
Impacted maxillary central incisor, canine, and second molar with 2 supernumerary teeth and an...
10
CASE REPORT Impacted maxillary central incisor, canine, and second molar with 2 supernumerary teeth and an odontoma K. Nagaraj, a Madhur Upadhyay, b and Sumit Yadav c Belgaum, India, Farmington, Conn, and Indianapolis, Ind This report describes the orthodontic treatment of a 14-year-old boy who had 3 impacted maxillary teeth (right canine, left central incisor, and left second molar), 2 supernumerary teeth, and an odontoma. The treatment protocol involved surgical intervention followed by sequential traction of the 3 impacted teeth. The patient’s smile dramatically improved after orthodontic treatment. Good posterior occlusion was achieved. However, long-term monitoring of the stability and periodontal health is critical. (Am J Orthod Dentofacial Orthop 2009;135:390-9) I mpaction is the total or partial lack of eruption of a tooth well after the normal age of eruption. 1 The most commonly impacted maxillary tooth is the canine, occurring in less than 2% of the general population, 2 followed by the central incisor with a frequency of 0.06% to 0.2%. 3 According to Kokich and Mathews, 4 the cause of labial impaction of the canines probably is related to either a retained deciduous tooth, diversion of the canine tooth bud, or idiopathic failure of eruption of unknown origin. The labial impaction of a maxillary central incisor can occur because of an un- treated mesiodens or supernumerary tooth. 5 Odontomas, anomalies in maxillary lateral incisors, and disturbances in the eruption path related to crowding can also cause impaction, but are somewhat less common. 6,7 Supernumerary teeth occur in both the deciduous and permanent dentitions. Like impactions, supernu- merary teeth can be unilateral or bilateral and can occur singly or a few at a time. 8 They are found more frequently in the maxilla, especially in the anterior segment, than in the mandible. 9 This report describes the sequential management of 3 impacted teeth, 2 supernumerary teeth, and 1 odon- toma in the maxillary arch. The treatment success was the result of the combined efforts of the orthodontist, the oral surgeon, and the patient. DIAGNOSIS AND ETIOLOGY A 14-year, 7-month-old boy came to the Depart- ment of Orthodontics at KLES’ Academy of Higher Education and Research, Belgaum, India, with the chief complaint of an unesthetic smile due to irregularly placed maxillary front teeth (Figs 1-3). He was physi- cally healthy and had no history of medical or dental trauma. No signs or symptoms of temporomandibular joint dysfunction were noted at the initial examination. The extraoral clinical examination showed a convex profile caused by a deficient chin. There were no gross asymmetries. The intraoral examination showed an Angle Class I malocclusion with moderate crowding of 2.5 mm in the mandibular arch. Three teeth were missing in the maxillary arch: right canine, left central incisor, and left second molar. The maxillary midline was shifted to the left by 3 mm. A supernumerary tooth was present between the right lateral and central inci- sors. Overbite was 60% to 70%, with an exaggerated curve of Spee of 3.5 mm. Cephalometrically, the patient had a Class II skel- etal relationship with slight retrognathism of the man- dible (ANB angle, 5°). The maxillary and mandibular incisors were retroclined, resulting in an excessive interincisal angle (Table). The panoramic radiograph showed all permanent teeth, including the maxillary and mandibular third molar buds. The maxillary left third molar bud was located lingually to the buccally impacted second molar; both were competing for the same space. The maxillary right canine and left central incisor were also impacted. The crown of the impacted a Assistant professor, Department of Orthodontics, KLES’ Institute of Dental Sciences, Belgaum, India. b Resident, Division of Orthodontics, Department of Craniofacial Sciences, School of Dental Medicine, University of Connecticut, Farmington, Conn; Assistant professor, Department of Orthodontics, KLES’ Institute of Dental Sciences, Belgaum, India. c PhD student, Mineralized Tissue Histology and Research Laboratory, Section of Orthodontics, Indiana School of Dentistry, Indiana University Purdue University, Indianapolis, Ind. Reprint requests to: Madhur Upadhyay, Division of Orthodontics, Department of Craniofacial Sciences, School of Dental Medicine, University of Connecticut, 263 Farmington Avenue, Farmington, CT 06105; e-mail, [email protected]. Submitted, August 2006; revised and accepted, December 2006. 0889-5406/$36.00 Copyright © 2009 by the American Association of Orthodontists. doi:10.1016/j.ajodo.2006.12.023 390
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Impacted maxillary central incisor, canine, and second molar with 2 supernumerary teeth and an...
CASE REPORT
Impacted maxillary central incisor, canine, andsecond molar with 2 supernumerary teeth andan odontomaK. Nagaraj,a Madhur Upadhyay,b and Sumit Yadavc
Belgaum, India, Farmington, Conn, and Indianapolis, Ind
This report describes the orthodontic treatment of a 14-year-old boy who had 3 impacted maxillary teeth(right canine, left central incisor, and left second molar), 2 supernumerary teeth, and an odontoma. Thetreatment protocol involved surgical intervention followed by sequential traction of the 3 impacted teeth. Thepatient’s smile dramatically improved after orthodontic treatment. Good posterior occlusion was achieved.However, long-term monitoring of the stability and periodontal health is critical. (Am J Orthod DentofacialOrthop 2009;135:390-9)
Impaction is the total or partial lack of eruption ofa tooth well after the normal age of eruption.1 Themost commonly impacted maxillary tooth is the
canine, occurring in less than 2% of the generalpopulation,2 followed by the central incisor with afrequency of 0.06% to 0.2%.3 According to Kokich andMathews,4 the cause of labial impaction of the caninesprobably is related to either a retained deciduous tooth,diversion of the canine tooth bud, or idiopathic failure oferuption of unknown origin. The labial impaction of amaxillary central incisor can occur because of an un-treated mesiodens or supernumerary tooth.5 Odontomas,anomalies in maxillary lateral incisors, and disturbances inthe eruption path related to crowding can also causeimpaction, but are somewhat less common.6,7
Supernumerary teeth occur in both the deciduousand permanent dentitions. Like impactions, supernu-merary teeth can be unilateral or bilateral and can occursingly or a few at a time.8 They are found morefrequently in the maxilla, especially in the anteriorsegment, than in the mandible.9
This report describes the sequential management of3 impacted teeth, 2 supernumerary teeth, and 1 odon-aAssistant professor, Department of Orthodontics, KLES’ Institute of DentalSciences, Belgaum, India.bResident, Division of Orthodontics, Department of Craniofacial Sciences,School of Dental Medicine, University of Connecticut, Farmington, Conn;Assistant professor, Department of Orthodontics, KLES’ Institute of DentalSciences, Belgaum, India.cPhD student, Mineralized Tissue Histology and Research Laboratory, Sectionof Orthodontics, Indiana School of Dentistry, Indiana University PurdueUniversity, Indianapolis, Ind.Reprint requests to: Madhur Upadhyay, Division of Orthodontics, Department ofCraniofacial Sciences, School of Dental Medicine, University of Connecticut, 263Farmington Avenue, Farmington, CT 06105; e-mail, [email protected], August 2006; revised and accepted, December 2006.0889-5406/$36.00Copyright © 2009 by the American Association of Orthodontists.doi:10.1016/j.ajodo.2006.12.023
390
toma in the maxillary arch. The treatment success wasthe result of the combined efforts of the orthodontist,the oral surgeon, and the patient.
DIAGNOSIS AND ETIOLOGY
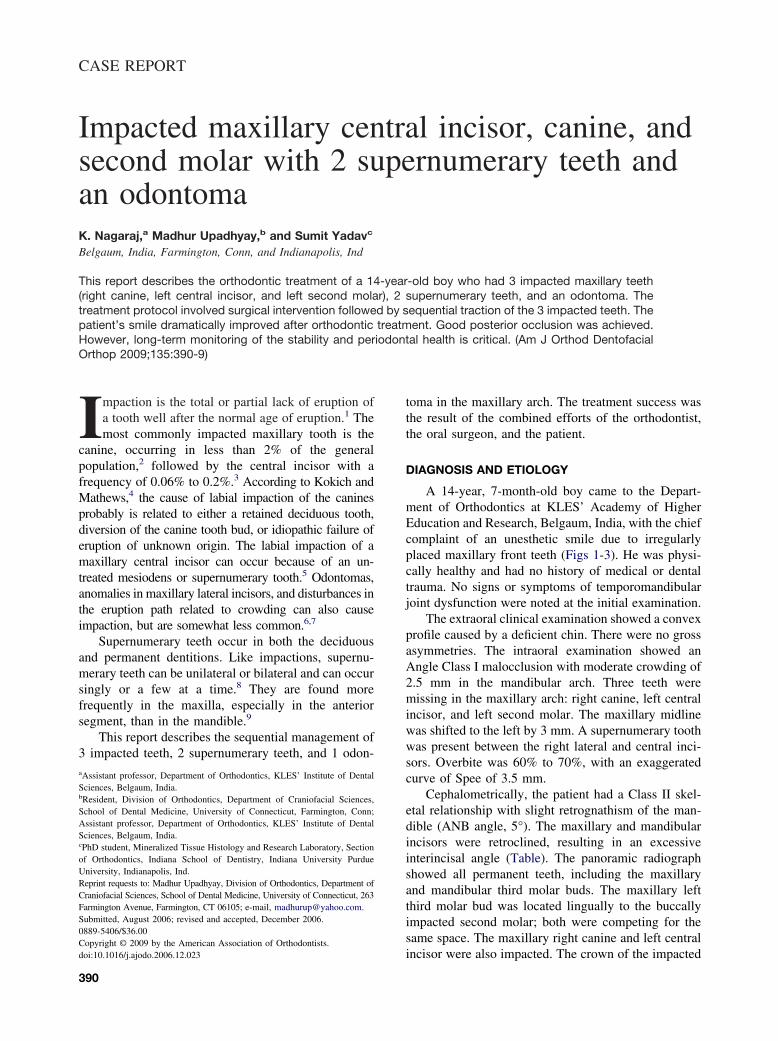
A 14-year, 7-month-old boy came to the Depart-ment of Orthodontics at KLES’ Academy of HigherEducation and Research, Belgaum, India, with the chiefcomplaint of an unesthetic smile due to irregularlyplaced maxillary front teeth (Figs 1-3). He was physi-cally healthy and had no history of medical or dentaltrauma. No signs or symptoms of temporomandibularjoint dysfunction were noted at the initial examination.
The extraoral clinical examination showed a convexprofile caused by a deficient chin. There were no grossasymmetries. The intraoral examination showed anAngle Class I malocclusion with moderate crowding of2.5 mm in the mandibular arch. Three teeth weremissing in the maxillary arch: right canine, left centralincisor, and left second molar. The maxillary midlinewas shifted to the left by 3 mm. A supernumerary toothwas present between the right lateral and central inci-sors. Overbite was 60% to 70%, with an exaggeratedcurve of Spee of 3.5 mm.
Cephalometrically, the patient had a Class II skel-etal relationship with slight retrognathism of the man-dible (ANB angle, 5°). The maxillary and mandibularincisors were retroclined, resulting in an excessiveinterincisal angle (Table). The panoramic radiographshowed all permanent teeth, including the maxillaryand mandibular third molar buds. The maxillary leftthird molar bud was located lingually to the buccallyimpacted second molar; both were competing for thesame space. The maxillary right canine and left centralincisor were also impacted. The crown of the impacted
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 135, Number 3
Nagaraj, Upadhyay, and Yadav 391
and intraoral photographs.
canine was displaced in the mesiobuccal directionpartially overlapping the adjacent lateral incisor. Theright maxillary lateral and central incisors had dilac-erated roots with an odontoma located apically totheir root tips; it was asymptomatic. Additionally, animpacted supernumerary tooth (mesiodens) waslocated palatally to the impacted central incisor(Fig 4). Periapical radiographs (Fig 5) were taken withthe Clark’s tube-shift technique to confirm the labialand buccal positions of the impacted teeth. Growthanalysis indicated that the patient was in the pubertalgrowth spurt.
TREATMENT OBJECTIVES
The initial treatment plan was to extract the super-numerary tooth between the maxillary right lateral
Fig 1. Pretreatment facial
incisor and the maxillary right central incisor, align andlevel the maxillary and mandibular teeth, and createspace for the impacted canine and incisor, and simul-taneously correct the midline. Subsequently, in thesurgical phase, the treatment plan was to extract theimpacted supernumerary tooth, the maxillary left thirdmolar bud, and the odontoma. In addition, we plannedto expose the impacted teeth and bond attachments toerupt them carefully to their normal positions in thedental arch to achieve a stable functional occlusion withnormal overbite and a Class I canine relationship, withminimal impact on the soft-tissue profile.
TREATMENT ALTERNATIVES
Several possible treatment options were explainedto the patient and his parents. Along with the supernu-
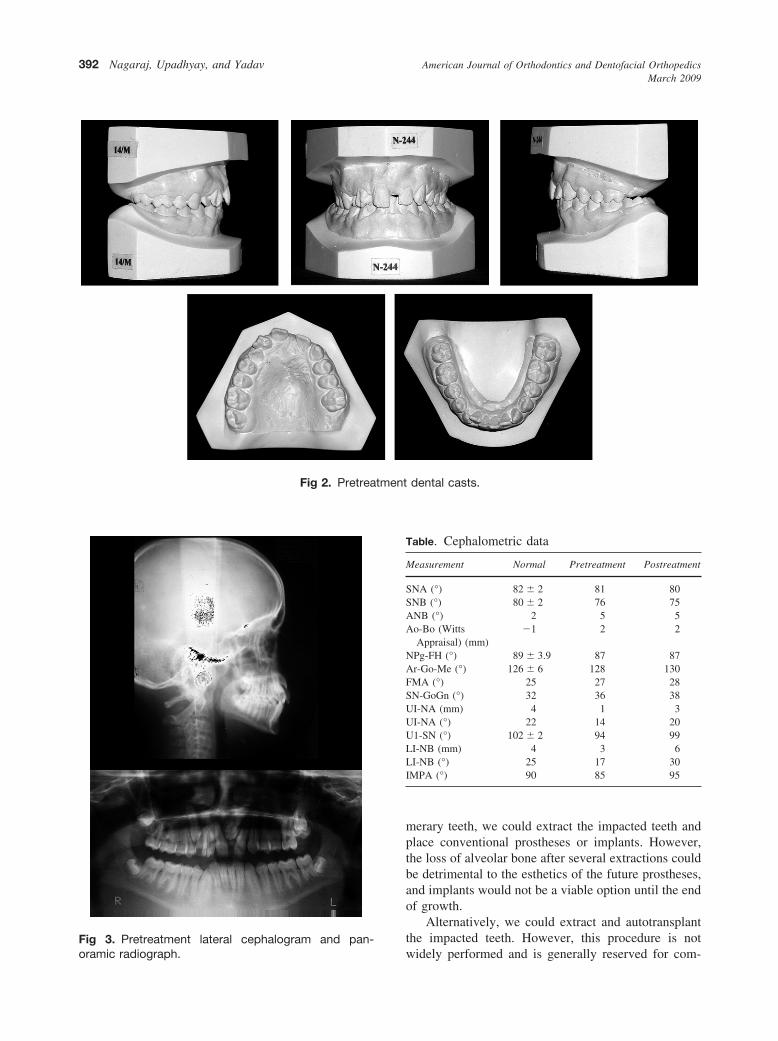
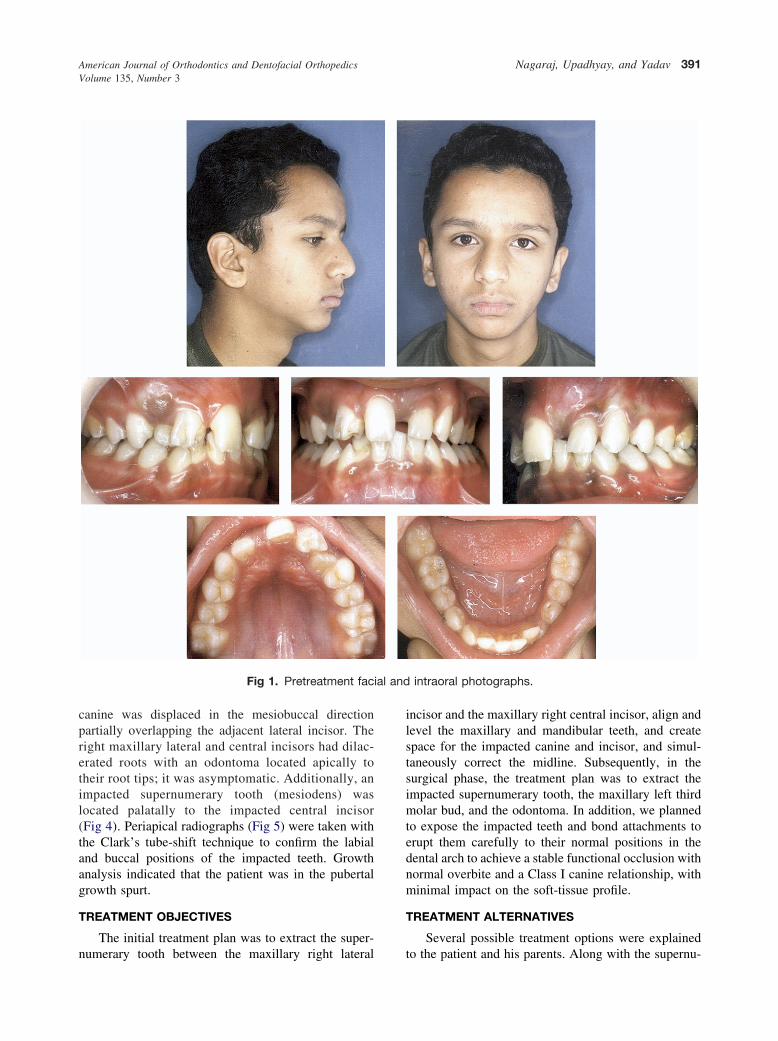
Fig 2. Pretreatment dental casts.
American Journal of Orthodontics and Dentofacial OrthopedicsMarch 2009
392 Nagaraj, Upadhyay, and Yadav
Fig 3. Pretreatment lateral cephalogram and pan-oramic radiograph.
merary teeth, we could extract the impacted teeth andplace conventional prostheses or implants. However,the loss of alveolar bone after several extractions couldbe detrimental to the esthetics of the future prostheses,and implants would not be a viable option until the endof growth.
Alternatively, we could extract and autotransplantthe impacted teeth. However, this procedure is notwidely performed and is generally reserved for com-
Table. Cephalometric data
Measurement Normal Pretreatment Postreatment
SNA (°) 82 � 2 81 80SNB (°) 80 � 2 76 75ANB (°) 2 5 5Ao-Bo (Witts
Appraisal) (mm)�1 2 2
NPg-FH (°) 89 � 3.9 87 87Ar-Go-Me (°) 126 � 6 128 130FMA (°) 25 27 28SN-GoGn (°) 32 36 38UI-NA (mm) 4 1 3UI-NA (°) 22 14 20U1-SN (°) 102 � 2 94 99LI-NB (mm) 4 3 6LI-NB (°) 25 17 30IMPA (°) 90 85 95

plex disorders, such as congenital cleidocranial dyspla-sia, cysts, and cleft palate.
Finally, it was decided to attempt forced eruption andalignment of the impacted teeth. Both a periodontist andan oral surgeon were consulted to formulate the finaltreatment plan. In spite of the fact that this treatment wasnot risk-free compared with other alternatives, the parentswanted to try to save the teeth and bring them to properocclusion. They were asked to sign a consent form.
TREATMENT PROGRESS
After the supernumerary tooth between the centraland lateral incisors was extracted, the maxillary molars
Fig 4. Schematic illustration of the dental anomalies inthe maxillary arch: 1, impacted right canine; 2, odon-toma; 3 and 4, dilacerated roots of right central andlateral incisors; 5, supernumerary tooth; 6, impactedsupernumerary tooth; 7, impacted left central incisor;8, left third molar bud; 9, impacted left second molar(buccally placed).
Fig 5. Pretreatment periapical radiographs: A and B,the maxillary anterior region (tube-shift technique);C, impacted maxillary left second molar.
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 135, Number 3
were banded, and the remaining teeth were bonded withan 0.022 � 0.028-in preadjusted edgewise appliance.The bracket on the lateral incisor was rotated 180° toobtain labial root torque on this tooth. After the initialleveling and aligning, a 0.017 � 0.025-in stainless steelarchwire was placed in the maxillary arch with anopen-coil spring in the position of the right impactedcanine to hold and, if necessary, create space for itseruption. Additionally, chain elastics were used to closethe space between the 2 incisors. After 6 months ofactive treatment, the maxillary canine started to eruptspontaneously (Fig 6). This was verified clinically bydigital palpation. At this stage, the mandibular arch wasbanded and bonded. Reverse curve archwires were usedto level and align the mandibular teeth.
After gaining sufficient space between the incisors,the patient was referred to the oral surgeon for thesurgical procedures of the initial treatment plan. A widemucoperiosteal flap, similar to that described in the
Fig 6. Maxillary occlusal radiograph showing sponta-neous eruption of the canine. Note the space created bythe open-coil spring.
Fig 7. Midtreatment panoramic radiograph taken im-mediately after bonding the Begg bracket on the im-pacted incisor.
Nagaraj, Upadhyay, and Yadav 393

Fig 8. Progress intraoral photographs showing eruption of the impacted incisor.
Fig 9. Schematic illustration of the treatment strategy used for eruption of the impacted centralincisor: A, elastic chain from the incisor to the left canine causing the crown to tip distally and theroot mesially; B, the incisor is moved vertically; C, the incisor in position.
Fig 10. Eruption of the impacted left second molar.
American Journal of Orthodontics and Dentofacial OrthopedicsMarch 2009
394 Nagaraj, Upadhyay, and Yadav
closed-eruption technique was raised over the impactedincisor.4 A Begg bracket was bonded on the labialsurface of the incisor. The flap was returned to the sameposition and sutured, leaving a tied 0.010-in ligaturewire protruding through the mucosa and attached to thearchwire (Fig 7). After a week, a light force of 60 to90 g was applied by an elastomeric chain from theligature wire to the maxillary left canine. This not onlycorrected the angulation of the impacted incisor, butalso pulled the crown tip away from the root of thecentral incisor (Figs 8 and 9).
For exposing the impacted second molar, only asmall incision was used. Within a week, a Begg bracketwas bonded. An auxiliary 0.016-in nickel-titanium wiresegment was engaged from the first molar tube to theBegg bracket for vertical eruption. Later, during finalalignment, preadjusted edgewise appliance brackets
were bonded on the impacted teeth (Fig 10). Afterdebonding, lingual retainers made from 0.017-in multi-stranded wire (Coaxial, 3M Unitek, Monrovia, Calif)were placed in the maxillary and mandibular arches.
TREATMENT RESULTS
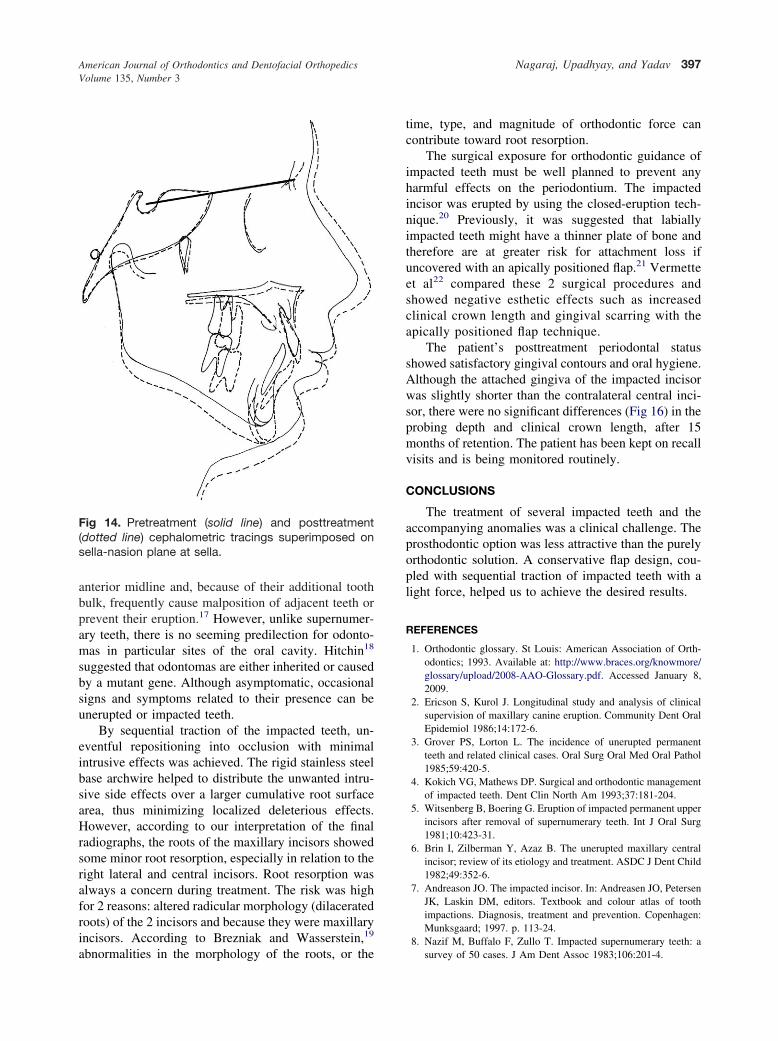
The overall active treatment time was 27 months.There was a dramatic improvement in the patient’s smile.The sequential traction of the 3 impacted teeth providedwell-interdigitated Class I canine and molar relationshipswith ideal overjet and overbite. Canine guidance wasestablished bilaterally during lateral excursive move-ments. The midlines were coincident and in line with theface (Figs 11-14). The interincisal angle decreased be-cause of the maxillary and mandibular incisor proclina-tion. (Table). The posttreatment panoramic radiographshowed that the roots were well angulated and aligned.

Fig 11. Posttreatment facial and intraoral photographs.
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 135, Number 3
Nagaraj, Upadhyay, and Yadav 395
However, minor root resorption was noticed in relation tothe 2 incisors (Fig 13, A-C). Overall, the patient’s skeletalpattern was not altered by the mechanics except for theexpected growth changes (Fig 14).
Records collected after 15 months of retention showthat the results were maintained during this time. Thegingiva is healthy, and the gingival attachments of thepreviously impacted teeth are intact (Figs 15 and 16).
DISCUSSION
Several reports have indicated that impacted teethcan be brought to proper alignment in the dentalarch10-12; however, only a few have dealt with as manydental anomalies as seen in this patient.13,14 The fol-lowing factors are used to determine whether successfulalignment of impacted teeth can take place: (1) position
and direction of the impacted teeth, (2) degree of rootcompletion, (3) degree of dilaceration, and (4) enoughspace for the impacted teeth.
It has been suggested that, in up to 75% ofpatients, impacted teeth erupt spontaneously afterremoval of supernumerary teeth. When spontaneouseruption does not occur, surgical exposure is indicat-ed.15 Power and Short16 showed that, of 22 impactedmaxillary canines that overlapped the lateral incisorsup to half the root width, 16 normalized into anormal eruptive position after removal of the decid-uous canines. In our patient, the impacted maxillarycanine showed spontaneous eruption once the super-numerary tooth was extracted and sufficient spacewas created for its eruption.
Most commonly, supernumerary teeth occur in the
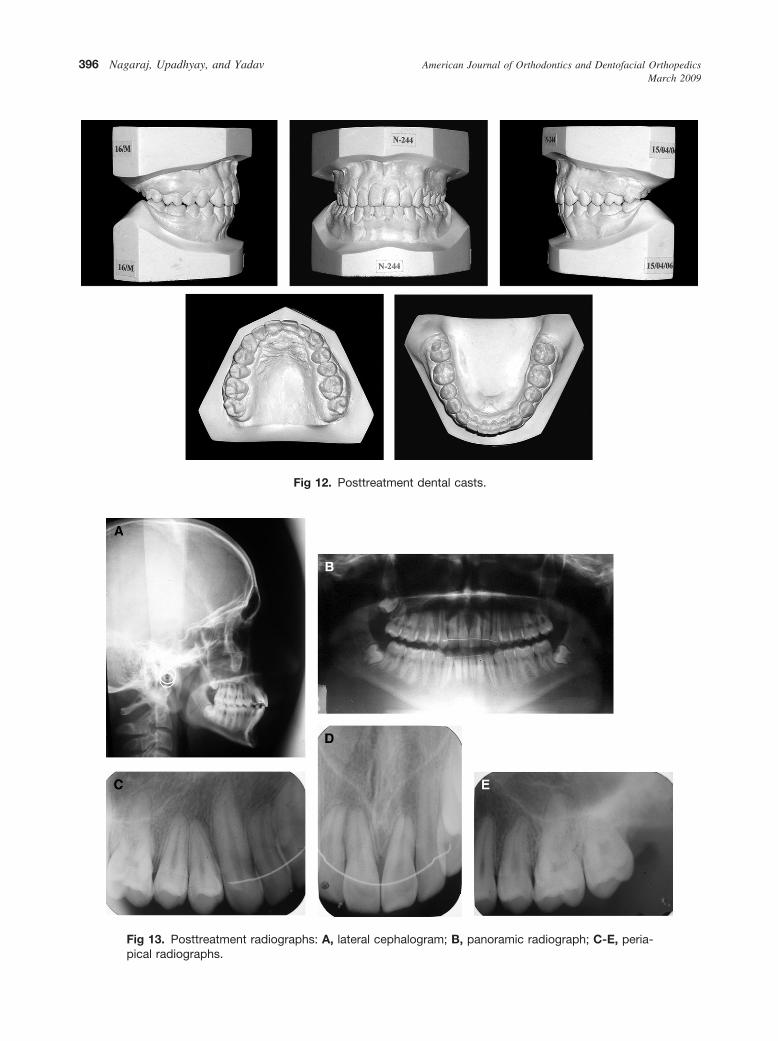
Fig 13. Posttreatment radiographs: A, lateral cephalogram; B, panoramic radiograph; C-E, peria-pical radiographs.
Fig 12. Posttreatment dental casts.
American Journal of Orthodontics and Dentofacial OrthopedicsMarch 2009
396 Nagaraj, Upadhyay, and Yadav
anterior midline and, because of their additional toothbulk, frequently cause malposition of adjacent teeth orprevent their eruption.17 However, unlike supernumer-ary teeth, there is no seeming predilection for odonto-mas in particular sites of the oral cavity. Hitchin18
suggested that odontomas are either inherited or causedby a mutant gene. Although asymptomatic, occasionalsigns and symptoms related to their presence can beunerupted or impacted teeth.
By sequential traction of the impacted teeth, un-eventful repositioning into occlusion with minimalintrusive effects was achieved. The rigid stainless steelbase archwire helped to distribute the unwanted intru-sive side effects over a larger cumulative root surfacearea, thus minimizing localized deleterious effects.However, according to our interpretation of the finalradiographs, the roots of the maxillary incisors showedsome minor root resorption, especially in relation to theright lateral and central incisors. Root resorption wasalways a concern during treatment. The risk was highfor 2 reasons: altered radicular morphology (dilaceratedroots) of the 2 incisors and because they were maxillaryincisors. According to Brezniak and Wasserstein,19
abnormalities in the morphology of the roots, or the
Fig 14. Pretreatment (solid line) and posttreatment(dotted line) cephalometric tracings superimposed onsella-nasion plane at sella.
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 135, Number 3
time, type, and magnitude of orthodontic force cancontribute toward root resorption.
The surgical exposure for orthodontic guidance ofimpacted teeth must be well planned to prevent anyharmful effects on the periodontium. The impactedincisor was erupted by using the closed-eruption tech-nique.20 Previously, it was suggested that labiallyimpacted teeth might have a thinner plate of bone andtherefore are at greater risk for attachment loss ifuncovered with an apically positioned flap.21 Vermetteet al22 compared these 2 surgical procedures andshowed negative esthetic effects such as increasedclinical crown length and gingival scarring with theapically positioned flap technique.
The patient’s posttreatment periodontal statusshowed satisfactory gingival contours and oral hygiene.Although the attached gingiva of the impacted incisorwas slightly shorter than the contralateral central inci-sor, there were no significant differences (Fig 16) in theprobing depth and clinical crown length, after 15months of retention. The patient has been kept on recallvisits and is being monitored routinely.
CONCLUSIONS
The treatment of several impacted teeth and theaccompanying anomalies was a clinical challenge. Theprosthodontic option was less attractive than the purelyorthodontic solution. A conservative flap design, cou-pled with sequential traction of impacted teeth with alight force, helped us to achieve the desired results.
REFERENCES
1. Orthodontic glossary. St Louis: American Association of Orth-odontics; 1993. Available at: http://www.braces.org/knowmore/glossary/upload/2008-AAO-Glossary.pdf. Accessed January 8,2009.
2. Ericson S, Kurol J. Longitudinal study and analysis of clinicalsupervision of maxillary canine eruption. Community Dent OralEpidemiol 1986;14:172-6.
3. Grover PS, Lorton L. The incidence of unerupted permanentteeth and related clinical cases. Oral Surg Oral Med Oral Pathol1985;59:420-5.
4. Kokich VG, Mathews DP. Surgical and orthodontic managementof impacted teeth. Dent Clin North Am 1993;37:181-204.
5. Witsenberg B, Boering G. Eruption of impacted permanent upperincisors after removal of supernumerary teeth. Int J Oral Surg1981;10:423-31.
6. Brin I, Zilberman Y, Azaz B. The unerupted maxillary centralincisor; review of its etiology and treatment. ASDC J Dent Child1982;49:352-6.
7. Andreason JO. The impacted incisor. In: Andreasen JO, PetersenJK, Laskin DM, editors. Textbook and colour atlas of toothimpactions. Diagnosis, treatment and prevention. Copenhagen:Munksgaard; 1997. p. 113-24.
8. Nazif M, Buffalo F, Zullo T. Impacted supernumerary teeth: asurvey of 50 cases. J Am Dent Assoc 1983;106:201-4.
Nagaraj, Upadhyay, and Yadav 397

9. Kramer RM, Williams AC. The incidence of impacted teeth. OralSurg 1970;29:237-41.
10. Lin YTJ. Treatment of an impacted dilacerated maxillary centralincisor. Am J Orthod Dentofacial Orthop 1999;115:406-9.
11. Wasserstein A, Tzur B, Brezniak N. Incomplete canine transpo-sition and maxillary central incisor impaction: a case report.Am J Orthod Dentofacial Orthop 1997;111:635-9.
12. Tanaka E, Watanabe M, Nagaoka K, Yamaguchi K, Tanne K.Orthodontic traction of an impacted maxillary central incisor.J Clin Orthod 2001;35:375-8.
13. Sato K, Mitani HM. Unerupted maxillary central and lateralincisors and canine with crossbite and asymmetry. Am J OrthodDentofacial Orthop 2003;123:87-92.
14. Adamczyk HL, Karmanska B. Similar locations of impacted andsupernumerary teeth in monozygotic twins: a report of 2 cases.Am J Orthod Dentofacial Orthop 2001;119:67-70.
15. Biggerstaff R. Cusp size, sexual dimorphism and heritabi-lity of cusp size in twins. Am J Phys Anthropol 1975;42:127-39.
16. Power S, Short M. An investigation into the response of
398 Nagaraj, Upadhyay, and Yadav
palatally displaced canines and an assessment of factorscontributing to favourable eruption. Br J Orthod 1993;20:215-23.
17. Shafer WG, Hine MK, Levy BM. A textbook of oral pathology.Philadelphia: W. B. Saunders; 1993.
18. Hitchin AD. The aetiology of the calcified composite odontomes.Br Dent J 1971;130:475-82.
19. Brezniak N, Wasserstein A. Root resorption after orthodontictreatment: part 2, literature review. Am J Orthod DentofacialOrthop 1993;103:138-46.
20. Becker A, Brin I, Ben-Bassat Y, Zilberman Y, Chaushu S.Closed-eruption surgical technique for impacted maxillary inci-sors: a postorthodontic periodontal evaluation. Am J OrthodDentofacial Orthop 2002;122:9-14.
21. Årtun J, Osterberg SK, Joondeph DR. Long-term periodontalstatus of labially erupted canines following orthodontic treat-ment. J Clin Periodontol 1986;13:856-61.
22. Vermette ME, Kokich VG, Kennedy DB. Uncovering labiallyimpacted teeth: apically positioned flap and closed-eruptiontechniques. Angle Orthod 1995;65:23-32.
American Journal of Orthodontics and Dentofacial OrthopedicsMarch 2009
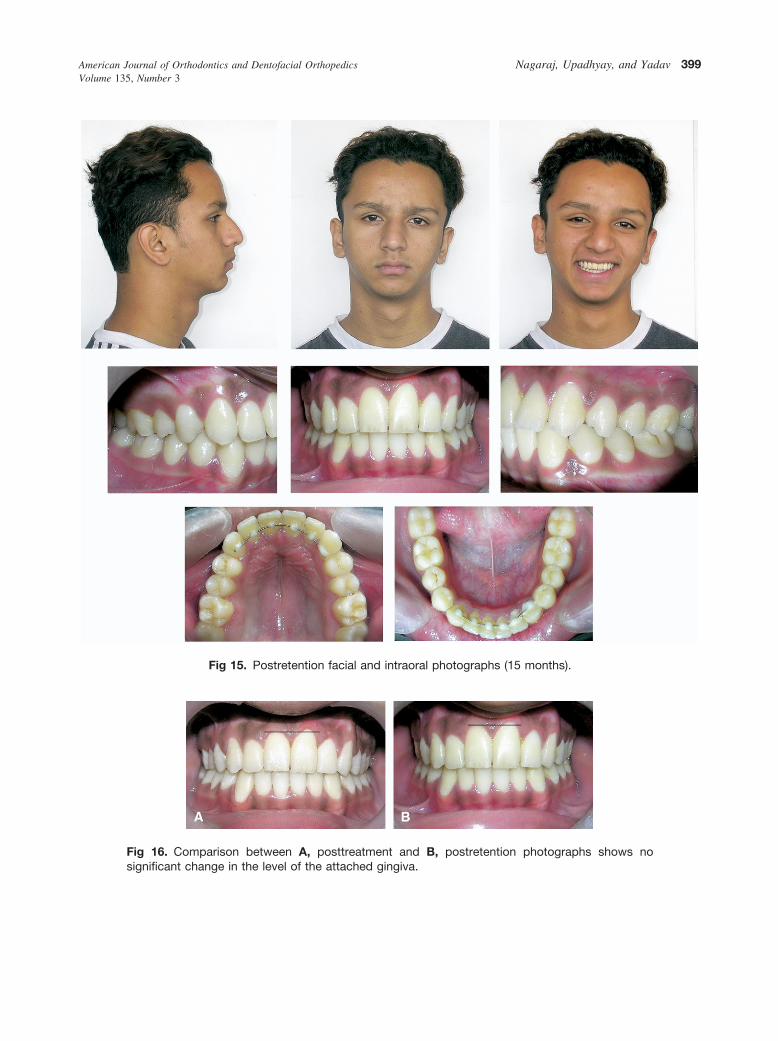
Fig 15. Postretention facial and intraoral photographs (15 months).
Fig 16. Comparison between A, posttreatment and B, postretention photographs shows nosignificant change in the level of the attached gingiva.
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 135, Number 3
Nagaraj, Upadhyay, and Yadav 399




















