Orthodontic Extraction: Riskless Extraction of Impacted Lower Third Molars Close to the Mandibular...
7
TECHNICAL NOTES J Oral Maxillofac Surg 65:2580-2586, 2007 Orthodontic Extraction: Riskless Extraction of Impacted Lower Third Molars Close to the Mandibular Canal Giulio Alessandri Bonetti, MD, DDS,* Michele Bendandi, MD, DDS,† Luigi Laino,‡ Vittorio Checchi, DDS,§ and Luigi Checchi, MD, DDS Extraction of a lower third molar is among the most common oral surgical procedures. It can entail vari- ous complications; among these, the neurologic ones (paresthesias) are the most feared, because they are more likely to lead to legal disputes between surgeons and patients. Nerve damage resulting from the surgi- cal procedure may be caused by either direct trauma of the lower alveolar nerve (more rarely of the lingual nerve) or indirect trauma due to nerve compression after edema or postextraction hematoma. This results in temporary or permanent paresthesias. 1-4 The onset of such complications is affected by various factors, including the following: ● Patient age. The older the patient, generally the greater the postextractive complications. 5 ● Medical history. A positive medical history is as- sociated with an increased risk of complications. ● Level of tooth impaction. The risk of neurologic damage increases as the impaction becomes deeper. 1 ● Tooth inclination. Neurologic complications are more frequent in vertical impactions. 1,6 ● Root morphology. Roots with hooked apices are dangerous; most dangerous of all are roots fused together. 1 ● Competency of the clinician. 1,7 First and foremost, however, it is the proximity of the roots and the mandibular canal that affects the incidence of neurologic complications. 1,2,6 For this reason, appropriate radiographic examinations are important to allow precise topographic diagnosis of the third molar before surgery, to ensure the ability to accurately assess the surgical risks and determine the most convenient surgical approach. The panoramic radiograph is one of the first tech- niques able to provide useful information in this re- gard. A recent survey demonstrated the reliability of 5 radiographic markers (superimposition of the tooth on the canal, increased radiolucency, interruption of the radiopaque border of the canal, diversion of the canal, and narrowing of the canal) visible in pan- oramic radiographs for detecting contact between the third molar and the mandibular canal. 8 The authors tested the predictive value of the radiographic mark- ers in detecting close proximity of the root and canal by comparing panoramic radiographs with computed tomography (CT) scans; these values were 38.5% for superimposition of the tooth on the canal, 71.4% for interruption of the radiopaque border of the canal, 73% for increased radiolucency, 78.6% for narrowing of the canal, 100% for diversion of the canal, and 100% for the concomitant presence of 2 or more markers. These findings demonstrate that superimpo- sition of the tooth on the canal is the marker with the least accuracy; the presence of diversion of the canal or 2 or more markers are indicative of a contact between root and canal. If a panoramic radiograph and/or periapical x-ray reveals a suspected close proximity between the tooth and the mandibular canal, then dental CT scans *Researcher, Department of Periodontology and Orthodontics, School of Dentistry, University of Bologna, Bologna, Italy. †Clinical Research Fellow, Department of Periodontology and Orthodontics, School of Dentistry, University of Bologna, Bologna, Italy. ‡Student, Department of Oral Surgery, School of Dentistry, Uni- versity of Naples, Naples, Italy. §Resident, Department of Periodontology and Orthodontics, School of Dentistry, University of Bologna, Bologna, Italy. Professor and Chairman, Department of Periodontology and Orthodontics, School of Dentistry, University of Bologna, Bologna, Italy. Address correspondence and reprint requests to Dr Alessandri Bonetti: Dipartimento di Scienze Odontostomatologiche, Via S.Vi- tale 59, 40125 Bologna Italy; e-mail: [email protected] © 2007 American Association of Oral and Maxillofacial Surgeons 0278-2391/07/6512-0029$32.00/0 doi:10.1016/j.joms.2007.06.686 2580
Transcript of Orthodontic Extraction: Riskless Extraction of Impacted Lower Third Molars Close to the Mandibular...
J6
Eco(maconai
v
S
O
I
v
S
O
I
B
t
©
0
d
TECHNICAL NOTES
Oral Maxillofac Surg5:2580-2586, 2007
Orthodontic Extraction: RisklessExtraction of Impacted Lower Third
Molars Close to the Mandibular CanalGiulio Alessandri Bonetti, MD, DDS,*
Michele Bendandi, MD, DDS,† Luigi Laino,‡
Vittorio Checchi, DDS,§ and Luigi Checchi, MD, DDS�
tiritam
ngrotcottebtsi7o1mslob
r
xtraction of a lower third molar is among the mostommon oral surgical procedures. It can entail vari-us complications; among these, the neurologic onesparesthesias) are the most feared, because they areore likely to lead to legal disputes between surgeons
nd patients. Nerve damage resulting from the surgi-al procedure may be caused by either direct traumaf the lower alveolar nerve (more rarely of the lingualerve) or indirect trauma due to nerve compressionfter edema or postextraction hematoma. This resultsn temporary or permanent paresthesias.1-4
The onset of such complications is affected byarious factors, including the following:
● Patient age. The older the patient, generally thegreater the postextractive complications.5
● Medical history. A positive medical history is as-sociated with an increased risk of complications.
● Level of tooth impaction. The risk of neurologicdamage increases as the impaction becomesdeeper.1
*Researcher, Department of Periodontology and Orthodontics,
chool of Dentistry, University of Bologna, Bologna, Italy.
†Clinical Research Fellow, Department of Periodontology and
rthodontics, School of Dentistry, University of Bologna, Bologna,
taly.
‡Student, Department of Oral Surgery, School of Dentistry, Uni-
ersity of Naples, Naples, Italy.
§Resident, Department of Periodontology and Orthodontics,
chool of Dentistry, University of Bologna, Bologna, Italy.
�Professor and Chairman, Department of Periodontology and
rthodontics, School of Dentistry, University of Bologna, Bologna,
taly.
Address correspondence and reprint requests to Dr Alessandri
onetti: Dipartimento di Scienze Odontostomatologiche, Via S.Vi-
ale 59, 40125 Bologna Italy; e-mail: [email protected]
2007 American Association of Oral and Maxillofacial Surgeons
278-2391/07/6512-0029$32.00/0
toi:10.1016/j.joms.2007.06.686
2580
● Tooth inclination. Neurologic complications aremore frequent in vertical impactions.1,6
● Root morphology. Roots with hooked apices aredangerous; most dangerous of all are roots fusedtogether.1
● Competency of the clinician.1,7
First and foremost, however, it is the proximity ofhe roots and the mandibular canal that affects thencidence of neurologic complications.1,2,6 For thiseason, appropriate radiographic examinations aremportant to allow precise topographic diagnosis ofhe third molar before surgery, to ensure the ability toccurately assess the surgical risks and determine theost convenient surgical approach.The panoramic radiograph is one of the first tech-
iques able to provide useful information in this re-ard. A recent survey demonstrated the reliability of 5adiographic markers (superimposition of the toothn the canal, increased radiolucency, interruption ofhe radiopaque border of the canal, diversion of theanal, and narrowing of the canal) visible in pan-ramic radiographs for detecting contact between thehird molar and the mandibular canal.8 The authorsested the predictive value of the radiographic mark-rs in detecting close proximity of the root and canaly comparing panoramic radiographs with computedomography (CT) scans; these values were 38.5% foruperimposition of the tooth on the canal, 71.4% fornterruption of the radiopaque border of the canal,3% for increased radiolucency, 78.6% for narrowingf the canal, 100% for diversion of the canal, and00% for the concomitant presence of 2 or morearkers. These findings demonstrate that superimpo-
ition of the tooth on the canal is the marker with theeast accuracy; the presence of diversion of the canalr 2 or more markers are indicative of a contactetween root and canal.If a panoramic radiograph and/or periapical x-ray
eveals a suspected close proximity between the
ooth and the mandibular canal, then dental CT scans
alba
po(t
D
pottmt
dqottce
at
fTdabdoc
eoiliftwTelm
ptcsdwtimc
Fm
A
ALESSANDRI BONETTI ET AL 2581
re needed to determine the precise topographic re-ationships among these anatomic structures so as toe able to assess the extractive risk before the oper-tion.
In this article we describe an orthodontic-surgicalrocedure that has proven useful for safe extractionf impacted third molars in the presence of high risksparticularly neurologic complications) due to theooth’s close proximity to the mandibular canal.
escription of the Operation
The orthodontic extraction operation comprises 6hases: 0, assessment of surgical risks; 1, creationf the orthodontic anchorage; 2, surgical exposure ofhe third molar crown; 3, orthodontic extrusion ofhe third molar; 4, clinical and radiographic assess-ent of the extrusion level; and 5, third molar extrac-
ion.
PHASE 0: ASSESSMENT OF SURGICAL RISKS
Once the need for third molar extraction has beenetermined, surgical risks must be assessed. This re-uires an initial topographic diagnosis through a pan-ramic radiograph (Fig 1). If close proximity betweenhe tooth root and the mandibular canal is suspected,hen a CT scan is obtained. If the CT scan confirms thelose proximity of the 2 structures, then the orthodonticxtraction will be started.
PHASE 1: CREATION OF THEORTHODONTIC ANCHORAGE
The anchorage consists of a stainless steel lingualrch welded to the first molar bands and, buccally onhe extrusion side, a stainless steel sectional wire tied
IGURE 1. Phase 0: Assessing surgical risks. A first topographic diagandibular canal is suspected, then a CT scan is performed.
lessandri Bonetti et al. Riskless Impacted Lower Third Molar Extractio
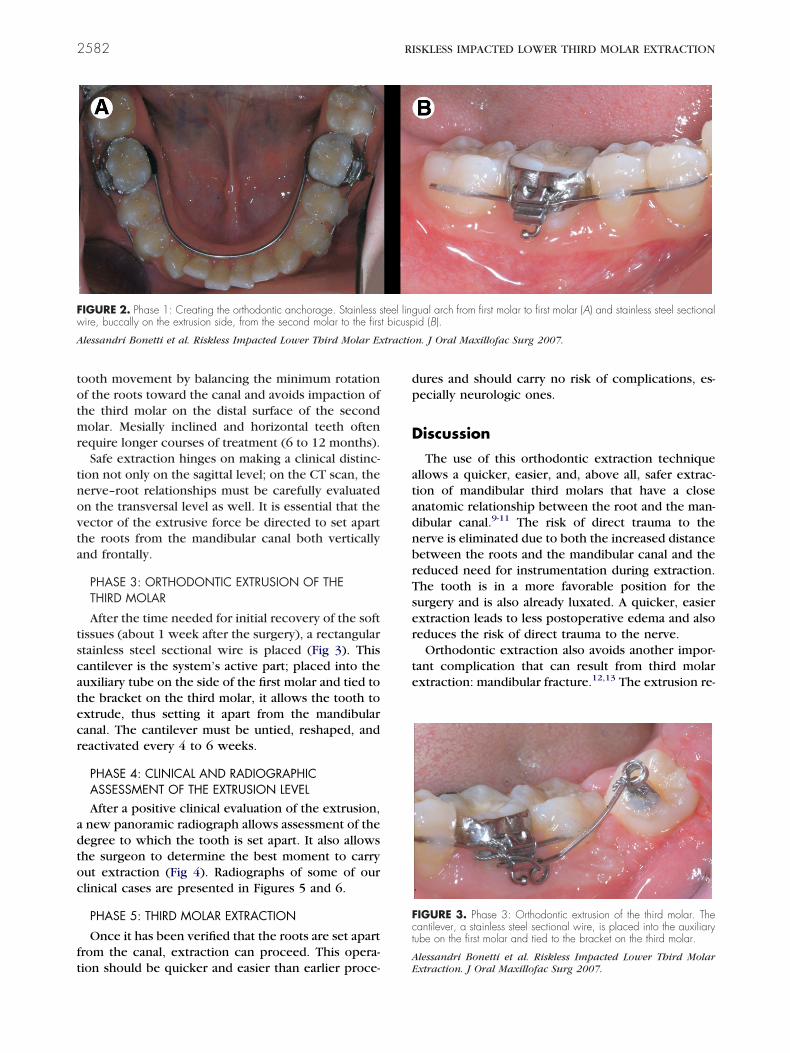
rom the second molar to the first bicuspid (Fig 2).hese patients usually have complete arches; it isifficult to have tooth impaction in incompleterches. The wire can be placed into orthodonticrackets applied to the teeth or (in a patient withental deep bite, to avoid bracket removal) directlyn the buccal surface by drowning the wire in theomposite.
PHASE 2: SURGICAL EXPOSURE OF THE THIRDMOLAR CROWN
In the first part of the procedure, surgical crownxposure of the impacted tooth requires applicationf an orthodontic bracket. There are 2 different clin-
cal types of third molar impaction, depending on theength of the extrusion therapy: vertically or distallynclined and horizontally or mesially inclined. In theormer case, the orthodontic bracket is placed on theooth’s occlusal surface, basically in an axial positionith reference to the molar’s center of resistance.he extrusive strength thus produces a movement ofxtrusion without rotation along the path of physio-ogical tooth eruption, and produces a quick (3 to 6
onths) setting apart from the mandibular canal.The mesially inclined and horizontal wisdom teeth
ose a tougher challenge. The bracket is placed onhe enamel of the distal or vestibular surface of thelinical crown distant from the tooth’s center of re-istance, normally at the furcation level. This makes itifficult to have a solely axial extrusion movementithout rotation. This movement can be negative in
hat it can possibly produce a deeper inlet of the rootsn the mandibular canal; this can be reduced to a
inimum by stripping the occlusal surface of therown during tooth exposure. Such a space facilitates
made using a panoramic radiograph. If contact between the root and
nosis isn. J Oral Maxillofac Surg 2007.
totmr
tnovta
tscatecr
adtoc
ft
dp
D
atadnbrTser
te
Fw
A tractio
Fct
2582 RISKLESS IMPACTED LOWER THIRD MOLAR EXTRACTION
ooth movement by balancing the minimum rotationf the roots toward the canal and avoids impaction ofhe third molar on the distal surface of the secondolar. Mesially inclined and horizontal teeth often
equire longer courses of treatment (6 to 12 months).Safe extraction hinges on making a clinical distinc-
ion not only on the sagittal level; on the CT scan, theerve–root relationships must be carefully evaluatedn the transversal level as well. It is essential that theector of the extrusive force be directed to set aparthe roots from the mandibular canal both verticallynd frontally.
PHASE 3: ORTHODONTIC EXTRUSION OF THETHIRD MOLAR
After the time needed for initial recovery of the softissues (about 1 week after the surgery), a rectangulartainless steel sectional wire is placed (Fig 3). Thisantilever is the system’s active part; placed into theuxiliary tube on the side of the first molar and tied tohe bracket on the third molar, it allows the tooth toxtrude, thus setting it apart from the mandibularanal. The cantilever must be untied, reshaped, andeactivated every 4 to 6 weeks.
PHASE 4: CLINICAL AND RADIOGRAPHICASSESSMENT OF THE EXTRUSION LEVELAfter a positive clinical evaluation of the extrusion,
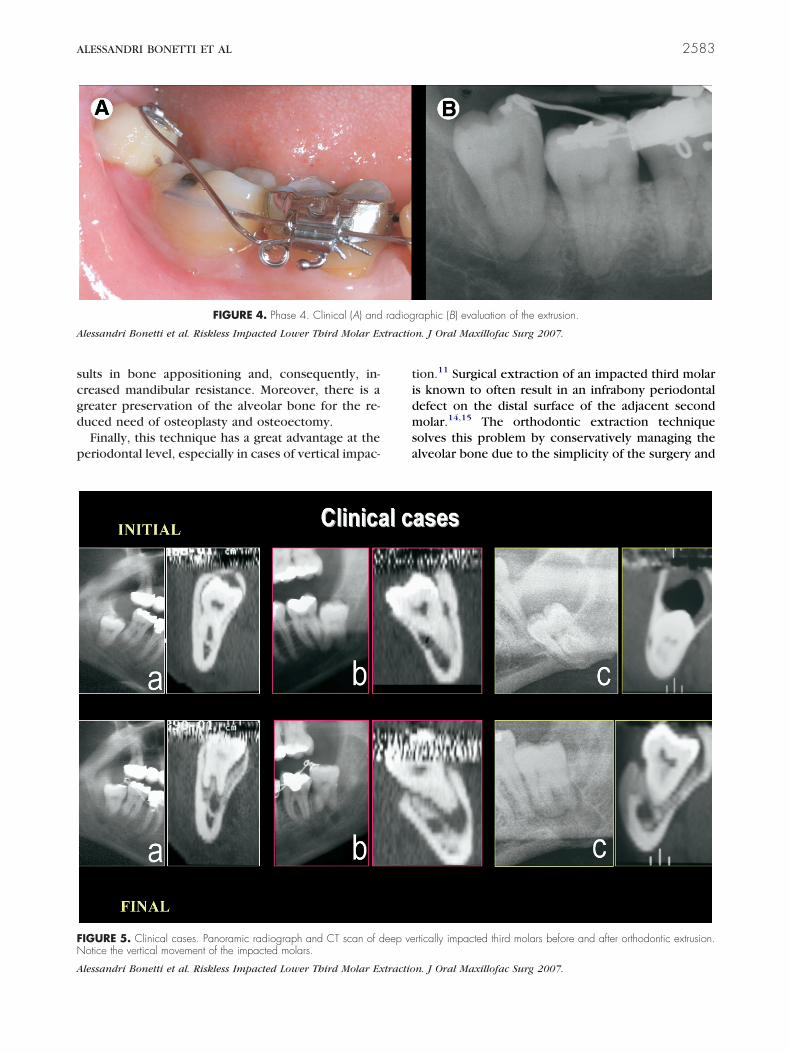
new panoramic radiograph allows assessment of theegree to which the tooth is set apart. It also allowshe surgeon to determine the best moment to carryut extraction (Fig 4). Radiographs of some of ourlinical cases are presented in Figures 5 and 6.
PHASE 5: THIRD MOLAR EXTRACTION
Once it has been verified that the roots are set apartrom the canal, extraction can proceed. This opera-
IGURE 2. Phase 1: Creating the orthodontic anchorage. Stainless sire, buccally on the extrusion side, from the second molar to the firs
lessandri Bonetti et al. Riskless Impacted Lower Third Molar Ex
ion should be quicker and easier than earlier proce-AE
ures and should carry no risk of complications, es-ecially neurologic ones.
iscussion
The use of this orthodontic extraction techniquellows a quicker, easier, and, above all, safer extrac-ion of mandibular third molars that have a closenatomic relationship between the root and the man-ibular canal.9-11 The risk of direct trauma to theerve is eliminated due to both the increased distanceetween the roots and the mandibular canal and theeduced need for instrumentation during extraction.he tooth is in a more favorable position for theurgery and is also already luxated. A quicker, easierxtraction leads to less postoperative edema and alsoeduces the risk of direct trauma to the nerve.
Orthodontic extraction also avoids another impor-ant complication that can result from third molarxtraction: mandibular fracture.12,13 The extrusion re-
ual arch from first molar to first molar (A) and stainless steel sectionalid (B).
n. J Oral Maxillofac Surg 2007.
IGURE 3. Phase 3: Orthodontic extrusion of the third molar. Theantilever, a stainless steel sectional wire, is placed into the auxiliaryube on the first molar and tied to the bracket on the third molar.
teel lingt bicusp
lessandri Bonetti et al. Riskless Impacted Lower Third Molarxtraction. J Oral Maxillofac Surg 2007.
scgd
p
tidmsa
A tractio
FN
A
ALESSANDRI BONETTI ET AL 2583
ults in bone appositioning and, consequently, in-reased mandibular resistance. Moreover, there is areater preservation of the alveolar bone for the re-uced need of osteoplasty and osteoectomy.Finally, this technique has a great advantage at the
eriodontal level, especially in cases of vertical impac-
FIGURE 4. Phase 4. Clinical (A) and
lessandri Bonetti et al. Riskless Impacted Lower Third Molar Ex
IGURE 5. Clinical cases. Panoramic radiograph and CT scan of dotice the vertical movement of the impacted molars.
lessandri Bonetti et al. Riskless Impacted Lower Third Molar Extractio
ion.11 Surgical extraction of an impacted third molars known to often result in an infrabony periodontalefect on the distal surface of the adjacent secondolar.14,15 The orthodontic extraction technique
olves this problem by conservatively managing thelveolar bone due to the simplicity of the surgery and
raphic (B) evaluation of the extrusion.
n. J Oral Maxillofac Surg 2007.
rtically impacted third molars before and after orthodontic extrusion.
radiog
eep ve
n. J Oral Maxillofac Surg 2007.

Fao
A
2584 RISKLESS IMPACTED LOWER THIRD MOLAR EXTRACTION
IGURE 6. Clinical cases. Panoramic radiograph controls before and after orthodontic extrusion. After a positive clinical evaluation of the extrusion,new panoramic radiograph is done to check the distance of the third molar roots from the canal and assist the surgeon to decide when to carry
ut the extraction.
lessandri Bonetti et al. Riskless Impacted Lower Third Molar Extraction. J Oral Maxillofac Surg 2007.

bs
mbhmnfalatw
hdtSsotouimoeeAthsnm
owoast
cbl
cbiacdtbt
nigteiwtbtctptec
laaeilto
R
1
ALESSANDRI BONETTI ET AL 2585
y coronally raising the alveolar bone distal to theecond molar by the extrusive movement.
Another aspect to consider is recovery after third-olar surgery. Extraction of mandibular third molars
elow the occlusal plane increases the risk of delayedealth-related quality-of-life recovery. Moreover, thirdolars in close proximity to the inferior alveolar
erve have a significant negative impact on recoveryor pain and oral function.16 The surgical-orthodonticpproach changes the anatomic aspect; the third mo-ars are extruded to the level of the occlusal plane andre moved away from the mandibular canal. The ex-raction is very fast and very easy, leaving the patientith only slight postoperative discomfort.This technique is not without some drawbacks,
owever. The orthodontic appliance may cause someiscomfort. Soft tissue damage from impingement onhe mucosa of the cheek and the gingiva is common.uch damage is practically unavoidable due to thepecific topographic localization; working in this areaf the mouth is difficult, and the action of the masse-er muscle leads to cheek compression against therthodontic appliances. This damage may be keptnder control by using orthodontic wax; regardless, it
s absolutely reversible once the appliance is re-oved. The procedure also involves 2 (albeit minor)
perations: exposure of the third molar crown andxtraction of the tooth. Finally, the procedure is gen-rally more time-consuming than simple extraction.n effective synergy between surgeon and orthodon-
ist, as well as a good periodontal support team, canelp minimize the efficiency of the operation andave time. Moreover, because it involves a greaterumber of appointments, this procedure may beore expensive than simple extraction.An important aspect to consider when considering
rthodontic extraction concerns the antagonist to theisdom tooth to be extruded. Such a tooth often isvererupted due to lack of occlusal contact with thentagonist, thus preventing extrusive therapy. If thisituation occurs, the upper third molar must be ex-racted before proceeding to the lower arch.
It is important to check for tooth movement beforehoosing orthodontic extraction. This operation wille ineffective if the tooth cannot move due to anky-
osis.Based on the aforementioned considerations, it is
lear that the orthodontic extraction approach cannote used on a routine basis. Each clinical case of tooth
mpaction must be considered separately, and thispproach should be chosen only in carefully selectedases. Such factors as tooth position, integrity of theental arch, overall periodontal situation, type of den-al occlusion, and patient psychological profile muste carefully evaluated, because these can influence
he final result.Modern dentistry often involves an interdiscipli-ary approach. Cooperation among various special-
sts in both the diagnostic and operative phases is ofreat importance in determining the best possiblereatment plan for each patient. The orthodonticxtraction technique for high-risk extraction of anmpacted lower third molar would not be possible
ithout close cooperation between the orthodon-ist and oral surgeon. This technique has proven toe quite simple for the surgeon and only minimallyraumatic for the patient.9,10 It is favorably ac-epted because it is considered a prudent and safeherapeutic choice, a biologically conservative ap-roach, and, above all, a technique that allows extrac-
ion of lower third molars considered impossible toxtract by other approaches, due to the high risk ofomplications.The orthodontic extraction technique that we out-
ine herein has been developed over years of practicend has been steadily improved in terms of predict-bility of clinical results and especially decreased op-ration and recovery time. It makes extraction ofmpacted lower third molar easier and quicker, withess postoperative discomfort, with no risk of pares-hesias or mandibular fracture, and with advantagesn a periodontal level.
eferences1. Kipp DP, Goldstein BH, Weiss WW Jr: Dysesthesia after
mandibular third molar surgery: A retrospective study andanalysis of 1377 surgical procedures. J Am Dent Assoc 100:185, 1980
2. Rud J: Third molar surgery: Relationship of root to mandibularcanal and injuries to inferior dental nerve. Dansk resumè.Tandlaegebladet 87:619, 1983
3. Wofford DT, Miller RI: Prospective study of dysesthesia follow-ing odontectomy of impacted mandibular third molars. J OralMaxillofac Surg 45:15, 1987
4. Chiapasco M, De Cicco L, Marrone G: Side effects and compli-cations associated with third molar surgery. Oral Surg Oral MedOral Pathol 76:412, 1993
5. Bruce RA, Frederickson GC, Small GS: Age of patients andmorbidity associated with mandibular third molar surgery.J Am Dent Assoc 101:240, 1980
6. Bui CH, Seldin EB, Dodson TB: Types, frequencies, and riskfactors for complications after third molar extraction. J OralMaxillofac Surg 61:1379, 2003
7. Brann CR, Brickley MR, Shepard JP: Factors influencing nervedamage during lower third molar surgery. Br Dent J 186:514,1999
8. Monaco G, Montevecchi M, Alessandri Bonetti G, et al: Reli-ability of panoramic radiography in evaluating the topographicrelationship between the mandibular canal and impacted thirdmolars. J Am Dent Assoc 135:312, 2004
9. Checchi L, Alessandri Bonetti G, Pelliccioni GA: Removinghigh-risk impacted mandibular third molars: A surgical-orth-odontic approach. J Am Dent Assoc 127:1214, 1996
0. Marchetti C, Alessandri Bonetti G, Pieri F, Checchi L: Orth-odontic extraction: Conservative treatment of impacted man-dibular third molar associated with a dentigerous cyst. A case
report. Quintessence Int 35L:371, 2004
1
1
1
1
1
1
2586 RISKLESS IMPACTED LOWER THIRD MOLAR EXTRACTION
1. Hirsch A, Shteiman S, Boyan BD, et al: Use of orthodontictreatment as an aid to third molar extraction: A method forprevention of mandibular nerve injury and improved periodon-tal status. J Periodontol 74:887, 2003
2. Libersa P, Roze D, Cachart T, et al: Immediate and late mand-bular fractures after third molar removal. J Oral Maxillofac Surg60:163, 2002
3. Halmos DR, Ellis E, Dodson TB: Mandibular third molars and
angle fractures. J Oral Maxillofac Surg 62:1076, 20044. Kugelberg CF, Ahlstrom U, Ericson S, et al: Periodontal healingafter impacted lower third molar surgery: A retrospectivestudy. Int J Oral Surg 14:29, 1985
5. Kugelberg CF, Ahlstrom U, Ericson S, et al: The influence ofanatomical, pathophysiological and other factors on periodon-tal healing after impacted lower third molar surgery: A multipleregression analysis. J Clin Periodontol 18:37, 1991
6. White RP: Recovery after third-molar surgery. Am J Orthod
Dentofacial Orthop 126:289, 2004



















