
Drug-Eluting Microarrays for Cell-Based Screening of Chemical-Induced Apoptosis
Upload
independentCategory
view
2download
0
Escaned, Raúl Moreno, Cristina Fernández, Francisco Fernández-Avilés and Carlos MacayaFernando Alfonso, Rosana Hernández-Antolín, Javier Goicolea, Camino Bañuelos, Javier
Manel Sabaté, Pilar Jiménez-Quevedo, Dominick J. Angiolillo, Joan Antoni Gómez-Hospital,Sirolimus-Eluting Stent (DIABETES) Trial
Percutaneous Coronary Revascularization in Diabetic Patients: The Diabetes and Randomized Comparison of Sirolimus-Eluting Stent Versus Standard Stent for
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2005 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.105.562421
2005;112:2175-2183Circulation.
http://circ.ahajournals.org/content/112/14/2175World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2007/09/06/112.14.2175.DC1.htmlData Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from

Randomized Comparison of Sirolimus-Eluting Stent VersusStandard Stent for Percutaneous Coronary
Revascularization in Diabetic PatientsThe Diabetes and Sirolimus-Eluting Stent (DIABETES) Trial
Manel Sabaté, MD, PhD; Pilar Jiménez-Quevedo, MD; Dominick J. Angiolillo, MD;Joan Antoni Gómez-Hospital, MD, PhD; Fernando Alfonso, MD, PhD;
Rosana Hernández-Antolín, MD, PhD; Javier Goicolea, MD; Camino Bañuelos, MD;Javier Escaned, MD, PhD; Raúl Moreno, MD; Cristina Fernández, MD, PhD;
Francisco Fernández-Avilés, MD, PhD; Carlos Macaya, MD, PhD; for the DIABETES Investigators*
Background—Outcomes after percutaneous coronary interventions in diabetic patients are shadowed by the increased rateof recurrence compared with nondiabetic patients.
Methods and Results—We conducted a multicenter, randomized trial to demonstrate the efficacy of sirolimus-elutingstents compared with standard stents to prevent restenosis in diabetic patients with de novo lesions in native coronaryarteries. The primary end point of the trial was in-segment late lumen loss as assessed by quantitative coronaryangiography at 9-month follow-up. The trial was stratified by diabetes treatment status. One hundred sixty patients wererandomized to sirolimus-eluting stents (80 patients; 111 lesions) or standard stent implantation (80 patients; 110 lesions).On average, reference diameter was 2.34�0.6 mm, lesion length was 15.0�8 mm, and 13.1% of lesions were chronictotal occlusions. In-segment late lumen loss was reduced from 0.47�0.5 mm for standard stents to 0.06�0.4 mm forsirolimus stents (P�0.001). Target-lesion revascularization and major adverse cardiac event rates were significantlylower in the sirolimus group (31.3% versus 7.3% and 36.3% versus 11.3%, respectively; both P�0.001). Non–insulin-and insulin-requiring patients demonstrated similar reductions in angiographic and clinical parameters of restenosis aftersirolimus-eluting stent implantation. During the 9-month follow-up, stent thrombosis occurred in 2 patients afterstandard stent implantation. Conversely, this phenomenon was not seen in the sirolimus stent group.
Conclusions—This randomized trial demonstrated that sirolimus stent implantation is safe and efficacious in reducing bothangiographic and clinical parameters of restenosis compared with standard stents in diabetic patients with de novocoronary stenoses. (Circulation. 2005;112:2175-2183.)
Key Words: diabetes mellitus � restenosis � stents � trials
Diabetes mellitus is a pandemic that currently affectsmore than 150 million people worldwide.1 Atheroscle-
rotic macrovascular disease accounts for the majority ofmorbidity and mortality associated with type 2 diabetesmellitus.2 Specifically, cardiovascular disease is responsiblefor 75% of all hospital admissions and 80% of deaths indiabetic patients.3–6 Furthermore, coronary artery disease indiabetics exhibits distinctive characteristics that infer anincreased risk. Likewise, it is characterized by being diffuse,affecting more often the main stem and also the distalcoronary tree,7 and it usually presents an accelerated progres-
sion.8,9 Revascularization procedures in this setting presentworse long-term outcomes and increased restenosis rates thanthose in the nondiabetic population.10,11 Drug-eluting stentshave been demonstrated to be efficacious in the treatment oflesions of low to moderate risk.12–17 The potential efficacy ofsuch stents in the diabetic population derives from subgroupanalyses from randomized trials in which only patients withsingle-vessel disease with relatively large vessels (�2.5 mm)were included.18–20 We conducted a trial specifically aimed toassess the efficacy of the sirolimus-eluting stent for thetreatment of de novo coronary stenoses in diabetic patients.
Received May 15, 2005; revision received July 7, 2005; accepted July 8, 2005.From the Cardiovascular Institute, San Carlos University Hospital, Madrid, Spain (M.S., P. J.-Q., D.J.A., F.A., R.H.-A., C.B., J.E., R.M., C.M.);
Research Unit, Hospital Clı́nico San Carlos, Madrid, Spain (C.F.); Prínceps d’Espanya University Hospital, Barcelona, Spain (J.A.G.-H.); do MeixoeiroUniversity Hospital, Vigo, Spain (J.G.); and Clínico University Hospital, Valladolid, Spain (F.F-A.).
*The DIABETES Investigators are listed in the Appendix contained in the online-only Data Supplement, which can be found athttp://circ.ahajournals.org/cgi/content/full/112/14/2175/DC1.
Correspondence to Manel Sabaté, MD, PhD, Servicio de Cardiología Intervencionista, San Carlos University Hospital, Madrid 28040, Spain. [email protected]
© 2005 American Heart Association, Inc.
Circulation is available at http://www.circulationaha.org DOI: 10.1161/CIRCULATIONAHA.105.562421
2175
Interventional Cardiology
by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from

MethodsStudy Design and EligibilityThis multicenter, prospective, randomized study complied with theprovisions of the Declaration of Helsinki with regard to investigationin humans and was approved by the institutional review boards at all4 investigational sites. Written informed consent was obtained fromall patients. Patients were eligible for the study if they were diabetic(either non–insulin-dependent or insulin-dependent), according tothe World Health Organization Report.21 All patients included wereundergoing pharmacological treatment (insulin or hypoglycemicagents) for at least 1 month and presented de novo coronary stenosesin 1, 2, or 3 native vessels with symptoms or objective evidence ofischemia. Stenoses had to be amenable for stent implantation, withvessel size smaller than 4.0 mm (as assessed visually on angiogra-phy). Major exclusion criteria included impaired glucose tolerancewithout pharmacological treatment, gestational diabetes, or transienthyperglycemia; stenoses located in saphenous bypass, arterial bypassgrafting, unprotected left main, or that involved important sidebranches (�2 mm) that should be treated during the procedure; leftventricle ejection fraction �25%; prior treatment with intracoronarybrachytherapy or other drug-eluting stent at target site; restenoticlesions; known allergies to aspirin, ticlopidine, and clopidogrel;acute coronary syndromes with persistent ST elevation �72 hoursand/or creatine kinase (CK) twice the upper normal limit; non–ST-elevation acute coronary syndromes with CK twice the upper normallimit; severe hepatic or renal disease (creatinine clearance �30mL/min or hepatic enzymes twice the upper normal limit); and lifeexpectancy �1 year.
Before the index procedure, a telephonic randomization wasperformed with a computer-generated code to randomly assigneligible patients to treatment with sirolimus-eluting stent (Cypher,Cordis) or standard stent (Bx Velocity/Sonic, Cordis) in a 1:1 ratio.Randomization was performed after written informed consent wassigned. For patients with a single chronic total occluded vessel,randomization was performed after the occlusion was crossed with awire. The randomization was centralized and stratified by diabetestreatment status: insulin-dependent or non–insulin-dependent.
Coronary Stent ProcedureCoronary angioplasty was performed according to standard rules andthe experience of the operator. Neither ablative techniques (rotabla-tor, directional atherectomy) nor cutting balloons were allowed.However, predilation with the use of a conventional balloon beforestent implantation was optional. In case of predilation, the use of aballoon shorter than the stent was required in accordance withpreviously reported recommendations in the attempt to avoid geo-graphic miss.22 Both stent types were available in lengths of 8, 13,18, 23, 28, and 33 mm and in sizes of 2.25, 2.5, 2.75, 3.0, and3.5 mm. Multiple stent implantations were allowed to cover theentire diseased segment. In this event, a minimal overlapping(�1 mm) between stents was recommended. When multisegment ormultivessel treatment was performed, all implanted stents had to beof the same randomly assigned type. All patients were treated withoral aspirin (100 to 300 mg/d) and clopidogrel (loading dose 300 mg,then 75 mg/d for 1 year). During the procedure, an intravenousheparin bolus (100 IU/kg, or 70 IU/kg in case of administration ofglycoprotein IIb/IIIa inhibitors) was administered. The use of gly-coprotein IIb/IIIa inhibitors was recommended per protocol.
Data Collection, Follow-Up, and CoreLaboratory AnalysesThe study was designed by the authors, who had full access to thedata, analyzed the data, and controlled all decisions with regard topublication. This trial was not sponsored by industry. Clinicalfollow-up information was obtained for all patients by the researchcoordinators at each site during hospitalization, at 30 days, and at270 days and sent to a centralized coordinating center (San CarlosUniversity Hospital, Madrid, Spain). Additional clinical follow-up isscheduled at 12 months, 13 months (1 month after clopidogrel
withdrawal), and 2 years. All clinical end points were adjudicated byan independent clinical events committee that was unaware of thetreatment group assignments.
Coronary angiograms, obtained at baseline, at completion of thestenting procedure, and at 270 days of follow-up, were submitted tothe independent angiographic core laboratory (Health Science CenterJacksonville, University of Florida, Jacksonville, Fla) and wereanalyzed with the use of a computer-based system (CASS). Theangiographic analysis was blinded to treatment assignment. Lateluminal loss was defined as the difference between the minimalluminal diameter at the completion of the stenting procedure and thatmeasured during follow-up. “Binary” restenosis was defined asstenosis of more than 50% of the luminal diameter in the target lesionat follow-up. Quantitative angiographic measurements of the targetlesion were obtained in the “in-stent” zone (which included only thestented segment) and in the “in-segment” zone (which includedthe stented segment and the margins 5 mm proximal and distal to thestent).
Study End PointsThe primary end point of this study was in-segment late lumen lossas assessed by quantitative coronary angiography at 270-day follow-up. The secondary end points included other angiographic parame-ters of restenosis, such as binary restenosis and minimal luminaldiameter at 270-day follow-up; major adverse cardiac events, includ-ing cardiac death, myocardial infarction, target lesion (in-segmentzone) revascularization at 1, 9, 12, and 24-month follow-up; andstent thrombosis. Myocardial infarction after the procedure wasdefined as the occurrence of prolonged typical chest pain and/oreither the development of pathological Q waves that lasted at least0.04 second in at least 2 contiguous leads with an elevated CK-MBfraction level or, in the absence of pathological Q waves, anelevation in CK levels to more than twice the upper limit of normalwith an elevated CK-MB level. For this purpose, CK, CK-MB, andtroponin levels were obtained before the index procedure and at 6 to8 hours and 24 hours after the procedure. Additional blood sampleswere obtained in the event of chest pain, abnormal ECG, or elevatedenzymes. Stent thrombosis was defined as an acute coronary syn-drome with angiographic documentation of either vessel occlusion orthrombus within or adjacent to a previously successfully stentedvessel. In the absence of angiographic confirmation, either acutemyocardial infarction in the distribution of the treated vessel orsudden death was considered as stent thrombosis.
Statistical AnalysisThe planned sample size of 160 patients provided 90% statisticalpower to detect a 56% difference in the primary end point at 270-dayfollow-up (from in-segment late loss of 0.73 mm in the standard stentgroup23 to 0.32 mm in the sirolimus stent group) with an SD of 0.79and �-error of 0.05. We prespecified that the efficacy analysis andthe safety evaluation were to be based on data from all patients whounderwent randomization (intention-to-treat analysis).
Quantitative variables are presented as mean�SD and categoricalvariables as percentages. Quantitative variables were compared bymeans of the Student t test after evaluation of normal distribution(Kolmogorov-Smirnov) test. Categorical variables were comparedby means of the �2 test or Fisher exact test when at least 25% ofvalues showed an expected cell frequency below 5. The analyses ofthe primary end point and quantitative secondary end points werebased on a test of differences in means. Clinical secondary end pointswere compared on a per patient basis. Stratified analyses wereperformed to assess efficacy in the following prespecified variables:diabetes status, gender, left anterior descending artery, use ofglycoprotein IIb/IIIa inhibitors, chronic total occlusion, lesionlength, and stent size. Risk ratio and 95% CIs for in-segmentrestenosis were assessed between stent types. To identify clinical andangiographic factors that might be related to restenosis, backwardlogistic-regression models were used that included those variableswith a probability value �0.1 on univariate analysis. In addition, totake into account the intraindividual variability, the analysis oflesions (repeated assessments) was adjusted by means of a general-
2176 Circulation October 4, 2005
by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from

ized estimating equations model. Risk ratio was evaluated from alogistic regression model by having the final expression for the ORas e to the �-coefficient. The number needed to treat was calculatedas the inverse of the absolute risk reduction. All statistical analyseswere performed with the use of SPSS software (version 12.0) orSTATA (version 9.0), and all reported probability values were2-sided. We assumed significance at the 5% level (P�0.05).
ResultsBaseline CharacteristicsThe flow diagram of patients included in the present trial isdepicted in Figure 1. Between February 2003 and November2003, 170 patients were eligible for the study. Seven of themrefused to be included in the trial, and 3 additional patientswere not finally randomized because of the impossibility ofcrossing a total chronic occlusion when this was the onlystenosis to be treated. In the end, 160 patients were randomlyallocated to one of the treatment groups. One hundred elevenlesions were treated with stents in the 80 patients allocated tosirolimus stents, whereas 110 lesions were stented in the 80patients allocated to standard stents. No crossover of stenttype was reported by the investigators.
Baseline characteristics are presented in Table 1. Thegroups were well matched, with no differences in cardiaccoronary risk factors or prior cardiac history. Mean age was
66.5�9 years, and 62.5% of the patients were male. Aftersubrandomization, one third of the patients were undergoingtreatment with insulin, whereas two thirds were non–insulin-dependent diabetics. No differences were observed with thetype of oral agents used between groups; glitazones wereused in only 1.9% of patients. Multivessel disease wasidentified in 65% of the patients.
Lesion characteristics were also well matched betweengroups (Table 2). The majority of treated lesions (80.1%)were class B2 or C according to the American College ofCardiology/American Heart Association classification, theaverage reference diameter was 2.34�0.6 mm, and meanlesion length was 15.0�8 mm after chronic total occlusions(13.1% of lesions) were excluded from the analysis. Insulin-dependent diabetics presented a trend toward a smallerreference diameter and more severe stenoses than non–insulin-dependent diabetics (reference diameter 2.24�0.5versus 2.39�0.6 mm, P�0.08 and percentage diameter ste-nosis 65�17% versus 60�13%, P�0.07).
The clinical and angiographic characteristics of the presentcohort of patients conferred upon them a much higher riskprofile than for diabetics in previously reported substud-ies18–20 (Tables 1 and 2). Indeed, in the present studypopulation, 66% of lesions presented a reference diameter
Figure 1. Flow diagram of patients included in the trial.
Sabaté et al Sirolimus-Eluting vs Standard Stents in Diabetics 2177
by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from

smaller than 2.5 mm, 13% were chronic total occlusions, and43% were longer than 20 mm by quantitative coronaryangiography. In addition, 65% of patients had multivesseldisease, 32% had a creatinine clearance �60 mL/min, and51% evidenced poor metabolic glycemic control at the indexprocedure, defined as glycohemoglobin A1c �7%.
Procedural Data and In-Hospital OutcomesThere were no differences between groups in terms ofprocedural data. Glycoprotein IIb/IIIa inhibitors were admin-istered in 59% of the patients. Multivessel stenting wasperformed in 23.1% of patients and multisegment stenting in
13.8%. Mean�SD stent length was 23�12 mm (range 8 to87 mm); 1.4�0.6 lesions were treated per patient, and1.6�0.9 stents were implanted per patient. Forty-six percentof the implanted stents were �3.0 mm. Overlapping stentingwas needed in 17.2% of lesions, whereas direct stenting wasperformed in 34.4% of lesions.
During hospitalization, no major adverse cardiac eventsoccurred in the sirolimus stent group. Conversely, 1 cardiacdeath secondary to cardiac rupture (confirmed at necropsy)and 3 periprocedural non–Q-wave myocardial infarctionswere observed in the standard stent group, with an increase inCK levels of �3 times the upper normal limit.
TABLE 1. Baseline Clinical and Lesion Characteristics
Clinical CharacteristicsAll Patients
(n�160)Sirolimus Stent Group
(n�80)Standard Stent Group
(n�80) P
Age, y 66.5�9 65.9�9 67.2�10 0.38
Male sex, % 62.5 62.5 62.5 1.0
Insulin-dependent, % 33.1 32.5 33.8 0.87
Non–insulin-dependent, % 66.9 67.5 66.3 0.87
Hyperlipidemia, % 61.3 61.3 61.3 1.0
Hypertension, % 66.3 66.3 66.3 1.0
Smoking, % 47.5 45.0 50.0 0.44
Body mass index, % 29.1�4 29.3�4 28.8�3 0.55
Previous myocardial infarction, % 36.9 31.3 42.5 0.14
Previous angioplasty or cardiac surgery, % 18.7 20.0 17.6 0.51
Clinical status, % 0.51
Silent ischemia 6.9 5.0 8.8
Exertional angina 30.0 30.0 30.0
Unstable angina troponin (�) 40.0 45.0 35.0
Unstable angina troponin (�) 17.5 15.0 20.0
Elective post–myocardial infarction 5.6 5.0 6.2
Multivessel disease, % 65.0 61.3 68.8 0.32
Ejection fraction, % 65.4�13 66.9�13 63.8�13 0.13
Glycated hemoglobin A1c, % 7.3�1.4 7.4�1.5 7.3�1.4 0.65
Creatinine clearance, mL/min 72.9�26 70.7�23 75.3�30 0.70
Peripheral vasculopathy, % 10.6 11.3 10.0 0.79
Continuous data are expressed as mean�SD.
TABLE 2. Baseline Lesion Characteristics
Lesion CharacteristicsAll Lesions(n�221)
Sirolimus Stent Lesions(n�111)
Standard Stent Lesions(n�110) P
Lesion length,* mm 15.0�8 14.6�8 15.3�8 0.50
Reference diameter, mm 2.34�0.6 2.33�0.6 2.35�0.6 0.80
Minimal luminal diameter, mm 0.9�0.4 0.9�0.4 0.9�0.4 0.57
Percentage diameter stenosis, % 62�17 61�17 63�16 0.40
Chronic total occlusion, % 13.1 12.6 13.6 0.82
B2/C class lesion, % 80.1 79.3 80.9 0.78
Treated artery, % 0.46
Left anterior descending 41.2 38.7 43.6
Left circumflex 22.6 21.6 23.6
Right 36.2 39.6 32.7
Continuous data are expressed as mean�SD.*Chronic total occlusions were excluded from the analysis of lesion length.
2178 Circulation October 4, 2005
by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from

Quantitative Coronary AngiographyQuantitative coronary angiography was available in 92.7% ofthe lesions allocated to the sirolimus stent group and 91.8% ofthe lesions allocated to the standard stent group. Meanin-segment late lumen loss (the primary end point of thestudy) was reduced significantly in the sirolimus stent group,with an 87% in-segment relative reduction (0.47�0.5 mm forstandard stent versus 0.06�0.4 mm for sirolimus stent;P�0.001). This was mainly due to a marked reduction inin-stent late lumen loss (87% relative reduction:0.67�0.5 mm for standard stent versus 0.09�0.4 mm forsirolimus stent; P�0.001; Table 3). Frequency distributioncurves of late loss in both groups are depicted in Figure 2.Similarly, binary restenosis was significantly reduced in bothin-segment and in-stent zones (33.7% for standard stentingversus 7.8% for sirolimus stenting and 31.7% for standardstent versus 3.9% for sirolimus stent, respectively; P�0.0001for both comparisons). The length of the restenotic segment(defined as the length of the coronary segment presenting�50% diameter stenosis at follow-up angiography) showed atrend to be shorter in the sirolimus stent group (18.4�11 mmfor standard stent versus 11.9�7 mm for sirolimus stent;P�0.07). In addition, lesions treated with standard stentsshowed a trend toward presenting occlusive restenosis moreoften than those treated with sirolimus stents (5.5% versus0.9%, respectively; P�0.07). The incidence of significantedge effect was low and comparable between groups (2% forstandard stenting versus 3.9% for sirolimus stenting, respec-tively; P�0.68). Cumulative frequency distribution curves ofminimal luminal diameter are depicted in Figure 3. A shift to
the left was observed in the standard stent curve comparedwith the sirolimus stent curve, which demonstrates the morefavorable late angiographic findings in that group.
Clinical Outcomes at 30 and 270 DaysAt 30-day follow-up, 1 additional cardiac death due to suddendeath occurred in the standard stent group that was adjudi-cated as stent thrombosis by the clinical events committee(6.3% cumulative major adverse event rate at 30 days),whereas no events were observed in the sirolimus stent group(0% cumulative major adverse event rate; P�0.10).
At 270-day follow-up, the rate of major cardiac adverseevents was significantly lower in the sirolimus stent group(36.3% versus 10.0%, P�0.001) at the expense of a signifi-cant reduction in the need for subsequent revascularization(31.3% versus 6.3%, P�0.001). One patient in the sirolimusstent group died of refractory heart failure. The late (between30 and 270 days) stent thrombosis rate was 0% in thesirolimus stent group. Conversely, 1 patient from the standardstent group presented with stent thrombosis that led to anon–Q-wave myocardial infarction 2 months after the indexprocedure. In this patient, clopidogrel treatment was with-drawn 1 week before the event owing to gastrointestinalsurgery.
Insulin-Dependent Versus Non–Insulin-Dependent DiabeticsIn-segment and in-stent late loss and restenosis rates weresignificantly reduced in both insulin-dependent and non–insulin-dependent diabetic patients treated with sirolimus
TABLE 3. Late Lumen Loss and Restenosis Rates at 270-Day Follow-Up
Sirolimus Stent Group Standard Stent Group P
Overall n�103 n�101
In-segment late loss, mm 0.06�0.4 0.47�0.5 �0.001
In-stent late loss, mm 0.09�0.4 0.67�0.5 �0.001
Proximal reference late loss, mm �0.03�0.4 0.05�0.4 0.18
Distal reference late loss, mm �0.08�0.3 �0.01�0.4 0.11
In-segment restenosis rate, % 7.8 33.7 �0.001
In-stent restenosis rate, % 3.9 31.7 �0.001
Non–insulin-dependent patients n�73 n�68
In-segment late loss, mm 0.09�0.4 0.42�0.4 �0.001
In-stent late loss, mm 0.10�0.4 0.61�0.5 �0.001
Proximal reference late loss, mm 0.01�0.4 0.05�0.4 0.66
Distal reference late loss, mm �0.07�0.3 �0.01�0.4 0.32
In-segment restenosis rate, % 8.2 29.0 0.001
In-stent restenosis rate, % 2.7 27.5 �0.001
Insulin dependent n�30 n�33
In-segment late loss, mm �0.02�0.3 0.56�0.6 �0.001
In-stent late loss, mm 0.05�0.3 0.78�0.5 �0.001
Proximal reference late loss, mm �0.13�0.3 0.06�0.3 0.06
Distal reference late loss, mm �0.12�0.3 �0.01�0.5 0.19
In-segment restenosis rate, % 6.7 43.8 0.001
In-stent restenosis rate, % 6.7 40.6 0.002
Data are presented as mean�SD or percentages.
Sabaté et al Sirolimus-Eluting vs Standard Stents in Diabetics 2179
by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from

stent implantation (Table 3), as were target-lesion revascu-larization rates (from 33.3% to 5.9% for insulin-dependentdiabetics, P�0.004, and from 23% to 5.2% for non–insulin-dependent diabetics, P�0.002).
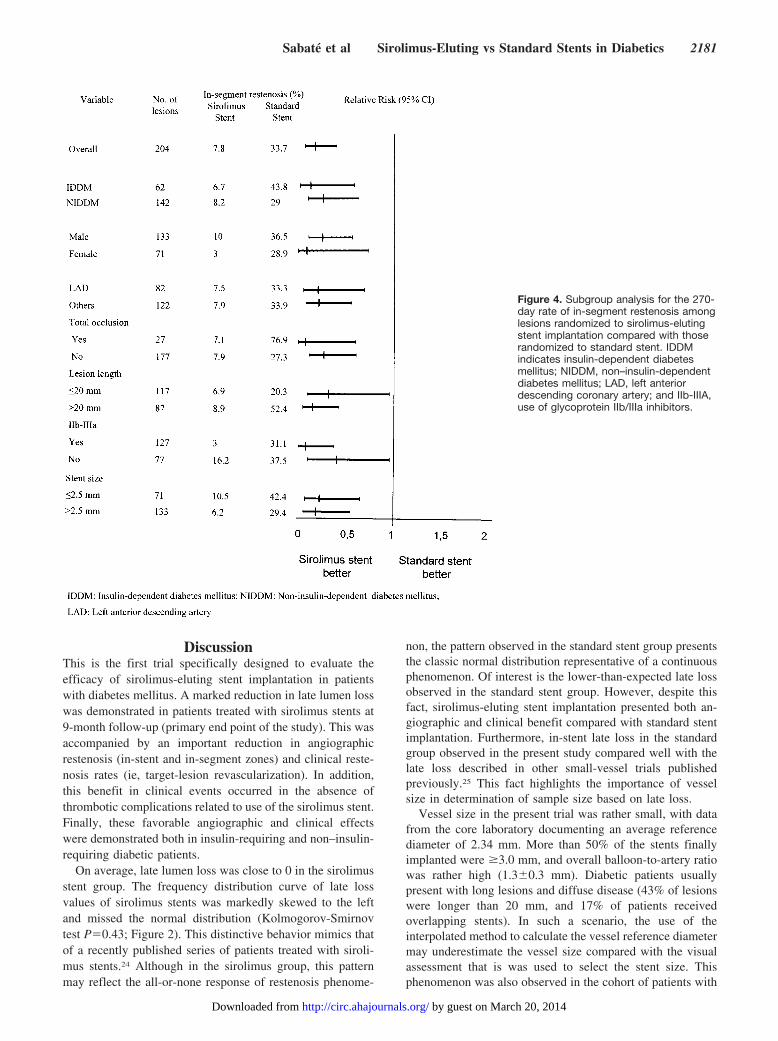
Subgroup AnalysesThe relative reduction in the risk of restenosis with the useof the sirolimus stent was concordant in all the prespeci-fied variables for subgroup analyses (Figure 4). Theassociation of known clinical angiographic risk factors forrestenosis with the treatment effect of the sirolimus stentwas evaluated with multivariable logistic regression mod-eling of the rate of in-segment restenosis within 270 days
adjusted by means of the generalized estimating equationmethod to account for repeated assessments. In this model,the sirolimus stent was significantly associated with areduced risk of restenosis (OR 0.28, 95% CI 0.10 to 0.76;P�0.01), as were age (OR 0.97, 95% CI 0.94 to 0.99,P�0.03) and minimal luminal diameter after stent implan-tation (OR per 1-mm increment 0.42, 95% CI 0.16 to 1.14,P�0.09). In addition, stent length was associated withan increased risk of restenosis (OR per 1-mm increment1.03, 95% CI 1.00 to 1.07, P�0.03). The number oflesions that needed to be treated with a sirolimus stent toavoid an episode of in-segment restenosis was 4 (95% CI3 to 6).
Figure 2. Frequency distribution of in-segment late lumen loss values at 270-day follow-up for all lesions treated with sirolimus-elutingstent (left) and standard stent (right). P�0.02 for sirolimus stents and P�0.43 for standard stent by Kolmogorov-Smirnov test.
Figure 3. Cumulative frequency distribu-tion curves for minimal luminal diameterin the group that received sirolimus-eluting stent and in the group thatreceived standard stent before andimmediately after the intervention and at270 days.
2180 Circulation October 4, 2005
by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from
DiscussionThis is the first trial specifically designed to evaluate theefficacy of sirolimus-eluting stent implantation in patientswith diabetes mellitus. A marked reduction in late lumen losswas demonstrated in patients treated with sirolimus stents at9-month follow-up (primary end point of the study). This wasaccompanied by an important reduction in angiographicrestenosis (in-stent and in-segment zones) and clinical reste-nosis rates (ie, target-lesion revascularization). In addition,this benefit in clinical events occurred in the absence ofthrombotic complications related to use of the sirolimus stent.Finally, these favorable angiographic and clinical effectswere demonstrated both in insulin-requiring and non–insulin-requiring diabetic patients.
On average, late lumen loss was close to 0 in the sirolimusstent group. The frequency distribution curve of late lossvalues of sirolimus stents was markedly skewed to the leftand missed the normal distribution (Kolmogorov-Smirnovtest P�0.43; Figure 2). This distinctive behavior mimics thatof a recently published series of patients treated with siroli-mus stents.24 Although in the sirolimus group, this patternmay reflect the all-or-none response of restenosis phenome-
non, the pattern observed in the standard stent group presentsthe classic normal distribution representative of a continuousphenomenon. Of interest is the lower-than-expected late lossobserved in the standard stent group. However, despite thisfact, sirolimus-eluting stent implantation presented both an-giographic and clinical benefit compared with standard stentimplantation. Furthermore, in-stent late loss in the standardgroup observed in the present study compared well with thelate loss described in other small-vessel trials publishedpreviously.25 This fact highlights the importance of vesselsize in determination of sample size based on late loss.
Vessel size in the present trial was rather small, with datafrom the core laboratory documenting an average referencediameter of 2.34 mm. More than 50% of the stents finallyimplanted were �3.0 mm, and overall balloon-to-artery ratiowas rather high (1.3�0.3 mm). Diabetic patients usuallypresent with long lesions and diffuse disease (43% of lesionswere longer than 20 mm, and 17% of patients receivedoverlapping stents). In such a scenario, the use of theinterpolated method to calculate the vessel reference diametermay underestimate the vessel size compared with the visualassessment that is was used to select the stent size. Thisphenomenon was also observed in the cohort of patients with
Figure 4. Subgroup analysis for the 270-day rate of in-segment restenosis amonglesions randomized to sirolimus-elutingstent implantation compared with thoserandomized to standard stent. IDDMindicates insulin-dependent diabetesmellitus; NIDDM, non–insulin-dependentdiabetes mellitus; LAD, left anteriordescending coronary artery; and IIb-IIIA,use of glycoprotein IIb/IIIa inhibitors.
Sabaté et al Sirolimus-Eluting vs Standard Stents in Diabetics 2181
by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from

very small vessels included in the Ravel trial.26 In that study,those vessels with reference diameter smaller than 2.36 mm(stratum I) presented a balloon-to-artery ratio of 1.3�0.1.Interestingly, 60.4% of the stents implanted in those vesselswere sized �3.0 mm. Conversely, in large vessels (stratumIII; �2.84 mm in reference vessel diameter), the balloon-to-artery ratio was 1.0�0.1.26
As observed in previous trials,12–17 the beneficial effect ofdrug-eluting stent implantation was tarnished by the occur-rence of edge effect. Overall, the degree of late loss at stentedges was comparable between the 2 groups (Table 3).However, in the sirolimus stent group, 50% of the restenosiswere located at the stent edges (3.9%). Conversely, in thestandard stent group, 94% of the restenoses were locatedwithin the stent. One of the plausible explanations for thisphenomenon includes the profound inhibitory effect of siroli-mus, as demonstrated by the virtual abolishment of late loss,which may magnify the small degree of lumen loss at theedges, resulting in significant restenosis by quantitativecoronary angiography analysis. Geographic miss may alsoexplain some of the failures at stent edges. Both injury at theperi-stent zone and incomplete coverage of the preexistinglesion may stimulate plaque proliferation,19,22 because itoccurred with the use of intracoronary brachytherapy.27
Insulin-dependent diabetics treated with a sirolimus stentevidenced the same degree of angiographic and clinicalbenefit as diabetics treated with oral agents. This findingexpands the benefit of rapamycin stents into a higher-riskpopulation with smaller vessels and more severe stenoses. Incontrast, the SIRIUS trial failed to demonstrate benefit fromsirolimus-eluting stent use in the subgroup of insulin-requiring diabetic patients owing to the high incidence ofedge effect.19
Dual antiplatelet treatment (aspirin and clopidogrel) wasprescribed for 1 year in both groups. In addition, the use ofglycoprotein IIb/IIIa inhibitors during the procedure wasultimately accomplished in �59% of patients. Under thisantiplatelet regimen, not a single stent thrombosis in thesirolimus-eluting stent group has been reported at 270-dayfollow-up, which suggests that the use of this stent in patientswith diabetes mellitus is safe.
Study LimitationsThis trial was not blinded; however, primary and secondaryangiographic end points were analyzed by an independentcore laboratory that had no access to randomization code. Inaddition, clinical events were adjudicated by the independentevents committee in a blinded manner.
Restenotic lesions were excluded from the trial. Thus, theefficacy of sirolimus-eluting stents in diabetic patients withrestenosis cannot be extrapolated from our results. Eightpercent of the patients did not return for angiographicfollow-up; however, baseline clinical and angiographic char-acteristics of this subgroup of patients did not differ fromthose who underwent the 9-month angiographic follow-up.
The use of stainless steel stents for the control group maymagnify the efficacy of sirolimus-eluting stents. The potentialof cobalt-chromium stents compared with drug-eluting stentrequires further assessment in randomized clinical trials.
The present trial was not designed to demonstrate whetherdiabetic patients had to be treated with percutaneous coronaryintervention or coronary bypass grafting. This will be ad-dressed in upcoming randomized trials comparing surgeryversus drug-eluting stent implantation.
AcknowledgmentsThis trial was supported in part by a grant from the Spanish Societyof Cardiology. Dr Jiménez-Quevedo received a Community ofMadrid and European Social Funding grant.
References1. King H, Aubert RE, Herman WH. Global burden of diabetes, 1995–2025:
prevalence, numerical estimates, and projections. Diabetes care. 1998;21:1414–1431.
2. American Diabetes Association. Role of cardiovascular risk factors inprevention and treatment of macrovascular disease in diabetes. DiabetesCare. 1989;12:573–579.
3. Laakso MLS. Epidemiology of macrovascular disease in diabetes.Diabetes Rev. 1997;5:294–315.
4. Geiss LS, Herman WH, Smith PJ. Mortality in non-insulin-dependentdiabetes. In: Harries MI, Cowie CC, Stern MP, et al, eds. Diabetes inAmerica. 2nd ed. Washington, DC: Government Printing Office; 1995:233–257.
5. Pyörolä K, Laakso M, Uusitupa M. Diabetes and atherosclerosis: anepidemiological view. Diabetes Metab Rev. 1987;3:463–524.
6. Barreto-Connor E. Does hyperglycaemia really cause coronary heartdisease? Diabetes Care. 1997;20:1620–1623.
7. Kip KE, Faxon DP, Detre KM, Yeh W, Kelsey SF, Currier JW. Coronaryangioplasty in diabetic patients: the National Heart, Lung, and BloodInstitute Percutaneous Transluminal Coronary Angioplasty Registry. Cir-culation. 1996;94:1818–1825.
8. Waller BF, Palumbo PJ, Lie JT, Roberts WC. Status of the coronaryarteries at necropsy in diabetes mellitus with onset after 30 years: analysisof 229 diabetic patients with and without clinical evidence of coronaryheart disease and comparison to 183 control subjects. Am J Med. 1980;69:498–506.
9. Rozenman Y, Sapoznikov D, Mosseri M, Gilon D, Lotan C, Nassar H,Weiss AT, Hasin Y, Gotsman MS. Long-term angiographic follow-up ofcoronary balloon angioplasty in patients with diabetes mellitus a clue tothe explanation of the results of the BARI study. J Am Coll Cardiol.1997;30:1420–1425.
10. Stein B, Weintraub WS, Gebhart SP, Cohen-Bernstein CL, Grosswald R,Liberman HA, Douglas JS Jr, Morris DC, King SB III. Influence ofdiabetes mellitus on early and late outcome after percutaneous coronaryangioplasty. Circulation. 1995;91:979–989.
11. Elezi S, Kastrati A, Pache J, Wehinger A, Hadamitzky M, Dirschinger J,Neumann FJ, Schomig A. Diabetes mellitus and the clinical and angio-graphic outcome after coronary stent placement. J Am Coll Cardiol.1998;32:1866–1873.
12. Morice MC, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E, Perin M,Colombo A, Schuler G, Barragan P, Guagliumi G, Molnar F, Falotico R;RAVEL Study Group. A randomized comparison of a sirolimus-elutingstent with a standard stent for coronary revascularization. N Engl J Med.2002;346:1773–1780.
13. Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR,O’Shaughnessy C, Caputo RP, Kereiakes DJ, Williams DO, Teirstein PS,Jaeger JL, Kuntz RE; SIRIUS Investigators. Sirolimus-eluting stentsversus standard stents in patients with stenosis in a native coronary artery.N Engl J Med. 2003;349:1315–1323.
14. Schofer J, Schluter M, Gershlick AH, Wijns W, Garcia E, Schampaert E,Breithardt G; E-SIRIUS Investigators. Sirolimus-eluting stents fortreatment of patients with long atherosclerotic lesions in small coronaryarteries: double-blind, randomised controlled trial (E-SIRIUS). Lancet.2003;362:1093–1099.
15. Schampaert E, Cohen EA, Schluter M, Reeves F, Traboulsi M, Title LM,Kuntz RE, Popma JJ; C-SIRIUS Investigators. The Canadian study of thesirolimus-eluting stent in the treatment of patients with long de novolesions in small native coronary arteries (C-SIRIUS). J Am Coll Cardiol.2004;43:1110–1115.
16. Colombo A, Drzewiecki J, Banning A, Grube E, Hauptmann K, Silber S,Dudek D, Fort S, Schiele F, Zmudka K, Guagliumi G, Russell ME;
2182 Circulation October 4, 2005
by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from

TAXUS II Study Group. Randomized study to assess the effectiveness ofslow- and moderate-release polymer-based paclitaxel-eluting stents forcoronary artery lesions. Circulation. 2003;108:788–794.
17. Stone GW, Ellis SG, Cox DA, Hermiller J, O’Shaughnessy C, Mann JT,Turco M, Caputo R, Bergin P, Greenberg J, Popma JJ, Russell ME;TAXUS-IV Investigators. A polymer-based, paclitaxel-eluting stent inpatients with coronary artery disease. N Engl J Med. 2004;350:221–231.
18. Abizaid A, Costa MA, Blanchard D, Albertal M, Eltchaninoff H,Guagliumi G, Geert-Jan L, Abizaid AS, Sousa AG, Wuelfert E, Wietze L,Sousa JE, Serruys PW, Morice MC; Ravel Investigators. Sirolimus-eluting stents inhibit neointimal hyperplasia in diabetic patients: insightsfrom the RAVEL trial. Eur Heart J. 2004;2:107–112.
19. Moussa I, Leon MB, Baim DS, O’Neill WW, Popma JJ, Buchbinder M,Midwall J, Simonton CA, Keim E, Wang P, Kuntz RE, Moses JW. Impactof sirolimus-eluting stents on outcome in diabetic patients: a SIRIUS(SIRolImUS-coated Bx Velocity balloon-expandable stent in thetreatment of patients with de novo coronary artery lesions) substudy.Circulation. 2004;109:2273–2278.
20. Hermiller JB, Raizner A, Cannon L, Gurbel PA, Kutcher MA, Wong SC,Russell ME, Ellis SG, Mehran R, Stone GW; TAXUS-IV Investigators.Outcomes with the polymer-based paclitaxel-eluting TAXUS stent inpatients with diabetes mellitus: the TAXUS-IV trial. J Am Coll Cardiol.2005;45:1172–1179.
21. Alberti KGMM, Zimmet PZ, for the WHO Consultation. Definition,diagnosis and classification of diabetes mellitus and its complications,part 1: diagnosis and classification of diabetes mellitus: provisional reportof a WHO consultation. Diabet Med. 1998;15:539–553.
22. Angiolillo DJ, Sabaté M, Alfonso F, Macaya C. “Candy wrapper” effectafter drug-eluting stent implantation: deja vu or stumbling over the samestone again? Cathet Cardiovasc Interv. 2004;61:387–391.
23. Sabaté M, Pimentel G, Prieto C, Corral JM, Bañuelos C, Angiolillo DJ,Alfonso F, Hernandez-Antolin R, Escaned J, Fantidis P, Fernandez C,Fernandez-Ortiz A, Moreno R, Macaya C. Intracoronary brachytherapyafter stenting de novo lesions in diabetic patients: results of a randomizedintravascular ultrasound study. J Am Coll Cardiol. 2004;44:520–527.
24. Lemos PA, Mercado N, van Domburg RT, Kuntz RE, O’Neill W, SerruysPW. Comparison of late luminal loss response pattern after sirolimus-eluting stent implantation or conventional stenting. Circulation. 2004;110:3199–3205.
25. Moreno R, Fernández C, Alfonso F, Hernández R, Pérez-Vizcayno MJ,Escaned J, Sabaté M, Bañuelos C, Angiolillo DJ, Azcona L, Macaya C.Coronary stenting versus balloon angioplasty in small vessels. J Am CollCardiol. 2004;43:1964–1972.
26. Regar, E, Serruys PW, Bode C, Holubarsch C, Guermonprez JL, WijnsW, Bartorelli A, Constatini C, Degertekin M, Tanabe K, Disco C,Wuelfert E, Morice MC, on behalf of the RAVEL Study Group. Angio-graphic findings of the multicenter randomized study with the sirolimus-eluting Bx Velocity balloon-expandable stent (RAVEL): sirolimus-eluting stents inhibit restenosis irrespective of the vessel size. Circulation.2002;106:1949–1956.
27. Sabaté M, Costa MA, Kozuma K, Kay IP, van der Giessen WJ, Coen VL,Ligthart JM, Serrano P, Levendag PC, Serruys PW. Geographic miss: acause of treatment failure in radio-oncology applied to intracoronaryradiation therapy. Circulation. 2000;101:2467–2471.
Sabaté et al Sirolimus-Eluting vs Standard Stents in Diabetics 2183
by guest on March 20, 2014http://circ.ahajournals.org/Downloaded from
Copyright © 2022 FDOKUMEN




















