Growth of kidney-transplanted pediatric patients treated with sirolimus
11
ABSTRACTS 8th Symposium on Growth and Nutrition in Children with Chronic Renal Disease Symposium of the International Pediatric Nephrology Association (IPNA) Oviedo, Spain, from 28 to 30 of May, 2009 Chairpersons Fernando Santos (Oviedo, Spain) Frederick J. Kaskel (New York, USA) Alberto Caldas (Porto, Portugal) Robert H. Mak (San Diego, USA) Scientific Committee Pierre Cochat (Lyon, France) Anthony A. Portale (San Francisco, USA) Jorge Ferraris (Buenos Aires, Argentina) Isidro B. Salusky (Los Ángeles, CA, USA) Aaron L. Friedman (Providence, RI, USA) Cheryl P. Sánchez (Madison, WI, USA) Mary B. Leonard (Philadelphia, USA) Franz S. Schaefer (Heidelberg, Germany) Otto Mehls (Heidelberg, Germany) Burkhard Tönshoff (Heidelberg, Germany Local Organizing Committee Óscar Álvarez-García; Lucía Mallada; Eduardo Carbajo; Flor Ángel Ordóñez; Enrique García; Julián Rodríguez; Helena Gil; Fernando Santos; Vanessa Loredo; Teresa Usín. Congress Venue "Principe Felipe" Congress Hall-Auditorium Plaza de la Gesta s/n. 33007. Oviedo, Asturias, Spain. E-mail: [email protected] 1 Final height after recombinant growth hormone therapy in children with chronic renal failure: a single centre experience M Van Dyck, T Van Damme-Lombaerts, W Proesmans University Hospitals Leuven, department of Paediatric Nephrology Background Recombinant human growth hormone (rhGH) is able to reverse progressive growth failure in chronic kidney disease. Objective of the study This study will analyse the final height after rhGH therapy in children with chronic renal failure (stage 3, 4 CRF), during dialysis and after renal transplantation. Patients and methods Between 1988 and 2007 rhGH therapy was given to 85 growth retarded patients (all of Caucasian origin) for at least 1 year. Twelve patients received rhGH therapy for a second and third period. Final height was reached in 46 patients. Patients were grouped according to the stage of chronic renal failure, in which rhGH has been initiated for the first time. Group A (CRF) consisted of 16 patients (of which 13 boys), most of them have a hypo-dysplastic kidney disease (n =11). In group B 8 patients (4 girls, 4 boys) were treated during dialysis. 22 patients (10 girls, 12 boys) initiated rhGH after the first year of transplantation (group C), 9 of them have hypo- dysplastic kidneys. Median age at the start in group A, B and C was 7.8 (2.8 to 16.4), 10.3 (6.1 to 16.4) and 13.6 (9.0–17.3) years (yrs). Growth data and biochemical analysis were collected every 6 months; bone age has been performed every year. Growth parameters were expressed as SDS according to Cole (1995), data were expressed as median and ranges. Non-parametric tests were used for statistical analysis. Results At the start median values of height SDS were respectively −2.3, −1.3 and −3.0 for group A, B and C. Median duration of rhGH was 5 yrs in group A and C and 1.6 yrs in group B. After rhGH has been stopped, median height SDS was −0.4 in group A, −0.8 in group B and −1.9 in group C. Median gain in height SDS was +1.6 (group A), +0.8 (group B) and +1.1 (group C). At adult height (median age 18.8 yrs) median height SDS was comparable to the data at the end of the period of rhGH therapy. Pediatr Nephrol (2010) 25:789–799 DOI 10.1007/s00467-009-1399-z
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Growth of kidney-transplanted pediatric patients treated with sirolimus
ABSTRACTS
8th Symposium on Growth and Nutrition in Childrenwith Chronic Renal DiseaseSymposium of the International Pediatric Nephrology Association (IPNA)Oviedo, Spain, from 28 to 30 of May, 2009
ChairpersonsFernando Santos (Oviedo, Spain)Frederick J. Kaskel (New York, USA)Alberto Caldas (Porto, Portugal)Robert H. Mak (San Diego, USA)
Scientific CommitteePierre Cochat (Lyon, France)Anthony A. Portale (San Francisco, USA)Jorge Ferraris (Buenos Aires, Argentina)Isidro B. Salusky (Los Ángeles, CA, USA)Aaron L. Friedman (Providence, RI, USA)Cheryl P. Sánchez (Madison, WI, USA)Mary B. Leonard (Philadelphia, USA)Franz S. Schaefer (Heidelberg, Germany)Otto Mehls (Heidelberg, Germany)Burkhard Tönshoff (Heidelberg, Germany
Local Organizing CommitteeÓscar Álvarez-García; Lucía Mallada; Eduardo Carbajo;Flor Ángel Ordóñez; Enrique García; Julián Rodríguez;Helena Gil; Fernando Santos; Vanessa Loredo; Teresa Usín.
Congress Venue"Principe Felipe" Congress Hall-AuditoriumPlaza de la Gesta s/n. 33007. Oviedo, Asturias, Spain.E-mail: [email protected]
1Final height after recombinant growth hormone therapyin children with chronic renal failure: a single centreexperience
M Van Dyck, T Van Damme-Lombaerts, W ProesmansUniversity Hospitals Leuven, department of PaediatricNephrology
Background Recombinant human growth hormone (rhGH)is able to reverse progressive growth failure in chronickidney disease.Objective of the study This study will analyse the finalheight after rhGH therapy in children with chronic renalfailure (stage 3, 4 CRF), during dialysis and after renaltransplantation.Patients and methods Between 1988 and 2007 rhGHtherapy was given to 85 growth retarded patients (all ofCaucasian origin) for at least 1 year. Twelve patientsreceived rhGH therapy for a second and third period. Finalheight was reached in 46 patients. Patients were groupedaccording to the stage of chronic renal failure, in whichrhGH has been initiated for the first time. Group A (CRF)consisted of 16 patients (of which 13 boys), most of themhave a hypo-dysplastic kidney disease (n =11). In group B8 patients (4 girls, 4 boys) were treated during dialysis. 22patients (10 girls, 12 boys) initiated rhGH after the firstyear of transplantation (group C), 9 of them have hypo-dysplastic kidneys. Median age at the start in group A, Band C was 7.8 (2.8 to 16.4), 10.3 (6.1 to 16.4) and 13.6(9.0–17.3) years (yrs). Growth data and biochemicalanalysis were collected every 6 months; bone age has beenperformed every year. Growth parameters were expressedas SDS according to Cole (1995), data were expressed asmedian and ranges. Non-parametric tests were used forstatistical analysis.Results At the start median values of height SDS wererespectively −2.3, −1.3 and −3.0 for group A, B and C.Median duration of rhGH was 5 yrs in group A and C and1.6 yrs in group B. After rhGH has been stopped, medianheight SDS was −0.4 in group A, −0.8 in group B and −1.9in group C. Median gain in height SDS was +1.6 (groupA), +0.8 (group B) and +1.1 (group C). At adult height(median age 18.8 yrs) median height SDS was comparableto the data at the end of the period of rhGH therapy.
Pediatr Nephrol (2010) 25:789–799DOI 10.1007/s00467-009-1399-z

Compared to group B and C, patients of group C have alower final height SDS. Initial height was in the normalrange for age in 6 patients in group A, in 6 patients in groupB and in 3 patients in group C. Adult height was within 0and −2.0 SDS in group A (n=15) and in group B (n=7), ingroup C normal height range was reached in only 12 of the22 patients.Conclusions Growth retardation was more severe in thechronic renal failure group and after transplantation. rhGHtherapy leads to a catch-up growth in all stages but wasmuch better in the chronic renal failure group. Final heightwas not optimal in the transplanted group. When startedearly (prepubertal, before dialysis), normal adult height canbe reached.
2Improvement in growth after one year of growthhormone therapy in well-nourished infants with growthretardation secondary to chronic renal failure: Resultsof a multi-center, controlled, randomized, open clinicaltrial
L Moreno, F Santos, A Neto, G Ariceta, J Vara, A Alonso,A Bueno, A Caldas, JA Correia, R Muley, V Barrios,C Gómez, J ArgenteSpanish and Portuguese Multicenter Study, clinical trialnumber NCT00184769, sponsored by Novo NordiskPharma, S.A. Spain
Objective Our aim was to evaluate the growth-promotingeffect of growth hormone (GH) treatment in infants withchronic renal failure and persistent growth retardationdespite adequate nutritional and metabolic management.Patients and Methods The study design included random-ized, parallel groups in an open, multicenter trial comparingGH (0.33 mg/kg/week) versus non-treatment with GHduring 12 months. Sixteen growth retarded infants aged12±3 months with chronic renal failure (glomerularfiltration rate≤60 ml/min/1.73 m2), adequate nutritionalintake and good metabolic control were recruited fromeight Pediatric Nephrology departments from Spain andPortugal. Main outcome measures were body length, bodyweight, bone age, biochemical and hormonal analyses,renal function, bone mass and adverse side-effects deter-mined quarterly.Results Length gain in infants treated with GH wasstatistically greater than that of non-treated children(14.5 cm/year vs 9.5 cm/year [p<0.01] and +1.43 SDS vs.−0.11 SDS [p<0.02]). The GH induced stimulation of growthwas associated with no undesirable effects on bone matura-tion, renal failure progression, or metabolic control. Inaddition, GH treatment improved forearm bone mass andincreased serum concentrations of total and free insulin-like
growth factor (IGF) I and IGF binding protein (IGFBP 3),whereas IGF-II, IGFBP-1, IGFBP-2, GHBP, ghrelin andleptin were not modified.Conclusions Infants with CRF and growth retardation inspite of good metabolic and nutritional control benefit fromGH treatment without adverse effects during 12 months oftherapy.
3Long term follow up of infants with severe chronickidney disease
D Mekahli*, S Bradley, L Wright, E Brennan, V Shaw,SE Ledermann, L ReesRenal Unit, Gt Ormond St Hospital for Children NHSTrust, Gt Ormond St, London WC1N 3JH, UK. *Universityhospital Gasthuisberg, Leuven, Belgium
Background and Objectives In 2000 we published themanagement, mortality and growth of 101 children whopresented aged <2 years to our unit with a GFR <20 ml/min/1.73 m2 between 1/1/86 and 31/12/98. Long-term dataon such young children is scarce. We have, therefore,restudied these factors in this group 10 years later.Methods The mortality, growth and treatment modalitywere reanalysed in this cohort.Results Of the 101 patients, 23 died in the first report and 5are lost to follow-up. Median (range) age at presentationwas 0.3 (0.0–1.5) years and follow-up 16.0 (3.6–22.2)years. One, 2, 3, 5, 10, 15, and 20 year survival was 82, 81,79, 77, 77, 75 and 75% respectively. Three patients weremanaged conservatively; 31 were transplanted pre-emptively at age 5.5 (1.4–15.6) years (22 deceased donor[DDT], 9 living related [LRT]); and 39 were dialysed at age1.8 (0.0–14.0) years before transplantation at age 3.2 (1.0–15.3) years (33 DDT, 6 LRT). Seventeen had 2 transplantsand 4 had 3. At last follow up 61 patients were trans-planted, 6 dialysed, 3 treated conservatively and 3 died.Sixty six (81%) of the patients were tube fed, from amedian age of 0.8 (range 0–4.9 years) and duration of 1.7(0.1–6.9) years. Thirty seven (46%) had a gastrostomy, and18 (22%) also had a Nissen fundoplication.Mean (SD) Ht SDS increased from −2.03 (1.37) at age0.5 years (n=54), to −1.88 (1.43) at 1 (n=67), −1.10 (1.13) at5 (n = 65), −1.04 (1.15) at 10 (n = 62), but decreased to −1.84(1.32) at 15 (n=40) and −2.06 (1.61) at 18 years (n=17). 12patients (16%) received rhGH.Median height at last follow upfor those aged >18 years (n=16) was 161.7 (149.9–190.5) cmfor males and 149.9 (143.5–161.2) cm for females.Conclusions Mortality in infants with severe CKD occursmainly in the first year of life. Most patients havetransplants. Despite good initial acceleration of growththere is a disappointing decline in the peripubertal years.
790 Pediatr Nephrol (2010) 25:789–799

4Nutritional status and body composition in children withrenal failure followed in a pediatric nephrology center
AP Brecheret, JTA Carvalhaes, ML Castro, U FagundesUNIFESP–Universidade Federal de São Paulo
Background Undernutrition is a frequent complicationamong children with renal diseases. Short stature is itsprincipal clinical sign. In order to better manage nutricionaltherapy we performed a nutricional evaluation of all children,that are followed in a pediatric nephrology service.Objectives Nutritional status and body composition ofchildren with renal failure evaluation and check on differencesbetween patients with chronic kidney disease stages 3 and 4and patients under dialysis treatment (stage 5) concerningnutritional status and body composition. Verify if there is anycorrelation between disease stage,, nutritional status and bodycomposition.Methods This cross sectional study enrolled 18 (42.8%) boysand 24 (57.2%) girls aged between 5.3/19.5 years old. Theywere distributed into two groups based on their glomerularfiltration rate (GFR): 1–GFR 59–15 ml/min/1.73 m2 (21children) 2–GFR below 15 (21children). Weight and heightwere obtained to calculate the following indexes: Weight/Age (W/A), Height/Age (H/A) and BMI/Age (B/A). Then Z-scores were obtained (NCHS/CDC-2000). Z-scores below−2.00 were considered under-nutrition. Body compositionwas measured by dual-energy x-ray absorptiometry (DXA -Hologic 4500A). Student's t-test was used to compare thegroups.Results There were no differences between groups foranthropometric data. 18 patients (42.8%) presented short-stature and 22 (52.4%) low-weight. Neither for W/A’s, H/A’s and BMI’s Z-scores. Body fat percentage ranged from11.3 to 35.6 (average: 18.7), and body mass percentage leanfrom 61.6 to 85.2 (average: 78.0). No statistical differencewas observed concerning body composition between the 2groups.Conclusion The studied children presented a high prevalenceof under-nutrition.. When kidney disease stage is considered,no differences in nutritional status indexes, neither in bodycomposition’s measuraments have been found.
5Calf muscle cross-sectional area in children with chronickidney disease
BJ Foster1, R Wetzsteon2, B Zemel2, H Kalkwarf3,M Thayu2, D Foerster2, MB Leonard21Montreal Children’s Hospital, McGill University, 2Chil-dren’s Hospital of Philadelphia, Univ. of Pennsylvania,3Cincinnati Children’s Medical Center
Background Adults with chronic kidney disease (CKD) areat risk for protein-energy wasting and muscle deficits. Musclemass has not been well characterized in children with CKD.Peripheral quantitative CT (pQCT) scans provide measures ofmuscle and fat cross-sectional area (CSA) in the lower leg.Objectives To assess calf muscle CSA relative to tibia lengthand maturation in children with CKD compared with healthycontrols, and to identify determinants of muscle deficits.Methods Calf muscle CSA was estimated from pQCT scansin the proximal 1/3 rd of the tibia in 156 children with CKD(median age 14.3 y; IQR 11.0, 17.5) and 861 healthy controls(11.7 y; IQR 8.6, 14.8). The LMS method was used togenerate sex- and race-specific muscle CSA- (muscleZ) andfat CSA- (fatZ) z-scores relative to tibia length. CKD stageswere classified based on estimated GFR (ml/min/1.73 m2)using the CKiD formula as CKD 2–3 (GFR 30 to 89; 35 M/33F), CKD 4–5 (GFR <30; 33 M/12F), or CKD 5D (dialysis;24 M/19F). Multivariable regression was used to determinethe differences in z-scores between CKD subjects andcontrols. A second model within the CKD subjects consid-ered the impact of disease and treatment characteristics. Allmodels were adjusted for sex, race, age, and pubertal status,and muscleZ models were also adjusted for fatZ.Results MuscleZ did not differ from controls in either CKD2–3 [difference: 0.08 (95% CI: −0.16, 0.31); p=0.5] or inCKD 4–5 [0.04 (−0.24, 0.32); p=0.8], but was significantlylower than in controls in CKD 5D [−0.48 (−0.77, −0.19); p=0.001]. Age and fatZ were the only significant covariates inthe model. In the model limited to CKD subjects, muscleZwas lower in dialysis subjects compared with predialysis[−0.51 (−0.89, −0.14); p=0.007]. Current growth hormoneuse was associated with a significantly higher muscleZ [0.62(0.01, 1.22); p=0.04]. None of race, age, pubertal status,diagnosis, dialysis modality, duration of CKD, time ondialysis, or current glucocorticoid use contributed significant-ly to the model. FatZ did not differ significantly between anyof the CKD groups and controls. Among CKD subjects,current growth hormone use was associated with a lower fat Z[−0.83 (−1.66, 0.0); p=0.05] compared with no use.Conclusions When adjustments are made for leg length andmaturation, there is no evidence of calf muscle wasting amongchildren with pre-dialysis CKD. Children on dialysis havemoderate calf muscle deficits. Growth hormone use isassociated with significantly higher muscle area and lowerfat area for leg length.
6Changes in body composition observed with a prototypeof infant formula, specially designed for children under3 years of age with chronic renal failure
RA Lama-More1, A Moráis-López1, A Alonso-Melgar2,M Navarro-Torres2, R Chifré-Petit3, M Rivero-Urgell3
Pediatr Nephrol (2010) 25:789–799 791

1Unidad de Nutrición Infantil. Hospital UniversitarioInfantil La Paz. UAM (Madrid), 2Servicio de NefrologíaInfantil. Hospital Universitario Infantil La Paz, 3DirecciónGeneral Científica. Grupo Ordesa. Sant Boi de Llobregat(Barcelona)
Background Body composition analysis is the main step ofnutritional assessment. Keeping an optimum nutritionalstatus has influence on growing and quality of life ofinfants and children with chronic renal failure (CRF).Objective To evaluate the changes in body compositionof children with CRF younger than 3 years of age fedwith an infant formula specially designed for thissituation, compared with those who received a standardinfant formula.Subjects and methods Prospective, randomized study.Children with CRF younger than 3 years of age weredivided in two groups. Group A (study) was fed with thespecial formula. Group B (control) received a standardformula, making the necessary adjustments to guaranteemetabolic control. Energy and protein intakes were similarwith both infant formulas. Changes in body compositionwere assessed using anthropometric and electric (bioimpe-dance) methods. Results are shown using z-score foranthropometric results and percentage of the normal valuefor bioimpedance results. Monitoring of both groups wasmade along 12 months.Results
– Seventeen children (mean 1.18±0.93 years old) ingroup A and 17 children (mean 1.03±0.83 years old) ingroup B were assessed. Glomerular filtration rate was41±30.5 ml/min/1.73 m2 in group A and 45±27 ml/min/1.73 m2 in group B.
– There were statistical differences between groups ininitial body weight (z-score −1.34±0.9 in group A,1.23±1.63 in group B, p<0.01). Final body weight wassimilar in both groups (z-score 0.99±1.2 in group A,−0.28±1.69 in group B).
– Improvement in height was observed in both groups.Group A: z-score for initial height −0.94±1.5, z-score forfinal height 0.27±1.5. Group B: z-score for initial height−0.02±2, z-score for final height 0.47±1.5. Z-score forlinear growth changed as follows: Δz-score in group Awas 1±3.39. Δz-score in group B was 0.21±3.88.
– Weight/height ratios showed no statistical differencesbetween groups.
– Bioimpedance analysis: statistical differences betweengroups were observed in body cell mass (BCM),expressed as percentage of lean body mass. Group A:initial BCM 41.68±4.1%, final BCM 44.6±3% (p<0.02). Group B: initial BCM 41.42±4%, final BCM42.7±3.8% (p<0.05).
Conclusion Although energy intake was similar with bothformulas, the use of a prototype specially designed forchildren with CRF determined a better linear growth andbody composition.
7Impact on metabolic control of a prototype of infantfeeding formula, specially designed for children under3 years of age with chronic renal failure
RA Lama-More1, A Moráis-López1, A Alonso-Melgar2,M Navarro-Torres2, R Chifré-Petit3, M Rivero-Urgell31Unidad de Nutrición Infantil. Hospital Universitario InfantilLa Paz. UAM (Madrid). 2Servicio de Nefrología Infantil.Hospital Universitario Infantil La Paz. 3Dirección GeneralCientífica. Grupo Ordesa. Sant Boi de Llobregat (Barcelona)
Background Adequate diet therapy can help to achievegood metabolic control in infants and children with chronicrenal failure (CRF).Objective To evaluate metabolic changes in children withCRF younger than 3 years of age and fed with an infantformula specially designed for this situation, compared withthose who received a standard infant formula.Subjects and methods Prospective, randomized study.Children with CRF younger than 3 years of age weredivided in two groups. Group A (study) was fed with thespecial formula. Group B (control) received a standardformula, making the necessary adjustments to guaranteemetabolic control. Changes in BUN/creatinine (BUN/cr)ratio, serum triacylglycerides (TAG) and potassium levelswere assessed. Calcium, phosphorus and parathyroidhormone (PTH) levels were also evaluated. Monitoring ofboth groups was made along 12 months.Results
– Seventeen children (mean 1.18±0.93 years old) in groupA and 17 children (mean 1.03±0.83 years old) in group Bwere assessed. Glomerular filtration rate was 41±30.5ml/min/1.73 m2 in group A and 45±27 ml/min/1.73 m2 ingroup B.
– BUN/cr in group A showed a tendency to decrease (initial33±34, final 28.3±21), whereas in group B it increasedfrom 32±42 (initial) to 46.5±34 (final) (p=0.05).
– There was significant correlation between BUN/cr ratioand the dietetic intake of non-protein kilocalories pergram of nitrogene consumed (non-protein Kcal/g N).There was significant negative correlation betweenBUN/cr ratio and TAG levels.
– Potassium levels remained high in group B, whereas ingroup A significantly decreased (initial 4.6±0.7 mEq/L,final 4.1±0.3 mEq/L, p=0.02). Two patients from groupB and none from group A required a change in the type of
792 Pediatr Nephrol (2010) 25:789–799

feeding formula administered to achieve good control ofpotassium levels.
– PTH levels increased in group B (initial 71±101 pg/ml,final 81±78 pg/ml) and decreased in group A (initial94.5±81 pg/ml, final 67.9±52 pg/ml), although differ-ences observed were not significant.
Conclusion The main goals achieved with the use of aninfant formula specially designed for children with CRFwere:
– Decrease in BUN/cr ratio.– Better control of serum potassium levels.– Better control of PTH levels.
8Bone metabolism in children with oxalosis
J Bacchetta1,2,3, S Fargue1, S Boutroy2,3, I Plotton3,4,P Cochat1,31Centre de Référence des Maladies Rénales Rares, HôpitalFemme Mère Enfant, 2INSERM 831, 3Université de Lyon,4Service d’Endocrinologie Moléculaire, Hôpital FemmeMère Enfant, Lyon, France
Background Primary hyperoxaluria type 1 (PH1) is a rareautosomal recessive disease resulting from a deficiency of aliver-specific, peroxisomal, enzyme. Deposition of calciumoxalate crystals in the kidney and bone is a hallmark ofprimary hyperoxaluria type 1.Objectives The aim of this study was to cross-sectionally eval-uate bone status in the 12 PH1 children followed at our center.Methods Bone biomarkers (PTH, vitamins D, FGF23),growth biomarkers (IGF1, IGFBP3) and radiological inves-tigations (skeletal age, three-dimensional High Resolutionperipheral Quantitative Computed Tomography) were cross-sectionally performed in a single-center cohort of 12 PH1children. Controls consisted of healthy and CKD childrenincluded in local bone and mineral metabolism studies.Results Mean±SD age was 99±63 months. Six children hada past of fracture. Bone maturation was accelerated in 5patients, 4 of whom were younger than 5 years. Serum IGF1levels were higher than normal pediatric values in all 5. In thewhole cohort, PH1 children had higher serum FGF23 levelsthan CKD pediatric controls (262±333 vs. 69±98 IU/mL, P0.002) with lower 1–25 OH2 vitamin D (109±54 vs. 156±74 pg/mL, P 0.046). In patients above the age of 10 years, HR-pQCT showed a significant decreased total volumetric bonemineral density (vBMD, 236±26 vs. 277±41 mgHA/cm3, P0.022) and a decreased cortical thickness (684±132 vs. 945±264 μm, P 0.008) in PH1 children compared to healthycontrols, with a trend for decreased cortical and trabecularvBMDs, without significant differences for trabecular micro-
architecture. When comparing PH1 patients receiving main-tenance dialysis to PH1 patients with conservative treatments,hemodialysis patients tended to have higher trabecular vBMDand trabecular thickness, with lower cortical thickness andmore disorganized trabecular microarchitecture.Conclusion Despite therapeutic improvement bone damageremains challenging in PH1 patients. A combination of newimaging techniques and biomarkers has highlighted newand unexplained features of PH1: advanced skeletal age andincreased IGF1 levels in younger PH1 patients, increasedFGF23 levels and decreased total vBMD with bone micro-architecture alteration. A regular bone follow-up in PH1patients should be scheduled whenever possible.
9Abnormal VEGF expression pattern in the growthplates of rapamycin-treated rats
O Alvarez-Garcia1, E Garcia-Lopez2, H. Gil-Peña1,V Loredo1, FA Ordoñez1, E Carbajo-Perez3, F Santos1,31Hospital Universitario Central de Asturias, 2HospitalÁlvarez Buylla, 3Facultad de Medicina de la Universidadde Oviedo. Asturias, Spain
Objectives and study Rapamycin has been shown toadversely impair longitudinal growth in young growingrats and alters growth plate structure and dynamics.Vascular endothelial growth factor (VEGF) plays a majorrole in the process of vascular invasion of growth platecartilage. The objective of this study was to find out theeffects of rapamycin administration on VEGF expression ingrowth plate.Methods Three groups (n=10) of young rats were used:control (C), treated with rapamycin (RAPA) and pair-fedwith the RAPA group (PF). Animals received 1 mg/kg ofrapamycin or vehicle during 14 days intraperitoneally.Longitudinal growth, body weight and food intake weremeasured. Growth plates of the tibial proximal ends werefrozen or embedded in methil-metracrilate for morpholog-ical study, measurement of osseous front advance as anindex of longitudinal growth rate and analysis of VEGFexpression by immunohistochemistry, in situ hybridization,real time PCR and Western bot.Results Rapamycin significantly decreased (X±SD) longi-tudinal growth rate (C=225±4, RAPA=130±2, PF=215±9 μm/day), body weight gain (C=94.7±3.9, RAPA=68.4±2.6, PF=81.8±3.2 g) and food intake (C=237.2±6.2,RAPA=222.4±5.1, PF=222.6±2.0 g). Morphologically,vascular invasion was markedly disturbed in RAPAanimals. VEGF immunohistochemical and in situ hybrid-ization signals were localized in the hypertrophic chondro-cites from the early hypertrophic zone to the most distalcells in C and PF groups. In RAPA animals, the terminal
Pediatr Nephrol (2010) 25:789–799 793

chondrocytes were rarely positive. VEGF protein levelswere not different among groups as assessed by Westernblot analysis. VEGF mRNA levels were slightly upregu-lated in RAPA animals when compared to controls.Conclusion Rapamycin induces longitudinal growth im-pairment and alterations of growth plate angiogenesis inyoung rats. This adverse effect is associated with anabnormal VEGF expression pattern in the growth plate oftreated animals.
10Prevalence of vitamin D insufficiency and the effectof cholecalciferol supplementation in children with chronickidney disease (CKD)
A Gulati, P Hari, *N Gupta, A BaggaDepartments of Pediatrics and Endocrinology*, All IndiaInstitute of Medical Sciences, New Delhi
Background Vitamin D insufficiency (serum 25-hydroxyvita-min D (25, OHD) level <30 ng/ml) is common in patientswith CKD and may contribute to mineral bone disease.Objective To estimate the prevalence of vitamin Dinsufficiency (serum 25-hydroxyvitamin D (25, OHD) level<30 ng/ml), and examine the effect of cholecalciferolsupplementation on serum levels of 25, OHD, intactparathyroid hormone (PTH), calcium and phosphorus inchildren with CKD.Methods In a prospective interventional study children withestimated GFR between 15 to 89 ml/min/1.73 m2 were given6, 00,000 IU of cholecalciferol. Children on vitamin Dsupplements and those with serum calcium level >10.5 mg/dland phosphorus >6.0 were excluded. Primary (25, OHD,PTH levels) and secondary (calcium, phosphorus, alkalinephosphatase levels and urinary protein excretion) outcomeswere measured at baseline and 6 weeks.Results 40 children (85% boys) with a mean age of 7.7±3.8(range 2–15) yr were studied. 33 (82.5%) children had vitaminD insufficiency at baseline. Of these, 15 children had 25,OHD levels <15 ng/ml. The median serum 25, OHD levelsincreased from 18.6 (95% confidence interval [CI], 15.4–23.4) ng/ml at baseline to 48.5 (42.1–56.8) ng/ml at 6 weeks(P=0.000) while the PTH levels declined from 55.3 (47.1–77.8) pg/ml to 41.4 (31.2–56.8) pg/ml (P=0.01). The calcium,phosphorus and alkaline phosphatase levels did not changesignificantly from the baseline. The median urinary protein tocreatinine ratio decreased from 0.30 (0.03–1.5) to 0.61 (0.08–2.26) mg/mg (P=0.07). There was no correlation betweenserum 25, OHD and PTH levels.Conclusion Vitamin D insufficiency is highly prevalent inchildren with CKD and cholecalciferol supplementationappears to be an effective treatment in correcting vitamin Dstatus and reducing PTH levels.
1125-(OH) Vitamin D3 Deficiency in a cohort of pediatricdialysis patients
S Menon, TK Mattoo, G Kapur, RP ValentiniDivision of Pediatric Nephrology, Children's Hospital ofMichigan. Detroit, MI, USA
Background K/DOQI Clinical practice guidelines for bonemetabolism in children with Chronic Kidney Disease recom-mend assessment of 25(OH) vitamin D [25(OH)D3] level inchildren with chronic kidney disease. There is insufficientdata on the prevalence of 25(OH)D3 deficiency and theappropriate treatment for CKD 5. It is also not known ifcorrection of 25(OH)D3 deficiency in dialysis patients willhave an effect on bone disease and hyperparathyroidism.Objective To assess the prevalence of Vitamin D deficiencyin pediatric dialysis patients and to see the response toergocalciferol.Methods A prospective observational study was done in 31patients followed in the dialysis clinic at Children’sHospital of Michigan. Included in the study were 11Caucasian, 17 African-American, and 3 Arabic patients.Their ages ranged from 1 to 17.8 (mean 11.1±5.3) years; 17were males and 14 females. Serum level of 25(OH)D3, Ca, Pand intact PTH were examined. None of these patients hadreceived ergocalciferol prior to the evaluation of Vitamin Dstores. The definitions for vitamin D insufficiency anddeficiency as well as its treatment were in accordance withthe K/DOQI Clinical practice guidelines for bone metabo-lism in children with Chronic Kidney Disease. The level of25(OH)D3 for all patients was determined at ARUPLaboratories using chemiluminiscent assay.Results Nineteen patients were on peritoneal dialysis and 12on hemodialysis. The mean 25(OH)D3 level for the entirecohort was 15.1±8.4 ng/mL. 28 (90.3%) had suboptimal 25(OH)D3 levels (<30 ng/mL) with a mean of 13.2±6.2 ng/mL, associated with an elevated PTH of 456.5±308.5.There was no significant difference in the vitamin D levelsbetween hemodialysis and peritoneal dialysis patients. Allthe non-caucasian patients had vitamin D level less than<30 ng/mL as compared to 8 (72.7 %) out of 11 Caucasians(p<0.05). The mean 25(OH)D3 level was significantly lowerin the non-caucasian population (11.4±5.2 ng/mL vs 21.9±9.1 ng/mL, p<0.05). At the time of this abstract, 16 patientshad received treatment with ergocalciferol according to K/DOQI guidelines and the mean 25(OH)D3 after treatmentwas 22.5±8.2 ng/mL. The response to ergocalciferol wasalso poorer in the non Caucasian population with the posttreatment 25(OH)D3 level being 20.5±9.5 ng/mL as com-pared to 28.5±5.2 ng/mL in the Caucasian population.Conclusions There was a high prevalence of vitamin Ddeficiency in our single center cohort of pediatric dialysis
794 Pediatr Nephrol (2010) 25:789–799

patients. Caucasians tend to have higher vitamin D levels andalso respond better to standard treatment with ergocalciferol.
12Prevalence and associations of 25-hydroxyvitamin Ddeficiency in children and adolescents in the UnitedStates: results from NHANES 2001–2004
J Kumar1; P Muntner2, FJ Kaskel1, SM Hailpern3,ML Melamed41Children’s Hospital at Montefiore, Albert Einstein Collegeof Medicine, Bronx, New York. 2Department of Medicine,Mount Sinai School of Medicine, New York, NY.3Northrup Grumman and Centers for Disease Control,Division of Diabetes Translation. 4Departments of Medicineand Epidemiology & Population Health, Albert EinsteinCollege of Medicine, Bronx, New York
Background Low 25-hydroxyvitamin D (25(OH)D) levelsare associated with adverse cardiovascular outcomes inadults.Objective To determine the prevalence of 25(OH)D deficien-cy and the associations between 25(OH)D deficiency andcardiovascular risk factors in children and adolescents.Population A nationally representative sample of childrenaged 1–21 years in the National Health and NutritionExamination Survey 2001–2004 (n=6275).Main Outcome Measure Serum 25(OH)D levels deficiencyand insufficiency (25(OH)D <15 ng/mL and 15 to 29 ng/mL,respectively) and cardiovascular risk factors.Results Overall, 9% of the pediatric population, representing7.6 million US children and adolescents were 25(OH)Ddeficient and 61%, or 50.8 million US children andadolescents were 25(OH)D insufficient. After multivariableadjustment, children and adolescents who were older (oddsratio, OR=1.16; 95% confidence interval (CI): 1.12, 1.20 peryear of age)), female (OR=1.9 (95% CI: 1.6, 2.4)),non-Hispanic black (OR=21.9 (95%CI: 13.4, 35.7)) orMexican-American (OR=3.5 (95%CI: 1.9, 6.4)) comparedto non-Hispanic white, obese (OR=1.9 (95%CI: 1.5, 2.5)) andthose who drank milk less than once a week (OR=2.9 (95%CI: 2.1–3.9)) or used more than 4 hours of TV, video orcomputers per day (OR=1.6 (95% CI: 1.1, 2.3)) were morelikely to be 25(OH)D deficient. Those who used vitaminD supplementation were less likely (OR=0.4 (95% CI:0.2–0.8) to be 25(OH)D deficient. Also after multivariableadjustment, 25(OH)D deficiency was associated withelevated parathyroid hormone levels (OR=3.8 (95% CI:2.0, 7.3), higher systolic blood pressure (2.24 mmHg(95% CI: 0.98, 3.50)) and lower serum calcium(−0.10 mg/dL (95% CI: −0.15, −0.04)) and HDLcholesterol (−3.03 mg/dL (95% CI: −5.02, −1.04)) levelscompared to those with 25(OH)D levels≥30 ng/mL.
Conclusions 25(OH)D deficiency is common in the generalUS pediatric population and associated with adversecardiovascular risk factors, suggesting the need for regularmonitoring of 25(OH)D levels in children, especially inhigh risk populations.
13Growth in pediatric dialysis patients with secondaryhyperparathyroidism (SHPT) treated with Cinacalcetand Calcitriol
DMatossian, A Idler, T Marson, J Eunice, Guillermo HidalgoPediatric Nephrology, Department of Pediatrics. Universityof Illinois at Chicago
Background Chronic Kidney Disease mineral and bonedisorder (CKD-MBD) is the new term that describeslaboratory, bone and growth abnormalities as a syndrome.Cinacalcet (CIN) suppresses parathyroid hormone (PTH)by activation of calcium-sensing receptor (CaSR) which isfound in a wide variety of tissues including the epiphysealplate. There is scarce information regarding the impact ongrowth of CIN in pediatric dialysis patients.Objective Learn the effect on growth in pediatric dialysispatients with severe SPTH who received CIN andCalcitriol.Methods Retrospective chart review (2005–2007). Calcium,phosphorous, PTH and height were measured. There wereseven patients on CIN and Calcitriol. Mean age was 16 yearsold±5.6 years. Age range was 5 to 21 years old. Gender, threefemale and four males. Ethnicity, three Hispanics and fourAfrican American. Height velocity charts for healthy boys andgirls used as control with standards.Results All patients grew in height except one (6/7, 86%).The patient whose height did not increase was a 20–21 yearold female. Maximum growth was 11 cm over 18 months,in the youngest patient (5 to 6 years old). Growth velocityfor that patient was 9.4 cm/year, which is 99th percentilefor age. Average age of the rest of the patients was 17 yearsand 9 months old±3 months. The 50th percentile of heightvelocity for that age is 1 cm/year. 50 % achieved the 50thpercentile for growth velocity.Discussion From this study, CIN does not impact growthadversely. Improvement of SHPT by CIN may favor bonehomeostasis and linear growth.
14Growth of kidney transplanted pediatric patients treatedwith rapamycin
DGonzález1, S Waller2, CD García3, A Alonso4. G Ariceta5,N Mejía6, O Álvarez-Garcia1, E Garcia1, J Rodríguez1,FA Ordoñez1, F Santos1
Pediatr Nephrol (2010) 25:789–799 795

1Hospital Central de Asturias, Oviedo, Spain. 2Royal SickChildren's Hospital, Glasgow, Scotland. 3Santo AntonioChildren ´s Hospital, Porto Alegre, Brazil. 4Hospital La Paz,Madrid, Spain. 5Hospital de Cruces, Barakaldo, Spain.6Hospital Universitario Fundación Santafé, Bogotá, Colombia
Background Experimental findings indicate that rapamycininhibits longitudinal growth by an unknown mechanismpotentially related with its inhibitory effects on cell prolifer-ation and vascular endothelial growth factor action. No datahave been published on growth of children treated withrapamycin.Objective To find out the growth pattern of kidneytransplanted children on rapamycin.Methods Multicenter observational clinical study. Heightand growth velocity Z scores (X±SD) of pediatricpatients with renal transplant treated with rapamycinwere calculated at 0, 6, 12 and 24 months after startingrapamycin and related with the dose of steroids and renalfunction (eGFR by Schwartz´s formula). A subgroup ofprepubertal patients younger than 6 years of age attransplantation, with good renal function (GFR >50 ml/min/1.73 m2), and low prednisone dose (<5 mg/day) wasspecifically analyzed.Results 25 children (19 males) were enrolled. The mean ageat transplantation was 8.0 years ( range 1.5–16.2) and the ageof rapamycin onset was 9.5 years (range 1.9–17.1). Nephro-toxicity was the most frequent indication to start therapy withrapamycin (11 patients). Rapamycin levels were between:6.35 and 8.32 ng/ml. Z score for height was −1.67±1.81,−1.74±1.71, −1.83±1.70 and −1.84±2.10 at 0, 6, 12 and24 months on rapamycin, respectively. During the rapamycintreatment period (between months 0 and 24), the eGFRincreased (p>0.05) from 68.3 to 85.5 ml/min/1.73 m2 and thesteroid dose decreased (p<0.05) from 9.1 to 2.6 mg/day. Inthe 10 prepubertal children with good renal function and lowsteroid dose, the Z height score was −1.59±1.81, −1.71±1.68, −1.77±1.75 and −1.68±1.93 at 0, 6, 12, and 24 monthson rapamycin, respectively.Conclusions Renal transplanted children on treatment withrapamycin do not exhibit catch-up growth, even those whoare prepubertal, have good renal function and receive lowsteroid dose.
15Increase in fat mass occurs rapidly after transplantation:predictor of future obesity?
S Eerens, K Van Hoeck, A Bael, D TrouetUniversity Hospital Antwerp, Belgium
Background Prednisone and calorie induced obesity is amajor concern after renal transplantation. We prospec-
tively monitored change in fat and lean tissue mass in6 children post transplantation with bio impedancespectroscopy.Methods In 6 patients receiving a renal transplant in 2008we assessed changes in body weight, lean tissue mass andfat mass from 1–3 months before to 3 months aftertransplantation. All had been treated with peritoneal dialysisand the immunosuppressive regimen consisted of basilix-imab, mycophenolate, cyclosporine and prednisone taperedfrom 60 mg/m² Body Surface Area at implantation to10 mg/m² BSA at 3 months.Results Four boys (age 3, 5, 6 and 14 year) and two girls(age 14y) had a change in bodyweight within 1 month aftertransplantation from 0 to ±10,7 kg. The largest increase offat mass in 4 patients (from 11,3 to 19,2%, 10,9 to 14,8%,29,2 to 35,6% and 5,2 to 14,1%) was already imminent at1 month after transplantation. The increase persisted in 2children but was reserved with reduction and arrest ofnasogastric tube feeding in a third patient, and in the fourthpatient there was a reduction due to obstructive ileusrequiring surgery.Conclusion Monitoring of fat mass changes early aftertransplantation might predict the development of obesityand offer the possibility of early intervention.
16Does kidney graft grow after transplantationin children?
LS Feltran, PC Koch-Nogueira, FA Silva, S Ajzen,AP Siva- FilhoUNIFESP–Hospital do Rim e Hipertensão–Brazil
Background Controversy exists with regard to the resultsof kidney transplants with pediatric donors.Objectives The aim of our study was to evaluate graftgrowth during the first year following transplantation,according to donor age.Methods Prospective study involving 63 children (boys=34), who underwent kidney transplantation and completed a12 months follow-up at Hospital do Rim e Hipertensão. Wecompared graft growth between: a) Group I–32 recipientsof pediatric deceased kidney donors (<16 years old) and b)Group II–31 recipients of adult living related kidney donors(>18 years old). Ultrasound graft volume measurementswere performed at 1 week, 1, 6 and 12 months aftertransplantation.Results Main demographic results were comparable be-tween groups, except for donor age. Anthropometric data(weight/age, height/age and BMI z score) were not differentbetween groups both before and after the kidney transplan-tation. Graft volume was statistically lower in Group I at1 week, 1 and 6 months, but was comparable between
796 Pediatr Nephrol (2010) 25:789–799
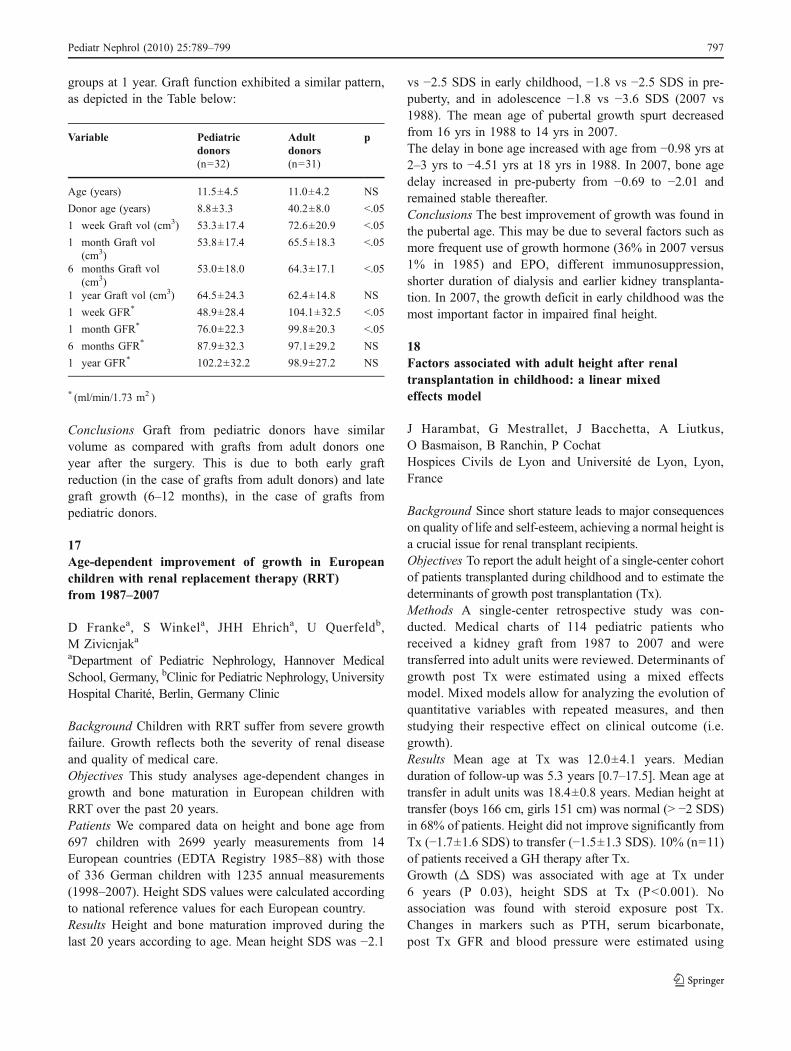
groups at 1 year. Graft function exhibited a similar pattern,as depicted in the Table below:
Variable Pediatricdonors
Adultdonors
p
(n=32) (n=31)
Age (years) 11.5±4.5 11.0±4.2 NS
Donor age (years) 8.8±3.3 40.2±8.0 <.05
1 week Graft vol (cm3) 53.3±17.4 72.6±20.9 <.05
1 month Graft vol(cm3)
53.8±17.4 65.5±18.3 <.05
6 months Graft vol(cm3)
53.0±18.0 64.3±17.1 <.05
1 year Graft vol (cm3) 64.5±24.3 62.4±14.8 NS
1 week GFR* 48.9±28.4 104.1±32.5 <.05
1 month GFR* 76.0±22.3 99.8±20.3 <.05
6 months GFR* 87.9±32.3 97.1±29.2 NS
1 year GFR* 102.2±32.2 98.9±27.2 NS
* (ml/min/1.73 m2 )
Conclusions Graft from pediatric donors have similarvolume as compared with grafts from adult donors oneyear after the surgery. This is due to both early graftreduction (in the case of grafts from adult donors) and lategraft growth (6–12 months), in the case of grafts frompediatric donors.
17Age-dependent improvement of growth in Europeanchildren with renal replacement therapy (RRT)from 1987–2007
D Frankea, S Winkela, JHH Ehricha, U Querfeldb,M ZivicnjakaaDepartment of Pediatric Nephrology, Hannover MedicalSchool, Germany, bClinic for Pediatric Nephrology, UniversityHospital Charité, Berlin, Germany Clinic
Background Children with RRT suffer from severe growthfailure. Growth reflects both the severity of renal diseaseand quality of medical care.Objectives This study analyses age-dependent changes ingrowth and bone maturation in European children withRRT over the past 20 years.Patients We compared data on height and bone age from697 children with 2699 yearly measurements from 14European countries (EDTA Registry 1985–88) with thoseof 336 German children with 1235 annual measurements(1998–2007). Height SDS values were calculated accordingto national reference values for each European country.Results Height and bone maturation improved during thelast 20 years according to age. Mean height SDS was −2.1
vs −2.5 SDS in early childhood, −1.8 vs −2.5 SDS in pre-puberty, and in adolescence −1.8 vs −3.6 SDS (2007 vs1988). The mean age of pubertal growth spurt decreasedfrom 16 yrs in 1988 to 14 yrs in 2007.The delay in bone age increased with age from −0.98 yrs at2–3 yrs to −4.51 yrs at 18 yrs in 1988. In 2007, bone agedelay increased in pre-puberty from −0.69 to −2.01 andremained stable thereafter.Conclusions The best improvement of growth was found inthe pubertal age. This may be due to several factors such asmore frequent use of growth hormone (36% in 2007 versus1% in 1985) and EPO, different immunosuppression,shorter duration of dialysis and earlier kidney transplanta-tion. In 2007, the growth deficit in early childhood was themost important factor in impaired final height.
18Factors associated with adult height after renaltransplantation in childhood: a linear mixedeffects model
J Harambat, G Mestrallet, J Bacchetta, A Liutkus,O Basmaison, B Ranchin, P CochatHospices Civils de Lyon and Université de Lyon, Lyon,France
Background Since short stature leads to major consequenceson quality of life and self-esteem, achieving a normal height isa crucial issue for renal transplant recipients.Objectives To report the adult height of a single-center cohortof patients transplanted during childhood and to estimate thedeterminants of growth post transplantation (Tx).Methods A single-center retrospective study was con-ducted. Medical charts of 114 pediatric patients whoreceived a kidney graft from 1987 to 2007 and weretransferred into adult units were reviewed. Determinants ofgrowth post Tx were estimated using a mixed effectsmodel. Mixed models allow for analyzing the evolution ofquantitative variables with repeated measures, and thenstudying their respective effect on clinical outcome (i.e.growth).Results Mean age at Tx was 12.0±4.1 years. Medianduration of follow-up was 5.3 years [0.7–17.5]. Mean age attransfer in adult units was 18.4±0.8 years. Median height attransfer (boys 166 cm, girls 151 cm) was normal (> −2 SDS)in 68% of patients. Height did not improve significantly fromTx (−1.7±1.6 SDS) to transfer (−1.5±1.3 SDS). 10% (n=11)of patients received a GH therapy after Tx.Growth (Δ SDS) was associated with age at Tx under6 years (P 0.03), height SDS at Tx (P<0.001). Noassociation was found with steroid exposure post Tx.Changes in markers such as PTH, serum bicarbonate,post Tx GFR and blood pressure were estimated using
Pediatr Nephrol (2010) 25:789–799 797
linear mixed models. The GFR drop was inverselyassociated with growth (P 0.05). Moreover, height SDSat transfer increased significantly according to thetransplantation era.Conclusions Renal transplantation in children does not leadto significant catch-up growth. Growth retardation postrenal transplantation is multifactorial and therefore influ-enced by the degree of pre Tx growth deficit, the age at Tx,and allograft function.
1925-(OH) vitamin D3 deficiency in pediatric renaltransplant recipients
S Menon, RP Valentini, G Kapur, V Bastian, TK MattooDivision of Pediatric Nephrology, Children's Hospital ofMichigan. Detroit, MI, USA
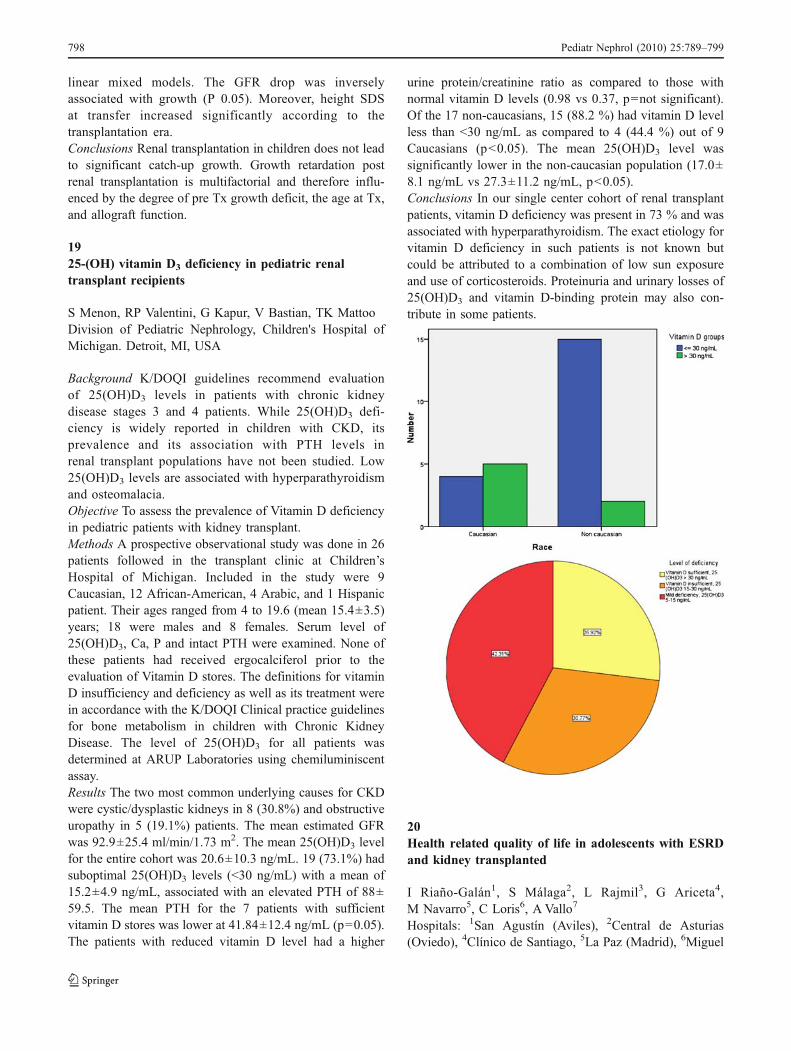
Background K/DOQI guidelines recommend evaluationof 25(OH)D3 levels in patients with chronic kidneydisease stages 3 and 4 patients. While 25(OH)D3 defi-ciency is widely reported in children with CKD, itsprevalence and its association with PTH levels inrenal transplant populations have not been studied. Low25(OH)D3 levels are associated with hyperparathyroidismand osteomalacia.Objective To assess the prevalence of Vitamin D deficiencyin pediatric patients with kidney transplant.Methods A prospective observational study was done in 26patients followed in the transplant clinic at Children’sHospital of Michigan. Included in the study were 9Caucasian, 12 African-American, 4 Arabic, and 1 Hispanicpatient. Their ages ranged from 4 to 19.6 (mean 15.4±3.5)years; 18 were males and 8 females. Serum level of25(OH)D3, Ca, P and intact PTH were examined. None ofthese patients had received ergocalciferol prior to theevaluation of Vitamin D stores. The definitions for vitaminD insufficiency and deficiency as well as its treatment werein accordance with the K/DOQI Clinical practice guidelinesfor bone metabolism in children with Chronic KidneyDisease. The level of 25(OH)D3 for all patients wasdetermined at ARUP Laboratories using chemiluminiscentassay.Results The two most common underlying causes for CKDwere cystic/dysplastic kidneys in 8 (30.8%) and obstructiveuropathy in 5 (19.1%) patients. The mean estimated GFRwas 92.9±25.4 ml/min/1.73 m2. The mean 25(OH)D3 levelfor the entire cohort was 20.6±10.3 ng/mL. 19 (73.1%) hadsuboptimal 25(OH)D3 levels (<30 ng/mL) with a mean of15.2±4.9 ng/mL, associated with an elevated PTH of 88±59.5. The mean PTH for the 7 patients with sufficientvitamin D stores was lower at 41.84±12.4 ng/mL (p=0.05).The patients with reduced vitamin D level had a higher
urine protein/creatinine ratio as compared to those withnormal vitamin D levels (0.98 vs 0.37, p=not significant).Of the 17 non-caucasians, 15 (88.2 %) had vitamin D levelless than <30 ng/mL as compared to 4 (44.4 %) out of 9Caucasians (p<0.05). The mean 25(OH)D3 level wassignificantly lower in the non-caucasian population (17.0±8.1 ng/mL vs 27.3±11.2 ng/mL, p<0.05).Conclusions In our single center cohort of renal transplantpatients, vitamin D deficiency was present in 73 % and wasassociated with hyperparathyroidism. The exact etiology forvitamin D deficiency in such patients is not known butcould be attributed to a combination of low sun exposureand use of corticosteroids. Proteinuria and urinary losses of25(OH)D3 and vitamin D-binding protein may also con-tribute in some patients.
20Health related quality of life in adolescents with ESRDand kidney transplanted
I Riaño-Galán1, S Málaga2, L Rajmil3, G Ariceta4,M Navarro5, C Loris6, A Vallo7
Hospitals: 1San Agustín (Aviles), 2Central de Asturias(Oviedo), 4Clínico de Santiago, 5La Paz (Madrid), 6Miguel
798 Pediatr Nephrol (2010) 25:789–799

Servet (Zaragoza), 7Cruces (Bilbao), 3Agència d’Avaluacióde Tecnologia (Barcelona)
Background Health-related quality of life (HRQOL) inadolescents with end-stage renal disease (ESRD) is animportant marker of disease burden. Our aim was toinvestigate HRQOL in a group of adolescents with ESRDand kidney transplanted.Methods A cross-sectional multicentric study wascarried out with 82 patients aged 10 to 21 years withESRD (70 kidney-transplanted and 12 on dialysis) atfive Spanish paediatric nephrology centres. HRQOL wasinvestigated with the Spanish version of the KidneyDisease Quality of Life Short Form (KDQOL-SF)instrument, consisting of kidney disease targeted scales(KDCS) to supplement the SF-36. Standardized scoresof the SF-·36 were computed according to the Spanishpopulation normative data. Clinical variables such asunderlying diagnosis, number of rejection episodes, pre-emptive transplantation, anaemia and height were alsoanalyzed.Results Kidney transplanted patients and patients ondialysis scored poorer than the general population in alldimensions of SF-36. Dialysis group scored lower thantransplanted patients in General Health (p=0,001). SpecificKDCS scales showed poorer HRQOL in dialysis than intransplanted patients on Symptoms/problems (81,8±12,7vs. 91,6±8,8; p=0,002), Effects of kidney disease on dailylife (78,2±11,8 vs. 87,0±14,9; p=0,05) and Burden ofKidney Disease (58,3±25,2 vs. 77,1±23,7; p=0,01). Trans-planted patients scored better on Health than dialysispatients (86,3±17,7 vs. 66,7±21,0; p=0,001). Anaemicpatients perceived more Burden of Kidney Disease(p=0,02). Height in transplanted patients was associatedwith Mental Health (p=0,04).Conclusions Kidney- transplanted adolescents had betterGeneral Health than dialysis group, but poorer than areference population. Hemoglobin levels and heightwere related with some scales of HRQOL evaluatedwith the KDQOL-SF. Further long-term prospectiveresearch is warranted.
21Different antenatal growth in children with congenital,hereditary and acquired chronic kidney disease
D Frankea, S Völkera, S Haasea, JHH Ehricha, U Querfeldb,L Pavicicc, M ZivicnjakaaDepartment of Pediatric Nephrology, Hannover MedicalSchool, Germany bClinic for Pediatric Nephrology, Uni-versity Hospital Charité Berlin, Germany, cFaculty ofKinesiology, University of Zagreb, Croatia
Background More than 50% of children with chronic kidneydisease (CKD) stage 3 and more have growth impairment.Data on intrauterine growth of these children is lacking.Objectives The extent of antenatal growth retardation wasstudied according to different aetiologies of CKD and itsimpact on postnatal growth failure was evaluated.Methods Birth data was collected in 427 children with a GFR<60 ml/min/1.73 m²; 257 newborns (NB) suffered fromcongenital, 90 from hereditary and 80 from acquired CKD.Results NB with congenital CKD had a significantly lowergestational age than NB with hereditary or acquired CKD(37.5 versus 39.2 and 38.9 weeks). The percentage ofpremature birth was 33% in congenital, 22% in hereditaryand 8%. NB with congenital CKD had a significantly lowerbirth weight (2918 g versus 3300 g in hereditary, 3205 gin acquired CKD), (p<0.001). Birth length and headcircumference differed significantly (p<0.001) in NB withcongenital compared to hereditary/acquired CRF. One fourthof children with congenital CKD were small for gestationalage.The APGAR after 5 und 10 min differed significantly (p<0.05) in NB with congenital CKD from NB with hereditaryand acquired CKD. No difference was found in umbilicalcord-pH.Conclusions Newborns with congenital CKD stage 3 weremore often premature and had a significantly higherintrauterine growth deficit than NB with hereditary andacquired CKD. This may lead to an increased risk for thedevelopment of a metabolic syndrome and cardiovascularcomorbidity later in life.
Pediatr Nephrol (2010) 25:789–799 799