Caries progression in primary molars: 24-month results from a ...
25
e S S Caries progression in primary molars: 24-month results from a minimal treatment programme G. G. CRAIG, K. R. PowELL’ AND M. H. CooPER 2 ‘Department of Preventive Dentistry, University of Sydney, Sydney. and 2 Health Commission of .‘Veu South Ilales, Dubbo, Australia Craig, G. C.. Powell. K. R. & Cooper. M. H.: Caries progression in primary molars: 24-month results from a minimal treatment programme. Community Dent. Oral Epidemiol. 1981: 9: 260-265. Abstract — A 2-stage topical treatment regimen (AgF followed by SnFs) was used in an attempt to limit caries progression in the primary molars of children participating in a minimal treatment programme. The children lived in an isolated community in western New South Wales (fluoride in water< 0.2 parts/I 06) and were from a low socioeconomic background. The progression, over a 24-month period, of 281 established lesions in the approximal and occlusal surfaces of primary molars in 54 subjects (mean age 7.0 years) was determined from bitewing radiographs. Of the lesions studied, the majority (69%) were in dentine at baseline. At 24 months, 74% of the approximal surface lesions and 90% of the occlusal surface lesions that were in enamel at baseline remained unchanged. The greatest change occurred in the approximal surface lcsions that were within 1 mm of the pulp at baseline. Only 35% of the lesions required any treatment other than topical metal fluoride therapy during the 24-month period. Key words: dental caries; fluorides; teeth, primary. G. G. Craig, Department of Preventive Dentistry, University of Sydney, 2 Chalmers Street, Sydney, N. S.W. 2010, Australia. Accepted for publication 4 August 1981. Data on the rate of progression of early carious lesions can be of particular value in the establish ment of treatment priorities where dental resources are limited. A number of studies have been carried out to determine the speed of development of early lesions in permanent teeth (1—3, 15). However, little attention has been given to the same problem in the primary dentition. The studies that have been conducted suggest that the rate of progression of lesions in primary molars is reasonably rapid (8, 13). The mean time taken for initial enamel lesions in approximal surfaces of primary mandibular molars to pene trate into dentine was found by VAN ERP & MEYER JANsEN (13) to range from 6.7 to 7.6 months. Subsequently, MURRAY & MAJID (8) observed that 97% of newly initiated enamel lesions in approxi mal surfaces of primary molars had progressed into dentine 1 year later. In 1978 a minimal treatment programme for schoolchildren was commenced in a socially and economically disadvantaged community in western New South Wales. Previous attempts to provide conventional dental treatment for school children from this area had been hampered by three factors: 1) a high incidence of dental disease; 2) a large backlog of unmet treatment needs; and 3) limited patient co-operation during dental pro cedures. The minimal treatment programme was designed to help overcome these problems. In the programme, emphasis was placed on the prevention of new lesions and the inhibition of growth of existing ones. Such an approach was regarded as essential if a systematic and gradual 0301-5661/81/060260-06 S02.50/0 © 1981 Munksgaard. Copenhagen
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Caries progression in primary molars: 24-month results from a ...

e S S
Caries progression in primary molars:24-month results from a minimal treatmentprogramme
G. G. CRAIG, K. R. PowELL’ AND M. H. CooPER2
‘Department of Preventive Dentistry, University of Sydney, Sydney. and2Health Commission of .‘Veu South Ilales, Dubbo, Australia
Craig, G. C.. Powell. K. R. & Cooper. M. H.: Caries progression in primary molars: 24-monthresults from a minimal treatment programme. Community Dent. Oral Epidemiol. 1981: 9:260-265.
Abstract — A 2-stage topical treatment regimen (AgF followed by SnFs) was used in an attempt tolimit caries progression in the primary molars of children participating in a minimal treatmentprogramme. The children lived in an isolated community in western New South Wales (fluoridein water< 0.2 parts/I 06) and were from a low socioeconomic background. The progression, over a24-month period, of 281 established lesions in the approximal and occlusal surfaces of primarymolars in 54 subjects (mean age 7.0 years) was determined from bitewing radiographs. Of thelesions studied, the majority (69%) were in dentine at baseline. At 24 months, 74% of theapproximal surface lesions and 90% of the occlusal surface lesions that were in enamel at baselineremained unchanged. The greatest change occurred in the approximal surface lcsions that werewithin 1 mm of the pulp at baseline. Only 35% of the lesions required any treatment other thantopical metal fluoride therapy during the 24-month period.
Key words: dental caries; fluorides; teeth, primary.
G. G. Craig, Department of Preventive Dentistry, University of Sydney, 2 Chalmers Street,Sydney, N. S.W. 2010, Australia.
Accepted for publication 4 August 1981.
Data on the rate of progression of early cariouslesions can be of particular value in the establishment of treatment priorities where dental resourcesare limited. A number of studies have been carriedout to determine the speed of development of earlylesions in permanent teeth (1—3, 15). However,little attention has been given to the same problemin the primary dentition.
The studies that have been conducted suggestthat the rate of progression of lesions in primarymolars is reasonably rapid (8, 13). The mean timetaken for initial enamel lesions in approximalsurfaces of primary mandibular molars to penetrate into dentine was found by VAN ERP & MEYER
JANsEN (13) to range from 6.7 to 7.6 months.Subsequently, MURRAY & MAJID (8) observed that97% of newly initiated enamel lesions in approxi
mal surfaces of primary molars had progressed intodentine 1 year later.
In 1978 a minimal treatment programme forschoolchildren was commenced in a socially andeconomically disadvantaged community inwestern New South Wales. Previous attempts toprovide conventional dental treatment for schoolchildren from this area had been hampered bythree factors: 1) a high incidence of dental disease;2) a large backlog of unmet treatment needs; and 3)limited patient co-operation during dental procedures. The minimal treatment programme wasdesigned to help overcome these problems.
In the programme, emphasis was placed on theprevention of new lesions and the inhibition ofgrowth of existing ones. Such an approach wasregarded as essential if a systematic and gradual
0301-5661/81/060260-06 S02.50/0 © 1981 Munksgaard. Copenhagen

Caries progression 26 1
reduction in the treatment backlog was to be made
with the dental manpower available. Furthermore,
by reducing reparative procedures to a bare mini
mum it was hoped that the acclimatisation of
children to dental procedures would be facilitated.
A 2-stage topical treatment regimen (AgF fol
lowed by SnF2) was used in an attempt to limit the
growth of existing lesions. This paper reports on the
development, over a 2-year period, of metal fluo
ride treated lesions in the approximal and occiusal
surfaces of primary molars.
MATERIAL AND METHODS
The minimal treatment programme was carried out in Bourke,
a small, isolated community in western New South Wales,
where the water supply contains less than 0.2 parts/lOb F.
Participants were selected from a list of Aboriginal and
Caucasian schoolchildren, from a low socioeconomic back
ground, who were awaiting treatment by the School Dental
Service. Preference was given to young children who had
received little or no previous dental care. Details regarding the
nature and objectives of the programme were given to the
children’s parents. For ethical reasons no placebo group was
included in the stud’. A total of 94 children commenced the
programme and, by 24 months, 71 still remained. Of the 23
children lost to the programme, two withdrew immediately
after the baseline examination and 21 moved away from the
area.
PATIENT EXAMINATION
At the initial visit a clinical examination was made using a
plane mirror and explorer (Ash® No. 49). Posterior bitewing
radiographs were taken using a standardised technique with a
56 kV X-ray machine (Siemens Heliodent®) and fast dental N-
ray films (Kodak Periapical Ultra Speed DF 54®). Primary
molars were photographed from an occiusal aspect at 1.5 N
magnification with a Nikon® camera fitted with a 200 mm
Medical Nikkor® lens (Nippon Kogaku K. K., Tokyo). Awax
impression was taken of the teeth in both arches. Wax was used
in preference to conventional impression materials, such as
alginates, because the impression taking could be done quickly
and required minimal patient co-operation. The height and
weight of each child was recorded.
A treatment plan was then formulated for each patient.
All procedures were carried out in mobile dental vans, each
equipped with a dental unit and light, compressed air and N-
ray unit. One operator (G.G.C.) carried out all examinations
whilst another (K.R.P.) took all radiographs.
CHEMICAL TREATMENTS
Established lesions in primary teeth were selected for treat
ment with metal fluorides if the affected teeth were asympto
matic and there was no radiographic or clinical evidence of the
lesions having reached the pulp. Any open lesion that had a
fir-rn darkened surface characteristic of arrested caries was not
treated.
Teeth with lesions to be treated were isolated with cotton
rolls. Garmers clamps® (Garmer Dental Instrument Co.,
Minneapolis) were used for lower arch isolation. In order to
minimise the treatment time for each patient, rio prophvlaxis
was performed prior to the topical treatments nor was any
attempt made to clean interproximal areas. Apart from the
removal of obvious food debris with an excavator, there was no
pretreatment of open carious lesions. A solution of 40% AgF
(Creighton Pharmaceuticals, Sydney) was applied to the
treatment sites on a small pellet of cotton wool and the sites
were kept wet with the solution for 60 seconds. With open
lesions the pellet was moved gently over the lesion surface with
the point of a probe. For approximal surface lesions that were
not directly accessible, the solution was applied to the
periphery of the contact area. In these instances no particular
measures were used to assist the interproximal penetration of
the solution, the end of the AgF application periods, a thin
layer of 10% SnF2 Spot Application Paste® (Creighton Phar
maceuticals, Sydney), was flowed over the treatment sites and
sealed in place with a small piece of Stomahesive Wafer® (E. R.
Squibb and Sons, New York). When adapting the wafer over
an open lesion, care was taken to seal it on sound enamel at the
periphery and not to exert any pressure on the lesion itself. In
preliminary studies it was found that pressure on an open lesion
could elicit a painful response in the tooth being treated.
Following wafer adaptation. the patients were permitted to
rinse out and than asked not to eat for 1 h. The wafers were
allowed to dissolve in the oral fluids.
The treatments were shared between two operators (G.G.C.
and K.R.P.).
RECALL VISITS
All treated teeth were examined clinically and radiographi
cally at 6-monthly inter’als. Photographic records and impres
sions were also taken as at baseline. At these recall visits, a
restoration was placed if a lesion appeared to be progressing
rapidly or if an open lesion was causing food impaction
between teeth. Pulpal therapy and restorative procedures were
instituted if there was any indication of pulpal involvement in
the teeth under observation. Special attention was given to
lesions that were close to the pulp at baseline. If there was a sign
of caries progression in such instances, a restoration was
placed. No treatment was given to the remaining lesions unless
there was evidence of caries development in which case AgF
and SnF2 were re-applied.
ASSESSMENT OF LESION PROGRESSION
Throughout the minimal treatment programme the status of
treated lesions was determined by clinical examination in
conjunction with radiographic and photographic assessments.
However, for this study, assessments of lesion progression were
made from bitewing radiogaphs only. Lesions initiated on
either occiusal or approximal surfaces of primary molars in
children who completed 24 months of the programme were
studied.All lesions studied were present at baseline and none had
penetrated as far as the pulp. None of the occlusal lesions had
spread laterally onto the adjacent smooth surfaces. A pro
portion of the approximal surface lesions were associated with
marginal ridge breakdown. Such lesions were included in the
study provided it was clear from their morphology that their
site of initiation had been an approximal surface and not anocciusal surface.
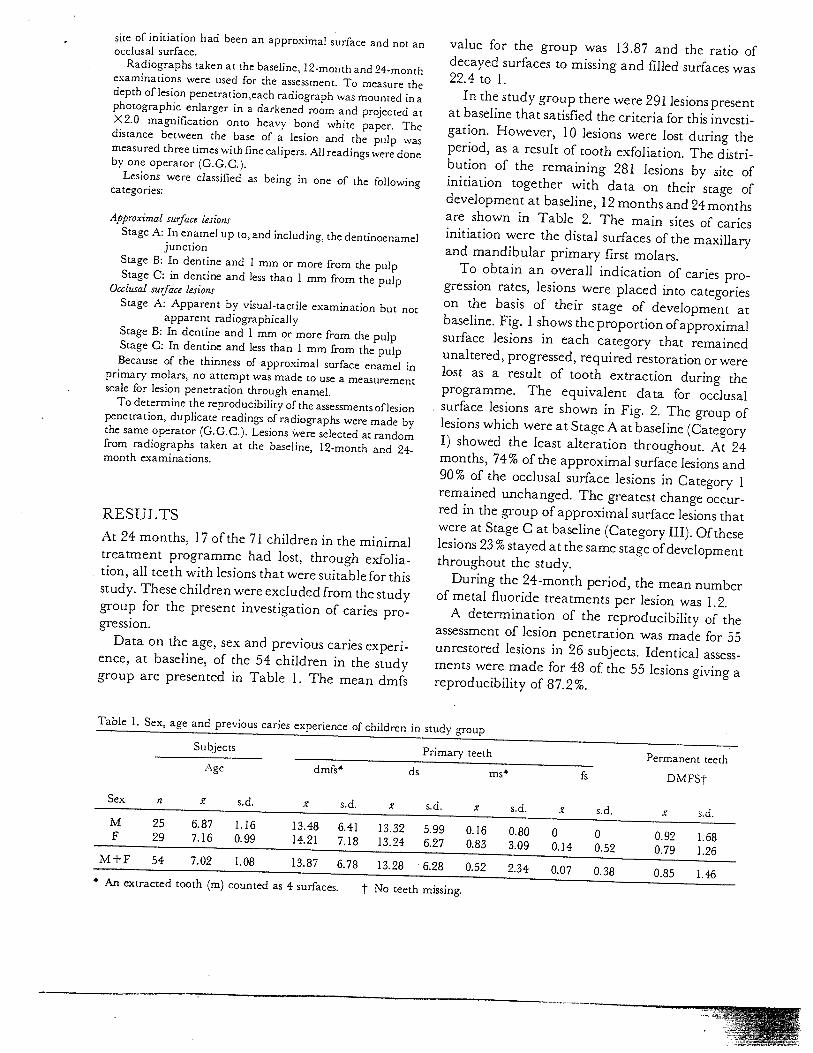
Radiographs taken at the baseline, 12-month and 24-monthexaminations were used for the assessment. To measure thedepth of lesion penetration,each radiograph was mounted in aphotographic enlarger in a darkened room and projected atX2.O magnification Onto heavy bond white paper. Thedistance between the base of a lesion and the pulp wasmeasured three times with fine calipers. All readings were doneby one operator (G.G.C.).
Lesions were classified as being in one of the followingcategories:
Approximal surface lesionsStage A: In enamel up to, and including, the dentinoenamel
junctionStage B: In dentine and 1 mm or more from the pulpStage C: in dentine and less than 1 mm from the pulp
Occiusal surface lesionsStage A: Apparent by visual-tactile examination but not
apparent radiographicallyStage B: In dentine and 1 mm or more from the pulpStage C: In dentine and less than 1 mm from the pulpBecause of the thinness of approximal surface enamel in
primary molars, no attempt was made to use a measurementscale for lesion penetration through enamel.
To determine the reproducibility of the assessments of lesionpenetration, duplicate readings of radiographs were made bythe same operator (CCC.). Lesions ere selected at randomfrom radiographs taken at the baseline, 12-month and 24-month examinations.
RESULTS
At 24 months, 17 of the 71 children in the minimaltreatment programme had lost, through exfoliation, all teeth with lesions that were suitable for thisstudy. These children were excluded from the studygroup for the present investigation of caries progression.
Data on the age, sex and previous caries experience, at baseline, of the 54 children in the studygroup are presented in Table 1. The mean dmfs
value for the group was 13.87 and the ratio ofdecayed surfaces to missing and filled surfaces was22.4 to 1.
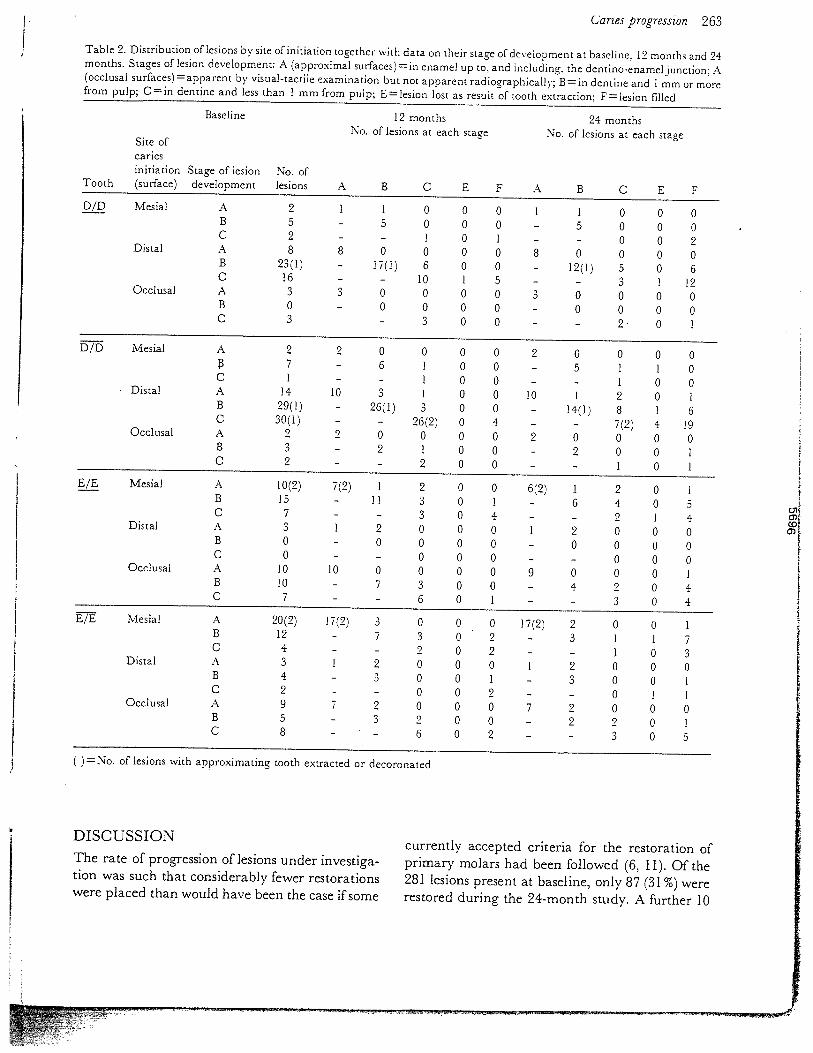
In the study group there were 291 lesions presentat baseline that satisfied the criteria for this investigation. However, 10 lesions were lost during theperiod, as a result of tooth exfoliation. The distribution of the remaining 281 lesions by site ofinitiation together with data on their stage ofdevelopment at baseline, 12 months and 24 monthsare shown in Table 2. The main sites of cariesinitiation were the distal surfaces of the maxillaryand mandibular primary first molars.
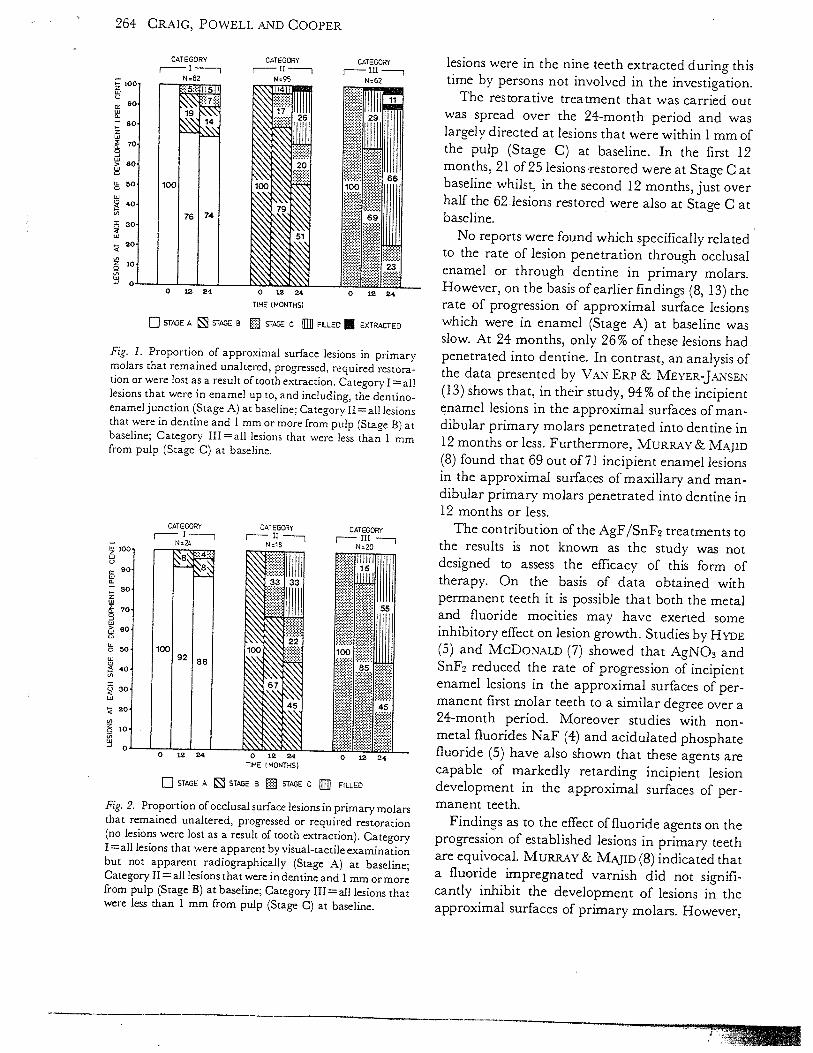
To obtain an overall indication of caries progression rates, lesions were placed into categorieson the basis of their stage of development atbaseline. Fig. I shows the proportion ofapproximalsurface lesions in each category that remainedunaltered, progressed, required restoration or werelost as a result of tooth extraction during theprogramme. The equivalent data for occiusalsurface lesions are shown in Fig. 2. The group oflesions which were at Stage A at baseline (CategoryI) showed the least alteration throughout. At 24months, 74% of the approximal surface lesions and90% of the occiusal surface lesions in Category 1remained unchanged. The greatest change occurred in the group of approximal surface lesions thatwere at Stage C at baseline (Category III). Of theselesions 23% stayed at the same stage of developmentthroughout the study.
During the 24-month period, the mean numberof metal fluoride treatments per lesion was 1.2.
A determination of the reproducibility of theassessment of lesion penetration was made for 55unrestored lesions in 26 subjects. Identical assessments were made for 48 of the 55 lesions giving areproducibility of 87.2%.
Table 1. Sex, age and previous caries experience of children in study group
Subjects Primary teeth Permanent teethAge dmfs* ds ms* fs DMFSt
Sex a z s.d. s.d. 2 s.d. x s.d. x s.d. .z s.d.M 25 6.87 1.16 13.48 6.41 13.32 5.99 0.16 0.80 0 0 0.92 1.68F 29 7.16 0.99 14.21 7.18 13.24 6.27 0.83 3.09 0.14 0.52 0.79 1.26
M+F 54 7.02 1.08 13.87 6.78 13.28 6.28 0.52 2.34 0.07 0.38 0.85 1.46* An extracted tooth (m) counted as 4 surfaces. t No teeth missing.
Caries progression 263
)No. of lesions with approximating tooth extracted or decoronated
DISCUSSION currently accepted criteria for the restoration ofThe rate of progression of lesions under investiga- primary molars had been followed (6, 1 1). Of thetion was such that considerably fewer restorations 281 lesions present at baseline, only 87 (31%) werewere placed than would have been the case if some restored during the 24-month study. A further 10
_
-
0)CD0)
Table 2. Distribution of lesions by site of initiation together with data on their stage of development at baseline. 12 months and 24months. Stages of lesion development: A (approximal surfaces)=in enamel up to. and including, the denuno-enameijunction: A(occiusal surfaces)apparent by visual-tactile examination but not apparent radiographically; Bin dentine and 1 mm ormorefrom pulp; Cin dentine and less than 1 mm from pulp; Elesion lost as result of tooth extraction; Flesion filled
Baseline 12 months 24 monthsNo. of lesions at each stage No. of lesions at each stage
Site ofcariesinitiation Stage of lesion No. of
Tooth (surface) development lesions A B C E F A B C E FD/D Mesial A 2 1 1 0 0 0 1 1 0 0 0
B 5 — 5 0 0 0 — 5 0 0 0C 2 — — 1 0 1 — - 0 0 2
Distal A 8 8 0 0 0 0 8 0 0 0 0B 23(1) — 17(1) 6 0 0 — 12(1) 5 0 6C 16 — — 10 1 5
— 3 1 12Occlusal A 3 3 0 0 0 0 3 0 0 0 0
B 0 — 0 0 0 0 — 0 0 0 0C 3
— 3 0 0 — — 2 0 1
D/D Mesial A 2 2 0 0 0 0 2 0 0 0 07 — 6 1 0 0 — 5 1 1 0
C I — - 1 0 0 — — 1 0 0• Distal A 14 10 3 1 0 0 10 1 2 0 1
B 29(1) — 26(1) 3 0 0 — 14(1) 8 1 6C 30(1) — — 26(2) 0 4 — — 7(2) 4 19
Occiusal A 2 2 0 0 0 0 2 0 0 0 0B 3 — 2 1 0 0 - 2 0 0 1C 2 - — 2 0 0 - — 1 0 1
E/F Mesial A 10(2) 7(2) 1 2 0 0 6(2) 1 2 0 1B 15 — 11 3 0 1 - 6 4 0 5C 7 -
— 3 0 4 — — 2 1 4Distal A 3 1 2 0 0 0 1 2 0 0 0
B 0 - 0 0 0 0 — 0 0 0 0C 0 — — 0 0 0 — - 0 0 0
Occlusal A 10 10 0 0 0 0 9 0 0 0 1B 10
- 7 3 0 0 - 4 2 0 4C 7 - - 6 0 1 — — 3 0 4
Mesial A 20(2) 17(2) 3 0 0 0 17(2) 2 0 0 1B 12 — 7 3 0 2 — 3 1 1 7C 4 -
— 2 0 2 — — 1 0 3Distal A 3 1 2 0 0 0 1 2 0 0 0
B 4— 3 0 0 1 - 3 0 0 1
C 2 - — 0 0 2 — — 0 1 1Occlusal A 9 7 2 0 0 0 7 2 0 0 0
B 5- 3 2 0 0 — 2 2 0 1
C 8 - — 6 0 2 — — 3 0 5
264 CRAIG, POwELL AND COOPER
zLuC,
CiC
Lu
0
>
C0
U,
Lu
Coz0
Lu
CATEGORY CATEGORY CATEGORYI 1-i U Itt-
N62
STAGE A STAGE B
Fig. 1. Proportion of approximal surface lesions in primarymolars that remained unaltered, progressed, required restoration or were lost as a result of tooth extraction. Category I = alllesions that were in enamel up to, and including, the dentinoenameijunction (Stage A) at baseline; Category 11= all lesionsthat were in dentine and 1 mm or more from pulp (Stage B) atbaseline; Category II1=all lesions that were less than 1 mmfrom pulp (Stage C) at baseline.
zLuC,
U,C
z
STAGE A STAGE B . STAGE C FILLEO
Fig. 2. Proportion of occiusal surface lesions in primary molarsthat remained unaltered, progressed or required restoration(no lesions were lost as a result of tooth extraction). Category1a11 lesions that were apparent by visual-tactileexaminationbut not apparent radiographically (Stage A) at baseline;Category II = all lesions that were in dentine and 1 mm or morefrom pulp (Stage B) at baseline; Category III all lesions thatwere less than 1 mm from pulp (Stage C) at baseline.
lesions were in the nine teeth extracted during thistime by persons not involved in the investigation.
The restorative treatment that was carried outwas spread over the 24-month period and waslargely directed at lesions that were within 1 mm ofthe pulp (Stage C) at baseline. In the first 12months, 21 of 25 lesions’restored were at Stage C atbaseline whilst, in the second 12 months, just overhalf the 62lesions restored were also at Stage C atbaseline.
No reports were found which specifically relatedto the rate of lesion penetration through occlusalenamel or through dentine in primary molars.However, on the basis of earlier findings (8, 13) therate of progression of approximal surface lesionswhich were in enamel (Stage A) at baseline wasslow. At 24 months, only 26% of these lesions hadpenetrated into dentine. In contrast, an analysis ofthe data presented by VAN ERP & MEYER-JANsEN(13) shows that, in their study, 94% of the incipientenamel lesions in the approximal surfaces of mandibular primary molars penetrated into dentine in12 months or less. Furthermore. MuRaAY & MAJID(8) found that 69 out of 71 incipient enamel lesionsin the approximal surfaces of maxillary and mandibular primary molars penetrated into dentine in12 months or less.
The contribution of the AgF/SnF2treatments tothe results is not known as the study was notdesigned to assess the efficacy of this form oftherapy. On the basis of data obtained withpermanent teeth it is possible that both the metaland fluoride moeities may have exerted someinhibitory effect on lesion growth. Studies by H’t’DE(5) and MCDONALD (7) showed that AgNO3 andSnF2 reduced the rate of progression of incipientenamel lesions in the approximal surfaces of permanent first molar teeth to a similar degree over a24-month period. Moreover studies with nonmetal fluorides NaF (4) and acidulated phosphatefluoride (5) have also shown that these agents arecapable of markedly retarding incipient lesiondevelopment in the approximal surfaces of permanent teeth.
Findings as to the effect of fluoride agents on theprogression of established lesions in primary teethare equivocal. Muiu & MAjrn (8) indicated thata fluoride impregnated varnish did not significantly inhibit the development of lesions in theapproximal surfaces of primary molars. However,
o 12 24 0 12 24 0 12 24
TtME MONTHS)
STAGE C FILLED EXTRACTED
CATEGORY CATEGORY CATEGORYI I I I INo24 N18 N2O
0 12 24 o 12 24TIME I MONTHS)
0 12 24

Caries progression 265
—
REFERENCES
1. Bcxs.-Dijus, 0.: Longitudinal dental caries study inchildren 9—15 years of age. Arch. Oral Biol. 1961: 6: Spec.Suppl. 94-108.
2. BERNLAN, D. S. & SLcx, C. L.: Caries progression andactivity in approximal tooth surfaces. Br. Dent. J. 1973:134: 51—57.
3. H. & H0LLENDER, L.: Dental caries andrestorations. IV. A six-year longitudinal study of the cariesincrement of proximal surfaces. Swed. Dent. .7. 1979: 3.47—55.
4. Hos.LEwna, L. & KocH, G.: Influence of topical application of fluoride on rate of progress of carious lesions inchildren. Odantol. Revy 1969: 20: 37—41.
5. Hyna, E. J.: Caries-inhibiting action of three differenttopically-applied agents on incipient lesions in newlyerupted teeth: Results after 24 months. .7. Can. Dent.Assoc. 1973: 39: 189—193.
6. KE.Ni.aoY, D. .B.: Paediatric operative dentistry. 2nd ed. JohnWright & Sons, Bristol 1979; pp. 59—69.
7. McDo.o, R. E.: Pedodontics. C. V. Mosby. St. Louis1963; p. 181.
8. MuRRAY, J. J. & Mjio, Z. A.: The prevalence andprogression of approximal caries in the deciduous dentidon in British children. Br. Dent. .7. 1978: 145: 161—164.
9. Nisi-no, M.: Studies on the topical application of ammoniacal silver fluoride for the arrestment ofdental caries..7. Osaka Univ. Dent. Soc. 1969: 14: 1—14. Cited from OralRes. Abstr. 1970: 5: 395.
10. OPPERwNN, R. V. &J0HAN5EN,J. R.: The effect offluorideand non-fluoride salts of copper, silver and tin on theacidogenicity of dental plaque in duo. Scand. .7. Dent. Res.1980: 88: 476—480.
11. Sut, J. M. & FINN, S. B.: Operative dentistry for children.In: FINN, S. B. (ed.): clinical pedodontics. 4th ed. W. B.Saunders. Philadelphia 1973; p. 146.
12. THIB0OEAu, E. A., F DELMAN, S. L. & MARQUIS, R. E.:Inhibition and killing of oral bacteria by silver ionsgenerated with low intensity direct current.]. Dent. Res.1978: 57: 922—926.
13. VAN Eap, N. A. K. M. & MEVER-JANsEN, A. C.: A cariesstudy of the temporary molars and its significance for theirregular conservative care. Yeth. Dent.]. 1970: 77: Suppi. 5.51—74.
14. yOST, K. G. & VAN DEMARK, P. J.: Growth inhibition ofStreptococcus mutans and Leuconostoc mesenteroides bysodium fluoride and ionic tin. Appi. Environ. Microbiol.1978: 35: 920—924.
15. Zii, T., FIsHER, D., FIssL, D. & Sa4.RAv, V.: Alongitudinal radiographic study of the rate of spread ofhuman approximal dental caries. Arch. Oral Biol. 1976: 21:523—526.
NIsHINO (9) reported that topical treatments withan ammoniated silver fluoride, Ag(NH3)2F, prevented the lateral spread of established lesions inprimary anterior teeth over a 30-month period.
One factor in the selection of AgF for the currentstudy was that this salt possesses appreciable antimicrobial activity, a propert7 of possible value inthe treatment of active lesions. Low concentrationsof AgF have been shown to be effective ininhibitingthe growth of S. mutans (12) and in reducing themetabolic activity of dental plaque (10). Theintended function of Sn2 ions from SnF2 was to actas a reducing agent for Ag ions. However, it shouldbe pointed out that SnF2 also possesses definiteantimicrobial properties (14).
A useful aspect of topical treatments with AgFfollowed by SnF2 was that this combination turnedthe surface of active lesions black. Preliminarystudies indicated that the presence of a continuousblack mat on a lesion surface appeared to beassociated with caries arrestment. Any lighteningof the lesion was suggestive of caries development.This phenomenon was regarded as being of sufficient value that it was used throughout theprogramme as a guide to the status of the treatedlesions in conjunction with radiographic and photographic assessments.
The findings suggest that, in general, it may bepossible to adopt less stringent guidelines for therestoration of primary molar teeth than somecurrently recommended (6, 11) if topical metalfluoride therapy is part of the treatment programme. Furthermore, there are implications forsituations where there is a large backlog of unmettreatment needs and where dental resources arelimited. In such circumstances distinct benefits canbe obtained by any slowing of the growth of existinglesions in primary teeth. Firstly, many of the teethmay exfoliate before restorative treatment is required. Secondly, priority can be given to therestoration of the larger cavities with little risk ofthe remaining lesions developing too rapidly.

ri7! /) \ibr 6 21%!
— ““ — ‘‘“
- ntroE rRedrd jn
Today, patients and their dental professionals are faced with a confusing array of oralhygiene products making a wide variety of either therapeutic or cosmetic claims.For many patients, mechanical oral hygiene measures alone may be insufficient toachieve the plaque removal necessary for gingival health or the perception of a cleanmouth and fresh breath. Mouthrinses are very commonly used adjunctively to supportmechanical measures and present an area of confusion for both dental professionalsand patients. A new anti-plaque mouthrinse with a novel mechanism of action willsoon be available in the United States. This review presents the rationale for the useof mouthrinses and compares and contrasts therapeutic agents, including this newmouthrinse, for reduction in plaque and gingivitis.
• Tfl
Ihe prevention and control c) gingivitis and periodontitisare challenges or the dental proFessional in the everyday’improvement and maintenance of oral health for their patients. Less than 20% of all gingivitis cases will advanceto periodontitis and the identification of those who willprogress is still impossible to determine, as there is cur
rently’ no method to identify patients who are vulnerableto this progression. Good oral hygiene, through adequateplaque control and management of gingival inflammation,are fundamental to oral health.
(;iigivitis and periodontitis are widespread diseases, andprevention is dependent on the control of supragingivalplaque. The experimental gingivitis studies of Löe and colleagues clearly’ illustrated the action of plaque accumulationin the development ofgingivitis. When accumulated plaquewas removed through normal oral hygiene. gingival inflammation subsided, validating the significance of plaque as theprimar’ etiological factor in gingival inflammation.
‘lbothbrushing with toothpaste is the most frequently employed method for basic oral hygiene in the United States,although very’ few patients are able to attain ideal plaqueremoval through this approach alone. Flossing and inter—proximal brushing are essential factors in decreasing plaquelevels further. While patients who employ these classic oralhygiene measures may’ exhibit less gingivitis and periodonti—tis, areas of pl1que accumulation may’ still remain especiallyin the dento—gingival areas. l’hese unreachable areas requireadditional efforts if gingival inflammation is to be avoided.Mouthrinses are easy’ to use and by’ the simple action of rinsingare distributed widely’ throughout the oral cavity, accessing notonly’ areas inadequatel’ treated by other oral hygiene methodsbut also soft tissue areas with significant bacterial reservoirs.
‘lie adjunctive use of anti-plaque mouthrinses can providesignificant benefits to those patients who are unable to maintain the highest levels of mechanical cleaning. Mouthrinsesare well accepted today and have been used for thousands ofyears, dating back to 2700 B.C. in Chinese mcdicine.

PLAQUE: CHALLENGES TO THE EUMINATIONOF GiNGIVAL iNFLAMMATiON( ;ingi Va! inflammation, and to sonw degree periodontitis. isstill highly prevalent despite Improvements in oral hygiene:’Clinical experiences of dentists and dental hygienists aremirrored by epidemiologic data from the United States andother countries, revealing the presence of gingivitis in a ma—joritv of people. As the largest studs’ in the United States, theIlurd National Health and Nutrition Examination Surveyrevealed that 63% of examined dentate people in the UnitedStates had gingivitIs.’l he prey lence of gingivitis was re
ported to be 50.3% in all people hetween the ages of 30 and90 years, with a mean of I 3.5% of teeth involved. There is
a strong correlation between su pragi ngival plaque levels and
chronic gingivitis.’ Subgingival plaque. derived fiom supra—gingival plaque. is also closely associated with the advanceof chrome periodontal diseases. ‘l’hereh.re, the control of
supragingival pl.iqoe is primary to the prevention of peri
odontal diseases. l’lw degree ofdifficultv in achieving high
levels of pl;tque removal was clearly demonstrated in a studyof adults in which the researchers found that no individualwas entirely plaque—free. Visible plaque on more than 90%of tooth surhices was found in 35.7% of study participants.’
ajo stages n the development of dental plaque
From clinical experience and population—based studies, it
is clear that while many people do use mechanical plaque—control methods, the’ do not use those methods at levels ef—6.ctive enough to maintain adequate oral hygiene. The needfor additional help in controlling bacterial plaque providesjustification for the use of anti—plaque mouthri nses withclinically proven anti—gingivitis effectiveness as adjuncts tomechanical oral hygiene proced u res.
Many bacterial species can adhere to both dental and
mueosal surfaces. Following initial attachment, the bacteria
multiply and form micro—colonies. I.eft undisturbed, these
m cr0-colonies glow and beco me con 11 tien t. hrm i ng a hio
film in which microorganisms are inti nate1 associated witheach other in a matrix of exopolvmers of bacterial and salivaryorigin. “ I)ental plaque exists as a complex biofllm in which
many species of bacteria co—exist in highly organized and
structured communities. ‘Ihis enables an ecosystem wherediflirent commun ties are not only dependent upon eachother, but have signaling pathways of communication. Ihe
protective matrix is difficult to penetrate and, therebare, thesusceptibility of microbes to antimicrobial agents is muchreduced in biofllms.’ ‘Ihe effect of antimicrobial agents inestablished biofilms is limited to the superficial layers. It hasbeen shown that bacterial microcosms are able to recover
rapidly after exposure to chlorhexidine. lhe bacteria inbiofilms undergo phenotvpic changes that may render thebacteria more resistant. Figure 1 illustrates the biofllm hrma—tim) on a tooth surface. An aggressive btofilm will progress
from the supragi ngival to the subgi ngival region. ultimately
MATURATION AND DETACHMENT
- , . -. ., . —- -. -. . - - -
,, Pellicle Layer
Enamel 1 ,i 1
ATTACHMENT AND COLONIZATION GROWTH AND PROLIFERATION

leading to gi flvi tis Or periodon ti tis.
Reservoirs of pathogenic bacteria eXiSt within the oral
ill ucosa. especial lv the sti riace of the tongue ‘tnd aroti nd
the tonsils. Continual streams of bacteria may he seeded
from these reservoirs and either transferred 1w direct ph’sicaIcontact to the tooth surface or via saliva. Classic mechanical oral hygiene is directed toward the dental and gingivalareas, which constitute only about 20% of the availablesurfaces of the oral cavity’. Even if this 20% were cleaned
i m maculatclv, the remaining 80% forms an ecosystem
maintaining a ready’ source of necessary organisms for the
rapid recolonization of the recently’ cleaned hard surfaces.
l’he challenge of achieving a clean denw—gingival complex
is almost impossible without addressing the ecosystem ofrecolonization. Supplementing mechanical plaque controlmethods with efictive anti—plaque mouthrinses is a way ofcountering this bacierial advance by reaching mucosal sites
unaffected by’ mechanical plaque control methods. Studies
have hosvn the efEctivencss of employing an antimicrobial
mouthrinse that significantly reduces both saltvarvi andmucosal ‘ levels of’ bacteria. Adding an anti—plaque mouth—
rinse to daily oral hygiene regimens will help to reduce the
total oral bacterial burden.
( occurs when supragingival plaque reaches quan
titative and qualitative levels of bacterial complexity thatcompromise giilgival health. Although the microbiology’
of gingivitis is not vet full understood, the sequencing of
plaque farmation indicates how interventions may’ prevent
the development of gingivitis. Opportunities exist at any of’these critical stages: bacterial attachment, bacterial succession
and proliferation, and maturation to disrupt and inhibit the
plaque mass. Although mechanical oral hygiene addresses
all of’ these stages. the use of chemical agents enables more(il’9cc1 ‘c targeting.
‘lidas’, patients are acutely’ aware and place a great deal ofimpoi’tance on oral health, Ihe perception of clean teeth andfresh breath provides an individual with positive fedback
regarding the health of’ the oral cavity, It is also important
For social a of emotional reasons and, therefti ‘c. general well
being. In many’ cases ft’equent oral h’gicnc is implemented itsone clement of daily grooming. rather than ‘or the preven
tion or avoidance of’ disease.
l)espitc this knowledge. many individu,t’. ::av not realize
that even when brushing far 2 minutes, only about half of
the plaque is removed from their teeth,’’l’his apparentl’occurs because certain tooth surfaces receive little or no attention during brushing. ‘‘ In considering this further, fewindividuals brush for more than 60 seconds, ‘l’herefare, theadjunctive use of antimicrobials provides a way of overcoming deftciencics in the mechanical tooth—cleaning habitspracticed by many individuals,
[‘or those few people who can achieve very’ high levels
of’ plaque removal, tooth cleaning only’ once every’ 2 day’shas been shown to prevent gingivitis. - Presumably’, the
plaque biofllm never reaches any level of maturation during this time. However, the profcssional recommendationis to brush twice a day’, which is evidenced as a benefit togingival health. ° Poor ot inadequate oral hygiene leads toexcessive plaque build—up and maturation within the oral
cavity’, which may’ subsequentl’ result in gingival inflamina—tion and periodontal ci isease,
While it is possible to maintain a level of oi’al hygiene stif—
ficient to control gingivitis using mechanical methods alone.
the majorit’ of people are unable to achieve this control on aconsistent basis. Mouthrinses provide an additional level of’effective care adjunctive to tooth and interproximal cleaning,
and proph’laxis. In support of this, the rationale for daily’use of’ anti—plaque mouthrinses is two—fold:
a component added ad ju nctivcly’ to mechanical oralhygiene regimens for the control and pi’evention of pert”
odontal diseases,
2. As a method of delivering anti—plaque agents to muco—
sal sites throughout the mouth that harbor pathogenicbacteria capable of’ recolonizing stipragingival and sub—gingival tooth surfaces,
long—term efcts of’ treatment far periodontal disease
patients reveal that success depends on maintaining plaquelevels that are consistent with gingival health,’ Soon afterden t:il prophvlax is, bacteria start to recolonize the tooth stir—face and plaque build—up begins again. Bacteria diffuse frommucosal anti tooth surfaces Ott) saliy’t md colonize otherareas of the mouth. L’nstimttlated saliva contains 5() millionto 1 00 million bacteria per mill il iter,’’ so the oral surfaces
are constantly immersed in a reservoir of microorganisms.’Advances in our knowledge of oral microbial ceolog’ have
enhanced our understanding of’ the role that antimici’obialmotithrinses can pla’ in controlling plaque biohlm antI

related penodontal diseases. Supragingival and subgingival
tooth surfaces are part ola larger ecological system that in
cludes oral mucosal surfaces and saliva. Studies comparing
the bacterial composition of supragingival and subgingival
plaque with that of saliva and various mucosal surfaces have
indicated that the mucosa serves as a source of bacteria. The
ni ucosa is the origin of pathogens that mac readily recolonize
teeth alter a dental prophvlaxis or periodontal therapvH’
Mechanical plaque control methods are limited in their reach
and have little effect upon reservoirs of microbes from the
larger areas of oral m ucosal tissue.
One of the preferred methods of controlling supragin—
gival plaque and preventing gingivitis is through the use
of chemical agents. The active agents should prevent bio—
film formation without a1hcting the microbial balance and
ecosystem within the oral cavity, avoiding an overgrowth
by resistant organisms. Depending upon the goals of the
preventive measures, various strategies mac be considered.
Anti—plaque agents with properties other then bactericidal
or bacteriostatic properties, such as anti—adhesive agents.
mac be primarily used to keep plaque from developing on a
clean tooth surfitce. True antimicrobial agents mac be more
appropriatclv used as a secon darv prevent ion met hod to
restore and achieve oral health. I )cn tal prulCssio nals ni tot
be attentive to patient proficiency in plaque removal, and
reinforce that using a moothrinse is not a substitute fir
mechanical oral hygiene procedures. but complementary
and supportive to patient mechanical efforts.
ENTS N TER.PLTC CCCJEC
Most currently available chemical plaque control and anti—
gingivitis agents have been tornutlatcd in mouthrinsc delivery
• Gram-positive Cocci
• Increasing numbers of
Gram-positive filamentous
and rod-shaped organisms
• Overall flora more mixed
and diverse
Mainly Streptococci
• Production of extracellular
slime layer helping anchor
bacteria to tooth surface
and provides a layer of
protection
• Biofilm begins to thicken
at gingival margin
• Gram-negative vibrios
and spirochetes
H CE
Anti-adhesives
• Selective colonization of
pellicle on tooth surface
by salivary I planktonic
microorganisms
• Cocci still dominant • Increasing numbers of
filamentous organisms

systems. Ihere arc man’ oral hygiene products that func
tion as delivery devices fr plaque control and anti—gingivitis
agents. of all these, toothpaste may be considered the ideal
vehicle, by virtue of widespread use and twice—daily applica
tion. However, its complex formulation of abrasives, thicken
ers. detergents. sweeteners, humectants, flavoring agents, and
other active agents such as sodium fluoride (caries prevention)
and polvphosphates (whitening or tartar control), presents
challenge. lhc issue is to keep the active agent for plaque
control from reacting with the other ingredients and compro
mising the effictiveness of the toothpaste itself Several deter
gents, such as sodium laurvi sulfine, are anionic (negatively
charged), whereas many commonly used antiseptic agents
are cationic (positively charged). 1 hey may compromise each
others activity when combined. As toothpaste is diluted with
saliva, a foam slurry develops and is dispersed within the oral
• Increasing numbers ofvibrios and spirochetes
• More anaerobes
• Some dense packing offilamentous organismsperpendicular to the toothsurface in palisade layers
cavity. A toothbrush and toothpaste may not effectively reach
all areas of the mouth, especially where many’ microorganisms
reside on the soft tissues and the intcrproximal surfices be
tween teeth. In reality, the act of toothbrushing is selectively
restricted to dental hard surfices.
Mouthrinses are the most common vehicle for chemical
plaque—control and anti—gingivitis agents. and are typically
less complex than tcothpastes in their formulation and in—
gredien ts. Most often, the formulations are aqueous solutions
composed of flavoring agents, colors, and prcsc atives as
well as an active agent and, perhaps, a solubilizing agent,
such as denatured ethyl alcohol. Recently, formulations that
previousl\ relied on alcohol for solubilization have undergone
reformulation and are now presented in either low— or no—
alcohol variants. The presence or absence of alcohol does not
necessarily indicate whether a specific rinse formulation has
therapeutic activity (Sr merel’ cosmetic.
vlouthrinses are dispersed easily throughout the oral cay—
i tv using a swish i ng action that reaches not only dental hard
surfices but most soft tissue areas as well. As a result, the ac
tion of mouthrinses extends to areas of microbial deposition,
such as the dorsum of the tongue, that may act as a reservoir
for recolonization of the dental plaque biofilm
Mans’ oral rinses are available in the marketplace today.
Ihe shopper is presented with a wide, perhaps confusing,
choice of products with many differing claims. lhereforc,
it behooves the dental professional to be knowledgeable and
up to date regarding the availability, effectiveness, and differ
ences of various oral rinse products. Patients routinely seek
advice about oral hygiene products—and expect an informed
review—from their dental professional. l’or many patients.
a recommendation for a specific agent will be necessar to
augment their mechanical oral hygiene efforts. Compliance
with any recommendations will be necessary to improve
gi ngival health.
Currently marketed mouthrinses are available either
over-the-cotinter ((YlC) or by prescription only. In OlC
therapeutic rinses, there are currently three classes (if ac
tive agents:
• Gingival inflammationobserved
Anti-septics
amine alcohols
2. a mixture of essential oi Is
.3. quaternarv am mon tins compounds
vlany 01 proc.iu.:s containing these active ingredi
ents have proven tl:vraveutic benefits that reduce levels of
• Older biofilm containsvibrios and spirochetes aswell as some cocci andfilamentous organisms
• Increasing virulence factors
• Some white blood cellsevident
• Appearance of mushroom- Gingivitis evidentshaped micro-coloniesattached to tooth surfaceby narrow base

both plaque and gingivitis. In order to make these thera
peutic claims, the Food and I)rug Administration requires
iandomii.cd controlled clinical trials. In the prescription—
onl category. chlorhexidinc is currently the only manu
factured formulation and is available as a 0.12% oral rinse.
Formulations that do not Fill into either of the therapeutic
categories are cosmetic in nature. “Cosmetic” oral rinses
do not reduce plaque or gingivitis but may claim to act as
mouth or breath fresheners. These cosmetic claims are not
supported by clinical evidence.
(Thlorhexidine digluconate 0.12% is the only formulation of
this group of antiseptics currently available as a mouthrinse in
the United States although different concentrations (0.06%
to 0.2%) are available in other countries. originally, this
prescription—onlY moiithrinse was formulated with alcohol
(approximately 1 1 .6%) but now alcohol—free formulations
arc available. Alcohol has been used in mouthrinses as an
emulsifier or solubilizing agent and as an astringent. However.
it is this astringency that may compromise patient compli
ance due to stinging, burning, or mucosal pain, which have
been demonstrated to be dose—dependent. Ethanol has been
shown to produce surhice softening of dental resins and com—
posue materials leading to increased wear rates. Alcohol—
containing formulations may be undesirable for patients
undergoing treatment Fir alcoholism, pregnant or ntirsing
women, diabetics, or those who choose to avoid alcohol for
cultural or religious needs or considerations. IhereFire, the
recommendation Fir alcohol—free Firmulations may enhance
patient compliance for a wide range of reasons.
Chlorhexidine has been widely used in medicine and stir—
gerv for prcsutgical disinfection since the I 940s and was ilrst
investigated Fir efFictiveoess in the oral cavity in I 970. The
chlorhcxidine molecule is a strong base, with two positive
charges (dicationic) at pH levels above .3.5.’ These two
positive charges make chlorhexidine extremely interactive
with anions and are the basis of its clinical effectiveness as
well as its unwanted effi.’cts.
Chlorhexidioe has a broad range of antimicrobial activity
that includes Gram—positive and Gram—negative bacteria:
some fungi and yeasts. including (‘a;idzt/tr; and some viruse.
including human mniiinodeficiencv virus (H IV). Bacteria.
resistance after long—term use has not been reported. Ih
antibacterial mode oation is thought to occur against rh
cell wall. Bacterial cell walls are characteristically negatively
charged. The positively charged ehlorhexidine molecule is
rapidly attracted to the negatively charged cell surfiice. 1 he
integrity of the cell membrane is altered at lower concert—
trations, leading to increased permeability and leakage of
intracellular, low molecular weight contents. This stage is
considered bacteriostatic and is reversible so the cell _iTi
recover. At higher concentrations, gross bactericidal dam
age will occur. l’his is reflected 1w educed leakage of the
low molecular weight contents and coagulation along with
precipitation of the cytoplasm, which is irreversible and.
therefore, bactericidal.
Chlorhexjdine also binds via adsorption to the different
surfaces in the oral cavity, as well as to the pellicle and saliva.
l’his effict has been postulated to provide several benefits
that may help explain its persistence in the oral cavity (sub—
stantivitv) and its mode of action. As chlorltcxidine binds
to surfitces, a ieservoir is Firmed. (;radual desorption allows
more chlorhexidine to be transported by saliva to the tooth
surfitce and the bacterial cell wall. ‘ In hi id tog directly with
the tooth surfitce, the clilorhexidine molectile occupies sites
that could be used by salivary proteins and bacteria to bind to
the tooth. This action by chlorhexidine may inhibit the early
stages of plaque Firmation. 1)epending on the concentraiion
of chlorhexidine, the bactericidal or bacteriosiatic effects will
compromise bacteria attaching to the tooth stirfitce. In this
mechanism, chlorhexicline may be more effective asa plaque
preventive agent. rather than a plaque removal agent.
‘l’his tooth surface activity may also explain the unwanted
efFct of staining. AclcIy has explained staining in terms of:t
local precipitation reaction between chiomogens Fund in
foods and beverages and the tooth—bound chlorhexidine.
Avoidance of these foods and beverages during treatmetir
with ehlorhexidine, especially soon after its application.
should reduce the degree of stain Firmation. Other tin—
wanted effects reported’’ include taste perturbatioti (to salt).
mucosal erosion (rare at the 0.12% concentration), enhanced
stipragingival calctiltis formation, a tingling sensation of
the tongtte. and anesthesia—like effixts For these reasons,
chlorhexidine rinses are prescribed only for a relativeI’ short
duration to help control acute or severe inflamtiiatorr’ condi—
tiotis, resulting in plaque reduction and improved gingival
health. Chlorhexidine is generallY not indicated Fir long—
:crm maintenance due to staining and calculus Firmation.
Chfarhexidiiie has been extensively studied in clinical tn—
and has been referred to as the gold standard.’ Clinical

Fixed Combinationof Essential Oilst
35, 36,55, 56
36, 39 to43, 55, 57
46
51, 53,54, 56
trials have demoflstrated typical reductions in plaque of21 6% to 60.9% and gingivitis of 18.2% to 42.5%.
Phenol—related essential oils have been used in mouthrins—
es for many years. listerine , a formulation derived Froml,isiers original work with carbolic acid, is a mouthrinse with
a very long history dating back to the 19th century. The rinsecontains two phenol—related essential oils. thymol (0.064%)and eucalvptol (0.092%) mixed with menthol (0.042%) andmethyl salicvlate (0.060%). lThis Fixed combination of essential oils is dispersed in a denatured alcohol vehicle (between21.6% to 26.9%). although reduced alcohol formulationsare now available. All mouthrinses containing alcohol maybe limited to the populations that can tolerate the localside effects; however, 1,isterine has been used by millions ofconsumers since its introduction more than 1 00 years agoand remains one of the most commonly available and used(Y1C therapeutic mouthrinses todaw’
Ihe mechanisms of action of this formulation against bacteria are complex. At high concentrations, there is a disrup—tion of the cell wall and precipitation of cell proteins; essentialenzymes are inhibited at lower concentrations. Ihis formulation of essential oils can penetrate the plaque biofllm andexert bactericidal activity. The bacterial load is reduced witha concomitant decrease in plaque mass and pathogenicitv.
A ii umber of long—term studies have been conducted on
this rinse of a fixed combination of essential oils that haveshown consistent adjunerive benefits. (Slinical trials havedemonstrated plaque reductions of 13.8% to) 56.3%. andgingivitis reductions of 14% to 35.9%. A stud in
volving flossing and brushing with the mouthrinsc showed
an additional I 5.8% reduction in interproximal gingivitis
compared to a reduction of only 7.7% in the flossing andbrushing group not using the mouthrinse.
QUAT7PNA ,-
(Setvlpvridinium chloride (CPC) is a cationic surface—activeagent that has a broad antimicrobial spectrum of activity, involving the rapid destruction of( ;rln)—3Ositive pathogcns andeasts. The mode of action against bacteria is through the disruption of the membrane function, the leakage of cvtoplasniicmaterial, and, ultimately, the collapse of the intracellular equilibrium. (PC is found in many mouthrinses, including thosewith a therapeutic benefit and also those with only cosmeticclaims. Clinical research has shown CPC mouthrinscs tohave anti—plaque activity when used alone or in combinationwith toothbrushing. A recent meta—analvsis from a systematicreview supported the plaque— and gingivitis—inhibiting effect
of CPC—containing mouthrinses. It concluded that CPCrinses, when used as adjuncts to oral hygiene, provide a smallbut significant additional benefit in reducing both plaqueaccumulation and gingival inFlammation.
Chiorhexidine60.9% 42.5% 77%0.12%
56.3% 35.9% 69.8%
Cetylpyridinium15.8% 15.4% 33.3%Chloride 0.07%
Delmopinol35% 18% 57%Hydrochloride 0.2%
Compared witn negative control at 6 months.- Thymol 0.064%, eucalyptol 0.092%, methyl salicylate 0.060%, menthol 0.042%, solubilized in 21.6% to 26.9% denatured alcohol.
Comar;son between agents is inadvisable due to differences in study design and indices reported.

However, not all formulations ofCPC—con tai ni ng mouth—
rinses provide the same degree of clinical benefit due to the
bioavailabilitv of the CPC. The formulation of the vehicle
ingredients, soluhilizers, preservatives, stabilizers, coloring
agents, etc, and the way they are combined together can have asignificant impact on the bioavailabilitv of the CPC. Increasedbioavailability is associated with higher probability of effec
tiveness, greater anti—plaque activity and greater reductions ingingivitis. Decreased bioavailabiliry and lower concentrations
are commonly associated with cosmetic claims alone suchas in—vitro germ killing, fresh breath. etc. The FDA Plaquesubcommittee deemed CPC to be safe and effective for the
treatment of plaque—induced gingivitis within a concentrationrange of 0.045% to 0.10% when present in a high—bioavailablcmatrix.H The substantivity of(2P(. is reported to he between
3 to 5 hours, due at least in part to its cationic nature. Stainingcaused by CPC has a similar dietary etiology to chlorhexidinesolutions but appears to he less severe.
In clinical trials, CPC rinses have shown reductions inplaque and gingivitis. A mouthrinsc Containing 0.07%high bioavailable CPC in an alcohol—free frrnulation (Pro—Health) demonstrated a 15.8% reduction in plaque, 15.4%reduction in gingival inflammation, and 33.3% less gingivalbleeding, relative to a placebo group after 6 months.
First— and second—generation versions of anti—plaque andanti—gingivitis agents have been on the market in the UnitedStates for many years. Their mechanism of action is theinhibition or killing of microbes of the oral flora. The nextgeneration of agents has begun to emerge that has a tin iqueability to inhibit or disrupt the formation of plaque. whilepossessing little if any effect on the bacteria, avoiding disruption to the balance of bacterial flora found in a healthymouth. Delmopinol hydrochloride (a morpholinoerhanolderivative) is an amine alcohol that is relatively new to oralhygiene products, and functions as a surface—active agentwith low antimicrobial potencv: Delmopinol has also beenshown to have the ability to interact with pellicle constituents and inhibit glucan synthesis by .Streptococcus muta;l.
Delmopinol has little or no demonstrable effect on the bacteria, but it interferes with plaque/biofllm matrix formation.It redtices the adherence ofprimarv plaque—forming bacteriain the development of plaque biohlm. Studies have ho.vnthat the nascent hiofilm mass is loosely adherent
there is a significant reduction in the proportion of dextran
producing cocci. The interference with plaque matrix bar—mation leads to the plaque deposit being loosely adherent
and possibly easier to remove.
Delmopinol hydrochloride 0.2% mourhrinse has beenshown to be effective against plaque and gingivitis in bothshort—term no—oral—hygiene studies and long—term home—uscstudies. Arguably, the short—term no—oral—hygiene studiesshowed plaque inhibition closer to that of chlorhexidinethan any other previous agen t.
Although recentl approved in the United States, delmopi—
nol hydrochloride 0.2% mouthrinses have undergone rigor—
otis clinical testing in no fewer than 29 clinical studies. 1 hefirst ever meta—analysis of mouthrinse efficacy data basedupon eight of these dclmopinol studies was published in2007. The conclusion of the meta—analvsis was that thisthird—generation agent was effective as an adunctive mea—sure bar redticing plaque burden and gingivitis, whether ornot used tinder supervision. It was also noted that delmopi—nol 0.2% met the efficacy criteria of the American DentalAssociation for anti—plaque and anti—gingivitis motithrinses.
In clinical trials, clelmopinol rinses have demonstratedplaqu_t reductions of 9.3% to 35%. hleedi rig on prohi ngreductions of I 8% to 3654>. and Si ngivi t is reductions of tipto I 8%. A meta—analvsis of eight double—blind, parallel group studies conducted 1w seven different independentresearch groups supported the effectiveness of delmopisol0.2% mouthrinse as an effective measure for educing plaqueand gingivitis.
MANAGNC T NEEDS OSPatients seldom achieve the expectations of dentists anddental hygienists about plaque removal. Few patients conducting mechanical—only plaque control (toothbrushing andintcrproximal cleaning) are able to achieve adequate andwidespread levels of plaque removal consistent with gingi—val health. Periodontal diseases are plaque—induced and ateinitiated Isv a host—inflammatory response to the maturingplaqtie biofilm. Plaque is the primary etiological FaCtor forgingival inflammation. Considering that plaque—inducedgingivitis always precedes the occurrence and re—ucctirreneeof periodontiris. the prevention of periodontal diseases depends upon the control of supragingival plaque.
Opportunities exist to broaden the armamentarium ofulaque control using various chemical agents. which act:aough various strategies:

interFerence with the initial adhesion oF the oral bacteria2. disruption of the co—aggregation mechanisms
.. suppression of the multiplication or direct killing of microorganisms through bacteriostatic or bactericidal means
Ihese agents may be delivered in various [orms: tooth—
pastes, gels, sprays, or mouthrinses. Mouthrinsing is a well—accepted cosmetic and therapeutic activity that delivers activeingredients throughout the oral cavity, reaching areas typi—calls inaccessible by mechanical oral hygiene methods alone.Mechanical oral hygiene is targeted only toward the toothsurfsces and the dento—gingival margins (approximately 20%of the total oral surbice area), neglecting the mucosal surfitces
in the single ecosystem of the oral cavity.
10d15 in the Lnitcd States, there are bntr categories of
anti—plaque agents available in n outhrinses: chlorhexidinc,dcl nmpi nol. cetvl pvrid tnt it n chloride, and a fixed com bi nation of essential oils.
(Thlorhexidine, often rekrred to as the gold standard, is
available by prescription only. It is highly effective whenused adjunetivelv to in—office and at—home procedures for
gaining control of periodontal diseases. It is also prescribedfollowing in—ofhce soft tissue procedures when mechanical
plaque control alone mae be insufficient For good hygiene.In such cases, the adjunetive use ofehlorhexidine may help
control plaque until regular mechanical cleaning can hereinstituted. Chlorbexidine is ideal to help control plaquefor a relatively short period during active treatment. ‘X/ithprolonged use, the unwanted effects of staining and calculusbuild—up become apparent. lhese, together with its bittertaste and burning sensation from its alcohol content, tendto compromise patient compliance and successful outcomesof’ treatment. Becaitsealcolsol is of no therapeutic “aloe,alcohol—lice brinulations of chlorlsexidine mouthrinse(Sitnstar (;LM ) are now available and should be routinely prescribed.
As gingival health is re—established, what can the patient doto maintain gi ngival health and support their less—than—opt—mal mechanical oral hygiene? In determining recommendations, many bictors should he considered, the most importantbeing patient compliance. It is critical that a patient adopts theadvocated behavior. Approved therapeutic tnouthrinses haveclinically demonstrated benefits, so it is essential to recommend or endorse the product that the patient is most likelyto use. Ihe recommendation is primarily based upon sensory
perceptions and should be balanced with the clinical need.
GlJ\4 PerioShield ‘ Oral Health Rinse (Delmopinol,
0.2%), about to be introditced in the united States as a
surface—active anti—plaque agent, interferes with plaque formation be disrupting the matrix and thus enabling ease removal.l’his approach is relatively new and does not rely upon killing or inhibiting the microbiota. I)elmopinol disrupts thedevelopment and maturation of the established and harmfulbiofilm while maintaining the biological equilibrium withinthe oral cavity. Given its inferred properties of keeping a cleantooth clean, the concept of using delmopinol for long—termdaily maintenance after active treatment with chlorhexidineis attractive and may help prevent relapse in the mane patients whose mechanical cleaning is not conducive to themaintenance of ongoing gtngival health. Delmopi nol hasvery few antimicrobial properties and, as its mechanism ofaction inhibits the development and matliratiots of the plaque
bioftlm. it is distinctly attractive h.r patients concerned aboutantimicrobial resistance, overgrowths of resistant strains, ormaintaining equilibrium of the oral ecosystem.
I’he formulation of a fixed combination of essential oilshas stood the test of time in the consumer marketplace andalso provides antimicrobial benefits. Many variants are nowavailable, with even lower concentrations of alcohol andmilder flavors.
(;ct’lf3’ridiithtIn chloride is available in many formulations. For therapeutic benefit, care most be taken in theselection of the formula to ensure a high degree of hioavail—ability of the active agent and, therefu)re, the ability to inhibitplaque and reduce gingival inflammation. Crest Pro Healthis a relatively new formulation containing bioavailable CPCin an alcohol—free presentation. CPC is a cationicallv chargedmolecule that, in some cases, may be associated with a degreeof stain after prolonged use.
Within the population, few patients will ever achieve the degreeof plaque control necessary for gingival health by mechanicalmeans. This paper has outlined the benefits of adding chemicalagents adjunctivelv to daily oral hygiene regimens to achievegreater reductions of both plaque and gingival inflammation.
Is’cj’ co,ls,sleiyltioiic GuC’S
• Adjunctive use of an of the therapeutic oral rinsesabove can provide significant benefits to the many patients who cannot maintain adequate levels of plaque

and gingivitis control through mechanical means alone.• It is imperative that patients understand that the use
of an anti—plaque/anti—gingivitis agent is not the silverbullet of oral hygiene.
• Ihe key to oral health begins with a well—designedtoothbrush ;iid toothpaste that encourages individualpatient compliance and adherence to the techniquerecommended by the dental professional.
• Adjuncrive agents for plaque and gingivitis control willnearly always be necessary.
• An individual approach to the factors determining apaient’s gingival condition is warranted.
lhcrapeutic mouthrinses, wirh their ability to reach bend inechan ical plaque control, have a very important role
in the reduction of dental plaque and gingivitis.
REFERENCES
1. l3ariic’ii XII thu rationaL fir thu daily usc olan .urrimicrirhial nrourlr—
ririsu. / zlm 14’ni ,(sco. 2006: 1 .37(srrppl I: I (iS—2 I S.
2. I us I I. Iruilads I.. Icnscrr SI). I.xpcrrrrieiiral riigivrrrs ri iran. /I’riodo;iinl. 965.36: —8.
3. MarrdcI ). C :thsrapcirr ic a9cn is ir ciini roll rig plaq nc arid gin—
gi 1 i.s. / (ii;? I3i0(//1O1l//. 1 988: 5(81:488—498
4. hasIniri (‘C.. l(iiriigsiiis 1)51. l41i11cirniolOgv ill periodontal healih arid
djsciss. ri: tang \l( Arrsrronii K. Io II. ds. I’rmssi/inç’s s/tii I:uinpir/n
mi .(Iiiirmnnca/ I’/mgiue (cm/no/. l)crliii: Qrrirircsseiics Pirhlisliinig
Zornpa iv: 998: I 9—34
5. Alharid.ir 51 Kinigrnnaii A. C ,i,ii!rval isCcssiiiii. giiiivaI hIccdnnir. arid
denial cilerilrrs inn adirirs 3)1 is-irs if age arid ,,Ider rn the l;iiuied Siaiss.
(988—1994. / Pevine/o,,/o/. (999:7(1(1 (:30—/iS.
6. Ash 51. C nun (5.. Sinniih \.\ C .orrelailoii hrveein ila9iisaiid giiigiviii.s.
/ I’,nio,Ioniol. 96n;.3S:4 25—4 29.
7.\1iSirld \‘C1irks(niip in rcpiiri un pneveniinuiin. /11/1/
/3;wi/uniium/. I096a:250-255.
8. F larierick Ill. Prevention. \\orld \Vorksliop inn l’eriodonnics. ,Inn
I’urnj,/o;iio/. (9961 F ):22.3—249.
9. C lirnsierssriir (A. (,r,rssi SO, Dirn6urd RO. ci al. Denial p1atie arid sa(cnr—
Firs: risk irrdininurrs dr ilrcir %rrnianiinri./1)ini lAs. F 992:710): (425—1.1.3(1.
10. I nsrgnrnen MA. (inrnnraiion of dental plaque arid oilier nra1 hinrOr:ns.
In: \esvinlatn F F N.. \\ilsoin 51. eds. /)rnrnn/ l’/ui//rin Rr’i’jirr,L ()ni I6syJu
in I/ca/i/i ,iic/ 1)/ill/ic. ( ardif% hiolinic: (999: (87—2(1).
I 1. F arsu’rn I. I slur N. I. Resrsranics nif Sircprocinuxnrs sanigrils Isirr .:::
.rririnrieriuhinl ngctrts .;(PSIJS. 1996:104(43:280—284.
12. I elvis K. Ricidic C Iriuntllnni resisranrce. /l,,/0110ro/) An;.: ( ,
21)1)1:450 ::99. :
13. DePaola lCd Nlinrah (1/. ()verholser (1). urn. lIlder if an rnrusepn
riioirihririsc nun salivary iriicrniliioia. zliii/ l)rui. I 9969)3)93.95
14. inc DII. I:inrgang I). Sinaira K. err( In vivnr ninininnicrohial eflecirve
ness of,nni esscriiia( inil—corniaininrg riiiirrnlr rinse (2 In alum a single ins arid
I u dau rise / (Jill I3’ii!mIIOl//OI. 2005:32(i) :335-3 4)).
15. De a dna SIR. /ae,iri.is (1. rlrrisrirri DA. Ikaulike -\\\. Plnqrie grirslilr
rind reiirirv;rl iviiln duly rnnrrrlihrrislninig. I I5;imumlmnnmu/ I 939:501(21:661
16. .\(ae( rcginr II). lkirgg—( ruin AJ. -S srrivsv oliiririlrhrnrslrinng seqrrcince Ill
elnildrein arid vrnirrig adirlus. I /SsAa/o;ren/ I/is. I 939:14(3)225—23)).
17. \(e\ahlr II. \lninnlrslli A. lang N.1’. Snrprrginigirl cleaning .3 lines
a week. lIre riricrirliiirlogie;nI elders 01 iuoclciaielv cice)i pluCkers I (I/n
I’i’io,Ioiitüh (99 I9(5) 348— 356
18. Fraiidseni .5. \(eeharnieal nina) hygiene practices In: I.iie I I. Kleinnnnnanr
I )V. eds. l)inia/ I’/uajun (niH/IS! .1 /in/li! 17 mliii! (hiil I/v nan /‘nininrS. I ‘ ed.
C)sfinrd: FRI. (‘russ: I 9869 3_ 116.
19. ,.ii.celssinnn P I.iiidlie I. thu signnihicaricc iii nr.ninnrennrnnue c,ire ni ilie
ircaniiieinr of (rerionIninrinl drscase./ (I;, /Ssnna/o;//nnl, 1981 :$(4):28 (—294
20. liiirev ‘13. C hiliiiri N\k. Pihlsirorni (SI. ci al. Rceuinrrnrenrded nevisionns inn
\nnieriC;nni 1)einnal ,\ssnneiar;nnnn gnnidcliines hnr,nceepianncc olclnennniuilicr.ipcnniin
prnndrreis for gingivitis nnnrrrinI. (keporr nil ihe dusI l1rree nun I )esignn mid
\natvsi. in Denial arid Oral Ikesc;ireln run the ( omnineil unmi 1 lnernpeiniies 01
ilis .\niieriCan Dental Assiieiarii,nr / J’n;,ev/o;,,,,/ I/i 9qmj.29)m2993fl
21. LS. Iood arid 1)rrrg .4dninirrisirariori. C )ral Ire,rlnli care drug pnrichincis Or
irver—iheciiiinnier lrrrrnuarr risc:.iririgirigi iris/rnrii)iI.ie(Ue drirg piirilmnens: esi,iln—
I Rh inneni r ola nrrniiiiugraphr: propose-cl rules. 1dm! lAin. 21 )OS:(i8:322(2—)2293.
22. lil(ernrark WI ISloiiinnqiiisn CC;. Reiflv lid. eral C;nissiln nlsnnnnucs in
niarirril lriiifilrnn rind ins irnrpaen inn oial disease nniinnagennrenni dc/n I/in,
//,. (993(1(11:1423
23. \(agcr 1)1.. Xinieinec—1-nmie IA. I l.iPijee -‘il) Soer.nnsk; 55 I )isnrilmunsinn
iii sclectcd bacterial species on iniramucal siirfiees. / (in;, !S-;uiilnn;ninm/.
20)).$:.SIIE 1:644—654
24. ‘iris 0. l’ianuirri K leary lAX ci il. I Inc ii vivin sIts is nil am inn.
repnie mouthwash ott oelor—prnndnicung iniicnmnnngannisinrs. / I/ini //il.
I1$(:6)I(IIl:I$9l—I$96
25. Ilolanuowski Si. (dcslnciclcr (.5. Sunroin 55. IkcI;nnioinsluip lreisneenn
niral pain arid erlnainnil ciiinccnnrr.iniiirn in nnniunirlrrirnses. I /‘n;nui/onnm/ I/IS.(1)1)5:5(1)51: 192— (93
26. I’crnnrginnda IS. Sernternnlrrini I. Selicrer \X . en il \lcnilnolcunnn;ninninig
niorrrliwashes: clFder inn eoinnposire hardness. 1 (un I/in,. I 994:5)21:611—6227. l.iie II. Se Iiionr (1k. I lie eflder iifnrnniunrhiriirscs rind topical .ipplicanininnnI eblorlnexicline nnr nbc develiipnnennr of dernr.il plaque nind giingiviris inn
nninn. / IS;IniInn,aI I/n:c I 93)I.5(2I:9$3
28. 1 )eiinnnii C \M ( :hlnirlnesidinne. ni: Block 55. cd. l)isin/dniinw SicR/inininnl,
‘n I’n:lun’nnlon. 4th eel. l’lnilaelelplnia. PA: lea anid 1-chiger: 11)1)1 :24-2$9
29. linnncs CC; Clihnnrhesidinnc: is it still lie gold siiinelnrd? /S;i,ii/nn;,iiui
I 99: I 5:5 5—62.

APPLIED AND ENvIR0Nam’rrAI. MICRoBIOLOGY, Apr. 2010, p. 2326—233400992240/10/$12.00 doi:10. 1128/AEM.02090-09Copyright © 2010, American Society for Microbiology. All Rights Reserved.
Vol. 76, No. 7
RealTime Microsensor Measurement of Local Metabolic Activitiesin Ex Vivo Dental Bioflims Exposed to Sucrose and
Treated with ChlorhexidineVChristiane von Ohle,l* Armin Gieseke,2Laura Nistico,3Eva Maria Decker,’
Dirk deBeer,2 and Paul Stoodley3’4University Hospita4 Dental Clinic, Department of Conservative Dentist, Osianderstr. 2-8, D-72076 Tubingen, Germany’;
Microsensor Group, Max Planck Institute for Marine Microbiology, Celsiusst, 1, D-28359 Bremen, Germany2;Allegheny-Singer Research Institutc, Allegheny General Hospita4 320 East North Ave., Pittsburgh,
Pennsylvania 15212-4772; and National Centre forAdvanced Tribology at Southampton,School of Engineering Sciences, University of Southampton,
S017 1BJ Southampton, United Kingdom4
Received 30 August 2009/Accepted 18 January 2010
Dental biofllms are characterized by structural and functional heterogeneity. Due to bacterial metabolism,gradients develop and diverse ecological microniches exist. The aims of this study were (i) to determine themetabolic activity of microorganisms in naturally grown dental biofllms ex vivo by measuring dissolved oxygen(DO) and pH profiles with microelectrodes with high spatial resolution and (ii) to analyze the impact of anantimicrobial chiorhexidine (Clix) treatment on microbial physiology during stimulation by sucrose in realtime. Bioffims were cultivated on standardized human enamel surfaces in vivo. DO and pH profiles weremeasured in a flow cell system in sterile human saliva, after sucrose addition (10%), again after alternativetreatment of the sucrose exposed biofllms with CHX (0.2%) for 1 or 10 mm or after being killed withparaformaldehyde (4%). Biofllm structure was visualized by vitality staining with confocal microscopy. Withsaliva as the sole nutrient source oxygen consumption was high within the superficial biofllm layers renderingdeeper layers (>220 jim) anoxic. Sucrose addition induced the thickness of the anaerobic zone to increase witha concurrent decrease in p11 (7.1 to 4.4). Clix exposure reduced metabolic activity and microbial viability atthe biofllm surface and drove metabolic activity deeper into the biofllm. CIIX treatment led to a reducedviability at the biofllm surface with minor influence on overall biofllm physiology after 1 mm; even after 10 mmthere was measurable respiration and fermentation inside the biofllm. However, the local microenvironmentwas more aerated, less acidogenic, and presumably less pathogenic.
Bioffims arc complex, surface-associated, microbiologicalcommunities (7) that are characterized by microscale spatial,structural, and functional heterogeneity (40). The biolilm Consists of microorganisms that are embedded in an extracellularslime matrix consisting of biopolymers of microbial origin suchas polysaccharides, proteins, and DNA (16). This extracellularpolymeric slime is highly hydrated and influences both thestructure and the diffusion behavior within the hiofllm (39).Bacterial metabolism results in the development of chemicaland physiologic/metabolic gradients within the hioflIm (17).Due to different concentrations of oxygen, nutrients, and microbial metabolic by-products, local microecological niches arecreated, allowing the coexistence of microorganisms with different growth requirements in close proximity (30). For example, the growth of anaerobic microorganisms within a generallyaerobic environment within the oral cavity is possible. Carbohydrates and sugar are the most important energy sources formicroorganisms in dental plaque (23) and, in the case of alacking external substrate supply, they are able to metabolize
* Corresponding author. Mailing address: Dental Clinic, Department of Conservative Dentistry, Osianderstr. 2-8, D-72076 Tubingen,Germany. Phone: 49-7071-2983498. Fax 49-7071-295462. E-mail:[email protected].
V Published ahead of print on 29 January 2010.
salivary glycoproteins (5). Nutrient depletion causes the microorganisms to either grow very slowly or to stop growing completely, entering a dormant-like state.
Changes in the ecologic balance of the oral microflora and indental bioffims are a causative factor for the development ofdental caries (43), gingivitis, and periodontitis (1); thus, thesediseases can be considered as bioffim mediated. Fundamentalfactors that may lead to a shift in the microflora and thepredominance of pathogens are the local pH value, the redoxpotential, and the availability of nutrients and/or carbohydrates(30). Caries, for instance, is a multifactorial disease. However,its main cause is the bacterial carbohydrate catabolism and therelease of organic acids by acidogenic bacteria in the biofilm.This promotes the predominance of cariogenic pathogens suchas Streptococcus mutans, Streptococcus sobrinus, and other acidogenic microorganisms (28, 43). Consequently, this results infurther acid production and a decreasing pH. Associated withthis is the demineralization and lesion development of dentalhard substance (54).
Next to individual improvement of mechanical oral hygiene(i.e., mechanical and manual brushing, as well as flossing),prevention and therapy of oral disease is achieved by adjunctive oral hygiene products containing antimicrobial agents (29,47). A concentration of 0.2% chlorhexidine (CHX) in oralmouth rinses showed the best efficacy in clinical studies and is
2326

VOL. 76, 2010 LOCAL METABOLIC ACTIVITIES IN DENTAL BIOFILMS 2327
still considered a “gold standard” (45). The antiplaque effect ofCHX is based on a broad antibacterial spectrum. During application it immediately shows bactericidal effect and continuous bacteriostatic effect due to its high substantivity in the oralcavity (20). Electron microscopic examinations showed thatCHX binds to and damages bacterial cell membranes and leadsto structural changes and leakage of cytoplasm (3). Furthermore, contraction of in vitro grown hiofllms after CIIX exposure was shown in addition to cell damage (19,44), which couldcause changes in the diffusion behavior by changes to extracellular polymeric slime density. However, in deep layers of oralbiofihus not all bacteria were reached (49). Direct visualizationby fluorescence microscopy of the CFJX effect was described byTakenaka et al. (44) for a three-species oral bioflim grown in
vitro. Cell damage started from the periphery of bacterial aggregates and slowly continued into the depths. Other authorshave reported the inability of CHX to completely kill all bacteria in different in vitro bioffim systems (15, 19, 32) and in vivo
studies (48, 55) when a normally used clinical concentrationwas applied at usual exposure times. The killing efficacy wasdependent on the age of the bioIilm and thus on its thicknessand composition.
Detection of concentration gradients in oxygen, pH, andmetabolites in undisturbed biofibms in situ requires a microsensor technique. Microelectrodes with a tip diameter of a fewmicrometers offer precisely localized measurements on themicroscale in three dimensions under real-time conditions (9,35). Thus far, microelectrodes have been applied for measuring plaque pH in dental research in a groove model rtr vivo (53,54) and in in vitro-grown S. mutans biolilms (13, 42). However,there is no information on direct measurements of oxygendistribution and consumption in dental biofllms grown in vivo
in the human oral cavity. In the field of environmental microbiology, analysis of the microenvironment, local activities, andgradients by microelectrodes is correlated with microscopicexamination of the bioflim structure, thus allowing a relationship to he made between hiofilm physiology and structure (18,37). We decided to take a similar approach to characterize theeffects of sucrose and CHX on es vivo plaque biolilm physiology. The goal of the present study was to examine the metabolic activity (oxygen consumption and acid formation) andviability and the effect of antimicrobial CFIX treatment on thephysiology of the dental bioflims during exposure to sucrose.The spatial distribution of live and dead bioflim cells wasexamined by confocal laser scanning microscopy (CLSM), aswell as by microbiological culture.
MATERIALS ANI) METHODS
Biofllm formation. An individually fabricated intraoral acsylic stent suppliedwith standardized human enamel slivers was worn by one healthy person for 3days, starting in the morning on different occasions to obtain in vivo generationof mature dental hinflims. A preceding dental examination revealed on clinicaland radiological signs of gingivitis, periodontitis, or caries. The enamel specimens were prepared from freshly extracted human third molars. After sterilization, they were processed to a surface roughness of 0.16 ± 0.02 m according tonatural interproximal enamel-enamel contact areas (52). The area (in mm2) ofthe enamel surface was calculated following digitalization (Scion Image Rel. 4;Scion Corp.). Afterward, the specimens were fixed to the stent in the region ofthe upper premolars and molars toward the natural teeth to simulate retentionareas (Fig. 1). During the time of binfihn fomsation, a regular diet was maintained and personal oral hygiene was performed using a toothbrush, dental floss,and water. During meals and tooth brushing the stent was stored in a humid
FIG. 1. Clinical picture of the upper jaw with the intraoral acrylicstent in situ. The enamel slivers (E) were fixed in the region of thepremolars and molars toward the natural teeth to simulate retentionareas (arrows).
chamber. At least 2 Ii before the biofilni samples were taken, the subject refrained from eating and drinking. At the end of each period the specimens werecarefully removed from the device for further analysis without interfering withthe adhering biofilm. The procedure was approved by the ethical cornnsittee ofthe medical faculty and informed consent was given.
Antimicrobial treatments. Untreated native dental plaque bioflims with nosucrose amendment served as control (—sue). The antimicrobial treatment ofpreviously sucrose exposed biofllms (+suc) was performed cc vii’o using a 0.2%CEIX formulation (Chlorhexamed Forte; Glaxo SmithKline, Bflhl, Germany).The biofllms were exposed to 10 ml of the CHX solution for either I ruin(CHX_1) or 10 mm (CHX 10). Afterward, they were carefully dipped intosterile saliva. As a negative control, bioffims were killed by fixation with 4%paraformaldehyde (PFA) overnight. After fixation, the biofilms were cleanedtwice in sterile saliva. The effective CFIX concentration was calculated withindifferent layers of the biofllm based on a simplified model (semi.infinite medium,the Clix surface concentration c5 equals the concentration in the liquid of0.2%) (8).
Microeledrode measur5menls. (I) Saliva. For saliva samples, 30-mi portionsof whole saliva were collected by paraffin stimulation from two healthy volunteers 2 h after breakfast. Sterilization was performed immediately (12). Aftersonification and separation of debris by filtration, each saliva sample was centrifuged at 25,524 x g for 30 mm at 3C (Biofuge 22R; Heraeus, Hanau, Germany). The supematant was filtered by two Millex low binding protein filters(0.45 and 0.22 i.m; Millipore, Eschborn, Germany). The sterile saliva was buffered weakly and adjusted to a pH of 7.1 to 7.2 by 0.2 mM Na,HPO4and 0.3 mMKH,P04,stored at 4’C, and used within 48 h. For experiments, saliva was diluted1:10 (volJvol) using sterile water.
(ii) Ex viso flow cell setup. After removal from the stent, the enamel couponswith biolilm were immediately placed in a small Ilow cell (6.75 cm3 for subsequent microelectrode measurements. The flow cell was fed from a total volumeof 250 cm3 of 1:10 saliva by use of two peristaltic pumps connected to both theinlet and outlet of the flow cell at a flow rate of 3 mI/rain. The sterile humansaliva as medium was aerated, and the temperature was kept constant at 24’C(room temperature). The limited volume of saliva due to the harvesting andhandling procedure necessitated recirculation. Each set of measurements werecollected within -60 mm and no longer than 90 min, after which the spent salivawas replaced with fresh saliva. Dental biofilm samples were subjected to thesalivary medium with no added sucrose (—sue) and with added sucrose (25 g;10% [wt/vol]) to stimulate microbial activity (+suc). Antimicrobial treatment wasperformed by removing the previously sucrose exposed specimens carefully fromthe flow cell and immersing them into the Clix formulation (CHX_1 andCHX_10) or PFA. After each treatment, the samples were gently dipped in 1:10saliva and immediately returned to the flow cell that contained the sucrose-supplemented 1:10 saliva. After removal from the oral cavity, the thickness of thecx vim biofilms was measured from microelectrode experiosents, as well as beingestimated from a stereomicroscope.
(iii) Microeledrodes. Microelectrodes were used to measure dissolved oxygen(DO) concentration and pH. They were fabricated as described by Revsbech (36)

2328 VON OHLE ET AL. APPL. ENvIRoN. MicRoBtoL.
and deBeer et al. (10) with tip diameters of 10 and 5 p.m. Measurements wereperformed by using a semiaulomated setup. Sensors were connected to a picoamperenseter and millivoltnseter, respectively, and positioned by using a micro-manipulator (model MM33; Maerzhaeuser, Wetzlar, Germany) with a motor-controlled z-axis (model VT-SO; Micos, Eschbach, Germany). Amplifier signalswere recorded by a data acquisition system (model DAOCard AI16XE5O; National Instruments. Austin, TX) on a portable computer. Positioning duringprofiling and data acquisition were controlled by using custom-made software.Profile measurements were started 30 mm after the biofilms were placed into theflow cell, allowing the biofilm to equilibrate and come to steady state (taken asno sigoiticant change to the profile or a depLh measurement Within a 2-mmperiod). We measured depth profiles at high spatial resolution (25-p.m increments) within the biofilin before and during exposure to sucrose (at least 20 mmupon sucrose addition) or after additional antimicrobial treatment (CHX andPFA). Each profile took about 5 nun. Also, the dynamic response (time series)of the biofllm to sucrose addition was recorded by leaving the microelectrode atone depth within the biofihn. For time series, the tip of the sensor was positionedeither at the surface of the biofilm (1)0) or near the biofilm base (pH). For fluxcalculations it is important that the profiles were at steady state. Steady state wasconfirmed by repeated profiling. Approximately 2 miii after steady-state conditions had been achieved repeated profiles were taken at slightly different locations. Each set of measurements was collected within 6)) ruin. Proliles, aerialrates, and local conversion rates were calculated from at least four to six profiles.Profile data were reported as means ± 2 (standard errors [SE]).
In order to obtain constant and reproducible experimental conditions for allmicroelectrode measurements, the ex vit’o measurements were conducted atroom temperature (24°C). In this way we ensured that there were no temperature fluctuations of the microelectrodes, the standardization solutions, nr themedia during measurements despite the various rapid medium exchanges, allowing the profiles to more rapidly come to steady state.
(iv) Rate calculations, Under the conditions of the setup, the biofilm surfaceis covered by a stagnant medium layer, through which transport occurs only bydiffusion. The diffusive transport of solutes through this diffusive boundary layer(DBL) is proportional to the concentration gradient in the DBL according toFick’s first law of diffusion: J = D5 (dc/ar), where 1 is the flux (in nmol cm 5 I)
D5 is the molecular diffusion coefficient (in cm° s), and dc/ar is the concentration gradient (in nmol cm4). Assuming a molecular diffusion coefficient ofoxygen of 2.3634 x iO- cm2 s (4) for oxygen at 24°C. aerial transport ratescan he calculated that represent the total hiottim activity. Assuming diffusion asthe dominant transport process within the biotlim, the curvature of the profileswithin the biofllm was used to calculate the local activities according to a mod’ified version of Fick’s second law of diffusion: D5 (i?c/1x2)= r, where D5. is theeffective diffusion coefficient within the biofilm, 52c/5r2 is the local change inconcentration gradient, and r is the local conversion rate (in mol m3s’) (35).We used a stepwise algorithm (18) to calculate local conversion rates (oxygen) asa measure for local oxygen consumption. To determine where acidification wasoccurring within the biofllm, we calculated rate data in terms of H productionor consumption from the pH data. However, since [H’J is a function of buffering(21), our concentrations should only be considered for purposes of relativecomparison in this system and not as absolute concentrations. First, we convertedthe pH to proton concentration [Wj in nmol cm3by using the equation [H’] =
1/10’. For the D5 of H we used 1.86 x iO em2 s’, which was based on aD.q of 9.31 x io cm2s at 25°C (26) and aD5JD,5 ratio of 0.2, which wasestimated by Stewart (39) from diffusion measurements in dental plaque. Negative uptake rates indicate net H production (acidification) and positive uptakerates indicate net consumption.
CLSM. The CLSM investigation was performed by using a Leica DM RXEmicroscope connected to a TCS SP2 AOBS confocal system (Leica Microsystems) equipped with an argon laser (488 nut) and an He-Ne laser (543 nm,633 005).
Analysis of microbial viability. The biofilm samples (—sue, ±suc, CHX_1,CHX1O, and PFA) were stained by using a Molecular Probes Live/DeadBacLight bacterial viability kit (Invitrogen). Each biofilm sample was incubatedin 500 p.1 of staining solution for 15mm The stained bioffims were subsequentlyexamined by CLSM. The green fluorescent DNA-binding dye SYTO 9 labeled allMO (detection. 500 to 535 mu), while the red fluorescent propidium iodide (P1)labeled MO with harmed bacterial membranes (detection, 600 to 720 nm).Sequential scanning mode was used to eliminate “bleed over.” Z-series of con-focal images (ty scan) were acquired with a 10 x 0.3 (NA) magnifying objectiveat 2-p.m intervals. We chose low magnification to provide a larger field of viewand a more general representation of the binfllm distribution in plan view at thetop of the biofllm and the base. The Ihickness of the optical sections was —6 pan;thus, we oversampled in the z dimension by a factor of 3 to ensure a continuous
-500
..40-0
-300
-200
-100;
a.
—0-— - SUC :01
—4— ÷ sec—w— CHX_t
.--—CHXl0-.—PFA
Biofibn
FIG. 2. Averaged oxygen profiles measured in situ on dental biofilms in salivary solution (1:10) without sucrose (—sue, n = 11), with10% (wtjvol) sucrose (+suc, it = 6), and with 10% sucrose after 1 mm(CHX1, it = 4) or 10 mm (CHX_l0, it = 5) of treatment with CHXand in a PFA-killed control (PFA, n = 3). Error bars were omitted forclarity.
data set. Additionally, the biofilm thickness (L,-) was measured as the distancebetween the substratum and the highest cell cluster of the entire biofllm. Thebinfllms were examined at two different locations in the middle of the enamelsurface. Digital image analysis of the optical sections was performed by using acustom-made software based on Axinvisinn (Zeiss, Germany). The analysis ofthe microbial viability (V) was based on the fluorescently labeled membraneintegrity. After thresholding, V svas calculated as the percentage of green (vital)voxels related to the whole number of red (dead) plus green voxels in everyoptical Section of the biolilma. l1or each hiolilm, the mean viubilily il alt layerswas calculated.
Culture method. In addition to the fluorescence-based microscopic viabilityassessment, conventional cultivation was also performed. The biofllm was mechanically detached from the enamel surface by scraping and transferred intosterile saline, followed by sonilleation on ice to disrupt larger clumps and chains,and then homogenized by vortexing. The total bacterial counts (BC) were measured by using a bacterial counting chamber (System HeUser, Saaringis, Germany; counting volume, 0.8 x iO mm3) under a dark-field microscope (iuagoification, 5(fix). For this purpose the number of single cells and particles (smallremaining chains were counted as one count) were enumerated. Thus, it ispossible that our BC were slightly underestimated. The BC were reported permm2 of the substrate surface (BC/mm2). Cultural viability was examined byplating the serially dfluted biofllm samples on Schaedler agar plates supplemented with sheep blood and vitamin K1 (Becton Dickinson, Heidelberg, Germany) using a spiral plater (Meintrup, Lahden, Gernsany). The CFU werecounted after anaerobic incubation for 48 h at 37°C and reported as CFU/mns2.
Statistics. BC and CPU values were log transformed. The data were reportedas mean and corresponding 05% confidence intervals (CT) unless otherwiseindicated. Statistical comparisons between data sets were made by using analysisof variance (Microsoft mcd 2(l))))). Diffcrenccs were considcrtd sitnilicant forP < 0.05. Each experiment was performed three times.
RESULTS
Microelectrode measurements. (i) Profiles of DO and pH.The bioflims were —300 p.m thick. Repeated profiles over thecourse of the experiment indicated no measurable increase inbioflim thickness over this time. All bioffims except the PFAkilled group showed an anaerobic zone in deep bioflim layers.Here, we define anaerobic regions according to the criteria ofLoesche (27) as oxygen saturation values of <0.5% (Fig. 2 and3). With no external substrate present (—suc), DO penetratedinto the biofllm to a dcpth of 220 p.m. Upon sucrose addition(+suc), DO penetration was reduced to the upper 150 jim,
0 20 40 60 SO tooOxygen (% air sat,)
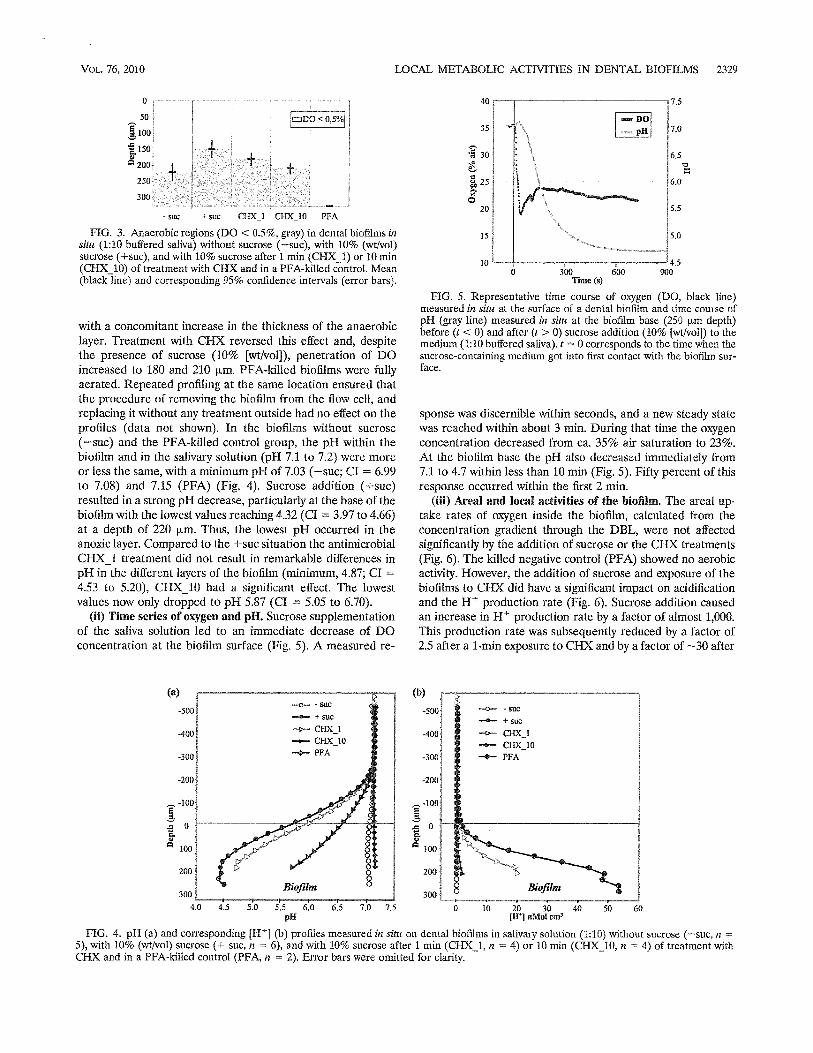
VoL. 76, 2010 LOCAL METABOLIC ACTIVITIES IN DENTAL BIOFILMS 2329
11001
1150
200-
250
300
- sue + sue CHXI CHXIO PFA
FIG. 3. Anaerobic regions (DO < 0.5%, gray) in dental biofairns insitu (1:10 buffered saliva) without sucrose (—suc), with 10% (wtfvol)sucrose (+suc), and with 10% sucrose after 1 mm (CHX_1) or 10 mm(CHX1O) of treatment with CHX and in a PFA-killed control. Meanlack line) and cnrresponding 95% confidence intervals (error bars).
with a concomitant increase in the thickness of the anaerobiclayer. Treatment with CI4X reversed this effect and, despitethe presence of sucrose (10% [wt/volj), penetration of DOincreased to 180 and 210 p.m. PFA-killed hiofilms were fullyaerated. Repeated profiling at the same location ensured thatthe procedure of removing the hioflim from the flow cell, andreplacing it without any treatment outside had no effect on theprofiles (data not shown). In the bioflims without sucrose(—sue) and the PFA-killed control group, the pH within thebiolilm and in the salivary solution (pH 7.1 to 7.2) were moreor less the same, with a minimum pH of 7.03 (—sue; CI = 6.99to 7.08) and 7.15 (PFA) (Fig. 4). Sucrose addition (+suc)resulted in a strong pH decrease, particularly at the base of thebioflim with the lowest values reaching 4.32 (CI 3.97 to 4.66)at a depth of 220 p.m. Thus, the lowest pH occurred in theanoxic layer. Compared to the +sue situation the antimicrobialCHX_1 treatment did not result in remarkable differences inpH in the different layers of the biofilm (minimum, 4.87; CI =
4.53 to 5.20), CHX_10 had a signilicant effect. The lowestvalues now only dropped to pH 5.87 (CI = 5.05 to 6.70).
(ii) Time series of oxygen and pH. Sucrose supplementationof the saliva solution led to an immediate decrease of DOconcentration at the biofilm surface (Fig. 5). A measured re
40
35
FIG. 5. Representative time course of oxygen (DO, black line)measured in situ at the surface of a dental hiofllm and time course ofpH (gray line) measured in situ at the biofllm base (250 p.m depth)before (t < 0) and after (t> 0) sucrose addition (10% [wt/vol]) to themedium (1:10 buffered saliva). t = 0 corresponds to the time when thesucrose-containing medium got into first contact with the biofllm surface.
sponse was discernible within seconds, and a new steady statewas reached within about 3 miii. During that time the oxygenconcentration decreased from ca. 35% air saturation to 23%.At the biolilm base the pH also decreased immediately from7.1 to 4.7 within less than 10 mm (Fig. 5). Fifty percent of thisresponse occurred within the first 2 mm.
(iii) Meal and local activities of the bioflim. The areal uptake rates of oxygen inside the biofilm, calculated from theconcentration gradient through the DBL, were not affectedsignificantly by the addition of sucrose or the CHX treatments(Fig. 6). The killed negative control (PFA) showed no aerobicactivity. However, the addition of sucrose and exposure of thebiolilms to CHX did have a significant impact on acidificationand the H production rate (Fig. 6). Sucrose addition causedan increase in H production rate by a factor of almost 1,000.This production rate was subsequently reduced by a factor of2.5 after a 1-mm exposure to CHX and by a factor of —30 after
0
50
+ +
DO<05]
+9 3
25
0
7.5
DOp11 7.0
6.5
116.0
V 5.5
5.0
4.50 300 600 900
Time (s)
20
15
10
—0— - SUC
—.— + sue—0-- CHX_1
CHX_10..4. PFA
(a)
-500
-400
-300
-200
-100
I
100
200
300
4.0
—0--- - sue- + sue
—--- CHXI—p— CHX_l0-4-- PFA
(b)
-5001
-400
-300
-200
-1001
I
100
200
300Biaflim
1 =t-4,5 5.0 5.5 6.0
p110 10 20 30 40 50 60
lH eMs! cm3
FIG. 4. pH (a) and corresponding [Hj (b) profiles measured in situ on dental bioflhns in salivary solution (1:10) without sucrose (—sue, n =
5), with 10% (wt/vol) sucrose (+ sue, n = 6), and with 10% sucrose after 1 mm (CHX1, n = 4) or 10 mm (Clix 10, n = 4) of treatment withCHX and in a PFA-killed control (PFA, n = 2). Error bars were omitted for clarity.

2330 VON OHLE FT AL. APPL. ENvIRoN. MICROBIOL
- sue + sue CHX_I CHX_l0 PFA
FIG. 6. Areal bioflim uptake rates of oxygen () and H (LI) indental biofilms in situ (1:10 buffered saliva) without sucrose (—suc),with 10% (wt/vol) sucrose (+sue), and with 10% sucrose after 1 mm(CHX1) or 10 mm (CHX 10) of treatment with CHX and in aPFA-killed control. Error bars correspond to 95% confidence intervals. For H negative uptake rates indicate proton production (acidification).
a 10-mm exposure. The PFA-killed control showed no acidification.
The local reaction in separate hiotllm layers to the differenttreatments, however, showed a more detailed picture and varying influence of CJIX on respiration and acidification insidethe dental bioflim (Fig. 7). With saliva alone, oxygen was consumed to a small extent in all biolilm layers down to 220 p.m.Although the oxygen flux into the bioflim was marginallychanged by sucrose addition, the distribution of local uptakerates at different depths within the bioflim was altered. Thehighest local uptake rates within the bioflim were localizedclose to the surface in the top 50 p.m of the hioflim. CHX_1inactivated the biofllm surface but led to increased oxygenuptake rates between depths of 50 to 120 p.m. After CHX_10treatment, the aerobic heterotrophic activity was depresseddeeper in the biolilm to between 75 and 175 p.m; thus, theoverall oxygen consumption remained constant. The PFAkilled control showed no aerobic activity in any of the biofilmlayers.
With unsupplemented saliva, there was little acid productionanywhere in the biofilm. However, when sucrose was addedacid was produced in the bottom region of the bioflim between
TABLE 1. Structure and viability of in situ dental biofilms assessedby CLSM”
Lm) V(%)Treatment
Mean 95% CI Mean 95% CI
—sue 226.7 148.7—304.6 63.4 53.6—73.08+suc 217.3 201.4—233.2 70.7 63.0—78.4CHX1 230.0 106.3—353.7 2.0 —1.6—5.6CNX_10 228.0 116.1—339.9 0.7 —0.2—1.6PFA 232.7 143.0—322.3 18.9 8.0—29.9
Bioffims were assessed without antimicrobial treatment (—soc. +sue) andafter 1 mm (CHXI) or 10 into (CHX 10) of CHX treatment or after PFAexposure (PFA). The mean biolilns thickness (L), the mean viability of allinvestigated dental hiofilni layers (V), and the cnrrespnnding 95% cnnfldenceintervals (CI) are indicated.
175 and 275 p.m. After exposure to CHX_1, acid productionwas elevated in the biofilm to 150 p.m. After exposure toCHX_10 and after PFA killing, local acidification was suppressed throughout the hioflim.
CLSM. Microbial viability. CLSM analysis revealed a comparable mean L of 230 to 240 p.m for all treatment modes(Table 1). Depending on the high density of in vivo-createddental bioflims. thc laser penetration depth was limited to theouter 40 to 100 p.m (65.6 ± 24.1 p.m) of the bioflim cellclusters. Thus, deeper areas could not reliably be visualized.The viability of untreated bioflims was Ca. 60 to 70%. Thedistribution of live and dead or damaged bacteria showed nodistinct distribution pattern. After CHX treatment, the meanviability was reduced to 2.0% (CHXj) and 0.7% (CHX_10),respectively. The microorganisms at the hiofilm surface werekilled or damaged by CHX (Fig. 8). The PFA-”killed” controlindicated a viability of almost 19% based on the Live/Deadstain.
Total bacterial counts and CFUImm2.The log BC/mm2values ranged between 7.27 (+suc) and 6.57 (PFA) and weresimilar for dental bioflims without and after treatment withCHX and PFA (Fig. 9). Almost 38% of the native bioflimmicroorganisms were culturable (log CFU/mm2 6.81; —sue).After sucrose exposure, the number of CFU increased (logCFU/mm2 7.13). CHXI treatment had a minor influence
-SaC + Sue clix I
25
5075
too. 125
150
175200
225
250275
clix to PFAi_
--
-. 1=—. E=D—.,.
===3—
_
I
. C —
0 5 -20 -II 0 20 30 -40 -30 -20 -10
Lucid O,/11 uptuke estes (nMot cm4 a’)
10 Oi 0
FIG. 7. Local oxygen () and H (LI) uptake rates in different layers of dental biofllms in situ (1:10 buffered saliva) without sucrose (—sue),with 10% (wt/vol) sucrose (+suc), and with 10% sucrose after 1 miii (CHX_1) or 10 mm (CHX 10) of CHX treatment and in a PFA-killed control(PFA). Error bars correspond to 95% confidence intervals. A negative uptake rate indicates net production, and a positive uptake rate indicatesnet consumption.

VoL. 76, 2010 LOCAL METABOLIC ACTIVITIES IN DENTAL BIOFILMS 2331
FIG. 8. Micrographs depicting the dental biofilms after staining with Live/Dead BacLight. Live or vital bacteria are green, and dead or damagedbacteria are red. Three-dimensional reconstructed confocal images and corresponding optical sections (xz andyz) at low magnification arc shown.Scale bar, 200 rim. (a) Native 3-day-old denial hiollim showing a haphazard arrangemenL of vital MO and damaged cells with unstained areas inbetween; (b) biofilni after 1 mm of CHX treatment (CHX1) displaying only damaged bacteria at the surface; (c) biofilm after 10-mm CHXtreatment (CHX 10) with a similar appearance; (d) PFA-killed control.
(log CFU/mm26.45), whereas CHX_1O led to a reduction tolog 4.93 CFU/mm2.The PFA exposure reduced the CFU byalmost 6 log units.
Diffusive transport of CHX within the bioflim. Assuming thetransport of CHX from the solution into the bioflim is driven bydiffusion, concentrations could be modeled along bioflim depthfor different incubation times (Fig. 10). An assumed critical concentration of 0.1% CHX was reached only in a depth of 70 p.mafter 1 mm and also after 10 mm in a biofilm dcpth of about 230pm, but not in the deepest biofllrn layers.
Statistics. A summary of the statistical analysis results forthe different investigation variables is given in Table 2.
DISCUSSION
Changes in the gradients of oxygen and pH in response tosucrose and additional CHX treatment in complex dental biofilms formed in vivo were measured by microelectrodes underreal-time nondestructive conditions. The local effects on respiration and acidification inside dental biofllms were docu

2332 voN OHLE ET AL. APPL. ENvIRoN. MICROBIOL.
EE 8T
;!i i ri- sue 4- sue CHXI CHX1O PFA
FIG. 9. Total bacterial cell counts (log BC/mm2,D) and CFU (logCFU/mm2.) in native dental biofiln]s (—sue). after sucrose exposure(+suc) or after 1 mm (CHX1) or 10 mm (F1X 10) of treatment withCHX and in a PFA-killed control. Error bars correspond to the 95%confidence intervals.
mented. With unsupplemented saliva, oxygen consumption inthe upper bioflim layer resulted in the bottom half of thehioflim being anoxic. Microbial respiration activity was obviously driven by endogenously produced substrates or salivarycomponents, as became evident from the complete lack ofactivity in the PFA-killed control. Similar gradients have beendocumented in Pseudornonas aeruginosa (51), Streptococcusepidermidis, and Staphylococcus aureus (33) biofllms. Oxygenconsumption in human dental biofllms has been found to becaused by Gram-positive microorganisms and especially oralstreptococci (28, 46), not only for respiration but also to produce 1420,, which is presumed to be a mechanism by which toattack competing bacteria (23, 31). The result is that an anoxicniche conducive to the survival of anaerobic or acidogenicbacteria is created in deeper layers of the biofilm (22, 32).After sucrose addition the thickness of the anoxic layer increased, presumably due to increased respiration and otheroxygen consuming metabolic activity in the upper layer. Concomitantly, a strong decrease in pH occurred in the anoxicregion. The dynamic response of the dental bioflim physiologyto environmental changes occurred instantly, and a new equilibrium was established within minutes. Comparable resultswere shown by Stoodley et al. (42) in S. mutans hioflims.
P value for:
Biofilni conditions Biofllm structureComparedtreatments Flux and viability
Anaerobic
0, H depth L, v Log BC! Log CFU/mm2 mm2
—suc/+suc 0.03 0.01 <0.01 0.85 0.33 0.91 0.20+suc/CHX 1 0.22 0.08 0.12 0.85 <0.01 0.14 0.04+sucJCHXlO 0.14 0.01 <0.01 0.86 <0.01 0.45 <0.01+suc/PFA 0.01 0.04 <0.01 0.76 <0.01 0.42 <0.01
Without supplemental sucrose, almost no acid formationwas detectable in the biolilms, but after sucrose addition thefermentation activity increased immediately in the anaerobicbiofilni layers (>200 tim). After about 10 mm a minimal pHvalue of 4.3 was obtained. The range of pH drop we measured(from pH 7 to between pH 5.5 and 4.3) was in agreement withthe results of microelectrode measurements in a dentinegroove model reported by other authors (13, 53, 54). Thedegree of acidification in thc hioflims will be expected to varybetween individuals, as a function of both host and bacterialfactors such as biofilm thickness, concentration of acidophilicbacteria, and saliva chemistry.
Because the temperature during the electrode measurements was below the physiological intraoral temperature (ca.36°C), it can be assumed that the metabolic activity of thebiofilms would have been higher at a higher temperature. Nevertheless, valuable information on microbial activity in dentalplaque has been gathered from experiments performed on esviva specimens conducted at room temperature (53, 54), andwe also point out that during the course of eating and drinkinghot and cold foods the hard surfaces of the teeth experience awide range of temperatures.
CHX effect on dental bioflim physiology and structure. Anideal prerequisite for a successful antimicrobial chemical treatment, such as CHX, is that all bacteria within the biofilm areexposed at an adequate concentration for an adequate time inorder to achieve a clinically relevant reduction in pathogenesis.We used a simple diffusion model to calculate CHX concentrations as a function of depth and time. The model did notaccount for adsorption, release, or consumption, which willalso iniluence transport (39). We assumed that a concentrationof 0.1% CHX would be a clinically relevant concentrationbased on (i) the reported MIC range of 8 to 500 mg/liter byStanley et al, (38) for different strains of oral bacteria and (ii)the finding that for some oral bacteria the BIC (biofilm inhibiting concentration) was up to 500 times (Streptococcus sanguinis) (25) that of the MIC. Furthermore, Vitkov et al. (49) wereable to verify damage to bacterial cell membranes by electronmicroscopy when using a concentration of 0.1%. The calculated concentration profiles showed that when using a 0.2%CHX solution with an exposure time of 1 mm a concentration
TABLE 2. Results (P values) of the statistical comparison betweendifferent treatment modes determined using ANOVA”
° Differences were considered significant for P < 005. Dental biofllms wereassessed in situ (1:10 buffered saliva) without sucrose (—suc), with 10% (wt/vol)sucrose (±suc). after 1 olin (CHX_1) or 10 mm (CHX_10) of CHX treatment.or after I’FA exposure (PFA). Boldfacing indicates a statistically signilicaoEdifference (P <0.05). L5, biofihn thickness: V, mean microbial viability; BC, totalbacterial count.
S
1
‘iofilm
lOs20s30 s60 a
———150s300 S
—60053QQ..
0.0 0.05 0.10 0t5 0.20c (Clix) l%l
FIG. 10. Modeled concentration profiles of a 0.2% CEX formula[ion in denial biolilms at different incubation times (t) between 10 and600 s.

VoL. 76, 2010 LOCAL METABOLIC ACTIVITIES IN DENTAL BIOFILMS 2333
of 0.1% or greater was achieved only to a depth of 70 p.m.Interestingly, this matches well with our experimental data,which showed that oxygen consumption had shifted from thetop 50 p.m to below 75 p.m after 1 mm of CHX exposure. Thediffusion model serves well for orientation where the diffusionbehavior of CHX in hioflims is concerned and provides insightinto optimization of routine hygiene maintenance. The modelpredicts that it would take 17.5 mm to achieve 0.1% Cl-DC atthe base of a 300-p.m-thick bioffim, e.g., interproximal or atother retention sites. However, if (he thickness of the biolilmwas reduced to 100 p.m the time will be reduced to <2 mm; ifit was reduced to 30 p.m, then it would only take 12 s. Theseobservations illustrate the clinical importance of limiting thephysical thickness of the biofilm by mechanical means (e.g.,brushing or scaling) prior to exposure to rinses and that dentalbiofilms are unlikely to be controlled by rinsing alone, unlessthe penetration time can be increased or the activity is moreaggressive than CHX.
Although the customary recommended exposure time fordaily CHX use is 1 mm (2), we found limited effect by viabilitystaining, oxygen consumption, acid formation, and culturabilityover this time period. Although CHX reduced the viability andmetabolism on the biofilm surface, it did not significantly reduce the overall oxygen metabolism. Even after a 10-mm treatment the biofilm was still physiologically active, demonstratingincomplete killing, and there was a relocation of activitiesdeeper in the biofllm.
The acidifying fcrmcntativc processes of the bioflim werealso relocated by treatment with CHX. With sucrose stimulation, acid production occurred at depths of >200 p.m and after1 mm of CHX treatment higher up in the bioffim, at 150 p.m.This upward shift in activity might reflect an ecological shiftcaused by CHX more adversely affecting competitors. After 10mm, CHX exposure acid fermentation was almost completelyabolished throughout the biouIlm, and the overall acidifyingactivity was reduced to 3%. Based on the local rate calculationsand the prevailing CHX concentrations, it could be demonstrated that Cl-TX inactivated bacteria from the top down andlayer by layer of dental biolilms were killed with the highestefficacy in the outer regions. Presumably, this is caused by acombination of several mechanisms: (i) the deeper penetrationof oxygen, reducing the appearance of anaerobic processes; (ii)the higher CHX concentrations and increased toxicity effectsin deeper layers strongly affecting the fermentative processes;and (iii) a differing susceptibility to CHX of the functionalgroup of organisms (i.e., aerobic heterotrophs versus anaerobicfermentative bacteria) could also exist, since oral microorganisms show diverse natural resistance toward CHX (14).
Since the primary effect of CHX on the bacterial structure isbased on damaging the cell membrane (3, 49), the effect ofCl-TX can be visualized by vital staining based on membraneintegrity of cells. General mechanisms and limitations concerning the application of SYTO 9 and PT for the detection ofbacterial cell viability are reported by Stocks (41). If the limitations are taken into account, the results of the Live/Deadstain should be seen as semiquantitative with regard to viability. In growth curves of oral streptococci (S. mutans and S.sanguinis), Decker (11) has demonstrated that staining withSYTO 9/PT reflected thc microbial viability well according tothe conventional microbiological investigation (optical density,
BC, and CFU). A ratio of 60% vital bacteria in untreateddental bioflims has been reported in other studies of 2- to3-day-old biofilms (48, 50, 55). Compared to that, the percentage of culturable microorganisms in our study was only 38%;we speculate that there were many bacteria in the bioflim thatwere either in an inactive metabolic state or nonculturable.However, sucrose exposure (+suc) led to an increased rate ofcultivable bacteria to almost 70%, suggesting that many bacteria in native dental biofilnis may be in an inactive stale duringperiods between eating. Similarly, for staphylococci it has beenshown that there is an active zone on the biofilm surface, withonly 10% of the bacteria being indeed dead, while the rest werelive but inactive (33). In contrast to the viability of 2% estimated by Live/Dead staining, the culturability after 1 mm exposure to CHX was 58%, so it might be assumed that for shortexposures some bacteria were still viable, even if they appearedto be membrane damaged. It was only after 10 mm of exposurethat the number of CFU was significantly reduced compared tothe corresponding BC. In all groups the applied cultivationconditions had influenced the growth of diverse bacterial species (streptococci versus nonstreptococci) and thus the difference between the counts and the CFU. After PFA fixation theviability based on the Live/Dead staining was 19%, It is anticipated that the PFA fixation affected the permeability of thecell membranes, and PT might not have been able to penetratethe fixated membranes. Compared to the absence of metabolicactivity by microelectrode measurements and the almost 6-logreduction in CFU, we interpreted that the 19% viability byLive/Dead staining included false-positive results. This phenomenon is reflected in contradictory literature. On one hand,it was reported that PFA did not interfere with the stainingproperties of SYTO 9/PT (15). On the other hand, it could beshown that treatment or fixation with formaldehyde affectedthe culturability and metabolic activity but not membrane integrity based on the Live/Dead stain (6, 24, 34).
Our study demonstrates the utility of using microelectrodesto measure the influence of nutrients and antimicrobial agentson the physiology of human dental biofllms nondestructivelyand in real time. The microelectrode data can be corroboratedwith microscopy and culture techniques. The effect of CHX onsucrose-exposed metabolically active dental bioflims was investigated. It was not possible to kill the in vivo formed dentalhiofilms by CHX completely. CJIX had a more pronouncedeffect on acidification than respiration, thereby creating a moreaerated and less acidogenic environment. The data suggestthat the microecology might be changed to one that was lesspathogenic. Sustaining this microecology longer might inhibitthe selection of pathogenic microorganisms like cariogenicpathogens such as S. mutans and other acidogenic bacteria orperiodontopathogenie anaerobcs and influence the composition of the oral microbial flora favorably.
ACKNOWLEDGMENTS
This study was partially supported by Philips Oral Healthcare,USA. P.S. has been a consultant for Philips Oral Healthcare, Snoqualmie, WA, and served on its scientific advisory board.
REFERENCES
1. Brading, M. G., and P. 1). Marsh. 2003. The oral environment: the challengefor antimicrobials in oral care products. mt. Dent. J. 53:353—362.
2. Breex, M., I... Netuschil, and T. Hoffmann. 2003. How to select the right

2334 VON OHLE ET AL. APPL Er’tvntoN. MICROBIOL.
mouth rinses in periodontal prevention and therapy. II. Clinical use andrecommendations. lot. J. Dent. Hyg. 1:188—194.
3. Brecx, M., and J. Thefiade. 1984. Effect of chiorhexidine rinses on themorphology of early dental plaque formed on plastic film. 1. Din. Periodontol. 11:553—564,
4. Broecker, W. S., and T. H. Peng. 1974. Gas exchange rates between air andsea. Tellus 26:21—35.
5. Carlsson, J. 1997. Bacterial metabulism in dental biolilms. Adv. Dent. Rca.11:75—80.
6. Comas, 3., and J. Vives-Rego. 1997. Assessment of the effects of gramicidin,formaldehyde, and surfactants on Escherichia coil by flow c3ltometly usingnucleic acid and membrane potential dyes. Cytometsy 29:58—64.
7. Costerton, 3. W., Z. Lewandowski, D. E. Caidwell, D. R. Korber, and H. M.Lappin-Scoft. 1995. Microbial biofilms, Anon. Rev. Microbiol. 49:711—745.
8. Crank, 3. 1975. The mathematics of diffusion, 2nd ed. Oxford UniversityPress, Inc., New York, NY.
9. Dc Beer, D. 2000. Potentiometric microsensors for in situ measurements inaquatic environments, p. 161—194. In J. Buifle and G. Horvai (ed), Os Situmonitoring of aquatic systems: chemical analysis and speciation. John Wiley& Sons, Ltd., New York, NY.
10. Dc Beer, D., A. Schramm, C. M. Santegoeds, and M. KuhI. 1997. A nitritenticrosensor for profiling environmental biofllms. AppI. Environ. Microbiol.63:973—977.
11. Decker, E. M. 2001. The ability of direct fluorescence-based, two-color assaysto detect different physiological states of oral streptococci. Lett. AppI. Microbiol. 33:188—192.
12. Decker, E. M., R. Weiger, I. Wiech, P. E. Heide, and M. Brecx. 2003.Comparison of antiadhesive and antibacterial effects of antiseptics on Streptococcus sanguinis. Fur. 3. Oral Sci. 111:144—148.
13. Deng, D. M., and 3. M. ten Cate. 2004. Demineralization of dentin byStreptococcus mutans hinfilnis grown in the cnnstant depth film fcrmcntnr.Caries Res. 38:54—61.
14. Emilson, C. G. 1994. Potential etlicacy of chiorhexidine against mutansstreptococci and human dental caries. J. Dent. Res. 73:682—691.
15. Filoche, S. K., M. J. Coleman, L. Angker, and C. H. Sissons. 2007. Alluorcsccnce assay to determine the viable biomass ui microcosm dentalplaque biofilms. 3. Microbiol. Methods 69:489—496.
16. Flemming, H. C., T. R. Neu, and D. J. Wozniak. 2007. The EPS matrix: the“house of biofllm cells.” 3. Bacteriol. 189:7945—7947.
17. Fux, C. A., J. W. Costerton, P. S. Stewart, and P. Stoodley. 2005. Survivalstrategies ol inlectious hiolilnss. Trends Microhiol. 13:34—40.
18. Gieseke, A., and D. Dc Beer. 2004. Use of microelectrodes to measure in situmicrobial activities in biofilms, sediments, and microbial mats, p. 15S1—1612.In G. G. Kowaichuk, F. 3. de Bruijn, I. M. Head, A. D. Akkermans, and 3. D.van Elsas (ed.), Molecular microbial ecology manual, 2nd ed. Springer,Heidelberg, Germany.
19. Hope, C. K., and M. Wilson. 2004. Analysis of the effects of chlorhexidine onoral biofllm vitality and structure based on viability profiling and an indicatorof membrane integrity. Antimicrob. Agents Chemother. 48:1461—1468.
20. Jenkins, S., M. Addy, and W. Wade. 1988. The mechanism of action ofchlorhexidine: a study of plaque growth on enamel inserts in vivo. 3. Clin.Periodontol. 15:415—424.
21. Junge, W., and S. McLaughlin. 1987. The role of fixed and mobile buffers inthe kinetics of proton movement. Biochim. Biophys. Acts 890:1—5.
22. Kolenbrander, P. E., K. 3. Palmer, Jr., A. H. Rickard, N. S. Jakubovics, N. LChalmers, and P. 1. Diaz. 2006. Bacterial interactions and successions duringplaque development. Periodontol. 2000 42:47—79.
23. Kuramitsu, II. K., X. He, K. Lux, M. H. Anderson, and W. Shi. 2007.Interspecies interactions within oral microbial communities. Microbiol. Mol.Biol. Rev. 71:653—670.
24. Lahiri, K., B. Randhawa, and J. Krahenbuhl. 2005. Application of a viability-staining method for Mycobacteriurn leprae derived from the athymic (no/no)mouse foot pad. 3. Med. Microbiol. 54:235—242.
25. Larsen, T., and N. E. Fiehia 1996. Resistance of Streptococcus sanguis biofilms to antimicrobial agents. APMIS 104:280—284.
26. Li, Y., and S. Gregory. 1974. Diffusion of ions in seawater and in deep-seasediments. Geocbim. Cosmochim. Acta 38:703—7 14.
27. Loesehe, W. J. 1969. Oxygen tensitivity of various anaerobic bacteria. AppI.Microbiol. 18:723—727.
28. Marquis, K. E. 1995. Oxygen metabolism, oxidative stress and acid-basephysiology of dental plaque biolilms. 3. md. Microbiol. 15:198—207.
29. Marsh, P. D. 2003. Plaque as a bioflins: pharmacological principles of drugdelivery and action in the sub- and supragingival environment. Oral Dis.9:16-22.
30. Marsh, P. D., and D. J. Bradshaw. 1997. Physiological approaches to thecontrol of oral biofllms. Adv. Dent. Rca. 11:176—185.
31. Nguyen, P. T., 3. Abranehes, T. N. Phan, and K. K. Marquis. 2002. Repressedrespiration of oral streptococci grown in biofilms. Curr. Microbiol. 44:262—266.
32. Pratten, 3., and M. Wilson. 1999. Antimicrobial susceptibility and composition of microcosm dental plaques supplemented with sucrose. Antimicrob.Agents Chemother. 43:1595—1599.
33. Haul, S. A., B. Pitts, H. Beyenal, K. A. Veluchamy, Z. Lewandowski, W. M.Davison, K. Buckingham-Meyer, and P. 5. Stewart. 2007. Spatial pattems ofDNA replication, protein synthesis, and oxygen concentration within bacterial biofilms reveal diverse physiological states. 3. Bscteriol. 189:4223—4233.
34. Renye, J. A., Jr., P. J. Piggot, L Daneo-Moore, and B. A. Buttaro. 2004.Persistence of Streptococcus mutans in stationary-phase batch cultures andbiofllms. AppI. Environ. Microbiol. 70:6181—6187.
35. Revsbech, N. P., and B. B. Jorgensen. 1986. Microelectrodes: their use inmicrobial ecology. Adv. Microb. Ecol. 9:293—352.
36. Reysbech, P. 1989. An oxygen microelectrode with guard cathode. Limnol.Oceanogr. 34:474—478.
37. Schramm, A., L H. Larsen, N. P. Revsbech, N. B. Ramsing, K. Amann, andK.-H. Schleifer. 1996. Structure and functinn nf a nitritying hinfllns as determined by in situ hybridization and the use of microelectrodes. Appl.Environ. Microbiol. 62:4641—4647.
38. Stanley, A., M. Wilson, and H. N. Newman. 1989. The in vitro effects ofchlorhexidine on subgingival plaque bacteria. 3. Din. Periodontol. 16:259—264.
39. Stewart, P. S. 2003. Diffusion in biotllms. I. Bacteriol. 185:1485—1491.40. Stewart, P. S., and M. 3. Franklin. 2008. Physiological heterogeneity in
biofilms. Nat. Rev. Microbiol. 6:199—210.41. Stocks, S. M. 2004. Mechanism and use of the commercially available via
bility stain, BacLight. Cytometry A 61:189—195.42. Stoodley, P., J. Wefel, A. Gieseke, D. Debeer, and C. von Ohle, 2008. Biofiha
plaque snd hydrodynsmic effects on mass transfer, fluoride delivery andcaries. 3. Am. Dent. Assoc. 139:1182—1190.
43. Takahashi, N., and B. Nyvad. 2008. Caries ecology revisited: nsicrobial dynamics and the caries process. Caries Res, 42:409—418.
44. Takenaka, S., H. M. Trivedi, A. Corbin, B. Pitts, and P. 5. Stewart. 2008.Direct visualization of spatial and temporal patterns of antinsicrobial actionwithin model oral biotllms. AppI. Environ. Microbiol, 74:1869—1875.
45. Tomas, 1,, M. C. Cousido, M. Tomas, 3. Limeres, L. Garcia-Caballero, andP. Diz. 2008. In vivo bactericidal effect of 0.2% chlorhexidine but not 0.12%on salivary obligate anaerobes. Arch. Oral Biol. 53:1186-1 191.
46. Traudt, M., and I. Kleinberg, 1996. Stoichiometry of oxygen consumptionand sugar, organic acid and amino acid utilization in salivary sediment andpure cultures of oral bacteria. Arch. Oral Biol. 41:965—978.
47. Trombelli, L., and D. N. Tatakis. 2003. Periodontal diseases: current andfuture indications for local antimicrobial therapy. Oral Dis. 9:11—15.
48. van der Mel, H. C., D. 3. White, 3. Atema-Smit, K. Belt-Gritter, and H. 3.Busscher. 2006. A method to study sustained antimicrobial activity of rinseand dentifrice consponents on biofllm viability in vivo. I. Din. Periodontol.33:14—20.
49. Vitkov, L, A. Hermann, W. D. Krautgartner, M. Herrmann, K. Fuchs, M.Klappacher, and M. Hannig. 2005. Chlorhexidine-induced ultrastructuralalterations in oral biofilm. Microsc. Res. Tech. 68:85—89.
50. von OhIe, C., and M. Brecx. 2007. Early human dental biofllm formation. J.Parodontol. Implantol. Orale 26:213—231.
51. Walters, M. C., III, F. Roe, A. Bugnicourt, M. 3. Franklin, and P. S. Stewart.2003. Contributions of antibiotic penetration, oxygen limitation, and lowmetabolic activity to tolerance of Pseudornonas aeniginosa biotilnts to ciprofluxaein sod tobramycin. Antimierub. Agents Chemuther. 47:317—323.
52. Willems, G., P. Lambrechts, M. Braem, M. Vuylsteke-Wauters, and G.Vanherle. 1991. The surface roughness of enamel-to-enamel contact areascompared with the intrinsic roughness of dental resin composites. 3. Dent.Res. 70:1299—1305.
53. Zaura, K., M. J. Buijs, and J. M. ten Cafe. 2002. The effects of the solubility(if artilicial insures on plsque p11. .1. 1)ent. Res. 81:567—571.
54. Zaura, K., and 3. M. ten Cate. 2004. Dental plaque as a biofllm: a pilot studyof the effects of nutrients on plaque pH and dentin demineralization. CariesRes. 38:9—15.
55. Zaura-Arite, K., J. van Marie, and 3. let, ten Cate. 2001. Conofocal microscopy study of undisturbed and chlurhexidine.treated dental biuffim. J. Dent.Res. 80:1436-1440.