor recurrence after liver transplan-tation in a model of hepatocellular carcinoma. Transplantation1999;67:510–513.
29. Hojo M, Morimoto T, Maluccio M, Asano T, Morimoto K,Lagman M, et al. Cyclosporine induces cancer progression bya cell-autonomous mechanism. Nature 1999;397:530 – 534.
30. Nabel GJ. A transformed view of cyclosporine. Nature 1999;397:471–472.
31. Guba M, von Breitenbuch P, Steinbauer M, Koehl G, FlegelS, Hornung M, et al. Rapamycin inhibits primary and meta-static tumor growth by antiangiogenesis: involvement of vas-cular endothelial growth factor. Nat Med 2002;8:128 – 135.
32. Folkman J, Merler E, Abernathy C, Williams G. Isolation of atumor factor responsible for angiogenesis. J Exp Med 1971;133:275–288.
33. Folkman J. Role of angiogenesis in tumor growth and metastasis.Semin Oncol 2002;29(6 Suppl 16):15–18.
1311Sirolimus and Extended Criteria for HCC
Copyright © 2022 FDOKUMEN




















